 Anatomy, Shoulder and Upper Limb, Elbow Cubital Fossa
Anatomy, Shoulder and Upper Limb, Elbow Cubital Fossa
Introduction
The cubital fossa is an area of transition between the anatomical arm and the forearm. It is located in a depression on the anterior surface of the elbow joint. It is also called the antecubital fossa because it lies anterior to the elbow (Latin cubitus) when in standard anatomical position. The cubital fossa is triangular and thus has three borders, with an inferiorly directed apex. It also has a floor and roof, and it is traversed by structures that make up its contents.[1][2][3][4]
Borders
- The lateral border is the medial border of the brachioradialis muscle.
- The medial border is the lateral border of the pronator teres muscle.
- Superior border is an imaginary line between the epicondyles of the humerus.
The floor of the cubital fossa is formed proximally by the brachialis and distally by the supinator muscle. The roof consists of skin and fascia and is reinforced by the bicipital aponeurosis, which is a sheet of tendon-like material that arises from the tendon of the biceps brachii. The bicipital aponeurosis forms a partial protective covering to the medial nerve, brachial artery, and ulnar artery. Within the roof runs the median cubital vein, which can be accessed for venipuncture (see clinical significance below).
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The cubital fossa contains four main vertical structures from lateral to medial.[5][6][7][8]
- The radial nerve is not always strictly considered part of the cubital fossa, but is in the vicinity, passing underneath the brachioradialis muscle. As it does so, the radial nerve divides into its deep and superficial branches.
- The biceps tendon runs through the cubital fossa, attaching to the radial tuberosity, just distal to the neck of the radius.
- Brachial artery supplies oxygenated blood to the forearm. It bifurcates into the radial and ulnar arteries at the apex of the cubital fossa.
- The median nerve leaves the cubital fossa between the two heads of the pronator teres. It supplies the majority of the flexor muscles in the forearm.
Physiologic Variants
Anatomically, the superficial veins of the cubital fossa are classified into four types according to the presence of the median cubital vein (MCV) or median antebrachial vein.
- Type I: The median antebrachial vein is dominant and joins both the cephalic vein (CV) and the basilic vein (BV) in the cubital region. This is also called N-type.
- Type II: The median cubital vein connects both the cephalic vein and the basilic vein in the cubital region. This type is also called type M.
- Type III: In the cubital region, development of the brachial cephalic vein is poor or missing.
- Type IV: No communicating branch between the cephalic vein and basilic vein.
Type II, presenting both the cephalic and basilic veins connected by the median cubital vein, is the most common, followed by type I. Although the most common types in males and females were different, as type I and type II, respectively, there is no statistical difference between them. The frequency of the types between the right and left upper limbs did not differ. Because of the wide variations in these superficial veins, adverse effects such as bruising, hematoma, and sensory changes have been reported to occur due to mispuncture across various health care systems. Most medical practitioners are aware of two patterns of venous return in the cubital fossa. This variation underlines the importance of using the intravenous illuminator for venipuncture.
Surgical Considerations
Brachial artery pseudoaneurysms are pulsatile hematomas caused by hemorrhage into the soft tissues. They are more common after interventional procedures than after diagnostic procedures, although brachial artery pseudoaneurysms are rare. Complications of pseudoaneurysms can cause a serious threat to the afflicted limb and the patient's life.
Clinical Significance
Blood Pressure and Brachial Pulse
During blood pressure measurements, the stethoscope is placed over the brachial artery in the cubital fossa. The artery runs medial to the biceps tendon. The brachial pulse may be palpated in the cubital fossa just medial to the tendon.
Venipuncture
The area just superficial to the cubital fossa is often used for venous access (phlebotomy). One of the most common sites for venipuncture is the superficial veins in the cubital fossa of the upper limbs, which include the cephalic, basilic, median cubital, and antebrachial veins and their tributaries. Many superficial veins can cross this region. The median cubital vein connects the basilic and cephalic veins and is easily accessible. This makes it a common site for venipuncture. It may also be used for the insertion of a peripherally inserted central catheter.
Supracondylar Fracture
This is a common fracture in young patients and usually occurs when a person falls onto a hyper-extended elbow. It is a transverse fracture, spanning between the two epicondyles. It can also happen by falling onto a flexed elbow, but this accounts for less than 5% of cases. The displaced fracture fragments may impinge and damage the contents of the cubital fossa. Direct damage or post-fracture swelling can cause interference with the blood supply of the forearm from the brachial artery. The resulting ischemia can cause Volkmann ischaemic contracture. Cubital tunnel syndrome is the second most common nerve compression syndrome in peripheral nerve compression disease. Although potential ulnar nerve entrapment can occur at multiple points along its course, for example, the Arcade of Struthers, the medial intermuscular septum, the medial epicondyle, the cubital tunnel, and the deep flexor pronator aponeurosis, the most common site of entrapment is the cubital tunnel. The uncontrolled flexion of the hand occurs when the flexor muscles become fibrotic and shortened.
Cubital Tunnel Syndrome
A condition that involves pressure or stretching of the ulnar nerve, which can cause numbness or tingling in the ring and small fingers, pain in the forearm, and/or weakness in the hand. These symptoms often occur when the elbow is bent for an extended period, such as when holding a phone or sleeping. Sometimes nerve testing (EMG/NCS) may be needed to see how much the nerve and muscle are being affected. The first treatment is to avoid actions that cause symptoms. Wrapping a pillow or towel loosely around the elbow or wearing a splint at night to keep the elbow from bending can help. Avoiding pressure on the “funny bone” can also help. Historically, when (venous) blood-letting was practiced, the bicipital aponeurosis (the ceiling of the cubital fossa) was known as the "grace of God" tendon because it protected the more important contents of the fossa (ie, the brachial artery and the median nerve).
Media
(Click Image to Enlarge)
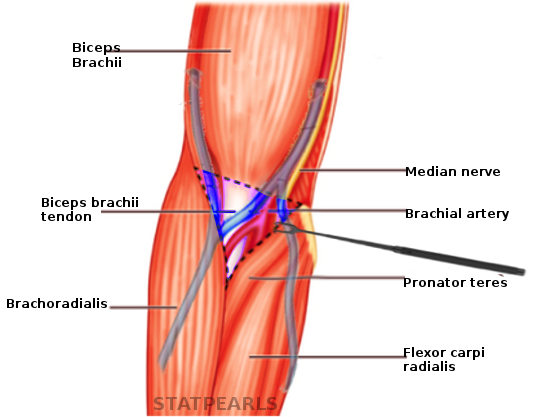
Cubital fossa Image courtesy S Bhimji MD
References
Ma CX, Pan WR, Liu ZA, Zeng FQ, Qiu ZQ, Liu MY. Deep lymphatic anatomy of the upper limb: An anatomical study and clinical implications. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2019 May:223():32-42. doi: 10.1016/j.aanat.2019.01.005. Epub 2019 Feb 1 [PubMed PMID: 30716466]
Level 2 (mid-level) evidenceKwon K, Shin BS, Chung MS, Chung BS. New Viewpoint of Surface Anatomy Using the Curved Sectional Planes of a Male Cadaver. Journal of Korean medical science. 2019 Jan 21:34(3):e15. doi: 10.3346/jkms.2019.34.e15. Epub 2019 Jan 3 [PubMed PMID: 30662383]
Lung BE, Ekblad J, Bisogno M. Anatomy, Shoulder and Upper Limb, Forearm Brachioradialis Muscle. StatPearls. 2026 Jan:(): [PubMed PMID: 30252366]
Pires L, Ráfare AL, Peixoto BU, Pereira TOJS, Pinheiro DMM, Siqueira MEB, Vaqueiro RD, de Paula RC, Babinski MA, Chagas CAA. The venous patterns of the cubital fossa in subjects from Brazil. Morphologie : bulletin de l'Association des anatomistes. 2018 Jun:102(337):78-82. doi: 10.1016/j.morpho.2018.02.001. Epub 2018 Apr 4 [PubMed PMID: 29625795]
Haładaj R, Wysiadecki G, Dudkiewicz Z, Polguj M, Topol M. The High Origin of the Radial Artery (Brachioradial Artery): Its Anatomical Variations, Clinical Significance, and Contribution to the Blood Supply of the Hand. BioMed research international. 2018:2018():1520929. doi: 10.1155/2018/1520929. Epub 2018 Jun 11 [PubMed PMID: 29992133]
Kota AA, Hazra D, Selvaraj AD. Basilic vein haemangioma: an unusual differential diagnosis for cubital fossa mass. BMJ case reports. 2018 Mar 28:2018():. pii: bcr-2015-211343. doi: 10.1136/bcr-2015-211343. Epub 2018 Mar 28 [PubMed PMID: 29599380]
Level 3 (low-level) evidenceSadeghi A, Setayesh Mehr M, Esfandiari E, Mohammadi S, Baharmian H. Variation of the cephalic and basilic veins: A case report. Journal of cardiovascular and thoracic research. 2017:9(4):232-234. doi: 10.15171/jcvtr.2017.40. Epub 2017 Oct 15 [PubMed PMID: 29391938]
Level 3 (low-level) evidenceMukai K, Nakajima Y, Nakano T, Okuhira M, Kasashima A, Hayashi R, Yamashita M, Urai T, Nakatani T. Safety of Venipuncture Sites at the Cubital Fossa as Assessed by Ultrasonography. Journal of patient safety. 2020 Mar:16(1):98-105. doi: 10.1097/PTS.0000000000000441. Epub [PubMed PMID: 29140886]