 Differentiating Pythium Keratitis From Fungal and Acanthamoeba Keratitis: A Practical Guide
Differentiating Pythium Keratitis From Fungal and Acanthamoeba Keratitis: A Practical Guide
Introduction
Microbial keratitis is a significant cause of corneal blindness worldwide. Important but frequently misdiagnosed pathogens include Pythium insidiosum, filamentous fungi, and Acanthamoeba species (spp). Their clinical presentations frequently overlap, and delayed or inappropriate treatment can lead to irreversible vision loss. Therefore, understanding the anatomical basis of infection, natural history, and patterns of spread among these entities is crucial for accurate diagnosis and timely management. Please see StatPearls' companion resource, "Pythium Keratitis," for further information.
The cornea, a transparent avascular structure composed of 5 layers: the epithelium, Bowman layer, stroma, Descemet membrane, and endothelium, which function as both a refractive medium and a barrier to infection. Microbial invasion typically begins with epithelial defects resulting from trauma, surgery, or contact lens wear, followed by stromal colonization. Differences in organismal biology determine the route of invasion, tissue response, and clinical evolution (Table 1).[1]
Table 1. Infection Characteristics by Corneal Layer
|
Layer |
Role in infection dynamics |
Pythium spp |
Fungal |
Acanthamoeba spp |
|
Epithelium |
Primary entry after trauma or contamination |
Rapid breach via enzymatic hydrolysis |
Penetration through microtrauma or contact lenses |
Adhesion through mannose-binding proteins |
|
Stroma |
Main site of colonization |
Dense reticular invasion |
Branching hyphae forming feathery margins |
Perineural spread via stromal nerves |
|
Descemet membrane |
Barrier to deep extension |
Early involvement → endothelial plaque |
Late involvement |
Rarely involved early |
|
Endothelium/ anterior chamber |
Secondary inflammatory response |
Hypopyon, endothelial plaque |
Severe inflammation with exudates |
Ring infiltrate with pain disproportionate to the signs |
Pythium insidiosum keratitis is caused by an aquatic oomycete belonging to the kingdom Straminipila that is found in stagnant water, rice paddies, and moist soil. Infection follows corneal inoculation by contaminated water, vegetation, or soil, particularly in humid, tropical environments. The organism produces slender, aseptate filaments that invade the corneal stroma radially, creating a characteristic reticular or tentacular appearance with limited necrosis but extensive enzymatic degradation. The absence of chitin and ergosterol in its cell wall renders antifungal drugs ineffective. Clinically, the disease progresses rapidly within days, causing severe pain, a grayish, dry-looking stromal infiltrate with tentacular projections, and endothelial plaques (See Image. Pathognomic Features of Pythium insidiosum Keratitis). Notably, the lesion may appear deceptively inactive despite aggressive antifungal therapy, a key diagnostic clue. The natural course is fulminant, often requiring early therapeutic keratoplasty to preserve the globe.[2]
Fungal keratitis, caused by Fusarium, Aspergillus, Curvularia, or Candida organisms, is more common and relatively more indolent than Pythium keratitis. Trauma with plant material or contact lenses is a typical cause. Septate hyphae invade the anterior and midstroma, resulting in necrosis and feathery-edged infiltrates with satellite lesions. The infection evolves over days to weeks and typically responds to natamycin or voriconazole. The infiltrate appears soft, raised, or fluffy, with surrounding edema; descemetocele formation or perforation occurs late in the disease course. Proper identification via potassium hydroxide preparation or Calcofluor White staining, which highlights septate branching hyphae, enables timely antifungal therapy and improves outcomes.[3]
Acanthamoeba keratitis, a parasitic infection caused by Acanthamoeba castellanii and related species, primarily affects contact lens wearers or those exposed to contaminated tap water. The organism adheres to the corneal epithelium through mannose-binding proteins and invades the stroma along corneal nerves. The hallmark feature is perineural inflammation, producing severe pain disproportionate to clinical findings. The disease course is chronic and relapsing, characterized by punctate epithelial erosions progressing to ring infiltrates over weeks. Confocal microscopy reveals double-walled cysts within the stroma. Because of its indolent course, Acanthamoeba keratitis is often misdiagnosed as herpetic or fungal keratitis, leading to delayed diagnosis and prolonged recovery.[4] Table 2 summarizes the distinguishing characteristics of each organism.
Table 2. Clinical Characteristics of Pythium, Fungal, and Acanthamoeba Infections
|
Parameter |
Pythium spp |
Fungal |
Acanthamoeba spp |
|
Incubation/onset |
Acute (3–5 days) |
Subacute (5–10 days) |
Chronic (weeks) |
|
Pain severity |
Severe |
Moderate |
Severe, disproportionate |
|
Infiltrate nature |
Gray, reticular, tentacular |
Fluffy, feathery |
Ring-shaped |
|
Lesion moisture |
Dry |
Wet/necrotic |
Variable |
|
Treatment response |
Poor to antifungals |
Good to antifungals |
Resistant, slow recovery |
|
Course |
Rapid destruction |
Gradual healing |
Relapsing–remitting |
|
Outcome |
Often needs therapeutic keratoplasty |
Medical cure possible |
Prolonged therapy |
The pattern of spread and host inflammatory response further differentiates these infections. Pythium spp spreads centrifugally through stromal lamellae to the Descemet membrane and limbus, provoking an intense neutrophilic reaction and tissue melt. Fungal hyphae, in contrast, cause granulomatous or mixed inflammation, progressing slowly through anterior and midstromal planes. Acanthamoeba spp exhibits unique perineural spread, resulting in radial keratoneuritis and a ring-shaped infiltrate with a lymphocytic host response.[5] Table 3 summarizes the patterns and characteristics of dissemination.
Table 3. Patterns of Dissemination of Pythrium, Fungal, and Acanthamoeba Keratitis
|
Aspect |
Pythium spp |
Fungal |
Acanthamoeba spp |
|
Spread pathway |
Stromal lamellae → Descemet membrane → limbus |
Anterior stroma → midstroma |
Perineural infiltration |
|
Host inflammatory response |
Neutrophilic with tissue necrosis |
Granulomatous or mixed |
Lymphocytic with perineural inflammation |
|
Ulcer margins |
Reticular with tentacles |
Feathery |
Smooth or ring-like |
|
Recurrence |
High post-TPK |
Rare |
Moderate |
|
Tissue reaction |
Cellulose-dominant |
Chitin-dominant |
Cystic |
|
Histopathology |
Aseptate filaments, PAS positive, GMS variable |
Septate, chitin-rich hyphae |
Double-walled cysts |
Abbreviations: GMS, Grocott-Gomori methenamine silver (stain); PAS, periodic acid Schiff (test); TPK, therapeutic keratoplasty.
Diagnostic differentiation among the 3 conditions is notoriously difficult. P insidiosum is often mistaken for filamentous fungal keratitis on smears because of its filamentous morphology.[6] Acanthamoebae cysts may be missed on routine staining unless special techniques such as Calcofluor White or periodic acid-Schiff (PAS) are used. Advanced diagnostic tools such as confocal microscopy, polymerase chain reaction (PCR), and culture on blood agar (for Pythium spp) or nonnutrient agar (for Acanthamoeba spp) enhance specificity.[7] Recently, artificial intelligence (AI)-based diagnostic models using slit-lamp and smartphone images have achieved greater than 90% accuracy in differentiating Pythium keratitis from fungal keratitis, offering promise for point-of-care screening in low-resource regions.
In summary, Pythium keratitis is an acute, aggressive, antifungal-resistant infection characterized by a reticular tentacular infiltrate. In contrast, fungal keratitis has a more indolent course, with fluffy, feathery margins that respond to antifungals. Acanthamoeba keratitis is characterized by a chronic, painful, ring-shaped infiltrate and cystic pathology. Recognizing these distinctions, supported by confocal imaging, microbiology, and AI-driven diagnostics, is vital for appropriate management and visual prognosis. Please see StatPearls' companion resource, "Corneal Ulcer," for further information.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiopathogenesis of Pythium, fungal, and Acanthamoeba keratitis illustrates how pathogens from different biological kingdoms can produce overlapping corneal infections that are often clinically indistinguishable. The differentiation depends not only on morphology and culture characteristics but also on biochemical composition, environmental reservoirs, and mechanisms of corneal invasion. Understanding these distinctions is critical to implementing appropriate therapy, as each pathogen responds differently to medical management.[8] Table 4 summarizes the differences between the 3 organisms.
Pythium Keratitis
Pythium insidiosum is an aquatic oomycete, a fungus-like eukaryote belonging to the kingdom Straminipila (Chromista), phylum Oomycota, and order Pythiales. P insidiosum is not a true fungus, although its hyphal morphology mimics fungal filaments on microscopy, often leading to initial diagnostic confusion.[9]
Biological and structural characteristics:
Unlike fungi, Pythium spp possess cellulose and β-glucans in their cell walls instead of chitin, and the plasma membrane lacks ergosterol. This structure explains intrinsic resistance to most antifungal agents. The organism reproduces both sexually (via oospores) and asexually (via biflagellate zoospores). These motile zoospores are the infective form responsible for corneal inoculation.[10]
Environmental and epidemiological context:
P insidiosum thrives in stagnant or slow-moving freshwater, paddy fields, and muddy soil, particularly in humid, tropical, and subtropical climates. The geographic distribution mirrors agricultural and monsoon patterns, with seasonal surges reported in India, Thailand, northern Australia, and the southeastern US. Studies from India (Gurnani et al, 2022) and Thailand have shown that P insidiosum accounts for 10% to 15% of culture-negative fungal keratitis cases in endemic regions, particularly during the monsoon months (June through September).[11]
Predisposing factors:
The infection commonly follows corneal trauma, contamination with soil or vegetative material, or direct exposure to muddy water during agricultural activities. Additional risk factors include the following:
- Prolonged use of topical antifungals without improvement (suggesting misdiagnosis)
- Contact lens wear with contaminated solutions or poor hygiene
- Ocular surface disease (dry eye, exposure keratopathy)
- Poor socioeconomic and sanitary conditions in rural populations [12]
Mechanism of infection:
The infection begins when zoospores adhere to damaged corneal epithelium, guided by chemotaxis toward exposed collagen. They encyst, germinate, and penetrate the stroma, secreting proteolytic, lipolytic, and cellulolytic enzymes that facilitate tissue invasion. Resulting stromal destruction produces the hallmark reticular or tentacular gray-white infiltrate with minimal necrosis but rapid progression.
Unique features:
Pythium spp filamentous hyphae are broad, ribbon-like, and aseptate, mimicking Mucorales spp but with distinct cellulosic staining patterns (PAS-positive, variably Grocott-Gomori methenamine silver [GMS]-positive). In culture, Pythium spp form a flat, colorless colony on blood agar and do not sporulate on routine fungal media, such as Sabouraud dextrose agar. Leaf-incubation methods and PCR assays targeting the internal transcribed spacer region confirm the diagnosis.[13]
Fungal Keratitis
Fungal keratitis (mycotic keratitis) is caused by true fungi, belonging to the kingdom Fungi, and represents the most common cause of microbial keratitis in tropical countries. Common etiologic agents include filamentous fungi (Fusarium spp, Aspergillus spp, Curvularia spp, and Alternaria spp) and yeasts (Candida albicans).[14]
Environmental and biological characteristics:
Fungal spores are ubiquitous, occurring as saprophytes in soil, on decomposing vegetation, and in the air. Their chitin-rich cell wall and ergosterol-containing plasma membrane are targets of antifungal agents such as natamycin and voriconazole.
Predisposing factors:
Fungal keratitis typically occurs after corneal trauma with vegetative matter, contact lens wear, or preexisting ocular surface disease. Additional risk factors include long-term corticosteroid use, diabetes mellitus, and chronic ocular surface inflammation.[15]
Mechanism of infection:
Following epithelial trauma, fungal spores adhere to the corneal surface and germinate into hyphae that invade through stromal lamellae. The infection progresses slowly, eliciting a granulomatous or mixed inflammatory response. Clinically, it manifests as a feathery-edged infiltrate with satellite lesions, necrotic slough, and stromal thinning. In severe cases, an endothelial plaque and hypopyon form, leading to late-stage perforation.
Geographic and climatic association:
Fungal keratitis is prevalent in tropical and subtropical regions, with Fusarium spp dominating in warm, humid areas and Aspergillus spp in temperate climates. Please see StatPearls' companion resource, "Keratoconjunctivitis," for further information.
Acanthamoeba Keratitis
Acanthamoeba keratitis is a protozoal infection of the cornea caused by Acanthamoeba castellanii, A polyphaga, or A culbertsoni. The organism belongs to the kingdom Protista and exists in 2 forms: the active trophozoite and the resistant double-walled cyst. Both forms can be pathogenic.
Environmental and biological characteristics:
Acanthamoebae organisms are free-living amoeba found in soil, freshwater, swimming pools, and contact lens solutions. The cyst form can survive extreme environmental conditions and disinfectants, thereby complicating eradication.[16]
Predisposing factors:
The most common predisposing factor is contact lens wear, particularly when lenses are rinsed with tap water or worn during swimming. Other risk factors include corneal trauma, exposure to contaminated water, poor hygiene, and use of homemade saline solutions.
Mechanism of infection:
Infection begins when trophozoites attach to the corneal epithelium via mannose-binding proteins, leading to epithelial disruption and stromal penetration. The organism follows perineural pathways, causing severe pain disproportionate to the lesion. Histologically, cysts and trophozoites can be found clustered along corneal nerves.[17]
Pathologic hallmark:
The disease is characterized by radial keratoneuritis in early stages and a ring-shaped stromal infiltrate in advanced stages. Chronic infection and cyst resistance to therapy make management prolonged and challenging.
Table 4. Comparative Etiologic Summary
|
Feature |
Pythium insidiosum keratitis |
Fungal keratitis |
Acanthamoeba keratitis |
|
Kingdom |
Straminipila (Chromista) |
Fungi |
Protista |
|
Taxonomic group |
Oomycete |
True fungi |
Free-living protozoa |
|
Infective form |
Biflagellate motile zoospore |
Spore or hyphae |
Trophozoite and cyst |
|
Reservoir |
Stagnant freshwater, muddy soil |
Soil, vegetation, air |
Water, soil, contact lenses |
|
Predisposing factors |
Water splash, soil exposure, trauma |
Vegetative trauma, lens wear |
Poor lens hygiene, swimming with lenses |
|
Cell wall composition |
Cellulose, β-glucans (no chitin) |
Chitin and glucans |
Cellulose and glycoprotein (cyst wall) |
|
Plasma membrane sterol |
No ergosterol |
Ergosterol present |
Absent |
|
Pathogenic enzymes |
Proteases, lipases, cellulases |
Keratinases, collagenases |
Proteases, neuraminidases |
|
Host response |
Neutrophilic inflammation |
Granulomatous |
Lymphocytic with perineural inflammation |
|
Histopathology |
Aseptate, ribbon-like filaments |
Septate, branching hyphae |
Double-walled cysts and trophozoites |
|
Therapeutic response |
Poor to antifungals; responds to linezolid + azithromycin |
Responds to natamycin and voriconazole |
Responds to biguanides, diamidines |
|
Outcome if untreated |
Rapid perforation, recurrence |
Chronic scarring, possible perforation |
Chronic relapsing, vision loss |
Integrative Perspective
While all 3 pathogens infect via an epithelial breach, their survival strategies and pathogenic mechanisms differ. P insidiosum exploits aquatic conditions and enzymatic destruction for rapid tissue invasion; fungi rely on spore germination and hyphal growth with necrotizing inflammation; Acanthamoeba spp capitalize on neural pathways and cystic resistance for chronic persistence. Misidentification is common because Pythium spp mimic fungal hyphae on microscopy, and Acanthamoeba spp can clinically resemble viral or sterile keratitis. The key differentiator lies in the biological composition of their cell walls and membranes, which dictates drug susceptibility: P insidiosum requires antibiotic-based antioomycete therapy, fungi respond to antifungal agents, and Acanthamoeba requires cysticidal biguanides. In summary, P insidiosum keratitis represents an emerging, environmentally acquired, waterborne corneal infection distinct in origin, structure, and treatment response from fungal and amoebic keratitis. Differentiation based on etiology, environmental exposure, and therapeutic behavior is the cornerstone of preventing mismanagement and improving visual outcomes.[18]
Epidemiology
The global epidemiology of infectious keratitis reveals distinct geographic, demographic, and environmental patterns for Pythium, fungal, and Acanthamoeba infections. While all 3 can cause corneal ulcers that clinically mimic one another, their distribution, seasonal trends, host profiles, and risk exposures vary considerably. Recognizing these epidemiologic nuances is crucial for early clinical suspicion and appropriate microbiological work-up.[19] Table 5 summarizes the epidemiology of each organism.
Pythium insidiosum keratitis is increasingly reported in tropical and subtropical regions, with the highest incidence in Southeast Asia and South Asia. First described in Thailand and India, it has emerged as an important pathogen in humid agricultural belts. In India, the disease is endemic in Tamil Nadu, Kerala, Madhya Pradesh, Rajasthan, and Odisha, particularly during the monsoon and postmonsoon seasons when exposure to muddy water is frequent. Epidemiologic studies by Gurnani et al and Bagga et al report that 10% to 15% of culture-negative fungal keratitis cases in western and southern India are later identified as P insidiosum using molecular testing or specialized culture methods. Globally, sporadic cases have been documented in Australia (Queensland and Northern Territory), China, and the US, typically associated with aquatic exposure or contact with animals (eg, horses, dogs). No strong sex predilection has been reported; however, a slight male predominance (60% to 65%) has been observed, likely reflecting occupational exposure among farmers and outdoor laborers. The affected age range is 30 to 50 years, although pediatric and geriatric cases are increasing. Seasonal peaks coincide with rainfall and irrigation cycles, with a surge from July to October in monsoon climates. The incidence is notably low in temperate regions, where P insidiosum is more commonly associated with zoonotic infections than with human ocular disease.[20]
In contrast, fungal keratitis has the highest global burden among microbial keratitis cases, accounting for 40% to 50% of all corneal ulcers in tropical regions. The prevalence varies widely by geography: highest in South and Southeast Asia, moderate in Africa and South America, and relatively low in North America and Europe. An extensive multicenter analysis (Ung et al, 2022) estimated that fungal keratitis affects more than 1 million people worldwide annually, with 100,000 eyes lost to perforation or blindness. Fusarium species predominate in humid agricultural zones (India, Nepal, Thailand, southern China, and sub-Saharan Africa), whereas Aspergillus spp and Curvularia spp are common in drier areas. The disease exhibits a male preponderance (70%-80%), primarily because men more frequently engage in outdoor, agricultural, or manual labor. The incidence peaks in those aged 20 to 55 years, corresponding to the economically active population. In resource-rich areas, contact lens-related fungal keratitis is more prevalent, particularly with Fusarium solani. Seasonal distribution aligns with harvest periods and monsoon months. Rural populations are disproportionately affected, and limited access to microbiologic testing contributes to misdiagnosis and delayed antifungal therapy.[21]
Acanthamoeba keratitis exhibits a bimodal geographic distribution, being more prevalent in developed, contact-lens–using populations and in rural regions with poor water hygiene. The global incidence is estimated at 1 to 2 cases per million contact lens wearers annually, but this estimate may be underreported. In the US and Europe, 85% to 90% of cases are associated with soft contact lens wear, particularly improper cleaning, exposure to tap water, or swimming with lenses. In contrast, in resource-limited regions like India, Nepal, and Africa, cases linked to trauma, contaminated water exposure, or topical corticosteroid misuse are more prevalent. The disease affects both sexes equally, with a median age of 20 to 40 years. Urban incidence correlates with the popularity of cosmetic and extended-wear lenses. Unlike infections caused by Pythium spp or other fungi, Acanthamoeba infections are not seasonal, although outbreaks often coincide with increased recreational water use in the summer months. Please see StatPearls' companion resource, "Acanthamoeba Keratitis," for further information.
The environmental niche of each pathogen explains its demographic pattern. Pythium spp infections are prevalent in agricultural zones, where standing water and wet soil promote zoospore survival, whereas fungal keratitis is associated with harvest-related corneal trauma from plant material. Conversely, Acanthamoeba keratitis is prevalent in urban, contact lens–using populations, where chlorinated water and inadequate hygiene enable cyst survival. In the US and Europe, Pythium and fungal keratitis are rare, typically acquired through travel or agricultural exposure, whereas Acanthamoeba infections are a recognized public health concern in ophthalmic practice. In India and Southeast Asia, Pythium and fungal keratitis together constitute the major causes of nonbacterial corneal ulcers, with Pythium increasingly recognized as an emerging zoonotic threat.
In summary, Pythium keratitis primarily affects men in rural, agricultural, humid, and tropical areas. Fungal keratitis remains the leading cause of microbial keratitis globally. Acanthamoeba keratitis is increasingly observed among urban contact lens users. These epidemiological distinctions are critical for early differential diagnosis, guiding clinicians toward appropriate microbiologic testing and tailored therapy based on regional exposure patterns. Please see StatPearls' companion resource, "Contact Lens-Related Complication," for further information.
Table 5. Epidemiology of Causative Organisms in Keratitis
|
Parameter |
Pythium keratitis |
Fungal keratitis |
Acanthamoeba keratitis |
|
Kingdom or organism type |
Oomycete (Straminipila) |
True fungi |
Protozoa (free-living amoeba) |
|
Geographic distribution |
Tropical & subtropical regions (India, Thailand, Australia, US) |
Global, especially Asia, Africa, and South America |
Global; higher in industrialized countries with lens wear |
|
Prevalence of microbial keratitis |
5% to 15% of culture-negative ulcers in endemic zones |
40% to 50% in tropical regions |
1% to 2% overall; higher in contact lens users |
|
Seasonal pattern |
Monsoon and postmonsoon (humid climate) |
Harvest and monsoon seasons |
Summer or year-round (recreational water exposure) |
|
Age group most affected |
30–50 years |
20–55 years |
20–40 years |
|
Sex ratio |
Slight male predominance (1.3:1) |
Male predominance (2:1) |
Equal sex distribution |
|
Common occupation |
Farmers, fishermen, rural laborers |
Agricultural workers, manual laborers |
Contact lens wearers (urban), swimmers |
|
Risk exposure |
Water splash, muddy soil, agricultural trauma |
Vegetative trauma, contaminated dust |
Tap water, contact lens solutions, and swimming |
|
Endemic zones |
India, Thailand, Queensland (Australia) |
India, Nepal, Africa, South America |
US, Europe, Japan, India |
|
Approximate annual incidence |
<5 per 100,000 in endemic regions |
100–500 per 100,000 (tropics) |
1–2 per million contact lens wearers |
Pathophysiology
The pathophysiology of Pythium insidiosum, fungal, and Acanthamoeba keratitis differs significantly, reflecting their distinct phylogenetic origins and modes of host interaction. While all 3 pathogens cause corneal inflammation through epithelial breach, stromal invasion, and immune activation, their patterns of tissue destruction, cellular tropism, and host inflammatory responses are distinct.
Pythium insidiosum Keratitis
Pythium insidiosum is an aquatic oomycete that mimics filamentous fungi morphologically but is phylogenetically closer to algae. The biflagellate motile zoospores are the infective stage. These zoospores exhibit chemotaxis toward injured corneal epithelium, attracted by corneal amino acids, lipids, and carbohydrates. Upon reaching the corneal surface, they encyst and germinate into aseptate, filamentous hyphae that penetrate the stroma. The organism’s cell wall is composed of cellulose and β-glucans instead of chitin, and its plasma membrane lacks ergosterol. This structural composition accounts for resistance to conventional antifungal agents and a predisposition to rapid stromal invasion. Once established in the corneal stroma, P insidiosum secretes an array of hydrolytic enzymes, including proteases, lipases, esterases, and cellulases, which digest collagen and keratocytes, resulting in stromal necrosis and lamellar disorganization. The infiltrate adopts a reticular or tenacular pattern, corresponding to hyphal extensions along stromal lamellae.[13]
Host recognition occurs through pattern recognition receptors on corneal epithelial and immune cells, triggering innate immune activation via Toll-like receptor–mediated pathways. The ensuing neutrophilic infiltration and cytokine release (IL-1β, IL-6, tumor necrosis factor–α [TNF-α]) exacerbate tissue damage. The organism’s biofilm-like growth and its ability to evade oxidative killing allow it to persist despite inflammation. In advanced stages, P insidiosum invades the Descemet membrane and endothelium, forming endothelial plaques and hypopyon, with potential extension into the sclera. The pathophysiologic hallmark of Pythium keratitis is rapid stromal destruction with minimal suppuration, producing a dry, gray-white reticular ulcer that progresses centrifugally. The organism’s enzymatic aggression, poor immune clearance, and antifungal resistance culminate in rapid perforation unless the organism is surgically excised.[22]
Fungal Keratitis
Fungal keratitis arises from infection by filamentous or yeast-like fungi, typically Fusarium, Aspergillus, or Candida spp. The infection begins when fungal spores adhere to a disrupted epithelial surface and germinate into septate branching hyphae. These hyphae penetrate the Bowman layer and corneal stroma, releasing keratinases, collagenases, and phospholipases that digest the extracellular matrix. The fungi elicit a granulomatous inflammatory response with macrophages, multinucleated giant cells, and lymphocytes surrounding fungal filaments. This immune reaction produces necrotic sloughing and stromal edema, resulting in the classic feathery-edged infiltrate with satellite lesions.[23]
As hyphae advance, they extend along corneal lamellae, promote localized ischemia, and contribute to endothelial damage. The host immune response contributes significantly to tissue injury. Toll-like receptor 2 and dectin-1 signaling activate nuclear factor kappa-light-chain enhancer of activated B-cell pathways, upregulating IL-8 and TNF-α, which recruit neutrophils. These cells, while microbicidal, also release matrix metalloproteinases that intensify stromal melt. The chronic phase is characterized by fibrosis and neovascularization, resulting in scarring. In Candida keratitis, the yeast invades deeper corneal layers, leading to suppuration and abscess formation rather than dry necrosis.[24]
Acanthamoeba Keratitis
Acanthamoeba species are freeliving protozoa with 2 life stages—trophozoite (active) and cyst (dormant). The trophozoite stage initiates infection by adhering to damaged corneal epithelium, a process mediated by mannose-binding proteins on the amoebic surface that recognize mannose residues on epithelial glycoproteins. After attachment, Acanthamoeba spp secretes proteases (serine and cysteine proteases), phospholipases, and neuraminidases, leading to epithelial lysis and apoptosis. The trophozoites penetrate the stroma, often traveling along corneal nerves (perineural spread). This neural invasion results in radial keratoneuritis, which explains the intense, disproportionate pain that is a hallmark of this disease.[25]
Within the stroma, Acanthamoeba organisms alternate between trophozoite and cyst forms in response to nutrient and oxygen availability. The cyst form, with a double-walled structure composed of cellulose and glycoproteins, confers resistance to host defenses and medications. Chronic infection leads to ring-shaped stromal infiltrate, dense scarring, and recurrent inflammation due to cyst reactivation. The host immune response is predominantly cell-mediated, involving T helper 1 cytokines (interleukin-12 and interferon γ) and macrophage activation. However, ineffective clearance allows persistent infection and chronic inflammation.[26]
Integrated Pathophysiologic Summary
All 3 pathogens exploit an epithelial breach as the entry point into the cornea, but their downstream mechanisms differ profoundly. Pythium spp uses motile zoospores to locate and colonize damaged tissue, spreading rapidly through enzymatic degradation and limited host containment. Fungal pathogens rely on spore germination and chronic granulomatous inflammation, resulting in necrotic slough and delayed healing. In contrast, Acanthamoeba spp exhibit neurotropic invasion and cystic persistence, leading to chronic pain and recurrent disease. In Pythium infections, the combination of rapid enzyme-mediated tissue lysis, antifungal resistance, and immune-mediated collateral damage results in a highly aggressive ulcer that often perforates early. In fungal infections, chronic inflammation and necrosis dominate, whereas Acanthamoeba infection primarily induces neuritis and chronic stromal inflammation.
Although the clinical manifestations (corneal ulcer, infiltrate, and hypopyon) may appear similar, the underlying cellular and immunopathologic mechanisms are distinct. This understanding underscores why Pythium infections require early antibiotic-based therapy or keratoplasty, fungi require antifungal therapy, and Acanthamoeba infections require cysticidal treatment with biguanides, each tailored to the organism’s unique biology and host interactions.[27] Table 6 compares the pathophysiology of the 3 organisms.
Table 6. Pathophysiology of Keratitis
|
Feature |
Pythium keratitis |
Fungal keratitis |
Acanthamoeba keratitis |
|
Causative group |
Oomycete (fungus-like) |
True fungi |
Protozoa |
|
Infective form |
Motile biflagellate zoospore |
Conidia/spores |
Trophozoite and cyst |
|
Initial site of infection |
Damaged corneal epithelium |
Corneal trauma or epithelium |
Epithelium, nerve plexus |
|
Mode of invasion |
Zoospore encystment → hyphal penetration |
Hyphal germination → stromal invasion |
Adhesion via mannose-binding protein → perineural migration |
|
Enzymes/toxins |
Proteases, lipases, cellulases |
Collagenases, keratinases, phospholipases |
Proteases, neuraminidases |
|
Host immune response |
Neutrophilic (acute destructive) |
Granulomatous/mixed |
Lymphocytic, T-helper 1–mediated |
|
Tissue pattern |
Reticular, tentacular stromal infiltration |
Feathery, necrotic infiltrate |
Ring infiltrate, keratoneuritis |
|
Pain severity |
Severe, early |
Moderate |
Severe, disproportionate |
|
Progression rate |
Rapid (days) |
Moderate (days to weeks) |
Slow (weeks to months) |
|
Histopathology |
Aseptate ribbon-like filaments |
Septate branching hyphae |
Double-walled cysts and trophozoites |
|
Drug response |
Resistant to antifungals; responds to antioomycete antibiotics |
Sensitive to natamycin/voriconazole |
Responds to biguanides, diamidines |
Histopathology
Microscopic examination of corneal tissue is pivotal for distinguishing Pythium insidiosum from fungal and Acanthamoeba keratitis. Each organism exhibits distinct morphologic and staining characteristics that reflect its biological composition and pathologic interaction with the cornea. Understanding these histopathological signatures is essential for accurate diagnosis, particularly in cases that are unresponsive to standard antifungal therapy. Table 7 compares the histopathology of each organism.
Pythium insidiosum Keratitis
Histopathologically, Pythium keratitis displays aseptate or sparsely septate, broad, ribbon-like filaments that infiltrate the stroma in a reticular or net-like pattern. The filaments typically measure 3 to 8 μm in diameter, have irregular contours, and often branch at right or wide angles. Unlike true fungal hyphae, Pythium filaments lack chitin and ergosterol, and they do not show parallel walls or dichotomous branching.[28]
Tissue localization and reaction:
The organism primarily affects the anterior and midstroma, although deeper layers, including the Descemet membrane, may be invaded in advanced disease. The stroma shows intense neutrophilic infiltration, stromal edema, and focal necrosis, with minimal granulomatous reaction. Limbal and scleral extension may be observed in progressive stages.
Staining characteristics:
- Hematoxylin and eosin (H&E): Filaments appear as refractile, eosinophilic, and poorly septate strands within a necrotic stromal matrix.
- Periodic acid–Schiff (PAS): Positive due to β-glucan and cellulose content; highlights Pythium filaments as light pink to magenta.
- Gomori methenamine silver (GMS): Variable staining, some filaments stain faintly or inconsistently due to the absence of chitin, unlike true fungi.
- Gram stain: Often weakly positive; filaments may appear as Gram-variable.
- Calcofluor White: May exhibit faint fluorescence due to minimal cellulose cross-linking.[29]
Distinctive features:
- Absence of chitin and ergosterol (unlike fungi).
- Lack of fruiting bodies or spores in tissue.
- Necrotic stroma with minimal suppuration, correlating with clinical dry appearance.
- Reticular stromal pattern consistent with tentacular infiltration.
Immunohistochemistry and PCR-based identification (amplification of the internal transcribed spacer 1 [ITS1] and cytochrome c oxidase [COX2] genes) confirm the diagnosis, especially when culture fails. The leaf-incubation technique facilitates sporulation and differentiation in zygomycetes.[19]
Fungal Keratitis
Fungal keratitis is characterized by septate or nonseptate hyphae, depending on the species. Fusarium and Aspergillus species demonstrate septate, slender hyphae (2–5 μm in diameter) with acute-angle (45°) branching, while Mucorales (eg, Rhizopus spp) are broad and aseptate, similar to Pythium but distinguished by their thick walls and stronger GMS affinity.
Tissue features:
The corneal stroma shows dense inflammatory infiltrate comprising neutrophils, macrophages, and multinucleated giant cells, forming a granulomatous reaction around fungal filaments. There is stromal necrosis, keratocyte loss, and edema, often associated with suppuration. In severe cases, fungi penetrate the Descemet membrane, resulting in an endothelial plaque and a hypopyon.[30]
Staining characteristics:
- H&E: Hyphae appear as eosinophilic, refractile, and septate filaments with acute branching.
- PAS and GMS: Strong positivity due to chitin-rich cell walls. GMS stains hyphae black against a green background, providing excellent contrast.
- Calcofluor White: Brilliant blue fluorescence of chitinous filaments under ultraviolet light.
Distinctive features:
- Septate branching hyphae with dichotomous (45°) branching.
- Chitin-rich cell wall confers uniform GMS and Calcofluor White positivity.
- Granulomatous inflammation with suppuration and necrosis.
- Possible endothelial and scleral invasion in advanced cases.[31]
Acanthamoeba Keratitis
Histopathology of Acanthamoeba keratitis demonstrates 2 morphologic forms within the corneal tissue: trophozoites (active) and cysts (dormant). Trophozoites are 15 to 45 μm, irregularly shaped with a single nucleus and a prominent central karyosome. They are usually located along stromal lamellae and corneal nerves, consistent with the organism’s neurotropic nature. Cysts are 10 to 25 μm, round or ovoid with a double-walled structure, an outer ectocyst (irregular, wrinkled) and an inner endocyst (spherical and refractile).
Tissue reaction:
In chronic cases, the stroma shows perineural inflammation (radial keratoneuritis), lymphocytic infiltration, and stromal necrosis. Early infection may show minimal cellular reaction, whereas late-stage disease presents with granulomatous inflammation and fibrosis.[32]
Staining characteristics:
- H&E: Trophozoites appear basophilic with a distinct nucleus and nucleolus; cysts show double-walled morphology.
- PAS: Highlights cyst walls due to polysaccharide content.
- GMS: May weakly stain cysts and trophozoites.
- Calcofluor White: Shows brilliant fluorescence outlining cyst walls.
- Giemsa: Stains trophozoites and cysts blue to violet, facilitating identification.
Distinctive features:
- Double-walled cysts are resistant to degeneration.
- Perineural localization causing neuritis.
- Coexistence of trophozoites and cysts, especially in chronic or recurrent disease.
- The absence of hyphae distinguishes Acanthamoeba keratitis from Pythium and other fungal infections.[9]
Table 7. Comparative Histopathologic Features
|
Feature |
Pythium keratitis |
Fungal keratitis |
Acanthamoeba keratitis |
|
Causative organism type |
Oomycete (fungus-like) |
True fungi |
Protozoa |
|
Filament morphology |
Aseptate, broad (3–8 μm), ribbon-like, right-angle branching |
Septate, narrow (2–5 μm), acute-angle branching |
No filaments; trophozoites and cysts |
|
Cell wall composition |
Cellulose and β-glucans (no chitin) |
Chitin and glucans |
Cellulose and glycoprotein (cyst) |
|
Stromal pattern |
Reticular/tentacular |
Feathery or necrotic |
Ring-like or perineural |
|
Inflammatory reaction |
Neutrophilic, necrotic, minimal granulomatous |
Granulomatous with suppuration |
Lymphocytic with perineural inflammation |
|
Staining (PAS) |
Positive (weak-moderate) |
Strongly positive |
Highlights the cyst wall |
|
Staining (GMS) |
Variable or weak |
Strongly positive |
Weak to moderate |
|
Special stains |
Calcofluor (faint), Gram (variable) |
Calcofluor (strong), GMS (black) |
Giemsa, Calcofluor highlight cysts |
|
Distinctive feature |
Ribbon-like aseptate filaments; no ergosterol |
Septate branching hyphae |
Double-walled cysts; perineural spread |
|
Host reaction severity |
Acute and destructive |
Chronic and necrotizing |
Chronic, relapsing inflammation |
Abbreviations: GMS, Gomori methenamine silver; PAS, periodic acid-Schiff staining.
Summary Interpretation
Histopathologically, Pythium keratitis is typified by aseptate, ribbon-like cellulose filaments within a necrotic, inflamed stroma and variable GMS staining, setting it apart from fungal keratitis, which shows septate, chitin-rich hyphae with strong silver staining and granulomatous reaction. Acanthamoeba keratitis is characterized by the presence of trophozoites and double-walled cysts, particularly around corneal nerves, which correlate with its neuritogenic pain. In conclusion, histopathology remains the gold standard for differentiating filamentous and protozoal keratitides, especially in antifungal-refractory ulcers. The combined evaluation of morphology, staining patterns, and host inflammatory response provides the diagnostic clarity necessary for targeted management: antibiotic therapy for Pythium, antifungal therapy for fungi, and cysticidal therapy for Acanthamoeba infections.[33]
Toxicokinetics
Although toxicokinetics traditionally pertains to the absorption, distribution, metabolism, and excretion of toxic substances, in the context of infectious keratitis, it can be interpreted as the pharmacokinetic and tissue-toxicity implications of therapeutic agents used against these pathogens and their interactions with corneal tissue. Understanding these pharmacokinetic and toxicologic relationships is crucial for optimizing treatment efficacy while minimizing iatrogenic damage in Pythium, fungal, and Acanthamoeba keratitis.[34] Table 8 compares the toxicokinetic features of keratitis treatments.
Pythium insidiosum Keratitis
The pharmacologic management of Pythium keratitis presents unique toxicokinetic challenges because the organism’s cell wall lacks chitin and ergosterol—the primary antifungal targets. This structural difference makes Pythium intrinsically resistant to most antifungal drugs (eg, natamycin, voriconazole, amphotericin B), leading to prolonged drug exposure, cumulative epithelial toxicity, and delayed healing.
Antimicrobial agents and kinetics:
The drugs most effective against Pythium are antioomycete antibiotics rather than antifungals, including the following:
- Linezolid (0.2%–0.5% suspension)
- Azithromycin (1% suspension)
- Minocycline (1% suspension)
- Cefazolin (5% suspension) [20]
These antibiotics exhibit concentration-dependent killing, and their therapeutic efficacy depends on maintaining high stromal bioavailability through frequent topical application. However, chronic dosing induces epithelial toxicity, superficial punctate keratopathy, and stromal haze, particularly with macrolides and oxazolidinones.
Corneal pharmacokinetics:
Topical linezolid penetrates the corneal stroma effectively but accumulates in the epithelium, resulting in dose-dependent mitochondrial dysfunction and oxidative stress. Because of its lipophilicity, azithromycin achieves sustained stromal concentrations, but long-term use may cause ocular surface dryness and punctate epithelial erosions.
Postkeratoplasty considerations:
Following therapeutic penetrating keratoplasty (TPK), systemic linezolid achieves moderate aqueous levels but may cause systemic myelosuppression and optic neuropathy with prolonged use (>2 weeks). Hence, systemic therapy is generally limited to short-term courses (7–10 days) and combined with topical maintenance therapy.[35]
Summary:
- Primary toxic-kinetic consideration: Epithelial mitochondrial toxicity from antibiotic accumulation.
- Unique feature: Drug–organism mismatch requiring prolonged antibiotic therapy and surgical excision for definitive cure.[36]
Fungal Keratitis
The toxicokinetic profiles of antifungal agents, particularly natamycin, amphotericin B, and voriconazole, play a significant role in determining therapeutic outcomes and corneal tolerance.
Natamycin (5% suspension):
- Kinetics: Poor stromal penetration; primarily acts on the anterior cornea.
- Toxicity: Prolonged use causes epithelial edema, punctate keratitis, and stromal haze.
- Mechanism: Binds ergosterol in fungal cell membranes, creating pores. Systemic absorption is minimal; however, cumulative irritation of the epithelium may occur with prolonged use.[37]
Voriconazole (1% solution or 200 mg oral):
- Kinetics: Excellent corneal and aqueous penetration; systemic bioavailability is approximately 90%.
- Toxicity: Photosensitivity, hepatotoxicity, and neurotoxicity with systemic administration; topical use may cause burning, redness, and delayed epithelialization.
- Corneal metabolism: The active drug persists in stromal tissue for approximately 6 hours; optimal dosing is every 2 to 3 hours.
Amphotericin B (0.15%–0.5% solution):
- Kinetics: Strong fungicidal action but poor tissue diffusion.
- Toxicity: Epithelial toxicity may cause dense epithelial defects, keratocyte apoptosis, and Descemet folds.
- Mechanism: Induces lipid peroxidation in both fungal and host cell membranes.[38]
Systemic implications:
Oral or intravenous antifungals such as itraconazole and fluconazole, although less toxic to the eye, undergo hepatic metabolism, necessitating monitoring of liver function during prolonged therapy.
Summary:
- Primary toxic kinetic mechanism: Ergosterol-targeted collateral membrane damage to the host corneal epithelium.
- Toxic pattern: Dose- and duration-dependent epithelial and stromal injury, potentiated by corticosteroid misuse.[39]
Acanthamoeba Keratitis
The agents used against Acanthamoeba organisms include biguanides (polyhexamethylene biguanide [PHMB] 0.02% solution, chlorhexidine 0.02%–0.06% solution) and diamidines (propamidine isethionate 0.1% solution, hexamidine 0.1% solution). These agents exhibit potent cysticidal activity but narrow therapeutic indices, resulting in significant epithelial and stromal toxicity during prolonged therapy.
Biguanides:
- Mechanism: Disrupts cytoplasmic membranes of trophozoites and cysts by binding to phospholipids.
- Kinetics: Limited corneal penetration; requires frequent dosing (hourly) for several weeks.
- Toxicity: Severe epithelial breakdown, stromal edema, and neurotrophic keratitis. Prolonged exposure can delay epithelial healing and lead to corneal melt in 10% to 15% of cases.
Diamidines:
- Mechanism: Interfere with DNA synthesis and membrane integrity.
- Kinetics: Good superficial corneal bioavailability but poor deep stromal penetration.
- Toxicity: Burning, photophobia, conjunctival hyperemia, and allergic blepharoconjunctivitis.[40]
Systemic safety: Both classes have minimal systemic absorption; however, combined long-term use (>3 months) increases the risk of ocular surface inflammation and fibrosis.
Summary:
- Major toxic kinetic mechanism: Nonselective cationic detergent effect on corneal epithelial membranes.
- Management challenge: Balancing cysticidal efficacy with tolerable epithelial toxicity through tapering or combination therapy.[41]
Table 8. Comparative Toxicokinetic Features
|
Parameter |
Pythium keratitis (antibiotics) |
Fungal keratitis (antifungals) |
Acanthamoeba keratitis (biguanides/diamidines) |
|
Primary drugs used |
Linezolid, azithromycin, minocycline |
Natamycin, voriconazole, and amphotericin B |
PHMB, chlorhexidine, propamidine |
|
Target structure |
Protein synthesis (ribosomal binding) |
Ergosterol in the fungal membrane |
Cytoplasmic membrane (trophozoites/cysts) |
|
Corneal penetration |
Moderate to good (lipophilic antibiotics) |
Variable (best with voriconazole) |
Poor to moderate (requires hourly dosing) |
|
Systemic metabolism |
Hepatic (linezolid), minimal local metabolism |
Hepatic (azole antifungals) |
Negligible systemic absorption |
|
Local toxicity |
Epithelial toxicity, mitochondrial inhibition |
Epithelial edema, stromal haze, necrosis |
Epithelial sloughing, keratopathy, melt |
|
Systemic toxicity |
Optic neuropathy, myelosuppression (linezolid) |
Hepatotoxicity (azole), nephrotoxicity (amphotericin) |
Minimal systemic risk |
|
Therapeutic index |
Moderate; surgical intervention may be required |
Narrow; dose-dependent corneal toxicity |
Narrow; frequent dosing limits tolerance |
|
Duration of therapy |
2–3 weeks (often post-TPK) |
4–6 weeks |
3–6 months |
|
Unique toxic kinetic issue |
Nonfungal target mismatch causing overexposure |
Ergosterol binding damages host membranes |
Cationic detergent effect on epithelium |
Abbreviations: PHMB, polyhexamethylene biguanide; TPK, therapeutic penetrating keratoplasty.
Integrative Perspective
From a toxicokinetic standpoint, Pythium keratitis represents a therapeutic paradox; antifungal agents are toxic yet ineffective, while antibacterial agents are effective but epitheliotoxic with prolonged exposure. In fungal keratitis, topical and systemic drugs may achieve deep tissue penetration but can produce dose- and duration-dependent epithelial degeneration and organ toxicity with long-term use. Treatment of Acanthamoeba keratitis, although vision-saving, carries the highest burden of ocular surface toxicity and necessitates vigilant epithelial support with lubricants, judicious corticosteroids (after cyst clearance), and amniotic membrane transplant (AMT). Understanding these drug–tissue kinetic interactions is crucial for tailoring regimens that maximize antimicrobial activity while minimizing host toxicity, ensuring visual rehabilitation and corneal integrity across all 3 conditions.[42]
History and Physical
Patients presenting with Pythium, fungal, or Acanthamoeba keratitis typically report acute ocular symptoms, including pain, redness, photophobia, watering, and reduced visual acuity. However, detailed history-taking reveals characteristic exposure patterns and treatment responses that help differentiate these conditions early. Pythium keratitis frequently occurs in individuals with recent exposure to agricultural settings or muddy water, especially during the monsoon or postmonsoon period. A history of minor corneal trauma with contaminated soil, paddy field water splash, or vegetative matter is common. Symptoms progress rapidly over 3 to 5 days, and a significant clue is a lack of improvement or worsening despite intensive antifungal therapy, leading clinicians to reconsider the initial diagnosis.
In contrast, fungal keratitis typically results from trauma, exposure to airborne fungal spores, or contact lens wear in humid environments. The onset is more indolent, progressing gradually over a week or more, and patients may report a blind spot or a foreign-body sensation. While pain is present, its severity correlates relatively more closely with the visible corneal findings. Patients may also have a history of topical corticosteroid use, which can exacerbate fungal invasion and deep stromal penetration.[22]
For Acanthamoeba keratitis, contact lens wear and water exposure (eg, swimming, rinsing lenses with tap water, or homemade solutions) are major risk factors. The hallmark clinical clue is disproportionately severe pain compared to early clinical signs, often described as stabbing or neuralgic in nature. In non–lens-wearing populations in resource-limited regions, exposure to contaminated water or trauma in soil-rich environments may be identified. Because symptoms may wax and wane for weeks to months, patients are often initially misdiagnosed with viral or fungal keratitis.
Physical examination using slit-lamp biomicroscopy further differentiates these conditions. Pythium keratitis classically demonstrates a dry, gray-white stromal infiltrate, with a reticular or tentacular pattern extending deep along stromal lamellae. Early endothelial plaques and dense hypopyon may develop even when the ulcer appears clinically inactive, reflecting rapid stromal invasion. Corneal melt and perforation may occur early if unrecognized. In fungal keratitis, the ulcer typically appears fluffy or raised with feathery margins and satellite lesions, indicating active granulomatous inflammation. The infiltrate is often centrally necrotic, and as the disease advances, a thick endothelial plaque and hypopyon may form.[43]
Conversely, Acanthamoeba keratitis initially presents with subtle epithelial changes, such as punctate erosions, pseudodendrites, or epithelial defects. A striking diagnostic sign is radial keratoneuritis, in which the corneal nerves appear thickened and inflamed, which accounts for the intense pain. As the disease progresses, a ring-shaped stromal infiltrate emerges, typically in the midstroma, accompanied by diffuse stromal edema. Despite aggressive early inflammation, corneal perforation is less common than in Pythium keratitis, unless secondary infection develops.
Overall, careful assessment of exposure history, disease progression, response to empirical antifungal therapy, and characteristic slit-lamp morphology enables early and accurate differentiation. Recognizing dry, rapidly destructive tentacular infiltrates that are unresponsive to antifungals strongly favors Pythium keratitis. Feathery infiltrates and satellite lesions are hallmarks of fungal infection, whereas severe pain disproportionate to the clinical appearance, especially in contact lens users, is highly suggestive of Acanthamoeba keratitis.[44]
History
A thorough history should focus on exposure, risk behaviors, and response to prior treatment. Table 9 summarizes the important elements of the patient history for each organism. Table 10 presents important physical examination cues, and Table 11 lists clinical diagnostic pearls. Table 12 presents a quick, clinical summary.
Table 9. Patient History Clues in Keratitis
|
Key history element |
Pythium keratitis |
Fungal keratitis |
Acanthamoeba keratitis |
|
Precipitating event |
Minor trauma with muddy water/paddy field soil splash |
Trauma with vegetative matter (eg, sugarcane leaf) |
Contact lens wear (poor hygiene or water exposure) |
|
Exposure setting |
Rural agricultural activities (monsoon season) |
Farming, gardening, and airborne spores |
Tap water rinsing, swimming, and hot tubs |
|
Onset and progression |
Acute, rapid worsening in days |
Subacute, gradual progression |
Chronic, waxing–waning |
|
Pain severity |
Severe early pain |
Moderate pain |
Disproportionately severe pain from slit-lamp examination |
|
Response to treatment |
No improvement with antifungals |
Partial improvement with natamycin or voriconazole |
Poor response to corticosteroids; temporary relief with antibiotics |
|
Laterality |
Usually unilateral |
Usually unilateral |
Can be bilateral in lens misuse |
|
Systemic symptoms |
Absent |
Occasional fever in fungal sepsis |
None |
A red flag strongly suggestive of Pythium keratitis: History of water or mud exposure with rapid worsening despite antifungals. Suspicion of Acanthamoeba keratitis increases if: Contact lens combined with water contact and extreme pain.[44]
Table 10. Physical Examination Characteristics of Keratitis
|
Slit-lamp feature |
Pythium keratitis |
Fungal keratitis |
Acanthamoeba keratitis |
|
Stromal infiltrate appearance |
Dry, gray-white, reticular or tentacular pattern |
Feathery-edged, raised soft infiltrate |
Patchy early → Ring-shaped infiltrate later |
|
Ulcer margins |
Ill-defined, irregular |
Feathery margins with satellite lesions |
Smooth borders; radial keratoneuritis |
|
Surface texture |
Dry, leathery |
Dense necrotic slough |
Rough due to epithelial erosions |
|
Endothelial involvement |
Early endothelial plaques, hypopyon |
Hypopyon later with severe disease |
Minimal until advanced stages |
|
Corneal nerves |
Not prominent |
Normal |
Radial nerve prominence (keratoneuritis) is a hallmark |
|
Pain correlation |
Severe, correlated with ulcer severity |
Matches clinical picture |
Pain > clinical signs |
|
Corneal thinning |
Rapid melt; early perforation |
Progressive thinning |
Late stromal melt in severe chronic cases |
|
Vascularization |
Limbal extension common |
Neovascularization in the chronic course |
Minimal early |
|
Recurrence |
High recurrence post-TPK |
Low recurrence |
Recurrence due to cyst survival |
Abbreviations: TPK, therapeutic penetrating keratoplasty.
Table 11. Clinical Differentiation Pearls for Clinicians
|
Pearl |
Diagnostic interpretation |
|
Rapid deep stromal infiltration + antifungal nonresponse |
Think Pythium keratitis |
|
Feathery margins + vegetative trauma |
Likely fungal |
|
Severe pain out of proportion + contact lens use |
Suggestive of Acanthamoeba spp |
|
Early endothelial plaque |
Strong indicator of Pythium spp |
|
Ring infiltrate |
Classic Acanthamoeba infection, late fungal, occasionally |
|
Chronic progression with granulomatous appearance |
Fungal infection is more likely |
Table 12. Summary for Clinical Use
|
Clinical feature |
Diagnosis |
|
Dry tentacular infiltration + antifungal failure |
Pythium keratitis |
|
Feathery infiltrates with slough and satellite lesions |
Fungal keratitis |
|
Severe pain + contact lens + ring infiltrate |
Acanthamoeba keratitis |
Need for Rapid Diagnosis and Treatment
Accurate differentiation at the bedside prevents inappropriate therapy:
- Pythium: Linezolid with azithromycin and early TPK
- Fungal: Natamycin and voriconazole are effective
- Acanthamoeba: Requires biguanides with neurotrophic pain control
Evaluation
Accurate evaluation of infectious keratitis relies on rapid microbiologic confirmation, imaging support, and assessment of treatment response. Because Pythium, fungal, and Acanthamoeba keratitis often present with similar clinical findings, a structured diagnostic approach aligned with international standards (American Academy of Ophthalmology [AAO]), International Council of Ophthalmology, and All India Ophthalmological Society) is essential to prevent delays in definitive therapy. Table 16 summarizes the recommendations based on the national guidelines.
Initial Bedside Evaluation
- Slit-lamp biomicroscopy: – Pythium: Dry reticular/tentacular infiltrate, early endothelial plaques. (See Image. Clinical Features of Pythium Keratitis.) and (See Image. Slit-Lamp Examination of Pythium Keratitis.) – Fungal: Feathery infiltrates, satellite lesions. (See Image. Slit-Lamp Examination of Fungal Keratitis.) – Acanthamoeba: Radial keratoneuritis and disproportionate pain. (See Image. Slit-Lamp Examination of Acanthamoeba Keratitis.)
- Fluorescein staining: Maps epithelial loss; dendritiform lesions suggest early Acanthamoeba keratitis
- Confocal microscopy (in vivo): A rapid, noninvasive test with high diagnostic value – Pythium: Long aseptate ribbon-like filaments – Fungal: Septate branching hyphae – Acanthamoeba: Double-walled cysts along nerves (highly specific)[45]
Laboratory Microbiology (Gold Standard)
Performed urgently in all patients with suspected microbial keratitis according to the American Academy of Ophthalmology guidelines. Table 13 summarizes the laboratory testing results for each organism.
Table 13. Laboratory Testing in Keratitis
|
Test |
Pythium keratitis |
Fungal |
Acanthamoeba keratitis |
|
Corneal scraping/smear |
Aseptate filaments, PAS+ |
Septate hyphae, KOH+ |
Cysts/trophozoites (Giemsa, Calcofluor White) |
|
Culture media |
Blood agar, brain-heart infusion (flat, colorless colonies) |
SDA, potato dextrose agar |
Nonnutrient agar + E coli overlay |
|
Incubation |
Wet environment (28°C–35°C) |
Standard fungal growth |
Requires ≥7–14 days |
|
Special culturing |
Leaf incubation method for sporulation |
Routine sporulation |
Slow growth → repeat cultures often needed |
Abbreviations: KOH, potassium hydroxide; PAS, periodic acid-Schiff; SDA, Sabouraud dextrose agar;
Stains useful for rapid differentiation: • PAS: Highlights Pythium filaments • GMS: Strongly positive only in fungi • Calcofluor White: Bright hyphae/cysts (needs ultraviolet scope)
Molecular Diagnostics (Advanced and Confirmatory)
International guidelines recommend PCR when smear or culture is inconclusive or an urgent diagnosis is required:
- Pythium spp: ITS gene region PCR and COX2 gene sequencing
- Fungal: Panfungal PCR with species identification
- Acanthamoeba spp: 18S ribosomal DNA PCR or real-time PCR. These tools provide high accuracy (>95%) and early species-level confirmation.[46] Table 14 summarizes the imaging and other testing.
Table 14. Imaging & Ancillary Investigations
|
Modality |
Diagnostic value |
|
AS-OCT |
Detects stromal depth, melt risk, and Descemet detachment |
|
Ultrasonography B-scan |
Used if hypopyon or media opacity hides the posterior segment |
|
In vivo confocal microscopy |
Near–real-time organism visualization guides early therapy |
|
Corneal sensitivity testing |
Reduced in Acanthamoeba infection due to nerve involvement |
Abbreviations: AS-OCT, anterior segment optical coherence tomography.
Radiologic imaging is rarely required unless scleral or intraocular extension is suspected.
Therapeutic Trial Response
Monitoring the response within the first 48 to 72 hours provides additional differentiation, as described in Table 15.[47]
Table 15. Therapeutic Trials by Organism
|
Topical antifungals |
Consider Pythium keratitis |
|
Topical antibiotics |
Consider fungal keratitis |
|
Empirical antivirals or corticosteroids |
Consider Acanthamoeba keratitis |
Key Diagnostic Pearls
If the ulcer worsens on antifungals → Pythium keratitis is likelyIf severe pain exceeds clinical signs → suspect Acanthamoeba keratitisIf feathery edges and satellite lesions → fungal keratitis
Early confocal microscopy and microbiological sampling are the global standards for differentiation.
- Day 1: Smear, culture, and confocal microscopy
- If unclear: PCR testing
- Management: Initiate organism-directed therapy based on microbiologic results and early treatment response [48]
Table 16. International Keratitis Guidelines
|
Organization |
Recommendation summary |
|
American Academy of Ophthalmology |
Perform smears + cultures for all suspected infectious keratitis |
|
International Council of Ophthalmology |
Rapid organism identification guides early targeted therapy |
|
All India Ophthalmological Society |
Confocal + PCR recommended in atypical or antifungal-refractory ulcers |
|
Thailand and Australia National Data |
Pythium infection suspected after water exposure + antifungal failure |
Abbreviations: PCR, polymerase chain reaction.
Treatment / Management
Early, organism-specific therapy is critical because misdirected treatment (eg, antifungals for Pythium spp or corticosteroids for active Acanthamoeba keratitis) rapidly worsens visual outcomes. Management includes targeted antimicrobial therapy, control of pain and inflammation, and surgical intervention when necessary.
Treatment of Pythium Keratitis (Antioomycete Strategy) Pythium lacks chitin and ergosterol, making it intrinsically resistant to most antifungals.[12] Table 17 summarizes the first-line treatment according to the Indian Pythium Study Group and the AIOS.(A1)
Table 17. First-Line Medical Therapy for Pythium Keratitis
|
Drug |
Dose |
Mechanism |
|
Linezolid 0.2%–0.5% |
every 1–2 hours |
Best stromal penetration; protein synthesis inhibition |
|
Azithromycin 1% |
every 2–3 hours |
Antioomycete effect; anti-inflammatory |
|
Oral linezolid 600 mg |
twice daily × 10–14 days |
For deep stromal and endothelial involvement |
|
Topical minocycline 1% |
Optional add-on |
Matrix metalloproteinase inhibition |
|
Topical isavuconazole |
For refractory cases |
Limited emerging data |
Therapy should continue until complete resolution (8–12 weeks).
Criteria for TPK
Surgical intervention should be earlier if any of the following are present:
- Rapid stromal melt or impending perforation
- Large central infiltrate (>6 mm)
- No improvement within 48 to 72 hours of antioomycete therapy
- Limbal extension or endothelial plaque progression
Large-graft TPK is (8–10 mm margin) to ensure full organism clearance. However, the recurrence risk is high, so topical therapy should continue after surgical intervention.[49](B2)
Management of Fungal Keratitis
The goal is to eradicate fungal hyphae and prevent stromal necrosis. Table 18 lists the first-line treatment options per the American Academy of Ophthalmology guidelines.
Table 18. First-Line Antifungals
|
Organism |
Preferred drug |
Dosing |
|
Fusarium spp |
Natamycin 5% solution |
Every 1 h × 48 h then taper gradually |
|
Aspergillus spp |
Voriconazole 1% solution |
Every 1–2 h, then taper |
|
Candida spp |
Amphotericin B 0.15% solution |
Every 1 h |
Adjunct systemic therapy: – Oral voriconazole 200 mg twice daily for deep stromal involvement or anterior chamber extension – Avoid corticosteroids during the acute phase [37](A1)
Indications for surgical intervention:
- Progressive infiltrate despite maximum medical therapy (72 to 96 h)
- Large central ulcer with thinning
- Descemet detachment or perforation
- Dense endothelial plaque with unresponsive hypopyon
Procedures:
- Therapeutic penetrating keratoplasty
- Tissue adhesive (glue) with a bandage contact lens for a small perforation
- AMT for neurotrophic surface support [50] (B3)
Management of Acanthamoeba Keratitis
Both trophozoites and cysts should be treated. Corticosteroids worsen early disease; therefore, they should be deferred until cyst clearance is confirmed. Table 19 summarizes treatment according to UK and European Union consensus.Corticosteroids should be delayed until cyst clearance is confirmed, as they worsen early disease.
Table 19. First-Line Medical Therapy
|
Drug class |
Agents |
Dose |
Role |
|
Biguanides |
PHMB 0.02% solution, chlorhexidine 0.02%–0.06% solution |
Hourly for 72 h, then every 2–3 h |
Strong cysticidal action |
|
Diamidines |
Propamidine 0.1% solution, hexamidine 0.1% solution |
Every 2–3 h |
Synergistic with biguanides |
|
Oral anti-inflammatory |
Nonsteroidal anti-inflammatory drugs |
As needed |
Pain control |
Abbreviations: PHMB, polyhexamethylene biguanide.
Therapy should be continued for 3 to 6 months, depending on symptom recurrence.
Corticosteroid use:
Corticosteroids should be considered only when:
- Clear improvement with negative confocal or PCR
- Persistent inflammation after the trophozoite kill
- Introduce 4 to 6 weeks after treatment; start low dose every 12–24 h
Surgical treatment:
- AMT for persistent epithelial defects
- Therapeutic penetrating keratoplasty only for perforation or end-stage scarring
- Recurrence risk is high if cysts remain [51]
Adjunctive Measures for All 3 Organisms
- Cycloplegics for pain control
- Aggressive lubrication for surface protection
- Intraocular pressure–lowering agents for secondary glaucoma
- Avoid empiric corticosteroids until the organism is confirmed
- Avoid contact lens wear throughout treatment
Table 20 lists treatment pearls for each organism.
Table 20. Treatment Pearls
|
Diagnosis |
What to start |
What to avoid |
|
Pythium spp |
Linezolid with azithromycin |
Antifungals alone (ineffective) |
|
Fungal |
Natamycin or voriconazole |
Corticosteroids in active infection |
|
Acanthamoeba spp |
PHMB with propamidine |
Early corticosteroids; monotherapy |
Abbreviations: PHMB, polyhexamethylene biguanide.
Management Escalation Algorithm (Clinical Pathway)
1. Suspected infectious keratitis 2. Perform corneal scraping for smear and culture, and obtain confocal microscopy immediately 3. Start empirical antifungal (natamycin) while awaiting smear results 4. Assess response after 48–72 h. Table 21 describes the next actions [52]
Table 21. Treatment Algorithm for Keratitis
|
Response |
Action |
|
Improvement |
Continue antifungal regimen |
|
No improvement + water exposure history with tentacular infiltrates |
Switch to antioomycete therapy (Pythium protocol) |
|
Severe pain out of proportion with radial keratoneuritis |
Start Acanthamoeba therapy |
Reassess every 48 hours. Consider TPK for progressive disease.
- Pythium is a surgical disease: Treat early and escalate with rapid progression.
- Fungal keratitis is a slow killer: Treat aggressively and continue long-term therapy.
- Acanthamoeba spp is a painful survivor: Treat persistently, avoid early corticosteroids.
Differential Diagnosis
Because Pythium, fungal, and Acanthamoeba keratitis share overlapping clinical features, such as stromal infiltrates, hypopyon, and epithelial defects, they are frequently misdiagnosed, especially at initial presentation. Several other infectious and inflammatory entities should also be considered. Careful integration of history, slit-lamp examination, microbiology, and confocal imaging is essential to reach the correct diagnosis. Table 22 compares the organisms in the differential diagnosis. Table 23 reviews the diagnostic pitfalls of the various causes of keratitis.
Key Differential Diagnoses
Fungal keratitis
Often confused with Pythium keratitis due to filamentous growth and a similar infiltrate appearance. – Feathery margins, satellite lesions – Better initial response to natamycin or voriconazole – Septate hyphae on microscopy [53]
Acanthamoeba keratitis
Major mimic in early disease. – Severe pain out of proportion to signs – Radial keratoneuritis – Ring infiltrate in late stages – Cysts on confocal microscopy or PCR [54]
Bacterial keratitis (especially Pseudomonas spp)
– Rapid course that resembles that of Pythium keratitis – Suppurative stromal melt, dense purulent discharge – Responds rapidly to fortified antibiotics. Please see StatPearls' companion resource, "Nocardia Keratitis," for further information.
Herpetic keratitis (herpes simplex virus/varicella zoster virus)
– Dendritiform lesions early suggest a neurotrophic ulcer – Reduced corneal sensation – Worsens with topical corticosteroids. Please see StatPearls' companion resource, "Herpes Zoster Ophthalmicus," for further information.
Noninfectious masqueraders – Autoimmune melt (eg, rheumatoid arthritis, Mooren ulcer) – Sterile infiltrates in contact lens users – Peripheral ulcerative keratitis [55]
Table 22. Differentiating Clinical Features
|
Feature |
Pythium spp |
Fungal |
Acanthamoeba spp |
Bacterial |
Herpetic |
|
Pain severity |
Severe |
Moderate |
Very severe |
Moderate–severe |
Mild–moderate |
|
Ulcer margins |
Reticular/tentacular |
Feathery |
Smooth early → ring later |
Dense edges |
Dendritic/geographic |
|
Surface appearance |
Dry, leathery |
Necrotic slough |
Elevated epithelium, erosions |
Wet, purulent |
Epithelial staining |
|
Hypopyon |
Early, small–moderate |
Late, thick |
Late |
Common, purulent |
Possible in severe |
|
Endothelial plaque |
Early prominent |
Late |
Rare |
Possible |
Rare |
|
Corneal nerves |
Normal |
Normal |
Radial keratoneuritis |
Normal |
Reduced sensation |
|
Treatment response |
Poor to antifungals |
Responds to antifungals |
Corticosteroids worsen early |
rapid antibiotic response |
antiviral response |
|
Microbiology |
Aseptate filaments |
Septate hyphae |
Cysts/trophozoites |
Gram stain |
PCR/Imaging |
|
Key clue |
Water/agriculture exposure with antifungal failure |
Vegetative trauma |
Contact lens with water exposure |
Purulent discharge |
Reduced corneal sensation |
Table 23. Diagnostic Pitfalls & Prevention
|
Pitfall |
How to Avoid |
|
Misdiagnosing Pythium spp as a fungus |
Perform confocal microscopy with PAS/GMS; suspect when there is no antifungal improvement. |
|
Treating Acanthamoeba keratitis with corticosteroids initially |
Delay steroids until cyst reduction; confirm with confocal microscopy/PCR |
|
Assuming vegetative trauma always means fungus |
Water-soil trauma in the monsoon strongly favors Pythium keratitis |
|
Overlooking pain–clinical mismatch in Acanthamoeba keratitis |
Check corneal nerves; ask about pain severity relative to findings |
|
Delayed corneal scraping or culture |
Always scrape before starting corticosteroids |
Abbreviations: GMS, Gomori methenamine silver; PAS, periodic acid-Schiff; PCR, polymerase chain reaction.
Decision-Making Rule of Thumb (Clinical Pearl Box)
- Dry, tentacular infiltrate with antifungal failure: Suspect Pythium infection
- Feathery edges with vegetable trauma: Suspect fungal keratitis
- Contact lens with severe pain and neural signs: Suspect Acanthamoeba keratitis
- Purulent discharge and rapid stromal thinning: Suspect bacterial keratitis
- Neurotrophic ulcer with dendrites: Suspect herpetic keratitis
The most challenging diagnostic overlap occurs between Pythium and fungal keratitis, as both exhibit a filamentous appearance. However, Pythium keratitis typically presents with a dry, reticular stromal infiltration and early endothelial plaques, and it rapidly progresses despite antifungal therapy. Acanthamoeba keratitis is characterized by disproportionate pain, perineural infiltrates, and ring lesions, particularly among contact lens wearers. Bacterial keratitis is characterized by purulent discharge and a rapid response to fortified antibiotics, whereas herpetic keratitis typically presents with reduced sensation and dendritic lesions. Accurate differentiation prevents vision-threatening delays in treatment, enabling organism-specific therapy that dramatically improves prognosis.[48]
Pertinent Studies and Ongoing Trials
The evolution of diagnostic and therapeutic strategies for Pythium, fungal, and Acanthamoeba keratitis has been supported by a growing body of clinical and translational research. Recent studies have focused on improving early diagnosis, optimizing antioomycete drug protocols, novel antifungal delivery systems, and cysticidal agents. The following section is a detailed review of critical evidence and emerging clinical trials that justify current management recommendations. Table 24 describes the results of the trials. Oomycete biology (lack of chitin & ergosterol) explains intrinsic resistance to most antifungal agents.
Table 24. Key Evidence and Trials for Pythium Keratitis
|
Study |
Key finding |
Clinical Impact |
|
Bagga et al (2021–2023, India) |
Demonstrated linezolid with azithromycin is superior to antifungals |
Established first-line therapy |
|
Gurnani et al (2022) |
Showed Pythium infection accounts for 10%–15% of culture-negative ulcers in India |
Increased awareness and screening |
|
Thai Ocular Oomycete Group Trials |
Improved outcomes with early large-graft TPK |
Surgical intervention guidelines refined |
|
Leaf Incubation Culture Method Studies |
Enhanced sporulation rates mean better microbiologic identification |
Faster, more accurate diagnosis |
Emerging investigational agents:
- Minocycline
- Isavuconazole
- Novel antioomycete peptides
These studies support antibiotic-based therapy and early TPK, rather than traditional antifungal regimens, to prevent delays that can lead to melt or perforation.[56]
Fungal Keratitis (Table 25)
Table 25. Key Trials and Innovations for Fungal Keratitis
|
Trial |
Significance |
Outcome |
|
Mycotic Ulcer Treatment Trials (MUTT I and II) |
Compared natamycin vs voriconazole |
Natamycin is superior for filamentous fungi |
|
Steroids for Corneal Ulcer Trial (SCUT) |
Corticosteroid use in bacterial keratitis |
Informs cautious steroid protocols |
Other critical findings:
- High failure rates with delayed antifungal therapy
- Voriconazole remains vital for Aspergillus infections
- PhotoActivated chromophore for keratitis-corneal cross (PACK-CXL) evaluated as an adjunct is promising in fungal but ineffective in Pythium keratitis
Device-based advances:
- Intrastromal antifungal injections
- Nanocarrier-based drug delivery [57]
These findings reinforce natamycin as first-line, identify voriconazole for deeper lesions, and discourage routine CXL in Pythium keratitis.
Acanthamoeba Keratitis
The primary mechanistic focus of research on Acanthamoeba keratitis is the cyst stage. Table 26 describes the major findings.
Table 26. Study Findings for Acanthamoeba Keratitis
|
Study |
Major contribution |
|
UK AK Consensus Guidelines |
Hourly PHMB/chlorhexidine remains the cornerstone |
|
Diamidine Synergy Trials |
Support combination therapy early |
|
Confocal Imaging Studies |
High sensitivity for detecting cyst clearance |
|
Case series on corticosteroid introduction |
Define safe timing for anti-inflammatory control |
Abbreviations: AK, Acanthamoeba keratitis; PHMB, polyhexamethylene biguanide.
Novel therapies under investigation:
- Miltefosine (antileishmanial): Superior cysticidal activity in refractory disease
- Photodynamic therapies: Laboratory models
- Gene-expression targeting: Encystment pathways
These findings suggest prolonged, staged therapy and delayed corticosteroid initiation based on cyst monitoring.[58]
Changes to Keratitis Treatment
Tables 27 and 28 describe the impact and changes to clinical practice.
Table 27. Integrated Clinical Impact Summary
|
Domain |
Pythium keratitis |
Fungal keratitis |
Acanthamoeba keratitis |
|
Treatment advances |
Antioomycete therapy Early surgery |
Optimized antifungals |
Potent cysticidal protocols |
|
Diagnostic advances |
Confocal + PCR rising |
Rapid PCR panels |
Confocal-guided therapy |
|
Ongoing research |
New antioomycete drugs |
Drug delivery & PACK-CXL |
Miltefosine & immunomodulation |
Abbreviations: PACK-CXL, photoactivated chromophore for keratitis-corneal cross; PCR, polymerase chain reaction.
Table 28. Changes in Clinical Practice for Keratitis
|
Previous concept |
Updated evidence-based practice |
|
Treat Pythium like a fungus |
Incorrect: antibiotics with early keratoplasty |
|
PACK-CXL helps all ulcers |
Contraindicated in Pythium keratitis |
|
Steroids early in all keratitis |
Harmful in early Acanthamoeba infection |
|
Surgery is a last resort |
Early TPK improves outcomes in Pythium and deep fungal disease |
Abbreviations: PACK-CXL, photoactivated chromophore for keratitis corneal cross; TPK, therapeutic penetrating keratoplasty.
Current management protocols are rooted in strong clinical evidence showing:
Pythium keratitis: A surgical and antibiotic diseaseFungal keratitis: A medical and selective surgical diseaseAcanthamoeba keratitis: A long-duration cysticidal therapy disease
Ongoing research will likely expand the use of targeted therapies, reduce morbidity, and improve visual outcomes, particularly among high-risk tropical populations.[59]
Treatment Planning
Treatment planning must be organism-specific, systematic, and time-bound because incorrect initial therapy significantly worsens prognosis, particularly in Pythium and Acanthamoeba keratitis. The framework below integrates dosages, response-based escalation, adjunctive treatment, and surgical indications consistent with key clinical trials.[42] Table 29 lists treatment pearls for keratitis due to each organism.
Treatment Planning for Pythium Keratitis
Time = Vision → aim for rapid organism control before stromal melt
Initial antioomycete regimen (initiate immediately once suspected)
Topical linezolid is typically administered at a concentration of 0.2% to 0.5%, with intensive dosing every 1 to 2 hours during the day and every 2 to 3 hours at night during the acute phase of infection. Topical azithromycin 1% may be used as an adjunctive therapy and is generally instilled every 2 to 3 hours. In cases with deep stromal involvement or severe disease, systemic linezolid is prescribed at 600 mg twice daily for 10 to 14 days, with close monitoring for systemic adverse effects.[42]
Adjunctive agents if indicated: • Minocycline, 100 mg/day • Topical isavuconazole in refractory cases [13]
Supportive therapy
- Cycloplegics
- Intensive lubrication
- Intraocular pressure control, if necessary
Escalation criteria for urgent surgery
Perform TPK when any of the following occur:
- Clinical deterioration within 48 to 72 hours
- Descemet membrane involvement (eg, endothelial plaque)
- Stromal melt or impending perforation
- Large central ulcer (> 6 mm)
- Limbus or scleral extension [60]
Large graft margins (≥ 1 mm in circumference) should be achieved to reduce recurrence risk. Continue antioomycete therapy post-TPK for at least 2 to 3 weeks. Please see StatPearls' companion resource, "Cornea Transplantation," for further information.
Treatment Planning for Fungal Keratitis
Drug selection based on etiology
- Fusarium spp: Natamycin 5% hourly for 48 hours, then taper every 2 to 3 hours
- Aspergillus spp: Voriconazole 1% hourly
- Candida spp: Amphotericin B 0.15%
Systemic therapy:
- Oral voriconazole 200 mg twice daily if deep stromal or anterior chamber involvement. Please see StatPearls' companion resource, "Cytomegalovirus Corneal Endotheliitis," for further information.
Adjunctive tools
- Epithelial ebridement to improve drug penetration
- Intrastromal antifungal injections for recalcitrant hyphae
- Photoactivated chromophore for keratitis–corneal cross-linking is not recommended for Pythium spp, selective for fungal keratitis
Surgical indications
- Nonresponse after 72 to 96 hours of maximal therapy
- Severe thinning or perforation
- Endothelial plaque unresponsive to medication
Surgical options:
- TPK or lamellar keratoplasty
- Cyanoacrylate glue with a bandage contact lens
- AMT for neurotrophic disease. Please see StatPearls' companion resource, "Iritis," for further information.
Treatment Planning for Acanthamoeba Keratitis
Staged protocol
In the early stage of epithelial disease, management focuses on intensive topical antiamebic therapy, typically using polyhexamethylene biguanide (PHMB) 0.02% administered hourly in combination with propamidine 0.1%. With stromal involvement, treatment with topical agents is continued, and systemic nonsteroidal anti-inflammatory drugs with adequate pain control are added for inflammation. Following successful eradication of trophozoites, delayed initiation of low-dose topical corticosteroids may be considered in selected cases to manage persistent inflammation, with careful monitoring for recurrence. In chronic disease with significant corneal scarring and fibrosis, keratoplasty may be required to restore visual function.[1]
- Total duration: 3–6 months
- Strict avoidance of early corticosteroids due to cyst proliferation
Confocal microscopy–guided tapering
- Reduce dosing only after cyst clearance evidence
- Reinstate intensive therapy if pain or infiltrates recur
Surgical planning
- Reserved for perforation or visual rehabilitation
- High recurrence risk if cysts remain in the host rim
- An AMT is often required for persistent epithelial defects
Unified response escalation timeline (applicable to all 3 etiologies)
Clinical response should be reassessed at 48 to 72 hours after initiating therapy. If improvement is significant, the current treatment regimen should be continued with close monitoring. If improvement is minimal, repeat corneal smears should be performed, and therapy should be modified based on the revised clinical suspicion. If the clinical condition worsens, urgent consideration of TPK is warranted, particularly in cases of suspected or confirmed Pythium keratitis.[6]
Table 29. Clinical Strategy Pearls
|
If you see… |
Think… |
Start… |
|
Dry tentacles + antifungal failure |
Pythium keratitis |
Linezolid + azithromycin + early TPK |
|
Feathery margins + vegetative trauma |
Fungal keratitis |
Natamycin/voriconazole |
|
Severe pain + contact lens + ring infiltrate |
Acanthamoeba keratitis |
PHMB + propamidine (no early corticosteroids) |
Abbreviations: PHMB, polyhexamethylene biguanide.
Treatment Strategy
Pythium keratitis is a surgical disease → treat aggressively earlyFungal keratitis is a medical disease → treat long and strongAcanthamoeba keratitis is a persistent cystic disease → treat slowly, avoid corticosteroids early in the disease [12]
Toxicity and Adverse Effect Management
Differentiating Pythium, Fungal, and Acanthamoeba Keratitis
Therapy for microbial keratitis often requires high-frequency topical regimens and prolonged treatment durations, which can cause significant ocular surface toxicity. Toxicity prevention and management must be proactive, organism-specific, and continuously monitored.
Pythium Keratitis
Antifungal therapy (not antifungal therapy) carries a risk of epithelial toxicity.
Primary toxicities
Topical linezolid may cause mitochondrial toxicity, which can manifest as epithelial defects and ocular surface haze; therefore, weekly monitoring of epithelial integrity is recommended during therapy. Topical azithromycin is generally well tolerated but may cause burning, dryness, or allergic conjunctivitis; the dosing frequency should be reduced if epithelial compromise develops. Systemic linezolid carries a risk of myelosuppression and, with prolonged use, optic neuropathy. Accordingly, weekly monitoring of the complete blood count is advised, and the drug should be discontinued promptly if visual symptoms occur.
Management strategies
- Lubrication with preservative-free formulations
- Temporary dose reduction if epitheliopathy is severe
- Earlier TPK if toxicity limits drug tolerance
- AMT for nonhealing epithelial defects [61]
- Avoid antifungal therapy alone because it is ineffective and toxic in Pythium keratitis.
Fungal Keratitis
Primary toxicities
Natamycin 5% may cause epithelial edema and punctate keratopathy, but it is generally considered the most surface-friendly antifungal agent; however, frequent dosing can cause ocular irritation. Topical voriconazole is associated with stromal toxicity and burning, and systemic administration increases hepatotoxicity risk, necessitating liver function monitoring when administered orally or intravenously. Amphotericin B has the lowest ocular surface tolerance among antifungal agents and can cause severe epithelial toxicity and stromal necrosis; it should be used cautiously and reserved for selected cases.
Toxicity mitigation
- Epithelial debridement to improve penetration and reduce the dose of medications
- Taper once clinical improvement is observed
- Use preservative-free, antifungal formulations when available
- Manage neurotrophic keratopathy, a frequent complication. Please see StatPearls' companion resource, "Therapeutic Keratoplasty," for further information.
Corticosteroids should be used only in the late healing phase, in small doses, and under close supervision.
Acanthamoeba Keratitis
Primary toxicities
Toxicity results from the detergent action of biguanides/diamidines on host membranes. Biguanides, such as PHMB and chlorhexidine, are associated with significant ocular surface toxicity, including severe punctate keratitis and, in advanced cases, stromal melt. This toxicity is most pronounced with prolonged hourly dosing. Diamidines may cause allergic blepharoconjunctivitis and should therefore be used judiciously, primarily as adjunctive agents for synergistic effect rather than as monotherapy.
Pain-related complications:
- Neurotrophic keratitis
- Corneal anesthesia
- Recurrent epithelial breakdown
Management strategies
- Frequent lubrication
- Pain control (eg, cycloplegia, nonsteroidal antiinflammatory drugs)
- AMT for persistent epithelial defects
- Delay corticosteroids until cyst clearance (4–6 weeks)
- Intraocular pressure management of secondary glaucoma [62]
Tapering should be slow because rapid reduction can cause cyst resurgence and clinical relapse.
Cross-Condition Toxicity Considerations
Long-term topical toxicity should be addressed by switching to preservative-free formulations to minimize ocular surface damage during prolonged therapy. Contact lens use should be strictly avoided throughout the treatment period to reduce the risk of persistent infection and delayed epithelial healing. In cases of secondary bacterial infection, management should be guided by culture-directed antibiotic therapy to ensure targeted and effective treatment. Ocular surface inflammation may be managed with the careful, delayed introduction of low-dose topical corticosteroids tailored to the underlying organism and clinical response. If intraocular pressure increases, topical β-blockers are preferred as first-line agents; prostaglandin analogs should be avoided because they may exacerbate inflammation. The following are important considerations:
- Begin toxicity monitoring from the first day.
- Adjust dosing interval based on epithelial health.
- Provide ocular surface protection with lubrication with a bandage contact lens in selected cases.
- Use confocal microscopy or PCR to avoid misdirected toxic treatments.
- Consider AMT if epithelial compromise persists despite tapering.[63]
Practical Pearls
- Pythium therapy is less toxic than antifungals, but delayed surgery can result in catastrophic outcomes.
- Antifungals are potent but toxic, and should be tapered as soon as the organism load reduces.
- Acanthamoeba therapy is the most toxic. Cysticidal efficacy should be balanced with ocular surface protection.
- Toxicity management is as critical as antimicrobial potency to preserve vision.
Staging
A standardized staging system helps to:
- Guide treatment escalation
- Plan surgical timing
- Determine visual prognosis
The following practical, clinically applicable staging framework integrates the most widely used classification elements and proposed refinements from recent literature, including conceptual guidance from Gurnani and Kaur (Proposed Clinical Severity Model). The staging model is summarized in Table 30; Table 31 lists the distinguishing features of each organism; and Table 32 presents therapy implications for each stage.[22]
Table 30. Proposed Gurnani–Kaur Composite Staging System for Infectious Filamentous Keratitis Differentiation
|
Stage |
Clinical features |
Initial management |
|
Stage 1: Epithelial disease (early) |
Superficial infiltrate, epithelium intact or minimal defect, absence of endothelial plaque |
Intensive topical therapy based on the suspected organism |
|
Stage 2: Stromal disease (progressive) |
Stromal infiltration, tentacular/feathery/perineural infiltrates depending on etiology, and early endothelial changes |
Confirm diagnosis and adjust therapy accordingly |
|
Stage 3: Advanced keratitis |
Deep stromal involvement, endothelial plaque, early AC reaction, persistent pain in AK |
Surgical evaluation; confocal/PCR required |
|
Stage 4: Preperforation disease |
Severe melt, descemetocele formation, large infiltrate (≥6 mm), persistent hypopyon |
Urgent TPK (strongly indicated in Pythium keratitis) |
|
Stage 5: Perforated disease or scleral extension |
Corneal perforation or scleral invasion |
TPK with scleral patch graft if required |
Abbreviations: AC, anterior chamber; AK, Acanthamoeba keratitis; PCR, polymerase chain reaction; TPK, therapeutic penetrating keratoplasty.
Severity Score Additions
- Pain score (in Acanthamoeba keratitis)
- Exposure history-based risk weighting
- Treatment response is critical for distinguishing Pythium from other types of keratitis [6]
Table 31. Organism-Specific Staging Clues
|
Etiology |
Distinguishing stage-defining feature |
|
Pythium spp |
Early endothelial plaque; rapid transition from stage 2 to stage 4 |
|
Fungal |
Satellite lesions in stage 2–3; slower melt progression |
|
Acanthamoeba spp |
Disproportionately severe pain in stages 1–2 and late ring infiltrate in stage 3 |
Pythium keratitis may progress rapidly, and early misclassification can lead to irreversible loss of the globe.
Table 32. Treatment Implications by Stage
|
Stage |
Pythium keratitis |
Fungal |
Acanthamoeba keratitis |
|
1 |
Antifungal therapy |
Natamycin/voriconazole |
PHMB + diamidine |
|
2 |
Consider early TPK if no response by 48–72 h |
Intensify antifungals |
Therapy intensification |
|
3 |
Plan TPK before the melt |
Intrastromal antifungals if needed |
Delayed corticosteroids after cyst elimination |
|
4–5 |
Urgent TPK |
TPK or glue |
TPK only if rescue |
Abbreviations: PHMB, polyhexamethylene biguanide; TPK, therapeutic penetrating keratoplasty.
Clinical Pearls
- Pythium keratitis: Endothelial plaque should prompt escalation to stage 3 or 4 immediately
- Fungal keratitis: Gradual melt with feathery margins
- Acanthamoeba keratitis: Pain is disproportionately severe in the early stages
Summary
The Gurnani–Kaur staging helps rapidly triage aggressive cases, enabling:
- Early antifungal therapy in Pythium keratitis
- Proper antifungal selection in fungal ulcers
- Prolonged cysticidal therapy with delayed corticosteroids in Acanthamoeba keratitis
- Early surgical referral before perforation [22]
Prognosis
The prognosis in microbial keratitis is primarily determined by the causative organism, the time to a correct diagnosis, the promptness of appropriate therapy, and the disease stage at presentation. Delays in organism-specific treatment significantly worsen outcomes, particularly in Pythium and Acanthamoeba infections. Table 33 compares the prognosis of the 3 conditions.
Prognostic Overview by Etiology
Pythium Keratitis (Most Aggressive Course)
- Poor prognosis if misdiagnosed initially as fungal keratitis
- Vision salvage is closely tied to early antifungal therapy and early TPK
- Delayed intervention results in rapid corneal melt, perforation, and scleral extension [29]
The presence of an endothelial plaque is a strong predictor of the need for TPK. A large corneal infiltrate (> 6 mm) is associated with higher rates of disease recurrence and graft failure. Limbal involvement signifies severe disease and carries a substantial risk of globe loss. Additionally, a delay in initiating appropriate therapy beyond 72 hours is associated with worse outcomes and overall prognosis. However, with appropriate, timely treatment, anatomical globe salvage has improved from less than 30% to greater than 70% in results from recent series.
Fungal Keratitis (Variable Prognosis)
- Moderate to guarded prognosis, depending on the pathogen and penetration depth
- Better outcomes with:
- Early natamycin for Fusarium spp
- Voriconazole for Aspergillus spp [19]
Complications leading to worse outcomes
- Macular scarring can lead to permanent visual loss
- Secondary glaucoma
- Postkeratoplasty recurrence [64]
Early response within 72 to 96 hours predicts a favorable outcome.
Acanthamoeba Keratitis (Slow but Persistent)
- Prognosis is highly dependent on timely diagnosis
- Late presentation is common, and vision is often affected despite organism eradication
Key prognostic issues
- Chronic keratopathy and neurotrophic sequelae
- Recurrence is common if cysts remain in the host rim
- Keratoplasty during the active phase leads to high graft failure [65]
If treated early with cysticidal therapy, functional vision is usually recovered.
Table 33. Prognostic Comparison Table
|
Parameter |
Pythium keratitis |
Fungal keratitis |
Acanthamoeba keratitis |
|
Natural course |
Rapid melt |
Slow to moderate |
Chronic, recurrent |
|
Vision salvage |
Poor unless early TPK |
Guarded to good |
Guarded |
|
Recurrence risk |
High |
Moderate |
High if surgery is done early |
|
Globe loss rate |
Highest |
Lower |
Low to moderate |
|
Response to therapy |
Poor to antifungals |
Good with the correct agent |
Slow response; toxic meds |
Abbreviations: TPK, therapeutic penetrating keratoplasty.
Predictors of Poor Visual Outcome (All Causes)
Delayed initiation of targeted therapy allows deeper stromal invasion and cyst maturation, leading to more aggressive disease and worse outcomes. Central large corneal ulcers are associated with macular scarring, which significantly limits final visual acuity even after infection resolution. Corneal thinning or perforation often necessitates surgical intervention, and graft survival in such cases is unpredictable. Endothelial involvement increases anterior chamber inflammation and the risk of recurrence, complicating medical and surgical management. Systemic immune compromise further contributes to delayed healing and a prolonged clinical course.[48]
Prognosis Pearls
Pythium keratitis: Diagnosis late = vision lostFungal keratitis: Treatment late = cornea lostAcanthamoeba keratitis: Corticosteroids early = disease worsened
Patient-Centered Prognostic Counseling
Patients should be informed that:
- Treatment duration may be prolonged (weeks to months).
- Even with the eradication of the organism, residual scarring may necessitate optical or therapeutic keratoplasty.
- Avoiding contact lenses and water exposure during treatment is critical to prevent recurrence.
Summary
Fungal infections often have the best outcomes, whereas Pythium keratitis has the worst. Acanthamoeba keratitis outcomes vary. Rapid recognition and pathogen-specific management are the strongest predictors of visual success.[66]
Complications
Microbial keratitis can lead to a broad spectrum of serious ocular complications, including corneal tissue destruction, severe inflammation, delayed identification of the causative organism, and toxicity from prolonged therapy. Complication risk and pattern vary significantly by pathogen. Table 34, Table 35, Table 36, and Table 37 summarize complications attributable to the organism, treatment, surgical intervention, and psychosocial factors, respectively.
Table 34. Major Complications by Etiology
|
Complication |
Pythium keratitis |
Fungal keratitis |
Acanthamoeba keratitis |
|
Corneal stromal melt |
Very rapid |
Moderate |
Can occur late |
|
Corneal perforation |
Highly likely |
Moderate |
Less common unless late |
|
Scleral extension |
Frequent, globe-threatening |
Rare |
Rare |
|
Endothelial plaque or AC invasion |
Early & aggressive |
Moderate |
Rare |
|
Graft failure after TPK |
High recurrence risk |
Moderate |
High if active cysts remain |
|
Neurotrophic keratopathy |
Secondary to melt |
Aggressive corticosteroids or toxicity |
Common from nerve inflammation |
|
Secondary glaucoma |
Inflammation-related |
Corticoteroid-induced |
Pain-induced corticosteroid overuse risk |
|
Macular scarring & poor visual recovery |
Very common |
Common |
Common |
|
Chronic keratitis recurrences |
If incomplete excision |
Moderate |
Frequent or premature corticosteroid use |
Abbreviations: AC, anterior chamber; TPK, therapeutic penetrating keratoplasty.
Table 35. Treatment-Related Complications
|
Cause |
Examples |
Prevention |
|
Medication toxicity |
Epitheliopathy, stromal toxicity (eg, PHMB, amphotericin B) |
Frequent lubrication, close follow-up, preservative-free formulations |
|
Corticosteroid misuse |
Worsening AK, delayed healing |
Avoid early corticosteroids; carefully supervised taper only |
|
Prolonged use of bandage CL |
Secondary microbial infection |
Strict monitoring, avoid when active keratitis is present |
Abbreviations: AK, Acanthamoeba keratitis; CL, contact lens; PHMB, polyhexamethylene biguanide.
Table 36. Surgical Complications
|
Complication |
Risk context |
|
Graft nonintegration, rejection, or failure |
Inflammation; recurrence of fungal/Pythium infection |
|
Persistent epithelial defect |
Medication toxicity & limbal damage |
|
Recurrence in the donor graft |
Pythium & Acanthamoeba infections are more likely |
|
Large optical aberrations |
Oversized graft margins in emergency TPK |
Abbreviations: TPK, therapeutic penetrating keratoplasty.
Delayed referral or emergent large-graft Pythium keratitis is associated with increased postoperative complications.
Table 37. Systemic and Psychosocial Complications
|
Long-term hospitalization and cost burden |
High in Pythium & resistant fungal infection |
|
Depression and anxiety due to chronic pain |
Characteristic of Acanthamoeba keratitis |
|
Quality-of-life reduction from vision loss |
Across all etiologies |
Key Clinical Pitfalls
- Misdiagnosing Pythium keratitis as fungal keratitis: Antifungal therapy delays effective care and worsens prognosis
- Early corticosteroids in Acanthamoeba keratitis: Explosive cyst proliferation causes rapid deterioration
- Delayed surgical intervention: Irreversible perforation and melt
- Misdiagnosis of endothelial plaque: Delayed TPK can lead to globe loss
- Toxicity misdiagnosed: Worsened scarring and poor visual outcomes
Summary
Severity of potential complications: Pythium > Acanthamoeba ≥ fungal keratitis. Rapid recognition, organism-targeted therapy, and timely surgical planning are the most powerful tools for reducing complications.[67]
Postoperative and Rehabilitation Care
Postoperative care following therapeutic keratoplasty or intensive medical therapy aims to:
- Ensure graft survival
- Prevent recurrence of infection
- Rehabilitate ocular surface integrity
- Optimize long-term visual recovery
Rehabilitation planning varies significantly depending on pathogen-specific recurrence risk and tissue healing characteristics.[68]
Postoperative Care After Pythium Keratitis Keratoplasty
The primary objective is to prevent recurrence in the donor graft. Linezolid and azithromycin should be continued for 2 to 3 weeks postoperatively to eradicate any residual organisms. Close surveillance of the graft–host junction, particularly along the edges of large grafts, is essential because this area is a common site of disease recurrence. Topical corticosteroids should be introduced in a delayed, cautious manner only after complete control of infection has been confirmed to reduce reactivation and graft-related complications.[8] Additional postoperative care includes:
- Slit-lamp exam every 48 to 72 hours initially
- Confocal microscopy or PCR if recurrence is suspected (eg, tentacular regrowth or endothelial plaque)
Visual rehabilitation
- Secondary optical keratoplasty if graft clarity is inadequate after stabilization [69]
Postoperative Care After Fungal Keratitis Keratoplasty
Postoperative management should focus on preventing fungal recurrence by continuing topical antifungal therapy, such as natamycin or voriconazole, for at least 2 weeks. Anterior chamber inflammation should be controlled with the early, cautious introduction of topical corticosteroids, balancing control of inflammation with the risk of infection reactivation. Epithelial healing should be supported by frequent lubrication and, when indicated, a bandage contact lens. Intraocular pressure should be closely monitored because corticosteroid-response glaucoma is a recognized postoperative complication.
Visual optimization
- Rigid gas permeable or scleral lenses for residual irregular astigmatism
Postoperative Care After Acanthamoeba Keratitis Keratoplasty
Recurrence within the graft is a significant concern because persistent cysts in the host rim can act as reservoirs for reinfection. Continued therapy with PHMB or diamidines for at least 4 to 6 weeks is recommended to ensure complete eradication. Chronic inflammation can lead to significant pain and delayed epithelial healing. Topical corticosteroids should be gradually reintroduced only after an apparent reduction in cyst burden has been achieved. Neurotrophic keratopathy, resulting from nerve damage caused by the infection itself or prolonged topical toxicity, requires aggressive surface support with intensive lubrication, consideration of an AMT, and, when available, cenegermin to promote corneal healing and restore ocular surface integrity. Please see StatPearls' companion resource, "Charles Bonnet Syndrome," for further information. If postoperative pain recurs, cyst reactivation should be suspected, and therapy should be intensified immediately.
Ongoing Rehabilitation Common to All Etiologies
Ocular surface management
- Preservative-free lubricants
- Eyelid hygiene
- Treat exposure keratopathy if lagophthalmos is present [9]
Scar and irregularity management
- Corneal rigid gas permeable or scleral lens trial
- Secondary optical penetrating keratoplasty or lamellar graft after stabilization
Visual and functional recovery
- Counseling regarding low vision aids early if macular damage
- Provide psychosocial support, especially in patients with Acanthamoeba keratitis with chronic pain [70]
Monitoring schedule
During the first 2 weeks postoperatively, patients should be evaluated every 48 to 72 hours to closely monitor for early recurrence, inflammation, and graft-related complications. From 2 to 8 weeks postoperatively, follow-up can be scheduled at weekly intervals as the clinical course stabilizes and medications are adjusted. After 2 months, evaluation may be scheduled every 2 to 4 weeks until ocular stability is achieved, with continued vigilance for late complications.[8]
Critical postoperative red flags
The reappearance of tentacle-like infiltrates suggests a possible recurrence of Pythium infection and warrants repeat corneal scraping with intensification of antioomycete therapy. The presence of a ring infiltrate or pain disproportionate to clinical findings raises suspicion for recurrent Acanthamoeba keratitis, and treatment should be escalated by restarting PHMB or diamidines. Rapid endothelial failure may indicate graft rejection or recurrent infection and requires prompt clinical assessment and, depending on the underlying cause, intensification of topical corticosteroids or antifungal therapy.[9]
Pearls for Better Outcomes
- Pythium keratitis: Delay corticosteroids, prioritize aggressive infection control
- Fungal keratitis: Continue antifungal medications early, moderate use of corticosteroids
- Acanthamoeba keratitis: Taper slowly, protect nerve recovery
- Begin regular corneal topography and optical rehab planning early [61]
Consultations
Coordinated interprofessional consultation is vital for managing severe infectious keratitis because of its rapid progression, diagnostic complexity, and high risk of permanent visual loss. Early involvement of specialists improves diagnostic accuracy, treatment success, and postoperative rehabilitation.
Primary Consultations
Management of complex infectious keratitis requires a coordinated interprofessional approach. The cornea and external disease specialist leads the diagnostic process, initiates organism-specific therapy, and determines the optimal timing for surgical intervention, including keratoplasty, when indicated. The clinical microbiologist plays a critical role by providing rapid microscopy, culture results, PCR identification, and antimicrobial sensitivity testing to guide targeted treatment. Infectious disease and ocular pharmacology specialists advise on systemic therapies such as linezolid, voriconazole, or miltefosine, and ensure appropriate monitoring for drug-related toxicities. A glaucoma specialist is essential for managing intraocular pressure elevation related to corticosteroid use or inflammation. In cases of severe pain, particularly in Acanthamoeba keratitis, consultation with a pain management specialist or a neurology team is crucial to address neuropathic pain and improve patient comfort and adherence to therapy. Please see StatPearls' companion resource, "Compressive Optic Neuropathy," for further information.
Surgical Planning Consultations
In cases of impending corneal perforation or scleral extension, management requires close coordination between a corneal surgeon and an oculoplastics team to achieve timely stabilization and reconstruction of the globe. Recurrent graft failure necessitates involvement of a specialized corneal transplant team with immunology support to optimize graft survival and manage immune-mediated complications. Following complete resolution of infection, patients undergoing optical keratoplasty benefit from care provided by a refractive or corneal surgical team, in conjunction with low-vision rehabilitation services, to maximize visual recovery and functional outcomes.[42]
Rehabilitation-Focused Consultations
A contact lens specialist plays a vital role in post-scar visual rehabilitation by fitting rigid gas-permeable or scleral contact lenses to optimize visual acuity once the ocular surface has stabilized. Low-vision and occupational therapists are essential for developing individualized rehabilitation strategies for patients with significant and permanent visual loss, thereby helping to restore functional independence. Psychology and counseling services are particularly valuable for patients with chronic disease, especially in Acanthamoeba keratitis, because prolonged pain, anxiety, and psychological distress can significantly impact quality of life and treatment adherence.
Urgent Consultation
Consultation should occur immediately if any of the following are present:
- No improvement: After 48–72 hours of empiric antifungal therapy, lack of improvement suggests Pythium keratitis
- Severe pain disproportionate to clinical signs: Acanthamoeba keratitis should be suspected
- Central ulcer ≥6 mm or limbal involvement: Surgical consultation and discussion early
- Postoperative signs of recurrence: Immediate microbiology and corneal evaluation [1]
Coordination of Care, Essential Communication Points
Assessment of the infection stage and the corneal layers involved is critical, as it directly determines the urgency and timing of surgical intervention. Close attention to dosing compliance and drug-related toxicity is essential to prevent ocular surface failure that may falsely suggest clinical improvement. Careful consideration of the corticosteroid timeline helps avoid premature corticosteroid use, particularly in cases of Acanthamoeba keratitis, because early corticosteroids can worsen outcomes. Finally, accurate interpretation of confocal microscopy, culture, and PCR results is necessary to ensure targeted therapy and avoid misdirected or ineffective treatment.
Clinical Pearls for Effective Consultation
- Pythium keratitis requires early involvement of a corneal surgeon because delayed TPK can result in loss of the eye.
- Acanthamoeba keratitis requires long-term team follow-up because chronic neuropathic sequelae are frequent.
- Interdisciplinary management significantly improves anatomical and functional success rates. [5]
Deterrence and Patient Education
Preventing infectious keratitis and delayed diagnosis requires strong patient education and public health strategies. Messaging must be clear, repetitive, and tailored to each pathogen's specific risk factors.
General Prevention Strategies for All Types
- Avoid contact lens use during water exposure (eg, swimming, showering)
- Maintain strict lens hygiene: clean lenses daily and avoid overnight wear unless specifically approved
- Seek prompt evaluation for any painful, red eye, especially after trauma or in contact lens users
- Avoid self-medication with leftover corticosteroids or antibiotics
- Counsel against traditional eye remedies that increase contamination risk [45]
Pathogen-Specific Education
Pythium keratitis: High-risk farming and monsoon settings
Patients should be educated to:
- Wear protective eyewear during agricultural work
- Avoid exposure to stagnant water or muddy environments after eye injuries
- Seek care immediately if redness or blurred vision develops after a water or soil splash
- Return immediately if symptoms worsen despite antifungal treatment (key diagnostic clue) [71]
Patient educational message:
“If antifungals aren’t helping within 2 to 3 days, Pythium keratitis could be the culprit.”
Fungal keratitis: Rural and trauma education
- Clean and protect eyes after vegetative injuries
- Avoid reliance on home remedies after trauma
- Early natamycin use improves the chances of vision recovery. Please see StatPearls' companion resource, "Fungal Keratitis," for further information.
Acanthamoeba keratitis: Contact lens focus
- Use fresh disinfecting solution, never tap water
- Replace cases every 1 to 3 months
- Remove lenses before sleeping, bathing, and swimming
- Report pain out of proportion to the clinical appearance immediately [72]
Patient educational message: “Severe pain with a mild-looking eye can be a serious infection.”
Treatment Adherence Counseling
Patients should be educated that:
- Therapy may require many drops and a long duration (especially for Acanthamoeba keratitis)
- Stopping treatment early leads to recurrence
- Follow-up visits cannot be skipped
- Adverse effects and toxicity symptoms must be reported early (eg, foreign body sensation, whitening of the cornea, worsening discomfort)[73]
Provide:
- Written drop schedules
- Alarm reminders
- Family involvement in care
Postoperative Education
- Watch for graft rejection: redness, photophobia, blurred vision.
- Continue topical therapy as instructed, even if the eye “looks okay.”
- Avoid injuries and rubbing the eye.
- Avoid contact lens use until cleared by a clinician.[74]
Community and Public Health Messaging
Prevention education should be tailored to specific at-risk groups. Farmers and outdoor workers should be counseled on the importance of wearing protective eyewear during the monsoon season and seeking prompt care after ocular trauma to reduce the risk of severe infections. Contact lens wearers must be advised to avoid water exposure, including swimming and washing lenses with tap water, and to maintain strict lens hygiene to prevent microbial keratitis. Primary care clinicians should consider Pythium infection when presumed fungal keratitis fails to respond to antifungal therapy, enabling earlier referral and targeted treatment. Finally, rural outreach programs play a crucial role in emphasizing that early referral to specialized eye care centers significantly improves visual outcomes in infectious keratitis.[67]
Patient-Friendly Take-Home Messages
Clear patient education messages prevent delayed diagnosis and recurrence of infection. Emphasizing that “a red eye after water or soil injury is an emergency” helps reduce delays in recognizing and treating Pythium keratitis. Reinforcing that “severe eye pain may indicate Acanthamoeba infection and requires urgent medical care” aids in preventing cyst maturation and disease progression. Advising patients to “complete all prescribed eye drops unless specifically instructed to stop by a clinician” is critical to avoid relapse and to ensure complete eradication of the infection.[75] Effective patient education is a sight-saving intervention. Empowered patients seek early care and adhere to life-changing treatments.
Pearls and Other Issues
Key Diagnostic Pearls
- In the setting of a history of stagnant water or agricultural exposure, and failure of antifungal therapy, Pythium keratitis should be strongly suspected, prompting a switch to linezolid and azithromycin, with early planning for TPK.
- Severe pain with minimal clinical signs is characteristic of Acanthamoeba keratitis and should prompt confocal microscopy and initiation of PHMB with a diamidine.
- In cases of vegetative ocular trauma with feathery stromal borders, fungal keratitis is most likely, and treatment should begin with natamycin or voriconazole.
- The presence of an early endothelial plaque suggests Pythium infection and warrants urgent escalation of therapy, with a high likelihood of surgical intervention.
- A ring infiltrate indicates late-stage Acanthamoeba keratitis and requires confirmation of cysts and avoidance of early corticosteroid use.[8]
Common Pitfalls to Avoid
- Treating Pythium keratitis as a fungal infection is a critical pitfall that can lead to rapid corneal melt and potential globe loss; this can be prevented by maintaining a high index of suspicion and initiating an antioomycete treatment protocol early when the clinical response to antifungal therapy is poor.
- Premature initiation of topical corticosteroids in Acanthamoeba keratitis may lead to cyst proliferation, underscoring the importance of delaying corticosteroid use until adequate cyst clearance is achieved.
- Failure to recognize medication-related ocular surface toxicity can lead to epithelial breakdown, which may be misinterpreted as worsening infection; this risk can be minimized through frequent monitoring, dose adjustments, and aggressive lubrication.
- Delayed surgical intervention in Pythium keratitis is associated with higher recurrence rates and scleral extension, and outcomes improve with therapeutic penetrating keratoplasty within 48 to 72 hours in the setting of an inadequate clinical response.[76]
Fast-Action Rules (Disposition Guidance)
- For suspected Pythium keratitis, early management should focus on initiating appropriate therapy, with concurrent confocal microscopy and PCR for confirmation, and prompt escalation to TPK if there is no clinical response within 72 hours.
- Fungal keratitis should be initially treated with maximal topical antifungal therapy; cases that fail to respond may require intrastromal antifungal injections or TPK.
- In Acanthamoeba keratitis, first-line management consists of intensive biguanide therapy combined with adequate pain control, with surgical intervention reserved for the quiescent phase once active infection has been controlled.[34]
Table 38 lists pearls for preventing keratitis.
Clinical disposition: Patients often require admission at advanced stages (eg, large ulcers, anterior chamber reaction, impending melt).
Red Flags
Immediate action is required if any of the following red flags are present:
- Rapidly expanding infiltrate despite therapy
- Early stromal melt or descemetocele
- Marked photophobia with disproportionate pain
- Endothelial plaque or ring infiltrate appearance
- Recurrence at graft–host junction post-TPK [77]
These findings warrant the urgent involvement of a corneal surgeon.
Table 38. Infection-Specific Prevention Pearls
|
Etiology |
Prevention tip |
|
Pythium spp |
Eye protection in the monsoon season, avoid stagnant water |
|
Fungal disease |
Early care after vegetative trauma, avoid home remedies |
|
Acanthamoeba spp |
Avoid tap water exposure with contact lenses |
Limitations and Future Directions
- Pythium keratitis remains underdiagnosed; rapid diagnostics are needed
- Photoactivated chromophore for keratitis– corneal cross-linking is contraindicated in Pythium keratitis, but is evolving for fungal keratitis
- Miltefosine and targeted antifungal agents are promising
- Artificial intelligence for early organism differentiation is under development
- Public health awareness is essential in rural and contact lens populations [48]
Clinical Pearls
- Dry tentacles: Pythium keratitis
- Pain out of proportion: Acanthamoeba keratitis
- Feathery ulcer: Fungal keratitis
- Antifungal failure: Switch to antioomycete therapy
- Avoid early corticosteroids in Acanthamoeba keratitis
- Early TPK in Pythium keratitis can be globe-saving
Early recognition, combined with appropriate therapy and toxicity mitigation, offers the best chance of preserving vision. These pearls are critical for residents, emergency clinicians, and noncorneal ophthalmologists who often encounter these infections first.[42]
Enhancing Healthcare Team Outcomes
Optimal outcomes for infectious keratitis, especially when caused by Pythium and Acanthamoeba organisms, require highly coordinated, interprofessional care due to diagnostic complexity, prolonged treatment courses, and a high risk of irreversible corneal damage. Seamless collaboration facilitates early detection of ocular disease, timely adjustments in therapy, and surgical decision-making to preserve vision and the globe.
Interprofessional Roles and Responsibilities
Optimal outcomes in complex infectious keratitis depend on an interdisciplinary team approach. The ophthalmologist or cornea specialist leads diagnosis, coordinates microbiological evaluation, formulates treatment plans, and makes timely decisions regarding keratoplasty, thereby preventing complications. The clinical microbiologist contributes by rapidly interpreting smears and correlating with PCR or confocal microscopy results, enabling accurate organism identification and targeted therapy. Infectious disease specialists and pharmacists play a crucial role in optimizing drug dosing, managing interactions, and monitoring toxicity, thereby reducing medication-related adverse effects and resistance. The nursing team ensures strict adherence to intensive treatment regimens through accurate drop scheduling, compliance checks, and patient education. In cases of Acanthamoeba keratitis, consultation with a pain specialist or neurologist is essential for managing chronic neuropathic pain and improving patient comfort. Low-vision and rehabilitation specialists assist with visual adaptation and the provision of assistive devices in irreversible cases, thereby maximizing functional independence. Additionally, psychology and counseling services address anxiety and depression associated with chronic illness, thereby improving coping skills and treatment adherence.[78]
Communication and Coordination Strategies
Effective management of complex infectious keratitis is strengthened by clear handoff documentation, including the suspected organism and current treatment stage, which helps prevent adverse treatment changes, such as premature initiation of corticosteroids. Using shared digital documentation systems and automated follow-up alerts reduces the risk of missed appointments during critical phases of healing. Regular interdisciplinary case reviews facilitate early identification of recurrence and enable rapid escalation of therapy. Providing patients with structured drop charts and mobile reminders improves adherence to intensive hourly treatment regimens. Finally, early surgical consultation when predefined red flags are identified significantly reduces the risk of corneal perforation, particularly in aggressive infections such as Pythium keratitis.[79]
Patient-Centered Safety Considerations
- Ensure informed consent for high-risk medications and TPK
- Reinforce avoidance of contact lens use until medically cleared
- Provide emergency access instructions for sudden worsening
- Monitor for psychological distress, especially in Acanthamoeba keratitis
- Encourage family involvement in drop administration [80]
Ethical Responsibilities of the Team
Ethical practice in the management of complex infectious keratitis requires a patient-centered and evidence-driven approach. Avoiding harm is paramount and includes preventing misdiagnosis-related treatment delays, such as mistaking Pythium keratitis for fungal infection. Equitable access to care should be ensured by establishing clear referral pathways for rural and low-resource patients, who are at higher risk of delayed presentation. Transparency in clinician–patient communication is essential, particularly regarding the likelihood of prolonged recovery, need for surgery, and visual prognosis. Evidence-based care requires tailored treatment regimens supported by clinical trial evidence and consensus guidelines. Finally, respect for patient autonomy is upheld through shared decision-making, particularly for high-risk surgical interventions such as TPK.[80]
Outcome Enhancement Metrics
Successful interprofessional care will demonstrate:
- Reduced time to diagnosis
- Lower rates of corneal melt and perforation
- Higher graft survival and better visual restoration
- Improved patient adherence and satisfaction
- Fewer severe toxic effects during prolonged therapy
Early interdisciplinary involvement transforms prognosis in aggressive keratitis. Correct expertise at the right moment saves vision, and often the eye. By strengthening collaborative communication, clinical vigilance, integration of microbiology, and patient support, healthcare teams significantly improve safety, outcomes, and overall quality of care in the management of infectious keratitis.[81]
Media
(Click Image to Enlarge)
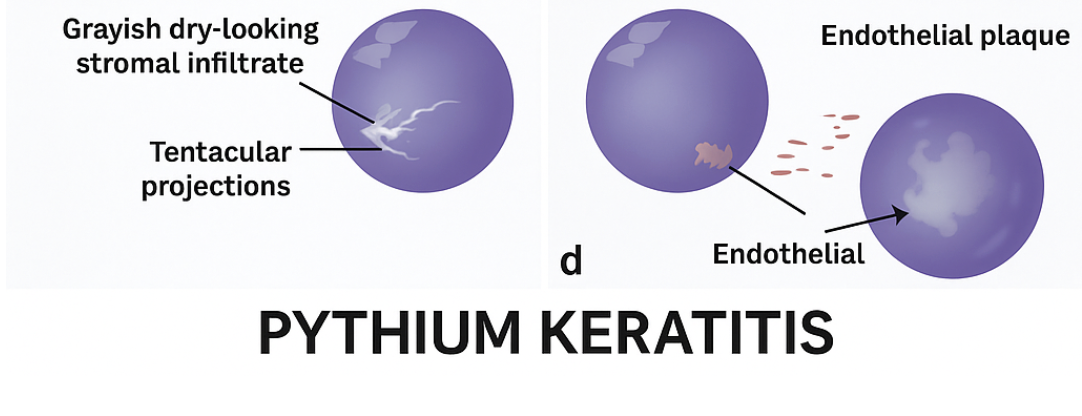
Pathognomic Features of Pythium insidiosum Keratitis. Characteristic dense, dry-looking stromal infiltrates with wispy tentacular projections and associated endothelial plaques characteristic of Pythium keratitis.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
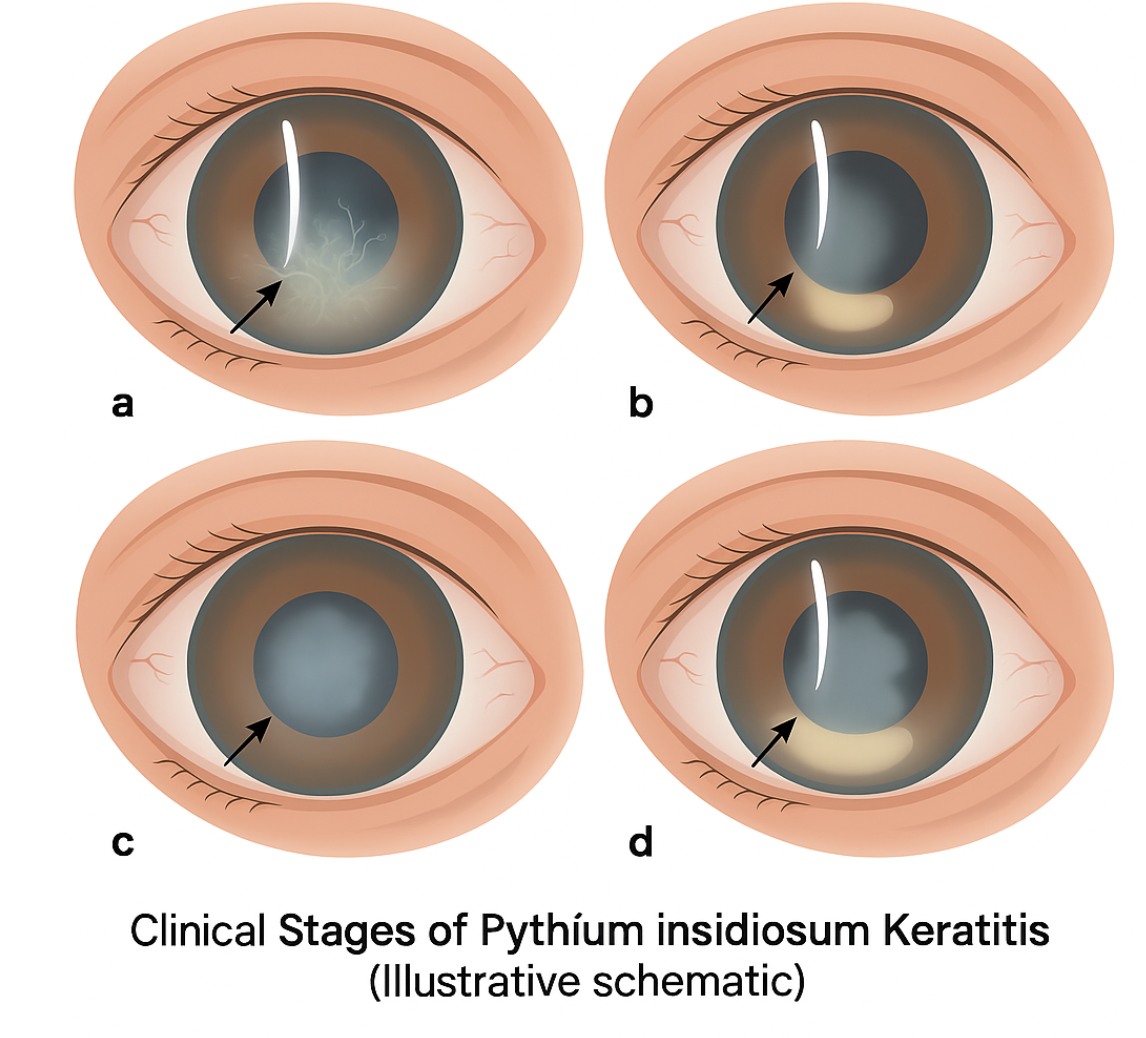
Clinical Features of Pythium Keratitis. A. Paracentral dry-looking cheesy infiltrate. B. Peripheral crescentric cheesy infiltrate C. Central dry-looking stromal infiltrate D. Progressive ulcer spreading to limbus.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
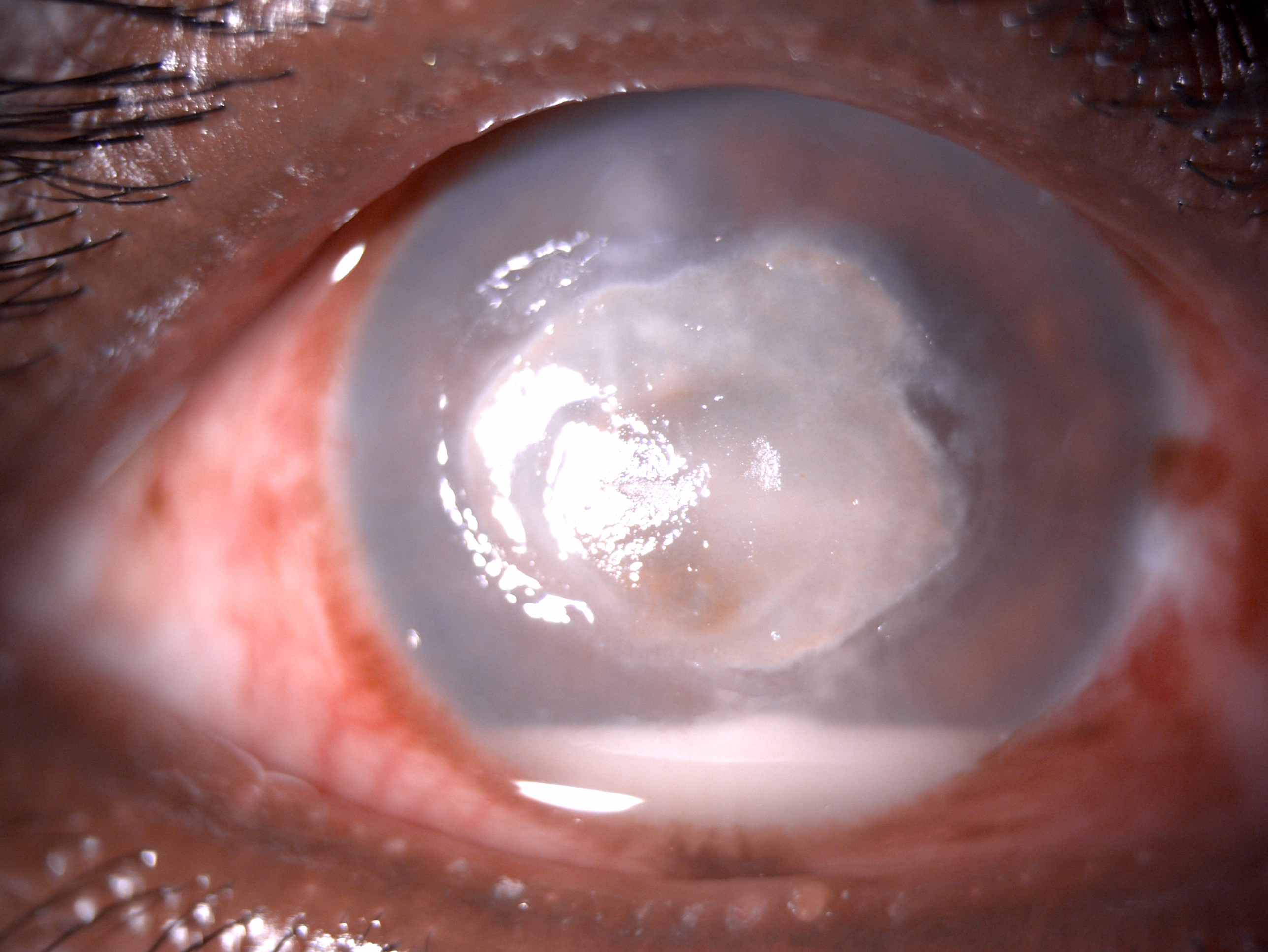
Slit-Lamp Examination of Pythium Keratitis. Healing anterior stromal plaque is present, along with a hypopyon. The presentation was similar to fungal keratitis, but culture results suggested Pythium keratitis.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
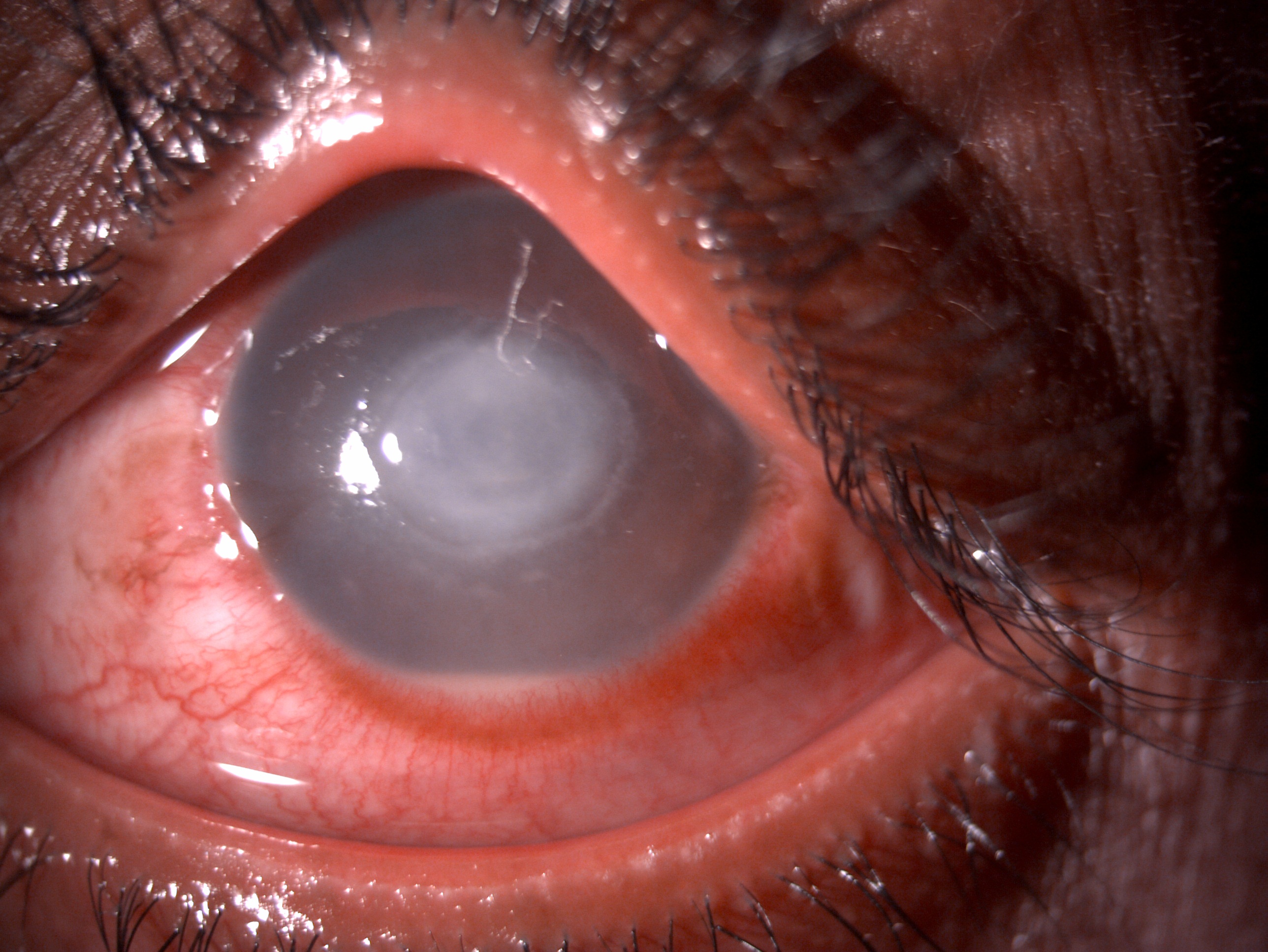
Slit-Lamp Examination of Fungal Keratitis. A central 4 X 4 mm anterior stromal infiltrate with hypopyon is suggestive of fungal keratitis.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
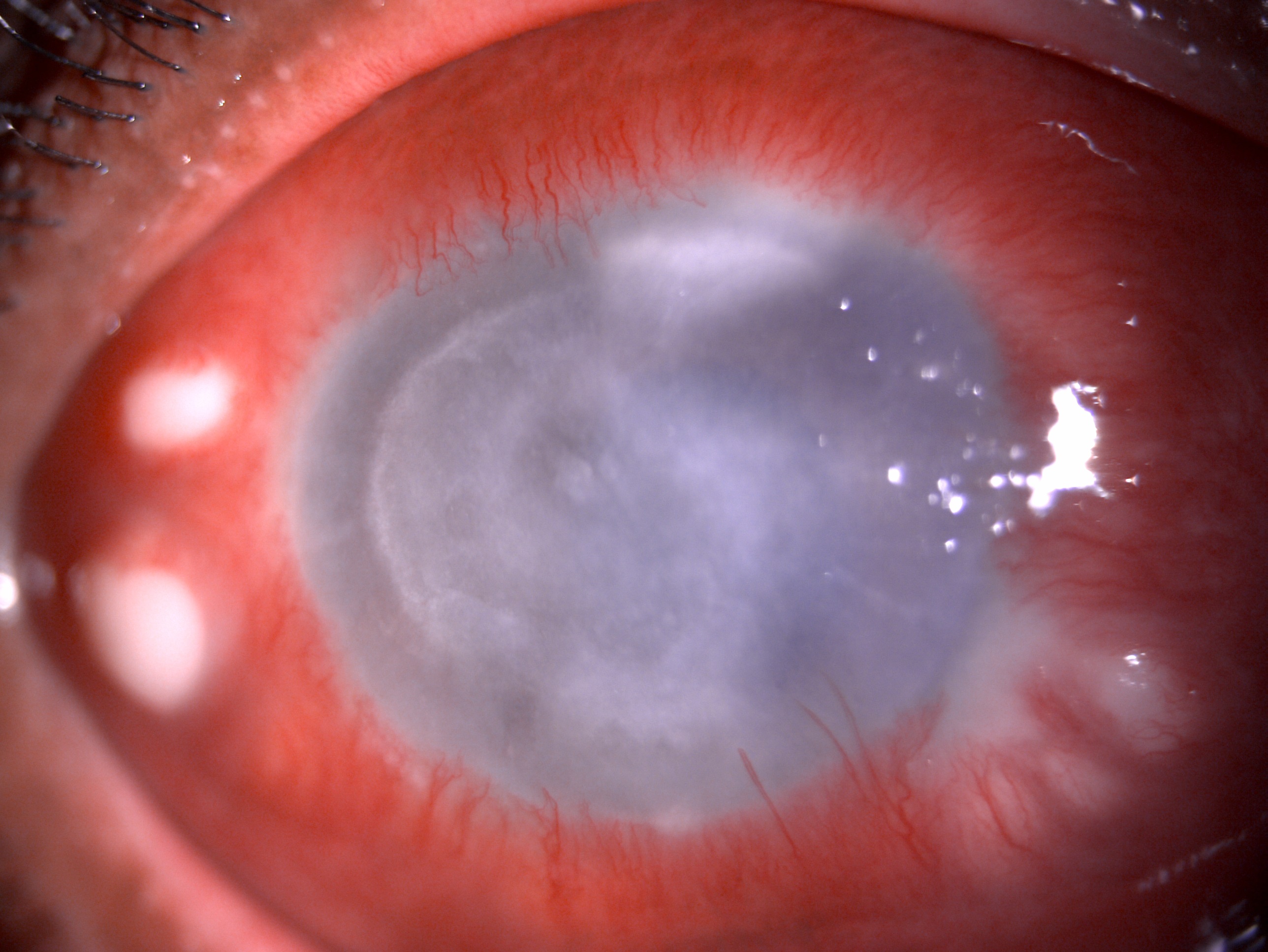
Slit-Lamp Examination of Acanthamoeba Keratitis. Diffuse congestion, a purulent point in the scleral pocket, and a diffuse midstromal infiltrate with thinning are suggestive of Acanthamoeba keratitis.
Contributed by B Gurnani, MD
References
Gurnani B, Kaur K. Anti-infective therapies for Pythium insidiosum keratitis. Expert review of anti-infective therapy. 2024 Oct:22(10):805-817. doi: 10.1080/14787210.2024.2403146. Epub 2024 Sep 13 [PubMed PMID: 39268901]
Gurnani B, Kaur K. Letter to the editor: Case series: Mixed infectious keratitis by Pythium insidiosum and fungal species. Optometry and vision science : official publication of the American Academy of Optometry. 2024 May 1:101(5):236. doi: 10.1097/OPX.0000000000002147. Epub [PubMed PMID: 38857033]
Level 2 (mid-level) evidenceGurnani B, Kaur K. Navigating the challenges of infective keratitis: A critical analysis of treatment and diagnostic approaches. Indian journal of ophthalmology. 2024 Aug 1:72(8):1227-1228. doi: 10.4103/IJO.IJO_706_24. Epub 2024 Jul 29 [PubMed PMID: 39078975]
Chang WH, Kuo YW, Hou YC. Optimizing early diagnosis and treatment of acanthamoeba keratitis through corneal scraping. Journal of optometry. 2026 Jan-Mar:19(1):100566. doi: 10.1016/j.optom.2025.100566. Epub 2025 Oct 15 [PubMed PMID: 41102075]
Gurnani B, Kaur K. Intricacies and solutions for interpretation of microbiologic samples of Pythium insidiosum keratitis. Indian journal of ophthalmology. 2024 Apr 1:72(4):602-603. doi: 10.4103/IJO.IJO_1573_23. Epub 2024 Mar 28 [PubMed PMID: 38546474]
Gurnani B, Natarajan R, Mohan M, Kaur K. Breaking-Down Barriers: Proposal of Using Cellulose Biosynthesis Inhibitors and Cellulase Enzyme as a Novel Treatment Modality for Vision Threatening Pythium Insidiosum Keratitis. Clinical ophthalmology (Auckland, N.Z.). 2024:18():765-776. doi: 10.2147/OPTH.S450665. Epub 2024 Mar 11 [PubMed PMID: 38495678]
Yu M, Li L, Liu Y, Wang T, Li H, Shi C, Guo X, Wu W, Gan C, Li M, Hong J, Dong K, Gong B. Pathogenesis and treatment strategies for infectious keratitis: Exploring antibiotics, antimicrobial peptides, nanotechnology, and emerging therapies. Journal of pharmaceutical analysis. 2025 Sep:15(9):101250. doi: 10.1016/j.jpha.2025.101250. Epub 2025 Feb 28 [PubMed PMID: 41050117]
Gurnani B, Kaur K. Understanding barriers, recommended solutions, and future prospects for the diagnosis and management of Pythium insidiosum keratitis. Indian journal of ophthalmology. 2023 Dec 1:71(12):3584-3586. doi: 10.4103/IJO.IJO_1041_23. Epub 2023 Nov 20 [PubMed PMID: 37991287]
Level 3 (low-level) evidenceGurnani B, Kaur K. Leap forward in clinical and photographic diagnosis of Pythium insidiosum keratitis. Indian journal of ophthalmology. 2023 Sep:71(9):3263-3264. doi: 10.4103/IJO.IJO_355_23. Epub [PubMed PMID: 37602622]
Gurnani B, Kaur K, Tandon A. Letter Regarding: Randomized Double-Masked Placebo-Controlled Trial for the Management of Pythium Keratitis: Combination of Antibiotics Versus Monotherapy. Cornea. 2023 Dec 1:42(12):e22-e23. doi: 10.1097/ICO.0000000000003350. Epub 2023 Jul 18 [PubMed PMID: 37487172]
Level 1 (high-level) evidenceGurnani B, Christy J, Narayana S, Rajkumar P, Kaur K, Gubert J. Retrospective multifactorial analysis of Pythium keratitis and review of literature. Indian journal of ophthalmology. 2021 May:69(5):1095-1101. doi: 10.4103/ijo.IJO_1808_20. Epub [PubMed PMID: 33913840]
Level 2 (mid-level) evidenceCao B, Gonugunta VT, Radhakrishnan N, Lalitha P, Gurnani B, Kaur K, Iyer G, Agarwal S, Srinivasan B, Keenan JD, Prajna NV. Outcomes of Pythium keratitis: a meta-analysis of individual patient data. Current ophthalmology reports. 2022 Dec:10(4):198-208. doi: 10.1007/s40135-022-00302-7. Epub 2022 Nov 10 [PubMed PMID: 37250102]
Level 1 (high-level) evidenceGurnani B, Kaur K, Kumar T. Commentary: Current concepts, recent updates, and future treatment options for Pythium insidiosum keratitis. Indian journal of ophthalmology. 2023 May:71(5):1874-1876. doi: 10.4103/IJO.IJO_80_23. Epub [PubMed PMID: 37203047]
Level 3 (low-level) evidenceZhang Y, Wang Y, Xu Y, Yang W. Effective automatic classification methods via deep learning for multi-type infectious keratitis diagnosis. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2026 Jan:264(1):171-183. doi: 10.1007/s00417-025-06996-2. Epub 2025 Oct 24 [PubMed PMID: 41134356]
Gurnani B, Kaur K, Gireesh P, Balakrishnan L, Mishra C. Evaluating the novel role of ChatGPT-4 in addressing corneal ulcer queries: An AI-powered insight. European journal of ophthalmology. 2025 Sep:35(5):1531-1541. doi: 10.1177/11206721251337290. Epub 2025 Apr 28 [PubMed PMID: 40295112]
Lorenzo-Morales J, Khan NA, Walochnik J. An update on Acanthamoeba keratitis: diagnosis, pathogenesis and treatment. Parasite (Paris, France). 2015:22():10. doi: 10.1051/parasite/2015010. Epub 2015 Feb 18 [PubMed PMID: 25687209]
Gurnani B, Kaur K. Post-market surveillance of ophthalmic implants: role of real-world evidence. Expert review of medical devices. 2025 Dec:22(12):1303-1308. doi: 10.1080/17434440.2025.2579578. Epub 2025 Oct 24 [PubMed PMID: 41123186]
Min K, Neiman AM, Konopka JB. Fungal Pathogens: Shape-Shifting Invaders. Trends in microbiology. 2020 Nov:28(11):922-933. doi: 10.1016/j.tim.2020.05.001. Epub 2020 May 27 [PubMed PMID: 32474010]
Gurnani B, Kaur K, Venugopal A, Srinivasan B, Bagga B, Iyer G, Christy J, Prajna L, Vanathi M, Garg P, Narayana S, Agarwal S, Sahu S. Pythium insidiosum keratitis - A review. Indian journal of ophthalmology. 2022 Apr:70(4):1107-1120. doi: 10.4103/ijo.IJO_1534_21. Epub [PubMed PMID: 35325996]
Gurnani B, Kaur K, Agarwal S, Lalgudi VG, Shekhawat NS, Venugopal A, Tripathy K, Srinivasan B, Iyer G, Gubert J. Pythium insidiosum Keratitis: Past, Present, and Future. Ophthalmology and therapy. 2022 Oct:11(5):1629-1653. doi: 10.1007/s40123-022-00542-7. Epub 2022 Jul 5 [PubMed PMID: 35788551]
Ung L, Bispo PJM, Shanbhag SS, Gilmore MS, Chodosh J. The persistent dilemma of microbial keratitis: Global burden, diagnosis, and antimicrobial resistance. Survey of ophthalmology. 2019 May-Jun:64(3):255-271. doi: 10.1016/j.survophthal.2018.12.003. Epub 2018 Dec 24 [PubMed PMID: 30590103]
Level 3 (low-level) evidenceGurnani B, Kaur K. Predicting Prognosis Based on Regional Prevalence, Ulcer Morphology and Treatment Strategy in Vision-Threatening Pythium insidiosum Keratitis. Clinical ophthalmology (Auckland, N.Z.). 2023:17():1307-1314. doi: 10.2147/OPTH.S412274. Epub 2023 May 5 [PubMed PMID: 37181081]
Gurnani B, Kaur K, Lalgudi VG, Kundu G, Mimouni M, Liu H, Jhanji V, Prakash G, Roy AS, Shetty R, Gurav JS. Role of artificial intelligence, machine learning and deep learning models in corneal disorders - A narrative review. Journal francais d'ophtalmologie. 2024 Sep:47(7):104242. doi: 10.1016/j.jfo.2024.104242. Epub 2024 Jul 15 [PubMed PMID: 39013268]
Level 3 (low-level) evidenceAbdelfattah NS, Amgad M, Zayed AA. Host immune cellular reactions in corneal neovascularization. International journal of ophthalmology. 2016:9(4):625-33. doi: 10.18240/ijo.2016.04.25. Epub 2016 Apr 18 [PubMed PMID: 27162740]
Hernández-Martínez D, Castro Pot E, Hernández Olmos P, Guzmán Hernández EA, Cobos DS, Villa Ramírez S, Villamar Duque TE, Durán Díaz Á, Omaña-Molina M. Acanthamoeba castellanii trophozoites that survive multipurpose solutions are able to adhere to cosmetic contact lenses, increasing the risk of infection. Heliyon. 2023 Sep:9(9):e19599. doi: 10.1016/j.heliyon.2023.e19599. Epub 2023 Aug 29 [PubMed PMID: 37809484]
Wang Y, Jiang L, Zhao Y, Ju X, Wang L, Jin L, Fine RD, Li M. Biological characteristics and pathogenicity of Acanthamoeba. Frontiers in microbiology. 2023:14():1147077. doi: 10.3389/fmicb.2023.1147077. Epub 2023 Apr 5 [PubMed PMID: 37089530]
Ruan Y, Jiang S, Musayeva A, Pfeiffer N, Gericke A. Corneal Epithelial Stem Cells-Physiology, Pathophysiology and Therapeutic Options. Cells. 2021 Sep 3:10(9):. doi: 10.3390/cells10092302. Epub 2021 Sep 3 [PubMed PMID: 34571952]
Gurnani B, Christy J, Kaur K, Moutappa F, Gubert J. Successful Management of Pythium insidiosum Keratitis Masquerading as Dematiaceous Fungal Keratitis in an Immunosuppressed Asian Male. Ocular immunology and inflammation. 2024 Jul:32(5):583-586. doi: 10.1080/09273948.2023.2179495. Epub 2023 Feb 22 [PubMed PMID: 36812410]
Gurnani B, Narayana S, Christy J, Rajkumar P, Kaur K, Gubert J. Successful management of pediatric pythium insidiosum keratitis with cyanoacrylate glue, linezolid, and azithromycin: Rare case report. European journal of ophthalmology. 2022 Sep:32(5):NP87-NP91. doi: 10.1177/11206721211006564. Epub 2021 Mar 28 [PubMed PMID: 33779337]
Level 3 (low-level) evidenceGurnani B, Kaur K, Gurav J. Natasol as a future management option to combat fungal keratitis. Indian journal of ophthalmology. 2023 May:71(5):2302-2303. doi: 10.4103/IJO.IJO_190_23. Epub [PubMed PMID: 37202986]
Jaiswal S, Kumari S, Kamboj A, Chandel A. Design and Evaluation of Econazole-Loaded Nanostructured Lipid Carriers for Ocular Treatment of Fungal Keratitis: In vitro and Ex vivo Studies. Pharmaceutical nanotechnology. 2025 Oct 8:():. doi: 10.2174/0122117385385940250917075923. Epub 2025 Oct 8 [PubMed PMID: 41088945]
Fanselow N, Sirajuddin N, Yin XT, Huang AJW, Stuart PM. Acanthamoeba Keratitis, Pathology, Diagnosis and Treatment. Pathogens (Basel, Switzerland). 2021 Mar 10:10(3):. doi: 10.3390/pathogens10030323. Epub 2021 Mar 10 [PubMed PMID: 33801905]
Gurnani B, Kaur K. Comment on: Sensitivity and specificity of potassium hydroxide and calcofluor white stain to differentiate between fungal and Pythium filaments in corneal scrapings from patients of Pythium keratitis. Indian journal of ophthalmology. 2022 Jun:70(6):2204. doi: 10.4103/ijo.IJO_345_22. Epub [PubMed PMID: 35648022]
Level 3 (low-level) evidenceGurnani B, Kaur K. Teleophthalmology-enabled devices: bridging the gap in rural eye care. Expert review of medical devices. 2025 Nov:22(11):1167-1172. doi: 10.1080/17434440.2025.2566741. Epub 2025 Oct 15 [PubMed PMID: 40990172]
Mittal R. Superficial punctate keratitis: A diagnostic dilemma. Oman journal of ophthalmology. 2021 Jan-Apr:14(1):62-63. doi: 10.4103/ojo.OJO_167_2019. Epub 2021 Feb 27 [PubMed PMID: 34084040]
Bagga B, Gowtham L, Djalilian AR, Sharma S. Clinical recommendations for the management of Pythium insidiosum keratitis. The ocular surface. 2025 Oct:38():242-250. doi: 10.1016/j.jtos.2025.08.003. Epub 2025 Aug 18 [PubMed PMID: 40835208]
Qiu S, Zhao GQ, Lin J, Wang X, Hu LT, Du ZD, Wang Q, Zhu CC. Natamycin in the treatment of fungal keratitis: a systematic review and Meta-analysis. International journal of ophthalmology. 2015:8(3):597-602. doi: 10.3980/j.issn.2222-3959.2015.03.29. Epub 2015 Jun 18 [PubMed PMID: 26086015]
Level 1 (high-level) evidenceSun MX, Chen JQ, Yao MC, Ye CT, Li J, Huang MM. [Ocular penetration and pharmacokinetics of topical voriconazole in rabbit eyes]. [Zhonghua yan ke za zhi] Chinese journal of ophthalmology. 2008 Apr:44(4):349-53 [PubMed PMID: 18844023]
Rakhshan A, Rahmati Kamel B, Saffaei A, Tavakoli-Ardakani M. Hepatotoxicity Induced by Azole Antifungal Agents: A Review Study. Iranian journal of pharmaceutical research : IJPR. 2023 Jan-Dec:22(1):e130336. doi: 10.5812/ijpr-130336. Epub 2023 Apr 9 [PubMed PMID: 38116543]
Larkin DF, Kilvington S, Dart JK. Treatment of Acanthamoeba keratitis with polyhexamethylene biguanide. Ophthalmology. 1992 Feb:99(2):185-91 [PubMed PMID: 1553206]
Al-Namaeh M. Systemic Medications and Their Ocular Side Effects. Cureus. 2024 Dec:16(12):e74976. doi: 10.7759/cureus.74976. Epub 2024 Dec 2 [PubMed PMID: 39744265]
Gurnani B, Kaur K. Advancing diagnostics in Pythium insidiosum keratitis: the emerging role of point-of-care imaging and biosensor-based detection devices. Expert review of medical devices. 2025 Dec:22(12):1287-1292. doi: 10.1080/17434440.2025.2582616. Epub 2025 Nov 2 [PubMed PMID: 41147335]
Connelly L, Anijeet D, Alexander CL. A descriptive case of persistent Acanthamoeba keratitis: raising awareness of this complex ocular disease. Access microbiology. 2020:2(3):acmi000084. doi: 10.1099/acmi.0.000084. Epub 2019 Nov 28 [PubMed PMID: 32974565]
Level 3 (low-level) evidenceLi G, Shekhawat N. Acanthamoeba epitheliopathy: Importance of early diagnosis. American journal of ophthalmology case reports. 2022 Jun:26():101499. doi: 10.1016/j.ajoc.2022.101499. Epub 2022 Mar 25 [PubMed PMID: 35402748]
Level 3 (low-level) evidenceCabrera-Aguas M, Khoo P, Watson SL. Infectious keratitis: A review. Clinical & experimental ophthalmology. 2022 Jul:50(5):543-562. doi: 10.1111/ceo.14113. Epub 2022 Jun 3 [PubMed PMID: 35610943]
Punjabi V, Patel S, Pathak J, Swain N. Comparative evaluation of staining efficacy of calcofluor white and acridine orange for detection of Candida species using fluorescence microscopy - A prospective microbiological study. Journal of oral and maxillofacial pathology : JOMFP. 2020 Jan-Apr:24(1):81-86. doi: 10.4103/jomfp.JOMFP_315_18. Epub 2020 May 8 [PubMed PMID: 32508453]
Level 2 (mid-level) evidenceRuggeri F, Rullo D, Maugliani E, Trotta N, Ciancimino C, Di Pippo M, Guglielmelli F, Abdolrahimzadeh S. The role of anterior segment optical coherence tomography in post-cataract surgery Descemet membrane detachment. International ophthalmology. 2025 Feb 18:45(1):74. doi: 10.1007/s10792-024-03397-y. Epub 2025 Feb 18 [PubMed PMID: 39964581]
Gurnani B, Kaur K. Pythium Keratitis. StatPearls. 2026 Jan:(): [PubMed PMID: 34424645]
Medsinge A, Gajdosova E, Moore W, Nischal KK. Management of inflammatory corneal melt leading to central perforation in children: a retrospective study and review of literature. Eye (London, England). 2016 Apr:30(4):593-601. doi: 10.1038/eye.2015.278. Epub 2016 Jan 29 [PubMed PMID: 26821761]
Level 2 (mid-level) evidenceThomas PA. Current perspectives on ophthalmic mycoses. Clinical microbiology reviews. 2003 Oct:16(4):730-97 [PubMed PMID: 14557297]
Level 3 (low-level) evidenceMcClellan K, Howard K, Niederkorn JY, Alizadeh H. Effect of steroids on Acanthamoeba cysts and trophozoites. Investigative ophthalmology & visual science. 2001 Nov:42(12):2885-93 [PubMed PMID: 11687533]
Schmier JK, Hulme-Lowe CK, Covert DW. Adjunctive therapy patterns in glaucoma patients using prostaglandin analogs. Clinical ophthalmology (Auckland, N.Z.). 2014:8():1097-104. doi: 10.2147/OPTH.S63760. Epub 2014 Jun 10 [PubMed PMID: 24959067]
Ma Y, Liu L, Yan M, Shi X, Yan M. Fungal Keratitis Caused by Alternaria alternata: A Rare Pathogen and Its Surgical Treatment. Experimental and clinical transplantation : official journal of the Middle East Society for Organ Transplantation. 2025 Sep:23(9):621-623. doi: 10.6002/ect.2025.0186. Epub [PubMed PMID: 41118139]
Kiyat P, Palamar M. Acanthamoeba keratitis: from pathophysiology to prevention, a contemporary clinical perspective. Medical hypothesis, discovery & innovation ophthalmology journal. 2025 Fall:14(3):146-162. doi: 10.51329/mehdiophthal1528. Epub 2025 Sep 27 [PubMed PMID: 41111636]
Level 3 (low-level) evidenceGurnani B, Christy J, Narayana S, Kaur K, Moutappa F. Corneal Perforation Secondary to Rosacea Keratitis Managed with Excellent Visual Outcome. Nepalese journal of ophthalmology : a biannual peer-reviewed academic journal of the Nepal Ophthalmic Society : NEPJOPH. 2022 Jan:14(27):162-167. doi: 10.3126/nepjoph.v14i1.36454. Epub [PubMed PMID: 35996914]
Lewis JS 2nd, Wiederhold NP, Hakki M, Thompson GR 3rd. New Perspectives on Antimicrobial Agents: Isavuconazole. Antimicrobial agents and chemotherapy. 2022 Sep 20:66(9):e0017722. doi: 10.1128/aac.00177-22. Epub 2022 Aug 15 [PubMed PMID: 35969068]
Level 3 (low-level) evidencePilmis B, Garcia-Hermoso D, Alanio A, Catherinot E, Scemla A, Jullien V, Bretagne S, Lortholary O. Failure of voriconazole therapy due to acquired azole resistance in Aspergillus fumigatus in a kidney transplant recipient with chronic necrotizing aspergillosis. American journal of transplantation : official journal of the American Society of Transplantation and the American Society of Transplant Surgeons. 2018 Sep:18(9):2352-2355. doi: 10.1111/ajt.14940. Epub 2018 Jul 12 [PubMed PMID: 29790292]
Das S, Pandey K, Rabidas VN, Mandal A, Das P. Effectiveness of miltefosine treatment in targeting anti-leishmanial HO-1/Nrf-2-mediated oxidative responses in visceral leishmaniasis patients. The Journal of antimicrobial chemotherapy. 2013 Sep:68(9):2059-65. doi: 10.1093/jac/dkt162. Epub 2013 May 31 [PubMed PMID: 23729024]
Medhasi S, Chindamporn A, Worasilchai N. A Review: Antimicrobial Therapy for Human Pythiosis. Antibiotics (Basel, Switzerland). 2022 Mar 26:11(4):. doi: 10.3390/antibiotics11040450. Epub 2022 Mar 26 [PubMed PMID: 35453202]
Yilmaz YC, Hayat SC, Bilgin GS, Altinkurt E. Tectonic and Therapeutic Urgent Penetrating Keratoplasty Outcomes. Beyoglu eye journal. 2024:9(2):61-68. doi: 10.14744/bej.2024.69772. Epub 2024 Jun 1 [PubMed PMID: 38854901]
Gurnani B, Kaur K. Comment on: Clinical and mycological profile of fungal keratitis from North and North-East India. Indian journal of ophthalmology. 2023 Jun:71(6):2607-2608. doi: 10.4103/ijo.IJO_1655_22. Epub [PubMed PMID: 37322697]
Level 3 (low-level) evidenceGurnani B, Kaur K. Contact Lens–Related Complications. StatPearls. 2026 Jan:(): [PubMed PMID: 36512659]
Gurnani B, Kaur K, Chaudhary S, Balakrishnan H. Ophthalmic manifestations of monkeypox infection. Indian journal of ophthalmology. 2023 May:71(5):1687-1697. doi: 10.4103/ijo.IJO_2032_22. Epub [PubMed PMID: 37203020]
Gurnani B, Kaur K, Chaudhary S, Kaur RP, Nayak S, Mishra D, Balakrishnan H, Parkash RO, Morya AK, Porwal A. Pediatric corneal transplantation: techniques, challenges, and outcomes. Therapeutic advances in ophthalmology. 2024 Jan-Dec:16():25158414241237906. doi: 10.1177/25158414241237906. Epub 2024 Mar 25 [PubMed PMID: 38533487]
Level 3 (low-level) evidenceClaerhout I, Goegebuer A, Van Den Broecke C, Kestelyn P. Delay in diagnosis and outcome of Acanthamoeba keratitis. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2004 Aug:242(8):648-53 [PubMed PMID: 15221303]
Thanathanee O, Bhoomibunchoo C, Anutarapongpan O, Suwan-Apichon O, Charoensuk K, Chindamporn A. Role of Immunotherapy in Pythium insidiosum Keratitis. The American journal of tropical medicine and hygiene. 2022 Jul 13:107(1):110-112. doi: 10.4269/ajtmh.22-0015. Epub 2022 Jun 6 [PubMed PMID: 35895358]
Byrd LB, Gurnani B, Martin N. Corneal Ulcer. StatPearls. 2026 Jan:(): [PubMed PMID: 30969511]
Chatterjee S, Agrawal D. Recurrence of Infection in Corneal Grafts After Therapeutic Penetrating Keratoplasty for Microbial Keratitis. Cornea. 2020 Jan:39(1):39-44. doi: 10.1097/ICO.0000000000002044. Epub [PubMed PMID: 31259861]
Wasielica-Poslednik J, Gericke A, Desuki A, Schlötzer-Schrehardt U, Pfeiffer N, Lisch W. Recurrence of paraproteinemic keratopathy after penetrating keratoplasty and its assessment with confocal microscopy. American journal of ophthalmology case reports. 2018 Sep:11():87-91. doi: 10.1016/j.ajoc.2018.06.014. Epub 2018 Jun 20 [PubMed PMID: 30014052]
Level 3 (low-level) evidenceShorter E, Harthan J, Nau CB, Nau A, Barr JT, Hodge DO, Schornack MM. Scleral Lenses in the Management of Corneal Irregularity and Ocular Surface Disease. Eye & contact lens. 2018 Nov:44(6):372-378. doi: 10.1097/ICL.0000000000000436. Epub [PubMed PMID: 28968300]
Lu SH, Qiao DN, Dong PF. A nursing report on a corneal contact lens wearer receiving keratoplasty due to corneal ulcer and perforation caused by Pythium insidiosum infection: A case report. Medicine. 2024 Apr 5:103(14):e37663. doi: 10.1097/MD.0000000000037663. Epub [PubMed PMID: 38579080]
Level 2 (mid-level) evidencePinna A. Acanthamoeba and disinfecting contact lens solutions. The British journal of ophthalmology. 2002 Dec:86(12):1461-2 [PubMed PMID: 12446410]
Burrow MK, Gurnani B, Patel BC. Keratoconjunctivitis. StatPearls. 2026 Jan:(): [PubMed PMID: 31194419]
Kaur H, Roy M, Jamir I, Yadav S, Gupta A, Ghosh A, Angrup A, Rudramurthy SM. Prospective study on combined use of Sabouraud dextrose agar and blood agar for improved recovery of etiological agents in mycotic and Pythium keratitis. Journal of microbiological methods. 2025 Oct:237():107247. doi: 10.1016/j.mimet.2025.107247. Epub 2025 Sep 5 [PubMed PMID: 40915617]
Gurnani B, Kaur K. Corneal cross-linking for keratoconus: a global economic and clinical perspective. Journal of medical economics. 2025 Dec:28(1):2119-2124. doi: 10.1080/13696998.2025.2587416. Epub 2025 Nov 30 [PubMed PMID: 41320236]
Level 3 (low-level) evidenceMurugan SB, Sunil Kumar, Gurnani B, Kaur K. Assessment of Subjective Visual Experiences During Intraocular Surgery and Intravitreal Injection Among Uveitis Patients at a Tertiary Eye Hospital: A Cross-Sectional Observational Study. Ophthalmology and therapy. 2026 Jan:15(1):173-191. doi: 10.1007/s40123-025-01264-2. Epub 2025 Nov 6 [PubMed PMID: 41196490]
Level 2 (mid-level) evidenceHossain P. The corneal melting point. Eye (London, England). 2012 Aug:26(8):1029-30. doi: 10.1038/eye.2012.136. Epub 2012 Jul 6 [PubMed PMID: 22766538]
Gurnani B, Kaur K. Response to letter regarding "Evaluating the novel role of ChatGPT-4 in addressing corneal ulcer queries: An AI-powered insight". European journal of ophthalmology. 2026 May:36(3):NP5-NP7. doi: 10.1177/11206721251357376. Epub 2025 Jul 9 [PubMed PMID: 40629931]
Level 3 (low-level) evidenceNishant P, Gurnani B, Singh P, Sinha S, Kaur K, Kumar A, Sinha RK. Current concepts and recent trends in endothelial keratoplasty. World journal of transplantation. 2025 Jun 18:15(2):102507. doi: 10.5500/wjt.v15.i2.102507. Epub [PubMed PMID: 40535500]
Sharma L, Prakash A, Medhi B. Ensuring medication and patient safety for better quality healthcare. Indian journal of pharmacology. 2024 Nov 1:56(6):375-378. doi: 10.4103/ijp.ijp_109_25. Epub 2025 Feb 19 [PubMed PMID: 39973825]
Level 2 (mid-level) evidenceHashemian MN, Zia MJ, Khorrami-Nejad M, Abed QS, Hashemian H. Long-term outcomes of corneal transplantation: a review of 8,378 patients. BMC ophthalmology. 2025 Jan 22:25(1):39. doi: 10.1186/s12886-024-03826-7. Epub 2025 Jan 22 [PubMed PMID: 39844058]