Introduction
Intravenous regional anesthesia (IVRA), also known as the Bier block, was first described in 1908 by August Bier. The procedure involves exsanguination of the extremity, proximal application of a tourniquet, and intravenous injection of local anesthetic to confine anesthesia to an extremity. Tourniquet pain often limits the duration of the block to less than 60 minutes. Although initially overlooked, the technique regained traction in the 1960s following Charles Holmes’ publications and has since become a staple for short-duration extremity procedures, especially in ambulatory, emergency, and resource-limited environments. The enduring appeal includes rapid onset, minimal equipment requirements, reliable anesthesia, and minimal systemic effects when performed correctly.[1][2][3][4]
Over the past decade, refinements in tourniquet placement, use of adjunctive medications, and safety protocols have enhanced patient comfort and workflow efficiency. Forearm tourniquet techniques, for example, reduce anesthetic volume and tourniquet pain, enabling faster turnover and, in some cases, bypassing the postanesthesia care unit. Emerging data from randomized controlled trials have further validated the efficacy and expanded the potential applications of the Bier block beyond its traditional scope.[5][6][7][8][9][10][11] The block is also successful in managing pain in patients with palmar hyperhidrosis receiving botulinum toxin injections; it serves as an adjunct for complex regional pain syndrome type 1, offering an alternative to repeated stellate ganglion blocks.[12][13] This article reviews anatomy, indications, and contraindications, while exploring technique variations, adjuncts, complications, and interprofessional care aligned with current practice standards.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Relevant anatomy for a Bier block includes the location and distribution of nerves and veins of the upper and lower extremities, especially in the hand and antecubital fossa of the upper extremity, and the foot and ankle of the lower extremity. The superficial and deep venous networks in the hand, forearm, and wrist facilitate anesthetic distribution after exsanguination and tourniquet inflation. The spread of local anesthetics then occurs rapidly. A similar mechanism applies to the lower extremity. Due to their lipophilic nature, local anesthetics, once administered intravenously, diffuse into nearby nerve fibers and block voltage-gated sodium channels on neuronal membranes. The influx of sodium ions into neurons ceases, and the initiation of neuronal depolarization and action potential propagation is inhibited; pain signal transmission to the central nervous system is interrupted.[14] A pneumatic tourniquet inflated to 50 to 100 mm Hg above the systolic blood pressure minimizes systemic distribution of the anesthetic.
Indications
The Bier block is ideal for patients at high risk for general anesthesia, procedures with minimal expected postoperative pain, mass casualty situations involving the extremities, and low-resource settings. Exsanguination is performed with an Esmarch bandage, which may be uncomfortable; adjunct analgesia is used.
Traditional Applications
Traditional indications for Bier block include lower-extremity (distal to the knee) and upper-extremity (hand, wrist, or forearm) procedures lasting less than 60 minutes and with minimal postoperative pain. Standard plastic surgery procedures include carpal tunnel release, trigger finger release, tendon repair, laceration repairs, burn debridement, and foreign body removal. Orthopedic procedures, including Colles fractures, noncomplex wrist and forearm fractures, and dislocations, are routinely performed with IVRA. The method effectively reduces upper extremity fractures in pediatric populations, providing safe, efficient, and cost-effective analgesia compared with conscious sedation. Lower complication rates and fewer interventions for cast tightness have been reported with the Bier block compared with sedation.[1]
Modern Expansions
Placing a tourniquet on the forearm provides equivalent anesthesia with a 50% to 70% reduction in lidocaine dose, improved patient comfort, and reduced need for sedation, without compromising surgical outcomes. Combined forearm IVRA plus hematoma block for distal radius fracture reduction improves analgesia and significantly reduces opioid use.[1][2][3][4][5][6][7][8] The Bier block has been used successfully for pain relief in patients with palmar hyperhidrosis receiving botulinum toxin injections and as an adjunct in the treatment of patients with complex regional pain syndrome type 1, offering an alternative to repeated stellate ganglion blocks.[12][13] These expanded indications highlight IVRA’s evolving versatility, particularly in outpatient and orthopedic trauma care.
Contraindications
Absolute and relative contraindications must be identified and evaluated during the preprocedure assessment to minimize the risk of complications. These contraindications are summarized in Table 1.
Table 1. Contraindications to the Bier block (IVRA)
| Absolute Contraindications | Relative Contraindications |
| Patient refusal or lack of consent | Poor cooperation (young children, cognitively impaired patients) |
| Hypersensitivity to local anesthetics | Obesity that affects cuff placement |
| Deep vein thrombosis or thrombophlebitis | Procedures longer than 60 to 90 minutes (risk of discomfort or loss of anesthesia) |
| Conditions preventing proper limb exsanguination (open fractures, wounds) | Paget disease |
| Uncontrolled hypertension | Sickle cell disease |
| Widespread cellulitis in the surgical limb | Arteriovenous shunts |
Preparation
The following are steps that should be undertaken in preparation for the procedure:
- Monitors and machine: Ensure that the anesthetic monitoring machine is fully operational and that standard monitors, including blood pressure, heart rate, pulse oximetry, and electrocardiogram (baseline and intraprocedure), are available.
- Intravenous access and fluids: Sterile skin preparation set, syringes (20–22 gauge), a 30 to 50 mL Luer-lock syringe, a 500-mL or 1-L bag of crystalloid intravenous fluid, and an infusion set.
- Exsanguination and occlusion: Rubber band, padding (eg, Webril), Esmarch bandage, adhesive tape, and a double pneumatic tourniquet system.
- Local anesthetic agents: Traditionally, lidocaine 0.25% to 0.1% or prilocaine 0.5% is used for this block. More recently, ropivacaine has demonstrated prolonged sensory blockade and fewer central nervous system adverse effects than lidocaine. Bupivacaine has been used successfully, even though routine use is not recommended due to the significant risk of refractory cardiac arrest.[1][2][3][4][15]
- Resuscitation drugs: In addition to standard emergency drugs, have 20% lipid emulsion for local anesthetic systemic toxicity management (and methylene blue for methemoglobinemia if prilocaine is used).
- Adjuncts: Additional medications can enhance analgesia, reduce tourniquet discomfort, shorten onset, improve postoperative pain, and increase patient satisfaction. Common agents include ketorolac (15–30 mg), ketamine, midazolam, dexmedetomidine (0.5–1 mcg/kg), and dexamethasone (4–8 mg). Table 2 lists common adjuncts for the Bier block.
When combined with lidocaine in forearm IVRA, ketorolac significantly reduces postoperative pain and tourniquet discomfort, lowers sedation needs, and is better supported than any other adjunct. Other nonsteroidal anti-inflammatory drugs have less favorable outcomes. α-2 Agonists (clonidine 1–2 mcg/kg, dexmedetomidine 0.5–1 mcg/kg) added to lidocaine extend sensory and motor block duration and improve pain control, though supporting evidence results from small trials. When added to lidocaine or ropivacaine, dexmedetomidine is superior to clonidine in terms of the onset time of sensorimotor blockade, prolongation of sensory recovery, and reduction of intraoperative and postoperative pain scores. Ketamine 50 mg reduces intraoperative analgesic needs and enhances postoperative pain relief.[1][2][5][16][17][18][19][20]
Results from several studies show that fentanyl and other adjuvants allow lower lidocaine concentrations with good results, but findings on their effectiveness and adverse effects are inconsistent. Meperidine 30 mg alone can also produce effective blocks, with higher rates of adverse effects such as nausea, vomiting, and dizziness. Neuromuscular blocking agents combined with IVRA accelerate the onset of sensory and motor blockade and prolong the duration of motor blockade, while maintaining anesthetic quality comparable to that of standard IVRA.
Several agents have been studied as adjuvants to local anesthetics in Bier blocks, such as corticosteroids in patients with rheumatoid arthritis, acetaminophen, nitroglycerin, midazolam, and magnesium sulfate. However, more studies are needed to establish the efficacy, cost-effectiveness, and optimal dosing of these agents. There is limited data on the use of neuromuscular blockers to improve motor block onset and surgical conditions; thus, their use lacks broad clinical validation.[1][21][22][23][24][25][26]
Table 2. Adjuvants to Local Anesthetics Used in Bier Block (IVRA)
|
Category and Adjuvant |
Summary of Evidence |
Adverse Effects |
Clinical Practice |
|
Nonsteroidal anti-inflammatory drug: ketorolac |
Strong evidence from randomized controlled trials supports the efficacy of this approach in improving tourniquet tolerance and extending postoperative analgesia |
Generally well-tolerated; potential for increased bleeding risk or gastrointestinal effects with systemic use |
A routine and effective adjuvant for improving tourniquet tolerance and postoperative pain relief |
|
N-methyl-D-aspartate receptor antagonist: ketamine
|
Reduces onset time, prolongs block duration, and decreases intraoperative and postoperative pain |
Dysphoria, dizziness, hypersalivation |
Anti-inflammatory and pain-signaling properties make it effective in reducing tourniquet and postoperative pain |
|
α-2 agonists: dexmedetomidine
clonidine
|
Effectively improves block quality, shortens onset, prolongs analgesia, and reduces the need for rescue analgesics Evidence is inconsistent, with weaker effects than with dexmedetomidine |
Sedation, bradycardia, or hypotension (dose-dependent)
Hypotension and bradycardia, particularly upon tourniquet release |
A very effective adjuvant for prolonging anesthesia and reducing tourniquet pain
Due to its less favorable safety profile and lower efficacy compared to dexmedetomidine, it is used less frequently |
|
Neuromuscular blocking agents: atracurium cisatracurium |
Shortens the onset of sensory and motor blocks and prolongs the duration of the motor block, which is valuable for more profound muscle relaxation |
Prolonged motor block could delay early patient mobilization. |
Indicated for procedures requiring enhanced muscle relaxation. Careful consideration of the risk of prolonged motor recovery |
|
Others: sodium bicarbonate
|
May accelerate the onset, but not prolong analgesia |
Precipitation, if improperly dosed, can cause metabolic alkalosis or tissue damage upon extravasation |
Useful when the onset is desired, especially for time-sensitive procedures; careful dosing to avoid precipitation |
|
Corticosteroid: dexamethasone |
Evidence for IVRA is limited and conflicting; primarily supports the use of systemic or perineural routes for peripheral nerve blocks |
Neurotoxicity concerns are not relevant to IVRA; systemic effects like hyperglycemia |
Efficacy is not well-established, and it is not a first-line option |
|
Others: magnesium sulfate
|
Evidence for improving block characteristics and tourniquet tolerance is inconsistent. |
Hypotension, bradycardia, and sedation. Toxicity (eg, hyporeflexia, respiratory depression) with high serum levels |
Not a first-line agent; consider in specific cases with careful monitoring |
|
Opioids: fentanyl morphine |
Evidence is consistently poor for improvement in analgesic effects for IVRA |
Not recommended for routine use due to negligible benefit and the risk of postoperative nausea and vomiting |
Not recommended due to unfavorable risk-benefit ratio |
Technique or Treatment
The following are the steps of the Bier block procedure (see Image. Steps of a Bier Block Procedure):
1. Intravenous access placement and exsanguination
- Using strict aseptic precautions, place a well-functioning intravenous catheter (20-gauge) distal to the surgical site. A second intravenous catheter should be placed in a nonoperated extremity site for perioperative use.
- Apply soft, conforming padding (eg, Webril) and place a double-pneumatic tourniquet on the proximal cuff high on the upper extremity.
- Elevate the limb for 1 to 2 minutes, then apply a rubber Esmarch bandage around the arm, spiraling from the fingertips to the distal cuff of the double tourniquet to exsanguinate the arm.
- Note: Improper exsanguination may result in incomplete anesthesia due to residual blood flow and increase the risk of local anesthetic systemic toxicity.
2. Tourniquet inflation
- Inflate the proximal cuff to 50 to 100 mm Hg above systolic blood pressure and confirm occlusion (no distal pulse/plethysmography). The Esmarch bandage is then removed before anesthetic injection.
- Forearm tourniquet technique (if using): Place the tourniquet just distal to the elbow crease. This technique provides a similar anesthetic quality with reduced medication requirements, improved comfort, and decreased sedation and postoperative care unit time.[3][4]
- Single cuff systems are simpler but less comfortable, especially for procedures lasting longer than 20 minutes. They are generally reserved for short interventions or when double-cuff systems are unavailable.[3][4][5]
- Inadequate pressure (fails to occlude circulation), deflation before the minimum time, and a poor seal that leads to leakage of anesthetic and incomplete anesthesia.
3. Anesthetic injection
- Administer preservative-free, epinephrine-free 0.5% lidocaine at a dose of approximately 3 to 4 mg/kg. The volume is typically 30 to 50 mL for the upper extremity technique, but with the forearm technique, 8 to 15 mL may suffice when administered with adjuncts like ketorolac. Conversely, 150 mL of 0.25% lidocaine is commonly used for lower extremity blocks. Ropivacaine and prilocaine 0.5% at a dose of 3 mg/kg are alternatives to lidocaine.[1][2][3][4][5][27]
- Using a proper dose of local anesthetic and adjuncts may mitigate the risk of inadequate anesthesia.
4. Tourniquet duration and release
- Maintain full inflation for at least 20 to 30 minutes; extended durations increase the risk of toxicity upon release. Employ cyclical deflation (deflate for 10 seconds, reinflate for 1 minute) or gradual release to minimize bolus systemic absorption of local anesthetics and metabolic waste.
Complications
Complications
Complications arising from the Bier block are rare. Recent randomized controlled clinical trials using forearm techniques report no significant complications, reinforcing the safety of contemporary practice.[1][2][3][4][5][27] From 1980 to 1999, the American Society of Anesthesiologists' Closed Claims Project reported 3 cases of death or brain damage related to IVRA. These complications and the necessary interventions are summarized in Table 3.
Table 3. Complications of the Bier Block (IVRA)
|
Potential Complication |
Summary of Mitigation Strategy |
|
Local anesthetic systemic toxicity (LAST) |
Prevent LAST by ensuring the tourniquet is fully inflated for at least 20 to 30 minutes, allowing the anesthetic to bind to tissues before release. Clinical signs: Perioral tingling, tinnitus, agitation, seizures, arrhythmias, and cardiovascular collapse. Stop the injection immediately, secure the airway, and administer a bolus of 20% lipid emulsion therapy (1.5 mL/kg) and continue to infuse at 0.25 mL/kg/min or according to established protocols, seizure control (benzodiazepines), and advanced cardiac life support as needed with adjusted drug doses, and continuously monitor the patient because symptoms can recur after several hours. |
|
Tourniquet pain |
This includes a dull, aching, or burning pain 30 to 45 minutes after inflation. Manage pain using the double tourniquet technique: deflate the proximal cuff and inflate the distal cuff over the anesthetized tissue. Ensure proper padding underneath the cuff and consider administering adjuncts (ketorolac, ketamine, or dexmedetomidine). |
|
Nerve injury |
Use the lowest pressure to occlude blood flow. Ensure the cuff is appropriately sized and padded to avoid pinching or excessive pressure on the underlying nerves. Limit the tourniquet inflation time to reduce pressure-related complications. |
|
Compartment syndrome |
This is a rare but severe complication; screen patients for risk factors such as underlying vascular disease or crush injuries. Immediately remove any constrictive dressings, elevate the extremity, and seek immediate surgical consultation for a fasciotomy. |
|
Thrombophlebitis and skin discoloration |
Apply firm pressure to the intravenous site after the intravenous line is removed. Choosing an appropriate intravenous catheter site can also help minimize the risk. Ensure proper tourniquet padding and minimal cuff pressure. |
|
Methemoglobinemia |
Associated with the use of prilocaine. Clinical signs include cyanosis, dyspnea, tachycardia, and acidosis, which may progress to lethargy and coma. There is also a discrepancy between peripheral and arterial oxygen saturation, refractory to oxygen therapy, and a peripheral oxygen saturation in the 85% to 87% range. Methylene blue at a dose of 1 to 2 mg/kg intravenously over 5 minutes (may be repeated hourly: maximum dose 7–8 mg/kg) and dextrose should be administered. Methylene blue is contraindicated in patients with glucose-6-dehydrogenase deficiency, and ascorbic acid (vitamin C) 2 mg/kg is the drug of choice. The risk of methemoglobinemia is mitigated by following strict dosing guidelines for prilocaine and by using the lowest effective dose. |
Clinical Significance
Bier blocks are widely used, providing safe, effective, and cost-efficient anesthesia for short-duration extremity surgeries in various environments.
- Efficiency: Rapid onset, simple equipment, potential to avoid postoperative care unit stays
- Safety: Low risk when standardized protocols are followed
- Comfort: Forearm techniques and adjuncts reduce pain and sedation needs
- Adaptability: Used in outpatient clinics, emergency departments, ambulatory surgery centers, and low-resource settings
Ketorolac is well supported as an adjunct to reduce postoperative pain. Broader use of IVRA may depend on ongoing trials confirming the safety of other agents like dexmedetomidine. Advances in monitoring, pharmacokinetics, and tourniquet technology will likely offer further improvements. Focusing on safety, role clarity, and standardized checklists underpins ongoing excellence in Bier block practice. Although local anesthesia systemic toxicity and methemoglobinemia are rare, knowledge and readiness for treatment are essential.
Enhancing Healthcare Team Outcomes
To enhance patient-centered care, outcomes, and patient safety, coordinated, interprofessional collaboration is necessary:
- Preprocedure teamwork: Nurses, anesthesiologists, and surgeons should identify the indication, assess contraindications, and obtain informed consent before the procedure.
- Equipment preparation: Operating room personnel should ensure the tourniquet is functional and that Esmarch bandages are available. Resuscitation equipment should be present, including 20% lipid emulsion and methylene blue if prilocaine is used.
- Intraprocedure monitoring: Standard American Society of Anesthesiologists' monitors should be used to monitor vital signs. The anesthesia team should monitor patient comfort and, together with the surgical and nursing teams, remain aware of the tourniquet status and duration of inflation, and address potential complications such as local anesthesia systemic toxicity.
- Postprocedure surveillance: After the cuff is deflated, the team should observe for signs of reperfusion syndrome and local anesthesia systemic toxicity, manage analgesia, and assess the extremity for ischemia or nerve injury.
- Quality improvement: The team should also collect outcomes data (eg, incidence of tourniquet pain, episodes of local anesthesia systemic toxicity, postoperative care unit time, and patient satisfaction) to refine protocols and drive continuous practice improvement.
Media
(Click Image to Enlarge)
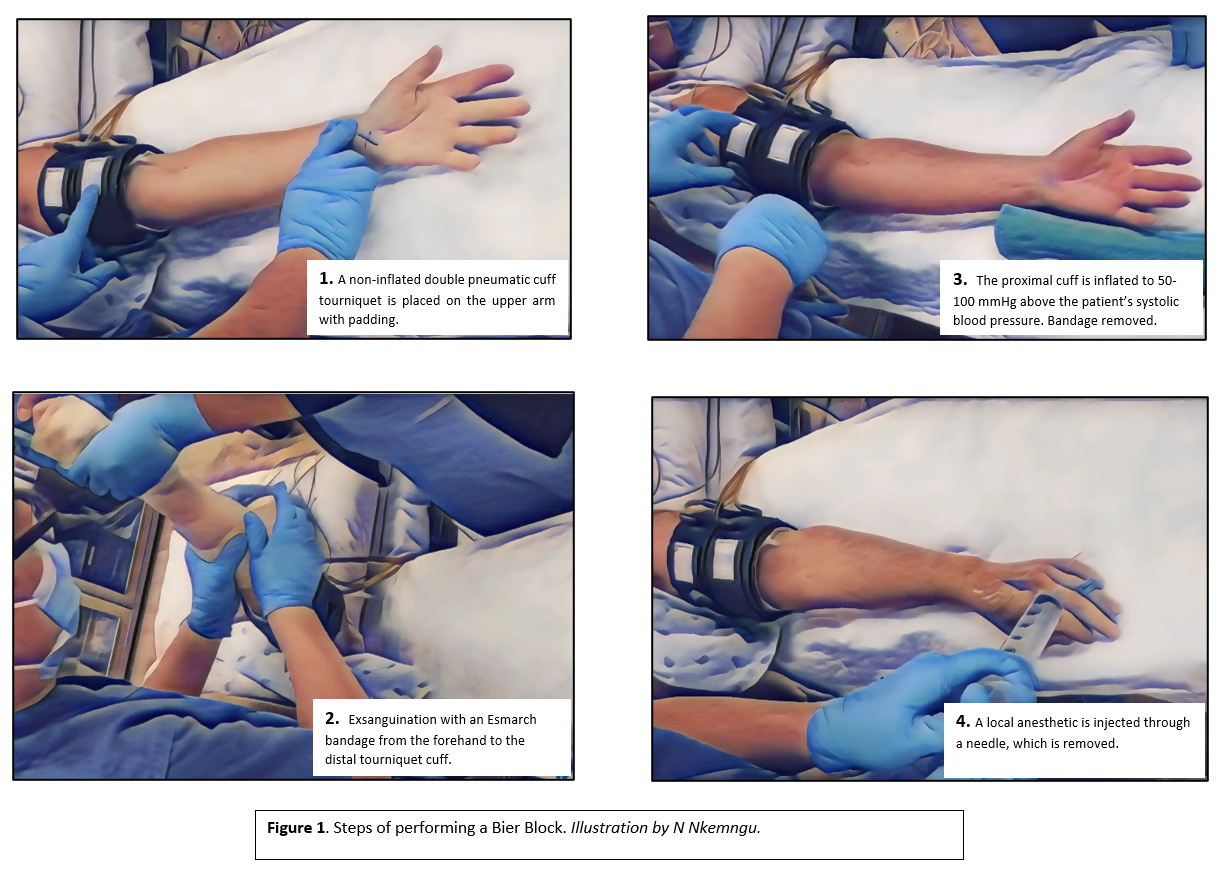
Steps of Performing a Bier Block. Tourniquet placement, exsanguination, inflation, and anesthetic administration during the Bier block procedure.
Contributed by N Nkemngu, MD
References
Löser B, Petzoldt M, Löser A, Bacon DR, Goerig M. Intravenous Regional Anesthesia: A Historical Overview and Clinical Review. Journal of anesthesia history. 2019 Jul:5(3):99-108. doi: 10.1016/j.janh.2018.10.007. Epub 2018 Nov 7 [PubMed PMID: 31570204]
Level 3 (low-level) evidenceTezval M, Spering C. [Intravenous regional anesthesia]. Operative Orthopadie und Traumatologie. 2020 Feb:32(1):13-17. doi: 10.1007/s00064-019-00627-w. Epub 2019 Aug 29 [PubMed PMID: 31468076]
Guay J. Adverse events associated with intravenous regional anesthesia (Bier block): a systematic review of complications. Journal of clinical anesthesia. 2009 Dec:21(8):585-94. doi: 10.1016/j.jclinane.2009.01.015. Epub [PubMed PMID: 20122591]
Level 1 (high-level) evidenceKohan J, Cabanas C, Edalatpour A, Seitz A, Kuei MC, Gander BH. Upper Extremity Blocks for Hand Surgeons: A Literature Review of Regional Anaesthesia Techniques, Efficacy, and Safety. Plastic surgery (Oakville, Ont.). 2024 Nov:32(4):667-676. doi: 10.1177/22925503231184260. Epub 2023 Jul 4 [PubMed PMID: 39430260]
Gola W, Zając M, Cugowski A. Adjuvants in peripheral nerve blocks - the current state of knowledge. Anaesthesiology intensive therapy. 2020:52(4):323-329. doi: 10.5114/ait.2020.98213. Epub [PubMed PMID: 33165883]
Volkmar AJ, Day MA, Fleury IG, Lawler EA, Seering M, Caldwell LS. Safety and Efficacy of Forearm Tourniquet Compared to Upper Arm Tourniquet for Local Intravenous Regional Anesthesia in Hand Surgery: A Randomized Clinical Trial. The Iowa orthopaedic journal. 2021:41(1):177-181 [PubMed PMID: 34552422]
Level 1 (high-level) evidenceDekoninck V, Hoydonckx Y, Van de Velde M, Ory JP, Dubois J, Jamaer L, Jalil H, Stessel B. The analgesic efficacy of intravenous regional anesthesia with a forearm versus conventional upper arm tourniquet: a systematic review. BMC anesthesiology. 2018 Jul 18:18(1):86. doi: 10.1186/s12871-018-0550-4. Epub 2018 Jul 18 [PubMed PMID: 30021514]
Level 1 (high-level) evidenceVaughn N, Rajan N, Darowish M. Intravenous Regional Anesthesia Using a Forearm Tourniquet: A Safe and Effective Technique for Outpatient Hand Procedures. Hand (New York, N.Y.). 2020 May:15(3):353-359. doi: 10.1177/1558944718812190. Epub 2018 Nov 21 [PubMed PMID: 30461326]
Farbood A, Khademi S, Tajvidi R, Hooshangi M, Salari S, Ghani M, Tahmasebi S, Jamali H. Comparison of Intravenous Regional Anesthesia with Single-Cuff Forearm Tourniquet and Hematoma Block and Traditional Method in Patients with Distal Radius Fractures; A Randomized Clinical Trial. Bulletin of emergency and trauma. 2020 Apr:8(2):77-82. doi: 10.30476/BEAT.2020.46446. Epub [PubMed PMID: 32420391]
Level 1 (high-level) evidenceHaghighi M, Mardani-Kivi M, Mirbolook A, Tehran SG, Saheli NA, Hashemi-Motlagh K, Sahbe-Ekhtiari K. A Comparison between Single and Double Tourniquet Technique in Distal Upper Limb Orthopedic Surgeries with Intravenous Regional Anesthesia. The archives of bone and joint surgery. 2018 Jan:6(1):63-70 [PubMed PMID: 29430498]
Fauteux-Lamarre E, Burstein B, Cheng A, Bretholz A. Reduced Length of Stay and Adverse Events Using Bier Block for Forearm Fracture Reduction in the Pediatric Emergency Department. Pediatric emergency care. 2019 Jan:35(1):58-62. doi: 10.1097/PEC.0000000000000963. Epub [PubMed PMID: 27918376]
Grabell DA, Hebert AA. Current and Emerging Medical Therapies for Primary Hyperhidrosis. Dermatology and therapy. 2017 Mar:7(1):25-36. doi: 10.1007/s13555-016-0148-z. Epub 2016 Oct 27 [PubMed PMID: 27787745]
Emami SA, Majedi H, Espahbodi E, Sanatkar M. Bier block as a successful management of a patient with intractable complex regional pain syndrome (CRPS) type 1: A case report. Clinical case reports. 2021 Jul:9(7):e04554. doi: 10.1002/ccr3.4554. Epub 2021 Jul 21 [PubMed PMID: 34306705]
Level 3 (low-level) evidenceGale AL, Liberman SR, Berry S, Zavlin D, Echo A. Fluorescent Imaging Evaluation of Lidocaine Distribution Following Bier Block in the Upper Extremity. Surgical technology international. 2017 Oct 12:31():31-34 [PubMed PMID: 29020710]
Hartmannsgruber MW, Silverman DG, Halaszynski TM, Bobart V, Brull SJ, Wilkerson C, Loepke AW, Atanassoff PG. Comparison of ropivacaine 0.2% and lidocaine 0.5% for intravenous regional anesthesia in volunteers. Anesthesia and analgesia. 1999 Sep:89(3):727-31 [PubMed PMID: 10475314]
Moshiri E, Modir H, Kamali A, Azami M, Molouk M. Comparative analgesic, hemodynamic, pain and duration of sensory and motor block effects of dexmedetomidine, granisetron, and nitroglycerin added to ropivacaine in intravenous anesthesia for forearm surgeries: a randomized clinical study. Medical gas research. 2022 Jul-Sep:12(3):77-82. doi: 10.4103/2045-9912.330690. Epub [PubMed PMID: 34854417]
Level 1 (high-level) evidenceSardesai SP, Patil KN, Sarkar A. Comparison of clonidine and dexmedetomidine as adjuncts to intravenous regional anaesthesia. Indian journal of anaesthesia. 2015 Nov:59(11):733-8. doi: 10.4103/0019-5049.170034. Epub [PubMed PMID: 26755839]
Kaur P, Kundra TS, Sood D. Comparative efficacy of clonidine versus magnesium sulfate as an adjunct to lignocaine in intravenous regional anesthesia for postoperative analgesia: A prospective, randomized, double-blind study. Journal of anaesthesiology, clinical pharmacology. 2017 Jul-Sep:33(3):387-390. doi: 10.4103/joacp.JOACP_18_16. Epub [PubMed PMID: 29109641]
Level 1 (high-level) evidenceKarmaniolou I, Staikou C, Surda P. The Role of Dexmedetomidine as an Additive to Intravenous Regional Anesthesia: A Systematic Review and Meta-analysis. Balkan medical journal. 2021 May:38(3):156-164. doi: 10.5152/balkanmedj.2021.20076. Epub [PubMed PMID: 33593724]
Level 1 (high-level) evidenceDu J, Li C, Zhang W, Lu X, Xia Y, Qin X. Efficacy and Safety of Adding Ketamine to Lidocaine in Intravenous Regional Anesthesia: A Meta-analysis of Randomized Controlled Trials. Journal of perianesthesia nursing : official journal of the American Society of PeriAnesthesia Nurses. 2025 Feb:40(1):195-204.e5. doi: 10.1016/j.jopan.2024.03.013. Epub 2024 Jul 10 [PubMed PMID: 39001742]
Level 1 (high-level) evidenceYektaş A, Gümüş F, Karayel A, Alagöl A. Effects of Addition of Systemic Tramadol or Adjunct Tramadol to Lidocaine Used for Intravenous Regional Anesthesia in Patients Undergoing Hand Surgery. Anesthesiology research and practice. 2016:2016():9161264. doi: 10.1155/2016/9161264. Epub 2016 May 30 [PubMed PMID: 27313608]
Yang Y, Sun S, Song G, Zhang J, Chen R. Efficacy evaluation of neuromuscular blocking agents as adjuncts to intravenous regional anesthesia: a meta-analysis of randomized controlled trials. Frontiers in medicine. 2025:12():1574711. doi: 10.3389/fmed.2025.1574711. Epub 2025 Jul 11 [PubMed PMID: 40718418]
Level 1 (high-level) evidenceMoallemy A, Jarineshin H, Fekrat F, Baghaaei AA, Kamali M, Razavi BM, Shaerzadeh Z. Effect of adding dexamethasone to lidocaine on the quality of intravenous regional anesthesia for upper extremity orthopedic operations: A randomized clinical trial. Electronic physician. 2018 Apr:10(4):6631-6639. doi: 10.19082/6631. Epub 2018 Apr 25 [PubMed PMID: 29881525]
Level 1 (high-level) evidenceKapusuz O, Argun G, Arikan M, Toğral G, Basarir A, Kadiogullari N. Comparison of the effects of low volume prilocaine and alkalinized prilocaine for the regional intravenous anesthesia technique in hand and wrist surgery. BioMed research international. 2014:2014():725893. doi: 10.1155/2014/725893. Epub 2014 Jul 15 [PubMed PMID: 25133177]
Mirkheshti A, Aryani MR, Shojaei P, Dabbagh A. The Effect of Adding Magnesium Sulfate to Lidocaine Compared with Paracetamol in Prevention of Acute Pain in Hand Surgery Patients Under Intravenous Regional Anesthesia (IVRA). International journal of preventive medicine. 2012 Sep:3(9):616-21 [PubMed PMID: 23024850]
Sahmeddini MA, Khosravi MB, Seyedi M, Hematfar Z, Abbasi S, Farbood A. Comparison of Magnesium Sulfate and Tramadol as an Adjuvant to Intravenous Regional Anesthesia for Upper Extremity Surgeries. Anesthesiology and pain medicine. 2017 Dec:7(6):e57102. doi: 10.5812/aapm.57102. Epub 2017 Dec 27 [PubMed PMID: 29696122]
Hilber N, Dodi A, Blumenthal S, Bruppacher H, Borgeat A, Aguirre J. The Impact of Regional Anesthesia in Masking Acute Compartment Syndrome after Limb Trauma. Journal of clinical medicine. 2024 Mar 20:13(6):. doi: 10.3390/jcm13061787. Epub 2024 Mar 20 [PubMed PMID: 38542011]