Introduction
The head and neck receive the majority of their arterial blood supply from the carotid and vertebral arteries. The common carotid arteries (CCAs) constitute the primary vessels delivering blood to the brain and face. The right CCA originates from the brachiocephalic artery in the neck, whereas the left CCA arises from the aortic arch in the thorax (see Images. Carotid Region Anatomy; Branches of the Aorta; Thyroid Arteries, Veins, and Muscles, Posterior View).[1] Both arteries bifurcate at the level of the carotid sinus into the internal carotid artery (ICA), which supplies intracranial structures, and the external carotid artery (ECA), which supplies the neck and face.[2]
The CCAs are critical landmarks in vascular, neurosurgical, and head-and-neck procedures, as inadvertent injury can result in cerebral ischemia or hemorrhage. Detailed knowledge of the carotid bifurcation, carotid sinus, and surrounding structures informs safe catheterization, endarterectomy, and trauma management. Mastery of the physiological and anatomical properties of these blood vessels allows clinicians to interpret findings from carotid auscultation, Doppler imaging, and blood pressure modulation accurately.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Like most vessels in the body, the CCAs consist of 3 layers. These layers are the tunica intima (inner layer), tunica media (middle layer), and tunica adventitia (outer layer). The tunica intima comprises endothelium supported by a delicate elastic layer and a collagenous layer of variable thickness. The tunica media consists of smooth muscle, which regulates vessel diameter, blood flow, and blood pressure. The tunica adventitia anchors the artery to the surrounding connective tissue.[3]
The CCAs originate posterior to the sternoclavicular joints and ascend within the carotid sheath, posterior to the sternocleidomastoid muscle.[4] At the upper border of the thyroid cartilage, typically at the level of the 4th or 5th cervical vertebra, each artery bifurcates into the ECA and ICA.[5] This bifurcation is clinically significant, as it contains the carotid body, a chemoreceptor, and the carotid sinus, a baroreceptor.
The carotid body responds to decreased partial pressure of oxygen (PO2), increased partial pressure of carbon dioxide (PCO2), and decreased pH, transmitting signals to adjust respiratory rate. The carotid sinus detects changes in arterial stretch, contributing to blood pressure regulation.[6] Following bifurcation, the ECA exits the carotid sheath to supply the face and neck, whereas the ICA remains within the sheath and enters the carotid canal of the temporal bone to supply intracranial structures.
The ECA possesses 8 branches that anastomose with branches of the contralateral ECA, providing collateral circulation. These branches include the following:
- Superior thyroid artery
- Ascending pharyngeal artery
- Lingual artery
- Facial artery
- Occipital artery
- Posterior auricular artery
- Maxillary artery
- Superficial temporal artery [7]
In contrast, the bilateral ICAs anastomose with branches of the basilar artery to form the circle of Willis.[8] At the circle of Willis, the ICA gives rise to the middle (MCA) and anterior (ACA) cerebral arteries. The MCA supplies the motor and sensory cortices of the upper limb and face, as well as the Wernicke area of the temporal lobe and the Broca area of the frontal lobe. The ACA supplies the motor and sensory cortices of the lower limb. The ophthalmic artery perfuses the inner retinal layers and also supplies structures within the orbit, meninges, face, and superior aspect of the nose.[9]
The ICA is divided into 4 segments according to its anatomical course: cervical, petrous, cavernous, and cerebral. The ophthalmic artery arises from the cavernous segment, whereas the MCA and ACA originate from the cerebral segment.[10]
In addition, the Bouthillier classification subdivides the ICA into 7 angiographic segments, C1 to C7, each giving rise to various branches. These branches are generally small, inconsistent, and may be absent, with the exception of the ophthalmic artery, which is present in nearly all cases.[11] The segmental description of this classification is outlined below (see Image. Skull Foramina).
- C1: Cervical segment
- Extends from the carotid bifurcation to the carotid canal
- No major branches
- C2: Petrous segment
- Traverses the petrous portion of the temporal bone
- Branches: Caroticotympanic artery, vidian artery
- C3: Lacerum segment
- Passes over the foramen lacerum; transitional segment
- No major branches
- C4: Cavernous segment
- Runs within the cavernous sinus
- Branches: Meningohypophyseal trunk, inferolateral trunk
- C5: Clinoid segment
- Between the proximal and distal dural rings (near the anterior clinoid process)
- No major branches
- C6: Ophthalmic (supraclinoid) segment
- Distal to the clinoid segment, proximal to the ICA bifurcation
- Branches: Ophthalmic artery, superior hypophyseal trunk
- C7: Communicating (terminal) segment
- Terminal portion of the ICA
- Branches: Posterior communicating artery, anterior choroidal artery, ACA, MCA [12]
The ICA segments delineate the anatomical origin of key cerebral and orbital arteries, highlighting areas prone to iatrogenic injury or vascular compromise (see Image. Carotid Artery Bifurcation and Intracranial Circulation). Familiarity with this segmental organization is indispensable for clinicians performing vascular imaging, surgical approaches, or interventional procedures.
Embryology
The embryological development of the carotid vascular system is complex (see Image. Embryologic Origins of Cranial and Cervical Arteries). During weeks 4 to 5 of gestation, the CCAs and proximal ICAs arise from the 3rd pharyngeal arch. The distal ICA originates from the dorsal aorta, whereas the ECA develops from the CCA through angiogenesis.[13]
Nerves
The glossopharyngeal nerve (CN IX) transmits baroreceptor afferent signals from the carotid sinus to the solitary nucleus of the medulla. The vagus nerve (CN X) courses posterolateral to the ICA and CCA and posteromedial to the internal jugular vein within the carotid sheath.[14]
Muscles
Understanding the vascular supply of the carotid arteries is essential for clinical practice. The maxillary and facial arteries, both branches of the ECA, supply the muscles of mastication. The facial artery also provides blood to the muscles of facial expression. The occipital artery, another ECA branch, perfuses the sternocleidomastoid, trapezius, and deep muscles of the back. The superficial temporal artery supplies the temporalis muscle. Branches of the ophthalmic artery, originating from the ICA, provide vascularization to the extraocular muscles.[15]
Physiologic Variants
The CCA typically bifurcates at the upper border of the thyroid cartilage. However, several studies report a variant in which the bifurcation occurs more distally.[16] This bifurcation is clinically significant, as it represents a common site of atherosclerosis, and a more distal bifurcation may influence the feasibility of standard surgical approaches.[17][18]
Rare case reports describe unilateral or bilateral agenesis, aplasia, or hypoplasia of the ICA and ECA. Collateral circulation is usually maintained via the circle of Willis.[19] Another variant, the retropharyngeal ICA, is generally asymptomatic but may present with atypical findings, including a submucosal pulsatile mass in the posterior pharynx, hoarseness, or respiratory compromise, depending on the medial displacement of the vessel.[20]
Surgical Considerations
The carotid arteries are essential for delivering oxygenated blood to the brain. Like all arteries, the carotids are susceptible to atherosclerosis, which may result in stenosis and distal embolization of plaque. Maintenance of cerebral perfusion is critical during aortic arch surgeries, and injury to the carotid arteries must be excluded in cases of penetrating neck trauma.
Atherosclerotic stenosis most commonly occurs at the bifurcation of the CCA into the ICA and ECA and represents a major cause of transient ischemic attack and stroke. Management typically involves optimized medical therapy. However, surgical intervention is indicated for patients who are asymptomatic with high-grade stenosis (70%–90%) or symptomatic with moderate (50%–69%) or high-grade stenosis. Surgical approaches include endovascular procedures, such as angioplasty and stenting, and open approaches, such as endarterectomy.[21]
Multiple clinical trials are ongoing to evaluate the efficacy of these approaches compared with each other and with optimized medical therapy. Selection of the appropriate modality depends on the degree of stenosis and the patient’s comorbid conditions, with consideration of the specific risks and benefits associated with each approach.[22][23][24]
Cerebral protection is essential during aortic arch repair. Techniques for neuroprotection include hypothermic circulatory arrest, retrograde cerebral perfusion, and antegrade selective cerebral perfusion via the carotid arteries. Evidence from existing studies supports hypothermic circulatory arrest and antegrade selective cerebral perfusion as preferred approaches, with retrospective reviews further validating their efficacy in reducing neurologic complications during aortic arch surgery.[25][26]
In cases of penetrating neck trauma, patients who become hemodynamically unstable or present with signs such as diminished carotid pulse, expanding hematoma, or active arterial bleeding require urgent surgical exploration.[27] Carotid artery injury occurs in an estimated 6% to 13% of penetrating neck traumas.[28] Arterial repair is strongly preferred, as it improves survival and reduces the risk of permanent neurologic deficits. Options for repair include primary repair, anastomosis, vein grafting, polytetrafluoroethylene patch, and transposition of the ECA to the injured ICA. Ligation is reserved for cases in which repair is not feasible but is associated with higher rates of mortality and neurologic complications, including stroke.[29]
Media
(Click Image to Enlarge)
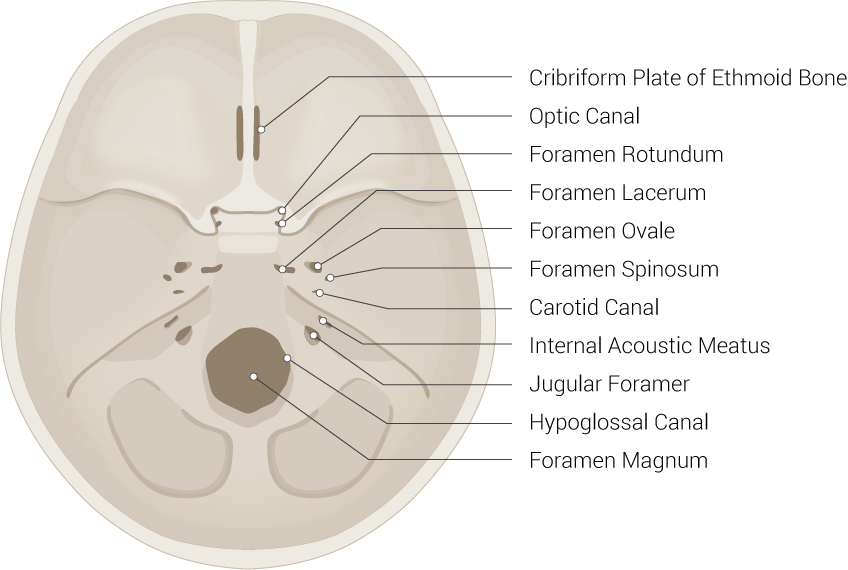
Skull Foramina. This illustration includes the cribriform plate of the ethmoid bone, optic canal, foramen rotundum, foramen lacerum, foramen ovale, foramen spinosum, carotid canal, internal acoustic meatus, jugular foramen, hypoglossal canal, and foramen magnum.
Illustrated by B Palmer
(Click Image to Enlarge)
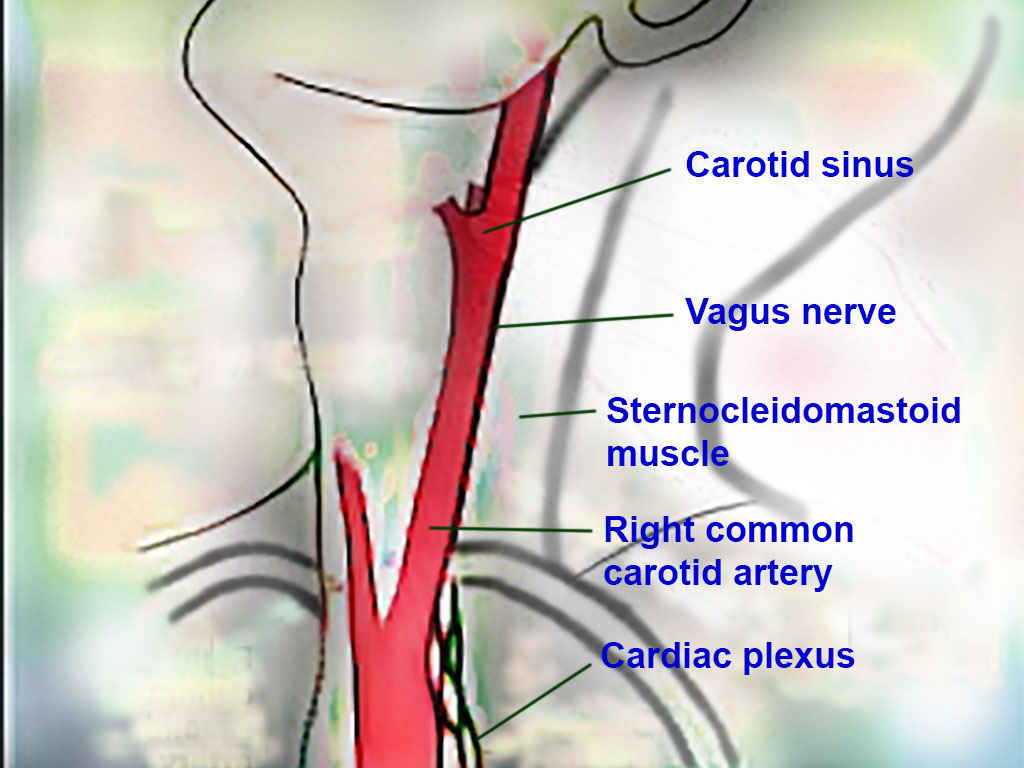
Carotid Region Anatomy. This image illustrates the carotid sinus, vagus nerve, sternocleidomastoid muscle, right common carotid artery, and cardiac plexus in the cervical region.
Contributed by T Silappathikaram, MD
(Click Image to Enlarge)
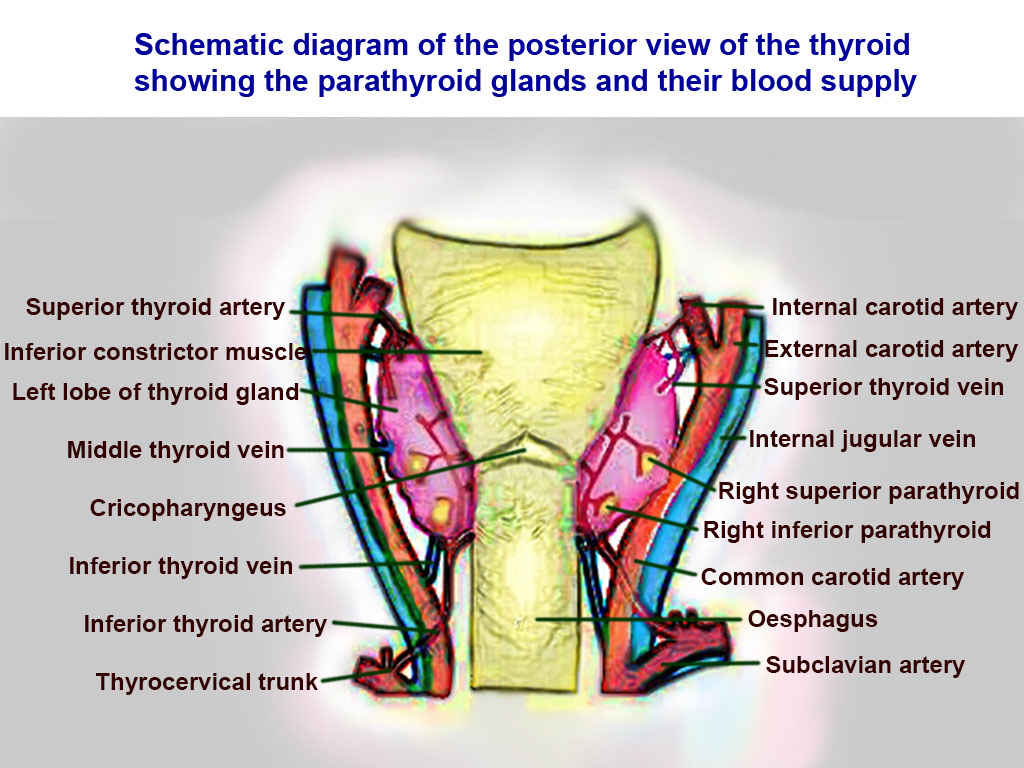
Thyroid Arteries, Veins, and Muscles, Posterior View. Structures include the superior thyroid artery, inferior thyroid artery, thyrocervical trunk, middle thyroid vein, inferior thyroid vein, internal carotid artery, external carotid artery, common carotid artery, internal jugular vein, cricopharyngeus muscle, inferior constrictor muscle, left lobe of the thyroid, esophagus, subclavian artery, right superior parathyroid, and right inferior parathyroid.
Contributed by T Silappathikaram, MD
(Click Image to Enlarge)
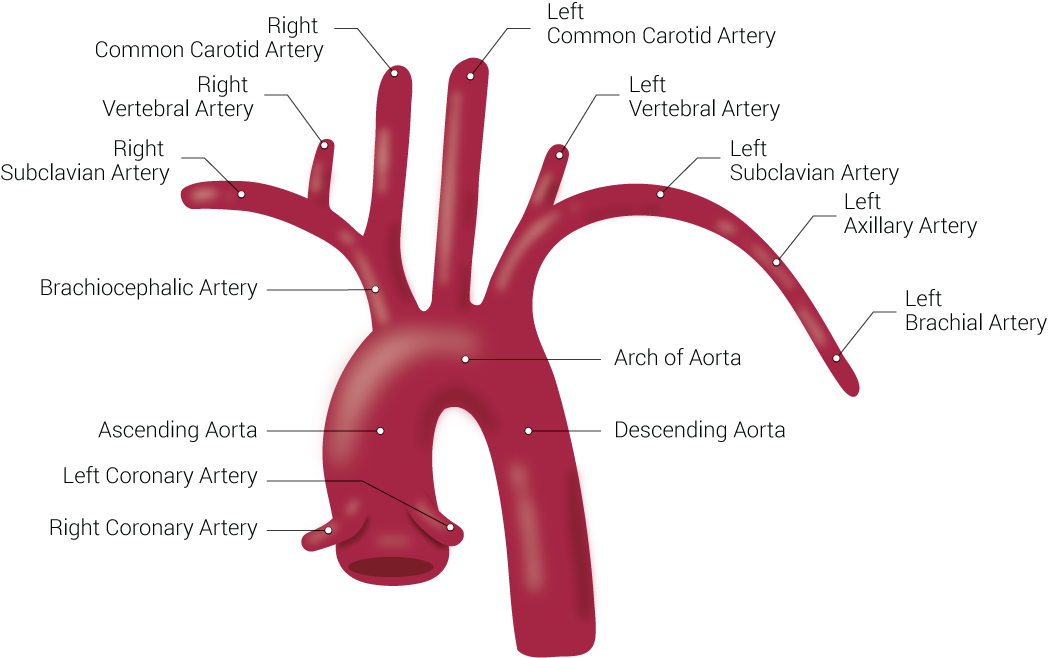
Branches of the Aorta. This illustration includes the right common carotid artery, right vertebral artery, right subclavian artery, brachiocephalic artery, ascending aorta, left coronary artery, right coronary artery, left common carotid artery, left vertebral artery, left subclavian artery, left axillary artery, left brachial artery, arch of aorta, and descending aorta.
Illustrated by B Palmer
(Click Image to Enlarge)
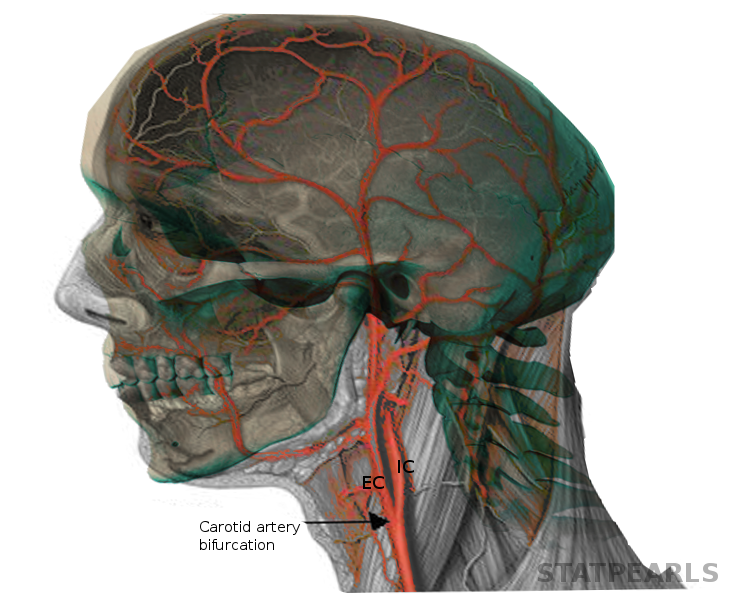
Carotid Artery Bifurcation and Intracranial Circulation. This image shows the carotid artery bifurcation into the external and internal carotid arteries and demonstrates their contribution to the intracranial arterial network.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
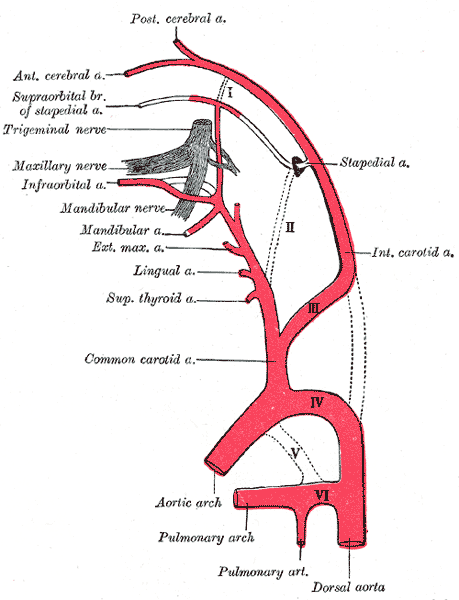
Embryologic Origins of Cranial and Cervical Arteries. The image depicts the posterior and anterior cerebral arteries, the supraorbital branch of the stapedial artery, the stapedial, infraorbital, mandibular, external maxillary, lingual, and superior thyroid arteries, and the common and internal carotid arteries, along with the aortic arch, pulmonary arch, pulmonary artery, dorsal aorta, and the trigeminal, maxillary, and mandibular nerves.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Choi IS. Functional vascular anatomy of the head and neck. Interventional neuroradiology : journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences. 2003 Oct 10:9(Suppl 2):29-30 [PubMed PMID: 20591274]
Omami G. Vascular Anatomy on Head and Neck Imaging. Oral and maxillofacial surgery clinics of North America. 2026 Feb:38(1):119-131. doi: 10.1016/j.coms.2025.08.012. Epub 2025 Oct 16 [PubMed PMID: 41107093]
Seidelmann SB, Lighthouse JK, Greif DM. Development and pathologies of the arterial wall. Cellular and molecular life sciences : CMLS. 2014 Jun:71(11):1977-99. doi: 10.1007/s00018-013-1478-y. Epub 2013 Sep 27 [PubMed PMID: 24071897]
Bond JD, Zheng F, Wang Q, Zhang M. The carotid sheath: Anatomy and clinical considerations. World neurosurgery: X. 2023 Apr:18():100158. doi: 10.1016/j.wnsx.2023.100158. Epub 2023 Jan 24 [PubMed PMID: 37081926]
Cobiella R, Quinones S, Konschake M, Aragones P, León X, Vazquez T, Sanudo J, Maranillo E. The carotid axis revisited. Scientific reports. 2021 Jul 5:11(1):13847. doi: 10.1038/s41598-021-93397-0. Epub 2021 Jul 5 [PubMed PMID: 34226652]
Salah HM, Gupta R, Hicks AJ 3rd, Mahmood K, Haglund NA, Bindra AS, Antoine SM, Garcia R, Yehya A, Yaranov DM, Patel PP, Feliberti JP, Rollins AT, Rao VN, Letarte L, Raje V, Alam AH, McCANN P, Raval NY, Howard B, Fudim M. Baroreflex Function in Cardiovascular Disease. Journal of cardiac failure. 2025 Jan:31(1):117-126. doi: 10.1016/j.cardfail.2024.08.062. Epub 2024 Sep 27 [PubMed PMID: 39341547]
Sasikumar N, S V, Raghunath G, Karunakaran B, S N, Ks PD, M K, G SN, Gurusamy K, Maria Francis Y. Morphometric Study and Branching Patterns of External Carotid Artery Using Computed Tomography Angiography Among the South Indian Population: A Retrospective Study. Cureus. 2023 Feb:15(2):e35624. doi: 10.7759/cureus.35624. Epub 2023 Feb 28 [PubMed PMID: 37007303]
Level 2 (mid-level) evidenceKızılgöz V, Kantarcı M, Kahraman Ş. Evaluation of Circle of Willis variants using magnetic resonance angiography. Scientific reports. 2022 Oct 20:12(1):17611. doi: 10.1038/s41598-022-21833-w. Epub 2022 Oct 20 [PubMed PMID: 36266391]
Wolman DN, Moraff AM, Heit JJ. Anatomy of the Intracranial Arteries: The Internal Carotid Artery. Neuroimaging clinics of North America. 2022 Aug:32(3):603-615. doi: 10.1016/j.nic.2022.04.006. Epub [PubMed PMID: 35843665]
Zhang Y, Yang W, Zhang H, Liu M, Yin X, Zhang L, Cheng K, Nan G, Li Y. Internal Carotid Artery and its Relationship with Structures in Sellar Region: Anatomic Study and Clinical Applications. World neurosurgery. 2018 Feb:110():e6-e19. doi: 10.1016/j.wneu.2017.09.145. Epub 2017 Oct 3 [PubMed PMID: 28986226]
Bouthillier A, van Loveren HR, Keller JT. Segments of the internal carotid artery: a new classification. Neurosurgery. 1996 Mar:38(3):425-32; discussion 432-3 [PubMed PMID: 8837792]
Ovalle Torres CS, Reyes Soto G, Campero Á, Castillo Rangel C, Gonzalez A, Cherian I, Núñez M, Perez LA, Nikolenko V, Espinosa Mora A, García Campos JA, Alonso RN, Rosario Rosario A, Nurmukhametov D, Encarnacion Ramirez MJ, Dorantes Argandar A. The trinity of the internal carotid artery: Unifying terminologies of the main classifications to improve its surgical understanding. Surgical neurology international. 2025:16():177. doi: 10.25259/SNI_27_2025. Epub 2025 May 16 [PubMed PMID: 40469375]
Level 3 (low-level) evidenceFrisdal A, Trainor PA. Development and evolution of the pharyngeal apparatus. Wiley interdisciplinary reviews. Developmental biology. 2014 Nov-Dec:3(6):403-18. doi: 10.1002/wdev.147. Epub 2014 Aug 29 [PubMed PMID: 25176500]
Level 3 (low-level) evidenceIturriaga R, Alcayaga J, Chapleau MW, Somers VK. Carotid body chemoreceptors: physiology, pathology, and implications for health and disease. Physiological reviews. 2021 Jul 1:101(3):1177-1235. doi: 10.1152/physrev.00039.2019. Epub 2021 Feb 11 [PubMed PMID: 33570461]
Siwetz M, Widni-Pajank H, Hammer N, Bruneder S, Wree A, Antipova V. Course and Relation of the Facial Vessels-An Anatomical Study. Medicina (Kaunas, Lithuania). 2024 May 13:60(5):. doi: 10.3390/medicina60050805. Epub 2024 May 13 [PubMed PMID: 38792988]
Mina V, Chrysikos D, Troupis T, Filippou D. Anatomical Variations of the Carotid Triangle: A Systematic Review. Cureus. 2025 Sep:17(9):e91547. doi: 10.7759/cureus.91547. Epub 2025 Sep 3 [PubMed PMID: 41049905]
Level 1 (high-level) evidenceDevadas D, Pillay M, Sukumaran TT. A cadaveric study on variations in branching pattern of external carotid artery. Anatomy & cell biology. 2018 Dec:51(4):225-231. doi: 10.5115/acb.2018.51.4.225. Epub 2018 Dec 29 [PubMed PMID: 30637155]
Abdalla M, Mohammed N, Abdallah R, Ahmed MK, Ismaiel M, Abdelrahim M, Salih A, Yousif E, Abdalla AA, Abdelrahim MA. Anatomical Variations of the Bifurcation Levels of the Common Carotid Artery and Superior Thyroid Artery. Cureus. 2024 Oct:16(10):e71120. doi: 10.7759/cureus.71120. Epub 2024 Oct 9 [PubMed PMID: 39386933]
Alexandre AM, Visconti E, Schiarelli C, Frassanito P, Pedicelli A. Bilateral Internal Carotid Artery Segmental Agenesis: Embryology, Common Collateral Pathways, Clinical Presentation, and Clinical Importance of a Rare Condition. World neurosurgery. 2016 Nov:95():620.e9-620.e15. doi: 10.1016/j.wneu.2016.08.012. Epub 2016 Aug 13 [PubMed PMID: 27535626]
Mousa AY, AbuRahma AF. Retropharyngeal internal carotid artery: a rare presentation with significant clinical implications. Annals of vascular surgery. 2013 Nov:27(8):1189.e1-4. doi: 10.1016/j.avsg.2013.02.023. Epub 2013 Aug 26 [PubMed PMID: 23988542]
Level 3 (low-level) evidenceNaylor R, Rantner B, Ancetti S, de Borst GJ, De Carlo M, Halliday A, Kakkos SK, Markus HS, McCabe DJH, Sillesen H, van den Berg JC, Vega de Ceniga M, Venermo MA, Vermassen FEG, Esvs Guidelines Committee, Antoniou GA, Bastos Goncalves F, Bjorck M, Chakfe N, Coscas R, Dias NV, Dick F, Hinchliffe RJ, Kolh P, Koncar IB, Lindholt JS, Mees BME, Resch TA, Trimarchi S, Tulamo R, Twine CP, Wanhainen A, Document Reviewers, Bellmunt-Montoya S, Bulbulia R, Darling RC 3rd, Eckstein HH, Giannoukas A, Koelemay MJW, Lindström D, Schermerhorn M, Stone DH. Editor's Choice - European Society for Vascular Surgery (ESVS) 2023 Clinical Practice Guidelines on the Management of Atherosclerotic Carotid and Vertebral Artery Disease. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2023 Jan:65(1):7-111. doi: 10.1016/j.ejvs.2022.04.011. Epub 2022 May 20 [PubMed PMID: 35598721]
Level 1 (high-level) evidencePuccinelli F, Roffi M, Murith N, Sztajzel R. [Management of carotid artery stenosis]. Revue medicale suisse. 2017 Apr 26:13(560):894-899 [PubMed PMID: 28727356]
Aday AW, Beckman JA. Medical Management of Asymptomatic Carotid Artery Stenosis. Progress in cardiovascular diseases. 2017 May-Jun:59(6):585-590. doi: 10.1016/j.pcad.2017.05.008. Epub 2017 May 21 [PubMed PMID: 28539213]
Paraskevas KI, Brown MM, Lal BK, Myrcha P, Lyden SP, Schneider PA, Poredos P, Mikhailidis DP, Secemsky EA, Musialek P, Mansilha A, Parikh SA, Silvestrini M, Lavie CJ, Dardik A, Blecha M, Liapis CD, Zeebregts CJ, Nederkoorn PJ, Poredos P, Gurevich V, Jawien A, Lanza G, Gray WA, Gupta A, Svetlikov AV, Fernandes E Fernandes J, Nicolaides AN, White CJ, Meschia JF, Cronenwett JL, Schermerhorn ML, AbuRahma AF. Recent advances and controversial issues in the optimal management of asymptomatic carotid stenosis. Journal of vascular surgery. 2024 Mar:79(3):695-703. doi: 10.1016/j.jvs.2023.11.004. Epub 2023 Nov 7 [PubMed PMID: 37939746]
Level 3 (low-level) evidenceMisfeld M, Mohr FW, Etz CD. Best strategy for cerebral protection in arch surgery - antegrade selective cerebral perfusion and adequate hypothermia. Annals of cardiothoracic surgery. 2013 May:2(3):331-8. doi: 10.3978/j.issn.2225-319X.2013.02.05. Epub [PubMed PMID: 23977602]
Keeling WB, Leshnower BG, Hunting JC, Binongo J, Chen EP. Hypothermia and Selective Antegrade Cerebral Perfusion Is Safe for Arch Repair in Type A Dissection. The Annals of thoracic surgery. 2017 Sep:104(3):767-772. doi: 10.1016/j.athoracsur.2017.02.066. Epub 2017 May 24 [PubMed PMID: 28551049]
Blitzer DN, Ottochian M, O'Connor J, Feliciano DV, Morrison JJ, DuBose JJ, Scalea TM. Penetrating Injury to the Carotid Artery: Characterizing Presentation and Outcomes from the National Trauma Data Bank. Annals of vascular surgery. 2020 Aug:67():192-199. doi: 10.1016/j.avsg.2020.03.013. Epub 2020 Mar 23 [PubMed PMID: 32217135]
Muñoz CA, Hadad AG, González P, Burgos A, Ordoñez CA, Serna JJ. Carotid artery penetrating trauma: Report of 4 cases and literature revision. International journal of surgery case reports. 2024 Aug:121():109940. doi: 10.1016/j.ijscr.2024.109940. Epub 2024 Jun 23 [PubMed PMID: 38971033]
Level 3 (low-level) evidenceLee TS, Ducic Y, Gordin E, Stroman D. Management of carotid artery trauma. Craniomaxillofacial trauma & reconstruction. 2014 Sep:7(3):175-89. doi: 10.1055/s-0034-1372521. Epub [PubMed PMID: 25136406]