Introduction
Medicine has made significant progress in understanding blood circulation in the past few hundred years. For millennia, medical practitioners believed in the 4 humors and used bloodletting as a treatment. In the 1600s, William Harvey demonstrated how the circulatory system functioned. Soon afterward, scientists became interested in blood transfusion, initially transfusing animal blood into humans. Dr Philip Syng Physick performed the first human blood transfusion in 1795, and Dr James Blundell performed the first transfusion of human blood to treat hemorrhage in England in 1818.[1] Substantial progress has occurred in understanding blood typing, blood components, and storage since the early 1900s. These advances led to the development of the field of transfusion medicine. Transfusion medicine involves laboratory and clinical medicine, and clinicians from multiple specialties, such as pathology, hematology, anesthesia, and pediatrics. Charles R. Drew was an American surgeon and one of the pioneers of blood banking during World War II. Transfusion of red blood cells has become a relatively common procedure. In the US, around 15 million units are transfused annually, while about 85 million units are transfused worldwide.[2][3][4]
Blood is typically stored in its various components. Fresh whole blood has historically been considered the transfusion standard; however, advances in medicine have enabled the efficient use of individual blood components, including packed red blood cells, factor concentrates, fresh-frozen plasma, platelet concentrates, and cryoprecipitate. Consequently, current indications for whole blood transfusion are generally limited. The US military buddy transfusion system is the most widely used whole-blood transfusion system.[5][6] Whole-blood transfusion is especially important in combat scenarios, and early transfusion is associated with improved outcomes.[7] Additionally, whole blood transfusion in civilian prehospital settings and the trauma bay is seeing a resurgence in some regions.
Indications
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Indications
Guidelines on red blood cell transfusion from the American Association of Blood Banks recommend a restrictive approach for patients with nonhemorrhagic anemia.[8] Although definitions may vary, anemia is typically defined as a hemoglobin level less than 13 g/dL in men and 12 g/dL in women. Current practice uses a more restrictive threshold to guide transfusion decisions; previously, a liberal strategy, typically using a cutoff of hemoglobin less than 10 g/dL, was used; however, hemoglobin target values have significantly changed over the years.[9]
Current guidelines for red blood cell transfusion generally use a restrictive threshold. Although there is some variation in threshold values, 7.0 g/dL is generally agreed upon for asymptomatic healthy patients. Results from multiple studies showed that this is an acceptable threshold in other patient populations, including those with gastrointestinal tract bleeding and critically ill patients. The guidelines recommend thresholds of 7.5 g/dL and 8 g/dL for patients with coronary artery disease and those undergoing orthopedic surgical procedures, respectively.[10] However, this may be due to a lack of literature on the use of a 7 g/dL threshold in studies evaluating these patient populations. The guidelines and clinical trials on Transfusion Requirements in Critical Care also recommend a threshold of 7 g/dL for critically ill patients.[10][11][12][13]
Transfusion Limits in Acute Myocardial Infarction
The landmark Myocardial Ischemia and Transfusion trial studied the effects of liberal versus conservative transfusion standards in patients with acute myocardial infarction. In the restrictive strategy group, hemoglobin was maintained between 7.0 and 8.0 g/dL, while in the liberal transfusion group, transfusion was initiated if hemoglobin was less than 10.0 g/dL. The liberal strategy group received a mean of 2.5 units of packed red blood cells, compared with 0.7 units in the restrictive group. Results from this study showed a trend toward increased 30-day mortality and recurrent myocardial infarction with lower transfusion limits, although this did not reach statistical significance. When stratified by 4 goal hemoglobin levels (greater than 7.0, 8.0, 9.0, and 10.0 g/dL), lower hemoglobin levels were associated with increased mortality and cardiac events.[9][14][15]
These findings contrast with results from the Restrictive and Liberal Transfusion Strategies in Patients With Acute Myocardial Infarction trial, which showed noninferiority when transfusion was initiated at a hemoglobin level less than 8.0 g/dL compared with initiation at a hemoglobin level less than 10.0 g/dL in patients with acute myocardial infarction. Results from this study showed that the lower transfusion threshold was noninferior to the higher transfusion threshold at 30 days; however, the major adverse cardiac event rate was overall higher with the lower transfusion threshold. At a 1-year follow-up, patients in the restrictive transfusion group had significantly higher major adverse cardiac event rates and mortality. This trial also had lower power, with approximately 630 participants compared with approximately 3500 participants in the Myocardial Ischemia and Transfusion trial.[9][16][17]
In patients who are actively bleeding after traumatic injury, results from one study of adult patients with severe trauma at risk for major bleeding showed that a restrictive transfusion strategy, with a target hemoglobin level of 7.0 to 9.0 g/dL, was not inferior to a more liberal approach of transfusing to a goal of 10 to 12 g/dL.[18] Transfusion may also be indicated in patients with active or acute bleeding, and in those with symptoms related to anemia (for example, tachycardia, weakness, and dyspnea on exertion) and hemoglobin levels less than 8 g/dL.[19] In such cases, anemia is defined as a decreased circulating red cell mass, measured as grams of hemoglobin per 100 mL of whole blood. Anemia may result from external loss, inadequate production, internal destruction, or a combination of these factors. Although many patients experiencing active bleeding become anemic, anemia alone is not an indication for transfusion. Severe hemorrhage can cause shock, which reflects an insufficient supply of oxygen to support cellular metabolism. Red cell mass repletion is one facet of the treatment of hemorrhagic shock.
Unless the patient is actively bleeding, clinicians should transfuse 1 unit of packed red blood cells at a time, which typically increases hemoglobin by 1 g/dL and hematocrit by 3%. Clinicians should then check the posttransfusion hemoglobin level.[20] However, in cases of major bleeding, a massive transfusion protocol may be necessary, with blood components administered in a balanced ratio of 1:1:1 or 2:1:1 for packed red cells, plasma, and platelets.[21] The American Society of Anesthesiologists advises transfusion at hemoglobin levels of 6 g/dL or less. However, results from more recent studies showed decreased mortality with preanesthetic hemoglobin levels greater than 8 g/dL, especially in patients undergoing renal transplant.[22]
Patients can be transfused with whole blood or component therapy (ie, red blood cells, plasma, and platelets). For most of the 1900s, whole blood was used for transfusions; however, advances in technology made component therapy more common. Results from studies evaluating whole-blood therapy compared with component therapy, especially in trauma, using low-titer type O whole blood, showed that whole-blood transfusion may reduce hemorrhage-related mortality in the prehospital setting, although whole blood has a shorter shelf life than red blood cell component therapy.[23]
The transfusion of fresh frozen plasma is common, but specific indications for its use are limited. Evidence is insufficient for its use in many clinical scenarios, such as prophylaxis in patients who are not bleeding.[24][25][26] Fresh-frozen plasma transfusion is sometimes indicated for bleeding patients to replace lost coagulation factors. Clinical situations that meet this criterion include cardiopulmonary bypass, massive transfusion, decompensated liver disease, extracorporeal pulmonary support techniques, and acute disseminated intravascular coagulation. In the past, fresh frozen plasma, combined with vitamin K, was indicated for warfarin excess in cases of life-threatening hemorrhage. Fresh-frozen plasma is rarely needed for vitamin K deficiency or warfarin reversal because prothrombin complex concentrate is widely available. The exception is concomitant plasma volume deficit.[27]
Platelet transfusion is beneficial in cases of platelet deficiency or dysfunction. In patients with bone marrow failure, prophylactic platelet transfusion is indicated when there are no additional bleeding risk factors and platelet counts are below 10 × 109/L. If other associated risk factors are present, the transfusion threshold may be raised to 20 ×109/L. Platelet counts greater than 50 ×109/L are required before invasive procedures. In active hemorrhage, platelet transfusion should be performed when thrombocytopenia contributes to the hemorrhage and the platelet count is less than 50 × 109/L. When diffuse microvascular bleeding is present, platelet count should be maintained above 100 ×109/L.[28][29]
Cryoprecipitate transfusion is indicated in dysfibrinogenemia or fibrinogen deficiency in the setting of bleeding, injury, invasive procedures, or acute disseminated intravascular coagulation. Cell salvage technology is available and is used to recover blood during surgical procedures for reinfusion to the patient. This technology can reduce the risks associated with allogeneic (donated) blood. Results from a Cochrane review found that in certain surgical procedures, cell salvage reduced blood loss volume and the need for allogeneic transfusions, without significant changes in adverse events.[30]
Contraindications
No absolute contraindications exist, but some patients or their parents (in pediatric cases) may refuse transfusions for religious reasons.[31]
Equipment
Blood products are transfused through intravenous tubing with filters. The filters, which typically have pore diameters of 170 to 260 µm, are also used to prevent particulate debris from being administered. However, particulate entrapment promotes bacterial growth, and the American Association of Blood Banks advises against using a filter for more than 4 hours. Before transfusion, the tubing should be primed with an isotonic, calcium-free, blood-compatible solution, such as normal saline. Citrate is used as a preservative in packed red blood cells, and clots will form in the intravenous line if the calcium level exceeds the amount that citrate can buffer.[32] The equipment required for a blood transfusion includes the following:
- Blood components or whole blood can be provided through various central venous access devices or peripheral intravenous catheters. The following sizes should be considered:
- 20- to 22-gauge for routine transfusion in adults
- 16- to 18-gauge for rapid transfusion in adults
- 22- to 25-gauge for pediatrics
- Blood filters
- The administration of platelet-poor plasma requires supplies that often differ by product and brand.
- Infusion devices, such as infusion pumps, blood warmers, rapid infusers, and pressure devices, can be used to transfuse blood components.
- A pressure infusion device may be needed for the rapid transfusion of blood components.
- A blood warmer device is often needed to prevent hypothermia in the rapid administration of cold blood components, for instance, in trauma settings or operating rooms.
Personnel
Two qualified healthcare professionals should verify blood products before administration, and patients should be monitored during transfusion by qualified personnel. Blood transfusions can be performed by various healthcare professionals, such as registered nurses, licensed vocational nurses, or licensed practical nurses. Nurses usually perform this task under the direction of a clinician. Regarding blood transfusion training requirements, most professionals, such as registered nurses and licensed vocational nurses, learn how to administer blood transfusions through medical training and educational programs.
Preparation
Preparation for blood transfusion involves pretransfusion compatibility testing between the recipient's antibodies and the donor's red blood cells. Pretransfusion testing involves obtaining a sample of the recipient’s blood for a type and screen. The type and screen test verifies the recipient’s blood type and determines whether the recipient has any unexpected non-ABO antibodies that might cause a reaction. Multiple methods are available for performing this screen. If the screen results are negative, a reaction is very unlikely. Blood should be obtained rapidly for the patient when required. If the screen results are positive, many blood banks will crossmatch and hold 2 units of blood for the patient in case transfusion is needed. Another prerequisite for blood transfusion is obtaining the patient's consent, if possible.[33]
The following list includes important steps to follow before proceeding with a blood transfusion:
Find Current Type and Crossmatch
- Obtain a blood sample, which lasts up to 72 hours
- Send the sample to the blood bank
- Ensure that the blood sample has the correct labeling with the date and time
- Wait for the blood bank to crossmatch and prepare the needed units
Obtain Informed Consent and Health History
- Discuss the procedure with the patient
- Confirm the past medical history and any allergies
- The supervising clinician should have obtained signed consent from the patient [33]
Obtain Large-Bore Intravenous Access
- Obtain 18-gauge or larger intravenous access
- Each unit should be transfused within 2 to 4 hours
- A second intravenous access site should be secured in case the patient needs additional intravenous medications
- Normal saline is the only fluid that can be administered with blood products
Assemble Supplies
- Y tubing with an inline filter
- 0.9% sodium chloride solution
- Blood warmer
Obtain Baseline Vital Signs
- Baseline vital signs include heart rate, temperature, blood pressure, pulse oximetry, and respiratory rate
- Respiratory sounds and urine output should also be documented
- The clinician should be notified if the temperature is greater than 100 °F
Obtain Blood from the Blood Bank
- Once the blood bank confirms that the blood is ready, ensure delivery from the blood bank
- Packed red blood cells can only be given one unit at a time
- Once the blood has been released for the patient, the transfusion should begin within 20 to 30 min and be completed within 4 hours.
Technique or Treatment
Here are some of the general steps healthcare professionals should follow when performing a blood transfusion:
- Verify the blood product.
- Explain the features of a transfusion reaction to the patient. The patient should inform the nursing staff of any signs or symptoms that occur during the transfusion.
- Obtain and document baseline vital signs, lung sounds, urine output, and skin color.
- Prepare the Y tube with 0.9% sodium chloride and have the blood unit ready on an infusion pump.
- The blood should infuse slowly for the first 15 min, for instance, 2 mL/min or 120 mL/h.
- Staff should supervise the patient for the first 15 min because most transfusion reactions occur during this period.
- The transfusion rate can be increased after this period if the patient is stable and shows no signs of a transfusion reaction.
- Document vital signs after 15 minutes, then every 1 hour, and finally at the end of the transfusion.
- During the transfusion, assess for any signs of transfusion reactions.If a reaction is suspected, stop the transfusion immediately.
- Disconnect the blood tubing from the patient.Inform the clinician, stay with the patient, and assess the patient’s status.
- After the transfusion, flush the Y tubing with normal saline and dispose of the used Y tubing in the biohazard bin.
- Obtain posttransfusion vital signs.
- After the procedure, some patients may experience soreness at the puncture site, but this should resolve quickly.
Complications
Blood transfusions have multiple complications, including infections, hemolytic reactions, allergic reactions, transfusion-related lung injury, transfusion-associated circulatory overload, and electrolyte imbalance (see Image. Transfusion Reaction Signs and Symptoms).[34][35][36] According to the American Association of Blood Banks, febrile reactions are the most common, followed by transfusion-associated circulatory overload, allergic reaction, transfusion-related lung injury, hepatitis C viral infection, hepatitis B viral infection, HIV infection, and fatal hemolysis, which is extremely rare and occurs in approximately 1 in 2 million transfused units of red blood cells. For comparison, the lifetime odds of dying from a lightning strike are about 1 in 161,000. A list of approximate risks per unit of red blood cell transfusion, adapted from the American Association of Blood Banks clinical guidelines published in October 2023, is provided below.[37]
Adverse Event and Approximate Risk per Unit Transfusion of Red Blood Cells
- Febrile reaction: 1:161
- Allergic reaction: 1:345
- Transfusion-associated circulatory overload: 1:125
- Transfusion-related lung injury: 1:1250
- Anaphylactic reaction: 1:5000
- Hepatitis B infection: 1: 1,100,000
- Hepatitis C infection: 1:1,200,000
- HIV infection: 1:1,600,000
Febrile Reactions
Transfusing with leukocyte-reduced blood products, as most blood products in the US are, may help reduce febrile reactions. If a febrile reaction occurs, the transfusion should be halted and the patient evaluated, as a hemolytic reaction can initially appear similar; clinicians should consider performing a hemolytic or infectious workup. Treatment includes acetaminophen and, if needed, diphenhydramine for symptomatic control. After treatment and exclusion of other causes, the transfusion can be resumed at a slower rate.[38]
Transfusion-Associated Circulatory Overload
Transfusion-associated circulatory overload is characterized by respiratory distress secondary to cardiogenic pulmonary edema. This reaction is most common in patients already in a fluid-overloaded state, such as patients with congestive heart failure or acute renal failure. Diagnosis is based on symptom onset within 6 to 12 hours of transfusion, clinical evidence of fluid overload, pulmonary edema, elevated brain natriuretic peptide levels, and a response to diuretics.[39] Preventive efforts and treatment include limiting transfusions to the minimum necessary, transfusing over the slowest possible time, and administering diuretics before or between transfusions.
Allergic Reaction
Allergic reactions often manifest as urticaria and pruritus and occur in less than 1% of transfusions. More severe symptoms, such as bronchospasm, wheezing, and anaphylaxis, are rare. Allergic reactions may occur in patients who are IgA-deficient because exposure to IgA in donor products can cause severe anaphylactoid reactions. Washing the plasma from the cells before transfusion can help prevent this reaction. Mild symptoms, such as pruritus and urticaria, can be treated with antihistamines. More severe symptoms can be treated with bronchodilators, corticosteroids, and epinephrine.[40]
Transfusion-Related Lung Injury
Transfusion-related lung injury is uncommon, occurring in about 1:12,000 transfusions. Patients develop symptoms within 2 to 4 hours after receiving a transfusion. Patients develop acute hypoxemic respiratory distress, similar to acute respiratory distress syndrome. Patients have pulmonary edema and normal central venous pressure without evidence of left heart failure. Diagnosis is made based on a history of recent transfusion, chest radiography findings showing diffuse patchy infiltrates, and the exclusion of other etiologies. Although transfusion-related lung injury has a 10% mortality rate, the remaining 90% of cases resolve within 96 hours with supportive care only.[41]
Infections
Infections are potential complications. However, the risk of infection has decreased due to screening of potential donors, so the risks of hepatitis C and human immunodeficiency virus infection are less than 1 in 1 million.[42] Bacterial infection can also occur, but it occurs rarely, at about 1 in every 250,000 units of transfused red blood cells.
Fatal Hemolysis
Fatal hemolysis is extremely rare, occurring only in 1 in nearly 2 million transfusions. Fatal hemolysis results from ABO incompatibility, and the recipient’s antibodies recognize and induce hemolysis in the donor’s transfused cells. Patients develop an acute onset of fevers and chills, low back pain, flushing, dyspnea, tachycardia, and shock. Treatment is to stop the transfusion, leave the intravenous access in place, administer normal saline intravenously, and maintain urine output greater than 100 mL/h; diuretics may also be needed. Cardiorespiratory support may be provided as appropriate. A hemolytic workup should also be performed, including sending the donor blood and tubing, as well as posttransfusion laboratory samples from the recipient, to the blood bank:
- Retype and crossmatch
- Direct and indirect Coombs tests
- Complete blood count, creatinine, prothrombin time, and partial thromboplastin time (draw from the other arm)
- Peripheral smear
- Haptoglobin, indirect bilirubin, lactate dehydrogenase, plasma-free hemoglobin
- Urinalysis for hemoglobin
Electrolyte Abnormalities
Electrolyte abnormalities can also occur, although they are rare and more likely associated with large-volume transfusion. Hypocalcemia can result because citrate, an anticoagulant in blood products, binds with calcium.[43] Hyperkalemia can occur from the release of potassium from cells during storage. Risk is higher in neonates and patients with renal insufficiency.[44] Hypokalemia can result from alkalinization of the blood because citrate is converted to bicarbonate by the liver in patients with normal hepatic function.
Clinical Significance
As mentioned in the introduction, the science of transfusion medicine, including red blood cell transfusion, has evolved significantly over the past century. The field of transfusion medicine has evolved and now encompasses multiple medical specialties. The ability to transfuse red blood cells into patients safely and rapidly has revolutionized the care of trauma patients, patients undergoing surgical procedures, and patients with gastrointestinal bleeding, among other conditions. Transfusion medicine will continue to evolve, and ongoing research will improve this process and evaluate alternative methods for delivering oxygen to cells. These advances could potentially reduce the risk of reactions and infection and improve storage.
Enhancing Healthcare Team Outcomes
Our understanding of blood transfusion has improved dramatically over the past 3 decades. Unlike before, empiric blood transfusions are no longer the norm. Although blood products provide clinical benefit, they can also cause harm. Healthcare professionals who treat patients needing a blood transfusion should consult a hematologist if uncertainty about the indications remains. Interprofessional team collaboration is crucial for treating patients undergoing blood transfusions and those having adverse reactions to transfusions. The key is to reduce harm associated with unnecessary blood transfusions.
Effective transfusion practice requires a coordinated interprofessional approach that emphasizes appropriate patient selection, safe administration, rapid recognition of adverse reactions, and clear communication across the care team. Physicians and advanced practitioners are responsible for assessing the indication for transfusion, obtaining informed consent when possible, selecting the appropriate blood product, and reassessing the patient’s response. Nurses play a central role in verifying patient and product identities, monitoring vital signs, educating patients about the symptoms of transfusion reactions, and promptly stopping the transfusion if a reaction is suspected. Pharmacists may assist with medication review, anticoagulation reversal strategies, blood conservation efforts, and evaluation of therapies that may reduce transfusion needs. Laboratory and blood bank professionals support patient safety through compatibility testing, product preparation, and communication of urgent findings. Ethical care requires respect for patient autonomy, including religious objections to transfusion, while ensuring that patients receive clear information about risks, benefits, and alternatives. Consistent documentation, closed-loop communication, and timely escalation of concerns enhance patient-centered outcomes, reduce preventable complications, and improve team performance.
Media
(Click Image to Enlarge)
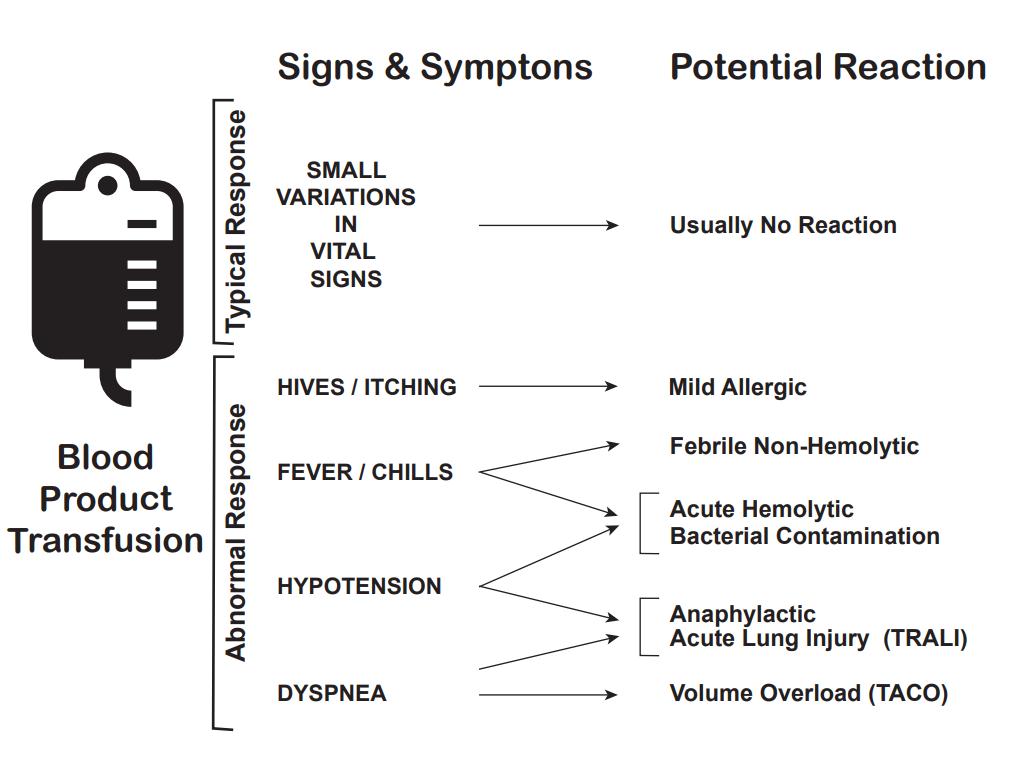
Transfusion Reaction Signs and Symptoms. Clinical signs and symptoms observed during blood product transfusion may indicate adverse reactions, helping distinguish typical physiological variations from critical complications such as acute hemolytic reactions, transfusion-related acute lung injury, and transfusion-associated circulatory overload.
Contributed by K Crookston, MD, PhD
References
Sturgis CC. THE HISTORY OF BLOOD TRANSFUSION. Bulletin of the Medical Library Association. 1942 Jan:30(2):105-12 [PubMed PMID: 16016531]
Bowman Z, Fei N, Ahn J, Wen S, Cumpston A, Shah N, Craig M, Perrotta PL, Kanate AS. Single versus double-unit transfusion: Safety and efficacy for patients with hematologic malignancies. European journal of haematology. 2019 May:102(5):383-388. doi: 10.1111/ejh.13211. Epub 2019 Feb 25 [PubMed PMID: 30664281]
D'Alessandro A. From omics technologies to personalized transfusion medicine. Expert review of proteomics. 2019 Mar:16(3):215-225. doi: 10.1080/14789450.2019.1571917. Epub 2019 Jan 28 [PubMed PMID: 30654673]
Yoshida T, Prudent M, D'alessandro A. Red blood cell storage lesion: causes and potential clinical consequences. Blood transfusion = Trasfusione del sangue. 2019 Jan:17(1):27-52. doi: 10.2450/2019.0217-18. Epub [PubMed PMID: 30653459]
Popovsky MA, Moore SB. Diagnostic and pathogenetic considerations in transfusion-related acute lung injury. Transfusion. 1985 Nov-Dec:25(6):573-7 [PubMed PMID: 4071603]
Daniel Y, Derkenne C, Mahe P, Travers S, Martinaud C. Where Do We Stand on "Buddy Transfusion" During Military Operations? Journal of special operations medicine : a peer reviewed journal for SOF medical professionals. 2022 Dec 16:22(4):46-49. doi: 10.55460/J1X0-4X05. Epub [PubMed PMID: 36525011]
Jarrassier A, Boutonnet M, Duranteau J, Travers S, Prat N, Dubourg O, Pasquier P, Libert N. Initial management of haemorrhagic war casualties: tactical priorities and innovative approaches in modern and future warfare. Critical care (London, England). 2025 Nov 28:29(1):509. doi: 10.1186/s13054-025-05752-6. Epub 2025 Nov 28 [PubMed PMID: 41316469]
Carson JL, Guyatt G, Heddle NM, Grossman BJ, Cohn CS, Fung MK, Gernsheimer T, Holcomb JB, Kaplan LJ, Katz LM, Peterson N, Ramsey G, Rao SV, Roback JD, Shander A, Tobian AA. Clinical Practice Guidelines From the AABB: Red Blood Cell Transfusion Thresholds and Storage. JAMA. 2016 Nov 15:316(19):2025-2035. doi: 10.1001/jama.2016.9185. Epub [PubMed PMID: 27732721]
Level 1 (high-level) evidencePortela GT, Carson JL, Swanson SA, Alexander JH, Hébert PC, Goodman SG, Steg PG, Bertolet M, Strom JB, Fergusson DA, Simon T, White HD, Cooper HA, Abbott JD, Rao SV, Chaitman BR, Fordyce CB, Lopes RD, Daneault B, Brooks MM, MINT Investigators. Effect of Four Hemoglobin Transfusion Threshold Strategies in Patients With Acute Myocardial Infarction and Anemia : A Target Trial Emulation Using MINT Trial Data. Annals of internal medicine. 2024 Nov:177(11):1489-1498. doi: 10.7326/M24-0571. Epub 2024 Oct 1 [PubMed PMID: 39348705]
Goobie SM, Gallagher T, Gross I, Shander A. Society for the advancement of blood management administrative and clinical standards for patient blood management programs. 4th edition (pediatric version). Paediatric anaesthesia. 2019 Mar:29(3):231-236. doi: 10.1111/pan.13574. Epub [PubMed PMID: 30609198]
Ring L, Landau R. Postpartum hemorrhage: Anesthesia management. Seminars in perinatology. 2019 Feb:43(1):35-43. doi: 10.1053/j.semperi.2018.11.007. Epub 2018 Nov 14 [PubMed PMID: 30578145]
Laurén E, Vikatmaa L, Kerkelä E, Kivipuro T, Krusius T, Syrjälä M, Ihalainen J, Pettilä V. Red blood cell transfusion in southern Finland from 2011 to 2016: a quality audit. Transfusion medicine (Oxford, England). 2019 Feb:29(1):41-47. doi: 10.1111/tme.12568. Epub 2018 Dec 6 [PubMed PMID: 30523663]
Level 2 (mid-level) evidenceKoo BN, Kwon MA, Kim SH, Kim JY, Moon YJ, Park SY, Lee EH, Chae MS, Choi SU, Choi JH, Hwang JY. Korean clinical practice guideline for perioperative red blood cell transfusion from Korean Society of Anesthesiologists. Korean journal of anesthesiology. 2019 Apr:72(2):91-118. doi: 10.4097/kja.d.18.00322. Epub 2018 Dec 5 [PubMed PMID: 30513567]
Level 1 (high-level) evidenceCarson JL, Brooks MM, Hébert PC, Goodman SG, Bertolet M, Glynn SA, Chaitman BR, Simon T, Lopes RD, Goldsweig AM, DeFilippis AP, Abbott JD, Potter BJ, Carrier FM, Rao SV, Cooper HA, Ghafghazi S, Fergusson DA, Kostis WJ, Noveck H, Kim S, Tessalee M, Ducrocq G, de Barros E Silva PGM, Triulzi DJ, Alsweiler C, Menegus MA, Neary JD, Uhl L, Strom JB, Fordyce CB, Ferrari E, Silvain J, Wood FO, Daneault B, Polonsky TS, Senaratne M, Puymirat E, Bouleti C, Lattuca B, White HD, Kelsey SF, Steg PG, Alexander JH, MINT Investigators. Restrictive or Liberal Transfusion Strategy in Myocardial Infarction and Anemia. The New England journal of medicine. 2023 Dec 28:389(26):2446-2456. doi: 10.1056/NEJMoa2307983. Epub 2023 Nov 11 [PubMed PMID: 37952133]
Rao SV, Brooks MM, D'Agostino HEA, Steg PG, Simon T, Aronow HD, Goldsweig AM, Malik S, Alsweiler C, Ho KKL, Dehghani P, Caixeta A, Quraishi AR, Robinson S, Traverse JH, Siddiqi O, Fergusson DA, Potter BJ, Schulman-Marcus J, Keating FK, Carson JL, MINT Trial Investigators. Effect of Red Blood Cell Transfusion Strategy on Clinical Outcomes Among Patients With Acute Myocardial Infarction Undergoing Revascularization: A Prespecified Analysis of the MINT Trial. Circulation. Cardiovascular interventions. 2025 May:18(5):e015249. doi: 10.1161/CIRCINTERVENTIONS.125.015249. Epub 2025 Mar 30 [PubMed PMID: 40159118]
Level 2 (mid-level) evidenceDucrocq G, Calvo G, González-Juanatey JR, Durand-Zaleski I, Avendano-Sola C, Puymirat E, Lemesle G, Arnaiz JA, Martínez-Sellés M, Rousseau A, Cachanado M, Vicaut E, Silvain J, Karam C, Danchin N, Simon T, Steg PG, REALITY investigators. Restrictive vs liberal red blood cell transfusion strategies in patients with acute myocardial infarction and anemia: Rationale and design of the REALITY trial. Clinical cardiology. 2021 Feb:44(2):143-150. doi: 10.1002/clc.23453. Epub 2021 Jan 6 [PubMed PMID: 33405291]
Gonzalez-Juanatey JR, Lemesle G, Puymirat E, Ducrocq G, Cachanado M, Arnaiz JA, Martínez-Sellés M, Silvain J, Ariza-Solé A, Ferrari E, Calvo G, Danchin N, Avendano-Solá C, Rousseau A, Vicaut E, Gonzalez-Ferrero T, Steg PG, Simon T, REALITY Investigators. One-Year Major Cardiovascular Events After Restrictive Versus Liberal Blood Transfusion Strategy in Patients With Acute Myocardial Infarction and Anemia: The REALITY Randomized Trial. Circulation. 2022 Feb 8:145(6):486-488. doi: 10.1161/CIRCULATIONAHA.121.057909. Epub 2022 Feb 7 [PubMed PMID: 35130052]
Level 1 (high-level) evidenceHayakawa M, Tagami T, Kudo D, Ono K, Aoki M, Endo A, Yumoto T, Matsumura Y, Irino S, Sekine K, Ushio N, Ogura T, Nachi S, Irie Y, Hayakawa K, Ito Y, Okishio Y, Muronoi T, Kosaki Y, Ito K, Nakatsutsumi K, Kondo Y, Ueda T, Fukuma H, Saisaka Y, Tominaga N, Kurita T, Nakayama F, Shibata T, Kushimoto S. The Restrictive Red Blood Cell Transfusion Strategy for Critically Injured Patients (RESTRIC) trial: a cluster-randomized, crossover, non-inferiority multicenter trial of restrictive transfusion in trauma. Journal of intensive care. 2023 Jul 24:11(1):34. doi: 10.1186/s40560-023-00682-3. Epub 2023 Jul 24 [PubMed PMID: 37488591]
Level 1 (high-level) evidenceSzczepiorkowski ZM, Dunbar NM. Transfusion guidelines: when to transfuse. Hematology. American Society of Hematology. Education Program. 2013:2013():638-44. doi: 10.1182/asheducation-2013.1.638. Epub [PubMed PMID: 24319244]
Carson JL, Triulzi DJ, Ness PM. Indications for and Adverse Effects of Red-Cell Transfusion. The New England journal of medicine. 2017 Sep 28:377(13):1261-1272. doi: 10.1056/NEJMra1612789. Epub [PubMed PMID: 28953438]
Saviano A, Perotti C, Zanza C, Longhitano Y, Ojetti V, Franceschi F, Bellou A, Piccioni A, Jannelli E, Ceresa IF, Savioli G. Blood Transfusion for Major Trauma in Emergency Department. Diagnostics (Basel, Switzerland). 2024 Mar 27:14(7):. doi: 10.3390/diagnostics14070708. Epub 2024 Mar 27 [PubMed PMID: 38611621]
American Society of Anesthesiologists Task Force on Perioperative Blood Management. Practice guidelines for perioperative blood management: an updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Management*. Anesthesiology. 2015 Feb:122(2):241-75. doi: 10.1097/ALN.0000000000000463. Epub [PubMed PMID: 25545654]
Level 1 (high-level) evidenceRangrass G. Whole blood use in trauma resuscitation: targeting prehospital transfusion. Current opinion in anaesthesiology. 2022 Apr 1:35(2):146-149. doi: 10.1097/ACO.0000000000001099. Epub [PubMed PMID: 35102044]
Level 3 (low-level) evidenceShah A, Stanworth SJ, McKechnie S. Evidence and triggers for the transfusion of blood and blood products. Anaesthesia. 2015 Jan:70 Suppl 1():10-9, e3-5. doi: 10.1111/anae.12893. Epub [PubMed PMID: 25440390]
Pybus S, MacCormac A, Houghton A, Martlew V, Thachil J. Inappropriateness of fresh frozen plasma for abnormal coagulation tests. The journal of the Royal College of Physicians of Edinburgh. 2012:42(4):294-300. doi: 10.4997/JRCPE.2012.403. Epub [PubMed PMID: 23240113]
Level 2 (mid-level) evidenceMüller MC, Arbous MS, Spoelstra-de Man AM, Vink R, Karakus A, Straat M, Binnekade JM, de Jonge E, Vroom MB, Juffermans NP. Transfusion of fresh-frozen plasma in critically ill patients with a coagulopathy before invasive procedures: a randomized clinical trial (CME). Transfusion. 2015 Jan:55(1):26-35; quiz 25. doi: 10.1111/trf.12750. Epub 2014 Jun 9 [PubMed PMID: 24912653]
Level 1 (high-level) evidenceTran HA, Chunilal SD, Tran H. An update of consensus guidelines for warfarin reversal. The Medical journal of Australia. 2014 Feb 3:200(2):82 [PubMed PMID: 24484098]
Level 3 (low-level) evidenceZeller MP, Al-Habsi KS, Heddle NM. Prophylactic platelet transfusions: should they be a treatment of the past? Current opinion in hematology. 2014 Nov:21(6):521-7. doi: 10.1097/MOH.0000000000000087. Epub [PubMed PMID: 25203535]
Level 3 (low-level) evidenceSquires JE. Indications for platelet transfusion in patients with thrombocytopenia. Blood transfusion = Trasfusione del sangue. 2015 Apr:13(2):221-6. doi: 10.2450/2014.0105-14. Epub 2014 Oct 23 [PubMed PMID: 25369586]
Lloyd TD, Geneen LJ, Bernhardt K, McClune W, Fernquest SJ, Brown T, Dorée C, Brunskill SJ, Murphy MF, Palmer AJ. Cell salvage for minimising perioperative allogeneic blood transfusion in adults undergoing elective surgery. The Cochrane database of systematic reviews. 2023 Sep 8:9(9):CD001888. doi: 10.1002/14651858.CD001888.pub5. Epub 2023 Sep 8 [PubMed PMID: 37681564]
Level 1 (high-level) evidenceConti A, Capasso E, Casella C, Fedeli P, Salzano FA, Policino F, Terracciano L, Delbon P. Blood Transfusion in Children: The Refusal of Jehovah's Witness Parents'. Open medicine (Warsaw, Poland). 2018:13():101-104. doi: 10.1515/med-2018-0016. Epub 2018 Apr 5 [PubMed PMID: 29666843]
Level 3 (low-level) evidenceBoulton F, Roberts DJ. Blood transfusion at the time of the First World War--practice and promise at the birth of transfusion medicine. Transfusion medicine (Oxford, England). 2014 Dec:24(6):325-34. doi: 10.1111/tme.12171. Epub [PubMed PMID: 25586955]
Friedman M, Arja W, Batra R, Daniel S, Hoehn D, Paniz AM, Selegean S, Slova D, Srivastava S, Vergara N. Informed consent for blood transfusion: what do medicine residents tell? What do patients understand? American journal of clinical pathology. 2012 Oct:138(4):559-65 [PubMed PMID: 23010711]
Kamyszek RW, Leraas HJ, Reed C, Ray CM, Nag UP, Poisson JL, Tracy ET. Massive transfusion in the pediatric population: A systematic review and summary of best-evidence practice strategies. The journal of trauma and acute care surgery. 2019 Apr:86(4):744-754. doi: 10.1097/TA.0000000000002188. Epub [PubMed PMID: 30629007]
Level 1 (high-level) evidenceNissen-Meyer LSH, Seghatchian J. Donor health assessment - When is blood donation safe? Transfusion and apheresis science : official journal of the World Apheresis Association : official journal of the European Society for Haemapheresis. 2019 Feb:58(1):113-116. doi: 10.1016/j.transci.2018.12.016. Epub 2018 Dec 31 [PubMed PMID: 30630765]
Sihler KC, Napolitano LM. Complications of massive transfusion. Chest. 2010 Jan:137(1):209-20. doi: 10.1378/chest.09-0252. Epub [PubMed PMID: 20051407]
Carson JL, Stanworth SJ, Guyatt G, Valentine S, Dennis J, Bakhtary S, Cohn CS, Dubon A, Grossman BJ, Gupta GK, Hess AS, Jacobson JL, Kaplan LJ, Lin Y, Metcalf RA, Murphy CH, Pavenski K, Prochaska MT, Raval JS, Salazar E, Saifee NH, Tobian AAR, So-Osman C, Waters J, Wood EM, Zantek ND, Pagano MB. Red Blood Cell Transfusion: 2023 AABB International Guidelines. JAMA. 2023 Nov 21:330(19):1892-1902. doi: 10.1001/jama.2023.12914. Epub [PubMed PMID: 37824153]
Negi G, Gaur DS, Kaur R. Blood transfusion safety: A study of adverse reactions at the blood bank of a tertiary care center. Advanced biomedical research. 2015:4():237. doi: 10.4103/2277-9175.168604. Epub 2015 Oct 29 [PubMed PMID: 26682203]
Jaworski K, Maślanka K, Kosior DA. Transfusion-related acute lung injury: a dangerous and underdiagnosed noncardiogenic pulmonary edema. Cardiology journal. 2013:20(4):337-44. doi: 10.5603/CJ.2013.0091. Epub [PubMed PMID: 23913451]
Sahu S, Hemlata, Verma A. Adverse events related to blood transfusion. Indian journal of anaesthesia. 2014 Sep:58(5):543-51. doi: 10.4103/0019-5049.144650. Epub [PubMed PMID: 25535415]
Tung JP, Fraser JF, Nataatmadja M, Colebourne KI, Barnett AG, Glenister KM, Zhou AY, Wood P, Silliman CC, Fung YL. Age of blood and recipient factors determine the severity of transfusion-related acute lung injury (TRALI). Critical care (London, England). 2012 Feb 1:16(1):R19. doi: 10.1186/cc11178. Epub 2012 Feb 1 [PubMed PMID: 22297161]
Level 3 (low-level) evidenceSimmonds P. The origin of hepatitis C virus. Current topics in microbiology and immunology. 2013:369():1-15. doi: 10.1007/978-3-642-27340-7_1. Epub [PubMed PMID: 23463195]
Level 3 (low-level) evidenceDiFrancesco NR, Gaffney TP, Lashley JL, Hickerson KA. Hypocalcemia and Massive Blood Transfusions: A Pilot Study in a Level I Trauma Center. Journal of trauma nursing : the official journal of the Society of Trauma Nurses. 2019 Jul/Aug:26(4):186-192. doi: 10.1097/JTN.0000000000000447. Epub [PubMed PMID: 31283747]
Level 3 (low-level) evidenceRaza S, Ali Baig M, Chang C, Dabas R, Akhtar M, Khan A, Nemani K, Alani R, Majumder O, Gazizova N, Biswas S, Patel P, Al-Hilli JA, Shad Y, Berger BJ, Zaman M. A prospective study on red blood cell transfusion related hyperkalemia in critically ill patients. Journal of clinical medicine research. 2015 Jun:7(6):417-21. doi: 10.14740/jocmr2123w. Epub 2015 Apr 8 [PubMed PMID: 25883703]