Introduction
Brain herniation is the pathologic displacement of brain tissue driven by pressure gradients between compartments (Image. Brain Herniation). The brain is encased within the skull; any rise in intracranial pressure is limited to some extent by the compensatory displacement of cerebrospinal fluid (CSF) and changes in cerebral blood volume, as evident by the Monro-Kellie doctrine.[1] When intracranial pressure increases despite these compensatory mechanisms, certain parts of the brain herniate across rigid dural folds (falx or tentorium) or through skull openings (eg, the foramen magnum), producing characteristic herniation syndromes.[2] Brain herniation is a life-threatening event and needs urgent attention. Common clinically described types of brain herniation include:
- Subfalcine herniation: This type of herniation involves the cingulate gyrus, which is pushed against the falx cerebri (Image. Subfalcine Hernation).
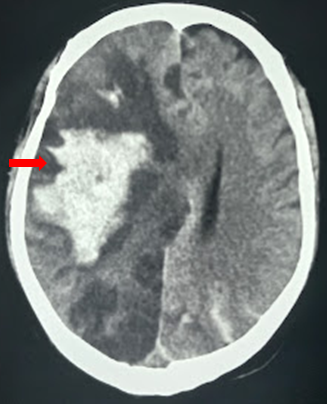
- Uncal herniation: This herniation involves the medial temporal lobe, which is often squeezed by a mass under and across the tentorium (Image. Subdural Hematoma and Uncal Herniation)
- Central descending transtentorial herniation: This herniation involves the downward displacement of the diencephalon and midbrain through the tentorial notch, typically due to diffuse cerebral edema or bilateral mass effect.
- Tonsillar herniation: This type of herniation forces the cerebellar tonsils through the foramen magnum.
- Upward (ascending) transtentorial herniation: This occurs when a posterior fossa mass effect drives cerebellar structures upward through the tentorial notch, distorting the midbrain and potentially obstructing CSF pathways and venous drainage.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Multiple factors can predispose to raised intracranial pressure and brain herniation syndrome, including:
- Hematoma (traumatic epidural and subdural hematoma, contusions, intracerebral hemorrhage)
- Missile and non-missile penetrating injuries
- Diffuse subarachnoid hemorrhage
- Pneumocephalus (traumatic or postoperative)
- Malignant infarction
- Tumors
- Infections (abscess, empyema, hydatid cyst)
- Hydrocephalus
- CSF overdrainage
- Fulminant hepatic failure with cerebral edema
- Open spinal dysraphism (intracranial hypotension after spinal CSF leak) [3][4][5][6]
Epidemiology
Traumatic brain injury (TBI) is the predominant cause of death after traumatic injury. Raised intracranial pressure (ICP) especially correlates with poor TBI outcomes.[7]
Pathophysiology
The pathogenesis of brain herniation is based on the Monro-Kellie doctrine, which governs intracranial dynamics and pressure.[8][9][10]
Evolution of Monro-Kellie Doctrine
Alexander Monro Secundus and his student, George Kellie, proposed that the volume of blood circulating in the cranium remains constant. Consequently, expulsion of an equivalent volume of blood from the skull must occur whenever any additional fluid enters the intracranial space. John Abercrombie further advanced this concept by asserting that cranial depression compresses brain parenchyma and diminishes cerebral blood flow, helping disseminate the doctrine within the medical community. At that time, knowledge of CSF and its function was lacking, preventing the completion of the theory. François Magendie later identified CSF as a third intracranial component.
George Burrows challenged the assumption of a perfectly spherical skull and fixed intracranial blood volume, reformulating the doctrine to state that brain tissue, blood, and CSF occupy interdependent volumes within the cranium. When compensatory thresholds fail, and displacement of these components cannot offset added volume, pathological processes ensue. Burrows also introduced intracranial pressure into the analysis of cranial dynamics. Subsequently, Henri Duret, Ernst von Bergmann, and Theodor Kocher demonstrated that CSF displacement into the spinal canal and vascular compression maintain intracranial pressure, while failed compensation produces ischemia and brain shift syndromes. Harvey Cushing later validated and clinically demonstrated the doctrine’s physiological principles.[8]
ICP Waveforms
Burrows first noticed pulsations within the meninges during the arterial systolic phase and during respiratory movements. Angelo Mosso first described the tricuspid variability of the cerebral blood pulse. The ICP pulse waveform is classically characterized by 3 components: P1 (percussion wave), P2 (tidal wave), and P3 (dicrotic wave), with a rising P2 suggesting reduced compliance.[8]
When the CSF and venous spaces become exhausted, the brain is compressed, generating a steeply rising ICP and increased brain swelling. This concept explains the exponential pressure-volume relationship of the intracranial system (elastance curve).[11] Acute intraoperative brain swelling/herniation reflects loss of compliance and pathological pressure gradients; cerebral perfusion pressure (CPP) may deteriorate as a consequence.[12] The Pressure Reactivity Index (PRx) is pivotal in governing cerebral autoregulation and compensatory reserve.[13] Cerebrovascular autoregulation, the glymphatic system, and cerebral compensatory reserve are major determinants governing ICP dynamics. Therefore, newer insights into the role of cisternal drainage, assessment of changes in ICP pulse morphology, and multimodality neuro-monitoring to determine brain compliance have been adopted in the management of intracranial compartment syndrome.”[9]
Patterns of Brain Herniation
Plum and Posner described the cephalocaudal sequential progression of the brain during herniation.[14] Brain herniation is classified as follows:
- Subfalcine herniation
- Transalar (transsphenoidal) herniation
- Uncal herniation
- Central (trans-tentorial) herniation (descending and ascending)
- Cerebellar tonsillar herniation
- Transcalvarial herniation
Subfalcine herniation
In subfalcine herniation, the ipsilateral cingulate gyrus gets migrated beneath the anterior falx, potentially causing anterior cerebral artery compression and infarction in its distal territory.[15]
Transalar (transsphenoidal) herniation
In the posterior (descending) variant of transalar herniation, infarction may occur within the middle cerebral artery territory, resulting from its compression within the sphenoid ridge. In anterior (ascending) transalar herniation, compression of the supraclinoid segment of the internal carotid artery against the anterior clinoid process leads to infarction within the territory of the anterior and middle cerebral arteries.
Uncal herniation
Transtentorial uncal herniation compresses the oculomotor nerve (CN III) against the tentorial edge, classically producing an ipsilateral dilated, poorly reactive pupil; a transient early constriction (Hutchinson pupil) may rarely precede dilation.[16][17]
Infarction may occur within the temporal or occipital lobe owing to compression of the calcarine branch of the posterior cerebral artery as well. Brainstem and tectal distortion may contribute to aqueductal obstruction and hydrocephalus in severe cases. Significant midline shift and transtentorial brain displacement may distort or compress the third ventricle and cerebral aqueduct, contributing to obstructive hydrocephalus in severe cases. As the midbrain is further displaced, sometimes the contralateral cerebral peduncle is forced against the tentorium edge, creating the Kernohan notch and damaging the contralateral corticospinal tract, thereby resulting in paresis or paralysis ipsilateral to the mass lesion.
Transtentorial central herniation (descending and ascending)
As the pathological descent of the brainstem through the incisura progresses, venous congestion, along with stretching and tearing of small perforators, creates Duret hemorrhages.[18] Clinically, progression from abnormal flexor posturing to abnormal extensor response occurs through the involvement of the rubrospinal and the vestibulospinal tracts. Progression leads to worsening brainstem dysfunction with respiratory and cardiovascular collapse; in extreme, terminal cases, continued downward shift may be accompanied by tonsillar herniation with medullary compression and death. Patients may exhibit characteristic triple components of Cushing triad, consisting of hypertension, bradycardia, and irregular respirations.
Ascending transtentorial herniation can compress the posterior cerebral or superior cerebellar arteries against the tentorium and can follow posterior fossa mass lesions, endoscopic third ventriculostomy, or excessive supratentorial CSF drainage, eg, following an external ventricular drainage.[19][20][21]
Cerebellar tonsillar herniation
Increased pressure in the posterior fossa forces the cerebellar tonsils through the foramen magnum. These forces will compress the lower part of the brain stem and upper cervical cord, resulting in life-threatening consequences. Compression usually occurs along with ascending or descending transtentorial herniation. Acute herniation can compress the posterior inferior cerebellar arteries, vertebral arteries, and their branches, or the origin of the anterior spinal artery, leading to ischemia of the brainstem, tonsils, and lower cerebellum. Severely elevated ICP (often >40–50 mm Hg), particularly when approaching or exceeding mean arterial pressure, can cause critically reduced CPP, global cerebral ischemia, and progression to brain death.[11]
Transcalvarial herniation
In cases of calvarial defects, eg, after decompressive hemicraniectomy, edematous brain tissue may herniate outward through the defect along the path of least resistance due to pressure gradients. This external herniation can compress cortical vessels against the bony margins, predisposing to venous congestion and hemorrhagic infarction.
Other patterns of brain herniation:
History and Physical
Rigorous neurological evaluation remains essential when assessing patients at risk for brain herniation, as deterioration may develop unexpectedly.[26] Early recognition of pupillary asymmetry and prompt correction of the underlying cause help to minimize secondary injury and improve outcomes.[27] As herniation syndromes evolve, characteristic neurological signs and symptoms emerge that reflect the pattern and progression of tissue displacement.
Subfalcine herniation produces lower limb weakness resulting from infarction of the corresponding motor homunculus after compression of the pericallosal and callosomarginal vessels. Uncal herniation classically presents with ipsilateral anisocoria and contralateral motor weakness, although the Kernohan–Woltman notch phenomenon may produce ipsilateral weakness. Abnormal posturing signals rostrocaudal deterioration: lesions at the diencephalon or above the red nucleus typically produce abnormal flexor (decorticate) posturing, whereas progression to involvement at or below the red nucleus in the midbrain or upper pons produces extensor (decerebrate) posturing.
Progressive intracranial hypertension with midline shift and downward diencephalic displacement alters sensorium through distortion of ascending arousal pathways and may obstruct the foramen of Monro or cerebral aqueduct, leading to hydrocephalus. The onset of downward transtentorial herniation is characterized by decorticate and decerebrate posturing, along with loss of brainstem reflexes. Respiratory patterns may become progressively abnormal. For example, Cheyne–Stokes, central neurogenic hyperventilation, ataxic breathing, potentially progressing to apnea with advanced brainstem failure. Upward transtentorial herniation may produce dorsal midbrain (Parinaud) features, while hypothalamic–pituitary dysfunction remains uncommon but possible in severe cases.
Evaluation
Vigilant neurological monitoring with the Glasgow Coma Scale (GCS) and pupillary assessment is the key to the evaluation of patients with brain herniation. When available, multimodality monitoring complements clinical examination and imaging by providing continuous, physiology-based markers of cerebral oxygenation, perfusion, autoregulation, and metabolism, helping clinicians detect evolving secondary injury early and individualize targets beyond ICP and CPP alone (see Table 1).
Table 1. Multimodality Monitoring
| PbtO2 (mm Hg) | Focal brain tissue oxygenation near the probe | Detects focal hypoxia even when ICP/CPP look acceptable; guides targeted fixes (oxygenation, anemia, CPP/ICP, ventilation, fever, seizures) | ≥15–20 | <15 | <10 if sustained |
| SjvO2 (%) | Global cerebral oxygen balance (delivery vs demand) | Distinguishes inadequate delivery (low) from low extraction/shunting or suppressed metabolism (high); helps tune CPP/oxygenation and metabolic control | 55–75 | <55 or >75 | <50 sustained |
| Continuous Electroencephalogram | Seizures and epileptiform activity when the exam is unreliable | Identifies treatable secondary injury (nonconvulsive seizures) and guides antiseizure therapy/sedation strategy | No seizures | Nonconvulsive seizures/increasing seizure burden | Status epilepticus or frequent recurrent seizures |
| Microdialysis: Laryngopharyngeal Reflux | Local metabolic crisis marker (energy failure/ischemia patterns) | Flags metabolic crisis despite acceptable ICP; prompts reassessment of CPP/oxygenation, seizure/fever control, anemia, and systemic drivers | <25 | 25–40 | >40 (esp. with low brain glucose) |
| Microdialysis: Brain Glucose (mmol/L) | Local substrate availability | Detects low substrate supply and risk of metabolic failure; supports adjustments to systemic glucose delivery and CPP/oxygenation strategy | >1.0 | 0.8–1.0 | <0.8 sustained |
| PRx | Pressure reactivity (autoregulation surrogate) | Helps judge whether raising CPP is likely to help or harm; supports individualizing CPP targets rather than fixed numbers | ≤0 to mildly positive | >0.2 | >0.3 sustained |
| Optimal Cerebral Perfusion Pressure (CPPopt) | Patient-specific CPP range with best autoregulation | Guidesthe individualized CPP goal to avoid under-perfusion and avoid harm from over-pressingthe CPP | Not a fixed number | CPP drifting away from CPPopt | Persistent CPP far from CPPopt with worsening physiology |
An automatic pupillometer can aid early detection of pupillary changes suggesting an ICP crisis or impending herniation, facilitating timely escalation and intervention.[28]
Radiological imaging also reveals the following characteristic markers associated with each herniation subtype:
- An effacement of the ipsilateral lateral horn with a displacement of the septum pellucidum in subfalcine herniation occurs, which is followed by progressive compression and obliteration of the basal cisterns along with hydrocephalus resulting from brain torsion (see Images. Hemispheric Infarction Radiologic Findings and Hemorrhagic Transformation Radiologic Finding).
- As a supratentorial mass expands, the ipsilateral temporal lobe uncus is displaced medially and downward through the tentorial notch. This causes the midbrain to shift away from the mass, compressing the contralateral cerebellopontine cistern between the midbrain and the petrous bone, resulting in its obliteration. Simultaneously, the ipsilateral cerebellopontine cistern is stretched and widened as the midbrain shifts toward the contralateral side, increasing the space on the side of the lesion. Thus, the uncal herniation causes widening of the ipsilateral cerebellopontine cisterns with the obliteration of the contralateral cerebellopontine cisterns.
- Central (descending) herniation is suggested by effacement of the perimesencephalic cisterns with downward displacement of the diencephalon/midbrain; duret hemorrhages may be present.
- The upward herniation variant leads to flattened quadrigeminal cisterns, "spinning top" appearance of the midbrain, and associated hydrocephalus.[29][30]
The imaging will also reveal characteristic infarction along with the vascular territory of compressed vessels. In severe diffuse cerebral edema with hypoxic–ischemic injury, a "white cerebellar sign" may be observed.
Cerebral autoregulation may become disrupted, rendering cerebral blood flow increasingly pressure-passive. As intracranial compliance diminishes and compensatory reserve is exhausted, ICP monitoring may reveal characteristic pathological wave patterns. Lundberg A (plateau) waves are abrupt, sustained ICP elevations (often 40–60 mm Hg) lasting 5 to 30 minutes, reflecting severely reduced intracranial compliance and an autoregulatory vasodilatory cascade. Lundberg B waves are lower-amplitude rhythmic oscillations occurring every 0.5 to 2 minutes, commonly seen in hydrocephalus and moderate compliance impairment, and may precede ICP decompensation. The ICP pulse waveform itself has 3 peaks: P1 (percussion), P2 (tidal), and P3 (dicrotic). With worsening compliance, P2 rises relative to P1, and the waveform becomes progressively rounded as individual peaks become indistinct.
Some institutions use the term "brain code" to denote suspected impending herniation or refractory intracranial hypertension requiring immediate escalation of care.[3] The following 10 time-critical red flags of ICP crisis or suspected herniation should trigger immediate escalation:
- New dilated and nonreactive pupil
- New asymmetric pupils or rapidly worsening anisocoria
- Progressive decline in neurological status, especially a drop in GCS by more than 2 points, not explained by nonneurological causes
- Motor exam showing extensor (decerebrate) posturing
- New abnormal posturing (decorticate or decerebrate), especially if worsening
- Cushing reflex (hypertension with bradycardia, often with irregular respirations)
- New irregular respirations, ataxic breathing, or apnea suggestive of brainstem involvement
- Sustained intracranial hypertension on monitoring despite initial measures (for example, ICP above commonly treated thresholds, eg, >22 mm Hg in adults)
- Sudden neurological deterioration during transport, repositioning, suctioning, or intubation
- Seizure with failure to return to baseline consciousness or suspicion of ongoing nonconvulsive seizure with worsening exam
Treatment / Management
Prehospital care during transport and effective emergency management of patients with traumatic brain injury are critical in preventing secondary damage (hypoxia, hypotension, seizure) to the brain resulting from the primary insult.[31][32](B2)
General Measures
The following general protocol is recommended for patients presenting with traumatic brain injury:
- Call for help and treat this as an ICP crisis. Escalate to a senior clinician, neurosurgery, and prepare for urgent imaging and definitive intervention.
- Position the patient to optimize for venous outflow. Elevate the head of the bed to greater than 30 degrees and keep the head midline; avoid neck obstruction (tight collars, tube ties, extreme rotation).
- Minimize noxious stimuli. Control pain, agitation, coughing, and ventilator dyssynchrony with adequate analgesia and sedation.
- Oxygenation: prevent hypoxemia (target SpO2 ≥94% and restore oxygenation immediately after airway interventions).
- Provide airway protection and mechanical ventilation as needed for patients with severe TBI. Consider neuromuscular blockade in selected cases of refractory agitation or ventilator dyssynchrony contributing to intracranial hypertension. Use sedatives to calm the patient.
- Hyperventilation may be used briefly as a temporizing measure for impending herniation (target PaCO2 about 30–35 mm Hg) while definitive treatment is arranged; prophylactic hyperventilation should be avoided, particularly in the first 24 hours after injury.
- Maintain euvolemia and avoid hypotension; avoid hypotonic fluids.
- Administer osmotherapy, eg, mannitol, to lower ICP.
- Control blood pressure while ensuring adequate perfusion of the brain.
- Consider corticosteroids to reduce vasogenic edema in patients with malignancies and abscesses.
- Target normothermia and avoid or correct hyponatremia (both worsen cerebral edema and ICP dynamics).
- If a CSF drain is present, ensure it is functioning and use CSF diversion (EVD drainage) as part of first-line ICP control. Continue urgent assessment to identify underlying etiologies requiring surgery or other definitive treatment.
Physiologic Targets
In patients with severe TBI, intracranial hypertension, or risk of herniation, the following clearly defined physiologic targets guide management:
- Oxygenation:
- SpO2 ≥94% (initial target)
- Avoid hypoxia (SpO2 <90% or PaO2 <60 mm Hg is associated with worse outcomes)
- Ventilation
- Normocapnia: PaCO2 approximately 35–40 mm Hg (or ETCO2 ~35–40 mm Hg)
- If impending herniation: brief temporizing hyperventilation to PaCO2 approximately 30–35 mm Hg while definitive therapy is arranged
- Blood pressure/perfusion
- Avoid hypotension; support systemic pressure to maintain cerebral perfusion.
- CPP target 60–70 mm Hg (individualize to autoregulation status; avoid aggressive CPP >70 with fluids/pressors)
- ICP
- Treat sustained ICP elevation >22 mm Hg (commonly used initial treatment threshold)
- When weighing higher-risk escalation, consider a practical treatment range of 20–25 mm Hg.
- Temperature
- Target normothermia; treat hyperthermia
- Sodium/osmolality
- Avoid and correct hyponatremia (Na <135 mEq/L)
- During hyperosmolar therapy: monitor sodium/osmolality closely; do not treat “to exceed” a serum osmolality threshold (use limits per local protocol rather than targets)
Brain Trauma Foundation guidelines recommend monitoring ICP in patients with severe TBI (ie, GCS of 3 to 8) and have either (1) abnormalities in CT of the head or (2) meet at least 2 of the following 3 criteria: age over 40 years; systolic blood pressure under 90 mm Hg, or abnormal posturing. The genesis of this approach is that ICP elevation may precede clinical deterioration, supporting early monitoring in selected severe TBI patients.[7] However, studies on ICP-guided rescue therapy have produced mixed results. Level I evidence for any strategies targeted for managing refractory intracranial hypertension remains lacking. Trials of ICP-guided management and decompressive craniectomy show mixed effects on functional outcomes; decompressive craniectomy reduces ICP and can improve survival in selected refractory cases, with important disability trade-offs (DECRA, RESCUEicp). Thresholds for ICP and CPP guided therapies are 22 mm Hg and 60 to 70 mm Hg, respectively.
Proposed tiers in the management of refractory intracranial hypertension and resultant brain herniation (see Table 2) include:
- Evacuation of mass lesions (hematoma, contusion, infarction, edema, tumors)
- Physiological neuroprotection
- Sedation (intravenous with early reversibility, midazolam, fentanyl), analgesics, and ventilation
- CSF drainage through external ventricular drain (EVD). External lumbar drainage (ELD) may be considered only in carefully selected patients (with appropriate imaging and without obstructive hydrocephalus or significant mass effect) and with close monitoring.
- Osmotherapy-Urea was used in the 1950s, mannitol (20%) in the 1960s, and hypertonic saline (3%/7.5%/10%/23.4%) in the 1990s. Mannitol and sodium (hypertonic saline) both have high reflection coefficients (σ ≈ 0.9), meaning they are largely excluded from crossing the blood-brain barrier and thus efficiently draw water from the brain parenchyma into the intravascular space, provided the blood-brain barrier is intact.[11]
- Hyperventilation (drives off CO2, thereby causing cerebral vasconstriction)
- Hypothermia (reduces cerebral metabolism)
- Barbiturate coma (burst suppression)
- Decompressive hemicraniectomy [3][33]
Table 2. Refractory Intracranial Hypertension Management Tiers
| STEP UP (SECOND TIER) | ADVANCE AS NEEDED (THIRD TIER) |
| Hypothermia- target of 35 °C | 33 °C |
| Hyperventillation- target pCO2 of 30-35 mm Hg | pCO2 <30 mm Hg |
| Serum osmolality ≤320 mOsm/kg (monitor) | ≤320 mOsm/kg (safety limit) + tighter monitoring |
| Sedation-Richmond Agitation-Sedation Scale (RASS) of -4 to -5 | Paralysis or Barbiturate coma |
| Target CPP: 50-70 mm Hg | Multimodality monitoring guided CPP optimization |
| CSF drainage and rescue craniotomy | Hemicraniectomy |
The Brain Trauma Foundation Level IIA recommendations (2020)
The following recommendations are supported by the Brain Trauma Foundation:
- Secondary decompressive craniectomy in the setting of late, refractory ICP elevations is recommended to improve mortality and favorable outcomes (based on results of RESCUEicp).
- Secondary decompressive craniectomy for early refractory ICP elevation is not recommended to improve mortality and favorable outcomes (based on results of DECRA).
- Secondary decompressive craniectomy, whether early or late, likely reduces ICP and ICU length of stay; however, its impact on functional outcomes remains unclear.
- Craniotomy is a good option versus decompressive craniectomy for ASDH in patients without brain swelling (RESCUE-ASDH trial)
- A large frontotemporoparietal decompressive craniectomy (12–15 cm in diameter) is recommended.[34]
Differential Diagnosis
Certain clinical entities can mimic brain herniation syndrome owing to rapid clinical and neurological deterioration in patients, including:
- Posttraumatic subclinical seizures
- Postictal state and nonconvulsive status epilepticus
- Medication or sedation effects (eg, opioids, benzodiazepines, and propofol) causing pupillary and consciousness changes
- Metabolic causes that mimic brainstem dysfunction (hypoglycemia, hypercapnia, severe hyponatremia)
- Paroxysmal sympathetic hyperactivity (formerly termed paroxysmal autonomic instability with dystonia)
- Acute hydrocephalus
- Tension pneumocephalus
- Dyselectroytemia
- Meningitis
- CSF over-drainage syndrome
- Ocular causes of anisocoria (topical anticholinergics, Adie pupil, prior eye surgery)
- Osteopetrosis
- Costello and posterior fossa crowding syndrome
Pertinent Studies and Ongoing Trials
Randomized trials demonstrate that decompressive craniectomy lowers mortality in refractory traumatic intracranial hypertension; however, this survival benefit often shifts outcome distribution toward survival with severe disability in a subset of patients. Outcomes vary according to timing and indication, with differences observed between early “neuroprotective” decompressive craniectomy and last-tier rescue decompressive craniectomy.[35]
Associations among ICP magnitude, cumulative burden, and outcome indicate that lower ICP generally correlates with improved prognosis, yet no single narrow optimal ICP range applies to all patients. Sustained ICP >22 mm Hg commonly prompts treatment, with targets individualized according to overall physiology and, when available, autoregulation status.[36][37] Evidence remains mixed. A randomized controlled trial comparing an ICP monitor–driven protocol with examination and CT-guided management failed to demonstrate superiority of the ICP-monitor strategy in that context, whereas observational studies and guideline syntheses suggest potential short-term mortality reduction in selected severe TBI populations.[7] Although ICP monitoring is a central tenet of many management algorithms, reliance on numeric thresholds may trigger interventions that inadvertently cause harm.
Recent research on intracranial hypertension management explores enhancing glymphatic “cooling and clearing” pathways through modulation of sleep patterns and targeting aquaporin channels, alongside strategies to attenuate catecholamine hyperactivity (glutamate storm).[9][38][39]
Prognosis
Prognosis in brain herniation and severe TBI depends on multiple variables, including duration of herniation, patient age, presenting GCS, presence of anisocoria, associated polytrauma, concurrent hypoxia and hypotension, lesion type such as extradural versus subdural hemorrhage, Marshall and Rotterdam CT scores, and ICP measurements. The advancing progression of a herniation syndrome correlates with an increasingly poor likelihood of recovery.[40][41][42]
The following factors affect prognosis:
- Increasing age is associated with an unfavorable outcome (centered at 40 years).[43][44]
- GCS score at admission is highly predictive of clinical outcomes.[45][46]
- Pupillary asymmetry is associated with an unfavorable prognosis.[47]
- Marshall and Rotterdam scores have high accuracy in predicting mortality in patients with acute and severe traumatic brain injury.[48][49]
- Hypoxia is an independent risk variable for poor prognosis in head injury.[50][51] Patients with prehospital saturation ≥94% had better outcomes among hypotensive patients with TBI.[52][53]
- Concurrent hypotension in TBI confers nearly 2-fold increased odds of mortality.[54]
- TBI is the most prevalent cause of death in polytrauma patients.[55] Mortality rates are higher in patients with TBI associated with polytrauma (35%) compared to those with isolated traumatic brain injury (24%).[56]
- Both hypertonic saline and mannitol reduce ICP; comparative superiority is inconsistent across studies, with several analyses suggesting hypertonic saline may provide more sustained ICP reduction.[57][58]
- EVD can control intracranial pressure and avoid third-tier therapeutic measures (therapeutic hypothermia, decompressive craniectomy, and barbiturate coma) or avoid a decision to withdraw life-sustaining treatment in almost 40% of cases.[59] ELD can be effective in carefully selected patients with close clinical and radiological vigilance to avoid precipitating herniation ("coning").[60] Meta-analysis has proven the benefits of lumbar drainage in ICP reduction, with complication rates similar to those of EVD therapy. However, clinical and radiological vigilance is needed to recognize coning early.[61]
- Early surgical evacuation of a hematoma within 6 hours of brain herniation can significantly reduce mortality and improve survival, especially in cases of cerebellar hemorrhage and traumatic subdural hematoma, but its effect on neurological recovery and long-term prognosis is less certain and depends on patient selection, hematoma characteristics, and surgical technique.[62]
- ICP-guided therapy has also been shown to reduce mortality and hospital length of stay.[63] Care focused on maintaining monitored intracranial pressure at 20 mm Hg or less has not been observed to be superior to a care bundle approach based on imaging and clinical examination.[64]
Complications
Brain herniation can progress from a subtle finding of pupillary asymmetry (uncal herniation) to an altered level of consciousness (compression of the reticular activating system), then progress to the moribund stage of abnormal posturing (dysfunction of the diencephalon and the brainstem), and finally death resulting from respiratory arrest (brainstem failure).
An associated infarction is seen along with the vascular territory of the compressed vessels associated with each herniation subtype. In advanced global hypoxic–ischemic injury with diffuse cerebral edema, noncontrast CT may show a "white cerebellum" (reversal) sign.[65]
Complications of Brain Herniation
Complications of brain herniation include:
- Cerebral infarction
- Seizure
- Coagulopathy
- Dyselectrolytemia
- Neurogenic pulmonary edema
- Dysautonomia
- Panhypopituitarism
- ICU-related complications (eg, critical illness neuropathy, pneumonia, sepsis, deep vein thrombosis, pressure ulcers)
- Chronic dependency
- Superficial siderosis
- Taupathies
- Persistent vegetative state
- Brainstem death
- Brain death [30][66][67][68]
Complications Relating to Management Strategies (Tiers)
Treatment-related complications include:
- EVD is associated with ventriculitis, track hematomas, mechanical failure, upward transtentorial herniation (rarely) in the setting of posterior fossa lesions/compartmental pressure gradients, inadvertent pull, misplacements, and critical cerebrospinal fluid hypovolemia.[69]
- Lumbar CSF drain is associated with similar complications to EVD, including inadvert brain coning.
- Postoperative hematoma is associated with recurrence and delayed traumatic intracranial hematoma.[26]
- Complications of craniectomy include reperfusion syndrome (hemorrhagic transformation), ventriculomegaly with or without hydrocephalus, and shrunken flap (trephination) syndrome.[70][71]
- Mannitol can cause acute renal failure. Hypertonic saline can cause hypernatremia, hyperchloremia/metabolic acidosis, and volume overload; rapid osmolar shifts may precipitate neurological complications, and cause skin sloughing if it extravasates into the subcutaneous tissues (higher concentrations and/or prolonged infusions may warrant central access per institutional protocol), and can cause rebound intracranial hypertension.[11] Mannitol, particularly with repeated dosing and brain-blood barrier disruption, has been associated with a reverse osmotic shift and rebound cerebral edema; both agents require careful laboratory and hemodynamic monitoring. Mannitol and hypertonic saline can cause a rebound increase in ICP owing to propagation of “idiogenic osmoles” (polyols, amino acids, and methylamines) via astrocytes.[11]
- Hyperventilation can lead to cerebral ischemia from reduced cerebral blood flow; abrupt normalization of PaCO2 may be followed by a rebound increase in ICP.
- Hypothermia is associated with arrhythmias, immunosuppression, and coagulation disorders.[72]
- Barbiturate coma is associated with hypotension, immunosuppression, and critical illness-related polyneuromyopathy.[73][74]
Deterrence and Patient Education
Deterrence of brain herniation centers on prevention of primary neurologic injury and early mitigation of secondary insults that precipitate intracranial hypertension. Public health strategies that reduce traumatic brain injury, including seatbelt use, helmet adherence, fall-prevention programs for older adults, avoidance of drunk driving, and violence prevention, remain foundational.[75] In hospitalized patients, meticulous avoidance of hypoxia, hypotension, hypercapnia, hyponatremia, and fever reduces the risk of intracranial pressure escalation. Early recognition of worsening headache, repeated vomiting, altered consciousness, new focal deficits, or pupillary asymmetry should prompt urgent medical evaluation, particularly in individuals with recent head trauma, intracranial hemorrhage, tumor, infection, or hydrocephalus.
Patient and family education should emphasize the time-sensitive nature of neurologic deterioration and the importance of adherence to follow-up, imaging, and prescribed therapies. Caregivers of high-risk patients should receive clear instructions on monitoring mental status changes and respiratory abnormalities and understand when to activate emergency services. Education regarding medication adherence, avoidance of unsupervised CSF drain manipulation, and recognition of complications, eg, seizure or shunt malfunction, further supports early intervention and improved outcomes.
Pearls and Other Issues
The central dogma in managing raised ICP is preventing secondary insults.[76]
Enhancing Healthcare Team Outcomes
Brain herniation represents life-threatening displacement of brain tissue driven by escalating intracranial pressure and failed compensatory mechanisms. Rapid progression from subtle pupillary asymmetry to coma and brainstem failure may occur without timely intervention. Effective management prioritizes early control of the primary insult and prevention of secondary injuries such as hypoxia, hypotension, seizures, and infection.[77] No single therapy reverses raised ICP; outcomes depend on multimodality monitoring, targeted resuscitation, early specialist involvement, and goal-directed care aimed at reducing ICP below 20 mm Hg and maintaining CPP around 60 mm Hg. High clinical vigilance and structured escalation pathways remain essential.[78]
Physicians and advanced practitioners lead diagnostic evaluation, initiate tiered interventions, coordinate neurosurgical consultation, and guide shared decision-making aligned with patient values and advanced directives. General practitioners contribute to early recognition and rapid referral. Nurses provide continuous neurologic monitoring, detect early deterioration, ensure DVT and stress ulcer prophylaxis, titrate ventilation to maintain normocapnia, monitor urinary output, and promptly communicate changes. Pharmacists optimize dosing of osmotherapy, barbiturates, and antiseizure medications while preventing interactions and adverse effects. Interprofessional care bundles, standardized brain herniation code alerts, and coordinated rehabilitation planning enhance patient-centered outcomes, safety, and team performance across the continuum of care.[26][79] Shared decision-making with advanced directives on future functional outcomes is mandatory.[34]
Media
(Click Image to Enlarge)
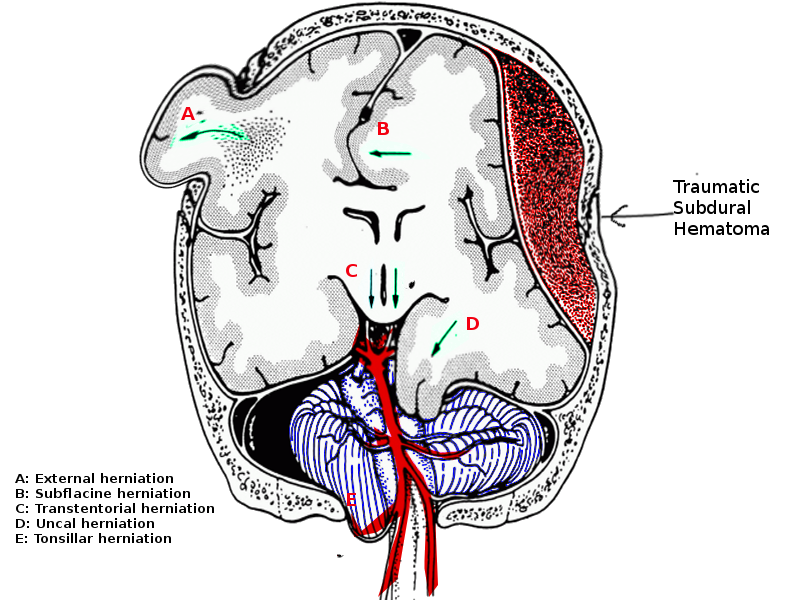
Brain Herniation. Brain herniation is the pathologic displacement of brain tissue driven by pressure gradients between compartments.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
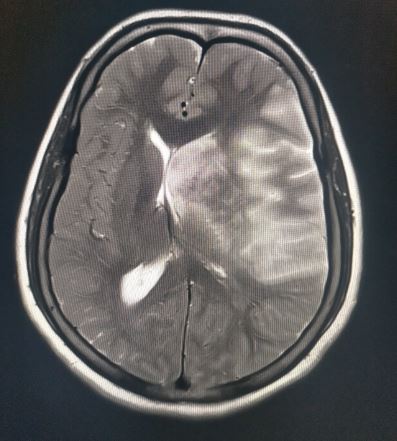
Subfalcine Herniation. This type of herniation involves the cingulate gyrus, which is pushed against the falx cerebri.
Contributed by S Munakomi, MD
(Click Image to Enlarge)
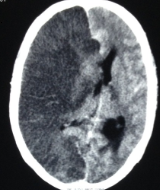
Hemispheric Infarction Radiologic Findings. Image demonstrating gross midline shift in hemispheric infarction.
Contributed by S Munakomi, MD
(Click Image to Enlarge)
Hemorrhagic Transformation Radiologic Finding. Image demonstrating gross midline shift in hemispheric infarction with hemorrhagic transformation.
Contributed by S Munakomi, MD
(Click Image to Enlarge)
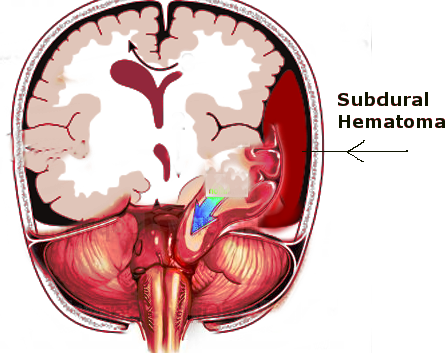
Subdural Hematoma and Uncal Herniation. Progressive limitation of intracranial space allows volumetric forces to displace the uncal portion of the temporal lobe toward the foramen magnum, resulting in cerebral herniation.
Contributed by S Bhimji, MD
References
Mokri B. The Monro-Kellie hypothesis: applications in CSF volume depletion. Neurology. 2001 Jun 26:56(12):1746-8 [PubMed PMID: 11425944]
Davidson CL, Kumar A. Intracranial Hypertension. StatPearls. 2025 Jan:(): [PubMed PMID: 29939588]
Stevens RD, Shoykhet M, Cadena R. Emergency Neurological Life Support: Intracranial Hypertension and Herniation. Neurocritical care. 2015 Dec:23 Suppl 2(Suppl 2):S76-82. doi: 10.1007/s12028-015-0168-z. Epub [PubMed PMID: 26438459]
Cardoso FS, Lee WM, Karvellas CJ, U.S. Acute Liver Failure Study Group. Brain CT Scan Diagnostic and Prognostic Value in Patients With Acute Liver Failure and Cerebral Edema: A Multicenter Cohort Study. Critical care explorations. 2025 Apr 1:7(4):e1251. doi: 10.1097/CCE.0000000000001251. Epub 2025 Apr 15 [PubMed PMID: 40232229]
Lapa DA, Rangwala S, Zebian B, Brown M, Chu J, Chmait RH. Late Prenatal Development of Hindbrain Herniation in Open Spina Bifida. Fetal diagnosis and therapy. 2025:52(4):429-438. doi: 10.1159/000543850. Epub 2025 Feb 13 [PubMed PMID: 39947152]
Hughes P, Lu L, Shi M, Syed D. Cerebral Edema Leading to Subfalcine and Uncal Herniation in a Patient With Retinal Vasculopathy With Cerebral Leukoencephalopathy and Systemic Manifestations. The Neurohospitalist. 2025 Jul:15(3):313-316. doi: 10.1177/19418744241310473. Epub 2024 Dec 20 [PubMed PMID: 39712866]
Adams CA, Stein DM, Morrison JJ, Scalea TM. Does intracranial pressure management hurt more than it helps in traumatic brain injury? Trauma surgery & acute care open. 2018:3(1):e000142. doi: 10.1136/tsaco-2017-000142. Epub 2018 Jan 12 [PubMed PMID: 29766131]
Rabelo NN, da Silva Brito J, da Silva JS, de Souza NB, Coelho G, Brasil S, Frigieri G. The historic evolution of intracranial pressure and cerebrospinal fluid pulse pressure concepts: Two centuries of challenges. Surgical neurology international. 2021:12():274. doi: 10.25259/SNI_53_2021. Epub 2021 Jun 14 [PubMed PMID: 34221605]
Brasil S, Patriota GC, Godoy DA, Paranhos JL, Rubiano AM, Paiva WS. Monro-Kellie 4.0: moving from intracranial pressure to intracranial dynamics. Critical care (London, England). 2025 Jun 5:29(1):229. doi: 10.1186/s13054-025-05476-7. Epub 2025 Jun 5 [PubMed PMID: 40474297]
Wilson MH. Monro-Kellie 2.0: The dynamic vascular and venous pathophysiological components of intracranial pressure. Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism. 2016 Aug:36(8):1338-50. doi: 10.1177/0271678X16648711. Epub 2016 May 12 [PubMed PMID: 27174995]
Ropper AH. Hyperosmolar therapy for raised intracranial pressure. The New England journal of medicine. 2012 Aug 23:367(8):746-52. doi: 10.1056/NEJMct1206321. Epub [PubMed PMID: 22913684]
Liang B, Hu S, Zhang L, Yang L, Wang Y. The Effects of Cerebral Perfusion Pressure Change on Acute Intraoperative Brain Herniation in Patients With Severe Traumatic Brain Injury. Cureus. 2025 Jun:17(6):e85890. doi: 10.7759/cureus.85890. Epub 2025 Jun 12 [PubMed PMID: 40656357]
Saadoun S, Asif H, Papadopoulos MC. The concepts of Intra Spinal Pressure (ISP), Intra Thecal Pressure (ITP), and Spinal Cord Perfusion Pressure (SCPP) in acute, severe traumatic spinal cord injury: Narrative review. Brain & spine. 2024:4():103919. doi: 10.1016/j.bas.2024.103919. Epub 2024 Oct 16 [PubMed PMID: 39654909]
Level 3 (low-level) evidencePlum F, Posner JB. The diagnosis of stupor and coma. Contemporary neurology series. 1972:10():1-286 [PubMed PMID: 4664014]
Kostecki K, De Jesus O, Pearson-Shaver AL. Subfalcine Herniation. StatPearls. 2025 Jan:(): [PubMed PMID: 30725631]
Decker R, Pearson-Shaver AL. Uncal Herniation. StatPearls. 2025 Jan:(): [PubMed PMID: 30725793]
Hall WA, Bhardwaj A. Duret Hemorrhages. StatPearls. 2025 Jan:(): [PubMed PMID: 32809330]
Knight J, Rayi A. Transtentorial Herniation. StatPearls. 2025 Jan:(): [PubMed PMID: 32809371]
Velpula S, Goyal N. Ascending Transtentorial Herniation: A Rare Complication of Posterior Cranial Fossa Tumors and Review of Literature. Asian journal of neurosurgery. 2025 Dec:20(4):842-847. doi: 10.1055/s-0045-1810024. Epub 2025 Aug 28 [PubMed PMID: 41340748]
Moscardini-Martelli J, Ponce-Gomez JA, Alcocer-Barradas V, Romano-Feinholz S, Padilla-Quiroz P, Zazueta MO, Ortega-Porcayo LA. Upward transtentorial herniation: A new role for endoscopic third ventriculostomy. Surgical neurology international. 2021:12():334. doi: 10.25259/SNI_140_2021. Epub 2021 Jul 6 [PubMed PMID: 34345475]
Woo PYM, Lo WHY, Wong HT, Chan KY. The "Negative" Impact of a Subgaleal Drain: Post-cranioplasty Negative Pressure Subgaleal Drain-induced Ascending Transtentorial Herniation. Asian journal of neurosurgery. 2019 Jan-Mar:14(1):256-261. doi: 10.4103/ajns.AJNS_285_17. Epub [PubMed PMID: 30937048]
Mehrvar R, Ebrahimi MJ, Eini P, Moafi M, Mahrooz MH, Gholampour F, Shojaee M. Early-Onset Sunken Brain Syndrome: An Exploratory Review of Risk Determinants and Surgical Implications. World neurosurgery. 2025 Sep:201():124267. doi: 10.1016/j.wneu.2025.124267. Epub 2025 Jul 8 [PubMed PMID: 40639755]
Ozer G, Ekinci HI, Kavak RP. Brain herniation into arachnoid granulations: an underrecognized posterior fossa finding. Neuroradiology. 2025 Nov:67(11):3075-3081. doi: 10.1007/s00234-025-03692-0. Epub 2025 Jul 8 [PubMed PMID: 40627191]
Gafen N, Sirotkin I, Pennington A, Rea B, Martinez CR. Uncommon Locations for Brain Herniations Into Arachnoid Granulations: 5 Cases and Literature Review. Federal practitioner : for the health care professionals of the VA, DoD, and PHS. 2025 Jan:42(1):48-52a. doi: 10.12788/fp.0489. Epub 2025 Jun 18 [PubMed PMID: 40529602]
Level 3 (low-level) evidenceAydin E, Yerli H, Gezmiş E. Temporal Lobe Parenchyma Herniation into the Transverse Sinus: MRI Findings in a Case. Journal of the Belgian Society of Radiology. 2016 Jan 29:100(1):7. doi: 10.5334/jbr-btr.1001. Epub 2016 Jan 29 [PubMed PMID: 30151437]
Level 3 (low-level) evidenceHang L, Zhong X, Cai Y. In-hospital unexpected cerebral herniation-New neurosurgical quality control standards: A case report. Medicine. 2025 Oct 3:104(40):e44855. doi: 10.1097/MD.0000000000044855. Epub [PubMed PMID: 41054146]
Level 2 (mid-level) evidencePapangelou A, Zink EK, Chang WW, Frattalone A, Gergen D, Gottschalk A, Geocadin RG. Automated Pupillometry and Detection of Clinical Transtentorial Brain Herniation: A Case Series. Military medicine. 2018 Jan 1:183(1-2):e113-e121. doi: 10.1093/milmed/usx018. Epub [PubMed PMID: 29315412]
Level 2 (mid-level) evidencePark C, Park SY, Kim M, Park B, Hong JM. Automated quantitative pupillometry as a predictor for transtentorial brain herniation in patients with malignant acute ischemic stroke. PloS one. 2025:20(1):e0316358. doi: 10.1371/journal.pone.0316358. Epub 2025 Jan 10 [PubMed PMID: 39792838]
Laine FJ, Shedden AI, Dunn MM, Ghatak NR. Acquired intracranial herniations: MR imaging findings. AJR. American journal of roentgenology. 1995 Oct:165(4):967-73 [PubMed PMID: 7677003]
Riveros Gilardi B, Muñoz López JI, Hernández Villegas AC, Garay Mora JA, Rico Rodríguez OC, Chávez Appendini R, De la Mora Malváez M, Higuera Calleja JA. Types of Cerebral Herniation and Their Imaging Features. Radiographics : a review publication of the Radiological Society of North America, Inc. 2019 Oct:39(6):1598-1610. doi: 10.1148/rg.2019190018. Epub [PubMed PMID: 31589570]
Parikh S, Hendrix CG, Norman J, Kurklinsky AK. Elevating Prehospital Traumatic Brain Injury Care: A Comparative Analysis of Civilian and Military Air Transport Guidelines. Air medical journal. 2024 Nov-Dec:43(6):548-552. doi: 10.1016/j.amj.2024.10.002. Epub 2024 Oct 28 [PubMed PMID: 39632036]
Level 2 (mid-level) evidenceCadena R, Shoykhet M, Ratcliff JJ. Emergency Neurological Life Support: Intracranial Hypertension and Herniation. Neurocritical care. 2017 Sep:27(Suppl 1):82-88. doi: 10.1007/s12028-017-0454-z. Epub [PubMed PMID: 28913634]
Choo YH, Seo Y, Oh HJ. Deep Sedation in Traumatic Brain Injury Patients. Korean journal of neurotrauma. 2023 Jun:19(2):185-194. doi: 10.13004/kjnt.2023.19.e19. Epub 2023 May 31 [PubMed PMID: 37431376]
Patel PP, Egodage T, Martin MJ. Decompressive craniectomy for traumatic brain injury: a review of recent landmark trials. Trauma surgery & acute care open. 2025:10(Suppl 1):e001784. doi: 10.1136/tsaco-2025-001784. Epub 2025 Apr 14 [PubMed PMID: 40260232]
Hutchinson PJ, Kolias AG, Timofeev IS, Corteen EA, Czosnyka M, Timothy J, Anderson I, Bulters DO, Belli A, Eynon CA, Wadley J, Mendelow AD, Mitchell PM, Wilson MH, Critchley G, Sahuquillo J, Unterberg A, Servadei F, Teasdale GM, Pickard JD, Menon DK, Murray GD, Kirkpatrick PJ, RESCUEicp Trial Collaborators. Trial of Decompressive Craniectomy for Traumatic Intracranial Hypertension. The New England journal of medicine. 2016 Sep 22:375(12):1119-30. doi: 10.1056/NEJMoa1605215. Epub 2016 Sep 7 [PubMed PMID: 27602507]
Zoerle T, Beqiri E, Åkerlund CAI, Gao G, Heldt T, Hawryluk GWJ, Stocchetti N. Intracranial pressure monitoring in adult patients with traumatic brain injury: challenges and innovations. The Lancet. Neurology. 2024 Sep:23(9):938-950. doi: 10.1016/S1474-4422(24)00235-7. Epub [PubMed PMID: 39152029]
Level 2 (mid-level) evidenceSauvigny T, Göttsche J, Czorlich P, Vettorazzi E, Westphal M, Regelsberger J. Intracranial pressure in patients undergoing decompressive craniectomy: new perspective on thresholds. Journal of neurosurgery. 2018 Mar:128(3):819-827. doi: 10.3171/2016.11.JNS162263. Epub 2017 Apr 14 [PubMed PMID: 28409728]
Level 3 (low-level) evidenceChen S, Wang H, Zhang L, Xi Y, Lu Y, Yu K, Zhu Y, Regina I, Bi Y, Tong F. Glymphatic system: a self-purification circulation in brain. Frontiers in cellular neuroscience. 2025:19():1528995. doi: 10.3389/fncel.2025.1528995. Epub 2025 Feb 12 [PubMed PMID: 40012567]
Reddy OC, van der Werf YD. The Sleeping Brain: Harnessing the Power of the Glymphatic System through Lifestyle Choices. Brain sciences. 2020 Nov 17:10(11):. doi: 10.3390/brainsci10110868. Epub 2020 Nov 17 [PubMed PMID: 33212927]
Peng J, Wang S, Wang J, Liu B, Yuan Y, Yin L. Predictive modeling of brain herniation risk factors and critical thresholds in spontaneous intracerebral hemorrhage: a pilot study. Frontiers in neurology. 2025:16():1612346. doi: 10.3389/fneur.2025.1612346. Epub 2025 Nov 3 [PubMed PMID: 41255783]
Level 3 (low-level) evidenceNaik A, Ramirez C, Hoglund B, Iyer A, Barrie U, Sandoval-Garcia C, Venteicher AS, Guillaume D, Arnold PM. Decompressive craniectomy following traumatic brain injury in pediatric patients: An aggregative and individual patient data meta-analysis. Clinical neurology and neurosurgery. 2025 Dec:259():109210. doi: 10.1016/j.clineuro.2025.109210. Epub 2025 Oct 22 [PubMed PMID: 41138514]
Level 1 (high-level) evidenceLara-Reyna J, Karabacak M, Wedderburn R, Legome E, Margetis K. Midbrain volume in brain herniation: A volumetric analysis in operative traumatic brain injury. Surgical neurology international. 2024:15():437. doi: 10.25259/SNI_389_2024. Epub 2024 Nov 29 [PubMed PMID: 39640336]
Dhandapani S, Manju D, Sharma B, Mahapatra A. Prognostic significance of age in traumatic brain injury. Journal of neurosciences in rural practice. 2012 May:3(2):131-5. doi: 10.4103/0976-3147.98208. Epub [PubMed PMID: 22865961]
Corriero A, Fornaciari A, Terrazzino S, Zangari R, Izzi A, Peluso L, Savi M, Faso C, Cavallini L, Polato M, Vitali E, Schuind S, Taccone FS, Bogossian EG. The impact of age and intensity of treatment on the outcome of traumatic brain injury. Frontiers in neurology. 2024:15():1471209. doi: 10.3389/fneur.2024.1471209. Epub 2024 Nov 22 [PubMed PMID: 39650242]
Vadan IM, Grad D, Strilciuc S, Stefanescu E, Verisezan Rosu O, Michalak M, Blesneag AV, Muresanu D. Glasgow Coma Scale Score at Admission in Traumatic Brain Injury Patients: A Multicenter Observational Analysis. Journal of clinical medicine. 2025 Jul 22:14(15):. doi: 10.3390/jcm14155195. Epub 2025 Jul 22 [PubMed PMID: 40806816]
Iyanna N, Donohue JK, Lorence JM, Guyette FX, Gimbel E, Brown JB, Daley BJ, Eastridge BJ, Miller RS, Nirula R, Harbrecht BG, Claridge JA, Phelan HA, Vercruysse GA, O'Keefe T, Joseph B, Shutter LA, Sperry JL. Early Glasgow Coma Scale Score and Prediction of Traumatic Brain Injury: A Secondary Analysis of Three Harmonized Prehospital Randomized Clinical Trials. Prehospital emergency care. 2025:29(5):615-623. doi: 10.1080/10903127.2024.2381048. Epub 2024 Aug 6 [PubMed PMID: 39042825]
Level 1 (high-level) evidenceVeerapaneni D, Arunachalam Sakthiyendran N, Du Y, Mallinger LA, Reinert A, Yeon Kim S, Nguyen C, Daneshmand A, Abdalkader M, Mohammed S, Dupuis J, Sheth KN, Gilmore EJ, Greer D, Ong CJ. Early Pupil Abnormality Frequency Predicts Poor Outcomes and Enhances International Mission for Prognosis and Analysis of Clinical Trials in Traumatic Brain Injury (IMPACT) Model Prognostication in Traumatic Brain Injury. Critical care explorations. 2025 May 1:7(5):e1257. doi: 10.1097/CCE.0000000000001257. Epub 2025 Apr 29 [PubMed PMID: 40299976]
Munakomi S. A comparative study between Marshall and Rotterdam CT scores in predicting early deaths in patients with traumatic brain injury in a major tertiary care hospital in Nepal. Chinese journal of traumatology = Zhonghua chuang shang za zhi. 2016:19(1):25-7 [PubMed PMID: 27033268]
Level 2 (mid-level) evidenceGiordano JC, Melo JRT, Tischer CMB, de Oliveira LD, Salazar MYO, Rocha AJD, de Oliveira JG, Veiga JCE. Performance of the Marshall and Rotterdam scales as predictors of mortality in children with severe traumatic brain injury. Neuro-Chirurgie. 2025 Sep:71(5):101699. doi: 10.1016/j.neuchi.2025.101699. Epub 2025 Jul 3 [PubMed PMID: 40617287]
Oddo M, Levine JM, Mackenzie L, Frangos S, Feihl F, Kasner SE, Katsnelson M, Pukenas B, Macmurtrie E, Maloney-Wilensky E, Kofke WA, LeRoux PD. Brain hypoxia is associated with short-term outcome after severe traumatic brain injury independently of intracranial hypertension and low cerebral perfusion pressure. Neurosurgery. 2011 Nov:69(5):1037-45; discussion 1045. doi: 10.1227/NEU.0b013e3182287ca7. Epub [PubMed PMID: 21673608]
Lacerte M, Hays Shapshak A, Mesfin FB. Hypoxic Brain Injury. StatPearls. 2025 Jan:(): [PubMed PMID: 30725995]
Thirawattanasoot N, Chantanakomes J, Pansiritanachot W, Rangabpai W, Surabenjawong U, Chaisirin W, Riyapan S, Shin SD, Song KJ, Chiang WC, Jamaluddin SF, Kajino K. Association between prehospital oxygen saturation and outcomes in hypotensive traumatic brain injury patients in Asia (Pan-Asian Trauma Outcomes Study (PATOS)). International journal of emergency medicine. 2025 Jun 17:18(1):104. doi: 10.1186/s12245-025-00914-3. Epub 2025 Jun 17 [PubMed PMID: 40528198]
Seo DE, Shin SD, Song KJ, Ro YS, Hong KJ, Park JH. Effect of hypoxia on mortality and disability in traumatic brain injury according to shock status: A cross-sectional analysis. The American journal of emergency medicine. 2019 Sep:37(9):1709-1715. doi: 10.1016/j.ajem.2018.12.022. Epub 2018 Dec 20 [PubMed PMID: 30583816]
Level 2 (mid-level) evidenceLee JW, Wang W, Rezk A, Mohammed A, Macabudbud K, Englesakis M, Lele A, Zeiler FA, Chowdhury T. Hypotension and Adverse Outcomes in Moderate to Severe Traumatic Brain Injury: A Systematic Review and Meta-Analysis. JAMA network open. 2024 Nov 4:7(11):e2444465. doi: 10.1001/jamanetworkopen.2024.44465. Epub 2024 Nov 4 [PubMed PMID: 39527054]
Level 1 (high-level) evidenceHardy BM, King KL, Enninghorst N, Balogh ZJ. Trends in polytrauma incidence among major trauma admissions. European journal of trauma and emergency surgery : official publication of the European Trauma Society. 2024 Jun:50(3):623-626. doi: 10.1007/s00068-022-02200-w. Epub 2022 Dec 19 [PubMed PMID: 36536173]
Niemeyer M, Jochems D, Houwert RM, van Es MA, Leenen L, van Wessem K. Mortality in polytrauma patients with moderate to severe TBI on par with isolated TBI patients: TBI as last frontier in polytrauma patients. Injury. 2022 Apr:53(4):1443-1448. doi: 10.1016/j.injury.2022.01.009. Epub 2022 Jan 5 [PubMed PMID: 35067344]
Mishra NR, Agrawal A, Das RR. Hypertonic Saline vs. Mannitol in Management of Elevated Intracranial Pressure in Children: A Meta-Analysis. Indian journal of pediatrics. 2023 Sep:90(9):899-906. doi: 10.1007/s12098-023-04532-w. Epub 2023 May 25 [PubMed PMID: 37225962]
Level 1 (high-level) evidenceGharizadeh N, Ghojazadeh M, Naseri A, Dolati S, Tarighat F, Soleimanpour H. Hypertonic saline for traumatic brain injury: a systematic review and meta-analysis. European journal of medical research. 2022 Nov 20:27(1):254. doi: 10.1186/s40001-022-00897-4. Epub 2022 Nov 20 [PubMed PMID: 36404350]
Level 1 (high-level) evidenceMoyer JD, Elouahmani S, Codorniu A, Abback PS, Jeantrelle C, Goutagny S, Gauss T, Sigaut S. External ventricular drainage for intracranial hypertension after traumatic brain injury: is it really useful? European journal of trauma and emergency surgery : official publication of the European Trauma Society. 2023 Jun:49(3):1227-1234. doi: 10.1007/s00068-022-01903-4. Epub 2022 Feb 16 [PubMed PMID: 35169869]
Dagod G, Laurens M, Roustan JP, Deras P, Courvalin E, Girard M, Weber H, Capdevila X, Charbit J. Impact of lumbar cerebrospinal fluid drainage to control intracranial hypertension in patients with severe traumatic brain injury: a retrospective monocentric cohort. Critical care (London, England). 2025 Jan 2:29(1):2. doi: 10.1186/s13054-024-05199-1. Epub 2025 Jan 2 [PubMed PMID: 39748237]
Level 2 (mid-level) evidenceStevens AR, Soon WC, Chowdhury YA, Toman E, Yim S, Veenith T, Chelvarajah R, Belli A, Davies D. External Lumbar Drainage for Refractory Intracranial Hypertension in Traumatic Brain Injury: A Systematic Review. Cureus. 2022 Oct:14(10):e30033. doi: 10.7759/cureus.30033. Epub 2022 Oct 7 [PubMed PMID: 36348893]
Level 1 (high-level) evidenceWu P, Ren S, Wu G, Wang L. Optimal Timing for Stereotactic Minimally Invasive Surgery in Supratentorial Spontaneous Intracerebral Hemorrhage With Tentorial Herniation: A Retrospective Study. Revista de neurologia. 2025 Nov 30:80(10):38627. doi: 10.31083/RN38627. Epub [PubMed PMID: 41351391]
Level 2 (mid-level) evidenceMouchtouris N, Luck T, Yudkoff C, Locke K, Momin A, Khanna O, Andrews C, Gonzalez G, Harrop J, Shah SO, Jallo J. Ventriculostomy Associated with Reduced Mortality in Severe Traumatic Brain Injury Compared to Parenchymal ICP Monitoring: A Propensity Score-Adjusted Analysis. World neurosurgery. 2023 Oct:178():e445-e452. doi: 10.1016/j.wneu.2023.07.096. Epub 2023 Jul 24 [PubMed PMID: 37495098]
Chesnut RM, Temkin N, Carney N, Dikmen S, Rondina C, Videtta W, Petroni G, Lujan S, Pridgeon J, Barber J, Machamer J, Chaddock K, Celix JM, Cherner M, Hendrix T, Global Neurotrauma Research Group. A trial of intracranial-pressure monitoring in traumatic brain injury. The New England journal of medicine. 2012 Dec 27:367(26):2471-81. doi: 10.1056/NEJMoa1207363. Epub 2012 Dec 12 [PubMed PMID: 23234472]
Level 1 (high-level) evidenceKrishnan P, Chowdhury SR. "White cerebellum" sign - A dark prognosticator. Journal of neurosciences in rural practice. 2014 Oct:5(4):433. doi: 10.4103/0976-3147.140015. Epub [PubMed PMID: 25288860]
Dampier CH, Boire NA, Fernandez K, Troncoso JC. Anteromedial striatum and globus pallidus infarcts: Uncommon complications of cerebral herniation in the setting of acute subdural hemorrhage. Journal of forensic sciences. 2025 Nov 11:():. doi: 10.1111/1556-4029.70224. Epub 2025 Nov 11 [PubMed PMID: 41219588]
Guo G, Cao H, Yang Z, Shi L. Neurogenic pulmonary edema in a child with traumatic epidural hematoma and brain herniation. Saudi journal of anaesthesia. 2025 Jul-Sep:19(3):406-409. doi: 10.4103/sja.sja_561_24. Epub 2025 Jun 16 [PubMed PMID: 40642649]
Chen A, Zhong H, Peng J, Luo T, Jun S. Machine Learning-Based Modeling for Predicting Hypopituitarism After Cranial Trauma. World neurosurgery. 2025 Jul:199():124018. doi: 10.1016/j.wneu.2025.124018. Epub 2025 May 13 [PubMed PMID: 40368087]
Chen S, Wang L, Kang Q. Herniation secondary to critical cerebrospinal fluid hypovolemia after supratentorial craniotomy: a single-center case series. Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology. 2025 Apr:46(4):1765-1775. doi: 10.1007/s10072-024-07940-8. Epub 2024 Dec 12 [PubMed PMID: 39666209]
Level 2 (mid-level) evidenceIdris Z, Mustapha M, Abdullah JM. Microgravity environment and compensatory: Decompensatory phases for intracranial hypertension form new perspectives to explain mechanism underlying communicating hydrocephalus and its related disorders. Asian journal of neurosurgery. 2014 Jan:9(1):7-13. doi: 10.4103/1793-5482.131058. Epub [PubMed PMID: 24891884]
Level 3 (low-level) evidenceGopalakrishnan MS, Shanbhag NC, Shukla DP, Konar SK, Bhat DI, Devi BI. Complications of Decompressive Craniectomy. Frontiers in neurology. 2018:9():977. doi: 10.3389/fneur.2018.00977. Epub 2018 Nov 20 [PubMed PMID: 30524359]
Kobata H. Clinical Insights and Future Directions in Hypothermia for Severe Traumatic Brain Injury: A Narrative Review. Journal of clinical medicine. 2024 Jul 19:13(14):. doi: 10.3390/jcm13144221. Epub 2024 Jul 19 [PubMed PMID: 39064261]
Level 3 (low-level) evidenceSkibiski J, Patel P, Abdijadid S. Barbiturates. StatPearls. 2025 Jan:(): [PubMed PMID: 30969553]
Mansour N, deSouza RM, Sikorski C, Kahana M, Frim D. Role of barbiturate coma in the management of focally induced, severe cerebral edema in children. Journal of neurosurgery. Pediatrics. 2013 Jul:12(1):37-43. doi: 10.3171/2013.3.PEDS12196. Epub 2013 May 3 [PubMed PMID: 23641961]
Robinson DL. Head injuries and bicycle helmet laws. Accident; analysis and prevention. 1996 Jul:28(4):463-75 [PubMed PMID: 8870773]
Smith M. Multimodality Neuromonitoring in Adult Traumatic Brain Injury: A Narrative Review. Anesthesiology. 2018 Feb:128(2):401-415. doi: 10.1097/ALN.0000000000001885. Epub [PubMed PMID: 28938277]
Level 3 (low-level) evidenceRoh D, Park S. Brain Multimodality Monitoring: Updated Perspectives. Current neurology and neuroscience reports. 2016 Jun:16(6):56. doi: 10.1007/s11910-016-0659-0. Epub [PubMed PMID: 27095434]
Level 3 (low-level) evidenceTripathy S, Ahmad SR. Raised Intracranial Pressure Syndrome: A Stepwise Approach. Indian journal of critical care medicine : peer-reviewed, official publication of Indian Society of Critical Care Medicine. 2019 Jun:23(Suppl 2):S129-S135. doi: 10.5005/jp-journals-10071-23190. Epub [PubMed PMID: 31485121]
Lee EJ, Maguire L, Dharia R, Shah SO. Protocol in Practice: Impact of Brain Herniation Code Alerts at a Tertiary Level Medical Center. Journal for healthcare quality : official publication of the National Association for Healthcare Quality. 2025 Jul-Sep 01:47(3):. pii: e0488. doi: 10.1097/JHQ.0000000000000488. Epub 2025 Jun 27 [PubMed PMID: 40577222]
Level 2 (mid-level) evidence