Introduction
Crohn disease is a chronic inflammatory bowel disease (IBD) distinct from ulcerative colitis, often presenting with subtle or nonspecific symptoms. Crohn disease is an immunologically mediated gastrointestinal disorder characterized by transmural inflammation that can involve any segment of the gastrointestinal tract.
Population-based studies from Northern Europe and Minnesota report ileal, ileocolonic, and colonic involvement in roughly equal proportions, with disease migration occurring in only 6% to 14% of patients.[1] Pathology limited to the upper gastrointestinal tract, ileum, or ileocolonic region is associated with a higher risk of stricturing and fistulizing complications than isolated colonic involvement.[2] Minnesota data indicate that 19% of patients present with stricturing or fistulizing disease within 90 days of diagnosis, and approximately 50% develop complications such as fistulae, phlegmons, strictures, or abscesses within 20 years. Extraintestinal manifestations may involve the eyes, skin, liver, and joints.
The disease follows a chronic, progressive course. Diarrhea, abdominal pain, nausea, and vomiting are common, while weight loss, fever, and fatigue reflect systemic inflammation. Without timely intervention, persistent inflammation can result in disabling complications. Early diagnosis and evidence-based management are essential to optimize long-term outcomes and preserve quality of life.[3][4][5][6][7]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The precise etiology of IBD is undefined. Evidence indicates that the condition arises from an inappropriate immune response to environmental antigens, including drugs, toxins, infections, and intestinal microbes, in genetically susceptible individuals. Large-scale genome-wide association studies have identified more than 200 IBD-associated genes and over 71 Crohn disease-susceptibility loci.[8][9][10] Specific genetic variants correlate with distinct Crohn disease phenotypes. Mutations in NOD2/CARD15, for example, are associated with ileal involvement, earlier onset, and increased disease severity, often necessitating surgical intervention. Although genotyping holds promise for prognostication and individualized treatment planning, genetic testing is not yet widely used in routine clinical practice and remains primarily a research tool.[11]
Epidemiology
Crohn disease is most prevalent in North America, Northern Europe, and New Zealand. The condition exhibits a bimodal age distribution, with peak onset between 15 and 30 years and 40 and 60 years. Incidence is higher in urban compared with rural populations and is particularly elevated among individuals of Northern European or Jewish descent, with incidence rates typically ranging from approximately 5 to over 12 per 100,000 person-years in these groups.[12][13] Prevalence is low in Asian, African, and South American populations.[14] However, recent evidence indicates a marked rise in incidence in rapidly industrializing regions of Asia, Africa, and Australasia.[15]
Pathophysiology
Crohn disease is a multifactorial condition influenced by genetic, infectious, immunological, environmental, and dietary factors. Dysregulated immune responses arise from innate and adaptive mechanisms involving intestinal macrophages, neutrophils, and T-helper cells, promoting proinflammatory mediators such as tumor necrosis factor α (TNF-α). T-helper 1 (Th1) and T-helper 17 (Th17) cells are central to the Crohn disease inflammatory cascade. Colonic lesions exhibit elevated levels of cytokines, including interferon γ and interleukins 2, 12, and 18.[16][17][18]
Inflammatory processes during the early stages of the illness generate systemic symptoms that are often nonspecific, such as fever and malaise. Intestinal injury leads to diarrhea and abdominal pain, with right lower quadrant (RLQ) discomfort commonly reflecting ileocecal involvement. Terminal ileal damage may result in malabsorption and vitamin deficiencies, while anemia can arise from vitamin B12 deficiency or chronic fecal blood loss, depending on the site of intestinal involvement. Transmural inflammation can extend to adjacent structures, forming fistulae and causing secondary organ dysfunction.
Extraintestinal manifestations, primarily driven by systemic inflammation, include arthritis, uveitis, pericholangitis, and renal disorders, which may precede gastrointestinal symptoms. Rare late complications include systemic amyloidosis.
Anatomy of the Small and Large Intestines
The gastrointestinal tract consists primarily of the small and large intestines. Mucosal specialization allows for efficient absorption of nutrients in the small intestine and water in the large intestine. Consequently, the gastrointestinal tract permits greater exposure to environmental antigens than the skin or respiratory tract.
The small intestine measures approximately 6 meters in length and is divided into the duodenum, jejunum, and ileum. The duodenum is retroperitoneal, whereas the jejunum and ileum are intraperitoneal. The ileum terminates at the ileocecal valve.
The small intestinal mucosa is composed of columnar absorptive epithelium interspersed with goblet, endocrine, and Paneth cells. Columnar cells, which occupy the majority of the mucosal surface, form villi that maximize nutrient absorption. Microscopically, these villi resemble a brush, hence the term “brush border.” Each villus contains a core of lamina propria housing blood and lymphatic vessels, leukocytes, fibroblasts, and smooth muscle cells. Crypts of Lieberkuhn are the invaginations between villus bases, extending to the muscularis mucosa. The normal villus-to-crypt height ratio ranges from 4:1 to 5.1:1.
Goblet, endocrine, and Paneth cells are interspersed among the columnar cells and within the crypts. Goblet cells secrete mucin, providing mucosal protection and lubrication. Enteroendocrine cells release peptides that regulate digestive function, while Paneth cells produce antimicrobial proteins, including defensins. Crypts also house stem cells, which replenish damaged or sloughed epithelial cells.
In the duodenum, the submucosa contains Brunner glands, which secrete mucus, bicarbonate, glycoproteins, and pepsinogen II. Histologically, Brunner glands resemble pyloric mucous glands.
The muscularis mucosa consists of smooth muscle sheets that anchor villi and crypts. Contraction of these muscle fibers facilitates villous folding and unfolding, optimizing absorptive surface area.
The large intestine measures approximately 1.5 meters in length and includes the cecum, ascending colon, transverse colon, and descending colon. The sigmoid colon extends from the pelvic brim within the peritoneum and transitions into the rectum at the S3 vertebral level. The distal rectum is extraperitoneal.
The colon's mucosal surface is lined primarily by columnar absorptive cells, which have shorter villi than those of the small intestine. Colonic crypts also contain goblet, endocrine, Paneth, and stem cells.
Both small and large intestinal mucosae exhibit high regenerative capacity, with complete epithelial turnover occurring within approximately 1 week. Thus, these segments possess remarkable reparative ability but remain susceptible to cytotoxic injury from cancer therapies.
Bacterial colonization occurs throughout the small and large intestine, with the highest density in the ileum. Nonpathogenic gram-negative strains, such as Escherichia coli, typically comprise the intestinal flora.
Mucosal and submucosal lymphoid nodules are distributed throughout the intestines. In the ileum, these nodules aggregate to form Peyer patches. M cells in the epithelium overlying lymphoid nodules transport intact antigens from the intestinal lumen to underlying antigen-presenting cells, which include macrophages and dendritic cells. T lymphocytes, activated B cells, and plasma cells are dispersed throughout the lamina propria. Immunoglobulins are also present, with immunoglobulin A being the most abundant.
The outer muscular layers of the intestines generate peristaltic movements, which are coordinated by the myenteric plexus. The serosa consists primarily of collagen and elastic fibers and is covered by a layer of mesothelial cells that secrete serous fluid to lubricate the outer intestinal surfaces (see Image. Large Intestine Transverse Section).
Histopathology
Crohn disease is characterized by transmural inflammation that can affect the entire gastrointestinal tract, from the oral cavity to the perianal region. The terminal ileum and right colon are most commonly involved. The initial lesion begins as an inflammatory infiltrate surrounding an intestinal crypt. Ulceration develops, initially limited to the superficial mucosa, and subsequently extends into deeper layers. Persistent inflammation may lead to noncaseating granuloma formation, which occurs in up to 33% of patients. Absence of granulomas does not exclude the diagnosis.
The classic mucosal cobblestone pattern with skip lesions develops along affected bowel segments, interspersed with areas of normal mucosa. Resolution of acute inflammation leaves fibrotic scarring in previously affected areas.[19] Recurrent cycles of inflammation and scarring may result in stricture formation and bowel obstruction. Extension of inflammation to adjacent organs can produce enterovesicular, enteroenteral, enterocutaneous, or enterovaginal fistulae.
History and Physical
History
Crohn disease presents variably, depending on the affected gastrointestinal segment. Initial symptoms often include recurrent mild abdominal pain, diarrhea, flatulence, and low-grade fever, interspersed with asymptomatic periods lasting weeks to months. Physical or emotional stress may precipitate symptom flares. Repeated exacerbations eventually produce more localized and severe manifestations. A family history of IBD may or may not be reported.
Ileocolic involvement
Patients with ileocolitis commonly report recurrent RLQ pain and diarrhea. The pain is often colicky and may be relieved by defecation. Crohn disease can mimic acute appendicitis, which also presents with RLQ pain, fever, and diarrhea. An inflammatory RLQ mass may be palpable in some cases.
Low-grade fever is typical. High-grade fever should prompt consideration of alternative pathology, such as an intra-abdominal abscess. Weight loss frequently occurs due to chronic diarrhea and reduced oral intake.
Chronic, recurrent inflammation commonly results in fibrostenotic changes and stricture formation at the ileocecal region. Diarrhea may be replaced by chronic bowel obstruction. Progressive ileocecal wall thinning can lead to microperforation and fistula formation involving adjacent organs. Enterovesical fistulae may present with dysuria, pneumaturia, or recurrent urinary tract infections. Enterocutaneous fistulae may manifest as drainage from surgical scars, which are structurally weaker than intact skin. Enterovaginal fistulae may produce dyspareunia and feculent vaginal discharge.
Jejunoileal disease
Involvement of the jejunum and ileum frequently leads to malabsorption and steatorrhea. Nutritional deficiencies may develop, compounded by reduced oral intake. Chronic diarrhea can result in loss of iron, albumin, calcium, magnesium, fat-soluble vitamins (A, D, E, and K), niacin, folic acid, vitamin B12, and trace elements such as zinc, selenium, and copper. Patients may present with clinical manifestations related to specific nutrient deficiencies. Jejunoileal pathology can also contribute to fistula formation and electrolyte imbalances.
Colitis with perianal involvement
Characteristic manifestations include hematochezia, pain on defecation, reduced rectal wall elasticity, incontinence, anorectal pain, fistulae, perirectal abscesses, anal strictures, and hemorrhoidal tags. Colonic strictures may cause bowel obstruction, occasionally requiring surgical intervention. Fistulization into the stomach can result in feculent emesis, while small bowel fistulae may lead to bacterial overgrowth and malabsorption. Rectovaginal fistulae may also occur in affected women.
Gastroduodenal pathology
Upper gastrointestinal involvement is more common in these patients than in other forms of Crohn disease. Symptoms include nausea, emesis, and epigastric pain. Gastric ulcer evaluation often reveals the absence of Helicobacter pylori infection. Upper gastrointestinal obstruction is frequent, and children may develop esophageal involvement.
Extraintestinal manifestations
Crohn disease is frequently associated with extraintestinal manifestations affecting multiple organ systems. These manifestations include the following:
- Eyes: Episcleritis, scleritis, uveitis
- Mouth: Stomatitis, aphthous ulcers
- Liver: Gallstones, cholangitis, primary sclerosing cholangitis
- Kidneys: Nephrolithiasis, hydronephrosis, urinary tract infections
- Joints: Axial (ankylosing spondylitis) or peripheral (knees, ankles, wrists, elbows) arthritis
- Skin: Erythema nodosum, pyoderma gangrenosum [20]
Crohn disease also promotes a hypercoagulable state, increasing the risk of thromboembolic events.[21] Reduced mobility, particularly in hospitalized patients, may predispose to deep vein thrombosis, stroke, or pulmonary embolism.
Physical Examination
A thorough physical examination, including a detailed abdominal assessment, is essential in patients presenting with abdominal complaints. General examination may reveal signs of malnutrition, such as pallor and low body weight. Vital signs may demonstrate fever, tachycardia, or hypotension.
Abdominal inspection can identify enterocutaneous fistulae in patients with advanced disease. Hyperactive bowel sounds may indicate inflammation or obstruction, whereas absent bowel sounds suggest ileus or severe inflammation. Palpation may elicit tenderness corresponding to the affected intestinal segment. Guarding is indicative of peritonitis in cases of intra-abdominal perforation or abscess. Advanced perianal disease may manifest as perianal fistulae or hemorrhoids, warranting a digital rectal examination.
The skin, eyes, oral cavity, and joints should be examined for extraintestinal manifestations of Crohn disease. Liver involvement may present with right upper quadrant tenderness and jaundice. Renal pathology should be considered in patients with flank tenderness or genitourinary abnormalities, including genital fistulae and perineal skin tags. Female patients with gynecological complaints require a pelvic examination. Neurologic deficits may arise from vitamin deficiencies, manifesting as diminished sensation, muscle atrophy, or gait abnormalities.
Comprehensive physical examination of patients with Crohn disease allows identification of active inflammation and evaluation of disease severity. The examination also aids in detecting complications and guiding subsequent diagnostic and management decisions.
Evaluation
Laboratory Tests
Stool tests to exclude infections include culture and sensitivity, ova and parasites, and Clostridioides difficile toxins. Stool calprotectin can detect active Crohn disease and is useful for monitoring disease activity.[22][23][24][25]
Blood tests, including complete blood count and metabolic panel, may reveal anemia secondary to vitamin B12 or iron deficiency and evidence of liver disease. Electrolyte disturbances may result from diarrhea. Elevated creatinine, blood urea nitrogen, or liver enzymes may indicate renal or hepatic involvement. Urinalysis can detect bacteriuria or leukocyturia. Specific nutrient deficiencies, such as iron and calcium, may be documented with serum measurements when results guide therapeutic correction.
Special serologic tests, including antineutrophil cytoplasmic antibodies and anti-Saccharomyces cerevisiae antibodies, are not routinely indicated to distinguish Crohn disease from ulcerative colitis. Elevated C-reactive protein (CRP) or erythrocyte sedimentation rate may reflect the severity of inflammation.[26][27]
Imaging
Plain radiographs are indicated when bowel obstruction is suspected. Small bowel follow-through is frequently used to evaluate terminal ileal involvement and can also detect fistulae. The classic “string sign,” caused by stricture formation or spasm, is often observed.
Gastroenterologists may perform abdominal ultrasonography to evaluate flare-ups or monitor treatment response (see Image. Periumbilical Fistula Ultrasonography). Ultrasound does not involve ionizing radiation and is widely accessible, although spatial resolution may be limited. Findings that can be assessed with this modality include fistulae, free intraperitoneal fluid, abscesses, and increased superior mesenteric artery flow. Doppler ultrasonography can document elevated flow volume in the superior mesenteric artery during active disease.
Abdominal and pelvic computed tomography (CT), magnetic resonance imaging (MRI), or magnetic resonance enterography can detect abscesses, strictures, and fistulae (see Image. Crohn Disease on Computed Tomography). These modalities provide clearer visualization of diseased intestinal segments, though MRI offers superior detail for evaluating fistulizing disease. MRI is preferred over CT in pediatric populations due to minimal exposure to ionizing radiation.
The bowel mucosa may be directly examined via upper endoscopy and colonoscopy. These procedures allow assessment of inflammation extent and permit tissue sampling for diagnostic confirmation. Endoscopy is also useful for monitoring treatment response.
Video capsule endoscopy (VCE) enables visualization of small bowel segments inaccessible by conventional endoscopy or colonoscopy. Caution is warranted in patients with known strictures, given the risk of capsule retention. Video capsule endoscopy is limited to detecting mucosal changes, whereas MRI can assess transmural inflammation and related complications.
Miscellaneous Tests
Crohn disease treatments suppress the immune system, making knowledge of the patient’s vaccination history essential prior to therapy initiation. Vaccines to review include tetanus, diphtheria, pertussis, human papillomavirus, influenza, pneumococcal, hepatitis A, hepatitis B, measles, mumps, rubella, varicella-zoster virus, and severe acute respiratory syndrome coronavirus 2.
Baseline tuberculosis screening is recommended, particularly for patients initiating anti-TNF biologics. Screening for latent tuberculosis may involve history taking, tuberculin skin testing, interferon-γ release assays, and chest radiography.[28]
Thiopurine methyltransferase (TPMT) activity should be assessed before selecting treatment options. Low TPMT activity increases the risk of adverse effects, whereas very high activity may reduce treatment efficacy.
Treatment / Management
Medical Management
Medical management of Crohn disease is generally divided into induction and maintenance phases. The induction phase aims to achieve inflammation control, ideally within 3 months. The maintenance phase is designed to prolong remission. Selection of medical therapy is guided by the patient’s risk profile and disease severity.
Mild-to-moderate disease
Mild-to-moderate Crohn disease may be managed with oral mesalamine, immunomodulators such as thiopurines (6-mercaptopurine, azathioprine) or methotrexate (MTX), and corticosteroids. Mesalamines (5-ASAs) and sulfasalazine, a 5-ASA linked to a sulfapyridine moiety, exert anti-inflammatory effects. The efficacy of these agensts is less established in Crohn disease than in ulcerative colitis. Oral anti-inflammatory 5-ASAs may be considered in mild colonic Crohn disease but are generally ineffective for small bowel involvement.[29] Corticosteroids are primarily used to induce remission during disease flares and stabilize patients until immunomodulators or biologics achieve therapeutic effect, particularly in moderate-to-severe disease. Prolonged corticosteroid therapy is avoided for maintenance because of chronic adverse effects, including osteoporosis, osteonecrosis, and adrenal insufficiency.(A1)
Immunomodulators are steroid-sparing drugs used effectively for maintenance therapy in moderate Crohn disease. These medications have a delayed onset of action, typically between 8 and 12 weeks, and are, therefore, not indicated for the induction of remission in active disease. Immunomodulators may be combined initially with corticosteroids to bridge this gap.[30][31][32][33](A1)
Standard dosing for Crohn disease includes azathioprine 1.5 to 2.5 mg/kg/day, 6-mercaptopurine 0.75 to 1.5 mg/kg/day, and MTX 15 to 25 mg once weekly. TPMT is the primary enzyme responsible for inactivating toxic thiopurine metabolites. As mentioned, low TPMT activity increases the risk of adverse effects, whereas high activity may reduce therapeutic efficacy.[34] MTX is teratogenic and may impair spermatogenesis. Therefore, women of childbearing potential and men should be counseled to use effective contraception for at least 3 months after MTX administration.
Moderate-to-severe disease
Moderate-to-severe Crohn disease, including fistulizing forms, is optimally managed with biologics alone or in combination with immunomodulators. Corticosteroids are primarily employed to induce remission in moderate-to-severe disease and should be used sparingly to minimize adverse effects. Immunomodulators act as adjuncts by reducing immunogenicity against biologic therapies. Combination therapy with an immunomodulator and an anti-TNF agent has demonstrated greater efficacy than monotherapy with either drug alone.[35]
Anti-TNF agents, including infliximab, adalimumab, and certolizumab pegol, inhibit downstream signaling in the TNF inflammatory cascade. These drugs are effective in steroid-resistant or immunomodulator-refractory Crohn disease, with clinical benefit often observed within 2 weeks of initiation. Anti-TNF therapy is particularly effective in treating fistulizing disease and reducing the risk of postsurgical endoscopic recurrence.[36] Caution is warranted in patients with a history of demyelinating disease, congestive heart failure, or malignancies such as lymphoma.[37] Current evidence indicates that anti-TNF therapy does not increase adverse maternal-fetal outcomes in pregnant patients.[38](A1)
Leukocyte trafficking agents selectively inhibit the adhesion protein integrin α4β7 on a subset of memory T cells, preventing their binding to gut mucosal cells. This mechanism produces gut-specific anti-inflammatory effects. Vedolizumab, the agent in this class used for Crohn disease, has demonstrated superior efficacy compared with placebo in both inducing and maintaining remission, with or without concomitant immunomodulators.[39] The onset of clinical effect is slower than that of anti-TNF agents, typically around 10 weeks, particularly in patients previously treated with anti-TNF therapy.[40] Gut-specific action limits systemic toxicity, resulting in a relatively favorable side effect profile.(A1)
Interleukin 12/23 (IL-12/23) inhibitors, including ustekinumab and risankizumab, are effective in patients with inadequate response to corticosteroids, immunomodulators, or anti-TNF therapy.[41][42][43] Ustekinumab acts as a nonselective IL-12/23 inhibitor, whereas risankizumab selectively targets IL-23. Safety surveillance data in patients with psoriasis indicate that these agents have a relatively favorable side effect profile.[44](A1)
Janus kinase (JAK) inhibitors target signaling pathways involved in abnormal immune responses. Upadacitinib is the first oral selective Janus kinase inhibitor approved by the U.S. Food and Drug Administration for Crohn disease and is effective in patients who have failed conventional or biologic therapies.[45] Clinical benefit is often observed within 2 weeks. However, upadacitinib increases the risk of herpes zoster infection, so shingles vaccination is recommended prior to treatment initiation. Use of upadacitinib during pregnancy is not advised due to teratogenicity observed in animal studies.[46](B3)
In 2021, the American Gastroenterology Association (AGA) published guidelines for the management of perianal and fistulizing Crohn disease, strongly recommending infliximab over no treatment for induction and maintenance of remission. Infliximab is the only biologic with dedicated randomized controlled trial evidence demonstrating efficacy.[47] The AGA also strongly advocated combining biologic therapy with an antibiotic rather than using biologic monotherapy to induce fistula healing. This recommendation was based on 2 randomized controlled trials showing that anti-TNF agents combined with ciprofloxacin were more effective in achieving fistula remission than anti-TNF monotherapy.
Surgical Management
Surgical intervention is indicated for Crohn disease complications, including bowel obstruction due to fibrostenotic strictures, fistulization despite appropriate medical therapy, recurrent abscesses, bowel perforation, dysplasia, malignancy, and medically refractory disease. Surgical resection and stricturoplasty are options for managing fibrostenotic disease, the most common indication for surgery (see Image. Subtotal Colectomy in Severe Crohn Colitis). Short-segment strictures may be amenable to endoscopic dilation.
Fistulotomy may be performed for simple fistulas, defined as superficial or low transsphincteric fistulas without associated proctitis. Complex fistulas may require chronic seton placement. Mesenchymal stem cell injection into the fistula tract to reduce inflammation shows therapeutic promise and is currently under investigation.[48](B3)
The American Society of Colon and Rectal Surgeons recommends total colectomy with ileorectal anastomosis or total proctocolectomy for patients with Crohn colitis exhibiting dysplasia not amenable to endoscopic resection. Additional indications include multifocal dysplasia and colorectal cancer. This recommendation is supported by the elevated risk of metachronous colorectal cancer (14%-40%) and the high prevalence of multifocal dysplasia in patients with Crohn colitis who underwent colectomy for low- or high-grade dysplasia.[49][50](A1)
A diverting ileostomy, rather than primary anastomosis, is generally considered during ileocolectomy in Crohn disease patients with multiple risk factors for anastomotic leak, including smoking, corticosteroid use, and weight loss. Residual postsurgical disease or a high risk of recurrence warrants initiation of postoperative biologic therapy, such as an anti-TNF agent, 2 to 4 weeks after surgery, once postoperative infections have been excluded.[51](A1)
Treatment Monitoring
The AGA recommended in 2023 that monitoring of Crohn disease treatment response be guided by clinical symptoms and biomarker levels.[52] Biomarkers may be assessed every 6 to 12 months in patients in remission and more frequently in those requiring therapy adjustment. Recommended biomarkers include fecal calprotectin and serum CRP. A fecal calprotectin level below 150 μg/g and a CRP level below 5 mg/L indicate minimal or absent inflammation, potentially obviating the need for routine endoscopic assessment of disease activity. The AGA further recommended the following:(A1)
- Endoscopic or radiologic confirmation of disease remission within 3 years of symptomatic remission
- Assessment of therapeutic response during active disease using biomarkers every 2 to 4 months
- Follow-up endoscopy 6 to 12 months after symptom resolution to document mucosal healing
A fecal calprotectin level below 50 μg/g is sufficient to exclude disease recurrence in patients who have remained asymptomatic for 12 months following surgical remission. Routine endoscopic evaluation is not required in these patients. The same biomarker threshold may be applied to asymptomatic individuals with low postoperative recurrence risk or those at higher risk who are already receiving prophylactic therapy. High-risk patients not on prophylactic therapy should undergo endoscopic assessment to evaluate disease activity.
Dietary Management
Diet serves as an adjunctive therapy in Crohn disease. Input from a dietitian and appropriate nutritional supplementation are strongly recommended, as symptomatic patients are at risk for malnutrition and micronutrient deficiencies. Patients with a history of terminal ileum inflammation or resection are particularly susceptible to vitamin B12 deficiency.[53][54][55][56] Evidence, primarily from pediatric populations, demonstrates that certain dietary interventions, including elemental and semielemental diets, can reduce mucosal inflammation.[57] However, these diets have been largely ineffective in adults due to poor adherence. Additionally, benefits are typically not durable, as inflammation often recurs after resumption of a nonrestrictive diet.(B3)
Differential Diagnosis
The differential diagnoses to consider in patients with suspected Crohn disease are listed below. Documentation of travel and exposure history, combined with judicious use of laboratory, imaging, and histologic investigations, facilitates differentiation among these conditions.
- Infectious enteritis and terminal ileitis
- Coccidioides
- Histoplasma
- Salmonella
- Mycobacterium tuberculosis
- Yersinia
- Infectious colitis
- Amebiasis
- Campylobacter
- Clostridium difficile
- Cytomegalovirus
- Escherichia coli
- Salmonella
- Shigella
- Noninfectious
- Behcet disease
- Common variable immunodeficiency
- Diverticulitis
- Drug-induced colitis, eg, from nonsteroidal anti-inflammatory drugs and immunotherapy
- Ischemic colitis
- Sarcoidosis
- Segmental colitis associated with diverticulosis
- Small vessel vasculitis
- Solitary rectal ulcer syndrome
These conditions can present with similar patterns of inflammation, infection, or immune-mediated injury. Precise identification is critical for optimizing patient outcomes and avoiding inappropriate treatment.
Prognosis
High-risk patients with moderate-to-severe Crohn disease often exhibit the following characteristics:
- Relatively younger age, typically younger than 30 years
- History of active or recent tobacco use
- Elevated CRP or fecal calprotectin levels
- Deep ulcers identified on colonoscopy
- Involvement of long bowel segments
- Perianal disease
- Extraintestinal manifestations
- History of bowel resections [58][59]
Without immunomodulator or biologic therapy, up to 50% of patients may develop steroid dependence or treatment resistance, with a cumulative incidence of abdominal surgery of 46.6% 10 years after diagnosis.[60] Postsurgical endoscopic recurrence at or above the surgical anastomosis occurs in approximately 90% of cases. Risk factors for early recurrence include cigarette smoking, a short interval from diagnosis to 1st surgery, multiple resections, and penetrating disease.[61] Surveillance ileocolonoscopy is recommended 6 to 12 months postoperatively and should be repeated every 1 to 3 years in the absence of endoscopic recurrence.
Prior meta-analyses indicate a modestly increased mortality risk in patients with Crohn disease, with a standardized pooled mortality ratio of 1.4 to 1.5 compared to the general population. This risk is primarily attributable to gastrointestinal disease, gastrointestinal cancer, and pulmonary pathology.[62][63] Current corticosteroid therapy further increases mortality risk.[64]
Complications
Crohn disease is a systemic disorder with both intestinal and extraintestinal manifestations. Complications associated with this condition include the following:
- Stricture formation
- Fistulae and abscesses
- Colorectal carcinoma
- Ankylosing spondylitis
- Episcleritis, iritis
- Erythema nodosum, pyoderma gangrenosum
- Nephrolithiasis
- Cholelithiasis
- Anemia
- Hypercoagulability
- Osteoporosis
- Osteonecrosis
- Macronutrient and micronutrient deficiencies
- Increased susceptibility to infections
Early detection and adherence to therapeutic regimens can mitigate the risk of these complications and improve long-term patient outcomes. An interprofessional approach allows comprehensive assessment, including nutritional, immunologic, and psychosocial factors, critical for optimizing disease management.
Deterrence and Patient Education
Preventing Crohn disease remains challenging due to its incompletely understood etiology. Nonetheless, several strategies may help reduce the risk of disease onset or mitigate severity.
Genetic counseling is advisable for individuals with a family history of Crohn disease, providing an understanding of their predisposition and guiding decisions on screening or preventive measures. Early recognition and prompt management of suggestive symptoms, such as persistent abdominal pain, diarrhea, rectal bleeding, unexplained weight loss, and fatigue, can help prevent complications and optimize long-term outcomes.
Although no specific diet has been proven to prevent Crohn disease, controlling sugar intake and avoiding foods that exacerbate symptoms may reduce the frequency of flare-ups. Minimizing exposure to environmental triggers, including cigarette smoke, air pollution, certain medications (eg, nonsteroidal anti-inflammatory drugs), and infections, may further decrease disease risk or severity.
Secondary prevention in Crohn disease focuses on measures that reduce the risk of complications following diagnosis. Adherence to prescribed medications is essential for controlling inflammation, managing symptoms, preventing disease flares, and minimizing complication risk. Patients should be counseled on the importance of taking medications as directed, attending scheduled follow-up appointments, and promptly reporting changes in symptoms. Cancer screening is recommended due to an increased risk of malignancies, including skin and gastrointestinal tumors. Skin examinations should be performed regularly, and a colonoscopy every 1 to 3 years is advised for patients with inflammation involving at least 1/3 of the colon to enable early detection of colorectal cancer.
Osteoporosis prevention is critical, as corticosteroid therapy and nutrient deficiencies associated with Crohn disease increase fracture risk. Periodic bone density assessments facilitate early recognition and management. Immunosuppressive therapy also elevates susceptibility to infections, making vaccination against pathogens such as pneumococcus, Haemophilus influenzae, and influenza virus advisable, with additional immunizations guided by patient-specific and regional considerations.
Individual responses to secondary prevention strategies may vary, and not all interventions are universally applicable or equally effective. Continued research is necessary to elucidate the underlying pathophysiology of Crohn disease and develop more targeted preventive and therapeutic approaches.
Enhancing Healthcare Team Outcomes
Crohn disease is a chronic inflammatory disorder with significant diagnostic and management challenges. The potential of this condition to cause multiorgan involvement necessitates an interprofessional care approach. Primary care physicians often provide the initial evaluation for patients presenting with mild abdominal complaints, initiate treatment, and refer patients to specialists for further assessment. Internists may assist in diagnosing recurrent abdominal symptoms accompanied by systemic manifestations such as fever and weight loss, prescribing adjunctive therapies as needed. Gastroenterologists perform diagnostic and therapeutic endoscopies, prescribe targeted therapies, and monitor disease progression. Colorectal surgeons are involved when complications such as fistulae or intestinal obstruction arise.
Dietitians guide nutritional management to prevent malnutrition and micronutrient deficiencies. Nurses administer treatments, educate patients who have undergone surgery on stoma and wound care, monitor progress, and coordinate care. Pharmacists provide education on medication regimens, emphasizing therapeutic benefits, potential adverse effects, and adherence. Additional specialists, including rheumatologists, neurologists, ophthalmologists, hepatologists, nephrologists, dermatologists, and otorhinolaryngologists, may be consulted to address extraintestinal manifestations. Mental health providers support patients experiencing depression or severe anxiety related to symptoms and complications.
The prognosis for patients with Crohn disease is guarded, and quality of life may be diminished.[65] Interprofessional management allows timely recognition and intervention for complications while providing support for patients’ psychosocial needs.
Media
(Click Image to Enlarge)

Periumbilical Fistula Ultrasonography. This abdominal ultrasound image shows a fistula tract, suggestive of Crohn disease.
Contributed by Sarah El-Nakeep, MD
(Click Image to Enlarge)

Subtotal Colectomy in Severe Crohn Colitis. Intraoperative image showing resected colon segment with evident inflammatory thickening and edema characteristic of severe Crohn disease involvement.
Contributed by Francesk Mulita, MD.
(Click Image to Enlarge)

Crohn Disease on Computed Tomography. This axial image shows segmental bowel wall thickening and surrounding mesenteric fat stranding consistent with inflammation from active Crohn disease.
Contributed by Steve Lange, MD
(Click Image to Enlarge)
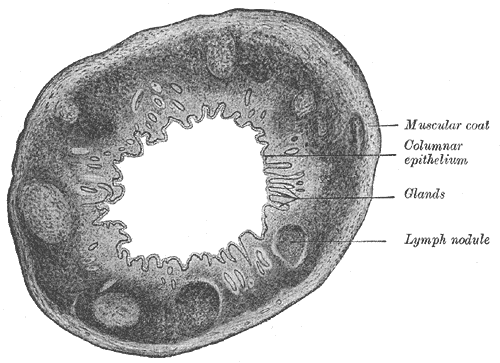
Large Intestine Transverse Section. This transverse section of the large intestine shows the human vermiform process, muscular coat, columnar epithelium, glands, and lymph nodule.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Peyrin-Biroulet L, Loftus EV Jr, Colombel JF, Sandborn WJ. The natural history of adult Crohn's disease in population-based cohorts. The American journal of gastroenterology. 2010 Feb:105(2):289-97. doi: 10.1038/ajg.2009.579. Epub 2009 Oct 27 [PubMed PMID: 19861953]
Thia KT, Sandborn WJ, Harmsen WS, Zinsmeister AR, Loftus EV Jr. Risk factors associated with progression to intestinal complications of Crohn's disease in a population-based cohort. Gastroenterology. 2010 Oct:139(4):1147-55. doi: 10.1053/j.gastro.2010.06.070. Epub 2010 Jul 14 [PubMed PMID: 20637205]
Level 2 (mid-level) evidenceLightner AL, McKenna NP, Alsughayer A, Loftus EV Jr, Raffals LE, Faubion WA, Moir C. Anti-TNF biologic therapy does not increase postoperative morbidity in pediatric Crohn's patients. Journal of pediatric surgery. 2019 Oct:54(10):2162-2165. doi: 10.1016/j.jpedsurg.2019.01.006. Epub 2019 Jan 18 [PubMed PMID: 30773391]
Marazuela García P, López-Frías López-Jurado A, Vicente Bártulos A. Acute abdominal pain in patients with Crohn's disease: what urgent imaging tests should be done? Radiologia. 2019 Jul-Aug:61(4):333-336. doi: 10.1016/j.rx.2018.12.003. Epub 2019 Feb 14 [PubMed PMID: 30772003]
Aksan A, Farrag K, Stein J. An update on the evaluation and management of iron deficiency anemia in inflammatory bowel disease. Expert review of gastroenterology & hepatology. 2019 Feb:13(2):95-97. doi: 10.1080/17474124.2019.1553618. Epub 2018 Dec 7 [PubMed PMID: 30791779]
Hwang JH, Yu CS. Depression and resilience in ulcerative colitis and Crohn's disease patients with ostomy. International wound journal. 2019 Mar:16 Suppl 1(Suppl 1):62-70. doi: 10.1111/iwj.13076. Epub [PubMed PMID: 30793856]
Khan S, Rupniewska E, Neighbors M, Singer D, Chiarappa J, Obando C. Real-world evidence on adherence, persistence, switching and dose escalation with biologics in adult inflammatory bowel disease in the United States: A systematic review. Journal of clinical pharmacy and therapeutics. 2019 Aug:44(4):495-507. doi: 10.1111/jcpt.12830. Epub 2019 Mar 14 [PubMed PMID: 30873648]
Level 1 (high-level) evidenceLiu JZ, van Sommeren S, Huang H, Ng SC, Alberts R, Takahashi A, Ripke S, Lee JC, Jostins L, Shah T, Abedian S, Cheon JH, Cho J, Dayani NE, Franke L, Fuyuno Y, Hart A, Juyal RC, Juyal G, Kim WH, Morris AP, Poustchi H, Newman WG, Midha V, Orchard TR, Vahedi H, Sood A, Sung JY, Malekzadeh R, Westra HJ, Yamazaki K, Yang SK, International Multiple Sclerosis Genetics Consortium, International IBD Genetics Consortium, Barrett JC, Alizadeh BZ, Parkes M, Bk T, Daly MJ, Kubo M, Anderson CA, Weersma RK. Association analyses identify 38 susceptibility loci for inflammatory bowel disease and highlight shared genetic risk across populations. Nature genetics. 2015 Sep:47(9):979-986. doi: 10.1038/ng.3359. Epub 2015 Jul 20 [PubMed PMID: 26192919]
Franke A, McGovern DP, Barrett JC, Wang K, Radford-Smith GL, Ahmad T, Lees CW, Balschun T, Lee J, Roberts R, Anderson CA, Bis JC, Bumpstead S, Ellinghaus D, Festen EM, Georges M, Green T, Haritunians T, Jostins L, Latiano A, Mathew CG, Montgomery GW, Prescott NJ, Raychaudhuri S, Rotter JI, Schumm P, Sharma Y, Simms LA, Taylor KD, Whiteman D, Wijmenga C, Baldassano RN, Barclay M, Bayless TM, Brand S, Büning C, Cohen A, Colombel JF, Cottone M, Stronati L, Denson T, De Vos M, D'Inca R, Dubinsky M, Edwards C, Florin T, Franchimont D, Gearry R, Glas J, Van Gossum A, Guthery SL, Halfvarson J, Verspaget HW, Hugot JP, Karban A, Laukens D, Lawrance I, Lemann M, Levine A, Libioulle C, Louis E, Mowat C, Newman W, Panés J, Phillips A, Proctor DD, Regueiro M, Russell R, Rutgeerts P, Sanderson J, Sans M, Seibold F, Steinhart AH, Stokkers PC, Torkvist L, Kullak-Ublick G, Wilson D, Walters T, Targan SR, Brant SR, Rioux JD, D'Amato M, Weersma RK, Kugathasan S, Griffiths AM, Mansfield JC, Vermeire S, Duerr RH, Silverberg MS, Satsangi J, Schreiber S, Cho JH, Annese V, Hakonarson H, Daly MJ, Parkes M. Genome-wide meta-analysis increases to 71 the number of confirmed Crohn's disease susceptibility loci. Nature genetics. 2010 Dec:42(12):1118-25. doi: 10.1038/ng.717. Epub [PubMed PMID: 21102463]
Level 1 (high-level) evidenceLee HS, Oh H, Yang SK, Baek J, Jung S, Hong M, Kim KM, Shin HD, Kim KJ, Park SH, Ye BD, Han B, Song K. X Chromosome-wide Association Study Identifies a Susceptibility Locus for Inflammatory Bowel Disease in Koreans. Journal of Crohn's & colitis. 2017 Jul 1:11(7):820-830. doi: 10.1093/ecco-jcc/jjx023. Epub [PubMed PMID: 28333213]
Zaidi D, Wine E. Regulation of Nuclear Factor Kappa-Light-Chain-Enhancer of Activated B Cells (NF-κβ) in Inflammatory Bowel Diseases. Frontiers in pediatrics. 2018:6():317. doi: 10.3389/fped.2018.00317. Epub 2018 Oct 30 [PubMed PMID: 30425977]
Stulman M, Focht G, Loewenberg Weisband Y, Greenfeld S, Ben Tov A, Ledderman N, Matz E, Paltiel O, Odes S, Dotan I, Benchimol EI, Turner D. Inflammatory bowel disease among first generation immigrants in Israel: A nationwide epi-Israeli Inflammatory Bowel Disease Research Nucleus study. World journal of methodology. 2023 Dec 20:13(5):475-483. doi: 10.5662/wjm.v13.i5.475. Epub 2023 Dec 20 [PubMed PMID: 38229941]
Heydari K, Rahnavard M, Ghahramani S, Hoseini A, Alizadeh-Navaei R, Rafati S, Raei M, Vahidipour M, Salehi F, Motafeghi F, Neshat S, Moosazadeh M, Yousefi M, Pourali A, Rasouli K, Shokrirad S, Lotfi P, Beladi SA, Hadizadeh Neisanghalb M, Sheydaee F, Moghadam S. Global prevalence and incidence of inflammatory bowel disease: a systematic review and meta-analysis of population-based studies. Gastroenterology and hepatology from bed to bench. 2025:18(2):132-146. doi: 10.22037/ghfbb.v18i2.3105. Epub [PubMed PMID: 40936779]
Level 1 (high-level) evidenceGhersin I, Khteeb N, Katz LH, Daher S, Shamir R, Assa A. Trends in the epidemiology of inflammatory bowel disease among Jewish Israeli adolescents: a population-based study. Alimentary pharmacology & therapeutics. 2019 Mar:49(5):556-563. doi: 10.1111/apt.15160. Epub 2019 Jan 27 [PubMed PMID: 30687945]
Coward S, Clement F, Benchimol EI, Bernstein CN, Avina-Zubieta JA, Bitton A, Carroll MW, Hazlewood G, Jacobson K, Jelinski S, Deardon R, Jones JL, Kuenzig ME, Leddin D, McBrien KA, Murthy SK, Nguyen GC, Otley AR, Panaccione R, Rezaie A, Rosenfeld G, Peña-Sánchez JN, Singh H, Targownik LE, Kaplan GG. Past and Future Burden of Inflammatory Bowel Diseases Based on Modeling of Population-Based Data. Gastroenterology. 2019 Apr:156(5):1345-1353.e4. doi: 10.1053/j.gastro.2019.01.002. Epub 2019 Jan 10 [PubMed PMID: 30639677]
Gálvez J. Role of Th17 Cells in the Pathogenesis of Human IBD. ISRN inflammation. 2014:2014():928461. doi: 10.1155/2014/928461. Epub 2014 Mar 25 [PubMed PMID: 25101191]
Targan SR. Biology of inflammation in Crohn's disease: mechanisms of action of anti-TNF-a therapy. Canadian journal of gastroenterology = Journal canadien de gastroenterologie. 2000 Sep:14 Suppl C():13C-16C [PubMed PMID: 11023555]
Level 3 (low-level) evidenceKanai T, Watanabe M, Okazawa A, Nakamaru K, Okamoto M, Naganuma M, Ishii H, Ikeda M, Kurimoto M, Hibi T. Interleukin 18 is a potent proliferative factor for intestinal mucosal lymphocytes in Crohn's disease. Gastroenterology. 2000 Dec:119(6):1514-23 [PubMed PMID: 11113073]
Greuter T, Piller A, Fournier N, Safroneeva E, Straumann A, Biedermann L, Godat S, Nydegger A, Scharl M, Rogler G, Vavricka SR, Schoepfer AM, Swiss IBD Cohort Study Group. Upper Gastrointestinal Tract Involvement in Crohn's Disease: Frequency, Risk Factors, and Disease Course. Journal of Crohn's & colitis. 2018 Nov 28:12(12):1399-1409. doi: 10.1093/ecco-jcc/jjy121. Epub [PubMed PMID: 30165603]
Fumery M, Pariente B, Sarter H, Savoye G, Spyckerelle C, Djeddi D, Mouterde O, Bouguen G, Ley D, Peneau A, Dupas JL, Turck D, Gower-Rousseau C, Epimad Group. Long-term outcome of pediatric-onset Crohn's disease: A population-based cohort study. Digestive and liver disease : official journal of the Italian Society of Gastroenterology and the Italian Association for the Study of the Liver. 2019 Apr:51(4):496-502. doi: 10.1016/j.dld.2018.11.033. Epub 2018 Dec 23 [PubMed PMID: 30611597]
Owczarek D, Cibor D, Głowacki MK, Rodacki T, Mach T. Inflammatory bowel disease: epidemiology, pathology and risk factors for hypercoagulability. World journal of gastroenterology. 2014 Jan 7:20(1):53-63. doi: 10.3748/wjg.v20.i1.53. Epub [PubMed PMID: 24415858]
Fadeeva NA, Korneeva IA, Knyazev OV, Parfenov AI. Biomarkers of inflammatory bowel disease activity. Terapevticheskii arkhiv. 2018 Dec 30:90(12):107-111. doi: 10.26442/00403660.2018.12.000018. Epub [PubMed PMID: 30701842]
Parfenov AI, Knyazev OV, Kagramanova AV, Fadeeva NA. Personalized medicine in the treatment of inflammatory bowel diseases. Terapevticheskii arkhiv. 2018 Feb 15:90(2):4-11. doi: 10.26442/terarkh20189024-11. Epub [PubMed PMID: 30701765]
Kedia S, Das P, Madhusudhan KS, Dattagupta S, Sharma R, Sahni P, Makharia G, Ahuja V. Differentiating Crohn's disease from intestinal tuberculosis. World journal of gastroenterology. 2019 Jan 28:25(4):418-432. doi: 10.3748/wjg.v25.i4.418. Epub [PubMed PMID: 30700939]
Moon JS. Clinical Aspects and Treatments for Pediatric Inflammatory Bowel Diseases. Pediatric gastroenterology, hepatology & nutrition. 2019 Jan:22(1):50-56. doi: 10.5223/pghn.2019.22.1.50. Epub 2019 Jan 10 [PubMed PMID: 30671373]
Lichtenstein GR, Loftus EV, Isaacs KL, Regueiro MD, Gerson LB, Sands BE. ACG Clinical Guideline: Management of Crohn's Disease in Adults. The American journal of gastroenterology. 2018 Apr:113(4):481-517. doi: 10.1038/ajg.2018.27. Epub 2018 Mar 27 [PubMed PMID: 29610508]
Torres J, Bonovas S, Doherty G, Kucharzik T, Gisbert JP, Raine T, Adamina M, Armuzzi A, Bachmann O, Bager P, Biancone L, Bokemeyer B, Bossuyt P, Burisch J, Collins P, El-Hussuna A, Ellul P, Frei-Lanter C, Furfaro F, Gingert C, Gionchetti P, Gomollon F, González-Lorenzo M, Gordon H, Hlavaty T, Juillerat P, Katsanos K, Kopylov U, Krustins E, Lytras T, Maaser C, Magro F, Marshall JK, Myrelid P, Pellino G, Rosa I, Sabino J, Savarino E, Spinelli A, Stassen L, Uzzan M, Vavricka S, Verstockt B, Warusavitarne J, Zmora O, Fiorino G. ECCO Guidelines on Therapeutics in Crohn's Disease: Medical Treatment. Journal of Crohn's & colitis. 2020 Jan 1:14(1):4-22. doi: 10.1093/ecco-jcc/jjz180. Epub [PubMed PMID: 31711158]
Rahier JF, Magro F, Abreu C, Armuzzi A, Ben-Horin S, Chowers Y, Cottone M, de Ridder L, Doherty G, Ehehalt R, Esteve M, Katsanos K, Lees CW, Macmahon E, Moreels T, Reinisch W, Tilg H, Tremblay L, Veereman-Wauters G, Viget N, Yazdanpanah Y, Eliakim R, Colombel JF, European Crohn's and Colitis Organisation (ECCO). Second European evidence-based consensus on the prevention, diagnosis and management of opportunistic infections in inflammatory bowel disease. Journal of Crohn's & colitis. 2014 Jun:8(6):443-68. doi: 10.1016/j.crohns.2013.12.013. Epub 2014 Mar 6 [PubMed PMID: 24613021]
Level 3 (low-level) evidenceFord AC, Kane SV, Khan KJ, Achkar JP, Talley NJ, Marshall JK, Moayyedi P. Efficacy of 5-aminosalicylates in Crohn's disease: systematic review and meta-analysis. The American journal of gastroenterology. 2011 Apr:106(4):617-29. doi: 10.1038/ajg.2011.71. Epub 2011 Mar 15 [PubMed PMID: 21407190]
Level 1 (high-level) evidenceChande N, Patton PH, Tsoulis DJ, Thomas BS, MacDonald JK. Azathioprine or 6-mercaptopurine for maintenance of remission in Crohn's disease. The Cochrane database of systematic reviews. 2015 Oct 30:2015(10):CD000067. doi: 10.1002/14651858.CD000067.pub3. Epub 2015 Oct 30 [PubMed PMID: 26517527]
Level 1 (high-level) evidenceChande N, Tsoulis DJ, MacDonald JK. Azathioprine or 6-mercaptopurine for induction of remission in Crohn's disease. The Cochrane database of systematic reviews. 2013 Apr 30:(4):CD000545. doi: 10.1002/14651858.CD000545.pub4. Epub 2013 Apr 30 [PubMed PMID: 23633304]
Level 1 (high-level) evidenceMcDonald JW, Wang Y, Tsoulis DJ, MacDonald JK, Feagan BG. Methotrexate for induction of remission in refractory Crohn's disease. The Cochrane database of systematic reviews. 2014 Aug 6:2014(8):CD003459. doi: 10.1002/14651858.CD003459.pub4. Epub 2014 Aug 6 [PubMed PMID: 25099640]
Level 1 (high-level) evidenceFeagan BG, Fedorak RN, Irvine EJ, Wild G, Sutherland L, Steinhart AH, Greenberg GR, Koval J, Wong CJ, Hopkins M, Hanauer SB, McDonald JW. A comparison of methotrexate with placebo for the maintenance of remission in Crohn's disease. North American Crohn's Study Group Investigators. The New England journal of medicine. 2000 Jun 1:342(22):1627-32 [PubMed PMID: 10833208]
Richard VS, Al-Ismail D, Salamat A. Should we test TPMT enzyme levels before starting azathioprine? Hematology (Amsterdam, Netherlands). 2007 Aug:12(4):359-60 [PubMed PMID: 17654066]
Colombel JF, Sandborn WJ, Reinisch W, Mantzaris GJ, Kornbluth A, Rachmilewitz D, Lichtiger S, D'Haens G, Diamond RH, Broussard DL, Tang KL, van der Woude CJ, Rutgeerts P, SONIC Study Group. Infliximab, azathioprine, or combination therapy for Crohn's disease. The New England journal of medicine. 2010 Apr 15:362(15):1383-95. doi: 10.1056/NEJMoa0904492. Epub [PubMed PMID: 20393175]
Kawalec P, Mikrut A, Wiśniewska N, Pilc A. Tumor necrosis factor-α antibodies (infliximab, adalimumab and certolizumab) in Crohn's disease: systematic review and meta-analysis. Archives of medical science : AMS. 2013 Oct 31:9(5):765-79. doi: 10.5114/aoms.2013.38670. Epub 2013 Nov 5 [PubMed PMID: 24273556]
Level 1 (high-level) evidenceVan Assche G, Lewis JD, Lichtenstein GR, Loftus EV, Ouyang Q, Panes J, Siegel CA, Sandborn WJ, Travis SP, Colombel JF. The London position statement of the World Congress of Gastroenterology on Biological Therapy for IBD with the European Crohn's and Colitis Organisation: safety. The American journal of gastroenterology. 2011 Sep:106(9):1594-602; quiz 1593, 1603. doi: 10.1038/ajg.2011.211. Epub 2011 Aug 16 [PubMed PMID: 21844919]
De Felice KM, Kane S. Safety of anti-TNF agents in pregnancy. The Journal of allergy and clinical immunology. 2021 Sep:148(3):661-667. doi: 10.1016/j.jaci.2021.07.005. Epub [PubMed PMID: 34489011]
Hui S, Sinopoulou V, Gordon M, Aali G, Krishna A, Ding NS, Boyapati RK. Vedolizumab for induction and maintenance of remission in Crohn's disease. The Cochrane database of systematic reviews. 2023 Jul 17:7(7):CD013611. doi: 10.1002/14651858.CD013611.pub2. Epub 2023 Jul 17 [PubMed PMID: 37458279]
Level 1 (high-level) evidenceHazlewood GS, Rezaie A, Borman M, Panaccione R, Ghosh S, Seow CH, Kuenzig E, Tomlinson G, Siegel CA, Melmed GY, Kaplan GG. Comparative effectiveness of immunosuppressants and biologics for inducing and maintaining remission in Crohn's disease: a network meta-analysis. Gastroenterology. 2015 Feb:148(2):344-54.e5; quiz e14-5. doi: 10.1053/j.gastro.2014.10.011. Epub 2014 Oct 16 [PubMed PMID: 25448924]
Level 1 (high-level) evidenceFeagan BG, Sandborn WJ, Gasink C, Jacobstein D, Lang Y, Friedman JR, Blank MA, Johanns J, Gao LL, Miao Y, Adedokun OJ, Sands BE, Hanauer SB, Vermeire S, Targan S, Ghosh S, de Villiers WJ, Colombel JF, Tulassay Z, Seidler U, Salzberg BA, Desreumaux P, Lee SD, Loftus EV Jr, Dieleman LA, Katz S, Rutgeerts P, UNITI–IM-UNITI Study Group. Ustekinumab as Induction and Maintenance Therapy for Crohn's Disease. The New England journal of medicine. 2016 Nov 17:375(20):1946-1960 [PubMed PMID: 27959607]
D'Haens G, Panaccione R, Baert F, Bossuyt P, Colombel JF, Danese S, Dubinsky M, Feagan BG, Hisamatsu T, Lim A, Lindsay JO, Loftus EV Jr, Panés J, Peyrin-Biroulet L, Ran Z, Rubin DT, Sandborn WJ, Schreiber S, Neimark E, Song A, Kligys K, Pang Y, Pivorunas V, Berg S, Duan WR, Huang B, Kalabic J, Liao X, Robinson A, Wallace K, Ferrante M. Risankizumab as induction therapy for Crohn's disease: results from the phase 3 ADVANCE and MOTIVATE induction trials. Lancet (London, England). 2022 May 28:399(10340):2015-2030. doi: 10.1016/S0140-6736(22)00467-6. Epub [PubMed PMID: 35644154]
Ferrante M, Panaccione R, Baert F, Bossuyt P, Colombel JF, Danese S, Dubinsky M, Feagan BG, Hisamatsu T, Lim A, Lindsay JO, Loftus EV Jr, Panés J, Peyrin-Biroulet L, Ran Z, Rubin DT, Sandborn WJ, Schreiber S, Neimark E, Song A, Kligys K, Pang Y, Pivorunas V, Berg S, Duan WR, Huang B, Kalabic J, Liao X, Robinson A, Wallace K, D'Haens G. Risankizumab as maintenance therapy for moderately to severely active Crohn's disease: results from the multicentre, randomised, double-blind, placebo-controlled, withdrawal phase 3 FORTIFY maintenance trial. Lancet (London, England). 2022 May 28:399(10340):2031-2046. doi: 10.1016/S0140-6736(22)00466-4. Epub [PubMed PMID: 35644155]
Level 1 (high-level) evidencePapp K, Gottlieb AB, Naldi L, Pariser D, Ho V, Goyal K, Fakharzadeh S, Chevrier M, Calabro S, Langholff W, Krueger G. Safety Surveillance for Ustekinumab and Other Psoriasis Treatments From the Psoriasis Longitudinal Assessment and Registry (PSOLAR). Journal of drugs in dermatology : JDD. 2015 Jul:14(7):706-14 [PubMed PMID: 26151787]
Loftus EV Jr, Panés J, Lacerda AP, Peyrin-Biroulet L, D'Haens G, Panaccione R, Reinisch W, Louis E, Chen M, Nakase H, Begun J, Boland BS, Phillips C, Mohamed MF, Liu J, Geng Z, Feng T, Dubcenco E, Colombel JF. Upadacitinib Induction and Maintenance Therapy for Crohn's Disease. The New England journal of medicine. 2023 May 25:388(21):1966-1980. doi: 10.1056/NEJMoa2212728. Epub [PubMed PMID: 37224198]
Akiyama S, Steinberg JM, Kobayashi M, Suzuki H, Tsuchiya K. Pregnancy and medications for inflammatory bowel disease: An updated narrative review. World journal of clinical cases. 2023 Mar 16:11(8):1730-1740. doi: 10.12998/wjcc.v11.i8.1730. Epub [PubMed PMID: 36969991]
Level 3 (low-level) evidenceSingh S, Proctor D, Scott FI, Falck-Ytter Y, Feuerstein JD. AGA Technical Review on the Medical Management of Moderate to Severe Luminal and Perianal Fistulizing Crohn's Disease. Gastroenterology. 2021 Jun:160(7):2512-2556.e9. doi: 10.1053/j.gastro.2021.04.023. Epub [PubMed PMID: 34051985]
Wang X, Shen B. Advances in Perianal Disease Associated with Crohn's Disease-Evolving Approaches. Gastrointestinal endoscopy clinics of North America. 2019 Jul:29(3):515-530. doi: 10.1016/j.giec.2019.02.011. Epub [PubMed PMID: 31078250]
Level 3 (low-level) evidenceMaser EA, Sachar DB, Kruse D, Harpaz N, Ullman T, Bauer JJ. High rates of metachronous colon cancer or dysplasia after segmental resection or subtotal colectomy in Crohn's colitis. Inflammatory bowel diseases. 2013 Aug:19(9):1827-32. doi: 10.1097/MIB.0b013e318289c166. Epub [PubMed PMID: 23669402]
Derikx LAAP, Nissen LHC, Smits LJT, Shen B, Hoentjen F. Risk of Neoplasia After Colectomy in Patients With Inflammatory Bowel Disease: A Systematic Review and Meta-analysis. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2016 Jun:14(6):798-806.e20. doi: 10.1016/j.cgh.2015.08.042. Epub 2015 Sep 25 [PubMed PMID: 26407752]
Level 1 (high-level) evidenceLightner AL, Vogel JD, Carmichael JC, Keller DS, Shah SA, Mahadevan U, Kane SV, Paquette IM, Steele SR, Feingold DL. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Surgical Management of Crohn's Disease. Diseases of the colon and rectum. 2020 Aug:63(8):1028-1052. doi: 10.1097/DCR.0000000000001716. Epub [PubMed PMID: 32692069]
Level 1 (high-level) evidenceAnanthakrishnan AN, Adler J, Chachu KA, Nguyen NH, Siddique SM, Weiss JM, Sultan S, Velayos FS, Cohen BL, Singh S, AGA Clinical Guidelines Committee. Electronic address: clinicalpractice@gastro.org. AGA Clinical Practice Guideline on the Role of Biomarkers for the Management of Crohn's Disease. Gastroenterology. 2023 Dec:165(6):1367-1399. doi: 10.1053/j.gastro.2023.09.029. Epub [PubMed PMID: 37981354]
Level 1 (high-level) evidenceBrown SR, Fearnhead NS, Faiz OD, Abercrombie JF, Acheson AG, Arnott RG, Clark SK, Clifford S, Davies RJ, Davies MM, Douie WJP, Dunlop MG, Epstein JC, Evans MD, George BD, Guy RJ, Hargest R, Hawthorne AB, Hill J, Hughes GW, Limdi JK, Maxwell-Armstrong CA, O'Connell PR, Pinkney TD, Pipe J, Sagar PM, Singh B, Soop M, Terry H, Torkington J, Verjee A, Walsh CJ, Warusavitarne JH, Williams AB, Williams GL, Wilson RG, ACPGBI IBD Surgery Consensus Collaboration. The Association of Coloproctology of Great Britain and Ireland consensus guidelines in surgery for inflammatory bowel disease. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. 2018 Dec:20 Suppl 8():3-117. doi: 10.1111/codi.14448. Epub [PubMed PMID: 30508274]
Level 3 (low-level) evidencede Kloet LC, Schagen SEE, van den Berg A, Clement-de Boers A, Houdijk MECAM, van der Kaay DCM. [Growth failure as a symptom of inflammatory bowel disease]. Nederlands tijdschrift voor geneeskunde. 2018 Nov 19:162():. pii: D2515. Epub 2018 Nov 19 [PubMed PMID: 30500117]
Rodríguez-Lago I, Ferreiro-Iglesias R, Nos P, Gisbert JP, en representación del Grupo Español de Trabajo en Enfermedad de Crohn y Colitis Ulcerosa (GETECCU). Management of acute severe ulcerative colitis in Spain: A nationwide clinical practice survey. Gastroenterologia y hepatologia. 2019 Feb:42(2):90-101. doi: 10.1016/j.gastrohep.2018.09.002. Epub 2018 Oct 4 [PubMed PMID: 30293913]
Level 3 (low-level) evidenceAmbruzs JM, Larsen CP. Renal Manifestations of Inflammatory Bowel Disease. Rheumatic diseases clinics of North America. 2018 Nov:44(4):699-714. doi: 10.1016/j.rdc.2018.06.007. Epub 2018 Sep 7 [PubMed PMID: 30274631]
Lewis JD, Abreu MT. Diet as a Trigger or Therapy for Inflammatory Bowel Diseases. Gastroenterology. 2017 Feb:152(2):398-414.e6. doi: 10.1053/j.gastro.2016.10.019. Epub 2016 Oct 25 [PubMed PMID: 27793606]
Peyrin-Biroulet L, Panés J, Sandborn WJ, Vermeire S, Danese S, Feagan BG, Colombel JF, Hanauer SB, Rycroft B. Defining Disease Severity in Inflammatory Bowel Diseases: Current and Future Directions. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2016 Mar:14(3):348-354.e17. doi: 10.1016/j.cgh.2015.06.001. Epub 2015 Jun 11 [PubMed PMID: 26071941]
Level 3 (low-level) evidenceSandborn WJ. Crohn's disease evaluation and treatment: clinical decision tool. Gastroenterology. 2014 Sep:147(3):702-5. doi: 10.1053/j.gastro.2014.07.022. Epub 2014 Jul 18 [PubMed PMID: 25046160]
Frolkis AD, Dykeman J, Negrón ME, Debruyn J, Jette N, Fiest KM, Frolkis T, Barkema HW, Rioux KP, Panaccione R, Ghosh S, Wiebe S, Kaplan GG. Risk of surgery for inflammatory bowel diseases has decreased over time: a systematic review and meta-analysis of population-based studies. Gastroenterology. 2013 Nov:145(5):996-1006. doi: 10.1053/j.gastro.2013.07.041. Epub 2013 Jul 27 [PubMed PMID: 23896172]
Level 1 (high-level) evidenceDe Cruz P, Kamm MA, Prideaux L, Allen PB, Desmond PV. Postoperative recurrent luminal Crohn's disease: a systematic review. Inflammatory bowel diseases. 2012 Apr:18(4):758-77. doi: 10.1002/ibd.21825. Epub 2011 Aug 9 [PubMed PMID: 21830279]
Level 1 (high-level) evidenceCanavan C, Abrams KR, Mayberry JF. Meta-analysis: mortality in Crohn's disease. Alimentary pharmacology & therapeutics. 2007 Apr 15:25(8):861-70 [PubMed PMID: 17402989]
Level 1 (high-level) evidenceBewtra M, Kaiser LM, TenHave T, Lewis JD. Crohn's disease and ulcerative colitis are associated with elevated standardized mortality ratios: a meta-analysis. Inflammatory bowel diseases. 2013 Mar:19(3):599-613. doi: 10.1097/MIB.0b013e31827f27ae. Epub [PubMed PMID: 23388544]
Level 1 (high-level) evidenceLewis JD, Gelfand JM, Troxel AB, Forde KA, Newcomb C, Kim H, Margolis DJ, Strom BL. Immunosuppressant medications and mortality in inflammatory bowel disease. The American journal of gastroenterology. 2008 Jun:103(6):1428-35; quiz 1436. doi: 10.1111/j.1572-0241.2008.01836.x. Epub 2008 May 20 [PubMed PMID: 18494836]
Inokuchi T, Takahashi S, Hiraoka S, Toyokawa T, Takagi S, Takemoto K, Miyaike J, Fujimoto T, Higashi R, Morito Y, Nawa T, Suzuki S, Nishimura M, Inoue M, Kato J, Okada H. Long-term outcomes of patients with Crohn's disease who received infliximab or adalimumab as the first-line biologics. Journal of gastroenterology and hepatology. 2019 Aug:34(8):1329-1336. doi: 10.1111/jgh.14624. Epub 2019 Feb 27 [PubMed PMID: 30724387]