Introduction
Chlamydia is a sexually transmitted infectious disease caused by the bacterium Chlamydia trachomatis. In the United States, chlamydia is the most commonly reported bacterial infection.[1] Globally, Chlamydia trachomatis is the most common sexually transmitted infection (STI), and reported rates of infection have been climbing in the last few decades.[2] C trachomatis causes the ocular infection trachoma, which is the leading infectious cause of blindness worldwide.[3]
In females, the cervix is the most commonly infected anatomic site. This can manifest as cervicitis, urethritis, pelvic inflammatory disease, perihepatitis, or proctitis. Chlamydial infections in women, especially if untreated, increase the risk of infertility and ectopic pregnancy, leading to high medical costs.[4] Associated risks of chlamydia infection during pregnancy are also present. Additionally, infants born vaginally to mothers infected with genital Chlamydia trachomatis may develop conjunctivitis or pneumonia.
In men, infection with Chlamydia trachomatis can lead to urethritis, epididymitis, prostatitis, proctitis, or reactive arthritis. Both men and women infected with C trachomatis may also experience conjunctivitis, pharyngitis, and lymphogranuloma venereum (see Image. Follicular Conjunctivitis). Lymphogranuloma venereum (LGV), caused by distinct serovars of Chlamydia trachomatis, is a less common disease characterized by enlarged lymph nodes or severe proctocolitis.[5]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Chlamydia trachomatis is a gram-negative, anaerobic, intracellular obligate bacterium that replicates within eukaryotic cells.[6] C trachomatis differentiates into 18 serovars (serologically variant strains) based on monoclonal antibody-based typing assays. These serovars correlate with multiple medical conditions as follows:
Epidemiology
Urogenital chlamydia infections are the most commonly reported bacterial infections in the United States and the most common cause of STIs in the world.[1][2] The overall rate of urogenital infection amongst United States women is roughly 2 times that of United States men, with a higher prevalence in people 15 to 24 years of age.[8] Epidemiological evidence strongly links lower socioeconomic status with a higher risk of Chlamydia trachomatis infection.[9] A recent study found higher rates of repeat chlamydia positivity more than 30 days but less than 365 days after a previous positive test among people of Black race, 13 to 19 years of age, and with a history of prior STI.[10]
Pathophysiology
Chlamydia is unique among bacteria, possessing an infectious cycle and 2 developmental forms: the infectious form, known as the elementary body, and the reticulate body. The elementary body is metabolically inactive and is taken up by host cells. Within the host cell, the elementary body will differentiate into the metabolically active reticulate body. The reticulate body will then use host energy sources and amino acids to replicate and form a new elementary body, which can then infect additional cells.[6]
C trachomatis targets the squamocolumnar epithelial cells of the endocervix and upper genital tract in women, and the conjunctiva, urethra, and rectum in both men and women.[11] The bacterium is transmitted through direct contact with infected tissue, including vaginal, anal, or oral sex, and can even be passed from an infected mother to the newborn during childbirth.[11]
Histopathology
Typical intracytoplasmic inclusions and free chlamydiae are identifiable in Giemsa-stained cell scrapings. Stained conjunctival scrapings are positive in 90% of infants with neonatal conjunctivitis and 50% of adults with inclusion conjunctivitis.[12] Cytology techniques can be used to evaluate endocervical scrapings; however, their sensitivity and specificity are low.[13]
History and Physical
C trachomatis can lead to many urogenital infections, including cervicitis, pelvic inflammatory disease, urethritis, epididymitis, prostatitis, and lymphogranuloma venereum.[14] Extragenital infections caused by C trachomatis include conjunctivitis, perihepatitis, pharyngitis, reactive arthritis, and proctitis (see Image. Alpha-1 Antitrypsin Deficiency in Emphysema).
More frequently, patients remain asymptomatic reservoirs of the disease. In the minority of patients who become symptomatic, clinical signs depend on the location of the infection. Below are the common signs and symptoms associated with C trachomatis urogenital infections.
- Cervicitis: Over 80% of women will be asymptomatic or have mild symptoms, eg, vaginal discharge, bleeding, abdominal pain, and dysuria.[15] Only a minority of women have the classic presentation of mucopurulent cervicitis with discharge and easily induced endocervical bleeding. Some women may complain of postcoital bleeding or intermenstrual bleeding.
- Pelvic inflammatory disease (PID): This occurs when C trachomatis ascends to the upper reproductive tract. Most commonly, these patients will have abdominal or pelvic pain with or without signs and symptoms of cervicitis. Other symptoms include nausea, vomiting, fevers, chills, low back pain, pain with intercourse, dysuria, or postcoital bleeding.[16]
- Urethritis: This condition is most commonly seen in men. Subtle clinical differences between gonococcal urethritis and chlamydial urethritis exist, but making a reliable distinction without testing is not possible. Urethritis presents with dysuria and urethral discharge, which is typically white, gray, or sometimes clear, and may only be evident after penile "stripping" or during morning hours. Women with urethritis may complain of frequency or dysuria and may mistake their symptoms for a urinary tract infection. Urinalysis will reveal pyuria, but neither bacterial culture nor Gram stain will reveal organisms.[14]
- Perihepatitis: Also known as Fitz-Hugh-Curtis syndrome, this syndrome occurs when a chlamydia infection leads to inflammation of the liver capsule and the surrounding peritoneal surfaces. This syndrome is most commonly seen in patients who have a pelvic inflammatory disease, and perihepatitis is associated with right upper quadrant or pleuritic pain. Unlike other conditions that may affect the liver or cause right upper quadrant pain, abnormalities in liver enzymes are not typically found.[17]
- Epididymitis: Typically, men will present with unilateral testicular pain and tenderness, possible hydrocele, palpable swelling of the epididymis, and fever.[11]
- Proctitis: Rectal infection with chlamydia can be asymptomatic if caused by genital serovars D through K. However, if LGV serovars L1-L3 are the cause of proctitis, patients may complain of rectal pain, discharge, and bleeding in the setting of receptive anal intercourse. Patients may also present with a fever or malaise. This is seen almost exclusively in males who have sex with males; however, anal intercourse is not uncommon in heterosexual intercourse.[11]
- Prostatitis: Symptoms include dysuria, urinary dysfunction, pelvic pain, and pain with ejaculation.[18] Expressed prostatic secretions may reveal increased leukocyte counts on microscopy.
- Reactive arthritis: Approximately 1% of men with urethritis due to chlamydial infection also develop reactive arthritis, and a third will have the reactive arthritis triad of arthritis, urethritis, and uveitis, formerly known as Reiter syndrome.[19]
- Conjunctivitis: Direct inoculation with genital secretions containing C trachomatis serovars can lead to conjunctival infection. Symptoms typically include nonpurulent conjunctivitis (erythematous injection of the surface epithelium). The conjunctiva may have a cobbled appearance. Conjunctivitis is the most common manifestation of chlamydial infection in newborns.[20]
- Pneumonia: Infants born to mothers who have a cervical infection with C trachomatis may develop pneumonia 5% to 30% of the time.[21] Recognition usually occurs between 4 to 12 weeks of age, though almost all infants have symptoms before 8 weeks. Nasal congestion and cough are common, and some infants may have thick nasal secretions.[22] Infants usually have no fever or only a minimal fever; they may have tachypnea, and they may have a characteristic paroxysmal staccato cough. In preterm infants, apneic spells may be seen. Rales may be heard on auscultation of the lungs, but wheezing is uncommon.
- Pharyngitis: Although C trachomatis is not typically considered a significant cause of pharyngitis, it can be detected in the pharynx via nucleic acid amplification tests.
- Lymphogranuloma venereum: Patients will present with painless genital ulcers. The ulcers typically have a small, stellate appearance. The development of inguinal lymphadenopathy typically follows the appearance of ulcers.
Evaluation
Among C trachomatis infections, trachoma is the only infection which is diagnosed clinically. Other chlamydial infections with specific clinical syndromes require laboratory confirmation. The gold standard for the diagnosis of urogenital chlamydia infections is nucleic acid amplification testing (NAAT). The preferred method for testing is via vaginal swabs for females or the first-catch urine for males. Urine can be used for females, however it may be less sensitive. Testing can also be performed on endocervical or urethral swabs. Swabs should have a wire or plastic shaft; the tip should be dacron or rayon, or a cytobrush. Other materials may inhibit Chlamydia trachomatis. Alternative methods of testing include culture, rapid testing, serology, antigen detection, and genetic probes. If no testing is available, treatment is recommended based on clinical presentation.[14]
When a patient presents with suspected chlamydia infection, a workup for other STDs should be carried out. A complete blood count is essential if PID is suspected. One may consider testing for HIV, gonorrhea, and syphilis. The sexual partner must be tested for chlamydia.[23] A pregnancy test should be performed, as pregnancy is a contraindication to doxycycline therapy.[24]
Additionally, cytology is often used in patients with conjunctivitis and ocular trachoma. Cultures are usually not done for chlamydia as the organism is difficult to grow in the laboratory. However, in patients with anal and rectal involvement, cultures are ideal as other tests are difficult to interpret.
The United States Preventive Services Task Force (USPSTF) recommends regular screening for chlamydia in all sexually active women 24 years or younger and in women 25 years and older who are at increased risk of infection because, if left untreated, the infection is associated with PID, infertility, and chronic pelvic pain.[25] In males, the leucocyte esterase test in urine is diagnostic for gonorrhea or chlamydia in the absence of a urinary tract infection.[23]
Treatment / Management
The goal of treatment is to prevent complications associated with infection (eg, PID, infertility), decrease the risk of transmission, and resolve symptoms. Treatment for uncomplicated urogenital chlamydia infection is with doxycycline or azithromycin.[23] A 2019 Cochrane review found that azithromycin had higher microbiological failure rates than doxycycline, but little to no difference in risk of clinical failure.[26] However, directly observed single-dose azithromycin therapy may be preferred to doxycycline when nonadherence is a substantial concern.[23] Levofloxacin is an alternative option.(A1)
Chlamydial infection and gonococcal infections often coexist. In men, the combined treatment for urogenital gonococcal infection should be based on the detection of the organism by NAAT or Gram stain. In women, the Gram stain is less helpful because of the possibility of colonization by typical Neisseria species within the vaginal flora. Therefore, combined treatment should be dependent on a patient's individual risk and local prevalence rates.[23]
Patients should have partners identified and tested. They should also be counseled on high-risk behaviors, avoid sexual activity for 1 week after initiating therapy, and consider testing for HIV. Doxycycline has also been recommended for postexposure prophylaxis in appropriate populations.[27]
Verification of cure should occur 3 weeks after treatment completion, and retesting should be performed 3 months after treatment.[23] If symptoms persist after treatment, consider secondary bacterium coinfection versus reinfection. Follow-up culture is not recommended for most people, but may be considered in pregnant females.[28](B3)
Differential Diagnosis
Because Chlamydia trachomatis can lead to a broad spectrum of clinical diseases or manifestations, the differential diagnosis of various presenting complaints is also broad. Clinicians should consider other etiologies that may affect each body area or organ system and may manifest similarly, including:
- Dysuria
- Gonorrhea
- Genital herpes
- Urinary tract infection
- Abdominal pain
- Appendicitis
- Cholecystitis
- Constipation
- Pelvic pain
- Endometriosis
- Ovarian cysts
- Adenomyosis
- Vaginal discharge
- Bacterial vaginosis
- Trichomonas vaginalis
- Gonorrhea
- Vaginal candidiasis
- Foreign body
- Mycoplasma genitalium infection
- Ureaplasma infection
- Rectal discharge
- Inflammatory bowel disease
- Gonorrhea
- Conjunctivitis
- Viral infection
- Allergy
- Gonococcal infection
- Postcoital or intermenstrual bleeding
- Cervical cancer
- Cervical or endometrial polyp
- Cervical ectropion
- Leiomyoma
- Pregnancy
- Genital ulceration
- Herpes simplex
- Syphilis
- Chancroid
- Granuloma inguinale
Treatment Planning
The World Health Organization (WHO) recommendations for treatment of C trachomatis infections are the following:
- Uncomplicated genital chlamydia (either of the following):
- Azithromycin 1000 mg orally as a single dose
- Doxycycline 100 mg orally twice a day for 7 days, or one of the following alternatives:
- Tetracycline 500 mg by mouth 4 times a day for 7 days
- Erythromycin 500 mg orally twice daily for 7 days
- Ofloxacin 200 to 400 mg orally twice daily for 7 days [29]
- Anorectal chlamydial infection: The WHO recommends oral doxycycline 100 mg twice daily for 7 days, compared with oral azithromycin 1 g as a single dose.
- Chlamydial infection in pregnancy (one of the following):
- Azithromycin is recommended over erythromycin or amoxicillin
- Azithromycin 1 g orally as a single dose
- Amoxicillin 500 mg orally 3 times daily for 7 days
- Erythromycin 500 mg orally twice daily for 7 days
- Lymphogranuloma venereum:
- In adults and adolescents with lymphogranuloma venereum, the guidelines recommend doxycycline 100 mg orally twice daily for 21 days, compared with azithromycin 1 g orally weekly for 3 weeks.
- Good practice dictates the treatment of LGV, particularly for men who have sex with men and for people with HIV infection.
- When contraindications to doxycycline are present, azithromycin should be the therapeutic choice.
- When other treatment options are unavailable, erythromycin 500 mg orally 4 times a day for 21 days is an alternative.
- Doxycycline should not be used in pregnancy.
- Infant disease (one of the following):
- Oral erythromycin 50 mg/kg by mouth in 4 divided doses for 14 days is the preferred treatment for both conjunctivitis and pneumonia in the neonate. Infants who fail an initial course of erythromycin are recommended to retreat with another 14-day course of erythromycin.
- Azithromycin 20 mg/kg by mouth daily for 3 days is an acceptable alternative.
- Ocular prophylaxis: In addition, the WHO recommends topical ocular prophylaxis for all neonates with one of the following antimicrobials applied to both eyes immediately after birth:
- Tetracycline hydrochloride 1% eye ointment
- Erythromycin 0.5% eye ointment
- Povidone iodine 2.5% solution
- Silver nitrate 1% solution
- Chloramphenicol 1% eye ointment
Toxicity and Adverse Effect Management
In neonates being treated for chlamydial infection, both azithromycin and erythromycin are associated with a risk of infantile hypertrophic pyloric stenosis.[23] This is particularly a concern for infants 2 weeks old or younger. Parents and physicians should carefully monitor infants for signs of intestinal obstruction.
Prognosis
Antibiotic treatment has a 95% effectiveness rate for first-time therapy. The prognosis is excellent when treatment is initiated promptly and the entire course of antibiotics is completed. Although treatment failures with primary therapies are quite rare, reinfection is common and is usually related to the nontreatment of infected sexual partners or acquisition from a new partner. Death is rare but can be caused by progression to salpingitis and tubo-ovarian abscess with rupture and peritonitis. The most significant morbidity occurs with repetitive infection with chlamydiae, which leads to scarring of the fallopian tubes and subsequent sterility.[30]
Complications
PID places women of childbearing age at increased risk for ectopic pregnancy. Inflammation and scarring within the upper genital tract may impair fertility or contribute to chronic pelvic pain. Chlamydial infection during pregnancy also elevates the likelihood of prelabour rupture of membranes (PROM), premature prelabour rupture of membranes (PPROM), and preterm delivery.[31]
Deterrence and Patient Education
Chlamydia trachomatis infection frequently progresses without symptoms, yet undiagnosed or untreated disease can lead to significant reproductive and systemic complications. Routine screening helps detect silent infection and prevent sequelae such as pelvic inflammatory disease, infertility, ectopic pregnancy, and adverse pregnancy outcomes. Annual screening is recommended for all sexually active females younger than 25, with targeted screening for older women at increased risk, men who have sex with men, individuals with HIV, and specific age groups entering correctional facilities. Because C trachomatis is a notifiable infection, timely reporting, partner notification, and appropriate treatment remain essential components of public health management.[25]
Effective care relies on coordinated efforts across the healthcare team. Physicians, general practitioners, advanced practitioners, nurses, and pharmacists must apply strong clinical assessment skills, evidence-based screening strategies, and clear patient education to support early detection and treatment. Interprofessional communication ensures accurate reporting, streamlined partner management, and consistent follow-up. Collaborative workflows strengthen patient-centered care by reducing barriers to screening, supporting adherence to therapy, and improving safety through timely diagnosis and prevention of complications. This shared approach promotes better outcomes, enhances team performance, and reinforces trust and engagement throughout the continuum of care.
Enhancing Healthcare Team Outcomes
Chlamydia trachomatis infection frequently progresses without symptoms, yet undiagnosed or untreated disease can lead to significant reproductive and systemic complications. Routine screening helps detect silent infection and prevent sequelae such as pelvic inflammatory disease, infertility, ectopic pregnancy, and adverse pregnancy outcomes. Annual screening is recommended for all sexually active females younger than 25, with targeted screening for older women at increased risk, men who have sex with men, individuals with HIV, and specific age groups entering correctional facilities. Because C trachomatis is a notifiable infection, timely reporting, partner notification, and appropriate treatment remain essential components of public health management.
Effective care relies on coordinated efforts across the healthcare team. Physicians, general practitioners, advanced practitioners, nurses, and pharmacists must apply strong clinical assessment skills, evidence-based screening strategies, and clear patient education to support early detection and treatment. Interprofessional communication ensures accurate reporting, streamlined partner management, and consistent follow-up. Primary care practitioners should educate patients on the importance of using a condom during sex, practicing safe sex, or abstaining from sexual activity to prevent chlamydia. Pharmacists should verify dosing and agent selection for antimicrobial therapy, check for drug interactions, and report any concerns to the prescriber. This approach results in decreased incidence and improved outcomes. Collaborative workflows strengthen patient-centered care by reducing barriers to screening, supporting adherence to therapy, and improving safety through timely diagnosis and prevention of complications.
Media
(Click Image to Enlarge)
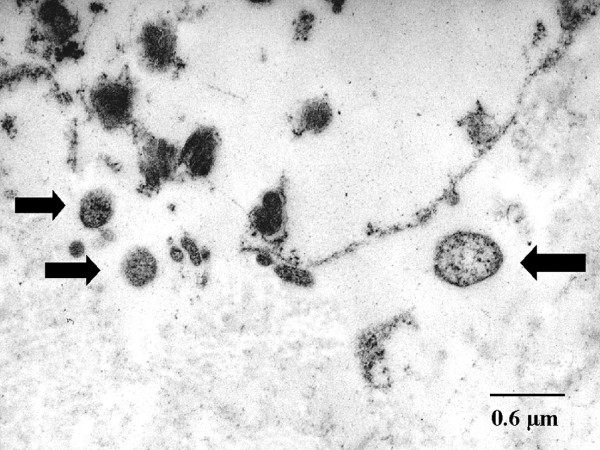
Alpha-1 Antitrypsin Deficiency in Emphysema, Transmission Electron Microscopy. Chlamydial bodies are shown by arrows; also seen is the destruction of the interstitial connective tissue, with the ultrastructure less well preserved after the fixation of formaldehyde.
Theegarten D, Anhenn O, Hotzel H, et al. A comparative ultrastructural and molecular biological study on Chlamydia psittaci infection in alpha-1 antitrypsin deficiency and non-alpha-1 antitrypsin deficiency emphysema versus lung tissue of patients with hamartochondroma. BMC Infect Dis. 2004;4:38. doi: 10.1186/1471-2334-4-38.
(Click Image to Enlarge)
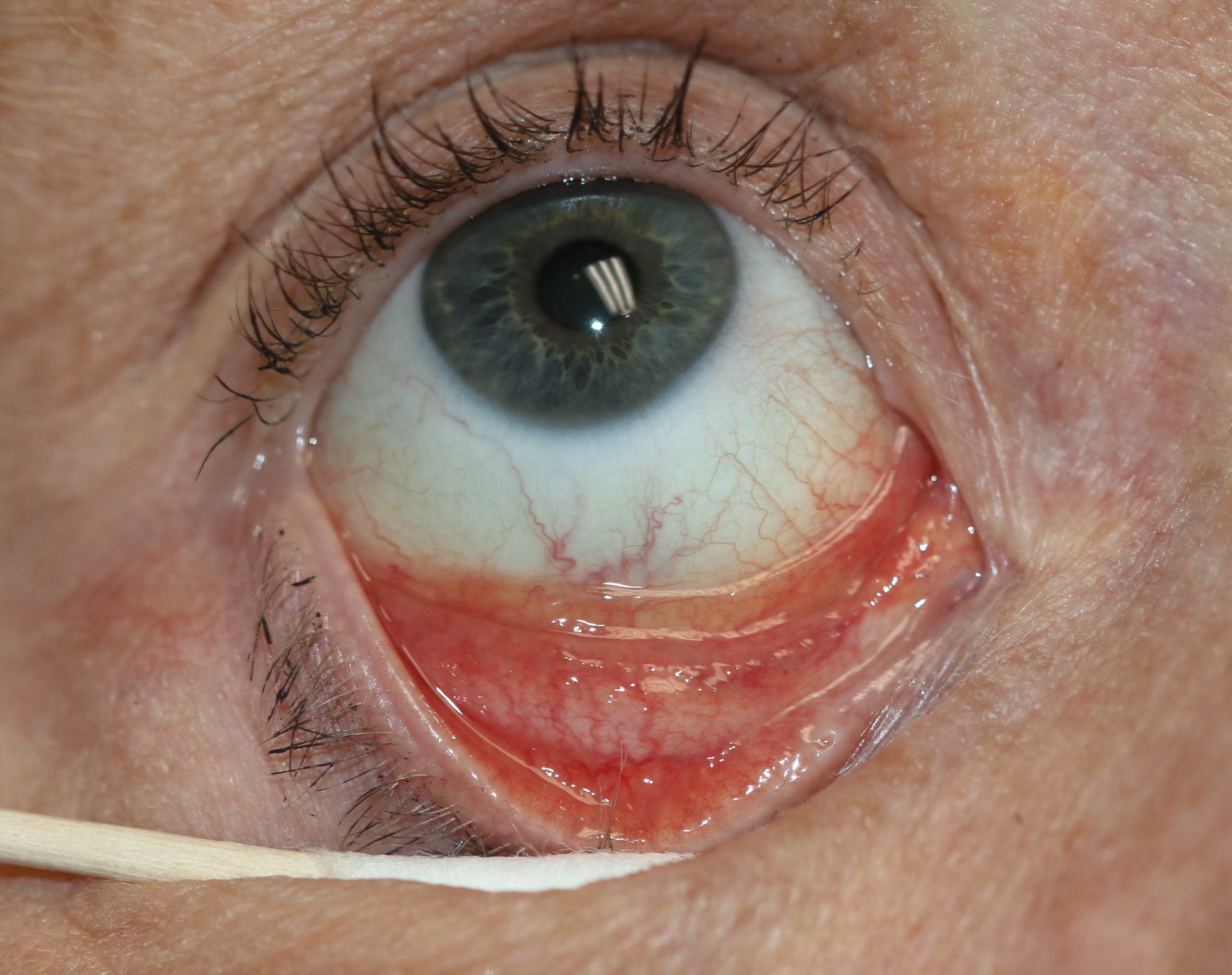
Follicular Conjunctivitis. Inflammation is noted with viral infections like herpes zoster, Epstein-Barr virus infection, infectious mononucleosis, and chlamydial infections, as well as in reaction to topical medications and molluscum contagiosum. Follicular conjunctivitis has been described in patients with COVID-19. The inferior and superior tarsal conjunctiva and the fornices show gray-white elevated swellings about 0.5 to 1 mm in diameter and have a velvety appearance.
Contributed by BCK Patel, MD, FRCS
References
Hao S, Tao G, Pearson WS, Rochlin I, Phillips RL, Rehkopf DH, Kamdar N. Treatment of Chlamydia and Gonorrhea in Primary Care and Its Patient-Level Variation: An American Family Cohort Study. Annals of family medicine. 2025 Mar 24:23(2):136-144. doi: 10.1370/afm.240164. Epub 2025 Mar 24 [PubMed PMID: 40127987]
Zhao P, Liang P, Wang J, Xu W, Huang S, Wang C. Chlamydia cases in women of reproductive age, 2006-2020: an analysis of surveillance data from Southern China. BMC public health. 2025 Jan 15:25(1):158. doi: 10.1186/s12889-025-21318-1. Epub 2025 Jan 15 [PubMed PMID: 39810099]
Level 3 (low-level) evidenceHabtamu E, Harding-Esch EM, Greenland K, Wamyil-Mshelia T, Talero SL, Mishra SK, Lietman TM, Solomon AW, Burton MJ. Trachoma. Lancet (London, England). 2025 May 24:405(10492):1865-1878. doi: 10.1016/S0140-6736(25)00551-3. Epub [PubMed PMID: 40412861]
Owusu-Edusei K Jr, Chesson HW, Gift TL, Tao G, Mahajan R, Ocfemia MC, Kent CK. The estimated direct medical cost of selected sexually transmitted infections in the United States, 2008. Sexually transmitted diseases. 2013 Mar:40(3):197-201. doi: 10.1097/OLQ.0b013e318285c6d2. Epub [PubMed PMID: 23403600]
Mabey D, Peeling RW. Lymphogranuloma venereum. Sexually transmitted infections. 2002 Apr:78(2):90-2 [PubMed PMID: 12081191]
Murray SM, McKay PF. Chlamydia trachomatis: Cell biology, immunology and vaccination. Vaccine. 2021 May 21:39(22):2965-2975. doi: 10.1016/j.vaccine.2021.03.043. Epub 2021 Mar 24 [PubMed PMID: 33771390]
Morré SA, Rozendaal L, van Valkengoed IG, Boeke AJ, van Voorst Vader PC, Schirm J, de Blok S, van Den Hoek JA, van Doornum GJ, Meijer CJ, van Den Brule AJ. Urogenital Chlamydia trachomatis serovars in men and women with a symptomatic or asymptomatic infection: an association with clinical manifestations? Journal of clinical microbiology. 2000 Jun:38(6):2292-6 [PubMed PMID: 10834991]
Torrone E, Papp J, Weinstock H, Centers for Disease Control and Prevention (CDC). Prevalence of Chlamydia trachomatis genital infection among persons aged 14-39 years--United States, 2007-2012. MMWR. Morbidity and mortality weekly report. 2014 Sep 26:63(38):834-8 [PubMed PMID: 25254560]
Crichton J, Hickman M, Campbell R, Batista-Ferrer H, Macleod J. Socioeconomic factors and other sources of variation in the prevalence of genital chlamydia infections: A systematic review and meta-analysis. BMC public health. 2015 Jul 30:15():729. doi: 10.1186/s12889-015-2069-7. Epub 2015 Jul 30 [PubMed PMID: 26224062]
Level 1 (high-level) evidenceCurrenti S, O'Grady T, Bomma S, Gurram N, Miranda W, Hart-Malloy R. Epidemiology of Chlamydia trachomatis and Repeat Positivity Following Detection in New York State. Journal of public health management and practice : JPHMP. 2024 Sep-Oct 01:30(5):E215-E223. doi: 10.1097/PHH.0000000000002022. Epub 2024 Jul 22 [PubMed PMID: 39041774]
O'Connell CM, Ferone ME. Chlamydia trachomatis Genital Infections. Microbial cell (Graz, Austria). 2016 Sep 5:3(9):390-403. doi: 10.15698/mic2016.09.525. Epub 2016 Sep 5 [PubMed PMID: 28357377]
Mordhorst CH, Dawson C. Sequelae of neonatal inclusion conjunctivitis and associated disease in parents. American journal of ophthalmology. 1971 Apr:71(4):861-7 [PubMed PMID: 4928532]
Taylor-Robinson D. Evaluation and comparison of tests to diagnose Chlamydia trachomatis genital infections. Human reproduction (Oxford, England). 1997 Nov:12(11 Suppl):113-20 [PubMed PMID: 9433967]
Hocking JS, Geisler WM, Kong FYS. Update on the Epidemiology, Screening, and Management of Chlamydia trachomatis Infection. Infectious disease clinics of North America. 2023 Jun:37(2):267-288. doi: 10.1016/j.idc.2023.02.007. Epub 2023 Mar 31 [PubMed PMID: 37005162]
Detels R, Green AM, Klausner JD, Katzenstein D, Gaydos C, Handsfield H, Pequegnat W, Mayer K, Hartwell TD, Quinn TC. The incidence and correlates of symptomatic and asymptomatic Chlamydia trachomatis and Neisseria gonorrhoeae infections in selected populations in five countries. Sexually transmitted diseases. 2011 Jun:38(6):503-9 [PubMed PMID: 22256336]
. Pelvic inflammatory disease. American family physician. 2012 Apr 15:85(8):797-8 [PubMed PMID: 22534389]
Ekabe CJ, Kehbila J, Njim T, Kadia BM, Tendonge CN, Monekosso GL. Chlamydia trachomatis-induced Fitz-Hugh-Curtis syndrome: a case report. BMC research notes. 2017 Jan 3:10(1):10. doi: 10.1186/s13104-016-2357-z. Epub 2017 Jan 3 [PubMed PMID: 28057084]
Level 3 (low-level) evidenceRedgrove KA, McLaughlin EA. The Role of the Immune Response in Chlamydia trachomatis Infection of the Male Genital Tract: A Double-Edged Sword. Frontiers in immunology. 2014:5():534. doi: 10.3389/fimmu.2014.00534. Epub 2014 Oct 27 [PubMed PMID: 25386180]
Kobayashi S, Kida I. Reactive arthritis: recent advances and clinical manifestations. Internal medicine (Tokyo, Japan). 2005 May:44(5):408-12 [PubMed PMID: 15942084]
Level 3 (low-level) evidenceBanniettis N, Wisecup K, Boland L, Watanabe I, Hammerschlag MR, Kohlhoff S. Association of Routine Chlamydia trachomatis Screening During Pregnancy and Seroprevalence of Chlamydial Infection in Children, 1991-2015. Journal of the Pediatric Infectious Diseases Society. 2021 Mar 26:10(2):172-174. doi: 10.1093/jpids/piaa002. Epub [PubMed PMID: 31958120]
Schachter J, Grossman M, Sweet RL, Holt J, Jordan C, Bishop E. Prospective study of perinatal transmission of Chlamydia trachomatis. JAMA. 1986 Jun 27:255(24):3374-7 [PubMed PMID: 3712696]
Tipple MA, Beem MO, Saxon EM. Clinical characteristics of the afebrile pneumonia associated with Chlamydia trachomatis infection in infants less than 6 months of age. Pediatrics. 1979 Feb:63(2):192-7 [PubMed PMID: 440806]
Level 3 (low-level) evidenceWorkowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, Reno H, Zenilman JM, Bolan GA. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR. Recommendations and reports : Morbidity and mortality weekly report. Recommendations and reports. 2021 Jul 23:70(4):1-187. doi: 10.15585/mmwr.rr7004a1. Epub 2021 Jul 23 [PubMed PMID: 34292926]
Shutter MC, Akhondi H. Tetracycline. StatPearls. 2026 Jan:(): [PubMed PMID: 31751095]
US Preventive Services Task Force, Davidson KW, Barry MJ, Mangione CM, Cabana M, Caughey AB, Davis EM, Donahue KE, Doubeni CA, Krist AH, Kubik M, Li L, Ogedegbe G, Pbert L, Silverstein M, Simon MA, Stevermer J, Tseng CW, Wong JB. Screening for Chlamydia and Gonorrhea: US Preventive Services Task Force Recommendation Statement. JAMA. 2021 Sep 14:326(10):949-956. doi: 10.1001/jama.2021.14081. Epub [PubMed PMID: 34519796]
Páez-Canro C, Alzate JP, González LM, Rubio-Romero JA, Lethaby A, Gaitán HG. Antibiotics for treating urogenital Chlamydia trachomatis infection in men and non-pregnant women. The Cochrane database of systematic reviews. 2019 Jan 25:1(1):CD010871. doi: 10.1002/14651858.CD010871.pub2. Epub 2019 Jan 25 [PubMed PMID: 30682211]
Level 1 (high-level) evidenceBachmann LH, Barbee LA, Chan P, Reno H, Workowski KA, Hoover K, Mermin J, Mena L. CDC Clinical Guidelines on the Use of Doxycycline Postexposure Prophylaxis for Bacterial Sexually Transmitted Infection Prevention, United States, 2024. MMWR. Recommendations and reports : Morbidity and mortality weekly report. Recommendations and reports. 2024 Jun 6:73(2):1-8. doi: 10.15585/mmwr.rr7302a1. Epub 2024 Jun 6 [PubMed PMID: 38833414]
Kohlhoff SA, Hammerschlag MR. Treatment of Chlamydial infections: 2014 update. Expert opinion on pharmacotherapy. 2015 Feb:16(2):205-12. doi: 10.1517/14656566.2015.999041. Epub [PubMed PMID: 25579069]
Level 3 (low-level) evidence. WHO Guidelines for the Treatment of Chlamydia trachomatis. 2016:(): [PubMed PMID: 27559553]
Tsevat DG, Wiesenfeld HC, Parks C, Peipert JF. Sexually transmitted diseases and infertility. American journal of obstetrics and gynecology. 2017 Jan:216(1):1-9. doi: 10.1016/j.ajog.2016.08.008. Epub [PubMed PMID: 28007229]
Rours GI, Duijts L, Moll HA, Arends LR, de Groot R, Jaddoe VW, Hofman A, Steegers EA, Mackenbach JP, Ott A, Willemse HF, van der Zwaan EA, Verkooijen RP, Verbrugh HA. Chlamydia trachomatis infection during pregnancy associated with preterm delivery: a population-based prospective cohort study. European journal of epidemiology. 2011 Jun:26(6):493-502. doi: 10.1007/s10654-011-9586-1. Epub 2011 May 3 [PubMed PMID: 21538042]
Level 2 (mid-level) evidence