Introduction
Cerebellar hemorrhage, or hematoma, represents a subtype of intracranial hemorrhage (ICH) in which bleeding occurs within the cerebellum and accounts for 9% to 10% of all cases.[1] The posterior fossa provides a limited reserve volume and houses both the cerebellum and the brainstem. Expansion of a hemorrhage in this confined space, particularly near the brainstem or fourth ventricle, may obstruct normal cerebrospinal fluid flow, resulting in hydrocephalus, elevated intracranial pressure, and rapid symptom onset. Cerebellar hemorrhage may occur spontaneously, as a consequence of stroke, or secondary to trauma, with higher prevalence among middle-aged and older adults.[2] Most patients have underlying risk factors, eg, hypertension or small-vessel disease. Clinical presentation varies according to hematoma size, location, and the extent of associated edema within posterior fossa structures.
Initial evaluation typically involves a noncontrast computed tomography (CT) scan, which offers rapid, widely available, and highly sensitive detection of acute hemorrhage, while magnetic resonance imaging serves as a complementary modality in selected cases.[3][2][4] The American Heart Association (AHA) and American Stroke Association recommend urgent surgical evacuation for patients demonstrating neurologic deterioration, brainstem compression, hydrocephalus due to ventricular obstruction, or hemorrhage volume of 15 mL or more. Randomized trials remain limited due to ethical challenges in withholding surgery in life-threatening cases, leaving uncertainty regarding long-term functional outcomes. Prognostic tools, eg, the ICH and ICH-grading scale (ICH-GS) scores, support risk stratification and clinical decision-making. Advances in imaging and supportive care have improved evaluation, yet no universally accepted management approach exists, necessitating individualized treatment based on clinical and radiographic findings.[4][5][6][7]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The most common nontraumatic etiologies for cerebellar hemorrhage are hypertensive vasculopathy, causing microaneurysms and resultant rupture, and cerebral amyloid angiopathy (CAA). Deep cerebellar hemorrhages involving the cerebellar nuclei, deep white matter, or peduncular region are predominantly associated with chronic hypertension and hypertensive arteriopathy, as evidenced by a higher prevalence of hypertension, left ventricular hypertrophy, deep lacunes, and deep or mixed cerebral microbleeds on neuroimaging.[8][9][10][11] In contrast, superficial cerebellar hemorrhages involving the cortex, surrounding white matter, or vermis are more frequently associated with CAA, as evidenced by the presence of strictly lobar cerebral microbleeds, cortical superficial siderosis, and increased amyloid deposition on advanced imaging modalities.[8][9][10][11][12][13] Antithrombotic therapy, advanced age, and the presence of other vascular risk factors further increase the risk of both hypertensive and CAA-related cerebellar hemorrhage.[2][14][13]
Additional causes account for a smaller proportion of cases but require consideration, particularly in younger patients or in the absence of typical vascular risk factors. These include trauma; coagulopathies related to cirrhosis, disseminated intravascular coagulation, or thrombocytopenia; primary or drug-induced bleeding disorders from anticoagulant, antiplatelet, or thrombolytic therapy; ischemic stroke with hemorrhagic transformation; and vascular lesions (eg arteriovenous malformation or dural arteriovenous fistula within the tentorium).[15] Other contributors include primary or metastatic brain tumors,[16][17] septic emboli, central nervous system infections, eg, encephalitis, moyamoya disease, or lupus-related vasculitis, sympathomimetic drug use including cocaine and amphetamines, posterior circulation aneurysms, and remote hemorrhage following supratentorial neurosurgical procedures.[18][19] Pregnancy and the postpartum period introduce additional risk from hypertensive disorders (eg, preeclampsia, eclampsia, and HELLP syndrome).[20]
Surface-based hemorrhage, subarachnoid extension, or identification of an irregular adjacent vessel should prompt concern for aneurysm, arteriovenous malformation, or dural fistula until vascular imaging clarifies the underlying cause. Among neoplastic causes, glioblastoma represents the most common primary central nervous system tumor associated with hemorrhagic transformation, driven by aggressive growth, rapid proliferation, and fragile neovascularization. Metastatic lesions with a higher propensity for hemorrhage commonly originate from the lung, breast, kidney (particularly renal cell carcinoma), and skin, especially melanoma.
Epidemiology
Cerebellar hemorrhage accounts for approximately 9% to 10% of all ICH, which independently represents about 28% to 29% of global incident strokes. The annual incidence of ICH in the United States has increased over the past 2 decades, now estimated at approximately 80,000 cases annually, with case fatality estimated at 30% to 40%. Globally, the absolute numbers of ICH cases, deaths, and disability-adjusted life years increased from 1990 to 2021, despite declines in age-standardized incidence and mortality rates, reflecting population growth and aging.
In 2021, the global age-standardized incidence rate for ICH was approximately 40.8 per 100,000 people, with the highest burden observed in low-sociodemographic-index regions across East Asia, Central Asia, and sub-Saharan Africa.[2][21][22][23][24][4][25][26] Racial and ethnic disparities persist; globally, the burden of ICH is disproportionately higher in low-and middle-income countries. In the United States, ICH incidence is approximately 1.6 times higher among Black and Hispanic individuals compared to White individuals, and the Black to White risk ratios are highest in young and middle-aged adults. ICH incidence increases sharply with age and is expected to remain substantial with aging populations. Males have a higher risk of ICH than females, particularly those older than 35.[2][4][9][23][21][25][27][28][22]
Pathophysiology
The cerebellar region is not unique with respect to the causes of intracranial hemorrhage. Cerebellar hemorrhage most commonly results from rupture of small penetrating arteries or arterioles within the cerebellum, typically due to chronic hypertensive arteriopathy or CAA.[8][2][9][10][12][11][13] The prevailing belief is that patients with long-standing hypertension have degenerative changes in the penetrating small blood vessel walls, leading to the subsequent formation of microaneurysms that rupture and hemorrhage.[29]
Deep cerebellar hemorrhages are strongly associated with hypertensive vasculopathy, characterized by lipohyalinosis, arteriolosclerosis, and vessel wall degeneration from long-standing hypertension.[8][2][9][10][11] Superficial cerebellar hemorrhages are more often linked to CAA, which involves β-amyloid deposition in small leptomeningeal and cortical vessels, leading to vessel fragility and rupture.[8][2][9][10][12][13] Tumors, blood disorders, amyloid, arteriovenous malformation, trauma, and stimulant drug abuse may also lead to cerebellar hemorrhage.[2][30] The pathophysiology of secondary brain injury after cerebellar hemorrhage involves mass effect, hydrocephalus from fourth ventricular obstruction, and perihematomal edema, which can rapidly lead to brainstem compression and herniation.[2][30]
Remote cerebellar hemorrhage after craniotomies is thought to be a result of a loss of cerebrospinal fluid, causing a "sag" in the cerebellum with resultant venous bleeding often tracking along the superior cerebellum, with most cases having a benign course.[31] This may specifically present as a "zebra sign", with hyperdense blood tracking between sulci and isodense brain matter interspersed with the blood. In the hyperacute phase, deterioration is driven by hematoma expansion, rising local tissue pressure, fourth ventricular obstruction, acute hydrocephalus, direct brainstem compression, and herniation. Given the low reserve volume of the posterior fossa, a small increase in the volume of a posterior fossa hematoma can abruptly alter consciousness or respiratory drive.
Secondary injury begins after the initial bleed. Thrombin activates inflammatory signaling and damages the blood-brain barrier, the endothelial interface that regulates fluid and protein movement. Erythrocyte lysis releases hemoglobin and iron, which drive oxidative stress, microglial activation, and perihematomal edema. These mechanisms help explain why patients may worsen after the initial CT even when major rebleeding does not occur.[32]
Obstructive hydrocephalus is the characteristic complication of posterior fossa hemorrhage. Blood within or adjacent to the fourth ventricle blocks cerebrospinal fluid outflow, producing rapid ventricular enlargement and a second wave of pressure-related injury. Hydrocephalus worsens headache, vomiting, sixth nerve dysfunction, and depressed consciousness, and it is one of the strongest predictors of poor outcome in cerebellar hemorrhage. Intraventricular hemorrhage (IVH), which is blood within the ventricular system, magnifies this risk by increasing both acute obstruction and later cerebrospinal fluid circulation failure.[33]
Brainstem effects are both compressive and ischemic. Compression distorts reticular activating pathways, cranial nerve nuclei, and long tracts, while local pressure can compromise perforator flow. The bedside correlates are declining arousal, abnormal ocular movements, respiratory irregularity, and posturing. Because these signs often appear late, treatment decisions should be driven by radiographic crowding before overt brainstem failure is established.[4]
History and Physical
Clinical History
Symptom onset is typically abrupt, with significant variation in symptom presentation depending on the location and size of the hemorrhage. Some patients with a smaller cerebellar hemorrhage remain awake and may complain of headache, nausea, vomiting, vertigo, or ataxia. If the hemorrhage is large, patients may present with an altered level of consciousness or even unresponsiveness. Symptoms can deteriorate rapidly, correlating with hematoma expansion. Symptoms may also occur during stressful situations or strenuous activity. Symptom severity reflects both clot size and the degree of ventricular obstruction or edema.
The clinical history must establish onset time, last known well time, tempo of decline, use of anticoagulants or antiplatelet agents, recent trauma, sympathomimetic exposure, chronic hypertension, cancer history, and symptoms suggesting aneurysm or vascular malformation. The current AHA and ASA guideline also emphasizes liver disease, uremia, hematologic disorders, smoking, alcohol, marijuana, and cognitive impairment because these data influence both etiology and emergency treatment. Medication history is especially important because reversal should often begin before specialized assays return results.[4]
Symptom presentation in descending order of frequency includes the following:
- Abrupt onset of headache
- Nausea and vomiting
- Difficulty with ambulation (truncal ataxia)
- Vertigo and dizziness
- Dysarthria
- Neck pain or nuchal rigidity
- Loss of consciousness or altered mental status
Physical Examination
The examination should prioritize airway safety, level of consciousness, ocular motility, bulbar function, appendicular coordination, and truncal stability. The Glasgow Coma Scale (GCS), a standardized consciousness score, remains essential because a declining GCS is both a prognostic marker and a surgical trigger. Dysarthria, dysphagia, poor cough, or inability to sit upright may be more informative than limb weakness, which is often absent. The National Institutes of Health Stroke Scale (NIHSS) underestimates the severity of posterior circulation stroke because this scale assigns little weight to gait and bulbar dysfunction. In posterior circulation stroke cohorts, adding abnormal cough, dysphagia, and truncal gait ataxia improved prognostic discrimination beyond baseline NIHSS. A low NIHSS score should therefore not reassure the clinician if the patient cannot swallow, stand, or remain alert.[34][4]
Physical examination is also variable and dependent on hemorrhage location, with some patients awake and others unresponsive. Cerebellar signs may include any combination of the following:
- Limb ataxia
- Dysarthria
- Nystagmus
- Abnormal gaze or facial weakness (cranial nerve palsy ipsilateral to the hematoma)
- Abnormal gait
Serial examination is as important as the first examination. New somnolence, repeated emesis, new cranial nerve findings, or a decline of even 2 GCS points should trigger immediate repeat imaging and renewed neurosurgical review. A stable posterior fossa hemorrhage, therefore, requires close monitoring and should not be considered benign.
Evaluation
Diagnostic Imaging
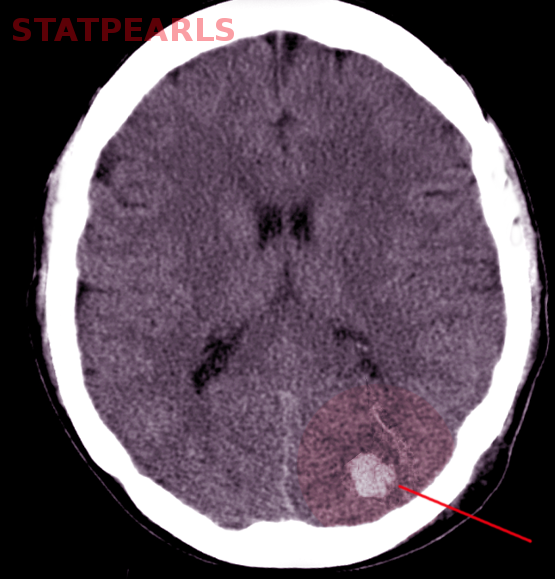
Noncontrast head CT provides a rapid, widely available, and highly efficient initial evaluation for patients presenting with signs and symptoms suggestive of cerebellar hemorrhage. Most hemorrhages appear as hyperdense lesions within the cerebellum (see Images. Cerebellar Hemorrhage and Cerebellar Hematoma). Dense calcification of the dentate nucleus may mimic hemorrhage; however, absence of mass effect, sharply defined margins, and bilateral symmetry favor calcification. Contrast extravasation following endovascular procedures may also appear hyperdense, though dual-energy CT allows accurate differentiation.[35]
Imaging features, eg, the CTA “spot sign,” along with heterogeneous density or irregular margins on noncontrast CT, predict hematoma expansion and correlate with worse outcomes. Early estimation of hematoma volume remains essential, as operative thresholds depend on size. The bedside standard uses the ABC/2 method, where A represents the greatest diameter, B the largest perpendicular diameter, and C estimates clot depth based on slice number and thickness.
Initial CT interpretation should systematically determine the following:
- Hematoma volume
- Fourth ventricular compression or obliteration
- Hydrocephalus
- Intraventricular extension
- Basal cistern effacement
- Any indication of a secondary cause, eg, calcification, atypical edema, or serpiginous vascular structures.
Vascular imaging becomes necessary in atypical presentations. CTA serves as the preferred initial modality in younger or normotensive patients, in cases with unusual imaging features, or when chronic hypertensive hemorrhage lacks convincing evidence. Further evaluation with magnetic resonance imaging (MRI), magnetic resonance angiography (MRA), or catheter angiography should be performed when suspicion persists despite negative CTA findings, particularly when tumor, cavernoma, cerebral amyloid angiopathy, or other macrovascular lesions remain possible.[36][37] Serial CT imaging within the first 24 hours assists in identifying hematoma expansion, hydrocephalus, edema, or herniation. Clinical changes, eg, new somnolence, vomiting, decline in GCS score, or new cranial nerve deficits, warrant immediate repeat imaging.
Laboratory Studies
Laboratory evaluation should directly inform management decisions and include complete blood count, platelet count, PT/INR, aPTT, creatinine, electrolytes, glucose, liver function tests, and type and screen. Additional studies, including fibrinogen, troponin, toxicology screening, pregnancy testing, inflammatory markers, or blood cultures, should be obtained selectively. Accurate identification of anticoagulant exposure remains critical, as reversal strategies for warfarin, dabigatran, and factor Xa inhibitors are time-sensitive and should proceed without delay when the history confirms use.
Additional Diagnostic Studies
Electroencephalography serves a limited role and may aid evaluation when mental status changes remain unexplained or fluctuate despite imaging findings. Airway and swallowing assessments are an essential component of early evaluation, as bulbar dysfunction, vomiting, and decreased alertness increase the risk of aspiration. Severity scoring systems (eg, the ICH score) assist with baseline risk communication but should not independently guide treatment limitation. Current guidelines advise against early do-not-resuscitate decisions within the first 24 hours, given the potential inaccuracy of early prognostic estimates.[38]
Key Evaluation Elements
A structured evaluation should determine the following:
- Is the lesion causing mass effect requiring surgical decompression?
- Initial noncontrast CT assesses hematoma volume, fourth ventricular compression, brainstem displacement, basal cistern effacement, and hydrocephalus (see Image. Noncontrast CT of Cerebellar Hematoma).
- Is the clot likely to expand?
- Irregular or heterogeneous density on noncontrast CT and the CTA spot sign predict hematoma expansion.
- Is there a coagulopathy requiring immediate reversal?
- Platelet count, PT/INR, aPTT, and medication history identify anticoagulant or platelet-related coagulopathy.
- Is the hemorrhage due to primary small vessel disease or a secondary structural lesion?
- Younger or normotensive patients, superficial cerebellar hemorrhage, or atypical imaging features raise suspicion for an underlying structural lesion, eg, a vascular malformation, aneurysm, tumor, or venous thrombosis.
- When such features are present, vascular imaging should be obtained.
Treatment / Management
Treatment of cerebellar hemorrhage focuses on preventing four early causes of poor outcomes: hematoma expansion, obstructive hydrocephalus, brainstem compression, and secondary systemic complications. Optimal care occurs in a specialized stroke or neurocritical care unit equipped for frequent neurologic assessments, protocolized blood pressure management, rapid pharmacologic reversal of coagulopathy, dysphagia screening, and immediate neurosurgical access.[38]
Management decisions regarding cerebellar hemorrhage depend heavily on both the hemorrhage size and the clinical presentation. Cerebellar hemorrhages above 22 mL/greater than 3 cm are significantly more likely to have poor outcomes in treatment.[39] Airway protection with endotracheal intubation may be necessary for patients who present with severely altered and a depressed level of consciousness or altered mental status (GCS less than 8). Neurosurgical consultation should be obtained urgently after diagnosis to assist with optimal management and treatment.(B2)
Conservative Management
Small hemorrhages without significant mass effect can often be managed conservatively with admission to a critical care unit that can provide frequent neurologic assessments. Large hemorrhages, typically greater than 3 cm or 15 mL, may require surgical intervention and evacuation, particularly if associated with edema, intraventricular extension, brainstem displacement, or hydrocephalus secondary to the high risk of cerebellar herniation.[4] However, patients presenting with intact neurological function may also benefit from more conservative management.[40]
Blood pressure management
Acute blood pressure elevation commonly accompanies cerebellar hemorrhage, and management must balance reducing hemorrhage growth and intracranial pressure while preserving cerebral perfusion. Consensus recommendations support lowering systolic blood pressure to less than 140 mm Hg with intensive therapy (2 or more intravenous medications).[41][42] The 2022 American Heart Association guidelines on the management of blood pressure in intracerebral hemorrhage recommend targeting systolic blood pressure between 130 and 150 mm Hg, with harm noted at systolic blood pressure below 130 mm Hg.[4] (A1)
Management to maintain this blood pressure range should be initiated within 2 hours of the onset of the hemorrhage, if possible, aiming to reach the goal systolic blood pressure within 1 hour without overshooting. Recent expert consensus similarly recommends lowering systolic blood pressure to less than 140 mm Hg within 6 hours in patients with minor or moderate intracerebral hemorrhage (hematoma volume <30 mL), ideally initiating therapy within 2 hours of symptom onset and minimizing blood pressure variability. Reductions greater than 70 mm Hg from baseline should be avoided.[38]
Body temperature maintenance
Body temperature should be maintained within the normal range. If the patient develops an elevated body temperature, pharmacotherapy or cooling measures should be instituted to maintain a core body temperature below 37.5 °C, as fever has been shown to worsen outcomes in the injured brain.[43] Current evidence does not show any benefit to instituting hypothermia for cerebellar hemorrhage.(B2)
Blood glucose management
Maintaining normal glucose levels is necessary as both hypoglycemia and hyperglycemia have correlations with poorer outcomes in patients with cerebellar hemorrhage.[44][45] Current practice suggests a reasonable glucose range of 100 to 180 mg/dL.[46] In the intensive care setting, insulin therapy is preferred over oral agents. Intensive compared to conventional glucose control did not demonstrate any significant difference in clinical outcomes; however, hypoglycemia is more clinically detrimental than mild hyperglycemia in critically ill patients such as these.[47][48] (A1)
Intravascular volume
Normovolemia should be maintained with isotonic fluids, with appropriate correction of serum electrolytes, including sodium, potassium, and magnesium.[49] Mild hypertonic fluid, eg, 1.5% hypertonic saline, may be used to correct hyponatremia. Cardiac arrhythmias may occur with brain injury, and maintaining potassium above 4.0 mmol/L and magnesium above 2.0 mg/dL is essential to prevent exacerbation of arrhythmias.
Coagulopathy concerns
Anticoagulation and antiplatelet medications should be immediately discontinued, and the effects reversed in cases of cerebellar hemorrhage. The coagulopathy should be reversed with an appropriate reversal agent. Patients on warfarin should receive vitamin K (10 mg) and factor replacement. The 2022 AHA guidelines recommend using 4-factor Prothrombin Complex Concentrate (PCC) over fresh frozen plasma (FFP) for faster reversal.[4] Individual reversal agents for specific anticoagulants should be used when applicable, eg, for dabigatran (Pradaxa) or protamine sulfate for unfractionated heparin (UFH). Factor replacement with 4-factor PCC should be considered for patients on novel oral anticoagulants without specific reversal agents, but supporting evidence is limited.[50][51]
Platelet replacement therapy in patients on antiplatelet medications or those with thrombocytopenia and platelet counts less than 50,000 platelets/mL of blood is often performed with severe bleeding and before surgical intervention. This may improve surgical outcomes, but for those not undergoing surgery, the benefit is unknown. Platelet replacement therapy may even cause harm if given to patients without severe thrombocytopenia.[4]
Other management considerations
If patients are intubated, normocarbia should be maintained. Prophylactic hyperventilation has not been shown to benefit in these cases, though no studies have shown harm either.[4] Corticosteroids have not demonstrated any benefit in the treatment of cerebellar hemorrhage. The use of antiseizure medications has been considered. However, prophylactic antiseizure medications generally do not improve morbidity or mortality; however, if fluctuating mental status or seizure activity occurs, EEG evaluation is warranted, and confirmed seizures should be treated appropriately.[52][53]
Intermittent pneumatic compression is recommended for venous thromboembolism prophylaxis in immobile patients and should be continued until hospital discharge or independent ambulation. If intermittent pneumatic compression is not feasible, pharmacologic prophylaxis with low-molecular-weight heparin may be considered in immobile patients or those at high thrombotic risk.[38]
Hydrocephalus management is central in posterior fossa hemorrhage. An external ventricular drain (EVD), a catheter placed into the ventricular system, can rapidly relieve obstructive hydrocephalus and improve consciousness. An EVD is indicated when hydrocephalus contributes to deterioration or threatens herniation. EVD alone, however, does not remove posterior fossa mass effect. If the clot continues to compress the brainstem or the fourth ventricle, ventricular drainage without clot evacuation may provide only partial benefit. This is why the guideline recommendation is framed as immediate surgical removal with or without EVD when any major posterior fossa criterion is present.[4]
Surgical Management
In cerebellar ICH, immediate surgical removal of the hemorrhage with or without EVD is recommended to reduce mortality when any one of the following is present: neurologic deterioration, brainstem compression, obstructive hydrocephalus, or hemorrhage volume at least 15 mL. This is a recommendation in the 2022 AHA and ASA guideline.[4] The 2025 ESO and EANS guidelines align on a practical direction and recommend evacuation for hematomas larger than 15 mL to improve survival, while acknowledging very low-quality evidence.[38]
The typical surgery is a suboccipital craniectomy or craniotomy with clot evacuation. The goals are decompression of the posterior fossa, relief of fourth ventricular obstruction, and removal of the mass lesion before irreversible brainstem injury occurs. In selected cases of space-occupying hemorrhages, some retrospective data suggest that extension to a C1 laminectomy can improve exposure and decompression. Evidence favoring one open technique over another is limited, so the preferred operation is the one that the available neurosurgical team can perform most rapidly and completely.[54]
Minimally invasive and endoscopic approaches are promising but not yet definitive. A 2025 systematic review and meta-analysis found less blood loss, shorter operative time, and fewer infections or cerebrospinal fluid leaks with neuroendoscopic evacuation than with open surgery, but no clear difference in mortality, rebleeding, or functional outcome.[55] Recent enthusiasm for minimally invasive ICH surgery is driven mainly by supratentorial evidence and should not be directly extrapolated to the cerebellum.(A1)
Key Management Components
The primary elements of cerebellar hemorrhage management include:
- Admit to a stroke or neurocritical care unit with frequent neurologic examinations and continuous blood pressure monitoring.
- Protect the airway early when consciousness, bulbar function, or vomiting creates aspiration risk.
- Lower blood pressure smoothly, usually toward a systolic blood pressure of about 140 mm Hg, while avoiding a systolic blood pressure below 130 mm Hg.
- Reverse the anticoagulant effect immediately, depending on the agent.
- Proceed to immediate hematoma evacuation with or without EVD if there is neurologic deterioration, brainstem compression, obstructive hydrocephalus, or volume of at least 15 mL.
Differential Diagnosis
The differential diagnosis for patients presenting with a sudden onset of symptoms, eg, headache, nausea, vomiting, dizziness, or vertigo, is broad and includes central, peripheral, and systemic causes.
Central causes include:
- Acute demyelinating disorder, eg, multiple sclerosis or encephalitis
- Alcohol use disorder
- Cerebellar hemorrhage
- Cerebellar infarction
- Cerebellar neoplasm
- Cerebellitis
- Illicit drug use
- Medication toxicity (phenytoin or carbamazepine)
Peripheral causes include:
- Benign paroxysmal positional vertigo (BPPV)
- Labyrinthitis
- Meniere disease
- Vestibular neuronitis
Other potential causes include:
- Anemia
- Electrolyte disturbances
- Dehydration
- Gastroenteritis
Prognosis
The mortality associated with cerebellar hemorrhage can range from 25% to 57%.[56][57] Outcomes following surgery are strongly correlated with the patient's clinical status before surgery, but are favorable in more than half of cases.[56][58] Therefore, recommendations are that in the absence of multiple comorbidities, surgical intervention should be pursued even in patients with poor preoperative neurologic status. Other factors influencing mortality and morbidity include association with the use of blood thinners and admission anemia.[4] If patients are discharged alive from the hospital, mortality within a year of cerebellar hemorrhage has been estimated at around 25%, consistent with intracerebral hemorrhages.[59]
Complications
Perihemorrhagic Edema and Mass Effect
Significant cerebellar hemorrhage may have associated perihemorrhagic edema and mass effect, which can lead to multiple complications, including brainstem compression, cerebellar herniation, compression of the fourth ventricle with resultant obstructive hydrocephalus, an extension of hemorrhage into the ventricular system, and recurrent hemorrhage typically within the first 24 hours. The 2 options for managing the mass effect from the cerebellar hemorrhage are hyperosmolar agents or decompressive surgery. However, decompressive surgery and an external ventricular drain are the only options that have been shown to improve mortality.[4]
Osmolar therapy is used to reduce the space-occupying effects of hemorrhage and edema by increasing serum osmolality and facilitating an osmotic movement of water into the vasculature with resultant reactive vasoconstriction. The goal is an overall reduction in intracranial pressure and tissue shrinkage. No superiority of hypertonic saline over mannitol, or vice versa, has been demonstrated in the treatment of intracranial hemorrhage. Hypertonic saline concentrations typically utilized for treatment are 3% (250 mL bolus), 10% (75 to 150 mL bolus), and 23.4% (30 mL bolus). Boluses and continuous infusions aim for sodium levels of 145 to 155 mmol/L and osmolality of 310 to 320 mOsm/kg.[60]
Complications may occur with infusions, eg, hypotension, pulmonary edema, heart failure, coagulopathy, hypokalemia, intravascular hemolysis, and encephalopathy, but these are rare.[61] Mannitol is a sugar alcohol that acts as a diuretic and is usually administered as a 1 to 2 g/kg bolus (20% concentration) with additional doses of 0.5 g/kg every 4 to 6 hours.[62]][63] Maintaining euvolemia during its administration is imperative, and caution is advised in patients with renal failure as the mannitol may lead to fluid overload, necessitating dialysis shortly after administration. Serum osmolality should remain below 320 mOsm/kg to prevent renal toxicity.
Surgical Complications
The decompressive surgery of choice for cerebellar hemorrhage is a suboccipital craniectomy with hematoma evacuation. Clinical outcomes are significantly improved when the procedure is performed as early as possible, especially in patients showing signs of neurological deterioration or radiographic evidence of mass effect.[64][65] The surgical approach is necessary when the patient's neurologic status continues to decline due to brainstem compression or obstructive hydrocephalus, and it appears secondary to the mass effect of the hemorrhage and perihemorrhagic edema. An EVD may be used to treat the obstructive hydrocephalus in addition to surgery.
Criteria for selecting patients for surgery or EVD placement are based on both clinical presentation and radiographic features, including hematoma size, ventricular extension, hydrocephalus, brainstem compression, and cisternal effacement.[66][67] Craniectomy has shown a mortality benefit in large (>12 mL) intracerebral hemorrhages, but has not shown a morbidity benefit; hemorrhages smaller than this removed surgically do not demonstrate a mortality or morbidity benefit.[5] This result may be secondary to treatment of hydrocephalus resulting from the hemorrhage rather than treatment of the hemorrhage itself.[68] Hemorrhages less than 3 cm in diameter without evidence of brainstem compression or hydrocephalus may be treated with close observation in an intensive care setting without surgery. A stereotactic burr-hole aspiration is an option for patients with smaller hemorrhages.[69]
Systemic and Procedure-Related Complications
Systemic complications are common and largely preventable. Aspiration, pneumonia, respiratory failure, urinary infection, venous thromboembolism, pressure injury, and deconditioning rise sharply when dysphagia and immobility are not addressed early. Procedure-related complications are also essential to consider. EVD may cause catheter tract hemorrhage, infection, malposition, obstruction, or need for revision, and posterior fossa surgery may be complicated by rebleeding, wound problems, or cerebrospinal fluid leak. Among survivors, gait ataxia, dysarthria, dysphagia, persistent vertigo, and recurrent vascular events often dominate long-term disability.
Deterrence and Patient Education
Most cerebellar hemorrhages are hypertensive in origin. Patients with hypertension should receive education so that they are aware of all the potential risks and complications associated with poor control of their disease process. These patients should be encouraged to seek medical attention urgently if they develop worrisome symptoms. In addition, patients who are discharged from the hospital following a cerebellar hemorrhage should be closely monitored and placed on an antihypertensive medication if indicated by their out-of-hospital blood pressures to prevent recurrence.
Enhancing Healthcare Team Outcomes
Cerebellar hemorrhage is a critical subtype of intracranial hemorrhage involving bleeding within the posterior fossa, where limited space predisposes to rapid neurologic decline. Expansion of a hematoma can obstruct cerebrospinal fluid flow, leading to hydrocephalus, elevated intracranial pressure, and brainstem compression. Most cases result from chronic hypertension or cerebral amyloid angiopathy, though trauma, coagulopathies, vascular malformations, tumors, and medications may contribute. Patients commonly present with sudden headache, nausea, vomiting, vertigo, ataxia, and possible deterioration in consciousness. Noncontrast CT enables rapid diagnosis and assessment of hematoma size, ventricular involvement, and mass effect. Management prioritizes airway protection, blood pressure control, reversal of anticoagulation, close neurologic monitoring, and timely neurosurgical evaluation, with surgical evacuation indicated in patients with neurologic decline, hydrocephalus, or significant hematoma burden.
Interprofessional collaboration is essential for optimizing outcomes and reducing morbidity and mortality. Physicians and advanced practice providers lead diagnosis, risk stratification, and management decisions, while primary care clinicians contribute to risk factor identification and long-term prevention. Nurses perform frequent neurologic assessments, monitor for deterioration, and support airway and hemodynamic stability. Pharmacists ensure timely anticoagulant reversal and safe medication management, as well as manage medication reconciliation and consider potential drug interactions. Neurosurgeons evaluate for operative intervention, and radiologists guide diagnostic accuracy. Coordinated communication, shared decision-making with patients and families, and timely escalation of care are critical to prevent complications such as herniation and hydrocephalus, ensure continuity of care, and support recovery and secondary prevention strategies.
Media
(Click Image to Enlarge)
Cerebellar Hemorrhage. Noncontrast head CT provides a rapid, widely available, and highly efficient initial evaluation for patients presenting with signs and symptoms suggestive of cerebellar hemorrhage.
Contributed by S Bhimji, MD
(Click Image to Enlarge)

Cerebellar Hematoma. Most hemorrhages appear as hyperdense lesions within the cerebellum.
Contributed by S Munakomi, MD
(Click Image to Enlarge)
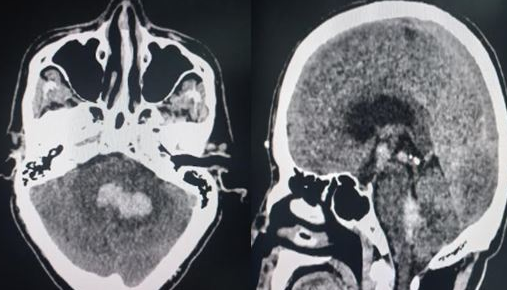
Noncontrast CT of Cerebellar Hematoma. Initial noncontrast CT assesses hematoma volume, fourth ventricular compression, brainstem displacement, basal cistern effacement, and hydrocephalus
Contributed by S Munakomi, MD
References
Datar S, Rabinstein AA. Cerebellar hemorrhage. Neurologic clinics. 2014 Nov:32(4):993-1007. doi: 10.1016/j.ncl.2014.07.006. Epub 2014 Sep 11 [PubMed PMID: 25439293]
Sheth KN. Spontaneous Intracerebral Hemorrhage. The New England journal of medicine. 2022 Oct 27:387(17):1589-1596. doi: 10.1056/NEJMra2201449. Epub [PubMed PMID: 36300975]
Expert Panel on Neurological Imaging, Pannell JS, Corey AS, Shih RY, Austin MJ, Chu S, Davis MA, Ducruet AF, Hunt CH, Ivanidze J, Kalnins A, Lacy ME, Lo BM, Setzen G, Shaines MD, Soares BP, Soderlund KA, Thaker AA, Wang LL, Burns J. ACR Appropriateness Criteria® Cerebrovascular Diseases-Stroke and Stroke-Related Conditions. Journal of the American College of Radiology : JACR. 2024 Jun:21(6S):S21-S64. doi: 10.1016/j.jacr.2024.02.015. Epub [PubMed PMID: 38823945]
Greenberg SM, Ziai WC, Cordonnier C, Dowlatshahi D, Francis B, Goldstein JN, Hemphill JC 3rd, Johnson R, Keigher KM, Mack WJ, Mocco J, Newton EJ, Ruff IM, Sansing LH, Schulman S, Selim MH, Sheth KN, Sprigg N, Sunnerhagen KS, American Heart Association/American Stroke Association. 2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage: A Guideline From the American Heart Association/American Stroke Association. Stroke. 2022 Jul:53(7):e282-e361. doi: 10.1161/STR.0000000000000407. Epub 2022 May 17 [PubMed PMID: 35579034]
Kuramatsu JB, Biffi A, Gerner ST, Sembill JA, Sprügel MI, Leasure A, Sansing L, Matouk C, Falcone GJ, Endres M, Haeusler KG, Sobesky J, Schurig J, Zweynert S, Bauer M, Vajkoczy P, Ringleb PA, Purrucker J, Rizos T, Volkmann J, Müllges W, Kraft P, Schubert AL, Erbguth F, Nueckel M, Schellinger PD, Glahn J, Knappe UJ, Fink GR, Dohmen C, Stetefeld H, Fisse AL, Minnerup J, Hagemann G, Rakers F, Reichmann H, Schneider H, Rahmig J, Ludolph AC, Stösser S, Neugebauer H, Röther J, Michels P, Schwarz M, Reimann G, Bäzner H, Schwert H, Claßen J, Michalski D, Grau A, Palm F, Urbanek C, Wöhrle JC, Alshammari F, Horn M, Bahner D, Witte OW, Günther A, Hamann GF, Hagen M, Roeder SS, Lücking H, Dörfler A, Testai FD, Woo D, Schwab S, Sheth KN, Huttner HB. Association of Surgical Hematoma Evacuation vs Conservative Treatment With Functional Outcome in Patients With Cerebellar Intracerebral Hemorrhage. JAMA. 2019 Oct 8:322(14):1392-1403. doi: 10.1001/jama.2019.13014. Epub [PubMed PMID: 31593272]
Won SY, Walter J, Hernandez-Duran S, Alhalabi OT, Behmanesh B, Bernstock JD, Czabanka M, Dinc N, Dubinski D, Flüh C, Freiman TM, Grosch AS, Herrmann E, Kang YS, Konczalla J, Kramer A, Lehmann F, Lemcke J, Melkonian R, Mielke D, Müller L, Ringel F, Rohde V, Schneider M, Senft C, Schuss P, Turgut MÖ, Synowitz M, Ullmann JM, Vatter H, Zweckberger K, Kilinc F, Gessler F. Reappraisal of Intracerebral Hemorrhages and Intracerebral Hemorrhage Grading Scale Score in Surgically and Medically Managed Cerebellar Intracerebral Hemorrhage. Neurosurgery. 2023 May 1:92(5):1021-1028. doi: 10.1227/neu.0000000000002318. Epub 2022 Dec 21 [PubMed PMID: 36700686]
Singh SD, Brouwers HB, Senff JR, Pasi M, Goldstein J, Viswanathan A, Klijn CJM, Rinkel GJE. Haematoma evacuation in cerebellar intracerebral haemorrhage: systematic review. Journal of neurology, neurosurgery, and psychiatry. 2020 Jan:91(1):82-87. doi: 10.1136/jnnp-2019-321461. Epub [PubMed PMID: 31848229]
Level 1 (high-level) evidenceIncontri D, Marchina S, Andreev A, Wilson M, Wang JY, Lin D, Heistand EC, Carvalho F, Selim M, Lioutas VA. Etiology of Primary Cerebellar Intracerebral Hemorrhage Based on Topographic Localization. Stroke. 2023 Dec:54(12):3074-3080. doi: 10.1161/STROKEAHA.123.044271. Epub 2023 Oct 16 [PubMed PMID: 37842779]
Pasi M, Marini S, Morotti A, Boulouis G, Xiong L, Charidimou A, Ayres AM, Lee MJ, Biffi A, Goldstein JN, Rosand J, Gurol ME, Greenberg SM, Viswanathan A. Cerebellar Hematoma Location: Implications for the Underlying Microangiopathy. Stroke. 2018 Jan:49(1):207-210. doi: 10.1161/STROKEAHA.117.019286. Epub 2017 Nov 28 [PubMed PMID: 29183952]
Pasi M, Charidimou A, Boulouis G, Fotiadis P, Morotti A, Xiong L, Marini S, Ayres A, Frosch MP, Goldstein JN, Rosand J, Gurol ME, Greenberg SM, Viswanathan A. Cerebral small vessel disease in patients with spontaneous cerebellar hemorrhage. Journal of neurology. 2019 Mar:266(3):625-630. doi: 10.1007/s00415-018-09177-w. Epub 2019 Jan 8 [PubMed PMID: 30617995]
Das AS, Abramovitz Fouks A, Gökçal E, Rotschild O, Pasi M, Regenhardt RW, Goldstein JN, Viswanathan A, Rosand J, Greenberg SM, Gurol ME. Characterizing the underlying microangiopathy of deep cerebellar intracerebral hemorrhage. Journal of neurology. 2025 Jan 24:272(2):167. doi: 10.1007/s00415-025-12905-8. Epub 2025 Jan 24 [PubMed PMID: 39853492]
Tsai HH, Pasi M, Tsai LK, Chen YF, Chen YW, Tang SC, Gurol ME, Yen RF, Jeng JS. Superficial Cerebellar Microbleeds and Cerebral Amyloid Angiopathy: A Magnetic Resonance Imaging/Positron Emission Tomography Study. Stroke. 2020 Jan:51(1):202-208. doi: 10.1161/STROKEAHA.119.026235. Epub 2019 Nov 15 [PubMed PMID: 31726962]
Fakan B, Reisz Z, Zadori D, Vecsei L, Klivenyi P, Szalardy L. Predictors of localization, outcome, and etiology of spontaneous intracerebral hemorrhages: focus on cerebral amyloid angiopathy. Journal of neural transmission (Vienna, Austria : 1996). 2020 Jun:127(6):963-972. doi: 10.1007/s00702-020-02174-2. Epub 2020 Mar 19 [PubMed PMID: 32193732]
Arndt P, Chahem C, Luchtmann M, Kuschel JN, Behme D, Pfister M, Neumann J, Görtler M, Dörner M, Pawlitzki M, Jansen R, Meuth SG, Vielhaber S, Henneicke S, Schreiber S. Risk factors for intracerebral hemorrhage in small-vessel disease and non-small-vessel disease etiologies-an observational proof-of-concept study. Frontiers in neurology. 2024:15():1322442. doi: 10.3389/fneur.2024.1322442. Epub 2024 Mar 7 [PubMed PMID: 38515448]
Satoh K, Satomi J, Nakajima N, Matsubara S, Nagahiro S. Cerebellar hemorrhage caused by dural arteriovenous fistula: a review of five cases. Journal of neurosurgery. 2001 Mar:94(3):422-6 [PubMed PMID: 11235946]
Level 3 (low-level) evidenceKim MS, Kim SW, Chang CH, Kim OL. Cerebellar pilocytic astrocytomas with spontaneous intratumoral hemorrhage in adult. Journal of Korean Neurosurgical Society. 2011 Jun:49(6):363-6. doi: 10.3340/jkns.2011.49.6.363. Epub 2011 Jun 30 [PubMed PMID: 21887396]
Level 3 (low-level) evidenceMesiwala AH, Avellino AM, Roberts TS, Ellenbogen RG. Spontaneous cerebellar hemorrhage due to a juvenile pilocytic astrocytoma: case report and review of the literature. Pediatric neurosurgery. 2001 May:34(5):235-8 [PubMed PMID: 11423772]
Level 3 (low-level) evidenceCordonnier C, Demchuk A, Ziai W, Anderson CS. Intracerebral haemorrhage: current approaches to acute management. Lancet (London, England). 2018 Oct 6:392(10154):1257-1268. doi: 10.1016/S0140-6736(18)31878-6. Epub [PubMed PMID: 30319113]
Friedman JA, Piepgras DG. Remote cerebellar hemorrhage. Journal of neurosurgery. 2002 Aug:97(2):498-9; author reply 499 [PubMed PMID: 12186489]
Level 3 (low-level) evidenceGhadimi K, Shapouran S. Epidemiology and pathophysiology of primary versus secondary intracranial hemorrhage in pregnant and nonpregnant patients: A literature review. Clinical neurology and neurosurgery. 2025 Oct:257():109056. doi: 10.1016/j.clineuro.2025.109056. Epub 2025 Jul 11 [PubMed PMID: 40652763]
GBD 2021 Stroke Risk Factor Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet. Neurology. 2024 Oct:23(10):973-1003. doi: 10.1016/S1474-4422(24)00369-7. Epub [PubMed PMID: 39304265]
Level 1 (high-level) evidenceGBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet. Neurology. 2021 Oct:20(10):795-820. doi: 10.1016/S1474-4422(21)00252-0. Epub 2021 Sep 3 [PubMed PMID: 34487721]
Level 1 (high-level) evidenceWang ZW, Wan MP, Tai JH, Wang Y, Yin MY. Global regional and national burden of intracerebral hemorrhage between 1990 and 2021. Scientific reports. 2025 Jan 29:15(1):3624. doi: 10.1038/s41598-025-88017-0. Epub 2025 Jan 29 [PubMed PMID: 39880918]
Bako AT, Pan A, Potter T, Tannous J, Johnson C, Baig E, Meeks J, Woo D, Vahidy FS. Contemporary Trends in the Nationwide Incidence of Primary Intracerebral Hemorrhage. Stroke. 2022 Mar:53(3):e70-e74. doi: 10.1161/STROKEAHA.121.037332. Epub 2022 Feb 3 [PubMed PMID: 35109682]
Song D, Xu D, Li M, Wang F, Feng M, Badr A, Rigamonti D, Cistola D, Yan D, Zhang J, Guo F. Global, regional, and national burdens of intracerebral hemorrhage and its risk factors from 1990 to 2021. European journal of neurology. 2025 Jan:32(1):e70031. doi: 10.1111/ene.70031. Epub [PubMed PMID: 39731311]
Hao Y, Xia X, Zhu J, Yang W, Zhao X, Wang A. Temporal trends in the incidence of intracerebral hemorrhage from 1992 to 2021: An age-period-cohort analysis based on the global burden of disease study 2021. Ageing research reviews. 2025 Aug:110():102789. doi: 10.1016/j.arr.2025.102789. Epub 2025 Jun 2 [PubMed PMID: 40466777]
Madsen TE, Ding L, Khoury JC, Haverbusch M, Woo D, Ferioli S, De Los Rios La Rosa F, Martini SR, Adeoye O, Khatri P, Flaherty ML, Mackey J, Mistry EA, Demel S, Coleman E, Jasne A, Slavin S, Walsh KB, Star M, Broderick JP, Kissela B, Kleindorfer DO. Trends Over Time in Stroke Incidence by Race in the Greater Cincinnati Northern Kentucky Stroke Study. Neurology. 2024 Feb 13:102(3):e208077. doi: 10.1212/WNL.0000000000208077. Epub 2024 Jan 10 [PubMed PMID: 38546235]
Carnethon MR, Pu J, Howard G, Albert MA, Anderson CAM, Bertoni AG, Mujahid MS, Palaniappan L, Taylor HA Jr, Willis M, Yancy CW, American Heart Association Council on Epidemiology and Prevention; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Functional Genomics and Translational Biology; and Stroke Council. Cardiovascular Health in African Americans: A Scientific Statement From the American Heart Association. Circulation. 2017 Nov 21:136(21):e393-e423. doi: 10.1161/CIR.0000000000000534. Epub 2017 Oct 23 [PubMed PMID: 29061565]
Garcia JH, Ho KL. Pathology of hypertensive arteriopathy. Neurosurgery clinics of North America. 1992 Jul:3(3):497-507 [PubMed PMID: 1633473]
de Oliveira Manoel AL, Goffi A, Zampieri FG, Turkel-Parrella D, Duggal A, Marotta TR, Macdonald RL, Abrahamson S. The critical care management of spontaneous intracranial hemorrhage: a contemporary review. Critical care (London, England). 2016 Sep 18:20():272. doi: 10.1186/s13054-016-1432-0. Epub 2016 Sep 18 [PubMed PMID: 27640182]
Friedman JA, Piepgras DG, Duke DA, McClelland RL, Bechtle PS, Maher CO, Morita A, Perkins WJ, Parisi JE, Brown RD Jr. Remote cerebellar hemorrhage after supratentorial surgery. Neurosurgery. 2001 Dec:49(6):1327-40 [PubMed PMID: 11846932]
Level 2 (mid-level) evidenceMagid-Bernstein J, Girard R, Polster S, Srinath A, Romanos S, Awad IA, Sansing LH. Cerebral Hemorrhage: Pathophysiology, Treatment, and Future Directions. Circulation research. 2022 Apr 15:130(8):1204-1229. doi: 10.1161/CIRCRESAHA.121.319949. Epub 2022 Apr 14 [PubMed PMID: 35420918]
Level 3 (low-level) evidenceShu J, Wang W, Ye R, Zhou Y, Tong J, Li X, Lv X, Zhang G, Xu F, Zhang J. Risk factors of prognosis for spontaneous cerebellar hemorrhage: a systematic review and meta-analysis. Acta neurochirurgica. 2024 Jul 10:166(1):291. doi: 10.1007/s00701-024-06174-z. Epub 2024 Jul 10 [PubMed PMID: 38985355]
Level 1 (high-level) evidenceAlemseged F, Rocco A, Arba F, Schwabova JP, Wu T, Cavicchia L, Ng F, Ng JL, Zhao H, Williams C, Sallustio F, Balabanski AH, Tomek A, Parson MW, Mitchell PJ, Diomedi M, Yassi N, Churilov L, Davis SM, Campbell BCV, Basilar Artery Treatment and Management (BATMAN) Collaboration Investigators. Posterior National Institutes of Health Stroke Scale Improves Prognostic Accuracy in Posterior Circulation Stroke. Stroke. 2022 Apr:53(4):1247-1255. doi: 10.1161/STROKEAHA.120.034019. Epub 2021 Dec 15 [PubMed PMID: 34905944]
Gupta R, Phan CM, Leidecker C, Brady TJ, Hirsch JA, Nogueira RG, Yoo AJ. Evaluation of dual-energy CT for differentiating intracerebral hemorrhage from iodinated contrast material staining. Radiology. 2010 Oct:257(1):205-11. doi: 10.1148/radiol.10091806. Epub 2010 Aug 2 [PubMed PMID: 20679449]
Level 2 (mid-level) evidenceHilkens NA, van Asch CJJ, Werring DJ, Wilson D, Rinkel GJE, Algra A, Velthuis BK, de Kort GAP, Witkamp TD, van Nieuwenhuizen KM, de Leeuw FE, Schonewille WJ, de Kort PLM, Dippel DWJ, Raaymakers TWM, Hofmeijer J, Wermer MJH, Kerkhoff H, Jellema K, Bronner IM, Remmers MJM, Bienfait HP, Witjes RJGM, Jäger HR, Greving JP, Klijn CJM, DIAGRAM study group. Predicting the presence of macrovascular causes in non-traumatic intracerebral haemorrhage: the DIAGRAM prediction score. Journal of neurology, neurosurgery, and psychiatry. 2018 Jul:89(7):674-679. doi: 10.1136/jnnp-2017-317262. Epub 2018 Jan 18 [PubMed PMID: 29348301]
van Asch CJ, Velthuis BK, Rinkel GJ, Algra A, de Kort GA, Witkamp TD, de Ridder JC, van Nieuwenhuizen KM, de Leeuw FE, Schonewille WJ, de Kort PL, Dippel DW, Raaymakers TW, Hofmeijer J, Wermer MJ, Kerkhoff H, Jellema K, Bronner IM, Remmers MJ, Bienfait HP, Witjes RJ, Greving JP, Klijn CJ, DIAGRAM Investigators. Diagnostic yield and accuracy of CT angiography, MR angiography, and digital subtraction angiography for detection of macrovascular causes of intracerebral haemorrhage: prospective, multicentre cohort study. BMJ (Clinical research ed.). 2015 Nov 9:351():h5762. doi: 10.1136/bmj.h5762. Epub 2015 Nov 9 [PubMed PMID: 26553142]
Steiner T, Purrucker JC, Aguiar de Sousa D, Apostolaki-Hansson T, Beck J, Christensen H, Cordonnier C, Downer MB, Eilertsen H, Gartly R, Gerner ST, Ho L, Holt Jahr S, Klijn CJ, Martinez-Majander N, Orav K, Petersson J, Raabe A, Sandset EC, Schreuder FH, Seiffge D, Al-Shahi Salman R. European Stroke Organisation (ESO) and European Association of Neurosurgical Societies (EANS) guideline on stroke due to spontaneous intracerebral haemorrhage. European stroke journal. 2025 Dec:10(4):1007-1086. doi: 10.1177/23969873251340815. Epub 2025 May 22 [PubMed PMID: 40401775]
Teo KC, Fong SM, Leung WCY, Leung IYH, Wong YK, Choi OMY, Yam KK, Lo RCN, Cheung RTF, Ho SL, Tsang ACO, Leung GKK, Chan KH, Lau KK. Location-Specific Hematoma Volume Cutoff and Clinical Outcomes in Intracerebral Hemorrhage. Stroke. 2023 Jun:54(6):1548-1557. doi: 10.1161/STROKEAHA.122.041246. Epub 2023 May 22 [PubMed PMID: 37216445]
Level 2 (mid-level) evidenceSingh SD, Schreuder FHBM, van Nieuwenhuizen KM, Jolink WM, Senff JR, Goldstein JN, Boogaarts J, Klijn CJM, Rinkel GJE, Brouwers HB. Secondary Hematoma Evacuation and Outcome After Initial Conservative Approach for Patients with Cerebellar Hematoma Larger than 3 cm. Neurocritical care. 2021 Dec:35(3):680-686. doi: 10.1007/s12028-021-01203-6. Epub 2021 Mar 2 [PubMed PMID: 33650011]
Anderson CS, Heeley E, Huang Y, Wang J, Stapf C, Delcourt C, Lindley R, Robinson T, Lavados P, Neal B, Hata J, Arima H, Parsons M, Li Y, Wang J, Heritier S, Li Q, Woodward M, Simes RJ, Davis SM, Chalmers J, INTERACT2 Investigators. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. The New England journal of medicine. 2013 Jun 20:368(25):2355-65. doi: 10.1056/NEJMoa1214609. Epub 2013 May 29 [PubMed PMID: 23713578]
Level 1 (high-level) evidenceArima H, Anderson CS, Wang JG, Huang Y, Heeley E, Neal B, Woodward M, Skulina C, Parsons MW, Peng B, Tao QL, Li YC, Jiang JD, Tai LW, Zhang JL, Xu E, Cheng Y, Morgenstern LB, Chalmers J, Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial Investigators. Lower treatment blood pressure is associated with greatest reduction in hematoma growth after acute intracerebral hemorrhage. Hypertension (Dallas, Tex. : 1979). 2010 Nov:56(5):852-8. doi: 10.1161/HYPERTENSIONAHA.110.154328. Epub 2010 Sep 7 [PubMed PMID: 20823381]
Level 1 (high-level) evidenceSchwarz S, Häfner K, Aschoff A, Schwab S. Incidence and prognostic significance of fever following intracerebral hemorrhage. Neurology. 2000 Jan 25:54(2):354-61 [PubMed PMID: 10668696]
Level 2 (mid-level) evidenceWu YT, Li TY, Lu SC, Chen LC, Chu HY, Chiang SL, Chang ST. Hyperglycemia as a predictor of poor outcome at discharge in patients with acute spontaneous cerebellar hemorrhage. Cerebellum (London, England). 2012 Jun:11(2):543-8. doi: 10.1007/s12311-011-0317-7. Epub [PubMed PMID: 21975857]
Level 2 (mid-level) evidenceKimura K, Iguchi Y, Inoue T, Shibazaki K, Matsumoto N, Kobayashi K, Yamashita S. Hyperglycemia independently increases the risk of early death in acute spontaneous intracerebral hemorrhage. Journal of the neurological sciences. 2007 Apr 15:255(1-2):90-4 [PubMed PMID: 17350046]
Godoy DA, Di Napoli M, Rabinstein AA. Treating hyperglycemia in neurocritical patients: benefits and perils. Neurocritical care. 2010 Dec:13(3):425-38. doi: 10.1007/s12028-010-9404-8. Epub [PubMed PMID: 20652767]
NICE-SUGAR Study Investigators, Finfer S, Chittock DR, Su SY, Blair D, Foster D, Dhingra V, Bellomo R, Cook D, Dodek P, Henderson WR, Hébert PC, Heritier S, Heyland DK, McArthur C, McDonald E, Mitchell I, Myburgh JA, Norton R, Potter J, Robinson BG, Ronco JJ. Intensive versus conventional glucose control in critically ill patients. The New England journal of medicine. 2009 Mar 26:360(13):1283-97. doi: 10.1056/NEJMoa0810625. Epub 2009 Mar 24 [PubMed PMID: 19318384]
Level 1 (high-level) evidenceNICE-SUGAR Study Investigators for the Australian and New Zealand Intensive Care Society Clinical Trials Group and the Canadian Critical Care Trials Group, Finfer S, Chittock D, Li Y, Foster D, Dhingra V, Bellomo R, Cook D, Dodek P, Hebert P, Henderson W, Heyland D, Higgins A, McArthur C, Mitchell I, Myburgh J, Robinson B, Ronco J. Intensive versus conventional glucose control in critically ill patients with traumatic brain injury: long-term follow-up of a subgroup of patients from the NICE-SUGAR study. Intensive care medicine. 2015 Jun:41(6):1037-47. doi: 10.1007/s00134-015-3757-6. Epub 2015 Jun 19 [PubMed PMID: 26088909]
Wijdicks EF, Sheth KN, Carter BS, Greer DM, Kasner SE, Kimberly WT, Schwab S, Smith EE, Tamargo RJ, Wintermark M, American Heart Association Stroke Council. Recommendations for the management of cerebral and cerebellar infarction with swelling: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014 Apr:45(4):1222-38. doi: 10.1161/01.str.0000441965.15164.d6. Epub 2014 Jan 30 [PubMed PMID: 24481970]
Siegal DM, Garcia DA, Crowther MA. How I treat target-specific oral anticoagulant-associated bleeding. Blood. 2014 Feb 20:123(8):1152-8. doi: 10.1182/blood-2013-09-529784. Epub 2014 Jan 2 [PubMed PMID: 24385535]
Pernod G, Albaladejo P, Godier A, Samama CM, Susen S, Gruel Y, Blais N, Fontana P, Cohen A, Llau JV, Rosencher N, Schved JF, de Maistre E, Samama MM, Mismetti P, Sié P, Working Group on Perioperative Haemostasis. Management of major bleeding complications and emergency surgery in patients on long-term treatment with direct oral anticoagulants, thrombin or factor-Xa inhibitors: proposals of the working group on perioperative haemostasis (GIHP) - March 2013. Archives of cardiovascular diseases. 2013 Jun-Jul:106(6-7):382-93. doi: 10.1016/j.acvd.2013.04.009. Epub 2013 Jun 25 [PubMed PMID: 23810130]
Zandieh A, Messé SR, Cucchiara B, Mullen MT, Kasner SE, VISTA-ICH Collaborators. Prophylactic Use of Antiepileptic Drugs in Patients with Spontaneous Intracerebral Hemorrhage. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association. 2016 Sep:25(9):2159-66. doi: 10.1016/j.jstrokecerebrovasdis.2016.05.026. Epub 2016 Jun 8 [PubMed PMID: 27289186]
Angriman F, Tirupakuzhi Vijayaraghavan BK, Dragoi L, Lopez Soto C, Chapman M, Scales DC. Antiepileptic Drugs to Prevent Seizures After Spontaneous Intracerebral Hemorrhage. Stroke. 2019 May:50(5):1095-1099. doi: 10.1161/STROKEAHA.118.024380. Epub [PubMed PMID: 30935318]
Hackenberg KA, Unterberg AW, Jung CS, Bösel J, Schönenberger S, Zweckberger K. Does suboccipital decompression and evacuation of intraparenchymal hematoma improve neurological outcome in patients with spontaneous cerebellar hemorrhage? Clinical neurology and neurosurgery. 2017 Apr:155():22-29. doi: 10.1016/j.clineuro.2017.01.019. Epub 2017 Feb 3 [PubMed PMID: 28226284]
Lobo K, Natali LD, Kotecki LBCDC, Santos CFNS, Filho FSMM, de Freitas MTO, da Silva VEB. Comparison of minimally invasive neuroendoscopic evacuation and conventional open surgery for spontaneous cerebellar hemorrhage: a systematic review and meta-analysis. Neurosurgical review. 2025 Feb 19:48(1):250. doi: 10.1007/s10143-025-03422-3. Epub 2025 Feb 19 [PubMed PMID: 39969621]
Level 1 (high-level) evidenceDammann P, Asgari S, Bassiouni H, Gasser T, Panagiotopoulos V, Gizewski ER, Stolke D, Sure U, Sandalcioglu IE. Spontaneous cerebellar hemorrhage--experience with 57 surgically treated patients and review of the literature. Neurosurgical review. 2011 Jan:34(1):77-86. doi: 10.1007/s10143-010-0279-0. Epub 2010 Aug 10 [PubMed PMID: 20697766]
Yanaka K, Meguro K, Fujita K, Narushima K, Nose T. Postoperative brainstem high intensity is correlated with poor outcomes for patients with spontaneous cerebellar hemorrhage. Neurosurgery. 1999 Dec:45(6):1323-7; discussion 1327-8 [PubMed PMID: 10598699]
Level 3 (low-level) evidenceOtt KH, Kase CS, Ojemann RG, Mohr JP. Cerebellar hemorrhage: diagnosis and treatment. A review of 56 cases. Archives of neurology. 1974 Sep:31(3):160-7 [PubMed PMID: 4546748]
Level 3 (low-level) evidenceSenff JR, Singh SD, Pasi M, Jolink WMT, Rodrigues MA, Schreuder FHBM, Staals J, Schreuder T, Douwes JPJ, Talsma J, McKaig BN, Kourkoulis C, Yechoor N, Anderson CD, Puy L, Cordonnier C, Wermer MJH, Rothwell PM, Rosand J, Klijn CJM, Al-Shahi Salman R, Rinkel GJE, Viswanathan A, Goldstein JN, Brouwers HB. Long-Term Outcomes in Patients With Spontaneous Cerebellar Hemorrhage: An International Cohort Study. Stroke. 2024 May:55(5):1210-1217. doi: 10.1161/STROKEAHA.123.044622. Epub 2024 Mar 15 [PubMed PMID: 38487876]
Hauer EM, Stark D, Staykov D, Steigleder T, Schwab S, Bardutzky J. Early continuous hypertonic saline infusion in patients with severe cerebrovascular disease. Critical care medicine. 2011 Jul:39(7):1766-72. doi: 10.1097/CCM.0b013e318218a390. Epub [PubMed PMID: 21494103]
Level 2 (mid-level) evidenceZiai WC, Toung TJ, Bhardwaj A. Hypertonic saline: first-line therapy for cerebral edema? Journal of the neurological sciences. 2007 Oct 15:261(1-2):157-66 [PubMed PMID: 17585941]
Videen TO, Zazulia AR, Manno EM, Derdeyn CP, Adams RE, Diringer MN, Powers WJ. Mannitol bolus preferentially shrinks non-infarcted brain in patients with ischemic stroke. Neurology. 2001 Dec 11:57(11):2120-2 [PubMed PMID: 11739839]
Diringer MN, Scalfani MT, Zazulia AR, Videen TO, Dhar R. Cerebral hemodynamic and metabolic effects of equi-osmolar doses mannitol and 23.4% saline in patients with edema following large ischemic stroke. Neurocritical care. 2011 Feb:14(1):11-7. doi: 10.1007/s12028-010-9465-8. Epub [PubMed PMID: 21042881]
Level 1 (high-level) evidenceYanaka K, Meguro K, Fujita K, Narushima K, Nose T. Immediate surgery reduces mortality in deeply comatose patients with spontaneous cerebellar hemorrhage. Neurologia medico-chirurgica. 2000 Jun:40(6):295-9; discussion 299-300 [PubMed PMID: 10892265]
Level 2 (mid-level) evidenceKobayashi S, Sato A, Kageyama Y, Nakamura H, Watanabe Y, Yamaura A. Treatment of hypertensive cerebellar hemorrhage--surgical or conservative management? Neurosurgery. 1994 Feb:34(2):246-50; discussion 250-1 [PubMed PMID: 8177384]
Level 2 (mid-level) evidenceTaneda M, Hayakawa T, Mogami H. Primary cerebellar hemorrhage. Quadrigeminal cistern obliteration on CT scans as a predictor of outcome. Journal of neurosurgery. 1987 Oct:67(4):545-52 [PubMed PMID: 3655893]
Luparello V, Canavero S. Treatment of hypertensive cerebellar hemorrhage--surgical or conservative management? Neurosurgery. 1995 Sep:37(3):552-3 [PubMed PMID: 7501127]
Level 3 (low-level) evidenceMezzadri JJ, Otero JM, Ottino CA. Management of 50 spontaneous cerebellar haemorrhages. Importance of obstructive hydrocephalus. Acta neurochirurgica. 1993:122(1-2):39-44 [PubMed PMID: 8333307]
Lee JH, Kim DW, Kang SD. Stereotactic burr hole aspiration surgery for spontaneous hypertensive cerebellar hemorrhage. Journal of cerebrovascular and endovascular neurosurgery. 2012 Sep:14(3):170-4. doi: 10.7461/jcen.2012.14.3.170. Epub 2012 Sep 28 [PubMed PMID: 23210043]