Introduction
Bladder stones are solid calculi that form within the urinary bladder and represent a distinct subset of urolithiasis. These calculi commonly consist of calcium-containing salts, such as calcium oxalate and calcium phosphate, which often originate in the kidneys. However, bladder stones also include noncalcific materials, such as uric acid, cystine, struvite (infection), ammonium acid urate, or various mixed mineral compositions (see Image. A Bladder Calculus).[1][2][3] Bladder stones differ from upper urinary tract calculi in their pathophysiology, clinical presentation, and management considerations.
The incidence of bladder stones is relatively low in industrialized countries but remains higher in resource-limited regions.[4] In adults, bladder stone formation is most often associated with urinary stasis resulting from bladder outlet obstruction, neurogenic bladder dysfunction, chronic infection, bladder augmentation procedures, or foreign bodies such as Foley catheters.[2][3][5][6] In contrast, endemic bladder stones in children from resource-limited regions are more commonly associated with nutritional deficiencies, particularly low–animal-protein diets; dehydration; high dietary oxalate intake; and other nutritional factors.[4][7][8][9][10][11][12][13]
Bladder stones account for approximately 5% of all urinary calculi and most frequently occur in older men with underlying lower urinary tract pathology, such as benign prostatic hyperplasia (BPH) or impaired bladder emptying.[1][2] Although uncommon, bladder stones may also develop in individuals without identifiable anatomic abnormalities or predisposing conditions, especially in children, where dietary factors are the primary underlying cause.[8][13] Although patients with bladder calculi have a higher incidence of nephrolithiasis, the mere presence of upper urinary tract calculi does not, by itself, increase the risk of vesical stone formation, which typically arises from local bladder factors rather than from stone migration from the kidneys.[14] Clinical manifestations range from asymptomatic disease to significant lower urinary tract symptoms, hematuria, suprapubic pain, urinary retention, and recurrent urinary tract infections.[15][16][17] Without identification and correction of underlying etiologic factors, bladder stones are prone to recurrence, underscoring the importance of comprehensive evaluation and targeted management. Please see StatPearls' companion reference, "Ultrasound of the Urinary Tract," for further information.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Most bladder stones in adults form de novo within the bladder (primary or endemic) rather than migrating from the upper urinary tract.[6][18] In developed countries, the main composition of pediatric bladder stones is struvite or calcium oxalate dihydrate.[7][8][19][20][21][22] Although small renal calculi or sloughed papillae may pass into the bladder, stones that remain intravesical typically enlarge by deposition of additional concentric layers, which may differ in composition from the original nidus.[1]
The presence of upper urinary tract calculi alone does not, by itself, increase the risk of bladder stone formation unless associated with bladder dysfunction or outlet obstruction, because most migratory stones are voided out of the bladder. However, adult patients with bladder stones are more likely than the general population to have a history of recurrent urinary tract infections or urolithiasis, a lower average urinary pH, reduced urinary magnesium levels, and higher urinary uric acid supersaturation levels.[6][14][16][23][24] Stones originating from the kidney that are small enough to pass through the ureters can easily leave the bladder and traverse the urethra unless significant bladder dysfunction or outlet obstruction is present. Please see StatPearls' companion reference, "Urolithiasis," for further information.
Several conditions commonly associated with bladder stones are outlined below.
Benign Prostatic Hyperplasia and Urinary Stasis
BPH and urinary stasis are the primary etiologic factors in bladder stone formation in adults and most commonly result from bladder outlet obstruction or impaired bladder emptying.[6] Bladder outlet obstruction, most frequently due to BPH, is the leading risk factor and is implicated in approximately 45% to 80% of bladder stone cases.[14][15][16][17][25] Among men undergoing surgical treatment for BPH, bladder stones are identified in approximately 3% to 4.7% of patients.[26][27]
Renal calculi small enough to pass through the ureters are typically smaller than 1 cm and can be easily voided from the body, especially in women, unless obstruction, bladder dysfunction, or BPH is present. The average adult male urethral diameter is approximately 8 to 9 mm; therefore, calculi of this size or larger are difficult to pass spontaneously.[28] Older men with intravesical extension of the prostate through BPH or enlarged median lobes (intravesical prostatic protrusion) also have greater difficulty passing bladder calculi and are at increased risk for their development.[16][17][29] In such cases, the stones remain in the bladder, where they tend to slowly grow and enlarge by adding concentric layers of lithogenic material around a central nidus.
Bladder Augmentation Surgery and Urinary Diversion
Bladder augmentation surgical procedures and continent urinary diversions are also strongly associated with bladder stone formation. After 10 years, the incidence of bladder stones in these patients is 28% to 36%, and after 20 years, the incidence increases to more than 40%.[30][31][32][33] The rate of recurrent bladder stones is highest during the first 2 years after the surgical procedure, at roughly 12% per year, after which the annual incidence declines.[34] Risk factors include exposed sutures, staples, or mesh that act as foreign bodies (niduses); chronic bacterial colonization; nonadherence to intermittent catheterization and recommended irrigation protocols; urinary alkalinity resulting from urine contacting intestinal mucosal surfaces, which promotes urinary chloride exchange for bicarbonate; significant mucus production from transplanted intestinal segments; incomplete bladder emptying; and prolonged urinary stasis.[30][35][36][37][38][39][40][41][42]
Regular bladder irrigation, performed daily or several times a week with 240 to 300 mL of sterile saline (or 0.25% acetic acid in severely alkaline bladders), significantly reduces the risk of bladder stone formation in these patients.[43][44][45][46][47][48][49] Evidence for the use of mucolytic agents, such as N-acetylcysteine and urea, in prophylaxis is limited, as the cornerstone of preventive therapy for bladder stones in augmented bladders remains regular irrigation and intermittent catheterization.[30][45][49][50][51][52][53][54][55][56][57] In contrast, standard ileal conduit urinary diversions are associated with a substantially lower incidence of bladder stones, typically about 3.5%.[58][59]
Chronic Inflammation
Chronic inflammation (cystitis) from radiation therapy and parasitic infection, such as schistosomiasis, as well as urinary stasis associated with bladder diverticula or sliding inguinal-scrotal-vesical hernias, may also predispose patients to bladder stone formation.[60][61][62][63][64] Women with bladder stones may have a spinal cord injury, neurogenic bladder, bladder diverticula, overly tight incontinence repair surgical procedures, cystoceles, pelvic organ prolapse, suture or staple exposure after pelvic surgical procedures, a ureterocele, or a urethral stricture.[65][66][67][68][69][70][71][72][73][74]
Foreign Bodies
Foreign bodies within the bladder represent another well-established cause of bladder calculi. Any nonabsorbable foreign material that remains intravesical may serve as a nidus for stone formation, including surgical staples, exposed permanent sutures, retained double-J ureteral stents, cable wires, migration of uterine or surgical devices, or fragments of ruptured Foley catheter balloons.[75][76][77][78][79][80][81][82][83] Please see StatPearls' companion reference, "Prevention of Inappropriate Self-Extraction of Foley Catheters," for further information. For this reason, absorbable suture material is always recommended for urinary tract surgical procedures, and all Foley catheters forcibly removed or spontaneously expelled should be carefully inspected to ensure balloon integrity and the absence of any balloon fragments.[84] When retained intravesical fragments are suspected, or the Foley catheter is unavailable for inspection, cystoscopic evaluation of the bladder is required.[81] Please see StatPearls' companion reference, "Cystoscopy," for further information. Chronic indwelling catheters are also a risk factor for bladder stone production, especially if neglected.[85] Rare causes of bladder foreign bodies that can lead to bladder stone formation include erosion of surgical wire used for cerclage, anorectal impalement, erosion of nonabsorbable sutures used in surgical procedures on nearby structures, migration of brachytherapy seeds, items introduced transurethrally by patients themselves, surgical gauze, forgotten double-J ureteral stents, contraceptive devices that have migrated intravesically, prostatic urethral stents, and hair introduced during self-intermittent catheterization.[73][75][76][86][87][88][89][90][91][92][93][94][95][96][97][98][99]
Laxative Abuse
Laxative use is associated with rare ammonium acid urate bladder stones in adults primarily through chronic diarrhea and excessive gastrointestinal tract fluid loss.[100][101] Chronic diarrhea causes significant dehydration, low urinary volume, high serum aldosterone, decreased urinary sodium excretion, and hypokalemia.[100][101] Severe dehydration increases aldosterone levels, leading to increased urinary ammonia production, which combines with urinary uric acid to form insoluble ammonium urate stones, particularly at a urinary pH of 6.2 to 6.3.[100][101] Patients with a history of inflammatory bowel disease and ileostomy diversions are also at higher risk for ammonium acid urate stones due to citrate loss and dehydration due to chronic diarrhea.[101][102]
Neurogenic Bladder Dysfunction
Neurogenic bladder dysfunction is a major risk factor for bladder stone formation, particularly in patients with spinal cord injuries.[103][104] Individuals with neurogenic bladders who require long-term indwelling catheterization are approximately 6 times more likely to develop bladder stones than those who void spontaneously.[105][106][107]
Spinal Cord Injuries
Rates of bladder stone formation in patients with spinal cord injuries range from 10% to over 60%, depending on duration of follow-up and bladder management strategy, with an estimated annual recurrence rate of approximately 16.6%.[103][104] Up to two-thirds of patients with spinal cord injuries and neurogenic bladders develop bladder stones at some point.[107] Bladder stone formation risk is highest in the first 6 months after the initial spinal injury, due to hypercalciuria from bone demineralization from forced immobilization.[103] Frequent encrustation of chronic indwelling catheters is a reasonably good predictor of bladder stone development.[106][108]
Among patients with chronic indwelling catheters, about 36% form bladder stones within 8 years.[106][108] A randomized controlled trial involving 78 patients with spinal cord injuries and permanent suprapubic catheters demonstrated that twice-weekly manual bladder irrigations over 6 months significantly reduced the incidence of bladder stone recurrences (49% vs 0%, P < .0001) and the number of urinary tract infections, as reported in the European Association of Urology 2026 Guidelines.[EAU. Urolithiasis]
Causative factors of bladder stones in patients with spinal cord injuries include immobilization, hypercalciuria, chronic bacterial colonization with persistent or recurrent urinary tract infections, urinary stasis, bladder dysfunction, and the use of permanent catheters.[103][105][109][110][111] Intermittent catheterization is associated with a substantially lower incidence of bladder stones compared with chronic indwelling Foley catheters.[104][105][108] The risk of bladder stone formation in patients with spinal cord injuries and permanent indwelling Foley catheters is 4% annually, but only 0.2% among those who use clean intermittent self-catheterization.[104][105]
Urease-Producing Bacteria
Urease-producing bacteria, including the most common urinary pathogens, except Escherichia coli, alter the urinary chemistry, thereby facilitating the formation of primary bladder stones. The urease produced by these bacteria converts urea into ammonia, which increases urinary pH, allowing the precipitation and growth of insoluble mineral salts, such as calcium phosphate and calcium magnesium ammonium phosphate (struvite).[17][112] Please see StatPearls' companion reference, "Struvite and Triple Phosphate Renal Calculi," for further information. Additional etiologic factors include urethral strictures, bladder diverticula, chronic urinary tract infections, pelvic radiation therapy, long-term indwelling catheters, and parasitic infections such as schistosomiasis, all of which may promote urinary stasis or provide a nidus for stone formation.[104][105][108][113][114] Rarely, viral protease inhibitors such as indinavir may cause noncalcific bladder calculus formation.[115]
In pediatric populations, particularly in resource-limited regions, bladder stone formation is commonly associated with poor diet (low animal protein, low phosphate, high cereal content), insufficient hydration, chronic diarrhea, malnutrition, persistent dehydration, personal hygiene issues, inadequate sanitation measures, recurrent lower urinary tract infections, low socioeconomic status, and limited access to clean drinking water.[4][7][8][9][10][11][116] Endemic bladder calculi in children are most often composed of ammonium acid urate, but may also contain calcium oxalate or calcium phosphate.[117] Low urinary volume is the most frequent laboratory abnormality identified in these children, followed by hypocitraturia.[118][119] Excessive or exclusive reliance on high-carbohydrate foods that replace milk and dairy feedings leads to a dietary phosphate deficiency, which promotes the formation of insoluble urinary salts, predominantly ammonium acid urate.[7] Primary endemic bladder stone development in children typically occurs in the absence of other urinary tract pathology.[8]
Epidemiology
Bladder stones account for approximately 5% of all urinary tract calculi worldwide, yet they account for almost 8% of all urolithiasis-related mortalities.[1][2][120][121] The epidemiology of bladder stone disease varies significantly by age, sex, geographic region, climate, diet, and underlying health conditions. In industrialized nations, the incidence of bladder stones is declining, and bladder stones are relatively uncommon. In contrast, in resource-limited regions, bladder stones remain an important cause of morbidity in pediatric populations.[7][8]
In adults, bladder stones occur most frequently in men older than 50 (up to 80%) and are strongly associated with bladder outlet obstruction, particularly due to BPH.[14][15][16][17][122] Peak age is 60 years, with a pronounced male predominance (male-to-female ratios ranging from 4:1 to 10:1).[123][124] Rare cases of such giant bladder stones have been reported to cause acute renal failure or obstruction of labor in pregnancy.[125][126][127][128][129][130][131][132][133][134][135][136][137][138][139]
In the United States and other developed high-income countries, bladder stones are most commonly identified in older men with lower urinary tract dysfunction, neurogenic bladder, a history of urologic surgical procedures, bladder augmentation, BPH with intravesical prostatic extension, gout, or chronic catheterization.[17][107] In contrast, endemic bladder stones—defined as calculus formation within the bladder in the absence of urinary tract anatomical abnormalities—are more prevalent among children in resource-limited regions, particularly in parts of the Middle East, North Africa, and Southeast Asia, including Indonesia, Myanmar, and Thailand.[4][8][140][141] In these populations, bladder stones often present between the ages of 2 and 5, with a peak at 3 years.[3][8][142] Among children, bladder stones show a very strong prevalence in boys compared with girls, with ratios of 9:1 to 33:1.[7][12] Pediatric bladder stones are now rare in industrialized nations due to improved nutrition and access to health care.
Patients with spinal cord injury and neurogenic bladder represent a high-risk population for bladder stones across all regions. Prevalence rates of bladder stones in individuals with spinal cord injury range from approximately 10% to 66%, depending on duration of follow-up, degree and severity of the neurological injury, and bladder management strategy.[104][108][143] For example, the use of long-term indwelling urinary catheters is associated with a substantially higher incidence of bladder stones compared with intermittent catheterization.[104][108] Overall, the epidemiology of bladder stones demonstrates distinct patterns between developed and resource-limited regions, with adult disease primarily driven by obstructive and neurogenic bladder conditions and pediatric disease largely influenced by nutritional and environmental factors.[117][144]
Pathophysiology
Bladder stone formation results from a combination of urinary stasis, altered urine chemistry, and the presence of a nidus that promotes crystallization and stone growth.[14] Unlike upper urinary tract calculi, which primarily form due to metabolic abnormalities, bladder stones most often arise in the setting of impaired bladder emptying, allowing prolonged urine retention and crystal aggregation. However, a correlation between the chemical composition of renal calculi and bladder stones has been observed in some patients.[1]
Ammonium Urate Stones
Ammonium urate stones are common in children in endemic areas but rare in adults.[117] When found in adult patients, they are associated with laxative abuse, primarily through chronic diarrhea and excessive gastrointestinal fluid loss.[100][101][145] Chronic diarrhea causes significant dehydration, low urinary volume, and hypokalemia.[100][101][145] Severe dehydration increases aldosterone levels, leading to increased urinary ammonia production, which combines with urinary uric acid to form insoluble ammonium urate stones, particularly at a urinary pH of 6.2 to 6.3.[100][101][145] Patients with obesity or a significant history of multiple previous uric acid calculi, recurrent urinary tract infections, inflammatory bowel disease, or ileostomy diversions are also at higher risk for ammonium urate stones.[101][102][145][146]
Calcium-Based Bladder Stones
Calcium-based bladder stones often originate as small renal calculi that pass into the bladder but are not expelled due to BPH, outlet obstruction, bladder neck strictures, or neurogenic (dysfunctional) voiding.[14] Once retained, these calculi undergo progressive concentric deposition of additional stone mineral in a complex pattern of layers over a specific nidus, a process called epitaxy.[147][148][149][150] In contrast to renal stone formation, ongoing urinary stasis plays a significant role in the growth of bladder calculi.[14]
Indwelling Catheters
Indwelling catheters substantially increase the risk of developing bladder stones, approximately 6 times that of individuals without catheters.[104][105][106][108] After catheter or double-J stent insertion, bacteria adhere and begin forming a biofilm. This material covers the exposed parts of the Foley catheter with sheets of microorganisms that produce an extracellular interlocking network composed of bacterial glycocalyces and host proteins.[104][108] Calcium phosphate and calcium-magnesium-ammonium phosphate crystals then become incorporated into this biofilm, forming encrustations.[25][104][108][151]
The process is accelerated by urease-producing organisms, particularly Proteus mirabilis.[108][152][153] Removing or changing the Foley catheter or double-J stent resolves the immediate problem of lumen obstruction but often leaves behind tiny stone fragments in the bladder, dislodged from the external stent or catheter surface, which can serve as a nidus for stone formation and eventually grow into bladder calculi.[78][108][150][154][155][156]
Jackstones
Jackstones are an uncommon subtype of bladder calculi characterized by a distinctive spiculated morphology resembling that of children's jacks.[157] These stones typically contain a proteinaceous core or nidus surrounded by concentric layers of calcium oxalate, usually very hard monohydrate.[158][159][160][161] Their unique structure is thought to result from chronic urinary stasis and repetitive mechanical contact with the bladder wall during contraction, influencing asymmetric crystal deposition.[158][159][160][161]
Struvite Stones
Struvite stones form in the presence of urease-producing bacteria, which hydrolyze urea into ammonia, increasing urinary pH and promoting precipitation of insoluble phosphate-containing salts such as calcium ammonium magnesium phosphate.[108][152][153] Patients with chronic bacteriuria, neurogenic bladder dysfunction, or long-term catheterization are therefore at increased risk for infection-related bladder stones. Please see StatPearls' companion reference, "Struvite and Triple Phosphate Renal Calculi," for further information. Struvite bladder stones can develop in as little as 4 to 6 weeks in alkaline environments.[162]
Uric Acid
Uric acid is a common constituent of bladder stones in adults, comprising over 50% of such calculi, particularly in patients with persistently acidic urine.[163] Surprisingly, most individuals with uric acid bladder stones do not have gout, systemic hyperuricemia, or hyperuricosuria.[163] Instead, the primary chemical etiological factors that promote uric acid precipitation and bladder stone formation include low urinary pH, dehydration, low urine volume, and reduced urinary buffering capacity.[164] Please see StatPearls' companion reference, "Hypocitruria and Renal Calculi," for further information. Uric acid crystals and bladder stones can form and stabilize at otherwise normal urinary concentrations if the urine pH is persistently low.[165] Because uric acid stones are radiolucent, they may go underrecognized without appropriate imaging, such as computed tomography (CT; preferred) or ultrasonography.[166] Confirmation is via cystoscopy. Other stone compositions include calcium oxalate, calcium phosphate, cystine, and magnesium ammonium phosphate (struvite). Please see StatPearls' companion references, "Struvite and Triple Phosphate Renal Calculi," "Renal Calculi, Nephrolithiasis," "Cystinuria," "Uric Acid Nephrolithiasis," and "Urolithiasis," for further information.
Children
In pediatric populations, particularly in resource-limited regions where such calculi are endemic, nutritional deficiencies, chronic dehydration, low dietary phosphorus, low urine pH, and hypocitraturia contribute to alterations in urinary chemistry that promote bladder stone formation.[167] The chemical composition of bladder stones in children differs from that in adults, with ammonium urate calculi being the most common type, followed by calcium oxalate.[8][22] The single most commonly identified abnormal laboratory finding in these patients is low urinary volume.[8][168][169] Additionally, elevated urinary pH, hypocitraturia, and high ammonia levels resulting from low-animal-protein, low-phosphorus diets further promote the formation of ammonium urate bladder stones.[170]
In these patients, hypocitraturia is due to the reduced intake of potassium-rich fruits and vegetables, along with a high intake of cereals, leading to chronic metabolic acidosis.[170] Hypocitraturia is often exacerbated by chronic diarrhea, which causes bicarbonate loss, and persistent dehydration from living in a hot climate.[119] In addition, diets rich in green vegetables may increase urinary oxalate excretion and raise the risk of stone disease.[167] High ammonia production is caused by a low-phosphorus diet and the need to buffer dietary metabolic acidosis without adequate phosphorus.[171][172][173] Ammonia is rapidly converted to ammonium in urine, creating an alkaline environment that promotes the precipitation of calcium, magnesium, and ammonium phosphate.[174] Please see StatPearls' companion reference, "Struvite and Triple Phosphate Renal Calculi," for further information.
Histopathology
Bladder stones are composed of crystalline mineral aggregates organized around an organic matrix that may include proteins, cellular debris, and, in infection-related stones, bacterial components.[175] Microscopic examination of stone fragments, when performed for research or compositional analysis, reveals concentric lamellar architecture indicative of sequential mineral deposition over time.[176] The specific crystalline morphology varies with stone composition, such as uric acid, calcium oxalate, calcium phosphate, or calcium-magnesium-ammonium phosphate.[177]
Histopathologic changes in the adjacent bladder mucosa, when biopsied, commonly show nonspecific chronic inflammatory features. These findings may include urothelial hyperplasia, submucosal edema, lymphocytic infiltration, and reactive epithelial changes resulting from prolonged mechanical irritation and recurrent infection. In longstanding cases, squamous metaplasia may be observed, particularly in regions of persistent stone contact. Overall, bladder stones and the associated chronic inflammation are considered risk factors for bladder malignancy, including both urothelial carcinoma and squamous cell carcinoma.[178][179][180][181]
Chronic bladder stone disease has been associated with persistent mucosal irritation, prolonged inflammation, and bladder cancer, including urothelial and squamous cell carcinoma.[182] In regions with endemic bladder stone disease, patients with bladder stones have roughly twice the urothelial bladder cancer rate of the general population.[178][179][180][183] Bladder stones are also considered a risk factor for the development of primary squamous cell carcinoma of the bladder, because the calculi cause chronic superficial mucosal injury and inflammation, damaging the protective glycosaminoglycan layer and increasing the risk of malignant transformation.[181][184][185][186][187][188][189] For this reason, some clinicians have suggested that random biopsies be performed at the time of the surgical procedure for large bladder stones to detect any early associated malignant neoplasm, along with a follow-up cystoscopy at a later date.[186]
Overall, histopathologic findings in bladder stone disease are nonspecific and typically reflect chronic irritation and inflammation rather than a primary tissue-based pathological disease process. In rare cases, bladder stones are associated with unexplained hematuria or suspicious lesions, and a biopsy may reveal dysplastic or neoplastic changes. Any abnormal histologic findings should prompt further evaluation to exclude concurrent urothelial pathology rather than attribute such findings solely to the presence of bladder stones.
History and Physical
Adult patients with bladder stones may be asymptomatic or present with a range of lower urinary tract symptoms, often in the setting of conditions associated with incomplete bladder emptying, most commonly BPH or neurogenic bladder dysfunction.[16] Symptoms are frequently nonspecific and may overlap with those of underlying bladder outlet obstruction, contributing to delays in diagnosis. Terminal hematuria is the characteristic finding in patients with bladder stones and may be gross or microscopic. A classic but not universal presentation is sudden interruption of the urinary stream at the end of micturition, sometimes accompanied by terminal gross hematuria, particularly in patients with larger bladder calculi. Terminal hematuria is not pathognomonic; other conditions, such as urinary tract infections or bladder malignancies, can also cause it, but bladder stones should certainly be ruled out. Because imaging studies, such as ultrasonography or CT of the abdomen and pelvis, along with cystoscopy, are routinely included in the evaluation of hematuria, bladder stones are likely to be identified during the diagnostic workup.[190] Please see StatPearls' companion references, "Gross and Microscopic Hematuria" and "Ultrasound of the Urinary Tract," for further information.
Approximately 66% of adult patients with bladder stones have overactive bladders, particularly with larger calculi (>4 cm), although sometimes the only symptom is recurrent urinary tract infections.[25][191] Other common presenting symptoms include dysuria, suprapubic pain, urinary frequency, urgency, weak or intermittent urinary stream, and urinary retention.[192][193][194] Pain associated with bladder stones is variable and may be localized to the suprapubic region, perineum, scrotum, pelvis, or referred to the tip of the penis.[195][196]
Recurrent urinary tract infections may be the only presenting feature in some patients.[6][25] Symptoms are often exacerbated by exercise or sudden movement. Two-thirds of men with larger bladder stones (>4 cm) have overactive bladder symptoms (detrusor overactivity).[25] On physical examination, findings are often nonspecific. A distended bladder may be palpable in patients with urinary retention, but the stone itself is typically not detectable on abdominal or pelvic examination. Uroflowmetry and postvoid residual urine volume measurements via bladder ultrasonography are useful noninvasive methods of investigating possible bladder outlet obstruction and dysfunctional or incomplete bladder emptying (see Images. Interior Anatomy of the Urinary Bladder and Vertical Section of the Urinary Bladder Wall).[197][198] Please see StatPearls' companion reference, "Postvoid Residual Volume," for further information.
In children, typical symptoms of bladder stones include dysuria, difficulty voiding, urinary frequency, hematuria (gross or microscopic), incontinence, lower abdominal pain, rectal prolapse resulting from repeated straining due to bladder spasms, urgency, urinary intermittency, weak stream, and fever in up to 50% of patients.[8][116][199] Bladder stones may rarely cause acute urinary retention and are an incidental finding in 10% of cases.[116][200][201][202] Bladder stones can cause referred pain to the tip of the penis, leading young boys with such stones to repeatedly pull or squeeze the penis in an effort to mitigate the discomfort.[195][196] Repeatedly pulling on the penis is a pathognomonic sign of bladder stones in young boys.[8][116][195][199]
Evaluation
The initial evaluation of suspected bladder stones includes laboratory testing, imaging, and endoscopic assessment. Diagnostic strategies are guided by clinical presentation, stone composition, symptoms, patient age, and specific clinical factors.[10][203] The clinical presentation is often vague and overlaps with other lower urinary tract disorders, so a definitive diagnosis generally requires imaging or cystoscopic evaluation. Historically, bladder stones were detected by sounding, in which a metal instrument (a urethral sound) is inserted transurethrally into the bladder and twisted, producing an audible click or positive tactile feedback upon contact with a calculus.[204] Sounding is now of historical interest only and has been replaced by modern imaging modalities and flexible cystoscopy, which provide a safer and more reliable diagnostic assessment.
Laboratory Evaluation
Laboratory evaluation consists primarily of a urinalysis, which commonly reveals hematuria and may show leukocytes, nitrites, bacteriuria, crystalluria, or an acidic urinary pH, particularly in patients with uric acid stones.[10] Urinary crystals are typically chemically identical to the composition of the bladder stone.[205] Please see StatPearls' companion reference, "Urinary Crystals Identification and Analysis," for further information. A urine culture should be obtained when an infection is suspected.[10] Although a full metabolic evaluation is not routinely required for all patients with bladder stones, serum creatinine, calcium, uric acid, sodium, and potassium levels, as well as blood cell count, are generally recommended, along with urine pH measurements and, when available, stone chemical composition, especially in first-time stones.[10] Full 24-hour urine testing for urolithiasis prophylaxis is recommended for high-risk individuals, those with recurrent stones without evidence of bladder outlet obstruction, those with a history of nephrolithiasis, cystine stone formers, and patients with multiple bladder stones, to guide dietary, pharmacological, and surgical prophylactic therapies. Please see StatPearls' companion reference, "24-Hour Urine Testing for Nephrolithiasis: Interpretation and Treatment Guidelines," for further information.
Imaging
Imaging plays a central role in diagnosing bladder stones and includes plain abdominal radiographs (kidney, ureter, and bladder [KUB]), ultrasonography, and CT. Upper tract imaging is recommended for patients with bladder stones who have a history of urolithiasis, flank pain, recurrent bladder stones, calcium oxalate-calcium phosphate stone chemical composition, recurrent urinary tract infections, or clinical suspicion.[10][146][203]
Ultrasonography: Ultrasonography of the bladder is recommended as the first-line imaging modality for suspected bladder stones by the European Association of Urology.[203] Ultrasonography provides an inexpensive, readily available, radiation-free imaging alternative and reliably detects most bladder calculi, which typically appear as mobile, hyperechoic intravesical structures with posterior acoustic shadowing that move with patient repositioning.[166] Immobile stones may indicate adherence to the bladder wall due to a suture, clip, cable, or staple; immobility may also indicate a ureterocele, bladder diverticulum, or urothelial cancer. A CT urogram, cystogram, or cystoscopy should then be performed to confirm the diagnosis or, if the ultrasonographic study is negative, but clinical suspicion for a bladder stone remains high. Please see StatPearls' companion reference, "Ultrasound of the Urinary Tract," for further information.
- The reported sensitivity of ultrasonography for bladder stones ranges from 20% to 83%, and the specificity ranges from 98% to 100%.[206][207]
- Ultrasonography can reliably detect bladder stones 3 mm or larger, but tends to overestimate their size.[208][209] Please see StatPearls' companion reference, "Ultrasound of the Urinary Tract," for further information.
- Ultrasonography is particularly useful in pediatric and pregnant patients, as well as those for whom radiation exposure should be minimized.[166] Please see StatPearls' companion reference, "Ultrasound of the Urinary Tract," for further information.
- A renal ultrasonographic screening study can be performed concurrently with the bladder imaging study.[166]
Plain abdominal radiography: Plain abdominal radiography can identify radiopaque stones but has limited sensitivity (21%-78%) and may fail to detect radiolucent or smaller stones, especially when overlying bowel is present; plain abdominal radiography is generally insufficient as a standalone diagnostic study.[25][166][191] However, plain abdominal radiography can be used to assess the calcium content of bladder calculi and generally detects larger stones (>2 cm).[191] For example, pure uric acid and ammonium urate are radiolucent but may develop a concentric calcific coating in the bladder, making them visible on kidney, ureter, and bladder radiographs.
Noncontrast computed tomography: Noncontrast CT of the abdomen and pelvis is the most sensitive and specific modality for detecting bladder stones and accurately characterizing stone size, number, and density, including radiolucent stones such as uric acid and ammonium acid urate calculi.[166][210] Sensitivity is reported at up to 98%, with a specificity of 96% to 100%.[211] CT can also identify small calcific and radiolucent stones in the kidneys that may not be detected by other imaging modalities.[166][210] Please see StatPearls' companion reference, "Renal Calculi, Nephrolithiasis," for further information. CT is therefore considered the imaging modality of choice in adults when bladder stones are suspected.[166][210] In complex or unusual situations, contrast can be added to help clarify the anatomy, although noncontrast studies are typically sufficient (see Image. Computed Tomography Scan of the Pelvis).
- Most pediatric and pregnant patients can be evaluated with ultrasonography or magnetic resonance imaging (MRI) without the need for potentially harmful ionizing radiation from CT, which should be reserved as a last resort when absolutely necessary.[212]
- If CT imaging is required during pregnancy, it should not be performed during the first trimester and should follow minimal-dose protocols.[132][213] Fortunately, such situations are rare.
Cystoscopy: Cystoscopy provides a definitive diagnosis and allows direct visualization of any bladder calculi, assessment of the stone burden, evaluation of the bladder mucosa, and identification of underlying pathology such as outlet obstruction, BPH, diverticula, bladder cancer, or foreign bodies. Cystoscopic evaluation is particularly important in patients with hematuria, recurrent urinary tract infections, or symptoms suggestive of concomitant bladder pathology. However, cystoscopy cannot evaluate the upper tracts for calculi, unlike CT. Please see StatPearls' companion reference, "Cystoscopy," for further information.
Magnetic resonance imaging: MRI is a promising modality for imaging bladder stones when CT cannot be performed, or ionizing radiation should be avoided, such as in pediatric patients and during pregnancy.[214][215] MRI typically demonstrates a calculus as an indistinct area without detail, surrounded by high-signal-strength water (urine), and is most reliable for stones greater than 5 mm.[166][214][215] However, MRI is time-consuming and expensive, provides no clear visual details of the stone, and is often unnecessary because ultrasonography or cystoscopy is generally sufficient.[166][216]
Cystoscopy
Cystoscopy is a minimally invasive surgical procedure that allows direct visualization of the urethra and bladder. Cystoscopy not only confirms the presence of stones but also allows assessment of their size, number, and configuration, as well as the presence or absence of associated bladder pathology. Cystoscopy can also identify outlet obstruction, BPH, and urethral strictures that affect treatment selection. Please see StatPearls' companion reference, "Cystoscopy," for further information.
Treatment / Management
The management of bladder stones is guided by stone size, composition, symptom burden, underlying etiology, patient age, and clinical factors. According to contemporary recommendations from the American Urological Association and European Association of Urology, definitive treatment is primarily surgical for most patients.[10][203] Medical therapy plays a limited role and is reserved for carefully selected cases. Identification and correction of underlying causes, particularly bladder outlet obstruction or impaired bladder emptying, as well as adequate hydration and the elimination of nutritional deficiencies, are essential to reduce recurrences.[217](A1)
Medical Therapy
Medical management has a limited role in bladder stone disease.[10] Dissolution therapy may be considered for select patients with radiolucent pure uric acid bladder stones who can adequately empty the bladder and reliably maintain therapeutic urinary alkalinization (pH >6.5).[10] Please see StatPearls' companion reference, "Uric Acid Nephrolithiasis," for further information.(A1)
Urinary alkalinization: For pure uric acid stones, urinary alkalinization is typically achieved with oral potassium citrate, often requiring approximately 60 mEq/d, titrated to maintain a urinary pH between 6.5 and 7.0.[10] Sodium bicarbonate may be used as an adjunct when necessary. Serum potassium levels and urinary pH should be monitored regularly during therapy.[10][218][219] Please see StatPearls' companion reference, "Uric Acid Nephrolithiasis," for further information. Allopurinol is not routinely recommended, but may be used in cases of gout, hyperuricemia, or hyperuricosuria, because urinary alkalinization is the primary therapy for uric acid bladder stones.[218][219][220](A1)
Irrigation chemolysis: Irrigation chemolysis is possible using a 2- or 3-way catheter, but the technique is logistically awkward, time-consuming, and inconvenient, and may cause bladder irritation.[10][221] Please see StatPearls' companion reference, "Uric Acid Nephrolithiasis," for further information. For all these reasons, this technique is not frequently used.[10][221][222] Chemical dissolution of infection-related (struvite) bladder stones using continuous bladder irrigation with agents such as citric acid (solution R) or renacidin (hemiacidrin: citric acid, glucono-δ-lactone, and magnesium carbonate solution) is rarely performed due to slow resolution rates, infection risk, hypermagnesemia, and the availability of more effective surgical options.[223][224][225][226] Toxicity with renacidin is associated with hypermagnesemia from use under pressure within the urinary system.[225][227](A1)
Indwelling catheters: In patients with chronic indwelling urinary catheters who experience recurrent catheter encrustation, periodic bladder instillation of dilute acetic acid (0.25%) may help dissolve calcium phosphate deposits that cause catheter obstruction and maintain luminal patency. This approach is intended to prevent encrustation rather than treat established bladder calculi. Calcium phosphate is the primary component of the encrustations and debris that typically clog urinary stents and catheters; it forms only in alkaline solutions and can be dissolved by mild acid.[228] Periodic bladder instillations of a 0.25% acetic acid solution can help dissolve calcium phosphate crystals, prevent encrustation, and reduce the risk of bladder stone formation.[229] Acetic acid instillations can also help maintain patency of Foley catheters and suprapubic tubes in patients whose urinary drainage tubes tend to clog prematurely with debris.[230](B3)
Routine metabolic evaluation is not required for all patients with bladder stones, though it is always an option for motivated individuals. Patients at high risk of recurrence; those with a history of nephrolithiasis; suspected metabolic abnormalities; significant underlying medical comorbidities, including those with a high surgical, anesthesia, or infection risk; or bladder calculi composed primarily of calcium oxalate, calcium phosphate, pure uric acid, or cystine may benefit from 24-hour urine testing to tailor optimal prophylactic therapies.[218] Please see StatPearls' companion reference, "24-Hour Urine Testing for Nephrolithiasis: Interpretation and Treatment Guidelines," for further information.
Pediatric patients: Treatment of children with primary bladder stones in endemic areas is mostly dietary. Dietary management includes treating any diarrhea, maintaining adequate hydration, and providing a diet that includes mixed cereal with vitamin A and B supplements, along with eggs, meat, and boiled cow's milk for children older than 1.[8]
Surgical Treatment
Surgical intervention is the treatment of choice for most bladder stones. Endoscopic approaches are preferred whenever feasible due to high stone-free rates and low morbidity. Transurethral cystolitholapaxy is the most commonly performed and recommended surgical procedure for bladder stones in adults and can be accomplished using laser, pneumatic, ultrasonic, or mechanical lithotripsy devices.[10][231] However, the narrower working channel of transurethral compared to percutaneous instrumentation requires a greater degree of stone fragmentation into pieces small enough to pass through the transurethral instrumentation. The narrower channel extends the surgical time and increases the risk of trauma to the urethra, urethral sphincter, and bladder.[19][232][233][234][235](A1)
Advantages of minimally invasive cystolithotripsy surgical procedures for bladder stone removal include shorter hospital stays, improved cost-effectiveness, less scarring, fewer complications, and a reduced risk of urinary extravasation compared with traditional open cystolithotomy.[10][19][236][237] When bladder outlet obstruction is present, most guidelines recommend addressing it at the time of stone removal, when clinically appropriate, such as performing transurethral resection of the prostate concurrently; however, a recent EAU review questioned whether this is true for all patients.[238][239][240] Given the multifactorial nature of bladder stone formation, individualized decision-making is advised.[240] A systematic review and meta-analysis conducted by the EAU concluded that endoscopic surgical procedures were as effective overall as open surgical procedures for bladder stones, while requiring shorter durations of Foley catheterization, causing less postoperative pain, and facilitating faster recovery in both children and adults.[10](A1)
Noninvasive surgery with extracorporeal shockwave lithotripsy: Extracorporeal shockwave lithotripsy (ESWL), a noninvasive treatment modality, has been successfully used as an alternative to surgery for radiopaque bladder stones measuring 25 mm or less. This approach is particularly useful in children and patients with limited urethral access; those at high risk for anesthesia; those who refuse general anesthesia, open surgical procedures, or endoscopy; and in situations where positioning is problematic.[10][241][242][243][244][245][246][247][248] ESWL can be performed on an outpatient basis, requires less anesthesia than alternative therapies, has a low complication rate, avoids skin and bladder incisions, and has an encouragingly high reported stone-free rate (90%-94%).[10][241][242](A1)
Stones impacted in the urethra can be repositioned into the bladder and treated with ESWL.[245] ESWL may also be used in children with bladder calculi.[10][249] ESWL is a reasonable, safe, and effective option for breaking up suitable bladder stones in augmented bladders and continent diversions, but endoscopy may be needed to completely remove all the fragments.[250][251][252] (A1)
ESWL is performed with the patient in either the prone or supine position. A Foley catheter is placed. If the bladder is left empty, the collapsed bladder helps hold the stone in place. The bladder can also be partially filled to facilitate imaging and help protect the bladder mucosa, but partial filling may increase stone mobility and motion during treatment. ESWL may require more than 1 treatment session to achieve optimal results and has a lower stone-free rate than alternative surgical therapies.[10][203][243] ESWL should generally not be used for bladder stones in patients with artificial sphincters or penile prostheses. Results from at least 1 randomized and 2 nonrandomized studies showed equivalent efficacy, with shorter hospital stays, with ESWL compared to transurethral cystolithotripsy for bladder stones.[10][203][243][253] Due to its low complication rate, safety, noninvasiveness, and overall effectiveness, ESWL is probably underused as a treatment modality for bladder stones.[241][242][243][253] (A1)
Minimally invasive surgery with laser lithotripsy: Minimally invasive treatment with laser lithotripsy, particularly using a Ho:YAG laser, is increasingly favored for its high efficacy, low complication rates, and ability to be combined with concurrent endourologic surgical procedures, such as treatment of bladder outlet obstruction or ureteroscopy, during the same operative session.[254][255] Ultrasonic and pneumatic lithotripsy devices may fragment stones more rapidly; however, stone mobility may pose issues, along with potential mucosal trauma.[19] All of these modalities are considered effective, but electrohydraulic lithotripsy is generally avoided in the bladder because it causes the greatest degree of stone mobility, thereby increasing the risk of mucosal injury and hematuria and unnecessarily prolonging operating time.[19]
Nephroscopes are preferred for endoscopic cystolitholapaxy surgical procedures due to their improved visualization and large working channel (24-26 French). The larger-caliber working channel accommodates larger lithotripsy probes and fibers, enabling more efficient stone fragmentation and superior irrigation flow.[10][256][257][258][259] Additionally, nephroscopes offer improved visualization, and their wider-bore working channel facilitates irrigation and evacuation of larger stone fragments.[10][256][257][258][259](A1)
Settings for laser cystolithotripsy are variable depending on the laser type, stone composition, hardness, and size. Higher frequency at low power settings with a longer pulse duration is most useful for dusting, whereas higher power levels at a slower frequency are better for fragmentation.[260][261][262][263][264][265][266] Please see StatPearls' companion reference, "Ureteroscopy," for further information. Irrigation is reduced to the lowest flow rate consistent with good visualization to minimize stone migration during treatment.(A1)
Transurethral cystolitholapaxy is generally the recommended and optimal surgical procedure for adults with small-to-medium–sized bladder stones and normal lower urinary tract anatomy.[10][19][235][267][268][269] Although the surgical procedure can be performed in children, great care should be taken when using transurethral access in prepubertal boys to avoid urethral trauma and strictures.[267][270][271] Please see StatPearls' companion reference, "Urethral Strictures," for further information. Transurethral cystolithotripsy avoids creating holes in the bladder or skin but is slower than the percutaneous approach, requires a higher degree of stone fragmentation, uses narrower instruments, and carries a greater risk of urethral trauma (strictures), especially in young boys, making transurethral cystolithotripsy more suitable for adults.[10][232][235][253][267][269][272][273](A1)
Stone size, urethral anatomy (size), and patient age are the most critical factors to consider when determining the best access route. Nephroscopes are preferred over cystoscopes for these surgical procedures.[10][257][274][275] In women, the use of a transurethral Amplatz sheath can facilitate treatment by providing a substantially larger lumen for stone extraction and avoiding urethral trauma from repeatedly reintroducing cystoscopic instruments.[276][277](A1)
Percutaneous suprapubic cystolitholapaxy: This procedure offers stone-free rates comparable to those of open surgical procedures and is the preferred surgical approach for pediatric bladder stones in younger boys and men with unusual urethral anatomy. The percutaneous approach minimizes urethral trauma by entering the bladder suprapubically, is quicker, and allows the safe use of larger instruments than can be passed transurethrally.[237][278][279] Percutaneous access is the preferred approach for patients with larger calculi, younger male pediatric patients, individuals with abnormal or strictured urethras, those with positioning issues, patients with augmented bladders or continent reservoirs, and those with complex or multiple stones.[10][19][235][237][267][268][269][280][281][282][283][284] Bladder entry may be challenging in some patients, and intraoperative imaging may be required to facilitate access. Additionally, intestinal or vascular injury may occur, especially in patients with previous pelvic or abdominal surgical procedures. Bladder cancer is a contraindication.(A1)
Instrumentation is similar to that used for percutaneous nephrolithotomy.[285] The use of large-diameter Amplatz sheaths (up to 36 French) can greatly facilitate the extraction of larger fragments, as less time is required for stone fragmentation, and larger instruments can be used for lithotripsy. Dual Amplatz sheaths have been successfully used in women (one placed percutaneously for surgical access, the other transurethrally for drainage and passage of fragments) and can greatly facilitate the treatment of larger or giant stones.[286][287](B3)
Technique:
- The bladder is distended with 300 to 400 mL of normal saline using a Veress or spinal needle for access.
- Ultrasonographic or fluoroscopic guidance may be used.
- After placing a guide wire, a suprapubic puncture can be made either directly or after a mini-cutdown to expose the bladder's external surface.
- After the tract is dilated, a nephroscope can be placed (nephroscopes are preferred over cystoscopes for this purpose).[257][274][275]
- Pneumatic fragmentation devices, ultrasonic probes, or laser fibers can then be used to fragment the calculi.
- The fragments are irrigated from the bladder, aspirated, or removed with graspers.[278][279][283][288] (A1)
Open suprapubic cystolithotomy: Open suprapubic cystolithotomy has been the standard treatment for large bladder stones, especially in children, because it is effective, quick, minimizes anesthesia and operating times, offers high stone-free rates, and does not require highly specialized training or endourological equipment, which may not be available in resource-limited regions.[19][289][290][291] Open suprapubic cystolithotomy is now increasingly reserved for patients with extremely large bladder stones (greater than 4 cm), multiple large calculi, pediatric patients (to avoid possible urethral injury during endoscopy), concomitant pathology requiring open surgical procedures, such as very large prostates, and where instrumentation for alternative approaches is unavailable.[255][289][291](B3)
Open cystolithotomy is being replaced by minimally invasive surgical procedures, including percutaneous suprapubic cystolithotripsy, endourological treatment with holmium laser litholapaxy, and robotic cystolithotomy.[289] Transurethral endourological techniques are typically used for stones smaller than 10 mm, whereas percutaneous cystolithotripsy and combined approaches are generally preferred for larger stones.[267][292] Although open surgical procedures allow rapid removal of intact stones and facilitate concurrent open prostatectomy when indicated, open surgical procedures are associated with large skin and bladder incisions, longer hospitalizations, more postoperative pain and morbidity, prolonged catheterization time, a greater risk of postoperative urinary extravasation, increased scarring, and usually require drains.[10][290](A1)
Laparoscopic and robotic cystolithotomy: These surgical techniques have been used in adult patients with bladder stones, typically in combination with a simple prostatectomy, in children, or in augmented bladders.[10][293][294][295][296][297] These advanced minimally invasive surgical procedures are designed to remove multiple, large, or complex bladder calculi through small abdominal incisions, while offering faster recovery time, less blood loss, fewer complications, reduced incidence of stone recurrences, and lower overall morbidity.[10][19][295][296][297][298](A1)
Many patients with bladder stones do quite well with medical therapy for BPH after their calculi are removed, especially if they have not had prior medical treatment for benign prostatic hyperplasia.[217][238][240][299] BPH causing bladder outlet obstruction associated with bladder stones has traditionally been an absolute indication for surgery, typically either transurethral resection or laser prostatectomy.[17][300][301] However, results from recent studies indicated that in many cases, conservative medical therapy for BPH may be sufficient.[217][238][240][299] (B2)
Special Patient Populations
Pregnant patients: Bladder stones in pregnant patients and those with augmented bladders, urinary diversions, or following renal transplant are managed similarly to those in native bladders, with the treatment modality selected based on anatomy, stone burden, clinical issues, available instrumentation, surgical training, and expertise, as well as relevant patient factors.[302] Combined endoscopic, percutaneous, robotic-assisted, and open approaches, particularly transurethral and percutaneous surgical procedures, may be required in complex cases.[303][304] The use of gastric segments for augmentation cystoplasty, rather than colon or ileum, significantly reduces the risk and incidence of bladder stones.[55][69][305][306](B2)
Bladder stones during pregnancy are quite rare, but bladder stones significantly increase the risk of complications, including preterm labor, recurrent urinary tract infections, suprapubic pain, and obstructed labor if the stones are large enough to interfere with the passage of the fetal head at delivery.[132][133][134][135][136][137][138][139] If obstruction occurs, a cesarean section is recommended with removal of the stone at the time of the surgical procedure or later.[132][307] In some cases where the stones are mobile and relatively small, clinicians may be able to manually move the stones above the fetal vertex and continue with a vaginal delivery.[132][134] In general, the risks of complications from bladder stones are deemed greater than the risks of surgical removal, so surgical treatment to eliminate bladder stones before delivery is generally recommended.[132][213][308] If the stone is large enough and not removed before delivery, it risks bladder rupture and obstructed labor.[134][135][136][137][138][139][309](B3)
Imaging during pregnancy is primarily with ultrasonography, followed by MRI, and, if necessary, a low-dose CT scan, except during the first trimester.[132][213] Fortunately, the frequent and routine use of ultrasonography during pregnancy generally allows early identification of significant bladder stones before delivery.[132][213] Traditional surgical therapy has been open cystolithotomy, particularly for larger stones, but open cystolithotomy carries a risk of creating a vesicocutaneous fistula.[310] Increasingly, percutaneous cystolitholapaxy with Ho:YAG laser therapy has become the treatment of choice.[132][308] Smaller stones can often be managed with transurethral cystolitholapaxy because the Ho:YAG laser is effective across all stone materials and has minimal tissue penetration.[132][308](B3)
Renal transplant: Patients who have had a renal transplant rarely form bladder stones, with an incidence of only 1% to 3%.[311][312][313] However, when bladder stones occur in this population, bladder stones present a unique challenge because bladder stones may require surgical removal in the setting of immunosuppression, which predisposes these patients to a higher risk of potential complications.[311] Risk factors for urinary stone production in this population include hyperparathyroidism, hypocitraturia, hypercalciuria, and a history of nephrolithiasis in a patient after transplant.[311][314][315] In results from a large review of 8835 patients with a renal transplant, the median time from renal transplant to bladder stone presentation was 13 years.[311] Calcium oxalate is the most common chemical composition of stones in this population.[311][312][316] Stones may develop over suture material, particularly nonabsorbable sutures, used during ureteroneocystostomy.[312] When stones occur, Ho:YAG laser therapy has generally been the preferred therapeutic option because it is safe, effective, minimally invasive, and causes less mucosal bleeding than ultrasonic, electrohydraulic, pneumatic, or mechanical lithotripsy.[312]
Summary of Surgical Options
- Transurethral laser cystolithotripsy using continuous-flow instrumentation is the preferred surgical procedure for bladder stone removal in adults and in children when possible.
- Percutaneous cystolithotripsy is recommended when transurethral access is not possible, not recommended, or not advisable.
- Percutaneous cystolithotripsy is preferred in children where transurethral access is difficult, or at a high risk of urethral trauma and stricture formation in younger children, those with prior urethral surgical procedures, known urethral strictures, or spinal cord injury.
- ESWL, laparoscopic, robotic, or open surgical procedures should be considered when endoscopic therapy is not possible or recommended (in adults and children).
- Open suprapubic cystolithotomy is recommended only for very large bladder stones or where minimally invasive therapies are unavailable.[EAU. Urolithiasis]
Differential Diagnosis
A key consideration in differentiating solid intravesical masses is their mobility.[146] Prone and supine positioning can demonstrate the mobility of bladder masses, such as blood clots and stones.[146] Accurate differentiation among these conditions relies on a combination of clinical presentation, medical history, laboratory findings, imaging characteristics, and cystoscopic assessment. Cystoscopy is typically the definitive study to confirm the diagnosis. Please see StatPearls' companion reference, "Cystoscopy," for further information. Several conditions may mimic the clinical presentation, symptoms, or imaging appearance of bladder stones and should be considered during evaluation. These conditions include the following:
- A passed renal or ureteral calculus may transiently remain in the bladder and occasionally cause acute symptoms. These stones generally pass spontaneously unless bladder outlet obstruction or dysfunctional voiding is present, but passage becomes problematic with calculi greater than 6 to 7 mm. Persistent intravesical calculi suggest impaired bladder emptying, outlet obstruction, or local stone growth rather than transient passage. Diagnosis is made by ultrasonography or CT, with cystoscopy used for confirmation if necessary.
- BPH commonly presents with lower urinary tract symptoms such as a weak stream, urinary retention, frequency, and urgency, which overlap with symptoms caused by bladder stones. Please see StatPearls' companion reference, "Benign Prostatic Hyperplasia," for further information. However, BPH does not produce a mobile intravesical filling defect on imaging, and cystoscopy distinguishes obstructive prostatic enlargement from intravesical calculi. Imaging may show a noncalcified tissue density filling defect in a characteristic location at the bladder neck.[146][211] Please see StatPearls' companion reference, "Ultrasound of the Urinary Tract," for further information.
- Blood clots in the bladder may appear as radiolucent filling defects on imaging and can cause hematuria, urinary retention, or intermittent urinary stream obstruction. Unlike bladder stones, clots are typically noncalcified, may change shape rather than position, and often resolve or fragment with bladder irrigation. On ultrasonography, blood clots appear as mobile, hyperechoic, low-density masses without shadowing.[146] They are avascular on color Doppler and typically collect at the most dependent (lowest) position within the bladder.[146] Prone and supine positioning can demonstrate the mobility of bladder masses, such as thrombi and stones.[146] Cystoscopy readily differentiates clots from calculi. Please see StatPearls' companion reference, "Cystoscopy," for further information.
- Fungal balls, most commonly caused by Candida species in patients who are immunocompromised or those with permanent indwelling catheters, appear as mobile, radiolucent intravesical filling defects.[317][318] These lesions are usually noncalcified, irregular, avascular, and associated with signs of infection.[317][318] Definitive diagnosis is established by cystoscopy and microbiologic evaluation. Please see StatPearls' companion reference, "Cystoscopy," for further information.
- Papillary urothelial carcinoma of the bladder (bladder cancer) may present with hematuria and appear as an intravesical mass or localized bladder wall thickening. Unlike bladder stones, urothelial tumors are typically fixed to the bladder wall, radiolucent, irregularly contoured, and immobile with patient repositioning. Please see StatPearls' companion reference, "Ultrasound of the Urinary Tract," for further information. Urothelial tumors may sometimes show some calcification. Cystoscopic evaluation is required to exclude a malignant neoplasm when a fixed bladder lesion is identified. Please see StatPearls' companion reference, "Bladder Cancer," for further information.
- Sloughed papillae from renal papillary necrosis may enter the bladder, mimicking stones.[319] Sloughed papillae occur most often in patients with diabetes mellitus, sickle cell disease, or analgesic nephropathy.[319] These fragments are typically mobile, radiolucent, irregular, and may be associated with upper urinary tract pathology.[320] A definitive diagnosis of a sloughed papilla in the bladder generally requires cystoscopy. Please see StatPearls' companion reference, "Cystoscopy," for further information.
- Urinary tract infections can cause dysuria, frequency, urgency, suprapubic pain, and hematuria, symptoms that closely resemble those of a bladder stone. Urinary tract infections may also cause bladder wall thickening, a finding that may suggest bladder cancer. However, infection alone does not produce a discrete intravesical filling defect, and symptoms usually resolve with appropriate antimicrobial therapy.[321][322] Please see StatPearls' companion reference, "Acute Cystitis," for further information. Persistent or recurrent infections should prompt evaluation for an underlying bladder stone.[321][322]
Prognosis
The prognosis for bladder stone disease is generally favorable when stones are promptly diagnosed and appropriately treated. Most patients experience total symptom resolution following complete stone removal, particularly when the underlying cause, such as bladder outlet obstruction, urinary stasis, or foreign material, is identified and corrected. Modern endoscopic and minimally invasive techniques, such as laser cystolitholapaxy, offer a safe, efficient means of removing bladder stones, with most patients resuming normal daily activities within a few days to 2 weeks.
Small bladder stones may pass spontaneously in patients with normal bladder emptying; however, larger calculi (6-7 mm or greater) are unlikely to pass spontaneously and may become lodged at the bladder neck or in the urethra, leading to urinary obstruction, significant discomfort, and acute urinary retention.[323][324][325][326][327] Without treatment, bladder stones tend to enlarge and can result in progressive lower urinary tract symptoms, recurrent urinary tract infections, hematuria, bladder wall inflammation, urinary retention, and, in severe cases, upper urinary tract damage.
Recurrence risk is closely related to the persistence of predisposing factors. Patients with untreated bladder outlet obstruction, neurogenic bladder dysfunction, chronic indwelling catheters, frequent urinary tract infections, nephrolithiasis, augmented bladders, or continent urinary diversions have a higher likelihood of recurrent bladder stone formation. When these underlying conditions are effectively managed, recurrence rates are significantly reduced. Overall, long-term outcomes are excellent in patients who undergo complete removal of bladder stones and appropriate management of contributing factors. Regular follow-up and preventive strategies are particularly important in high-risk populations to minimize recurrences and associated complications.
Complications
Bladder stones can lead to a range of complications, particularly when stones are large, long-standing, or associated with underlying urinary tract dysfunction. Urinary tract infection is a common complication. Symptoms such as urinary frequency, urgency, dysuria, transient hematuria, and suprapubic pain are common and result from chronic mechanical irritation of the bladder mucosa. Recurrences are common if the underlying causative factors are not identified and corrected. Hematuria, either microscopic or gross, may result from mucosal abrasion or inflammation. Larger calculi can cause intermittent or complete urinary obstruction, particularly when they lodge at the bladder neck or migrate into the urethra, leading to acute urinary retention. Urethral obstruction is more likely in men and may require urgent intervention.
Recurrent urinary tract infections are a frequent complication because bladder stones can serve as a nidus for bacterial colonization and impair complete bladder emptying. Persistent infection further promotes stone growth and increases the risk of recurrent calculi. In severe or untreated cases, chronic obstruction and infection may result in bladder wall damage, reduced bladder compliance, and, less commonly, deterioration of the upper urinary tract. Bladder stones may also contribute to urinary incontinence, especially urge incontinence, due to detrusor overactivity triggered by chronic irritation, and overflow incontinence.[328] A rare complication of bladder stones is fistula formation, particularly in patients with prolonged stone disease or prior pelvic operations.[329][330][331][332]
Medical therapy can cause bladder inflammatory changes or fail to dissolve the stone. As stones shrink, they may become small enough to enter the urethra and become stuck, causing an obstruction.
Surgical management carries procedure-related risks that vary by technique:
- Transurethral cystolitholapaxy may result in transient hematuria, urinary tract infection, bladder mucosal injury, urethral trauma (and possible urethral strictures), bladder perforation, or temporary urinary retention.[267][333] These complications are typically self-limited and managed with supportive care, short-term catheterization, or antimicrobial therapy when indicated. Electrohydraulic lithotripsy is generally avoided due to its association with a higher risk of mucosal injury.
- Percutaneous cystolitholapaxy may result in urinary extravasation, additional pain, postoperative fever, abdominal distension from extravasated irrigation fluid, transient ileus, urinary retention, the need for prolonged catheter drainage, and wound issues, such as infection or dehiscence.[237][267][237][334][335]
- Open surgical procedures carry risks of urinary extravasation (urinoma), significant bleeding requiring transfusions, prolonged urinary leakage, bladder perforation, incidental bowel damage, wound issues, and scarring.[335]
An association between chronic bladder stones and bladder cancer has been reported, likely related to long-standing inflammation and mucosal irritation; however, a definitive causal relationship has not been established.[185][186][237][336] Nonetheless, persistent hematuria, suspicious cytology, or abnormal cystoscopic findings in patients with bladder stones should prompt an evaluation for concurrent malignant neoplasm, such as a biopsy.[185]
Postoperative and Rehabilitation Care
Postoperative care following bladder stone treatment depends on the surgical approach, stone burden, comorbidities, patient age, and presence of underlying urinary tract pathology. Most patients undergoing endoscopic cystolitholapaxy experience rapid recovery and can be managed with short-term observation or same-day discharge. After endoscopic or percutaneous stone removal, transient hematuria, dysuria, and urinary frequency are common and typically resolve within several days. Short-term bladder catheterization may be required to ensure adequate drainage, particularly in patients with preexisting bladder outlet obstruction or postoperative edema. Adequate hydration is encouraged to promote urinary flow and prevent clot retention. Analgesics and anticholinergic agents may be used as needed for pain or bladder spasms.
Patients should be monitored for early postoperative complications, including urinary tract infections, acute urinary retention, persistent hematuria, or urethral injury. Antibiotics are administered perioperatively when indicated and continued postoperatively only if an infection is documented. In patients with chronic indwelling catheters or augmented bladders, catheter care protocols and bladder irrigation regimens may be resumed to reduce the risk of encrustation and stone recurrence.
Rehabilitation focuses on addressing underlying contributors to bladder stone formation. Patients with bladder outlet obstruction may require medical or surgical management to optimize bladder emptying. Individuals with neurogenic bladder dysfunction benefit from structured bladder management programs, including clean intermittent catheterization, scheduled voiding, or urodynamic follow-up when appropriate. Urine testing with a 24-hour collection for stone prophylaxis is reasonable and appropriate in some high-risk, highly motivated patients, particularly if they also have recurrent nephrolithiasis.
Long-term follow-up is tailored to the individual's recurrence risk. High-risk patients, including those with neurogenic bladders, augmented bladders, chronic catheterization, or prior recurrent stones, may require periodic surveillance with imaging, urinalysis, or cystoscopic evaluation. A standard follow-up protocol would be at 1 month postoperatively, with either a kidney, ureter, and bladder radiograph or ultrasonography to confirm the elimination of all stone fragments. At this point, a metabolic evaluation can be ordered. Follow-up radiography or ultrasonography is recommended at 6- to 12-month intervals. Patient education on optimizing hydration, catheter care, infection prevention, and symptom recognition is essential to minimize recurrences and avoid complications. Overall, postoperative outcomes are favorable when stone removal is combined with appropriate rehabilitation strategies, treatment of underlying nutritional deficiencies, correction of any urinary tract dysfunction, and, as appropriate, metabolic testing.
Consultations
Possible consultations include the following:
- Although pediatric and adult urologists are the primary specialists in managing bladder stones, other specialties may need to be consulted for optimal patient outcomes.
- Nephrology can be helpful in patients with recurrent urolithiasis (although nephrolithiasis management may be performed by urology) or metabolic abnormalities.
- Physical medicine and rehabilitation specialists can help patients with spinal cord injuries optimize management of their neurogenic bladders.
- Anesthesia may need to be consulted in some patients with high-risk conditions before the surgical procedure.
- Infectious disease consultations may be useful for complicated or recurrent urinary tract infections, particularly in patients with indwelling catheters, multidrug-resistant organisms, or immunocompromised states.
- Oncology consultations are warranted only when a concurrent bladder malignant neoplasm is present.
- Primary care clinicians need to be aware of the signs and symptoms of recurrent bladder stones to allow early diagnosis and treatment.
Deterrence and Patient Education
Once bladder stones have developed, patients are at increased risk for recurrence, particularly if underlying predisposing factors are not addressed. Effective deterrence focuses on identifying and correcting the causes of stone formation, such as bladder outlet obstruction, impaired bladder emptying, chronic infection, foreign bodies, or neurogenic bladder dysfunction. Patients should be counseled on the importance of maintaining adequate hydration. Increased fluid intake helps dilute urinary solutes, reduces crystal precipitation, and promotes regular bladder emptying. Hydration goals should be individualized based on patient comorbidities, but patients are generally advised to maintain sufficient urine output to keep urine light in color. For most adult patients, a 24-hour urine output of at least 2000 mL is suggested.
Education should also emphasize the need for appropriate management of bladder outlet obstruction. In patients with BPH or other obstructive conditions, medical or surgical treatment may be necessary to prevent urinary stasis, improve bladder emptying, and reduce the risk of recurrent bladder stones. Patients with neurogenic bladder should be instructed in appropriate bladder management strategies, including clean intermittent catheterization, scheduled voiding, and optimal catheter care protocols, as appropriate.
Patients with chronic indwelling catheters, augmented bladders, or urinary diversions should receive education on catheter hygiene, appropriate bladder irrigation techniques and protocols, and early recognition of symptoms suggestive of stone recurrence or infection. Patients at high risk should adhere to follow-up appointments and regular surveillance plans. Finally, patients should be advised to seek medical evaluation for recurrent urinary tract infections, hematuria, worsening lower urinary tract symptoms, or difficulty voiding because these may indicate recurrent stone formation or underlying pathology requiring further assessment and treatment.
Pearls and Other Issues
Pearls regarding bladder stones include the following:
- ESWL is effective, safe, noninvasive, and significantly underused in the surgical treatment of bladder stones.
- Bladder stones most commonly result from urinary stasis rather than from primary metabolic abnormalities. Consequently, definitive management requires not only complete stone removal but also identification and correction of these underlying causes, such as bladder outlet obstruction, neurogenic bladder dysfunction, foreign bodies, nephrolithiasis, or chronic infection. Failure to address these factors is a common pitfall and a major contributor to recurrence.
- Routine bladder irrigation is not recommended; it should be used only in augmented bladders, continent diversions, or when specific problems, such as rapid encrustation and frequent catheter obstructions, arise.
- The presence of bladder stones in patients with BPH is not an absolute indication for surgical treatment of the prostate, because medical therapy produces acceptable outcomes in selected individuals.[217][238][240][299]
- Nephroscopes are preferred over cystoscopes and other endoscopic instruments for cystolitholapaxy, when available.[10][256][257][258][259] Improved visualization and larger working channel facilitate cystolithotripsy procedures and the evacuation of fragments.[10][256][257][258][259]
- Clinicians should consider using a transurethral Amplatz sheath in women with giant bladder stones or use a dual Amplatz sheath technique.[276][277][286][287]
- Metabolic evaluation, including 24-hour urine testing, is not routinely required for all patients with bladder stones but should be considered in selected individuals. These individuals include patients with uric acid or cystine bladder stones; those with a history of nephrolithiasis or previous bladder stones; patients without an identifiable obstruction, voiding dysfunction, or intravesical nidus; or those with a strong family history of urinary stone disease. In such cases, evaluation may consist of 24-hour urine testing and serum chemistries, including uric acid levels, to guide preventive strategies.
- Radiolucent bladder stones, particularly uric acid stones, may be missed on plain radiography; therefore, ultrasonography, noncontrast CT, or cystoscopy should be performed when clinical suspicion remains high despite negative initial imaging results.
- A common pitfall is attributing lower urinary tract symptoms solely to BPH or infection without considering concomitant bladder calculi.
- Allopurinol is not the primary recommended treatment for pure uric acid stones, which are best treated with urinary alkalinization.[219][337] Please see StatPearls' companion reference, "Uric Acid Nephrolithiasis," for further information.
- Routine bladder irrigation is not recommended for most patients with chronic indwelling Foley catheters or suprapubic tubes, except in those with continent urinary diversions or augmented bladders); however, periodic irrigation with an acidifying solution may be helpful for patients with long-term catheters who experience rapid encrustation and recurrent blockages that require frequent catheter changes.[48][49][338][339]
- Medical dissolution therapy has a limited role in treating bladder stones and should be reserved for carefully selected patients with pure uric acid stones who can demonstrate adequate bladder emptying and maintain sustained urinary alkalinization. Surgical removal remains the definitive treatment for most patients.
- Laser settings for laser cystolithotripsy are variable depending on the laser type, stone composition, hardness, and size. Higher frequency at low power settings with a longer pulse duration is most useful for dusting, while higher power levels at a slower frequency are better for fragmentation.[260][261][262][263][264][265] Irrigation is reduced to the lowest flow rate that allows good visualization, minimizing stone migration during treatment. Please see StatPearls' companion reference, "Ureteroscopy," for further information.
- Patients with traumatic Foley catheter removals, particularly if unobserved, need to have the extracted catheters carefully inspected.[81] If any suspicion of a missing balloon fragment exists or the catheter is unavailable for inspection, a cystoscopy must be performed. Retained Foley balloon fragments in such situations can become a nidus for bladder stone formation.[81] Please see StatPearls' companion reference, "Prevention of Inappropriate Self-Extraction of Foley Catheters," for further information.
Enhancing Healthcare Team Outcomes
Bladder stone disease requires coordinated, interprofessional management to optimize patient outcomes and reduce recurrences. Although bladder stones are relatively uncommon in industrialized nations, they remain clinically significant in resource-limited regions of the world, especially in children. In high-income countries, bladder stones occur in patients with impaired bladder emptying, chronic catheterization, neurogenic bladder dysfunction, augmented bladders, and spinal cord injuries. Clinicians play a central role in identifying patients at risk, recognizing symptoms suggestive of bladder calculi, initiating appropriate diagnostic evaluations, and addressing underlying etiologies such as bladder outlet obstruction or urinary stasis. Early referral to urology is essential for definitive diagnosis, timely procedural management, and prevention of recurrences.
Nurses are critical to prevention and early detection through patient education and prompt recognition of symptoms suggestive of bladder stones. Proper catheter care, including adherence to catheter change schedules, aseptic technique, and patient education, significantly reduces the risk of stone formation. When Foley catheters are removed traumatically or dislodged, healthcare professionals and nursing staff must inspect the catheter to ensure balloon integrity and promptly report concerns. Retained balloon fragments or foreign material can serve as a nidus for stone formation, and timely communication with the medical team facilitates early cystoscopic evaluation and removal of balloon fragments when indicated.
Pharmacists contribute by reviewing prescribed therapies, monitoring for drug interactions, counseling patients on urine pH monitoring and the proper use of alkalinizing agents, and supporting medication adherence. In patients requiring bladder irrigation or chemical agents to reduce catheter encrustation, pharmacists assist in verifying appropriate formulations, concentrations, and safety considerations. Effective interprofessional communication among primary care clinicians, urologists, nurses, pharmacists, rehabilitation specialists, and, when applicable, home health personnel is essential for coordinating follow-up care, reinforcing preventive strategies, and educating patients and caregivers. Ethical, patient-centered care emphasizes prevention, early recognition of complications, and shared decision-making, particularly in high-risk populations. Through coordinated care, vigilant catheter management, patient education, and timely specialist involvement, the interprofessional healthcare team can significantly reduce the risk of preventable bladder stone formation, improve long-term outcomes, and enhance overall team performance.
Media
(Click Image to Enlarge)

A Bladder Calculus. The image shows a bladder calculus (cystolith), a mineralized mass that typically forms when urinary stasis leads to the supersaturation and precipitation of crystals, often secondary to underlying conditions such as bladder outlet obstruction or chronic infection.
Contributed by S Munakomi, MD
(Click Image to Enlarge)
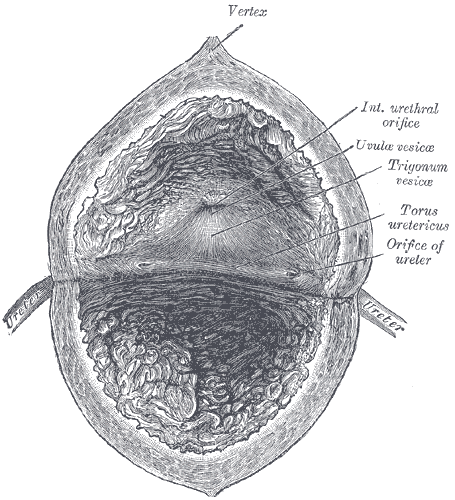
Interior Anatomy of the Urinary Bladder. The image shows the interior of the bladder, including the vertex, internal urethral orifice, uvula vesicae, torus ureteric, and the orifice of the ureter.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
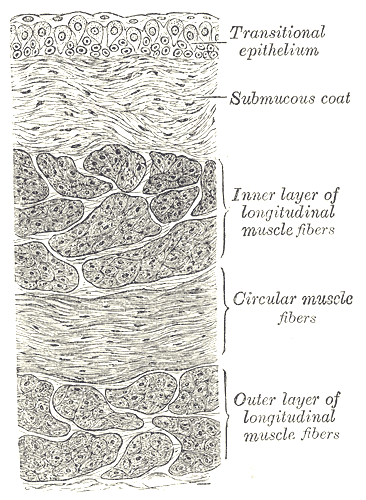
Vertical Section of the Urinary Bladder Wall. The image shows the anatomical features of the urinary bladder wall, including the transitional epithelium, submucous coat, inner layer of longitudinal muscle fibers, circular muscle fibers, and outer layer of longitudinal muscle fibers.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)

Computed Tomography Scan of the Pelvis. A CT scan image of the pelvis in a 65-year-old male patient shows multiple bladder stones with benign prostatic hyperplasia.
Contributed by PJ Shenot, MD
References
Nevo A, Moore JP, Humphreys MR, Salih S, Keddis MA, Rose KM, Cheney SS, Stern KL. Does bladder stone composition predict kidney stone composition? The Canadian journal of urology. 2020 Dec:27(6):10450-10455 [PubMed PMID: 33325347]
Schwartz BF, Stoller ML. The vesical calculus. The Urologic clinics of North America. 2000 May:27(2):333-46 [PubMed PMID: 10778475]
Takasaki E, Suzuki T, Honda M, Imai T, Maeda S, Hosoya Y. Chemical compositions of 300 lower urinary tract calculi and associated disorders in the urinary tract. Urologia internationalis. 1995:54(2):89-94 [PubMed PMID: 7538235]
López M, Hoppe B. History, epidemiology and regional diversities of urolithiasis. Pediatric nephrology (Berlin, Germany). 2010 Jan:25(1):49-59. doi: 10.1007/s00467-008-0960-5. Epub [PubMed PMID: 21476230]
Lu J, Gao W, Fei C, Liao W, Hou G, Lin Y, Rao W, Yang Q, Sui X. Associated factors for benign prostatic hyperplasia in patients with bladder calculi. Urologia. 2025 Aug:92(3):406-414. doi: 10.1177/03915603251318869. Epub 2025 Feb 20 [PubMed PMID: 39980325]
Douenias R, Rich M, Badlani G, Mazor D, Smith A. Predisposing factors in bladder calculi. Review of 100 cases. Urology. 1991 Mar:37(3):240-3 [PubMed PMID: 2000681]
Level 3 (low-level) evidenceHalstead SB. Epidemiology of bladder stone of children: precipitating events. Urolithiasis. 2016 Apr:44(2):101-8. doi: 10.1007/s00240-015-0835-8. Epub 2015 Nov 11 [PubMed PMID: 26559057]
Soliman NA, Rizvi SAH. Endemic bladder calculi in children. Pediatric nephrology (Berlin, Germany). 2017 Sep:32(9):1489-1499. doi: 10.1007/s00467-016-3492-4. Epub 2016 Nov 15 [PubMed PMID: 27848095]
Rauturier C, Machon C, Demède D, Dubourg L, Bacchetta J, Bertholet-Thomas A. Composition of urinary stones in children: clinical and metabolic determinants in a French tertiary care center. European journal of pediatrics. 2021 Dec:180(12):3555-3563. doi: 10.1007/s00431-021-04151-7. Epub 2021 Jun 24 [PubMed PMID: 34165592]
Donaldson JF, Ruhayel Y, Skolarikos A, MacLennan S, Yuan Y, Shepherd R, Thomas K, Seitz C, Petrik A, Türk C, Neisius A. Treatment of Bladder Stones in Adults and Children: A Systematic Review and Meta-analysis on Behalf of the European Association of Urology Urolithiasis Guideline Panel. European urology. 2019 Sep:76(3):352-367. doi: 10.1016/j.eururo.2019.06.018. Epub 2019 Jul 13 [PubMed PMID: 31311676]
Level 1 (high-level) evidenceRobertson WG. Renal stones in the tropics. Seminars in nephrology. 2003 Jan:23(1):77-87 [PubMed PMID: 12563603]
ANDERSEN DA. The nutritional significance of primary bladder stones. British journal of urology. 1962 Jun:34():160-77 [PubMed PMID: 13861160]
Sayasone S, Odermatt P, Khammanivong K, Phomluangsyl S, Vinhl CV, Thin HM, Strobeli M. Bladder stones in childhood: a descriptive study in a rural setting in Saravan Province, Lao PDR. The Southeast Asian journal of tropical medicine and public health. 2004:35 Suppl 2():50-2 [PubMed PMID: 15906634]
Childs MA, Mynderse LA, Rangel LJ, Wilson TM, Lingeman JE, Krambeck AE. Pathogenesis of bladder calculi in the presence of urinary stasis. The Journal of urology. 2013 Apr:189(4):1347-51. doi: 10.1016/j.juro.2012.11.079. Epub 2012 Nov 15 [PubMed PMID: 23159588]
Jung JH, Park J, Kim WT, Kim HW, Kim HJ, Hong S, Yang HJ, Chung H. The association of benign prostatic hyperplasia with lower urinary tract stones in adult men: A retrospective multicenter study. Asian journal of urology. 2018 Apr:5(2):118-121. doi: 10.1016/j.ajur.2017.06.008. Epub 2017 Jun 20 [PubMed PMID: 29736374]
Level 2 (mid-level) evidenceHuang W, Cao JJ, Cao M, Wu HS, Yang YY, Xu ZM, Jin XD. Risk factors for bladder calculi in patients with benign prostatic hyperplasia. Medicine. 2017 Aug:96(32):e7728. doi: 10.1097/MD.0000000000007728. Epub [PubMed PMID: 28796057]
Bibi F, Ali B, Alam U, Maham Hassan V, Khan U, Ahmed S, Akram QU, Devi G, Hassan MM. From Prostate Enlargement to Bladder Stone: Large Bladder Stone as a Complication of Long-Standing BPH: A Case Study. Clinical case reports. 2025 Oct:13(10):e71264. doi: 10.1002/ccr3.71264. Epub 2025 Oct 14 [PubMed PMID: 41098196]
Level 3 (low-level) evidenceTahtalı İN, Karataş T. Giant bladder stone: A case report and review of the literature. Turkish journal of urology. 2014 Sep:40(3):189-91. doi: 10.5152/tud.2014.02603. Epub [PubMed PMID: 26328176]
Level 3 (low-level) evidenceEsposito C, Autorino G, Masieri L, Castagnetti M, Del Conte F, Coppola V, Cerulo M, Crocetto F, Escolino M. Minimally Invasive Management of Bladder Stones in Children. Frontiers in pediatrics. 2020:8():618756. doi: 10.3389/fped.2020.618756. Epub 2021 Jan 26 [PubMed PMID: 33575232]
Zafar MN, Ayub S, Tanwri H, Naqvi SAA, Rizvi SAH. Composition of urinary calculi in infants: a report from an endemic country. Urolithiasis. 2018 Oct:46(5):445-452. doi: 10.1007/s00240-017-1010-1. Epub 2017 Nov 3 [PubMed PMID: 29101428]
Meiouet F, El Kabbaj S, Daudon M. Pediatric urolithiasis in Morocco: Composition of 432 urinary calculi analyzed by infrared spectroscopy. Progres en urologie : journal de l'Association francaise d'urologie et de la Societe francaise d'urologie. 2019 Mar:29(3):173-182. doi: 10.1016/j.purol.2019.02.002. Epub 2019 Feb 25 [PubMed PMID: 30819635]
Kamoun A, Daudon M, Abdelmoula J, Hamzaoui M, Chaouachi B, Houissa T, Zghal A, Ben Ammar S, Belkahia C, Lakhoua R. Urolithiasis in Tunisian children: a study of 120 cases based on stone composition. Pediatric nephrology (Berlin, Germany). 1999 Nov:13(9):920-5; discussion 926 [PubMed PMID: 10603149]
Level 3 (low-level) evidenceErinmez M, Ozturk M. Urinary Tract Infection in Patients with Urolithiasis: A Large Retrospective Observational Study of Clinical Features and Microbiological Spectrum. Pathogens (Basel, Switzerland). 2026 Jan 16:15(1):. doi: 10.3390/pathogens15010098. Epub 2026 Jan 16 [PubMed PMID: 41599082]
Level 2 (mid-level) evidenceRipa F, Pietropaolo A, Montanari E, Hameed BMZ, Gauhar V, Somani BK. Association of Kidney Stones and Recurrent UTIs: the Chicken and Egg Situation. A Systematic Review of Literature. Current urology reports. 2022 Sep:23(9):165-174. doi: 10.1007/s11934-022-01103-y. Epub 2022 Jul 25 [PubMed PMID: 35877059]
Level 1 (high-level) evidenceSmith JM, O'Flynn JD. Vesical stone: The clinical features of 652 cases. Irish medical journal. 1975 Feb 22:68(4):85-9 [PubMed PMID: 1112692]
Level 3 (low-level) evidenceKrambeck AE, Handa SE, Lingeman JE. Experience with more than 1,000 holmium laser prostate enucleations for benign prostatic hyperplasia. The Journal of urology. 2010 Mar:183(3):1105-9. doi: 10.1016/j.juro.2009.11.034. Epub 2010 Jan 21 [PubMed PMID: 20092844]
Mebust WK, Holtgrewe HL, Cockett AT, Peters PC. Transurethral prostatectomy: immediate and postoperative complications. a cooperative study of 13 participating institutions evaluating 3,885 patients. 1989. The Journal of urology. 2002 Feb:167(2 Pt 2):999-1003; discussion 1004 [PubMed PMID: 11908420]
Abelson B, Sun D, Que L, Nebel RA, Baker D, Popiel P, Amundsen CL, Chai T, Close C, DiSanto M, Fraser MO, Kielb SJ, Kuchel G, Mueller ER, Palmer MH, Parker-Autry C, Wolfe AJ, Damaser MS. Sex differences in lower urinary tract biology and physiology. Biology of sex differences. 2018 Oct 22:9(1):45. doi: 10.1186/s13293-018-0204-8. Epub 2018 Oct 22 [PubMed PMID: 30343668]
Kim JW, Oh MM, Park HS, Cheon J, Lee JG, Kim JJ, Moon du G. Intravesical prostatic protrusion is a risk factor for bladder stone in patients with benign prostatic hyperplasia. Urology. 2014 Nov:84(5):1026-9. doi: 10.1016/j.urology.2014.06.038. Epub 2014 Sep 8 [PubMed PMID: 25214201]
Husmann DA. Long-term complications following bladder augmentations in patients with spina bifida: bladder calculi, perforation of the augmented bladder and upper tract deterioration. Translational andrology and urology. 2016 Feb:5(1):3-11. doi: 10.3978/j.issn.2223-4683.2015.12.06. Epub [PubMed PMID: 26904407]
Romero-Otero J, García-Gómez B, García-González L, García-Rojo E, Abad-López P, Justo-Quintas J, Duarte-Ojeda J, Rodríguez-Antolín A. Critical analysis of a multicentric experience with holmium laser enucleation of the prostate for benign prostatic hyperplasia: outcomes and complications of 10 years of routine clinical practice. BJU international. 2020 Jul:126(1):177-182. doi: 10.1111/bju.15028. Epub 2020 Feb 27 [PubMed PMID: 32020749]
Schlomer BJ, Copp HL. Cumulative incidence of outcomes and urologic procedures after augmentation cystoplasty. Journal of pediatric urology. 2014 Dec:10(6):1043-50. doi: 10.1016/j.jpurol.2014.03.007. Epub 2014 Apr 13 [PubMed PMID: 24766857]
Szymanski KM, Misseri R, Whittam B, Hollowell N, Hardacker RE, Swenson CR, Kaefer M, Rink RC, Cain MP. Additional Surgeries after Bladder Augmentation in Patients with Spina Bifida in the 21st Century. The Journal of urology. 2020 Jun:203(6):1207-1213. doi: 10.1097/JU.0000000000000751. Epub 2020 Jan 17 [PubMed PMID: 31951496]
Szymanski KM, Misseri R, Whittam B, Amstutz S, Kaefer M, Rink RC, Cain MP. Cutting for stone in augmented bladders-what is the risk of recurrence and is it impacted by treatment modality? The Journal of urology. 2014 May:191(5):1375-80. doi: 10.1016/j.juro.2013.11.057. Epub 2013 Dec 5 [PubMed PMID: 24316089]
Terai A, Arai Y, Kawakita M, Okada Y, Yoshida O. Effect of urinary intestinal diversion on urinary risk factors for urolithiasis. The Journal of urology. 1995 Jan:153(1):37-41 [PubMed PMID: 7966785]
Terai A, Ueda T, Kakehi Y, Terachi T, Arai Y, Okada Y, Yoshida O. Urinary calculi as a late complication of the Indiana continent urinary diversion: comparison with the Kock pouch procedure. The Journal of urology. 1996 Jan:155(1):66-8 [PubMed PMID: 7490900]
N'Dow J, Pearson J, Neal D. Mucus production after transposition of intestinal segments into the urinary tract. World journal of urology. 2004 Sep:22(3):178-85 [PubMed PMID: 15290207]
Blyth B, Ewalt DH, Duckett JW, Snyder HM 3rd. Lithogenic properties of enterocystoplasty. The Journal of urology. 1992 Aug:148(2 Pt 2):575-7; discussion 578-9 [PubMed PMID: 1640525]
Welk B, Herschorn S, Law C, Nam R. Population based assessment of enterocystoplasty complications in adults. The Journal of urology. 2012 Aug:188(2):464-9. doi: 10.1016/j.juro.2012.04.013. Epub 2012 Jun 14 [PubMed PMID: 22704106]
Metcalfe PD, Cain MP, Kaefer M, Gilley DA, Meldrum KK, Misseri R, King SJ, Casale AJ, Rink RC. What is the need for additional bladder surgery after bladder augmentation in childhood? The Journal of urology. 2006 Oct:176(4 Pt 2):1801-5; discussion 1805 [PubMed PMID: 16945653]
Kronner KM, Casale AJ, Cain MP, Zerin MJ, Keating MA, Rink RC. Bladder calculi in the pediatric augmented bladder. The Journal of urology. 1998 Sep:160(3 Pt 2):1096-8; discussion 1103 [PubMed PMID: 9719284]
Palmer LS, Franco I, Kogan SJ, Reda E, Gill B, Levitt SB. Urolithiasis in children following augmentation cystoplasty. The Journal of urology. 1993 Aug:150(2 Pt 2):726-9 [PubMed PMID: 8326634]
Clayman RV. Preventing reservoir calculi after augmentation cystoplasty and continent urinary diversion: the influence of an irrigation protocol. The Journal of urology. 2005 Mar:173(3):866-7 [PubMed PMID: 15711295]
Mathoera RB, Kok DJ, Nijman RJ. Bladder calculi in augmentation cystoplasty in children. Urology. 2000 Sep 1:56(3):482-7 [PubMed PMID: 10962320]
DeFoor W, Minevich E, Reddy P, Sekhon D, Polsky E, Wacksman J, Sheldon C. Bladder calculi after augmentation cystoplasty: risk factors and prevention strategies. The Journal of urology. 2004 Nov:172(5 Pt 1):1964-6 [PubMed PMID: 15540766]
Maxon V, Haffar A, Michel CA, Hirsch AM, Robey C, Heap D, Galansky L, Gearhart J, Di Carlo H, Crigger CB. A Rocky Road: Bladder Stones in the Augmented Exstrophy-Epispadias Complex Patient. Urology. 2024 Oct:192():100-104. doi: 10.1016/j.urology.2024.07.001. Epub 2024 Jul 8 [PubMed PMID: 38986957]
López Cubillana P, Gómez Gómez G, Ruiz Gómez JM, Prieto González A, Asensio Egea LJ, Rigabert Montiel M, Nicolás Torralba JA, Bañón Pérez V, Server Pastor G, Pérez Albacete M. [Incidence and risk factors for calculi formation in patients treated with augmentation cystoplasty or intestinal substitution]. Archivos espanoles de urologia. 1998 May:51(4):347-52 [PubMed PMID: 9656556]
van den Heijkant M, Haider N, Taylor C, Subramaniam R. Efficacy of bladder irrigation and surveillance program in prevention of urinary tract infections and bladder calculi in children with an ileocystoplasty and bladder neck repair. Pediatric surgery international. 2011 Jul:27(7):781-5. doi: 10.1007/s00383-011-2913-5. Epub 2011 May 8 [PubMed PMID: 21553274]
Hensle TW, Bingham J, Lam J, Shabsigh A. Preventing reservoir calculi after augmentation cystoplasty and continent urinary diversion: the influence of an irrigation protocol. BJU international. 2004 Mar:93(4):585-7 [PubMed PMID: 15008735]
Caponegro PJ, Leadbetter GW Jr. Acute ureteral obstruction secondary to mucoid impaction in supravesical diversion. Treatment with N-acetylcysteine. Urology. 1974 Apr:3(4):486-7 [PubMed PMID: 4822699]
Benderev TV. Acetylcysteine for urinary tract mucolysis. The Journal of urology. 1988 Feb:139(2):353-4 [PubMed PMID: 3339742]
Gillon G, Mundy AR. The dissolution of urinary mucus after cystoplasty. British journal of urology. 1989 Apr:63(4):372-4 [PubMed PMID: 2713619]
Schrier BP, Lichtendonk WJ, Witjes JA. The effect of N-acetyl-L-cysteine on the viscosity of ileal neobladder mucus. World journal of urology. 2002 May:20(1):64-7 [PubMed PMID: 12088194]
Covert WM, Westin SN, Soliman PT, Langley GD. The role of mucoregulatory agents after continence-preserving urinary diversion surgery. American journal of health-system pharmacy : AJHP : official journal of the American Society of Health-System Pharmacists. 2012 Mar 15:69(6):483-6. doi: 10.2146/ajhp110212. Epub [PubMed PMID: 22382478]
Khoury AE, Salomon M, Doche R, Soboh F, Ackerley C, Jayanthi R, McLorie GA, Mittelman MW. Stone formation after augmentation cystoplasty: the role of intestinal mucus. The Journal of urology. 1997 Sep:158(3 Pt 2):1133-7 [PubMed PMID: 9258156]
Woodhouse CR, Robertson WG. Urolithiasis in enterocystoplasties. World journal of urology. 2004 Sep:22(3):215-21 [PubMed PMID: 15349748]
Ong K, Murtagh K. Large bladder stones in an augmented bladder - An open approach to a big problem. Urology case reports. 2023 Sep:50():102536. doi: 10.1016/j.eucr.2023.102536. Epub 2023 Aug 17 [PubMed PMID: 37621389]
Level 3 (low-level) evidenceKobayashi K, Goel A, Coelho MP, Medina Perez M, Klumpp M, Tewari SO, Appleton-Figueira T, Pinter DJ, Shapiro O, Jawed M. Complications of Ileal Conduits after Radical Cystectomy: Interventional Radiologic Management. Radiographics : a review publication of the Radiological Society of North America, Inc. 2021 Jan-Feb:41(1):249-267. doi: 10.1148/rg.2021200067. Epub 2020 Dec 11 [PubMed PMID: 33306453]
Kihara C, Patel AN, Oakley K, Gay C, Stolzenberg L, Seale J. The Incidental Discovery of an Ileal Conduit Calculus: A Case Report. Cureus. 2023 Aug:15(8):e43299. doi: 10.7759/cureus.43299. Epub 2023 Aug 10 [PubMed PMID: 37692572]
Level 3 (low-level) evidenceNg AC, Leung AK, Robson WL. Urinary bladder calculi in a sliding vesical-inguinal-scrotal hernia diagnosed preoperatively by plain abdominal radiography. Advances in therapy. 2007 Sep-Oct:24(5):1016-9 [PubMed PMID: 18029327]
Level 3 (low-level) evidenceKubo N, Furusawa N, Fukai H, Terada M. A Case of One-Stage Surgical Treatment for a Bladder Hernia with Bladder Calculi. Surgical case reports. 2026:12(1):. doi: 10.70352/scrj.cr.25-0558. Epub 2026 Jan 20 [PubMed PMID: 41568082]
Level 3 (low-level) evidenceKuzaka P, Sumit S, Kuzaka B, Radziszewski P. Schistosomiasis in urology. Outline of the problem. Polski merkuriusz lekarski : organ Polskiego Towarzystwa Lekarskiego. 2025:53(2):256-266. doi: 10.36740/Merkur202502115. Epub [PubMed PMID: 40322810]
Alkhamees MA. Bladder stones in a closed diverticulum caused by Schistosoma mansoni: A case report. World journal of clinical cases. 2020 Oct 6:8(19):4475-4480. doi: 10.12998/wjcc.v8.i19.4475. Epub [PubMed PMID: 33083406]
Level 3 (low-level) evidenceKhalaf I, Shokeir A, Shalaby M. Urologic complications of genitourinary schistosomiasis. World journal of urology. 2012 Feb:30(1):31-8. doi: 10.1007/s00345-011-0751-7. Epub 2011 Sep 10 [PubMed PMID: 21909645]
Level 1 (high-level) evidenceMizuno K, Kamisawa H, Hamamoto S, Okamura T, Kohri K. Bilateral single-system ureteroceles with multiple calculi in an adult woman. Urology. 2008 Aug:72(2):294-5. doi: 10.1016/j.urology.2008.03.058. Epub 2008 Jun 4 [PubMed PMID: 18533235]
Tomaszewski JJ, Turner RM 2nd, Ost MC. Stone cobras: adult bilateral single system ureteroceles presenting with multiple calculi. Urology. 2011 Oct:78(4):782-3. doi: 10.1016/j.urology.2010.12.047. Epub 2011 Feb 18 [PubMed PMID: 21334046]
AlSary S, Al-Zahrani EF, Al Baalharith M. Vesical Calculi and Female Pelvic Organ Prolapse: A Case Report and Literature Review. Cureus. 2023 Sep:15(9):e44578. doi: 10.7759/cureus.44578. Epub 2023 Sep 2 [PubMed PMID: 37790022]
Level 3 (low-level) evidenceKomon W, Saraluck A, Viseshsindh W, Chinthakanan O. The Surgical Management of Large Bladder Calculi and Irreducible Uterine Prolapse: A Case Report and Review of Literature. Urologia internationalis. 2023:107(8):835-838. doi: 10.1159/000531523. Epub 2023 Jul 24 [PubMed PMID: 37487475]
Level 3 (low-level) evidenceThompson CD, Henderson BE, Stanley R. Bladder calculi causing irreducible urogenital prolapse. BMJ case reports. 2018 Sep 12:2018():. pii: bcr-2018-225695. doi: 10.1136/bcr-2018-225695. Epub 2018 Sep 12 [PubMed PMID: 30209144]
Level 3 (low-level) evidenceHiremath AC, K S S. Cystolitholapaxy and laparoscopic sacrocolpopexy in a case of multiple urinary bladder calculi & vault prolapse. European journal of obstetrics, gynecology, and reproductive biology. 2019 Dec:243():12-15. doi: 10.1016/j.ejogrb.2019.10.002. Epub 2019 Oct 11 [PubMed PMID: 31629924]
Level 3 (low-level) evidenceDahiya P, Gupta A, Sangwan K. Multiple bladder calculi: a rare cause of irreducible uterine prolapse. Archives of gynecology and obstetrics. 2007 May:275(5):411-2 [PubMed PMID: 17103181]
Chaudhary R, Tiwari T, Sharma R, Goyal S. Neglected pelvic viscera prolapse complicated by irreducible cystocele containing a large vesicle calculus. BMJ case reports. 2022 Mar 7:15(3):. doi: 10.1136/bcr-2021-246939. Epub 2022 Mar 7 [PubMed PMID: 35256365]
Level 3 (low-level) evidenceEkenci BY, Erkartal AS, Kokurcan A, Sari H, Karakoyunlu AN. Bladder Stone Formation Due to Suture Migration After Burch Colposuspension: A Case Report. Cureus. 2026 Jan:18(1):e101020. doi: 10.7759/cureus.101020. Epub 2026 Jan 7 [PubMed PMID: 41658632]
Level 3 (low-level) evidenceŞam E, Atar M, Alemdar E, Turan A, Karabulut İ. Bladder Stone Formation due to Intravesical Migration of the Intrauterine Device: A Report of 2 Cases. Urologia internationalis. 2024:108(3):272-275. doi: 10.1159/000537931. Epub 2024 Feb 20 [PubMed PMID: 38377979]
Level 3 (low-level) evidenceMartin-Dorantes MA, Rochel-Perez EA, Bastarrachea-Solis MA, Flores-Tapia JP, Sotelo-Casas AY, Méndez-Domínguez N. Bladder Stone Secondary to Migration of an Intrauterine Device: A Case Report. Clinical case reports. 2026 Apr:14(4):e72566. doi: 10.1002/ccr3.72566. Epub 2026 Apr 12 [PubMed PMID: 41982856]
Level 3 (low-level) evidenceSoni JS, Kumar S, Rathore JS, Bhirud DP. From contraception to calculus: copper-T migration resulting in vesical calculus formation. BMJ case reports. 2025 Jun 12:18(6):. pii: e266448. doi: 10.1136/bcr-2025-266448. Epub 2025 Jun 12 [PubMed PMID: 40506108]
Level 3 (low-level) evidenceMalki EG, Sbeih D, Bael P, Alsarabta H, Alzawahra A. The rolling stone: migration of an intrauterine device leading to bladder stone formation nine years after insertion: a case report. BMC urology. 2025 Apr 17:25(1):93. doi: 10.1186/s12894-025-01780-0. Epub 2025 Apr 17 [PubMed PMID: 40247326]
Level 3 (low-level) evidenceHuang WY, Kwan KJS, Tang D, Xiong L. A Forgotten Double-J Ureteric Stent as the Core of a Bladder Stone: A Case Report and Literature Review. The American journal of case reports. 2024 May 31:25():e943781. doi: 10.12659/AJCR.943781. Epub 2024 May 31 [PubMed PMID: 38816969]
Level 3 (low-level) evidenceFatahajjad HH, Ompusunggu RA, Laksita TB, Soebadi MA. Multiple lower urinary tract calculi induced by foreign bodies insertion: A case report. Radiology case reports. 2024 Jun:19(6):2443-2447. doi: 10.1016/j.radcr.2024.02.100. Epub 2024 Mar 28 [PubMed PMID: 38585402]
Level 3 (low-level) evidenceGazzah W, Mansi Z, Zaidi B. Contraceptive complication: Emergence of a bladder stone - A case report. International journal of surgery case reports. 2024 May:118():109622. doi: 10.1016/j.ijscr.2024.109622. Epub 2024 Apr 6 [PubMed PMID: 38615469]
Level 3 (low-level) evidenceAziz el M, Amrani M, Abdelhak K, Hassan FM. A fragment of Foley catheter balloon as a cause of Bladder stone in woman. The Pan African medical journal. 2015:21():284. doi: 10.11604/pamj.2015.21.284.6770. Epub 2015 Aug 13 [PubMed PMID: 26587134]
Prihadi JC, Hengky A, Ongga L. Cable Wire as a Nidus for Vesicolithiasis: A Case Report. Research and reports in urology. 2025:17():153-157. doi: 10.2147/RRU.S517497. Epub 2025 May 8 [PubMed PMID: 40357371]
Level 3 (low-level) evidenceMishra S. Tragedy of Inappropriately Managed Foley Catheter. Journal of obstetrics and gynaecology of India. 2016 Oct:66(Suppl 2):679-682 [PubMed PMID: 27803543]
Chrisp JM, Nacey JN. Foley catheter balloon puncture and the risk of free fragment formation. British journal of urology. 1990 Nov:66(5):500-2 [PubMed PMID: 2249119]
Khalid A, Abdulwahab-Ahmed A, Muhammad AS, Jesini G, Agwu NP, Mungadi IA. An enigma: case series of vesical calculi from prolonged and neglected indwelling catheter. Journal of surgical case reports. 2023 Jan:2023(1):rjad018. doi: 10.1093/jscr/rjad018. Epub 2023 Jan 31 [PubMed PMID: 36741079]
Level 2 (mid-level) evidenceLi S, Zhao S, Zhang Y, Zhang B. Bladder Erosion and stone formation: a rare complication of laparoscopic cervical cerclage. BMC women's health. 2025 Jul 5:25(1):329. doi: 10.1186/s12905-025-03873-2. Epub 2025 Jul 5 [PubMed PMID: 40618156]
Chaabouni A, Samet A, Fourati M, Harbi H, Amine Mseddi M, Hadjslimene M. A bladder stone surrounding a foreign body: A rare case. Urology case reports. 2022 Jan:40():101943. doi: 10.1016/j.eucr.2021.101943. Epub 2021 Nov 11 [PubMed PMID: 34824980]
Level 3 (low-level) evidenceKamisawa K, Kosaka T, Hongo H, Mizuno R, Oya M. Brachytherapy seeds as a nidus for urethral stone formation: A case report. IJU case reports. 2019 Jul:2(4):206-208. doi: 10.1002/iju5.12082. Epub 2019 May 22 [PubMed PMID: 32743414]
Level 3 (low-level) evidenceMahdavi A, Mostafavi H. Hanging Bladder calculi Secondary to Misplaced Surgical Suture. Iranian journal of radiology : a quarterly journal published by the Iranian Radiological Society. 2015 Apr:12(2):e11303. doi: 10.5812/iranjradiol.11303. Epub 2015 Apr 15 [PubMed PMID: 26060550]
Fauzi MF, Djojodimedjo T, Renaldo J. Neglected double-J stent presenting as giant bladder and ureteral stone: A case report. Radiology case reports. 2024 Nov:19(11):5216-5220. doi: 10.1016/j.radcr.2024.07.148. Epub 2024 Aug 24 [PubMed PMID: 39263508]
Level 3 (low-level) evidenceWu CC, Hsieh ML, Wang TM. Retained vaginal gauze with unusual complication: a case report. Changgeng yi xue za zhi. 1997 Mar:20(1):62-5 [PubMed PMID: 9178596]
Level 3 (low-level) evidencePerz S, Ellimoottil C, Rao M, Bresler L. A unique complication of urethral catheterization: pubic hair associated with struvite bladder calculi. Urologic nursing. 2013 Sep-Oct:33(5):233-5 [PubMed PMID: 24354112]
Jaziri Y, Saidani B, Saadi A, Haroun A, Chakroun M, Ben Slama R. Intrauterine device migration into the bladder with urolithiasis: A case report. International journal of surgery case reports. 2025 Jun:131():111409. doi: 10.1016/j.ijscr.2025.111409. Epub 2025 May 10 [PubMed PMID: 40349496]
Level 3 (low-level) evidenceAhmad J, Omran A, Aqel S, Khalil IA, Alkabbani M, Alobaidy A, Al-Ansari AA. Migrated Hem-o-lok clip in the bladder: A rare cause of bladder stone for cystolitholapaxy. Urology case reports. 2023 Sep:50():102534. doi: 10.1016/j.eucr.2023.102534. Epub 2023 Aug 16 [PubMed PMID: 37681116]
Level 3 (low-level) evidenceSharma UK, Rauniyar D, Shah WF. Intravesical foreign body: case report. Kathmandu University medical journal (KUMJ). 2006 Jul-Sep:4(3):342-4 [PubMed PMID: 18603932]
Level 3 (low-level) evidenceIrekpita E, Imomoh P, Kesieme E, Onuora V. Intravesical foreign bodies: a case report and a review of the literature. International medical case reports journal. 2011:4():35-9. doi: 10.2147/IMCRJ.S18857. Epub 2011 May 3 [PubMed PMID: 23754903]
Level 3 (low-level) evidenceRafique M. Intravesical foreign bodies: review and current management strategies. Urology journal. 2008 Fall:5(4):223-31 [PubMed PMID: 19101894]
Ratkal JM, Raykar R, Shirol SS. Electric Wire as Foreign Body in the Bladder and Urethra-a Case Report and Review of Literature. The Indian journal of surgery. 2015 Dec:77(Suppl 3):1323-5. doi: 10.1007/s12262-014-1162-y. Epub 2014 Sep 12 [PubMed PMID: 27011559]
Level 3 (low-level) evidenceOgbetere FE, Irekpita E. A Self-Insertion of an Uncommon Urethrovesical Foreign Body for Autoerotism. Nigerian journal of surgery : official publication of the Nigerian Surgical Research Society. 2021 Jan-Jun:27(1):81-83. doi: 10.4103/njs.NJS_6_20. Epub 2021 Mar 9 [PubMed PMID: 34012250]
Dick WH, Lingeman JE, Preminger GM, Smith LH, Wilson DM, Shirrell WL. Laxative abuse as a cause for ammonium urate renal calculi. The Journal of urology. 1990 Feb:143(2):244-7 [PubMed PMID: 2299711]
Kato Y, Hou K, Saga Y, Yamaguchi S, Yachiku S, Kawakami N. [Ammonium acid urate stone due to laxative abuse: a case report]. Hinyokika kiyo. Acta urologica Japonica. 2004 Nov:50(11):799-803 [PubMed PMID: 15628542]
Level 3 (low-level) evidenceSoble JJ, Hamilton BD, Streem SB. Ammonium acid urate calculi: a reevaluation of risk factors. The Journal of urology. 1999 Mar:161(3):869-73 [PubMed PMID: 10022703]
Zhang W, Shen R, Shang Z, Wang Z, Yu Y, Zhang K, Yang Y, Pang M. Incidence of and Risk Factors for Urinary Stones Among Patients with Spinal Cord Injury: A Systematic Review with Meta-analysis. European urology open science. 2024 Dec:70():79-85. doi: 10.1016/j.euros.2024.10.003. Epub 2024 Oct 22 [PubMed PMID: 39507510]
Level 1 (high-level) evidenceOrd J, Lunn D, Reynard J. Bladder management and risk of bladder stone formation in spinal cord injured patients. The Journal of urology. 2003 Nov:170(5):1734-7 [PubMed PMID: 14532765]
Bartel P, Krebs J, Wöllner J, Göcking K, Pannek J. Bladder stones in patients with spinal cord injury: a long-term study. Spinal cord. 2014 Apr:52(4):295-7. doi: 10.1038/sc.2014.1. Epub 2014 Jan 28 [PubMed PMID: 24469146]
DeVivo MJ, Fine PR, Cutter GR, Maetz HM. The risk of bladder calculi in patients with spinal cord injuries. Archives of internal medicine. 1985 Mar:145(3):428-30 [PubMed PMID: 3977510]
Möhr S, Fassbind S, Gahl B, Seifert HH, Bausch K. Risk factors of bladder stones in neurogenic lower urinary tract dysfunction: A real-world study. BJUI compass. 2024 Mar:5(3):359-365. doi: 10.1002/bco2.330. Epub 2024 Feb 1 [PubMed PMID: 38481672]
Linsenmeyer MA, Linsenmeyer TA. Accuracy of predicting bladder stones based on catheter encrustation in individuals with spinal cord injury. The journal of spinal cord medicine. 2006:29(4):402-5 [PubMed PMID: 17044391]
Burr RG, Chem C, Nuseibeh I. Creatinine, calcium, citrate and acid-base in spinal cord injured patients. Paraplegia. 1993 Nov:31(11):742-50 [PubMed PMID: 8295783]
Lai EC, Kao Yang YH, Kuo HC. Complication rate of neurogenic lower urinary tract dysfunction after spinal cord injury in Taiwan. International urology and nephrology. 2014 Jun:46(6):1063-71. doi: 10.1007/s11255-013-0625-6. Epub 2013 Dec 18 [PubMed PMID: 24346963]
Linsenmeyer TA. Catheter-associated urinary tract infections in persons with neurogenic bladders. The journal of spinal cord medicine. 2018 Mar:41(2):132-141. doi: 10.1080/10790268.2017.1415419. Epub 2018 Jan 11 [PubMed PMID: 29323625]
Szczerbiec D, Słaba M, Torzewska A. Substances Secreted by Lactobacillus spp. from the Urinary Tract Microbiota Play a Protective Role against Proteus mirabilis Infections and Their Complications. International journal of molecular sciences. 2023 Dec 20:25(1):. doi: 10.3390/ijms25010103. Epub 2023 Dec 20 [PubMed PMID: 38203274]
Hiya U, Endo M, Okada K, Takahashi S, Ogawa K, Nakagawa M, Nakamura M, Shibayama C, Fukuda Y, Akahane K, Kawahara M, Mori H, Shirai K. Asymptomatic Bladder Stones Exacerbate Acute Genitourinary Adverse Events During Radiation Therapy for Prostate Cancer: Insights From Two Case Reports. Advances in radiation oncology. 2025 Aug:10(8):101833. doi: 10.1016/j.adro.2025.101833. Epub 2025 Jun 11 [PubMed PMID: 40686744]
Level 3 (low-level) evidenceHird AE, Saskin R, Liu Y, Lee Y, Ajib K, Matta R, Kodama R, Carr L, Kulkarni GS, Herschorn S, Narod SA, Nam RK. Association between chronic bladder catheterisation and bladder cancer incidence and mortality: a population-based retrospective cohort study in Ontario, Canada. BMJ open. 2021 Sep 2:11(9):e050728. doi: 10.1136/bmjopen-2021-050728. Epub 2021 Sep 2 [PubMed PMID: 34475180]
Level 2 (mid-level) evidenceMatlaga BR, Shah OD, Assimos DG. Drug-induced urinary calculi. Reviews in urology. 2003 Fall:5(4):227-31 [PubMed PMID: 16985842]
Lal B, Paryani JP, Memon SU. CHILDHOOD BLADDER STONES-AN ENDEMIC DISEASE OF DEVELOPING COUNTRIES. Journal of Ayub Medical College, Abbottabad : JAMC. 2015 Jan-Mar:27(1):17-21 [PubMed PMID: 26182729]
Sharma AP, Filler G. Epidemiology of pediatric urolithiasis. Indian journal of urology : IJU : journal of the Urological Society of India. 2010 Oct:26(4):516-22. doi: 10.4103/0970-1591.74450. Epub [PubMed PMID: 21369384]
Pięta J, Szyszka M, Lipiński P, Skrzypczyk P. Urolithiasis in Children-Clinical Picture, Pathogenesis, and Diagnostic Approach. Biomolecules. 2026 Jan 9:16(1):. doi: 10.3390/biom16010119. Epub 2026 Jan 9 [PubMed PMID: 41594659]
Önal B, Kırlı EA. Pediatric stone disease: Current management and future concepts. Turkish archives of pediatrics. 2021 Mar:56(2):99-107. doi: 10.5152/TurkArchPediatr.2021.20273. Epub 2021 Feb 3 [PubMed PMID: 34286317]
Juliebø-Jones P, Ulvik Ø, Æsøy MS, Gjengstø P, Beisland C, Somani BK. Mortality due to urolithiasis in England and Wales: updated findings from a national database over a 23-year period. Central European journal of urology. 2023:76(2):141-143. doi: 10.5173/ceju.2023.054. Epub 2023 May 12 [PubMed PMID: 37483861]
Kum F, Mahmalji W, Hale J, Thomas K, Bultitude M, Glass J. Do stones still kill? An analysis of death from stone disease 1999-2013 in England and Wales. BJU international. 2016 Jul:118(1):140-4. doi: 10.1111/bju.13409. Epub 2016 Feb 12 [PubMed PMID: 26765522]
Firasi AA, Soebadi MA, Himawan B, Diarsvitri W. Age, Benign Prostatic Hyperplasia, Geography of Residence, and Occupation are Predictors of Bladder Calculi in Men: A Three-Year Data Analysis. Archivos espanoles de urologia. 2023 Mar:76(2):145-151. doi: 10.56434/j.arch.esp.urol.20237602.16. Epub [PubMed PMID: 37139620]
Mosa MM, Alsayed-Ahmad ZA, Razzouk Q, Alhmaidy O, Ismaeel H, Al Ahmad Y. Extraction of a giant bladder stone (560 g) in a young female: A case report. International journal of surgery case reports. 2024 Jun:119():109653. doi: 10.1016/j.ijscr.2024.109653. Epub 2024 Apr 20 [PubMed PMID: 38678989]
Level 3 (low-level) evidenceBecher RM, Tolia BM, Newman HR. Giant vesical calculus. JAMA. 1978 May 26:239(21):2272-3 [PubMed PMID: 650809]
Komeya M, Sahoda T, Sugiura S, Sawada T, Kitami K. A huge bladder calculus causing acute renal failure. Urolithiasis. 2013 Feb:41(1):85-7. doi: 10.1007/s00240-012-0517-8. Epub 2012 Dec 21 [PubMed PMID: 23532429]
Wei W, Wang J. A huge bladder calculus causing acute renal failure. Urological research. 2010 Aug:38(4):231-2. doi: 10.1007/s00240-009-0246-9. Epub 2009 Dec 22 [PubMed PMID: 20033143]
Celik O, Suelozgen T, Budak S, Ilbey YO. Post-renal acute renal failure due to a huge bladder stone. Archivio italiano di urologia, andrologia : organo ufficiale [di] Societa italiana di ecografia urologica e nefrologica. 2014 Jun 30:86(2):146-7. doi: 10.4081/aiua.2014.2.146. Epub 2014 Jun 30 [PubMed PMID: 25017601]
Vidhyarthy AK, Hameed T, Lal R, Kumar A, Sahni S, Mendoza N. Giant Bladder Calculus in an Adult- A Persistent Problem in the Developing World: A Case Report. Clinical practice and cases in emergency medicine. 2020 Nov:4(4):544-547. doi: 10.5811/cpcem.2020.7.47653. Epub [PubMed PMID: 33217268]
Level 3 (low-level) evidenceKumar S, Jayant K. Massive vesical calculi formation as a complication of augmentation cystoplasty. Nephro-urology monthly. 2015 Jan:7(1):e22297. doi: 10.5812/numonthly.22297. Epub 2014 Nov 15 [PubMed PMID: 25738119]
Minter J, Chiovaro J. Renal failure with a large bladder calculus related to a foreign body: a case report. Clinical case reports. 2014 Apr:2(2):48-50. doi: 10.1002/ccr3.52. Epub 2014 Mar 3 [PubMed PMID: 25356243]
Level 3 (low-level) evidenceJoshi A, Prasai P, Phuyal MP, Rokaya P, Paudyal P. Giant Vesicle Calculus Presenting With Azotemia and Hydroureteronephrosis: A Case Report. Clinical case reports. 2025 Apr:13(4):e70358. doi: 10.1002/ccr3.70358. Epub 2025 Mar 24 [PubMed PMID: 40134961]
Level 3 (low-level) evidenceWhittington JR, Simmons PM, Eltahawy EA, Magann EF. Bladder Stone in Pregnancy: A Case Report and Review of the Literature. The American journal of case reports. 2018 Dec 30:19():1546-1549. doi: 10.12659/AJCR.912614. Epub 2018 Dec 30 [PubMed PMID: 30594944]
Level 3 (low-level) evidencePais VM Jr, Payton AL, LaGrange CA. Urolithiasis in pregnancy. The Urologic clinics of North America. 2007 Feb:34(1):43-52 [PubMed PMID: 17145360]
COPE E. Obstructed labour due to vesical calculus. The Journal of obstetrics and gynaecology of the British Commonwealth. 1961 Jun:68():476-8 [PubMed PMID: 13695352]
Rai L, Ramesh K. Obstructed labour due to a vesical calculus. The Australian & New Zealand journal of obstetrics & gynaecology. 1998 Nov:38(4):474 [PubMed PMID: 9890239]
Keepanasseril A, Nanjappa B, Prasad GV, Saha SC, Mandal AK. Vesical calculus: an unusual cause of labour dystocia. Journal of obstetrics and gynaecology : the journal of the Institute of Obstetrics and Gynaecology. 2012 Aug:32(6):596-7. doi: 10.3109/01443615.2012.687022. Epub [PubMed PMID: 22779973]
Seth S, Malik S, Salhan S. Vesical calculus causing dystocia. European journal of obstetrics, gynecology, and reproductive biology. 2002 Mar 10:101(2):199-200 [PubMed PMID: 11858899]
Dave A, Mathur P, Mathuriya G. Vesical calculus: an uncommon cause of obstructed labor. Journal of obstetrics and gynaecology of India. 2012 Dec:62(6):687-8. doi: 10.1007/s13224-012-0145-9. Epub 2012 Apr 17 [PubMed PMID: 24293848]
Ait Benkaddour Y, Aboulfalah A, Abbassi H. Bladder stone: uncommon cause of mechanical dystocia. Archives of gynecology and obstetrics. 2006 Aug:274(5):323-4 [PubMed PMID: 16649039]
Akhtar J, Ahmed S, Zamir N. Management of impacted urethral stones in children. Journal of the College of Physicians and Surgeons--Pakistan : JCPSP. 2012 Aug:22(8):510-3 [PubMed PMID: 22868017]
Lyrdal F, Hofvander Y. Urinary bladder stones. Their occurrence in children in South-East Asia. Tropical doctor. 1988 Jul:18(3):102-4 [PubMed PMID: 3043853]
Naqvi SA, Rizvi SA, Shahjehan S. Bladder stone disease in children: clinical studies. JPMA. The Journal of the Pakistan Medical Association. 1984 Apr:34(4):94-101 [PubMed PMID: 6429380]
Adegeest CY, van Gent JAN, Stolwijk-Swüste JM, Post MWM, Vandertop WP, Öner FC, Peul WC, Wengel PVT. Influence of severity and level of injury on the occurrence of complications during the subacute and chronic stage of traumatic spinal cord injury: a systematic review. Journal of neurosurgery. Spine. 2022 Apr 1:36(4):632-652. doi: 10.3171/2021.7.SPINE21537. Epub 2021 Nov 12 [PubMed PMID: 34767527]
Level 1 (high-level) evidenceTrinchieri A. Epidemiology of urolithiasis: an update. Clinical cases in mineral and bone metabolism : the official journal of the Italian Society of Osteoporosis, Mineral Metabolism, and Skeletal Diseases. 2008 May:5(2):101-6 [PubMed PMID: 22460989]
Level 3 (low-level) evidenceChou YH, Huang CN, Li WM, Huang SP, Wu WJ, Tsai CC, Chang AW, Chen SM, Lin YL, Lin YP. Clinical study of ammonium acid urate urolithiasis. The Kaohsiung journal of medical sciences. 2012 May:28(5):259-64. doi: 10.1016/j.kjms.2011.11.004. Epub 2012 Feb 22 [PubMed PMID: 22531304]
Klohn M, Bolle JF, Reverdin NP, Susini A, Baud CA, Graber P. Ammonium urate urinary stones. Urological research. 1986:14(6):315-8 [PubMed PMID: 3811079]
Dong C, Zhou J, Su X, He Z, Song Q, Song C, Ke H, Wang C, Liao W, Yang S. Understanding formation processes of calcareous nephrolithiasis in renal interstitium and tubule lumen. Journal of cellular and molecular medicine. 2024 Apr:28(7):e18235. doi: 10.1111/jcmm.18235. Epub [PubMed PMID: 38509735]
Level 3 (low-level) evidenceMeyer JL, Bergert JH, Smith LH. Epitaxial relationships in urolithiasis: the brushite-whewellite system. Clinical science and molecular medicine. 1977 Feb:52(2):143-8 [PubMed PMID: 844247]
Koutsoukos PG, Lam-Erwin CY, Nancollas GH. Epitaxial considerations in urinary stone formation. I. The urate-oxalate-phosphate system. Investigative urology. 1980 Sep:18(2):178-84 [PubMed PMID: 7410035]
Ali RN, Anwaar A, Ul Haq I, Irfan S, Irfan W, Karamat RI, Akilimali A, Zafar M. Pearl in a seashell: epitaxy of solitary cystolith on the leftover curl of a double j stent - a case report. Annals of medicine and surgery (2012). 2025 Jun:87(6):3874-3879. doi: 10.1097/MS9.0000000000003248. Epub 2025 Apr 10 [PubMed PMID: 40486589]
Level 3 (low-level) evidenceHedelin H, Eddeland A, Larsson L, Pettersson S, Ohman S. The composition of catheter encrustations, including the effects of allopurinol treatment. British journal of urology. 1984 Jun:56(3):250-4 [PubMed PMID: 6399983]
Stickler D, Ganderton L, King J, Nettleton J, Winters C. Proteus mirabilis biofilms and the encrustation of urethral catheters. Urological research. 1993:21(6):407-11 [PubMed PMID: 8171763]
Mobley HL, Warren JW. Urease-positive bacteriuria and obstruction of long-term urinary catheters. Journal of clinical microbiology. 1987 Nov:25(11):2216-7 [PubMed PMID: 3320089]
Ho CC, Khandasamy Y, Singam P, Hong Goh E, Zainuddin ZM. Encrusted and incarcerated urinary bladder catheter: what are the options? The Libyan journal of medicine. 2010 Nov 25:5():. doi: 10.3402/ljm.v5i0.5686. Epub 2010 Nov 25 [PubMed PMID: 21483557]
Yassin A, Mohamed O. Long-Term Complications of Neglected Double-J Stent With Renal and Bladder Stone Formation: A Case Report From Sudan. Clinical case reports. 2025 Oct:13(10):e70995. doi: 10.1002/ccr3.70995. Epub 2025 Sep 28 [PubMed PMID: 41031275]
Level 3 (low-level) evidenceKohler-Ockmore J. Chronic urinary catheter blockage. Nursing standard (Royal College of Nursing (Great Britain) : 1987). 1991 Jul 24-30:5(44):26-8 [PubMed PMID: 1907481]
Quaranta BP, Wright ET. Jackstone Calculus. Practical radiation oncology. 2026 Mar-Apr:16(2):95-96. doi: 10.1016/j.prro.2025.10.007. Epub 2025 Nov 1 [PubMed PMID: 41183663]
Wei B, Pan Y, Gan S. A systematic scoping review of Jackstone Calculi: clinical presentation and management. Urolithiasis. 2024 Nov 30:53(1):1. doi: 10.1007/s00240-024-01670-4. Epub 2024 Nov 30 [PubMed PMID: 39614889]
Level 1 (high-level) evidenceSubasinghe D, Goonewardena S, Kathiragamathamby V. Jack stone in the bladder: case report of a rare entity. BMC urology. 2017 Jun 5:17(1):40. doi: 10.1186/s12894-017-0230-6. Epub 2017 Jun 5 [PubMed PMID: 28583110]
Level 3 (low-level) evidenceMashiach D, Singh S, Anjum M, Polivka A, Alnajjar R, Wang L, Lee P, Szurmant H, Fricano E. The anatomy of a jackstone: a novel morphometric analysis of a rare urinary calculus. Urolithiasis. 2026 Mar 17:54(1):. doi: 10.1007/s00240-026-01968-5. Epub 2026 Mar 17 [PubMed PMID: 41842983]
Symeonidis EN, Memmos D, Anastasiadis A, Mykoniatis I, Savvides E, Langas G, Baniotis P, Bouchalakis A, Tsiakaras S, Stefanidis P, Stratis M, Mutomba WF, Vakalopoulos I, Dimitriadis G. Jackstone: A Calculus "Toy" in the Bladder. A Case Report of Rare Entity and Comprehensive Review of the Literature. Acta medica Lituanica. 2022:29(1):149-156. doi: 10.15388/Amed.2021.29.1.6. Epub 2022 Jan 26 [PubMed PMID: 36061940]
Level 3 (low-level) evidenceBichler KH, Eipper E, Naber K. [Infection-induced urinary stones]. Der Urologe. Ausg. A. 2003 Jan:42(1):47-55 [PubMed PMID: 12574884]
Li WM, Chou YH, Li CC, Liu CC, Huang SP, Wu WJ, Huang CH. Local factors compared with systemic factors in the formation of bladder uric acid stones. Urologia internationalis. 2009:82(1):48-52. doi: 10.1159/000176025. Epub 2009 Jan 20 [PubMed PMID: 19172097]
Level 2 (mid-level) evidenceAbou-Elela A. Epidemiology, pathophysiology, and management of uric acid urolithiasis: A narrative review. Journal of advanced research. 2017 Sep:8(5):513-527. doi: 10.1016/j.jare.2017.04.005. Epub 2017 Apr 28 [PubMed PMID: 28748117]
Level 3 (low-level) evidenceShah A, Keir M, Ducas R, Crean AM. Uric acid bladder stones in congenital cyanotic heart disease. Lancet (London, England). 2016 Oct 15:388(10054):1921. doi: 10.1016/S0140-6736(16)00347-0. Epub 2016 May 5 [PubMed PMID: 27156932]
Brisbane W, Bailey MR, Sorensen MD. An overview of kidney stone imaging techniques. Nature reviews. Urology. 2016 Nov:13(11):654-662. doi: 10.1038/nrurol.2016.154. Epub 2016 Aug 31 [PubMed PMID: 27578040]
Level 3 (low-level) evidenceWard JB, Feinstein L, Pierce C, Lim J, Abbott KC, Bavendam T, Kirkali Z, Matlaga BR, NIDDK Urologic Diseases in America Project. Pediatric Urinary Stone Disease in the United States: The Urologic Diseases in America Project. Urology. 2019 Jul:129():180-187. doi: 10.1016/j.urology.2019.04.012. Epub 2019 Apr 18 [PubMed PMID: 31005657]
Aurora AL, Taneja OP, Gupta DN. Bladder stone disease of childhood. II. A clinico-pathological study. Acta paediatrica Scandinavica. 1970 Jul:59(4):385-98 [PubMed PMID: 5447682]
Valyasevi A, Halstead SB, Dhanamitta S. Studies of bladder stone disease in Thailand. VI. Urinary studies in children, 2-10 years old, resident in a hypo- and hyperendemic area. The American journal of clinical nutrition. 1967 Dec:20(12):1362-8 [PubMed PMID: 6074673]
Zuckerman JM, Assimos DG. Hypocitraturia: pathophysiology and medical management. Reviews in urology. 2009 Summer:11(3):134-44 [PubMed PMID: 19918339]
Carnauba RA, Baptistella AB, Paschoal V, Hübscher GH. Diet-Induced Low-Grade Metabolic Acidosis and Clinical Outcomes: A Review. Nutrients. 2017 May 25:9(6):. doi: 10.3390/nu9060538. Epub 2017 May 25 [PubMed PMID: 28587067]
Level 2 (mid-level) evidenceAdeva MM, Souto G. Diet-induced metabolic acidosis. Clinical nutrition (Edinburgh, Scotland). 2011 Aug:30(4):416-21. doi: 10.1016/j.clnu.2011.03.008. Epub 2011 Apr 9 [PubMed PMID: 21481501]
Pizzorno J, Frassetto LA, Katzinger J. Diet-induced acidosis: is it real and clinically relevant? The British journal of nutrition. 2010 Apr:103(8):1185-94. doi: 10.1017/S0007114509993047. Epub 2009 Dec 15 [PubMed PMID: 20003625]
Han H, Segal AM, Seifter JL, Dwyer JT. Nutritional Management of Kidney Stones (Nephrolithiasis). Clinical nutrition research. 2015 Jul:4(3):137-52. doi: 10.7762/cnr.2015.4.3.137. Epub 2015 Jul 31 [PubMed PMID: 26251832]
Khan SR, Pearle MS, Robertson WG, Gambaro G, Canales BK, Doizi S, Traxer O, Tiselius HG. Kidney stones. Nature reviews. Disease primers. 2016 Feb 25:2():16008. doi: 10.1038/nrdp.2016.8. Epub 2016 Feb 25 [PubMed PMID: 27188687]
Sperrin M, Rogers K, Lane D, Southerden P. An investigation into the architecture and composition of a urinary calculus. Journal of materials science. Materials in medicine. 2002 Jan:13(1):7-9 [PubMed PMID: 15348197]
He Z, Jing Z, Jing-Cun Z, Chuan-Yi H, Fei G. Compositional analysis of various layers of upper urinary tract stones by infrared spectroscopy. Experimental and therapeutic medicine. 2017 Oct:14(4):3165-3169. doi: 10.3892/etm.2017.4864. Epub 2017 Aug 2 [PubMed PMID: 28912866]
Cohen SM, Johansson SL, Arnold LL, Lawson TA. Urinary tract calculi and thresholds in carcinogenesis. Food and chemical toxicology : an international journal published for the British Industrial Biological Research Association. 2002 Jun:40(6):793-9 [PubMed PMID: 11983274]
Yu Z, Yue W, Jiuzhi L, Youtao J, Guofei Z, Wenbin G. The risk of bladder cancer in patients with urinary calculi: a meta-analysis. Urolithiasis. 2018 Nov:46(6):573-579. doi: 10.1007/s00240-017-1033-7. Epub 2018 Jan 5 [PubMed PMID: 29305631]
Level 1 (high-level) evidenceKirakoya B, Kabore M, Pare AK, Abubakar BM. GIANT BLADDER STONE IN A PATIENT WITH TUMOR OF THE BLADDER: A RARE CO-MORBIDITY. Journal of the West African College of Surgeons. 2018 Jul-Sep:8(3):114-120 [PubMed PMID: 32754460]
Cho JH, Holley JL. Squamous cell carcinoma of the bladder in a female associated with multiple bladder stones. BMC research notes. 2013 Sep 4:6():354. doi: 10.1186/1756-0500-6-354. Epub 2013 Sep 4 [PubMed PMID: 24007445]
Michaud DS. Chronic inflammation and bladder cancer. Urologic oncology. 2007 May-Jun:25(3):260-8 [PubMed PMID: 17483025]
Kantor AF, Hartge P, Hoover RN, Narayana AS, Sullivan JW, Fraumeni JF Jr. Urinary tract infection and risk of bladder cancer. American journal of epidemiology. 1984 Apr:119(4):510-5 [PubMed PMID: 6711540]
Manley KV, Hubbard R, Swallow D, Finch W, Wood SJ, Biers SM. Risk factors for development of primary bladder squamous cell carcinoma. Annals of the Royal College of Surgeons of England. 2017 Feb:99(2):155-160. doi: 10.1308/rcsann.2016.0343. Epub 2016 Nov 21 [PubMed PMID: 27869492]
Subba S, Dorji N, Tshering S. Coincidental finding of a giant bladder calculus and squamous cell carcinoma of bladder: A case report. SAGE open medical case reports. 2022:10():2050313X221091411. doi: 10.1177/2050313X221091411. Epub 2022 Apr 14 [PubMed PMID: 35449528]
Level 3 (low-level) evidenceFernando MH, Jayarajah U, Herath KB, de Silva MVC, Goonewardena SAS. Aggressive squamous cell carcinoma of the bladder associated with a history of large bladder stone - a case report. Clinical case reports. 2017 Oct:5(10):1616-1619. doi: 10.1002/ccr3.1133. Epub 2017 Aug 22 [PubMed PMID: 29026557]
Level 3 (low-level) evidenceHaddad FS, Chinichian A. Postprostatectomy lithiasis. Urologia internationalis. 1991:46(2):221-31 [PubMed PMID: 2053239]
Kassouf W, Spiess PE, Siefker-Radtke A, Swanson D, Grossman HB, Kamat AM, Munsell MF, Guo CC, Czerniak BA, Dinney CP. Outcome and patterns of recurrence of nonbilharzial pure squamous cell carcinoma of the bladder: a contemporary review of The University of Texas M D Anderson Cancer Center experience. Cancer. 2007 Aug 15:110(4):764-9 [PubMed PMID: 17614317]
Dahm P, Gschwend JE. Malignant non-urothelial neoplasms of the urinary bladder: a review. European urology. 2003 Dec:44(6):672-81 [PubMed PMID: 14644119]
Barocas DA, Boorjian SA, Alvarez RD, Downs TM, Gross CP, Hamilton BD, Kobashi KC, Lipman RR, Lotan Y, Ng CK, Nielsen ME, Peterson AC, Raman JD, Smith-Bindman R, Souter LH. Microhematuria: AUA/SUFU Guideline. The Journal of urology. 2020 Oct:204(4):778-786. doi: 10.1097/JU.0000000000001297. Epub 2020 Jul 23 [PubMed PMID: 32698717]
Linsenmeyer MA, Linsenmeyer TA. Accuracy of bladder stone detection using abdominal x-ray after spinal cord injury. The journal of spinal cord medicine. 2004:27(5):438-42 [PubMed PMID: 15648797]
Mahdy A. Comments on Badejoko et al.: Overflow urinary incontinence due to bladder stones. International urogynecology journal. 2014 Oct:25(10):1445. doi: 10.1007/s00192-014-2472-0. Epub [PubMed PMID: 25047899]
Level 3 (low-level) evidenceAdhikari R, Baral HP, Bhattarai U, Gautam RK, Kunwar KJ, Shrestha D, Katwal BM. A Rare Case Report of Giant Urinary Bladder Stone Causing Recurrent Dysuria in a Woman. Case reports in urology. 2022:2022():4835945. doi: 10.1155/2022/4835945. Epub 2022 Aug 27 [PubMed PMID: 36065329]
Level 3 (low-level) evidenceMukherjee S, Sinha RK, Hamdoon M, Abbaraju J. Obstructive uropathy from a giant urinary bladder stone: a rare urological emergency. BMJ case reports. 2021 Jan 19:14(1):. doi: 10.1136/bcr-2020-234339. Epub 2021 Jan 19 [PubMed PMID: 33468632]
Level 3 (low-level) evidenceRaveenthiran V. Abnormally long penis in children with vesical calculus. The Indian journal of surgery. 2013 Feb:75(1):62-3. doi: 10.1007/s12262-012-0768-1. Epub 2012 Nov 18 [PubMed PMID: 24426390]
Singh KJ, Tiwari A, Goyal A. Jackstone: A rare entity of vesical calculus. Indian journal of urology : IJU : journal of the Urological Society of India. 2011 Oct:27(4):543-4. doi: 10.4103/0970-1591.91449. Epub [PubMed PMID: 22279326]
Kelly CE. Evaluation of voiding dysfunction and measurement of bladder volume. Reviews in urology. 2004:6 Suppl 1(Suppl 1):S32-7 [PubMed PMID: 16985853]
Cheng Y, Li T, Wu X, Ling Q, Rao K, Yuan X, Chen Z, Du G, Xu S. The diagnostic value of non-invasive methods for diagnosing bladder outlet obstruction in men with lower urinary tract symptoms: A meta-analysis. Frontiers in surgery. 2022:9():986679. doi: 10.3389/fsurg.2022.986679. Epub 2022 Sep 20 [PubMed PMID: 36338622]
Level 1 (high-level) evidenceChow KS, Chou CY. A boy with a large bladder stone. Pediatrics and neonatology. 2008 Aug:49(4):150-3. doi: 10.1016/S1875-9572(08)60031-5. Epub [PubMed PMID: 19054922]
Mbouché LO, Andzé GO, Makon ASN, Bob DN, Tamufor EN, Amenglé AL, Tambo FFM, Mure PY, Mikandé JZ, Angwafo FF 3rd. Acute Urinary Retention in the Male Child from Urethral Calculi: A Report of Three Cases. Case reports in urology. 2019:2019():5762139. doi: 10.1155/2019/5762139. Epub 2019 May 14 [PubMed PMID: 31218090]
Level 3 (low-level) evidenceMuhumuza J, Musinguzi B, Bukyana S, Kajoba D, Kithinji SM, Molen SF. A rare presentation of urolithiasis in a child with urine retention from a nonendemic area: a case report and literature review. Annals of medicine and surgery (2012). 2023 Apr:85(4):1015-1017. doi: 10.1097/MS9.0000000000000301. Epub 2023 Mar 25 [PubMed PMID: 37113865]
Level 3 (low-level) evidenceHoffmann KS, Godse A. Impacted urethral stone presenting as urinary retention in a child. BMJ case reports. 2021 Jan 25:14(1):. doi: 10.1136/bcr-2020-235022. Epub 2021 Jan 25 [PubMed PMID: 33495172]
Level 3 (low-level) evidenceHughes T, Ho HC, Pietropaolo A, Somani BK. Guideline of guidelines for kidney and bladder stones. Turkish journal of urology. 2020 Nov:46(Supp. 1):S104-S112. doi: 10.5152/tud.2020.20315. Epub 2020 Oct 9 [PubMed PMID: 33052834]
Bowen DK, Wan J, Engel R, Lyon RP, Dielubanza E, Bloom DA. Sounds and Charrière: the rest of the story. Journal of pediatric urology. 2014 Dec:10(6):1106-10. doi: 10.1016/j.jpurol.2014.04.010. Epub 2014 May 21 [PubMed PMID: 24942595]
Dyer R, Nordin BE. Urinary crystals and their relation to stone formation. Nature. 1967 Aug 12:215(5102):751-2 [PubMed PMID: 6059548]
Salinawati B, Hing EY, Fam XI, Zulfiqar MA. Accuracy of ultrasound versus computed tomography urogram in detecting urinary tract calculi. The Medical journal of Malaysia. 2015 Aug:70(4):238-42 [PubMed PMID: 26358021]
Ahmed FO, Hamdan HZ, Abdelgalil HB, Sharfi AA. A comparison between transabdominal ultrasonographic and cystourethroscopy findings in adult Sudanese patients presenting with haematuria. International urology and nephrology. 2015 Feb:47(2):223-8. doi: 10.1007/s11255-014-0869-9. Epub 2014 Nov 6 [PubMed PMID: 25374263]
Ahmed F, Askarpour MR, Eslahi A, Nikbakht HA, Jafari SH, Hassanpour A, Makarem A, Salama H, Ayoub A. The role of ultrasonography in detecting urinary tract calculi compared to CT scan. Research and reports in urology. 2018:10():199-203. doi: 10.2147/RRU.S178902. Epub 2018 Nov 15 [PubMed PMID: 30510920]
Ray AA, Ghiculete D, Pace KT, Honey RJ. Limitations to ultrasound in the detection and measurement of urinary tract calculi. Urology. 2010 Aug:76(2):295-300. doi: 10.1016/j.urology.2009.12.015. Epub 2010 Mar 5 [PubMed PMID: 20206970]
Adwan A, Binsaleh S. The accuracy of noncontrast spiral computerized tomography in detecting lucent renal stones: A case report and literature review. Urology annals. 2015 Jan-Mar:7(1):109-11. doi: 10.4103/0974-7796.148649. Epub [PubMed PMID: 25657560]
Level 3 (low-level) evidenceAndrabi Y, Patino M, Das CJ, Eisner B, Sahani DV, Kambadakone A. Advances in CT imaging for urolithiasis. Indian journal of urology : IJU : journal of the Urological Society of India. 2015 Jul-Sep:31(3):185-93. doi: 10.4103/0970-1591.156924. Epub [PubMed PMID: 26166961]
Level 3 (low-level) evidenceJohnson EK, Faerber GJ, Roberts WW, Wolf JS Jr, Park JM, Bloom DA, Wan J. Are stone protocol computed tomography scans mandatory for children with suspected urinary calculi? Urology. 2011 Sep:78(3):662-6. doi: 10.1016/j.urology.2011.02.062. Epub 2011 Jun 30 [PubMed PMID: 21722946]
Masselli G, Derme M, Bernieri MG, Polettini E, Casciani E, Monti R, Laghi F, Framarino-Dei-Malatesta M, Guida M, Brunelli R, Gualdi G. Stone disease in pregnancy: imaging-guided therapy. Insights into imaging. 2014 Dec:5(6):691-6. doi: 10.1007/s13244-014-0352-2. Epub 2014 Sep 24 [PubMed PMID: 25249333]
Ozcan HN, Ozer G, Dogan HS, Karakaya J, Oguz B, Tekgul S, Haliloglu M. Zero-echo time MRI: an alternative method for the diagnosis of urinary stones in children. European radiology. 2025 Jan:35(1):289-296. doi: 10.1007/s00330-024-10950-x. Epub 2024 Jul 12 [PubMed PMID: 38992108]
Ibrahim el-SH, Pooley RA, Bridges MD, Cernigliaro JG, Haley WE. Kidney stone imaging with 3D ultra-short echo time (UTE) magnetic resonance imaging. A phantom study. Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE Engineering in Medicine and Biology Society. Annual International Conference. 2014:2014():2356-9. doi: 10.1109/EMBC.2014.6944094. Epub [PubMed PMID: 25570462]
Ibrahim EH, Cernigliaro JG, Bridges MD, Pooley RA, Haley WE. The Capabilities and Limitations of Clinical Magnetic Resonance Imaging for Detecting Kidney Stones: A Retrospective Study. International journal of biomedical imaging. 2016:2016():4935656 [PubMed PMID: 27980535]
Level 2 (mid-level) evidenceO'Connor RC, Laven BA, Bales GT, Gerber GS. Nonsurgical management of benign prostatic hyperplasia in men with bladder calculi. Urology. 2002 Aug:60(2):288-91 [PubMed PMID: 12137828]
Pearle MS, Goldfarb DS, Assimos DG, Curhan G, Denu-Ciocca CJ, Matlaga BR, Monga M, Penniston KL, Preminger GM, Turk TM, White JR, American Urological Assocation. Medical management of kidney stones: AUA guideline. The Journal of urology. 2014 Aug:192(2):316-24. doi: 10.1016/j.juro.2014.05.006. Epub 2014 May 20 [PubMed PMID: 24857648]
Normand M, Haymann JP, Daudon M. Medical treatment of uric acid kidney stones. Canadian Urological Association journal = Journal de l'Association des urologues du Canada. 2024 Nov:18(11):E339-E345. doi: 10.5489/cuaj.8774. Epub [PubMed PMID: 38976892]
Jahrreiss V, Seitz C, Quhal F. Medical management of urolithiasis: Great efforts and limited progress. Asian journal of urology. 2024 Apr:11(2):149-155. doi: 10.1016/j.ajur.2023.05.001. Epub 2023 Jun 29 [PubMed PMID: 38680579]
Rodman JS, Williams JJ, Peterson CM. Dissolution of uric acid calculi. The Journal of urology. 1984 Jun:131(6):1039-44 [PubMed PMID: 6726897]
Lopez JR, Jenkins CE, Millares M. Irrigating solutions in bladder stone dissolution. Drug intelligence & clinical pharmacy. 1987 Nov:21(11):872-4 [PubMed PMID: 3678056]
Mallon D. Renacidin irrigation for struvite stones. Nursing. 1986 Aug:16(8):26-8 [PubMed PMID: 3636660]
Gonzalez RD, Whiting BM, Canales BK. The history of kidney stone dissolution therapy: 50 years of optimism and frustration with renacidin. Journal of endourology. 2012 Feb:26(2):110-8. doi: 10.1089/end.2011.0380. Epub 2011 Oct 14 [PubMed PMID: 21999455]
Level 1 (high-level) evidenceJoshi HB, Kumar PV, Timoney AG. Citric acid (solution R) irrigation in the treatment of refractory infection (struvite) stone disease: is it useful? European urology. 2001 May:39(5):586-90 [PubMed PMID: 11464042]
Øbro LF, Sloth Osther S, Osther PJS, Jung H. Case of the month from Lillebaelt hospital, University Hospital of South Denmark, Denmark: Renacidin(®) - still a useful adjunct to endoscopic surgery for complex renal struvite stone disease. BJU international. 2022 Oct:130(4):437-440. doi: 10.1111/bju.15822. Epub [PubMed PMID: 36102583]
Level 3 (low-level) evidenceAUERBACH S, MAINWARING R, SCHWARZ F. Renal and ureteral damage following clinical use of Renacidin. JAMA. 1963 Jan 5:183():61-3 [PubMed PMID: 13965494]
Wang L, Nancollas GH. Calcium orthophosphates: crystallization and dissolution. Chemical reviews. 2008 Nov:108(11):4628-69. doi: 10.1021/cr0782574. Epub 2008 Sep 25 [PubMed PMID: 18816145]
Schillebeeckx C, Vander Eeckt K, Ost D, Van den Branden M, Deconinck S. Kidney Stone Dissolution Therapy in Phosphate Stones: A Case Report. Journal of endourology case reports. 2020:6(1):45-48. doi: 10.1089/cren.2019.0076. Epub 2020 Mar 11 [PubMed PMID: 32775674]
Level 3 (low-level) evidenceCravens DD, Zweig S. Urinary catheter management. American family physician. 2000 Jan 15:61(2):369-76 [PubMed PMID: 10670503]
Li A, Ji C, Wang H, Lang G, Lu H, Liu S, Li W, Zhang B, Fang W. Transurethral cystolitholapaxy with the AH-1 stone removal system for the treatment of bladder stones of variable size. BMC urology. 2015 Feb 21:15(1):9. doi: 10.1186/s12894-015-0003-z. Epub 2015 Feb 21 [PubMed PMID: 25887148]
Tugcu V, Polat H, Ozbay B, Gurbuz N, Eren GA, Tasci AI. Percutaneous versus transurethral cystolithotripsy. Journal of endourology. 2009 Feb:23(2):237-41. doi: 10.1089/end.2008.0455. Epub [PubMed PMID: 19196058]
Yalcin K. Comparison of three techniques in bladder stone surgery: Which technique is more effective and safe? Nigerian journal of clinical practice. 2023 Aug:26(8):1128-1133. doi: 10.4103/njcp.njcp_9_23. Epub [PubMed PMID: 37635606]
Mishra DK, Bhatt S, Mukhilesh R, Somani BK, Agrawal MS. Mini-percutaneous cystolithotripsy (mPCCL) versus transurethral cystolithotripsy (TUC) in pre-school children: Prospective comparative non-randomized outcomes over 8 years. Journal of pediatric urology. 2020 Dec:16(6):782.e1-782.e6. doi: 10.1016/j.jpurol.2020.09.021. Epub 2020 Sep 28 [PubMed PMID: 33051129]
Level 1 (high-level) evidenceShahat AA, Kamel AA, Taha TM, Abonnoor AEI, Reda A, Faddan AA, Elderwy AA, Safwat AS, Kurkar A, Abdelkawi IF. A randomised trial comparing transurethral to percutaneous cystolithotripsy in boys. BJU international. 2022 Aug:130(2):254-261. doi: 10.1111/bju.15693. Epub 2022 Feb 8 [PubMed PMID: 35044035]
Level 1 (high-level) evidenceMahar N, Soomro AS, Abbasi SN, Hussain M, Naqvi SA, Rizvi SA. Endemic Bladder Stone Disease in Children, Pattern And Current Management: Experience From A Centre In Peri-Urban Setting In Pakistan. Urology journal. 2024 Oct 12:21(5):325-330. doi: 10.22037/uj.v21i.8046. Epub 2024 Oct 12 [PubMed PMID: 38822627]
Fauzan R, Herman H, Rachman W, Sitompul AP, Astram A. Endourological versus open cystolithotomy for bladder stone management among children: A systematic review and meta-analysis. F1000Research. 2023:12():124. doi: 10.12688/f1000research.129270.1. Epub 2023 Feb 2 [PubMed PMID: 39291145]
Level 1 (high-level) evidenceMaresca G, Mc Clinton S, Swami S, El-Mokadem I, Donaldson JF. Do men with bladder stones benefit from treatment of benign prostatic obstruction? BJU international. 2022 Nov:130(5):619-627. doi: 10.1111/bju.15761. Epub 2022 May 17 [PubMed PMID: 35482471]
Cabral JD, Gannon M, Raster G, Nusbaum DJ, Bouhadana D, Arezki A, Hamouda A, Leathead A, Ohana I, Foucault R, Sadri I, Sioufi JA, Lee N, Benzouak T, Murad L, Corsi NJ, Klein J, Singh I, Kearns J, Chang C, Justo Quintas J, Zorn KC, Rodrigues T, Marhamati SH, Helfand BT, Glaser AP. Outcomes of Aquablation in BPH with bladder stones: Analysis of the ICARUS database. BJUI compass. 2026 Feb:7(2):e70156. doi: 10.1002/bco2.70156. Epub 2026 Jan 30 [PubMed PMID: 41625209]
Dogan E, Soytürk S, Altunhan A, Bhojani N, Kumar Somani B, Ahmed K, Rw Herrmann T, Guven S. Simultaneous outlet surgery for bladder stones and BPO: a scoping review from EAU endourology - challenging the traditional approach. World journal of urology. 2026 Apr 6:44(1):. doi: 10.1007/s00345-026-06369-2. Epub 2026 Apr 6 [PubMed PMID: 41941012]
Level 2 (mid-level) evidenceTelha KA, Alkohlany K, Alnono I. Extracorporeal shockwave lithotripsy monotherapy for treating patients with bladder stones. Arab journal of urology. 2016 Sep:14(3):207-10. doi: 10.1016/j.aju.2016.06.001. Epub 2016 Jul 25 [PubMed PMID: 27547462]
Bhatia V, Biyani CS. Vesical lithiasis: open surgery versus cystolithotripsy versus extracorporeal shock wave therapy. The Journal of urology. 1994 Mar:151(3):660-2 [PubMed PMID: 8308976]
Ali M, Hashem A, Helmy TE, Zewin T, Sheir KZ, Shokeir AA. Shock wave lithotripsy versus endoscopic cystolitholapaxy in the management of patients presenting with calcular acute urinary retention: a randomised controlled trial. World journal of urology. 2019 May:37(5):879-884. doi: 10.1007/s00345-018-2434-0. Epub 2018 Aug 13 [PubMed PMID: 30105456]
Level 1 (high-level) evidenceGarcía Cardoso JV, González Enguita C, Cabrera Pérez J, Rodriguez Miñón JL, Calahorra Fernández FJ, Vela Navarrete R. [Bladder calculi. Is extracorporeal shock wave lithotripsy the first choice treatment?]. Archivos espanoles de urologia. 2003 Dec:56(10):1111-6 [PubMed PMID: 14763416]
el-Sherif AE, Prasad K. Treatment of urethral stones by retrograde manipulation and extracorporeal shock wave lithotripsy. British journal of urology. 1995 Dec:76(6):761-4 [PubMed PMID: 8535722]
Al-Ansari A, Shamsodini A, Younis N, Jaleel OA, Al-Rubaiai A, Shokeir AA. Extracorporeal shock wave lithotripsy monotherapy for treatment of patients with urethral and bladder stones presenting with acute urinary retention. Urology. 2005 Dec:66(6):1169-71 [PubMed PMID: 16360434]
Davis NF, Donaldson JF, Shepherd R, Neisius A, Petrik A, Seitz C, Thomas K, Lombardo R, Tzelves L, Somani B, Gambarro G, Ruhayel Y, Türk C, Skolarikos A. Treatment outcomes of bladder stones in children with intact bladders in developing countries: A systematic review of }1000 cases on behalf of the European Association of Urology Bladder Stones Guideline panel. Journal of pediatric urology. 2022 Apr:18(2):132-140. doi: 10.1016/j.jpurol.2022.01.007. Epub 2022 Jan 23 [PubMed PMID: 35148953]
Level 1 (high-level) evidenceEl-Halwagy S, Osman Y, Sheir KZ. Shock wave lithotripsy of vesical stones in patients with infravesical obstruction: an underused noninvasive approach. Urology. 2013 Mar:81(3):508-10. doi: 10.1016/j.urology.2012.11.027. Epub 2013 Jan 17 [PubMed PMID: 23332999]
Rizvi SA, Naqvi SA, Hussain Z, Hashmi A, Hussain M, Zafar MN, Sultan S, Mehdi H. Management of pediatric urolithiasis in Pakistan: experience with 1,440 children. The Journal of urology. 2003 Feb:169(2):634-7 [PubMed PMID: 12544331]
Benson MC, Olsson CA. Continent urinary diversion. The Urologic clinics of North America. 1999 Feb:26(1):125-47, ix [PubMed PMID: 10086055]
Claus C, Jorion JI, Libon E. [Continent urinary diversion and calculus]. Acta urologica Belgica. 1997 Dec:65(4):33-7 [PubMed PMID: 9497595]
Wilhelm K, Frankenschmidt A, Miernik A. Analgesia-free flexible ureteroscopic treatment and laser lithotripsy for removal of a large urinary stone: a case report. Journal of medical case reports. 2015 Oct 2:9():225. doi: 10.1186/s13256-015-0699-0. Epub 2015 Oct 2 [PubMed PMID: 26431958]
Level 3 (low-level) evidenceBhatia V, Biyani CS. A comparative study of cystolithotripsy and extracorporeal shock wave therapy for bladder stones. International urology and nephrology. 1994:26(1):26-31 [PubMed PMID: 8026920]
Level 2 (mid-level) evidenceRamakrishnan PA, Medhat M, Al-Bulushi YH, Gopakumar KP, Sampige VP, Al-Busaidy SS. Holmium laser cystolithotripsy in children: initial experience. The Canadian journal of urology. 2005 Dec:12(6):2880-6 [PubMed PMID: 16401373]
Papatsoris AG, Varkarakis I, Dellis A, Deliveliotis C. Bladder lithiasis: from open surgery to lithotripsy. Urological research. 2006 Jun:34(3):163-7 [PubMed PMID: 16470391]
Ener K, Agras K, Aldemir M, Okulu E, Kayigil O. The randomized comparison of two different endoscopic techniques in the management of large bladder stones: transurethral use of nephroscope or cystoscope? Journal of endourology. 2009 Jul:23(7):1151-5. doi: 10.1089/end.2008.0647. Epub [PubMed PMID: 19530944]
Level 1 (high-level) evidenceJang JY, Ko YH, Song PH, Choi JY. Comparison of three different endoscopic approaches in the treatment of bladder calculi. Yeungnam University journal of medicine. 2019 Jan:36(1):16-19. doi: 10.12701/yujm.2019.00045. Epub 2018 Dec 19 [PubMed PMID: 31620607]
Gupta R, Gupta S, Das RK, Basu S, Agrawal V. Comparative study of a new technique using nephroscope and resectoscope sheath and the percutaneous cystolithotripsy for the treatment of bladder calculus. Central European journal of urology. 2017:70(4):400-404. doi: 10.5173/ceju.2017.1379. Epub 2017 Sep 18 [PubMed PMID: 29410893]
Level 2 (mid-level) evidenceBansal A, Kumar M, Sankhwar S, Goel S, Patodia M, Aeron R, Bhaskar V. Prospective randomized comparison of three endoscopic modalities used in treatment of bladder stones. Urologia. 2016 May 24:83(2):87-92. doi: 10.5301/uro.5000171. Epub 2016 Apr 9 [PubMed PMID: 27103095]
Level 1 (high-level) evidenceBlack KM, Aldoukhi AH, Ghani KR. A Users Guide to Holmium Laser Lithotripsy Settings in the Modern Era. Frontiers in surgery. 2019:6():48. doi: 10.3389/fsurg.2019.00048. Epub 2019 Aug 14 [PubMed PMID: 31475152]
Aldoukhi AH, Roberts WW, Hall TL, Ghani KR. Holmium Laser Lithotripsy in the New Stone Age: Dust or Bust? Frontiers in surgery. 2017:4():57. doi: 10.3389/fsurg.2017.00057. Epub 2017 Sep 29 [PubMed PMID: 29067287]
Aldoukhi AH, Black KM, Ghani KR. Emerging Laser Techniques for the Management of Stones. The Urologic clinics of North America. 2019 May:46(2):193-205. doi: 10.1016/j.ucl.2018.12.005. Epub 2019 Mar 4 [PubMed PMID: 30961853]
Buzescu B, Cozma C, Geavlete P, Multescu R, Georgescu D, Ene C, Bulai C, Geavlete B. Laser Lithotripsy in Renal Lithiasis - 2023 Update - a Narative Review. Maedica. 2024 Jun:19(2):388-392. doi: 10.26574/maedica.2024.19.2.388. Epub [PubMed PMID: 39188844]
Mishra A, Medairos R, Chen J, Soto-Palou F, Wu Y, Antonelli J, Preminger GM, Lipkin ME, Zhong P. Exploring optimal settings for safe and effective thulium fibre laser lithotripsy in a kidney model. BJU international. 2024 Feb:133(2):223-230. doi: 10.1111/bju.16218. Epub 2023 Nov 27 [PubMed PMID: 37942684]
Hajiha M, Farkouh A, Amasyali AS, Buell MI, Leu R, Groegler J, Smith J, Goyne A, Baldwin DD, Moghisi R, Baldwin DD. Which Laser System Is Optimal for Cystolithotripsy of Large Bladder Calculi? Journal of endourology. 2023 Nov:37(11):1221-1227. doi: 10.1089/end.2023.0078. Epub [PubMed PMID: 37698888]
Cerrato C, Frascheri MF, Fernandez SN, Emiliani E, Arena P, Pietropaolo A, Somani BK. Emerging Role of Laser Lithotripsy for Bladder Stones: Real-World Outcomes from Two European Endourology Centers with a Systematic Review of Literature. Journal of endourology. 2025 Mar:39(3):285-291. doi: 10.1089/end.2024.0640. Epub 2025 Feb 5 [PubMed PMID: 39909483]
Level 1 (high-level) evidenceZhao X, Guo Q, Ren S, Song Y, Li C, Wang J. Transurethral Cystolithotripsy vs Percutaneous Cystolithotomy for Bladder Stones in Children: A Systematic Review and Meta-Analysis Comparing Clinical Outcomes and Complications. Journal of endourology. 2025 Sep:39(9):960-967. doi: 10.1089/end.2024.0677. Epub 2025 May 12 [PubMed PMID: 40354160]
Level 1 (high-level) evidenceJavanmard B, Fallah Karkan M, Razzaghi MR, Ghiasy S, Ranjbar A, Rahavian A. Surgical Management of Vesical Stones in Children: A Comparison Between Open Cystolithotomy, Percutaneous Cystolithotomy and Transurethral Cystolithotripsy With Holmium-YAG Laser. Journal of lasers in medical sciences. 2018 Summer:9(3):183-187. doi: 10.15171/jlms.2018.33. Epub 2018 Jul 28 [PubMed PMID: 30809329]
Dahril, Ismy J, Asnafi A, Pratama R. Percutaneous cystolithotripsy of bladder stones in children: A case series, an experience from a tertiary hospital. Urology annals. 2022 Jan-Mar:14(1):85-88. doi: 10.4103/UA.UA_177_20. Epub 2022 Jan 20 [PubMed PMID: 35197709]
Level 2 (mid-level) evidenceAnsari MS, Yadav P, Srivastava A, Kapoor R, Ashwin Shekar P. Etiology and characteristics of pediatric urethral strictures in a developing country in the 21st century. Journal of pediatric urology. 2019 Aug:15(4):403.e1-403.e8. doi: 10.1016/j.jpurol.2019.05.020. Epub 2019 May 24 [PubMed PMID: 31301979]
Vetterlein MW, Weisbach L, Riechardt S, Fisch M. Anterior Urethral Strictures in Children: Disease Etiology and Comparative Effectiveness of Endoscopic Treatment vs. Open Surgical Reconstruction. Frontiers in pediatrics. 2019:7():5. doi: 10.3389/fped.2019.00005. Epub 2019 Jan 31 [PubMed PMID: 30805317]
Level 2 (mid-level) evidenceHasan AM, Mohammed AA, Abdel-Kader MS, Abdelhamid AM, Abdeldayem AM, Ahmed MA. Percutaneous versus transurethral cystolithotripsy for the management of bladder calculi in the pre-school boys: Prospective randomized study. Journal of pediatric urology. 2025 Dec:21(6):1411-1417. doi: 10.1016/j.jpurol.2025.07.016. Epub 2025 Jul 17 [PubMed PMID: 40701892]
Level 1 (high-level) evidenceYağmur İ, Demir M, Katı B, Pelit ES, Ördek E, Çiftçi H. Comparison of two different minimally invasive techniques used in bladder stone surgery for preschool-aged children. Turkish journal of medical sciences. 2022 Aug:52(4):1274-1280. doi: 10.55730/1300-0144.5433. Epub 2022 Aug 10 [PubMed PMID: 36326399]
Gou L, Wang Z, Zhou Y, Zheng X. Comparison of nephroscopy and cystoscopy used in the treatment of bladder stones: a systematic review and meta-analysis of randomized controlled trials. BMC surgery. 2021 Dec 31:21(1):448. doi: 10.1186/s12893-021-01461-3. Epub 2021 Dec 31 [PubMed PMID: 34972510]
Level 1 (high-level) evidenceSingh KJ, Kaur J. Comparison of three different endoscopic techniques in management of bladder calculi. Indian journal of urology : IJU : journal of the Urological Society of India. 2011 Jan:27(1):10-3. doi: 10.4103/0970-1591.78402. Epub [PubMed PMID: 21716932]
Kawahara T, Ito H, Terao H, Kato Y, Ogawa T, Uemura H, Kubota Y, Matsuzaki J. Amplatz sheath for cystolithotripsy using Ho: YAG laser in female patients. Urology. 2012 Nov:80(5):1154-5. doi: 10.1016/j.urology.2012.07.046. Epub 2012 Sep 23 [PubMed PMID: 23010340]
Tabei T, Kawahara T, Kuroda S, Ito H, Kobayashi K, Uemura H, Matsuzaki J. Effect of Amplatz Sheath on Cystolithotripsy for Women with Large Bladder Stone. BioMed research international. 2017:2017():9341042. doi: 10.1155/2017/9341042. Epub 2017 May 24 [PubMed PMID: 28626768]
Wollin TA, Singal RK, Whelan T, Dicecco R, Razvi HA, Denstedt JD. Percutaneous suprapubic cystolithotripsy for treatment of large bladder calculi. Journal of endourology. 1999 Dec:13(10):739-44 [PubMed PMID: 10646681]
Agrawal MS, Aron M, Goyal J, Elhence IP, Asopa HS. Percutaneous suprapubic cystolithotripsy for vesical calculi in children. Journal of endourology. 1999 Apr:13(3):173-5 [PubMed PMID: 10360496]
Chatterjee US, Chatterjee I. Percutaneous Cystolithotomy in Augmented Bladders. Journal of Indian Association of Pediatric Surgeons. 2021 Jul-Aug:26(4):250-252. doi: 10.4103/jiaps.JIAPS_128_20. Epub 2021 Jul 12 [PubMed PMID: 34385769]
Cain MP, Casale AJ, Kaefer M, Yerkes E, Rink RC. Percutaneous cystolithotomy in the pediatric augmented bladder. The Journal of urology. 2002 Oct:168(4 Pt 2):1881-2 [PubMed PMID: 12352381]
Lee MS, Sledge TR, Seyer AK, Qi R, Koo K. How I do it: percutaneous cystolitholapaxy for bladder stones with complex lower urinary tract anatomy. The Canadian journal of urology. 2025 Aug 29:32(4):325-333. doi: 10.32604/cju.2025.064255. Epub 2025 Aug 29 [PubMed PMID: 40910330]
Level 2 (mid-level) evidenceAl Saffar H, Radhakrishnan T, Adhami M, Tempo J, Cetti R. Large stone in neobladder: percutaneous neocystolithotomy. Translational andrology and urology. 2025 Oct 31:14(10):3321-3327. doi: 10.21037/tau-2025-509. Epub 2025 Oct 28 [PubMed PMID: 41230138]
Burns R, Hardesty J, Schmidt J, Risk N, Vasquez R, Soyster M, Mellon M, Rivera M. Percutaneous Cystolitholapaxy Is Safe and Effective in Adult Patients With Lower Urinary Tract Reconstruction Utilizing Bowel. Urology. 2023 Aug:178():37-41. doi: 10.1016/j.urology.2023.04.024. Epub 2023 May 5 [PubMed PMID: 37150405]
Beiko D, Razvi H, Bhojani N, Bjazevic J, Bayne DB, Tzou DT, Stoller ML, Chi T. Techniques - Ultrasound-guided percutaneous nephrolithotomy: How we do it. Canadian Urological Association journal = Journal de l'Association des urologues du Canada. 2020 Mar:14(3):E104-E110. doi: 10.5489/cuaj.6076. Epub 2019 Sep 27 [PubMed PMID: 31599714]
Kumar A, Dalela D, Dalela D, Goel A, Paul S, Sankhwar SN. The twin amplatz sheath method: a modified technique of percutaneous cystolithotripsy for large bladder stones in female patients. Journal of surgical technique and case report. 2013 Jul:5(2):109-11. doi: 10.4103/2006-8808.128757. Epub [PubMed PMID: 24741433]
Level 3 (low-level) evidencePapatsoris A. Twin amplatz sheath method: a modified technique of percutaneous cystolithotripsy for large bladder stone in females. Journal of surgical technique and case report. 2013 Jul:5(2):111-2. doi: 10.4103/2006-8808.128755. Epub [PubMed PMID: 24741434]
Level 3 (low-level) evidenceMaheshwari PN, Oswal AT, Bansal M. Percutaneous cystolithotomy for vesical calculi: a better approach. Techniques in urology. 1999 Mar:5(1):40-2 [PubMed PMID: 10374793]
Abarchi H, Hachem A, Erraji M, Belkacem R, Outarahout N, Barahioui M. [Pediatric vesical lithiasis. 70 case reports]. Annales d'urologie. 2003 Jun:37(3):117-9 [PubMed PMID: 12872601]
Level 3 (low-level) evidenceÇakici ÖU, Ener K, Keske M, Altinova S, Canda AE, Aldemir M, Ardicoglu A. Open stone surgery: a still-in-use approach for complex stone burden. Central European journal of urology. 2017 Jun 30:70(2):179-184. doi: 10.5173/ceju.2017.1205. Epub 2017 Mar 20 [PubMed PMID: 28721286]
El-Husseiny T, Buchholz N. The role of open stone surgery. Arab journal of urology. 2012 Sep:10(3):284-8. doi: 10.1016/j.aju.2012.03.004. Epub 2012 May 2 [PubMed PMID: 26558038]
Xie Y, Zhang M, Liu K. Comparison of the Efficacy of Transurethral Cystolithotripsy and Percutaneous Cystolithotomy in the Treatment of Male Children with 20-30 mm Bladder Stones: A Retrospective Study. Archivos espanoles de urologia. 2025 Jan:78(1):71-76. doi: 10.56434/j.arch.esp.urol.20257801.9. Epub [PubMed PMID: 39943636]
Level 2 (mid-level) evidenceAutorino R, Zargar H, Mariano MB, Sanchez-Salas R, Sotelo RJ, Chlosta PL, Castillo O, Matei DV, Celia A, Koc G, Vora A, Aron M, Parsons JK, Pini G, Jensen JC, Sutherland D, Cathelineau X, Nuñez Bragayrac LA, Varkarakis IM, Amparore D, Ferro M, Gallo G, Volpe A, Vuruskan H, Bandi G, Hwang J, Nething J, Muruve N, Chopra S, Patel ND, Derweesh I, Champ Weeks D, Spier R, Kowalczyk K, Lynch J, Harbin A, Verghese M, Samavedi S, Molina WR, Dias E, Ahallal Y, Laydner H, Cherullo E, De Cobelli O, Thiel DD, Lagerkvist M, Haber GP, Kaouk J, Kim FJ, Lima E, Patel V, White W, Mottrie A, Porpiglia F. Perioperative Outcomes of Robotic and Laparoscopic Simple Prostatectomy: A European-American Multi-institutional Analysis. European urology. 2015 Jul:68(1):86-94. doi: 10.1016/j.eururo.2014.11.044. Epub 2014 Dec 4 [PubMed PMID: 25484140]
Matei DV, Brescia A, Mazzoleni F, Spinelli M, Musi G, Melegari S, Galasso G, Detti S, de Cobelli O. Robot-assisted simple prostatectomy (RASP): does it make sense? BJU international. 2012 Dec:110(11 Pt C):E972-9. doi: 10.1111/j.1464-410X.2012.11192.x. Epub 2012 May 18 [PubMed PMID: 22607242]
Haffar A, Crigger C, Trump T, Jessop M, Salkini MW. Minimally Invasive Robotic-Assisted Cystolithotomy in a Complicated Urinary Diversion: A Feasible and Safe Approach. Case reports in urology. 2021:2021():8345092. doi: 10.1155/2021/8345092. Epub 2021 Dec 14 [PubMed PMID: 34950523]
Level 3 (low-level) evidenceEsposito C, Masieri L, Blanc T, Lendvay T, Escolino M. Robot-assisted laparoscopic surgery for treatment of urinary tract stones in children: report of a multicenter international experience. Urolithiasis. 2021 Dec:49(6):575-583. doi: 10.1007/s00240-021-01271-5. Epub 2021 May 16 [PubMed PMID: 33993337]
Tan GY, Sooriakumaran P, Peters DL, Srivastava A, Tewari A. Cystolithotomy during robotic radical prostatectomy: Single-stage procedure for concomitant bladder stones. Indian journal of urology : IJU : journal of the Urological Society of India. 2012 Jan:28(1):99-101. doi: 10.4103/0970-1591.94968. Epub [PubMed PMID: 22557729]
Breda A, Mossanen M, Leppert J, Harper J, Schulam PG, Churchill B. Percutaneous cystolithotomy for calculi in reconstructed bladders: initial UCLA experience. The Journal of urology. 2010 May:183(5):1989-93. doi: 10.1016/j.juro.2010.01.033. Epub 2010 Mar 19 [PubMed PMID: 20303534]
Yoshida T, Kinoshita H, Nakamoto T, Yanishi M, Sugi M, Murota T, Matsuda T. Conservative Treatment for Benign Prostatic Hyperplasia in Patients With Bladder Stones. Urology. 2015 Sep:86(3):450-3. doi: 10.1016/j.urology.2015.04.022. Epub 2015 Jul 30 [PubMed PMID: 26235850]
Descazeaud A, Robert G, de La Taille A. [Management of the bladder outlet obstruction associated with BPH in patients with special circumstances and/or complications]. Progres en urologie : journal de l'Association francaise d'urologie et de la Societe francaise d'urologie. 2018 Nov:28(15):868-874. doi: 10.1016/j.purol.2018.08.006. Epub 2018 Sep 13 [PubMed PMID: 30220535]
Mekke S, Roshani H, van Zanten P, Palacios LG, Egberts J, Hendriks N, Wijffelman M, Zonneveld W, Merks B, van Loopik S, Buddingh T. Simultaneous transurethral resection of the prostate and cystolithotripsy: A urological dilemma examined. Canadian Urological Association journal = Journal de l'Association des urologues du Canada. 2021 Jul:15(7):E361-E365. doi: 10.5489/cuaj.6743. Epub [PubMed PMID: 33382366]
Asutay MK, Kilinc C, Bozkurt O, Coktu K, Celik S. Multiple Giant Stones in an Augmented Bladder: A Case Report. Cureus. 2025 Mar:17(3):e81430. doi: 10.7759/cureus.81430. Epub 2025 Mar 29 [PubMed PMID: 40296962]
Level 3 (low-level) evidenceSofer M, Kaver I, Greenstein A, Bar Yosef Y, Mabjeesh NJ, Chen J, Ben-Chaim J, Matzkin H. Refinements in treatment of large bladder calculi: simultaneous percutaneous suprapubic and transurethral cystolithotripsy. Urology. 2004 Oct:64(4):651-4 [PubMed PMID: 15491692]
Darrad M, Collins M, Inglis J. Combined endoscopic approach for patients with multiple bladder stones. Annals of the Royal College of Surgeons of England. 2015 Apr:97(3):241-2. doi: 10.1308/rcsann.2015.97.3.241. Epub [PubMed PMID: 26263816]
Casey JT, Chan KH, Hasegawa Y, Large T, Judge B, Kaefer M, Misseri R, Rink RC, Ueoka K, Cain MP. Long-term follow-up of composite bladder augmentation incorporating stomach in a multi-institutional cohort of patients with cloacal exstrophy. Journal of pediatric urology. 2017 Feb:13(1):43.e1-43.e6. doi: 10.1016/j.jpurol.2016.09.013. Epub 2016 Oct 28 [PubMed PMID: 27889222]
Level 3 (low-level) evidenceKaefer M, Hendren WH, Bauer SB, Goldenblatt P, Peters CA, Atala A, Retik AB. Reservoir calculi: a comparison of reservoirs constructed from stomach and other enteric segments. The Journal of urology. 1998 Dec:160(6 Pt 1):2187-90 [PubMed PMID: 9817364]
Level 2 (mid-level) evidenceNdirangu K. Bladder calculus causing vesicovaginal fistula in pregnancy. British journal of urology. 1991 Oct:68(4):433-4 [PubMed PMID: 1933171]
Duvdevani M, Sfoungaristos S, Bensalah K, Peyronnet B, Krambeck A, Khadji S, Muslumanuglu A, Leavitt D, Divers J, Okeke Z, Smith A, Fox J, Ost M, Gross AJ, Razvi H. Stones in special situations. World journal of urology. 2017 Sep:35(9):1381-1393. doi: 10.1007/s00345-017-2011-y. Epub 2017 Mar 7 [PubMed PMID: 28271156]
Chakraborty B, Mondal PC, Sahana R, Barman SC. A Giant Vesical Stone Causing Impending Rupture of Bladder During Labor. Journal of obstetrics and gynaecology of India. 2015 Jul:65(4):267-70. doi: 10.1007/s13224-014-0543-2. Epub 2014 Jun 1 [PubMed PMID: 26243995]
Penning SR, Cohen B, Tewari D, Curran M, Weber P. Pregnancy complicated by vesical calculus and vesicocutaneous fistula. American journal of obstetrics and gynecology. 1997 Mar:176(3):728-9 [PubMed PMID: 9077643]
Sandberg M, Cohen A, Escott M, Temple D, Marie-Costa C, Rodriguez R, Gordon A, Rong A, Andres-Robusto B, Roebuck EH, Whitman W, Webb CJ, Stratta RJ, Assimos D, Wood K, Mirzazadeh M. Bladder Stones in Renal Transplant Patients: Presentation, Management, and Follow-up. Urologia internationalis. 2024:108(5):399-405. doi: 10.1159/000539091. Epub 2024 Apr 29 [PubMed PMID: 38684150]
Lipke M, Schulsinger D, Sheynkin Y, Frischer Z, Waltzer W. Endoscopic treatment of bladder calculi in post-renal transplant patients: a 10-year experience. Journal of endourology. 2004 Oct:18(8):787-90 [PubMed PMID: 15659904]
Hahnfeld LE, Nakada SY, Sollinger HW, Rayhill SC, Heisey DM. Endourologic therapy of bladder calculi in simultaneous kidney-pancreas transplant recipients. Urology. 1998 Mar:51(3):404-7 [PubMed PMID: 9510343]
Kim H, Cheigh JS, Ham HW. Urinary stones following renal transplantation. The Korean journal of internal medicine. 2001 Jun:16(2):118-22 [PubMed PMID: 11590898]
Bolen E, Stern K, Humphreys M, Brady A, Leavitt T, Zhang N, Keddis M. Urine metabolic risk factors and outcomes of patients with kidney transplant nephrolithiasis. Clinical kidney journal. 2022 Mar:15(3):500-506. doi: 10.1093/ckj/sfab208. Epub 2021 Oct 20 [PubMed PMID: 35211306]
Cho DK, Zackson DA, Cheigh J, Stubenbord WT, Stenzel KH. Urinary calculi in renal transplant recipients. Transplantation. 1988 May:45(5):899-902 [PubMed PMID: 3285534]
Takemura K, Takazawa R, Kohno Y, Yoshida S, Kato H, Tsujii T. Vesical fungus balls (fungal bezoars) by Candida albicans mimicking urothelial carcinoma in a patient with diabetic neurogenic bladder. Urology case reports. 2018 May:18():50-51. doi: 10.1016/j.eucr.2018.03.005. Epub 2018 Mar 9 [PubMed PMID: 29556476]
Level 3 (low-level) evidenceShievitz M. Male with urinary urgency, frequency, and dysuria. Journal of the American College of Emergency Physicians open. 2022 Apr:3(2):e12696. doi: 10.1002/emp2.12696. Epub 2022 Mar 14 [PubMed PMID: 35316969]
Geller SA, de Campos FPF. Renal papillary necrosis. Autopsy & case reports. 2013 Oct-Dec:3(4):69-71. doi: 10.4322/acr.2013.042. Epub 2013 Dec 31 [PubMed PMID: 28584810]
Level 3 (low-level) evidenceDagrosa LM, Ghali F, Gormley EA. Renal Papillary Necrosis Appearing as Bladder Cancer on Imaging. Journal of endourology case reports. 2016:2(1):27-9. doi: 10.1089/cren.2016.0011. Epub 2016 Feb 1 [PubMed PMID: 27579408]
Level 3 (low-level) evidenceDarwesh S, Chipongo H. An unusual cause of recurrent urinary tract infection in a male patient and diagnostic challenge: a case report. International journal of surgery case reports. 2025 Aug:133():111543. doi: 10.1016/j.ijscr.2025.111543. Epub 2025 Jun 19 [PubMed PMID: 40543444]
Level 3 (low-level) evidenceIshtiaq R, Randhawa A, Zulfiqar L, Shabbir N. An Uncommon Cause of Dysuria in a Female Patient: Huge Urinary Bladder Stones. Cureus. 2017 Oct 20:9(10):e1788. doi: 10.7759/cureus.1788. Epub 2017 Oct 20 [PubMed PMID: 29279814]
Lee P, Haber J. Urethral Calculi. Clinical practice and cases in emergency medicine. 2020 May:4(2):134-136. doi: 10.5811/cpcem.2019.5.43182. Epub 2020 Feb 24 [PubMed PMID: 32426654]
Level 3 (low-level) evidenceMorton A, Tariq A, Dunglison N, Esler R, Roberts MJ. Etiology and management of urethral calculi: A systematic review of contemporary series. Asian journal of urology. 2024 Jan:11(1):10-18. doi: 10.1016/j.ajur.2021.12.011. Epub 2022 Oct 22 [PubMed PMID: 38312816]
Level 1 (high-level) evidencePlanchamp T, Estournes P, Boileau A, Joseph S, Piraprez M, Laclergerie F, Carfagna L, Abbo O. Acute Urinary Retention Secondary to Urethral Lithiasis in a 4-Year-Old Boy: How We Managed This Rare Case. European journal of pediatric surgery reports. 2025 Jan:13(1):e35-e40. doi: 10.1055/a-2663-1933. Epub 2025 Aug 5 [PubMed PMID: 40765700]
Level 3 (low-level) evidenceEl Omri G, Taghouan A, Rais H, Younes H, Rachid M, Heddat A. Urethral Calculus as an Uncommon Cause of Acute Urinary Retention in Women Diagnosis and Management: A Case Report. Clinical medicine insights. Case reports. 2024:17():11795476241274690. doi: 10.1177/11795476241274690. Epub 2024 Aug 20 [PubMed PMID: 39171209]
Level 3 (low-level) evidenceKamal BA, Anikwe RM, Darawani H, Hashish M, Taha SA. Urethral calculi: presentation and management. BJU international. 2004 Mar:93(4):549-52 [PubMed PMID: 15008727]
Badejoko OO, Salako AA, Egharevba P. Overflow urinary incontinence due to bladder stones. International urogynecology journal. 2014 Mar:25(3):425-7. doi: 10.1007/s00192-013-2153-4. Epub 2013 Jun 26 [PubMed PMID: 23801485]
Francisca, Kholis K, Palinrungi MA, Syahrir S, Syarif, Faruk M. Bladder stones associated with vesicovaginal fistula: A case report. International journal of surgery case reports. 2020:75():122-125. doi: 10.1016/j.ijscr.2020.09.028. Epub 2020 Sep 11 [PubMed PMID: 32950941]
Level 3 (low-level) evidenceZhou X, Wei Z, Shi J, Wang M, Xiong Z, Zhang X. Bladder stone as the first clue to a hidden vesicovaginal fistula: diagnostic and surgical insights from a multidisciplinary approach-a case report. Translational andrology and urology. 2026 Feb 28:15(2):70. doi: 10.21037/tau-2025-aw-760. Epub 2026 Feb 11 [PubMed PMID: 41809791]
Level 3 (low-level) evidenceKurmanov TA, Kulkayeva GU, Shakirova AF, Shalekenov SB, Mugalbekov S, Mustafinov DD. Primary vaginal stone associated with vesicovaginal fistula: A case report. Urology case reports. 2022 Jan:40():101917. doi: 10.1016/j.eucr.2021.101917. Epub 2021 Oct 23 [PubMed PMID: 34745904]
Level 3 (low-level) evidenceSharma M, Karn M, Adhikari H, Basnet B, Bhattarai I, Chapagain S, Pandit C. Vesicovaginal fistula associated with massive bladder calculi: An urogynecological case report. Clinical case reports. 2023 Dec:11(12):e8281. doi: 10.1002/ccr3.8281. Epub 2023 Dec 5 [PubMed PMID: 38076019]
Level 2 (mid-level) evidenceNameirakpam S, Naorem S, Faridi MS, Akoijam KS, Sinam RS. Transurethral Cystolithotripsy of Large Bladder Stones by Holmium Laser as a Day Care Procedure. Journal of clinical and diagnostic research : JCDR. 2016 Dec:10(12):PC01-PC02. doi: 10.7860/JCDR/2016/22493.8958. Epub 2016 Dec 1 [PubMed PMID: 28208921]
Vaidyanathan S, Singh G, Selmi F, Hughes PL, Soni BM, Oo T. Complications and salvage options after laser lithotripsy for a vesical calculus in a tetraplegic patient: a case report. Patient safety in surgery. 2015:9(1):3. doi: 10.1186/s13037-014-0052-3. Epub 2015 Jan 23 [PubMed PMID: 25621008]
Level 3 (low-level) evidenceDemirel F, Cakan M, Yalçinkaya F, Demirel AC, Aygün A, Altuğ UU. Percutaneous suprapubic cystolithotripsy approach: for whom? Why? Journal of endourology. 2006 Jun:20(6):429-31 [PubMed PMID: 16808658]
Alsheikh M, Zaman MF, Gopinath P, Qteishat A. Bladder Stones Associated with an Aggressive Plasmacytoid Variant of Urothelial Cancer: A Rare Case and Literature Review. Current urology. 2020 Jan:13(4):217-223. doi: 10.1159/000499268. Epub 2020 Jan 7 [PubMed PMID: 31998055]
Level 3 (low-level) evidenceCoşkun A, Can U, Çanakçı C, Can M. A Fresh Look at Oral Chemolysis for Non-Symptomatic Kidney Stones-Comparative Research of Potassium Citrate and Allopurinol Combination-Is Treatment Possible Without Stone Analysis? Journal of clinical medicine. 2025 Jun 4:14(11):. doi: 10.3390/jcm14113970. Epub 2025 Jun 4 [PubMed PMID: 40507732]
Level 2 (mid-level) evidenceShepherd AJ, Mackay WG, Hagen S. Washout policies in long-term indwelling urinary catheterisation in adults. The Cochrane database of systematic reviews. 2017 Mar 6:3(3):CD004012. doi: 10.1002/14651858.CD004012.pub5. Epub 2017 Mar 6 [PubMed PMID: 28262925]
Level 1 (high-level) evidenceHagen S, Sinclair L, Cross S. Washout policies in long-term indwelling urinary catheterisation in adults. The Cochrane database of systematic reviews. 2010 Mar 17:(3):CD004012. doi: 10.1002/14651858.CD004012.pub4. Epub 2010 Mar 17 [PubMed PMID: 20238325]
Level 1 (high-level) evidence