Introduction
The pelvic floor is a musculofascial complex forming the inferior boundary of the pelvis, composed primarily of the levator ani (pubococcygeus, puborectalis, iliococcygeus) and coccygeus muscles, supported by the endopelvic fascia and perineal membrane (see Image. Anatomy of the Pelvic Floor). The region encloses the urinary, genital, and anorectal compartments. Vascular supply arises mainly from the internal pudendal vessels, while innervation is provided by the pudendal nerve and contributions from the sacral plexus. The pelvic floor supports pelvic viscera, maintains continence, facilitates defecation and micturition, and contributes to respiration and lumbopelvic stability. Physiologic variation occurs with age, sex, and body habitus, influencing muscle tone, support, and functional capacity.
Pelvic floor dysfunction manifests as urinary and fecal incontinence, organ prolapse, constipation, and chronic pelvic pain, reflecting impaired muscular support, coordination, or neural control. Clinical procedures involving the prostate, pelvic organs, and continence mechanisms depend on preservation or restoration of pelvic floor integrity to optimize postoperative function and outcomes. Detailed knowledge of pelvic floor anatomy and function enables accurate diagnosis, targeted rehabilitation, appropriate selection of imaging and interventions, and improved management of complex pelvic disorders.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The pelvic floor is a distinct anatomical region in which the balance of visceral, muscular, and fluid pressures plays a fundamental role in the physiological function of the contained structures. The pelvis is bounded superiorly by an imaginary line extending from the pubis to the sacral promontory and inferiorly by a line between the ischial tuberosities and the apex of the coccyx, separating the pelvis from the perineum.[1][2][3] From an anatomical perspective, the pelvic floor is divided into 4 compartments, as follows:
- Anterior (urinary): bladder, bladder neck, urethra
- Middle (genital): vagina and uterus in females individuals; prostate in male individuals
- Posterior: anus, anal canal, sigmoid colon, rectum
- Peritoneal: endopelvic fascia, perineal membrane
The anatomical organization of the pelvic floor includes the following components:
- Pelvic diaphragm: composed of the ischiococcygeus muscle and levator ani muscles; superiorly reinforced by the endopelvic fascia.
- Urogenital diaphragm (triangular ligament or fascia of Carcassonne): located caudally between the ischium and pubic symphysis; traversed by the urethra and, in female individuals, the vagina.
- Perineum (perineal membrane): continuation of the fascial system; connects the deep pelvic floor musculature with the coccyx and the anal sphincter complex.
This organizational framework provides a structured anatomical perspective of the pelvic floor by delineating its principal supporting layers and their spatial relationships. Clear compartmentalization facilitates correlation between structural anatomy and functional interactions relevant to continence, pelvic support, and surgical orientation.
Respiration
At rest, the pelvic floor maintains a cupuliform shape resembling the respiratory diaphragm. During contraction, the pelvic floor ascends in an anterosuperior direction toward the pubis, whereas relaxation produces a posteroinferior displacement toward the sacrum and ischium, with an overall excursion of approximately 3 cm. Coccygeal movement accompanies these changes, with anterosuperior displacement during contraction and posteroinferior displacement during relaxation.
The pubococcygeal line is defined as the line extending between the pubic symphysis and the coccyx, whereas the anorectal angle denotes the angle formed between the posterior rectal wall and the axis of the anal canal. Both parameters may be assessed using pelvic magnetic resonance imaging (MRI). In healthy individuals, the base of the bladder, the upper 1/3 of the vagina, and the peritoneal cavity are positioned at or adjacent to the pubococcygeal line, whereas the anorectal angle remains cranial or adjacent to this reference line.
Pelvic floor contraction results in visceral elevation and conversion of the anorectal angle into a more acute configuration. Pelvic floor musculature supports the male and female pelvic viscera and the rectum, contributing to coordinated pressure regulation during contraction and relaxation. Pressure modulation generated by pelvic floor activity assists visceral function, including continence and evacuation mechanisms, and contributes to sexual function.
Respiratory mechanics are integrated with pelvic floor dynamics. Respiratory diaphragm descent during inspiration is accompanied by caudal displacement of the pelvic diaphragm, reducing resistance to respiratory movement, whereas the opposite pattern occurs during expiration. Therefore, pelvic diaphragm activity contributes to respiratory biomechanics through coordinated contractile behavior.[4][5] Clinical understanding of pelvic floor function requires concurrent consideration of respiratory mechanics and their integrated physiological interactions.[6][7]
Posture
Another important function of the pelvic floor is postural stabilization, in coordination with the respiratory diaphragm and abdominal musculature. Muscular groups responsible for stabilization of the thoracolumbar and lumbosacral columns require coordinated activation to permit trunk rotation, transition between sitting and standing, maintenance of orthostatism, and execution of the cough and sneeze reflexes. Coordinated activation involves the abdominal musculature, including the diaphragm, transverse abdominis, and oblique muscles. The pelvic floor musculature also participates in coordinated activation, together with associated muscles such as the obturator internus, piriformis, and adductors. The gluteus maximus is likewise engaged as part of this integrated muscular system.
The diaphragm integrates anteriorly through the transversalis fascia and posteriorly through the thoracolumbar fascia, establishing continuity with the anterior pelvic floor at the pubic region and the posterior pelvic floor at the sacrum. The rectus abdominis and its fascial system merge at the pubic symphysis with the adductor musculature, both contributing to pelvic floor contraction.
Anatomical continuity between the pelvic floor and the gluteus maximus contributes to coordinated pelvic and lower limb function. Pelvic floor contraction facilitates load transfer between the trunk, upper limbs, and lower limbs during gait and orthostatism through these myofascial connections. Foot positioning is influenced by pelvic floor tone through effects on hip rotator muscle activity, with downstream modulation of adjacent contractile regions.
Embryology
From an embryological perspective, the muscular component of the pelvic region, together with the initial development of the pelvic organs, arises from 2 distinct muscle groups. These groups include the pubocaudal and Gegenbauer muscles, the latter located in proximity to the cloacal region.
The pubocaudal muscle group gives rise to the ischiococcygeus and levator ani muscles. This group also forms the pubosacral or pubourethral–bladder–rectosacral ligaments in male embryos. In female embryos, the same group contributes to the pubourethral–bladder–uterus–rectosacral ligaments.
The Gegenbauer muscle group contributes to the formation of pelvic floor musculature following the descent of the genitourinary septum. This septum separates the rectum posteriorly from the bladder and urethra in male embryos, and from the bladder, urethra, and vagina in female embryos. This muscle group gives rise to the sphincter musculature of the anus and urethra. Additional derivatives include the bulbocavernosus, ischiocavernosus, and superficial and deep transverse perineal muscles.
In the fetus, these muscular and ligamentous structures are organized as a functional unit. This organization is characterized by coordinated contraction and integrated physiological activity.
Blood Supply and Lymphatics
The internal pudendal artery is the primary arterial supply (see Image. Neurovascular Structures of the Perineal Region). The vessel originates from the internal iliac artery and subsequently divides into the inferior rectal and perineal arteries. Anterior branches include the urethral artery, penile arteries in male individuals, and arteries of the vestibule and clitoris in female individuals. Venous drainage via the internal pudendal veins terminates in the internal iliac vein within the pelvis (see Image. Pelvic Blood Vessels). The external pudendal veins drain anteriorly into the femoral vein of the thigh. Deep lymphatic drainage primarily targets the internal iliac lymph nodes within the pelvis. Lymphatic drainage from the external genitalia primarily courses toward the superficial inguinal lymph nodes.
Nerves
Pelvic muscle innervation is complex and involves both autonomic and somatic systems. Key components include the superior hypogastric plexus with hypogastric nerves, the pelvic splanchnic nerves, the inferior hypogastric (pelvic) plexus, and the pudendal nerve. The autonomic system, particularly the parasympathetic component, forms synaptic connections with the myenteric plexus of the rectum and the anal canal.
Pelvic musculature demonstrates both voluntary and involuntary control. Voluntary contraction of the pelvic floor occurs during intentional motor activities, such as physiotherapy. Involuntary activation occurs during coordinated motor patterns involving the upper and lower limbs, trunk musculature, breathing, and coughing. Neural substrates underlying these automatic synergies are incompletely understood.
Cortical representation of pelvic musculature is located along the medial aspect of the precentral gyrus. Activation occurs in association with voluntary motor commands and coordinated pelvic motor activity. Premotor cortical activation precedes contraction and is modulated by higher cortical centers that determine functional necessity. Additional involvement in involuntary pelvic floor activity associated with respiration has been described within brainstem centers, including the retroambiguus nucleus of the medulla oblongata. Integration involves coordinated activity between the respiratory diaphragm, abdominal wall, and tongue during respiratory cycles, including inspiratory and expiratory phases. Neurophysiological mechanisms governing these interactions are not fully elucidated.[8][9]
Muscles
The pelvic diaphragm, first described in 1861, consists of the levator ani complex, formed by the coccygeus (ischiococcygeus), iliococcygeus, pubococcygeus, and puborectalis (see Image. Levator Ani Components).[10][11][12] The iliococcygeus and pubococcygeus originate from the pectineal line of the pubic bone and the fascia of the obturator internus muscle. Insertion occurs toward the coccyx, ischial spine, sacrum, and triangular ligament (urogenital diaphragm). The puborectalis originates from the inferior pubic ramus.
The pubococcygeus and related components are also described as pubovisceral muscles due to functional continuity with pelvic viscera. These muscular components connect with the urethra, vagina, perineal body, and anal canal, forming pubourethral, pubovaginal, puboperineal, and puboanal functional units.
Approximately 2/3 of the contractile fibers consist of type I (slow-twitch, oxidative) fibers, while the remaining proportion consists of type II (fast-twitch, glycolytic) fibers. These muscles function as an integrated unit with limited structural separation between individual components. Fiber orientation demonstrates multidirectional organization within a 3-dimensional functional architecture. Tractographic analyses describe a complex fiber network consistent with integrated pelvic floor mechanics.
Urogenital Diaphragm
The urogenital diaphragm, located beneath the pelvic floor, is formed by the perineal medial aponeurosis or fascia, including the deep transverse perineal muscle, and serves as a reinforcement connecting the pelvic diaphragm to the perineum. The anterior portion is traversed by the urinary and genital tracts, situated between the 2 ischiopubic rami and oriented with its apex directed toward the pubic symphysis. The pre-urethral region, or transverse ligament of the perineum, maintains continuity with the ischiopubic rami and the obturator fascia. The retro-urethral region is divided into superior and inferior layers, with the Guthrie muscle (deep transverse perineal muscle) located between these layers. The superior aponeurotic lamina extends toward the transverse perineal muscle, whereas the deeper lamina merges with the Denonvilliers fascia, which covers the prostate and seminal vesicles.
Perineum
The perineum is the continuation of the urogenital diaphragm posteriorly and the levator ani muscle inferiorly, with boundaries that are difficult to delineate. Muscular continuity extends to the urethra, vagina or prostate, and rectum, reaching the coccyx via the anococcygeal raphe. Muscles and viscera are embedded within a network of connective tissue or fascia. Within this matrix, all enclosed structures perceive and transmit changes in tension, reflecting integrated mechanical behavior consistent with the concept of biotensegrity. Fascia functions as a mechanical force-transmission system involving the entire body. Cervical flexion involving the deep cervical fascia influences the position of distal musculoskeletal regions, including the lower limb, through fascial continuity and tension transfer. The fascial system precedes the development and organization of contractile muscle units.
Endopelvic Fascia
Below the peritoneum, the endopelvic fascia covers the superior aspect of the pelvic floor (see Image. Anatomic Reflections of the Endopelvic Fascia). Coverage extends to the obturator internus, piriformis, and levator ani muscles, with continuation through a transverse band that merges with the pubic periosteum. Along the fascial course, posterior integration occurs with the pubosacral ligament, forming a connective “cup” that envelops the musculoskeletal structures of the pelvic floor, the urogenital diaphragm, and the perineal region. The endopelvic fascia encloses pelvic viscera and establishes structural continuity with surrounding musculature and osseous elements.
Fascial pathways guide vascular structures through defined connective sheaths, including the hypogastric sheath (connecting the pubic bone to the sacrum), the umbilical-prevesical sheath (defining the retropubic space), and the vesicorectal sheath associated with vesicular-deferential vessels. The fascia of Denonvilliers also contributes to posterior pelvic compartmentalization, enveloping the middle rectal vascular structures.
Recent studies demonstrate anatomical and functional continuity between the gluteus maximus and the levator ani within the ischioanal region. Connectivity is mediated by the gluteoperineal muscle and associated connective tissue bundles linking the gluteus maximus directly to the pelvic floor musculature.[13][14]
Physiologic Variants
Advanced age in women alters key characteristics of the pelvic floor. Muscular tone decreases, resulting in widening of the genital hiatus, more caudal orientation of the iliococcygeus fiber vectors, and reduced thickness of the posterior portion of the puborectalis muscle. Furthermore, excessive body weight contributes to increased rectal distension and caudal displacement of the perineal region, cervix, and bladder neck.[15]
In men, body weight exerts a greater influence on pelvic floor morphology and function. Excess weight with aging leads to increased tissue distension, resulting in elongation of the perineal region and reduced muscular strength, with associated thinning of the ischiocavernosus and puborectalis.
Surgical Considerations
Pelvic floor dysfunction may arise from obstetric, urologic, and colorectal surgical interventions through disruption of structural support or neural pathways. Vaginal delivery involves the passage of the fetus through the birth canal, producing distension of the pelvic outlet with mechanical stress on the levator ani, perineal body, and pudendal nerve, potentially resulting in avulsion, perineal trauma, or pudendal nerve neuropraxia (transient conduction block due to stretch or compression) and subsequent pelvic floor dysfunction. Cesarean section, indicated when vaginal delivery poses maternal or fetal risk, avoids direct pelvic floor strain during delivery, thereby preventing stretch-related injury mechanisms inherent in vaginal birth.[16]
Radical prostatectomy may affect continence through disruption of the external urethral sphincter complex, endopelvic fascia, and associated autonomic or somatic innervation.[17] Colorectal cancer surgery may compromise continence and defecatory function through injury to the anorectal sphincter complex, pelvic autonomic plexus, or distortion of the anorectal angle. [Almughamsi & Elhassan. Pelvic Neuroanatomy in Colorectal Surgery: Advances in Nerve Preservation for Optimized Functional Outcomes. 2025]
Clinical Significance
Deficiency in pelvic floor muscle tone or electrical dysfunction within these regions is associated with multiple disorders and pathologies, including visceral prolapse, urinary incontinence, and fecal constipation. The estimated prevalence of pelvic floor muscle disorders is projected to increase by approximately 35% over the next 2 decades, reaching an average of 1.6 million visits annually by 2030. The highly variable and complex pathogenesis may involve the following:
- Birth injury
- Advanced age
- Obesity
- Chronic pathological conditions associated with increased intra-abdominal pressure
- Previous surgical interventions in the pelvic region
Major disorders of the anterior compartment include dysuria, urinary frequency, cystocele, and urinary incontinence. Vaginal or uterine prolapse typically represents central compartment involvement. Posterior compartment changes are associated with pelvic or anal pain, constipation, rectal prolapse, and fecal incontinence. Peritoneal compartment involvement may result in dyspareunia, constipation, and low back pain secondary to alterations in the rectum and sigmoid colon.
Stress Urinary Incontinence
Pelvic floor disorders may involve isolated compartments or the entire pelvic floor complex. Stress urinary incontinence (SUI), the most common form of urinary incontinence, occurs during increases in intra-abdominal pressure, such as coughing or sneezing, when pressure exceeds the capacity of muscular control mechanisms. SUI affects approximately 26% of women aged 30 to 59 years, with peak prevalence between 40 and 49 years. Etiology involves not only the levator ani muscle but also its functional interaction with adjacent musculature and joint structures. Evidence indicates that pelvic floor activity may act in opposition to the respiratory diaphragm. Impaired pelvic floor function may result in inadequate distribution of forces generated during trunk and limb movements.
Decreased electrical activity or altered electromyographic patterns may be observed in affected musculature. Postural alterations of the lumbar spine influence pelvic floor electrical activity. Loss of pelvic tilt associated with lumbar hypolordosis alters pelvic alignment, including posterior pelvic inclination, anterior sacral displacement, and anterior-inferior orientation of the pubis. These biomechanical changes increase vertical loading on pelvic floor structures during gait, resulting in repetitive fiber strain. Progressive weakening of the levator ani may occur under sustained mechanical stress.
In individuals with hypolordosis, increased visceral pressure within the pelvic cavity during orthostasis is associated with altered electromyographic activity of pelvic musculature. These changes are considered by clinicians to affect continence mechanisms negatively in patients with pelvic floor dysfunction. SUI in male individuals is commonly associated with prior surgical prostatectomy.
Urinary incontinence is frequently observed in patients who have undergone radical prostatectomy. A recent systematic review emphasizes the potential for improved urinary control through pelvic floor muscle training (PFMT) prior to surgery as a preventive intervention. PFMT may assist in the recovery of urinary continence in some patients within 3 months postoperatively. However, further studies are required to confirm these findings.[18] In women, PFMT following pregnancy-related urinary incontinence contributes to restoration of bladder function, whether applied alone or in combination with therapeutic modalities like electrical stimulation and biofeedback.[19]
Sacral neuromodulation, developed in the 1990s, is a minimally invasive surgical technique involving implantation of a sacral “pacemaker.” This device delivers electrical impulses to modulate pelvic organ function, including the bladder and bowel, thereby alleviating pelvic floor–related symptoms. Sacral neuromodulation is widely accepted when PFMT is insufficient. Despite procedural safety and established clinical utility, the precise mechanisms underlying sacral neuromodulation remain incompletely understood.[20][21]
Nonrelaxing pelvic floor dysfunction is a poorly understood and frequently misdiagnosed condition. Clinical presentation may mimic impaired neuromuscular control of pelvic musculature and visceral function. Diagnostic evaluation may include superficial electromyography and video urodynamics to support diagnostic accuracy.[22]
Pelvic Organ Prolapse and Constipation
Pelvic organ prolapse resulting from pelvic floor muscle weakness affects approximately 30% to 50% of women and may lead to urinary and rectal dysfunction, as well as sexual dysfunction. Data regarding rectal prolapse in men remain limited. Constipation affects approximately 27% of the population, with higher prevalence in women. Contributing factors include pelvic floor dysfunction, paradoxical muscle contraction, generalized muscular weakness, and incomplete relaxation following contraction. Fecal accumulation within the rectum may contribute to urinary or visceral prolapse.
Pain
Pelvic floor–related pain is another clinical manifestation of pelvic floor dysfunction. Several conditions, including interstitial cystitis (bladder pain syndrome), chronic prostatitis, provoked vestibulodynia, and chronic vulvar pain disorder, may present with heterogeneous symptoms but share a common underlying feature of painful muscle dysfunction, including spasm, trigger points, and hypotonia.
Myofascial pelvic pain affects approximately 14% to 23% of women, although prevalence estimates are likely underestimated and less reliable in men. Myofascial pelvic pain is characterized by pain originating from muscular and connective tissue and may present as an isolated symptom or as a constellation of urological, gynecological, and colorectal manifestations. Pain sources extend beyond the pelvic floor, urogenital diaphragm, and perineal membrane to include adjacent myofascial structures, such as the piriformis and obturator internus muscles.
Pain may radiate from an initial site to the gluteal region, abdomen, lumbar spine, thorax, pelvis, and lower limbs. Musculature may develop trigger points under various conditions. Etiological factors are diverse and may be concomitant, including trauma or injury, scar formation, chronic postural alterations, metabolic dysfunction, nutritional deficiencies, and psychological stress. Persistent alteration in muscle fiber length may result in impaired circulation, hypoperfusion, and ischemia, with the development of trigger points, which may remain latent for extended periods.
Pain arises when a trigger point is activated, for example, during movement or physiological activity that involves stretching or compression of myofascial tissue. Persistent nociceptive stimulation may induce neuroplastic changes in the peripheral or central nervous system, resulting in central sensitization. Central sensitization is associated with increased responsiveness of medullary neurons, manifested as allodynia, and may persist after removal of the initial stimulus, resulting in hyperalgesia and secondary hyperalgesia involving noninjured tissues.
Connective tissue may function as a source of pain when metabolic activity decreases, and adaptability to mechanical stress is reduced. Connective tissue contains nociceptors capable of transmitting pain signals by converting mechanical stimuli into nociceptive information. Under nonphysiological mechanical loading, proprioceptors may undergo phenotypic change into nociceptors.
Reduced sliding between fascial layers limits endocannabinoid system function. The fascial system also contributes to the regulation of contractile tissue tension. Proprioceptors within connective tissue, including ligaments, respond to stretching through medullary reflex pathways, inducing muscle contraction that counteracts fascial tension and maintains appropriate balance between contraction and relaxation.
Altered muscle tone may lead to dysfunction of pelvic joints, with subsequent joint-related pain generation. A self-perpetuating cycle may develop in which load-transfer mechanisms fail during movement, resulting in progressive pain and dysfunction. Pelvic floor dysfunction may be associated with nonspecific symptoms, including respiratory disorders, low back pain, sacroiliac joint pain (SIJ), and pelvic girdle pain.
Abnormal pelvic floor muscle tension may also contribute to compression or entrapment neuropathies analogous to those observed in the upper and lower limbs. Pudendal nerve syndrome, also known as Alcock canal syndrome, is frequently associated with muscular hypertonia. The pudendal nerve (S2–S4) traverses the Alcock canal between the sacrospinous and sacrotuberous ligaments at the level of the ischial spine, in relation to the fascia of the obturator internus muscle. Entrapment of the pudendal nerve results in unilateral pain involving the genital region, anus, and pelvic area.
Evaluation of the Pelvic Floor
General manual and instrumental medical evaluation of the pelvic floor is described in the literature. No single manual examination technique provides a comprehensive assessment of all pelvic floor components. Evaluation begins with an anamnestic interview and visual assessment for nonphysiological changes. Active movements of the lower limbs and lumbar spine are examined, along with associated symptoms. Posture, orthostatism, and gait are inspected, as altered body alignment may generate compensatory stress on the pelvic floor.
Manual examination primarily focuses on the assessment of pelvic muscle contraction, quantification of strength, and identification of trigger points. External examination of the abdominal region, thigh, gluteal region, and perineal area is performed to detect trigger points. Intravaginal or rectal palpation is also used to identify areas of tenderness.
Internal examination includes voluntary pelvic floor contraction to assess motor control and pain response. The Q-tip test is used to evaluate trigger points and painful areas during intravaginal palpation. Pain is graded on a scale from 0 to 10, with 0 indicating the absence of pain and 10 indicating maximal pain. Muscle strength is graded from 0 to 5 based on the Chiararelli scale, where 0 indicates no contraction, and 5 indicates normal physiological function.
A proposed method involves external assessment of the coccyx by placing the palm over the coccygeal region in both sitting and lateral decubitus positions. Pelvic floor contraction is then assessed through palpation of coccygeal movement.
Diagnostic Tools
Pelvic floor muscle strength can be measured using intravaginal instruments, such as manometers and dynamometers. Manometry quantifies force in millimeters of mercury (mm Hg), whereas dynamometry measures force in newtons (N). Differential tests are also performed to assess SIJ pain, including the active straight leg raise test. This test is is considered key for identifying SIJ pain, differentiating lumbar spine and hip joint dysfunction, and detecting possible SIJ dislocation. Intravaginal cones are devices used to assess pelvic floor contraction and provide feedback on therapeutic response. Available in various shapes and sizes, these devices serve a dual purpose: assessment of muscle function and facilitation of patient education regarding voluntary pelvic floor muscle control.
Additional diagnostic instruments include intravaginal, transrectal, suprapubic, and perineal ultrasound, depending on clinical indication and physician judgment. Ultrasound imaging provides 2- or 3-dimensional visualization, enabling assessment of both muscular and visceral dynamics.
Electromyography (EMG) provides information on pelvic floor muscle activity during voluntary and involuntary contraction. Electrode placement may be superficial or intramuscular, depending on the anatomical region under evaluation. Surface electrodes are used for general assessment, whereas intramuscular placement is reserved for deeper or more localized evaluation. Interpretation of EMG signals depends on electrode positioning and patient posture during examination. EMG activity is lower in the supine position with flexed lower limbs compared with sitting or orthostatic positions.
MRI is the preferred diagnostic modality. MRI provides detailed visualization of muscular, visceral, and connective tissue structures within the pelvic region, with the capability for real-time assessment of pelvic floor position, contraction, and visceral behavior without patient discomfort (see Image. Prostate and Adjacent Structures on Magnetic Resonance Imaging). In healthy individuals, the relaxed pelvic floor descends approximately 3 cm below the pubococcygeal line. Imaging modality selection depends on clinical judgment and the physician's experience.
Computed tomography may provide a dynamic assessment of pelvic floor function during contraction and defecation but is generally considered secondary to MRI due to radiation exposure. Diagnostic strategy selection is ultimately guided by clinical indication and patient-specific considerations.
Other Issues
Recent studies demonstrate that adjacent muscle groups may directly influence pelvic floor function. Levator ani muscle insertions extend beyond the superior pubic ramus into the obturator fascia. External stimulation of the obturator muscles has been shown to induce contraction of the levator ani, particularly within the iliococcygeus region, also described as the tendinous arch.[23]
Gluteus maximus activity also influences pelvic floor muscle tension. A tendinous expansion originating from the gluteus maximus inserts into the levator ani region, contributing to pelvic floor activation.
Anatomical variation of the gluteus maximus includes the gluteoperinealis muscle. This variant extends from the gluteus maximus to the levator ani within the ischioanal fossa, contributing to increased pelvic floor tension.
Media
(Click Image to Enlarge)
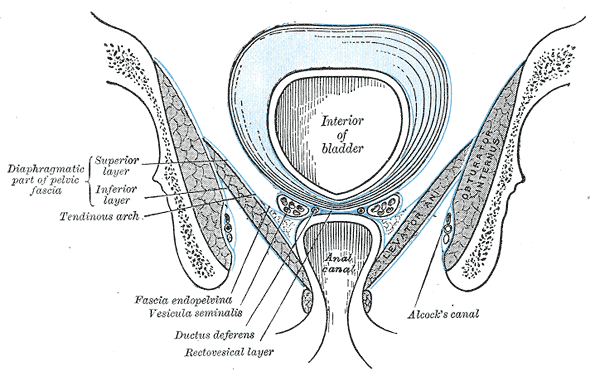
Anatomy of the Pelvic Floor. Coronal (frontal) section of the pelvis viewed posteriorly, illustrating the organization of pelvic fasciae and their relationships to adjacent musculature and pelvic viscera.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
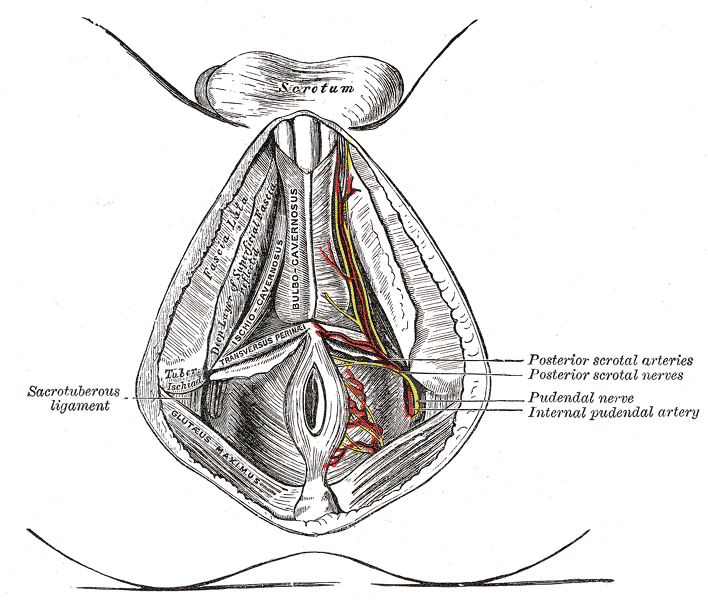
Neurovascular Structures of the Perineal Region. This anatomical illustration demonstrates the superficial and deep structures of the male perineal region. Labeled components include the sacrotuberous ligament, bulbocavernosus and ischiocavernosus muscles, pudendal nerve, and internal pudendal artery.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
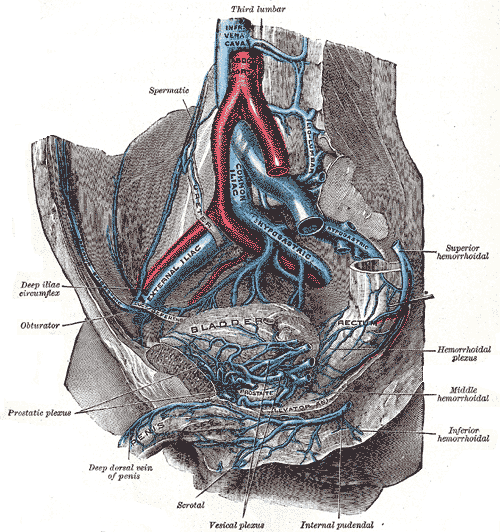
Pelvic Blood Vessels. In this medial view, the abdominal aorta bifurcates and the inferior vena cava forms at the level of the 4th lumbar vertebra, giving rise to the common iliac vessels. External iliac vessels continue toward the lower limbs, whereas internal iliac (hypogastric) vessels descend into the lesser pelvis. Venous drainage is provided by extensive pelvic plexuses, including the vesical, prostatic, and rectal plexuses, with superior, middle, and inferior rectal veins contributing to outflow. Additional vessels include the obturator, internal pudendal, and iliolumbar veins, as well as the deep dorsal vein of the penis and scrotal branches. Surrounding musculature and pelvic viscera are oriented relative to the pelvic floor and adjacent osseous landmarks.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
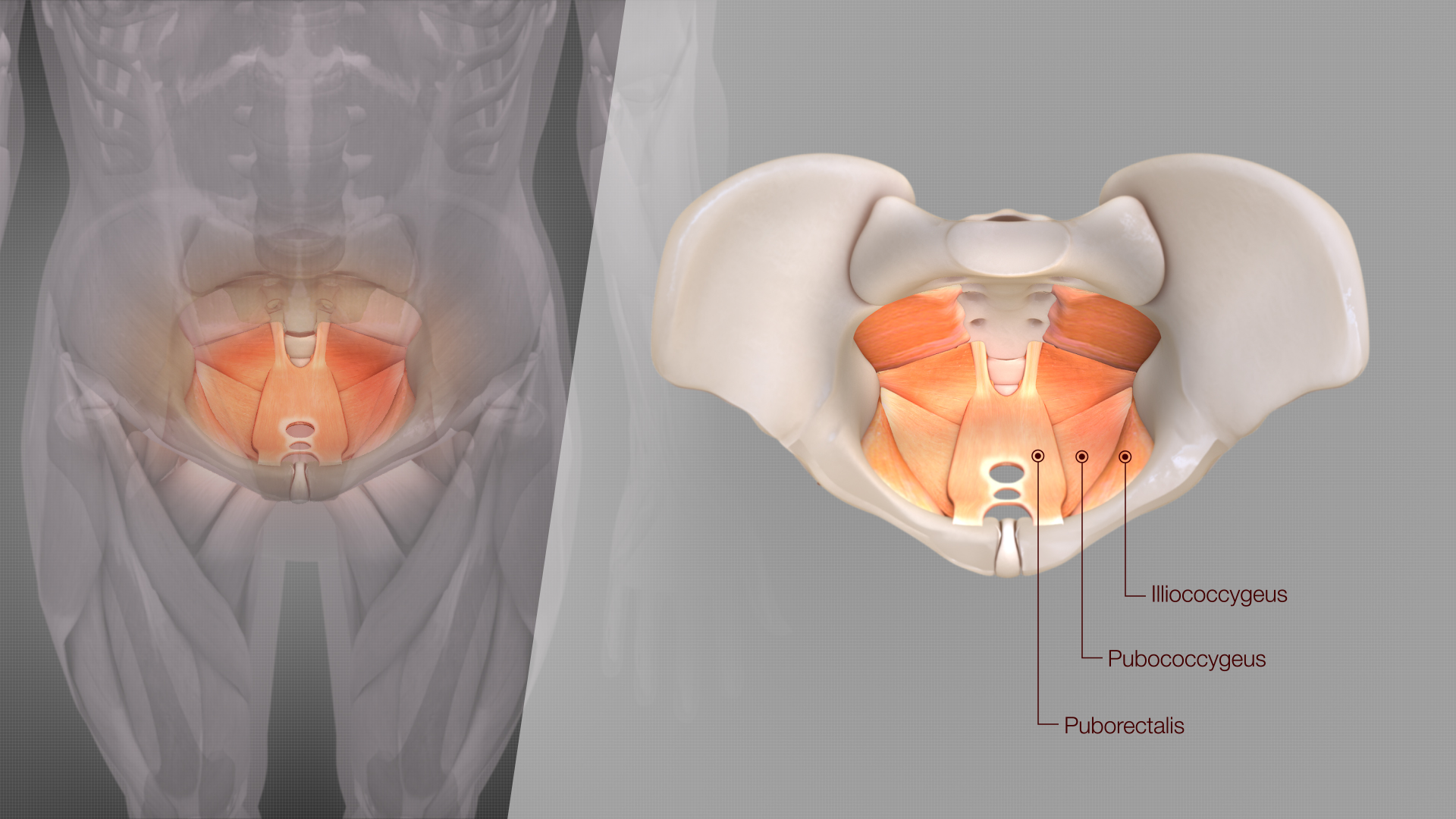
Levator Ani Components. This 3-dimensional, anterosuperior view displays the relationship between the puborectalis, pubococcygeus, and iliococcygeus muscles.
Scientific Animations, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)

Anatomic Reflections of the Endopelvic Fascia. The blue line represents the pelvic fascia, highlighting the endopelvic and perineal layers that invest pelvic organs and define surgical planes. Superiorly, the line traces the vesical layer over the bladder, then descends to form the rectovesical septum (Denonvilliers fascia) between the rectum and prostate, a key landmark separating urogenital and digestive structures. Posteriorly, the line marks the rectal layer. Inferiorly, the line represents the Colles fascia as it reflects toward the posterior margin of the urogenital diaphragm. The diagram demonstrates continuity of fascial planes, their role in structural support, compartmentalization, and guidance of fluid spread or surgical dissection within the pelvis.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
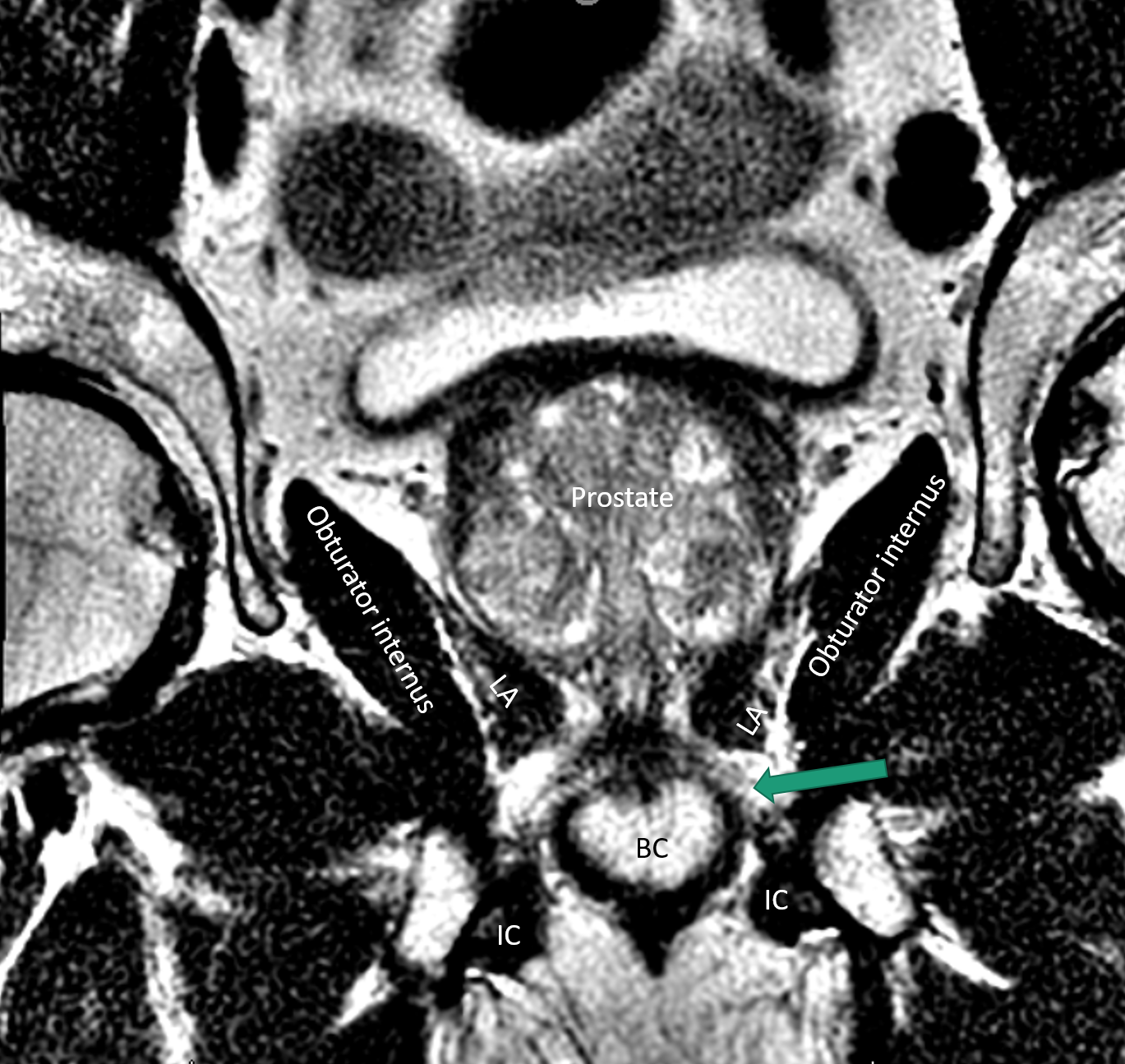
Prostate and Adjacent Structures on Magnetic Resonance Imaging. This coronal T2-weighted image shows the prostate, obturator internus, levator ani (LA), bulbocavernosus (BC), ischiocavernosus (IC), and urogenital diaphragm (arrow) in relation to adjacent pelvic structures.
Contributed by SK Selvarajan, MD
References
Sam P, LaGrange CA. Anatomy, Abdomen and Pelvis, Penis. StatPearls. 2026 Jan:(): [PubMed PMID: 29489230]
Simunovic M, Pinthus J, Coates AJ, DeNardi F. Anterior-entry abdominoperineal resection: a variation in the method of perineal dissection. Annals of surgical oncology. 2012 Mar:19(3):794-800. doi: 10.1245/s10434-011-2016-5. Epub 2011 Aug 23 [PubMed PMID: 21861220]
Kalra A, Wehrle CJ, Tuma F. Anatomy, Abdomen and Pelvis, Peritoneum. StatPearls. 2026 Jan:(): [PubMed PMID: 30521209]
Arbuckle JL, Parden AM, Hoover K, Griffin RL, Richter HE. Prevalence and Awareness of Pelvic Floor Disorders in Female Adolescents Seeking Gynecologic Care. Journal of pediatric and adolescent gynecology. 2019 Jun:32(3):288-292. doi: 10.1016/j.jpag.2018.11.010. Epub 2018 Dec 6 [PubMed PMID: 30529498]
Emerich Gordon K, Reed O. The Role of the Pelvic Floor in Respiration: A Multidisciplinary Literature Review. Journal of voice : official journal of the Voice Foundation. 2020 Mar:34(2):243-249. doi: 10.1016/j.jvoice.2018.09.024. Epub 2018 Nov 14 [PubMed PMID: 30447797]
Bordoni B. The pelvic floor is the function of the body unit. American journal of obstetrics and gynecology. 2024 Jun:230(6):e121. doi: 10.1016/j.ajog.2024.02.018. Epub 2024 Feb 16 [PubMed PMID: 38367757]
Bordoni B. We need to take a broader view of the function of the pelvic floor. European journal of obstetrics, gynecology, and reproductive biology. 2024 Dec:303():366. doi: 10.1016/j.ejogrb.2024.11.011. Epub 2024 Nov 9 [PubMed PMID: 39542802]
Pinto RA, Corrêa Neto IJF, Nahas SC, Bustamante Lopes LA, Sobrado Júnior CW, Cecconello I. FUNCTIONAL AND ANATOMICAL ANALYSIS OF THE ANORECTUM OF FEMALE SCLERODERMA PATIENTS AT A CENTER FOR PELVIC FLOOR DISORDERS. Arquivos de gastroenterologia. 2018 Nov:55Suppl 1(Suppl 1):47-51. doi: 10.1590/S0004-2803.201800000-49. Epub 2018 Oct 4 [PubMed PMID: 30304292]
Jalalizadeh M, Alshiek J, Santoro GA, Wieczorek AP, Shobeiri SA. Six-Year Experience in Teaching Pelvic Floor Ultrasonography Using Pelvic Floor Phantoms. Obstetrics and gynecology. 2018 Aug:132(2):337-344. doi: 10.1097/AOG.0000000000002729. Epub [PubMed PMID: 29995748]
Escalona-Vargas D, Oliphant S, Siegel ER, Eswaran H. Characterizing pelvic floor muscles activities using magnetomyography. Neurourology and urodynamics. 2019 Jan:38(1):151-157. doi: 10.1002/nau.23870. Epub 2018 Nov 2 [PubMed PMID: 30387530]
Radzimińska A, Weber-Rajek M, Strączyńska A, Podhorecka M, Kozakiewicz M, Kędziora-Kornatowska K, Goch A. The impact of pelvic floor muscle training on the myostatin concentration and severity of urinary incontinence in elderly women with stress urinary incontinence - a pilot study. Clinical interventions in aging. 2018:13():1893-1898. doi: 10.2147/CIA.S177730. Epub 2018 Oct 4 [PubMed PMID: 30323575]
Level 3 (low-level) evidenceLemos AQ, Brasil CA, Alvares CM, Passos JCG, Lordêlo P, Sá KN. The relation of the pelvis and the perineal function in incontinent women: A neglected subject. Neurourology and urodynamics. 2018 Nov:37(8):2799-2809. doi: 10.1002/nau.23772. Epub 2018 Jul 19 [PubMed PMID: 30024050]
Soljanik I, Janssen U, May F, Fritsch H, Stief CG, Weissenbacher ER, Friese K, Lienemann A. Functional interactions between the fossa ischioanalis, levator ani and gluteus maximus muscles of the female pelvic floor: a prospective study in nulliparous women. Archives of gynecology and obstetrics. 2012 Oct:286(4):931-8. doi: 10.1007/s00404-012-2377-4. Epub 2012 Jun 13 [PubMed PMID: 22692630]
Sen S, Senol GB, Ormeci T, Cetinkaya M, Sakul BU. Gluteoperinealis muscle: a surgically important variation. Surgical and radiologic anatomy : SRA. 2021 Sep:43(9):1467-1470. doi: 10.1007/s00276-021-02766-x. Epub 2021 May 16 [PubMed PMID: 33993323]
Stansfield E, Mitteroecker P, Umek W, Fischer B. The variation in shape and thickness of the pelvic floor musculature in males and females: a geometric-morphometric analysis. International urogynecology journal. 2023 Feb:34(2):453-461. doi: 10.1007/s00192-022-05311-5. Epub 2022 Aug 5 [PubMed PMID: 35930006]
Memon H, Handa VL. Pelvic floor disorders following vaginal or cesarean delivery. Current opinion in obstetrics & gynecology. 2012 Oct:24(5):349-54. doi: 10.1097/GCO.0b013e328357628b. Epub [PubMed PMID: 22907482]
Level 3 (low-level) evidencePacik D, Fedorko M. Literature review of factors affecting continence after radical prostatectomy. Saudi medical journal. 2017 Jan:38(1):9-17. doi: 10.15537/smj.2017.1.15293. Epub [PubMed PMID: 28042624]
Terzoni S, Maruccia S, Di Prisco L, Parozzi M, Caruso R, Ferrara P, Cilluffo S, Barbuiani G, Ricci C, Togni S, Rocco B, Gaia G, Sighinolfi MC, Mora C, Lusignani M. Preoperative Pelvic Muscle Training for Continence Recovery After Prostatectomy: Yet Another Meta-Analysis? Neurourology and urodynamics. 2026 Jan:45(1):127-136. doi: 10.1002/nau.70167. Epub 2025 Oct 17 [PubMed PMID: 41104623]
Level 1 (high-level) evidenceGallego-Gómez C, Núñez de Arenas-Arroyo S, Torres-Costoso A, Rodríguez-Gutiérrez E, Martínez-Vizcaíno V, Martínez-Bustelo S, Quezada-Bascuñán CA, Basco-López JÁ, Ferri-Morales A. Effects of Training Interventions to Treat Postpartum Urinary Incontinence: A Meta-Analysis. BJOG : an international journal of obstetrics and gynaecology. 2026 Jan:133(2):243-252. doi: 10.1111/1471-0528.70014. Epub 2025 Sep 24 [PubMed PMID: 40993838]
Level 1 (high-level) evidenceFu J, Li Z, Pu J, Liu Y, Mao Q, Li C, Li L, Gai X. Advancing women's health: innovative applications of sacral neuromodulation in pelvic floor dysfunctions. Archives of gynecology and obstetrics. 2025 Nov:312(5):1489-1501. doi: 10.1007/s00404-025-08182-5. Epub 2025 Sep 16 [PubMed PMID: 40956334]
Dequirez PL, De Wachter S, Biardeau X. Sacral neuromodulation for low urinary tract dysfunction: overview and mechanisms of action. Autonomic neuroscience : basic & clinical. 2025 Oct:261():103337. doi: 10.1016/j.autneu.2025.103337. Epub 2025 Aug 19 [PubMed PMID: 40858056]
Level 3 (low-level) evidenceAfyouni AS, Khanmammadova N, Bozorgi A, Das AK, Gelman J, Sadeghi Z. Urologic Manifestations of Nonrelaxing Pelvic Floor Dysfunction: Insights on Clinical Workup and Management. Current urology reports. 2025 Oct 16:26(1):66. doi: 10.1007/s11934-025-01290-4. Epub 2025 Oct 16 [PubMed PMID: 41094314]
Chin HY, Peng CW, Wu MP, Chen CH, Feng YT, Fong TH. Attachment of the levator ani muscle extends to the superior ramus of the pubic bone through electrophysiological and anatomical examinations. Scientific reports. 2021 May 4:11(1):9483. doi: 10.1038/s41598-021-89041-6. Epub 2021 May 4 [PubMed PMID: 33947899]