Introduction
Colonic diverticular disease includes diverticulosis and diverticulitis. Diverticulosis is characterized by outpouchings in the wall of the gastrointestinal tract called diverticula. These diverticula are most commonly found in the colon, especially in the sigmoid colon. Diverticulosis is usually asymptomatic, but diverticulitis develops when diverticula become inflamed or infected. Diverticulitis is categorized as uncomplicated or complicated. While milder cases of diverticulitis can be managed conservatively without antibiotics, most are successfully managed in the outpatient setting with oral antibiotics and temporary dietary restrictions. More complicated cases may require hospitalization for parenteral hydration and antibiotics, and percutaneous drainage or surgery may be required. The decision to perform elective sigmoid colectomy in patients who recover from uncomplicated diverticulitis is controversial, requiring case-by-case consideration, whereas surgery is more often recommended for complicated diverticulitis.[1]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Diverticulosis is composed of outpouchings of the colonic mucosa and submucosa with or without the serosa protruding through the muscularis layer (see Image. Colon, Diverticulum). Inflammation of these outpouchings may lead to diverticulitis. The presumed cause of diverticulitis is fecal obstruction of diverticula, leading to bacterial overgrowth and subsequent mucosal inflammation and microperforations. This theory has been challenged in recent years, and some studies have shown that patients with acute uncomplicated diverticulitis may be managed without antibiotics.[2]
Epidemiology
The prevalence of diverticulosis is highest in Western countries and in those that follow Western lifestyles and diets. The prevalence increases with age, with over 50% of individuals aged 60 and older having diverticulosis.[3] However, more recent studies demonstrate that the prevalence of diverticulosis is also increasing in younger populations. Between 1997 and 2018, the number of hospitalizations for diverticular disease increased by 32%.[4] Right-sidedness is more common in Asian countries than in the West, although its prevalence varies widely across reported studies.[5] One particular study found that vegetarians in Asia have a lower incidence of right-sided diverticulosis than a control group that ingested a more varied diet (6.1% versus 9.9%).[6]
Diverticulosis is left-sided in up to 90% of affected individuals in Western countries, while diverticular bleeding occurs in the right colon in 50% to 90% of people with diverticulosis. Right-sided diverticulosis and diverticular bleeding are substantially more frequent in Black than in White individuals. In Asia, diverticular bleeding is twice as common in men as in women and is more common (47%) in people with both left and right-sided diverticulosis. In Asia, while diverticular bleeding is more common in men aged 70 and older, this condition is becoming more common in younger people.[7]
The rates of diverticulitis are higher in males among patients younger than 50, whereas among those older than 50, they are higher in females. Despite the significant prevalence of diverticulosis, only approximately 4% of individuals with diverticulosis develop diverticulitis in their lifetime. In contrast, the prevalence of diverticulosis in Asian countries is estimated to be 10% to 29%.[8] The approximate incidence of diverticulitis in the United States is 180 per 100,000 people annually. Furthermore, diverticulitis is responsible for about 200,000 hospital admissions annually, and its health care expenditure exceeds $6.3 billion.[9]
Pathophysiology
The pathophysiology of diverticulosis and diverticulitis is not well understood. However, multiple theories exist, with more recent evidence suggesting an interaction among connective tissue degradation, lifestyle factors, and genetic predisposition.[10] A diverticulum can form at a point of natural weakness where the vasa recta penetrates the colonic wall to supply blood to the mucosa and submucosa. Dysregulation of colonic peristalsis results in nonpropulsive segments with high intraluminal pressure, leading to herniation through the muscularis layer.
The sigmoid colon frequently exhibits impaired motility in patients with diverticulosis.[10] Increased pressure from straining and constipation was once thought to be the initiating factor resulting in this colonic wall herniation. However, this theory is currently under question.[11] Genetic susceptibility and dysregulation in host immune response are also associated with diverticulum development.[2] Similar mechanisms are thought to be responsible for the formation of right colon diverticula as for those elsewhere in the colon. While some right colon diverticula are congenital, the majority are acquired.
The role of fiber in the development of diverticula has been questioned because stool liquidity and luminal diameter differ between the right and left colon. However, wall tension in the right colon is greater in patients with right-sided diverticulosis than in controls, so these differences may not be significant.[12][13][14] Genetic factors seem to be more important in the development of right colon diverticulosis.[2]
The anatomic distribution of diverticulosis and diverticulitis varies by population demographics. In the United States and Western Europe, diverticular disease occurs predominantly in the left colon, with up to 90% of cases exclusively in the sigmoid colon. In Asia, diverticular disease often occurs in younger people and predominantly occurs in the right colon.[8]
In the past, patients with diverticular disease were discouraged from eating nuts, seeds, and popcorn, but a large prospective study has determined that these foods do not increase the risk of developing diverticulitis.[15] Although environmental factors play a significant role in the development of diverticulosis, studies of identical twins have also identified a strong genetic predisposition.
Risk factors for diverticular disease include:
- Age older than 65 years
- White race (for diverticulosis, but not for diverticulitis)
- Hypertension
- Type 2 diabetes
- Overweight (body mass index ≥30 kg/m2)
- Low insoluble fiber diet, high red meat consumption
- Medications eg, opioids, steroids, and nonsteroidal anti-inflammatory drugs
- Low levels of exercise
- Tobacco use [16]
- A variant in the tumor necrosis factor superfamily member 15 (TNFSF15) gene
- Connective tissue disorders, eg, polycystic kidney disease, Marfan syndrome, and Ehlers-Danlos syndrome [2]
Histopathology
False diverticula involve the mucosa and submucosa of the colonic wall and are typically congenital, whereas true diverticula involve the serosa and are usually acquired. Diverticula protrude through defects in the circular muscle layer, where the vasa recta (blood vessels) usually penetrate, covered by a thin layer of longitudinal muscle or adventitia. The mucosa within diverticula typically shows lymphocytic infiltration, indicative of chronic inflammation, and may also show fibrosis and surface erosions, especially when associated with intradiverticular fecaliths. Left-sided diverticula are acquired false diverticula, whereas right-sided diverticula are solitary true diverticula, or more often a combination of both false and true lesions.[17]
Additional findings in the histopathology of diverticula include myochosis, a prominent hypertrophy or hyperplasia of the circular muscle layer, shortening of the taenia coli, and chronic inflammatory cells (lymphocytes and plasma cells) infiltrating the lamina propria. The mucosa may show depletion of mucin, lymphoid hyperplasia, or pseudohypertrophy, similar to findings in inflammatory bowel disease (IBD). The submucosa may show hemosiderin deposits, indicative of previous hemorrhage. In the setting of acute diverticulitis, neutrophilic infiltration, ulceration, and, in some cases, microabscess formation or mucosal perforation are noted.[18]
History and Physical
Most patients with diverticulosis remain asymptomatic, with diverticula often identified incidentally on imaging or colonoscopy. No characteristic symptoms reliably indicate the presence of diverticulosis. Suspicion for acute diverticulitis arises when a patient presents with fever and abdominal pain, most commonly localized to the left lower quadrant. Left lower quadrant pain represents the most frequent presenting symptom, occurring in 70% of patients with acute diverticulitis.
Acute complicated diverticulitis may manifest with diffuse abdominal pain, fecaluria, pneumaturia, or peritonitis, accompanied by signs and symptoms of sepsis. Physical examination may reveal abdominal distension, lower abdominal tenderness, typically in the left lower quadrant, and localized or diffuse peritoneal signs, including involuntary guarding and rebound tenderness.
Evaluation
When the clinical presentation and physical exam are suspicious for acute diverticulitis, laboratory testing and confirmatory imaging studies are the next steps (see Image. Acute Uncomplicated Diverticulitis). Laboratory findings include leukocytosis and elevated inflammatory markers, most often a C-reactive protein (CRP). A computed tomography (CT) scan of the abdomen and pelvis with intravenous (IV) contrast is the gold standard for diagnosis, with 98% to 99% sensitivity and 99% to 100% specificity.[9][6] CT findings of colonic wall thickening and fat stranding are consistent with diverticulitis (see Image. Uncomplicated Diverticulitis). Evidence of an intra-abdominal phlegmon, abscesses, extraluminal free air, and fistula formation indicates complicated diverticulitis (see Image. Complicated Diverticulitis).[19] Repeat CT imaging is warranted if complications are suspected or if symptoms of uncomplicated diverticulitis fail to improve or worsen despite treatment.[20] Colonoscopy during an acute episode of diverticulitis is contraindicated due to the risk of intestinal perforation.
Treatment / Management
The management of uncomplicated diverticulosis focuses on reducing the risk of additional diverticula by following a high-insoluble-fiber diet, with or without fiber supplementation. Adequate hydration is important, as it helps prevent constipation from the additional fiber.
Uncomplicated Diverticulitis
The management of acute diverticulitis differs for uncomplicated and complicated disease. Medical management of acute uncomplicated diverticulitis is performed on an outpatient basis, and consists of pain control (usually with acetaminophen and not with NSAIDs and a clear liquid diet. The traditional practice of treating all cases of acute uncomplicated diverticulitis with routine antibiotics is changing. The American Gastroenterology Association (AGA) recommends that antibiotic treatment be used selectively rather than routinely in immunocompetent patients with mild, acute, uncomplicated diverticulitis. However, antibiotics remain strongly advised for immunocompromised patients.[21] Despite multiple recent studies demonstrating no differences in recurrence or complications in the management of acute uncomplicated diverticulitis without antibiotics, adoption of this practice remains controversial, with 50% of surgeons reporting they would continue to treat uncomplicated diverticulitis with antibiotics.[21][22][23](A1)
Antibiotics should cover gram-negative bacteria and anaerobes. The most commonly prescribed regimens include oral amoxicillin-clavulanate or a combination of an oral fluoroquinolone and metronidazole for 7 to 10 days. Alternatives when these regimens cannot be prescribed include trimethoprim-sulfamethoxazole with metronidazole, moxifloxacin alone, or aztreonam/avibactam. Bowel rest or a clear liquid diet until symptoms improve is recommended for comfort. As symptoms subside, a low-residue diet should be started. Over several weeks, fiber should be gradually increased, and a high-fiber diet should be resumed to reduce the risk of diverticulitis recurrence.
Patients who are febrile, unable to maintain hydration, immunocompromised, or who have multiple medical comorbidities require hospitalization for treatment with IV antibiotics. Any patient who fails to improve within 72 hours or whose clinical condition worsens on treatment should undergo repeat evaluation, including laboratory studies and a CT scan, to rule out evolving complications.[24]
After the resolution of an acute episode of diverticulitis, colon cancer should be ruled out, as the 2 illnesses can be mistaken for one another on a CT scan. One study found that the risk of colon cancer was higher in patients with complicated diverticulitis (7.9%) compared with patients with uncomplicated diverticulitis (1.3%).[25] According to the AGA and American Society of Colon and Rectal Surgeons (ASCRS) guidelines, an interval colonoscopy should be considered 6 to 8 weeks after an acute episode of uncomplicated diverticulitis if a patient has not had a colonoscopy within the past year, and in all cases of complicated diverticulitis.[21][22](A1)
Complicated Diverticulitis
Current recommendations emphasize that selection criteria for elective surgery should be individualized to the patient based on disease severity, comorbidities, and patient preferences and values. The ASCRS recommends elective sigmoid colectomy for acute complicated diverticulitis.[22] The decision to pursue elective sigmoid colectomy should not be based solely on the number of episodes of acute uncomplicated diverticulitis; an informed decision should be made by considering the benefits and risks in each patient's situation. Surgery for recurrent uncomplicated diverticulitis, or after resolution of complicated diverticulitis, is performed via an open, laparoscopic, or robotic approach and involves removing the sigmoid colon and performing a primary anastomosis to reconnect the healthy colon to the rectum. Recurrent diverticulitis is still possible, however, as it may affect any part of the colon.(A1)
Management of acute complicated diverticulitis usually requires admission and is guided by the modified Hinchey classification (see Table. Management of Diverticulitis Based on Modified Hinchey Classification).[19] Patients presenting with hemodynamic instability and signs of peritonitis are candidates for emergent surgery. If intraoperative findings are consistent with complicated diverticulitis, the traditional operation to perform is a Hartmann procedure (proctosigmoidectomy), which includes resection of the diseased sigmoid colon, preservation of the healthy rectum with closure of the rectal stump, and creation of an end colostomy. This procedure eliminates the risk of an anastomotic leak. Takedown of the colostomy with reanastomosis may be considered in 3 to 6 months. However, it is performed in only 31% to 69% of patients due to older age and multiple comorbidities.[26][27](B2)
The decision to perform a primary anastomosis with or without a diverting ostomy during the index operation is based on patient factors, intraoperative findings, and surgeon preference. Based on more recent evidence showing no difference in wound infections, morbidity, or mortality between the Hartmann procedure and primary anastomosis for Hinchey III and IV diverticulitis, the ASCRS clinical practice guideline supports primary anastomosis when possible.[28][29][30] The modified Hinchey classification system is useful for grading disease severity in diverticulitis based on CT findings and helps guide treatment (see Image. Modified Hinchey Classification of Diverticulitis).(A1)
Table. Management of Diverticulitis Based on Modified Hinchey Classification
| Modified Hinchey Classification | Description | Management |
| 0 | Acute uncomplicated diverticulitis | Liquid diet, advanced as tolerated; avoid antibiotics unless immunocompromised, multiple comorbidities, CRP >140 |
| I | Pericolonic abscess | Antibiotics; liquid diet, advanced as tolerated |
| IIa | Abscess separate from the colonic wall, accessible for percutaneous drainage | Percutaneous drainage |
| IIb | Complex abscesses fistulized from a diverticulum | Percutaneous drainage |
| III | Generalized peritonitis with purulent drainage | Surgery |
| IV | Fecal peritonitis | Surgery |
Differential Diagnosis
Diverticulitis can occur anywhere in the colon, with presenting symptoms often reflecting the involved segment. Therefore, a high index of suspicion for acute diverticulitis is required as it can mimic other gastrointestinal, urogenital, and vascular diseases.[31] The list of differential diagnoses for acute diverticulitis is extensive, including:
- Infectious or ischemic colitis
- Inflammatory bowel disease
- Irritable bowel syndrome
- Sigmoid volvulus
- Endometriosis
- Ureterolithiasis
- Acute cystitis
- Ovarian torsion
- Acute gastritis
- Acute pancreatitis
- Acute appendicitis
- Acute cholecystitis
- Acute pyelonephritis
- Mesenteric ischemia
- Constipation
- Pelvic inflammatory disease
- Ectopic pregnancy
Pertinent Studies and Ongoing Trials
Multiple studies have demonstrated that well-selected immunocompetent patients with mild, uncomplicated acute diverticulitis may be treated without antibiotics. The DIABOLO trial is a key randomized controlled trial that showed no significant difference in recovery between patients without antibiotics and those receiving traditional antibiotic treatment.[32] The DINAMO study is another key randomized controlled trial that showed no significant difference in emergency department revisits or hospitalization rates among patients with mild, acute, uncomplicated diverticulitis treated with or without antibiotics.[33]
According to the modified Hinchey classification, patients with Hinchey III and IV lesions require surgical intervention to achieve source control. Traditionally, patients with generalized peritonitis from perforated diverticulitis undergo a Hartmann procedure. However, multiple studies have demonstrated similar or improved outcomes with primary anastomosis with or without a diverting ostomy during the index surgery. The DIVERTI trial was the first prospective, multicenter, randomized controlled trial that evaluated primary anastomosis in patients with Hinchey III and IV diverticulitis. The trial found no significant differences in complication rates, ICU or hospital length of stay, or morbidity between patients undergoing a Hartmann procedure and those undergoing primary anastomosis with diverting ostomy.[34] A follow-up study by the same research team concluded that patients who underwent a primary anastomosis experienced fewer long-term complications and higher quality-of-life scores than those who underwent a Hartmann procedure.[35]
Prognosis
The prognosis for patients with diverticulitis depends on individual patient factors and disease severity, including the presence of complications. After the first episode of acute diverticulitis, up to 30% of patients will experience a recurrent episode, with a progressively higher likelihood of further recurrences with successive episodes.[8]
The 30-day mortality rate for all patients admitted to the hospital with acute diverticulitis is 2.7%. This number is skewed by the mortality rate of high-risk patients with acute complicated diverticulitis requiring emergent surgery, which is about 7%, as well as the majority of acute diverticulitis patients who do not require hospitalization.[8] Immunocompromised patients have higher morbidity and mortality from acute sigmoid diverticulitis.[36]
Complications
Many complications can occur in a patient with diverticulitis. Immunocompromised patients are more likely to present with severe cases and complicated disease, require a Hartmann procedure when surgery is indicated, and stay longer in the hospital.[37] The following are the possible complications of diverticulitis:
- Intestinal perforation
- Intra-abdominal abscess or phlegmon
- Bleeding
- Intestinal fistula (eg, colovesical fistula, colovaginal fistula, colocolonic fistula, coloenteric fistula)
- Intestinal obstruction
- Generalized peritonitis (purulent, feculent)
- Colonic stricture formation
- Sepsis
- Portal vein thrombosis or pylephlebitis: Diverticulitis causes a hypercoagulable state, leading to clot formation in the portal, superior mesenteric, or inferior mesenteric vein. Mortality is up to 25%, and treatment with antibiotics and anticoagulation, the latter for up to 6 months, is critical and must be instituted promptly.[38] Surgery is indicated if this complication results in bowel infarction, persistent infection, or perforation.[39]
Consultations
The care of patients with diverticulitis depends on interprofessional teams, including primary care clinicians, internists, gastroenterologists, general or colorectal surgeons, infectious disease specialists, pharmacists, dietitians, and colostomy care nurses, all working collaboratively to provide optimal patient care.
Deterrence and Patient Education
Deterrence in diverticular disease focuses on risk reduction and prevention of progression from asymptomatic diverticulosis to diverticulitis. Although diverticulosis is highly prevalent and often requires no treatment when asymptomatic, clinicians should counsel patients on modifiable risk factors that influence disease development and recurrence. Evidence supports a high-fiber diet, reduced red meat intake, regular physical activity, weight optimization, and avoidance of tobacco use to mitigate inflammation and improve colonic health. Medication review is also essential, with efforts to minimize corticosteroids, opioids, and nonsteroidal anti-inflammatory drugs when clinically appropriate. Patients should be informed that consumption of nuts, seeds, and popcorn has not been shown to increase the risk of diverticular disease, helping to dispel outdated dietary restrictions.
Patient education plays a central role in early recognition and timely care. Individuals should be instructed to seek medical evaluation for symptoms such as abdominal pain, fever, or blood in the stool, which may indicate complications or alternative diagnoses. Clear communication regarding symptom monitoring, adherence to dietary recommendations, and follow-up care enhances patient engagement, supports shared decision-making, and reduces the risk of delayed diagnosis and preventable complications.
Enhancing Healthcare Team Outcomes
Colonic diverticular disease includes diverticulosis, characterized by mucosal outpouchings, and diverticulitis, which arises from inflammation or infection, likely due to obstruction, bacterial overgrowth, and microperforation. The increasing incidence across all age groups contributes to a substantial healthcare burden in the United States. Patients commonly present with left lower quadrant abdominal pain, fever, and leukocytosis, though presentations may be atypical in immunocompromised individuals. CT imaging confirms the diagnosis and distinguishes uncomplicated from complicated disease. Most uncomplicated cases are managed outpatient with analgesia, dietary modification, and selective antibiotic use, while complicated diverticulitis may require hospitalization, drainage, or surgery. Individualized decisions regarding elective colectomy and interval colonoscopy are essential to reduce recurrence and exclude malignancy.
Interprofessional collaboration enhances outcomes through coordinated, patient-centered care. Physicians, primary care clinicians, and advanced practitioners lead diagnosis, risk stratification, and management decisions, while surgeons evaluate for operative indications and ensure informed consent. Nurses monitor symptoms and reinforce education, pharmacists support antibiotic stewardship and medication safety, and dietitians guide nutritional modification. Effective communication, shared decision-making, and timely referral reduce complications, support adherence, and ensure appropriate follow-up, improving safety and quality of care.
Media
(Click Image to Enlarge)
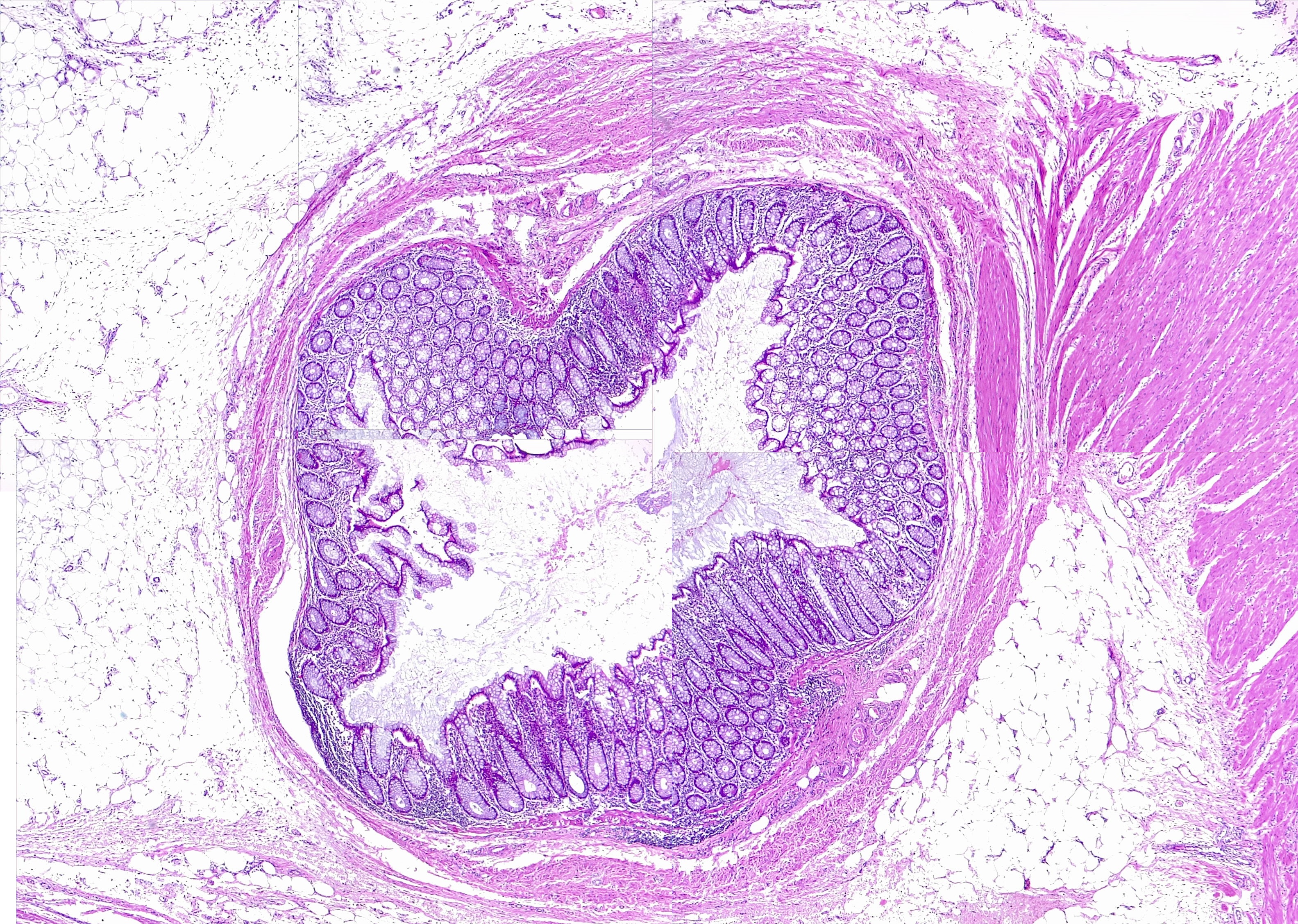
Colon, Diverticulum. Diverticulosis. H/E 1×
Contributed by F Farci, MD
(Click Image to Enlarge)

Acute Uncomplicated Diverticulitis. When the clinical presentation and physical exam are suspicious for acute diverticulitis, laboratory testing and confirmatory imaging studies are the next steps.
Contributed by S Lange, MD
(Click Image to Enlarge)

Uncomplicated Diverticulitis. CT findings of colonic wall thickening and fat stranding are consistent with diverticulitis.
Contributed by S Carr, MD, and A Velasco, MD
(Click Image to Enlarge)

Complicated Diverticulitis. Evidence of an intra-abdominal phlegmon, abscesses, extraluminal free air, and fistula formation indicates complicated diverticulitis.
Contributed by S Carr, MD, and A Velasco, MD
References
Hall JK, Supiano MA, Cohan JN. Diverticulitis in Older Adults: A Review of Etiology, Diagnosis, and Management. Journal of the American Geriatrics Society. 2025 May:73(5):1598-1607. doi: 10.1111/jgs.19388. Epub 2025 Feb 8 [PubMed PMID: 39921851]
Schieffer KM, Kline BP, Yochum GS, Koltun WA. Pathophysiology of diverticular disease. Expert review of gastroenterology & hepatology. 2018 Jul:12(7):683-692. doi: 10.1080/17474124.2018.1481746. Epub 2018 Jun 7 [PubMed PMID: 29846097]
Everhart JE, Ruhl CE. Burden of digestive diseases in the United States part II: lower gastrointestinal diseases. Gastroenterology. 2009 Mar:136(3):741-54. doi: 10.1053/j.gastro.2009.01.015. Epub 2009 Jan 21 [PubMed PMID: 19166855]
Fialho A, Fialho A, Shuja A. Analysis of the Epidemiological Trends on Inpatient Diverticulosis Admissions in the US: A Longitudinal Analysis From 1997-2018. Cureus. 2023 Feb:15(2):e34493. doi: 10.7759/cureus.34493. Epub 2023 Feb 1 [PubMed PMID: 36743907]
Level 2 (mid-level) evidenceTurner GA, O'Grady MJ, Purcell RV, Frizelle FA. The Epidemiology and Etiology of Right-Sided Colonic Diverticulosis: A Review. Annals of coloproctology. 2021 Aug:37(4):196-203. doi: 10.3393/ac.2021.00192.0027. Epub 2021 Jul 21 [PubMed PMID: 34284562]
Tursi A, Scarpignato C, Strate LL, Lanas A, Kruis W, Lahat A, Danese S. Colonic diverticular disease. Nature reviews. Disease primers. 2020 Mar 26:6(1):20. doi: 10.1038/s41572-020-0153-5. Epub 2020 Mar 26 [PubMed PMID: 32218442]
Imaeda H, Hibi T. The Burden of Diverticular Disease and Its Complications: West versus East. Inflammatory intestinal diseases. 2018 Dec:3(2):61-68. doi: 10.1159/000492178. Epub 2018 Aug 7 [PubMed PMID: 30733949]
Neylan CJ, Kim A, Amy M, Hernandez PT. The Epidemiology of Diverticulitis. Clinics in colon and rectal surgery. 2025 Jul:38(4):241-248. doi: 10.1055/s-0044-1791282. Epub 2024 Oct 4 [PubMed PMID: 40501530]
Brown RF, Lopez K, Smith CB, Charles A. Diverticulitis: A Review. JAMA. 2025 Jul 24:():. doi: 10.1001/jama.2025.10234. Epub 2025 Jul 24 [PubMed PMID: 40705318]
Tursi A. Current and Evolving Concepts on the Pathogenesis of Diverticular Disease. Journal of gastrointestinal and liver diseases : JGLD. 2019 Jun 1:28():225-235. doi: 10.15403/jgld-184. Epub 2019 Jun 1 [PubMed PMID: 31204408]
Rezapour M, Ali S, Stollman N. Diverticular Disease: An Update on Pathogenesis and Management. Gut and liver. 2018 Mar 15:12(2):125-132. doi: 10.5009/gnl16552. Epub [PubMed PMID: 28494576]
Elisei W, Tursi A. The Pathophysiology of Colonic Diverticulosis: Inflammation versus Constipation? Inflammatory intestinal diseases. 2018 Dec:3(2):55-60. doi: 10.1159/000489173. Epub 2018 Jun 28 [PubMed PMID: 30733948]
Munie ST, Nalamati SPM. Epidemiology and Pathophysiology of Diverticular Disease. Clinics in colon and rectal surgery. 2018 Jul:31(4):209-213. doi: 10.1055/s-0037-1607464. Epub 2018 Jun 22 [PubMed PMID: 29942208]
Sasaki D, Kido A, Yoshida Y. An endoscopic method to study the relationship between bowel habit and motility of the ascending and sigmoid colon. Gastrointestinal endoscopy. 1986 Jun:32(3):185-9 [PubMed PMID: 3721137]
Strate LL, Liu YL, Syngal S, Aldoori WH, Giovannucci EL. Nut, corn, and popcorn consumption and the incidence of diverticular disease. JAMA. 2008 Aug 27:300(8):907-14. doi: 10.1001/jama.300.8.907. Epub [PubMed PMID: 18728264]
Wijarnpreecha K, Boonpheng B, Thongprayoon C, Jaruvongvanich V, Ungprasert P. Smoking and risk of colonic diverticulosis: A meta-analysis. Journal of postgraduate medicine. 2018 Jan-Mar:64(1):35-39. doi: 10.4103/jpgm.JPGM_319_17. Epub [PubMed PMID: 29067919]
Level 1 (high-level) evidenceGoldstein NS, Ahmad E. Histology of the mucosa in sigmoid colon specimens with diverticular disease: observations for the interpretation of sigmoid colonoscopic biopsy specimens. American journal of clinical pathology. 1997 Apr:107(4):438-44 [PubMed PMID: 9124212]
West AB, Losada M. The pathology of diverticulosis coli. Journal of clinical gastroenterology. 2004 May-Jun:38(5 Suppl 1):S11-6 [PubMed PMID: 15115923]
Simsar M, Yuruk YY, Sahin O, Sahin H. Radiological insights into diverticulitis: Clinical manifestations, complications, and differential diagnosis. World journal of radiology. 2025 Aug 28:17(8):107463. doi: 10.4329/wjr.v17.i8.107463. Epub [PubMed PMID: 40901353]
Rottier SJ, van Dijk ST, Ünlü Ç, van Geloven AAW, Schreurs WH, Boermeester MA. Complicated Disease Course in Initially Computed Tomography-Proven Uncomplicated Acute Diverticulitis. Surgical infections. 2019 Sep:20(6):453-459. doi: 10.1089/sur.2018.289. Epub 2019 Mar 30 [PubMed PMID: 30932745]
Peery AF, Shaukat A, Strate LL. AGA Clinical Practice Update on Medical Management of Colonic Diverticulitis: Expert Review. Gastroenterology. 2021 Feb:160(3):906-911.e1. doi: 10.1053/j.gastro.2020.09.059. Epub 2020 Dec 3 [PubMed PMID: 33279517]
Hall J, Hardiman K, Lee S, Lightner A, Stocchi L, Paquette IM, Steele SR, Feingold DL, Prepared on behalf of the Clinical Practice Guidelines Committee of the American Society of Colon and Rectal Surgeons. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Treatment of Left-Sided Colonic Diverticulitis. Diseases of the colon and rectum. 2020 Jun:63(6):728-747. doi: 10.1097/DCR.0000000000001679. Epub [PubMed PMID: 32384404]
Level 1 (high-level) evidenceFrancis NK, Sylla P, Abou-Khalil M, Arolfo S, Berler D, Curtis NJ, Dolejs SC, Garfinkle R, Gorter-Stam M, Hashimoto DA, Hassinger TE, Molenaar CJL, Pucher PH, Schuermans V, Arezzo A, Agresta F, Antoniou SA, Arulampalam T, Boutros M, Bouvy N, Campbell K, Francone T, Haggerty SP, Hedrick TL, Stefanidis D, Truitt MS, Kelly J, Ket H, Dunkin BJ, Pietrabissa A. EAES and SAGES 2018 consensus conference on acute diverticulitis management: evidence-based recommendations for clinical practice. Surgical endoscopy. 2019 Sep:33(9):2726-2741. doi: 10.1007/s00464-019-06882-z. Epub 2019 Jun 27 [PubMed PMID: 31250244]
Level 3 (low-level) evidenceYoung-Fadok TM. Diverticulitis. The New England journal of medicine. 2018 Oct 25:379(17):1635-1642. doi: 10.1056/NEJMcp1800468. Epub [PubMed PMID: 30354951]
Meyer J, Orci LA, Combescure C, Balaphas A, Morel P, Buchs NC, Ris F. Risk of Colorectal Cancer in Patients With Acute Diverticulitis: A Systematic Review and Meta-analysis of Observational Studies. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2019 Jul:17(8):1448-1456.e17. doi: 10.1016/j.cgh.2018.07.031. Epub 2018 Jul 26 [PubMed PMID: 30056181]
Level 1 (high-level) evidenceFleischl W, Clifford K, Wright D. Prevalence and outcomes of Hartmann's reversal following Hartmann's procedure in a regional center, a retrospective cohort study. Langenbeck's archives of surgery. 2024 Dec 3:409(1):369. doi: 10.1007/s00423-024-03558-8. Epub 2024 Dec 3 [PubMed PMID: 39625525]
Level 2 (mid-level) evidenceFleming FJ, Gillen P. Reversal of Hartmann's procedure following acute diverticulitis: is timing everything? International journal of colorectal disease. 2009 Oct:24(10):1219-25. doi: 10.1007/s00384-009-0747-6. Epub 2009 Jun 5 [PubMed PMID: 19499234]
Lambrichts DPV, Vennix S, Musters GD, Mulder IM, Swank HA, Hoofwijk AGM, Belgers EHJ, Stockmann HBAC, Eijsbouts QAJ, Gerhards MF, van Wagensveld BA, van Geloven AAW, Crolla RMPH, Nienhuijs SW, Govaert MJPM, di Saverio S, D'Hoore AJL, Consten ECJ, van Grevenstein WMU, Pierik REGJM, Kruyt PM, van der Hoeven JAB, Steup WH, Catena F, Konsten JLM, Vermeulen J, van Dieren S, Bemelman WA, Lange JF, LADIES trial collaborators. Hartmann's procedure versus sigmoidectomy with primary anastomosis for perforated diverticulitis with purulent or faecal peritonitis (LADIES): a multicentre, parallel-group, randomised, open-label, superiority trial. The lancet. Gastroenterology & hepatology. 2019 Aug:4(8):599-610. doi: 10.1016/S2468-1253(19)30174-8. Epub 2019 Jun 6 [PubMed PMID: 31178342]
Level 1 (high-level) evidenceHalim H, Askari A, Nunn R, Hollingshead J. Primary resection anastomosis versus Hartmann's procedure in Hinchey III and IV diverticulitis. World journal of emergency surgery : WJES. 2019:14():32. doi: 10.1186/s13017-019-0251-4. Epub 2019 Jul 11 [PubMed PMID: 31338117]
Edomskis PP, Hoek VT, Stark PW, Lambrichts DPV, Draaisma WA, Consten ECJ, Bemelman WA, Lange JF, LADIES trial collaborators. Hartmann's procedure versus sigmoidectomy with primary anastomosis for perforated diverticulitis with purulent or fecal peritonitis: Three-year follow-up of a randomised controlled trial. International journal of surgery (London, England). 2022 Feb:98():106221. doi: 10.1016/j.ijsu.2021.106221. Epub 2022 Jan 10 [PubMed PMID: 35026462]
Level 1 (high-level) evidenceLembcke B. Diagnosis, Differential Diagnoses, and Classification of Diverticular Disease. Viszeralmedizin. 2015 Apr:31(2):95-102. doi: 10.1159/000380833. Epub 2015 Apr 29 [PubMed PMID: 26989378]
Unlü C, de Korte N, Daniels L, Consten EC, Cuesta MA, Gerhards MF, van Geloven AA, van der Zaag ES, van der Hoeven JA, Klicks R, Cense HA, Roumen RM, Eijsbouts QA, Lange JF, Fockens P, de Borgie CA, Bemelman WA, Reitsma JB, Stockmann HB, Vrouenraets BC, Boermeester MA, Dutch Diverticular Disease 3D Collaborative Study Group. A multicenter randomized clinical trial investigating the cost-effectiveness of treatment strategies with or without antibiotics for uncomplicated acute diverticulitis (DIABOLO trial). BMC surgery. 2010 Jul 20:10():23. doi: 10.1186/1471-2482-10-23. Epub 2010 Jul 20 [PubMed PMID: 20646266]
Level 1 (high-level) evidenceMora-López L, Ruiz-Edo N, Estrada-Ferrer O, Piñana-Campón ML, Labró-Ciurans M, Escuder-Perez J, Sales-Mallafré R, Rebasa-Cladera P, Navarro-Soto S, Serra-Aracil X, DINAMO-study Group. Efficacy and Safety of Nonantibiotic Outpatient Treatment in Mild Acute Diverticulitis (DINAMO-study): A Multicentre, Randomised, Open-label, Noninferiority Trial. Annals of surgery. 2021 Nov 1:274(5):e435-e442. doi: 10.1097/SLA.0000000000005031. Epub [PubMed PMID: 34183510]
Level 1 (high-level) evidenceBridoux V, Regimbeau JM, Ouaissi M, Mathonnet M, Mauvais F, Houivet E, Schwarz L, Mege D, Sielezneff I, Sabbagh C, Tuech JJ. Hartmann's Procedure or Primary Anastomosis for Generalized Peritonitis due to Perforated Diverticulitis: A Prospective Multicenter Randomized Trial (DIVERTI). Journal of the American College of Surgeons. 2017 Dec:225(6):798-805. doi: 10.1016/j.jamcollsurg.2017.09.004. Epub 2017 Sep 22 [PubMed PMID: 28943323]
Level 1 (high-level) evidenceLoire M, Bridoux V, Mege D, Mathonnet M, Mauvais F, Massonnaud C, Regimbeau JM, Tuech JJ. Long-term outcomes of Hartmann's procedure versus primary anastomosis for generalized peritonitis due to perforated diverticulitis: follow-up of a prospective multicenter randomized trial (DIVERTI). International journal of colorectal disease. 2021 Oct:36(10):2159-2164. doi: 10.1007/s00384-021-03962-2. Epub 2021 Jun 4 [PubMed PMID: 34086087]
Level 1 (high-level) evidenceBrandl A, Kratzer T, Kafka-Ritsch R, Braunwarth E, Denecke C, Weiss S, Atanasov G, Sucher R, Biebl M, Aigner F, Pratschke J, Öllinger R. Diverticulitis in immunosuppressed patients: A fatal outcome requiring a new approach? Canadian journal of surgery. Journal canadien de chirurgie. 2016 Aug:59(4):254-61. doi: 10.1503/cjs.012915. Epub [PubMed PMID: 27240131]
Tartaglia D, Cremonini C, Annunziata E, Catena F, Sartelli M, Kirkpatrick AW, Musetti S, Strambi S, Chiarugi M, Coccolini F, WIRES-T for Acute Diverticulitis Study Group. Acute diverticulitis in immunocompromised patients: evidence from an international multicenter observational registry (Web-based International Register of Emergency Surgery and Trauma, Wires-T). Techniques in coloproctology. 2023 Sep:27(9):747-757. doi: 10.1007/s10151-023-02758-6. Epub 2023 Feb 7 [PubMed PMID: 36749438]
Ryou S, Nam K, Kim J. Duodenal Diverticulitis Accompanied by Portal Vein Thrombosis Treated with Endoscopic Therapy. The Korean journal of gastroenterology = Taehan Sohwagi Hakhoe chi. 2021 Aug 25:78(2):129-133. doi: 10.4166/kjg.2021.054. Epub [PubMed PMID: 34446635]
Waack A, Ranabothu A, Persaud A, Ranabothu M, Vattipally V. Inferior mesenteric vein thrombophlebitis secondary to acute diverticulitis. Radiology case reports. 2023 May:18(5):1882-1885. doi: 10.1016/j.radcr.2023.02.014. Epub 2023 Mar 9 [PubMed PMID: 36936803]
Level 3 (low-level) evidence