Introduction
The carotid sinus, also referred to as the "carotid bulb," is a neurovascular structure that appears as a dilation at the bifurcation of the common carotid artery (CCA). The structure is located inferior to the angle of the mandible at the level of the thyroid cartilage (see Image. Carotid Region Anatomy).
Baroreceptors (stretch receptors) within the carotid sinus are sensitive to changes in arterial blood pressure. Dense innervation by multiple receptor types contributes to the regulation of vascular tone and cardiac function. The carotid sinus baroreceptor plays a critical role in regulating blood pressure and heart rate.
Afferent signals from carotid baroreceptors travel to the cardiovascular control center in the medulla oblongata via the glossopharyngeal nerve (cranial nerve IX). Efferent signals are transmitted through parasympathetic and sympathetic pathways to the heart and blood vessels. This reflex pathway produces appropriate adjustments that maintain heart rate and blood pressure within normal physiological limits, a process termed the "carotid sinus baroreflex."[1] The carotid sinus demonstrates considerable interindividual and intraindividual variation in location, a feature of significant clinical importance.
Carotid sinus stimulation or injury can produce significant hemodynamic effects, including reflex bradycardia, hypotension, syncope, and a potential contribution to thromboembolic stroke in the presence of atheromatous disease. Procedures involving the carotid bifurcation, such as carotid endarterectomy (CEA), carotid stenting, or surgical denervation, require precise localization and careful handling to avoid exaggerated baroreflex responses, intraoperative instability, or postoperative complications. Detailed understanding of carotid sinus anatomy and physiology enables clinicians to anticipate reflex cardiovascular changes, perform interventions safely, and recognize carotid sinus hypersensitivity (CSH) and orthostatic hypotension.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The CCA ascends through the neck and bifurcates at the level of the upper thyroid cartilage into the internal (ICA) and external (ECA) carotid arteries on both sides. The carotid sinus, a neurovascular structure, appears as a dilatation of the arterial wall, most commonly at the origin of the ICA. This structure is located within the adventitial layer of the carotid bulb of the ICA.
The carotid sinus baroreceptor functions as a sensor that detects mechanical stretch in the carotid artery resulting from increases in arterial blood pressure. Two types of baroreceptors exist. Type 1 (dynamic) baroreceptors contain large myelinated A fibers, whereas type 2 (tonic) baroreceptors contain small A fibers and unmyelinated C fibers.
Baroreceptors in the carotid sinus and aortic arch transmit afferent signals via the glossopharyngeal nerve to the cardiovascular control center when mean arterial pressure (MAP) rises. Baroreceptor input targets the commissural, medial, dorsomedial, and dorsolateral subnuclei of the nucleus tractus solitarius in the brainstem.[2] This input stimulates parasympathetic activity and inhibits sympathetic activity. Increased parasympathetic output acts on the sinoatrial node to decrease heart rate, while reduced sympathetic tone lowers blood pressure. Consequently, elevated arterial pressure at the carotid sinus activates stretch receptors, producing reflex bradycardia and systemic vasodilatation.
The baroreceptor reflex plays a critical role in maintaining heart rate and blood pressure during postural changes.[3] Transitioning from the supine to the standing position causes pooling of 500 to 1000 mL of blood in the lower extremities and the splanchnic circulation. This pooling decreases venous return, resulting in reduced cardiac output and a subsequent drop in blood pressure.
Reduced arterial pressure decreases carotid sinus baroreceptor stretch. Reflex activation increases sympathetic outflow and decreases parasympathetic outflow, leading to elevated heart rate and systemic vasoconstriction, which raises blood pressure. Therefore, postural change from supine to standing produces only a modest decrease in systolic and diastolic blood pressure (5–10 mm Hg) and an increase in heart rate (10–25 bpm). Failure of the baroreceptor reflex produces a blood pressure drop exceeding 10 mm Hg upon assuming upright posture, a condition termed "orthostatic hypotension."
Baroreceptors in the carotid sinus and aortic arch represent the terminal endings of sensory nerve fibers that express multiple nonselective cation channels of the transient receptor potential (TRP) family.[4] TRP1 channels respond to mechanical stretch. Transmural pressure induces expansion of the vessel, generating an inward current that depolarizes the receptor and produces a receptor potential. The amplitude of this potential is proportional to the degree of vessel stretch.
Embryology
The CCA, the proximal segment of the ICA, and the carotid sinus originate from the 3rd pharyngeal arch.[5] The CCA develops from the proximal segment of the 3rd aortic arch, whereas the ICA and carotid sinus arise from the distal segment of the 3rd aortic arch.[6] The carotid sinus arises from ectoderm-derived neural-crest tissues in the 3rd pharyngeal arch region. Although the ICA undergoes substantial growth from childhood to young adulthood, the carotid sinus near the base of the artery becomes apparent only during the teenage years.[7][8]
Blood Supply and Lymphatics
The carotid sinus is a dilation at the base of the ICA. The adjacent carotid body is a fibrous-covered structure located posterior to the carotid bifurcation. Blood supply to the carotid sinus is provided by the vasa vasorum. Atherosclerotic plaques can stimulate serotonin release, which traverses the vasa vasorum of the carotid sinus and affects nerve cells, resulting in baroreceptor dysfunction.[9] Lymphatic drainage from the carotid sinus flows directly into the deep cervical lymph nodes contained within the carotid sheath.[10]
Nerves
The glossopharyngeal nerve primarily innervates the carotid sinus, particularly through the branch known as the sinus nerve of Hering.[11] Afferent fibers from this nerve synapse in the nucleus tractus solitarius of the medullary brainstem, which relays information to the autonomic nervous system to regulate MAP. The glossopharyngeal nerve is a mixed nerve, with its general visceral afferent component transmitting sensory signals from the carotid sinus (see Image. Hypoglossal, Vagus, and Glossopharyngeal Nerves in the Neck).[12][13]
Muscles
The carotid sinus is a highly sensitive structure capable of markedly altering blood pressure. Superficial muscles, such as the sternocleidomastoid (SCM), and deep neck muscles, particularly the suprahyoid group, provide protective coverage.[14][15] Tight SCM contraction or neck-position changes may compress the carotid sinus and alter baroreceptor activity. Such interference may produce syncope in patients with CSH, a mechanism that underlies carotid sinus massage and elicits cardioinhibitory and vasodepressor responses (see Image. Carotid Sinus Massage Technique).[16]
Physiologic Variants
The carotid sinus exhibits considerable interindividual and intraindividual variation in location.[17] Knowledge of these variations is essential for surgeons performing interventions, such as CEA or carotid stenting, because inadvertent stimulation can cause severe hypotension, bradycardia, or, in rare cases, cardiac arrest.
Four anatomical sites of the carotid sinus have been identified. Site 1 originates in the distal CCA and extends to the proximal ICA, representing the most common location (74.3%).[18] Site 2 begins in the distal CCA and extends to both the proximal ICA and proximal ECA (7.3%). Site 3 starts in the distal CCA without extending beyond the bifurcation (17.1%). Site 4 originates in the distal CCA and extends to the proximal ECA, representing the least common location (1.22%).[19]
Surgical Considerations
The carotid sinus is a frequent site for atheromatous plaque formation, increasing the risk of significant disability and fatal strokes. Detection and removal of such plaques are performed through procedures such as CEA.[20] The region also serves as a site for distinctive tumors, known as carotid bifurcation paragangliomas, which arise from the carotid bodies.[21] Surgical denervation in the vicinity of the carotid sinus may be required in cases of carotid sinus syndrome with symptoms unresponsive to medical therapy.[22] The SCM contributes to carotid sinus protection, and age-related changes in neck musculature and tissue compliance may unmask CSH.[23]
Clinical Significance
The carotid sinus exhibits high sensitivity to touch and pressure. The carotid bifurcation is a common site for atheromatous plaque formation, which can result in thromboembolic stroke.[24] Anatomical variation in carotid sinus location among individuals increases the risk of injury or unintended stimulation by angioplasty stents or balloons during interventions. Surgical damage to the carotid sinus can produce postoperative hemodynamic instability. Stimulation of the carotid sinus during procedures may precipitate coronary vasospasm and myocardial infarction. CEA typically involves desensitization of the carotid sinus through injection of a small volume of lidocaine into the carotid adventitia to prevent baroreceptor activation during the operation.[25]
Some individuals develop CSH or carotid sinus syncope.[26] CSH is defined by a pause in heart rate exceeding 3 seconds and a blood pressure drop greater than 50 mm Hg during carotid sinus massage. Clinical manifestations may include syncope, presyncope (lightheadedness), near-syncope, or unexplained falls, particularly in older individuals.[27]
CSH accompanied by these symptoms is termed "carotid sinus syndrome."[28] The condition occurs more frequently in older adults, especially men (approximately twice the prevalence in women), and in patients with atherosclerotic vascular disease, tumors in the carotid sinus region, or a history of neck surgery or irradiation.[29][30] The etiology may involve heightened sensitivity of peripheral receptors or abnormal central reflex responses. Stimulation of carotid sinus baroreceptors in affected individuals produces a greater-than-expected reduction in heart rate and blood pressure. Minor stimuli, such as shaving the neck, turning the head, or looking upward, may provoke syncope and loss of consciousness.
Diagnosis may be established by performing a carotid sinus massage, an external stimulation of baroreceptors.[31] The patient is placed in the supine position with the neck flexed, and gentle pressure is applied to a single carotid sinus for 5 to 10 seconds. The head-up tilt test demonstrates greater sensitivity than carotid sinus massage. Heart rate and blood pressure are monitored continuously using a beat-by-beat monitoring system.
Responses to stimulation may be cardioinhibitory (pause in heart rate exceeding 3 seconds), vasodepressor (blood pressure decrease greater than 50 mm Hg), or mixed. This procedure should be performed only in a controlled setting with resuscitation equipment available. Preprocedure ultrasound is essential to exclude thrombus or atheroma in the carotid artery, which could dislodge and cause cerebrovascular thromboembolism.
Carotid sinus massage may also help differentiate supraventricular tachycardia from ventricular tachycardia. Research indicates that carotid sinus massage improves diagnostic accuracy for coronary artery disease, with greater blood pressure and pulse drops observed in patients with more extensive coronary vessel involvement.[32]
Treatment
Asymptomatic individuals with a normal response to carotid sinus massage do not require intervention. Avoidance of positions or movements that may inadvertently stimulate carotid baroreceptors is recommended.
Symptomatic patients exhibiting a cardioinhibitory or mixed response may receive permanent cardiac pacing through implantation of a dual-chamber pacemaker, the preferred approach. Individuals with abnormal vasodilator responses may be treated with vasoconstrictor agents, such as midodrine.
Baroreflex activation therapy (eg, Barostim) has received approval for heart failure with reduced ejection fraction in selected patients.[33] Recent studies demonstrate regional variability in sympathetic drive modulation during carotid baroreceptor stimulation in chronic heart failure, indicating that responses are not uniform across vascular beds.[34]
Media
(Click Image to Enlarge)
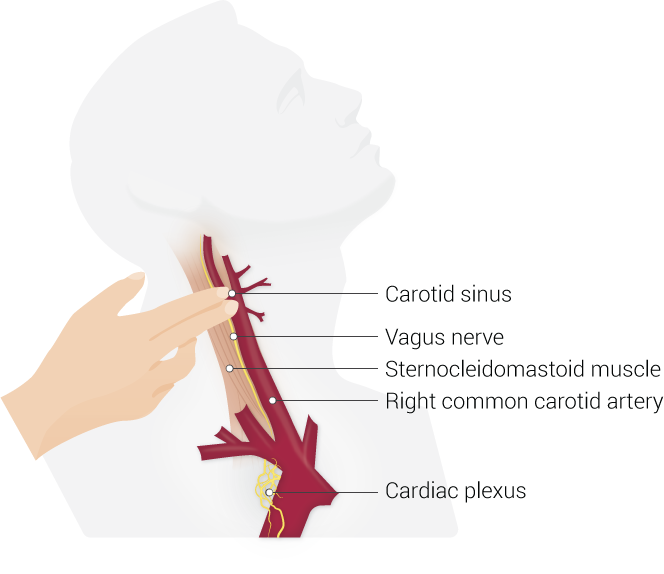
Carotid Sinus Massage Technique. The carotid sinus is identified at the bifurcation of the right common carotid artery, medial to the sternocleidomastoid muscle. Manual pressure here triggers the vagus nerve to send inhibitory signals to the cardiac plexus to lower the heart rate.
Illustrated by B Palmer
(Click Image to Enlarge)
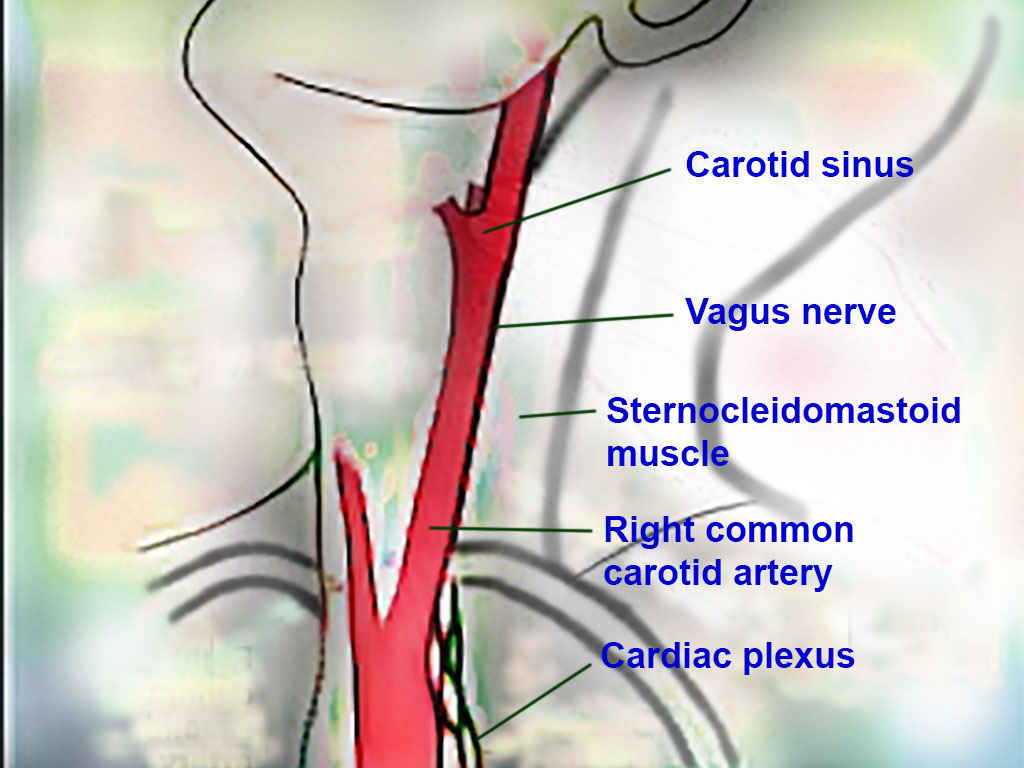
Carotid Region Anatomy. This image illustrates the carotid sinus, vagus nerve, sternocleidomastoid muscle, right common carotid artery, and cardiac plexus in the cervical region.
Contributed by T Silappathikaram, MD
(Click Image to Enlarge)
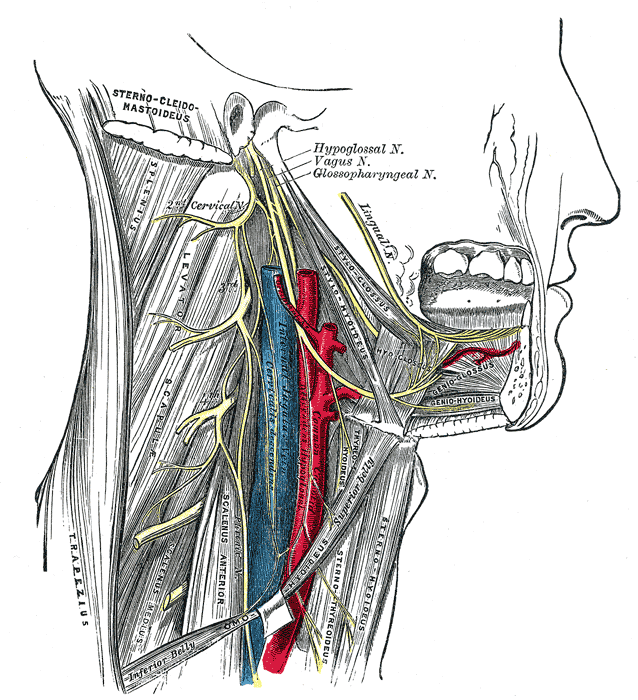
Hypoglossal, Vagus, and Glossopharyngeal Nerves in the Neck. This diagram shows the course of these cranial nerves in relation to the sternocleidomastoid, levator scapulae, scalenus anterior, geniohyoid, and stylohyoid muscles, as well as the cervical plexus, common carotid artery, and surrounding anatomical structures.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Kikuta S, Iwanaga J, Kusukawa J, Tubbs RS. Carotid Sinus Nerve: A Comprehensive Review of Its Anatomy, Variations, Pathology, and Clinical Applications. World neurosurgery. 2019 Jul:127():370-374. doi: 10.1016/j.wneu.2019.04.064. Epub 2019 Apr 14 [PubMed PMID: 30995553]
Porzionato A, Macchi V, Stecco C, De Caro R. The Carotid Sinus Nerve-Structure, Function, and Clinical Implications. Anatomical record (Hoboken, N.J. : 2007). 2019 Apr:302(4):575-587. doi: 10.1002/ar.23829. Epub 2018 May 2 [PubMed PMID: 29663677]
Silburn A. Counteracting microgravity: preserving cardiovascular health in low earth orbit. Military Medical Research. 2025 Sep 1:12(1):53. doi: 10.1186/s40779-025-00642-y. Epub 2025 Sep 1 [PubMed PMID: 40890798]
Numaga-Tomita T, Nishida M. TRPC3 and TRPC6: Multimodal Cation-Conducting Channels Regulating Cardiovascular Contractility and Remodeling. Cells. 2026 Jan 14:15(2):. doi: 10.3390/cells15020144. Epub 2026 Jan 14 [PubMed PMID: 41597219]
Jozsa F, Munakomi S. Anatomy, Head and Neck: Carotid Arteries. StatPearls. 2026 Jan:(): [PubMed PMID: 31424822]
Kau T, Sinzig M, Gasser J, Lesnik G, Rabitsch E, Celedin S, Eicher W, Illiasch H, Hausegger KA. Aortic development and anomalies. Seminars in interventional radiology. 2007 Jun:24(2):141-52. doi: 10.1055/s-2007-980040. Epub [PubMed PMID: 21326792]
Seong J, Jeong W, Smith N, Towner RA. Hemodynamic effects of long-term morphological changes in the human carotid sinus. Journal of biomechanics. 2015 Apr 13:48(6):956-62. doi: 10.1016/j.jbiomech.2015.02.009. Epub 2015 Feb 12 [PubMed PMID: 25702250]
Seong J, Lieber BB, Wakhloo AK. Morphological age-dependent development of the human carotid bifurcation. Journal of biomechanics. 2005 Mar:38(3):453-65 [PubMed PMID: 15652543]
Williams JK, Orgren KI, Armstrong ML, Heistad DD. Vasa vasorum in the carotid sinus of atherosclerotic monkeys: implications for baroreceptor function. Atherosclerosis. 1989 Jul:78(1):25-32 [PubMed PMID: 2757684]
Level 3 (low-level) evidenceClapham R, O'Sullivan E, Weller RO, Carare RO. Cervical lymph nodes are found in direct relationship with the internal carotid artery: significance for the lymphatic drainage of the brain. Clinical anatomy (New York, N.Y.). 2010 Jan:23(1):43-7. doi: 10.1002/ca.20887. Epub [PubMed PMID: 19918869]
Bryant D, McCormack E, Cardona JJ, Chaiyamoon A, Shekhawat D, Reina F, Carrera A, Iwanaga J, Dumont AS, Tubbs RS. Histology and immunohistochemistry of the human carotid sinus nerve. Anatomy & cell biology. 2023 Dec 31:56(4):463-468. doi: 10.5115/acb.23.084. Epub 2023 Sep 12 [PubMed PMID: 37696755]
Joo W. Microsurgical anatomy of the glossopharyngeal nerve. Clinical anatomy (New York, N.Y.). 2024 Jul:37(5):486-495. doi: 10.1002/ca.24143. Epub 2024 Feb 21 [PubMed PMID: 38380502]
Ağırman E, Peksöz R, Uygur FA, Yıldırım M, Atamanalp SS, Aydın MD. The First Description of Auerbach Ganglia Injury by Acidic Blood Following Subarachnoid Hemorrhage: An Experimental Study. Neurogastroenterology and motility. 2026 Jan:38(1):e70214. doi: 10.1111/nmo.70214. Epub 2025 Dec 7 [PubMed PMID: 41353773]
Silawal S, Schulze-Tanzil G. The sternocleidomastoid muscle variations: a mini literature review. Folia morphologica. 2023:82(3):507-512. doi: 10.5603/FM.a2022.0045. Epub 2022 May 24 [PubMed PMID: 35607877]
Bhat NP, Sumalatha S, Shetty A, Prabhath S. A clinical perspective on the anatomical study of digastric muscle. Anatomy & cell biology. 2023 Dec 31:56(4):441-447. doi: 10.5115/acb.23.043. Epub 2023 Oct 6 [PubMed PMID: 37798015]
Level 3 (low-level) evidencede Lange FJ, de Jong JSY, van Zanten S, Hofland WPME, Tabak R, Cammenga M, Francisco-Pascual J, Russo V, Fedorowski A, Deharo JC, Brignole M. Carotid sinus massage in clinical practice: the Six-Step-Method. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2024 Nov 1:26(11):. doi: 10.1093/europace/euae266. Epub [PubMed PMID: 39397761]
Fazaldad N, Sirasanagandla SR, Al-Shuaili A, Mogali SR, Chandrasekaran R, Dhuhli HA, Al-Ajmi E. Anatomical Variations and Morphometry of Carotid Sinus: A Computed Tomography Study. Tomography (Ann Arbor, Mich.). 2025 Apr 7:11(4):. doi: 10.3390/tomography11040045. Epub 2025 Apr 7 [PubMed PMID: 40278712]
Baz RA, Scheau C, Rusali AC, Bordei P. Computed tomography-assessed variations of the carotid sinus. Surgical and radiologic anatomy : SRA. 2022 Feb:44(2):293-298. doi: 10.1007/s00276-021-02871-x. Epub 2022 Jan 30 [PubMed PMID: 35094129]
West CT, Brassett C, Gaunt ME. Variations in carotid sinus anatomy and their relevance to carotid interventions. Folia morphologica. 2018:77(4):693-697. doi: 10.5603/FM.a2018.0017. Epub 2018 Mar 3 [PubMed PMID: 29500893]
Hakimi A, Choi ES, Aziz FF, Aziz F. Evolution of Medical and Surgical Management of Carotid Disease from Carotid Endarterectomy to Transfemoral Carotid Stenting to TCAR. Annals of vascular surgery. 2025 Apr:113():311-318. doi: 10.1016/j.avsg.2024.09.042. Epub 2024 Sep 26 [PubMed PMID: 39332702]
Michalinos A, Chatzimarkos M, Arkadopoulos N, Safioleas M, Troupis T. Anatomical Considerations on Surgical Anatomy of the Carotid Bifurcation. Anatomy research international. 2016:2016():6907472. doi: 10.1155/2016/6907472. Epub 2016 Mar 7 [PubMed PMID: 27047690]
Toorop RJ, Scheltinga MR, Moll FL, Bleys RL. Anatomy of the carotid sinus nerve and surgical implications in carotid sinus syndrome. Journal of vascular surgery. 2009 Jul:50(1):177-82. doi: 10.1016/j.jvs.2009.03.029. Epub [PubMed PMID: 19563966]
Lloyd MG, Wakeling JM, Koehle MS, Drapala RJ, Claydon VE. Carotid sinus hypersensitivity: block of the sternocleidomastoid muscle does not affect responses to carotid sinus massage in healthy young adults. Physiological reports. 2017 Oct:5(19):. doi: 10.14814/phy2.13448. Epub 2017 Oct 16 [PubMed PMID: 29038360]
Li S, Cao S, Li P, Zhang F, Ren G, Wang X, Zhao J, Liu C, Gao Y, Xu J, Wang Y, Xia Z, Xu Y. Endothelial BMP6 Drives Hemodynamic-Dependent VSMCs Calcification in Carotid Atherosclerosis. Advanced science (Weinheim, Baden-Wurttemberg, Germany). 2026 Jan:13(2):e02801. doi: 10.1002/advs.202502801. Epub 2025 Oct 13 [PubMed PMID: 41082328]
Pauza AG, Thakkar P, Shen X, Felippe ISA, Roßmann K, Oya M, McBryde FD, Nakamura K, Broichhagen J, Hodson DJ, Pauza DH, Murphy D, Paton JFR. Melanocortin System Activates Carotid Body Arterial Chemoreceptors in Hypertension. Circulation research. 2025 Sep 12:137(7):967-982. doi: 10.1161/CIRCRESAHA.125.326394. Epub 2025 Aug 26 [PubMed PMID: 40874981]
Moosavi V, Paymard M. Carotid sinus hypersensitivity. The Medical journal of Australia. 2019 Apr:210(6):257-257.e1. doi: 10.5694/mja2.50056. Epub 2019 Mar 4 [PubMed PMID: 30829401]
van den Brink RB, de Lange FJ. [Carotid sinus massage is not a benign intervention]. Nederlands tijdschrift voor geneeskunde. 2017:161():D1312 [PubMed PMID: 28378703]
Sutton R. Carotid sinus syndrome: Progress in understanding and management. Global cardiology science & practice. 2014:2014(2):1-8. doi: 10.5339/gcsp.2014.18. Epub 2014 Jun 18 [PubMed PMID: 25405171]
Level 3 (low-level) evidenceTan MP, Newton JL, Reeve P, Murray A, Chadwick TJ, Parry SW. Results of carotid sinus massage in a tertiary referral unit--is carotid sinus syndrome still relevant? Age and ageing. 2009 Nov:38(6):680-6. doi: 10.1093/ageing/afp160. Epub 2009 Sep 7 [PubMed PMID: 19736287]
Level 2 (mid-level) evidenceKumar NP, Thomas A, Mudd P, Morris RO, Masud T. The usefulness of carotid sinus massage in different patient groups. Age and ageing. 2003 Nov:32(6):666-9 [PubMed PMID: 14600010]
Level 2 (mid-level) evidenceTomcsányi J, Tomcsányi K, Bózsik B. Electrical alternans exposed by carotid sinus massage. The American journal of medicine. 2026 Jan 24:():. pii: S0002-9343(26)00060-4. doi: 10.1016/j.amjmed.2026.01.015. Epub 2026 Jan 24 [PubMed PMID: 41587684]
Ulgen MS, Karadede A, Alan S, Toprak N. The value of hemodynamic changes induced by carotid sinus massage on the diagnosis of coronary artery disease. Angiology. 2001 Oct:52(10):703-9 [PubMed PMID: 11666135]
Letarte LA, Raje V, Feliberti JP, Antoine SM, Bindra AS, Yaranov DM, Yehya A, Garcia RA, Patel P, Fudim M, Howard B, Rao VN, Hicks A 3rd, Mahmood K, Gupta R, Rollins A, Alam A, McCann P, Raval NY, Succeeding with Innovation, Future Technologies in Heart Failure (SWIFT-HF) Collaborative. Beyond GDMT: bridging the therapeutic gap in heart failure. Heart failure reviews. 2025 Sep:30(5):855-868. doi: 10.1007/s10741-025-10512-3. Epub 2025 Apr 30 [PubMed PMID: 40304825]
Dell'Oro R, Quarti-Trevano F, Gronda E, Grassi G. Contrasting effects of carotid baroreceptor stimulation on regional sympathetic drive in chronic human heart failure. Clinical research in cardiology : official journal of the German Cardiac Society. 2024 Sep:113(9):1369-1372. doi: 10.1007/s00392-023-02270-9. Epub 2023 Jul 28 [PubMed PMID: 37505275]