Introduction
A bruit (French pronunciation “brooee”), unlike a murmur arising from coronary valves, represents a higher-pitched swooshing or whooshing sound auscultated over a noncardiac blood vessel, either an artery or a vein. Turbulent blood flow through a narrowed lumen produces this sound, most often when luminal narrowing exceeds 50% of the original cross-sectional diameter, primarily because of atherosclerotic plaque formation. Following the invention of the stethoscope (“chest scope”) by René Laënnec in 1816, who also introduced the terms auscultation, bruit, and rales, and the subsequent development of the binaural stethoscope by Arthur Leared and George Cammann by the mid-1850s, clinicians gained the ability to detect bruits over the anterior triangle of the neck where the carotid arteries course.[1][2] During the mid-20th century, identification of a carotid bruit on auscultation suggested increased stroke risk and stimulated interest in carotid bypass surgery for asymptomatic patients; however, contemporary evidence has challenged these perceived benefits. Large studies, including those involving older adult populations, demonstrate that many asymptomatic bruits fail to progress to stroke, and some resolve over time.[3]
In current practice, a carotid bruit functions as one component of a comprehensive clinical diagnostic index that also includes age, blood pressure, cholesterol levels, diabetes status, and smoking history. Among patients classified as high risk, additional evaluation with carotid duplex ultrasonography may remain appropriate, regardless of the presence or absence of a bruit on auscultation.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Atherosclerotic plaques commonly form within arteries arising from the aortic arch. Approximately 80% of these lesions localize at the bifurcation of the common carotid arteries.[5] During the physical examination, clinicians perform carotid artery auscultation to evaluate whether carotid stenosis may predispose a patient to stroke. Among patients with a 2 mm reduction in carotid artery luminal diameter, a carotid bruit appears in 70% to 89% of cases.[6]
Luminal narrowing, however, does not represent the sole cause of a carotid bruit. Cardiac valvular murmurs that radiate into the neck, cervical venous hums, and intracranial arteriovenous malformations may generate vascular sounds that resemble a carotid bruit.[5] Arterial tortuosity, kinking, and high-output physiologic states also can produce bruits in normal or minimally stenotic arteries. In thyrotoxicosis, a 5- to 10-fold increase in blood flow to an enlarged thyroid gland may lead to a systolic bruit heard directly over the glandular isthmus.[5] Rarely, a bovine-type aortic arch combined with compression of kissing carotid arteries by a retrosternal goiter may serve as the source of a carotid bruit.[7][8]
Extrinsic vascular compression causing occlusion, including carotid body tumors and carotid paragangliomas, has also been reported to generate carotid bruits.[5][9][10] Structural disruption of the arterial wall occurs in conditions, eg, carotid artery dissection and aneurysm, both of which have been associated with bruit formation.[11][12]
Inflammatory involvement of the carotid vessels, as seen in disorders, eg, Takayasu arteritis, may also produce a carotid bruit.[13] Arterial bruit now serves as a component of the updated classification criteria for Takayasu arteritis.[14] Nonsclerotic and noninflammatory disorders, including fibromuscular dysplasia, frequently involve the internal carotid arteries and may result in an incidental carotid bruit during examination. Cervical fibromuscular dysplasia typically follows an asymptomatic course.[15][16]
Epidemiology
A carotid bruit represents a nonspecific clinical finding with wide sensitivity ranging from 24% to 84%.[17] Approximately 5% of individuals aged 45 to 80 years without clinically significant internal carotid artery disease demonstrate a carotid bruit on examination.[18] Among patients with an audible carotid bruit, one-third have hemodynamically significant stenosis defined as 70% to 90% luminal narrowing. Conversely, among patients with high-grade carotid artery stenosis, only about half exhibit a bruit during carotid auscultation.[19][20]
A soft, early systolic sound emerges when the arterial lumen narrows by approximately 50%. As stenosis progresses toward 60%, the bruit increases in intensity and pitch and extends throughout systole. With further reduction of luminal diameter to 70% to 80%, the bruit may persist into early diastole. Progressive occlusion eventually reduces turbulent flow to a degree that fails to generate arterial wall vibrations, leading to attenuation or disappearance of the bruit.[5]
Carotid bruits also appear in approximately 20% of healthy children younger than 15 years. Nearly 22% of patients diagnosed with cervical fibromuscular dysplasia demonstrate carotid bruits, although most affected individuals remain asymptomatic.[21]
Pathophysiology
The bruit typically implies stenosis at or proximal to the area of auscultation. The auscultated sound is usually the result of turbulent, nonlaminar blood flow through a stenotic area. The turbulent flow creates vibrations in the arterial wall that transmit to the body surface, where auscultation is possible. Critical stenosis, however, occurs only when the cross-sectional area decreases to 70%, corresponding to a reduction in luminal diameter by half. The auscultatory quality and timing of the bruit change with the degree of stenosis and pressure gradients. (Please refer to the Epidemiology section for more information.)
History and Physical
Assessment of cerebrovascular risk begins with a thorough medical history followed by a focused physical examination. Patients undergoing evaluation for carotid bruits should assume a supine or seated position. During seated examinations, carotid palpation and auscultation achieve optimal accuracy when the clinician approaches from behind. With the patient’s chin directed straight forward, placement of either the stethoscope bell or diaphragm over each carotid artery should create a complete seal with the overlying skin.
The diaphragm facilitates detection of high-frequency sounds, including respiratory noises, and requires firm pressure against the skin, whereas the bell enhances perception of low-frequency sounds such as selected cardiac murmurs and vascular bruits when applied with light pressure. Clinicians then instruct the patient to hold a deep breath without performing a Valsalva maneuver for 10 to 20 seconds. Breath-holding minimizes extraneous sounds and enhances the audibility of a carotid bruit.[5]
Auscultation yields the most clinically relevant information when performed at the following 3 key locations:
- The proximal carotid artery, where the murmurs from the heart valves and great vessels radiate upward
- The common carotid artery bifurcation at the angle of the mandible (the usual site of plaque buildup)
- Over the orbit where carotid-cavernous fistulas occur [22]
Nonobstructive lesions typically generate a brief, low-pitched, rumbling bruit, whereas high-grade obstructive lesions more often produce a high-pitched, prolonged bruit that may extend into diastole.[23][24] Lesions associated with severe stenosis exceeding 90% commonly produce faint sounds or no audible bruit at all.[23]
Evaluation
Detection of a carotid bruit may prompt clinical suspicion for carotid artery disease, yet auscultation alone lacks sufficient sensitivity and specificity to establish a definitive diagnosis.[25] An electronic stethoscope with spectral analysis shows promise for identifying severe carotid stenosis, although limited sensitivity restricts reliable detection of atherosclerotic plaque.[26] Following recognition of a carotid bruit, clinicians must determine the need for additional diagnostic testing or specialty referral by integrating vascular risk factors with associated signs and symptoms suggestive of neurologic or vascular disease.
Diagnostic imaging modalities, including carotid duplex ultrasonography, computed tomography angiography, and magnetic resonance angiography of the head and neck, support confirmation of disease and delineation of vascular anatomy when surgical or endovascular intervention becomes a consideration.[27] Interprofessional collaboration with neurology and cardiology specialists is frequently employed to help guide comprehensive evaluation and management decisions.
Treatment / Management
Upon confirmation of carotid artery disease as the source of the carotid bruit, a management approach comprising medical and surgical treatment should be initiated based on the severity of stenosis, the presence or absence of neurological symptoms, and the patient's comorbidities. Surgical options include conventional endarterectomy or the minimally invasive TCAR (TransCarotid Artery Revascularization) procedure via open cut-down access to the proximal common carotid artery for sheath insertion, creating an arteriovenous shunt for flow reversal, and endovascular stent insertion.[28] (B2)
Although the common practice has been to provide longitudinal monitoring and aggressive medical management in asymptomatic carotid stenosis of 90% or less, in the well-anticipated multicenter CREST2 trial, carotid-artery stenting plus intensive medical management demonstrated a lower risk of a composite of perioperative stroke or death or ipsilateral stroke within 4 years than intensive medical management alone.[29] Furthermore, carotid endarterectomy did not produce any significant benefit in the CREST2 study, reaffirming the long-held belief.
Differential Diagnosis
Differential diagnosis for carotid bruit includes:
- Cardiac valvular murmurs
- Carotid artery vasculitis (Takayasu arteritis)
- Carotid body tumor (paraganglioma)
- Carotid dissection and aneurysm
- Goiter and thyrotoxicosis
- Carotid-venous fistula
- Cervical fibromuscular dysplasia
- Subclavian venous hum
Prognosis
While carotid bruits have been regarded as markers of generalized atherosclerosis, the data have failed to show them as strong predictors of cerebrovascular events. However, carotid bruit auscultation is a rapid, noninvasive assessment that may help identify patients who might benefit most from aggressive cardiovascular risk stratification and therapeutic interventions.[30]
Complications
The annual incidence of cerebrovascular accidents in people with asymptomatic bruits is about 1% to 3%.[19] Carotid artery disease contributes to 15% to 20% of all ischemic strokes.[31]
Consultations
Consultations typically requested for people with carotid bruit include neurology, vascular surgery, and cardiology.
Deterrence and Patient Education
Deterrence of adverse cerebrovascular outcomes in patients with a carotid bruit centers on risk modification rather than reliance on the auscultatory finding alone. Patient education should clarify that a carotid bruit does not reliably predict stroke or the severity of carotid artery disease, yet the finding often reflects underlying vascular risk that warrants attention. Clinicians play a key role in explaining the multifactorial nature of cerebrovascular risk, including the contributions of hypertension, hyperlipidemia, diabetes, smoking, and age, and in reinforcing that the absence or presence of a bruit does not equate to safety or danger in isolation. Clear communication reduces anxiety, discourages unnecessary expectations for invasive procedures, and promotes informed participation in care decisions.
Patient education should also emphasize the importance of aggressive lifestyle modification and adherence to evidence-based medical therapy when vascular risk factors exist. Counseling should address smoking cessation, dietary changes, physical activity, and adherence to antihypertensive, lipid-lowering, and antiplatelet therapies when indicated. Clinicians should individualize recommendations based on comorbidities and overall risk profile while stressing the long-term benefits of compliance. Ongoing follow-up and coordination with primary care, cardiology, and neurology support sustained risk reduction and reinforce preventive strategies aimed at lowering the likelihood of future cerebrovascular events.
Pearls and Other Issues
Asymptomatic carotid bruits are not infrequent, and their prevalence increases with age. The physical finding of carotid bruit on examination has low accuracy, and a bruit alone does not indicate carotid artery disease. However, if sensibly incorporated into the patient's clinical assessment and risk stratification, it remains a viable tool in identifying patients at risk for a neurovascular event.
Enhancing Healthcare Team Outcomes
Carotid bruits represent auscultatory sounds generated by turbulent blood flow within cervical vessels, most commonly associated with atherosclerotic narrowing of the carotid arteries but also arising from nonsclerotic, inflammatory, structural, or high-output states. Historically viewed as a strong marker of stroke risk, carotid bruits now function as a nonspecific clinical sign with limited sensitivity and specificity. Contemporary evidence supports interpretation of a bruit within a broader vascular risk assessment that includes age, blood pressure, lipid status, diabetes, and smoking. Proper auscultation technique and recognition of alternative causes remain essential, while confirmatory imaging and selective referral guide further evaluation and management.
Optimal care requires coordinated skills and strategies across the interprofessional team. Physicians, general practitioners, and advanced practitioners integrate history, physical examination, and risk stratification to determine the need for imaging or specialty referral. Nurses reinforce education, perform focused assessments, and monitor adherence to preventive strategies. Pharmacists optimize medical therapy and counsel on medication safety and compliance. Effective communication among cardiology, neurology, vascular specialists, and primary care ensures timely diagnosis, minimizes unnecessary interventions, and supports individualized risk reduction, enhancing patient safety, outcomes, and overall team performance.
Media
(Click Image to Enlarge)
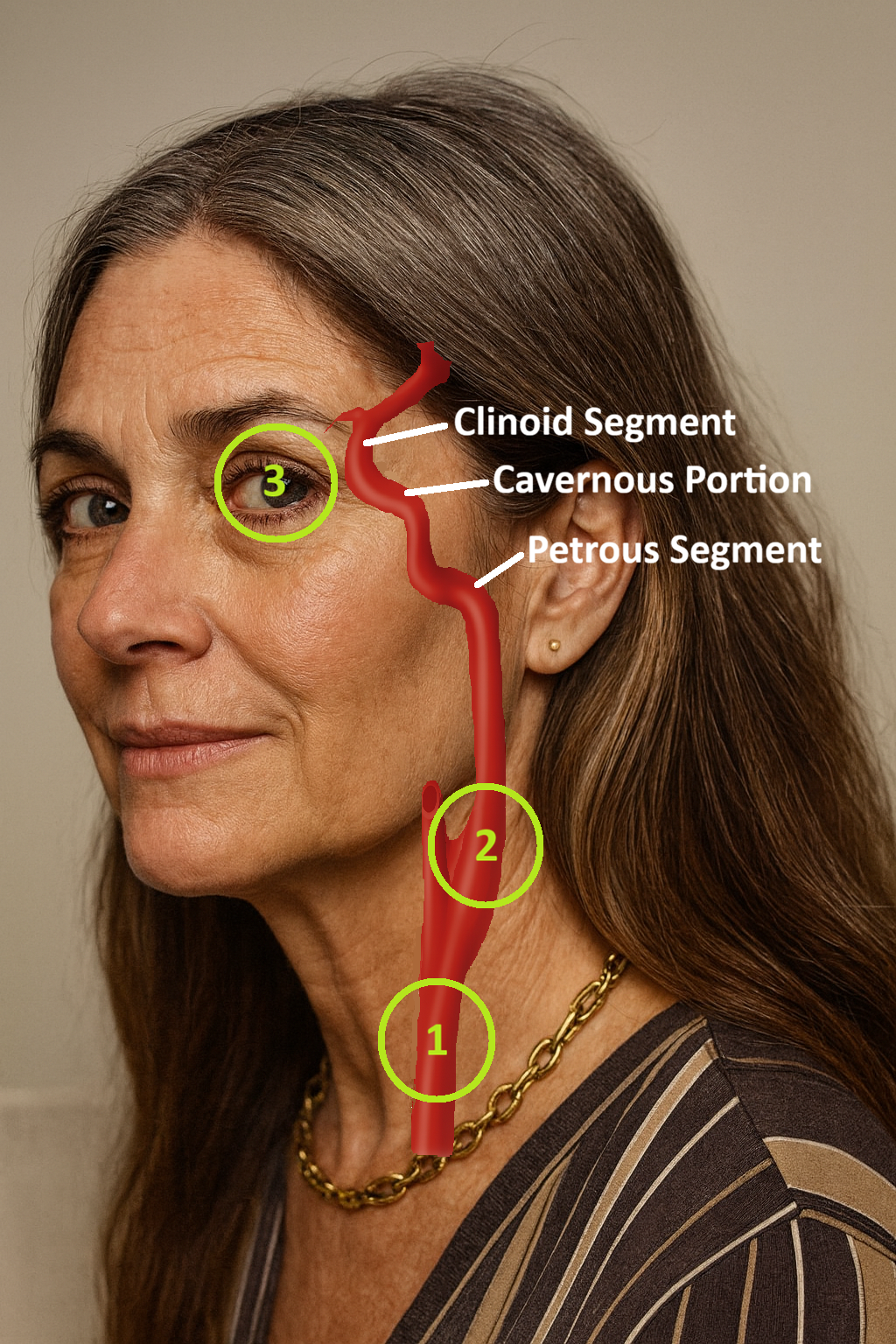
Bruit Assessment Sites. The 3 most frequent sites to assess for a bruit: (1) proximal to the upstroke of cardiac murmurs; (2) at the angle of the mandible and the carotid bifurcation; and (3) over the orbit to assess for carotid-cavernous fistula.
Contributed by R Benjamin, MD, MPH
References
Choudry M, Stead TS, Mangal RK, Ganti L. The History and Evolution of the Stethoscope. Cureus. 2022 Aug:14(8):e28171. doi: 10.7759/cureus.28171. Epub 2022 Aug 19 [PubMed PMID: 36148191]
Donoso F A, Arriagada S D. René Théophile Hyacinthe Laënnec (1781-1826). Two hundred years of the stethoscope. A brief overview. Archivos argentinos de pediatria. 2020 Oct:118(5):e444-e448. doi: 10.5546/aap.2020.eng.e444. Epub [PubMed PMID: 32924399]
Level 3 (low-level) evidenceVan Ruiswyk J, Noble H, Sigmann P. The natural history of carotid bruits in elderly persons. Annals of internal medicine. 1990 Mar 1:112(5):340-3 [PubMed PMID: 2306062]
Ratchford EV, Jin Z, Di Tullio MR, Salameh MJ, Homma S, Gan R, Boden-Albala B, Sacco RL, Rundek T. Carotid bruit for detection of hemodynamically significant carotid stenosis: the Northern Manhattan Study. Neurological research. 2009 Sep:31(7):748-52. doi: 10.1179/174313209X382458. Epub 2009 Jan 7 [PubMed PMID: 19133168]
Walker HK, Hall WD, Hurst JW, Kurtz KJ. Bruits and Hums of the Head and Neck. Clinical Methods: The History, Physical, and Laboratory Examinations. 1990:(): [PubMed PMID: 21250132]
Aronson L, Landefeld CS. Examining older people for carotid bruits: listen to your patient, not her neck. Journal of general internal medicine. 1998 Feb:13(2):140-1 [PubMed PMID: 9502377]
Aykan AÇ, Karadeniz A, Çavuşoğlu İG. Case Image: Bovine-type aortic arch and compression of the kissing carotid arteries by a retrosternal goiter: An uncommon cause of carotid bruit. Turk Kardiyoloji Dernegi arsivi : Turk Kardiyoloji Derneginin yayin organidir. 2018 Mar:46(2):165. doi: 10.5543/tkda.2017.23483. Epub [PubMed PMID: 29512622]
Level 3 (low-level) evidenceYagi T, Kawasaki T. Goiter, Bounding Pulses, and Thyroid Bruit in Thyroid Storm. The New England journal of medicine. 2025 Nov 6:393(18):e31. doi: 10.1056/NEJMicm2509136. Epub 2025 Nov 1 [PubMed PMID: 41181906]
Anand J, Singh JP. Bilateral sporadic carotid body tumors-A rare case report. Radiology case reports. 2018 Oct:13(5):988-992. doi: 10.1016/j.radcr.2018.07.001. Epub 2018 Aug 9 [PubMed PMID: 30116460]
Level 3 (low-level) evidencePeric B, Marinsek ZP, Skrbinc B, Music M, Zagar I, Hocevar M. A patient with a painless neck tumour revealed as a carotid paraganglioma: a case report. World journal of surgical oncology. 2014 Aug 20:12():267. doi: 10.1186/1477-7819-12-267. Epub 2014 Aug 20 [PubMed PMID: 25141773]
Level 3 (low-level) evidenceDemiryoguran NS, Karcioglu O, Topacoglu H, Aksakalli S. Painless aortic dissection with bilateral carotid involvement presenting with vertigo as the chief complaint. Emergency medicine journal : EMJ. 2006 Feb:23(2):e15 [PubMed PMID: 16439729]
Level 3 (low-level) evidenceJaha L, Ademi B, Rudari H, Vokrri L, Gjikolli B, Koshi A, Kuçi A, Jaha A. Surgical management of extracranial internal carotid artery aneurysm-Case report and literature review. Clinical case reports. 2023 Oct:11(10):e8015. doi: 10.1002/ccr3.8015. Epub 2023 Oct 3 [PubMed PMID: 37799567]
Level 3 (low-level) evidenceSilver M. Takayasu's Arteritis - An Unusual Cause of Stroke in a Young Patient. The western journal of emergency medicine. 2012 Dec:13(6):484-7. doi: 10.5811/westjem.2011.12.6881. Epub [PubMed PMID: 23359834]
Grayson PC, Ponte C, Suppiah R, Robson JC, Gribbons KB, Judge A, Craven A, Khalid S, Hutchings A, Danda D, Luqmani RA, Watts RA, Merkel PA, DCVAS Study Group. 2022 American College of Rheumatology/EULAR classification criteria for Takayasu arteritis. Annals of the rheumatic diseases. 2022 Dec:81(12):1654-1660. doi: 10.1136/ard-2022-223482. Epub 2022 Nov 9 [PubMed PMID: 36351705]
Plouin PF, Perdu J, La Batide-Alanore A, Boutouyrie P, Gimenez-Roqueplo AP, Jeunemaitre X. Fibromuscular dysplasia. Orphanet journal of rare diseases. 2007 Jun 7:2():28 [PubMed PMID: 17555581]
Dicks AB, Gornik HL, Gu X, Bacharach JM, Fendrikova Mahlay N, Froehlich JB, Gupta K, Gray BH, Kim ESH, Mahmood R, Sharma AM, Wells BJ, Olin JW, Weinberg I. Association of Fibromuscular Dysplasia and Pulsatile Tinnitus: A Report of the US Registry for Fibromuscular Dysplasia. Journal of the American Heart Association. 2021 Sep 7:10(17):e021962. doi: 10.1161/JAHA.121.021962. Epub 2021 Aug 28 [PubMed PMID: 34459232]
McColgan P, Bentley P, McCarron M, Sharma P. Evaluation of the clinical utility of a carotid bruit. QJM : monthly journal of the Association of Physicians. 2012 Dec:105(12):1171-7. doi: 10.1093/qjmed/hcs140. Epub 2012 Aug 11 [PubMed PMID: 22886230]
Level 1 (high-level) evidenceGrotta JC. Carotid stenosis. The New England journal of medicine. 2013 Dec 12:369(24):2360-1. doi: 10.1056/NEJMc1312990. Epub [PubMed PMID: 24328480]
Louridas G, Junaid A. Management of carotid artery stenosis. Update for family physicians. Canadian family physician Medecin de famille canadien. 2005 Jul:51(7):984-9 [PubMed PMID: 16060177]
Sauvé JS, Thorpe KE, Sackett DL, Taylor W, Barnett HJ, Haynes RB, Fox AJ. Can bruits distinguish high-grade from moderate symptomatic carotid stenosis? The North American Symptomatic Carotid Endarterectomy Trial. Annals of internal medicine. 1994 Apr 15:120(8):633-7 [PubMed PMID: 8135446]
Olin JW, Froehlich J, Gu X, Bacharach JM, Eagle K, Gray BH, Jaff MR, Kim ES, Mace P, Matsumoto AH, McBane RD, Kline-Rogers E, White CJ, Gornik HL. The United States Registry for Fibromuscular Dysplasia: results in the first 447 patients. Circulation. 2012 Jun 26:125(25):3182-90. doi: 10.1161/CIRCULATIONAHA.112.091223. Epub 2012 May 21 [PubMed PMID: 22615343]
Level 2 (mid-level) evidenceEkvtimishvil E, Meher A, Johnson J. Echoes of Trauma: DSA-Guided Coil Embolization for Carotid Cavernous Fistula Presenting with Ocular Bruit and Pulsatile Exophthalmos. Discoveries (Craiova, Romania). 2025 Jan-Mar:13(1):e203. doi: 10.15190/d.2025.2. Epub 2025 Mar 31 [PubMed PMID: 40351506]
Machleder HI. Strokes, transient ischemic attacks and asymptomatic bruits. The Western journal of medicine. 1979 Mar:130(3):205-17 [PubMed PMID: 371149]
Ochsner JL. Carotid bruit. The physician's dilemma. Postgraduate medicine. 1981 Oct:70(4):57-9, 62-6 [PubMed PMID: 7291094]
van der Worp HB, van Gijn J. Clinical practice. Acute ischemic stroke. The New England journal of medicine. 2007 Aug 9:357(6):572-9 [PubMed PMID: 17687132]
Malik AEF, Giudici A, Lubrecht JM, Prinzen FW, Delhaas T, Mess WH, Reesink KD. Spectral analysis of bruits with an electronic stethoscope enhances screening of carotid stenosis and plaques beyond conventional auscultation. Annals of translational medicine. 2025 Oct 31:13(5):55. doi: 10.21037/atm-24-191. Epub 2025 Oct 28 [PubMed PMID: 41211110]
Qaja E, Tadi P, Theetha Kariyanna P. Symptomatic Carotid Artery Stenosis. StatPearls. 2025 Jan:(): [PubMed PMID: 28723054]
Jim J, Dermody M, Peterson B, Berman SS, Mouawad NJ, Ricotta J, Saqib N, Faries P, Martin A, Adams JD, Tripathy U, Calderon D, O'Connor D, Shah R, Macdonald S, Schermerhorn ML. Prospective, Multicenter Evaluation of Transcarotid Artery Revascularization in Standard-Risk Patients: 30-Day Outcomes of the ROADSTER 3 Study. Annals of neurology. 2025 Nov 24:():. doi: 10.1002/ana.78104. Epub 2025 Nov 24 [PubMed PMID: 41277872]
Level 2 (mid-level) evidenceBrott TG, Howard G, Lal BK, Voeks JH, Turan TN, Roubin GS, Lazar RM, Brown RD Jr, Huston J 3rd, Edwards LJ, Jones M, Clark WM, Chamorro Á, Llull L, Mena-Hurtado C, Heck D, Marshall RS, Howard VJ, Moore WS, Barrett KM, Demaerschalk BM, Sangha N, Aronow H, Foster M, Sternbergh WC 3rd, Shawl F, Lanzino G, Rapp J, Tran HS, Ecker R, Mackey A, Ali V, Given C 2nd, Teal P, Kashyap VS, Mukherjee D, Harrigan M, Silverman S, Koopmann M, Wadley VG, Zhang Y, Rhodes JD, Chaturvedi S, Meschia JF, CREST-2 Investigators. Medical Management and Revascularization for Asymptomatic Carotid Stenosis. The New England journal of medicine. 2026 Jan 15:394(3):219-231. doi: 10.1056/NEJMoa2508800. Epub 2025 Nov 21 [PubMed PMID: 41269206]
Pickett CA, Jackson JL, Hemann BA, Atwood JE. Carotid bruits as a prognostic indicator of cardiovascular death and myocardial infarction: a meta-analysis. Lancet (London, England). 2008 May 10:371(9624):1587-94. doi: 10.1016/S0140-6736(08)60691-1. Epub [PubMed PMID: 18468542]
Level 1 (high-level) evidenceMughal MM, Khan MK, DeMarco JK, Majid A, Shamoun F, Abela GS. Symptomatic and asymptomatic carotid artery plaque. Expert review of cardiovascular therapy. 2011 Oct:9(10):1315-30. doi: 10.1586/erc.11.120. Epub [PubMed PMID: 21985544]