Introduction
Blastomycosis is a fungal infection most commonly caused by either Blastomyces dermatitidis or Blastomyces gilchristii, which are endemic in soil in the Ohio and Mississippi River valleys, the Great Lakes region (including Canadian provinces bordering the Great Lakes), and the southeastern United States.[1] Blastomycosis is also endemic in much of Africa, some countries in the Middle East, and India.[2] Blastomycosis most commonly presents as either an asymptomatic infection or a pulmonary infection following inhalation of Blastomyces spores (conidia).
An estimated 50% of individuals with blastomycosis have minimal to no symptoms.[2] Of the individuals who develop symptomatic infection, approximately 90% have pulmonary involvement, with a subset also having extrapulmonary infection.[3] Extrapulmonary disease occurs in approximately 25% to 30% of patients after hematogenous dissemination from the lungs, with the skin being the most common site.[3] Disseminated disease and life-threatening infections can occur, particularly in those who are immunocompromised.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Blastomyces is a member of the family Ajellomycetaceae and order Onygenales. B dermatitidis and B gilchristii are the most common causative agents of blastomycosis. Blastomyces helicus (formerly Emmonsia helica) is morphologically distinct from B dermatitidis and B gilchristii and can cause infection in both humans and animals. Blastomyces helicus typically affects immunocompromised individuals, producing severe, frequently fatal systemic infection.[4]
B dermatitidis and B gilchristii are thermally dimorphic fungi and are genetically distinct but morphologically indistinguishable. At 25 °C, the mycelial form grows as a fluffy white mold (see Image. Blastomycosis Culture), whereas at 37 °C, the organism grows as a brown, folded yeast. The fungus can be isolated in the soil, where it forms a mycelium that penetrates the substratum on which it grows.
The fungus reproduces asexually by producing small conidia, 2 to 10 µm in diameter. In infected cells, Blastomyces organisms appear as relatively large, multinucleated, budding yeast cells, measuring 8 to 15 µm in diameter, with thick, refractile cell walls. Reproduction occurs through a single broad-based bud (see Image. Blastomycosis dermatitidis in Lung Tissue).[5]
Epidemiology
Blastomycosis is endemic in the Ohio and Mississippi River valleys in the US, near the Great Lakes, and in the southeastern United States. Both B dermatitidis and B gilchristii are endemic in the midwestern United States and parts of Canada, including Ontario, Quebec, and Manitoba. B dermatitidis is more widespread in North America, whereas B gilchristii is restricted to certain areas in northwestern Ontario, Minnesota, and northern Wisconsin.[6][7] The geographic distribution of Blastomyces species has expanded beyond these traditional regions, in part due to climate change. Cases of blastomycosis have been found in the following: New York,[8] Vermont,[9] Ontario,[10] and Colorado.[11]
Blastomyces species are widely endemic throughout Africa, the Middle East, and India. Results from 1 study identified cases of blastomycosis among individuals in 25 African countries and 5 Middle Eastern countries. Blastomyces percursus is widely endemic in this region, with Blastomyces emzantsi found in South Africa, B dermatitidis in the Democratic Republic of the Congo, and B gilchristii in South Africa and Zimbabwe.[12] B dermatitidis is also endemic in India.[13][14] B helicus, by comparison, has been more commonly isolated in the western United States, including Nebraska, Texas, Colorado, Idaho, Montana, Utah, and California, as well as in Alberta and Saskatchewan in western Canada, although the precise geographic distribution remains unknown.[4]
The annual incidence of blastomycosis is approximately 2 cases per 100,000 population, with rates varying substantially between and within states in the United States. Wisconsin reports the highest incidence of blastomycosis in the United States; however, only 8 states report cases (Arkansas, Colorado, Connecticut, Louisiana, Michigan, Minnesota, Vermont, and Wisconsin).[CDC. Reportable Fungal Diseases by State] Thus, the true incidence of blastomycosis is unknown because cases are frequently underdiagnosed and underreported.
Blastomycosis primarily affects middle-aged adults, with roughly 70% of cases occurring in men. Although cases most commonly occur in White individuals, higher rates have been observed in American Indian or Alaska Native and Asian populations.[15] Risk is highest in the Midwest and Southern United States, and parts of Canada. Occupational and recreational exposure to Blastomyces species appears to be a risk factor for infection, with a high incidence of blastomycosis among individuals who visit rivers and waterways.[16] In 2022 to 2023, a large outbreak of blastomycosis associated with a paper mill in Michigan, United States, resulted in 131 diagnosed cases.[17]
Pathophysiology
Blastomyces species are thermally dimorphic fungi that exist as a mold (mycelium) in the environment and a budding yeast in the host. Blastomycosis occurs following the inhalation of Blastomyces conidia from disturbed soil. After conidia are inhaled, they pass into the lower respiratory tract and are converted from the mycelial form into budding yeast. The conidia can be phagocytosed by bronchopulmonary mononuclear cells and killed by neutrophils and macrophages, resulting in asymptomatic infection.
When Blastomyces converts to the yeast form, the thick cell wall confers resistance to phagocytosis and killing, leading to symptomatic pulmonary infection. In addition, the immunomodulatory glycoprotein Blastomyces adhesin-1 (BAD-1) facilitates binding to macrophages, allowing dissemination through the blood and lymphatics to other areas of the body. The pyogranulomatous inflammatory response is a unique feature of blastomycosis and is characterized by an influx of neutrophils and macrophages, followed by granuloma formation.[18]
Histopathology
Histopathologic changes are characterized by a mixed suppurative and granulomatous tissue response, often featuring prominent pseudoepitheliomatous hyperplasia (see Image. Blastomyces dermatitidis of Skin). Thick-walled yeast with characteristic single, broad-based budding is seen (see Image. Blastomyces dermatitidis). Pyogranulomatous inflammation and microabscesses with neutrophils are commonly seen, particularly in cutaneous and lung tissue.
History and Physical
Because pulmonary involvement is the most common manifestation of blastomycosis, presenting symptoms frequently include pulmonary and systemic infectious symptoms. Results from 1 study of 326 cases of blastomycosis showed that the most common presenting symptom was cough, occurring in 73% of individuals. Other common symptoms included fever (54%) and sputum production (50%). Approximately 40% of individuals experienced chest pain, shortness of breath, and weight loss, and approximately 30% experienced night sweats and chills.[3] An estimated 50% of individuals have minimal to no symptoms.[2]
The incubation period for pulmonary blastomycosis ranges from approximately 3 weeks to 3 months following exposure. In individuals with acute pneumonia, the incubation period typically ranges from 4 to 6 weeks.[19] Differentiating the symptoms of pulmonary blastomycosis from those of viral and bacterial pneumonia can be challenging.
With acute blastomycosis, chest radiography most commonly reveals airspace consolidation, often in the upper lobes and involving more than 1 lobe.[20] Individuals with chronic pulmonary blastomycosis often present with cough, chest pain, and systemic infectious symptoms, including fever, night sweats, and weight loss. Symptoms can be indistinguishable from tuberculosis and other fungal etiologies. On chest radiography, individuals with chronic blastomycosis can have airspace consolidation, similar to acute pulmonary blastomycosis, but more commonly present with mass lesions and cavitation.[19]
Acute respiratory distress syndrome is a rare presentation of pulmonary blastomycosis, occurring in up to 10% of cases. Acute respiratory distress syndrome is associated with a mortality rate of 50% to 90%.[21] In contrast, extrapulmonary infection typically results from hematogenous spread. Cutaneous blastomycosis is the second most common manifestation of blastomycosis, typically presenting as papules that progress to crusted, vegetative plaques, often with central clearing or ulceration. Lymphangitis and lymphadenopathy may also be present.
Osteomyelitis is the second most common extrapulmonary manifestation of blastomycosis, occurring in 25% of extrapulmonary cases.[5] Although osteomyelitis can involve any bone or joint, the lower spine and pelvis are most commonly affected. Individuals often present with soft tissue swelling or a chronically draining sinus. Other findings of extrapulmonary infection can include prostatitis, orchitis, or epididymitis. The central nervous system is involved in 5% to 10% of extrapulmonary cases, including cases of meningitis and intracranial or epidural abscesses.[22]
Evaluation
As with other dimorphic fungi (eg, Coccidioides and Histoplasma), clinicians need a high index of suspicion to diagnose blastomycosis because infection is uncommon compared with many other causes of community-acquired pneumonia (eg, bacteria and viruses), and Blastomyces grows slowly on culture. Although culture is highly specific (approximately 100%), sensitivity is much lower, ranging from 66% to 86%.[23] Blastomycosis should be suspected in individuals with community-acquired pneumonia who live in or have traveled to a Blastomyces-endemic area within the prior 3 years and have:
- Pulmonary symptoms that did not improve with empiric antibiotics
- Skin lesions characteristic of cutaneous blastomycosis
- Clinical findings of extrapulmonary blastomycosis with negative bacterial cultures
- Findings on radiography that are suspicious for malignant neoplasm, mycobacterial infections, or fungal infection
- Granulomas with neutrophilic predominance on histopathology [24]
Additionally, engaging in frequent outdoor recreational activities (eg, fishing, canoeing, or rafting) in areas endemic for Blastomyces or working in occupations that may increase the risk of exposure to Blastomyces (eg, construction work, working in a paper mill, or logging) should also increase the suspicion for blastomycosis in the right clinical setting. Clinicians should send a Blastomyces urine antigen test in addition to specimens for culture (or tissue for histopathology and culture, if applicable), if blastomycosis is suspected. Biopsy and histopathological examination of skin lesions reveal pseudoepitheliomatous hyperplasia with neutrophilic abscesses.
Organisms can be difficult to identify and are often found within histiocytes or abscesses in the dermis. The yeast cells are 8 to 15 µm in diameter, have thick, double-contoured walls, and display broad-based budding. Culture has variable sensitivity, and growth typically takes 2 to 4 weeks, although growth can take up to 6 weeks in some cases.
Clinicians should alert laboratory staff when blastomycosis is suspected so they can take appropriate precautions to protect themselves from exposure and incubate cultures for 6 weeks, which is longer than many laboratories typically incubate fungal cultures. Molecular testing (eg, polymerase chain reaction) is increasingly used to diagnose blastomycosis, although, as with polymerase chain reaction testing for other pathogens, it is expensive, has variable sensitivity and specificity, and lacks standardization. Serology has low sensitivity for Blastomyces and a high degree of cross-reactivity with other dimorphic fungi (eg, Coccidioides and Histoplasma), so it is not a preferred modality for the diagnosis of blastomycosis.
Treatment / Management
Although mild pulmonary blastomycosis may be self-limiting in immunocompetent individuals,[25] antifungal therapy is recommended for all infected individuals to prevent extrapulmonary dissemination. All individuals with moderate to severe pneumonia, disseminated blastomycosis, and individuals who are immunocompromised should be treated with antifungals.(B3)
Pulmonary Blastomycosis
First-line treatment of mild to moderate pulmonary blastomycosis is oral itraconazole 200 mg 3 times daily for 3 days, followed by 200 mg twice daily for 6 to 12 months. For moderately severe or severe disease, initial treatment with liposomal amphotericin B is recommended, at 3 to 5 mg/kg intravenously daily. If a lipid formulation of amphotericin B is unavailable, amphotericin B deoxycholate 0.7 to 1.0 mg/kg intravenously daily should be used.
Once clinical improvement is noted, individuals can be transitioned to oral itraconazole and should be treated for 6 to 12 months. Therapeutic drug monitoring is recommended after at least 2 weeks of antifungal treatment.[26] Other azoles, such as posaconazole, isavuconazole, voriconazole, and fluconazole, can be used in place of itraconazole, although they are less well-studied for the treatment of blastomycosis.(A1)
Disseminated Extrapulmonary Blastomycosis
For mild to moderate disease, oral itraconazole 200 mg 3 times daily for 3 days, followed by 200 mg twice daily for 6 to 12 months, is recommended. Individuals with osteoarticular blastomycosis should receive at least 12 months of antifungal treatment. For moderately severe and severe disease, initial treatment with liposomal amphotericin B is recommended: 3 to 5 mg/kg intravenously daily for 1 to 2 weeks or until improvement is noted, followed by oral itraconazole 200 mg 3 times daily for 3 days, then 200 mg twice daily for 12 months. If a lipid formulation of amphotericin B is unavailable, amphotericin B deoxycholate 0.7 to 1.0 mg/kg intravenously daily should be used. Therapeutic drug monitoring is recommended after at least 2 weeks of antifungal treatment.[26](A1)
Central Nervous System Blastomycosis
Liposomal amphotericin B at 5 mg/kg intravenously daily for 4 to 6 weeks is recommended, followed by an oral azole. If a lipid formulation of amphotericin B is unavailable, amphotericin B deoxycholate 1.0 mg/kg intravenously daily should be used. Fluconazole 800 mg daily, itraconazole 200 mg 2 or 3 times daily, or voriconazole 200 to 400 mg twice daily for at least 12 months and until resolution of cerebrospinal fluid abnormalities is recommended.[26](A1)
Immunosuppressed Individuals with Blastomycosis
Liposomal amphotericin B at 3 to 5 mg/kg intravenously daily for 1 to 2 weeks or until clinical improvement is recommended, followed by oral itraconazole 200 mg 3 times daily for 3 days, followed by 200 mg twice daily for 12 months. If a lipid formulation of amphotericin B is unavailable, amphotericin B deoxycholate 0.7 to 1.0 mg/kg intravenously daily should be used. Therapeutic drug monitoring is recommended after at least 2 weeks of antifungal treatment. Lifelong suppressive therapy with oral itraconazole 200 mg daily may be required in cases where immunosuppression cannot be reversed.[26](A1)
Blastomycosis in Pregnant Women and Children
During pregnancy, liposomal amphotericin B at 3 to 5 mg/kg intravenously daily is recommended as azoles are contraindicated due to concerns about teratogenicity. If the newborn shows evidence of infection, amphotericin B deoxycholate 1.0 mg/kg intravenously daily is recommended. For children with mild to moderate blastomycosis, oral itraconazole 10 mg/kg daily (maximum dose 400 mg) for 6 to 12 months is recommended. For severe blastomycosis, amphotericin B deoxycholate at 0.7 to 1.0 mg/kg intravenously daily, or liposomal amphotericin B at 3 to 5 mg/kg intravenously daily, is recommended, followed by oral itraconazole at 10 mg/kg daily (maximum dose, 400 mg) for a total of 12 months. Therapeutic drug monitoring is recommended after at least 2 weeks of antifungal treatment.[26](A1)
Differential Diagnosis
The differential diagnosis of blastomycosis includes the following:
Pulmonary
- Bacterial pneumonia
- Other fungal infections (eg, histoplasmosis or coccidioidomycosis)
- Pulmonary tuberculosis
- Lung cancer
- Sarcoidosis
Cutaneous
- Squamous cell carcinoma
- Pyoderma gangrenosum
- Keratoacanthoma
- Other deep fungal infections (eg, sporotrichosis)
- Tuberculosis verrucosa cutis
Extrapulmonary
- Lymphoma
- Bone tumors
- Tuberculous osteomyelitis
Prognosis
Individuals who are immunocompetent generally have a good prognosis, with successful treatment occurring in approximately 80% to 95% of cases.[3][27] Results from 1 large study spanning 20 years (1990–2010) showed that risk factors for poor prognosis included increased age, male sex, individuals living in the South and Midwest United States, American Indian ethnicity, and Black race.[28] Individuals who are immunocompromised have a notably poorer prognosis, with mortality rates of approximately 30%.[29] If acute respiratory distress syndrome occurs, the mortality rate can be much higher, often greater than 50%.[18]
Complications
Complications of blastomycosis include relapse and severe, life-threatening conditions such as acute respiratory distress syndrome. If dissemination occurs, cutaneous lesions, osteomyelitis, prostatitis, and meningitis can occur. Disseminated blastomycosis is associated with longer treatment duration and increased morbidity and mortality.
Deterrence and Patient Education
Individuals who are immunocompromised should be educated about avoiding areas and activities associated with an increased risk of Blastomyces species exposure.
Pearls and Other Issues
Blastomycosis often mimics other causes of community-acquired pneumonia, tuberculosis, or lung cancer, often leading to delayed diagnosis. Infection often follows exposure to moist soil, decaying wood, or waterways (eg, during recreational activities). Recreational exposures may include activities near waterways.
Enhancing Healthcare Team Outcomes
Blastomycosis is a thermally dimorphic fungal infection caused primarily by Blastomyces dermatitidis and Blastomyces gilchristii, endemic to regions surrounding the Ohio and Mississippi River valleys, the Great Lakes, and portions of the southeastern United States. Infection follows inhalation of fungal conidia from disturbed soil, leading most commonly to pulmonary disease that may mimic bacterial pneumonia, tuberculosis, or malignancy. Although many infections are asymptomatic, symptomatic disease may present with cough, fever, weight loss, chest pain, cavitary pulmonary lesions, or extrapulmonary dissemination involving the skin, bone, genitourinary tract, or central nervous system. Diagnosis requires a high index of suspicion and is supported by culture, histopathology demonstrating broad-based budding yeast, antigen testing, and imaging studies. Antifungal therapy is recommended for all patients to prevent dissemination, with itraconazole used for mild to moderate disease and amphotericin B reserved for severe, disseminated, central nervous system, or immunocompromised cases.
The diagnosis and treatment of blastomycosis are complex and best performed with an interprofessional team that includes a microbiologist, primary care clinician, dermatologist (if skin lesions are present), infectious disease expert, and a pulmonologist or critical care specialist for severely ill hospitalized individuals. Pharmacists play a critical role in therapeutic drug monitoring, management of drug interactions, and patient counseling regarding prolonged antifungal regimens and adverse effects. Nurses reinforce adherence, monitor clinical response and toxicity, facilitate communication across care settings, and support follow-up care.
Advanced clinicians and rehabilitation professionals assist with ongoing symptom management, functional recovery, and monitoring for relapse or complications. Shared decision-making, prompt referral for severe or disseminated disease, surveillance for medication toxicity, and coordinated longitudinal follow-up improve patient safety, reduce delayed diagnosis and recurrence, and support systems-based, patient-centered care for individuals with blastomycosis. All individuals with blastomycosis should be treated to avoid dissemination and recurrence. Additionally, individuals who are immunocompromised may have a good prognosis with appropriate treatment, but the treatment duration is prolonged. These individuals can experience increased morbidity and mortality, and if immunosuppression cannot be reversed, they may require lifelong antifungal therapy, requiring long-term monitoring with an infectious disease specialist.
Media
(Click Image to Enlarge)
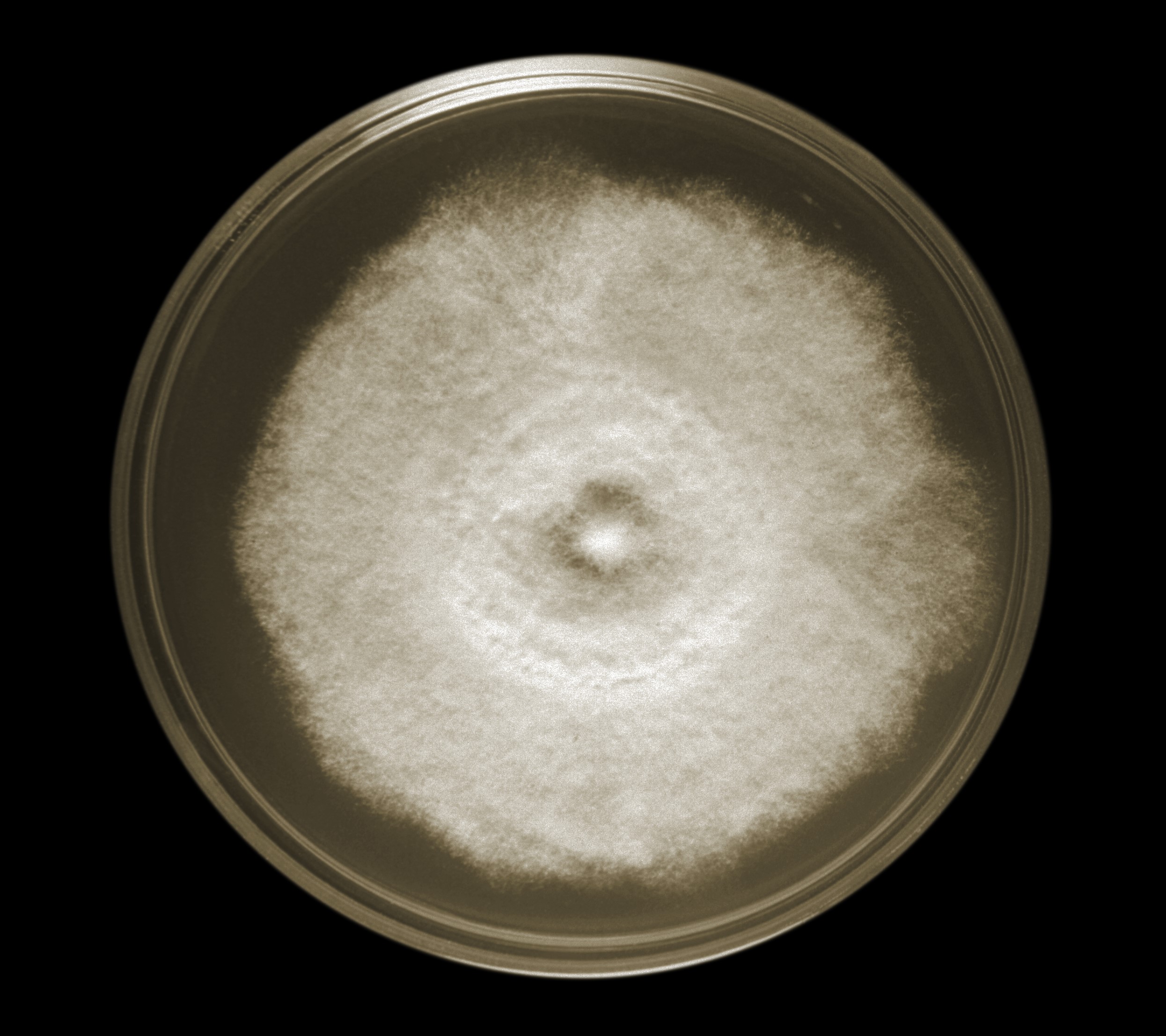
Blastomycosis Culture. Blastomyces dermatitidis strain A-507 and the characteristic woolly-textured, light-colored colony.
RW Menges, Public Domain, Public Health Image Library, Centers for Disease Control and Prevention
(Click Image to Enlarge)
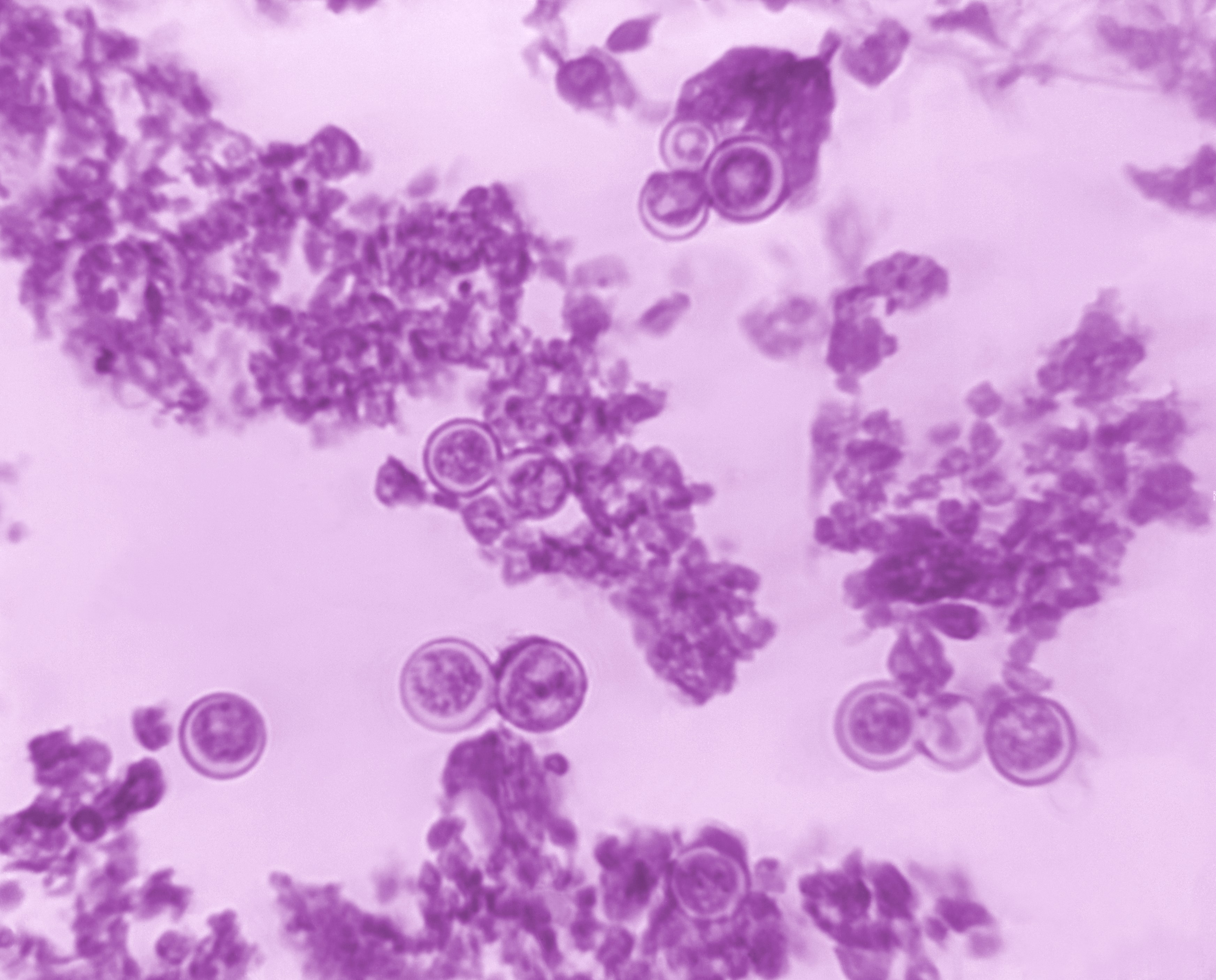
Blastomycosis dermatitidis in Lung Tissue. Photomicrograph of lung tissue at magnification 618× from a patient with blastomycosis, demonstrating thick-walled, round yeast forms and broad-based budding.
Lucille K Georg, MD, Public Domain, Public Health Image Library, Centers for Disease Control and Prevention
(Click Image to Enlarge)
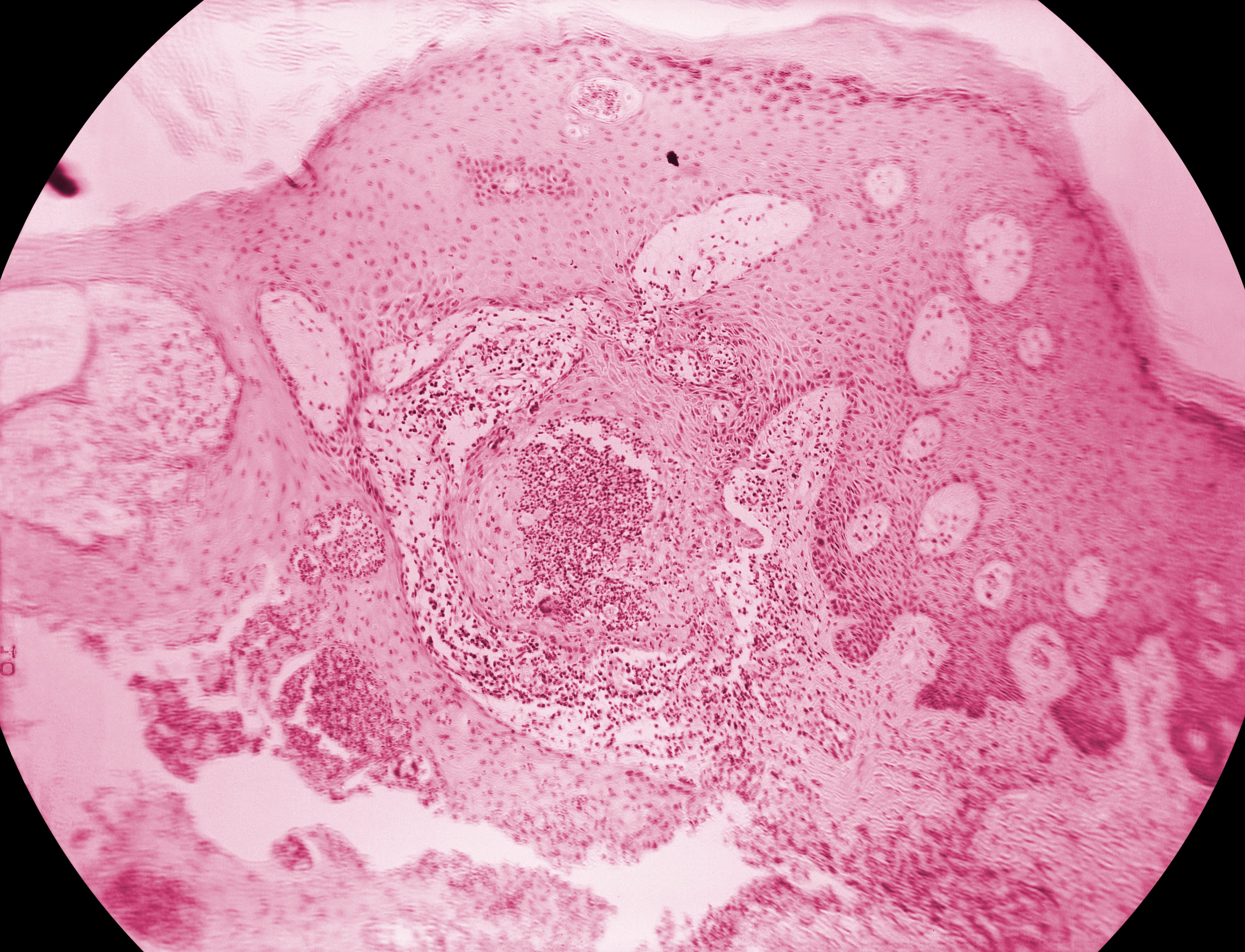
Blastomyces dermatitidis of Skin. Cutaneous tissue demonstrating the histopathological changes typical of North American blastomycosis with characteristic pseudoepitheliomatous hyperplasia and a small developing granulomatous inflammatory nodule at the center.
Libero Ajello, MD, Public Domain, Public Health Image Library, Centers for Disease Control and Prevention
(Click Image to Enlarge)
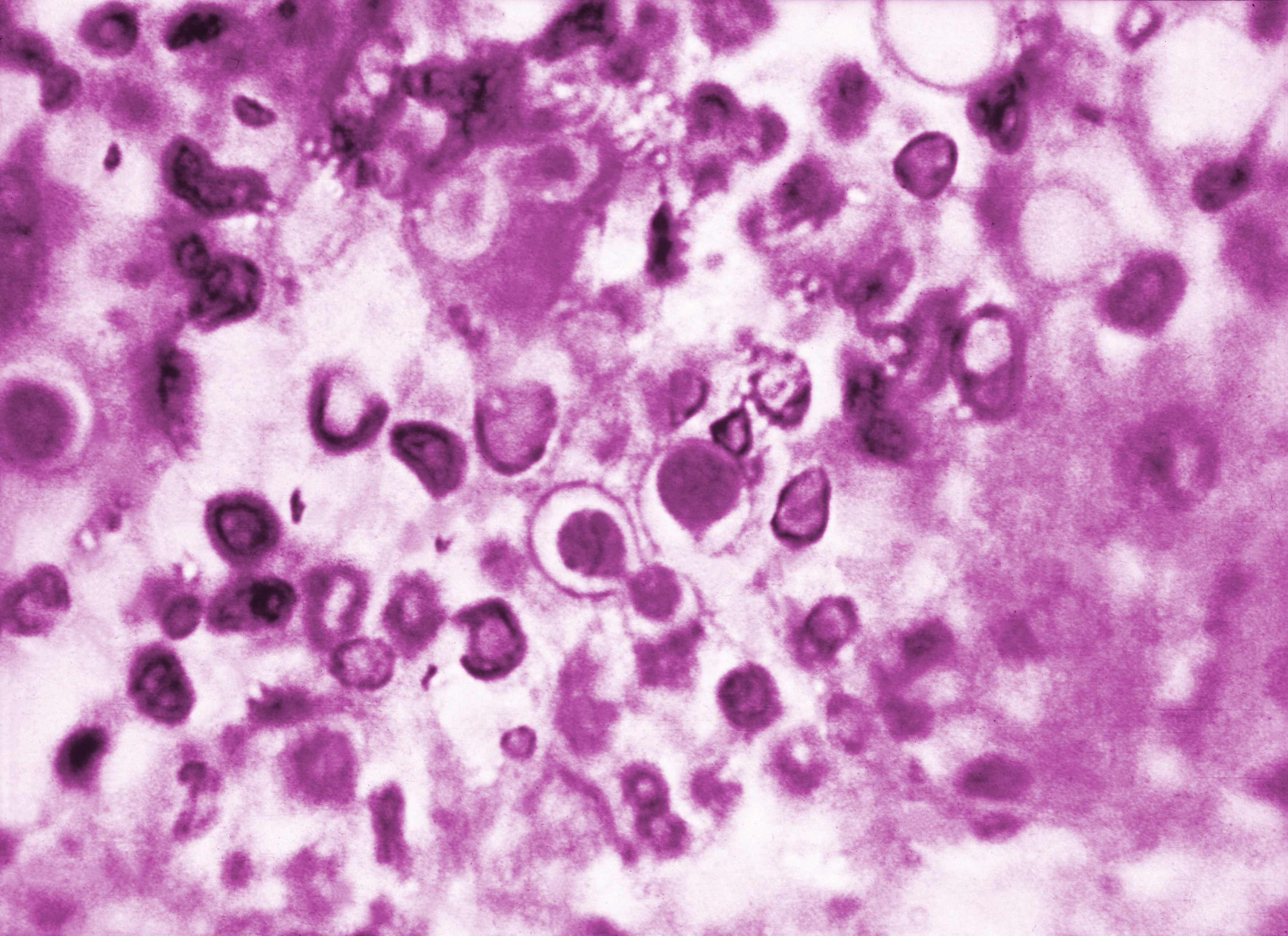
Blastomyces dermatitidis. This photomicrograph demonstrates the histopathologic features of North American blastomycosis, including broad-based budding organisms.
Lucille K Georg, MD, Public Domain, Public Health Image Library, Centers for Disease Control and Prevention
References
Smith JA, Riddell J 4th, Kauffman CA. Cutaneous manifestations of endemic mycoses. Current infectious disease reports. 2013 Oct:15(5):440-9. doi: 10.1007/s11908-013-0352-2. Epub [PubMed PMID: 23917880]
Pullen MF, Alpern JD, Bahr NC. Blastomycosis-Some Progress but Still Much to Learn. Journal of fungi (Basel, Switzerland). 2022 Aug 7:8(8):. doi: 10.3390/jof8080824. Epub 2022 Aug 7 [PubMed PMID: 36012812]
Chapman SW, Lin AC, Hendricks KA, Nolan RL, Currier MM, Morris KR, Turner HR. Endemic blastomycosis in Mississippi: epidemiological and clinical studies. Seminars in respiratory infections. 1997 Sep:12(3):219-28 [PubMed PMID: 9313293]
Level 2 (mid-level) evidenceSchwartz IS, Wiederhold NP, Hanson KE, Patterson TF, Sigler L. Blastomyces helicus, a New Dimorphic Fungus Causing Fatal Pulmonary and Systemic Disease in Humans and Animals in Western Canada and the United States. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2019 Jan 7:68(2):188-195. doi: 10.1093/cid/ciy483. Epub [PubMed PMID: 29878145]
Level 3 (low-level) evidenceSaccente M, Woods GL. Clinical and laboratory update on blastomycosis. Clinical microbiology reviews. 2010 Apr:23(2):367-81. doi: 10.1128/CMR.00056-09. Epub [PubMed PMID: 20375357]
Brown EM, McTaggart LR, Zhang SX, Low DE, Stevens DA, Richardson SE. Phylogenetic analysis reveals a cryptic species Blastomyces gilchristii, sp. nov. within the human pathogenic fungus Blastomyces dermatitidis. PloS one. 2013:8(3):e59237. doi: 10.1371/journal.pone.0059237. Epub 2013 Mar 22 [PubMed PMID: 23533607]
McTaggart LR, Brown EM, Richardson SE. Phylogeographic Analysis of Blastomyces dermatitidis and Blastomyces gilchristii Reveals an Association with North American Freshwater Drainage Basins. PloS one. 2016:11(7):e0159396. doi: 10.1371/journal.pone.0159396. Epub 2016 Jul 18 [PubMed PMID: 27428521]
Ramirez LE, Kostowniak C, Kumar J, Chaturvedi S, Ramani A, Chopra A. Emerging Endemic Area for Blastomycosis, New York, USA, 2000-2024. Emerging infectious diseases. 2026 Mar:32(3):414-418. doi: 10.3201/eid3203.251306. Epub [PubMed PMID: 41863539]
Borah BF, Meddaugh P, Fialkowski V, Kwit N. Using Insurance Claims Data to Estimate Blastomycosis Incidence, Vermont, USA, 2011-2020. Emerging infectious diseases. 2024 Feb:30(2):372-375. doi: 10.3201/eid3002.230825. Epub [PubMed PMID: 38270123]
Brown EM, McTaggart LR, Dunn D, Pszczolko E, Tsui KG, Morris SK, Stephens D, Kus JV, Richardson SE. Epidemiology and Geographic Distribution of Blastomycosis, Histoplasmosis, and Coccidioidomycosis, Ontario, Canada, 1990-2015. Emerging infectious diseases. 2018 Jul:24(7):1257-1266. doi: 10.3201/eid2407.172063. Epub [PubMed PMID: 29912691]
Cuddapah GV, Malik MZ, Arremsetty A Jr, Fagelman A. A Case of Blastomyces dermatitidis Diagnosed Following Travel to Colorado: A Case Report and Review of Literature. Cureus. 2023 Sep:15(9):e44733. doi: 10.7759/cureus.44733. Epub 2023 Sep 5 [PubMed PMID: 37692175]
Level 3 (low-level) evidenceSchwartz IS, Muñoz JF, Kenyon CR, Govender NP, McTaggart L, Maphanga TG, Richardson S, Becker P, Cuomo CA, McEwen JG, Sigler L. Blastomycosis in Africa and the Middle East: A Comprehensive Review of Reported Cases and Reanalysis of Historical Isolates Based on Molecular Data. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2021 Oct 5:73(7):e1560-e1569. doi: 10.1093/cid/ciaa1100. Epub [PubMed PMID: 32766820]
Level 3 (low-level) evidenceRandhawa HS, Chowdhary A, Kathuria S, Roy P, Misra DS, Jain S, Chugh TD. Blastomycosis in India: report of an imported case and current status. Medical mycology. 2013 Feb:51(2):185-92. doi: 10.3109/13693786.2012.685960. Epub 2012 May 31 [PubMed PMID: 22646243]
Level 3 (low-level) evidenceChowdhary A, Jofre GI, Singh A, Dagilis AJ, Sepúlveda VE, McClure AT, Matute DR. Autochthonous Blastomyces dermatitidis, India. Emerging infectious diseases. 2024 Dec:30(12):2577-2582. doi: 10.3201/eid3012.240830. Epub [PubMed PMID: 39592392]
Benedict K, Gibbons-Burgener S, Kocharian A, Ireland M, Rothfeldt L, Christophe N, Signs K, Jackson BR. Blastomycosis Surveillance in 5 States, United States, 1987-2018. Emerging infectious diseases. 2021 Apr:27(4):999-1006. doi: 10.3201/eid2704.204078. Epub [PubMed PMID: 33757624]
Jenks JD, Prattes J, Wurster S, Sprute R, Seidel D, Oliverio M, Egger M, Del Rio C, Sati H, Cornely OA, Thompson GR, Kontoyiannis DP, Hoenigl M. Social determinants of health as drivers of fungal disease. EClinicalMedicine. 2023 Dec:66():102325. doi: 10.1016/j.eclinm.2023.102325. Epub 2023 Nov 18 [PubMed PMID: 38053535]
Hennessee I, Palmer S, Reik R, Miles-Jay A, Nawaz MY, Blankenship HM, Kramer R, Hughes A, Snyder M, Yin RL, Litvintseva AP, Parnell LA, Gade L, Chiller T, de Perio MA, Stobierski MG, McFadden J, Toda M, Michigan Blastomycosis Outbreak Investigation Team. Epidemiological and Clinical Features of a Large Blastomycosis Outbreak at a Paper Mill in Michigan. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2025 Feb 24:80(2):356-363. doi: 10.1093/cid/ciae513. Epub [PubMed PMID: 39422247]
Level 2 (mid-level) evidenceMcBride JA, Gauthier GM, Klein BS. Clinical Manifestations and Treatment of Blastomycosis. Clinics in chest medicine. 2017 Sep:38(3):435-449. doi: 10.1016/j.ccm.2017.04.006. Epub 2017 Jun 12 [PubMed PMID: 28797487]
Khadilkar A, Waddell L, Acheson ES, Ogden NH. Perspectives on blastomycosis in Canada in the face of climate change. Canada communicable disease report = Releve des maladies transmissibles au Canada. 2024 Nov:50(11):400-411. doi: 10.14745/ccdr.v50i11a04. Epub 2024 Nov 7 [PubMed PMID: 39525076]
Level 3 (low-level) evidenceSheflin JR, Campbell JA, Thompson GP. Pulmonary blastomycosis: findings on chest radiographs in 63 patients. AJR. American journal of roentgenology. 1990 Jun:154(6):1177-80 [PubMed PMID: 2110723]
Bednarczyk JM, Kethireddy S, White CW, Freed DH, Singal RK, Bell D, Ahmed SZ, Kumar A, Light B. Extracorporeal membrane oxygenation for blastomycosis-related acute respiratory distress syndrome: a case series. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 2015 Jul:62(7):807-15. doi: 10.1007/s12630-015-0378-z. Epub 2015 Apr 8 [PubMed PMID: 25851019]
Level 2 (mid-level) evidenceKazmer A, El-Baba R, Kontosis A, Borys E, Siddiqui M. Blastomycosis of the Central Nervous System. Journal of radiology case reports. 2023 May:17(12):13-21. doi: 10.3941/jrcr.v17i12.5167. Epub 2024 May 31 [PubMed PMID: 38828027]
Level 3 (low-level) evidenceSaravanababu T, Elsayed S, Gupta R, Delport J, Rahimi Shahmirzadi M, AlMutawa F. Diagnosing Blastomycosis: A Review of Laboratory Methods and Clinical Utility. Journal of fungi (Basel, Switzerland). 2025 Aug 12:11(8):. doi: 10.3390/jof11080589. Epub 2025 Aug 12 [PubMed PMID: 40863541]
Smith DJ, Free RJ, Thompson GR 3rd, Baddley JW, Pappas PG, Benedict K, Gold JAW, Endemic Mycoses Diagnostic Algorithm Subject Matter Expert Group, Tushla LA, Chiller T, Jackson BR, Toda M. Clinical Testing Guidance for Coccidioidomycosis, Histoplasmosis, and Blastomycosis in Patients With Community-Acquired Pneumonia for Primary and Urgent Care Providers. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2024 Jun 14:78(6):1559-1563. doi: 10.1093/cid/ciad619. Epub [PubMed PMID: 37802909]
Sarosi GA, Davies SF, Phillips JR. Self-limited blastomycosis: a report of 39 cases. Seminars in respiratory infections. 1986 Mar:1(1):40-4 [PubMed PMID: 3685662]
Level 3 (low-level) evidenceChapman SW, Dismukes WE, Proia LA, Bradsher RW, Pappas PG, Threlkeld MG, Kauffman CA, Infectious Diseases Society of America. Clinical practice guidelines for the management of blastomycosis: 2008 update by the Infectious Diseases Society of America. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2008 Jun 15:46(12):1801-12. doi: 10.1086/588300. Epub [PubMed PMID: 18462107]
Level 1 (high-level) evidenceDismukes WE, Bradsher RW Jr, Cloud GC, Kauffman CA, Chapman SW, George RB, Stevens DA, Girard WM, Saag MS, Bowles-Patton C. Itraconazole therapy for blastomycosis and histoplasmosis. NIAID Mycoses Study Group. The American journal of medicine. 1992 Nov:93(5):489-97 [PubMed PMID: 1332471]
Khuu D, Shafir S, Bristow B, Sorvillo F. Blastomycosis mortality rates, United States, 1990-2010. Emerging infectious diseases. 2014 Nov:20(11):1789-94. doi: 10.3201/eid2011.131175. Epub [PubMed PMID: 25339251]
Pappas PG, Threlkeld MG, Bedsole GD, Cleveland KO, Gelfand MS, Dismukes WE. Blastomycosis in immunocompromised patients. Medicine. 1993 Sep:72(5):311-25 [PubMed PMID: 8412644]