 Anatomy, Abdomen and Pelvis: Deep Perineal Space
Anatomy, Abdomen and Pelvis: Deep Perineal Space
Introduction
The perineum is the region situated inferior to the pelvic diaphragm, which comprises the levator ani and coccygeus muscles, and is bounded by the pelvic outlet or inferior pelvic aperture. The perineum approximates a diamond-shaped area formed anterolaterally by the ischiopubic rami and posterolaterally by the sacrotuberous ligaments.
An imaginary line joining the ischial tuberosities separates the perineum into anterior urogenital and posterior anal triangles. The perineal body lies centrally along this line, serving as the point of convergence between both triangles.
A dense fascial layer, the perineal membrane—historically referred to as the "inferior fascia of the urogenital diaphragm"—further subdivides the urogenital triangle into the superficial and deep perineal spaces. The superficial perineal space is positioned inferior to the perineal membrane, while the deep perineal space lies superior to this structure.
The deep perineal space (pouch) is bounded inferiorly by the perineal membrane, superiorly by the inferior fascia of the pelvic diaphragm, and laterally by the inferior portion of the obturator fascia, which overlies the obturator internus muscle. In both sexes, this space contains the urethra, the muscles of the external urethral sphincter complex, and the neurovascular structures supplying the external genitalia. In male individuals, the deep perineal space also contains the bulbourethral glands (see Image. Male Pelvic Floor Anatomy). In female individuals, this region includes the vagina (see Image. Female Perineum).
Clinically, the deep perineal space serves as a key landmark for urethral and pelvic floor surgery. Familiarity with the muscular and fascial architecture of this region allows clinicians to anticipate the course of neurovascular structures and localize sites of fluid extravasation or trauma. A deep understanding of the anatomy of the deep perineal space helps clinicians prevent complications and refine operative techniques.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The perineal membrane forms the inferior boundary of the deep perineal space. This structure is a dense fibrous sheath extending from the pubis to the ischial tuberosities. The membrane's triangular configuration accounts for the historical designation triangular ligament.[1]
In the female body, the anterior portion of the perineal membrane continues with the pubourethral ligament. In the male body, the membrane thickens to form the transverse ligament of the perineum.[2] The interval between the transverse ligament and the pubic symphysis accommodates the deep dorsal vein of the penis. Posteriorly, the membrane blends with the perineal body.
Openings within the membrane include a central aperture for the urethra and, in female individuals, a posterior opening for the vagina. The region inferior to the perineal membrane constitutes the superficial perineal space, whereas the region superior to it corresponds to the deep perineal space.
Laterally, the deep perineal space is bounded by the fascia of the obturator internus muscle. A fold of this fascia forms the pudendal canal (of Alcock), which encloses the dorsal nerve and artery of the penis or clitoris as these structures course anterolaterally through the space.[3]
Muscles of the external urethral sphincter complex attach to the superior surface of the perineal membrane and occupy the interval between the pudendal canals.[4] The inferior surface provides attachment to the muscles and erectile bodies of the superficial perineal space. No distinct superior fascial layer encloses the muscles of the deep perineal space. The superior boundary is instead represented by the inferior fascia of the pelvic floor, which communicates openly with the pelvis through the urogenital hiatus.[5]
Therefore, the deep perineal space does not constitute a closed compartment. This characteristic contrasts with the superficial perineal space, which possesses well-defined fascial boundaries—an important distinction in understanding patterns of fluid extravasation.
The deep perineal space, though sexually dimorphic in its contents, performs shared functional roles in both sexes, which include the maintenance of voluntary urinary continence and the provision of structural support to the perineum. The structures within this compartment are arranged in close association with the perineal membrane and contribute significantly to the integrity of the pelvic floor.
In male individuals, the deep perineal space contains the sphincter urethrae muscle, deep transverse perineal muscles, the membranous urethra, the anterior recesses of the ischioanal fossa, and the neurovascular structures of the penis. The bulbourethral (Cowper) glands, paired exocrine glands embedded within the base of the sphincter urethrae on either side of the membranous urethra, are also situated in this space. The ducts of the bulbourethral glands traverse the perineal membrane and open into the bulbar urethra, secreting clear mucus during sexual arousal. These glands are homologous to the Bartholin glands in female individuals.
In the female body, the deep perineal space contains the sphincter urethrae, compressor urethrae, and sphincter urethrovaginalis muscles, as well as smooth muscle fibers continuous with the pelvic floor. The proximal urethra, vagina, anterior recesses of the ischioanal fossa, and neurovascular structures of the clitoris are also contained within this space. The vagina lies posterior to the urethra and traverses the perineal membrane at the level of the hymenal ring, where it is anchored to the bony pelvis and supported by the surrounding musculature.
Embryology
Development of the perineum begins during the 4th to 6th weeks of gestation, when the cloaca divides into the primary urogenital sinus and the rectum.[6] A mesenchymal ridge, the urorectal septum, forms between these 2 structures and subsequently expands to give rise to the perineal body. The muscles and fascial layers of the perineum develop from this central condensation. Owing to this origin, the perineal body serves as the common attachment site for multiple perineal structures and is frequently termed the central tendon of the perineum.[7] In male embryos, the prostatic and membranous urethra, along with the bulbourethral glands, derive from the inferior portion of the urogenital sinus. In female embryos, the entire urethra develops from the urogenital sinus.
The striated urethral sphincter originates from a mesenchymal primordium identifiable by the 10th week of gestation. This primordium forms a horseshoe-shaped structure encircling the urethra from the perineal membrane to the vesicourethral junction.[8] Sexual differentiation subsequently modifies this structure throughout fetal development and continues into adolescence.
In male fetuses, the prostate develops as a diverticulum of the urethra, leading to progressive thinning and atrophy of the surrounding striated muscle. The muscular layer enlarges and exceeds the thickness of the urethral wall inferior to the prostate. No fascial layer separates these 2 components, a key distinction from the inaccurate historical description of the urogenital diaphragm.
In female fetuses, a portion of the sphincteric muscle extends around the lateral vaginal wall, forming 2 discrete elements: a sphincter of the urethra and a sphincter of the urogenital sinus, designated the compressor urethrae and sphincter urethrovaginalis, respectively. By term, the infraprostatic portion in male fetuses and the proximal urethral portion in female fetuses completely encircle the urethra, forming the sphincter urethrae. These muscles consist entirely of type I, slow-twitch muscle fibers.[9]
Blood Supply and Lymphatics
The perineum receives its principal vascular supply from the internal pudendal artery, a branch of the internal iliac artery. The internal pudendal artery exits the pelvis through the greater sciatic foramen, passes posterior to the sacrospinous ligament, and reenters the perineum via the lesser sciatic foramen.
Within the perineum, the artery traverses the pudendal canal (of Alcock) and gives rise to the inferior rectal artery before bifurcating near the distal end of the canal. Major branches of the internal pudendal artery include the perineal artery, the common penile artery in the male body, and the common clitoral artery in the female body.
Terminal branches of the perineal artery penetrate the Colles fascia, supplying the superficial perineal space and portions of the external genitalia. The common dorsal artery continues within the pudendal canal, superior to the perineal membrane, and terminates in 3 branches that supply the erectile bodies. In the male body, these branches comprise the bulbourethral artery, cavernosal artery, and dorsal artery of the penis. In the female body, the corresponding terminal branch is the deep artery of the clitoris.
Substantial anatomical variation exists in the branching patterns, course, and anastomotic connections of these vessels.[10] Accessory pudendal arteries have been identified in up to 70% of cases.[11] Transection of accessory pudendal arteries during prostatectomy has been associated with postoperative erectile dysfunction.[12] Venous drainage of the deep perineal space occurs primarily through the internal pudendal veins, which communicate with the dorsal vein and dorsal vein complex after perforating the levator ani.[13]
Lymphatic drainage of the perineum follows the venous tributaries of the internal iliac system, reaching the internal iliac lymph nodes either directly or indirectly through the sacral lymph nodes. Additional channels may communicate with the external iliac and inguinal lymph nodes. From the iliac nodal groups, lymphatic flow proceeds to the lumbar lymph nodes, which unite to form the paired lumbar lymphatic trunks that converge at the cisterna chyli.
Nerves
Innervation of the perineum is primarily provided by the pudendal nerve, originating from the anterior rami of the S2 to S4 spinal nerves.[14] The pudendal nerve accompanies the internal pudendal artery, exiting the pelvis through the greater sciatic foramen, passing posterior to the sacrospinous ligament, and entering the perineum via the lesser sciatic foramen.
Within the perineum, the nerve traverses the pudendal canal, where it gives rise to the inferior rectal nerve before bifurcating near the distal end of the canal. Major branches include the perineal nerve and the dorsal nerve of the penis in the male body or the dorsal nerve of the clitoris in the female body. The dorsal nerve represents the direct continuation of the pudendal trunk and courses anteriorly through the deep perineal space alongside the common dorsal artery. The perineal nerve follows the perineal artery, descending below the perineal membrane to supply the superficial perineal space and portions of the external genitalia.
The urethral sphincter complex exhibits dual somatic innervation, receiving fibers from both the pudendal nerve and direct branches of the sacral plexus. The latter descend along the surface of the levator ani to reach the sphincteric musculature.[15]
Muscles
The muscular architecture of the deep perineal space demonstrates greater complexity in the female body than in the male. In the male body, these muscles are collectively referred to as the "external urethral sphincter." In the female body, the presence of the vagina necessitates the use of the broader and anatomically precise term "urogenital sphincter."
The urogenital sphincter in female individuals comprises 3 distinct components: the sphincter urethrae, the compressor urethrae, and the sphincter urethrovaginalis. In both sexes, the muscular fibers of these structures are oriented vertically, perpendicular to the perineal membrane, rather than arranged in a plane parallel to this membrane.
This distinction corrects a long-standing misconception based on the outdated concept of the “urogenital diaphragm.” Although contemporary anatomical studies have refuted the existence of a discrete urogenital diaphragm, the term persists in medical literature and illustrations, leading to continued misrepresentation of pelvic anatomy.[16] Cadaveric dissections and 3-dimensional computed tomography reconstructions demonstrate that the urethral sphincter muscles extend beyond the deep perineal space, incorporating the prostatic isthmus and the bladder base within their configuration.[17][18]
Modern anatomic understanding recognizes that the deep perineal space contains several muscles essential to continence and pelvic support. The composition and arrangement of these structures differ between male and female anatomy.
In the male body, the muscles of the deep perineal space include the sphincter urethrae and the deep transverse perineal muscles. The sphincter urethrae, or external urethral sphincter, serves as the principal muscle responsible for voluntary urinary continence. The muscle forms a vertically oriented structure extending from the perineal membrane to the base of the bladder. Only the inferior segment of this muscle encircles the urethra, thereby forming a true sphincter. The sphincter urethrae is composed of striated muscle fibers and receives dual somatic innervation from the pudendal nerve and branches of the sacral plexus. This muscle differs from the internal urethral sphincter (sphincter vesicae), which consists of smooth muscle and functions under autonomic control via the vesical plexus.
The deep transverse perineal muscles, or deep transverse perinei, form a paired structure arising from the medial surfaces of the ischial tuberosities. Each muscle extends medially to attach to the perineal body, contributing to the stabilization of the perineal region. Considerable variation has been reported in the morphology and development of these muscles, and their precise anatomy remains a topic of ongoing discussion in the literature.[19]
In the female body, the deep perineal space contains several components collectively referred to as the "urogenital sphincter". The most proximal element is the sphincter urethrae, which originates at the base of the bladder and encircles the middle 3rd of the urethra. Distally, this muscle continues as the compressor urethrae, forming a broad arch across the anterior aspect of the urethra and inserting bilaterally into the ischiopubic rami through small tendinous attachments.
The sphincter urethrovaginalis encircles both the distal urethra and the vagina without interposing between them. This muscle anchors to the perineal body and functions as a sphincter for both the urethral and vaginal orifices, contributing to pelvic floor support and continence. In place of the deep transverse perineal muscles, which are often less developed or absent in female individuals, smooth muscle fibers of variable thickness and morphology are present, providing additional reinforcement to the perineal region.
Surgical Considerations
Effective surgical management of the perineum requires a precise understanding of its regional anatomy. In pelvic trauma, detailed knowledge of fascial planes is critical for distinguishing patterns of fluid extravasation. In anterior urethral injuries, the Buck fascia confines extravasation to the superficial perineal space. In cases of penile fracture, this injury pattern produces ecchymosis of the penile shaft, commonly referred to as the "aubergine sign."[20] Fluid extends into the dartos fascia when the Buck fascia is disrupted, resulting in scrotal and suprapubic ecchymosis, known as the butterfly sign.[21] In posterior urethral injuries, the perineal membrane limits extravasation, directing the spread of fluid into the pelvis instead.[22]
A thorough understanding of perineal neurovascular anatomy, including common variations, is equally essential for avoiding complications during pelvic and urogenital surgery. During procedures such as radical prostatectomy, inadvertent injury to these structures may result in incontinence, urethral stenosis, or rectourethral fistula. Similar care is warranted during urethral dilation to ensure preservation of the sphincter urethrae.
Clinical Significance
The perineal membrane has traditionally served as the anatomical landmark dividing the urethra into 2 clinically distinct segments: anterior and posterior. This distinction has been instrumental in describing and classifying urethral pathology, particularly in explaining characteristic patterns of extravasation. The same classification applies to urethral stricture disease, which by definition involves only the anterior urethra.[23] Lesions of the posterior urethra are instead termed "urethral stenoses" and are recognized to have distinct etiologies.[24]
Following the World Health Organization Consensus Conference in 2002, the anterior-posterior terminology was replaced by a 6-segment model of the urethra. These segments include the fossa navicularis, penile urethra, bulbous urethra, membranous urethra, prostatic urethra, and bladder neck.[25] Of these segments, only the membranous urethra lies within the deep perineal space.
Other Issues
The deep perineal space has traditionally been described as a triangular, trilaminar structure composed of a muscular layer enclosed between 2 fascial planes. Since its initial description in 1873, this composite structure has been collectively referred to as the "urogenital diaphragm" and has often been used synonymously with the deep perineal space.
Contemporary anatomical and imaging studies have since demonstrated that this terminology is inaccurate. The concept of a discrete urogenital diaphragm has been disproven through 3-dimensional computed tomography reconstructions and cadaveric dissections, which show that the muscles of the deep perineal space are not flat, planar structures. Furthermore, no distinct superior fascial boundary exists.
Instead, the space is open and bounded only by the inferior surface of the pelvic diaphragm. The muscular fibers of the urethral sphincter extend vertically, incorporating the proximal urethra and the base of the bladder. The term "perineal membrane" has since replaced "urogenital diaphragm" in the Terminologia Anatomica and is now recognized as the inferior fascial boundary of this region. Despite clear evidence to the contrary, references to the urogenital diaphragm remain common in anatomical literature and illustrations, necessitating awareness of its inaccuracy.
Media
(Click Image to Enlarge)
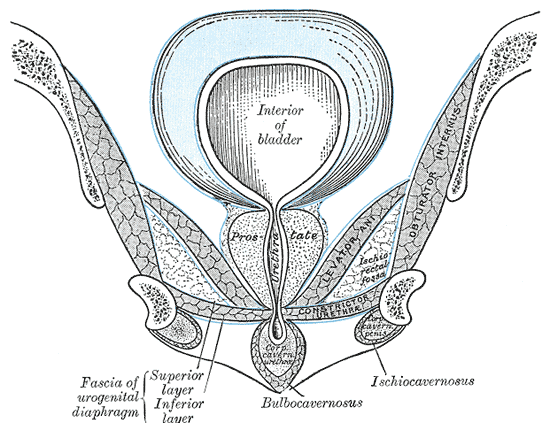
Male Pelvic Floor Anatomy. This illustration displays a coronal section of the male perineum, showing the bladder, prostate, urogenital diaphragm, and associated muscles in relation to the perineal membrane.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
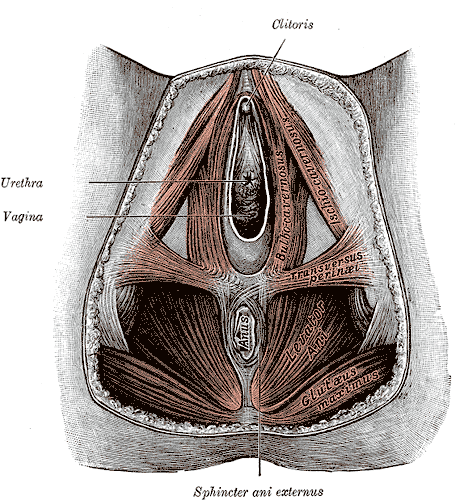
Female Perineum. This illustration shows the perineal membrane, clitoris, urethra, vagina, bulbocavernosus, ischiocavernosus, transversus perineal, levator ani, gluteus maximus, anus, and sphincter ani externus (external anal sphincter).
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Bordoni B, Sugumar K, Leslie SW. Anatomy, Abdomen and Pelvis, Pelvic Floor. StatPearls. 2025 Jan:(): [PubMed PMID: 29489277]
Milley PS, Nichols DH. The relationship between the pubo-urethral ligaments and the urogenital diaphragm in the human female. The Anatomical record. 1971 Jul:170(3):281-3 [PubMed PMID: 5104318]
Colebunders B, Matthew MK, Broer N, Persing JA, Dellon AL. Benjamin Alcock and the pudendal canal. Journal of reconstructive microsurgery. 2011 Jul:27(6):349-54. doi: 10.1055/s-0031-1278705. Epub 2011 May 27 [PubMed PMID: 21623563]
Oelrich TM. The urethral sphincter muscle in the male. The American journal of anatomy. 1980 Jun:158(2):229-46 [PubMed PMID: 7416058]
Oelrich TM. The striated urogenital sphincter muscle in the female. The Anatomical record. 1983 Feb:205(2):223-32 [PubMed PMID: 6846873]
van der Putte SC. The devlopment of the perineum in the human. A comprehensive histological study with a special reference to the role of the stromal components. Advances in anatomy, embryology, and cell biology. 2005:177():1-131 [PubMed PMID: 15615037]
Level 3 (low-level) evidenceBordoni B, Launico MV. Anatomy, Abdomen and Pelvis, Perineal Body. StatPearls. 2026 Jan:(): [PubMed PMID: 30726030]
Tichý M. The morphogenesis of human sphincter urethrae muscle. Anatomy and embryology. 1989:180(6):577-82 [PubMed PMID: 2610390]
Gosling JA, Dixon JS, Critchley HO, Thompson SA. A comparative study of the human external sphincter and periurethral levator ani muscles. British journal of urology. 1981 Feb:53(1):35-41 [PubMed PMID: 6451256]
Level 2 (mid-level) evidenceBare RL, DeFranzo A, Jarow JP. Intraoperative arteriography facilitates penile revascularization. The Journal of urology. 1994 Apr:151(4):1019-21 [PubMed PMID: 8126776]
Breza J, Aboseif SR, Orvis BR, Lue TF, Tanagho EA. Detailed anatomy of penile neurovascular structures: surgical significance. The Journal of urology. 1989 Feb:141(2):437-43 [PubMed PMID: 2913372]
Droupy S, Hessel A, Benoît G, Blanchet P, Jardin A, Giuliano F. Assessment of the functional role of accessory pudendal arteries in erection by transrectal color Doppler ultrasound. The Journal of urology. 1999 Dec:162(6):1987-91 [PubMed PMID: 10569553]
Reiner WG, Walsh PC. An anatomical approach to the surgical management of the dorsal vein and Santorini's plexus during radical retropubic surgery. The Journal of urology. 1979 Feb:121(2):198-200 [PubMed PMID: 423333]
Tanagho EA, Schmidt RA, de Araujo CG. Urinary striated sphincter: what is its nerve supply? Urology. 1982 Oct:20(4):415-7 [PubMed PMID: 6183812]
Zvara P, Carrier S, Kour NW, Tanagho EA. The detailed neuroanatomy of the human striated urethral sphincter. British journal of urology. 1994 Aug:74(2):182-7 [PubMed PMID: 7921935]
Mirilas P, Skandalakis JE. Urogenital diaphragm: an erroneous concept casting its shadow over the sphincter urethrae and deep perineal space. Journal of the American College of Surgeons. 2004 Feb:198(2):279-90 [PubMed PMID: 14759786]
Kaye KW, Milne N, Creed K, van der Werf B. The 'urogenital diaphragm', external urethral sphincter and radical prostatectomy. The Australian and New Zealand journal of surgery. 1997 Jan:67(1):40-4 [PubMed PMID: 9033375]
Brooks JD, Chao WM, Kerr J. Male pelvic anatomy reconstructed from the visible human data set. The Journal of urology. 1998 Mar:159(3):868-72 [PubMed PMID: 9474171]
Level 2 (mid-level) evidenceDorschner W, Biesold M, Schmidt F, Stolzenburg JU. The dispute about the external sphincter and the urogenital diaphragm. The Journal of urology. 1999 Dec:162(6):1942-5 [PubMed PMID: 10569543]
Diaz KC, Leslie SW, Cronovich HA. Penile Fracture. StatPearls. 2025 Jan:(): [PubMed PMID: 31869082]
Gottenger EE, Wagner JR. Penile fracture with complete urethral disruption. The Journal of trauma. 2000 Aug:49(2):339-41 [PubMed PMID: 10963550]
Level 3 (low-level) evidenceNorton SM, Qaoud Y, Doherty E, Daly K, Keenan R, Quinlan M, Mohammed W, Davis N, Mohan P. Surgical management and post-operative functional outcomes of patients with a penile fracture-a single centre experience over 10 years. Irish journal of medical science. 2024 Apr:193(2):917-920. doi: 10.1007/s11845-023-03548-7. Epub 2023 Oct 21 [PubMed PMID: 37864674]
Latini JM, McAninch JW, Brandes SB, Chung JY, Rosenstein D. SIU/ICUD Consultation On Urethral Strictures: Epidemiology, etiology, anatomy, and nomenclature of urethral stenoses, strictures, and pelvic fracture urethral disruption injuries. Urology. 2014 Mar:83(3 Suppl):S1-7. doi: 10.1016/j.urology.2013.09.009. Epub 2013 Nov 8 [PubMed PMID: 24210733]
Gómez RG, Mundy T, Dubey D, El-Kassaby AW, Firdaoessaleh, Kodama R, Santucci R. SIU/ICUD Consultation on Urethral Strictures: Pelvic fracture urethral injuries. Urology. 2014 Mar:83(3 Suppl):S48-58. doi: 10.1016/j.urology.2013.09.023. Epub 2013 Nov 8 [PubMed PMID: 24210734]
Abdeen BM, Leslie SW, Badreldin AM. Urethral Strictures. StatPearls. 2025 Jan:(): [PubMed PMID: 33231967]