 Catheter Management of Ventricular Septal Defect
Catheter Management of Ventricular Septal Defect
Introduction
Ventricular septal defect (VSD) is currently the most common congenital heart disease in the pediatric population (see Image. Ventricular Septal Defect). As the population ages, VSDs have become the second most common congenital heart disease, right behind bicuspid aortic valves. This disease is most likely due to the early spontaneous closure of VSDs.[1] While many VSDs close spontaneously, some do not.
Depending on the size and flow of the VSD, hemodynamic compromise may occur. Treatment options include surveillance for small, asymptomatic VSDs in the absence of pulmonary artery hypertension; surgical repair is recommended for medium to large-sized VSDs in the presence of hemodynamic compromise. Traditionally, VSDs have been closed with an open approach, but now there is a new emerging intervention- the percutaneous transcatheter closure, currently reserved for nonsurgical candidates.[2] Whereas the closure of a VSD can pose a significant risk to the rare patient, some congenital disabilities benefit from the percutaneous closure of a VSD. The very first percutaneous transcatheter VSD closure was performed in 2013 by Lin et al.[3]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The ventricular septum is a structurally complex, 3-dimensional entity composed of membranous and muscular components that ensures effective pressure separation between the systemic and pulmonary circulations. In normal physiology, higher left ventricular pressure maintains unidirectional systemic output without intracardiac shunting. In a VSD, a pathological interventricular communication permits left-to-right shunting, resulting in increased pulmonary blood flow, progressive left ventricular volume overload, and, if untreated, pulmonary vascular remodeling. From an interventional standpoint, shunt magnitude is determined by defect size, location, septal rims, and pulmonary vascular resistance. These variables directly influence candidacy for transcatheter closure, device selection, and procedural timing.
Precise anatomical characterization is fundamental for procedural success. Most VSDs are elliptical rather than circular; therefore, reliance on a single linear measurement may underestimate true defect dimensions. The maximal diameter measured during the phase when the defect is largest should guide device sizing.[4]
En-face visualization using electrocardiogram (ECG)-gated cardiac computed tomography (CT) can be particularly helpful for defining:
- True defect geometry
- Relationship to the aortic valve and tricuspid valve
- Rim adequacy
- Presence of aneurysmal tissue
However, interpreting imaging becomes more complex in aneurysmal perimembranous defects. Septal aneurysms may create multiple fenestrations with a tortuous, multilobulated (“cauliflower-like”) morphology. In these cases, the procedural strategy should focus on identifying the dominant left ventricular entry or exit orifice rather than attempting to close each fenestration individually. Device positioning within aneurysmal tissue requires careful assessment to avoid residual shunting or device instability.
Percutaneous closure of perimembranous VSDs remains technically challenging and continues to generate debate. The proximity of the defect to the atrioventricular conduction system and the aortic valve introduces risks of:
- Complete heart block
- Aortic valve distortion or regurgitation
- Residual shunt
- Device embolization
Meticulous preprocedural imaging, careful avoidance of device oversizing, and continuous intraprocedural echocardiographic guidance are essential to minimize complications. Patient selection remains critical, particularly in small, restrictive defects without a significant hemodynamic burden.
Indications
According to the American Heart Association/American College of Cardiology (AHA/ACC), recommendations for VSD closure are as follows:
- Patients with left ventricular volume overload and hemodynamically significant shunts (Qp: Qs ≥1.5:1) should undergo VSD closure if pulmonary artery systolic pressure is less than 50% of systemic pressure and pulmonary vascular resistance is less than one-third of systemic vascular resistance.
- Surgical closure of perimembranous or supracristal VSD is reasonable in adults in the presence of worsening aortic regurgitation secondary to the VSD.
- Surgical closure of a VSD may also be reasonable in adults with a history of infective endocarditis secondary to a VSD if not otherwise contraindicated.
- Consider VSD closure in a net left-to-right shunt (Qp: Qs ≥1.5:1) when pulmonary artery systolic pressure is 50% or more than systemic, or pulmonary vascular resistance is greater than one-third systemic.
- Surgical VSD closure is currently the recommended approach. Meanwhile, percutaneous transcatheter VSD closure is recommended for patients who are nonsurgical candidates. Transcatheter closure is also a viable alternative to surgical intervention if conduction abnormalities are a concern.[2]
Contraindications
According to the AHA/ACC guidelines, VSD closure should not be performed in adults with severe pulmonary artery hypertension with pulmonary artery systolic pressure greater than two-thirds systemic, pulmonary vascular resistance greater than two-thirds systemic, and a net right-to-left shunt.[2] Several complications may occur even in patients with small VSDs and may warrant surgical closure, including left or right ventricular outflow tract obstruction and prolapse of an aortic valve cusp.
Equipment
The following equipment is necessary for the catheter management of ventricular septal defects:
Vascular Access Equipment:
- Sterile preparation and draping set
- Local anesthetic agents
- Arterial and venous sheaths (5F–8F or larger depending on device size)
- Introducer needles and guidewires (0.035″ standard, hydrophilic wires)
Diagnostic Catheters:
- Judkins Right catheter
- Multipurpose catheter
- Right coronary or internal mammary catheter (for crossing the defect if needed)
- Pigtail catheter (for left ventricular angiography)
Guidewires:
- 0.035″ J-tip guidewire
- Hydrophilic-coated guidewire
- Exchange-length stiff guidewire
- Coronary wire (in selected cases for defect crossing)
Arteriovenous Loop Equipment
- Gooseneck snare system
- Long sheath for externalization of wire
Delivery System
- Long delivery sheath (appropriate size based on device)
- Delivery cable
- Loader system
Occluder Devices
- Muscular VSD occluder device (Amplatzer muscular VSD device, ADO type I and II)
- Perimembranous VSD occluder (new Amplatzer perimembranous VSD occluders include a symmetrical type and an asymmetrical type)
- Alternative devices (eg, duct occluder II in small muscular VSDs)
- Other devices available for VSD closure include the Cocoon VSD occluder (A), the aneurysmal type; the Nit-Occlud VSD coil (B); and the KONAR-Multifunctional VSD occluder (C).
Imaging Equipment
- Fluoroscopy with cineangiography capability
- Transesophageal echocardiography or intracardiac echocardiography
- Transthoracic echocardiography for follow-up
Hemodynamic Monitoring
- Pressure transducers
- Manifold system
- Contrast media
Personnel
An interprofessional team is needed for successful percutaneous catheterization of a VSD, including, but not limited to, an interventional/structural cardiologist, pediatric cardiologist, anesthesiologist, cardiothoracic surgeon, radiologist, and ancillary staff.[5]
Preparation
Preparation for percutaneous transcatheter VSD closure begins with an evaluation of the patient to assess if he qualifies for catheter closure. This evaluation is most commonly performed with a TTE, which assesses the size and location of the VSD, followed by cardiac catheterization to evaluate for pulmonary hypertension. For safe VSD closure using devices, an adequate distance (≥2 mm) from the aortic valves should be maintained. Additional preoperative tests may include chest x-rays, ECGs, and blood tests to assess the patient's general health and kidney function.
Before the procedure, all patients undergoing VSD closure should be pretreated with antiplatelet therapy, commonly with both aspirin and clopidogrel daily. Warfarin therapy alone may be an option in patients who need chronic antithrombotic therapy, followed by bridging with low-molecular-weight heparin before and after VSD closure. An intravenous antibiotic dose should be given 1 hour before percutaneous access, typically cefazolin or vancomycin, if the patient is allergic to penicillin.
Patients should also receive intravenous normal saline before and during the procedure to avoid left atrial hypovolemia. All patients should be evaluated by anesthesia before the procedure. Typically, patients under 10 undergo general anesthesia, and conscious sedation is used for patients older than 10.[6]
Technique or Treatment
The antegrade approach remains the traditional and most widely adopted technique for transcatheter VSD closure. This strategy involves creating an arteriovenous wire loop, with device delivery through the venous system, most commonly through the femoral vein or, in selected cases, the internal jugular vein. The internal jugular approach may offer improved alignment and support for muscular VSDs located in the apical septum.
In contrast, a retrograde approach via the femoral artery may be considered in selected small defects. This technique eliminates the need for arteriovenous loop formation and is particularly suited to low-profile, symmetrical occluder devices. Careful patient and device selection are essential when considering this strategy.
Systemic anticoagulation is mandatory before device manipulation. A bolus of intravenous heparin, followed by a continuous infusion, should be administered to maintain adequate anticoagulation throughout the procedure. Angiographic profiling of the VSD is typically performed using left ventricular injection in a 55-degree left anterior oblique projection with 20-degree cranial angulation. This view allows optimal delineation of:
- Defect location
- Maximal diameter
- Septal rims
- Relationship to the aortic valve
The VSD diameter should be measured at peak diastole, when the defect is largest. Device selection must be individualized according to VSD type, morphology, and measured dimensions.
Antegrade Technique
Following confirmation of suitability for intervention, femoral venous access is obtained, and an arteriovenous circuit is established. A 5 Fr Judkins right catheter and a hydrophilic J-tipped guidewire are advanced from the left ventricle across the defect. The wire is then snared in the pulmonary artery or superior/inferior vena cava to create an AV loop.
Meticulous care is required during this step to avoid entanglement with tricuspid valve chordae. Once the arteriovenous loop is secured, a long delivery sheath (typically 6–12 Fr) is advanced over the wire into the left ventricle and positioned just below the aortic valve. The occluder device is then deployed under combined fluoroscopic and echocardiographic guidance. Postdeployment angiography of the left ventricle and ascending aorta is essential to confirm:
- Adequate device position
- Complete or near-complete occlusion
- Absence of new-onset aortic regurgitation
Retrograde Technique
When employing the retrograde approach, the delivery catheter is advanced from the femoral artery across the VSD into the right ventricle without formation of an arteriovenous loop. The device is typically partially deployed within the right ventricle before final positioning and complete deployment across the defect. This technique may reduce procedural complexity in appropriately selected small defects.
Patients should be monitored in an inpatient setting for at least 24 hours with continuous ECG surveillance, as the early postprocedural period carries the highest risk of conduction disturbances and arrhythmias. Antiplatelet therapy with aspirin is recommended for 6 months to reduce the risk of device-related thromboembolism.
Complications
Complications of catheter use in VSDs include:
- Arrhythmias
- The most common complication of VSD closure is. Patients have a 4.6% to 17% risk of arrhythmia following device implantation.[7] While most arrhythmias occur within 1 day to 1 week postoperatively, transient atrioventricular block and complete heart block have been noted intraoperatively, with a prevalence of about 1.6%. Common postoperative arrhythmias include right bundle branch block (6.4%), left bundle branch block (1.6%), sinus tachycardia (3.2%), and second-degree atrioventricular block (1.09%).[8] The risk of pacemaker dependence is approximately 3.8%, according to Carminatti et al.[9] There is evidence that arrhythmia risk varies by VSD type. For example, complete heart block seems to occur more often in perimembranous VSD compared to muscular VSDs.[9] Trivial residual shunt: A trivial residual shunt occurs when venous blood enters the bloodstream without passing through functional lung tissue without hemodynamic compromise. Approximately 5 to 6.7% of patients who undergo VSD closure develop a trivial residual shunt.[9][10]
- Trivial residual shunt
- Aortic regurgitation
- According to the results from a study, the rate of aortic regurgitation following VSD device closure is approximately 3.4%.[7]
- Tricuspid Regurgitation
- Tricuspid regurgitation was noted in several case studies. Post-VSD closure tricuspid regurgitation is thought to be secondary to direct trauma to the tricuspid valve.[11]
- Iatrogenic embolization of the VSD occluder
- The rate of device embolization is approximately 0.82%.[12] Data suggest an association between device embolization, small device sizes, and incompetent aortic rims. Despite possible device embolization, most embolic phenomena are retrievable by percutaneous catheter extraction.
- Endocarditis
- While rare, the occurrence rate ranges from 0.3% to 0.9%. More extensive studies may be needed to determine a more accurate prevalence estimate.[13]
- Pulmonary hypertension
Clinical Significance
The development of percutaneous transcatheter interventions for VSD is a considerable advancement in cardiology today. While VSD is one of the most common cardiac defects worldwide, this technique now provides a treatment option for a large population who previously would have only been offered medical management.
Enhancing Healthcare Team Outcomes
Catheter-based management of VSDs requires coordinated interprofessional collaboration among interventional cardiologists, cardiothoracic surgeons, advanced practitioners, anesthesiologists, imaging specialists, nurses, pharmacists, and catheterization laboratory personnel to optimize procedural safety and patient outcomes.[5] Successful patient-centered care begins with careful patient selection and multidisciplinary evaluation of defect size, location, hemodynamic significance, ventricular function, pulmonary pressures, and surrounding cardiac anatomy using echocardiography and advanced imaging modalities. Interventional cardiologists and congenital heart specialists collaborate with cardiac surgeons to determine whether transcatheter closure or surgical repair is the most appropriate treatment strategy, particularly in complex defects or patients with associated congenital anomalies. Imaging specialists play a critical role in procedural planning and real-time intraprocedural guidance using transesophageal or intracardiac echocardiography. Advanced practitioners and nursing staff contribute to patient education, preprocedural preparation, vascular access management, hemodynamic monitoring, and postprocedural surveillance for arrhythmias, residual shunting, device embolization, or vascular complications.
Effective communication and procedural coordination among all team members are essential during catheter-based VSD closure because device positioning, hemodynamic assessment, anticoagulation management, and rapid recognition of complications require continuous multidisciplinary interaction. Anesthesiologists maintain hemodynamic stability and facilitate imaging guidance, while pharmacists assist with anticoagulation protocols, medication reconciliation, and prevention of drug-related adverse events. Postprocedural care requires coordinated monitoring by physicians, nurses, telemetry personnel, and rehabilitation teams to identify conduction abnormalities, hemolysis, residual defects, thromboembolic complications, or heart failure symptoms. Structured communication, standardized procedural protocols, and collaborative decision-making enhance patient safety, improve procedural success rates, reduce complications, and support long-term functional outcomes in patients undergoing catheter management of ventricular septal defects.
Media
(Click Image to Enlarge)
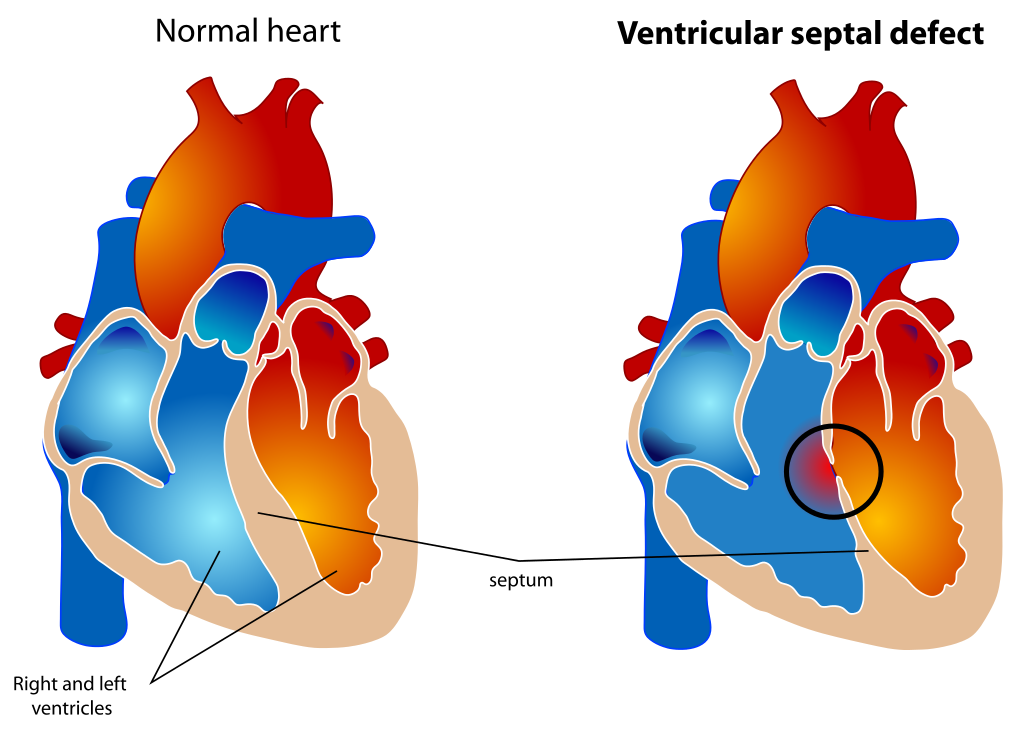
Ventricular Septal Defect. The diagram depicts a healthy heart on the left and a heart with the 4 anatomic malformations characteristic of the Tetralogy of Fallot on the right.
Mariana Ruiz, Public Domain, via Wikimedia Commons.
References
Liu F, Yang YN, Xie X, Li XM, Ma X, Fu ZY, Chen BD, Huang Y, Shan CF, Ma YT, Gao XM. Prevalence of Congenital Heart Disease in Xinjiang Multi-Ethnic Region of China. PloS one. 2015:10(8):e0133961. doi: 10.1371/journal.pone.0133961. Epub 2015 Aug 28 [PubMed PMID: 26317413]
Lock JE, Block PC, McKay RG, Baim DS, Keane JF. Transcatheter closure of ventricular septal defects. Circulation. 1988 Aug:78(2):361-8 [PubMed PMID: 3396173]
Lin CH, Huddleston C, Balzer DT. Transcatheter ventricular septal defect (VSD) creation for restrictive VSD in double-outlet right ventricle. Pediatric cardiology. 2013 Mar:34(3):743-7. doi: 10.1007/s00246-012-0337-1. Epub 2012 May 12 [PubMed PMID: 22580772]
Level 3 (low-level) evidencePrakoso R, Ariani R, Kurniawati Y, Mendel B, Lilyasari O. Transthoracic echocardiography-guided subaortic ventricular septal defect closure in infants: a case report. Frontiers in cardiovascular medicine. 2025:12():1647073. doi: 10.3389/fcvm.2025.1647073. Epub 2025 Sep 24 [PubMed PMID: 41070087]
Level 3 (low-level) evidenceKutty S, Delaney JW, Latson LA, Danford DA. Can we talk? Reflections on effective communication between imager and interventionalist in congenital heart disease. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2013 Aug:26(8):813-27. doi: 10.1016/j.echo.2013.05.006. Epub 2013 Jun 13 [PubMed PMID: 23768692]
Thakkar B, Patel N, Bohora S, Bhalodiya D, Singh T, Madan T, Shah S, Poptani V, Shukla A. Transcatheter device closure of perimembranous ventricular septal defect in children treated with prophylactic oral steroids: acute and mid-term results of a single-centre, prospective, observational study. Cardiology in the young. 2016 Apr:26(4):669-76. doi: 10.1017/S1047951115001018. Epub 2015 Jun 24 [PubMed PMID: 26105182]
Level 2 (mid-level) evidenceJortveit J, Leirgul E, Eskedal L, Greve G, Fomina T, Døhlen G, Tell GS, Birkeland S, Øyen N, Holmstrøm H. Mortality and complications in 3495 children with isolated ventricular septal defects. Archives of disease in childhood. 2016 Sep:101(9):808-13. doi: 10.1136/archdischild-2015-310154. Epub 2016 Apr 18 [PubMed PMID: 27091847]
Xie YM, Zhang ZW, Li YF, Qian MY, Wang HS. [Management of the arrhythmia around the procedure of transcatheter closure of ventricular septal defects in pediatric patients]. Zhonghua xin xue guan bing za zhi. 2005 Dec:33(12):1092-4 [PubMed PMID: 16563277]
Level 2 (mid-level) evidenceCarminati M, Butera G, Chessa M, De Giovanni J, Fisher G, Gewillig M, Peuster M, Piechaud JF, Santoro G, Sievert H, Spadoni I, Walsh K, Investigators of the European VSD Registry. Transcatheter closure of congenital ventricular septal defects: results of the European Registry. European heart journal. 2007 Oct:28(19):2361-8 [PubMed PMID: 17684082]
Level 2 (mid-level) evidenceChessa M, Carrozza M, Butera G, Negura D, Piazza L, Giamberti A, Feslova V, Bossone E, Vigna C, Carminati M. The impact of interventional cardiology for the management of adults with congenital heart defects. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions. 2006 Feb:67(2):258-64 [PubMed PMID: 16416475]
Matyal R, Wang A, Mahmood F. Percutaneous ventricular septal defect closure with Amplatzer devices resulting in severe tricuspid regurgitation. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions. 2013 Nov 15:82(6):E817-20. doi: 10.1002/ccd.24803. Epub 2013 Jul 1 [PubMed PMID: 23553968]
Level 3 (low-level) evidenceDurham JA, Scansen BA, Bonagura JD, Schober KE, Cheatham SL, Cheatham JP. Iatrogenic embolization and transcatheter retrieval of a ventricular septal defect occluder in a dog. Journal of veterinary cardiology : the official journal of the European Society of Veterinary Cardiology. 2015 Dec:17(4):304-13. doi: 10.1016/j.jvc.2015.08.003. Epub 2015 Oct 26 [PubMed PMID: 26515420]
Nguyen HL, Phan QT, Dinh LH, Tran HB, Won H, Thottian JJ, Duc DD, Quang TN, Kim SW. Nit-Occlud Lê VSD coil versus Duct Occluders for percutaneous perimembranous ventricular septal defect closure. Congenital heart disease. 2018 Jul:13(4):584-593. doi: 10.1111/chd.12613. Epub 2018 Jul 17 [PubMed PMID: 30019378]
Bambul Heck P, Eicken A, Kasnar-Samprec J, Ewert P, Hager A. Early pulmonary arterial hypertension immediately after closure of a ventricular or complete atrioventricular septal defect beyond 6months of age. International journal of cardiology. 2017 Feb 1:228():313-318. doi: 10.1016/j.ijcard.2016.11.056. Epub 2016 Nov 9 [PubMed PMID: 27866021]