Introduction
Three trematodes belonging to the family Opithorchiidae cause human infections that primarily target the liver and biliary tract. They are Clonorchis sinensis, Opisthorchis viverrine, and Opisthorchis felineus. The 3 liver flukes differ slightly in size, ultrastructure, and epidemiology. They have similar complex life cycles, modes of transmission, and clinical implications. Thus, common features of infection caused by these parasites will be the focus of this activity, and where applicable, important differences will be discussed.
The World Health Organization (WHO) classifies these parasites as significant neglected tropical diseases, and an estimated 27 million people are infected.[WHO. Ending the Neglect to Attain the Sustainable Development Goals: A Road Map for Neglected Tropical Diseases 2021–2030][1] In endemic regions, approximately 700 million people are at risk of acquiring infection.[2][3] The infection tends to be chronic; in endemic regions, liver fluke infection is a major cause of gallstones, cholecystitis, cirrhosis, cholangiocarcinoma, and liver cancer.[4][5]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The 3 species of adult flukes share a similar life cycle and differ slightly in size and in the arrangement of their testes and vitelline glands (see Image. Clonorchis Life Cycle). Infected mammalian hosts, notably humans, cats, dogs, and pigs, excrete parasite eggs in their stool. The eggs containing miracida contaminate freshwater bodies, where snails (the first intermediate host) ingest them. The miracidia undergo asexual proliferation and develop into cercariae that leave the snail host. The cercariae attach to freshwater fish (the second intermediate host) where they develop into infective metacercariae within fish skin and muscle tissue.
When mammalian hosts (the final host) ingest undercooked fish, the metacercariae enter the bile ducts, where they develop into adult flukes. Over the course of approximately 4 weeks, the adult flukes lay several thousand eggs per day. The eggs are passed into the intestine and excreted in stool, thereby completing the parasite's life cycle. The adult flukes can survive for many years within the bile ducts.
Epidemiology
Approximately 27 million people are infected with a liver fluke. Endemic regions include East and South Asia, parts of Russia, and Ukraine. Liver flukes were prevalent in Japan until modern agricultural and hygiene methods were adopted.[6][7] Immigrants and travelers from endemic areas represent at-risk populations in nonendemic countries.[8]
China has the highest number of people infected by C sinensis.[3] In a recent study by Qian et al, the presence of C sinensis eggs was identified in approximately 20% of stool samples from 500 schoolchildren aged 10 to 17 years in the hyperendemic Hunan province of southeastern China.[9] A study of the economic burden of clonorchiasis in Guangdong province, China, estimated a cost of more than $200 million.[10] Infection is also endemic in South Korea, Vietnam, and parts of eastern Russia. O viverrini is endemic in Laos, Cambodia, Myanmar, and Thailand. Furthermore, O felineus is endemic in parts of Russia, Ukraine, Kazakhstan, and Belarus. Cases of O felineus infection have also been traced to lakes in central Italy.[11]
Pathophysiology
The pathophysiology of infection has not been fully elucidated. Excretory-secretory products (ESPs) released by the parasite cause inflammation, leading to periductal fibroplasia and liver fibrosis.[12] Animal models and cell culture systems identify upregulation of cancer-associated genes, downregulation of tumor suppressor genes, and increased oxidative stress.[13][14] The presence of worms in the bile ducts causes them to dilate. Increased intraductal pressure contributes to inflammation and can damage surrounding liver tissue.[5]
Histopathology
Histopathologic sections of infected liver tissues demonstrate the presence of flukes within the duct lumen. Duct epithelial cells adjacent to the flukes become hyperplastic. Adenomatous hyperplasia and metaplasia can be seen on histologic examination.[5] Characteristic histopathologic findings include epithelial hyperplasia, periductal fibrosis, and bile duct dilatation (see Image. Histopathology of Clonorchis Sinensis).
History and Physical
Clinical consequences of infection correlate with both the intensity and duration of parasitic burden. Worm burden can be estimated by quantifying eggs in feces, which become detectable in stool after 3 to 4 weeks (see Image. Photomicrograph of Clonorchiasis).[15] Higher egg counts correspond with greater symptom severity.[16][17] Early manifestations develop 10 to 30 days after ingestion of infected fish and persist for 2 to 4 weeks.
Many patients remain asymptomatic during the early phase or in cases of low-intensity infection.[5] When present, early symptoms are typically nonspecific and include nausea, fatigue, and vague abdominal pain. Patients with a heavy parasitic burden may develop features consistent with acute cholangitis, including jaundice, right upper quadrant pain, nausea, vomiting, anorexia, malaise, and fever.[8] Chronic or recurrent infection can lead to cholecystitis, cholangitis, and steatosis, and increase the risk of pancreatitis and liver abscess formation.[18] Liver flukes are classified as carcinogens, with cholangiocarcinoma representing a major complication.[19][5]
In Thailand, approximately 20,000 deaths per year are attributed to opisthorchis-associated cholangiocarcinoma.[2] Children with a high parasitic load are at risk for developmental delays related to ongoing diarrhea, malnutrition, and anemia.[8]
Evaluation
Infection from liver flukes should be considered in the differential diagnosis in patients who consume raw fish and who complain of nausea, fatigue, anorexia, and abdominal pain. Liver fluke infection should also be considered as a likely cause of jaundice, cholecystitis, cholangitis, liver abscess, and cholangiocarcinoma in patients from endemic regions.
Identification of the characteristic operculated eggs in stool samples confirms the diagnosis. Stool analysis does not require elaborate laboratory equipment, but this study is labor-intensive and requires experienced microscopists. Eggs can also be detected in bile and in gallstones.[1] Concentration techniques, eg, the Kato-Katz and formalin-ether methods, increase stool test sensitivity and are particularly useful in low-intensity infections. Notably, the eggs of Clonorchis and Opisthorchis are very similar in appearance.[10][20]
Serodiagnostic tests, such as enzyme-linked immunosorbent assay (ELISA), are commonly used. Specific antigens used in ELISA include crude extracellular polymeric substance extracts, though these assays may cross-react with infections caused by other trematodes.[21] Rapid immunochromatographic tests provide a relatively simple diagnostic platform. The serodiagnostic tests are being used clinically and in epidemiologic surveys. ELISA is also being used to detect antigens in urine samples.[1]
Several nucleic acid amplification tests are currently in use.[1] Newer diagnostic tools include loop-mediated isothermal amplification (LAMP), which targets C sinensis DNA and is well-suited for point-of-care diagnosis.[22][20] Despite these technical achievements over the past few years, the underdiagnosis of liver flukes remains a major issue due to a lack of diagnostic tools and training in endemic areas.[8]
Imaging modalities, eg, ultrasound, cholangiography, computed tomography (CT), and magnetic resonance imaging (MRI), are useful for determining the infection's location, progression, and extent. On ultrasound, diffuse dilatation of intrahepatic bile ducts is commonly seen in infected patients. The finding is nonspecific for diagnostic purposes and is significantly operator-dependent.[23][24] Choi et al reported that enhanced periductal echogenicity and floating echogenic foci in the gallbladder are useful for diagnosing clonorchiasis.[25] CT imaging can help delineate the diagnosis, as it shows a regular caliber of the unaffected larger bile ducts (extrahepatic ducts) compared with the more frequently affected intrahepatic bile ducts.[18] MR cholangiographic imaging is also helpful in the diagnosis.
Treatment / Management
Praziquantel is the drug of choice for the treatment of clonorchiasis and opisthorchiasis. The WHO recommends 25 mg/kg orally 3 times daily for 2 to 3 days, or 40 mg/kg as a single dose, resulting in cure rates above 90%.[26][27] Regional policies might vary, including higher dosing with less frequent administration, eg, 75 mg/kg of praziquantel twice daily within 48 hours.[26] In cases of heavy parasitic infections or persistent egg presence in feces after treatment, retreatment is necessary.[26] Associated adverse effects of praziquantel include abdominal discomfort, vomiting, and dizziness.[28] An alternative regimen includes albendazole (10 mg/kg) for 5 to 7 days.[29][8] Adverse effects of albendazole include headache and dizziness. Patients’ family members and close contacts should also be tested for infection. Tribendimidine, a relatively new drug with promising cure rates and a favorable adverse effect profile, has been approved for treatment in China.[30][26] (B2)
Mass antiparasitic drug administration of humans and animal reservoirs is being performed in efforts to reduce the rate of infection within communities living in highly endemic regions.[31] Unfortunately, in hyperendemic regions, reinfection rates are high due to traditional cultural practices involving the consumption of raw fish. In Thailand, public health screening for cholangiocarcinoma is being performed.[32] Public health efforts are also being directed at community education, treatment of animal reservoirs, and waste management of feces.(B2)
Differential Diagnosis
The differential diagnosis includes acute hepatitis, cholecystitis, choledocholithiasis, cholangiocarcinoma, primary sclerosing cholangitis, primary biliary cholangitis, and parasitic infections such as schistosomiasis, fascioliasis, and ascariasis.[21]
Prognosis
An initial prognosis can be based on the number of eggs found in feces, as higher egg counts indicate greater disease intensity.[15][16][17] Initial infections are often left untreated, as most patients remain asymptomatic or present with nonspecific symptoms. The reversibility of pathological changes induced by liver flukes largely depends on the timing of treatment initiation; when praziquantel treatment is delayed, the recovery period for bile duct pathology may be up to 12 weeks, and may be even longer or irreversible if the infection is severe or prolonged.[33] Chronic complications like cholecystitis, cholangitis, or liver abscesses usually respond to symptomatic treatment. Cholangiocarcinoma is associated with high mortality.[34][5]
Complications
The liver flukes reside within the biliary tree and cause obstruction, inflammation, and fibrosis, which may lead to cholangiocarcinoma.[35] Long-standing infection also increases the risk of bile duct strictures and, together with the mechanical obstruction caused by the parasite, can result in recurrent pyogenic cholangitis, pancreatitis, and liver abscesses.[18] Children are at risk for potential developmental delays related to ongoing diarrhea, malnutrition, and anemia.[8]
Deterrence and Patient Education
Patient Education
Infections with liver flukes, specifically clonorchiasis and opisthorchiasis, are primarily acquired through the consumption of raw or undercooked freshwater fish. Patients should be advised to avoid these practices and to ensure that fish is thoroughly cooked or properly frozen before consumption. Culturally sensitive education is essential in regions where raw fish consumption is traditional. Improving sanitation is equally important, as proper disposal of human waste and access to clean water reduce contamination of freshwater sources. Patients should seek medical evaluation if they develop symptoms such as abdominal pain, jaundice, or fatigue after potential exposure.
Deterrence
Key deterrents include reducing the consumption of raw freshwater fish, improving sanitation to prevent fecal contamination of water sources, and strengthening diagnostic capacity. Enhancing clinicians' awareness of and access to appropriate diagnostic tools supports early detection and treatment of clonorchiasis and opisthorchiasis, helping to reduce transmission and complications.
Enhancing Healthcare Team Outcomes
Infection with hepatobiliary trematodes, including Clonorchis sinensis, Opisthorchis viverrini, and Opisthorchis felineus, remains a major cause of chronic biliary disease in endemic regions. Transmission occurs through ingestion of undercooked freshwater fish containing metacercariae, which mature in the bile ducts and induce chronic inflammation, periductal fibrosis, and ductal dilation. Excretory-secretory products contribute to oxidative stress and oncogenic changes, increasing the risk of cholangiocarcinoma. Clinical presentation ranges from asymptomatic infection to nonspecific symptoms such as nausea and abdominal pain, with severe cases progressing to cholangitis, cholecystitis, pancreatitis, or liver abscess. Diagnosis relies on stool microscopy, supported by serologic, molecular, and imaging modalities. Praziquantel remains first-line therapy, with retreatment required in persistent infection, and prevention focused on dietary modification and public health interventions.
Interprofessional collaboration strengthens early recognition, accurate diagnosis, and effective management. Primary care clinicians and infectious disease specialists identify at-risk patients and coordinate evaluation, while microbiologists and microscopists ensure diagnostic accuracy. Radiologists and gastroenterologists contribute to disease localization and therapeutic interventions, and surgeons manage complications requiring operative care. Pharmacists guide safe antiparasitic use, and nurses support patient education, adherence, and monitoring. Coordinated communication, shared decision-making, and timely referral improve outcomes, reduce complications, and support preventive strategies, including community education and mass treatment programs.
Media
(Click Image to Enlarge)
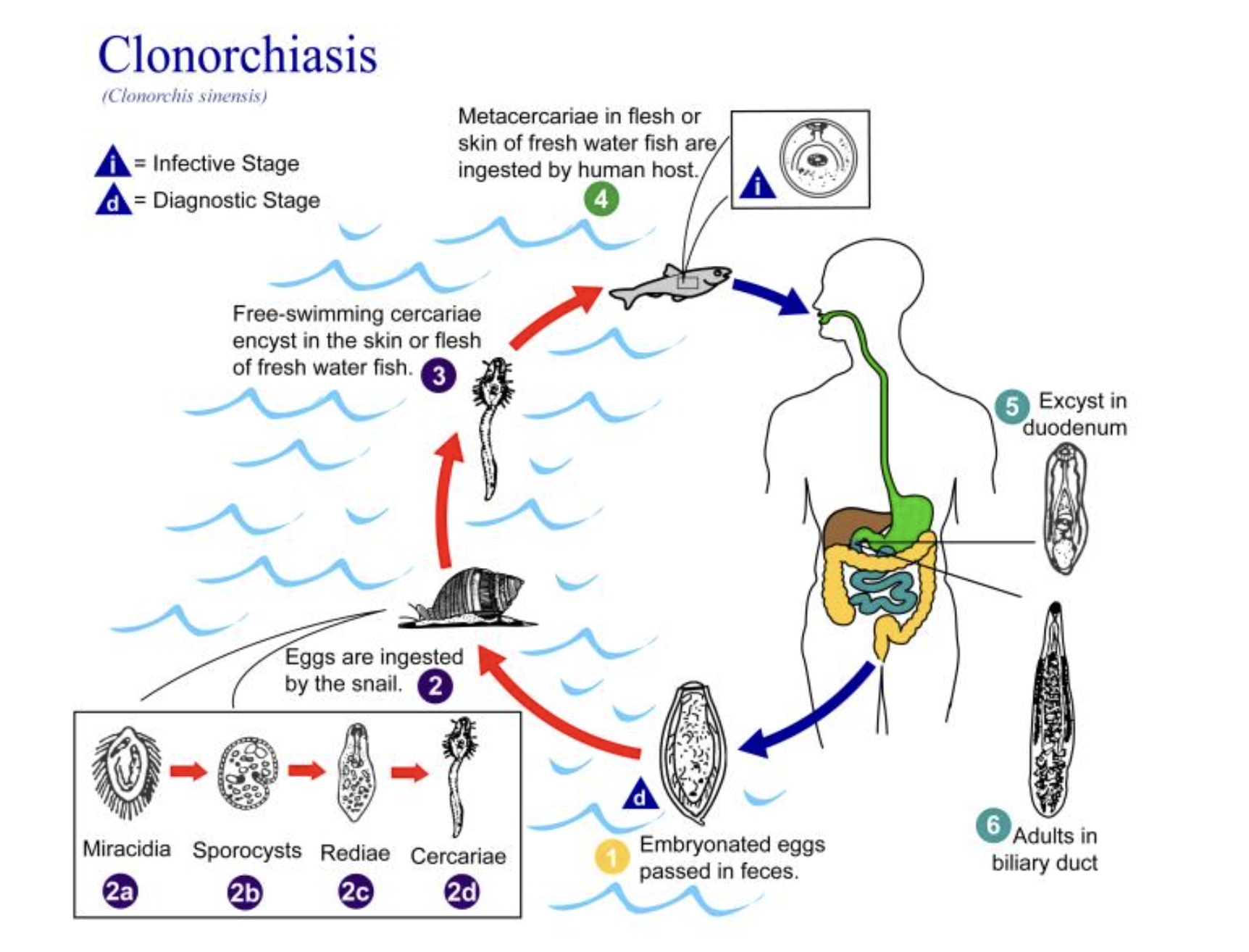
Clonorchis Life Cycle. The 3 species of adult flukes share a similar life cycle and differ slightly in size and in the arrangement of their testes and vitelline glands.
Alexander J da Silva, PhD; Melanie Moser, Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)
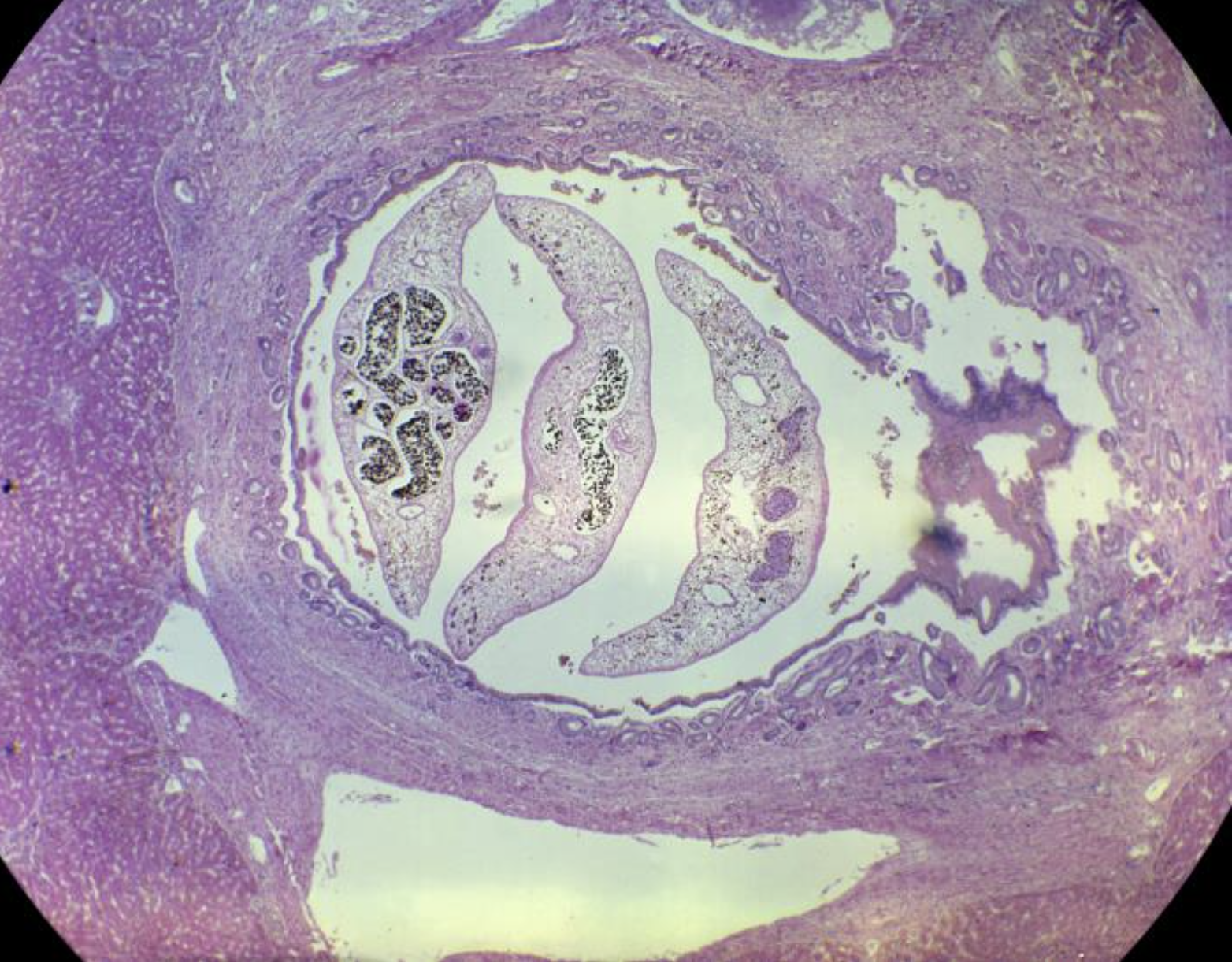
Histopathology of Clonorchis Sinensis. This photomicrograph of a human liver tissue specimen shows multiple adult Chinese liver flukes, Clonorchis sinensis, in a case of clonorchiasis. Characteristic histopathologic findings include epithelial hyperplasia, periductal fibrosis, and bile duct dilatation.
Martin D Hicklin, MD, MPH, Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)
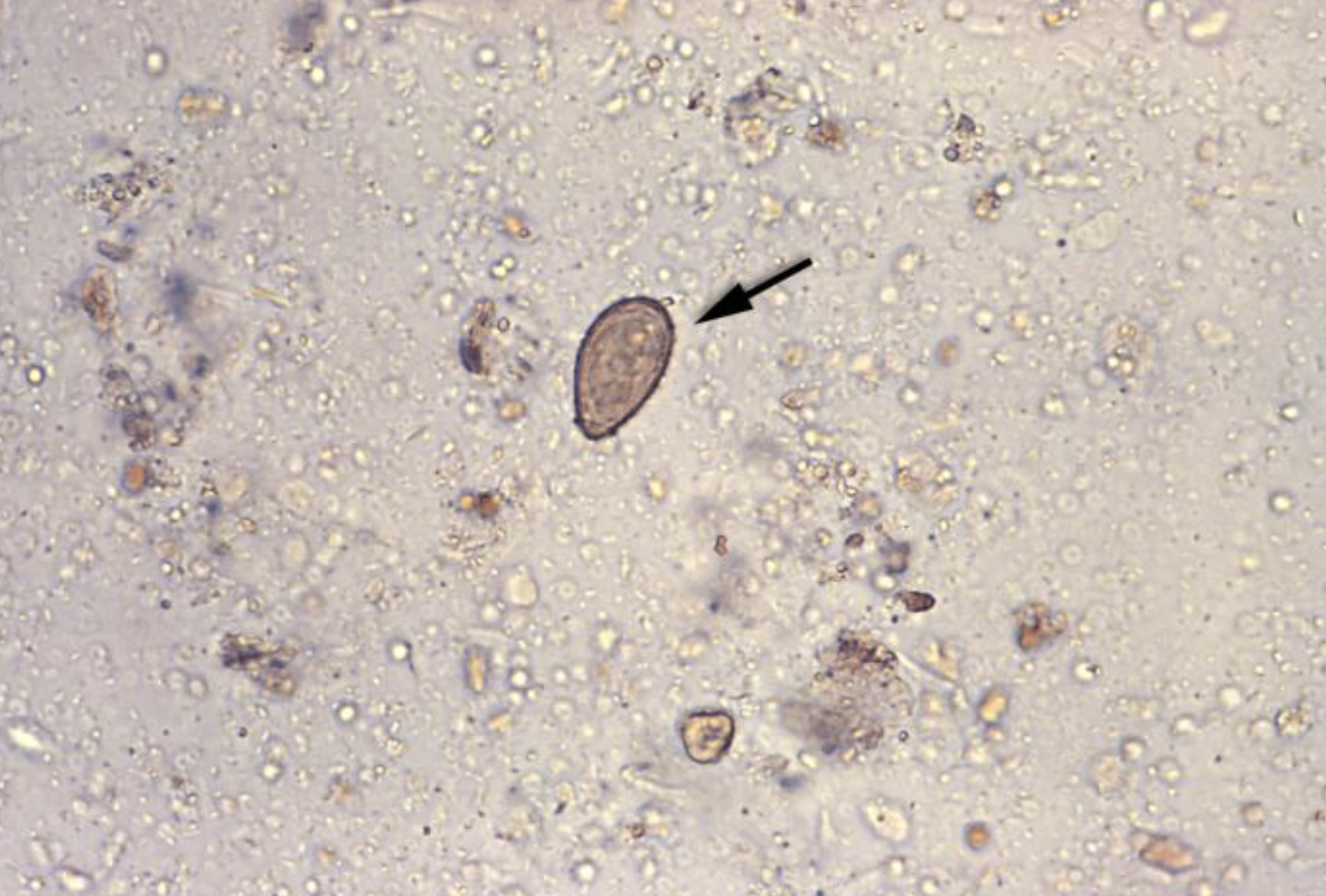
Photomicrograph of Clonorchiasis. Under a magnification of 400×, this photomicrograph revealed the presence of an ovum of the Oriental, or Chinese liver fluke, Clonorchis sinensis in a stool specimen. After ingestion, the metacercariae encyst in the duodenum and ascend the biliary tract through the ampulla of Vater. Maturation takes approximately 1-month. The adult flukes, which measure 10-25 mm X 3-5 mm, reside in small and medium-sized biliary ducts.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
References
Qian M-B, Keiser J, Utzinger J, Zhou X-N. Clonorchiasis and opisthorchiasis: epidemiology, transmission, clinical features, morbidity, diagnosis, treatment, and control. Clinical microbiology reviews. 2024 Mar 14:37(1):e0000923. doi: 10.1128/cmr.00009-23. Epub 2024 Jan 3 [PubMed PMID: 38169283]
Level 2 (mid-level) evidenceSaijuntha W, Sithithaworn P, Kiatsopit N, Andrews RH, Petney TN. Liver Flukes: Clonorchis and Opisthorchis. Advances in experimental medicine and biology. 2019:1154():139-180. doi: 10.1007/978-3-030-18616-6_6. Epub [PubMed PMID: 31297762]
Level 3 (low-level) evidenceKeiser J, Utzinger J. Emerging foodborne trematodiasis. Emerging infectious diseases. 2005 Oct:11(10):1507-14 [PubMed PMID: 16318688]
Huang YL, Zhang KY, Sun YL, Qian MB, Wang Z. The risk of hepatobiliary complications in Clonorchis and Opisthorchis infection: A systematic review and meta-analysis. Acta tropica. 2024 Dec:260():107457. doi: 10.1016/j.actatropica.2024.107457. Epub 2024 Nov 7 [PubMed PMID: 39521195]
Level 1 (high-level) evidenceKim EM, Hong ST. Clonorchis sinensis and Cholangiocarcinoma. Journal of Korean medical science. 2025 Apr 28:40(16):e145. doi: 10.3346/jkms.2025.40.e145. Epub 2025 Apr 28 [PubMed PMID: 40296827]
Yoshida Y. Clonorchiasis--a historical review of contributions of Japanese parasitologists. Parasitology international. 2012 Mar:61(1):5-9. doi: 10.1016/j.parint.2011.06.003. Epub 2011 Jul 3 [PubMed PMID: 21749930]
Level 3 (low-level) evidence. Control of foodborne trematode infections. Report of a WHO Study Group. World Health Organization technical report series. 1995:849():1-157 [PubMed PMID: 7740791]
Level 3 (low-level) evidenceQian MB, Utzinger J, Keiser J, Zhou XN. Clonorchiasis. Lancet (London, England). 2016 Feb 20:387(10020):800-10. doi: 10.1016/S0140-6736(15)60313-0. Epub 2015 Aug 21 [PubMed PMID: 26299184]
Level 2 (mid-level) evidenceQian MB, Zhuang SF, Zhu SQ, Deng XM, Li ZX, Zhou XN. Epidemiology and determinants of clonorchiasis in school children in southeastern China. Acta tropica. 2021 Apr:216():105752. doi: 10.1016/j.actatropica.2020.105752. Epub 2020 Nov 12 [PubMed PMID: 33188749]
Level 2 (mid-level) evidenceTang ZL, Huang Y, Yu XB. Current status and perspectives of Clonorchis sinensis and clonorchiasis: epidemiology, pathogenesis, omics, prevention and control. Infectious diseases of poverty. 2016 Jul 6:5(1):71. doi: 10.1186/s40249-016-0166-1. Epub 2016 Jul 6 [PubMed PMID: 27384714]
Level 3 (low-level) evidenceTraverso A, Repetto E, Magnani S, Meloni T, Natrella M, Marchisio P, Giacomazzi C, Bernardi P, Gatti S, Gomez Morales MA, Pozio E. A large outbreak of Opisthorchis felineus in Italy suggests that opisthorchiasis develops as a febrile eosinophilic syndrome with cholestasis rather than a hepatitis-like syndrome. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology. 2012 Jun:31(6):1089-93. doi: 10.1007/s10096-011-1411-y. Epub 2011 Sep 22 [PubMed PMID: 21938537]
Zheng M, Hu K, Liu W, Hu X, Hu F, Huang L, Wang P, Hu Y, Huang Y, Li W, Liang C, Yin X, He Q, Yu X. Proteomic analysis of excretory secretory products from Clonorchis sinensis adult worms: molecular characterization and serological reactivity of a excretory-secretory antigen-fructose-1,6-bisphosphatase. Parasitology research. 2011 Sep:109(3):737-44. doi: 10.1007/s00436-011-2316-5. Epub 2011 Mar 22 [PubMed PMID: 21424807]
Level 3 (low-level) evidenceUddin MH, Choi MH, Kim WH, Jang JJ, Hong ST. Involvement of PSMD10, CDK4, and Tumor Suppressors in Development of Intrahepatic Cholangiocarcinoma of Syrian Golden Hamsters Induced by Clonorchis sinensis and N-Nitrosodimethylamine. PLoS neglected tropical diseases. 2015:9(8):e0004008. doi: 10.1371/journal.pntd.0004008. Epub 2015 Aug 27 [PubMed PMID: 26313366]
Bian M, Xu Q, Xu Y, Li S, Wang X, Sheng J, Wu Z, Huang Y, Yu X. Investigation on oxidative stress of nitric oxide synthase interacting protein from Clonorchis sinensis. Parasitology research. 2016 Jan:115(1):77-83. doi: 10.1007/s00436-015-4723-5. Epub 2015 Sep 22 [PubMed PMID: 26391171]
Qian MB, Zhou XN. Clonorchis sinensis. Trends in parasitology. 2021 Nov:37(11):1014-1015. doi: 10.1016/j.pt.2021.05.011. Epub 2021 Jul 3 [PubMed PMID: 34229953]
Level 2 (mid-level) evidenceKim JH, Choi MH, Bae YM, Oh JK, Lim MK, Hong ST. Correlation between discharged worms and fecal egg counts in human clonorchiasis. PLoS neglected tropical diseases. 2011 Oct:5(10):e1339. doi: 10.1371/journal.pntd.0001339. Epub 2011 Oct 4 [PubMed PMID: 21991401]
Level 3 (low-level) evidenceLun ZR, Gasser RB, Lai DH, Li AX, Zhu XQ, Yu XB, Fang YY. Clonorchiasis: a key foodborne zoonosis in China. The Lancet. Infectious diseases. 2005 Jan:5(1):31-41 [PubMed PMID: 15620559]
Level 3 (low-level) evidenceLim JH. Radiologic findings of clonorchiasis. AJR. American journal of roentgenology. 1990 Nov:155(5):1001-8 [PubMed PMID: 2120925]
Papachristou GI, Schoedel KE, Ramanathan R, Rabinovitz M. Clonorchis sinensis-associated cholangiocarcinoma: a case report and review of the literature. Digestive diseases and sciences. 2005 Nov:50(11):2159-62 [PubMed PMID: 16240232]
Level 3 (low-level) evidenceNa BK, Pak JH, Hong SJ. Clonorchis sinensis and clonorchiasis. Acta tropica. 2020 Mar:203():105309. doi: 10.1016/j.actatropica.2019.105309. Epub 2019 Dec 17 [PubMed PMID: 31862466]
Hong ST, Fang Y. Clonorchis sinensis and clonorchiasis, an update. Parasitology international. 2012 Mar:61(1):17-24. doi: 10.1016/j.parint.2011.06.007. Epub 2011 Jun 30 [PubMed PMID: 21741496]
Level 3 (low-level) evidenceKim EM, Verweij JJ, Jalili A, van Lieshout L, Choi MH, Bae YM, Lim MK, Hong ST. Detection of Clonorchis sinensis in stool samples using real-time PCR. Annals of tropical medicine and parasitology. 2009 Sep:103(6):513-8. doi: 10.1179/136485909X451834. Epub [PubMed PMID: 19695156]
Level 3 (low-level) evidenceHong ST, Yoon K, Lee M, Seo M, Choi MH, Sim JS, Choi BI, Yun CK, Lee SH. Control of clonorchiasis by repeated praziquantel treatment and low diagnostic efficacy of sonography. The Korean journal of parasitology. 1998 Dec:36(4):249-54 [PubMed PMID: 9868890]
Level 3 (low-level) evidenceChoi D, Hong ST. Imaging diagnosis of clonorchiasis. The Korean journal of parasitology. 2007 Jun:45(2):77-85 [PubMed PMID: 17570969]
Choi D, Hong ST, Lim JH, Cho SY, Rim HJ, Ji Z, Yuan R, Wang S. Sonographic findings of active Clonorchis sinensis infection. Journal of clinical ultrasound : JCU. 2004 Jan:32(1):17-23 [PubMed PMID: 14705173]
Level 3 (low-level) evidenceXu LL, Jiang B, Duan JH, Zhuang SF, Liu YC, Zhu SQ, Zhang LP, Zhang HB, Xiao SH, Zhou XN. Efficacy and safety of praziquantel, tribendimidine and mebendazole in patients with co-infection of Clonorchis sinensis and other helminths. PLoS neglected tropical diseases. 2014 Aug:8(8):e3046. doi: 10.1371/journal.pntd.0003046. Epub 2014 Aug 14 [PubMed PMID: 25122121]
Level 3 (low-level) evidenceKeiser J, Utzinger J. The drugs we have and the drugs we need against major helminth infections. Advances in parasitology. 2010:73():197-230. doi: 10.1016/S0065-308X(10)73008-6. Epub [PubMed PMID: 20627144]
Level 3 (low-level) evidenceLee SH. Large scale treatment of Clonorchis sinensis infections with praziquantel under field conditions. Arzneimittel-Forschung. 1984:34(9B):1227-30 [PubMed PMID: 6542401]
Liu YH, Wang XG, Gao P, Qian MX. Experimental and clinical trial of albendazole in the treatment of Clonorchiasis sinensis. Chinese medical journal. 1991 Jan:104(1):27-31 [PubMed PMID: 1879192]
Level 3 (low-level) evidenceQian MB, Yap P, Yang YC, Liang H, Jiang ZH, Li W, Tan YG, Zhou H, Utzinger J, Zhou XN, Keiser J. Efficacy and safety of tribendimidine against Clonorchis sinensis. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2013 Apr:56(7):e76-82. doi: 10.1093/cid/cis1011. Epub 2012 Dec 7 [PubMed PMID: 23223597]
Level 3 (low-level) evidenceQian MB, Zhou CH, Zhu HH, Chen YD, Zhou XN. Cost yield of different treatment strategies against Clonorchis sinensis infection. Infectious diseases of poverty. 2021 Dec 22:10(1):136. doi: 10.1186/s40249-021-00917-1. Epub 2021 Dec 22 [PubMed PMID: 34933693]
Level 2 (mid-level) evidenceKhuntikeo N, Loilome W, Thinkhamrop B, Chamadol N, Yongvanit P. A Comprehensive Public Health Conceptual Framework and Strategy to Effectively Combat Cholangiocarcinoma in Thailand. PLoS neglected tropical diseases. 2016 Jan:10(1):e0004293. doi: 10.1371/journal.pntd.0004293. Epub 2016 Jan 21 [PubMed PMID: 26797527]
Lee SH, Hong ST, Kim CS, Sohn WM, Chai JY, Lee YS. Histopathological changes of the liver after praziquantel treatment in Clonorchis sinensis infected rabbits. Kisaengch'unghak chapchi. The Korean journal of parasitology. 1987 Dec:25(2):110-122 [PubMed PMID: 12886061]
Zhang GW, Lin JH, Qian JP, Zhou J. Identification of risk and prognostic factors for patients with clonorchiasis-associated intrahepatic cholangiocarcinoma. Annals of surgical oncology. 2014 Oct:21(11):3628-37. doi: 10.1245/s10434-014-3710-x. Epub 2014 Apr 30 [PubMed PMID: 24781504]
Level 3 (low-level) evidenceQian MB, Chen YD, Liang S, Yang GJ, Zhou XN. The global epidemiology of clonorchiasis and its relation with cholangiocarcinoma. Infectious diseases of poverty. 2012 Oct 25:1(1):4. doi: 10.1186/2049-9957-1-4. Epub 2012 Oct 25 [PubMed PMID: 23849183]
Level 2 (mid-level) evidence