Introduction
Ankle sprains frequently prompt presentation to the emergency department, accounting for approximately 7% to 10% of visits and up to 40% of all sports-related injuries.[1] Most ankle injuries occur during athletic activity and involve the lateral ankle following an inversion mechanism. The lateral ligament complex includes the anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL), and posterior talofibular ligament (PTFL). Distinguishing ATFL-superimposed CFL injuries from isolated CFL injuries remains challenging because clinical examination demonstrates low sensitivity. Despite this limitation, the ATFL contributes to most ankle sprains and accounts for two-thirds of lateral ankle injuries.[2]
Literature addressing isolated CFL injuries remains limited, whereas combined ATFL and CFL involvement represents the second most common lateral ankle injury pattern.[3] Published discussions of CFL pathology often appear within broader analyses of lateral ankle injuries rather than as distinct entities.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Sports activities account for a large percentage of lateral ankle injuries. Indoor and court sports pose the highest risk of ankle injury.[4] The only published risk factor for ankle sprain is prior injury.[5]
Epidemiology
Approximately 30,000 ankle sprains occur each day in the United States, accounting for 25% to 40% of sports injuries. Incidence rates of ankle injuries are the highest in field hockey, followed by volleyball, football, basketball, cheerleading, ice hockey, lacrosse, soccer, rugby, track and field, gymnastics, and softball. The lateral ligament compartment is involved in 85% of ankle injuries, with a daily incidence of 1 in 10,000. Isolated CFL injuries are rare; reported cases are often classified as lateral ankle ligament injuries.[1][6][7][5]
Pathophysiology
The CFL measures approximately 20 mm in length and 6 to 8 mm in diameter, originating at the anterior-lateral malleolus and attaching to the posterior-lateral tubercle of the calcaneus.[3] The peroneus brevis and longus tendons and their sheaths cross superficial to the CFL ligament. The CFL is reinforced by either the lateral talocalcaneal ligament or the anterior talocalcaneal ligament in 35% and 42% of cases, respectively.[8] The CFL resists inversion in both plantarflexion and dorsiflexion and stabilizes the subtalar joint during plantarflexion.
While combined inversion and supination is the mechanism of injury to the lateral ankle, an isolated CFL injury occurs from inversion in extreme dorsiflexion.[3][7] The CFL can sustain a load of 109 ± 28 N and, during ATFL stretch during high-grade ankle sprains, withstand a force of 345 N.[1] Common mechanisms of injury include landing from jumps, stepping on another athlete's lower extremity, sustaining trauma at heel strike during running, and stressing the foot in a fixed position.[5]
History and Physical
History and physical examination are important for triaging injuries to ensure appropriate intervention. Patients may report a cracking sound, swelling, redness, pain, and cessation of activities. As such, the physical examination should focus on inspection, palpation, and special maneuvers, eg, the anterior drawer and talar tilt tests.[9] The anterior drawer test is performed with the patient's foot in a neutral position while the examiner applies anterior force to the ankle. Laxity of the injured ankle in comparison to the unaffected foot is positive for the anterior drawer test.[10]
Similarly, the talar tilt test can be performed with the patient’s foot in a neutral position as the examiner exerts a tilting force to invert the ankle. The injured ankle is compared to the unaffected side for laxity.[11] As such, the anterior drawer and talar tilt test can be subjective. Following the initial assessment, physical findings of ecchymosis with localized pain on palpation 4 to 5 days posttrauma carry a 90% chance of lateral ligament injury.[9] Patients with tenderness to palpation over the CFL have a 72% risk of ligament injury.[3] The Ottawa ankle rule for initial assessment of radiographic stewardship uses palpation of 4 pain sites (posterior edge or tip of either malleolus, navicular bone, or base of the fifth metatarsal) and the ability to bear weight. This assessment tool has a sensitivity of 96.4% to 99.6%, making it valuable for excluding ankle fractures.[12]
Evaluation
Patients with positive Ottawa ankle test results warrant referral for ankle radiography (see Image. Ligaments of the Foot, Lateral Aspect). Ankle fractures comprise less than 15% of fractures.[12] Ultrasonography provides dynamic imaging, whereas magnetic resonance imaging (MRI) serves as an additional modality in cases with a strong suspicion of ligament injury. Ultrasound accuracy depends on clinician technique and expertise, with reported sensitivity of 92% and specificity of 64% for detecting ligamentous injury.[9] When clinical suspicion for fracture remains high, clinicians may obtain an MRI, which demonstrates a sensitivity of 93% to 96% and a specificity of 100%.[13]
Following physical examination, a lateral ankle injury is classified into the following 3 grades:
- Grade I reflects ligament stretching.
- Grade II is a moderate sprain.
- Grade III involves severe sprain and full ligament lesions.
Increasing grade corresponds to greater injury severity and guides treatment selection, prognosis, and anticipation of potential complications.[9]
Treatment / Management
Conservative Management
Conservative management is often effective in treating CFL injuries. The progression of healing following initial injury has 3 distinct phases: inflammatory (1–10 days), proliferative (4–8 weeks), and remodeling phase (up to 1 year).[14] As such, each biological phase offers a unique therapeutic window for intervention.(A1)
During the initial inflammatory response, RICE (rest, ice, compression, and elevation) is implemented in the first 4 to 5 days. Immobilization with a cast or boots is often applied in the first week to reduce swelling and pain; after that, a brace or taping can be provided to facilitate return to activity.[9] Rigid immobilization during the proliferative stage is not recommended, as functional stress promotes remodeling and flexibility. An ankle support with a semi-rigid ankle brace is used for grade I to II injuries, whereas cast immobilization followed by a semi-rigid orthosis is used for grade III injuries.[14] Medications (eg, NSAIDs or acetaminophen) can be used to assist with pain.(A1)
Emerging evidence supports early functional rehabilitation, including flexible mobilization, progressive weight-bearing, and external support strategies, eg, taping or bracing, for grade I to II sprains. Compared with rigid immobilization, functional rehabilitation for lower-grade sprains is associated with faster recovery and earlier return to activity. Multiple randomized trials and consensus guidelines support this approach, demonstrating that patients treated with functional bracing rather than prolonged rigid (cast) immobilization return to normal activities more quickly while experiencing less pain.[15][5][16] Short-term rigid immobilization with a maximum duration of 10 days remains a viable option for more severe grade III injuries.[17](A1)
Operative Interventions
Most lateral ankle injuries are managed nonoperatively, while surgical interventions are recommended for patients with chronic instability.[9] Surgical options have evolved toward minimally invasive and anatomic techniques. Endoscopic anatomic ligament reconstruction, including all-inside and remnant-preserving approaches, has demonstrated functional improvements with low complication rates in cases of chronic instability.[18]][19]
Rigby et al described 2 cases of isolated calcaneofibular ligament injury, with one undergoing surgical intervention, while another patient had conservative management with immobilization and physical therapy. Both patients had optimal outcomes. Surgical intervention should be evaluated on an individualized basis and may reduce the risk of recurrence and ankle instability. Clinical outcomes are similar between conservative and surgical management.[9][14](A1)
Regenerative Interventions
Regenerative interventions, eg, hyaluronic acid, shock wave, laser, bone marrow aspirate, mesenchymal stem cells, and platelet-rich plasma (PRP) therapies, are increasingly being explored for ligament healing. These biologics aim to enhance tissue regeneration and recovery by stimulating the healing process while also managing symptoms. Intraligamentously injected growth factors are thought to enhance cellular activities—including extracellular matrix deposition and differentiation of mesenchymal stem cells into fibroblasts—that facilitate repair of torn ligaments. Current evidence supporting the efficacy of biologics in treating ligamentous injuries is limited to small studies and short-term outcomes. Given this lack of robust clinical data, biologics remain investigational rather than the standard of care.[20][21][22]
Differential Diagnosis
CFL injury often involves the ATFL, and this should be considered in the differential diagnosis. Importantly, other diagnoses to consider are osteochondral injury, plantar fascia rupture, peroneal tendon injury, ankle fractures, calcaneal beak and other avulsion fractures, Achilles or plantaris tendon rupture, and peroneal tendon subluxation with or without retinaclum rupture. Lastly, injuries to the subtalar joint should be considered in the context of potential CFL injuries, as they are adjacent to this joint.[23]
Prognosis
Return to play or work is important to discuss at the time of diagnosis, given that 25% of patients are expected to miss school or work.[24] Moreover, patients may experience long-term instability or pain. Approximately 74% of patients experience chronic symptoms of pain, swelling, weakness, or instability 4 years after injury. Additionally, 32% of patients have reported symptoms up to 7 years from the original injury.[24] A systematic review by Thompson et al found that characteristics such as initial pain intensity, weight-bearing status, and range of motion were inconsistent prognostic factors in many studies. Thus, these clinical findings should be used with caution when anticipating recovery.
Complications
Lateral ankle injuries are not sentinel events but have long-term sequelae. Reinjury is common in low-grade ankle sprains.[25] Patients may experience instability and pain, both of which can reduce function. Chronic joint instability can even progress to posttraumatic ankle joint osteoarthritis.[4]
Postoperative and Rehabilitation Care
Rehabilitation incorporating early mobilization and daily exercise programs promotes functional recovery and restores mobility.[26] A systematic review by Doherty et al examining exercise therapy for acute ankle sprains reported consistent improvement in self-reported function across studies.[26] Rehabilitation sessions averaged between 3.5 and 21 hours. Although no standardized protocols exist for exercise therapy, patients focus on regaining strength and balance.[27] Initiating therapy within the first week of injury helps reduce arthrogenic muscle inhibition caused by edema and pain, enabling earlier reactivation of ankle musculature and improved functionality.[26]
Ankle support through bracing or taping can alleviate pain and serve as a secondary preventive measure during rehabilitation. Proprioceptive training presents the greatest challenge during recovery, as restoring joint position sense remains a critical and often elusive component of the healing process. Structured early mobilization and targeted exercises facilitate both functional gains and long-term joint stability.
Deterrence and Patient Education
Calcaneofibular ligament injuries are rarely discussed as isolated cases in the literature. As such, much of our understanding is derived from lateral ankle injuries. The physical examination can assist clinicians in triaging patients for further evaluation and imaging modalities. Patients should be informed about the expected recovery time and the injury's prognosis. Moreover, patients should be advised to aggressively rehabilitate after injury, as a premature return to activity without proper function may aggravate or prolong CFL injuries. Weight-bearing status should be determined on an individual basis.
Enhancing Healthcare Team Outcomes
Lateral ankle injuries, particularly sprains involving the anterior talofibular and calcaneofibular ligaments, are a common presentation in emergency and sports medicine settings, accounting for up to 40% of sports-related injuries. Most injuries result from inversion with supination, while isolated calcaneofibular ligament injuries are less frequent and often under-recognized due to overlapping clinical features. Accurate assessment relies on detailed history, physical examination—including anterior drawer and talar tilt tests—and judicious use of imaging guided by the Ottawa ankle rules. Evidence-based management emphasizes early functional rehabilitation, phase-specific interventions, and selective use of immobilization or surgery to optimize ligament healing and reduce the risk of chronic instability. Emerging biologic therapies offer potential adjunctive benefits but remain investigational.
Effective patient-centered care for lateral ankle injuries requires coordinated efforts across healthcare professionals. Physicians, advanced practitioners, and general practitioners are responsible for accurate diagnosis, injury grading, and the development of individualized treatment plans. Nurses play a key role in patient education, pain monitoring, and functional rehabilitation. Pharmacists assist with safe analgesic use and medication management, while physical therapists guide progressive mobilization and strengthening. Open communication, collaboration, and care coordination among these professionals ensure timely interventions, minimize complications, and promote optimal recovery, safety, and long-term functional outcomes for patients.
Media
(Click Image to Enlarge)
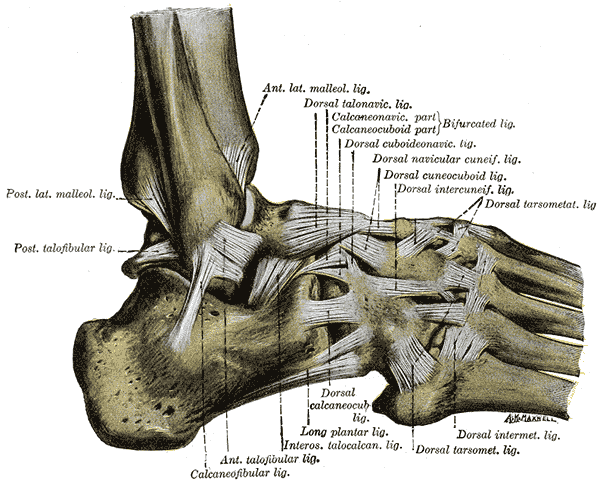
Ligaments of the Lateral Aspect of the Right Foot and Ankle. This anatomical illustration details the complex connective tissues of the foot, including the anterior and posterior lateral malleolar ligaments and the anterior and posterior talofibular ligaments. The calcaneofibular ligament and interosseous talocalcaneal ligament are shown stabilizing the heel, while the bifurcated ligament (comprising the calcaneonavicular and calcaneocuboid parts), the long plantar ligament, and the dorsal talonavicular ligament support the midfoot. Further distal structures include the dorsal cuboideonavicular, dorsal navicular cuneiform, dorsal cuneocuboid, dorsal intercuneiform, dorsal calcaneocuboid, dorsal tarsometatarsal, and dorsal intermetatarsal ligaments.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Hunt KJ, Pereira H, Kelley J, Anderson N, Fuld R, Baldini T, Kumparatana P, D'Hooghe P. The Role of Calcaneofibular Ligament Injury in Ankle Instability: Implications for Surgical Management. The American journal of sports medicine. 2019 Feb:47(2):431-437. doi: 10.1177/0363546518815160. Epub 2018 Dec 20 [PubMed PMID: 30571138]
Fujii T, Luo ZP, Kitaoka HB, An KN. The manual stress test may not be sufficient to differentiate ankle ligament injuries. Clinical biomechanics (Bristol, Avon). 2000 Oct:15(8):619-23 [PubMed PMID: 10936435]
Rigby R, Cottom JM, Rozin R. Isolated calcaneofibular ligament injury: a report of two cases. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons. 2015 May-Jun:54(3):487-9. doi: 10.1053/j.jfas.2014.08.017. Epub 2014 Oct 16 [PubMed PMID: 25441852]
Level 3 (low-level) evidenceDoherty C, Delahunt E, Caulfield B, Hertel J, Ryan J, Bleakley C. The incidence and prevalence of ankle sprain injury: a systematic review and meta-analysis of prospective epidemiological studies. Sports medicine (Auckland, N.Z.). 2014 Jan:44(1):123-40. doi: 10.1007/s40279-013-0102-5. Epub [PubMed PMID: 24105612]
Level 1 (high-level) evidenceKaminski TW, Hertel J, Amendola N, Docherty CL, Dolan MG, Hopkins JT, Nussbaum E, Poppy W, Richie D, National Athletic Trainers' Association. National Athletic Trainers' Association position statement: conservative management and prevention of ankle sprains in athletes. Journal of athletic training. 2013 Jul-Aug:48(4):528-45. doi: 10.4085/1062-6050-48.4.02. Epub [PubMed PMID: 23855363]
Dimmick S, Kennedy D, Daunt N. Evaluation of thickness and appearance of anterior talofibular and calcaneofibular ligaments in normal versus abnormal ankles with MRI. Journal of medical imaging and radiation oncology. 2008 Dec:52(6):559-63. doi: 10.1111/j.1440-1673.2008.02018.x. Epub [PubMed PMID: 19178629]
Struijs PA, Kerkhoffs GM. Ankle sprain. BMJ clinical evidence. 2010 May 13:2010():. pii: 1115. Epub 2010 May 13 [PubMed PMID: 21718566]
Level 1 (high-level) evidenceGolanó P, Vega J, de Leeuw PA, Malagelada F, Manzanares MC, Götzens V, van Dijk CN. Anatomy of the ankle ligaments: a pictorial essay. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2010 May:18(5):557-69. doi: 10.1007/s00167-010-1100-x. Epub 2010 Mar 23 [PubMed PMID: 20309522]
van den Bekerom MP, Kerkhoffs GM, McCollum GA, Calder JD, van Dijk CN. Management of acute lateral ankle ligament injury in the athlete. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2013 Jun:21(6):1390-5. doi: 10.1007/s00167-012-2252-7. Epub 2012 Oct 30 [PubMed PMID: 23108678]
Kovaleski JE, Norrell PM, Heitman RJ, Hollis JM, Pearsall AW. Knee and ankle position, anterior drawer laxity, and stiffness of the ankle complex. Journal of athletic training. 2008 May-Jun:43(3):242-8. doi: 10.4085/1062-6050-43.3.242. Epub [PubMed PMID: 18523573]
Hubbard TJ, Hicks-Little CA. Ankle ligament healing after an acute ankle sprain: an evidence-based approach. Journal of athletic training. 2008 Sep-Oct:43(5):523-9. doi: 10.4085/1062-6050-43.5.523. Epub [PubMed PMID: 18833315]
Level 1 (high-level) evidenceBachmann LM, Kolb E, Koller MT, Steurer J, ter Riet G. Accuracy of Ottawa ankle rules to exclude fractures of the ankle and mid-foot: systematic review. BMJ (Clinical research ed.). 2003 Feb 22:326(7386):417 [PubMed PMID: 12595378]
Level 1 (high-level) evidenceVuurberg G, Hoorntje A, Wink LM, van der Doelen BFW, van den Bekerom MP, Dekker R, van Dijk CN, Krips R, Loogman MCM, Ridderikhof ML, Smithuis FF, Stufkens SAS, Verhagen EALM, de Bie RA, Kerkhoffs GMMJ. Diagnosis, treatment and prevention of ankle sprains: update of an evidence-based clinical guideline. British journal of sports medicine. 2018 Aug:52(15):956. doi: 10.1136/bjsports-2017-098106. Epub 2018 Mar 7 [PubMed PMID: 29514819]
Petersen W, Rembitzki IV, Koppenburg AG, Ellermann A, Liebau C, Brüggemann GP, Best R. Treatment of acute ankle ligament injuries: a systematic review. Archives of orthopaedic and trauma surgery. 2013 Aug:133(8):1129-41. doi: 10.1007/s00402-013-1742-5. Epub 2013 May 28 [PubMed PMID: 23712708]
Level 1 (high-level) evidenceHerring SA, Kibler WB, Putukian M, Boyajian-O'Neill LA, Chang CJ, Franks RR, Hutchinson M, Indelicato PA, O'Connor FG, Powell A, Roach R, Safran M, Statuta SM, Sutton K. Initial Assessment and Management of Select Musculoskeletal Injuries: A Team Physician Consensus Statement. Medicine and science in sports and exercise. 2024 Mar 1:56(3):385-401. doi: 10.1249/MSS.0000000000003324. Epub 2023 Oct 16 [PubMed PMID: 37847756]
Level 3 (low-level) evidenceBeynnon BD, Renström PA, Haugh L, Uh BS, Barker H. A prospective, randomized clinical investigation of the treatment of first-time ankle sprains. The American journal of sports medicine. 2006 Sep:34(9):1401-12 [PubMed PMID: 16801691]
Level 1 (high-level) evidenceMartin RL, Davenport TE, Fraser JJ, Sawdon-Bea J, Carcia CR, Carroll LA, Kivlan BR, Carreira D. Ankle Stability and Movement Coordination Impairments: Lateral Ankle Ligament Sprains Revision 2021. The Journal of orthopaedic and sports physical therapy. 2021 Apr:51(4):CPG1-CPG80. doi: 10.2519/jospt.2021.0302. Epub [PubMed PMID: 33789434]
Cordier G, Ovigue J, Dalmau-Pastor M, Michels F. Endoscopic anatomic ligament reconstruction is a reliable option to treat chronic lateral ankle instability. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2020 Jan:28(1):86-92. doi: 10.1007/s00167-019-05793-9. Epub 2019 Nov 14 [PubMed PMID: 31728603]
Dong P, Gu S, Jiang Y, Yao W, Zhang K, Tao T, Li Y, Li W, Gui J. All arthroscopic remnant-preserving reconstruction of the lateral ligaments of the ankle: A biomechanical study and clinical application. Biochemical and biophysical research communications. 2018 Nov 10:505(4):985-990. doi: 10.1016/j.bbrc.2018.10.041. Epub 2018 Oct 9 [PubMed PMID: 30314696]
Danilkowicz R, Murawski C, Pellegrini M, Walther M, Valderrabano V, Angthong C, Adams S. Nonoperative and Operative Soft-Tissue and Cartilage Regeneration and Orthopaedic Biologics of the Foot and Ankle: An Orthoregeneration Network Foundation Review. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2022 Jul:38(7):2350-2358. doi: 10.1016/j.arthro.2022.04.018. Epub 2022 May 21 [PubMed PMID: 35605840]
Urits I, Hasegawa M, Orhurhu V, Peck J, Kelly AC, Kaye RJ, Orhurhu MS, Brinkman J, Giacomazzi S, Foster L, Manchikanti L, Kaye AD, Viswanath O. Minimally Invasive Treatment of Chronic Ankle Instability: a Comprehensive Review. Current pain and headache reports. 2020 Feb 4:24(3):8. doi: 10.1007/s11916-020-0840-7. Epub 2020 Feb 4 [PubMed PMID: 32020393]
Chahla J, Kennedy MI, Aman ZS, LaPrade RF. Ortho-Biologics for Ligament Repair and Reconstruction. Clinics in sports medicine. 2019 Jan:38(1):97-107. doi: 10.1016/j.csm.2018.08.003. Epub [PubMed PMID: 30466725]
Sugimoto K, Samoto N, Takaoka T, Takakura Y, Tamai S. Subtalar arthrography in acute injuries of the calcaneofibular ligament. The Journal of bone and joint surgery. British volume. 1998 Sep:80(5):785-90 [PubMed PMID: 9768887]
Thompson JY, Byrne C, Williams MA, Keene DJ, Schlussel MM, Lamb SE. Prognostic factors for recovery following acute lateral ankle ligament sprain: a systematic review. BMC musculoskeletal disorders. 2017 Oct 23:18(1):421. doi: 10.1186/s12891-017-1777-9. Epub 2017 Oct 23 [PubMed PMID: 29061135]
Level 1 (high-level) evidenceMalliaropoulos N, Ntessalen M, Papacostas E, Longo UG, Maffulli N. Reinjury after acute lateral ankle sprains in elite track and field athletes. The American journal of sports medicine. 2009 Sep:37(9):1755-61. doi: 10.1177/0363546509338107. Epub 2009 Jul 17 [PubMed PMID: 19617530]
Level 2 (mid-level) evidenceBleakley CM, O'Connor SR, Tully MA, Rocke LG, Macauley DC, Bradbury I, Keegan S, McDonough SM. Effect of accelerated rehabilitation on function after ankle sprain: randomised controlled trial. BMJ (Clinical research ed.). 2010 May 10:340():c1964. doi: 10.1136/bmj.c1964. Epub 2010 May 10 [PubMed PMID: 20457737]
Level 1 (high-level) evidenceBleakley CM, Taylor JB, Dischiavi SL, Doherty C, Delahunt E. Rehabilitation Exercises Reduce Reinjury Post Ankle Sprain, But the Content and Parameters of an Optimal Exercise Program Have Yet to Be Established: A Systematic Review and Meta-analysis. Archives of physical medicine and rehabilitation. 2019 Jul:100(7):1367-1375. doi: 10.1016/j.apmr.2018.10.005. Epub 2018 Oct 26 [PubMed PMID: 30612980]
Level 1 (high-level) evidence