Introduction
Candidiasis serves as the overarching term for a spectrum of fungal infections caused by yeasts of the genus Candida and represents the most common fungal infection worldwide. Candida species function as commensal organisms within the normal mycobiome, a fungal community that inhabits the skin, mucosal surfaces, and gastrointestinal tract. The mycobiome constitutes an essential component of the broader human microbiome. Disruption of microbial balance or impairment of host immune function allows Candida species to proliferate, invade host tissues, and produce clinical disease. The mycobiome plays a critical role in immune system development, metabolic regulation, and maintenance of microbial homeostasis. Alterations within this fungal community, referred to as mycobiome dysbiosis, have demonstrated associations with multiple disease states, including inflammatory bowel disease, liver disease, and certain malignancies.[1]
Most mild Candida infections result from localized overgrowth on mucous membranes secondary to changes in the normal microbiota, leading to conditions, eg, oropharyngeal candidiasis, esophagitis, mastitis, balanitis, and vulvovaginitis. Patients with impaired immune responses, including deficiencies in cell-mediated immunity, eg, acquired immunodeficiency syndrome (AIDS), neutropenia, or critical illness requiring intensive care unit (ICU) admission, may develop extensive mucosal disease, bloodstream infections, or invasive dissemination. Candida species exhibit adhesive properties that facilitate biofilm formation on endothelial surfaces, heart valves, osteoarticular structures, prosthetic devices, intravascular catheters, and central nervous system shunts.
Management strategies for candidiasis vary according to infection type and severity, the identified Candida species, and patient-specific health status and risk factors. This article presents a comprehensive overview of candidiasis, including risk factors, epidemiology, clinical manifestations, physical examination findings, diagnostic approaches, and management principles.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Over 200 species of Candida have been identified, with approximately 20 known to cause human infections.[2] Candida albicans (C albicans) is the predominant species worldwide and tends to be susceptible to most of the limited number of widely used antifungal antibiotics. Please see StatPearls' companion resource, "Candidemia," for further information. Several Candida species other than Candida albicans cause human disease and hold growing clinical significance. These organisms pose multiple challenges, including difficulty in clinical and microbiologic differentiation from C albicans, reduced susceptibility to commonly prescribed antifungal agents, and an increasing prevalence worldwide.[3][4] Recognition of nonalbicans Candida species remains essential for accurate diagnosis and effective management. The most common Candida species other than Candida albicans responsible for infections include:
- C glabrata (Nakaseomyces glabratus)
- C parapsilosis
- C tropicalis
- C krusei (Pichia kudriavzevii)
- C auris
- C guilliermondii
- C lusitaniae
- C dubliniensis
Candidiasis can generally be divided into superficial localized and deep-tissue invasive infections. The pathophysiology, clinical characteristics, management, and prognosis differ significantly for each.
Common Localized Candida Infections
Intertrigo
Intertrigo is an inflammatory condition of the epidermis that often becomes secondarily infected by Candida (see Images. Candida Intertrigo and Candida-Associated Intertrigo). Warm, moist regions of the skin, including the axilla, underlying areas of the breast, groin, and buttock folds, are most commonly involved. Diaper dermatitis is a common form of intertrigo. Please see StatPearls' companion resource, "Intertrigo," for further information.
Thrush
Oropharyngeal candidiasis is commonly seen in infants, older adults who wear dentures, people treated with antibacterials, and those treated with immunosuppressants. Individuals with impaired cellular immunity, eg, those with AIDS, are also at risk. In addition, individuals who use inhaled glucocorticoids for asthma or rhinitis are also at risk (see Image. Oropharyngeal Candidiasis). Please see StatPearls' companion resource, "Fungal Infections of the Oral Mucosa," for further information.
Esophageal Candidiasis
Esophageal candidiasis most commonly occurs in individuals with impaired cellular immunity, eg, those with AIDS (see Images. Candida Esophagitis and Candida Esophagitis Photomicrograph). However, other risk factors include cancer, diabetes mellitus, the use of proton pump inhibitors, chemotherapy, glucocorticoid use, recent antibiotic use, alcohol use, smoking, and peptic ulcer disease.[5][6] Before the advent of highly active antiretroviral therapy, HIV infection represented a significant risk factor. In immunocompetent people, the use of proton pump inhibitors represents a common risk factor.[7] Please see StatPearls' companion resource, "Esophageal Candidiasis," for further information.
Candidal Balanitis
Balanitis is an inflammation of the glans and foreskin, and most commonly occurs in uncircumcised men (see Image. Candida Balanitis). Candida is the most common cause of balanitis. Candida intertrigo is a risk factor in neonates and incontinent older adults. Additionally, diabetes in adults is an associated risk factor. Sexual transmission is a common source.[8] Please see StatPearls' companion resource, "Balanitis," for further information.
Vulvovaginal Candidiasis
Vulvovaginal candidiasis can occur due to hormonal changes, eg, pregnancy, oral contraceptive use, and menopause, as well as the treatment of infections (eg, bacterial vaginosis and trichomoniasis), which disrupts the microbiome in the vagina, allowing for Candida to overgrow (see Image. Vulvovaginal Candida Infection). C albicans is the etiology of approximately 40% to 90% of the cases, with the remainder due to species other than Candida albicans.[9] The use of products, eg, vaginal sprays, spermicides, and douches, can also increase the risk for vulvovaginitis, as well as wearing tight-fitting, wet, or perspiration-soaked clothing.[10] Please see StatPearls' companion resource, "Vaginal Candidiasis," for further information.
Mastitis
The relationship between Candida and mastitis is highly controversial.[11][12] Recent data indicate that bacteria, not yeast, are responsible for the majority of the cases of nipple and breast pain that may occur in nursing mothers. Candida cultured from the inflamed nipple and areola tissue in nursing women most likely represent commensal organisms that are present in the infant's oral cavity. Please see StatPearls' companion resource, "Acute Mastitis," for further information.
Invasive Candidiasis
Invasive candidiasis is a life-threatening infection that includes candidemia and can involve many organ systems (see Images. Candida Endocarditis and Invasive Candida Infection of the Kidney.[13][3] Please see StatPearls' companion resource, "Candidemia," for further information.
Risk factors for invasive candidiasis include:
- Premature birth
- Admission to an intensive care unit (ICU)
- Vascular catheters
- Total parenteral nutrition
- Gastrointestinal perforation and anastomotic leak
- Use of broad-spectrum antibacterials
- Hyperglycemia
- Immunosuppression
- Immunodeficiencies
- Hematologic malignancy
- Solid organ or hematopoietic stem cell transplants
- Severe burns
- Major trauma
Epidemiology
Candida infections are most prevalent at the extremes of age. Approximately 45% of neonates, 45% to 65% of healthy children, 30% to 45% of healthy adults, and 50% to 65% of adults who wear removable dentures are colonized with C albicans in the oral cavity. The colonization rate is even higher in certain populations, eg, individuals living in acute and long-term care facilities (65% to 88%), individuals with acute leukemia undergoing chemotherapy (90%), and individuals living with HIV (95%).[14] In most cases, candidiasis occurs from a Candida strain that is a part of an individual's mycobiome. However, acquisition of new strains, eg, in the hospital environment, can also occur.[15]
Superficial mucocutaneous Candida infections, eg, oropharyngeal candidiasis and diaper dermatitis, are prevalent in newborns, affecting approximately 10% to 20% of healthy infants at least once during the first few months of life.[16] Invasive infections are much less common, affecting neonates at a rate of approximately 5 to 10 cases per 100,000 live births.[17][18] Infections in neonates in the neonatal intensive care unit (NICU), particularly extremely low birth weight neonates, are more common.[19] C albicans accounts for approximately 50% to 60% of candidiasis in newborns, with C parapsilosis accounting for around 20% to 40% of cases.[20][21][22] Infections from other Candida species are less common. Infections caused by species other than Candida albicans tend to occur later in life and are more likely to be acquired in the hospital environment.[23]
Oral candidiasis develops in 9% to 31% of adults living with AIDS, and in 20% of individuals with cancer.[24] Up to 75% of women will have at least 1 episode of vulvovaginal candidiasis in their lifetime, with most episodes occurring during the reproductive years. Recurrent vulvovaginal candidiasis occurs in approximately 9% of women, with C albicans accounting for up to 90% of infections.[25] [9]
Globally, an estimated 1.5 million people develop candidemia or invasive candidiasis annually.[26] Approximately 25,000 cases of candidemia occur in the United States every year, with an estimated incidence of 7 cases per 100,000 persons.[27] In one survey, C albicans accounted for 37% of cases, followed by C glabrata (30%), C parapsilosis (14%), C tropicalis (6%), and C auris (0.4%).[28] Invasive candidiasis is associated with longer hospitalizations and higher costs. The annual economic burden in the United States is approximately $1.8 billion.[3]
Pathophysiology
Candidiasis develops following overgrowth of Candida species associated with breakdown of host immune defenses or localized disruption of the microbiome. This overgrowth promotes pathogenicity through multiple virulence factors, including surface adhesion molecules that facilitate attachment to host cells. Tissue invasion occurs through several mechanisms, including the secretion of enzymes that facilitate tissue damage and enable deeper penetration, as well as switching from the yeast form to the hyphal form.[29]
Candida vulvovaginitis likely occurs from the migration of yeast from the rectum to the perineal region with subsequent vaginal colonization. Progression from asymptomatic colonization to symptomatic infection reflects a combination of factors, including organism overgrowth, penetration of the superficial epithelium, host inflammatory responses, and Candida virulence factors.[30]
Candida colonization in the neonate is typically a result of vertical transmission from the mother. Heavy maternal colonization with Candida or vulvovaginal candidiasis at the time of birth has been shown to increase the chance of neonatal colonization, particularly in the context of vaginal delivery or prolonged duration of premature rupture of membranes.[31] Horizontal transmission from either health care workers or the hospital environment has also been shown to play an important role in neonatal Candida colonization.[32][33]
Invasive candidiasis in children and adults develops after Candida species gain access to the bloodstream and disseminate to target organs. The 3 main routes by which Candida species gain access to the bloodstream are translocation across the gastrointestinal mucosal barrier, which represents the most frequent mechanism, especially among neutropenic patients and individuals in the ICU, colonization of medical devices, including intravascular catheters, which serves as another major source of candidemia, and localized infection (eg, one involving the urinary tract).[34][35]
Histopathology
When Candida species invade superficial tissues, histopathology of biopsied sections will show predominantly spongiotic changes in the epidermis, including irregular acanthosis, mild spongiosis, and inflammatory changes. The distinguishing feature of the superficial epidermis is the presence of neutrophils in the stratum corneum and upper layers of the epidermis. A small collection of neutrophils (spongiform pustulation) may form, which resembles impetigo or psoriasis.[36]
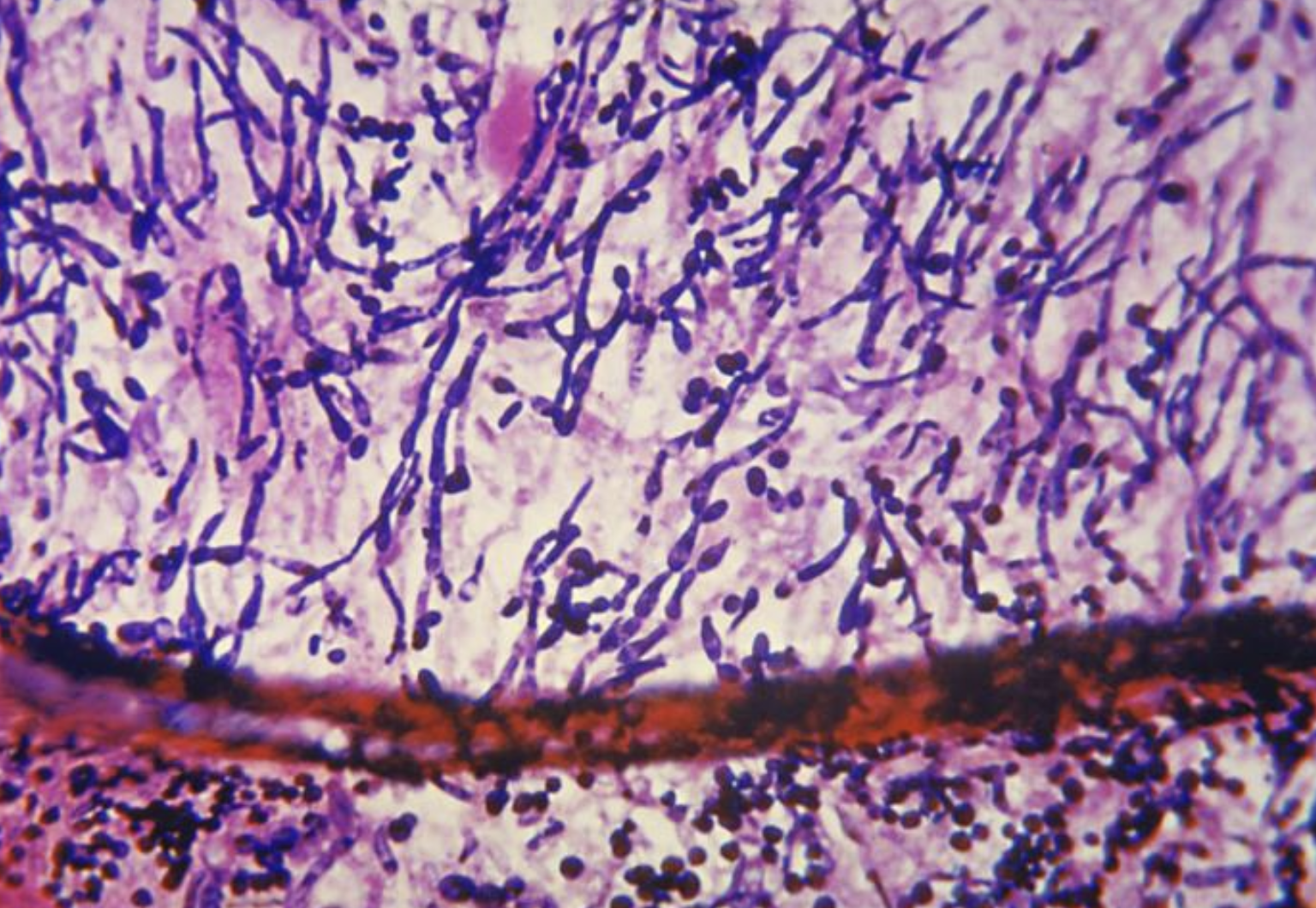
C albicans grows partly as yeast and partly as elongated cells resembling hyphae, which form pseudomycelium (see Image. Candida Albicans Skin Scraping and Candida Albicans Yeast Form With Germ Tube). C albicans can be identified from other Candida species by growth characteristics, sugar assimilation, and fermentation tests. It produces germ tubes within 2 hours when incubated in human serum at 37 °C.
History and Physical
The clinical features of candidiasis vary based on the site of infection.
Intertrigo
Regions of the skin that are prone to friction and hyperhidrosis initially demonstrate erythema on both sides of the skin folds. Pruritus often leads to excoriations that evolve into macerated, crusting, and weeping patches (see Images. Chorioretinal Candida Lesion and Candida-Associated Intertrigo).
Thrush
Individuals with oropharyngeal candidiasis may lack symptoms. When symptoms are present, patients may experience a cotton-like feeling in the mouth, a loss of taste or unpleasant taste, and angular cheilitis. Denture stomatitis typically presents with erythema and swelling underneath the dentures, often appearing as a red or red-and-white patch on the palate, gums, or buccal mucosa. Individuals with denture stomatitis often will experience some pain, and those with Candida infection of the larynx may experience hoarseness. On physical exam, white plaques are often visualized on the tongue, palate, buccal mucosa, and oropharynx (see Image. Oropharyngeal Candidiasis).
Esophageal Candidiasis
Esophageal candidiasis typically causes dysphagia or odynophagia, most commonly over the retrosternum. Oropharyngeal candidiasis is often present on exam as well.
Candidal Balanitis
Balanitis is often associated with burning and itching of the distal shaft of the penis near the glans or foreskin and can also involve the thighs, buttocks, and scrotum. Diabetes is a risk factor. On exam, erythema, white patches, or white exudate can be present (see Image. Candida Balanitis). Inflammation of the foreskin can lead to constriction of the foreskin over the glans penis (phimosis), or trapping of the foreskin behind the glans penis (paraphimosis), which is a urologic emergency.[8]
Vulvovaginal Candidiasis
Candida vulvovaginitis typically presents with vulvar itching, burning, and soreness. Dysuria and dyspareunia can also occur. Physical examination often reveals erythema of the vulva and vaginal mucosa. Excoriations and fissures of the vulva may be present. Vaginal discharge may be absent or copious, and when present, can range from thin and watery to white, thick, and clumpy (see Image. Vulvovaginal Candida Infection).
Invasive Candidiasis
An appreciation of the risk factors for invasive candidiasis is very important when reviewing a patient's history. Signs and symptoms of candidemia and invasive candidiasis can include skin pustules due to cutaneous dissemination of the yeast, chorioretinitis resulting from ocular dissemination, sepsis, and multiorgan system failure (see Image. Chorioretinal Candida Lesion).
Evaluation
Evaluation will vary based on the suspected site of infection.
Intertrigo
Intertriginous areas of skin characteristically include the skin folds between the buttocks, axillae, groin, and beneath the breasts. Erythema evolves into excoriated, macerated, and crusted patches. Diaper dermatitis is a common form of intertrigo.
Thrush
The diagnosis of oropharyngeal candidiasis is presumptively based on physical exam findings and risk factors. A definitive diagnosis is established by scraping the white plaques with a tongue depressor and performing a Gram stain or potassium hydroxide (KOH) preparation, which, on microscopy, reveals budding yeast with or without hyphae. Candida speciation, if needed, is determined by a fungal culture.
Esophageal Candidiasis
Esophageal candidiasis is typically diagnosed on upper endoscopy by visualization of white plaques attached to the mucosa. Microscopy of a biopsied sample will reveal yeast and hyphae invading mucosal cells (see Image. Candida Esophagitis Photomicrograph). Cultures can be performed on the biopsied tissue.
Candidal Balanitis
A presumptive diagnosis can often be made based on clinical appearance. Microscopic analysis of KOH or Gram stain smear of a skin scraping will reveal the typical yeast and pseudohyphal forms of Candida.
Vulvovaginal Candidiasis
In patients where Candida vulvovaginitis is clinically suspected, a sample of vaginal discharge can be collected for point-of-care testing with vaginal pH detection and microscopy. With Candida infections, vaginal pH is typically normal (4 to 4.5), which helps distinguish it from trichomoniasis and bacterial vaginosis, where the pH is typically greater than 4.5. Candida are often seen on a wet mount of the vaginal discharge after adding KOH, which destroys human cells and makes it easier to see budding yeast, pseudohyphae, and hyphae. However, microscopy is negative in up to 50% of patients with culture-confirmed Candida vulvovaginitis.[37] Alternatively, the vaginal discharge can be sent for a nucleic acid amplification test (NAAT), which is more sensitive than wet mount but has a longer turnaround time. In individuals with persistent or recurrent symptoms, cultures and antimicrobial sensitivity testing are indicated. Similar symptoms can result from a variety of etiologies, which should be considered among the differential diagnoses.[9]
Invasive Candidiasis
Positive blood cultures and tissue biopsies establish a diagnosis of candidemia and invasive candidiasis, respectively. A positive Candida blood culture should never be interpreted as a contaminant. Blood cultures may be negative in 30% to 50% of individuals with disseminated candidiasis.[38][39] Growth in blood cultures can be slow, and the turnaround time is further delayed during species identification and analysis of antifungal susceptibilities. Certain species other than Candida albicans, eg, C glabrata, grow significantly more slowly in culture.[40] The absence of growth and the lag in identification contribute to delays in diagnosis and the initiation of therapy. Prior exposure to antifungals contributes to false-negative blood cultures. Thus, non-culture-based methods are increasingly being utilized.
Beta-D-glucan (BDG), a component of the Candida cell wall, can be detected in an assay of blood. BDG is also present in other fungi; the BDG assay has sensitivities of 70% to 80% and specificities of 55% to 80%, respectively.[41] A false positive BDG assay may result from a variety of causes, including bacterial infections, beta-lactam antibiotics, hemodialysis, immunoglobulin, albumin, bowel ischemia, mucositis, gauze bandages, extensive burns, uremia, and liver failure.[42] Matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF-MS) can reduce the time to speciate and obtain susceptibilities from positive blood cultures.[43] Peptide nucleic acid-fluorescence in situ hybridization (PNA-FISH) is capable of identifying Candida species directly from positive blood cultures within 1.5 hours.[44] Molecular methods, including NAAT and the T2Candida assay, are rapid, nonculture diagnostic technologies with high sensitivity and specificity.[45][46] Mouratidou et al provide an excellent, detailed discussion of diagnostic techniques.[47]
Treatment / Management
Intertrigo
Intertrigo treatment involves minimizing the causes of the skin irritation and inflammation. This may include the use of drying agents, loose clothing, anti-persperants, petrolatum ointment, and absorbent diapers. The use of topical and oral antifungal agents may be required in severe and recalcitrant cases. Please see StatPearls' companion resource, "Intertrigo," for further information.
Thrush
The topical agents, nystatin, clotrimazole, and miconazole, are recommended for mild cases of oropharyngeal candidiasis. For moderate-to-severe cases, oral fluconazole is recommended. Itraconazole oral solution, posaconazole suspension, voriconazole, and isavuconazole are used to treat fluconazole-resistant Candida. Amphotericin B oral suspension has been used to treat azole-resistant infections. The echinocandins are an option for severe and recalcitrant thrush.
The choice of antifungal agent and the duration of therapy should be based on pharmacologic principles that consider potential drug interactions, pregnancy and lactation, cost, and the patient's immune status.[48] Please see StatPearls' companion resource, "Antifungal Agents," for further information on antifungal therapies. Inhaled glucocorticoids are a risk factor for thrush, and patients should be instructed to rinse with water immediately after use.[49] Dentures should be properly fitted and disinfected after use.[50] Please see StatPearls' companion resource, "Fungal Infections of the Oral Mucosa," for further information.(B3)
Esophageal Candidiasis
Treatment requires systemic antifungals. If tolerated, oral fluconazole is preferred and is generally given daily for 14 to 21 days. For patients unable to take oral medications, intravenous administration is required. In cases of fluconazole resistance or a recalcitrant infection, other azoles, echinocandins, and amphotericin B are alternative options. As noted above, the choice of therapy should be individualized and based on sound pharmacologic principles. When possible, efforts to minimize exposure to antibacterials and immunosuppressants should be attempted.[51]
Candidal Balanitis
Either topical or oral antifungals are recommended for treatment. A single oral dose of fluconazole was found to be equivalent to a 7-day multiple-dose regimen of clotrimazole ointment.[52] The single-dose strategy led to improved compliance and overall response. Proper hygiene should be encouraged. In recalcitrant cases, consideration should be given to the presence of fluconazole-resistant Candida, and antifungal therapy should be modified on that basis.
Vulvovaginal Candidiasis
Both topical and oral azole antifungal agents are equally efficacious in the treatment of uncomplicated vulvovaginal candidiasis.[53] A 3-day course of topical treatment is recommended. Oral azole antifungals should be avoided in pregnancy due to concerns about teratogenicity, whereas topical azoles are safe to use. Approximately 10% of women who have had an episode of vulvovaginal candidiasis will experience a recurrence, and more than 50% of that population will experience additional recurrences after completing courses of maintenance therapy.(B3)
Confirming that their symptoms are, in fact, due to Candida and obtaining antifungal sensitivities is key to management. Infections due to non-albicans Candida are increasing in frequency. Fluconazole is commonly used in this setting, and long-term suppressive therapy lasting several months is recommended. Oteseconazole is a new azole that is indicated for recurrent Candida vulvovaginitis.[54] This medication has a half-life of 138 days, retains activity against many fluconazole-resistant Candida species, and may be a preferred azole agent in this setting. Ibrexafungerp, a new oral beta-D-glucan synthase inhibitor, has been approved for treatment.[55] This medication achieves high vaginal concentrations, is active against fluconazole-resistant Candida, and is effective in treating recurrences; however, Ibrexafungerp is not approved for treatment in pregnant women. Please see StatPearls' companion resource, "Vaginal Candidiasis," for further information.
Invasive Candidiasis
Detailed treatment recommendations are beyond the scope of this article due to the variety of Candida species, their antifungal susceptibility profiles, the diverse characteristics of the host, the source of the Candida, and the varying complexities of the infection. Excellent, published treatment guidelines are recommended.[56][57][58] While C albicans is the predominant species of infection in many parts of the world, non-albicans Candida can predominate in several geographic regions; they are increasing in prevalence worldwide and vary in their antifungal susceptibilities. Adding to the complexity of treatment are the cumulative delays associated with Candida growth in culture (assuming they grow in the first place), speciation, and antifungal susceptibilities. (Please refer to the Evaluation section for more information on Candida culture.)(A1)
In general, several strategies are designed to initiate treatment as promptly as possible, including antifungal prophylaxis for high-risk patients, empiric therapy administered before Candida is identified, and targeted therapy once the organism and its susceptibility are confirmed.[58] Please see StatPearls' companion resource, "Antifungal Agents," "Candidemia," "Candida auris," "Febrile Neutropenia," "Fungal Endopthalmitis," "Fungal Endocarditis," "Renal Abscess," and "Splenic Abscess," for further information.
Prophylactic antifungal treatment
Prophylaxis is recommended for newborns weighing less than 1000 g, patients experiencing prolonged neutropenia, critically ill patients with gastrointestinal perforation or anastomotic leak, and solid organ and hematopoietic transplant patients. In low-weight neonates, fluconazole prophylaxis is recommended. Patients receiving cytoreductive chemotherapy are at risk of invasive candidiasis due to drug-induced mucosal damage as well as the presence of central vascular access catheters. Prophylaxis with either fluconazole or voriconazole is recommended during the duration of neutropenia.
Antifungal prophylaxis is recommended for critically ill patients in the intensive care unit (ICU) who have any of the following: gastrointestinal perforation, anastomotic leak, solid organ transplant, or hematopoietic transplant.[47] Fluconazole prophylaxis is recommended unless there has been recent exposure or high rates of azole resistance in the ICU, in which case echinocandins should be used.
Empiric therapy
Empiric therapy is initiated in high-risk patients with suspected candidemia while awaiting culture results. Patients with neutropenia who remain persistently febrile despite receiving prophylactic azoles and broad-spectrum antibacterials should receive an echinocandin. Liposomal amphotericin B is an alternative if echinocandins are unavailable or not tolerated. High-risk, critically ill nonneutropenic patients should be carefully assessed for surrogate markers of invasive candidiasis, including yeast colonization and the BDG assay.
In the presence of unexplained fever or sepsis despite broad-spectrum antibacterial therapy, echinocandin antifungal therapy should be considered because of its broad antifungal activity and safety profile.[59][57] Fluconazole is an acceptable alternative if the patient has not received recent azole therapy and when the prevalence of azole-resistant Candida is low. Liposomal amphotericin B is an acceptable alternative when echinocandins are unavailable or not tolerated. Clinicians should note that, currently, no studies have demonstrated a definite mortality benefit in the cohort of critically ill patients who receive preemptive antifungal therapy. Clinical risk prediction scores are being assessed in an effort to identify patients most likely to benefit from empiric and preemptive therapy.[60][61](A1)
Targeted therapy
In neonates with invasive candidiasis, amphotericin B deoxycholate is recommended as initial treatment. Fluconazole is an alternative for neonates who have not received azole prophylaxis. Neonates with candidemia should have an ophthalmic exam and a lumbar puncture. For the treatment of neonatal central nervous system Candida infections, either amphotericin B deoxycholate or liposomal amphotericin B is recommended as initial therapy. Fluconazole can be administered as step-down therapy should azole-sensitive Candida be identified.[57](A1)
In neutropenic patients with candidemia, echinocandins are recommended. Liposomal amphotericin B is an acceptable alternative, although comparatively higher rates of toxicity should be anticipated. In patients who have not received azole prophylaxis and when the prevalence of azole resistance is low, fluconazole is an acceptable alternative. A transition from echinocandins or liposomal amphotericin B to fluconazole can be made if the candidemia is subsequently found to be susceptible and blood cultures have turned negative.[57] Central vascular catheters should be removed as soon as feasible if they are considered a potential source of infection. (A1)
Echinocandins should be considered first-line therapy in nonneutropenic patients with candidemia and invasive candidiasis. Liposomal amphotericin B is an acceptable alternative if the Candida is likely to be resistant to echinocandins and azoles. The transition from an echinocandin or liposomal amphotericin B to fluconazole should be considered if the Candida is susceptible and follow-up blood cultures are negative. A central vascular catheter should be removed if the catheter is likely to be the source of the infection. Patients with candidemia should receive an ophthalmologic examination. Follow-up blood cultures should be obtained either daily or every other day until negative. Should fungemia persist after removal of the vascular catheter and while on antifungal therapy, a search for metastatic foci of infection should be undertaken. Common sites of metastatic infection include the eye, heart valves, kidney, liver, spleen, and osteoarticular structures.
Differential Diagnosis
Intertigo
Differential diagnoses that should be considered along with intertigo include:
- Other infectious causes
- bacteria
- viruses
- dermatophytes
- tinea, trichophyton, microsporum, and epidermophyon
- Seborrheic dermatitis
- Irritant or allergic contact dermatitis
- Atopic dermatitis
- Inverse psoriasis
- Pemphigus
- Scabies
- Metabolic derangements
- Malignancies
Thrush
Differential diagnoses that have similar clinical features to thrush include:
- Oral mucositis
- Erythroplakia
- Thermal burns
- Erythema migrans
- Anemia
- Leucoplakia
- Angioedema
- Apthus stomatitis
- Herpes gingivostomatitis
- Measles (Koplik spots)
- Perioral dermatitis
- Stevens-Johnson syndrome
- Histiocytosis
- Blastomycosis
- Lymphohistiocytosis
- Diphtheria
- Syphilis
- Streptococcal pharyngitis
Esophageal Candidiasis
Differential diagnoses that should be considered along with esophageal candidiasis:
- Other causes of odynophagia
- Esophageal stricture
- Neoplasia
- Eosinophilic esophagitis
- Achalasia
- Medication-induced esophagitis
- Radiation-induced esophagitis
- Bacterial, viral, other fungi, and parasitic causes of esophagitis
Candidal Balanitis
Differential diagnoses that have similar clinical features to balanitis include:
- Bacteria
- Other fungi
- Viruses
- Scabies
- Contact dermatitis
- Drug allergy
- Lichen planus
- Lichen sclerosis
- Psoriasis
- Eczema
- Edema
- Neoplasia
- Chemical irritants
- Trauma
Vulvovaginal Candidiasis
Differential diagnoses that have similar clinical features to vaginal candidiasis include:
- Allergic reaction
- Atopic dermatitis
- Lichen sclerosis
- Lichen simplex chronicus
- Neoplasm
- Paget disease
- Physiologic leukorrhea
- Psoriasis
- Sexual abuse
- Vulvodynia
- Bacterial vaginosis
- Trichomoniasis
Invasive Candidiasis
The differential diagnosis is extensive and includes all the causes of fever, sepsis, septic shock, and multiorgan system failure.
Prognosis
Intertrigo
The prognosis is excellent when the underlying risk factors, eg, diabetes, hyperhidrosis, and obesity, are addressed.
Thrush
The prognosis is excellent with proper management.
Esophageal Candidiasis
The prognosis is excellent when the underlying risk factors, eg, immunocompromised states, are treated.
Candidal Balanitis
The prognosis is excellent when the underlying risk factors, eg, diabetes, incontinence, poor hygiene, immunosuppression, and a tight foreskin, are addressed.
Vulvovaginal Candidiasis
Recurrences are common and can be caused by endogenous relapse of persisting organisms, exogenous reinfection with the same Candida strain, or by a new exogenous strain.
Invasive Candidiasis
Mortality rates range from 35% to 70%. Factors that negatively affect survival rates include delays in initiating antifungal therapy, poor underlying health, lack of source control, and infections caused by species other than Candida albicans species, eg, C auris and C tropicalis.
Complications
Intertrigo
If left untreated, Candida intertrigo can become secondarily infected by bacteria and progress to cellulitis. On rare occasions, topical antifungals can cause contact dermatitis.
Thrush
In immunocompromised hosts, thrush can progress to esophageal candidiasis.
Esophageal Candidiasis
Complications that are associated with esophageal candidiasis include:
- Ulcerations
- Perforation
- Malnourishment
- Candidemia
- Stricture
- Bronchial fistula
Candidal Balanitis
Complications associated with balanitis include phimosis.
Vulvovaginal Candidiasis
Complications associated with vulvovaginal candidiasis include:
- Chronic and recurrent vulvovaginal candidiasis
- Dyspaerunia
Invasive Candidiasis
Candidemia and invasive candidiasis can potentially involve every organ system and result in sepsis syndrome and multiorgan system failure.
Deterrence and Patient Education
Symptoms of Candida infection may mimic other conditions, so appropriate evaluation and diagnostic workup are important. Ameliorating risk factors for Candida infection, when possible, is important for prevention. This may include addressing underlying risk factors, eg, diabetes mellitus, limiting the duration of immunosuppression (when possible), and limiting unnecessary antibiotic use. Promptly diagnosing Candida infection is essential so antifungal therapy can be initiated, particularly in cases of candidemia and invasive candidiasis.
Enhancing Healthcare Team Outcomes
Candidiasis encompasses a wide spectrum of fungal infections caused by Candida species, affecting every organ system and age group. Clinical presentations range from mild superficial infections to life-threatening invasive disease. Diagnosis can be straightforward in cases of localized infection or challenging when the involvement is systemic, influenced by host immune status, anatomical site, and specific Candida species. Management strategies vary accordingly, from simple antifungal therapy in uncomplicated cases to complex, individualized regimens requiring advanced diagnostics and ongoing monitoring. Primary care clinicians often manage mild cases, while severe or refractory infections demand a coordinated, interprofessional approach to optimize outcomes.
Effective management of candidiasis relies on a combination of specialized skills, strategic decision-making, and clearly defined responsibilities across the healthcare team. Physicians, advanced practitioners, nurses, pharmacists, clinical microbiologists, and other allied health professionals must communicate effectively and coordinate care throughout diagnosis, treatment, and follow-up. Collaborative approaches enhance patient safety, reduce errors, and ensure continuity of care. By integrating interprofessional communication, care coordination, and evidence-based practice, healthcare professionals can provide patient-centered care, improve clinical outcomes, and strengthen team performance in addressing the diverse manifestations of candidiasis.
Media
(Click Image to Enlarge)

Oropharyngeal Candidiasis. Oropharyngeal candidiasis is commonly seen in infants, older adults who wear dentures, people treated with antibacterials, and those treated with immunosuppressants.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)

Candida Esophagitis. Image demonstrating endoscopic findings of esophageal candidiasis. Esophageal candidiasis most commonly occurs in individuals with impaired cellular immunity, such as those with AIDS.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
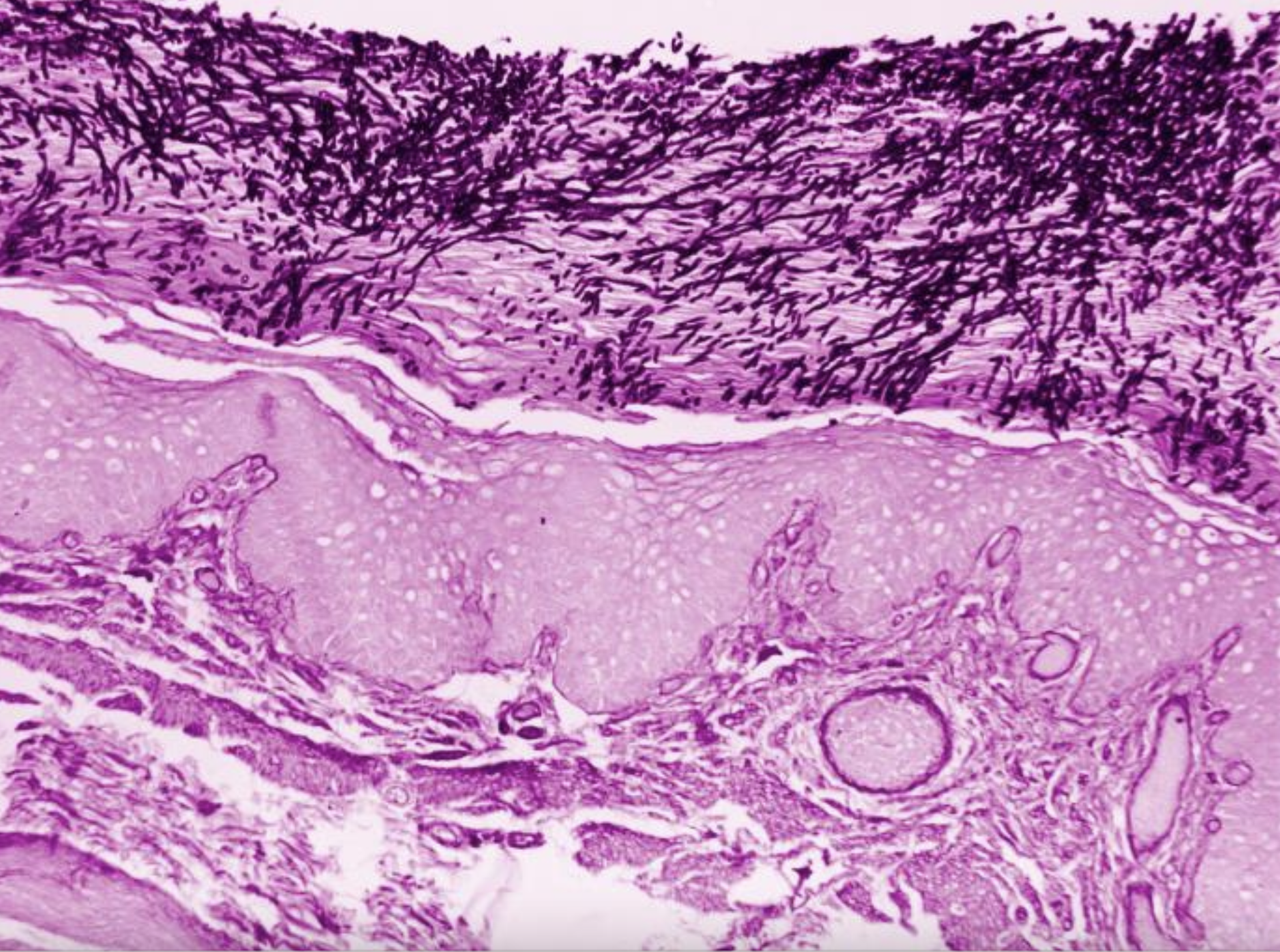
Candida Esophagitis Photomicrograph. Histologic findings of esophageal candidiasis.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)

Candida Balanitis. Photograph of a patient with balanitis of his uncircumcised penis.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)

Vulvovaginal Candida Infection. Photomicroscopic features of Candida vulvovaginitis.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)
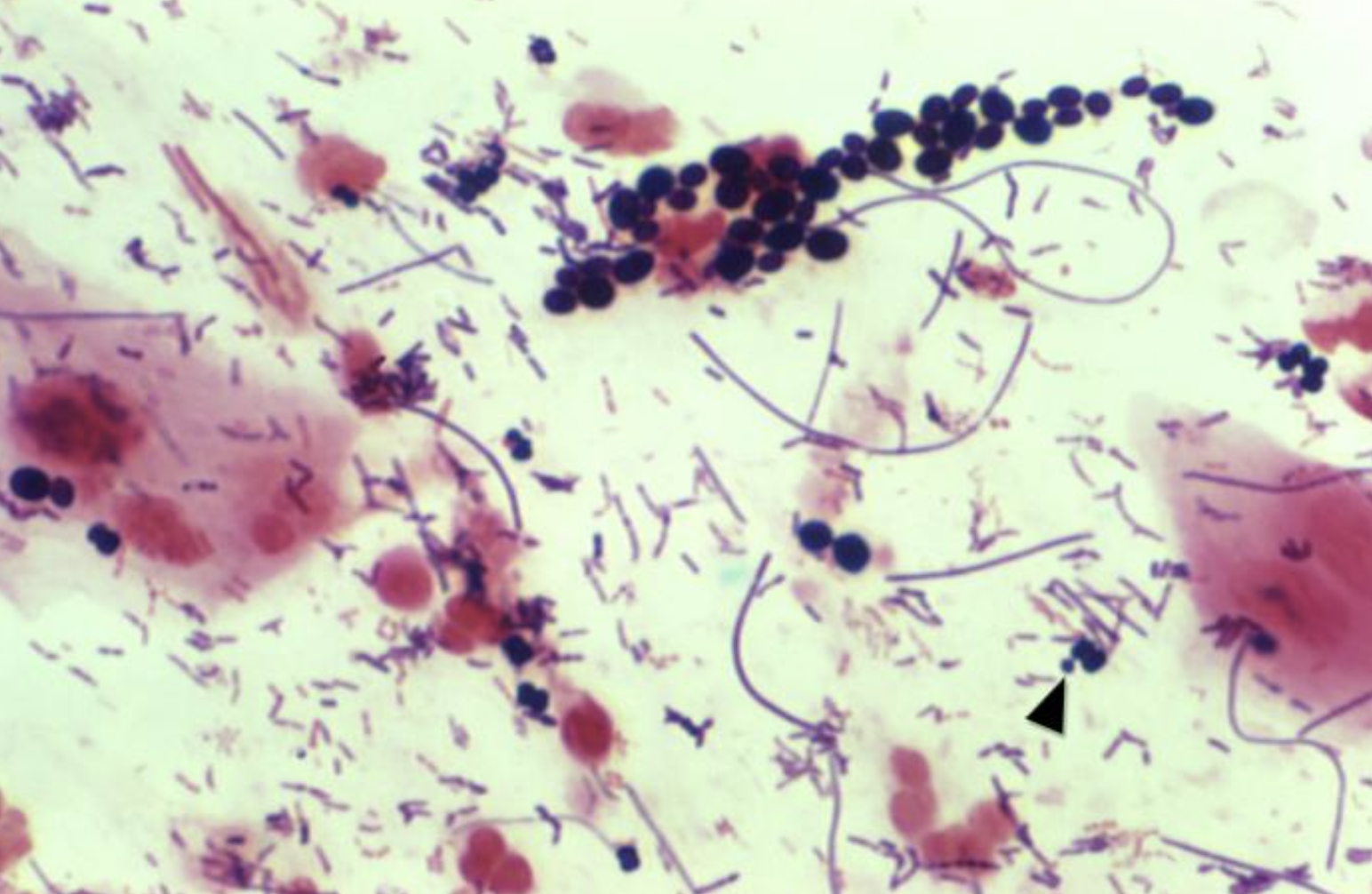
Gram Stain of Candida. Gram stain of various forms of Candida.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)
Candida Endocarditis. Photomicrographic features of Candida endocarditis.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)
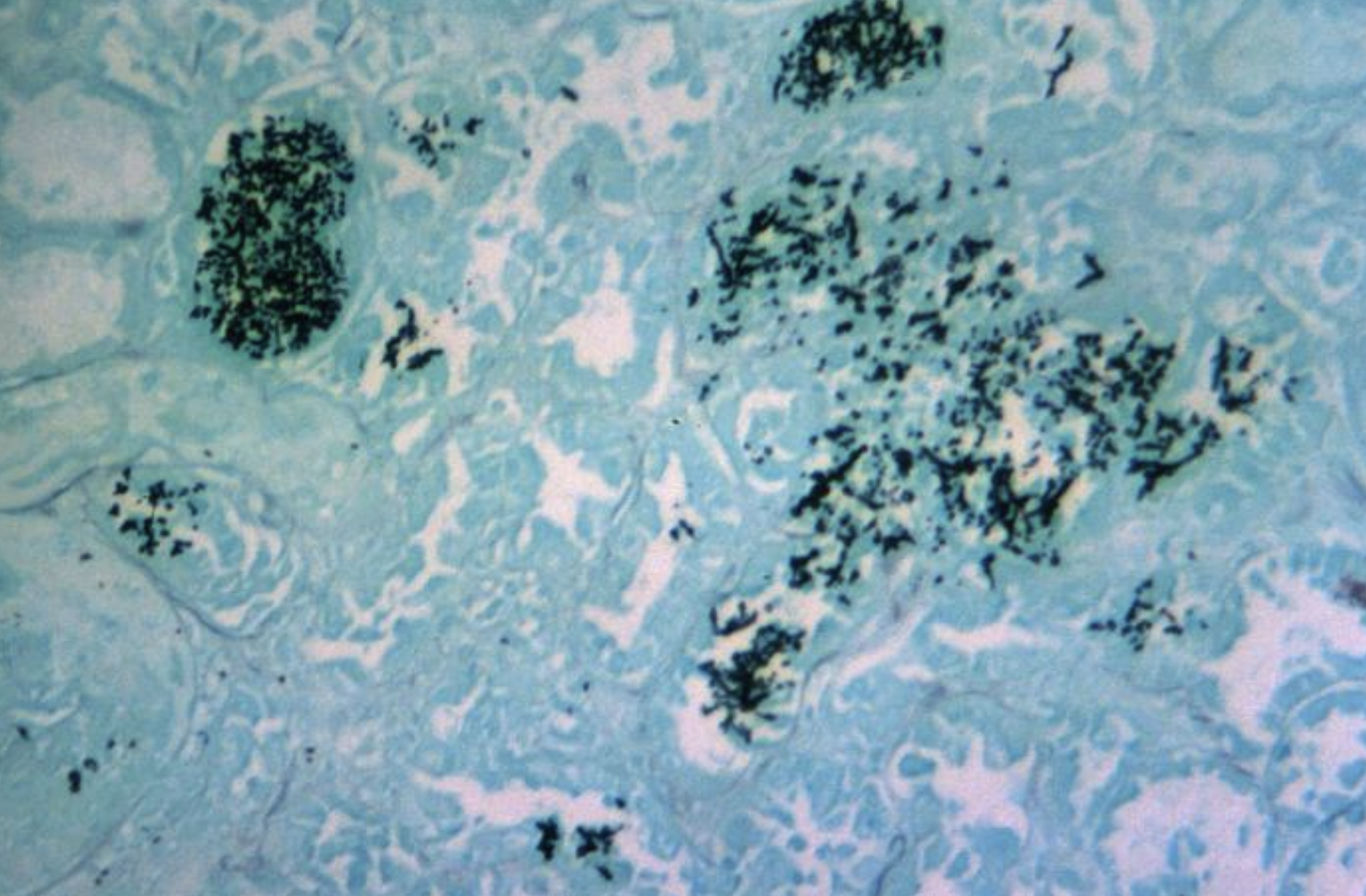
Invasive Candida Infection of the Kidney. Invasive candidiasis is a life-threatening infection that includes candidemia and can involve many organ systems.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)
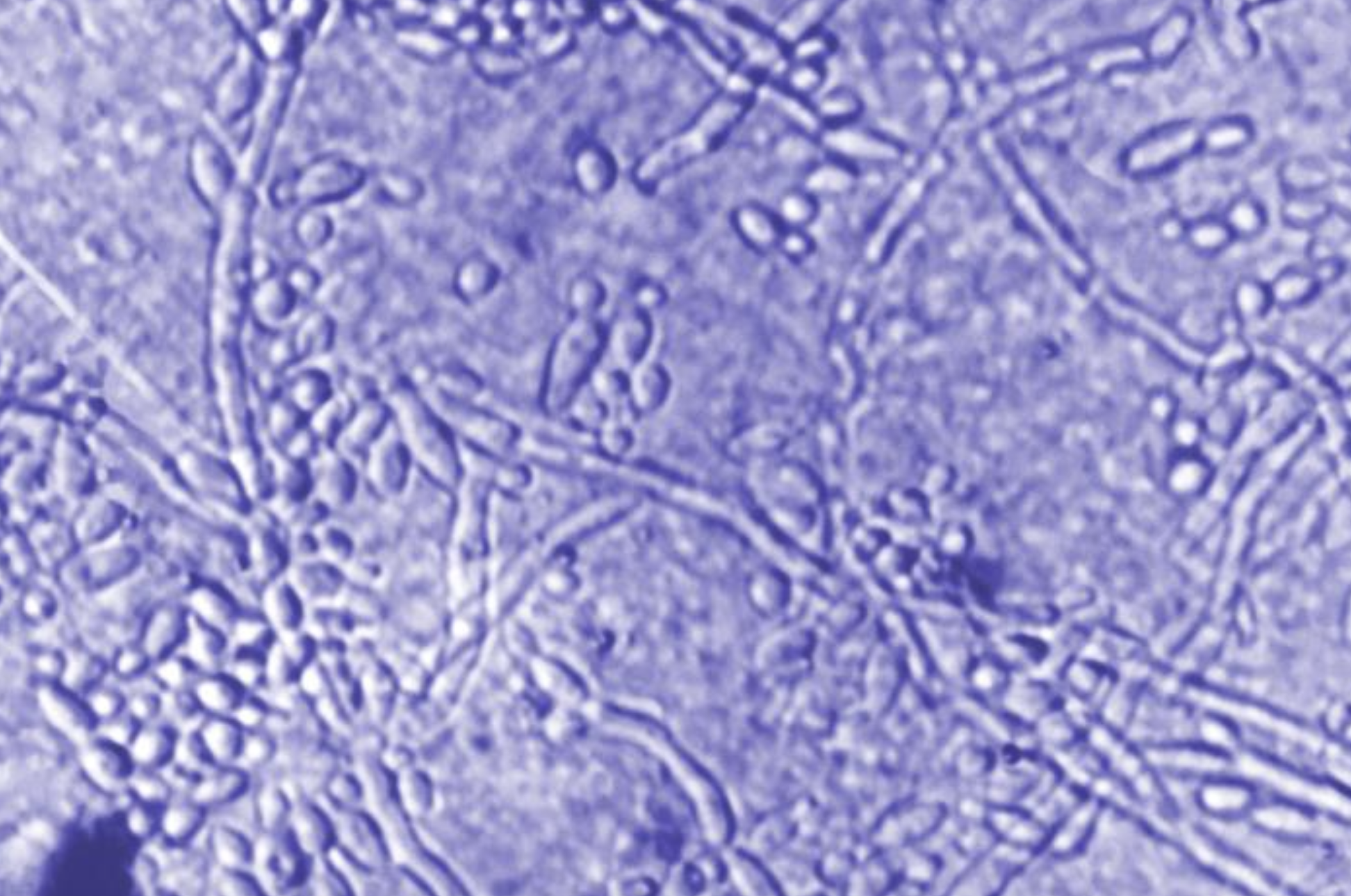
Candida Albicans Skin Scraping. Photomicrographic characteristics of the yeast and pseudomycelium forms.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)
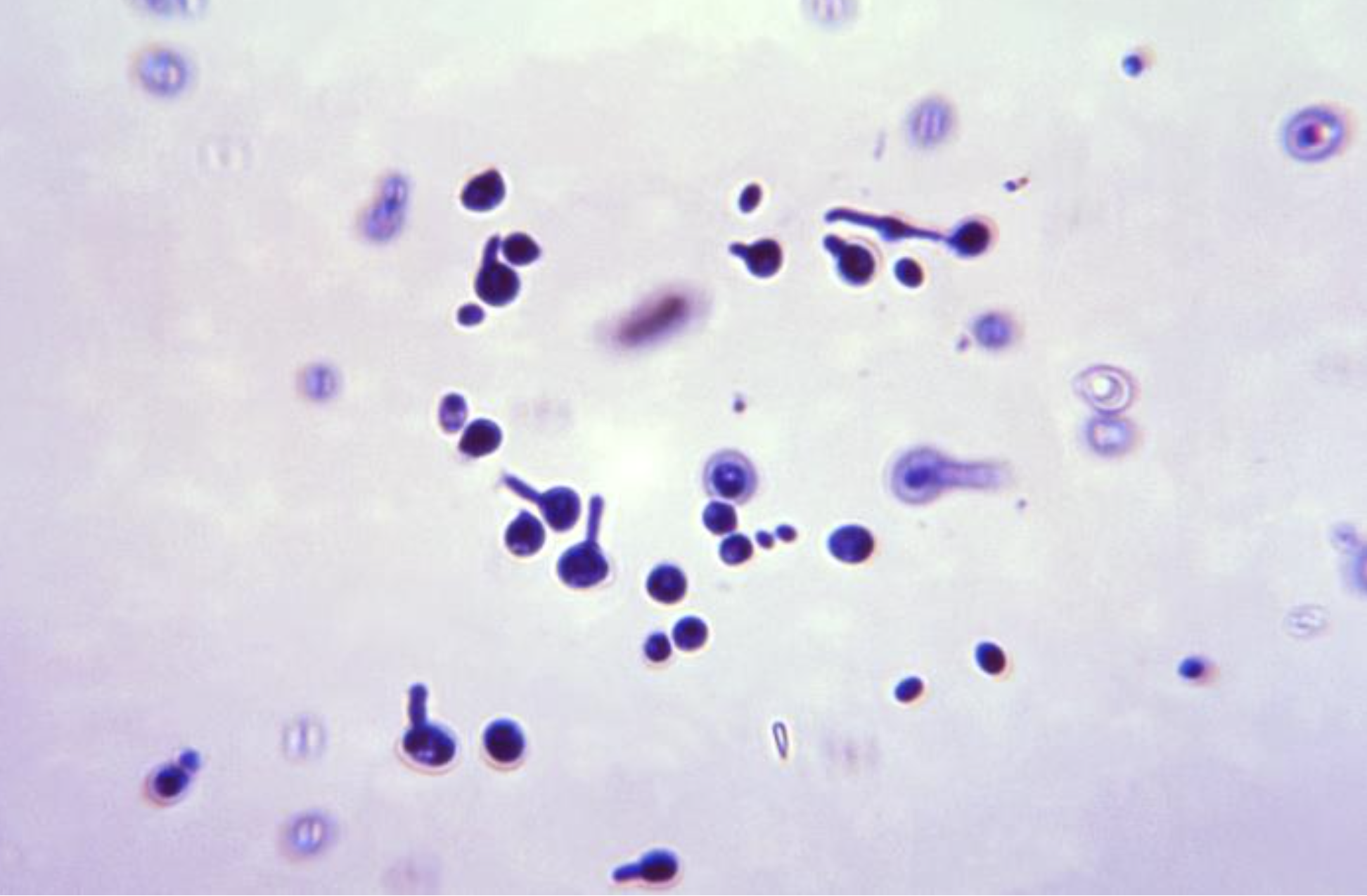
Candida Albicans Yeast Form With Germ Tube. Photomicrographic features of C albicans yeast forms and their germ tube formation.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)
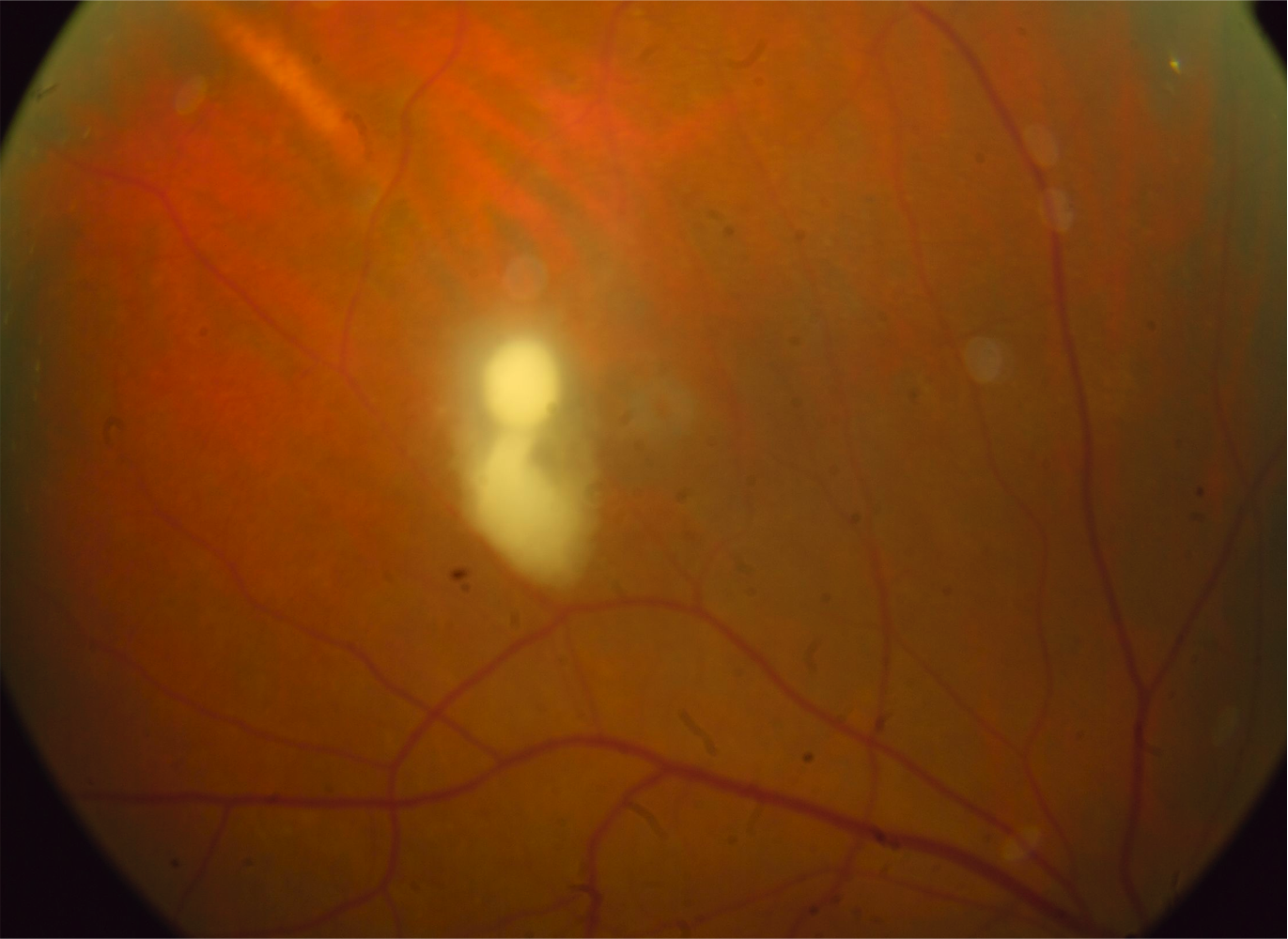
Chorioretinal Candida Lesion. Pruritus often leads to excoriations that evolve into macerated, crusting, and weeping patches.
Contributed by A Sallam, MD, PhD, FRCOphth
(Click Image to Enlarge)

Candida-Associated Intertrigo. Warm, moist regions of the skin, including the axilla, underlying areas of the breast, groin, and buttock folds, are most commonly involved. Diaper dermatitis is a common form of intertrigo.
(Click Image to Enlarge)

Candida Intertrigo. Intertrigo is an inflammatory condition of the epidermis that often becomes secondarily infected by Candida.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
References
Fan Y, Wu L, Zhai B. The mycobiome: interactions with host and implications in diseases. Current opinion in microbiology. 2023 Oct:75():102361. doi: 10.1016/j.mib.2023.102361. Epub 2023 Jul 30 [PubMed PMID: 37527562]
Level 3 (low-level) evidenceSilva S, Negri M, Henriques M, Oliveira R, Williams DW, Azeredo J. Candida glabrata, Candida parapsilosis and Candida tropicalis: biology, epidemiology, pathogenicity and antifungal resistance. FEMS microbiology reviews. 2012 Mar:36(2):288-305. doi: 10.1111/j.1574-6976.2011.00278.x. Epub 2011 Jun 6 [PubMed PMID: 21569057]
Bays DJ, Jenkins EN, Lyman M, Chiller T, Strong N, Ostrosky-Zeichner L, Hoenigl M, Pappas PG, Thompson Iii GR. Epidemiology of Invasive Candidiasis. Clinical epidemiology. 2024:16():549-566. doi: 10.2147/CLEP.S459600. Epub 2024 Aug 28 [PubMed PMID: 39219747]
Lee Y, Puumala E, Robbins N, Cowen LE. Antifungal Drug Resistance: Molecular Mechanisms in Candida albicans and Beyond. Chemical reviews. 2021 Mar 24:121(6):3390-3411. doi: 10.1021/acs.chemrev.0c00199. Epub 2020 May 22 [PubMed PMID: 32441527]
Ogiso H, Adachi S, Mabuchi M, Horibe Y, Ohno T, Suzuki Y, Yamauchi O, Kojima T, Takada E, Iwama M, Saito K, Iwashita T, Ibuka T, Yasuda I, Shimizu M. Risk factors for the development of esophageal candidiasis among patients in community hospital. Scientific reports. 2021 Oct 19:11(1):20663. doi: 10.1038/s41598-021-00132-w. Epub 2021 Oct 19 [PubMed PMID: 34667198]
Mushi MF, Ngeta N, Mirambo MM, Mshana SE. Predictors of esophageal candidiasis among patients attending endoscopy unit in a tertiary hospital, Tanzania: a retrospective cross-sectional study. African health sciences. 2018 Mar:18(1):66-71. doi: 10.4314/ahs.v18i1.10. Epub [PubMed PMID: 29977259]
Level 2 (mid-level) evidenceHoversten P, Otaki F, Katzka DA. Course of Esophageal Candidiasis and Outcomes of Patients at a Single Center. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2019 Jan:17(1):200-202.e1. doi: 10.1016/j.cgh.2018.04.035. Epub 2018 Apr 24 [PubMed PMID: 29702297]
Edwards S. Balanitis and balanoposthitis: a review. Genitourinary medicine. 1996 Jun:72(3):155-9 [PubMed PMID: 8707315]
Grando D, Watson CJ. Perspectives on Vaginal Ecology and Management of Recurrent Vulvovaginal Candidiasis: A Narrative Review. Journal of fungi (Basel, Switzerland). 2025 Nov 13:11(11):. doi: 10.3390/jof11110806. Epub 2025 Nov 13 [PubMed PMID: 41295186]
Level 3 (low-level) evidenceYano J, Sobel JD, Nyirjesy P, Sobel R, Williams VL, Yu Q, Noverr MC, Fidel PL Jr. Current patient perspectives of vulvovaginal candidiasis: incidence, symptoms, management and post-treatment outcomes. BMC women's health. 2019 Mar 29:19(1):48. doi: 10.1186/s12905-019-0748-8. Epub 2019 Mar 29 [PubMed PMID: 30925872]
Level 3 (low-level) evidenceJiménez E, Arroyo R, Cárdenas N, Marín M, Serrano P, Fernández L, Rodríguez JM. Mammary candidiasis: A medical condition without scientific evidence? PloS one. 2017:12(7):e0181071. doi: 10.1371/journal.pone.0181071. Epub 2017 Jul 13 [PubMed PMID: 28704470]
Douglas P. Overdiagnosis and overtreatment of nipple and breast candidiasis: A review of the relationship between diagnoses of mammary candidiasis and Candida albicans in breastfeeding women. Women's health (London, England). 2021 Jan-Dec:17():17455065211031480. doi: 10.1177/17455065211031480. Epub [PubMed PMID: 34269140]
Thomas-Rüddel DO, Schlattmann P, Pletz M, Kurzai O, Bloos F. Risk Factors for Invasive Candida Infection in Critically Ill Patients: A Systematic Review and Meta-analysis. Chest. 2022 Feb:161(2):345-355. doi: 10.1016/j.chest.2021.08.081. Epub 2021 Oct 18 [PubMed PMID: 34673022]
Level 1 (high-level) evidenceAkpan A, Morgan R. Oral candidiasis. Postgraduate medical journal. 2002 Aug:78(922):455-9 [PubMed PMID: 12185216]
Pfaller MA, Diekema DJ. Epidemiology of invasive candidiasis: a persistent public health problem. Clinical microbiology reviews. 2007 Jan:20(1):133-63 [PubMed PMID: 17223626]
Stecksén-Blicks C, Granström E, Silfverdal SA, West CE. Prevalence of oral Candida in the first year of life. Mycoses. 2015 Sep:58(9):550-6. doi: 10.1111/myc.12355. Epub 2015 Jul 27 [PubMed PMID: 26214300]
Benedict K, Roy M, Kabbani S, Anderson EJ, Farley MM, Harb S, Harrison LH, Bonner L, Wadu VL, Marceaux K, Hollick R, Beldavs ZG, Zhang AY, Schaffner W, Graber CR, Derado G, Chiller TM, Lockhart SR, Vallabhaneni S. Neonatal and Pediatric Candidemia: Results From Population-Based Active Laboratory Surveillance in Four US Locations, 2009-2015. Journal of the Pediatric Infectious Diseases Society. 2018 Aug 17:7(3):e78-e85. doi: 10.1093/jpids/piy009. Epub [PubMed PMID: 29522195]
Lausch KR, Schultz Dungu KH, Callesen MT, Schrøder H, Rosthøj S, Poulsen A, Østergaard L, Mortensen KL, Storgaard M, Schønheyder HC, Søgaard M, Arendrup MC. Pediatric Candidemia Epidemiology and Morbidities: A Nationwide Cohort. The Pediatric infectious disease journal. 2019 May:38(5):464-469. doi: 10.1097/INF.0000000000002207. Epub [PubMed PMID: 30281546]
Benjamin DK Jr, Stoll BJ, Gantz MG, Walsh MC, Sánchez PJ, Das A, Shankaran S, Higgins RD, Auten KJ, Miller NA, Walsh TJ, Laptook AR, Carlo WA, Kennedy KA, Finer NN, Duara S, Schibler K, Chapman RL, Van Meurs KP, Frantz ID 3rd, Phelps DL, Poindexter BB, Bell EF, O'Shea TM, Watterberg KL, Goldberg RN, Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Neonatal candidiasis: epidemiology, risk factors, and clinical judgment. Pediatrics. 2010 Oct:126(4):e865-73. doi: 10.1542/peds.2009-3412. Epub 2010 Sep 27 [PubMed PMID: 20876174]
Liu SH, Mitchell H, Nasser Al-Rawahi G. Epidemiology and associated risk factors for candidemia in a Canadian tertiary paediatric hospital: An 11-year review. Journal of the Association of Medical Microbiology and Infectious Disease Canada = Journal officiel de l'Association pour la microbiologie medicale et l'infectiologie Canada. 2023 Mar:8(1):29-39. doi: 10.3138/jammi-2022-0021. Epub 2023 Mar 1 [PubMed PMID: 37008577]
Pammi M, Holland L, Butler G, Gacser A, Bliss JM. Candida parapsilosis is a significant neonatal pathogen: a systematic review and meta-analysis. The Pediatric infectious disease journal. 2013 May:32(5):e206-16. doi: 10.1097/INF.0b013e3182863a1c. Epub [PubMed PMID: 23340551]
Level 1 (high-level) evidenceWarris A, Pana ZD, Oletto A, Lundin R, Castagnola E, Lehrnbecher T, Groll AH, Roilides E, EUROCANDY Study Group. Etiology and Outcome of Candidemia in Neonates and Children in Europe: An 11-year Multinational Retrospective Study. The Pediatric infectious disease journal. 2020 Feb:39(2):114-120. doi: 10.1097/INF.0000000000002530. Epub [PubMed PMID: 31725552]
Level 2 (mid-level) evidenceSaiman L, Ludington E, Dawson JD, Patterson JE, Rangel-Frausto S, Wiblin RT, Blumberg HM, Pfaller M, Rinaldi M, Edwards JE, Wenzel RP, Jarvis W, National Epidemiology of Mycoses Study Group. Risk factors for Candida species colonization of neonatal intensive care unit patients. The Pediatric infectious disease journal. 2001 Dec:20(12):1119-24 [PubMed PMID: 11740316]
Patil S, Rao RS, Majumdar B, Anil S. Clinical Appearance of Oral Candida Infection and Therapeutic Strategies. Frontiers in microbiology. 2015:6():1391. doi: 10.3389/fmicb.2015.01391. Epub 2015 Dec 17 [PubMed PMID: 26733948]
Neal CM, Martens MG. Clinical challenges in diagnosis and treatment of recurrent vulvovaginal candidiasis. SAGE open medicine. 2022:10():20503121221115201. doi: 10.1177/20503121221115201. Epub 2022 Sep 8 [PubMed PMID: 36105548]
Denning DW. Global incidence and mortality of severe fungal disease. The Lancet. Infectious diseases. 2024 Jul:24(7):e428-e438. doi: 10.1016/S1473-3099(23)00692-8. Epub 2024 Jan 12 [PubMed PMID: 38224705]
Tsay SV, Mu Y, Williams S, Epson E, Nadle J, Bamberg WM, Barter DM, Johnston HL, Farley MM, Harb S, Thomas S, Bonner LA, Harrison LH, Hollick R, Marceaux K, Mody RK, Pattee B, Shrum Davis S, Phipps EC, Tesini BL, Gellert AB, Zhang AY, Schaffner W, Hillis S, Ndi D, Graber CR, Jackson BR, Chiller T, Magill S, Vallabhaneni S. Burden of Candidemia in the United States, 2017. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2020 Dec 3:71(9):e449-e453. doi: 10.1093/cid/ciaa193. Epub [PubMed PMID: 32107534]
Jenkins EN, Gold JAW, Benedict K, Lockhart SR, Berkow EL, Dixon T, Shack SL, Witt LS, Harrison LH, Seopaul S, Correa MA, Fitzsimons M, Jabarkhyl Y, Barter D, Czaja CA, Johnston H, Markus T, Schaffner W, Gross A, Lynfield R, Tourdot L, Nadle J, Roland J, Escutia G, Zhang AY, Gellert A, Hurley C, Tesini BL, Phipps EC, Davis SS, Lyman M. Population-Based Active Surveillance for Culture-Confirmed Candidemia - 10 Sites, United States, 2017-2021. Morbidity and mortality weekly report. Surveillance summaries (Washington, D.C. : 2002). 2025 May 29:74(4):1-15. doi: 10.15585/mmwr.ss7404a1. Epub 2025 May 29 [PubMed PMID: 40424200]
Mayer FL, Wilson D, Hube B. Candida albicans pathogenicity mechanisms. Virulence. 2013 Feb 15:4(2):119-28. doi: 10.4161/viru.22913. Epub 2013 Jan 9 [PubMed PMID: 23302789]
Srb N, Talapko J, Meštrović T, Fureš R, Stupnišek M, Srb AM, Škrlec I. A Comprehensive Overview of Candida albicans as the Leading Pathogen in Vulvovaginal Candidiasis. Journal of fungi (Basel, Switzerland). 2025 Aug 28:11(9):. doi: 10.3390/jof11090632. Epub 2025 Aug 28 [PubMed PMID: 41003178]
Level 3 (low-level) evidenceAli GY, Algohary EH, Rashed KA, Almoghanum M, Khalifa AA. Prevalence of Candida colonization in preterm newborns and VLBW in neonatal intensive care unit: role of maternal colonization as a risk factor in transmission of disease. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians. 2012 Jun:25(6):789-95. doi: 10.3109/14767058.2011.622005. Epub 2011 Oct 17 [PubMed PMID: 21919548]
Hernández-Castro R, Arroyo-Escalante S, Carrillo-Casas EM, Moncada-Barrón D, Alvarez-Verona E, Hernández-Delgado L, Torres-Narváez P, Lavalle-Villalobos A. Outbreak of Candida parapsilosis in a neonatal intensive care unit: a health care workers source. European journal of pediatrics. 2010 Jul:169(7):783-7. doi: 10.1007/s00431-009-1109-7. Epub 2009 Dec 4 [PubMed PMID: 19957192]
Miyake A, Gotoh K, Iwahashi J, Togo A, Horita R, Miura M, Kinoshita M, Ohta K, Yamashita Y, Watanabe H. Characteristics of Biofilms Formed by C. parapsilosis Causing an Outbreak in a Neonatal Intensive Care Unit. Journal of fungi (Basel, Switzerland). 2022 Jul 1:8(7):. doi: 10.3390/jof8070700. Epub 2022 Jul 1 [PubMed PMID: 35887456]
Pappas PG, Lionakis MS, Arendrup MC, Ostrosky-Zeichner L, Kullberg BJ. Invasive candidiasis. Nature reviews. Disease primers. 2018 May 11:4():18026. doi: 10.1038/nrdp.2018.26. Epub 2018 May 11 [PubMed PMID: 29749387]
Fisher JF, Kavanagh K, Sobel JD, Kauffman CA, Newman CA. Candida urinary tract infection: pathogenesis. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2011 May:52 Suppl 6():S437-51. doi: 10.1093/cid/cir110. Epub [PubMed PMID: 21498837]
Zlotogorski Hurvitz A, Zadik Y, Gillman L, Platner O, Shani T, Goldman Y, Chaushu G, Kaplan I, Barzilai A, Astman N, Reiter S, Vered M. Palatal Erythema with Histological Psoriasiform Pattern: An Enigmatic Oral Finding Shared by a Range of Conditions. Head and neck pathology. 2020 Dec:14(4):1111-1116. doi: 10.1007/s12105-020-01127-1. Epub 2020 Jan 27 [PubMed PMID: 31989432]
Sobel JD. Epidemiology and pathogenesis of recurrent vulvovaginal candidiasis. American journal of obstetrics and gynecology. 1985 Aug 1:152(7 Pt 2):924-35 [PubMed PMID: 3895958]
Clancy CJ, Nguyen MH. Finding the "missing 50%" of invasive candidiasis: how nonculture diagnostics will improve understanding of disease spectrum and transform patient care. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2013 May:56(9):1284-92. doi: 10.1093/cid/cit006. Epub 2013 Jan 11 [PubMed PMID: 23315320]
Level 3 (low-level) evidenceHankovszky P, Társy D, Öveges N, Molnár Z. Invasive Candida Infections in the ICU: Diagnosis and Therapy. Journal of critical care medicine (Universitatea de Medicina si Farmacie din Targu-Mures). 2015 Oct:1(4):129-139. doi: 10.1515/jccm-2015-0025. Epub 2015 Nov 10 [PubMed PMID: 29967821]
Fernandez J, Erstad BL, Petty W, Nix DE. Time to positive culture and identification for Candida blood stream infections. Diagnostic microbiology and infectious disease. 2009 Aug:64(4):402-7. doi: 10.1016/j.diagmicrobio.2009.04.002. Epub 2009 May 15 [PubMed PMID: 19446982]
Ullah N, Muccio M, Magnasco L, Sepulcri C, Giacobbe DR, Vena A, Bassetti M, Mikulska M. Species-Specific Sensitivity and Levels of Beta-D-Glucan for the Diagnosis of Candidemia-A Systematic Review and Meta-Analysis. Journal of fungi (Basel, Switzerland). 2025 Feb 15:11(2):. doi: 10.3390/jof11020149. Epub 2025 Feb 15 [PubMed PMID: 39997443]
Level 1 (high-level) evidenceMikulska M, Balletto E, Castagnola E, Mularoni A. Beta-D-Glucan in Patients with Haematological Malignancies. Journal of fungi (Basel, Switzerland). 2021 Dec 7:7(12):. doi: 10.3390/jof7121046. Epub 2021 Dec 7 [PubMed PMID: 34947028]
Delavy M, Dos Santos AR, Heiman CM, Coste AT. Investigating Antifungal Susceptibility in Candida Species With MALDI-TOF MS-Based Assays. Frontiers in cellular and infection microbiology. 2019:9():19. doi: 10.3389/fcimb.2019.00019. Epub 2019 Feb 7 [PubMed PMID: 30792970]
Gherna M, Merz WG. Identification of Candida albicans and Candida glabrata within 1.5 hours directly from positive blood culture bottles with a shortened peptide nucleic acid fluorescence in situ hybridization protocol. Journal of clinical microbiology. 2009 Jan:47(1):247-8. doi: 10.1128/JCM.01241-08. Epub 2008 Nov 5 [PubMed PMID: 18987173]
Azim A, Ahmed A. Diagnosis and management of invasive fungal diseases in non-neutropenic ICU patients, with focus on candidiasis and aspergillosis: a comprehensive review. Frontiers in cellular and infection microbiology. 2024:14():1256158. doi: 10.3389/fcimb.2024.1256158. Epub 2024 Mar 5 [PubMed PMID: 38505289]
Clancy CJ, Pappas PG, Vazquez J, Judson MA, Kontoyiannis DP, Thompson GR 3rd, Garey KW, Reboli A, Greenberg RN, Apewokin S, Lyon GM 3rd, Ostrosky-Zeichner L, Wu AHB, Tobin E, Nguyen MH, Caliendo AM. Detecting Infections Rapidly and Easily for Candidemia Trial, Part 2 (DIRECT2): A Prospective, Multicenter Study of the T2Candida Panel. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2018 May 17:66(11):1678-1686. doi: 10.1093/cid/cix1095. Epub [PubMed PMID: 29438475]
Level 2 (mid-level) evidenceMouratidou C, Tsakiri K, Dourliou V, Marneri A, Stougianni M, Pavlidis E. Early-Onset Candidemia in Adult Intensive Care Units. Diagnostics (Basel, Switzerland). 2025 May 31:15(11):. doi: 10.3390/diagnostics15111402. Epub 2025 May 31 [PubMed PMID: 40506974]
Quindós G, Gil-Alonso S, Marcos-Arias C, Sevillano E, Mateo E, Jauregizar N, Eraso E. Therapeutic tools for oral candidiasis: Current and new antifungal drugs. Medicina oral, patologia oral y cirugia bucal. 2019 Mar 1:24(2):e172-e180. doi: 10.4317/medoral.22978. Epub 2019 Mar 1 [PubMed PMID: 30818309]
Yokoyama H, Yamamura Y, Ozeki T, Iga T, Yamada Y. Influence of mouth washing procedures on the removal of drug residues following inhalation of corticosteroids. Biological & pharmaceutical bulletin. 2006 Sep:29(9):1923-5 [PubMed PMID: 16946510]
Abuhajar E, Ali K, Zulfiqar G, Al Ansari K, Raja HZ, Bishti S, Anweigi L. Management of Chronic Atrophic Candidiasis (Denture Stomatitis)-A Narrative Review. International journal of environmental research and public health. 2023 Feb 9:20(4):. doi: 10.3390/ijerph20043029. Epub 2023 Feb 9 [PubMed PMID: 36833718]
Level 3 (low-level) evidenceMohamed AA, Lu XL, Mounmin FA. Diagnosis and Treatment of Esophageal Candidiasis: Current Updates. Canadian journal of gastroenterology & hepatology. 2019:2019():3585136. doi: 10.1155/2019/3585136. Epub 2019 Oct 20 [PubMed PMID: 31772927]
Stary A, Soeltz-Szoets J, Ziegler C, Kinghorn GR, Roy RB. Comparison of the efficacy and safety of oral fluconazole and topical clotrimazole in patients with candida balanitis. Genitourinary medicine. 1996 Apr:72(2):98-102 [PubMed PMID: 8698375]
Satora M, Grunwald A, Zaremba B, Frankowska K, Żak K, Tarkowski R, Kułak K. Treatment of Vulvovaginal Candidiasis-An Overview of Guidelines and the Latest Treatment Methods. Journal of clinical medicine. 2023 Aug 18:12(16):. doi: 10.3390/jcm12165376. Epub 2023 Aug 18 [PubMed PMID: 37629418]
Level 3 (low-level) evidenceLederman SN, Sobel R, Sobel JD, Curelop SB, Brand SR. Sustained Efficacy of Oteseconazole in Women with Recurrent Vulvovaginal Candidiasis. Journal of women's health (2002). 2025 Nov 5:():. doi: 10.1177/15409996251394811. Epub 2025 Nov 5 [PubMed PMID: 41204724]
Phillips NA, Rocktashel M, Merjanian L. Ibrexafungerp for the Treatment of Vulvovaginal Candidiasis: Design, Development and Place in Therapy. Drug design, development and therapy. 2023:17():363-367. doi: 10.2147/DDDT.S339349. Epub 2023 Feb 7 [PubMed PMID: 36785761]
Martin-Loeches I, Antonelli M, Cuenca-Estrella M, Dimopoulos G, Einav S, De Waele JJ, Garnacho-Montero J, Kanj SS, Machado FR, Montravers P, Sakr Y, Sanguinetti M, Timsit JF, Bassetti M. ESICM/ESCMID task force on practical management of invasive candidiasis in critically ill patients. Intensive care medicine. 2019 Jun:45(6):789-805. doi: 10.1007/s00134-019-05599-w. Epub 2019 Mar 25 [PubMed PMID: 30911804]
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, Reboli AC, Schuster MG, Vazquez JA, Walsh TJ, Zaoutis TE, Sobel JD. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2016 Feb 15:62(4):e1-50. doi: 10.1093/cid/civ933. Epub 2015 Dec 16 [PubMed PMID: 26679628]
Level 1 (high-level) evidenceCabrera-Guerrero JP, García-Salazar E, Hernandez Silva G, Chinney Herrera A, Martínez-Herrera E, Pinto-Almazán R, Frías-De-León MG, Castro-Fuentes CA. Candidemia: An Update on Epidemiology, Risk Factors, Diagnosis, Susceptibility, and Treatment. Pathogens (Basel, Switzerland). 2025 Aug 14:14(8):. doi: 10.3390/pathogens14080806. Epub 2025 Aug 14 [PubMed PMID: 40872317]
Andes DR, Safdar N, Baddley JW, Playford G, Reboli AC, Rex JH, Sobel JD, Pappas PG, Kullberg BJ, Mycoses Study Group. Impact of treatment strategy on outcomes in patients with candidemia and other forms of invasive candidiasis: a patient-level quantitative review of randomized trials. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2012 Apr:54(8):1110-22. doi: 10.1093/cid/cis021. Epub 2012 Mar 12 [PubMed PMID: 22412055]
Level 1 (high-level) evidenceAbdullah NM, Cheah SK, Abdul Rahman R, Nor NM, Maaya M, Musthafa QA. External Validation of Risk Prediction Score for Candidemia in Critically Ill Patients: A Retrospective Observational Study. Journal of fungi (Basel, Switzerland). 2025 Mar 6:11(3):. doi: 10.3390/jof11030204. Epub 2025 Mar 6 [PubMed PMID: 40137242]
Level 1 (high-level) evidenceMustafayev K, Kuşkucu MA, Akkoç-Mustafayev FN, Ürkmez S, Mete B, Aygün G. Early Diagnosis of Candidemia in the Intensive Care Unit by Clinical and Molecular Methods: A Prospective Observational Study. Infectious diseases & clinical microbiology. 2024 Dec:6(4):306-319. doi: 10.36519/idcm.2024.443. Epub 2024 Dec 19 [PubMed PMID: 39744668]
Level 2 (mid-level) evidence