Introduction
The septum pellucidum (meaning translucent wall in Latin) is a thin, triangular double membrane separating the frontal horns of the right and left lateral ventricles of the brain. The septum pellucidum extends between the anterior portion of the corpus callosum and the body of the fornix, and its thickness varies from 1.5 to 3.0 mm.[1] The cavum septi pellucidi (CSP) is a potential cavity between the membranous leaves of the septum pellucidum, often defined radiologically as separation of the septal leaflets by at least 1 mm. CSP persistence after infancy is usually an incidental normal variant when isolated (see Image. Cavum Septi Pellucidi). CSP contains fluid similar to cerebrospinal fluid and is not part of the ventricular system because it lacks ependymal or choroid plexus lining and does not communicate with the ventricular system or the subarachnoid space. CSP may be continuous posteriorly with the cavum vergae, which is separated from CSP by an arbitrary vertical plane at the columns of the fornix. CSP and the cavum vergae were previously incorrectly referred to as the fifth and sixth ventricles, respectively (see Image. Cavum Septi Pellucidi With Cavum Vergae). Neither is part of the ventricular system, because these structures have different embryological origins and lack a lining of ependymal or choroid plexus cells. In repetitive head trauma, particularly boxing and collision sports, CSP may represent an acquired or trauma-associated change (boxer cavum). However, CSP identified on imaging is nonspecific and should not be interpreted as diagnostic of chronic traumatic encephalopathy.
Boundaries of the Septum Pellucidum
- Superiorly: Inferior surface of the body of the corpus callosum
- Anteroinferiorly: Superior surface of the genu of the corpus callosum
- Posteroinferiorly: Corpus and columns of the fornix
- Laterally: Medial wall of the frontal horns of the lateral ventricles
- Medially: Opposing septal leaflet, with a potential intervening cavum when unfused
Boundaries of the Cavum Septi Pellucidi
- Anteriorly: Genu of the corpus callosum
- Superiorly: Body of the corpus callosum
- Posteriorly: Columns and pillars of the fornix
- Inferiorly: Anterior commissure and the rostrum of the corpus callosum
- Laterally: Leaflets of the septum pellucidum [2]
The septi pellucidi is an important part of the limbic system, with prominent connections to both the medial and the basolateral limbic circuit. A simple CSP is usually asymptomatic. When present, symptoms are more often related to CSP cysts and may result from mass effect, obstruction of the foramina of Monro, hydrocephalus, compression of hypothalamoseptal pathways, or venous displacement.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The septum pellucidum forms embryologically from 2 closely opposed leaves enclosing a cavity called the CSP. The 2 leaflets of the septum pellucidum begin to fuse at around 6 months of gestation, progressing from posterior to anterior. Consequently, the posterior cavity, the cavum vergae, is usually closed by birth in term neonates, whereas the anterior cavity, the cavum septi pellucidi, commonly persists after birth and usually closes by 3 to 6 months of age. However, an unclosed gap allows CSP to persist, and CSP may be identified even in adults. Cumulative exposure to heavy explosives has been proposed as an etiological factor for CSP enlargement, making it a potential imaging marker of blast-related neurotrauma.[3]
Epidemiology
CSP is estimated to occur in all premature infants, in 85% of full-term neonates, and in 12% of children aged 6 months to 16 years. Eighty-five percent of CSPs fuse around 3 to 6 mo after birth.[4] In adults, the prevalence varies from 4% to 74%, depending on detection methods and anatomical definition. Cysts of CSP are rarer, with an incidence of 0.04%, according to a study by Wang et al, whereas symptomatic CSP and cavum vergae cysts remain rare and are mainly described in case reports and small series.[5]
Pathophysiology
A simple incidental CSP is usually asymptomatic. Symptoms are more likely to occur with CSP cysts, although most CSP cysts are incidental findings. Three mechanisms are mainly described:
- Ball-valve phenomenon: Obstruction of the interventricular foramina by the cyst, leading to hydrocephalus and increased intracranial pressure.
- Compression of the hypothalamoseptal triangle: Compression of structures formed by the septal and periseptal nuclei and their associated projection pathways has been proposed to contribute to neuropsychiatric or behavioral symptoms. However, causality is often difficult to establish. Compression of the optic chiasm and visual pathways has also been proposed.
- Chronic deep venous impairment: Displacement and stretching of the internal cerebral and subependymal veins may result in progressive focal neurologic deficits.[6]
The mechanism of cyst enlargement is uncertain; proposed mechanisms include fluid accumulation due to valve-like communication or altered cerebrospinal fluid dynamics. The commonly used definition of a CSP cyst is a cystic structure with a width of 10 mm or more in the septal region, with walls that exhibit lateral bowing.[7] No strict definition differentiates a large CSP from a CSP cyst. CSP cysts are classified into 2 categories: communicating and noncommunicating, depending on whether they communicate with the ventricles. A noncommunicating cyst may become communicating due to spontaneous rupture or during head trauma, historical diagnostic procedures such as ventriculography and pneumoencephalography, or a surgical procedure. The reverse is also possible if fibrosis occurs at the site of communication. CSP cysts can also be classified as symptomatic or asymptomatic.
Histopathology
The walls of the CSP are composed of septal leaflets containing glial and neuronal elements; unlike true ventricles, the cavity is not lined by ependyma and has no choroid plexus.[8] Boxer cavum has been described as a septal fenestration with detachment of the fornix from the undersurface of the corpus callosum and horizontal splaying of the flattened forniceal bodies.[9]
History and Physical
Many symptoms and diseases have historically been attributed to cysts of the CSP, including mental disturbances, ataxia, disordered speech, epilepsy, and bilateral pyramidal signs. However, these associations are now being questioned because proper evidence is lacking. CSP cysts may present with headache (sometimes exertional), vomiting, papilledema, syncope, hydrocephalus, visual or sensorimotor findings, and occasionally cognitive, emotional, or behavioral symptoms, although causality is often difficult to establish for the latter.
Evaluation
Evaluation of a symptomatic, enlarged, or atypical CSP is best performed with a brain MRI. In fetal life, visualization of the CSP between 18 and 20 weeks of gestation is an expected finding and is used as part of the routine assessment of midline forebrain development.[10] CSP assessment is a mandatory part of second-trimester ultrasonography. The absence of CSP is a marker of associated fetal anomalies. Nonvisualization of the fetal CSP should prompt targeted neurosonography or fetal MRI to assess the corpus callosum, optic pathways, hypothalamic-pituitary axis, cortical development, ventricles, and associated midline anomalies. However, isolated nonvisualization is not synonymous with callosal agenesis and may rarely represent a normal variant.
When absent CSP or septal agenesis is suspected prenatally, postnatal ophthalmological and endocrine assessment is important to exclude septo-optic dysplasia, even when prenatal imaging appears otherwise isolated. When obliteration of the cavum septi pellucidi appears isolated at midpregnancy, CSP obliteration is often transient; CSP fluid becomes visible later in gestation in up to 70% of cases, although detailed neurosonographic assessment remains important.[11] Fetuses with a normally developed corpus callosum typically show a rectangular cavum septi pellucidi, with a CSP length-to-width ratio greater than 1.5 during the second half of gestation. In many cases of partial agenesis of the corpus callosum, the CSP appears abnormally short and wide, resulting in a reduced ratio. A low CSP ratio may therefore raise suspicion for partial callosal agenesis and should prompt a detailed assessment of the corpus callosum, although a normal ratio does not exclude the diagnosis.[12]
The ratio of the width of the cavum septi pellucidi to the anteroposterior cerebellar diameter (CSP to APCD ratio) may serve as an adjunctive prenatal ultrasonographic marker for trisomy 18. An increased ratio, reflecting a relatively widened CSP or a small cerebellum, should prompt detailed fetal anomaly screening and genetic counseling.[13] Enlarged or persistent CSP has been reported in association with several neuropsychiatric, neurodevelopmental, and trauma-related conditions, but these associations are not diagnostic, and causality remains uncertain.
Reported associations of CSP include schizophrenia, which was first reported by De Greef, alcohol use disorder with aggressive behavior, neurodevelopmental disorders, repeated head trauma in boxers, posttraumatic stress disorder, military service during active war conflicts or veteran status, and obsessive-compulsive disorder. However, these associations are nonspecific and should not be interpreted as diagnostic or causal.[8][14][15][16] Recent evidence indicates that an enlarged CSP is better interpreted as a correlate of neurodevelopmental liability, rather than as an individual biomarker for schizophrenia.[17] The absence or nonvisualization of the CSP in utero may be associated with holoprosencephaly, septo-optic dysplasia, agenesis or dysgenesis of the corpus callosum, schizencephaly, severe or chronic hydrocephalus, porencephaly or hydranencephaly, syntelencephaly, basilar encephalocele, or acquired fetal brain injury.
Treatment / Management
Association of a CSP cyst on imaging studies with clinical signs and symptoms caused by obstruction of cerebrospinal fluid flow at the foramen of Monro, direct compression of the surrounding tissues by the cyst, or mental status changes or focal neurologic deficits attributable to the CSP cyst are indications for treatment. Because symptomatic CSP and cavum vergae cysts are rare and evidence is limited to case reports and small series, treatment decisions should be based on careful correlation between symptoms, cyst enlargement, mass effect, cerebrospinal fluid obstruction, hydrocephalus, and progression.
When treatment is indicated, the goal is to relieve cerebrospinal fluid obstruction, hydrocephalus, or clinically significant mass effect; treatment is usually surgical, most commonly endoscopic fenestration. The classic treatment in these cases is surgical, including open procedures, conventional shunting, and stereotactic fenestration. Dandy published the first report of a treated CSP cyst in 1931; he treated a 4.5-year-old boy with transcallosal fenestration.[18] Since 1995, when Jacowski et al described the first endoscopic approach, neuroendoscopic fenestration has become a well-established therapeutic option and is currently the treatment of choice for symptomatic CSP cysts.[19] Surgical planning should account for the proximity of the fornices, internal cerebral veins, septal veins, and foramina of Monro; postoperative imaging is used to confirm cyst decompression, ventricular size, and fenestration patency.(B3)
Three endoscopic approaches have been described: a frontal approach to the coronal suture 3 cm from the midline that targets the frontal horn of the lateral ventricle, which is used by most authors; a cortical frontal approach directly targeting the cyst, followed by cyst puncture and fenestration of the 2 walls; and an occipital burr hole to optimize the trajectory into the atrium of the lateral ventricle, allowing a perpendicular approach to both leaflets of the cyst is a third method.[20](B3)
Endoscopic fenestration offers a less invasive approach, direct visualization, and effectiveness. Direct visualization of neural and vascular structures prevents inadvertent injury. Inspection of the foramina of Monro is also important to identify potential adhesions, which may play a role in persistent hydrocephalus after apparently successful cyst drainage. Additionally, endoscopic fenestration avoids the need to place a shunt and allows cyst wall biopsy. In selected patients with a prominent CSP and a cavum vergae, the transcavum-interforaminal route may provide an alternative trajectory to the third ventricle when the transforaminal approach is anatomically limited.[8]
Differential Diagnosis
The differential diagnoses of a midline CSF-like cavity or cyst include:
- The cavum vergae extends from the CSP posterior to the anterior columns of the fornix, lying anterior to the splenium of the corpus callosum (see Image. Cavum Vergae)
- The cavum veli interpositi extends from below the splenium of the corpus callosum and the column of the fornix to above the internal cerebral veins. The cavum veli interpositi has a triangular shape, with the apex pointing anteriorly and reaching as far forward as the foramen of Monro
- Vein of Galen aneurysmal malformation is distinguished by vascular flow on Doppler ultrasonography and further characterized with MRI, magnetic resonance angiography, or angiography when required
- Arachnoid cyst
- Dilated third ventricle (distinguished by its location between the thalami)
Prognosis
CSP is usually an incidental diagnosis and typically asymptomatic. Rarely, a CSP cyst can undergo spontaneous resolution.[21] A recent small study of 16 children with prenatally detected obliterated CSP found that most had typical neurodevelopment on detailed follow-up.[22]
Complications
An isolated cavum septi pellucidi is usually asymptomatic and has no inherent complications. Clinically relevant complications are rare and limited to enlarged or cystic CSP, which can cause mass effect or cerebrospinal fluid pathway obstruction. In fetal imaging, absent or nonvisualized CSP is not a complication but rather a marker that should prompt evaluation for associated brain malformations.
Deterrence and Patient Education
Patients need reassurance that CSP is a normal anatomical variant, requires no surgical intervention, and is unlikely to progress. A CSP wider than 1 cm, progressive enlargement, associated mass effect, hydrocephalus, or relevant symptoms should prompt further evaluation; treatment is reserved for cases in which symptoms are attributable to the cyst.
Pearls and Other Issues
Symptomatic enlargement of the CSP is rare and may present with headache, features of raised intracranial pressure, obstructive hydrocephalus, syncope, focal neurologic deficits, or neuropsychiatric symptoms. When a surgical procedure is indicated, endoscopic fenestration is now the preferred approach in most cases; shunting or open excision is generally reserved for selected or recurrent cases. CSP is an important marker for evaluating the normal development of the fetal neural axis.
Enhancing Healthcare Team Outcomes
A rigorous evaluation, including neurologic and radiologic examinations, is necessary before treatment. Before a surgical procedure, symptoms should be correlated carefully with MRI findings, including cyst size, mass effect, foraminal obstruction, hydrocephalus, and progression. Interdisciplinary input from a neurologist and neuropsychiatrist is useful when symptoms are nonspecific, particularly cognitive, behavioral, or psychiatric symptoms.
Media
(Click Image to Enlarge)
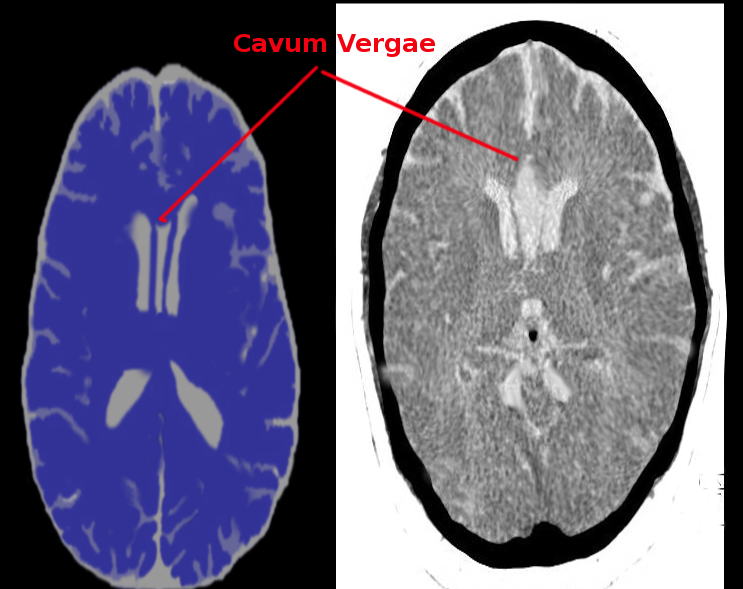
Cavum Septi Pellucidi and Cavum Vergae. Axial CT scan images of the brain demonstrate a cavum vergae, which is a midline cerebrospinal fluid-filled anatomical variant situated between the lateral ventricles posterior to the cavum septi pellucidi.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
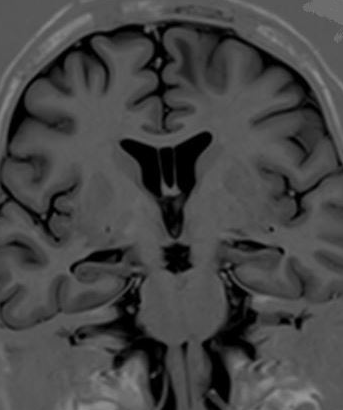
Cavum Septi Pellucidi. MRI of the brain demonstrates a midline, cerebrospinal fluid-filled space between the frontal horns of the lateral ventricles consistent with the cavum septi pellucidi.
Contributed by S Munakomi, MD
(Click Image to Enlarge)
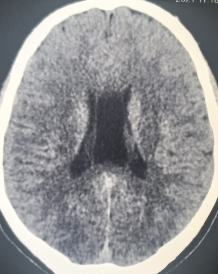
Cavum Vergae. Axial CT scan of the brain demonstrates a cavum vergae, appearing as an elongated, midline cerebrospinal fluid-filled cavity located between the bodies of the lateral ventricles and posterior to the septi pellucidi.
Contributed by S Munakomi, MD
References
Pendergrass EP, Hodes PJ. DILATATIONS OF THE CAVUM SEPTI PELLUCIDI AND CAVUM VERGAE. Annals of surgery. 1935 Jan:101(1):269-95 [PubMed PMID: 17856447]
Born CM, Meisenzahl EM, Frodl T, Pfluger T, Reiser M, Möller HJ, Leinsinger GL. The septum pellucidum and its variants. An MRI study. European archives of psychiatry and clinical neuroscience. 2004 Oct:254(5):295-302 [PubMed PMID: 15365704]
De Giorgi S, Diociasi A, Khalid RN, Degn P, Rand KE, Gabali S, Hirschberg RE, Sorg SF, Lev M, Gupta R. Cavum Septum Pellucidum Enlargement in Special Operations Forces Members Is Associated with Lifetime Exposure to Large Explosives. Journal of neurotrauma. 2026 Feb 28:():8977151261424705. doi: 10.1177/08977151261424705. Epub 2026 Feb 28 [PubMed PMID: 41761850]
Farruggia S, Babcock DS. The cavum septi pellucidi: its appearance and incidence with cranial ultrasonography in infancy. Radiology. 1981 Apr:139(1):147-50 [PubMed PMID: 7208915]
Wang KC, Fuh JL, Lirng JF, Huang WC, Wang SJ. Headache profiles in patients with a dilatated cyst of the cavum septi pellucidi. Cephalalgia : an international journal of headache. 2004 Oct:24(10):867-74 [PubMed PMID: 15377318]
Fratzoglou M, Grunert P, Leite dos Santos A, Hwang P, Fries G. Symptomatic cysts of the cavum septi pellucidi and cavum vergae: the role of endoscopic neurosurgery in the treatment of four consecutive cases. Minimally invasive neurosurgery : MIN. 2003 Aug:46(4):243-9 [PubMed PMID: 14506571]
Level 3 (low-level) evidenceSener RN. Cysts of the septum pellucidum. Computerized medical imaging and graphics : the official journal of the Computerized Medical Imaging Society. 1995 Jul-Aug:19(4):357-60 [PubMed PMID: 8653673]
Tubbs RS, Krishnamurthy S, Verma K, Shoja MM, Loukas M, Mortazavi MM, Cohen-Gadol AA. Cavum velum interpositum, cavum septum pellucidum, and cavum vergae: a review. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2011 Nov:27(11):1927-30. doi: 10.1007/s00381-011-1457-2. Epub 2011 Jun 18 [PubMed PMID: 21687999]
Pearce JM. Some observations on the septum pellucidum. European neurology. 2008:59(6):332-4. doi: 10.1159/000121428. Epub 2008 Apr 11 [PubMed PMID: 18408379]
Coleridge-Smith P, Labropoulos N, Partsch H, Myers K, Nicolaides A, Cavezzi A. Duplex ultrasound investigation of the veins in chronic venous disease of the lower limbs--UIP consensus document. Part I. Basic principles. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2006 Jan:31(1):83-92 [PubMed PMID: 16226898]
Level 3 (low-level) evidenceFantasia I, Ciardo C, Bracalente G, Filippi E, Murru FM, Spezzacatene A, Bin M, Mendez Quintero O, Montaguti E, Lees C, Papanikolaou K, Pilu G, Prefumo F, Thilaganathan B, Stampalija T. Obliterated cavum septi pellucidi: Clinical significance and role of fetal magnetic resonance. Acta obstetricia et gynecologica Scandinavica. 2023 Jun:102(6):744-750. doi: 10.1111/aogs.14575. Epub 2023 Apr 14 [PubMed PMID: 37059118]
Karl K, Esser T, Heling KS, Chaoui R. Cavum septi pellucidi (CSP) ratio: a marker for partial agenesis of the fetal corpus callosum. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2017 Sep:50(3):336-341. doi: 10.1002/uog.17409. Epub 2017 Aug 9 [PubMed PMID: 28078790]
He M, Du L, Xie H, Lei T, Zheng Q, Wu L. The ratio of cavum septi pellucidi width to anteroposterior cerebellar diameter: A novel index as a diagnostic adjunct for prenatal diagnosis of trisomy 18. The journal of obstetrics and gynaecology research. 2019 Jul:45(7):1245-1250. doi: 10.1111/jog.13960. Epub 2019 Apr 1 [PubMed PMID: 30932268]
Trzesniak C, Oliveira IR, Kempton MJ, Galvão-de Almeida A, Chagas MH, Ferrari MC, Filho AS, Zuardi AW, Prado DA, Busatto GF, McGuire PK, Hallak JE, Crippa JA. Are cavum septum pellucidum abnormalities more common in schizophrenia spectrum disorders? A systematic review and meta-analysis. Schizophrenia research. 2011 Jan:125(1):1-12. doi: 10.1016/j.schres.2010.09.016. Epub 2010 Oct 20 [PubMed PMID: 20965698]
Level 1 (high-level) evidenceDegreef G, Lantos G, Bogerts B, Ashtari M, Lieberman J. Abnormalities of the septum pellucidum on MR scans in first-episode schizophrenic patients. AJNR. American journal of neuroradiology. 1992 May-Jun:13(3):835-40 [PubMed PMID: 1590179]
Chon MW, Choi JS, Kang DH, Jung MH, Kwon JS. MRI study of the cavum septum pellucidum in obsessive-compulsive disorder. European archives of psychiatry and clinical neuroscience. 2010 Jun:260(4):337-43. doi: 10.1007/s00406-009-0081-6. Epub 2009 Oct 25 [PubMed PMID: 19856198]
Level 2 (mid-level) evidenceTendulkar M, Tendulkar DR. Enlarged cavum septum pellucidum & increased incidence of schizophrenia: Narrative review for neurodevelopmental correlate. Psychiatry research. Neuroimaging. 2026 Apr:357():112134. doi: 10.1016/j.pscychresns.2025.112134. Epub 2026 Jan 1 [PubMed PMID: 41499820]
Level 3 (low-level) evidenceAmin BH. Symptomatic cyst of the septum pellucidum. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 1986:2(6):320-2 [PubMed PMID: 3829032]
Level 3 (low-level) evidenceJackowski A, Kulshresta M, Sgouros S. Laser-assisted flexible endoscopic fenestration of giant cyst of the septum pellucidum. British journal of neurosurgery. 1995:9(4):527-31 [PubMed PMID: 7576280]
Level 3 (low-level) evidenceTamburrini G, Mattogno PP, Narenthiran G, Caldarelli M, Di Rocco C. Cavum septi pellucidi cysts: a survey about clinical indications and surgical management strategies. British journal of neurosurgery. 2017 Aug:31(4):464-467. doi: 10.1080/02688697.2016.1229743. Epub 2016 Sep 13 [PubMed PMID: 27619551]
Level 3 (low-level) evidenceAl Hatmi A, Khan MN, Mehan U. Spontaneous Resolution of a Cavum Septum Pellucidum Cyst: A Rare Entity. The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques. 2025 Oct 8:():1-3. doi: 10.1017/cjn.2025.10446. Epub 2025 Oct 8 [PubMed PMID: 41058226]
Montaguti E, Soliani L, Montedoro C, Pizzoli C, Della Volpe F, Corsini C, Cordelli DM, Pilu G. Neurocognitive Assessment in Children With Prenatal Diagnosis of Apparently Isolated Obliteration of Cavum Septi Pellucidi. Prenatal diagnosis. 2026 Feb:46(2):176-182. doi: 10.1002/pd.70032. Epub 2025 Nov 29 [PubMed PMID: 41318951]