Introduction
Approximately 300,000 individuals in the United States live with spinal cord injury (SCI), with roughly 18,000 new cases reported annually.[1] Central cord syndrome (CCS), first described in 1954, represents the most common form of incomplete SCI and accounts for an estimated 11,000 new cases each year in the United States.[2][3] In contemporary clinical practice, CCS predominantly affects older adults with cervical stenosis following a low-energy fall or hyperextension injury. The syndrome produces motor deficits that are disproportionately greater in the upper extremities than the lower extremities, often accompanied by bladder dysfunction, typically retention, while preserving sacral sensation.[4][5][6] The distinctive clinical presentation of CCS has led to its inclusion in the differential diagnosis of "man in a barrel" syndrome.[7] The severity of neurological impairment varies and correlates with the extent of spinal cord injury and the degree of residual cord compression.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
CCS most commonly follows a hyperextension injury of the cervical spine that produces spinal cord impingement, often in a stenotic canal. The proposed mechanism of action is hyperextension resulting in anteriorly simultaneous compression of the spinal cord, either by bony spurs or intervertebral disc material, and posteriorly by the ligamentum flavum. In older adults, this usually reflects low-energy extension injury superimposed on cervical spondylosis or stenosis, whereas younger patients more often present after higher-energy trauma. This theory was aligned with early myelogram studies performed on cadavers.[8][9] Initially, Schneider et al postulated that spinal cord compression caused central hemorrhaging, resulting in adjacent white matter compression.[10]
Furthermore, Schneider believed that the upper limbs were more affected than the lower limbs because of the somatotropic organization of the lateral corticospinal tract, with arm function lying more medial within the tract. Neuroanatomic studies have since shown a diffuse distribution of upper- and lower-limb nerve fibers within the corticospinal tract, suggesting that the unique presentation of CCS may be due to the hand and upper limb being more densely represented in the lateral corticospinal tract.[3] More recent studies have revealed intact gray matter within the central canal, with no evidence of hemorrhage. Conversely, white matter axonal disruption, particularly in the lateral corticospinal tracts, appears to be the primary feature.[11]
Other less common causes include cervical spondylosis, atlantoaxial instability, tethered cord, osteoporosis, and spinal arthropathies.[12] The impairment of large fibers disrupts signal conduction and consequently results in motor and sensory problems, especially in the upper limbs and, to some extent, in the lower limbs. Overall, the amount of functional loss depends on the extent of spinal cord injury and ongoing compression.[13]
The boundary between CCS and degenerative cervical myelopathy is increasingly blurred. A patient with chronic gait imbalance or hand clumsiness may sustain a mild fall and then develop abrupt neurologic worsening that is labeled CCS, even though part of the examination reflects preexisting cord dysfunction. Recent authors have argued that many such cases are better understood as acute traumatic myelopathy in a stenotic but stable spine. Clinically, that framing is useful because it keeps attention on the actual combination of chronic compression, new trauma, residual stenosis, and neurologic trajectory.[14][15]
Epidemiology
A retrospective review by McKinley et al of 839 spinal cord injury patients at a tertiary care level 1 trauma center found CCS to be the most common clinical spinal cord syndrome.[16] CCS mostly affects males in a bimodal distribution (falls/motor vehicle collision in those who are young and hyperextension injury in older patients with likely underlying spinal disease, including osteoarthritis or cervical spondylosis).
In a Finnish prospective traumatic spinal cord injury cohort, the mean annual incidence was 36.6 per million, falls dominated in patients older than 60 years, and cervical injuries were especially common in that older group.[17] The United States epidemiologic data similarly describe CCS as increasingly associated with older age and falls.[18] The approximate annual incidence of CCS in the United States is 11,000 cases.[3]
Pathophysiology
CCS occurs most commonly in those who suffer a hyperextension injury. This usually happens with a forward fall, striking the chin and extending the neck backward at the time of the fall. Older patients generally have underlying cervical spondylosis. This leads to the cord being compressed posteriorly by the posterior ligamentum flavum or anteriorly by underlying spondylosis. These 2 contusion-type injuries to the cord can lead to clinical symptoms due to cord edema at the site of injury. It could also lead to bleeding into the cord at the injury site, which understandably has a worse prognosis.[19][20][21]
Usually, young patients often have a higher velocity of trauma, leading to cervical spine subluxation or fracture that leads to the above-described compression, contusion, and bleeding. The classic explanation held that CCS reflects a central gray matter lesion or a centrally located corticospinal tract injury that selectively damages upper extremity fibers. That model is now considered too simple. A 2002 clinical-pathologic analysis concluded that acute traumatic CCS could not be explained by isolated gray matter injury at the hand motor neuron level.[22] More recent conceptual work has shown that the classic somatotopic explanation rests on a weak anatomic premise and that many cases likely reflect more diffuse corticospinal and interneuronal dysfunction within a compressed, edematous cervical cord.[15]
History and Physical
Clinical History
The history should establish the mechanism, the preinjury neurological condition, and the neurologic time course. A ground-level fall with head strike in an older adult with prior neck stiffness, hand numbness, gait imbalance, or reduced manual dexterity strongly suggests extension injury in a stenotic canal. A high-speed collision, diving injury, or fall from height raises suspicion for fracture, translation, or traumatic disc herniation. Neck pain at the site of spinal cord impingement is common. Immediate hand weakness, burning dysesthesias in the shoulders or forearms, and early urinary retention support a cervical cord process. A history of progressive imbalance or hand clumsiness before the trauma suggests preexisting degenerative cervical myelopathy that has been unmasked or worsened by the injury.[23]
The signature examination finding is disproportionate upper-extremity weakness, usually maximal in the distal hand muscles. Shoulder and elbow strength may be less impaired than grip, finger flexion, and finger abduction. Sensory symptoms are variable, and bladder dysfunction is supportive but not necessary for the diagnosis. The most common sensory deficits are in a "cape-like" distribution across their upper back and down their posterior upper extremities. In an expert consensus study, most clinicians regarded greater upper than lower-extremity impairment as the core descriptor of CCS, while sensory loss and bladder dysfunction were considered less consistent accompanying features. For research purposes, many experts recommend a difference of at least 10 motor points in favor of the lower extremities. That threshold improves reproducibility, but it should not override bedside judgment when the clinical pattern is otherwise convincing.[24][23]
Physical Examination
Serial examinations are essential in the evaluation of CCS. Improvement over the first hours suggests reversible edema or transient cord deformation. Plateau, progression, or new urinary retention implies ongoing compression or expanding secondary injury and should lower the threshold for urgent magnetic resonance imaging and surgical consultation. The examiner must also look for confounders, eg, shoulder trauma, brachial plexus injury, pain-limited effort, intoxication, or traumatic brain injury. Reflexes may be absent early because spinal shock can suppress long-tract signs. A careful preinjury functional history adds prognostic value because many patients recover gait before they recover hand speed and self-care.
Bladder dysfunction (most commonly urinary retention) and priapism can also be signs of upper motor neuron dysfunction. The sacral sensation is usually preserved, but the clinician should assess the rectal tone to evaluate the severity of the compression.[25] Finally, clinicians must also assess for pressure injuries to the skin, neurogenic bowel and bladder, spasticity, autonomic dysreflexia, and temperature dysregulation.
Evaluation
International Standards Evaluation
Evaluation begins with standard trauma resuscitation and cervical immobilization, but the neurologic deficit must be characterized early because treatment windows are time-sensitive. Hypoxia and hypotension worsen secondary cord injury, so oxygenation, ventilation, and perfusion require the same priority as fracture identification. Once the patient is resuscitated, the clinician should perform and document a structured International Standards examination, including sacral testing, upper- and lower-extremity motor scores, and the American Spinal Injury Association Impairment Scale grade.[26] This establishes whether the patient has a motor incomplete injury and whether the phenotype is severe enough to indicate early surgical decompression, especially in AIS C presentations.[27]
Computed Tomography
Computed tomography (CT) is the first-line imaging study for acute cervical trauma because it rapidly identifies fractures, malalignment, locked facets, translational injury, and most clinically relevant osseous instability. The updated American College of Radiology criteria continue to support CT over radiographs for the initial assessment of suspected spine trauma. In practice, a patient with objective cervical myelopathy after trauma should undergo high-quality cervical CT immediately, even if the external trauma seems minor. A normal CT scan does not exclude CCS, but an abnormal scan can immediately reclassify the patient from a stable stenosis phenotype to an unstable traumatic reconstruction problem.[28][29]
When CT shows a subaxial injury, the radiologic description should be translated into a structured cervical trauma language because that changes operative urgency and approach. The Subaxial Injury Classification system formalizes injury morphology, neurologic status, and the integrity of the disc-ligamentous complex.[30] The AO Spine subaxial system similarly captures morphology, facet injury, neurologic status, and modifiers.[31] In CCS, these frameworks are most useful when the clinical syndrome coexists with fracture, translation, or suspected ligamentous instability.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) provides the anatomic detail of soft tissues that CT cannot. The 2017 acute spinal cord injury guideline recommends MRI before surgery, when feasible, to improve clinical decision-making, and also recommends it during the acute period, before or after surgery, to improve neurologic prognostication. Those recommendations are highly relevant in CCS because many patients have no fracture yet do have surgically meaningful ventral disc material, dorsal buckling, epidural hematoma, or multilevel stenosis with persistent cord compression.[32]
In clinical practice, early MRI is indicated when a patient has a convincing cervical cord examination and either no explanatory lesion on CT or persistent uncertainty about the degree and source of compression. MRI is also indicated when surgery is being considered, because the operative plan depends on whether compression is ventral, dorsal, focal, multilevel, unilateral, or circumferential. MRI is especially valuable for detecting acute disc herniation, epidural hematoma, ligamentous disruption, and noncontiguous compressive levels that would change the choice between anterior, posterior, and combined decompression.
CCS often presents as a spinal cord injury without a fracture on CT. In this setting, MRI determines whether the deficit reflects edema alone or a persistent compressive target, eg, a traumatic disc, epidural hematoma, or severe multilevel stenosis. Because the baseline MRI study also informs prognosis and operative planning, it should be obtained early, whenever the patient has an unexplained abnormal cervical cord examination and is stable enough for transport.[32][23]
The MRI findings that matter most in CCS are those that identify persistent compression and those that predict recovery. T2 hyperintensity marks edema or contusion and is common. Greater lesion length, more severe maximum canal compromise, more severe maximum spinal cord compression, and smaller midsagittal canal diameter correlate with worse neurologic and functional recovery. In a surgical cohort of CCS caused by spinal stenosis, long-term outcome was associated with admission American Spinal Injury Association motor score, midsagittal diameter, maximum canal compromise, and T2 lesion length.[33] Axial MRI grading also sharpens risk stratification. The Brain and Spinal Injury Center score, usually abbreviated BASIC, is an axial T2 severity scale that captures the transverse extent of cord signal abnormality and aids prognostication.[34]
The Central Cord Score
Efforts to standardize CCS evaluation are accelerating. The Central Cord Score integrates distal upper-extremity motor function, upper-extremity sensation, ambulation, urinary retention, and MRI signal change.[35] More recent comparative work has evaluated the Acute Traumatic Central Cord Syndrome Severity Score and other CCS-oriented systems for their ability to guide surgical timing. In a 2025 validation study, the Acute Traumatic Central Cord Syndrome Severity Score performed best for early surgical decision-making, but the available scores did not predict neurologic or functional recovery well enough for stand-alone use.[36] At present, these tools are best viewed as adjuncts for communication, not as replacements for clinical judgment.
Additional Diagnostic Studies
No laboratory test confirms CCS. Laboratory studies support resuscitation and prepare the patient for surgery or vasopressor therapy. In most patients with acute traumatic cervical myelopathy, the baseline panel should include complete blood count, electrolytes, creatinine, coagulation studies, and type and screen when operative intervention is plausible. Older adults and patients with cardiac symptoms may also need electrocardiography and troponin testing before prolonged vasopressor support or urgent anesthesia. Urinalysis is useful when urinary retention, catheter dependence, fever, or delirium raises concern for urinary tract infection. Additional testing should be individualized to the trauma burden, anticoagulant exposure, and comorbidity profile.
Treatment / Management
Prehospital Management
Management of spinal cord injuries begins at the scene of the injury with a primary survey involving the airway, breathing, circulation, and disability (ABCD). Disability includes calculating the Glasgow Coma Scale (GCS), performing a pupil examination, and identifying any lateralizing signs. This should be repeated as often as necessary whenever the patient's status changes. Next, a secondary survey should be performed, involving a focused examination of the patient, including a spinal examination (3-person logroll to assess and palpate the spine), assessment of distal motor function in both upper and lower limbs, incontinence, and skin appearance. Lastly, clinicians in the field should collect as much patient history as possible, noting any subjective complaints of neck pain. Restricting spinal motion is of the utmost importance in patients with suspected spinal cord injuries.[37]
Hospital Management
Any backboards should be removed as soon as possible to reduce the occurrence of pressure ulcers. All patients with concerns for spinal cord injury should have a thorough trauma evaluation performed in the emergency department. These patients should have cervical immobilization maintained during the initial evaluation.
In the immediate period following a spinal cord injury, clinicians should pay particular attention to optimizing tissue perfusion to the penumbra to reduce secondary injury. Hemodynamic stability and mitigation of the meta-inflammatory response are the primary initial focus.[3][38] Contemporary hemodynamic guidance suggests maintaining mean arterial pressure between 75 and 80 mm Hg, not exceeding 90 to 95 mm Hg, for 3 to 7 days after acute traumatic spinal cord injury.[39] The evidence is very low, but this recommendation is clinically relevant in CCS because many patients are older, stenotic, and poorly tolerant of even modest hypotension. The upper bound also matters because vasopressor-related complications increase as pressure targets rise without clear neurologic gain.[40](A1)
The use of corticosteroids in spinal cord injury has a long history of controversy. The goal of intravenous (IV) methylprednisolone therapy is to halt the inflammatory cascade that results in secondary spinal cord injury. The landmark Second National Spinal Cord Injury Study (NASCIS-II) did show statistically significant neurological benefits with the administration of IV methylprednisolone if given within 8 hours of initial injury; however, an increased risk of adverse events was also noted. Therefore, the Congress of Neurological Surgeons recommends against IV methylprednisolone administration.[41] On the other hand, in 2016, AO Spine published a position statement recommending a 24-hour IV infusion of methylprednisolone within 8 hours of injury, but not offering infusion to patients who present more than 8 hours after the initial injury. Additionally, AO Spine does not recommend a 48-hour infusion of methylprednisolone.[42] From a practical standpoint, in older CCS patients with diabetes, frailty, or infection risk, the downside often outweighs the uncertain neurologic benefit.(A1)
Conservative management should only be considered in situations without fracture, dislocation, disc herniation, or spinal instability; otherwise, surgical intervention is preferred.[3] Conservative management includes physical and occupational therapy in addition to standard medical care for sequelae of CCS.(B3)
The more controversial case is the patient with cervical stenosis, no fracture or spinal instability, and an incomplete neurologic syndrome consistent with CCS. The 2017 guideline suggests that early surgery within 24 hours be considered in adult traumatic CCS when there is radiologic cord compression and no radiologic mechanical instability.[43] The 2025 AO Spine recommendations go further and issue a strong recommendation to consider early surgery within 24 hours in AIS grade C CCS.[27] (A1)
The evidence supporting that recommendation is strongest for more severe motor-incomplete injuries. In a propensity-matched cohort of 186 CCS patients, decompression within 24 hours improved upper-extremity motor recovery at 1 year, and the effect was larger in AIS C injuries, with overall motor recovery improving by 9.5 points.[44] A 2024 meta-analysis of 13 studies and 8424 patients also demonstrated better motor recovery and fewer complications with early surgery, without an increased mortality risk.[45] Uncertainty remains for milder phenotypes. Clinically, this means that an improving AIS D patient with stable anatomy can be observed briefly, but an AIS C patient, or any patient with persistent major compression or worsening examination, should be pushed toward early decompression. Shared decision-making is especially important in older adults with severe stenosis and borderline deficits. (A1)
Venous thromboembolism prevention should start early once bleeding risk allows. The acute spinal cord injury guideline suggests routine anticoagulant thromboprophylaxis and supports low-molecular-weight heparin or fixed low-dose unfractionated heparin, while avoiding adjusted-dose heparin. Initiation within 72 hours, when safe, reduces the risk of thromboembolic complications.[46] Pulmonary hygiene, pressure injury prevention, bowel and bladder protocols, and early mobilization are equally important.(A1)
Surgical Approach
At this time, no guidelines have been established for the surgical approach, and the most appropriate course of intervention to optimize outcomes and reduce complications remains at the surgeon's discretion. An anterior approach is favored when compression is focal and ventral, particularly in cases of acute disc herniation, retropulsed body fragments, or limited-level spondylotic bars. Anterior cervical discectomy and fusion is commonly used for 1- or 2-level ventral lesions. Corpectomy is useful when compression is retrovertebral or too extensive for discectomy alone.
A posterior approach is preferred for multilevel dorsal or circumferential stenosis when cervical alignment permits posterior cord drift after decompression, or when stabilization is required across several levels. Laminectomy with fusion is the usual reconstructive option in acute trauma. Laminoplasty can be considered in selected multilevel stenosis cases without meaningful instability, though its role in acute trauma is narrower than in elective myelopathy practice.[23]
Combined anterior-posterior surgery is reserved for injuries in which 1 corridor cannot achieve adequate decompression and stability, eg, major translation, circumferential compression, or severe deformity. The recent AO Spine acute spinal cord injury recommendations also conditionally support laminectomy with or without anterior surgery when circumferential decompression is required and suggest intraoperative ultrasound when the adequacy of decompression is uncertain.[27]
Differential Diagnosis
When evaluating patients with CCS, conditions that closely mimic CCS should be ruled out, including cruciate paralysis and the avulsion of cervical roots. Cruciate paralysis is a rare neurological disease involving the cervicomedullary junction. The main precipitating factors of cruciate paralysis are mechanical trauma, metabolic disorders, or postsurgical complications. Typically, the patient with cruciate paralysis presents with bilateral upper extremity paresis while sparing the lower extremities in most cases.[47][48] Besides other features, the main differentiating feature in cruciate paralysis is that it affects the selective descending fibers of the corticospinal tract, as these fibers decussate at the cervicomedullary junction.[49]
A cervical root avulsion is a severe form of nerve root injury that usually results from high-energy trauma to the neck or ipsilateral arm. Neurological deficits from nerve avulsion range from a mild motor function deficit to complete paralysis that requires surgical correction.[50][51]
The most important differential diagnosis is acute worsening of degenerative cervical myelopathy. Many older patients labeled with CCS had preexisting cervical cord compression and some degree of chronic hand or gait dysfunction before the trauma. The fall acts as the decompensating event, but the examination may reflect both chronic and acute disease. This distinction matters because residual postoperative limitation may partly represent longstanding myelopathy. Other incomplete spinal cord syndromes must also be separated (see Image. Spinal Cord Syndromes). Anterior cord syndrome produces severe motor loss and pain-temperature impairment with preserved dorsal column function. Brown-Séquard syndrome produces marked asymmetry with ipsilateral weakness and dorsal column loss. CCS differs by its bilateral arm-predominant weakness and frequent hand-selective disability.
Bilateral brachial plexus traction injury, bilateral shoulder trauma, cervical radiculopathy, and peripheral nerve palsies can all create apparent arm-predominant weakness after trauma. Spinal epidural hematoma, inflammatory myelitis, demyelinating disease, and spinal cord infarction should also remain in view when the mechanism is atypical or the imaging does not match the clinical pattern.
Prognosis
CCS carries a more favorable overall prognosis than complete cervical spinal cord injury, but a favorable prognosis does not imply full recovery. Ambulation and bladder function often improve substantially, particularly in younger patients.[52] By contrast, deficits in hand dexterity, neuropathic pain, and loss of self-care independence frequently persist as the principal long-term sequelae of CCS.[53] In inpatient rehabilitation cohorts, motor scores, activities of daily living measures, and bladder continence improved, although residual spasticity and sensory symptoms remained common.[54]
Age and baseline neurologic severity are the most consistent predictors of outcome. Older natural history and rehabilitation series consistently found better functional recovery in younger patients.[52][55] Higher American Spinal Injury Association (ASIA) motor scores at admission and better initial ASIA Impairment Scale (AIS) grades also predict superior motor and functional recovery.[33] In surgically treated CCS due to spinal stenosis, admission ASIA motor score, age, midsagittal diameter, maximum canal compromise, and lesion length predicted long-term outcome.[33] In more recent series of CCS without fracture-dislocation, age, intrinsic hand muscle strength, degree of cord and canal compression, T2 hyperintensity length, and admission motor score also identified patients with greater recovery potential.[56] Younger age, earlier surgery, and a better preoperative AIS grade were also associated with a better prognosis in patients with multilevel stenosis without fracture-dislocation.[57]
MRI further refines prognostication. Shorter intramedullary lesion length, less canal compromise, and lower Brain and Spinal Injury Center (BASIC) severity grades are associated with better recovery.[58] Specifically, an ASIA motor score on admission greater than 61 predicted favorable recovery, whereas cervical stenosis length greater than 3.9 cm and a BASIC score greater than 1 identified a subgroup with poor recovery.[58] These imaging markers should calibrate expectations, not be used in isolation to deny treatment. Even when imaging is unfavorable, decisions about decompression remain clinical and should account for persistent cord compression and the functional significance of the deficit.
Surgical timing influences outcome, although not uniformly across subgroups. The clearest contemporary signal is that early decompression improves upper-extremity recovery overall and total motor recovery in patients with AIS grade C CCS.[44][27] Meta-analyses also suggest lower complication rates with earlier surgery.[59][45] In patients with AIS grade D injury, early and late surgery yielded comparable long-term outcomes, suggesting that timing may matter less for the eventual neurologic endpoint in milder cases.[44] Prognosis is therefore best framed by subgroup: in severe motor-incomplete CCS with persistent compression, early surgery may raise the recovery ceiling. In mild, improving CCS, surgery may affect the pace and reliability of recovery more than the eventual neurologic endpoint.
Recovery of walking does not ensure recovery of self-care. In a multicenter matched analysis, patients with CCS had persistently worse self-care outcomes than patients with other incomplete cervical spinal cord injuries.[53] In a surgical prognostic series, manual dexterity at 1 year reached only 64.4% of baseline.[33]These findings should be stated plainly during counseling, because persistent dissatisfaction after CCS more often reflects residual hand disability than failure to regain ambulation.
Recent studies suggest that prognostication may improve, but not through any single score. CCS-specific severity instruments, including the Central Cord Score and Acute Traumatic Central Cord Syndrome Score, may help stratify severity and inform decisions about surgery and surgical timing.[36] However, current scoring systems do not yet predict long-term motor and functional recovery with sufficient accuracy to replace serial neurologic examination and MRI. For now, prognosis is best estimated by integrating age, initial AIS grade, admission motor score, hand strength, residual compression, lesion length, and the early neurologic trajectory.
Complications
Patients with CCS are at risk for a multitude of complications, like other spinal cord injuries.
Pulmonary Complications
Respiratory complications are the most common cause of morbidity and mortality in patients with spinal cord injuries.[60] Patients with cervical spinal cord injury are most at risk due to impaired respiratory drive, especially above the C5 vertebral level, due to diaphragmatic impairment. Common complications include acute respiratory failure, pneumonia, pleural effusion, pneumothorax, pulmonary embolism, and mucus plug.[60]
Cardiovascular Complications
Cardiovascular complications arise largely due to impaired autonomic function.[61] CCS patients should be at lower risk of common cardiovascular complications due to the retained ability of lower limb function and usually of ambulation. However, patients with decreased lower limb function are at higher risk for low baseline blood pressure, orthostatic hypotension, and venous thromboembolism.[62][63]
Low baseline blood pressures in acute injury are managed with fluid resuscitation. Orthostatic hypotension can be managed both with and without medications. Nonpharmacologic strategies include reducing rapid changes in posture, avoiding hot environments, and eating smaller meals to reduce postprandial cardiovascular shunting to gastrointestinal organs.[64][65] Pharmacologic options for orthostatic hypotension include fludrocortisone, ephedrine, and midodrine; however, only midodrine is approved by the Food and Drug Administration (FDA) for treating neurogenic orthostatic hypotension.[64][66][67][68]
Furthermore, venous thromboembolism (VTE) is a significant problem in spinal cord injury patients. Due to the nature of CCS, patients are less likely to develop VTE. The incidence of VTE in spinal cord patients ranges from 12% to 100%. While most commonly occurring in the lower limbs, VTE can also occur in the upper limbs.[69] The Consortium of Spinal Medicine recommends VTE prophylaxis for a minimum of 8 weeks after injury and prefers low-molecular-weight heparin (LMWH) over other anticoagulant medications. However, research is needed on the safety and efficacy of direct oral anticoagulants.[63][46] Currently, low-dose subcutaneous heparin and vitamin K antagonists are not recommended therapies.[63]
Patients with CCS are usually prone to autonomic dysreflexia, a potentially life-threatening emergency that is more common in patients with spinal cord injury above the T6 level. Autonomic dysreflexia is an uncoordinated response of the autonomic nervous system involving the heart and blood vessels. This phenomenon usually occurs in the first month of the injury. Common clinical presentations include headaches, flushing, piloerection, increased blood pressure, anxiety, and nausea.[70] These symptoms are usually episodic and are managed conservatively. The initial management strategy is prevention through education of patients, caregivers, and hospital staff about the potential for autonomic dysreflexia and its warning signs. During an acute episode, management should begin by placing the patient upright, removing all tight clothing, and eliminating noxious stimuli such as skin pressure, urinary catheter dysfunction, and bowel impaction. A survey for noxious stimuli should be repeated until the patient’s autonomic dysreflexia episode has subsided.[71]
Blood pressure monitoring may be required in selective cases for the long term, even if the patient is not diagnosed as hypertensive. For blood pressure control, nitrates, hydralazine, and labetalol are used, but prescribers should avoid giving nitrates to patients taking sildenafil.[72] Lastly, Readdy et al showed that cardiogenic complications appeared in 68% of patients with no relation to conservative management, surgical management, or surgical timing. Furthermore, they noted that in patients 55 years or older, a significant increase in complications occurred with dopamine compared to phenylephrine (83% versus 50%, respectively).[72] The utmost priority in managing cardiometabolic syndrome is essential.[73]
Neuropathic Pain
Patients with CCS can develop neuropathic pain at the level of the injury and below the level of injury. Neuropathic pain can be caused by damage to either the spinal cord or nerve roots. Neuropathic pain is typically described as “hot,” burning,” tingling,” “pins and needles,” “sharp,” “shooting,” or “electric.”[74] First-line treatment for neuropathic pain in spinal cord injury is gabapentinoids (gabapentin and pregabalin) and tricyclic antidepressants (TCA), with additional consideration for selective serotonin reuptake inhibitors (SSRI) and serotonin and norepinephrine reuptake inhibitors (SNRI).[75][76] Guidelines published by the CanPainSCI Working Group recommended tramadol as a second-line medication.[77][78] Lamotrigine was considered a second-line medication, specifically in patients with incomplete spinal cord injury. Additional interventions to consider are visual illusion therapy, transcranial direct current stimulation, and physical and occupational therapy.[77] Methylprednisolone has been advocated for acute neuropathic pain with allodynia.[79]
Spasticity
Spasticity can be defined as “disordered sensory-motor control resulting from an upper motor neuron lesion, presenting as intermittent or sustained involuntary activation of muscles,” and is a significant problem in spinal cord injury patients.[80][81] A systematic review by Bovend’Erdt et al found inconclusive evidence of the beneficial effects of stretching on spasticity.[82] Physical modalities, eg, cryotherapy and heat therapy (both superficial and deep), provide only short-term effects on spasticity.[83] Neuromuscular stimulation and functional electrical stimulation have shown positive results in reducing spasticity.[84] Transcranial and spinal cord magnetic stimulation has been proposed, but more research is required.[85]
Common oral pharmacologic options include gamma-aminobutyric acid (GABA) agonists baclofen, gabapentinoids, and benzodiazepines, alpha-2-adrenergic agonists tizanidine and clonidine, and peripherally acting dantrolene.[86] Alternative medications that are not FDA-approved include cyproheptadine, cannabinoids, and 4-aminopyridine.[87][88][89]
In patients with minimal response to oral medications or with contraindications to oral medications, chemodenervation with botulinum toxin or chemolysis with alcohol are alternative interventions.[90][91] Boviatsis et al. found that intrathecal baclofen pumps improved functional improvement and reduced pain in spinal cord injury and multiple sclerosis.[92] Surgical interventions for spasticity refractory to conservative management include tendon lengthening, tendon transfers, neurotomy, and selective rhizotomy.[93][94] Spinal cord stimulators have shown promising results in the past, but current clinical trials are needed to provide data on their safety and efficacy, given advances in technology and in the understanding of spasticity pathophysiology.[95]
Chronic Pain, Spasticity, and Autonomic Dysreflexia have been postulated to result from the loss of descending serotonergic fibers. Therefore bolstering 5-HT function and ionic plasticity may provide therapeutic benefits.[96][97]
Genitourinary
Neurogenic bladder is another prevalent condition among patients with CCS. In CCS, the sensation of bladder fullness, bladder sphincter function, and bladder motor control are impaired. Patients experience urgency, spasms, and frequency, along with urine incontinence.[98] A Foley catheter is used for this purpose, and the majority of the patients regain bladder function. Patients who require long-term catheterization either use a clean intermittent catheter or an indwelling catheter. A clean intermittent catheter is preferred over an indwelling catheter because the infection rate is much higher with an indwelling catheter.[25]
Pressure Injury
Pressure ulcers result from tissue damage that typically occurs at bony prominences. Approximately one-third of the patients with CCS have multiple pressure ulcers. Pressure ulcers are usually managed by avoiding immobility, regularly examining prone areas, applying an emollient to areas exposed to friction, using cushions, and maintaining adequate weight and nutrition.[99]
Postoperative and Rehabilitation Care
Currently, no studies have compared CCS patients who received acute inpatient rehabilitative services with those who did not. CCS patients should receive occupational and physical therapy after discharge from acute care facilities. While each rehabilitation program should be tailored specifically to the patient and their functional goals, some generalizations can be made. Physical therapy focuses on maintaining an adequate range of motion, increasing strength, and fine-tuning coordination of the lower limbs and trunk to improve ambulation (with or without assistive devices), transfers, and balance.[3][100]
Interventions include stretching, therapeutic exercise, aerobic conditioning, stair and transfer training, gait training, functional electrical stimulation, and aquatic therapy. Since upper-limb strength and function are more affected than lower-limb function in CCS, occupational therapy should focus on hand strength and dexterity to maximize patient function in activities of daily living (ADLs), eg, feeding, dressing, bathing, and self-hygiene.[43][100] Splinting may be used outside therapy to prevent contracture development.[25]
Deterrence and Patient Education
Patients with CCS are challenged not only physically but also psychologically. Effective communication between interprofessional teams, including neurologists, internists, neurosurgeons, psychiatrists, physiatrists, physical and occupational therapists, and nurses, can lead to better outcomes. These patients are prone to depression and suicidal ideation. Furthermore, the lack of motivation can delay the treatment progress and may lead to permanent disability.
The following strategies can assist in achieving better recovery:
- Close routine follow-up with the neurologist, physiatrist, or internist
- Patient education on clean intermittent catheterization to reduce the risk of urinary tract infections and secondary complications
- Avoidance of immobility and regular change of position after 2 to 4 hours
- Close follow-up with a physical therapist for muscle and core-strengthening exercises to prevent muscle atrophy
- Blood pressure monitoring at home
- Close follow-up with the psychiatrist to look for signs of depression and suicidal ideation
Pearls and Other Issues
CCS patients usually require extensive physical therapy for significant neurologic recovery. These patients may develop chronic issues, including autonomic dysregulation with uncontrolled blood pressure, neurogenic bladder requiring catheterization, pressure ulcers, neuropathic pain, and spasticity with chronic pain issues. Autonomic dysreflexia should be initially managed by positioning the patient upright, loosening tight clothing, and removing any noxious stimuli. Hypertension due to autonomic dysreflexia may be managed with nifedipine or transdermal nitroglycerin if conservative measures do not resolve the autonomic dysreflexia.
Patients with neurogenic bladder may require intermittent self-catheterization but will remain at risk for iatrogenic bladder infections. The majority of patients will regain bladder function within 6 to 8 months. Neuropathic pain and spasticity are common. First-line medications for neuropathic pain are gabapentinoids and TCAs. Other considerations include SSRIs and SNRIs, transcranial electrical stimulation, and physiotherapy. Spasticity should be managed with a regular stretching program and antispasmodic medications. Baclofen is the hallmark of spasticity management. Patients may require additional medicinal therapy in consultation with a pain specialist or neurologist for their neuropathic pain and spasticity. Also, clinicians should consider chemodenervation with botulinum toxin or alcohol injections. Lastly, baclofen pumps can also be implanted.
Enhancing Healthcare Team Outcomes
CCS is the most common form of spinal cord injury, frequently affecting older adults with preexisting cervical stenosis after low-energy hyperextension injuries. The pathophysiology involves axonal disruption of the white matter within the lateral corticospinal tracts, often exacerbated by cord compression from spondylotic changes, ligamentous hypertrophy, or acute disc herniation. Clinically, patients present with disproportionate upper-extremity weakness, variable sensory deficits, and possible bladder dysfunction with sacral sparing. Severity depends on the extent of cord injury and the degree of residual compression. Evaluation requires careful neurologic assessment, serial examinations, and timely imaging, including computed tomography for bony assessment and magnetic resonance imaging for soft-tissue and cord characterization. Early recognition and risk stratification guide decisions regarding conservative management, hemodynamic optimization, and urgent surgical decompression in patients with persistent or severe deficits. Secondary complications, including neuropathic pain, spasticity, autonomic dysreflexia, and pressure injuries, require proactive monitoring and intervention.
Interprofessional collaboration enhances patient-centered outcomes by integrating expertise across the care team. Physicians and advanced practice providers lead diagnosis, surgical decision-making, and ongoing neurologic assessment. Nurses perform continuous monitoring, assist with mobility, prevent pressure injuries, and provide patient education on bladder and bowel management and spasticity management. Pharmacists optimize medication regimens for neuropathic pain, spasticity, and thromboprophylaxis while monitoring for adverse effects. Physical and occupational therapists develop individualized rehabilitation plans to restore function and independence. Effective communication among team members supports timely referrals, shared decision-making with patients and families, and coordinated discharge planning. This collaborative approach reduces preventable complications, ensures evidence-based interventions, and promotes functional recovery, safety, and long-term quality of care.
Media
(Click Image to Enlarge)
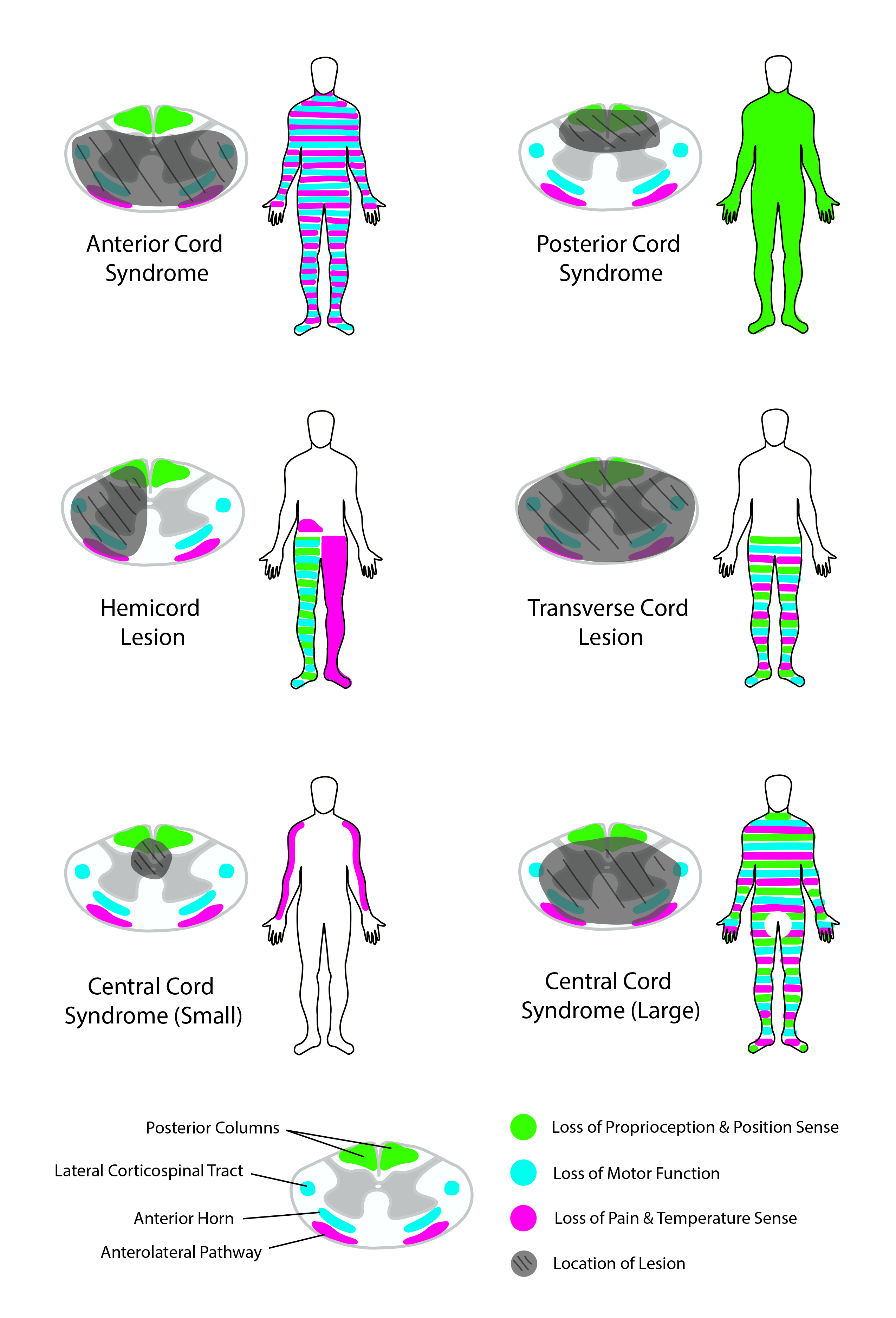
Spinal Cord Syndromes. This image details common spinal cord syndromes and the neurological deficits they may cause.
Contributed by R Kabir, MD
References
Lo J, Chan L, Flynn S. A Systematic Review of the Incidence, Prevalence, Costs, and Activity and Work Limitations of Amputation, Osteoarthritis, Rheumatoid Arthritis, Back Pain, Multiple Sclerosis, Spinal Cord Injury, Stroke, and Traumatic Brain Injury in the United States: A 2019 Update. Archives of physical medicine and rehabilitation. 2021 Jan:102(1):115-131. doi: 10.1016/j.apmr.2020.04.001. Epub 2020 Apr 24 [PubMed PMID: 32339483]
Level 1 (high-level) evidenceBrooks NP. Central Cord Syndrome. Neurosurgery clinics of North America. 2017 Jan:28(1):41-47. doi: 10.1016/j.nec.2016.08.002. Epub 2016 Nov 1 [PubMed PMID: 27886881]
Divi SN, Schroeder GD, Mangan JJ, Tadley M, Ramey WL, Badhiwala JH, Fehlings MG, Oner FC, Kandziora F, Benneker LM, Vialle EN, Rajasekaran S, Chapman JR, Vaccaro AR. Management of Acute Traumatic Central Cord Syndrome: A Narrative Review. Global spine journal. 2019 May:9(1 Suppl):89S-97S. doi: 10.1177/2192568219830943. Epub 2019 May 8 [PubMed PMID: 31157150]
Level 3 (low-level) evidenceKhorasanizadeh M, Yousefifard M, Eskian M, Lu Y, Chalangari M, Harrop JS, Jazayeri SB, Seyedpour S, Khodaei B, Hosseini M, Rahimi-Movaghar V. Neurological recovery following traumatic spinal cord injury: a systematic review and meta-analysis. Journal of neurosurgery. Spine. 2019 May 1:30(5):683-699. doi: 10.3171/2018.10.SPINE18802. Epub 2019 Feb 15 [PubMed PMID: 30771786]
Level 1 (high-level) evidenceEmos MC, Agarwal S. Neuroanatomy, Upper Motor Neuron Lesion. StatPearls. 2026 Jan:(): [PubMed PMID: 30725990]
Dimova V, Birklein F. [Complex regional pain syndrome (CRPS) : An update]. Der Anaesthesist. 2019 Feb:68(2):115-128. doi: 10.1007/s00101-019-0539-5. Epub [PubMed PMID: 30719529]
Butterfield MC, DeBlieux P, Palacios E. Man in a barrel: acute central cord syndrome after minor injury. The Journal of emergency medicine. 2015 Mar:48(3):333-4. doi: 10.1016/j.jemermed.2014.10.024. Epub 2014 Dec 17 [PubMed PMID: 25534252]
Level 3 (low-level) evidenceSCHNEIDER RC, THOMPSON JM, BEBIN J. The syndrome of acute central cervical spinal cord injury. Journal of neurology, neurosurgery, and psychiatry. 1958 Aug:21(3):216-27 [PubMed PMID: 13576174]
TAYLOR AR. The mechanism of injury to the spinal cord in the neck without damage to vertebral column. The Journal of bone and joint surgery. British volume. 1951 Nov:33-B(4):543-7 [PubMed PMID: 14880573]
SCHNEIDER RC, CHERRY G, PANTEK H. The syndrome of acute central cervical spinal cord injury; with special reference to the mechanisms involved in hyperextension injuries of cervical spine. Journal of neurosurgery. 1954 Nov:11(6):546-77 [PubMed PMID: 13222164]
Quencer RM, Bunge RP, Egnor M, Green BA, Puckett W, Naidich TP, Post MJ, Norenberg M. Acute traumatic central cord syndrome: MRI-pathological correlations. Neuroradiology. 1992:34(2):85-94 [PubMed PMID: 1603319]
Dydyk AM, Chiebuka E, Stretanski MF, Givler A. Central Pain Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 31971703]
Arul K, Ge L, Ikpeze T, Baldwin A, Mesfin A. Traumatic spinal cord injuries in geriatric population: etiology, management, and complications. Journal of spine surgery (Hong Kong). 2019 Mar:5(1):38-45. doi: 10.21037/jss.2019.02.02. Epub [PubMed PMID: 31032437]
Bulloch LR, Spector L, Patel A. Acute Traumatic Myelopathy: Rethinking Central Cord Syndrome. The Journal of the American Academy of Orthopaedic Surgeons. 2022 Dec 1:30(23):1099-1107. doi: 10.5435/JAAOS-D-22-00260. Epub [PubMed PMID: 36400056]
Shakil H, Santaguida C, Wilson JR, Farhadi HF, Levi AD, Wilcox JT. Pathophysiology and surgical decision-making in central cord syndrome and degenerative cervical myelopathy: correcting the somatotopic fallacy. Frontiers in neurology. 2023:14():1276399. doi: 10.3389/fneur.2023.1276399. Epub 2023 Nov 17 [PubMed PMID: 38046579]
McKinley W, Santos K, Meade M, Brooke K. Incidence and outcomes of spinal cord injury clinical syndromes. The journal of spinal cord medicine. 2007:30(3):215-24 [PubMed PMID: 17684887]
Level 2 (mid-level) evidenceJohansson E, Luoto TM, Vainionpää A, Kauppila AM, Kallinen M, Väärälä E, Koskinen E. Epidemiology of traumatic spinal cord injury in Finland. Spinal cord. 2021 Jul:59(7):761-768. doi: 10.1038/s41393-020-00575-4. Epub 2020 Nov 4 [PubMed PMID: 33149235]
Segal DN, Grabel ZJ, Heller JG, Rhee JM, Michael KW, Yoon ST, Jain A. Epidemiology and treatment of central cord syndrome in the United States. Journal of spine surgery (Hong Kong). 2018 Dec:4(4):712-716. doi: 10.21037/jss.2018.11.02. Epub [PubMed PMID: 30714002]
Badhiwala JH, Ahuja CS, Fehlings MG. Time is spine: a review of translational advances in spinal cord injury. Journal of neurosurgery. Spine. 2019 Jan 1:30(1):1-18. doi: 10.3171/2018.9.SPINE18682. Epub 2018 Dec 20 [PubMed PMID: 30611186]
Level 3 (low-level) evidenceHashmi SZ, Marra A, Jenis LG, Patel AA. Current Concepts: Central Cord Syndrome. Clinical spine surgery. 2018 Dec:31(10):407-412. doi: 10.1097/BSD.0000000000000731. Epub [PubMed PMID: 30346310]
Baude M, Nielsen JB, Gracies JM. The neurophysiology of deforming spastic paresis: A revised taxonomy. Annals of physical and rehabilitation medicine. 2019 Nov:62(6):426-430. doi: 10.1016/j.rehab.2018.10.004. Epub 2018 Nov 28 [PubMed PMID: 30500361]
Collignon F, Martin D, Lénelle J, Stevenaert A. Acute traumatic central cord syndrome: magnetic resonance imaging and clinical observations. Journal of neurosurgery. 2002 Jan:96(1 Suppl):29-33 [PubMed PMID: 11795711]
Carr MT, Harrop JS, Houten JK. Traumatic Central Cord Syndrome. Clinical spine surgery. 2024 Nov 1:37(9):379-387. doi: 10.1097/BSD.0000000000001703. Epub 2024 Sep 30 [PubMed PMID: 39480046]
van Middendorp JJ, Pouw MH, Hayes KC, Williams R, Chhabra HS, Putz C, Veth RP, Geurts AC, Aito S, Kriz J, McKinley W, van Asbeck FW, Curt A, Fehlings MG, Van de Meent H, Hosman AJ, EM-SCI Study Group Collaborators. Diagnostic criteria of traumatic central cord syndrome. Part 2: a questionnaire survey among spine specialists. Spinal cord. 2010 Sep:48(9):657-63. doi: 10.1038/sc.2010.72. Epub 2010 Jun 29 [PubMed PMID: 20585327]
Level 3 (low-level) evidenceSacco E. [Physiopathology of overactive bladder syndrome]. Urologia. 2012:79(1):24-35. doi: 10.5301/RU.2012.8972. Epub [PubMed PMID: 22287269]
Level 3 (low-level) evidenceRupp R, Biering-Sørensen F, Burns SP, Graves DE, Guest J, Jones L, Read MS, Rodriguez GM, Schuld C, Tansey-Md KE, Walden K, Kirshblum S. International Standards for Neurological Classification of Spinal Cord Injury: Revised 2019. Topics in spinal cord injury rehabilitation. 2021 Spring:27(2):1-22. doi: 10.46292/sci2702-1. Epub [PubMed PMID: 34108832]
Hubertus V, Badhiwala JH, Hejrati N, Nouri A, Ter Wengel PV, Farahbakhsh F, Hofstetter C, Neal CJ, Ganau M, Agarwal N, Arnold P, Koljonen P, Harrop J, Aarabi B, Guest J, Rodrigues-Pinto R, Fehlings MG, Evaniew N, Margetis K, Guha D, Grassner L, Kwon BK, Fisher CG, Kurpad S, On Behalf Of The Ao Spine Knowledge Forum Spinal Cord Injury. AO Spine Clinical Practice Recommendations for the Surgical Management of Acute Traumatic Spinal Cord Injury: Contemporary Concepts. Global spine journal. 2025 Nov:15(8):3572-3579. doi: 10.1177/21925682251350941. Epub 2025 Jun 8 [PubMed PMID: 40483581]
Expert Panel on Neurological Imaging and Musculoskeletal Imaging:, Beckmann NM, West OC, Nunez D Jr, Kirsch CFE, Aulino JM, Broder JS, Cassidy RC, Czuczman GJ, Demertzis JL, Johnson MM, Motamedi K, Reitman C, Shah LM, Than K, Ying-Kou Yung E, Beaman FD, Kransdorf MJ, Bykowski J. ACR Appropriateness Criteria(®) Suspected Spine Trauma. Journal of the American College of Radiology : JACR. 2019 May:16(5S):S264-S285. doi: 10.1016/j.jacr.2019.02.002. Epub [PubMed PMID: 31054754]
Expert Panel on Neurological Imaging, Hassankhani A, Freeman CW, Banks J, Parsons MS, Wessell DE, Hutchins TA, Lenchik L, Burns J, Eldaya RW, Griffith B, Hickey SM, Khan MA, Lawrence B, Paisley TS, Reitman C, Ropper AE, Shah VN, Steenburg SD, Timpone VM, Yahyavi-Firouz-Abadi N, Chang EY, Policeni B. ACR Appropriateness Criteria® Acute Spinal Trauma: 2024 Update. Journal of the American College of Radiology : JACR. 2025 May:22(5S):S48-S66. doi: 10.1016/j.jacr.2025.02.013. Epub [PubMed PMID: 40409895]
Vaccaro AR, Hulbert RJ, Patel AA, Fisher C, Dvorak M, Lehman RA Jr, Anderson P, Harrop J, Oner FC, Arnold P, Fehlings M, Hedlund R, Madrazo I, Rechtine G, Aarabi B, Shainline M, Spine Trauma Study Group. The subaxial cervical spine injury classification system: a novel approach to recognize the importance of morphology, neurology, and integrity of the disco-ligamentous complex. Spine. 2007 Oct 1:32(21):2365-74 [PubMed PMID: 17906580]
Vaccaro AR, Koerner JD, Radcliff KE, Oner FC, Reinhold M, Schnake KJ, Kandziora F, Fehlings MG, Dvorak MF, Aarabi B, Rajasekaran S, Schroeder GD, Kepler CK, Vialle LR. AOSpine subaxial cervical spine injury classification system. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2016 Jul:25(7):2173-84. doi: 10.1007/s00586-015-3831-3. Epub 2015 Feb 26 [PubMed PMID: 25716661]
Fehlings MG, Martin AR, Tetreault LA, Aarabi B, Anderson P, Arnold PM, Brodke D, Burns AS, Chiba K, Dettori JR, Furlan JC, Hawryluk G, Holly LT, Howley S, Jeji T, Kalsi-Ryan S, Kotter M, Kurpad S, Kwon BK, Marino RJ, Massicotte E, Merli G, Middleton JW, Nakashima H, Nagoshi N, Palmieri K, Singh A, Skelly AC, Tsai EC, Vaccaro A, Wilson JR, Yee A, Harrop JS. A Clinical Practice Guideline for the Management of Patients With Acute Spinal Cord Injury: Recommendations on the Role of Baseline Magnetic Resonance Imaging in Clinical Decision Making and Outcome Prediction. Global spine journal. 2017 Sep:7(3 Suppl):221S-230S. doi: 10.1177/2192568217703089. Epub 2017 Sep 5 [PubMed PMID: 29164028]
Level 1 (high-level) evidenceAarabi B, Alexander M, Mirvis SE, Shanmuganathan K, Chesler D, Maulucci C, Iguchi M, Aresco C, Blacklock T. Predictors of outcome in acute traumatic central cord syndrome due to spinal stenosis. Journal of neurosurgery. Spine. 2011 Jan:14(1):122-30. doi: 10.3171/2010.9.SPINE09922. Epub 2010 Dec 17 [PubMed PMID: 21166485]
Talbott JF, Whetstone WD, Readdy WJ, Ferguson AR, Bresnahan JC, Saigal R, Hawryluk GW, Beattie MS, Mabray MC, Pan JZ, Manley GT, Dhall SS. The Brain and Spinal Injury Center score: a novel, simple, and reproducible method for assessing the severity of acute cervical spinal cord injury with axial T2-weighted MRI findings. Journal of neurosurgery. Spine. 2015 Oct:23(4):495-504. doi: 10.3171/2015.1.SPINE141033. Epub 2015 Jul 10 [PubMed PMID: 26161519]
Ramey WL, Reyes AA, Avila MJ, Hurlbert RJ, Chapman JR, Dumont TM. The Central Cord Score: A Novel Classification and Scoring System Specific to Acute Traumatic Central Cord Syndrome. World neurosurgery. 2021 Dec:156():e235-e242. doi: 10.1016/j.wneu.2021.09.037. Epub 2021 Sep 15 [PubMed PMID: 34536617]
Kumar AA, Lim HL, Saffari SE, Zaw S, Feng QJ, Ang E, Lee ZD, Shree Kumar D, Lee L, Pillay R, Ling JM. Comparative Validation of Scoring Systems in Acute Traumatic Central Cord Syndrome: Acute Traumatic Central Cord Syndrome Score, Central Cord Score, and Subaxial Cervical AO Spine Injury Score for Surgical Decision Making, Recovery, and Timing of Surgery. Journal of neurotrauma. 2025 Dec 15:():. doi: 10.1177/08977151251406611. Epub 2025 Dec 15 [PubMed PMID: 41457684]
Level 1 (high-level) evidenceGalvagno SM Jr, Nahmias JT, Young DA. Advanced Trauma Life Support(®) Update 2019: Management and Applications for Adults and Special Populations. Anesthesiology clinics. 2019 Mar:37(1):13-32. doi: 10.1016/j.anclin.2018.09.009. Epub 2018 Dec 27 [PubMed PMID: 30711226]
Fouad K, Popovich PG, Kopp MA, Schwab JM. The neuroanatomical-functional paradox in spinal cord injury. Nature reviews. Neurology. 2021 Jan:17(1):53-62. doi: 10.1038/s41582-020-00436-x. Epub 2020 Dec 11 [PubMed PMID: 33311711]
Kwon BK, Tetreault LA, Martin AR, Arnold PM, Marco RAW, Newcombe VFJ, Zipser CM, McKenna SL, Korupolu R, Neal CJ, Saigal R, Glass NE, Douglas S, Ganau M, Rahimi-Movaghar V, Harrop JS, Aarabi B, Wilson JR, Evaniew N, Skelly AC, Fehlings MG. A Clinical Practice Guideline for the Management of Patients With Acute Spinal Cord Injury: Recommendations on Hemodynamic Management. Global spine journal. 2024 Mar:14(3_suppl):187S-211S. doi: 10.1177/21925682231202348. Epub [PubMed PMID: 38526923]
Level 1 (high-level) evidenceZeller SL, Stein A, Frid I, Carpenter AB, Soldozy S, Rawanduzy C, Rosenberg J, Bauerschmidt A, Al-Mufti F, Mayer SA, Kinon MD, Wainwright JV. Critical Care of Spinal Cord Injury. Current neurology and neuroscience reports. 2024 Sep:24(9):355-363. doi: 10.1007/s11910-024-01357-8. Epub 2024 Jul 15 [PubMed PMID: 39008022]
Evaniew N, Noonan VK, Fallah N, Kwon BK, Rivers CS, Ahn H, Bailey CS, Christie SD, Fourney DR, Hurlbert RJ, Linassi AG, Fehlings MG, Dvorak MF, RHSCIR Network. Methylprednisolone for the Treatment of Patients with Acute Spinal Cord Injuries: A Propensity Score-Matched Cohort Study from a Canadian Multi-Center Spinal Cord Injury Registry. Journal of neurotrauma. 2015 Nov 1:32(21):1674-83. doi: 10.1089/neu.2015.3963. Epub 2015 Jul 17 [PubMed PMID: 26065706]
Fehlings MG, Tetreault LA, Wilson JR, Kwon BK, Burns AS, Martin AR, Hawryluk G, Harrop JS. A Clinical Practice Guideline for the Management of Acute Spinal Cord Injury: Introduction, Rationale, and Scope. Global spine journal. 2017 Sep:7(3 Suppl):84S-94S. doi: 10.1177/2192568217703387. Epub 2017 Sep 5 [PubMed PMID: 29164036]
Level 1 (high-level) evidenceFehlings MG, Tetreault LA, Wilson JR, Aarabi B, Anderson P, Arnold PM, Brodke DS, Burns AS, Chiba K, Dettori JR, Furlan JC, Hawryluk G, Holly LT, Howley S, Jeji T, Kalsi-Ryan S, Kotter M, Kurpad S, Marino RJ, Martin AR, Massicotte E, Merli G, Middleton JW, Nakashima H, Nagoshi N, Palmieri K, Singh A, Skelly AC, Tsai EC, Vaccaro A, Yee A, Harrop JS. A Clinical Practice Guideline for the Management of Patients With Acute Spinal Cord Injury and Central Cord Syndrome: Recommendations on the Timing (≤24 Hours Versus }24 Hours) of Decompressive Surgery. Global spine journal. 2017 Sep:7(3 Suppl):195S-202S. doi: 10.1177/2192568217706367. Epub 2017 Sep 5 [PubMed PMID: 29164024]
Level 1 (high-level) evidenceBadhiwala JH, Wilson JR, Harrop JS, Vaccaro AR, Aarabi B, Geisler FH, Fehlings MG. Early vs Late Surgical Decompression for Central Cord Syndrome. JAMA surgery. 2022 Nov 1:157(11):1024-1032. doi: 10.1001/jamasurg.2022.4454. Epub [PubMed PMID: 36169962]
Xu L, Zhong W, Liu C, Zhao H, Xiong Y, Zhou S, Ma Y, Yang Y, Yu X. Timing of decompression in central cord syndrome: a systematic review and meta-analysis. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2024 Sep:33(9):3593-3601. doi: 10.1007/s00586-024-08244-3. Epub 2024 Apr 16 [PubMed PMID: 38625584]
Level 1 (high-level) evidenceFehlings MG, Tetreault LA, Aarabi B, Anderson P, Arnold PM, Brodke DS, Burns AS, Chiba K, Dettori JR, Furlan JC, Hawryluk G, Holly LT, Howley S, Jeji T, Kalsi-Ryan S, Kotter M, Kurpad S, Kwon BK, Marino RJ, Martin AR, Massicotte E, Merli G, Middleton JW, Nakashima H, Nagoshi N, Palmieri K, Singh A, Skelly AC, Tsai EC, Vaccaro A, Wilson JR, Yee A, Harrop JS. A Clinical Practice Guideline for the Management of Patients With Acute Spinal Cord Injury: Recommendations on the Type and Timing of Anticoagulant Thromboprophylaxis. Global spine journal. 2017 Sep:7(3 Suppl):212S-220S. doi: 10.1177/2192568217702107. Epub 2017 Sep 5 [PubMed PMID: 29164026]
Level 1 (high-level) evidenceA MS, V TS, B DS. Cruciate Paralysis in a 20- year -old Male with an Undisplaced Type III Odontoid Fracture. Journal of orthopaedic case reports. 2016 Apr-Jun:6(2):40-42. doi: 10.13107/jocr.2250-0685.424. Epub [PubMed PMID: 28111622]
Level 3 (low-level) evidenceHopkins B, Khanna R, Dahdaleh NS. Revisiting cruciate paralysis: A case report and systematic review. Journal of craniovertebral junction & spine. 2016 Oct-Dec:7(4):265-272 [PubMed PMID: 27891037]
Level 3 (low-level) evidenceLevi AD, Tator CH, Bunge RP. Clinical syndromes associated with disproportionate weakness of the upper versus the lower extremities after cervical spinal cord injury. Neurosurgery. 1996 Jan:38(1):179-83; discussion 183-5 [PubMed PMID: 8747967]
Level 3 (low-level) evidenceNasri A, Kacem I, Sidhom Y, Djebara MB, Gargouri A, Gouider R. Isolated spinal cord compression syndrome revealing delayed extensive superficial siderosis of the central nervous system secondary to cervical root avulsion. The journal of spinal cord medicine. 2018 Jul:41(4):490-495. doi: 10.1080/10790268.2017.1329053. Epub 2017 Jun 5 [PubMed PMID: 28580859]
Edeiken-Monroe B, Wagner LK, Harris JH Jr. Hyperextension dislocation of the cervical spine. AJR. American journal of roentgenology. 1986 Apr:146(4):803-8 [PubMed PMID: 3485356]
Penrod LE, Hegde SK, Ditunno JF Jr. Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Archives of physical medicine and rehabilitation. 1990 Nov:71(12):963-8 [PubMed PMID: 2241542]
Blasetti G, Pavese C, Maier DD, Weidner N, Rupp R, Abel R, Yorck BK, Jiri K, Curt A, Molinari M, Schubert M, Scivoletto G. Comparison of outcomes between people with and without central cord syndrome. Spinal cord. 2020 Dec:58(12):1263-1273. doi: 10.1038/s41393-020-0491-x. Epub 2020 Jun 2 [PubMed PMID: 32488195]
Tow AM, Kong KH. Central cord syndrome: functional outcome after rehabilitation. Spinal cord. 1998 Mar:36(3):156-60 [PubMed PMID: 9554013]
Newey ML, Sen PK, Fraser RD. The long-term outcome after central cord syndrome: a study of the natural history. The Journal of bone and joint surgery. British volume. 2000 Aug:82(6):851-5 [PubMed PMID: 10990310]
Liu G, Liu L, Wang Y. Surgical Efficacy and Prognostic Factors for Acute Traumatic Central Cord Syndrome Without Fracture and Dislocation. Orthopedics. 2022 Nov-Dec:45(6):325-332. doi: 10.3928/01477447-20220907-07. Epub 2022 Sep 13 [PubMed PMID: 36098568]
Zhou Q, Zhang J, Liu H, Zhou X, He W, Jin Z, Yang H, Liu T. Comparison of Anterior and Posterior Approaches for Acute Traumatic Central Spinal Cord Syndrome with Multilevel Cervical Canal Stenosis without Cervical Fracture or Dislocation. International journal of clinical practice. 2022:2022():5132134. doi: 10.1155/2022/5132134. Epub 2022 Feb 16 [PubMed PMID: 35685581]
Zhang C, Lee VKH, Yu JML, Cheung JPY, Koljonen PA, Shea GKH. Length of Cervical Stenosis, Admission ASIA Motor Scores, and BASIC Scores Are Predictors of Recovery Rate Following Central Cord Syndrome. Spine. 2022 Feb 1:47(3):212-219. doi: 10.1097/BRS.0000000000004178. Epub [PubMed PMID: 34310538]
Bin-Alamer O, Qedair J, Abou-Al-Shaar H, Mallela AN, Balasubramanian K, Alnefaie N, Abou Al-Shaar AR, Plute T, Lu VM, McCarthy DJ, Fields DP, Agarwal N, Gerszten PC, Hamilton DK. Surgical intervention ≤ 24 hours versus } 24 hours after injury for the management of acute traumatic central cord syndrome: a systematic review and meta-analysis. Journal of neurosurgery. Spine. 2024 May 1:40(5):653-661. doi: 10.3171/2023.11.SPINE23789. Epub 2024 Feb 9 [PubMed PMID: 38335527]
Level 1 (high-level) evidenceAarabi B, Harrop JS, Tator CH, Alexander M, Dettori JR, Grossman RG, Fehlings MG, Mirvis SE, Shanmuganathan K, Zacherl KM, Burau KD, Frankowski RF, Toups E, Shaffrey CI, Guest JD, Harkema SJ, Habashi NM, Andrews P, Johnson MM, Rosner MK. Predictors of pulmonary complications in blunt traumatic spinal cord injury. Journal of neurosurgery. Spine. 2012 Sep:17(1 Suppl):38-45. doi: 10.3171/2012.4.AOSPINE1295. Epub [PubMed PMID: 22985369]
Biering-Sørensen F, Biering-Sørensen T, Liu N, Malmqvist L, Wecht JM, Krassioukov A. Alterations in cardiac autonomic control in spinal cord injury. Autonomic neuroscience : basic & clinical. 2018 Jan:209():4-18. doi: 10.1016/j.autneu.2017.02.004. Epub 2017 Feb 15 [PubMed PMID: 28228335]
Teasell RW, Arnold JM, Krassioukov A, Delaney GA. Cardiovascular consequences of loss of supraspinal control of the sympathetic nervous system after spinal cord injury. Archives of physical medicine and rehabilitation. 2000 Apr:81(4):506-16 [PubMed PMID: 10768544]
. Prevention of Venous Thromboembolism in Individuals with Spinal Cord Injury: Clinical Practice Guidelines for Health Care Providers, 3rd ed.: Consortium for Spinal Cord Medicine. Topics in spinal cord injury rehabilitation. 2016 Summer:22(3):209-240. doi: 10.1310/sci2203-209. Epub [PubMed PMID: 29339863]
Level 1 (high-level) evidenceGibbons CH, Schmidt P, Biaggioni I, Frazier-Mills C, Freeman R, Isaacson S, Karabin B, Kuritzky L, Lew M, Low P, Mehdirad A, Raj SR, Vernino S, Kaufmann H. The recommendations of a consensus panel for the screening, diagnosis, and treatment of neurogenic orthostatic hypotension and associated supine hypertension. Journal of neurology. 2017 Aug:264(8):1567-1582. doi: 10.1007/s00415-016-8375-x. Epub 2017 Jan 3 [PubMed PMID: 28050656]
Level 3 (low-level) evidenceJansen RW, Lipsitz LA. Postprandial hypotension: epidemiology, pathophysiology, and clinical management. Annals of internal medicine. 1995 Feb 15:122(4):286-95 [PubMed PMID: 7825766]
Barber DB, Rogers SJ, Fredrickson MD, Able AC. Midodrine hydrochloride and the treatment of orthostatic hypotension in tetraplegia: two cases and a review of the literature. Spinal cord. 2000 Feb:38(2):109-11 [PubMed PMID: 10762185]
Level 3 (low-level) evidenceDavies B, Bannister R, Sever P. Pressor amines and monoamine-oxidase inhibitors for treatment of postural hypotension in autonomic failure. Limitations and hazards. Lancet (London, England). 1978 Jan 28:1(8057):172-5 [PubMed PMID: 74603]
Groomes TE, Huang CT. Orthostatic hypotension after spinal cord injury: treatment with fludrocortisone and ergotamine. Archives of physical medicine and rehabilitation. 1991 Jan:72(1):56-8 [PubMed PMID: 1985624]
Level 3 (low-level) evidenceOnmez H, Cingoz HT, Kucuksen S, Anliacık E, Yaşar O, Yilmaz H, Salli A. Bilateral upper-extremity deep vein thrombosis following central cord syndrome. The journal of spinal cord medicine. 2013 May:36(3):243-6. doi: 10.1179/2045772313Y.0000000096. Epub [PubMed PMID: 23809596]
Level 3 (low-level) evidenceYelamarthy PKK, Chhabra HS, Vaccaro A, Vishwakarma G, Kluger P, Nanda A, Abel R, Tan WF, Gardner B, Chandra PS, Chatterjee S, Kahraman S, Naderi S, Basu S, Theron F. Management and prognosis of acute traumatic cervical central cord syndrome: systematic review and Spinal Cord Society-Spine Trauma Study Group position statement. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2019 Oct:28(10):2390-2407. doi: 10.1007/s00586-019-06085-z. Epub 2019 Jul 31 [PubMed PMID: 31367852]
Level 1 (high-level) evidenceKrassioukov A, Warburton DE, Teasell R, Eng JJ, Spinal Cord Injury Rehabilitation Evidence Research Team. A systematic review of the management of autonomic dysreflexia after spinal cord injury. Archives of physical medicine and rehabilitation. 2009 Apr:90(4):682-95. doi: 10.1016/j.apmr.2008.10.017. Epub [PubMed PMID: 19345787]
Level 1 (high-level) evidenceReaddy WJ, Whetstone WD, Ferguson AR, Talbott JF, Inoue T, Saigal R, Bresnahan JC, Beattie MS, Pan JZ, Manley GT, Dhall SS. Complications and outcomes of vasopressor usage in acute traumatic central cord syndrome. Journal of neurosurgery. Spine. 2015 Nov:23(5):574-580. doi: 10.3171/2015.2.SPINE14746. Epub 2015 Jul 31 [PubMed PMID: 26230417]
Farkas GJ, Burton AM, McMillan DW, Sneij A, Gater DR Jr. The Diagnosis and Management of Cardiometabolic Risk and Cardiometabolic Syndrome after Spinal Cord Injury. Journal of personalized medicine. 2022 Jun 30:12(7):. doi: 10.3390/jpm12071088. Epub 2022 Jun 30 [PubMed PMID: 35887592]
Gilron I, Baron R, Jensen T. Neuropathic pain: principles of diagnosis and treatment. Mayo Clinic proceedings. 2015 Apr:90(4):532-45. doi: 10.1016/j.mayocp.2015.01.018. Epub [PubMed PMID: 25841257]
Levendoglu F, Ogün CO, Ozerbil O, Ogün TC, Ugurlu H. Gabapentin is a first line drug for the treatment of neuropathic pain in spinal cord injury. Spine. 2004 Apr 1:29(7):743-51 [PubMed PMID: 15087796]
Level 1 (high-level) evidenceBates D, Schultheis BC, Hanes MC, Jolly SM, Chakravarthy KV, Deer TR, Levy RM, Hunter CW. A Comprehensive Algorithm for Management of Neuropathic Pain. Pain medicine (Malden, Mass.). 2019 Jun 1:20(Suppl 1):S2-S12. doi: 10.1093/pm/pnz075. Epub [PubMed PMID: 31152178]
Guy SD, Mehta S, Casalino A, Côté I, Kras-Dupuis A, Moulin DE, Parrent AG, Potter P, Short C, Teasell R, Bradbury CL, Bryce TN, Craven BC, Finnerup NB, Harvey D, Hitzig SL, Lau B, Middleton JW, O'Connell C, Orenczuk S, Siddall PJ, Townson A, Truchon C, Widerström-Noga E, Wolfe D, Loh E. The CanPain SCI Clinical Practice Guidelines for Rehabilitation Management of Neuropathic Pain after Spinal Cord: Recommendations for treatment. Spinal cord. 2016 Aug:54 Suppl 1():S14-23. doi: 10.1038/sc.2016.90. Epub [PubMed PMID: 27444715]
Level 1 (high-level) evidenceNorrbrink C, Lundeberg T. Tramadol in neuropathic pain after spinal cord injury: a randomized, double-blind, placebo-controlled trial. The Clinical journal of pain. 2009 Mar-Apr:25(3):177-84. doi: 10.1097/AJP.0b013e31818a744d. Epub [PubMed PMID: 19333166]
Level 1 (high-level) evidenceLi L, Han Y, Li T, Zhou J, Sun C, Xue Y. The analgesic effect of intravenous methylprednisolone on acute neuropathic pain with allodynia due to central cord syndrome: a retrospective study. Journal of pain research. 2018:11():1231-1238. doi: 10.2147/JPR.S160463. Epub 2018 Jun 25 [PubMed PMID: 29983586]
Level 2 (mid-level) evidencevan den Noort JC, Bar-On L, Aertbeliën E, Bonikowski M, Braendvik SM, Broström EW, Buizer AI, Burridge JH, van Campenhout A, Dan B, Fleuren JF, Grunt S, Heinen F, Horemans HL, Jansen C, Kranzl A, Krautwurst BK, van der Krogt M, Lerma Lara S, Lidbeck CM, Lin JP, Martinez I, Meskers C, Metaxiotis D, Molenaers G, Patikas DA, Rémy-Néris O, Roeleveld K, Shortland AP, Sikkens J, Sloot L, Vermeulen RJ, Wimmer C, Schröder AS, Schless S, Becher JG, Desloovere K, Harlaar J. European consensus on the concepts and measurement of the pathophysiological neuromuscular responses to passive muscle stretch. European journal of neurology. 2017 Jul:24(7):981-e38. doi: 10.1111/ene.13322. Epub 2017 May 29 [PubMed PMID: 28557247]
Level 3 (low-level) evidenceHsieh JT, Wolfe DL, Miller WC, Curt A, SCIRE Research Team. Spasticity outcome measures in spinal cord injury: psychometric properties and clinical utility. Spinal cord. 2008 Feb:46(2):86-95 [PubMed PMID: 17909559]
Bovend'Eerdt TJ, Newman M, Barker K, Dawes H, Minelli C, Wade DT. The effects of stretching in spasticity: a systematic review. Archives of physical medicine and rehabilitation. 2008 Jul:89(7):1395-406. doi: 10.1016/j.apmr.2008.02.015. Epub 2008 Jun 13 [PubMed PMID: 18534551]
Level 1 (high-level) evidenceOttoson D. The effects of temperature on the isolated muscle spindle. The Journal of physiology. 1965 Oct:180(3):636-48 [PubMed PMID: 4221242]
Level 3 (low-level) evidenceBekhet AH, Bochkezanian V, Saab IM, Gorgey AS. The Effects of Electrical Stimulation Parameters in Managing Spasticity After Spinal Cord Injury: A Systematic Review. American journal of physical medicine & rehabilitation. 2019 Jun:98(6):484-499. doi: 10.1097/PHM.0000000000001064. Epub [PubMed PMID: 30300228]
Level 1 (high-level) evidenceKorzhova J, Sinitsyn D, Chervyakov A, Poydasheva A, Zakharova M, Suponeva N, Chernikova L, Piradov M. Transcranial and spinal cord magnetic stimulation in treatment of spasticity: a literature review and meta-analysis. European journal of physical and rehabilitation medicine. 2018 Feb:54(1):75-84. doi: 10.23736/S1973-9087.16.04433-6. Epub 2016 Dec 22 [PubMed PMID: 28004906]
Level 1 (high-level) evidenceCabahug P, Pickard C, Edmiston T, Lieberman JA. A Primary Care Provider's Guide to Spasticity Management in Spinal Cord Injury. Topics in spinal cord injury rehabilitation. 2020 Summer:26(3):157-165. doi: 10.46292/sci2603-157. Epub [PubMed PMID: 33192042]
Barbeau H, Richards CL, Bédard PJ. Action of cyproheptadine in spastic paraparetic patients. Journal of neurology, neurosurgery, and psychiatry. 1982 Oct:45(10):923-6 [PubMed PMID: 7143011]
Level 1 (high-level) evidenceWhiting PF, Wolff RF, Deshpande S, Di Nisio M, Duffy S, Hernandez AV, Keurentjes JC, Lang S, Misso K, Ryder S, Schmidlkofer S, Westwood M, Kleijnen J. Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA. 2015 Jun 23-30:313(24):2456-73. doi: 10.1001/jama.2015.6358. Epub [PubMed PMID: 26103030]
Level 1 (high-level) evidenceWiener J, Hsieh J, McIntyre A, Teasell R. Effectiveness of 4-Aminopyridine for the Management of Spasticity in Spinal Cord Injury: A Systematic Review. Topics in spinal cord injury rehabilitation. 2018 Fall:24(4):353-362. doi: 10.1310/sci17-00048. Epub 2018 May 3 [PubMed PMID: 30459498]
Level 1 (high-level) evidenceMoeini-Naghani I, Hashemi-Zonouz T, Jabbari B. Botulinum Toxin Treatment of Spasticity in Adults and Children. Seminars in neurology. 2016 Feb:36(1):64-72. doi: 10.1055/s-0036-1571847. Epub 2016 Feb 11 [PubMed PMID: 26866498]
Lui J, Sarai M, Mills PB. Chemodenervation for treatment of limb spasticity following spinal cord injury: a systematic review. Spinal cord. 2015 Apr:53(4):252-64. doi: 10.1038/sc.2014.241. Epub 2015 Jan 13 [PubMed PMID: 25582713]
Level 1 (high-level) evidenceBoviatsis EJ, Kouyialis AT, Korfias S, Sakas DE. Functional outcome of intrathecal baclofen administration for severe spasticity. Clinical neurology and neurosurgery. 2005 Jun:107(4):289-95 [PubMed PMID: 15885386]
Jozefczyk PB. The management of focal spasticity. Clinical neuropharmacology. 2002 May-Jun:25(3):158-73 [PubMed PMID: 12023570]
Madsen PJ, Isaac Chen HC, Lang SS. Neurosurgical Approaches. Physical medicine and rehabilitation clinics of North America. 2018 Aug:29(3):553-565. doi: 10.1016/j.pmr.2018.04.002. Epub 2018 May 29 [PubMed PMID: 30626515]
Nagel SJ, Wilson S, Johnson MD, Machado A, Frizon L, Chardon MK, Reddy CG, Gillies GT, Howard MA 3rd. Spinal Cord Stimulation for Spasticity: Historical Approaches, Current Status, and Future Directions. Neuromodulation : journal of the International Neuromodulation Society. 2017 Jun:20(4):307-321. doi: 10.1111/ner.12591. Epub 2017 Apr 2 [PubMed PMID: 28370802]
Level 3 (low-level) evidenceFauss GNK, Hudson KE, Grau JW. Role of Descending Serotonergic Fibers in the Development of Pathophysiology after Spinal Cord Injury (SCI): Contribution to Chronic Pain, Spasticity, and Autonomic Dysreflexia. Biology. 2022 Feb 1:11(2):. doi: 10.3390/biology11020234. Epub 2022 Feb 1 [PubMed PMID: 35205100]
Viswanath O, Urits I, Burns J, Charipova K, Gress K, McNally A, Urman RD, Welschmeyer A, Berger AA, Kassem H, Sanchez MG, Kaye AD, Eubanks TN, Cornett EM, Ngo AL. Central Neuropathic Mechanisms in Pain Signaling Pathways: Current Evidence and Recommendations. Advances in therapy. 2020 May:37(5):1946-1959. doi: 10.1007/s12325-020-01334-w. Epub 2020 Apr 10 [PubMed PMID: 32291648]
Level 3 (low-level) evidenceGrundy L, Caldwell A, Brierley SM. Mechanisms Underlying Overactive Bladder and Interstitial Cystitis/Painful Bladder Syndrome. Frontiers in neuroscience. 2018:12():931. doi: 10.3389/fnins.2018.00931. Epub 2018 Dec 12 [PubMed PMID: 30618560]
Dulamea AO, Sirbu-Boeti MP, Bleotu C, Dragu D, Moldovan L, Lupescu I, Comi G. Autologous mesenchymal stem cells applied on the pressure ulcers had produced a surprising outcome in a severe case of neuromyelitis optica. Neural regeneration research. 2015 Nov:10(11):1841-5. doi: 10.4103/1673-5374.165325. Epub [PubMed PMID: 26807122]
Level 3 (low-level) evidenceVining RD, Gosselin DM, Thurmond J, Case K, Bruch FR. Interdisciplinary rehabilitation for a patient with incomplete cervical spinal cord injury and multimorbidity: A case report. Medicine. 2017 Aug:96(34):e7837. doi: 10.1097/MD.0000000000007837. Epub [PubMed PMID: 28834891]
Level 3 (low-level) evidence