Introduction
Blood pressure is a fundamental vital sign that guides acute and long-term clinical decision-making. Given its central role in directing care, accurate, consistent measurement of blood pressure is essential. Two primary values are recorded during blood pressure assessment. Systolic blood pressure (SBP) reflects the peak arterial pressure during ventricular systole, while diastolic blood pressure (DBP) represents the lowest arterial pressure during ventricular diastole. A third parameter, mean arterial pressure (MAP), can be derived from SBP and DBP and approximates the average arterial pressure throughout the cardiac cycle. Blood pressure is calculated using the following formula:
- MAP = (SBP + 2 x DBP) / 3
Indications
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Indications
Blood pressure measurement is essential for detecting hemodynamic instability and assessing cardiovascular risk; it guides both acute management and long-term treatment decisions across clinical settings. Indications for measuring blood pressure include the following:
Contraindications
Although blood pressure measurement is a routine and generally safe procedure, certain clinical situations warrant caution or avoidance. Recognizing contraindications helps prevent patient harm and ensures accurate, reliable readings. Contraindications to cuff-based blood pressure measurement on a specific limb may be classified as relative or absolute. These conditions should be carefully evaluated before selecting the arm for measurement. When present, an alternative limb or measurement site should be used to minimize the risk of complications and ensure accurate results.
- Relative contraindications
- Lymphedema
- Paresis or paralysis [3]
- Presence of arterial or venous lines (eg, indwelling venous catheters)
- Absolute contraindications
- Dialysis arteriovenous fistula or shunt
- Recent surgical wounds
- History of mastectomy on the affected side
Equipment
Accurate blood pressure measurement requires appropriate, well-maintained equipment. Selecting the correct device and cuff size is essential to ensure reliable readings and optimal patient care.
Manual Auscultation
The auscultatory method using Korotkoff sounds remains a standard technique for measuring blood pressure.[4] This method utilizes a sphygmomanometer with an inflatable cuff and pressure gauge, typically a mercury column. The cuff is inflated around the upper arm to a pressure above the systolic level, temporarily occluding the arterial flow and eliminating brachial artery sounds until gradual deflation begins.
The cuff is gradually deflated while auscultation is performed over the brachial artery. When cuff pressure falls to the systolic level, pulsatile blood flow resumes, producing characteristic tapping sounds known as Korotkoff sounds. As pressure decreases to the diastolic level, blood flow becomes laminar, and the sound disappears. The onset of Korotkoff sounds corresponds to systolic pressure, and their disappearance indicates diastolic pressure.[5][6]
The Korotkoff sounds heard during blood pressure measurement are classified into 5 phases:
- Phase 1: A faint, clear tapping sound gradually increases in intensity
- Phase 2: A softer, blowing, or swishing sound as the tapping quality diminishes
- Phase 3: The return of sharper sounds, though less intense than in phase 1
- Phase 4: A distinct muffling of sounds that become soft and blowing
- Phase 5: Complete disappearance of sounds
Medical professionals should be aware of the auscultatory gap, which may lead to underestimating systolic pressure or premature recording of diastolic pressure. In some patients, particularly those with wide pulse pressure, Korotkoff sounds can temporarily fade and then reappear as the cuff continues to deflate. To avoid this error, auscultation over the brachial artery should continue despite a transient loss of sound. The diastolic pressure should be recorded only at the final disappearance of Korotkoff sounds.[5]
Automated Devices
Automated devices may also be used to measure blood pressure. Instead of detecting Korotkoff sounds, these devices analyze oscillations in arterial wall motion during cuff deflation. Device-specific algorithms are then used to indirectly calculate systolic and diastolic blood pressure. An advantage of automated devices is their ease of use, which makes them suitable for patients and laypeople in nonclinical settings.
Automated Office Blood Pressure
A common challenge in blood pressure measurement is transient elevation or suppression of readings in the presence of a healthcare professional, known as white-coat hypertension or masked hypertension. To address this, automated devices may be used to obtain measurements without direct clinician involvement. Automated office blood pressure monitoring records multiple readings over several minutes while the patient rests alone. This approach yields values that more closely reflect ambulatory awake blood pressure and reduces the impact of white-coat effects.[7]
Invasive Monitoring
The most accurate method of measuring blood pressure is invasive arterial monitoring, in which a catheter is placed directly into the lumen of an artery.[8] This technique allows continuous, beat-to-beat measurement of blood pressure. However, due to its invasive nature and associated risks, it is generally reserved for operative and critical care settings. Therefore, this review focuses on noninvasive methods for measuring blood pressure.
Personnel
Any healthcare provider or caregiver trained to measure blood pressure can perform this examination. Proper training in technique, cuff selection, and patient positioning is essential to ensure accurate and reproducible measurements. Ongoing competency assessment further helps minimize measurement error and improve clinical decision-making.
Preparation
Proper preparation is essential to ensure accurate and reliable blood pressure measurement. Attention to patient positioning, environmental factors, and equipment selection helps minimize measurement error and variability.
The following preparatory steps are recommended before measuring blood pressure:
- Explain the procedure and obtain informed consent.
- Reassure the patient to reduce anxiety and prevent inaccurate readings.
- Select the appropriate cuff size; improper sizing can distort results. Many guidelines recommend using a larger cuff when in doubt.
- Ensure the patient is seated comfortably at rest, with back supported and both feet flat on the floor.
Technique or Treatment
Blood pressure is highly labile, and even minor activities can significantly alter readings. Therefore, clinicians must ensure proper patient and environmental preparation before cuff inflation, regardless of whether a manual or automated method is used. First, ask the patient about recent caffeine intake, exercise, or smoking. If any of these occurred within the past 30 minutes, delay measurement until at least 30 minutes have elapsed. The patient should then empty their bladder and be seated in a quiet room with back support, feet flat on the floor, and legs uncrossed. This position should be maintained for at least 5 minutes before measurement.
At this point, a properly sized cuff should be placed directly on the patient’s bare upper arm, with no clothing beneath it and without constricting rolled sleeves above it. The arm should be supported so that the midpoint of the cuff is at the level of the right atrium. Measurement may then begin, ensuring the patient remains still and does not speak during the reading.
Automated devices vary considerably; therefore, users should follow the manufacturer’s instructions for cuff inflation and measurement. For manual measurement, place the stethoscope bell or diaphragm over the medial antecubital fossa at the approximate location of the brachial artery. Inflate the cuff to 30 mm Hg above the level at which the radial pulse disappears, then deflate slowly at a rate of 2 to 3 mm Hg per second. The onset of Korotkoff sounds indicates systolic pressure, and their disappearance marks diastolic pressure.[5][6][9][10] Invasive arterial blood pressure monitoring is the gold standard in intensive care settings; it provides continuous, beat-to-beat measurements that reflect real-time fluctuations in blood pressure.[11]
Complications
The most common source of error in blood pressure measurement is failure to follow proper technique. Results from multiple studies have quantified the effects of common mistakes. Smoking within 30 minutes of measurement can increase systolic blood pressure by up to 20 mm Hg, whereas a distended bladder may raise systolic and diastolic blood pressure by 10 to 15 mm Hg. Sitting without back support or crossing the legs can increase systolic pressure by approximately 10 mm Hg. Placing the cuff over clothing may alter readings by up to 50 mm Hg. Talking or active listening during measurement can increase systolic and diastolic blood pressure by approximately 10 mm Hg.
Improper cuff size and arm positioning also introduce significant error. A cuff that is too large may produce falsely low readings, whereas one that is too small may yield falsely elevated values. Positioning the arm below the level of the right atrium yields higher readings, whereas positioning it above heart level yields lower values. These wide variations underscore the importance of strict adherence to proper measurement technique.[10]
In addition to modifiable sources of error, unavoidable factors may also affect blood pressure measurement. Study results have demonstrated differences between readings obtained in clinical settings and those recorded in ambulatory environments. Hypertension may be overdiagnosed in patients with white-coat hypertension, in which anxiety related to the clinical setting causes a transient elevation in blood pressure. These individuals are normotensive outside the healthcare environment. Conversely, hypertension may be missed in patients with masked hypertension, who exhibit normal readings in the clinic but elevated pressures at other times of the day. This phenomenon may result from temporary lifestyle changes made before medical appointments.[9]
Clinical Significance
Blood pressure is fundamental to the diagnosis, risk stratification, and management of cardiovascular disease. Accurate assessment directly influences therapeutic decisions and long-term patient outcomes.
Hypertension
When clinically feasible, 3 or more blood pressure measurements obtained at separate visits should be used to diagnose hypertension. Diagnostic thresholds continue to evolve as new evidence emerges. Earlier guidelines defined hypertension as blood pressure greater than 140/90 mm Hg; however, more recent recommendations have lowered this threshold to reflect the benefits of earlier intervention.[9] Current classification criteria are summarized in the table (see Image. Stages of Hypertension).
Undiagnosed hypertension significantly increases the risk of coronary artery disease, stroke, end-stage renal disease, and other major complications. In the United States, hypertension is the second leading preventable cause of death, and globally, it remains the leading contributor to mortality and disability-adjusted life years.[12][13] Therefore, timely and accurate diagnosis is critical for initiating treatment and reducing the burden of these adverse outcomes.
Hypotension
Hypotension is less common than hypertension and is typically attributable to an identifiable cause, such as dehydration, acute illness, or medication effects. Although there is no universal diagnostic threshold, clinicians often define hypotension as a systolic blood pressure of less than 90 mm Hg or a diastolic blood pressure of less than 60 mm Hg.[14][15] In practice, diagnosis is guided primarily by clinical context and associated symptoms, including light-headedness, dizziness, blurred vision, nausea, and weakness.
Orthostatic Hypotension
Some patients are normotensive at rest but develop symptoms upon standing. Orthostatic hypotension is defined as a decrease in systolic blood pressure of 20 mm Hg or a reduction in diastolic blood pressure of 10 mm Hg within 3 minutes of standing from a seated or supine position.[9]
Enhancing Healthcare Team Outcomes
All healthcare professionals who measure blood pressure must understand the clinical significance of the values obtained. Familiarity with current guidelines and appropriate treatment thresholds is essential for timely and effective management.[15][16] Blood pressure measurement is a fundamental skill expected of clinicians, nurses, chiropractors, and other allied health professionals.
Media
(Click Image to Enlarge)
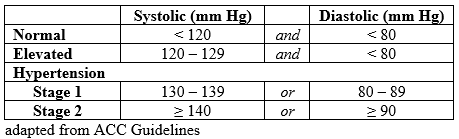
Stages of Hypertension. The stages of hypertension according to the 2017 ACC/AHA guidelines.
Contributed by S Rehman, MD
References
O'Brien E, Dolan E. Ambulatory Blood Pressure Monitoring for the Effective Management of Antihypertensive Drug Treatment. Clinical therapeutics. 2016 Oct:38(10):2142-2151. doi: 10.1016/j.clinthera.2016.08.006. Epub 2016 Sep 13 [PubMed PMID: 27615192]
Kjeldsen SE. Hypertension and cardiovascular risk: General aspects. Pharmacological research. 2018 Mar:129():95-99. doi: 10.1016/j.phrs.2017.11.003. Epub 2017 Nov 7 [PubMed PMID: 29127059]
Kallioinen N, Hill A, Horswill MS, Ward HE, Watson MO. Sources of inaccuracy in the measurement of adult patients' resting blood pressure in clinical settings: a systematic review. Journal of hypertension. 2017 Mar:35(3):421-441. doi: 10.1097/HJH.0000000000001197. Epub [PubMed PMID: 27977471]
Level 1 (high-level) evidenceVischer AS, Burkard T. Principles of Blood Pressure Measurement - Current Techniques, Office vs Ambulatory Blood Pressure Measurement. Advances in experimental medicine and biology. 2017:956():85-96. doi: 10.1007/5584_2016_49. Epub [PubMed PMID: 27417699]
Level 3 (low-level) evidencePickering TG, Hall JE, Appel LJ, Falkner BE, Graves J, Hill MN, Jones DW, Kurtz T, Sheps SG, Roccella EJ. Recommendations for blood pressure measurement in humans and experimental animals: part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Circulation. 2005 Feb 8:111(5):697-716 [PubMed PMID: 15699287]
Level 3 (low-level) evidenceDieterle T. Blood pressure measurement--an overview. Swiss medical weekly. 2012:142():w13517. doi: 10.4414/smw.2012.13517. Epub 2012 Jan 27 [PubMed PMID: 22287317]
Level 3 (low-level) evidenceArmstrong D, Matangi M, Brouillard D, Myers MG. Automated office blood pressure - being alone and not location is what matters most. Blood pressure monitoring. 2015 Aug:20(4):204-8. doi: 10.1097/MBP.0000000000000133. Epub [PubMed PMID: 26154710]
Petersen NH, Ortega-Gutierrez S, Reccius A, Masurkar A, Huang A, Marshall RS. Comparison of non-invasive and invasive arterial blood pressure measurement for assessment of dynamic cerebral autoregulation. Neurocritical care. 2014 Feb:20(1):60-8. doi: 10.1007/s12028-013-9949-4. Epub [PubMed PMID: 24452959]
Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr, Williamson JD, Wright JT Jr. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Journal of the American College of Cardiology. 2018 May 15:71(19):e127-e248. doi: 10.1016/j.jacc.2017.11.006. Epub 2017 Nov 13 [PubMed PMID: 29146535]
Level 1 (high-level) evidenceHandler J. The importance of accurate blood pressure measurement. The Permanente journal. 2009 Summer:13(3):51-4 [PubMed PMID: 20740091]
Pittman JA, Ping JS, Mark JB. Arterial and central venous pressure monitoring. International anesthesiology clinics. 2004 Winter:42(1):13-30 [PubMed PMID: 14716195]
Wang KM, Sirich TL, Chang TI. Timing of blood pressure medications and intradialytic hypotension. Seminars in dialysis. 2019 May:32(3):201-204. doi: 10.1111/sdi.12777. Epub 2019 Mar 5 [PubMed PMID: 30836447]
Mühlbauer V, Dallmeier D, Brefka S, Bollig C, Voigt-Radloff S, Denkinger M. The Pharmacological Treatment of Arterial Hypertension in Frail, Older Patients—a Systematic Review. Deutsches Arzteblatt international. 2019 Jan 18:116(3):23-30. doi: 10.3238/arztebl.2019.0023. Epub [PubMed PMID: 30832759]
Leal J, Morrow LM, Khurshid W, Pagano E, Feenstra T. Decision models of prediabetes populations: A systematic review. Diabetes, obesity & metabolism. 2019 Jul:21(7):1558-1569. doi: 10.1111/dom.13684. Epub 2019 Apr 1 [PubMed PMID: 30828927]
Level 1 (high-level) evidencePhelps PK, Kelley EF, Walla DM, Ross JK, Simmons JJ, Bulock EK, Ayres A, Akre MK, Sprissler R, Olson TP, Snyder EM. Relationship between a Weighted Multi-Gene Algorithm and Blood Pressure Control in Hypertension. Journal of clinical medicine. 2019 Feb 28:8(3):. doi: 10.3390/jcm8030289. Epub 2019 Feb 28 [PubMed PMID: 30823438]
Di Bonito P, Valerio G, Pacifico L, Chiesa C, Invitti C, Morandi A, Licenziati MR, Manco M, Giudice EMD, Baroni MG, Loche S, Tornese G, Franco F, Maffeis C, de Simone G, CARITALY Study group, on the behalf of the Childhood Obesity Study Group of the Italian Society of Pediatric Endocrinology, Diabetology. Impact of the 2017 Blood Pressure Guidelines by the American Academy of Pediatrics in overweight/obese youth. Journal of hypertension. 2019 Apr:37(4):732-738. doi: 10.1097/HJH.0000000000001954. Epub [PubMed PMID: 30817454]