Introduction
The process of medical death certification is a challenging and daunting task for most healthcare professionals and clinicians responsible for it. In most instances in the United States, when a death certificate must be completed, the clinician is responsible for completing it. In instances where a crime or foul play is suspected, the medical examiner or coroner takes responsibility for completing the death certificate. Clinicians should not be concerned if the manner of death is natural, suicide, homicide, accident, or undetermined. The burden of determination lies with the medical examiner.[1][2] In rare instances, for example, the death of a hospice patient, a nurse practitioner may complete the death certificate if a physician is not available.
If the death certificate is not completed or filled out properly, it is usually rejected by the official public registrar of vital statistics in the jurisdiction where it is completed.[1][2] The death certificate is a public record that can be accessed by the decedent's family, clinical researchers, lawyers, and insurance companies when there is litigation involved. The death certificate should document the immediate cause of death, which can be an event, clinical condition, or disease process that is unsuitable for the continuation of life. The mechanism of death is less important than the event or condition that precipitated it. The physiologic process of respiratory failure or cardiac failure does not explain the event preceding death. For this reason, clinicians are discouraged from using terms such as:
- Cardiac arrest
- Respiratory arrest
- Cardiopulmonary arrest
- Old age
The main purpose of death certification is for governmental agencies to compile vital statistics. Death certification is used as official documentation of deaths and their causes. The death certificate is not intended to document the history of the present illness or the decedent’s clinical problems but rather to focus on the immediate cause of death. The World Health Organization (WHO) has a mission statement that includes the collection and classification of mortality data. The collection and classification allow researchers to compare data from different countries. The United States is a signatory to this mission statement and follows the WHO's policies, procedures, and regulations. The responsibility for collecting national data in the United States is vested in the National Center for Health Statistics (NCHS), which is part of the Centers for Disease Control and Prevention (CDC). The responsibilities of the NCHS include, but are not limited to, the collection of national data in the United States on the causes of mortality. To meet WHO standards, the NCHS periodically reviews the United States standard certificate of death. Each state is required to comply with the rules and regulations set forth by the NCHS to receive federal funding.
In the United States, there are about 2.6 million annual deaths that are reported to the NCHS. Each US state has specific requirements regarding when a death certificate must be filed. In Wisconsin, for example, the medical portion of the death certificate must be completed within 6 days of death. Willfully and knowingly falsifying information on the death certificate is considered a class 1 felony. In about 33% to 41% of cases, errors are made on the death certificate.[3][4][5] Cardiovascular diseases are significantly overrepresented as the primary cause of death.[6][7] The most commonly cited reasons for errors in death certification are inexperienced clinicians, including clinicians in training, and insufficient training among attending clinicians. Results from studies suggest that organizing seminars and workshops that teach the processes and procedures involved in death certification can greatly improve the accuracy of documentation.[8]
Some healthcare professionals are wary of signing a death certificate, believing that the signature might impose some legal responsibility on the practitioner. The death certificate is a medical opinion regarding the cause of death based on the available information at the time of death. Lawsuits against healthcare professionals for signing a death certificate are extremely rare, and when there is a lawsuit, the certifier of death is usually not held liable. The death certificate can be amended.
Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Function
In the United States, there are similarities and variations in the function and content of the death certificate. Nevertheless, the death certificate in almost all states conforms to the US standard. Death certificates contain 3 categories of information:
Demographics and Statistics
- Name
- Age
- Social Security number
- Race
- Sex
Method of Body Disposition
- Funeral home
- Crematorium
- Burial
- Cemetery site
Death Information
- Date of death
- Time of death
- Manner of death [9]
Pronouncement is the term for the time when an individual is found to be legally dead. In forensic or medical examiner cases, pronouncement might not always correspond to the actual time of death. An individual living alone or in a remote area might have been dead for days or even years before the pronouncement is made.
Pronouncement of Death
Pronouncement of death is the specific date and time when an individual is found to be legally dead. The declaration can be made by a clinician, medical examiner, or coroner.[9]
Date and Time of Death
Date and time of death refer to the date and time when an individual is thought to have actually died. The date and time might be actual or estimated. The date and time of death can be determined by a medical clinician, medical examiner, or coroner.
Cause of Death
Cause of death is the causal chain of events that ultimately leads to death.
The Immediate Cause of Death
The immediate cause of death is the final event in the sequence leading to death. The immediate cause of death is listed as the top diagnosis on the death certificate.
The Underlying Cause of Death
The underlying cause of death is the initial event in the causal sequence that is the most remote from the time of death. Clinicians enter this information last, at the bottom of the death certificate.
Manner of Death
Manner of death describes how death is classified based on the circumstances surrounding the death.
- Natural
- Accident
- Homicide
- Suicide
- Undetermined
Medical Certifier of Death
The medical certifier of death is the individual responsible for completing the medical portion of the death certificate. The medical portion includes the time, date, cause, and manner of death.
Electronic Death Registry
The nonmedical part of the death certificate can be completed by the funeral director after the pronouncement of death. In the United States, most states file the nonmedical portion using an electronic death filing system. The electronic death filing system has several advantages in medical certification:
- Accuracy
- Timeliness
- Better surveillance of mortality
- Efficiency
In electronic death filing, the funeral director fills in information related to the decedent's demographics, statistics, and bodily disposition. An appropriate medical certifier is then selected. In most states, online training or other forms of formal training are required before a healthcare practitioner can be a registered certifier of death. Most states have statutes that specify which individuals are authorized to certify death. Once the nonmedical part is completed, a Fax Attestation for Medical Certification is sent to the healthcare practitioner, who must then complete the medical part of the death certificate. The Fax Attestation for Medical Certification has a section that can only be completed by a medical certifier. After the form is completed, the funeral director can verify the information before it is entered in the state registry. The process differs by state death certificate statute.
Medical Certification of Death
Accuracy is the most important factor to consider in medical death certification. All dates should be indicated by day, month, and year. The time of death should be reported in 24-hour clock format. For example, if the time of death is 1 PM, the time should be recorded as 1300 on the death certificate.
Part I
The cause of death section in the death certificate should be completed as specifically as possible. Part I reports the causal events that led to death and is made up of Part Ia to Part Id. The most immediate or recent event that led to death is listed in line a. The other conditions are listed in line b and then sequentially. The last and most remote condition leading to death is listed as the underlying cause of death. All conditions that fall between the immediate and underlying cause of death are known as intermediate causes. The approximate interval between the onset of each event and the time of death should be listed in hours, days, weeks, or months.
Part II
All other diseases and injuries that may have contributed to death but did not necessarily precipitate the cascade of events leading to death are listed in Part II.
Examples of Completing a Death Certificate
Example 1:
- Part I
- a. Pulmonary edema (2 days) due to or as a consequence of
- b. Anasarca (2 months) due to or as a consequence of
- c. Chronic renal failure (5 years) due to or as a consequence of
- d. Systemic lupus erythematosus (15 years)
- Part II
- Chronic obstructive pulmonary disease (20 years)
- The manner of death: natural
- Autopsy: yes/no
In this example, the immediate cause of death is pulmonary edema. Anasarca and chronic renal failure are the intermediate causes of death related to systemic lupus erythematosus, the underlying cause of death. The death certificate must be very specific. Edema has to specify the location: pulmonary edema. Clinicians should be as specific as possible when listing the cause of death. Abbreviations and acronyms are also best avoided.
Example 2
- Part I
- a. Fat embolism (2 hours) due to or as a consequence of
- b. Chronic tissue hypoxia (12 years) due to or as a consequence of
- c. Sickle cell anemia (12 years)
- Part II
- Moderate persistent asthma (7 years)
- The manner of death: natural
- Autopsy: yes/no
In this example, the immediate cause of death is a fat embolism. Chronic tissue hypoxia from sickle cell disease can cause fatty tissue to dislodge from the bone marrow. Chronic tissue hypoxia is the intermediate cause of death. The underlying cause of death is sickle cell disease, which is the primary disease causing chronic hypoxia from abnormal hemoglobin with impaired oxygen-carrying capacity. The cause of death is required in the death certificate, not the mechanism. The mechanism of most deaths is usually cardiopulmonary arrest. Clinicians should avoid using this diagnosis in the death certificate because it does not specify the cause of death.
Issues of Concern
Special Cases
Injuries:
Death can occur because of an injury sustained in the hospital or outside the hospital setting. Injury-related death has no statute of limitations. A patient may develop overwhelming sepsis secondary to empyema and necrotizing pneumonia from a knife stab wound to the chest. Even though the immediate cause of death in this instance is overwhelming sepsis, the manner of death for medicolegal reasons is still homicide. Hip fractures from falls, especially in frail older adults, are very common. The presence of a hip fracture can predispose patients to sepsis and a thromboembolic event that can ultimately cause death. If, as a sequela of a hip fracture from a fall, a patient later develops pulmonary embolism from prolonged immobilization, the manner of death in this instance would be accidental. Even if an injury is listed only in part 2 of the death certificate, the nonnatural cause, in this instance, the accident, prevails and is used as a determinant of the manner of death. The cause of death on a death certificate can be changed or amended, if needed, based on the specific circumstances related to the death. If death occurs because of injury or poisoning, nonnatural causes are listed as the manner of death.
Example
- Part I
- a. Sepsis and septic shock
- b. Empyema and necrotizing pneumonia
- c. Knife wounds to the chest
- Part II
- Type 2 diabetes
- The manner of death: homicide
- Autopsy: yes/no
Place of injury: The place of injury should be specified in the death certificate. The place of injury might also be the place where the pronouncement of death is made. For example, the location of the injury can be listed as a shopping mall, a fast-food restaurant, a hotel, or a resort. Location of injury should include the street name, ZIP code, county where the injury happened, or where the decedent is found.
Injury at work: This is usually a yes-or-no. This part is important to complete, especially if there is an employer-employee relationship.
How the injury happened: The way the injury happened should be described precisely, for example, skiing on a steep slope, lost control, and hit a tree, or driving a car, struck from behind, and ejected from a vehicle. In most jurisdictions, if the cause of death is not natural, the medical examiner or coroner is responsible for completing the death certificate.
Acute and chronic substance use disorder:
Acute and chronic consumption of illicit drugs or alcohol can cause death. Chronic alcohol use disorder can cause pancreatitis, seizures from alcohol withdrawal, or hepatic cirrhosis. Bacterial endocarditis can develop from chronic intravenous drug use. Oral carcinoma can develop from tobacco chewing, and chronic obstructive lung disease can develop from smoking. Death from a chronic condition is classified as natural. Conversely, death resulting from acute drug toxicity, for example, overdose with cocaine, phencyclidine, or an opiate, is classified as suicide or accident. Classification of death as suicide as a manner of death depends on whether evidence supports self-harm or injury. When death results from therapeutic intervention, for example, overwhelming sepsis from bone marrow suppression secondary to the initiation of chemotherapy, the manner of death in this instance is natural.
Physician-assisted suicide or euthanasia:
In some states, this form of death is classified as “other” or “unclassified.”
Terminal Events
Events such as electromechanical dissociation, ventricular fibrillation, pulseless ventricular tachycardia, asystole, respiratory arrest, or respiratory failure are common and nonspecific. Clinicians should not use these terms in the death certificate.[9][10]
Amending a Death Certificate
At the time of certifying death, the certifier fills in information in the death certificate based on the information available at that time. In other words, the death certificate reflects the best medical opinion at the time of completion. Most states have provisions in their laws to amend the death certificate. If an autopsy is requested and completed within a reasonable time, waiting for the autopsy results before completing the death certificate is best. Some institutions have policies to ensure that the pathologist performing the autopsy consults with the medical certifier of death, and both assume responsibility for signing the death certificate. These policies help prevent discordance between the autopsy report and the cause of death certification. The medical examiner or coroner can amend the death certificate if additional information comes to light.
Clinical Significance
The clinical significance of a death certificate cannot be overemphasized. The 2 most important events in life are birth and death. Legal existence is from the time of birth to death. Records of death and birth are part of the vital statistics that governments collect to plan for food, housing, health care delivery, and education. The statistical analysis of cause-of-death data forms the backbone of vital statistics, which governments use to plan and implement health care policy.
Other Issues
Brain Death
Brain death is defined as the irreversible cessation of all brain functions, including those of the brainstem. Traditionally, the concept of death has always been historically linked to the cessation of heartbeat, but with advances in technology, including mechanical ventilation and inotropic support therapy, an individual might have a beating heart but an irreversible loss of brain functions.[11][12] Brain death declaration is a wholly clinical diagnosis. Practitioners are not required to perform another test if 2 tests for brain stem function and an apnea test are conclusive for brain death.
Determination of Brain Death
History and physical examination that point to a clear-cut etiology of brain death include anoxic brain injury, fulminant hepatic encephalopathy, or severe head injury.[13][14][15]
Exclusion of other causes of coma:
- Severe electrolyte abnormalities
- Ingestion of drugs or toxins that are potential central nervous system depressants, for example, neuromuscular blocking agents, benzodiazepines
- Hypothermia with core body temperature less than 32°C
- Encephalopathy associated with hepatic, renal failure, or hyperosmolar coma
- Severe hypophosphatemia
A detailed neurological examination that includes:
- Examination for spontaneous movement, decerebrate, and decorticate posturing
- Stimulation with noxious stimuli
- Absence of pupillary response to consensual light
- Absent oculocephalic, corneal, cough, and gag reflexes on stimulation
- Absence of oculovestibular reflex on instillation of water
Apnea Test
An apnea test can then be performed once the neurological assessment is complete.[16][17]
The patient must meet the following criteria prior to the initiation of the apnea test:
- The core body temperature should be greater than 36.5°C or 97°F
- Euvolemic status with normal blood pressure
- The partial pressure of carbon dioxide in the blood (PCO2) is equal to or greater than 45 mm Hg.
- The normal partial pressure of oxygen; the clinician preoxygenates the patient to 200 mm Hg.
After satisfaction of the above prerequisite, the apnea test can then be conducted in the following manner:
- Connect the patient to 100% via a T-tube or cannula after disconnecting from mechanical ventilation.
- Watch the patient closely for any spontaneous breaths.
- Take blood samples for blood gas analysis at 4- to 5-minute intervals twice (8 to 10 minutes).
In the absence of spontaneous respiration, and the PCO2 is greater than 60 mm Hg or has risen about 20 mmHg above baseline, the apnea test is positive. If the patient develops spontaneous breaths during the test, the test is considered negative.
The patient should be connected back to mechanical ventilation if:
- Systolic blood pressure falls below 90 mm Hg. In children, if the systolic blood pressure is below the threshold for age
- Significant desaturation on pulse oximetry [17]
- Presence of arrhythmia or dysrhythmia
The clinician should draw and analyze an arterial blood gas sample.
- If PCO2 is greater than 60 mm Hg or PCO2 increase is by more than 20 mm Hg over baseline normal PCO2, the apnea test result is considered to be positive, meaning it supports the clinical diagnosis of brain death.
- If PCO2 is less than 60 mm Hg and the PCO2 increase is less than 20 mm Hg over baseline normal PCO2, the result is considered to be indeterminate.
- In this case, a confirmatory test can be considered.
Confirmatory Test
Confirmatory test for brain death includes:
- Angiography, magnetic resonance imaging, or computed tomography might be used; brain death is demonstrated by the absence of intracerebral filling at the level of the circle of Willis or the carotid bifurcations.
- Electroencephalography: Brain death can be confirmed by demonstrating the absence of electrical activities
- Nuclear brain scanning
Cerebral Scintigraphy (Technetium Tc 9m Exametazime)
Brain death is demonstrated by the absence of radioscopic uptake in the brain parenchyma. Transcranial Doppler ultrasonography flow studies show small systolic peaks and no flow during the diastolic phase. This is indicative of a high vascular resistance to blood flow from increased intracranial pressure associated with brain death.
Brain Death in Children
Brain death determination in pediatrics is a clinical diagnosis. There is not enough data on brain death in an infant less than 37 weeks of age. Therefore, the recommendations listed below do not apply to infants less than 37 weeks of age. Prior to the initiation of brain death protocol, hypothermia, hypotension, and electrolyte abnormalities should be treated as in adults. Medications that interfere with the apnea test or neurological examination should be discontinued. The physical examination should be performed by 2 clinicians. The apnea test can be performed by 1 clinician.
Observation Period
The 2 examinations are separated by an observation period of:
- Twenty-four hours, for newborns up to 30 days
- Twelve hours for infants and children older than 30 days to 18 years [18]
The first examination determines if the child has met all the required criteria for brain death. The second examination is to confirm brain death based on the fact that the condition is irreversible. The assessment of neurological status after cardiopulmonary resuscitation or other severe injuries to the brain should be deferred for about 24 hours or longer if there are inconsistencies in the neurological examination. The protocol for the apnea test is the same as in adults.
Certification of Brain Death
A single clinician with institutional privileges can certify brain death. If the question of organ donation arises, the state of New York requires that the brain death certification be done by the clinician who attended to the patient at the time of death and another clinician. Both clinicians should confirm that the clinical evaluation meets an accepted medical standard.
All the processes and phases involved in the brain death determination should be properly documented:
- The cause of the irreversibility of coma and unresponsiveness
- The absence of motor response to noxious stimuli
- The absence of brainstem reflexes in 2 separate examinations separated by at least 6 hours.
- The absence of respiration with PaCO2 greater than 60 mm Hg
- The rationale and justification for ancillary studies and confirmatory tests
A death certificate can be issued after the test is completed. Once a patient is declared brain dead, mechanical ventilation can be discontinued. However, the family should be treated with sensitivity and respect. Reasonable accommodation should be made for the families to come to terms with brain death. Institutional policies are usually put in place to address the issues and concerns family members might have during the process of certification of death based on brain death criteria.[19]
Media
(Click Image to Enlarge)
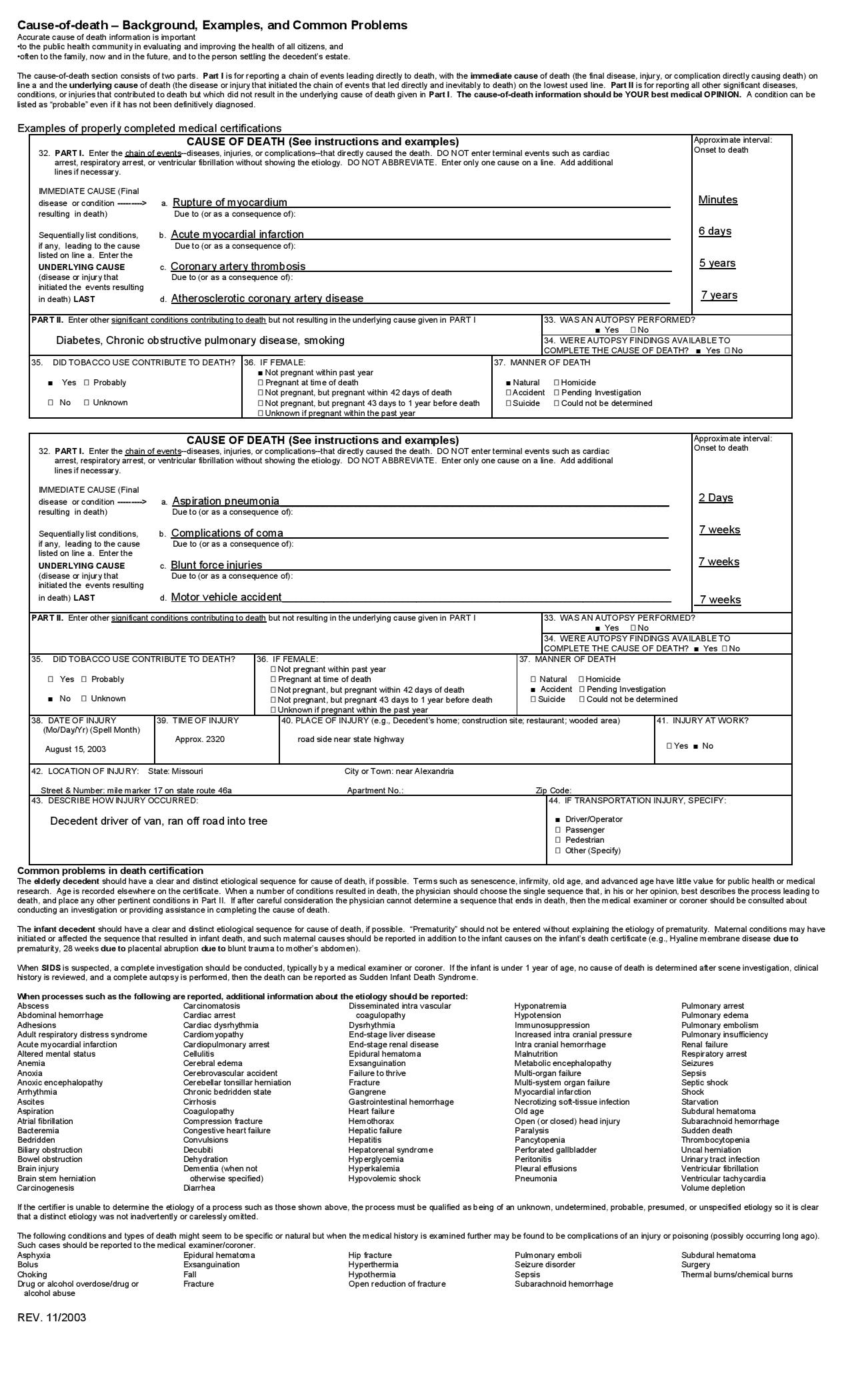
US STANDARD DEATH CERTIFICATION Contributed by the Centers for Disease Control and Prevention, CDC (https://www.cdc.gov/nchs/nvss/revisions-of-the-us-standard-certificates-and-reports.htm)
References
Breaux S, Perez CA. Pitfalls in the use of death certificates for assessing cause of death: a study of tonsil carcinoma patients. American journal of clinical oncology. 1984 Aug:7(4):375-80 [PubMed PMID: 6377867]
Level 2 (mid-level) evidenceKlatt EC, Noguchi TT. Death certification. Purposes, procedures, and pitfalls. The Western journal of medicine. 1989 Sep:151(3):345-7 [PubMed PMID: 2588577]
Pritt BS, Hardin NJ, Richmond JA, Shapiro SL. Death certification errors at an academic institution. Archives of pathology & laboratory medicine. 2005 Nov:129(11):1476-9 [PubMed PMID: 16253030]
Level 2 (mid-level) evidenceSmith Sehdev AE, Hutchins GM. Problems with proper completion and accuracy of the cause-of-death statement. Archives of internal medicine. 2001 Jan 22:161(2):277-84 [PubMed PMID: 11176744]
Myers KA, Farquhar DR. Improving the accuracy of death certification. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 1998 May 19:158(10):1317-23 [PubMed PMID: 9614825]
Lakkireddy DR, Gowda MS, Murray CW, Basarakodu KR, Vacek JL. Death certificate completion: how well are physicians trained and are cardiovascular causes overstated? The American journal of medicine. 2004 Oct 1:117(7):492-8 [PubMed PMID: 15464706]
Level 2 (mid-level) evidenceLakkireddy DR, Basarakodu KR, Vacek JL, Kondur AK, Ramachandruni SK, Esterbrooks DJ, Markert RJ, Gowda MS. Improving death certificate completion: a trial of two training interventions. Journal of general internal medicine. 2007 Apr:22(4):544-8 [PubMed PMID: 17372807]
Level 1 (high-level) evidenceCirera L, Salmerón D, Martínez C, Bañón RM, Navarro C. [More than a decade improving medical and judicial certification in mortality statistics of death causes]. Revista espanola de salud publica. 2018 Jun 6:92():. pii: e201806031. Epub 2018 Jun 6 [PubMed PMID: 29855461]
Brooks EG, Reed KD. Principles and Pitfalls: a Guide to Death Certification. Clinical medicine & research. 2015 Jun:13(2):74-82; quiz 83-4. doi: 10.3121/cmr.2015.1276. Epub [PubMed PMID: 26185270]
Mieno MN, Tanaka N, Arai T, Kawahara T, Kuchiba A, Ishikawa S, Sawabe M. Accuracy of Death Certificates and Assessment of Factors for Misclassification of Underlying Cause of Death. Journal of epidemiology. 2016:26(4):191-8. doi: 10.2188/jea.JE20150010. Epub 2015 Dec 5 [PubMed PMID: 26639750]
Srivastava V, Nakra M, K AS, Dhull P, Ramprasad R, Lamba NS. Brain stem death certification protocol. Medical journal, Armed Forces India. 2018 Jul:74(3):213-216. doi: 10.1016/j.mjafi.2017.04.002. Epub 2017 Jun 17 [PubMed PMID: 30093762]
Al-Wali W, Deshmukh A, Hamed M, Shaukat A. Death certification reforms are an opportunity for wider quality improvement. BMJ (Clinical research ed.). 2018 Aug 1:362():k3240. doi: 10.1136/bmj.k3240. Epub 2018 Aug 1 [PubMed PMID: 30068657]
Level 2 (mid-level) evidenceWijdicks EF. Determining brain death in adults [RETIRED]. Neurology. 1995 May:45(5):1003-11 [PubMed PMID: 7746373]
. Practice parameters for determining brain death in adults (summary statement). The Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 1995 May:45(5):1012-4 [PubMed PMID: 7746374]
Level 1 (high-level) evidenceWijdicks EF, Varelas PN, Gronseth GS, Greer DM, American Academy of Neurology. Evidence-based guideline update: determining brain death in adults: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2010 Jun 8:74(23):1911-8. doi: 10.1212/WNL.0b013e3181e242a8. Epub [PubMed PMID: 20530327]
Level 1 (high-level) evidenceBelsh JM, Blatt R, Schiffman PL. Apnea testing in brain death. Archives of internal medicine. 1986 Dec:146(12):2385-8 [PubMed PMID: 3778074]
Goudreau JL, Wijdicks EF, Emery SF. Complications during apnea testing in the determination of brain death: predisposing factors. Neurology. 2000 Oct 10:55(7):1045-8 [PubMed PMID: 11061269]
Nakagawa TA, Ashwal S, Mathur M, Mysore M, Committee For Determination Of Brain Death In Infants Children. Guidelines for the determination of brain death in infants and children: an update of the 1987 task force recommendations-executive summary. Annals of neurology. 2012 Apr:71(4):573-85. doi: 10.1002/ana.23552. Epub [PubMed PMID: 22522447]
Kotabagi RB, Chaturvedi RK, Banerjee A. Medical Certification of Cause of Death. Medical journal, Armed Forces India. 2004 Jul:60(3):261-72. doi: 10.1016/S0377-1237(04)80060-1. Epub 2011 Jul 21 [PubMed PMID: 27407646]