Definition/Introduction
Corneal Anatomy
The cornea is an avascular, transparent structure located at the anterior aspect of the eye. This protective membrane shields against foreign substances and supports the eye's ability to focus incoming light onto the retina.[1] Clarity is essential for proper light refraction, necessitating the absence of blood vessels. Nutritional support is supplied by the tear film and the aqueous humor, the latter occupying the anterior chamber between the cornea and the iris-pupil complex.
The cornea is traditionally described as being composed of 5 layers: the epithelium, Bowman layer, stroma, Descemet membrane, and endothelium (see Image. Corneal Microanatomy and Reflex Pathways).[2] The epithelium constitutes the outermost layer of the cornea. This section provides a smooth surface that absorbs oxygen from the environment and nutrients from tears, supplying the underlying corneal layers. The epithelium also functions as a barrier against foreign substances. The Bowman layer, located deep to the epithelium, consists of collagen fibers that confer structural strength. Injury to this zone can result in scarring and impaired vision.
The stroma is the thickest corneal layer, predominantly composed of water with small amounts of collagen. Deep to the stroma is the Descemet membrane, a dense collagenous layer that provides additional protection against injury and infection. This layer is synthesized by the underlying endothelial cells and retains regenerative capacity if damaged. The endothelium, the innermost corneal layer, functions as a pump that removes excess fluid from the stroma, which normally leaks into the anterior chamber. Failure of the endothelial pump leads to stromal edema. Damage to endothelial cells can result in permanent vision loss due to their lack of regenerative capacity. The only definitive treatment for endothelial injury is corneal transplantation.[3]
The human cornea is the most richly innervated tissue in the body, exhibiting sensitivity 300 to 600 times that of skin.[4] Sensory innervation is provided by the long ciliary branches of the ophthalmic division (cranial nerve V1) of the trigeminal nerve (cranial nerve V). These branches form nerve plexuses that run parallel to the corneal surface, situated between the epithelium and the Bowman layer.[5][6] Corneal sensory fibers consist of myelinated Aβ and Aδ fibers, as well as unmyelinated C fibers.[7]
The Corneal Reflex
The cornea is the first ocular structure contacted by irritants or foreign objects. Contact with the cornea elicits 2 protective reflexes: the blink (corneal) and lacrimation (tear production) reflexes. The corneal blink reflex is mediated by a neural pathway connecting the sensory fibers of the trigeminal nerve (cranial nerve V) with the motor fibers of the facial nerve (cranial nerve VII), which innervate the orbicularis oculi muscles. The reflex is initiated when a sensory stimulus activates either free nerve endings or mechanoreceptors within the corneal epithelium.
Sensory information is transmitted via the ophthalmic nerve to synapse within the spinal trigeminal nucleus in the brainstem. Neurons in the spinal trigeminal nucleus project to the facial nucleus, forming synapses with the facial nerve. The facial nerve exits the facial nucleus, encircles the abducens (cranial nerve VI) nucleus, and leaves the skull at the stylomastoid foramen. After exiting, the facial nerve courses medially across the facial surface to activate the orbicularis oculi muscle. Contraction of this muscle produces eyelid closure.[8]
The blink reflex comprises 2 stages: early and late. Aβ fibers trigger the initial movement of the eyelid (early response) on the ipsilateral side, whereas other fiber types mediate the late stage. The late-stage reflex activates facial nerves bilaterally, producing simultaneous blinking of both eyes. Input from secondary motor systems, including the interpositus nucleus of the cerebellum, red nucleus, and reticular activating system, can modulate this late-stage reflex.[9][10][11]
Motor output of each blink exhibits variability under nonpathological conditions. Factors influencing the blink response include the duration and intensity of the sensory stimulus.[12] Additional modulation arises from brainstem and cortical circuits that synapse directly or indirectly with the trigeminal, spinal, and facial nuclei, adjusting blink strength in response to conditioning.[13][14]
The blink response results in eyelid closure. Reopening of the eyelid is mediated by a secondary pathway involving the oculomotor (cranial nerve III) nucleus. This pathway is activated by afferent fibers from the ophthalmic division of the trigeminal nerve (cranial nerve V1), which also mediate the blink reflex. These fibers provide secondary input to neurons in the spinal trigeminal nucleus that project to the oculomotor nucleus. These neurons synapse onto oculomotor neurons that activate the levator palpebrae superioris, initiating eyelid reopening. The oculomotor pathway functions in coordination with the facial motor pathway to ensure complete blink cycle execution.
Tear Production
Touching the corneal surface can also activate neural circuits that initiate tear production. This reflex pathway parallels that of the blink reflex, with the distinction that parasympathetic fibers within the facial nerve innervate the lacrimal and meibomian (tarsal) glands rather than the orbicularis oculi muscle. The lacrimal gland secretes aqueous tears, whereas the meibomian glands produce an oily film that reduces tear evaporation and maintains corneal surface stability.[15] Parasympathetic fibers reach these glands via the zygomatic branch of the facial nerve, synapsing in the pterygopalatine ganglion before continuing as the lacrimal nerve.
Tears serve multiple functions, including forming a smooth optical surface, maintaining corneal hydration, washing away debris or irritants, and providing antibacterial activity to prevent infection. The corneal blink reflex is not the sole mechanism triggering tear production. Visual and gustatory reflexes can also activate these glands. Bright light elicits visual reflexes, whereas certain noxious chemicals in food, such as spicy or hot substances, activate taste reflexes. Both pathways converge on parasympathetic circuits that mediate lacrimation.[16]
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
Several disorders and environmental substances can alter the corneal blink reflex by modifying the anatomy of trigeminal nerve fibers within the cornea. For instance, glaucoma is characterized by increased intraocular pressure. Progressive disease induces bending of trigeminal nerve fibers, which correlates with worsening ocular symptoms and reduced corneal blink reflex sensitivity. Results from studies examining glaucoma treatments indicate that patients receiving topical medications containing benzalkonium chloride have a higher prevalence of nerve fiber bending than those prescribed preservative-free formulations.[17][18][19] Clinical consideration of topical medication selection is essential, as the choice of formulation can significantly influence prognosis.
Diabetes mellitus induces peripheral neuropathy that affects corneal innervation. Unmyelinated C fibers and small Aδ fibers are most commonly affected. Disease progression is associated with decreased nerve plexus density, reduced nerve branching, and increased nerve fiber bending.[20][21] These structural alterations result in diminished ocular pain and temperature sensation, producing bilateral reductions in the late phase of the corneal blink reflex.[22][23][24]
Corneal nerve injuries, ocular pathology, inflammatory responses, aging, hormonal alterations, and certain medications can reduce tear production, resulting in dry eye disease (keratoconjunctivitis sicca). Reduced tear production can further compromise corneal integrity, perpetuating a cycle of pathology. Recognition of this cyclical process is essential for clinicians to prevent progressive corneal damage. Mild dry eye disease associated with corneal reflex deficits may be managed with artificial tear application, warm compresses, and improved eyelid hygiene to maintain ocular surface hydration. Management of moderate-to-severe cases requires a referral to an ophthalmologist.
Dry eye disorders are commonly classified as either aqueous-deficient or evaporative. Aqueous-deficient dry eye may result from inflammation of lacrimal gland epithelial cells (as in Sjögren syndrome), obstruction of the lacrimal gland, damage to corneal reflex nerves, changes due to aging, or reactions to medications, such as antihistamines, β-blockers, and diuretics. Evaporative dry eye is characterized by tear hyperosmolarity and may occur despite normal tear production.[25]
Bogorad syndrome, also known as “Crocodile tears syndrome,” affects tear production circuits. The condition arises from abnormal neural reconnections that form during regeneration of the facial nerve after Bell palsy. During recovery, efferent fibers from the superior salivary nucleus form synapses with parasympathetic fibers of the facial nerve, leading to lacrimation during salivation, such as when smelling or consuming food.[26]
A vast spectrum of neurological disorders, including Alzheimer disease, Parkinson disease, Guillain-Barré syndrome, Charcot-Marie-Tooth disease, and multiple sclerosis, exhibit symptoms that impact corneal structure and function. Manifestations may include reduced blink rate, decreased tear production, diminished corneal nerve density, and impaired corneal sensitivity. Clinical recognition of these corneal manifestations can help optimize patient care.[27]
Clinical Significance
The corneal blink reflex serves as a critical diagnostic tool for clinicians, dentists, maxillofacial surgeons, and ophthalmologists when evaluating trigeminal or facial nerve pathology. Deficits identified through this test can localize pathology to central or peripheral regions without the need for imaging modalities, including radiography.[28] Abnormalities in the corneal blink reflex can arise from lesions at any site in the reflex pathway. Peripheral lesions produce ipsilateral reflex deficits, whereas central lesions result in bilateral deficits.[29]
Peripheral disruption of the corneal blink circuit arises from damage to the trigeminal or facial nerve. Assessment of peripheral nerve injury involves evaluating the early and late stages of the blink reflex or examining secondary symptoms associated with nerve impairment.[30] In stage-specific testing, lesions of the trigeminal nerve typically manifest as ipsilateral deficits in the early stage, whereas lesions of the facial nerve produce ipsilateral deficits in both the early and late stages.[31]
Secondary symptom assessment includes evaluation of motor and sensory function. The ophthalmic nerve mediates sensation of the forehead. Functional testing of this nerve involves having the patient close their eyes while indicating perception of tactile stimuli applied to various areas of the face. Damage to the ophthalmic nerve results in absent or diminished sensation on the affected side of the forehead.
Damage to the facial nerve produces ipsilateral paresis of the muscles of facial expression, producing drooping of the mouth and flattening of the forehead and nasolabial fold on the affected side.[32] Assessment of facial motor activity may be performed by instructing the patient to smile or perform other facial expressions. Muscles of facial expression on the affected side remain immobile in cases of facial nerve injury.
Central nervous system lesions produce bilateral deficits in the corneal blink reflex, typically affecting the late stage while sparing the early stage. A common lesion that alters the blink response is Wallenberg syndrome, caused by a lateral medullary infarct. Relaying the blink reflex depends on the spinal trigeminal nucleus located in the lateral medulla. Disruption of this region interrupts the reflex pathway, resulting in absent late-stage responses bilaterally upon corneal stimulation on the affected side.[33] Injury or dysfunction of the reticular activating system, red nucleus, or cerebellum also modifies the corneal blink reflex. These structures modulate facial nerve output and can alter the strength or velocity of the late-stage blink response bilaterally.[34][35][36]
Anatomy, Function, and Clinical Significance of the Dua Layer
The Dua layer, first reported by Professor Harminder Dua in 2013, is a distinct, acellular layer located between the posterior stroma and the Descemet membrane. Measuring approximately 6 to 16 µm in thickness, this layer consists mainly of compact collagen lamellae and abundant elastin, conferring remarkable strength and air impermeability.[37] Also referred to as the "pre–Descemet layer," this region plays a crucial role in corneal biomechanics and surgical outcomes, particularly in deep anterior lamellar keratoplasty, by resisting separation and reducing the risk of perforation during procedures. The Dua layer is also implicated in pathologies such as acute corneal hydrops and Descemet membrane detachment, enhancing understanding of posterior corneal disorders.[38] The discovery of the Dua layer has refined the classification of corneal anatomy to 6 layers, affecting both clinical practice and anatomical teaching.
No studies have documented the direct impact of a Dua layer injury on the corneal reflex. Owing to its structural function, disruption of this layer primarily affects corneal stability and biomechanics rather than sensory pathways. However, such damage may result in edema or detachment-related complications that could secondarily alter corneal sensitivity or curvature, thereby indirectly influencing the corneal reflex.
Nursing, Allied Health, and Interprofessional Team Interventions
Although the corneal blink reflex serves as a diagnostic tool for clinicians, including dentists, maxillofacial surgeons, and ophthalmologists, interprofessional collaboration and comprehensive team-based care can improve patient outcomes. This approach may involve pharmacists and nurses who ensure accurate drug dosing and administration, occupational and physical therapists who provide neurological rehabilitation for sensory or motor deficits, and social workers who assist patients and their families in addressing circumstances contributing to the initial injury.
Nursing, Allied Health, and Interprofessional Team Monitoring
The corneal blink reflex also serves as a useful indicator of neurological health. This reflex is simple, safe, cost-effective, and easily administered by various members of the healthcare team. Regular assessment of the blink reflex has been associated with improved corneal sensitivity in patients with neurological disorders. A decline in reflex activity may indicate early neurological deterioration. Interprofessional healthcare personnel can employ the corneal blink reflex as an objective measure of neurological stability to facilitate timely detection and intervention. Prompt management following early recognition generally improves clinical outcomes across a wide range of neurological conditions.[39]
Media
(Click Image to Enlarge)
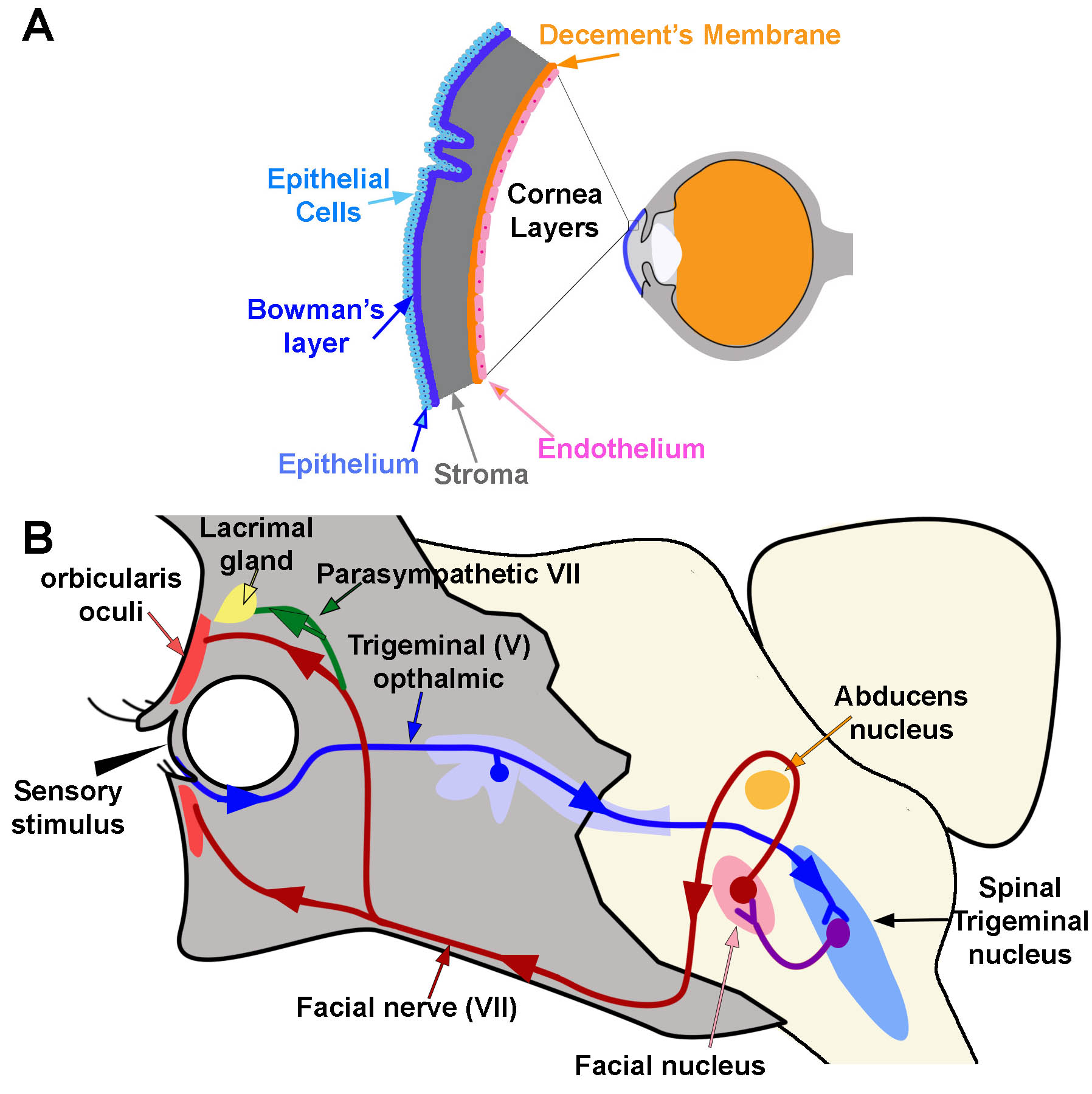
Corneal Microanatomy and Reflex Pathways. Panel A illustrates the major corneal layers and their relative locations. Panel B depicts the neural circuits underlying the corneal blink and tear production reflexes. The blink reflex pathway is indicated with blue, purple, and red arrows showing the direction of signal transmission. The tear production reflex follows the same sensory pathways but activates the lacrimal gland via parasympathetic fibers of the facial nerve, indicated in green.
Contributed and Created by Dr. Diana Peterson
References
Yang AY, Chow J, Liu J. Corneal Innervation and Sensation: The Eye and Beyond. The Yale journal of biology and medicine. 2018 Mar:91(1):13-21 [PubMed PMID: 29599653]
Ludwig PE, Lopez MJ, Sevensma KE. Anatomy, Head and Neck, Eye Cornea. StatPearls. 2025 Jan:(): [PubMed PMID: 29262108]
Vereertbrugghen A, Galletti JG. Corneal nerves and their role in dry eye pathophysiology. Experimental eye research. 2022 Sep:222():109191. doi: 10.1016/j.exer.2022.109191. Epub 2022 Jul 16 [PubMed PMID: 35850173]
ZANDER E, WEDDELL G. Observations on the innervation of the cornea. Journal of anatomy. 1951 Jan:85(1):68-99 [PubMed PMID: 14814019]
Müller LJ, Marfurt CF, Kruse F, Tervo TM. Corneal nerves: structure, contents and function. Experimental eye research. 2003 May:76(5):521-42 [PubMed PMID: 12697417]
Level 3 (low-level) evidenceCruzat A, Qazi Y, Hamrah P. In Vivo Confocal Microscopy of Corneal Nerves in Health and Disease. The ocular surface. 2017 Jan:15(1):15-47. doi: 10.1016/j.jtos.2016.09.004. Epub 2016 Oct 19 [PubMed PMID: 27771327]
Casale R, Frazzitta G, Fundarò C, Balbi P, Del Rosso A, Bertinotti L, Matucci-Cerinic M. Blink reflex discloses CNS dysfunction in neurologically asymptomatic patients with systemic sclerosis. Clinical neurophysiology : official journal of the International Federation of Clinical Neurophysiology. 2004 Aug:115(8):1917-20 [PubMed PMID: 15261870]
Bologna M, Paparella G, Valls-Solé J, Hallett M, Berardelli A. Neural control of blinking. Clinical neurophysiology : official journal of the International Federation of Clinical Neurophysiology. 2024 May:161():59-68. doi: 10.1016/j.clinph.2024.02.023. Epub 2024 Feb 22 [PubMed PMID: 38447495]
Holstege G, van Ham JJ, Tan J. Afferent projections to the orbicularis oculi motoneuronal cell group. An autoradiographical tracing study in the cat. Brain research. 1986 May 28:374(2):306-20 [PubMed PMID: 3719340]
Level 3 (low-level) evidenceWikgren J, Korhonen T. Interpositus nucleus inactivation reduces unconditioned response amplitude after paired but not explicitly unpaired treatment in rabbit eyeblink conditioning. Neuroscience letters. 2001 Aug 10:308(3):181-4 [PubMed PMID: 11479018]
Level 3 (low-level) evidenceWikgren J, Ruusuvirta T, Korhonen T. Reflex facilitation during eyeblink conditioning and subsequent interpositus nucleus inactivation in the rabbit (Oryctolagus cuniculus). Behavioral neuroscience. 2002 Dec:116(6):1052-8 [PubMed PMID: 12492303]
Level 3 (low-level) evidenceManning KA, Evinger C. Different forms of blinks and their two-stage control. Experimental brain research. 1986:64(3):579-88 [PubMed PMID: 3803493]
Level 3 (low-level) evidenceFreeman JH, Steinmetz AB. Neural circuitry and plasticity mechanisms underlying delay eyeblink conditioning. Learning & memory (Cold Spring Harbor, N.Y.). 2011:18(10):666-77. doi: 10.1101/lm.2023011. Epub 2011 Oct 3 [PubMed PMID: 21969489]
Level 3 (low-level) evidenceDelgado-García JM, Gruart A. Building new motor responses: eyelid conditioning revisited. Trends in neurosciences. 2006 Jun:29(6):330-8 [PubMed PMID: 16713636]
Level 3 (low-level) evidenceBron AJ, Tiffany JM, Gouveia SM, Yokoi N, Voon LW. Functional aspects of the tear film lipid layer. Experimental eye research. 2004 Mar:78(3):347-60 [PubMed PMID: 15106912]
Shaheen BS, Bakir M, Jain S. Corneal nerves in health and disease. Survey of ophthalmology. 2014 May-Jun:59(3):263-85. doi: 10.1016/j.survophthal.2013.09.002. Epub 2014 Jan 23 [PubMed PMID: 24461367]
Level 3 (low-level) evidenceSkalicky SE, Goldberg I, McCluskey P. Ocular surface disease and quality of life in patients with glaucoma. American journal of ophthalmology. 2012 Jan:153(1):1-9.e2. doi: 10.1016/j.ajo.2011.05.033. Epub 2011 Aug 26 [PubMed PMID: 21872203]
Level 2 (mid-level) evidenceFechtner RD, Godfrey DG, Budenz D, Stewart JA, Stewart WC, Jasek MC. Prevalence of ocular surface complaints in patients with glaucoma using topical intraocular pressure-lowering medications. Cornea. 2010 Jun:29(6):618-21. doi: 10.1097/ICO.0b013e3181c325b2. Epub [PubMed PMID: 20386433]
Rossi GC, Blini M, Scudeller L, Ricciardelli G, Depolo L, Amisano A, Bossolesi L, Pasinetti GM, Bianchi PE. Effect of preservative-free tafluprost on keratocytes, sub-basal nerves, and endothelium: a single-blind one-year confocal study on naïve or treated glaucoma and hypertensive patients versus a control group. Journal of ocular pharmacology and therapeutics : the official journal of the Association for Ocular Pharmacology and Therapeutics. 2013 Nov:29(9):821-5. doi: 10.1089/jop.2013.0069. Epub 2013 Aug 14 [PubMed PMID: 23944905]
Level 2 (mid-level) evidenceKallinikos P, Berhanu M, O'Donnell C, Boulton AJ, Efron N, Malik RA. Corneal nerve tortuosity in diabetic patients with neuropathy. Investigative ophthalmology & visual science. 2004 Feb:45(2):418-22 [PubMed PMID: 14744880]
Chang PY, Carrel H, Huang JS, Wang IJ, Hou YC, Chen WL, Wang JY, Hu FR. Decreased density of corneal basal epithelium and subbasal corneal nerve bundle changes in patients with diabetic retinopathy. American journal of ophthalmology. 2006 Sep:142(3):488-90 [PubMed PMID: 16935596]
Level 2 (mid-level) evidenceRosenberg ME, Tervo TM, Immonen IJ, Müller LJ, Grönhagen-Riska C, Vesaluoma MH. Corneal structure and sensitivity in type 1 diabetes mellitus. Investigative ophthalmology & visual science. 2000 Sep:41(10):2915-21 [PubMed PMID: 10967045]
Petropoulos IN, Green P, Chan AW, Alam U, Fadavi H, Marshall A, Asghar O, Efron N, Tavakoli M, Malik RA. Corneal confocal microscopy detects neuropathy in patients with type 1 diabetes without retinopathy or microalbuminuria. PloS one. 2015:10(4):e0123517. doi: 10.1371/journal.pone.0123517. Epub 2015 Apr 8 [PubMed PMID: 25853247]
Bitirgen G, Ozkagnici A, Malik RA, Kerimoglu H. Corneal nerve fibre damage precedes diabetic retinopathy in patients with type 2 diabetes mellitus. Diabetic medicine : a journal of the British Diabetic Association. 2014 Apr:31(4):431-8. doi: 10.1111/dme.12324. Epub 2013 Nov 5 [PubMed PMID: 24117485]
Level 2 (mid-level) evidenceKwon J, Moghtader A, Kang C, Bibak Bejandi Z, Shahjahan S, Alzein A, Djalilian AR. Overview of Dry Eye Disease for Primary Care Physicians. Medicina (Kaunas, Lithuania). 2025 Mar 6:61(3):. doi: 10.3390/medicina61030460. Epub 2025 Mar 6 [PubMed PMID: 40142272]
Level 3 (low-level) evidenceTripathy K, Arsiwalla T. Crocodile Tears Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 30247828]
Zemaitiene R, Gorgadze G, Mockaitiene L. Ocular Surface Changes Associated with Neurological Diseases. Medicina (Kaunas, Lithuania). 2025 Sep 18:61(9):. doi: 10.3390/medicina61091693. Epub 2025 Sep 18 [PubMed PMID: 41011084]
Khan ZA. Revisiting the Corneal and Blink Reflexes for Primary and Secondary Trigeminal Facial Pain Differentiation. Pain research & management. 2021:2021():6664736. doi: 10.1155/2021/6664736. Epub 2021 Feb 9 [PubMed PMID: 33628353]
Valls-Sole J. Spontaneous, Voluntary, and Reflex Blinking in Clinical Practice. Journal of clinical neurophysiology : official publication of the American Electroencephalographic Society. 2019 Nov:36(6):415-421. doi: 10.1097/WNP.0000000000000561. Epub [PubMed PMID: 31688324]
Kimura J, Powers JM, Van Allen MW. Reflex response of orbicularis oculi muscle to supraorbital nerve stimulation. Study in normal subjects and in peripheral facial paresis. Archives of neurology. 1969 Aug:21(2):193-9 [PubMed PMID: 5797352]
Cruccu G, Deuschl G. The clinical use of brainstem reflexes and hand-muscle reflexes. Clinical neurophysiology : official journal of the International Federation of Clinical Neurophysiology. 2000 Mar:111(3):371-87 [PubMed PMID: 10699396]
Portela RC, Miller AC. Antivirals With Corticosteroids for the Treatment of Acute Bell's Palsy. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2019 Mar:26(3):342-344. doi: 10.1111/acem.13563. Epub 2018 Oct 23 [PubMed PMID: 30182458]
Ongerboer de Visser BW, Kuypers HG. Late blink reflex changes in lateral medullary lesions. An electrophysiological and neuro-anatomical study of Wallenberg's Syndrome. Brain : a journal of neurology. 1978 Jun:101(2):285-94 [PubMed PMID: 667600]
Delgado-García JM, Gruart A. The role of interpositus nucleus in eyelid conditioned responses. Cerebellum (London, England). 2002 Dec:1(4):289-308 [PubMed PMID: 12879967]
Level 3 (low-level) evidenceFanardjian VV, Manvelyan LR. Peculiarities of cerebellar excitation of facial nucleus motoneurons. Neuroscience letters. 1984 Aug 31:49(3):265-70 [PubMed PMID: 6493608]
Level 3 (low-level) evidenceMorcuende S, Delgado-Garcia JM, Ugolini G. Neuronal premotor networks involved in eyelid responses: retrograde transneuronal tracing with rabies virus from the orbicularis oculi muscle in the rat. The Journal of neuroscience : the official journal of the Society for Neuroscience. 2002 Oct 15:22(20):8808-18 [PubMed PMID: 12388587]
Level 3 (low-level) evidenceDua HS, Freitas R, Mohammed I, Ting DSJ, Said DG. The pre-Descemet's layer (Dua's layer, also known as the Dua-Fine layer and the pre-posterior limiting lamina layer): Discovery, characterisation, clinical and surgical applications, and the controversy. Progress in retinal and eye research. 2023 Nov:97():101161. doi: 10.1016/j.preteyeres.2022.101161. Epub 2023 Jan 14 [PubMed PMID: 36642673]
Level 3 (low-level) evidenceDua HS, Said DG. Clinical evidence of the pre-Descemets layer (Dua's layer) in corneal pathology. Eye (London, England). 2016 Aug:30(8):1144-5. doi: 10.1038/eye.2016.62. Epub 2016 Apr 8 [PubMed PMID: 27055671]
Lee MWY, Chau SW. Intra-operative blink reflex neurophysiological monitoring in posterior skull base neurosurgery. Frontiers in surgery. 2025:12():1485459. doi: 10.3389/fsurg.2025.1485459. Epub 2025 Jun 25 [PubMed PMID: 40636915]