 Corneal Trauma: Evaluation and Management of Ocular Surface Injuries
Corneal Trauma: Evaluation and Management of Ocular Surface Injuries
Introduction
Ocular trauma is a significant health challenge. The Global Burden of Diseases, Injuries, and Risk Factors Study recorded more than 59 million cases of ocular trauma and 438,000 years of added disability in 2019.[1] Similarly, the World Health Organization estimates 55 million ocular trauma incidents and 1.6 million eye injuries resulting in blindness each year.[2][3][4] Between 2022 and 2040, childhood and adolescent ocular trauma is projected to increase across the globe.[5]
Corneal trauma can arise from the direct impact of physical objects or from environmental exposures that alter the corneal surface. Mechanical injuries from physical objects include corneal abrasions and retained foreign bodies. Exposures to chemical, thermal, and radiation sources degrade the corneal surface, causing ocular burns.[6][7][8][9][10] The morbidity from corneal traumatic injuries varies from minor and insignificant to vision-threatening, with some estimates attributing 1.5 million cases of blindness to corneal neovascularization and trauma.[11] Penetrating trauma involving other anterior and posterior segment structures and ocular surface burns are considered more severe.
The cornea, being the most anterior and exposed structure of the eye, is particularly vulnerable to traumatic insults due to its direct interaction with the external environment and absence of protective adnexal coverage in certain situations such as high-velocity injuries or chemical exposures.[12] The cornea's unique avascular structure, coupled with dense innervation primarily from the ophthalmic division of the trigeminal nerve, renders even minor injuries significantly symptomatic, often presenting with pain, photophobia, tearing, and blepharospasm.[13] The structural integrity of the cornea is maintained by a highly organized arrangement of collagen lamellae and specialized epithelial and endothelial layers, which are essential for maintaining transparency and refractive function.[14] Disruption of these layers following trauma can lead to immediate visual impairment and long-term sequelae such as scarring, irregular astigmatism, and corneal opacity.
The pathophysiology of corneal trauma is complex and varies depending on the mechanism of injury.[15] Mechanical trauma, including abrasions and lacerations, primarily affects the epithelial and stromal layers, triggering a cascade of inflammatory responses characterized by cytokine release, leukocyte infiltration, and keratocyte activation.[14] This response is essential for wound healing but may also contribute to stromal haze and fibrosis if dysregulated.[16] In contrast, chemical injuries, particularly alkali burns, penetrate rapidly through the corneal stroma due to saponification of cell membranes, leading to widespread cellular destruction and potential involvement of deeper ocular structures.[17] Acid injuries tend to cause protein coagulation, which may limit deeper penetration but still result in significant surface damage.[18]
Corneal wound healing is a highly coordinated process involving epithelial cell migration, proliferation, and differentiation, as well as stromal remodeling and extracellular matrix deposition. Growth factors such as epidermal growth factor, transforming growth factor-beta, and platelet-derived growth factor play critical roles in modulating this response. However, excessive activation of these pathways may lead to pathological fibrosis and neovascularization, thereby compromising corneal transparency. The balance between regenerative healing and scarring is influenced by factors such as the extent of injury, the presence of infection, and the underlying ocular surface health.[19]
Infectious complications represent a significant concern following corneal trauma, particularly in cases involving organic matter or delayed presentation. Traumatic disruption of the epithelial barrier facilitates microbial invasion, predisposing to bacterial, fungal, and protozoal keratitis. In tropical and agricultural settings, fungal keratitis is especially prevalent, often associated with vegetative injuries. Emerging pathogens such as Pythium insidiosum have further complicated the diagnostic and therapeutic landscape, often mimicking fungal keratitis but demonstrating resistance to conventional antifungal therapy. Early recognition and targeted management are crucial to prevent rapid progression and globe-threatening complications.[20]
The role of the ocular surface microenvironment in determining outcomes following trauma has gained increasing attention. Tear film instability, limbal stem cell deficiency, and preexisting ocular surface disorders such as dry eye disease can significantly impair epithelial healing and increase the risk of complications. The limbal stem cell niche is particularly important in maintaining corneal epithelial integrity; damage to this area from severe chemical burns can lead to conjunctivalization, persistent epithelial defects, and vascularization. Advances in regenerative therapies, including amniotic membrane transplantation (AMT) and limbal stem cell transplantation (LSCT), have shown promise in restoring ocular surface integrity in such cases.[21]
Recent years have witnessed significant advancements in diagnostic modalities for corneal trauma. High-resolution anterior segment optical coherence tomography (AS-OCT) provides detailed visualization of corneal layers, aiding assessment of the depth and extent of injury. In vivo confocal microscopy (IVCM) provides cellular-level imaging, enabling early detection of infectious organisms and assessment of corneal nerve damage. These imaging techniques have enabled clinicians to tailor management strategies and monitor healing progression more effectively.[22]
Therapeutic approaches to corneal trauma have evolved with the advent of novel pharmacologic and surgical interventions. Topical antibiotics remain the mainstay of prophylaxis against infection in epithelial defects, whereas corticosteroids are used judiciously to control inflammation and prevent scarring. Emerging therapies, including matrix metalloproteinase inhibitors, anti-vascular endothelial growth factor (anti-VEGF) agents, and biologics targeting specific inflammatory pathways, are being explored to improve outcomes in severe injuries. Additionally, the use of bandage contact lenses, tissue adhesives, and advanced keratoplasty techniques has expanded the armamentarium for managing complex corneal injuries.[23]
The integration of artificial intelligence (AI) and digital technologies into ophthalmology has opened new avenues for managing corneal trauma. AI-based image analysis systems can assist in the early detection and classification of corneal injuries, supporting timely intervention, particularly in resource-limited settings. Teleophthalmology platforms have also facilitated remote triage and management, improving access to care for patients in underserved regions. These innovations have the potential to reduce the global burden of corneal blindness by enabling earlier diagnosis and optimizing treatment pathways.[24]
Preventive strategies remain a cornerstone in reducing the incidence and impact of corneal trauma. Public health initiatives promoting the use of protective eyewear in high-risk occupations, along with education on the safe handling of chemicals and hazardous materials, are essential for minimizing the risk of injury. Workplace safety regulations and community awareness programs play a vital role in mitigating preventable causes of ocular trauma. Furthermore, early recognition and prompt referral to specialized eye care centers are critical in improving visual outcomes and reducing long-term morbidity. In summary, corneal trauma represents a multifaceted clinical entity with significant implications for vision and quality of life. A comprehensive understanding of its pathophysiology, risk factors, and evolving management strategies is essential for optimizing patient outcomes. Continued research and innovation in diagnostics, therapeutics, and preventive measures are necessary to address the growing global burden of corneal injuries and to improve the standard of care in this challenging field.[23]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Corneal trauma arises from a broad spectrum of mechanical, chemical, thermal, infectious, and iatrogenic causes, each with distinct mechanisms of injury and clinical implications (see Table. Etiological Classification of Corneal Trauma). Understanding the underlying etiology of the injury is essential for accurate diagnosis, risk stratification, and selection of appropriate management strategies. The following sections categorize common causes of corneal injury and highlight key features that inform clinical evaluation and treatment.
Corneal Abrasions and Foreign Bodies
Corneal abrasions and foreign body injuries occur when objects strike or embed within the ocular surface. Common causative objects include fingernails, contact lenses, and plant branches. Certain activities, such as agricultural work, landscaping, and metalwork, also predispose patients to injury from particulate wood, vegetative matter, and metal. In the absence of eye protection, high-speed projectile objects may penetrate through the cornea and create additional serious damage past the initial corneal insult.[15]
Corneal Lacerations and Perforations
Corneal lacerations and perforations can occur under any of the same circumstances as corneal abrasions. However, these injuries more often involve equipment or activities that generate high-speed projectiles, such as saws, angle grinders, and metal-pounding tools. Clinicians should elicit from the history the type of causative object (eg, wood and metal) and its estimated projectile speed.[25]
Ocular Burns
Exposure to chemical substances, ultraviolet light, and excessive heat can alter the surface structure of the cornea and cause ocular burns. Alkali chemical injuries are more common than acidic chemical injuries due to the prevalence of household cleaning agents containing ammonia and lye. Acidic burns are typically work-related insults involving industrial processes, but such burns can also be intentional assaults.[26] Ultraviolet keratitis from radiation burns is associated with tanning beds, high-altitude environments, welding arcs, and the occasional solar eclipse. Thermal burns are distinctly uncommon but can occur with objects such as curling irons, hot liquids, and fire-related injuries.[27]
Infectious and Posttraumatic Etiologies
Trauma to the corneal epithelium significantly increases susceptibility to infectious keratitis by disrupting the natural barrier against microbial invasion. Bacterial pathogens such as Staphylococcus aureus and Pseudomonas aeruginosa are commonly implicated, particularly in contact lens wearers. Fungal infections, particularly those caused by Fusarium and Aspergillus spp, are more commonly associated with vegetative trauma. Protozoal infections, such as Acanthamoeba keratitis, may occur following exposure to contaminated water sources, especially among contact lens users. Emerging organisms such as P insidiosum have been increasingly recognized as significant causes of severe keratitis following trauma, often mimicking fungal infections but requiring distinct therapeutic approaches.[28][29][30]
Iatrogenic and Environmental Factors
Iatrogenic causes of corneal trauma include surgical procedures, improper use of ophthalmic instruments, and complications from refractive surgeries such as laser-assisted in situ keratomileusis (LASIK) or photorefractive keratectomy. Inadequate lubrication during surgery or postoperative epithelial defects can predispose to delayed healing and secondary infection. Environmental factors such as air pollution, occupational chemical exposure, and UV radiation can exacerbate corneal injury or delay healing. Chronic exposure to particulate matter may lead to repeated microtrauma and inflammation, further compromising ocular surface integrity.[31]
Table 1. Etiological Classification of Corneal Trauma
|
Category |
Mechanism |
Common Sources |
Risk Factors |
Key Clinical Concerns |
|
Mechanical (abrasions and FB) |
Direct epithelial disruption |
Fingernails, contact lenses, plant material, and metal particles |
Agriculture, construction, and poor eye protection |
Infection, recurrent erosion, and rust ring |
|
Penetrating trauma |
Full-thickness corneal breach |
High-speed projectiles, tools, and industrial accidents |
Metalwork and lack of protective gear |
Open globe, IOFB, and endophthalmitis |
|
Blunt trauma |
Compression and shockwave injury |
Sports injuries and motor vehicle accidents |
Contact sports and road trauma |
Edema, Descemet tears, and endothelial loss |
|
Chemical burns |
Tissue destruction via chemical reactions |
Alkali (ammonia and lime) and acids |
Household or industrial exposure |
Limbal stem cell damage and scarring |
|
Thermal burns |
Heat-induced protein denaturation |
Hot liquids, fire, and heated tools |
Domestic or occupational exposure |
Surface necrosis and epithelial loss |
|
Radiation (UV) |
DNA damage to epithelial cells |
Welding arcs, sunlight, and tanning beds |
Outdoor work and inadequate eye protection |
Photokeratitis and delayed symptoms |
|
Posttraumatic infectious |
Microbial invasion post-epithelial breach |
Bacteria, fungi, protozoa, and Pythium |
Contact lens use and vegetative injury |
Keratitis and corneal melt |
|
Iatrogenic |
Procedure-related injury |
Surgery and diagnostic tools |
Refractive surgery and poor technique |
Epithelial defects and delayed healing |
|
Environmental |
Chronic microtrauma or inflammation |
Dust, pollutants, and UV exposure |
Occupational hazards |
Chronic surface damage |
Abbreviations: FB, foreign body; IOFB, intraocular foreign body.
Epidemiology
Recent global studies estimate that nearly 60 million eye injuries occur annually (see Table. Global Epidemiologic Patterns of Corneal Trauma).[1][2] Over the past 3 decades, the number of incident cases increased by 24%.[1] Unintentional trauma was the leading cause of eye injuries worldwide, followed by self-harm, assault, and transportation accidents. According to the Global Burden of Diseases, Injuries, and Risk Factors Study, the most common causes of unintentional eye trauma were foreign bodies, mechanical forces, and falls. Males in each age group were more likely than females to experience ocular trauma. Both male and female adults aged 25 to 49 had the highest years lived with disability rates of any age group.[1]
The highest total number of eye injuries occurred in South Asia and East Asia, whereas the highest eye injury burden was found in Australasia. Increasing eye injuries from conflict and terrorism were found in Eastern Europe, the Middle East, and North Africa. Rates of foreign-body eye injuries increased in Southeast Asia, sub-Saharan Africa, and Europe. West sub-Saharan Africa and North America had higher rates of eye injury due to self-harm than in previous decades.[1]
Similar patterns exist in childhood eye injury. Most eye trauma is unintentional, with the highest incidence in India and the highest injury burden in Australasia. Male adolescents aged 15 to 19 had the highest risk of injury.[5] Timely intervention and treatment are especially important in children because of the ongoing development of visual processing pathways and the risk of amblyopia.[32]
In England and Wales, corneal trauma accompanies 6.6% of major trauma cases with ophthalmic findings.[3] In the United States, ocular trauma contributes to 2.4 million annual emergency department visits.[33] Superficial ocular injuries accounted for 44%, and external ocular foreign bodies accounted for 16% of the total ocular trauma emergency visits over 10 years.[34] Ophthalmic trauma was also slightly more common in emergency departments in the southern US.[34]
Ocular chemical burns are an emergency, accounting for 11.5% to 22.1% of all ocular injuries.[35] Haring et al found that young children in the United States were the highest-risk individual group for ocular chemical burns, with ages 1 to 2 years at greatest risk.[36] Generally, ocular chemical injuries occur in individuals aged 18 to 64; they are the second most common cause of workplace ocular injuries after ocular foreign bodies.[37][38] Further epidemiologic information on ocular burns remains sparse. A recent study in the United States indicates that ocular burns may affect males and females at similar rates and at older ages than previously documented (mean ages of 45 and 52, respectively). The prevalence of ocular burn cases also increased by 20% during the study period.[39]
Beyond global estimates, regional epidemiologic variability in corneal trauma is strongly influenced by occupational exposure, socioeconomic factors, and access to eye care services. Low- and middle-income countries bear a disproportionately higher burden of ocular trauma due to increased involvement in high-risk occupations such as agriculture, construction, and manual labor. In these regions, delayed presentation and limited access to specialized ophthalmic care contribute significantly to poor visual outcomes.[40]
Occupational ocular trauma accounts for a substantial proportion of cases worldwide, with studies suggesting that up to 70% of eye injuries in certain populations are work-related. Lack of protective eyewear remains a critical modifiable risk factor, particularly in industrial and agricultural settings. In high-resource countries, although workplace safety regulations have reduced the incidence of severe injuries, recreational and sports-related trauma has emerged as a significant contributor.[15] Seasonal variation in ocular trauma has also been reported, with higher incidence rates during harvesting seasons and warmer months, particularly in agrarian societies. This pattern is attributed to increased outdoor activity and exposure to vegetative matter, which also correlates with a higher incidence of fungal keratitis following trauma.
Pediatric ocular trauma demonstrates distinct epidemiological trends compared to adults. In children, common causes include household injuries, school-related accidents, and sports activities, whereas occupational exposure is the predominant cause among adults. Boys are consistently reported to have a higher incidence of ocular trauma than girls, likely due to behavioral and activity-related differences. Importantly, visual outcomes in children are often worse due to delayed diagnosis and the risk of amblyopia development following corneal injury.[40]
Geriatric populations represent another at-risk group, with falls being a leading cause of ocular trauma. Age-related factors such as reduced visual acuity, impaired coordination, and systemic comorbidities contribute to increased susceptibility. Additionally, older patients may experience poorer healing responses due to reduced corneal regenerative capacity.
Contact lens–associated trauma has become increasingly relevant in modern epidemiology, particularly in urban populations. Improper hygiene practices, extended wear, and exposure to contaminated water sources significantly increase the risk of corneal abrasions and subsequent microbial keratitis. This category represents a preventable cause of vision-threatening complications with appropriate patient education.[41]
Emerging trends also highlight the increasing role of environmental and behavioral risk factors, including air pollution, UV exposure, and digital device–related eye strain, which may predispose individuals to ocular surface compromise and increase susceptibility to trauma. Climate change and increasing environmental hazards may further influence the epidemiology of ocular trauma, particularly in regions prone to extreme weather conditions.[42]
Table 2. Global Epidemiologic Patterns of Corneal Trauma
|
Parameter |
Key Findings |
High-Risk Groups |
Regional Trends |
Clinical Implication |
|
Global burden |
~60 million eye injuries annually |
All age groups |
Increasing trend over decades |
Major public health issue |
|
Gender distribution |
Male predominance |
Young adult males |
Universal pattern |
Occupational exposure link |
|
Age distribution |
Peak: 25 to 49 years |
Working population |
Global |
Economic burden |
|
Pediatric trauma |
High in adolescents |
Boys > girls |
India, Asia |
Risk of amblyopia |
|
Occupational trauma |
Up to 70% in some regions |
Laborers and farmers |
LMICs |
Preventable with PPE |
|
Chemical burns |
11% to 22% of injuries |
Workers and children |
Industrial regions |
Emergency management |
|
Sports or recreational |
Increasing trend |
Young adults |
Developed countries |
Need for eye protection |
|
Elderly trauma |
Fall-related injuries |
>60 years |
Global |
Poor healing outcomes |
|
Contact lens–related |
Rising incidence |
Urban population |
Developed regions |
Preventable infections |
|
Seasonal variation |
Peaks in harvest/summer |
Agricultural workers |
Tropical regions |
Fungal keratitis risk |
Abbreviations: LMICs, lower- and middle-income countries; PPE, personal protective equipment.
Pathophysiology
Corneal Injury
The corneal epithelium is avascular, fragile, and richly innervated. Therefore, any injury in an otherwise healthy cornea is very painful. In superficial injury, the epithelium regenerates quickly, with most abrasions healing within 24 to 48 hours.[43] For alcohol-related injuries, the de-epithelialization of the ocular surface typically heals without further sequelae.
In cases of chemical eye injuries, the extent of damage varies depending on the substance involved. Acids cause tissue proteins to bind and get neutralized, leading to coagulation and tissue necrosis. Theoretically, this coagulation acts as a barrier to further acid penetration and damage.[43] One notable anomaly is hydrofluoric acid, commonly used in glasswork and metal refinement. Here, dissociated fluoride ions can quickly traverse the cornea and enter deeper ocular structures.[44]
Alkali ocular injuries are more prevalent and cause hydrophilic and lipophilic degeneration. The fatty acids of cellular membranes undergo saponification upon contact with alkalis. Unlike acid exposure, saponification allows rapid penetration of alkali into epithelial cells and eventual release of proteolytic enzymes, making the involved tissue more susceptible to enzymatic degradation and damage.[43] Rapid tissue damage to the trabecular meshwork and aqueous outflow in the early injury phase, and subsequent inflammation and adhesions in later phases, can all contribute to elevated intraocular pressure (IOP).[45]
Corneal Healing
Superficial corneal healing requires corneal epithelium regeneration via cellular migration, proliferation, and differentiation as well as extracellular matrix remodeling. Limbal stem cells migrate and differentiate to cover the defect with a single layer of epithelial cells. Proliferation from the basal layer restores the normal thickness of the epithelium. The healing response to a corneal abrasion depends on the size and depth of the defect. Larger abrasions require greater cellular migration and proliferation, and the restoration of normal adhesions can take up to 6 weeks.[43] Recurrent corneal erosion (RCE) can occur over time if the process is incomplete.
For deeper injuries involving the corneal stroma, healing requires keratocytes to transform into fibroblasts and myofibroblasts, which can lead to corneal opacification and scarring. Extensive chemical injuries initiate a similar cascade of inflammation, oxidative stress, and neovascularization, creating fibrosis.[45] These modifications compromise the cornea's optical clarity and can significantly affect vision.
Beyond the immediate structural disruption, corneal injury initiates a complex neuroinflammatory cascade mediated by corneal nerves and resident immune cells. Injury-induced release of neuropeptides such as substance P and calcitonin gene-related peptide amplifies local inflammation and modulates nociceptive signaling and epithelial healing. This neurogenic inflammation plays a critical role in both acute pain and subsequent tissue repair.
The innate immune response is rapidly activated following corneal trauma, with epithelial cells and keratocytes releasing cytokines such as interleukin-1 and tumor necrosis factor-alpha, as well as chemokines that recruit neutrophils and macrophages to the site of injury. While this response is essential for debris clearance and microbial defense, excessive or prolonged inflammation can result in stromal degradation and delayed epithelial healing.[46]
Matrix metalloproteinases (MMPs), particularly MMP-9, are significantly upregulated after corneal injury and play a key role in extracellular matrix remodeling. Dysregulation of MMP activity may lead to corneal melting and ulceration, especially in severe trauma or secondary infections. Concurrently, oxidative stress induced by reactive oxygen species contributes to cellular apoptosis and further tissue damage.
Corneal nerve injury is another important component of pathophysiology, often resulting in reduced corneal sensitivity and impaired epithelial healing. Damage to the subbasal nerve plexus can lead to neurotrophic keratopathy, characterized by persistent epithelial defects and increased risk of ulceration. The regeneration of corneal nerves is a slow process and may be incomplete in severe injuries.[47]
In cases of limbal involvement, damage to limbal stem cells disrupts the normal homeostasis of the corneal epithelium, resulting in conjunctivalization of the corneal surface, vascular ingrowth, and chronic epithelial instability. The severity of limbal stem cell deficiency directly correlates with the extent of chemical or thermal injury. Endothelial cell injuries, although less common in superficial trauma, can have profound consequences due to the limited regenerative capacity of these cells. Loss of endothelial function leads to stromal edema and loss of corneal transparency, which may necessitate surgical intervention such as endothelial keratoplasty.[48]
Additionally, posttraumatic angiogenic signaling mediated by VEGF promotes corneal neovascularization. Neovascularization not only impairs corneal clarity but also increases the risk of graft rejection in future corneal transplantation. This effect is particularly pronounced in cases of chronic inflammation or hypoxia.
Finally, aberrant wound healing responses may lead to fibrosis and permanent stromal scarring through myofibroblast activation and disorganized collagen deposition. These structural alterations result in irregular astigmatism and reduced visual acuity, representing a major cause of long-term visual morbidity following corneal trauma.[49] Together, these pathophysiologic processes underscore the importance of timely and targeted intervention to preserve corneal integrity and visual function.
Histopathology
Corneal trauma induces distinct histopathological changes that vary according to the depth, mechanism, and chronicity of injury, affecting all layers of the cornea, including the epithelium, Bowman layer, stroma, Descemet membrane, and endothelium. The earliest microscopic changes are typically observed in the epithelium, where cellular loss, disruption of tight junctions, and intercellular edema occur following mechanical or chemical insult. In superficial injuries, epithelial cells demonstrate increased mitotic activity with migration of basal epithelial cells to cover the defect, often accompanied by loss of hemidesmosomal attachments and basement membrane irregularities. Electron microscopy studies have shown cytoplasmic vacuolization and microvillar disruption in damaged epithelial cells, reflecting impaired barrier function (see Image. Pathophysiology and Histopathologic Changes in Corneal Trauma).[43]
The Bowman layer, once disrupted, does not regenerate and is replaced by fibrous scar tissue, leading to permanent structural alteration and light scattering. This acellular layer acts as a critical barrier, and its damage contributes significantly to long-term corneal opacity. Stromal involvement is characterized by activation of quiescent keratocytes into fibroblasts and myofibroblasts, which produce a disorganized extracellular matrix, including type III collagen and fibronectin. These cells are responsible for stromal fibrosis and haze formation by depositing opaque scar tissue. Inflammatory cell infiltration, predominantly neutrophils and macrophages, is commonly observed during the acute phase, particularly in contaminated or infected trauma.[50]
In chemical injuries, histopathological examination reveals widespread stromal necrosis, collagen degradation, and loss of keratocytes, particularly in alkali burns, where rapid penetration leads to diffuse tissue destruction. Acid injuries, although more localized, demonstrate coagulative necrosis with preservation of deeper structures in early stages. Severe burns may also lead to limbal ischemia, resulting in depletion of limbal stem cells and subsequent conjunctivalization of the corneal surface.
Neovascularization is a hallmark of chronic corneal injury and is characterized by the ingrowth of new blood vessels from the limbus into the normally avascular corneal stroma. Histologically, neovascularization is associated with increased expression of angiogenic factors such as VEGF and inflammatory mediators. These vessels disrupt corneal transparency and increase the risk of lipid deposition and graft rejection in future keratoplasty.[45]
The Descemet membrane may show folds, ruptures, or detachment in cases of blunt trauma or severe edema, often accompanied by endothelial cell loss. Endothelial damage is particularly significant because these cells have limited regenerative capacity, and their loss leads to stromal hydration and corneal edema. Persistent endothelial dysfunction may culminate in bullous keratopathy. Corneal nerve alterations are also evident histologically, with reduced density and fragmentation of the subbasal nerve plexus following trauma. These changes contribute to decreased corneal sensitivity and impaired epithelial healing, especially when it progresses to neurotrophic keratopathy.[51]
In cases complicated by infection, histopathology may reveal organism-specific features such as fungal hyphae within the stroma, bacterial colonies, or cyst forms in protozoal infections. In P insidiosum keratitis, characteristic sparsely septate hyphae-like structures with surrounding inflammatory infiltrates may be observed, often mimicking fungal morphology but lacking chitin in the cell wall. Chronic or poorly healed injuries may demonstrate epithelial hyperplasia, stromal thinning, and persistent inflammatory cell presence, reflecting ongoing tissue remodeling and failed resolution of injury. These histopathological changes correlate clinically with persistent epithelial defects, scarring, and visual impairment.[52]
Toxicokinetics
The toxicokinetics of ocular surface injuries primarily depend on the nature of the offending agent, namely its chemical properties, concentration, and duration of exposure, which determine the rate of penetration and extent of tissue damage. Lipophilic substances penetrate the corneal epithelium more rapidly due to disruption of cellular membranes, whereas hydrophilic agents tend to remain more superficial unless epithelial integrity is compromised. Alkali substances rapidly diffuse through the cornea by saponifying membrane lipids and denaturing stromal collagen, thereby penetrating the anterior chamber within minutes. This process facilitates the release of hydroxyl ions, which induce cellular necrosis, proteoglycan degradation, and activation of proteolytic enzymes.[27]
Acidic agents, in contrast, cause protein coagulation at the epithelial and stromal levels, forming a barrier that limits deeper penetration, although strong acids such as hydrofluoric acid can bypass this mechanism due to its lipophilic fluoride ions. UV radiation causes direct DNA damage in epithelial cells via the formation of pyrimidine dimers, leading to apoptosis and delayed epithelial desquamation. Thermal injuries induce protein denaturation and coagulative necrosis, primarily affecting the superficial layers, with the extent depending on the intensity of exposure. Toxic substances also disrupt tear film stability and alter ocular surface pH, further impairing epithelial barrier function and facilitating the progression of secondary inflammation and injury.[53]
History and Physical
A systematic history and a thorough physical examination are essential for accurately characterizing corneal trauma, identifying high-risk features, and guiding timely management. Particular attention should be given to the mechanism of injury, symptom onset and progression, and associated risk factors, as these elements help differentiate superficial injuries from vision-threatening pathology. The following subsections outline key components of the clinical evaluation.
History
A focused ocular history is critical for elucidating the mechanism of injury and identifying risk factors for complications (see Table. Key Historical Clues and Their Clinical Significance). Patients with small corneal abrasions are most likely to report eye pain or a foreign-body sensation. In these cases, presentation can be delayed for several hours after the inciting event. Healthcare practitioners should ask about the circumstances under which the injury occurred and specifically about the use of high-speed machinery and metalworking, as these injuries are more often associated with corneal laceration and globe perforation. A history of eye pain following metal-on-metal hammering suggests a metal projectile as the cause of the ocular injury, and the possibility of globe rupture should be thoroughly investigated. Patients with radiation and thermal corneal burns typically present with a history of exposure in a susceptible environment. For example, eye pain following welding without a welder's shield and eye pain following a house fire are suggestive of radiation burns and thermal burns, respectively.[54]
Patients with chemical ocular injuries are more likely to present immediately. For these ocular burns, identification of the chemical to which the eye was exposed is extremely important, as treatment and prognosis vary significantly depending on the offending agent. Clinicians should also ask if the patient ingested or inhaled any chemical substances, as respiratory passage edema can lead to asphyxiation. Unless an open globe injury is suspected, emergency treatment of potential chemical burns must begin immediately before proceeding with the typical ocular examination, including the deferral of visual acuity testing.[55]
A detailed history should also assess the interval between injury and presentation, as delayed presentation is associated with an increased risk of infection, stromal involvement, and poor visual outcomes. The nature of symptom progression, including worsening pain, decreased vision, or discharge, may indicate secondary complications such as infectious keratitis. Clinicians should inquire about contact lens use, including hygiene practices, overnight wear, and exposure to water sources, as these significantly increase the risk of microbial keratitis following trauma. A history of previous ocular surface disease, including dry eye, blepharitis, or prior trauma, may impair epithelial healing and predispose to recurrent erosions.[56]
Medication history is essential, particularly the use of topical corticosteroids or anesthetics, which may mask symptoms, delay healing, and increase the risk of corneal melting. Occupational history should be expanded to include the use or absence of protective eyewear, duration of exposure, and prior similar injuries. In pediatric and elderly populations, additional history should include the mechanism of injury (accidental versus non-accidental trauma) and functional status, as these groups may present atypically or with delayed symptoms.[57]
Physical Examination
A thorough physical examination is essential to confirm the diagnosis, assess injury severity, and identify associated ocular or adnexal involvement. A comprehensive ocular examination should begin with a visual acuity assessment unless contraindicated, as in chemical injuries requiring immediate irrigation. External inspection should evaluate for periocular edema, lid lacerations, and adnexal injuries, which may coexist with corneal trauma. Slit-lamp examination remains the cornerstone of evaluation (see Table. Slit-Lamp Findings and Diagnostic Correlation). Clinicians should assess for:
- Epithelial defects using fluorescein staining
- Depth of stromal involvement
- Presence of foreign bodies or rust rings
- Anterior chamber reaction (cells, flare, and hypopyon) [25]
Corneal staining patterns provide critical diagnostic clues, including linear abrasions, which suggest a foreign body under the lid, and diffuse punctate staining, which suggests a toxic or radiation injury. A positive Seidel test indicates aqueous leakage and confirms corneal perforation. IOP measurement should be performed cautiously and avoided in suspected open globe injuries. Pupillary examination may reveal afferent pupillary defects, suggesting deeper ocular involvement. Fundus examination, when feasible, helps identify posterior segment involvement, particularly in high-velocity injuries. If visualization is limited, B-scan ultrasonography may be considered, provided globe rupture is excluded.[53]
Red Flag Features (Must Not Miss)
- Sudden decrease in vision → Possible globe rupture
- Severe pain with minimal findings → Neurotrophic or early infection
- History of metal-on-metal injury → Intraocular foreign body (IOFB)
- Chemical exposure → Immediate irrigation required
- Contact lens use → Risk of Pseudomonas keratitis [12]
Table 3. Key Historical Clues and Their Clinical Significance
|
History Feature |
Likely Etiology |
Clinical Implication |
|
Metal-on-metal injury |
High-velocity projectile |
Risk of intraocular foreign body and globe rupture |
|
Contact lens wear |
Microbial keratitis |
Pseudomonas and Acanthamoeba risk |
|
Vegetative trauma |
Fungal or Pythium keratitis |
Delayed infection |
|
Chemical exposure |
Alkali or acid burn |
Emergency irrigation |
|
Welding exposure |
UV keratitis |
Delayed epithelial damage |
|
Fire or heat exposure |
Thermal burn |
Surface necrosis |
|
Recurrent symptoms |
Recurrent erosion |
Basement membrane defect |
Table 4. Slit-Lamp Findings and Diagnostic Correlation
|
Clinical Finding |
Interpretation |
Next Step |
|
Fluorescein uptake |
Epithelial defect |
Size or depth assessment |
|
Linear abrasion |
Foreign body under lid |
Lid eversion |
|
Rust ring |
Metallic foreign body |
Removal |
|
Stromal haze |
Deeper injury |
Close monitoring |
|
Hypopyon |
Infection or inflammation |
Urgent treatment |
|
Positive Seidel test |
Corneal perforation |
Emergency referral |
|
Decreased corneal sensation |
Neurotrophic keratopathy |
Specialized management |
Evaluation
Traumatic Corneal Abrasions
Gross examination may reveal conjunctival erythema, lid swelling, tearing, and blepharospasm. Visual acuity is considered the vital sign of the eye and should be determined in every patient with an ocular complaint. If the patient wears corrective lenses, acuity should be assessed with the lenses in place. Best corrected visual acuity is typically normal in the setting of corneal abrasions, except in the case of an associated iritis or corneal defect in the central visual axis. The corneal defect can often be visualized under magnification, even without fluorescein. In the event of severe pain, a topical anesthetic may be necessary to obtain a complete ocular examination. Pain relief with a topical anesthetic such as proparacaine strongly suggests a superficial (corneal) etiology of ocular pain. Fluorescein staining followed by examination under cobalt blue illumination highlights the corneal abrasion as a bright green, superficial defect of the cornea.[58][59][60][61]
Corneal Foreign Bodies
As with corneal abrasions, patients usually experience pain, foreign-body sensation, tearing, and blepharospasm. Likewise, application of a topical anesthetic often aids in slit lamp examination and diagnosis. Ocular foreign bodies may lodge beneath the upper eyelid and cause repeated corneal abrasions with each blink. The resulting corneal injury may appear as numerous vertical or curvilinear abrasions. The upper eyelid should be everted and examined for foreign bodies when a corneal or conjunctival foreign body is suspected. In the setting of a metallic foreign body, a rust ring generally forms in the surrounding cornea within several hours.
If the patient's history suggests a high-velocity projectile, special attention should be given to rule out a possible globe rupture with an IOFB.[62] Signs on examination of an IOFB include a positive Seidel test (described below), iris transillumination defects, anterior chamber inflammation, and the presence of a traumatic cataract. In the presence of these indicators, a hard shield should be placed over the eye, an orbital computed tomography (CT) scan should be obtained, and a referral to ophthalmology should be made for further evaluation.
Corneal Laceration or Perforation
Clinicians must evaluate the entire cornea with a slit lamp. Signs that suggest a full-thickness corneal laceration or perforation include a misshapen iris or irregular pupil, hyphema, microhyphema, decreased visual acuity, and a shallow anterior chamber compared to the fellow eye. Aqueous humor leaking from the anterior chamber during fluorescein examination indicates a corneal perforation (Seidel test). For small lacerations, the Seidel test can be negative with grossly normal-appearing ocular anatomy. Therefore, a high index of suspicion for globe penetration should be maintained, and a CT of the orbit should be obtained when the history or physical examination suggests the possibility of such an injury. While fairly accurate, CT is an imperfect diagnostic test. Consequently, an ophthalmology consultation is recommended in situations with a very high index of suspicion, even when the orbital CT is unremarkable.[16]
If a full-thickness traumatic corneal laceration or perforation is suspected, the eye should be treated as a potential ruptured globe. Further manipulation of the eye at the slit lamp should be avoided to prevent additional extrusion of ocular contents. Instead, a hard shield should be placed over the eye, and further physical examination can be performed in the operating room. If not treated promptly, the long-term sequelae of a full-thickness corneal laceration or perforation include permanent hypotony, ciliary body shutdown, and phthisis bulbi.[40]
Ocular Burns
Chemical burns to the eye are ocular emergencies due to the risk of scarring and permanent vision loss. Irrigation of the eyes and removal of any chemical substances must be performed immediately, before any evaluation or examination, including visual acuity testing. Once neutral pH is achieved, bilateral visual acuity and IOP should be documented. IOP may be measured more effectively with a Tonopen than with applanation tonometry, especially in cases of corneal distortion. Clinicians must also ascertain whether the patient has inhaled or ingested any chemical substance and assess for signs of respiratory compromise.[63]
Mild to moderate chemical burns may present with superficial punctate keratopathy on fluorescein staining, sloughing of the corneal epithelium, chemosis (mild to moderate), hyperemia, subconjunctival hemorrhage, anterior chamber reaction (mild to moderate), and first- or second-degree burns to the eyelids and surrounding skin. Significant perilimbal ischemia, defined by blanching of the surrounding conjunctival and episcleral vessels, should be absent.[64]
In contrast, severe chemical burns present with conjunctival blanching, significant chemosis, and an edematous, often opaque cornea. A significant anterior chamber reaction may be present, but it may be difficult to appreciate if the cornea is cloudy. IOP may be elevated, and necrotic retinopathy may be present if chemicals have penetrated the sclera. Second- or third-degree burns are often accompanied by damage to the surrounding tissue. Grading systems can be used to assess ocular ischemic damage and visual prognosis.[65]
Patients with radiation burns and photokeratitis are typically in severe pain and discomfort. On examination, superficial punctate keratopathy, decreased vision, tearing, and chemosis are often present. In all cases of chemical ocular burn, once the pH has been neutralized, prompt ophthalmologic follow-up is essential for further care and management.
Advanced Diagnostic Modalities
Beyond slit-lamp examination, AS-OCT provides high-resolution cross-sectional imaging of the cornea and is particularly useful in assessing the depth of corneal lacerations, detecting Descemet membrane detachment, and identifying occult perforations. AS-OCT is especially valuable in cases where corneal edema or opacity limits direct visualization.
IVCM enables cellular-level evaluation of the cornea and is particularly useful for identifying infectious etiologies (eg, fungal filaments and Acanthamoeba cysts) in posttraumatic keratitis. IVCM also aids in assessing corneal nerve damage and inflammatory cell infiltration. This modality may facilitate earlier diagnosis and targeted therapy in cases where conventional diagnostic methods are inconclusive.
Ultrasound biomicroscopy can be employed when anterior segment structures are obscured, allowing evaluation of anterior chamber depth, angle structures, and intraocular foreign bodies.[66] This modality is particularly useful when direct visualization is limited or contraindicated and intraocular extension of the injury is suspected. Together, these advanced imaging modalities complement clinical examination by refining diagnostic accuracy and guiding management decisions in complex cases of corneal trauma (see Table. Diagnostic Modalities in Corneal Trauma).
Microbiological and Laboratory Evaluation
In cases of suspected infectious keratitis following trauma, corneal scraping for microbiological analysis is essential (see Table. Microbiological Workup in Posttraumatic Keratitis). Samples should be examined using:
- Gram stain for bacterial pathogens
- Potassium hydroxide mount for fungal elements
- Giemsa stain for cellular morphology
Culture media, including blood agar, chocolate agar, and Sabouraud dextrose agar, are used to isolate causative organisms. Advanced diagnostic techniques such as polymerase chain reaction and next-generation sequencing have improved the detection of atypical organisms, including P insidiosum. Tear film analysis and inflammatory markers may be considered in chronic or non-healing cases to evaluate underlying ocular surface dysfunction.[67]
Radiologic Evaluation
Orbital CT remains the imaging modality of choice in suspected IOFBs or orbital fractures, particularly for detecting metallic foreign bodies. CT has high sensitivity for radiopaque objects but may miss small or non-metallic foreign bodies. Magnetic resonance imaging is contraindicated in suspected metallic foreign bodies due to the risk of migration and further tissue damage. However, magnetic resonance imaging may be considered in select cases of non-metallic foreign bodies when CT findings are inconclusive.[68]
Functional and Adjunctive Testing
- Corneal sensitivity testing: Useful in identifying neurotrophic keratopathy following trauma; performed with a cotton wisp or esthesiometer. Reduced corneal sensation is associated with delayed epithelial healing and increased risk of ulceration.
- Tear film assessment (including tear breakup time and Schirmer testing): May be helpful in patients with persistent epithelial defects or chronic ocular surface instability
- Specular microscopy: Can evaluate endothelial cell density and morphology, particularly in cases with suspected endothelial damage or corneal edema.[69]
Guideline-Based Evaluation (National and International)
- American Academy of Ophthalmology: Recommends immediate assessment of visual acuity, a slit-lamp examination, and prompt imaging in cases of suspected open-globe injuries.
- Royal College of Ophthalmologists: Emphasizes urgent irrigation for chemical injuries before any diagnostic evaluation and the use of early grading systems such as the Roper-Hall or Dua classification.
- World Health Organization: Highlights early identification and referral of ocular trauma cases as critical in preventing long-term visual impairment, particularly in low-resource settings.[70]
Table 5. Diagnostic Modalities in Corneal Trauma
|
Modality |
Indication |
Advantage |
Limitation |
|
Slit-lamp + fluorescein |
Initial evaluation |
Widely available, rapid |
Limited in severe edema |
|
AS-OCT |
Depth assessment and DM detachment |
Noninvasive, high-resolution |
Limited availability |
|
IVCM |
Infectious keratitis |
Cellular-level detail |
Operator-dependent |
|
Orbital CT |
IOFB and fractures |
Detects metallic FB |
Misses organic FB |
|
UBM |
Anterior segment evaluation |
Useful in an opaque cornea |
Requires expertise |
|
Specular microscopy |
Endothelial damage |
Quantitative analysis |
Limited in acute trauma |
Abbreviations: AS-OCT, anterior segment optical coherence tomography; CT, computed tomography; DM, Descemet membrane; FB, foreign body; IOFB, intraocular foreign body; IVCM, in vivo confocal microscopy; UBM, ultrasound biomicroscopy.
Table 6. Microbiological Workup in Posttraumatic Keratitis
|
Test |
Target |
Clinical Utility |
|
Gram stain |
Bacteria |
Rapid diagnosis |
|
KOH mount |
Fungi |
Early fungal detection |
|
Giemsa stain |
Cells or protozoa |
Inflammatory profile |
|
Culture (agar media) |
All organisms |
Gold standard |
|
PCR |
Bacteria, fungi, or Pythium |
High sensitivity |
|
NGS |
Rare pathogens |
Advanced diagnosis |
Abbreviations: KOH, potassium hydroxide; NGS, next-generation sequencing; PCR, polymerase chain reaction.
Treatment / Management
Management of corneal trauma is guided by the type, depth, and severity of injury, with priorities focused on preserving ocular integrity, preventing infection, and promoting epithelial healing. Early recognition of vision-threatening conditions, such as globe perforation and severe chemical burns, is critical, as these require immediate intervention and specialist involvement. Treatment strategies range from supportive care for minor injuries to advanced medical and surgical therapies for more complex presentations, often necessitating coordinated care across an interprofessional team (see Table. Stepwise Management Approach in Corneal Trauma).
Traumatic Corneal Abrasions
The majority of corneal abrasions heal spontaneously; thus, treatment consists primarily of pain control and infection prevention. Loose or hanging epithelium can be debrided at the slit lamp to aid in healing. Large epithelial defects should be measured on initial examination and monitored for improvement. For abrasions greater than 2 mm, or for those that are very painful, a cycloplegic agent such as cyclopentolate 1% or homatropine 5% can help control discomfort by relaxing the ciliary body and relieving pain from ciliary spasm. The cycloplegia of both these agents lasts approximately 24 hours, so a single administration at the time of care should be adequate. In the event of coexisting traumatic iritis, cyclopentolate can be prescribed for several days.
Although topical anesthetics are useful for patient examination, they should not be prescribed for corneal abrasion treatment, even as a temporary measure.[71] First, the efficacy of topical anesthetics in long-term outcomes (eg, epithelial healing) is unclear.[72] Second, the adverse effects of topical anesthetic use can be severe. Continual use of topical ocular anesthetics can inhibit corneal healing, impair the protective blinking reflex, and obscure the identification of pathological progression or additional complications. Miller et al describe the persistence of ocular complications following the use of prescribed topical anesthetics in the days after the initial evaluation.[73] Symptoms of prolonged anesthetic use include increased vision loss, ring infiltrates, eye redness, and corneal ulceration.[74] Some patients can also develop topical anesthetic abuse syndrome, which can lead to corneal perforation and phthisis bulbi.[75](A1)
Although 2 recent reviews have challenged the routine use of antibiotics in corneal abrasions, antibiotic prophylaxis remains widely practiced.[76][77] In cases unrelated to contact lens wear, fingernails, or vegetative matter, erythromycin ophthalmic ointment or polymyxin B sulfate/trimethoprim drops are suitable choices. Corneal abrasions involving organic matter (eg, wood, fingernails, plant material, and animal material) carry a higher risk of infection and complications.[78] In these cases, broader coverage with fluoroquinolones is appropriate [Gervasio KA, Peck TJ, Fathy CA, et al. The Wills Eye Manual. 8th ed. Wolters Kluwer; 2022]. Similarly, contact lens–related abrasions require antipseudomonal coverage, as contact lens use is associated with increased risk of infectious keratitis [Gervasio KA, Peck TJ, Fathy CA, et al. The Wills Eye Manual. 8th ed. Wolters Kluwer; 2022]. Patients should be counseled not to wear contact lenses until the abrasion has completely healed. If necessary, tetanus prophylaxis should also be administered. Corneal abrasions should be reevaluated within 24 to 48 hours of presentation to ensure complete resolution.(A1)
Corneal Foreign Bodies
Nonperforating superficial corneal foreign bodies should be removed at the time of diagnosis. Removal is preferably performed under slit-lamp magnification once anesthesia has been achieved with a topical anesthetic such as proparacaine 0.5%. Occasionally, a cotton applicator may be effective in removing a foreign body. Often, a sterile needle or an ophthalmic corneal burr is necessary.[79] Following foreign body removal, the remaining corneal defect should be managed as a corneal abrasion. In these cases, antibiotic prophylaxis is prudent given the higher likelihood of microbial contamination.[80] (B3)
Inert foreign bodies, such as glass or plastic, can be closely observed. Metallic foreign bodies should be removed to minimize oxidative damage. If a residual rust ring remains after removal of a metallic foreign body, rust removal can either be attempted at the initial visit or deferred to an ophthalmologist for removal the following day. Small rust rings outside the visual axis can be eliminated in stages.
Corneal scarring may follow removal of a foreign body and rust. Therefore, referral to an ophthalmologist should be considered, especially in cases involving the central visual axis. Similarly, deeper corneal foreign bodies, or those with signs of inflammation or infection, should be referred to an ophthalmologist for further evaluation and management.
Complex corneal foreign bodies may benefit from AS-OCT to determine the depth and extent of injury.[81] If the clinician has any suspicion that the foreign body traveled through the full thickness of the cornea, foreign body removal at the slit lamp should not be performed, and the injury should be treated as a globe perforation. Ophthalmology should be consulted immediately.(B3)
Corneal Laceration or Perforation
Partial-thickness corneal lacerations with gaping wound edges should be sutured in the operating room to minimize scarring and optimize restoration of corneal curvature. However, partial-thickness corneal lacerations associated with a shallower anterior chamber compared to the contralateral eye may actually represent full-thickness corneal lacerations that have self-sealed. [Gervasio KA, Peck TJ, Fathy CA, et al. The Wills Eye Manual. 8th ed. Wolters Kluwer; 2022]. Unrecognized corneal perforations and full-thickness corneal lacerations can quickly result in endophthalmitis or traumatic cataract. Therefore, both conditions should be treated as globe ruptures with the placement of a protective eye shield to prevent accidental pressure on the globe, and broad-spectrum intravenous antibiotics should be administered to cover common organisms that cause posttraumatic endophthalmitis. Vancomycin and ceftazadime, or a second- or fourth-generation fluoroquinolone, are appropriate.[82] Moderate evidence suggests that oral antibiotics are noninferior to intravenous antibiotics.[82] Antiemetics are commonly administered to prevent increases in IOP. In the context of traumatic injury, a CT orbit may be indicated to rule out other orbital injuries or retained IOFBs. Ruptured globes and the potential complication of endophthalmitis are ophthalmic emergencies and require intraoperative surgical management by an ophthalmologist. The priorities in ruptured globe repair are to close the globe and address potential infection. Many ruptured globes require subsequent surgeries to address any additional conditions or complications that may exist, such as traumatic cataracts, retinal detachments, or secondary glaucoma.(A1)
Ocular Burns
Treatment of radiation burns (UV keratitis) is supportive and consists of pain control and topical antibiotics, although evidence is limited for the latter. While UV keratitis is generally a self-limiting condition, ophthalmology follow-up in 24 hours is needed if symptoms have not resolved. Patients should be counseled on the adverse effects of UV radiation, including cataract formation, pterygium, and skin cancer, as well as the importance of protective eyewear, such as welder's shields and sunglasses, for future prevention.
Treatment of ocular chemical burns begins at the scene of the injury with copious irrigation with water for at least 30 minutes and continues upon arrival to the hospital. Contact lenses worn at the time of exposure should be removed. In the event of unilateral injury, irrigating fluid should be directed away from the unaffected eye. The use of irrigation devices, such as a Morgan Lens, helps deliver continuous irrigation. The amount of irrigating solution needed varies widely depending on the duration and extent of exposure. If available, buffered eyewash solutions may be better than standard normal saline for irrigating the eyes after caustic exposure. Sterile hypertonic solutions are also helpful, as they use osmotic pressure to draw water and unwanted compounds out of the cornea.[83] Irrigation should continue until the pH remains neutral (pH 7-7.2) for 5 to 10 minutes after the last irrigation in both eyes. Fresh litmus paper should be used for each pH testing, and the conjunctiva and fornices should be checked for any particulate matter.
Ophthalmology consultation should be obtained for all but minor burns. Any patient with corneal clouding or an epithelial defect should be promptly referred to an ophthalmologist. The principles of acute management include:
- Removal of inciting chemical agents
- Promotion of ocular surface epithelial healing (ascorbate and citrate)
- Control of inflammation (topical steroids, citrate, and acetylcysteine)
- Prevention of infection (topical antibiotics)
- Control of pain (cycloplegia and systemic oral analgesia)
- Control of IOP
AMT is often performed in the acute phase to accelerate corneal re-epithelialization and decrease complications, such as corneal neovascularization. However, a recent review of AMT efficacy in treating moderate and severe burns found no significant benefit over standard medical therapy alone.[84] Overall, management should be individualized based on burn severity, with close follow-up to monitor for complications such as limbal stem cell deficiency, scarring, and elevated IOP.(A1)
Advanced Medical Therapies
Beyond conventional antibiotic prophylaxis and lubrication, preservative-free artificial tears play a crucial role in maintaining ocular surface hydration and promoting epithelial healing by reducing mechanical friction. Topical nonsteroidal anti-inflammatory drugs such as ketorolac may be used selectively for pain control; however, prolonged use should be avoided due to the risk of corneal toxicity and delayed epithelial healing. Autologous serum eye drops have emerged as an effective therapy in persistent epithelial defects by providing essential growth factors, vitamins, and fibronectin that support epithelial regeneration. Recombinant human nerve growth factor, such as cenegermin, is increasingly used for neurotrophic keratitis following trauma to promote corneal nerve regeneration and epithelial healing (see Table. Drug Classes and Their Role).[85](B3)
Biologic and Anticollagenolytic Therapy
In moderate to severe corneal injuries, especially chemical burns, anticollagenolytic agents such as oral doxycycline and topical citrate are used to inhibit MMPs and prevent stromal melting. Vitamin C (ascorbate) supplementation is recommended to promote collagen synthesis and reduce the risk of corneal ulceration and perforation. Emerging therapies targeting inflammatory pathways, including anti-VEGF agents, have shown promise in reducing corneal neovascularization and improving long-term visual outcomes.[86]
Surgical and Interventional Management
Bandage contact lenses (BCLs) are widely used to promote epithelial healing, reduce pain, and protect the corneal surface from mechanical trauma. Tissue adhesives (cyanoacrylate glue) may be used in small corneal perforations to provide tectonic support and prevent aqueous leakage. AMT serves as a biological scaffold with anti-inflammatory and antifibrotic properties, facilitating epithelial healing and reducing scarring. In severe cases, therapeutic keratoplasty (penetrating or lamellar) may be required to restore structural integrity and remove necrotic or infected tissue (see Image. Corneal Trauma: Clinical Presentations and Surgical Management). LSCT is indicated in cases of limbal stem cell deficiency following severe chemical burns or trauma.[87]
Management of Special Situations
- Neurotrophic cornea: Management includes lubrication, BCLs, autologous serum, and nerve growth factor therapy to restore epithelial integrity.
- Posttraumatic infectious keratitis: Empirical broad-spectrum antimicrobial therapy should be initiated promptly and tailored based on microbiological results.
- Pythium keratitis (posttraumatic): Requires early recognition and treatment with antibacterial agents, such as linezolid or azithromycin, rather than antifungals due to intrinsic resistance.[88]
Guideline-Based Management
- American Academy of Ophthalmology guidelines: Emphasize early antibiotic prophylaxis, avoid misuse of topical anesthetics, and make urgent referral for suspected globe injury.
- Royal College of Ophthalmologists guidelines: Recommend immediate irrigation in chemical burns and early use of anti-inflammatory and anticollagenolytic therapy.
- World Health Organization recommendations: Highlight prevention strategies and early intervention to reduce blindness from ocular trauma [12]
Table 7. Stepwise Management Approach in Corneal Trauma
|
Step |
Intervention |
Clinical Goal |
|
Initial |
Irrigation (chemical burns) and shield eye (globe injury) |
Prevent further damage |
|
Assessment |
VA, slit-lamp, and imaging |
Diagnose severity |
|
Medical |
Antibiotics, cycloplegics, and lubrication |
Prevent infection and pain |
|
Adjunct |
Serum tears, doxycycline, and vitamin C |
Promote healing |
|
Interventional |
BCL, glue, and AMT |
Structural support |
|
Surgical |
Keratoplasty and LSCT |
Restore anatomy |
Abbreviations: AMT, amniotic membrane transplantation; BCL, bandage contact lenses; LSCT, limbal stem cell transplantation; VA, visual acuity.
Table 8. Drug Classes and Their Role
|
Drug/Class |
Indication |
Mechanism |
|
Antibiotics |
Abrasion/FB |
Prevent infection |
|
Cycloplegics |
Pain relief |
Reduce ciliary spasm |
|
NSAIDs |
Pain control |
Reduce inflammation |
|
Steroids |
Severe inflammation |
Suppress immune response |
|
Doxycycline |
Melting cornea |
MMP inhibition |
|
Ascorbate |
Chemical burns |
Collagen synthesis |
|
Anti-VEGF |
Neovascularization |
Inhibit angiogenesis |
|
NGF (cenegermin) |
Neurotrophic keratitis |
Nerve regeneration |
Abbreviations: Anti-VEGF, anti-vascular endothelial growth factor; FB, foreign body; MMP, matrix metalloproteinase; NGF, nerve growth factor; NSAIDs, nonsteroidal anti-inflammatory drugs.
Differential Diagnosis
Although patients with corneal injuries typically present with a clear history of trauma or toxic exposure, several ocular conditions may mimic the presentation of corneal injury; commonly overlapping symptoms include pain, photophobia, tearing, and decreased vision (see Table. Differential Diagnosis of Ocular Findings in Corneal Trauma). In cases where the history is unclear or atypical, careful differentiation is essential to avoid misdiagnosis and inappropriate management (see Table. Red Flag Differentiation). Non-traumatic conditions often lack a clear inciting event and may demonstrate bilateral involvement, chronicity, or systemic associations, which help distinguish them from acute traumatic insults (see Table. Advanced Comparative Differentiation). Additionally, certain conditions may present with similar fluorescein staining patterns or epithelial defects, necessitating detailed slit-lamp evaluation and adjunctive testing.[18] If the source of the injury cannot be confirmed in the patient history, the following alternative diagnoses with corneal findings should be considered:
- Acute angle-closure glaucoma
- Corneal ulcer
- RCE
- Epithelial basement membrane dystrophy or map-dot-fingerprint dystrophy
- Acute conjunctivitis and epidemic keratoconjunctivitis
- Blepharitis, entropion, and trichiasis
- Non-traumatic iritis and uveitis
Table 9. Differential Diagnosis of Ocular Findings in Corneal Trauma
|
Condition |
Key Symptoms |
Slit-Lamp Findings |
Distinguishing Feature |
Laterality |
|
Acute angle-closure glaucoma |
Severe pain, headache, nausea, and blurred vision |
Corneal edema and mid-dilated pupil |
Elevated IOP and shallow AC |
Unilateral |
|
Corneal ulcer (infectious keratitis) |
Pain, discharge, and decreased vision |
Stromal infiltrate, epithelial defect, and hypopyon |
Progressive infiltrate and microbial etiology |
Usually unilateral |
|
Recurrent corneal erosion |
Recurrent morning pain |
Loose epithelium and negative staining |
History of prior trauma and recurrent episodes |
Unilateral |
|
EBMD or map-dot-fingerprint dystrophy |
Mild irritation and fluctuating vision |
Map-like lines, dots, and fingerprint patterns |
Bilateral and chronic course |
Bilateral |
|
Epidemic keratoconjunctivitis |
Redness, tearing, and photophobia |
Subepithelial infiltrates and follicles |
Viral prodrome and preauricular LN |
Bilateral |
|
Blepharitis/trichiasis/entropion |
Foreign body sensation and irritation |
Lid margin inflammation and lashes touching the cornea |
Chronic lid disease |
Bilateral |
|
Anterior uveitis (non-traumatic) |
Pain and photophobia |
Cells, flare, and keratic precipitates |
No epithelial defect |
Unilateral |
Abbreviations: AC, anterior chamber; EBMD, epithelial basement membrane dystrophy; IOP, intraocular pressure; LN, lymph node.
Table 10. Red Flag Differentiation
|
Red Flag Feature |
Possible Diagnosis |
Clinical Action |
|
Severe pain + high IOP |
Acute glaucoma |
Immediate pressure control |
|
Corneal infiltrate + discharge |
Infectious keratitis |
Urgent culture + antibiotics |
|
Recurrent morning symptoms |
RCE |
Long-term lubrication |
|
Bilateral red eye + follicles |
Viral conjunctivitis |
Supportive care |
|
Lash–cornea touch |
Trichiasis |
Lid correction |
|
Cells + flare |
Uveitis |
Steroids + referral |
Abbreviations: IOP, intraocular pressure; RCE, recurrent corneal erosion.
Table 11. Advanced Comparative Differentiation
|
Feature |
Corneal Trauma |
Infectious Keratitis |
Recurrent Corneal Erosion |
Acute Glaucoma |
Uveitis |
|
History |
Clear injury |
Often none or CL use |
Prior trauma |
Sudden onset |
Systemic disease |
|
Pain |
Acute, severe |
Severe, progressive |
Recurrent |
Severe + headache |
Deep aching |
|
Vision loss |
Variable |
Progressive |
Mild |
Marked |
Moderate |
|
Fluorescein staining |
Linear or geographic |
Irregular + infiltrate |
Loose epithelium |
Minimal |
Absent |
|
Anterior chamber |
Usually quiet |
Hypopyon possible |
Quiet |
Shallow, high IOP |
Cells or flare |
|
IOP |
Normal/low |
Variable |
Normal |
Very high |
Low or normal |
|
Laterality |
Usually unilateral |
Unilateral |
Unilateral |
Unilateral |
Usually unilateral |
Abbreviations: CL, contact lens; IOP, intraocular pressure.
Pertinent Studies and Ongoing Trials
The current management strategies for corneal trauma and ocular surface injuries are supported by randomized controlled trials (RCTs), prospective cohort studies, and systematic reviews evaluating biologic scaffolds, anti-inflammatory therapies, and regenerative interventions (see Table. Evidence Hierarchy).
AMT represents one of the most extensively studied interventions in ocular surface reconstruction. Early clinical evidence demonstrated successful restoration of corneal epithelial integrity and improved visual outcomes in chemical and thermal injuries. Subsequent randomized clinical trials have shown that early AMT, when combined with antimicrobial therapy in infectious keratitis, significantly enhances epithelial healing and reduces corneal vascularization compared to medical therapy alone.[89]
Further comparative trials evaluating AMT versus lamellar corneal transplantation have demonstrated that while AMT provides rapid epithelialization and anti-inflammatory benefits, lamellar keratoplasty may offer superior restoration of corneal thickness in advanced stromal disease. Recent systematic reviews and meta-analyses that include multiple RCTs and prospective studies have confirmed that AMT accelerates epithelial healing, reduces pain, and improves functional visual outcomes, particularly in cases of moderate to severe corneal injury. Additionally, pooled data suggest that AMT reduces corneal neovascularization and improves ocular surface stability in refractory ulcers.[90]
In the setting of corneal perforations and severe stromal thinning, prospective and retrospective clinical studies have demonstrated that multilayer AMT provides effective tectonic support, with successful closure rates in small perforations and avoidance of emergent keratoplasty in selected cases. More recent clinical studies have further supported its role in maintaining globe integrity and facilitating stromal remodeling in infectious and inflammatory corneal melts.[91]
Systematic evaluations of AMT as an adjunct to antimicrobial therapy in infectious keratitis have shown improved visual acuity outcomes and faster resolution of inflammation. However, the overall quality of evidence remains moderate due to heterogeneity among trials. Emerging clinical studies are also evaluating sutureless amniotic membrane devices and cryopreserved membrane systems, which aim to improve patient comfort, reduce surgical time, and enhance epithelial healing kinetics. These approaches represent a shift toward minimally invasive ocular surface reconstruction strategies.[92]
In neurotrophic keratopathy, RCTs have demonstrated the efficacy of recombinant human nerve growth factor (cenegermin) in promoting corneal healing and restoring nerve integrity, with significantly higher rates of complete epithelial healing compared to placebo. Despite these advances, large, multicenter randomized trials specifically addressing severe ocular trauma and rare posttraumatic infections such as P insidiosum remain limited. Current literature highlights the need for standardized treatment protocols and well-designed clinical trials to optimize therapeutic timing and long-term outcomes.[69]
Table 12. Evidence Hierarchy
|
Intervention |
Evidence Level |
Key Outcome |
|
AMT (chemical or infectious injury) |
RCT + Meta-analysis |
Faster epithelial healing ↓ inflammation |
|
AMT versus keratoplasty |
Comparative trials |
Better healing versus better structure |
|
Multilayer AMT (perforation) |
Prospective studies |
Globe preservation |
|
NGF (cenegermin) |
RCT |
Improved epithelial healing |
|
Sutureless AM devices |
Emerging studies |
Faster recovery and comfort |
Abbreviations: AM, amniotic membrane; AMT, amniotic membrane transplantation; NGF, nerve growth factor; RCT, randomized controlled trial.
Treatment Planning
After acute management, most superficial corneal abrasions and foreign bodies require no further intervention.[16] However, severe corneal trauma such as chemical burns and globe rupture require intermediate and long-term care. Long-term management of chemical ocular burns focuses on 3 areas: encouraging re-epithelialization, treating symptomatic LSCD, and diagnosing and managing secondary glaucoma. A heightened immune response and fibrovascular pannus formation can make intermediate and long-term treatment especially challenging.
After the acute phase of AMT, treatment options for chronic phase ocular burns include limbal cell transplantation and various reconstructive surgeries.[4] For bilateral cases, allogeneic stem cell transplants may be considered but carry the risks associated with systemic immunosuppression.[93] Cultivated oral mucosal epithelial transplantation is an alternative therapy that reduces inflammation and promotes re-epithelialization, using autologous buccal mucosal cells.[94] Management of globe rupture focuses first on closing the open globe and preventing infection, then on addressing other ocular injuries and complications.[95]
Management of corneal trauma requires a structured, stepwise approach that integrates rapid triage, targeted evaluation, mechanism-based therapy, and timely intervention to preserve vision and ocular integrity (see Table. Clinical Decision Framework). The following clinical decision framework outlines an approach to triage, evaluation, investigation, treatment, and follow-up across the continuum of corneal injury management.
Step 1: Immediate Triage
Principle: Stabilize before you analyze.[12]
- Rule out open globe injury
- Shield eye (no pressure) and avoid manipulation
- Chemical injury → Irrigate immediately
- Do not delay the examination
- Assess vision quickly (if safe)
- Identify red flags:
- Severe vision loss
- Hypopyon or infiltrate
- Positive Seidel
- High-velocity injury
Step 2: Focused Clinical Evaluation
Goal: Define depth, contamination, and risk.[18]
- Establish the mechanism of injury (mechanical, chemical, thermal, or radiation)
- Perform slit-lamp biomicroscopy to assess:
- Epithelial defect (fluorescein)
- Stromal involvement
- Foreign body/rust ring
- Evaluate:
- Anterior chamber reaction
- Corneal sensation
- IOP (only if globe is intact)
Step 3: Targeted Investigations
Principle: Investigate only that will change management.[16]
- Suspected infection → Corneal scraping
- High-velocity injury → CT orbit
- Opaque cornea → AS-OCT or UBM
- Non-healing defect → Tear film + neurotrophic evaluation
Step 4: Mechanism-Based Treatment
Principle: Treat the mechanism, not just the defect.[40]
Superficial injury (abrasions/FB):
- Topical antibiotics
- Lubricants ± bandage contact lens
- Cycloplegics for pain
Chemical burns:
- Copious irrigation → pH normalization
- Steroids (short-term), ascorbate, doxycycline
- Early AMT in moderate to severe cases
Infectious/contaminated trauma:
- Empirical broad-spectrum therapy
- Tailor based on microbiology
- Consider fungal or Pythium in vegetative injuries
Structural damage (laceration or perforation):
- Tissue adhesive or BCL (small defects)
- Surgical repair or keratoplasty (large defects)
Step 5: Healing Optimization:
- Lubrication (preservative-free)
- Autologous serum (non-healing defects)
- Control inflammation (judicious steroids)
- Address:
- Lid abnormalities
- Tear film dysfunction
- LSCD [96]
Step 6: Follow-Up Strategy
- Daily review in the acute phase
- Monitor:
- Epithelial closure
- Infection signs
- Stromal thinning
- Escalate early in the case of:
- Non-healing defect
- Increasing infiltrate
- Risk of perforation [97]
Table 13. Clinical Decision Framework
|
Scenario |
First Action |
Key Treatment |
Escalation |
|
Abrasion |
Fluorescein |
Antibiotic + lubricant |
BCL |
|
IOFB |
Remove IOFB |
Antibiotic |
Rust ring removal |
|
Chemical burn |
Irrigate |
Steroid + ascorbate |
AMT |
|
Infection |
Scrape |
Targeted therapy |
Keratoplasty |
|
Perforation |
Shield |
Glue/surgery |
Emergency PK |
Abbreviations: AMT, amniotic membrane transplantation; BCL, bandage contact lenses; IOFB, intraocular foreign body; PK, penetrating keratoplasty.
Principles
- Urgent management is prioritized over diagnostic perfection.Infection is presumed in all doubtful cases.In chemical injuries, time is considered equivalent to tissue loss.
- Neurotrophic or stem cell dysfunction is considered in non-healing epithelial defects.Prevention of late surgical burden is achieved through early intervention.
Toxicity and Adverse Effect Management
Management of corneal trauma must balance therapeutic efficacy with the prevention of treatment-related ocular surface toxicity, which can delay epithelial healing and worsen outcomes.
Topical Medication Toxicity
Prolonged or inappropriate use of topical anesthetics is a well-recognized cause of corneal toxicity, leading to epithelial breakdown, stromal infiltration, ring ulcers, and even corneal perforation. Close follow-up is essential to monitor for progression and to ensure timely intervention if complications such as stromal thinning or ulceration develop. Management involves immediate discontinuation, aggressive lubrication, and treatment of any secondary infection.[98]
Topical antibiotics, particularly aminoglycosides and fluoroquinolones, may induce epithelial toxicity and delay healing when used excessively. Preservative-free formulations and appropriate dosing schedules are recommended to minimize toxicity.[99] Therapy should be reassessed regularly and de-escalated when clinically appropriate to reduce unnecessary exposure and promote epithelial recovery.
Topical corticosteroids, while effective in controlling inflammation, can impair epithelial regeneration, increase susceptibility to infection, and exacerbate corneal melting if used indiscriminately. The use of corticosteroids should be carefully timed and closely monitored, especially in infectious or epithelial-defective states.[100] Topical steroids are generally reserved for cases with controlled infection and intact epithelium.
Drug-Induced Corneal Toxicity
Nonsteroidal anti-inflammatory drugs have been associated with corneal epithelial defects, thinning, and rare cases of corneal melt, particularly with prolonged use.[101] Discontinuation and supportive therapy are required if toxicity is suspected. Preservatives such as benzalkonium chloride can disrupt tear film stability and epithelial integrity, especially in patients requiring frequent dosing.[13] Switching to preservative-free alternatives is recommended in such cases.[102]
Procedure-Related Complications
Use of bandage contact lenses may predispose to microbial keratitis if hygiene is inadequate or follow-up is poor. Regular monitoring and prophylactic antibiotics are essential. AMT is generally safe but may rarely be associated with membrane displacement, infection, or delayed epithelialization. Proper surgical technique and follow-up minimize these risks.[15]
Systemic Therapy–Related Effects
Systemic agents such as oral doxycycline, used for their anticollagenolytic properties, may cause gastrointestinal intolerance and photosensitivity. Dose adjustment and patient counseling are advised. High-dose ascorbate therapy, used in chemical burns, may lead to gastrointestinal upset but is generally well tolerated and beneficial for collagen synthesis.[103]
Clinical Monitoring and Prevention Strategy
- Use the minimum effective dose of topical medications.
- Prefer preservative-free formulations in prolonged therapy.
- Avoid unsupervised use of anesthetics or steroids.
- Monitor for:
- Persistent epithelial defect
- Stromal thinning
- New infiltrates
- Early identification of toxicity allows reversal before structural damage occurs.
Key Clinical Pearls
- Non-healing corneal defect → Always rule out drug toxicity
- Topical anesthetic misuse → Vision-threatening emergency
- Steroids without infection control → Corneal melt risk
- Preservatives → Silent contributors to chronic epithelial damage [104]
Staging
Staging of ocular surface burns is essential for clinical assessment and visual prognosis. The Dua classification is the most widely used grading system for this purpose (see Table. Dua Classification of Ocular Surface Burns).[45][65] Limbal ischemia is quantified in clock hours, whereas conjunctival involvement is expressed as a percentage. The analog scale correlates the extent of limbal ischemia (measured in clock hours) with the percentage of involved bulbar and forniceal conjunctiva. Staging of ocular surface burns is essential not only for prognostication but also for guiding timing and intensity of therapeutic interventions, particularly decisions regarding early surgical procedures such as AMT and LSCT.
Dua Classification
The Dua classification is a comprehensive grading system based on 2 critical parameters:
- Extent of limbal ischemia (clock hours: 0-12)
- Extent of conjunctival involvement (percentage: 0%-100%) [55]
The analog relationship between limbal involvement and conjunctival damage reflects the extent of limbal stem cell loss, which is the key determinant of epithelial healing potential (see Table. Grades of Dua Classification).
Table 14. Grades of Dua Classification
|
Grade |
Limbal Involvement |
Conjunctival Involvement |
Prognosis |
|
I |
0 clock hours |
0% |
Very good |
|
II |
≤3 clock hours |
≤30% |
Good |
|
III |
>3-6 clock hours |
30%-50% |
Good to guarded |
|
IV |
>6-9 clock hours |
50%-75% |
Guarded |
|
V |
>9 to <12 clock hours |
75% to <100% |
Poor |
|
VI |
12 clock hours |
100% |
Very poor |
Pathophysiologic Correlation of Staging
Higher grades are associated with:
- LSCD → Persistent epithelial defects
- Stromal ischemia and necrosis
- Increased inflammatory cytokine load
- Neovascularization and conjunctivalization
The severity of limbal ischemia directly correlates with the loss of regenerative capacity of the corneal epithelium, making it the most critical prognostic indicator.[105]
Comparison with the Roper-Hall Classification
The Roper-Hall classification is an older grading system based on corneal haze and limbal ischemia. However, this classification system is less precise because it does not quantify conjunctival involvement and tends to underestimate injury severity (see Table. Roper-Hall Classification).[106] As such, the Dua classification is preferred due to better prognostic accuracy and reproducibility.
Table 15. Roper-Hall Classification
|
Grade |
Corneal Appearance |
Limbal Ischemia |
Prognosis |
|
I |
Epithelial damage only |
None |
Good |
|
II |
Hazy, but iris is visible |
<33% |
Good |
|
III |
Opaque, iris details obscured |
33%-50% |
Guarded |
|
IV |
Opaque cornea |
>50% |
Poor |
Clinical Utility of Staging
Staging directly influences management decisions (see Table. Staging-Based Management Approach):
- Grades I to II
- Conservative management sufficient
- Rapid epithelial healing expected
- Grades III to IV
- Require aggressive medical therapy
- Early consideration of AMT
- Grades V to VI
- High risk of LSCD and corneal melt
- Require early surgical intervention (AMT and LSCT) [19]
Table 16. Staging-Based Management Approach
|
Grade |
Risk |
Key Pathology |
Management Strategy |
|
I-II |
Low |
Superficial epithelial injury |
Lubrication and antibiotics |
|
III-IV |
Moderate |
Partial LSCD and inflammation |
Steroids and AMT |
|
V-VI |
Severe |
Total LSCD and ischemia |
LSCT and keratoplasty |
Abbreviations: AMT, amniotic membrane transplantation; LSCD, limbal stem cell deficiency; LSCT, limbal stem cell transplantation.
Prognosis
Superficial corneal abrasions and superficial corneal foreign body injuries generally have an excellent prognosis, particularly when the visual axis is not involved. For anterior stromal scarring involving the visual axis, long-term visual rehabilitation may include excimer laser correction or lamellar corneal transplantation. In ocular chemical burns, greater than 50% conjunctival involvement or greater than 6 clock hours of limbal involvement indicate a poor visual prognosis. For these severe cases, corneal transplants are more frequently rejected, and keratoprosthesis surgery may be required.[107] The prognosis for perforating corneal injuries is also more guarded and dependent on the individual circumstances of each case.
Early intervention, particularly timely irrigation in cases of chemical injury, is one of the most critical determinants of visual outcomes and can significantly reduce long-term ocular surface damage. The extent of limbal stem cell damage remains the single most important predictor of epithelial healing and long-term ocular surface stability, with total limbal ischemia often resulting in persistent epithelial defects and conjunctivalization.[55]
The presence of a secondary infection, especially fungal or atypical organisms such as P insidiosum, is associated with poorer outcomes due to delayed diagnosis and limited therapeutic options. Corneal nerve damage and subsequent neurotrophic keratopathy may adversely affect prognosis by impairing epithelial regeneration and increasing the risk of chronic ulceration. Depth of stromal involvement is another key factor, as deeper injuries are more likely to result in fibrosis, irregular astigmatism, and permanent visual impairment. Posttraumatic corneal neovascularization further worsens prognosis by compromising corneal transparency and increasing the risk of graft rejection in future keratoplasty. Patient-related factors such as age, comorbid ocular surface disease, and delayed presentation also influence healing outcomes and visual recovery.[108]
Key Prognostic Indicators
- Limbal ischemia extent → Strongest predictor
- Time to treatment → Critical in burns
- Infection → Worsens outcome significantly
- Stromal depth → Determines scarring
- Neovascularization → Predicts graft failure
Complications
Complications of corneal trauma include scarring affecting the visual axis, recurrent corneal erosion due to weak adhesions between the healed corneal epithelium and underlying corneal layers, reduced limbal stem cell function and failure, secondary glaucoma due to trabecular meshwork damage, traumatic cataract, retinal detachment, endophthalmitis, and loss of vision or the eye.[109][110] In chemical ocular injuries, pseudomembranes, symblepharon, and cicatricial entropion or ectropion can also occur.
Persistent epithelial defects are a common sequela following corneal trauma, particularly in cases associated with LSCD or neurotrophic keratopathy, leading to delayed healing and increased risk of infection. Corneal thinning and stromal melt may result from an excessive inflammatory response and MMP activity, potentially progressing to perforation if not managed promptly. Posttraumatic corneal neovascularization can develop secondary to chronic inflammation and hypoxia, compromising corneal transparency and increasing the likelihood of graft rejection in future keratoplasty.[111]
Irregular astigmatism resulting from stromal scarring and surface irregularity is a frequent cause of long-term visual impairment even after structural healing. Neurotrophic keratopathy may develop following damage to corneal nerves, resulting in reduced corneal sensitivity, impaired epithelial healing, and recurrent ulceration. Anterior segment complications such as peripheral anterior synechiae and chronic angle damage may contribute to long-term IOP elevation and secondary glaucoma. In severe ocular surface burns, chronic cicatrization may lead to dry eye disease, ocular surface keratinization, and ankyloblepharon, significantly affecting ocular function and cosmesis. The negative psychosocial impact, including reduced quality of life and functional disability, is also increasingly recognized as an important long-term consequence of vision-threatening ocular trauma.[69]
Table 17. Comprehensive Classification of Complications in Corneal Trauma
|
Category |
Complication |
Pathophysiology |
Clinical Impact |
Long-term Outcome |
|
Epithelial |
Persistent epithelial defect |
Impaired healing or LSCD |
Non-healing ulcer |
Chronic keratopathy |
|
Recurrent corneal erosion |
Weak epithelial adhesion |
Recurrent pain |
Visual fluctuation |
|
|
Stromal |
Corneal scarring |
Collagen disorganization |
Reduced vision |
Permanent opacity |
|
Corneal melt |
MMP-mediated degradation |
Thinning/perforation |
Emergency surgery |
|
|
Neovascularization |
VEGF-driven angiogenesis |
Loss of transparency |
Graft rejection risk |
|
|
Endothelial |
Corneal edema |
Endothelial cell loss |
Blurred vision |
Bullous keratopathy |
|
Neurogenic |
Neurotrophic keratopathy |
Nerve damage |
Reduced sensation |
Chronic ulcers |
|
Limbal |
LSCD |
Stem cell loss |
Conjunctivalization |
Severe visual loss |
|
Anterior segment |
Secondary glaucoma |
TM damage/synechiae |
Raised IOP |
Optic nerve damage |
|
Traumatic cataract |
Lens damage |
Visual impairment |
Surgical need |
|
|
Posterior segment |
Retinal detachment |
Traction/trauma |
Severe vision loss |
Poor prognosis |
|
Endophthalmitis |
Infection |
Pain and vision loss |
Globe loss risk |
|
|
Adnexal/surface |
Symblepharon |
Cicatrization |
Restricted movement |
Surgical correction |
|
Entropion/ectropion |
Lid scarring |
Surface irritation |
Chronic damage |
|
|
Refractive |
Irregular astigmatism |
Surface distortion |
Blurred vision |
Optical correction |
|
Systemic/functional |
Psychosocial impact |
Visual disability |
Reduced QOL |
Long-term burden |
Abbreviations: IOP, intraocular pressure; LSCD, limbal stem cell deficiency; MMP, matrix metalloproteinase; QOL, quality of life; TM, trabecular meshwork; VEGF, vascular endothelial growth factor.
Key Clinical Pearls
- Persistent epithelial defect → LSCD or neurotrophic cause
- Corneal melt → Vision-threatening emergency
- Neovascularization → Future graft failure risk
- Chemical burns → Chronic cicatricial complications [111]
Postoperative and Rehabilitation Care
Postoperative and rehabilitation care following corneal trauma is critical for optimizing visual outcomes, preventing complications, and restoring ocular surface integrity. Management is individualized based on the severity of injury, the type of intervention performed, and the presence of associated ocular or systemic factors (see Table. Postoperative Care and Rehabilitation Strategy).
Immediate Postoperative Care
In the early postoperative period, the primary goals are epithelial healing, infection prevention, and control of inflammation.
- Topical broad-spectrum antibiotics: Routinely prescribed to prevent secondary infection, particularly in cases with epithelial defects or surgical intervention
- Topical corticosteroids: Used judiciously to reduce inflammation and limit stromal scarring, with careful monitoring to avoid delayed healing or exacerbation of infection
- Cycloplegic agents: Help relieve ciliary spasm and associated pain
- Preservative-free lubricants: Essential for maintaining tear film stability and supporting epithelial regeneration.
In cases of chemical injury or extensive trauma, frequent follow-up (daily or alternate-day) is required to monitor epithelial closure, stromal integrity, and signs of infection or melt.[112]
Ocular Surface Rehabilitation
Restoration of a stable ocular surface is fundamental to long-term success.
- Autologous serum eye drops: Provide growth factors and cytokines that enhance epithelial healing in persistent defects
- BCLs: Protect the corneal surface and reduce mechanical trauma during blinking
- AMT: Serves as a biological scaffold that promotes epithelialization and reduces inflammation in moderate-to-severe injuries
In cases of LSCD, ocular surface reconstruction with LSCT may be required for long-term rehabilitation.[113]
Visual Rehabilitation
Visual recovery depends on the extent of corneal involvement and residual scarring.
- Spectacles or rigid gas-permeable (RGP) lenses: Used for the correction of irregular astigmatism
- Scleral contact lenses: Particularly beneficial in patients with severe ocular surface irregularity or dryness
- Excimer laser procedures (photorefractive keratectomy or phototherapeutic keratectomy): May be considered for superficial scarring that affects vision
For advanced structural damage:
- Lamellar or penetrating keratoplasty may be required for visual rehabilitation.
- Keratoprosthesis is reserved for end-stage cases with severe ocular surface failure.[114]
Long-Term Monitoring
Patients require regular follow-up to detect late complications such as:
- Corneal neovascularization
- Secondary glaucoma
- Recurrent epithelial defects
- Graft rejection (if keratoplasty is performed)
Monitoring IOP and ocular surface stability is essential, particularly in patients with severe burns or those undergoing multiple interventions.[115]
Rehabilitation Beyond the Eye
In patients with significant visual impairment:
- Low vision aids and visual rehabilitation programs should be introduced early.
- Psychological support may be required due to the impact on quality of life and daily functioning.[116]
Table 18. Postoperative Care and Rehabilitation Strategy
|
Phase |
Focus |
Key Interventions |
Goal |
|
Immediate (0-7 days) |
Healing + infection control |
Antibiotics, steroids, and lubricants |
Epithelial closure |
|
Early (1-4 weeks) |
Surface stabilization |
BCL, serum tears, and AMT |
Prevent complications |
|
Intermediate (1-3 months) |
Visual recovery |
RGP/scleral lenses |
Improve vision |
|
Late (>3 months) |
Structural rehab |
Keratoplasty and LSCT |
Restore anatomy |
Abbreviations: AMT, amniotic membrane transplantation; BCL, bandage contact lens; LSCT, limbal stem cell transplantation; RGP, rigid gas-permeable.
Consultations
Management of corneal trauma often requires a multidisciplinary approach, particularly in moderate to severe injuries, to optimize structural and functional outcomes.
Ophthalmology Subspecialty Consultation
- Cornea and external disease specialist
- Essential in cases of:
- Non-healing epithelial defects
- Infectious keratitis
- LSCD
- Need for AMT or keratoplasty [117]
- Vitreoretinal specialist
- Indicated when:
- Posterior segment involvement suspected
- IOFB present
- Associated with retinal detachment or vitreous hemorrhage [118]
- Glaucoma specialist
- Required in:
- Secondary glaucoma due to angle damage or inflammation
- Steroid-induced IOP elevation [119]
- Oculoplasty specialist
- Needed for:
- Eyelid lacerations
- Symblepharon, entropion, and ectropion
- Adnexal reconstruction in chemical burns [120]
Emergency and Systemic Consultations
- Emergency medicine/trauma team
- Necessary for:
- Polytrauma cases
- Suspected open globe injuries
- Chemical exposure requiring systemic stabilization
- Toxicology/poison control
- Particularly in:
- Chemical injuries with ingestion or inhalation risk
- Industrial or unknown chemical exposure
- Otolaryngology/pulmonology
- Indicated if:
- Airway compromise suspected due to chemical exposure [121]
Rehabilitation and Support Services
- Low vision specialist
- For patients with permanent visual impairment requiring visual aids and rehabilitation
- Optometry/contact lens specialist
- For fitting:
- RGP or scleral lenses
- Posttraumatic irregular astigmatism correction
- Psychological support/counseling
- Recommended in:
- Severe vision loss
- Trauma-related psychosocial distress [122]
Deterrence and Patient Education
A substantial portion of corneal injuries are related to activities and objects common to home or work.[18] Eye protection during high-risk activities and patient education could mitigate the incidence and severity of corneal trauma in many cases. Delayed presentation and poor adherence to treatment plans and follow-up can adversely affect final visual outcomes. Given the projected increase in global childhood and adolescent trauma from 2022 to 2040, targeted patient education and public health awareness can potentially improve treatment outcomes in these groups of patients and in the generations to follow.[5][32]
The use of protective eyewear, including polycarbonate safety glasses, has been shown to significantly reduce the incidence of occupational ocular injuries, particularly in high-risk environments such as construction, agriculture, and metalwork. Workplace safety interventions, including mandatory eye-protection policies and hazard-awareness training, play a critical role in reducing preventable ocular trauma. Public education should emphasize the importance of immediate irrigation in chemical exposures, as early intervention can dramatically improve prognosis and reduce long-term complications. Patients should be counseled regarding the risks associated with contact lens misuse, including overnight wear and poor hygiene, which increase susceptibility to trauma-related infections.
In pediatric populations, preventive strategies should include supervision during play, avoidance of sharp objects, and caregiver education, as children are particularly vulnerable to accidental eye injuries. Awareness campaigns targeting sports-related injuries should promote the use of sport-specific protective eyewear, especially in high-risk activities such as racquet sports and cricket. Early recognition of symptoms, such as pain, photophobia, and vision changes, and prompt consultation with an eye care specialist are essential to prevent progression of injury and complications. Adherence to prescribed therapy and scheduled follow-up visits should be strongly emphasized, as non-adherence is a major contributor to poor outcomes and chronic ocular surface disease.[16]
Pearls and Other Issues
Although corneal trauma often appears straightforward, a high index of clinical suspicion is essential, as subtle examination findings may conceal vision-threatening injuries.
Clinical Pearls
- An IOFB should be suspected in any patient with a history of metal-on-metal injury until excluded.
- The severity of pain correlates more closely with epithelial nerve exposure than with the size of the defect.
- A quiet eye with reduced vision should raise suspicion for deeper pathology, such as retinal involvement or occult globe injury.
- Chemical injuries require immediate irrigation before detailed examination; delay significantly worsens prognosis.
- Persistent epithelial defects should prompt evaluation for neurotrophic keratopathy or LSCD.[123]
Common Pitfalls
- Failure to recognize a small penetrating injury or a Seidel-positive leak, leading to a delayed diagnosis of open globe injury.
- Inappropriate use of topical anesthetics, causing corneal toxicity and delayed healing.
- Premature or unsupervised use of topical steroids in infectious keratitis, leading to worsening infection and corneal melt.
- Failure to evert the eyelid in unexplained abrasions or missing retained subtarsal foreign bodies.
- Underestimating chemical injuries due to their initially mild appearance, despite ongoing tissue damage.[124]
Disposition and Follow-Up
- Minor corneal abrasion: Outpatient management with close follow-up within 24 to 48 hours.
- High-risk injury (chemical burn, deep stromal involvement, infection): Requires urgent ophthalmology referral and frequent monitoring.
- Open globe injury or suspected IOFB: Immediate referral to a tertiary care center with surgical capability.[125]
Prevention Insights
- Protective eyewear significantly reduces occupational and sports-related ocular injuries.
- Early intervention and adherence to treatment protocols are key to preventing long-term visual morbidity.
- Public awareness regarding contact lens hygiene and chemical safety can prevent a large proportion of avoidable injuries.[126]
Enhancing Healthcare Team Outcomes
The management of traumatic corneal injuries requires an interprofessional approach involving nurses, emergency department clinicians, and ophthalmologists.[127] Effective care coordination is essential for providing patient-centered care and enhancing recovery. Ophthalmology consultation should be obtained promptly whenever a significant corneal injury is suspected in the emergency setting. Patient outcomes depend on the type and severity of the corneal injury as well as the timing of evaluation and treatment. Most small abrasions heal without sequelae. Shallow corneal foreign bodies also have good outcomes. However, the prognosis after ocular burns and corneal perforations is guarded. Many of these patients require prolonged care, and some may have permanent visual loss even after adequate treatment.[128][129][130]
Additional Interprofessional Strategies and Team-Based Care
Effective management of corneal trauma requires clear communication between emergency clinicians and ophthalmologists, particularly in time-sensitive conditions such as chemical burns and open globe injuries. Early recognition and prompt referral significantly improve visual outcomes and reduce complications. Nursing staff play a critical role in initial triage, especially in initiating immediate ocular irrigation in chemical injuries and ensuring adherence to sterile protocols during examination and treatment. Proper documentation and monitoring by nursing teams contribute to early detection of complications such as infection or corneal melt. Pharmacists contribute by ensuring appropriate drug selection, avoiding medication-related toxicity (eg, preservative toxicity and anesthetic misuse), and optimizing dosing regimens for antibiotics, steroids, and adjunctive therapies. Interprofessional collaboration is particularly important in managing complex cases requiring surgical intervention, where coordination among cornea specialists, vitreoretinal surgeons, and anesthesiology teams ensures optimal perioperative outcomes.[131]
Patient Safety and Quality Improvement
Standardized clinical protocols and checklists help reduce errors in the management of ocular trauma, particularly in emergency settings where time-critical decisions are required. Ensuring timely follow-up and patient compliance is a shared responsibility among healthcare providers, as missed appointments and poor adherence significantly impact outcomes in corneal trauma. Incorporation of electronic health records and teleophthalmology platforms facilitates better communication, early triage, and continuity of care, especially in resource-limited settings.[132]
Ethical and Patient-Centered Considerations
Providing clear patient counseling regarding prognosis, treatment expectations, and potential complications is essential for informed decision-making and adherence to therapy. In severe cases involving visual loss, early involvement of rehabilitation services and psychological support is important to address the broader impact on quality of life. Equitable access to care, especially in low-resource settings, remains a key ethical consideration, emphasizing the need for public health initiatives and preventive strategies.[133]
Key Team-Based Pearls
- Early involvement of ophthalmology leads to better outcomes.
- Chemical burns require a team-based rapid response.
- Medication safety is a shared responsibility.
- Follow-up adherence is as important as initial treatment.[12]
Media
(Click Image to Enlarge)
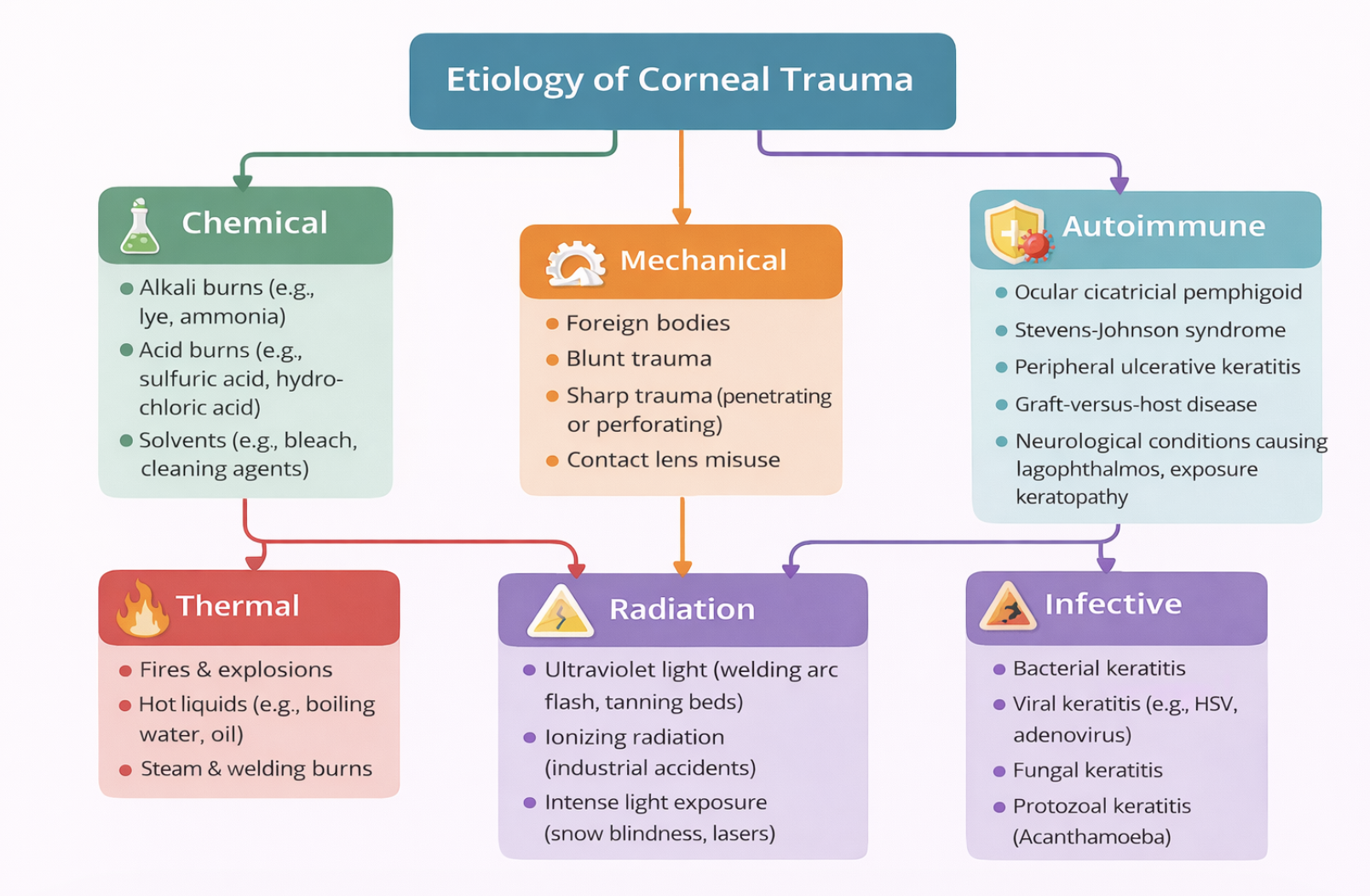
Etiology of Corneal Trauma. Schematic diagram illustrating major causes of corneal injury, including mechanical, chemical, thermal, radiation, autoimmune, and infectious etiologies, with representative examples for each category.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
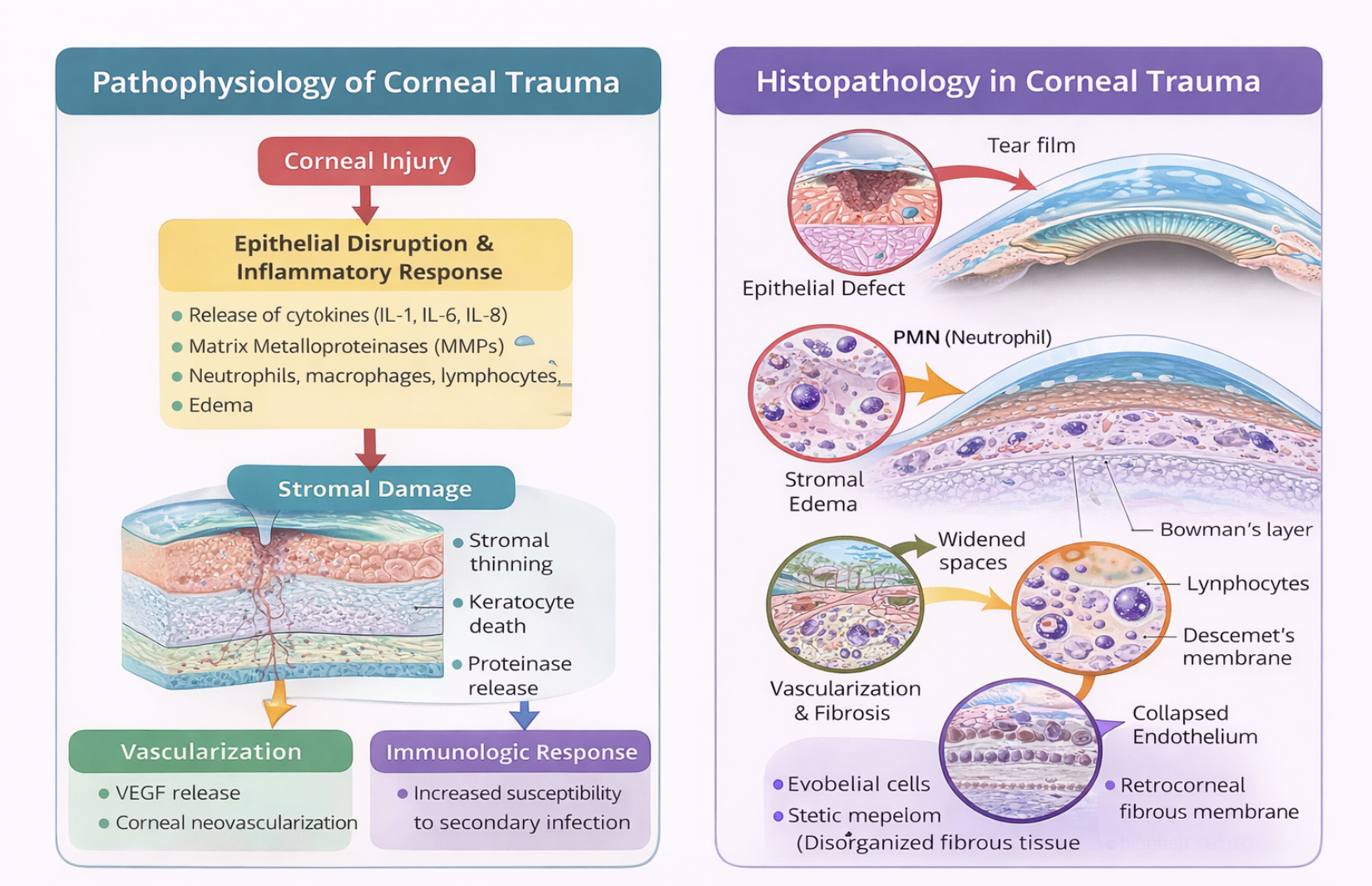
Pathophysiology and Histopathologic Changes in Corneal Trauma. Schematic illustration demonstrating epithelial disruption, inflammatory cascade activation, stromal damage, neovascularization, and associated histopathologic features, including edema, inflammatory cell infiltration, and fibrotic remodeling.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
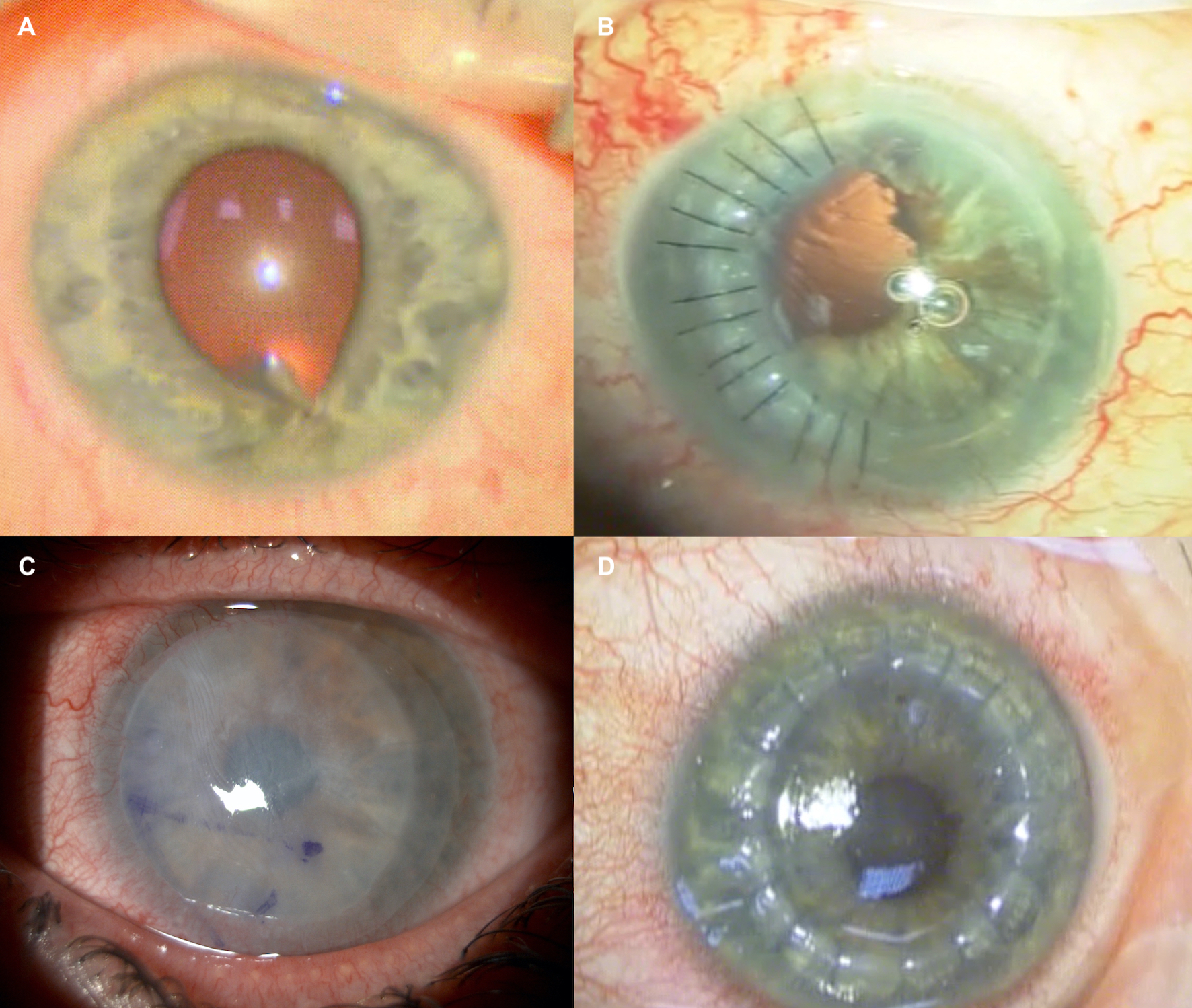
Corneal Trauma: Clinical Presentations and Surgical Management. Composite images demonstrate (A) penetrating corneal injury with inferior iris prolapse, (B) corneal laceration repair with sutures, (C) amniotic membrane placement within a contact lens delivery system (Omnigen) to promote re-epithelialization after chemical injury, and (D) corneal transplantation performed for visually significant stromal scarring.
Contributed by L Fu, MD
References
Li C, Fu Y, Liu S, Yu H, Yang X, Zhang M, Liu L. The global incidence and disability of eye injury: an analysis from the Global Burden of Disease Study 2019. EClinicalMedicine. 2023 Aug:62():102134. doi: 10.1016/j.eclinm.2023.102134. Epub 2023 Aug 9 [PubMed PMID: 37599904]
Négrel AD, Thylefors B. The global impact of eye injuries. Ophthalmic epidemiology. 1998 Sep:5(3):143-69 [PubMed PMID: 9805347]
Bashir MT, Bouamra O, Kirwan JF, Lecky FE, Bourne RRA. Ocular injuries among patients with major trauma in England and Wales from 2004 to 2021. Eye (London, England). 2024 Oct:38(14):2761-2767. doi: 10.1038/s41433-024-03116-y. Epub 2024 May 24 [PubMed PMID: 38789787]
Mohan RR, Kempuraj D, D'Souza S, Ghosh A. Corneal stromal repair and regeneration. Progress in retinal and eye research. 2022 Nov:91():101090. doi: 10.1016/j.preteyeres.2022.101090. Epub 2022 May 29 [PubMed PMID: 35649962]
Meng Y, Liu Y, Ma Y, Chen Z, Tsai CL, Li T. Epidemiological Trends and Inequalities in Eye Injuries Among Children and Adolescents Aged 0-19 Years: A Comprehensive Analysis of Global, Regional, and National Data From 1990 to 2021. Journal of ophthalmology. 2026:2026():7411787. doi: 10.1155/joph/7411787. Epub 2026 Mar 4 [PubMed PMID: 41800189]
Level 2 (mid-level) evidenceKwok SS, Shih KC, Bu Y, Lo AC, Chan TC, Lai JS, Jhanji V, Tong L. Systematic Review on Therapeutic Strategies to Minimize Corneal Stromal Scarring After Injury. Eye & contact lens. 2019 Nov:45(6):347-355. doi: 10.1097/ICL.0000000000000584. Epub [PubMed PMID: 30724841]
Level 1 (high-level) evidenceMartin LM, Jeyabalan N, Tripathi R, Panigrahi T, Johnson PJ, Ghosh A, Mohan RR. Autophagy in corneal health and disease: A concise review. The ocular surface. 2019 Apr:17(2):186-197. doi: 10.1016/j.jtos.2019.01.008. Epub 2019 Jan 25 [PubMed PMID: 30690084]
Slaughter RJ, Watts M, Vale JA, Grieve JR, Schep LJ. The clinical toxicology of sodium hypochlorite. Clinical toxicology (Philadelphia, Pa.). 2019 May:57(5):303-311. doi: 10.1080/15563650.2018.1543889. Epub 2019 Jan 28 [PubMed PMID: 30689457]
Saka ES, Monsudi KF, Olatuji V. TRAUMATIC CORNEAL LACERATION IN NORTHWESTERN NIGERIA. Journal of the West African College of Surgeons. 2017 Oct-Dec:7(4):72-84 [PubMed PMID: 30479992]
Bremond-Gignac D, Copin H, Benkhalifa M. Corneal epithelial stem cells for corneal injury. Expert opinion on biological therapy. 2018 Sep:18(9):997-1003. doi: 10.1080/14712598.2018.1508443. Epub 2018 Aug 9 [PubMed PMID: 30092649]
Level 3 (low-level) evidenceKumar A, Yun H, Funderburgh ML, Du Y. Regenerative therapy for the Cornea. Progress in retinal and eye research. 2022 Mar:87():101011. doi: 10.1016/j.preteyeres.2021.101011. Epub 2021 Sep 14 [PubMed PMID: 34530154]
Cao L, Wang C, Zhang K, You Z, Chen Y. Correlation between tear cytokine profiles and corneal injury degree in patients with dry eye syndrome. Frontiers in immunology. 2026:17():1756076. doi: 10.3389/fimmu.2026.1756076. Epub 2026 Mar 19 [PubMed PMID: 41939866]
Smaali K, Lenfant S, Karpe S, Oçafrain M, Blanchard P, Deresmes D, Godey S, Rochefort A, Roncali J, Vuillaume D. High on-off conductance switching ratio in optically-driven self-assembled conjugated molecular systems. ACS nano. 2010 Apr 27:4(4):2411-21. doi: 10.1021/nn100295x. Epub [PubMed PMID: 20349942]
Utman SAK, Moate BJR. A 51-year-old man with photopsias. Digital journal of ophthalmology : DJO. 2008:14():18-19. doi: 10.5693/djo.03.2008.006. Epub 2008 Apr 4 [PubMed PMID: 29440973]
Cooper CM, Berg E, Ashurst J. Scratching the Surface: Re-evaluating the Management of Corneal Abrasions. Cureus. 2026 Feb:18(2):e103351. doi: 10.7759/cureus.103351. Epub 2026 Feb 10 [PubMed PMID: 41835781]
Vatkar V, Bora R, Magdum R, Abraham P. Break in Corneal Shine due to Lime: Successful Restoration of Cornea after Accidental Chemical Injury - A Case Report. Annals of African medicine. 2026 Feb 27:():. doi: 10.4103/aam.aam_398_25. Epub 2026 Feb 27 [PubMed PMID: 41769951]
Level 3 (low-level) evidenceFu L, Gurnani B, Hollick EJ. Artificial Corneal Transplantation. StatPearls. 2026 Jan:(): [PubMed PMID: 33760451]
Bin Helayel H, Bin Dakhil N, Alnutaifi R, Alkathery F, Abukhaled Y, Alsaif BA, Aldayel A, Kirat O, Fairaq R. Corneal thinning and perforation: a narrative review of diagnostic and stepwise management strategies. International ophthalmology. 2026 Mar 24:46(1):. pii: 173. doi: 10.1007/s10792-026-04036-4. Epub 2026 Mar 24 [PubMed PMID: 41874780]
Level 3 (low-level) evidencePatek GC, Bates A, Gurnani B. Ocular Burns. StatPearls. 2026 Jan:(): [PubMed PMID: 29083604]
Wu D, Lin Y, Wu H, Cai J. Systematic inflammatory indicators and clinical management of exogenous endophthalmitis due to metal penetrating injury of eyeball. Frontiers in medicine. 2024:11():1466530. doi: 10.3389/fmed.2024.1466530. Epub 2024 Dec 9 [PubMed PMID: 39717174]
Level 1 (high-level) evidenceColeman DJ, Good KL, Charnock LN, Epstein SE. Clinical signs, treatment, and outcomes for ophthalmic thermal injury in 108 cats exposed to northern California wildfires between 2015 and 2020. Journal of the American Veterinary Medical Association. 2025 Sep 1:263(9):1153-1160. doi: 10.2460/javma.25.03.0187. Epub 2025 Jun 4 [PubMed PMID: 40466660]
Gour A, Garg A, Singh K, Patel NV, Sangwan VS. A Case-Based Approach to the Management of Corneal Melts and Perforations in Ocular Surface Disorders. Cureus. 2025 Mar:17(3):e81293. doi: 10.7759/cureus.81293. Epub 2025 Mar 27 [PubMed PMID: 40291310]
Level 3 (low-level) evidenceVeldman PB, Greiner MA, Cortina MS, Kuo AN, Li JY, Miller DD, Shtein RM, Weikert MP, Yin J, Kim SJ, Shen JF. Efficacy of Amniotic Membrane Grafting for the Treatment of Chemical and Thermal Ocular Surface Injuries: A Report by the American Academy of Ophthalmology. Ophthalmology. 2025 Feb:132(2):154-163. doi: 10.1016/j.ophtha.2024.08.021. Epub 2024 Oct 10 [PubMed PMID: 39387749]
Li Q, Tan J, Xie H, Zhang X, Dai Q, Li Z, Yan LL, Chen W. Evaluating the accuracy of the Ophthalmologist Robot for multiple blindness-causing eye diseases: a multicentre, prospective study protocol. BMJ open. 2024 Mar 1:14(3):e077859. doi: 10.1136/bmjopen-2023-077859. Epub 2024 Mar 1 [PubMed PMID: 38431298]
Zhao X, Zuo X, Zhong J, Wang B, Li S, Xiao Y, Yuan J. Heparin-Modified Amniotic Membrane Combined With Growth Factors for Promoting Corneal Wound Healing After Alkali Burn. Frontiers in bioengineering and biotechnology. 2020:8():599800. doi: 10.3389/fbioe.2020.599800. Epub 2020 Nov 23 [PubMed PMID: 33330430]
Hossain RR, Papamichael E, Coombes A. East London deliberate corrosive fluid injuries. Eye (London, England). 2020 Apr:34(4):733-739. doi: 10.1038/s41433-019-0593-x. Epub 2019 Sep 25 [PubMed PMID: 31554950]
Lam SS, Sklar BA, Schoen M, Rapuano CJ. Severe ocular alkali injury managed with an externally sutured amniotic membrane and customized symblepharon ring. Taiwan journal of ophthalmology. 2023 Jan-Mar:13(1):101-105. doi: 10.4103/2211-5056.362597. Epub 2022 Dec 2 [PubMed PMID: 37252174]
Gurnani B, Kaur K. Renaissance of an Emerging Pathogen-Pythium insidiosum Keratitis: An Indian Perspective. Clinical ophthalmology (Auckland, N.Z.). 2025:19():4811-4830. doi: 10.2147/OPTH.S568552. Epub 2025 Dec 18 [PubMed PMID: 41446894]
Level 3 (low-level) evidenceGurnani B, Kaur K. Immune Camouflage in Pythium insidiosum Keratitis: A Hypothesis on Molecular Mimicry and Host Pattern Recognition Receptor Evasion. Clinical ophthalmology (Auckland, N.Z.). 2025:19():4855-4873. doi: 10.2147/OPTH.S560311. Epub 2025 Dec 19 [PubMed PMID: 41446892]
Gurnani B, Christy J, Narayana S, Rajkumar P, Kaur K, Gubert J. Retrospective multifactorial analysis of Pythium keratitis and review of literature. Indian journal of ophthalmology. 2021 May:69(5):1095-1101. doi: 10.4103/ijo.IJO_1808_20. Epub [PubMed PMID: 33913840]
Level 2 (mid-level) evidenceEl-Fadaly G, Ghorab DM, Sorogy HME, Eldin SS, Sabet MA, Teba HE. Sustained Ocular Delivery of Moxifloxacin-Ufasomes-Laden In Situ Gel for Keratitis Management. Pharmaceuticals (Basel, Switzerland). 2026 Feb 13:19(2):. doi: 10.3390/ph19020313. Epub 2026 Feb 13 [PubMed PMID: 41754853]
Agrawal R, See A, Yu Ci FN, Sundar S, Hoskin A, Blanch R, Bhalerao S, Mishra C, Romero J, Natarajan S, Sundar G, Asia Pacific Ophthalmic Trauma Society (APOTS) Taskforce for the Prevention of Blindness and Disability from Ophthalmic Trauma. Ophthalmic Trauma: An Overlooked Global Cause of Preventable Blindness and Disability. American journal of ophthalmology. 2026 May:285():8-15. doi: 10.1016/j.ajo.2026.01.022. Epub 2026 Jan 24 [PubMed PMID: 41587598]
Haring RS, Canner JK, Haider AH, Schneider EB. Ocular injury in the United States: Emergency department visits from 2006-2011. Injury. 2016 Jan:47(1):104-8. doi: 10.1016/j.injury.2015.07.020. Epub 2015 Jul 23 [PubMed PMID: 26275512]
Iftikhar M, Canner JK, Latif A, Shah SMA, Justin GA, Woreta FA. Epidemiology of ophthalmic trauma in the United States from 2009-2018: A Nationwide Emergency Department Sample Analysis. Injury. 2024 Mar:55(3):111209. doi: 10.1016/j.injury.2023.111209. Epub 2023 Nov 17 [PubMed PMID: 38012902]
Sharma N, Kaur M, Agarwal T, Sangwan VS, Vajpayee RB. Treatment of acute ocular chemical burns. Survey of ophthalmology. 2018 Mar-Apr:63(2):214-235. doi: 10.1016/j.survophthal.2017.09.005. Epub 2017 Sep 19 [PubMed PMID: 28935121]
Level 3 (low-level) evidenceHaring RS, Sheffield ID, Channa R, Canner JK, Schneider EB. Epidemiologic Trends of Chemical Ocular Burns in the United States. JAMA ophthalmology. 2016 Oct 1:134(10):1119-1124. doi: 10.1001/jamaophthalmol.2016.2645. Epub [PubMed PMID: 27490908]
Quesada JM, Lloves JM, Delgado DV. Ocular chemical burns in the workplace: Epidemiological characteristics. Burns : journal of the International Society for Burn Injuries. 2020 Aug:46(5):1212-1218. doi: 10.1016/j.burns.2019.11.007. Epub 2019 Nov 30 [PubMed PMID: 31791857]
Level 2 (mid-level) evidenceGhosh S, Salvador-Culla B, Kotagiri A, Pushpoth S, Tey A, Johnson ZK, Figueiredo FC. Acute Chemical Eye Injury and Limbal Stem Cell Deficiency-A Prospective Study in the United Kingdom. Cornea. 2019 Jan:38(1):8-12. doi: 10.1097/ICO.0000000000001739. Epub [PubMed PMID: 30199398]
Anchouche S, Hall N, Bal S, Dana R, Elze T, Miller JW, Lorch AC, Yin J, IRIS Registry Data Analytic Centers. Chemical and thermal ocular burns in the United States: An IRIS registry analysis. The ocular surface. 2021 Jul:21():345-347. doi: 10.1016/j.jtos.2021.03.008. Epub 2021 Mar 31 [PubMed PMID: 33812088]
Kaplan AT, Yalcin SO, Günaydın NT, Kaymak NZ, Gün RD. Ocular-periocular burns in a tertiary hospital: Epidemiologic characteristics. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2023 Jan:76():208-215. doi: 10.1016/j.bjps.2022.10.049. Epub 2022 Nov 2 [PubMed PMID: 36527902]
Gong D, Yan C, Yu F, Yan D, Wu N, Chen L, Zhang S, Fu Y. Direct oral mucosal epithelial transplantation supplies stem cells and promotes corneal wound healing to treat refractory persistent corneal epithelial defects. Experimental eye research. 2022 Feb:215():108934. doi: 10.1016/j.exer.2022.108934. Epub 2022 Jan 7 [PubMed PMID: 35007520]
Poon SHL, Wong WHL, Bu Y, Lo ACY, Jhanji V, Chan YK, Shih KC. A Systematic Review of Emerging Therapeutic Strategies in the Management of Chemical Injuries of the Ocular Surface. Eye & contact lens. 2020 Nov:46(6):329-340. doi: 10.1097/ICL.0000000000000715. Epub [PubMed PMID: 32452924]
Level 1 (high-level) evidenceBarrientez B, Nicholas SE, Whelchel A, Sharif R, Hjortdal J, Karamichos D. Corneal injury: Clinical and molecular aspects. Experimental eye research. 2019 Sep:186():107709. doi: 10.1016/j.exer.2019.107709. Epub 2019 Jun 22 [PubMed PMID: 31238077]
McCulley JP. Ocular hydrofluoric acid burns: animal model, mechanism of injury and therapy. Transactions of the American Ophthalmological Society. 1990:88():649-84 [PubMed PMID: 2095035]
Level 3 (low-level) evidenceXie M, Jie Y. Transforming corneal alkali burn treatment: unveiling mechanisms and pioneering therapies from bench to bedside. Journal of translational medicine. 2025 Oct 21:23(1):1132. doi: 10.1186/s12967-025-07102-0. Epub 2025 Oct 21 [PubMed PMID: 41121132]
Mohseni M, Gurnani B, Blair K. Blunt Eye Trauma. StatPearls. 2026 Jan:(): [PubMed PMID: 29261988]
Gurnani B, Kaur K. Advancing diagnostics in Pythium insidiosum keratitis: the emerging role of point-of-care imaging and biosensor-based detection devices. Expert review of medical devices. 2025 Dec:22(12):1287-1292. doi: 10.1080/17434440.2025.2582616. Epub 2025 Nov 2 [PubMed PMID: 41147335]
Gurnani B, Kaur K. Pythium Keratitis. StatPearls. 2026 Jan:(): [PubMed PMID: 34424645]
Balamurugan S, Gurnani B, Kaur K, Gireesh P, Narayana S. Traumatic intralenticular abscess-What is so different? The Indian journal of radiology & imaging. 2020 Jan-Mar:30(1):92-94. doi: 10.4103/ijri.IJRI_369_19. Epub 2020 Mar 30 [PubMed PMID: 32476758]
Wilson SE. Bowman's layer in the cornea- structure and function and regeneration. Experimental eye research. 2020 Jun:195():108033. doi: 10.1016/j.exer.2020.108033. Epub 2020 Apr 24 [PubMed PMID: 32339517]
Gurnani B, Kaur K. Tips to prevent inadvertent stromal staining and Descemet membrane detachment while performing paracentesis during cataract surgery. Indian journal of ophthalmology. 2023 May:71(5):2300-2301. doi: 10.4103/IJO.IJO_3310_22. Epub [PubMed PMID: 37202984]
Parkash RO, Gurnani B, Kaur K, Parkash TO, Vajpayee RB. Novel trocar assisted intraocular lens and capsular bag complex fixation. European journal of ophthalmology. 2024 Mar:34(2):583-588. doi: 10.1177/11206721231208662. Epub 2023 Oct 26 [PubMed PMID: 37882171]
Meer E, Grob S, Antonsen EL, Sawyer A. Ocular conditions and injuries, detection and management in spaceflight. NPJ microgravity. 2023 May 16:9(1):37. doi: 10.1038/s41526-023-00279-y. Epub 2023 May 16 [PubMed PMID: 37193709]
Willmann D, Fu L, Melanson SW. Corneal Injury. StatPearls. 2026 Jan:(): [PubMed PMID: 29083785]
Dua HS, Ting DSJ, Al Saadi A, Said DG. Chemical eye injury: pathophysiology, assessment and management. Eye (London, England). 2020 Nov:34(11):2001-2019. doi: 10.1038/s41433-020-1026-6. Epub 2020 Jun 22 [PubMed PMID: 32572184]
Agarwal-Harding KJ, Chokotho LC, Mkandawire NC, Martin C Jr, Losina E, Katz JN. Risk Factors for Delayed Presentation Among Patients with Musculoskeletal Injuries in Malawi. The Journal of bone and joint surgery. American volume. 2019 May 15:101(10):920-931. doi: 10.2106/JBJS.18.00516. Epub [PubMed PMID: 31094984]
Fung AT, Tran T, Lim LL, Samarawickrama C, Arnold J, Gillies M, Catt C, Mitchell L, Symons A, Buttery R, Cottee L, Tumuluri K, Beaumont P. Local delivery of corticosteroids in clinical ophthalmology: A review. Clinical & experimental ophthalmology. 2020 Apr:48(3):366-401. doi: 10.1111/ceo.13702. Epub 2020 Jan 22 [PubMed PMID: 31860766]
Jolly R, Arjunan M, Theodorou M, Dahlmann-Noor AH. Eye injuries in children - incidence and outcomes: An observational study at a dedicated children's eye casualty. European journal of ophthalmology. 2019 Sep:29(5):499-503. doi: 10.1177/1120672118803512. Epub 2018 Oct 1 [PubMed PMID: 30270661]
Level 2 (mid-level) evidenceWatson SL, Leung V. Interventions for recurrent corneal erosions. The Cochrane database of systematic reviews. 2018 Jul 9:7(7):CD001861. doi: 10.1002/14651858.CD001861.pub4. Epub 2018 Jul 9 [PubMed PMID: 29985545]
Level 1 (high-level) evidenceFrench Society for Anaesthesia and Intensive Care (SFAR), French Ophthalmology Society (SFO), French-speaking Intensive Care Society (SRLF), Keita H, Devys JM, Ripart J, Frost M, Cochereau I, Boutin F, Guérin C, Fletcher D, Compère V. Eye protection in anaesthesia and intensive care. Anaesthesia, critical care & pain medicine. 2017 Dec:36(6):411-418. doi: 10.1016/j.accpm.2017.08.001. Epub 2017 Aug 5 [PubMed PMID: 28790010]
Rainsbury PG, Cambridge K, Selby S, Lochhead J. Red eyes in children: red flags and a case to learn from. The British journal of general practice : the journal of the Royal College of General Practitioners. 2016 Dec:66(653):633-634 [PubMed PMID: 27884914]
Level 3 (low-level) evidenceSpicer AR, Meleis MM, Buchanan HW 4th, Elliott NC. Endophthalmitis due to a retained intraocular metallic object. The American journal of emergency medicine. 2025 Oct:96():301.e1-301.e2. doi: 10.1016/j.ajem.2025.07.007. Epub 2025 Jul 3 [PubMed PMID: 40653426]
Grosu-Bularda A, Andrei MC, Mladin AD, Ionescu Sanda M, Dringa MM, Lunca DC, Lascar I, Teodoreanu RN. Periorbital lesions in severely burned patients. Romanian journal of ophthalmology. 2019 Jan-Mar:63(1):38-55 [PubMed PMID: 31198897]
El-Hofi AH, Helaly HA. Evaluation of limbal transplantation in eyes with bilateral severe ocular surface damage secondary to chemical injury. Clinical ophthalmology (Auckland, N.Z.). 2019:13():383-390. doi: 10.2147/OPTH.S192316. Epub 2019 Feb 18 [PubMed PMID: 30858688]
Dua HS, King AJ, Joseph A. A new classification of ocular surface burns. The British journal of ophthalmology. 2001 Nov:85(11):1379-83 [PubMed PMID: 11673310]
Asadigandomani H, Momeni A, Nusair O, Daneshvar K, Esmaeilkhanian H, Ghochani G, Ahmadi P, Razavi A, Esfandiari H, Soleimani M. Clinical application of anterior segment optical coherence tomography in ocular emergencies: A comprehensive review. The Journal of international medical research. 2025 Oct:53(10):3000605251382298. doi: 10.1177/03000605251382298. Epub 2025 Oct 8 [PubMed PMID: 41062104]
Gurnani B, Natarajan R, Mohan M, Kaur K. Breaking-Down Barriers: Proposal of Using Cellulose Biosynthesis Inhibitors and Cellulase Enzyme as a Novel Treatment Modality for Vision Threatening Pythium Insidiosum Keratitis. Clinical ophthalmology (Auckland, N.Z.). 2024:18():765-776. doi: 10.2147/OPTH.S450665. Epub 2024 Mar 11 [PubMed PMID: 38495678]
Pokhraj P S, Jigar J P, Mehta C, Narottam A P. Intraocular metallic foreign body: role of computed tomography. Journal of clinical and diagnostic research : JCDR. 2014 Dec:8(12):RD01-3. doi: 10.7860/JCDR/2014/9949.5271. Epub 2014 Dec 5 [PubMed PMID: 25654008]
Level 3 (low-level) evidenceGurnani B, Feroze KB, Patel BC. Neurotrophic Keratitis. StatPearls. 2026 Jan:(): [PubMed PMID: 28613758]
Zhou Y, DiSclafani M, Jeang L, Shah AA. Open Globe Injuries: Review of Evaluation, Management, and Surgical Pearls. Clinical ophthalmology (Auckland, N.Z.). 2022:16():2545-2559. doi: 10.2147/OPTH.S372011. Epub 2022 Aug 10 [PubMed PMID: 35983163]
Chuck RS, Jeng BH, Lum F. Consensus Guidelines versus Evidence-Based Medicine in the Treatment of Corneal Abrasions. Ophthalmology. 2024 May:131(5):524-525. doi: 10.1016/j.ophtha.2024.02.027. Epub [PubMed PMID: 38642953]
Level 3 (low-level) evidenceSulewski M, Leslie L, Liu SH, Ifantides C, Cho K, Kuo IC. Topical ophthalmic anesthetics for corneal abrasions. The Cochrane database of systematic reviews. 2023 Aug 9:8(8):CD015091. doi: 10.1002/14651858.CD015091.pub2. Epub 2023 Aug 9 [PubMed PMID: 37555621]
Level 1 (high-level) evidenceMiller DD, Wagner IV, Ten Hulzen RD, Dorairaj S, Mashayekhi A, Krambeer C, Boopathiraj N, Stewart M. Delayed Corneal Healing After the Use of Topical Ophthalmic Anesthetics. Cureus. 2024 Sep:16(9):e70455. doi: 10.7759/cureus.70455. Epub 2024 Sep 29 [PubMed PMID: 39473690]
Sharifi A, Naisiri N, Shams M, Sharifi M, Sharifi H. Adverse Reactions from Topical Ophthalmic Anesthetic Abuse. Journal of ophthalmic & vision research. 2022 Oct-Dec:17(4):470-478. doi: 10.18502/jovr.v17i4.12297. Epub 2022 Nov 29 [PubMed PMID: 36620720]
Attar A, Chiu ALS, Razmjooei F, Karagiannidou Z, Ranjbar M, Mohammadi M. Topical anesthetic abuse keratopathy: an overlooked occupational eye health concern. Journal of occupational medicine and toxicology (London, England). 2025 Dec 11:21(1):1. doi: 10.1186/s12995-025-00492-3. Epub 2025 Dec 11 [PubMed PMID: 41382108]
Algarni AM, Guyatt GH, Turner A, Alamri S. Antibiotic prophylaxis for corneal abrasion. The Cochrane database of systematic reviews. 2022 May 27:5(5):CD014617. doi: 10.1002/14651858.CD014617.pub2. Epub 2022 May 27 [PubMed PMID: 35622535]
Level 1 (high-level) evidenceNg SM, Leslie L, Tzang CC, Algarni AM, Kuo IC, Lawrenson AL, supported by the Cochrane Eyes and Vision Review Group. Antibiotic prophylaxis for corneal abrasion. The Cochrane database of systematic reviews. 2025 Sep 29:9(9):CD014617. doi: 10.1002/14651858.CD014617.pub3. Epub 2025 Sep 29 [PubMed PMID: 41017778]
Level 1 (high-level) evidenceBrekke SR, Giri P, Byanju R, Pradhan S, Bhandari G, Bhandari S, Kandel RP, Poudyal B, Gonzales JA, Srinivasan M, Upadhyay M, Whitcher JP, O'Brien KS, Lietman TM, Keenan JD, VIEW Trial Study Group. Risk factors for corneal abrasions in Nepal: a community-based study. Eye (London, England). 2024 Apr:38(5):945-950. doi: 10.1038/s41433-023-02809-0. Epub 2023 Nov 10 [PubMed PMID: 37949975]
Cheng ML, Fu L, Cackett P. A novel, safe and cost effective way for teaching corneal foreign body removal. Emergency medicine journal : EMJ. 2015 Jun:32(6):501-2. doi: 10.1136/emermed-2014-204545. Epub 2015 Jan 8 [PubMed PMID: 25573065]
Level 3 (low-level) evidenceMacedo Filho ET, Lago A, Duarte K, Liang SJ, Lima AL, Freitas Dd. Superficial corneal foreign body: laboratory and epidemiologic aspects. Arquivos brasileiros de oftalmologia. 2005 Nov-Dec:68(6):821-3 [PubMed PMID: 17344985]
Moutei H, Tanout S, Bennis A, Chraibi F, Abdellaoui M, Benatiya I. Anterior Segment Optical Coherence Tomography-Assisted Surgical Planning for Removal of a Corneal Foreign Body: A Case Report and Literature Review. La Tunisie medicale. 2024 Nov 5:102(11):955-959. doi: 10.62438/tunismed.v102i11.5209. Epub 2024 Nov 5 [PubMed PMID: 39564643]
Level 3 (low-level) evidencePatterson TJ, McKinney D, Ritson J, McLean C, Gu W, Colyer M, McClellan SF, Miller SC, Justin GA, Hoskin AK, Cavuoto K, Leong J, Ascarza AR, Woreta FA, Miller KE, Caldwell MC, Gensheimer WG, Williamson T, Dhawahir-Scala F, Shah P, Coombes A, Sundar G, Mazzoli RA, Woodcock M, Kuhn F, Watson SL, Gomes RSM, Agrawal R, Blanch RJ. The Use of Preoperative Prophylactic Systemic Antibiotics for the Prevention of Endopthalmitis in Open Globe Injuries: A Meta-Analysis. Ophthalmology. Retina. 2023 Nov:7(11):972-981. doi: 10.1016/j.oret.2023.06.022. Epub 2023 Jul 4 [PubMed PMID: 37406735]
Level 1 (high-level) evidenceKuckelkorn R, Schrage N, Keller G, Redbrake C. Emergency treatment of chemical and thermal eye burns. Acta ophthalmologica Scandinavica. 2002 Feb:80(1):4-10 [PubMed PMID: 11906296]
Clare G, Bunce C, Tuft S. Amniotic membrane transplantation for acute ocular burns. The Cochrane database of systematic reviews. 2022 Sep 1:9(9):CD009379. doi: 10.1002/14651858.CD009379.pub3. Epub 2022 Sep 1 [PubMed PMID: 36047788]
Level 1 (high-level) evidenceGurnani B, Kaur K. Redefining Dry Eye Disease Management: Emerging Pharmacologic and Device-Based Therapies in the Era of Precision Care: A Narrative Review. Ophthalmology and therapy. 2026 May:15(5):1561-1584. doi: 10.1007/s40123-026-01354-9. Epub 2026 Mar 23 [PubMed PMID: 41866434]
Level 3 (low-level) evidenceZareh H, Shahriary A, Razei A, Ameri R, Fasihi-Ramandi M, Aghamollaei H. Doxycycline versus Curcumin for Inhibition of Matrix Metalloproteinase Expression and Activity Following Chemically Induced Inflammation in Corneal Cells. Journal of ophthalmic & vision research. 2024 Jul-Sep:19(3):273-283. doi: 10.18502/jovr.v19i3.13689. Epub 2024 Sep 16 [PubMed PMID: 39359528]
Sharma A, Sharma N, Basu S, Sharma R, Aggarwal S, Gupta PC, Ram J, Nirankari VS. Tissue Adhesives for the Management of Corneal Perforations and Challenging Corneal Conditions. Clinical ophthalmology (Auckland, N.Z.). 2023:17():209-223. doi: 10.2147/OPTH.S394454. Epub 2023 Jan 15 [PubMed PMID: 36685088]
Sacchetti M, Lambiase A. Diagnosis and management of neurotrophic keratitis. Clinical ophthalmology (Auckland, N.Z.). 2014:8():571-9. doi: 10.2147/OPTH.S45921. Epub 2014 Mar 19 [PubMed PMID: 24672223]
Hopkinson A, Figueiredo FC. A Narrative Review of Amniotic Membrane Transplantation in Ocular Surface Repair: Unveiling the Immunoregulatory Pathways for Timely Intervention. Ophthalmology and therapy. 2025 Jul:14(7):1385-1409. doi: 10.1007/s40123-025-01143-w. Epub 2025 May 14 [PubMed PMID: 40360962]
Level 3 (low-level) evidenceGiannaccare G, Lixi F, Slidsborg C, Ozkan G, Gheorghe AG, Arghirescu AM, Namazbayeva A, Monfared M, Singh RB, Jhanji V, Nucci C, Coco G. Current Landscape and Future Prospects of Corneal Regenerative Medicine. Ophthalmology and therapy. 2026 Jan:15(1):85-128. doi: 10.1007/s40123-025-01286-w. Epub 2025 Dec 4 [PubMed PMID: 41343141]
Elhardt C, Schweikert R, Kamnig R, Vounotrypidis E, Wolf A, Wertheimer CM. Recurrence of perforation and overall patient survival after penetrating keratoplasty versus amniotic membrane transplantation in corneal perforation. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2023 Jul:261(7):1933-1940. doi: 10.1007/s00417-022-05914-0. Epub 2023 Jan 21 [PubMed PMID: 36680612]
Gurnani B, Kaur K, Lalgudi VG, Kundu G, Mimouni M, Liu H, Jhanji V, Prakash G, Roy AS, Shetty R, Gurav JS. Role of artificial intelligence, machine learning and deep learning models in corneal disorders - A narrative review. Journal francais d'ophtalmologie. 2024 Sep:47(7):104242. doi: 10.1016/j.jfo.2024.104242. Epub 2024 Jul 15 [PubMed PMID: 39013268]
Level 3 (low-level) evidenceAgarwal S, Srinivasan B, Gupta R, Iyer G. Allogenic Simple Limbal Epithelial Transplantation Versus Amniotic Membrane Grafting in the Early Management of Severe-Grade Ocular Chemical Injuries-A Retrospective Comparative Study. American journal of ophthalmology. 2020 Sep:217():297-304. doi: 10.1016/j.ajo.2020.05.001. Epub 2020 May 11 [PubMed PMID: 32437668]
Level 2 (mid-level) evidenceNakamura T, Takeda K, Inatomi T, Sotozono C, Kinoshita S. Long-term results of autologous cultivated oral mucosal epithelial transplantation in the scar phase of severe ocular surface disorders. The British journal of ophthalmology. 2011 Jul:95(7):942-6. doi: 10.1136/bjo.2010.188714. Epub 2010 Nov 19 [PubMed PMID: 21097786]
McMaster D, Bapty J, Bush L, Serra G, Kempapidis T, McClellan SF, Woreta FA, Justin GA, Agrawal R, Hoskin AK, Cavuoto K, Leong J, Ascarza AR, Cason J, Miller KE, Caldwell MC, Gensheimer WG, Williamson TH, Dhawahir-Scala F, Shah P, Coombes A, Sundar G, Mazzoli RA, Woodcock M, Watson SL, Kuhn F, Colyer M, Gomes RSM, Blanch RJ. Early versus Delayed Timing of Primary Repair after Open-Globe Injury: A Systematic Review and Meta-analysis. Ophthalmology. 2025 Apr:132(4):431-441. doi: 10.1016/j.ophtha.2024.08.030. Epub 2024 Aug 31 [PubMed PMID: 39218161]
Level 1 (high-level) evidenceGeerling G, Maclennan S, Hartwig D. Autologous serum eye drops for ocular surface disorders. The British journal of ophthalmology. 2004 Nov:88(11):1467-74 [PubMed PMID: 15489495]
Ou S, Zhang Y, Feng Y, Zheng X, Lin Y, Zhang L, Zhao S, Su Y, Cai H, Lin L, Gu H, Wu H, Wu Y. Mooren's ulcer: a multifactorial autoimmune peripheral ulcerative keratitis and current treatment protocols. Frontiers in medicine. 2025:12():1630585. doi: 10.3389/fmed.2025.1630585. Epub 2025 Nov 11 [PubMed PMID: 41306497]
Murugan SB, Sunil Kumar, Gurnani B, Kaur K. Assessment of Subjective Visual Experiences During Intraocular Surgery and Intravitreal Injection Among Uveitis Patients at a Tertiary Eye Hospital: A Cross-Sectional Observational Study. Ophthalmology and therapy. 2026 Jan:15(1):173-191. doi: 10.1007/s40123-025-01264-2. Epub 2025 Nov 6 [PubMed PMID: 41196490]
Level 2 (mid-level) evidenceGurnani B, Christy J, Kaur K, Moutappa F, Gubert J. Successful Management of Pythium insidiosum Keratitis Masquerading as Dematiaceous Fungal Keratitis in an Immunosuppressed Asian Male. Ocular immunology and inflammation. 2024 Jul:32(5):583-586. doi: 10.1080/09273948.2023.2179495. Epub 2023 Feb 22 [PubMed PMID: 36812410]
Paulbuddhe V, Addya S, Gurnani B, Singh D, Tripathy K, Chawla R. Sympathetic Ophthalmia: Where Do We Currently Stand on Treatment Strategies? Clinical ophthalmology (Auckland, N.Z.). 2021:15():4201-4218. doi: 10.2147/OPTH.S289688. Epub 2021 Oct 20 [PubMed PMID: 34707340]
Rodríguez-Ares MT, Touriño R, López-Valladares MJ, Gude F. Multilayer amniotic membrane transplantation in the treatment of corneal perforations. Cornea. 2004 Aug:23(6):577-83 [PubMed PMID: 15256996]
Mikropoulos DG, Kymionis GD, Chatzea MS, Xanthopoulou K, Ageladarakis PK, Voudouragkaki IC, Konstas AG. Acute Corneal Melting Induced by the Concomitant Use of a Non-steroidal Anti-inflammatory Agent with an Antiseptic Eye Drop. Ophthalmology and therapy. 2024 Feb:13(2):645-649. doi: 10.1007/s40123-023-00864-0. Epub 2023 Dec 21 [PubMed PMID: 38127195]
Velušček M, Bajrović FF, Strle F, Stupica D. Doxycycline-induced photosensitivity in patients treated for erythema migrans. BMC infectious diseases. 2018 Aug 3:18(1):365. doi: 10.1186/s12879-018-3270-y. Epub 2018 Aug 3 [PubMed PMID: 30075748]
Katzman LR, Jeng BH. Management strategies for persistent epithelial defects of the cornea. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2014 Jul:28(3):168-72. doi: 10.1016/j.sjopt.2014.06.011. Epub 2014 Jul 2 [PubMed PMID: 25278792]
Ahmad S. Concise review: limbal stem cell deficiency, dysfunction, and distress. Stem cells translational medicine. 2012 Feb:1(2):110-5. doi: 10.5966/sctm.2011-0037. Epub 2012 Jan 26 [PubMed PMID: 23197757]
Gupta N, Kalaivani M, Tandon R. Comparison of prognostic value of Roper Hall and Dua classification systems in acute ocular burns. The British journal of ophthalmology. 2011 Feb:95(2):194-8. doi: 10.1136/bjo.2009.173724. Epub 2010 Aug 30 [PubMed PMID: 20805137]
Awasthi P, Singh P, Raj A. Surgical Management and Recent Advances in Chemical Injury: A 5-year Review. Seminars in ophthalmology. 2022 Jan 2:37(1):49-56. doi: 10.1080/08820538.2021.1909076. Epub 2021 Apr 25 [PubMed PMID: 33896370]
Level 3 (low-level) evidenceHe H, Liu H, Chen X, Wu J, He M, Zhong X. Diagnosis and Treatment of Pythium Insidiosum Corneal Ulcer in a Chinese Child: A Case Report and Literature Review. The American journal of case reports. 2016 Dec 27:17():982-988 [PubMed PMID: 28025573]
Level 3 (low-level) evidenceEslani M, Baradaran-Rafii A, Cheung AY, Kurji KH, Hasani H, Djalilian AR, Holland EJ. Amniotic Membrane Transplantation in Acute Severe Ocular Chemical Injury: A Randomized Clinical Trial. American journal of ophthalmology. 2019 Mar:199():209-215. doi: 10.1016/j.ajo.2018.11.001. Epub 2018 Nov 10 [PubMed PMID: 30419194]
Level 1 (high-level) evidenceChoi SH, Kim MK, Oh JY. Glaucoma after ocular chemical burns: Incidence, risk factors, and outcome. Scientific reports. 2020 Mar 16:10(1):4763. doi: 10.1038/s41598-020-61822-5. Epub 2020 Mar 16 [PubMed PMID: 32179804]
Vaidyanathan U, Hopping GC, Liu HY, Somani AN, Ronquillo YC, Hoopes PC, Moshirfar M. Persistent Corneal Epithelial Defects: A Review Article. Medical hypothesis, discovery & innovation ophthalmology journal. 2019 Fall:8(3):163-176 [PubMed PMID: 31598519]
Shah SS, Gurnani B. Lens-Induced Glaucoma. StatPearls. 2026 Jan:(): [PubMed PMID: 34662038]
Ray A, Gurnani B. Pediatric Cataract. StatPearls. 2026 Jan:(): [PubMed PMID: 34283446]
Gurnani B, Kaur K. Post-market surveillance of ophthalmic implants: role of real-world evidence. Expert review of medical devices. 2025 Dec:22(12):1303-1308. doi: 10.1080/17434440.2025.2579578. Epub 2025 Oct 24 [PubMed PMID: 41123186]
Ghafarian S, Koo EH. Long-Term Graft Survival and Visual Outcomes in Deep Anterior Lamellar Keratoplasty (DALK): A Narrative Review. Journal of ophthalmology. 2026:2026():8120487. doi: 10.1155/joph/8120487. Epub 2026 Feb 23 [PubMed PMID: 41737287]
Level 3 (low-level) evidencevan Nispen RM, Virgili G, Hoeben M, Langelaan M, Klevering J, Keunen JE, van Rens GH. Low vision rehabilitation for better quality of life in visually impaired adults. The Cochrane database of systematic reviews. 2020 Jan 27:1(1):CD006543. doi: 10.1002/14651858.CD006543.pub2. Epub 2020 Jan 27 [PubMed PMID: 31985055]
Level 1 (high-level) evidenceAl-Saleh GS, Alfawaz AM. Management of traumatic corneal abrasion by a sample of practicing ophthalmologists in Saudi Arabia. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2018 Apr-Jun:32(2):105-109. doi: 10.1016/j.sjopt.2017.10.007. Epub 2017 Oct 31 [PubMed PMID: 29942177]
Guevara-Villarreal DA, Rodríguez-Valdés PJ. Posterior Segment Intraocular Foreign Body: Extraction Surgical Techniques, Timing, and Indications for Vitrectomy. Journal of ophthalmology. 2016:2016():2034509. doi: 10.1155/2016/2034509. Epub 2016 Nov 29 [PubMed PMID: 28025619]
Gurnani B, Kaur K. Teleophthalmology-enabled devices: bridging the gap in rural eye care. Expert review of medical devices. 2025 Nov:22(11):1167-1172. doi: 10.1080/17434440.2025.2566741. Epub 2025 Oct 15 [PubMed PMID: 40990172]
Nishant P, Gurnani B, Singh P, Sinha S, Kaur K, Kumar A, Sinha RK. Current concepts and recent trends in endothelial keratoplasty. World journal of transplantation. 2025 Jun 18:15(2):102507. doi: 10.5500/wjt.v15.i2.102507. Epub [PubMed PMID: 40535500]
Gurnani B, Kaur K, Chaudhary S, Gandhi AS, Balakrishnan H, Mishra C, Gosalia H, Dhiman S, Joshi S, Nagtode AH, Jain S, Aguiar M, Rustagi IM. Nystagmus in Clinical Practice: From Diagnosis to Treatment-A Comprehensive Review. Clinical ophthalmology (Auckland, N.Z.). 2025:19():1617-1657. doi: 10.2147/OPTH.S523224. Epub 2025 May 17 [PubMed PMID: 40401036]
Burrow MK, Gurnani B, Patel BC. Keratoconjunctivitis. StatPearls. 2026 Jan:(): [PubMed PMID: 31194419]
Okoye GS, Bonabe D, Obasi CU, Munikrishna D, Osho F, Mutali M, Ogwumu K, Oke-Ifidon EO, Nathan IG, Enaholo ES, Suleman AI, Chukwuyem C, Enang AE, Oji RC, Ogechukwu VN, Chidera SP, Ogechukwu HC, Kaur K, Gurnani B. Visual outcomes and complications after phacoemulsification and small incision manual cataract surgery in two eye hospitals. Journal francais d'ophtalmologie. 2025 Jan:48(1):104353. doi: 10.1016/j.jfo.2024.104353. Epub 2024 Nov 18 [PubMed PMID: 39561679]
Gurnani B, Kaur K, Chaudhary S, Kaur RP, Nayak S, Mishra D, Balakrishnan H, Parkash RO, Morya AK, Porwal A. Pediatric corneal transplantation: techniques, challenges, and outcomes. Therapeutic advances in ophthalmology. 2024 Jan-Dec:16():25158414241237906. doi: 10.1177/25158414241237906. Epub 2024 Mar 25 [PubMed PMID: 38533487]
Level 3 (low-level) evidenceKaur K, Srividya KS, Kabra N, Saranath R, Gurnani B, Venkatesh R. Patterns of ophthalmic emergencies presenting to a tertiary eye care hospital in India. Indian journal of ophthalmology. 2024 Feb 1:72(2):296-297. doi: 10.4103/IJO.IJO_1578_23. Epub 2024 Jan 25 [PubMed PMID: 38273691]
Gurnani B, Tripathy K. Minimally Invasive Glaucoma Surgery. StatPearls. 2026 Jan:(): [PubMed PMID: 35881761]
Christensen JM, Shanbhag SS, Shih GC, Goverman J, Pomahac B, Chodosh J, Ehrlichman RJ. Multidisciplinary Treatment to Restore Vision in Ocular Burns. Journal of burn care & research : official publication of the American Burn Association. 2020 Jul 3:41(4):859-865. doi: 10.1093/jbcr/irz201. Epub [PubMed PMID: 31808803]
Dave VP, Pathengay A, Braimah IZ, Panchal B, Sharma S, Pappuru RR, Mathai A, Tyagi M, Narayanan R, Jalali S, Das T. ENTEROCOCCUS ENDOPHTHALMITIS: Clinical Settings, Antimicrobial Susceptibility, and Management Outcomes. Retina (Philadelphia, Pa.). 2020 May:40(5):898-902. doi: 10.1097/IAE.0000000000002462. Epub [PubMed PMID: 30681640]
Ross M, Deschênes J. Practice patterns in the interdisciplinary management of corneal abrasions. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 2017 Dec:52(6):548-551. doi: 10.1016/j.jcjo.2017.03.016. Epub 2017 May 10 [PubMed PMID: 29217021]
Morya AK, Shrivastava AK, Janti SS, Tejaswini A, Gupta R, Gurnani B, Venkatesh D, Prasad R. Effect of Asanas in Yoga on Intraocular Pressure of Practicing Healthy Individuals: a Prospective Observational Study. Maedica. 2023 Jun:18(2):238-245. doi: 10.26574/maedica.2023.18.2.238. Epub [PubMed PMID: 37588839]
Level 2 (mid-level) evidenceGurnani B, Kaur K. Intricate clinical evaluation and management strategies in vision-threatening phacomorphic glaucoma. Taiwan journal of ophthalmology. 2023 Apr-Jun:13(2):259-260. doi: 10.4103/2211-5056.353131. Epub 2022 Aug 2 [PubMed PMID: 37484623]
Bejjenki P, Gurnani B, Kaur K, Tejaswini A, Sinha A, Venkatesh D, Morya AK. Commentary: Impact of manual small-incision cataract surgery on outreach and training curriculum across the world. Indian journal of ophthalmology. 2023 Jun:71(6):2478-2479. doi: 10.4103/ijo.IJO_2230_22. Epub [PubMed PMID: 37322665]
Level 3 (low-level) evidenceEngle RL, Mohr DC, Holmes SK, Seibert MN, Afable M, Leyson J, Meterko M. Evidence-based practice and patient-centered care: Doing both well. Health care management review. 2021 Jul-Sep 01:46(3):174-184. doi: 10.1097/HMR.0000000000000254. Epub 2019 Jun 24 [PubMed PMID: 31233424]