Introduction
The use of forceps in infant delivery has declined significantly in the United States over the past 3 decades. In 2023, forceps deliveries accounted for approximately 0.98% of vaginal births, while vacuum extraction comprised about 0.68% of all deliveries.[1] This downward trend is attributed to multiple factors, including fear of litigation, limited training opportunities, and the increasing complexity of pregnancies.
Despite these challenges, operative vaginal delivery with forceps remains a valuable skill. When applied correctly during the second stage of labor arrest, forceps can reduce the need for cesarean delivery, which carries higher risks of complications, eg, infection, hemorrhage, and uterine rupture (see Image. Forceps Delivery).[2] Additionally, a meta-analysis indicated that a previous cesarean delivery increases the risk of spontaneous preterm birth in subsequent pregnancies, whereas operative vaginal delivery does not.[3]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Knowing the anatomy of the female pelvis is essential for performing a forceps delivery, as visibility is limited once the instrument is in place. Successful delivery depends largely on individual maternal pelvic dimensions in addition to clinical findings of the fetus on pelvic exam (eg, cranial molding and fetal descent). One of the requirements for performing a delivery with forceps is ruling out cephalopelvic disproportion; this requires knowledge of pelvimetry, which is divided into 4 major types of pelvic categories:
- Anthropoid
- Android
- Gynecoid
- Platypelloid
The gynecoid pelvis, with its round inlet and spacious dimensions, is most favorable for vaginal delivery. Android and platypelloid pelvises can make vaginal birth more challenging, and the anthropoid pelvis, while elongated front to back, may also pose difficulties. Previously, in certain instances, x-ray pelvimetry was used to determine the type of pelvis. However, due to radiation concerns x-ray pelvimetry is now rarely used. Instead, clinicians currently rely on a combination of clinical assessment and ultrasound to evaluate pelvic adequacy. Furthermore, the obstetrical conjugate was historically used to assess pelvic adequacy; however, routine measurement of the obstetrical conjugate is seldom performed today.[4][5][4] Due to limited training in clinical cephalopelvimetry, this obstetric assessment is less frequently relied on in current practice. Additionally, a 2024 study found that the obstetric conjugate diameter has remained unchanged since the mid-20th century, indicating that routine pelvimetry is uncommon in modern clinical practice.[4]
Knowledge of fetal anatomy plays an essential role in determining fetal station and position. The fetal station is determined by palpating the fetal head and using the bipyramidal distance as a landmark to assess fetal position in reference to the ischial spines. The ischial spines identify zero station, and a fetal head palpated above the ischial spines is subsequently considered a "negative" position. Conversely, a fetal head below the ischial spines is considered a positive station. Furthermore, the birth canal can be divided into thirds above and below the ischial spines, resulting in a numerical system with values ranging from -3 to +3. Another numbering system involves using centimeters to measure fetal station with values ranging from -5 to +5.[6] Assessing fetal station is crucial for clinicians to evaluate labor progress and inform decisions regarding delivery.
Additionally, fetal position should be assessed at the same time as station, as both influence the approach to delivery. The most favorable position is occiput anterior, where the back of the baby’s head is directed toward the front of the maternal pelvis. On clinical pelvic exam, fetal position is confirmed by palpating the posterior fontanelle in the midline. Clinical assessment alone, however, is not always a reliable method. Recent studies show that intrapartum ultrasound is more accurate than vaginal examination for detecting malpositions, and combining both techniques provides the most accurate assessment. When the fetus is not in the occiput anterior position, eg, occiput posterior or transverse positions, operative vaginal delivery can be more challenging, often requiring rotation of the head before safe use of forceps or vacuum.[7]
Indications
Operative vaginal delivery, comprising both forceps and vacuum extraction, is sometimes indicated when certain maternal or fetal conditions arise, though in no single situation is an operative vaginal delivery an absolute requirement. Fetal indications for forceps or vacuum vaginal delivery often involve a nonreassuring heart rate pattern when the fetal head is already low in the birth canal, particularly when a cesarean delivery might not be easily accessible or considered higher risk. Maternal indications for operative vaginal delivery include maternal exhaustion or a prolonged second stage of labor, for which forceps and vacuum intervention may be helpful. Maternal medical conditions, eg, cardiac or neurologic disease that make maternal pushing efforts during delivery unsafe or ineffective, are also indications for operative vaginal delivery. According to the American College of Obstetricians and Gynecologists (ACOG), a prolonged second stage is defined as 3 or more hours for a first-time vaginal delivery with regional anesthesia or 2 hours or more of maternal pushing effort without regional anesthesia. In multiparous individuals, a prolonged second stage of labor is defined as maternal pushing effort without regional anesthesia for 2 or more hours or 1 hour or more, with and without regional anesthesia, respectively.[8][5]
Professional societies, including the Royal College of Obstetricians and Gynaecologists (RCOG) and ACOG, have recommended that the following criteria be met before proceeding with either vacuum or forceps delivery:
- The cervix is fully dilated.
- Membranes are ruptured.
- Fetal head engaged (vertex presentation) with a station at the level of the ischial spines or below, and fetal caput and molding are moderate or less.
- The fetal head position is known.
- Fetal weight has been estimated with abdominal palpation and review of any available recent ultrasound imaging.
- The maternal pelvis is considered adequate for vaginal delivery.
- Appropriate anesthesia has been administered.
- The maternal bladder is empty, and the indwelling catheter has been removed or the balloon deflated if previously placed.
- Maternal consent obtained, risks and benefits thoroughly explained.
- A backup plan is in place if the operative delivery method fails.
- Access to an operating room, adequate facilities, and appropriately trained staff are present.[8][2]
Contraindications
Absolute Contraindications
Absolute maternal contraindications for operative vaginal delivery include the following:
- Cervix not fully dilated: Attempting an operative vaginal delivery before full dilation can lead to cervical lacerations and other complications.
- Membranes intact: Intact membranes can hinder the application of forceps or vacuum and increase the risk of infection.
- Fetal head not engaged: If the fetal head has not descended into the pelvis, a risk of head entrapment or uterine rupture is present.
- Unknown fetal position
- Cephalopelvic disproportion
Absolute fetal contraindications include the presence of a bleeding disorder (eg, hemophilia, thrombocytopenia, von Willebrand disease) or bone demineralization (osteogenesis imperfecta).[2]
Relative Contraindications
Relative maternal contraindications for which operative vaginal delivery may need to be avoided include malpresentation (unless planned breech extraction) and connective tissue disorders, as these factors can increase the risk of maternal and fetal injury. Similarly, relative fetal contraindications include prematurity (underdeveloped skulls increasing the risk of injury) and macrosomia. No consensus has been established on the minimum or maximum estimated fetal weight for forceps delivery.[8]
Equipment
Although forceps are less frequently used in current practice, obstetric clinicians should have knowledge of the different types of forceps as well as how to employ them safely and effectively during an operative vaginal delivery when indicated.[8] All forceps have 4 main components: the handle, lock, shank, and blade. The blade has 2 curves consisting of the cephalic curve, which matches the shape of the baby’s head, and the pelvic curve, which fits the mother’s pelvis. Various types of forceps in different shapes and designs have been developed, each suited for use during an assisted vaginal birth in specific situations during delivery.
For instance, the blades can be either fenestrated or smooth. Fenestrated forceps, like the Simpson and Elliot, have crossed branches. Additionally, the Simpson forceps have parallel shanks that work best with a long, molded fetal head, while the Elliot forceps have overlapping shanks that are used when the fetal head is unmolded. On the other hand, the Tucker McLane forceps have a smooth blade without fenestrations, making this type ideal for babies with a round head.
Most traditional forceps, eg, Simpson, Elliot, and Tucker McLane, have an English lock, which only allows for partial rotation. Keilland forceps, in contrast, have a sliding lock and minimal pelvic curve, allowing them to rotate and disengage when needed. Rotational forceps (eg, Keilland) are very useful for some complex deliveries; however, they carry a higher risk of complications, including maternal issues like vaginal lacerations and bleeding, and fetal injuries (eg, scalp lacerations or shoulder dystocia). For breech deliveries, Piper forceps are usually preferred for the aftercoming head. Their longer shank and pelvic curve provide some protection for the fetal head while flexed during delivery.[8]
Personnel
A successful operative vaginal delivery demands the expertise of a well-trained and experienced obstetric clinician. Mastery of this procedure often requires participation in hundreds of forceps deliveries to develop the skill necessary to prevent or manage potential maternal and fetal complications effectively. Moreover, the presence of a pediatrician and neonatologist during the delivery ensures immediate evaluation and management of newborns requiring resuscitation, promoting optimal neonatal outcomes. Additionally, personnel should be prepared for potential complications (eg, shoulder dystocia) and trained in the performance of neonatal resuscitation when needed.[2]
Preparation
The initial step in preparing for a forceps delivery involves comprehensive patient counseling and obtaining informed consent. The discussion must include an explanation of the risks and benefits of forceps use, along with alternative options, eg, vacuum-assisted delivery or cesarean section. Consent for a possible cesarean delivery should be obtained simultaneously in case the forceps attempt does not result in a successful outcome. The operating room team must be alerted and prepared, particularly when a nonreassuring fetal heart rate tracing is present.
All necessary equipment should be inspected before the procedure. The selected forceps must be available and in proper working condition, with a backup instrument ready if needed. Vacuum extraction following a failed forceps attempt should be avoided because of an increased risk of fetal complications.[9] Because maternal perineal and vaginal lacerations occur frequently with forceps deliveries, instruments and sutures for laceration repair must be arranged on the operative table.
Additionally, collaboration with anesthesia and pediatric teams plays an essential role in optimizing safety and readiness. Regional anesthesia, eg, an epidural or pudendal block, is generally required, while local perineal anesthesia is often administered when a right mediolateral episiotomy is planned to increase space and minimize laceration severity. For complex deliveries, preparation for cord blood gas analysis is recommended.[10]
Before forceps application, the maternal bladder should be emptied to facilitate fetal head descent and to prevent obstruction in the event that an emergency cesarean delivery becomes necessary. Routine prophylactic antibiotic use is not advised for uncomplicated forceps deliveries, as current evidence demonstrates no significant reduction in maternal infection rates or hospital length of stay. Antibiotics may be warranted, however, when significant perineal trauma or other infection risk factors are present.[11]
Technique or Treatment
Forceps Delivery Classification
Deliveries assisted by forceps are classified based on various factors, including the amount of rotation required and the station of the fetal head at the time the forceps are applied. This classification can indicate the degree of risk, as studies have demonstrated that the risk of maternal-fetal injury associated with forceps deliveries decreases the lower the station of the fetal head is.[12] The following criteria are used to categorize the types of forceps delivery:
- Outlet forceps
- Scalp at introitus without separating labia
- Skull at the pelvic floor
- Sagittal suture in anterior-posterior diameter or right occiput anterior, left occiput anterior, or occiput anterior position
- Fetal head on the perineum
- Rotation less than 45 degrees [13]
- Low forceps
- Skull greater than +2 station
- Without rotation: Rotation less than 45 degrees (ie, rotating from right or left occiput anterior to occiput anterior, or from right or left occiput posterior to occiput posterior)
- With rotation: Rotation greater than 45 degrees
- Mid forceps: Fetal head is above +2 station, but engaged [13]
- High forceps: Above +2 station; however, the fetal head is not engaged. High forceps is rarely performed in the United States due to higher complication rates. Proceeding with a cesarean delivery instead is recommended in these cases.[12]
Forceps Application
Specific application techniques for forceps vary depending on the type of forceps used. Generally, however, during application, the sagittal suture should remain equidistant between the forceps branches, and the posterior fontanelle should lie approximately 1 fingerbreadth above the shanks. The tips of the blades must rest over the fetal cheeks, and the fenestrated blades should allow 1 finger between the heel of the blade and the fetal head. The delivering clinicians should ensure that maternal tissue is not caught within the forceps.
The primary function of forceps involves applying traction with minimal compression during contractions while guiding the narrowest fetal head diameter—the suboccipitobregmatic—through the birth canal, thereby facilitating the probability of a successful vaginal delivery. Any required rotation should occur between contractions. The obstetrician applies the forceps from beneath the fetal head while in a seated position. Traction originates from the forearms rather than the chest, following the pelvic curve, as described by the Saxtorph-Pajot maneuver. Steady, controlled traction without rocking motion ensures safe progress. The direction of traction must follow the natural pelvic curve, mimicking the physiological movement that occurs during an unassisted birth.[2]
An early right mediolateral episiotomy is often performed to create additional space and reduce the risk of rectal or vaginal injury. However, routine episiotomy is unnecessary but may be performed when additional space is needed or when laceration risk increases, with a right mediolateral incision preferred. Once the biparietal diameter passes the vulvar ring, the forceps are removed in reverse order. Most deliveries progress with 1 or 2 pulls, with completion occurring by the third or fourth pull. Current guidance focuses less on the number of pulls and emphasizes gentle, controlled traction, with the procedure discontinued if progress fails to occur.[14]
Complications
Accurately determining complication rates associated with forceps deliveries remains challenging because most studies lack adequate control groups. Despite this limitation, consistent trends in maternal and neonatal complications have been documented across available research.
Maternal complications with the use of forceps-assisted deliveries include a higher incidence of perineal and vaginal lacerations, hematomas, and anal sphincter injuries compared with vacuum deliveries.[15] Furthermore, long-term maternal complications, including pelvic organ prolapse and pelvic floor dysfunction, occur more frequently in cases involving severe perineal trauma. Women with a history of forceps delivery face an increased risk of levator ani muscle injury, anal sphincter damage, and other forms of pelvic floor dysfunction years after childbirth.[16][17]
For neonates, most complications following forceps delivery tend to be mild and temporary, eg, facial bruising, superficial lacerations, or facial nerve palsy. More serious outcomes, including ocular trauma, skull fractures, intracranial hemorrhage, and subgaleal hematomas, occur infrequently but may arise during difficult or rotational deliveries. A recent systematic review of Kielland rotational forceps demonstrated that rotational techniques resulted in fewer overall birth injuries than nonrotational forceps or second-stage cesarean deliveries, although shoulder dystocia occurred more frequently in these cases.[18]
Clinical Significance
Forceps allow for an alternative to vacuum-assisted delivery or cesarean section, particularly with a nonreassuring tracing when delivery is imminent, maternal exhaustion from pushing, or medical comorbidities that preclude pushing or operative delivery. Advantages of forceps as compared to vacuum-assisted deliveries include:
- Forceps are unlikely to detach from the fetal head.
- Forceps can be used in premature fetuses.
- Forceps allow for rotation.
- Less bleeding from the scalp is typically noted with forceps.
- Fewer cases of encephalopathy are associated with the use of forceps.
Therefore, in general, vacuum extraction is safer for the mother than forceps, while forceps is safer for the fetus than vacuum extraction. Forceps and vacuum-assisted deliveries both serve as valuable alternatives to cesarean section when appropriately selected and performed by skilled clinicians. Forceps delivery generally achieves a higher success rate for vaginal birth but carries a greater risk of severe perineal trauma, including third- or fourth-degree tears and subsequent urinary incontinence. Neonatal risks with forceps include facial lacerations, nerve palsy, corneal abrasions, and, rarely, skull fractures. In contrast, vacuum extraction presents a slightly lower success rate but reduces the likelihood of severe maternal lacerations. However, infants delivered by vacuum face higher risks of scalp lacerations, cephalohematoma, and hyperbilirubinemia. According to ACOG, both techniques share similar rates of severe fetal injury or death and should be chosen based on the specific clinical context. Forceps may be more suitable for cases requiring rotation of the fetal head, while vacuum extraction may offer advantages in others. Ultimately, clinician expertise and patient-informed consent remain central to optimizing safety and avoiding unnecessary cesarean deliveries.
Enhancing Healthcare Team Outcomes
Forceps-assisted delivery, though declining in the United States, remains a critical obstetric skill that provides a safe alternative to cesarean delivery when maternal or fetal conditions necessitate operative intervention. Proper use requires a thorough understanding of maternal pelvic anatomy, fetal position, and station, as well as the ability to identify absolute and relative contraindications. Mastery of evidence-based techniques minimizes maternal trauma, reduces neonatal injury, and optimizes labor outcomes. Clinicians must balance procedural proficiency with careful patient assessment to ensure safety and effectiveness during the second stage of labor.
Effective patient-centered care in operative vaginal delivery relies on coordinated skills and communication among the interprofessional team. Physicians and advanced practitioners lead assessment and procedural execution, while nurses monitor maternal and fetal status and provide essential support during labor. Neonatal clinicians are critical when neonatal resuscitation is required. Pharmacists ensure the appropriate administration of analgesia and manage medications, while general practitioners may assist in follow-up care. Clear communication and collaborative decision-making enhance patient safety, reduce complications, and improve team performance, ensuring optimal maternal and neonatal outcomes.[19]
Media
(Click Image to Enlarge)
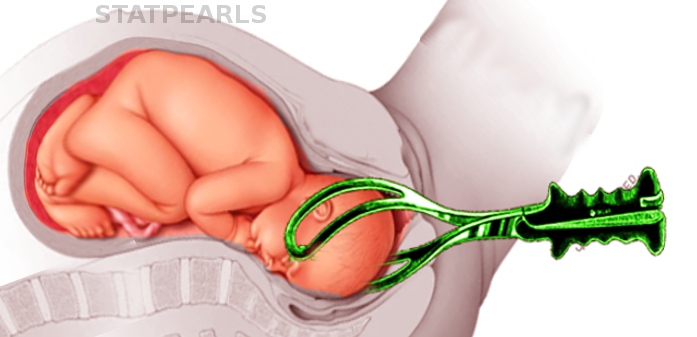
Forceps Delivery. This image demonstrates the application of forceps during a vaginal delivery.
Contributed by S Bhimji, MD
References
Hayati K, Ritonga MA, Djuwantono T. Trends in vacuum and forceps delivery in teaching hospitals and academic health systems in West Java, Indonesia: A retrospective study. SAGE open medicine. 2024:12():20503121241239813. doi: 10.1177/20503121241239813. Epub 2024 Mar 28 [PubMed PMID: 38558771]
Level 2 (mid-level) evidenceBahl R, Hotton E, Crofts J, Draycott T. Assisted vaginal birth in 21st century: current practice and new innovations. American journal of obstetrics and gynecology. 2024 Mar:230(3S):S917-S931. doi: 10.1016/j.ajog.2022.12.305. Epub 2023 Jul 28 [PubMed PMID: 38462263]
Kirubarajan A, Thangavelu N, Rottenstreich M, Muraca GM. Operative delivery in the second stage of labor and preterm birth in a subsequent pregnancy: a systematic review and meta-analysis. American journal of obstetrics and gynecology. 2024 Mar:230(3):295-307.e2. doi: 10.1016/j.ajog.2023.08.033. Epub 2023 Sep 4 [PubMed PMID: 37673234]
Level 1 (high-level) evidenceTresch C, Lallemant M, Nallet C, Offringa Y, Ramanah R, Guerby P, Mottet N. Updating of pelvimetry standards in modern obstetrics. Scientific reports. 2024 Feb 6:14(1):3080. doi: 10.1038/s41598-024-53603-1. Epub 2024 Feb 6 [PubMed PMID: 38321054]
Cohen WR, Friedman EA. The second stage of labor. American journal of obstetrics and gynecology. 2024 Mar:230(3S):S865-S875. doi: 10.1016/j.ajog.2022.06.014. Epub 2023 Jul 24 [PubMed PMID: 38462260]
Carollo TC, Reuter JM, Galan HL, Jones RO. Defining fetal station. American journal of obstetrics and gynecology. 2004 Nov:191(5):1793-6 [PubMed PMID: 15547566]
Ghi T, Dall'Asta A. Sonographic evaluation of the fetal head position and attitude during labor. American journal of obstetrics and gynecology. 2024 Mar:230(3S):S890-S900. doi: 10.1016/j.ajog.2022.06.003. Epub 2023 May 19 [PubMed PMID: 37278991]
. Operative Vaginal Birth: ACOG Practice Bulletin, Number 219. Obstetrics and gynecology. 2020 Apr:135(4):e149-e159. doi: 10.1097/AOG.0000000000003764. Epub [PubMed PMID: 32217976]
Gardella C, Taylor M, Benedetti T, Hitti J, Critchlow C. The effect of sequential use of vacuum and forceps for assisted vaginal delivery on neonatal and maternal outcomes. American journal of obstetrics and gynecology. 2001 Oct:185(4):896-902 [PubMed PMID: 11641674]
Level 2 (mid-level) evidence. Operative Vaginal Birth: ACOG Practice Bulletin Summary, Number 219. Obstetrics and gynecology. 2020 Apr:135(4):982-984. doi: 10.1097/AOG.0000000000003765. Epub [PubMed PMID: 32217970]
Liabsuetrakul T, Choobun T, Peeyananjarassri K, Islam QM. Antibiotic prophylaxis for operative vaginal delivery. The Cochrane database of systematic reviews. 2017 Aug 5:8(8):CD004455. doi: 10.1002/14651858.CD004455.pub4. Epub 2017 Aug 5 [PubMed PMID: 28779515]
Level 1 (high-level) evidence. ACOG Practice Bulletin No. 154: Operative Vaginal Delivery. Obstetrics and gynecology. 2015 Nov:126(5):e56-e65. doi: 10.1097/AOG.0000000000001147. Epub [PubMed PMID: 26488523]
Patient Safety and Quality Committee, Society for Maternal-Fetal Medicine. Electronic address: smfm@smfm.org, Staat B, Combs CA. SMFM Special Statement: Operative vaginal delivery: checklists for performance and documentation. American journal of obstetrics and gynecology. 2020 May:222(5):B15-B21. doi: 10.1016/j.ajog.2020.02.011. Epub [PubMed PMID: 32354409]
Level 2 (mid-level) evidenceAlves ÁLL, Silva LBD, Filho BJA, Nunes RD. Operative vaginal delivery. Revista brasileira de ginecologia e obstetricia : revista da Federacao Brasileira das Sociedades de Ginecologia e Obstetricia. 2023 Jul:45(7):422-434. doi: 10.1055/s-0043-1772581. Epub 2023 Aug 18 [PubMed PMID: 37595600]
Muraca GM, Boutin A, Razaz N, Lisonkova S, John S, Ting JY, Scott H, Kramer MS, Joseph KS. Maternal and neonatal trauma following operative vaginal delivery. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2022 Jan 10:194(1):E1-E12. doi: 10.1503/cmaj.210841. Epub [PubMed PMID: 35012946]
Dvorak J, Poncova R, Fucik T, Dietz HP, Masata J, Martan A, Svabik K. Impact of the type of vaginal assisted delivery on the pelvic floor and OASI - Ultrasound study. European journal of obstetrics, gynecology, and reproductive biology. 2025 Feb:305():142-146. doi: 10.1016/j.ejogrb.2024.12.023. Epub 2024 Dec 16 [PubMed PMID: 39701008]
Hagen S, Sellers C, Elders A, Glazener C, MacArthur C, Toozs-Hobson P, Hemming C, Herbison P, Wilson D. Urinary incontinence, faecal incontinence and pelvic organ prolapse symptoms 20-26 years after childbirth: A longitudinal cohort study. BJOG : an international journal of obstetrics and gynaecology. 2024 Dec:131(13):1815-1823. doi: 10.1111/1471-0528.17913. Epub 2024 Jul 30 [PubMed PMID: 39079703]
Giacchino T, Karkia R, Ahmed H, Akolekar R. Maternal and neonatal complications following Kielland's rotational forceps delivery: A systematic review and meta-analysis. BJOG : an international journal of obstetrics and gynaecology. 2023 Jul:130(8):856-864. doi: 10.1111/1471-0528.17402. Epub 2023 Feb 13 [PubMed PMID: 36694989]
Level 1 (high-level) evidenceBrogaard L, Rosvig L, Hjorth-Hansen KR, Hvidman L, Hinshaw K, Kierkegaard O, Uldbjerg N, Manser T. Team performance during vacuum-assisted vaginal delivery: video review of obstetric multidisciplinary teams. Frontiers in medicine. 2024:11():1330457. doi: 10.3389/fmed.2024.1330457. Epub 2024 Mar 20 [PubMed PMID: 38572162]