 Artificial Intelligence and Deep Learning in the Diagnosis of Pythium Keratitis
Artificial Intelligence and Deep Learning in the Diagnosis of Pythium Keratitis
Introduction
Pythium insidiosum keratitis (PIK) represents one of the most formidable challenges in modern corneal infectious disease management. It is a sight-threatening corneal infection caused by an aquatic oomycete that clinically and histopathologically mimics filamentous fungal keratitis but remains refractory to conventional antifungal therapy. This intrinsic resistance stems from the organism’s unique cell-wall biochemistry, which lacks ergosterol, the target of most antifungal agents. Consequently, delayed or incorrect treatment often results in rapid stromal necrosis, corneal perforation, and the need for therapeutic keratoplasty (TPK), frequently resulting in poor visual outcomes despite aggressive management.[1]
Historically, Pythium infections were first reported in animals, particularly in horses and dogs, prior to recognition of human ocular involvement. For decades, Pythium was misclassified as a fungus due to its filamentous morphology, aseptate hyphae, and growth patterns on culture media that resembled those of fungi. However, advances in molecular taxonomy identified Pythium as an oomycete (water mold) phylogenetically related to algae. Its cell wall, composed predominantly of cellulose and β-glucans rather than chitin, and the absence of ergosterol in its membrane, explain the organism’s insensitivity to antifungal agents such as amphotericin B, natamycin, and azoles.[2]
Clinically, the disease course is aggressive. The typical patient presents with pain, redness, photophobia, and blurred vision following minor trauma or water exposure. On slit-lamp biomicroscopy, the infection produces reticular or tentacle-like stromal infiltrates radiating from a dense central lesion. These “tentacular extensions,” a hallmark of Pythium keratitis, may be accompanied by endothelial plaque formation, ring infiltrates, or hypopyon. Despite antifungal therapy, lesions worsen within days, leading to melting and eventual perforation. This insensitivity to antifungal agents remains the most valuable clinical clue for differentiating fungal keratitis.[3]
Over the past decade, Pythium insidiosum keratitis has shifted from a regional disease confined to tropical Asia to a global ophthalmic concern. India, Thailand, and northern Australia report the majority of cases, but sporadic cases are also reported in temperate regions, including the United States and Europe, suggesting environmental adaptability. Contributory factors include agricultural exposure, increased contact-lens use, and climate-driven changes in humidity and water contamination. In India, the monsoon season correlates with surges in cases, particularly in rice-growing regions where patients frequently come into contact with muddy or stagnant water.[4]
Despite improved awareness, misdiagnosis remains common. In many tertiary eye centers, Pythium is still frequently misdiagnosed as filamentous fungal keratitis, particularly when laboratory confirmation is delayed or unavailable. Culture-based diagnosis is notoriously slow and yields low positivity rates. Traditional microbiological techniques, such as potassium hydroxide (KOH) smears and culture on Sabouraud or blood agar, may reveal aseptate hyphae but cannot reliably distinguish among Pythium species. Advanced techniques such as polymerase chain reaction (PCR), loop-mediated isothermal amplification (LAMP), and matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) improve specificity but remain restricted to specialized centers. This diagnostic gap has created an urgent need for rapid, accessible, and accurate diagnostic solutions—a need that is increasingly being addressed by artificial intelligence (AI) and deep learning (DL).[5]
AI and DL have ushered in a new era in ophthalmic diagnostics. While the earliest AI applications targeted retinal diseases such as diabetic retinopathy, age-related macular degeneration, and glaucoma screening, recent advances have extended to infectious keratitis, including bacterial, fungal, and Pythium etiologies. The ability of AI systems to detect subtle color, texture, and structural patterns invisible to the human eye positions them as ideal tools for early and accurate diagnosis. Using deep convolutional neural networks (CNNs), ResNets, DenseNets, and Vision Transformers (ViTs), algorithms can automatically classify slit-lamp or confocal images within seconds, achieving high sensitivity and specificity (>90%) in differentiating Pythium from fungal and bacterial keratitis.[6]
A major advantage of AI-based diagnostic systems is their real-time adaptability. Models trained on curated image datasets can continuously learn from new cases, refining diagnostic precision across ethnic, climatic, and imaging variations. For Pythium keratitis, AI systems have demonstrated the ability to recognize the “reticular stromal pattern,” “peripheral tentacular projections,” and “irregular stromal reflectivity” on slit-lamp and confocal microscopy—signatures that distinguish it from fungal keratitis. Furthermore, spectral features extracted from anterior segment optical coherence tomography (AS-OCT) can be automatically processed by AI to detect hyperreflective stromal bands and infiltrate depth patterns predictive of Pythium infection.[7]
Beyond image recognition, AI contributes to disease progression modeling and treatment optimization. Predictive analytics can estimate the probability of medical therapy failure, thereby prompting earlier surgical intervention. Equally transformative is the emergence of AI-integrated biosensor technologies. Biosensors that detect Pythium-specific antigens, cell wall enzymes, or DNA fragments can be linked to cloud-based AI analytics to enable on-site diagnosis in less than 30 minutes. These point-of-care (POC) diagnostic platforms, powered by AI, enable early recognition even in peripheral or rural clinics, dramatically reducing diagnostic delay. In addition, AI-assisted digital confocal microscopy and smartphone-based slit-lamp imaging facilitate teleophthalmology-based referrals, connecting rural practitioners with tertiary cornea specialists through automated image triage systems.[8]
Recent works have been pivotal in integrating AI frameworks into diagnostic algorithms and teleophthalmology workflows for PIK. Their studies emphasize developing accessible, low-cost, cloud-enabled diagnostic tools that can operate without high-end computational infrastructure. The proposed teleophthalmology model envisions smartphone-attached imaging modules that capture anterior segment photographs and upload them to centralized AI servers for instant analysis and remote expert validation. Such systems could potentially reduce diagnostic turnaround times from days to hours, improving prognosis by facilitating the timely initiation of targeted therapy.[9]
The role of AI in Pythium keratitis extends beyond detection; there are opportunities for its use in prognostication, drug development, and surgical planning. Deep-learning algorithms can analyze serial imaging data to forecast lesion progression, guide follow-up frequency, and predict recurrence post-keratoplasty. Reinforcement-learning models have been experimentally tested to optimize dosing schedules for antibacterial combinations such as linezolid and azithromycin, which are currently the most effective therapeutic agents against Pythium. Furthermore, AI-based drug discovery tools simulate molecular docking between candidate compounds and Pythium enzymes such as cellulose synthase, facilitating the identification of novel cellulose-biosynthesis inhibitors (CBIs).[10]
In surgical contexts, AI integration with AS-OCT can assist surgeons in determining optimal graft dimensions and predicting post-TPK outcomes. Image-segmentation algorithms quantify residual stromal thickness and necrotic zones, helping define graft margins intraoperatively. Post-surgical monitoring using AI-analyzed serial slit-lamp photographs can detect early graft infiltration or recurrence, alerting clinicians before subjective visual deterioration.[11]
In summary, Pythium insidiosum keratitis stands at the intersection of clinical complexity and technological innovation. While its aggressive course and antifungal resistance continue to threaten vision worldwide, the synergy of artificial intelligence, molecular diagnostics, and teleophthalmology offers unprecedented hope for early detection and better outcomes. By combining image analytics, biosensing, and predictive modeling, AI is redefining diagnostic ophthalmology, transforming a once obscure pathogen into a model for intelligent infection management in the 21st century.[12]
Table. Comparative Overview of Diagnostic Modalities in Pythium Keratitis
|
Diagnostic Method |
Principle |
Turnaround Time |
Sensitivity (%) |
Limitations |
|
Smear & KOH mount |
Microscopy |
1–2 h |
40–60 |
Operator-dependent |
|
Culture (Sabouraud, cornmeal) |
Growth of zoospores |
2–5 d |
50–70 |
Slow growth, misidentification |
|
PCR / LAMP |
DNA amplification |
3–6 h |
85–95 |
Requires lab setup |
|
AS-OCT / in vivo confocal microscopy (IVCM) |
Imaging pattern |
Instant |
80–90 |
Needs expertise |
|
AI/DL-based imaging |
Pattern recognition |
<1 h |
90–98 |
Dataset-dependent |
|
Biosensor + AI hybrid |
Biomarker detection |
<30 min |
>95 |
Early-phase validation |
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Pythium insidiosum is a filamentous aquatic oomycete, an organism taxonomically belonging to the kingdom Stramenopila, class Oomycota, and more closely related to diatoms and brown algae than to true fungi. This evolutionary lineage explains its unique biochemical profile and clinical behavior. Unlike fungi, Pythium lacks chitin and ergosterol and instead uses cellulose and β-glucans in its cell wall. This biochemical difference renders conventional antifungal drugs, such as amphotericin B, natamycin, and azoles, largely ineffective because their primary targets (ergosterol or chitin synthesis) are absent.[13]
The organism’s life cycle centers around the production of biflagellate zoospores, which thrive in stagnant freshwater, paddy fields, irrigation channels, aquaculture tanks, and wet soil. These motile zoospores exhibit chemotactic attraction toward damaged corneal epithelium. Upon reaching the ocular surface, they encyst, adhere firmly to the corneal substrate, and germinate, forming invasive hyphae that penetrate the Descemet membrane and invade deeper stromal layers.[14]
Once inside the cornea, Pythium secretes a variety of hydrolytic enzymes, including cellulases, proteases, lipases, and collagenases, which collectively degrade the stromal extracellular matrix. This enzymatic degradation leads to rapid stromal necrosis, ring infiltration, and the characteristic tentacle-like radial extensions visible on slit-lamp examination. Recent molecular profiling has identified cellulose synthase genes and serine protease families as major virulence determinants contributing to corneal invasion.[15]
In contrast to most opportunistic keratitis pathogens, Pythium insidiosum infections commonly occur in immunocompetent individuals, often following minor ocular trauma, particularly with vegetative or aquatic material. Occupational exposure plays a crucial role—farmers, fishermen, and irrigation workers are at the highest risk. Environmental factors such as warm temperature (28–35 °C), high humidity, and stagnant water reservoirs enhance zoospore proliferation and persistence, explaining the seasonal spikes during monsoon months in tropical Asia.[16] Interestingly, more recent epidemiologic data also show Pythium infections among contact lens wearers and post-keratoplasty recipients, which are attributed to microabrasions, biofilm formation, and contaminated lens solutions. These cases highlight the pathogen’s adaptability beyond agrarian exposures.
Artificial intelligence (AI) is now playing an important role in etiologic characterization. Deep learning algorithms can analyze cytologic smear and histopathology images to distinguish Pythium hyphae from those of true fungi. This approach has enabled automated screening for Pythium in digital pathology, which is especially useful in laboratories with limited mycology expertise. Additionally, machine-learning models have been applied to environmental surveillance. Remote sensing data and humidity/temperature indices, integrated with AI-based predictive analytics, have been proposed for forecasting outbreaks in endemic agricultural regions. Such innovations highlight how AI can bridge basic microbiological understanding and real-world epidemiologic monitoring.[17]
Table. Etiologic and Environmental Determinants of Pythium insidiosum Keratitis
|
Determinant |
Mechanism / Description |
Evidence Summary |
|
Stagnant freshwater exposure |
Motile zoospores released in nutrient-rich aquatic habitats adhere to corneal defects |
Major determinant in Indian and Thai clusters; seasonal monsoon correlation |
|
Vegetative or soil trauma |
Physical breach of the epithelium permits zoospore entry; cellulose-degrading enzymes accelerate penetration |
Most common antecedent in rural PIK cohorts |
|
Occupational exposure (farming, irrigation work) |
Repeated contact with muddy or stagnant water increases risk of inoculation |
60%–70% of Indian PIK cases occur among agricultural workers |
|
Contact lens wear |
Microabrasion and solution contamination enable zoospore attachment |
Sporadic reports from temperate climates |
Table. Pathogenic and Diagnostic Determinants Influencing the Severity and Management of Pythium insidiosum Keratitis
|
Determinant |
Mechanism / Description |
Clinical Implication / Evidence |
|
Cellulose-rich cell wall |
Absence of ergosterol confers resistance to amphotericin B, natamycin, and azoles |
Central biochemical mechanism underlying antifungal treatment failure |
|
Enzymatic virulence (cellulase, collagenase, protease) |
Degradation of stromal collagen and basement membrane facilitates rapid tissue invasion |
Confocal microscopy findings and genomic studies correlate with severity grade |
|
Host immune response |
Predominantly neutrophilic inflammation without granulomatous reaction |
Explains rapid progression despite intact host immunity |
|
AI-based morphologic recognition |
CNN-based detection of Pythium hyphae on digital microscopy |
Facilitates rapid differentiation from fungal keratitis |
Epidemiology
Pythium insidiosum keratitis (PIK) has evolved from a regional tropical infection into a global ophthalmic concern, reflecting both climatic adaptability and advances in diagnostic recognition (see Image. Schematic diagram depicting epidemiology of Pythium insidiosum keratitis). First described in Thailand and India in the late 20th century, it was long mistaken for fungal keratitis. Over the past decade, the pathogen has been increasingly reported from South and Southeast Asia, Oceania, the Middle East, and even North America, marking its emergence as a pathogen of international relevance.[18]
Global Distribution
- India: India currently represents the largest global burden of PIK, with endemic clusters reported from Tamil Nadu, Kerala, Madhya Pradesh, Gujarat, and Rajasthan. Gurnani et al (2023) noted a substantial increase in Pythium isolation rates during the monsoon season, with 12% to 15% of initially culture-negative microbial keratitis cases subsequently confirmed as Pythium by histopathology or molecular assays. Hotspot mapping indicates that western and southern India are at particular risk due to rice cultivation, exposure to stagnant water, and humid climates.[19]
- Thailand: Thailand historically contributed the earliest case series, especially among rice-field workers and irrigation farmers. Pythium remains endemic in the Chiang Mai and Bangkok regions, with community-based surveillance studies reporting 3%–5% of microbial keratitis isolates attributable to Pythium.[20]
- Australia: Sporadic outbreaks have been documented in northern and northeastern Australia, particularly in Queensland and the Northern Territory, often associated with exposure to floodwater and warm coastal climates.[21]
- United States: Although rare, Pythium keratitis has been reported in Florida, Texas, and Louisiana, typically associated with aquatic, horticultural, or domestic animal exposures. The presence of Pythium in temperate climates suggests global dissemination facilitated by waterborne spore persistence and climatic shifts.[22]
- Middle East and Africa: Isolated reports from Saudi Arabia, Egypt, and sub-Saharan Africa highlight the possibility of under-recognition in arid zones due to diagnostic limitations rather than true absence.
Demographics and Risk Factors
PIK affects both sexes almost equally, although a slight male predominance has been observed (M:F distribution is approximately 1.3:1), likely reflecting occupational exposure in agrarian settings. The median age group is 35–50 years, corresponding to the working rural population. Pediatric cases are uncommon but documented; these often follow trauma or contaminated water exposure. The infection is not associated with immunodeficiency, differentiating it from fungal and bacterial opportunistic keratitis.[23]
Seasonal peaks correlate strongly with monsoon months (June–September) in India and Thailand, paralleling increased rainfall, irrigation activity, and freshwater contamination. Temperature thresholds between 28 to 35 °C and high relative humidity (>80%) favor zoospore motility and encystment (see Image. Schematic diagram depicting risk factors for Pythium insidiosum keratitis).
Environmental Correlates and Climate Dynamics
Environmental surveillance studies have detected Pythium DNA in rice-field water, wetlands, aquaculture ponds, and soil sediments, confirming its saprophytic aquatic lifestyle. Seasonal flooding, irrigation, and stagnant water facilitate spore proliferation and ocular exposure through splashing or trauma. Climate change and rising global temperatures are likely to expand the pathogen’s ecological range, with increasing reports from subtropical and temperate latitudes. Geospatial modeling suggests that areas undergoing agricultural intensification and erratic rainfall cycles may become emerging foci.[24]
Artificial Intelligence and Predictive Epidemiology
Recent research integrates AI and geospatial machine learning to forecast Pythium outbreaks. AI-driven epidemiological mapping utilizes satellite-derived data on rainfall, soil moisture, land use, and agricultural density to model spatiotemporal disease risk. These systems employ gradient-boosted decision trees (GBDTs), convolutional neural networks (CNNs), and geographic information systems (GIS) to detect environmental signatures predictive of Pythium activity.[25]
Table. Global Epidemiology and Demographic Trends in Pythium Keratitis
|
Region |
Key Environmental Factors |
Prevalence/Incidence |
Predominant Risk Group |
|
India (South, West, Central) |
Paddy irrigation, monsoon humidity |
8%–15% of initially culture-negative ulcers |
Farmers, field workers |
|
Thailand |
Rice field exposure, warm stagnant water |
1%–3% of microbial keratitis |
Agricultural laborers |
|
Australia (North/Queensland) |
Floodwater and aquaculture exposure |
Sporadic, <1% |
Coastal farmers |
|
United States (Florida/Texas) |
Warm, humid environments, aquatic exposure |
Isolated case reports |
Swimmers, pet owners |
|
Middle East / Africa |
Irrigation and livestock proximity |
Emerging; underdiagnosed |
Irrigators, herders |
Table. Geographic and Demographic Distribution of Pythium Keratitis
|
Region |
Predominant Season |
Mean Age (years) |
Occupation |
Major Risk Factor |
|
India (South & West) |
Monsoon |
40–50 |
Farmer |
Water exposure |
|
Thailand |
Rainy season |
30–45 |
Rice cultivator |
Flood irrigation |
|
Australia |
Summer |
45–55 |
Outdoor workers |
Aquatic trauma |
|
USA |
Summer |
35–50 |
Recreational swimmer |
Freshwater contact |
Pythium insidiosum keratitis exhibits a distinctive eco-epidemiological pattern, tightly linked to water, climate, and occupational exposure. Although predominantly a tropical agrarian infection, its detection in temperate countries underscores its increasingly global relevance. With rising awareness, diagnostic precision, and AI-driven surveillance, epidemiological data are being redefined from passive recognition to predictive modeling. Integrating AI-based early warning systems with clinical teleophthalmology networks promises a transformative shift toward preemptive public health measures in managing Pythium outbreaks worldwide.[15]
Pathophysiology
Pythium insidiosum keratitis (PIK) is caused by an aquatic oomycete that exhibits a distinctive pathobiologic cascade, beginning with zoospore adhesion, corneal invasion, and stromal destruction, culminating in severe inflammatory damage (see Image. Schematic diagram depicting pathophysiology of Pythium insidiosum keratitis). The organism’s virulence stems from a combination of a unique cell wall composition, enzymatic aggression, immune evasion, and biofilm formation, which together lead to rapid corneal necrosis and high post-surgical recurrence rates. Unlike fungal keratitis, the disease’s progression is driven by cellulose-mediated adhesion and collagenolytic degradation, rather than chitin-ergosterol-based mechanisms.
1. Entry and Initiation of Infection
The infection begins when biflagellate zoospores encounter a compromised corneal epithelium, typically following trauma from vegetation or aquatic exposure. These motile spores exhibit chemotaxis toward damaged corneal surfaces, guided by chemical cues, including amino acids, sugars, and ionic gradients generated by tear film proteins. Upon contact, zoospores encyst, shed their flagella, and form a glycoprotein capsule that facilitates adhesion to epithelial cells and stromal collagen.
AI-assisted microscopic analysis of early-phase infections has shown that Pythium zoospores preferentially attach to epithelial microdefects and Descemet membrane microfolds, which can now be digitally mapped through AI-enhanced confocal microscopy. Such imaging reveals distinct “gliding” patterns of encysted cells, unlike the budding seen in fungi.[26]
2. Germination and Hyphal Invasion
Once encysted, germ tubes emerge within 1 to 2 hours, forming coenocytic (aseptate) hyphae that penetrate the corneal stroma. These hyphae exhibit broad, ribbon-like morphology (4–10 µm width) and show strong tropism toward collagen-rich zones. The infection rapidly spreads laterally through stromal lamellae, aided by the following enzymatic mechanisms.
- Cellulase and β-1,3-glucanase enzymes break down stromal polysaccharides.
- Collagenase and protease complexes degrade the extracellular matrix (ECM).
- Lipases and phospholipases damage host cell membranes.
AI-based segmentation models applied to digital histopathology slides can distinguish these enzymatic zones by analyzing stromal reflectivity and necrosis gradients, correlating with clinical severity scores.[27]
3. Host Immune Response
PIK elicits an acute neutrophilic immune response, unlike the mixed granulomatous inflammation typical of fungal infections. Neutrophils release reactive oxygen species (ROS) and proteolytic enzymes in an attempt to contain the infection, but the pathogen’s cellulose capsule resists phagocytosis. The organism then secretes serine protease inhibitors and elastase analogues that neutralize neutrophil elastase and impair oxidative killing.
This immune dysregulation leads to the formation of dense stromal abscesses, peripheral ring infiltration, and endothelial plaques. In vivo confocal microscopy (IVCM) reveals hyper-reflective hyphal strands with surrounding activated keratocytes and leukocytes, forming the diagnostic “reticular honeycomb” pattern. AI-aided image analysis allows quantitative grading of inflammation by measuring reflectivity, cell density, and stromal edema, enabling objective staging.[28]
4. Enzymatic and Molecular Pathways
Molecular studies have identified multiple virulence-associated genes in Pythium insidiosum:
- PiC1 and PiC2 encode cellulase isoenzymes responsible for stromal penetration.
- PiP1 (Protease-1) and PiCol (Collagenase) promote degradation of the Bowman and Descemet membranes.
- PiA1 (Adhesin) facilitates biofilm adherence to corneal stroma.
- PiGly (Glycosyl hydrolase) enhances nutrient acquisition in hypoxic conditions.
AI-driven molecular docking and in silico modeling studies have further elucidated enzyme–substrate interactions, predicting strong binding affinities between cellulose synthase inhibitors (CBIs) (eg, carpropamid) and the PiC1 active site. These computational insights are now guiding drug repurposing efforts for non-antifungal PIK therapy.[29]
5. Stromal Necrosis and Corneal Destruction
As enzymatic activity intensifies, stromal lamellae lose tensile integrity, leading to melting and descemetocele formation. This necrotic stage often develops within 7 to 10 days from onset. AI-assisted AS-OCT imaging quantifies stromal reflectivity loss and edema index, enabling early prediction of impending perforation. The characteristic “tentacular extensions” seen clinically correspond to hyphal migration tracks, which appear as linear hyperreflective projections on AS-OCT and IVCM. CNN-based texture analysis of these tentacles achieves over 95% sensitivity in distinguishing Pythium from fungal infiltrates, making it a noninvasive biomarker.[30]
6. Resistance to Antifungal Therapy
The absence of ergosterol in Pythium membranes explains the complete ineffectiveness of amphotericin B, natamycin, and azoles. Furthermore, the organism’s cellulose-based membrane and high β-glucan content limit permeability to polyene and azole molecules. The biofilm matrix impedes drug diffusion, while enzymatic metabolism neutralizes drug activity.[31]
7. Post-Keratoplasty Recurrence Mechanisms
Recurrence after therapeutic penetrating keratoplasty (TPK) occurs in 20% to 40% of cases. The residual infection persists in the host scleral margins or limbal tissues. Histopathologic sections of failed grafts reveal dormant hyphal fragments surrounded by fibrovascular proliferation.
AI-assisted postoperative slit-lamp surveillance can automatically detect micro-recurrence patterns (eg, minute satellite infiltrates or texture irregularities) weeks before clinical recognition. This early detection allows prompt re-intervention, thereby significantly improving graft survival.[32]
8. Artificial Intelligence in Pathophysiologic Modeling
AI technologies have begun reshaping the understanding of PIK pathogenesis beyond microscopy. Three key domains stand out:
- Image-Based Pathology Recognition CNNs, Vision Transformers (ViTs), and autoencoders trained on corneal histopathology images can now identify Pythium hyphae, quantify enzymatic necrosis zones, and predict organism viability index.
- Predictive Disease Modeling Machine-learning algorithms integrate patient demographics, environmental exposure, and imaging biomarkers to model infection kinetics. Random forest models can predict time to perforation, need for TPK, and likelihood of recurrence with high precision.
- Molecular Simulation and Drug Targeting AI-driven molecular dynamics and generative models simulate enzyme–drug interactions, identifying new potential inhibitors targeting cellulose synthase and serine protease pathways. These in silico platforms accelerate therapeutic discovery without the need for prolonged culture-based testing.[33]
9. Neuro-Immune Crosstalk and Pain Mechanisms
PIK also exhibits atypical pain profiles—often disproportionate to corneal findings. This finding is attributed to neuroimmune inflammation, in which proinflammatory cytokines (IL-1β, TNF-α) released by keratocytes sensitize corneal nociceptors. AI-based ocular-surface thermography and optical flow analysis can quantify inflammation-induced microvascular dilation and correlate pain intensity with disease activity.[34]
10. Systemic Correlation and Future Directions
Although primarily ocular, disseminated Pythium infection has been reported in immunocompromised hosts, particularly involving the skin or arteries. Understanding the pathophysiology of ocular disease helps identify systemic manifestations earlier.
Future research integrating AI-based 4D modeling of stromal degradation with real-time confocal video analytics could revolutionize early detection and risk prediction, offering dynamic insights into pathogen–host interactions.
In summary, the pathophysiology of Pythium insidiosum keratitis is characterized by rapid stromal destruction driven by enzymatic virulence and immune dysregulation, compounded by antifungal resistance due to its unique oomycete cell wall composition. Artificial intelligence provides unprecedented tools for visualizing, quantifying, and predicting these microscopic processes, bridging the gap between bench-level microbiology and real-time clinical decision support. By combining deep-learning image analytics, molecular modeling, and predictive algorithms, AI is transforming Pythium keratitis from a diagnostic challenge into a model of data-driven ocular pathology.[15]
Table. Comparison of Structural and Functional Pathophysiology: Pythium vs Fungal Keratitis
|
Feature |
Pythium Keratitis |
Fungal Keratitis |
Diagnostic Relevance |
|
Cell wall |
Cellulose |
Chitin |
Mechanism for antifungal resistance |
|
Infiltrate margins |
Tentacle-like |
Feathery |
AI classification |
|
Inflammation |
Neutrophilic |
Mixed granulomatous |
AI differentiation |
|
Progression |
Rapid (days) |
Slower (weeks) |
Prognostic modeling |
Histopathology
Histopathological evaluation remains the cornerstone for confirming Pythium insidiosum keratitis (PIK), particularly when culture or PCR results are inconclusive (see Image. Schematic diagram depicting histopathology of Pythium insidiosum keratitis). The microscopic features of Pythium infection closely mimic those of filamentous fungal keratitis, but subtle morphological and staining differences—especially when interpreted through digital or AI-assisted microscopy—enable accurate distinction.
Gross and Microscopic Morphology
The corneal tissue involved in PIK shows dense stromal infiltration, necrosis, and loss of normal lamellar architecture. The hallmark finding is the presence of broad, ribbon-like, sparsely septate hyphae (width: 3–10 µm) that infiltrate throughout the corneal stroma and sometimes extend up to the Descemet membrane or anterior chamber angle (see Image. Schematic diagram depicting histopathology of Pythium insidiosum keratitis). These hyphae are poorly refractile, with irregular branching at right or obtuse angles—unlike the regular dichotomous branching seen in Aspergillus or Fusarium infections. The organism typically demonstrates a paucity of septa, though occasional pseudo-septa may appear due to degenerative changes.[2]
The inflammatory response is predominantly neutrophilic, with scattered necrotic keratocytes and fibrin deposition. Epithelial ulceration, stromal edema, and microabscess formation are frequent. The absence of granulomatous inflammation, a common feature in fungal infections, is diagnostically relevant. In chronic stages, fibrovascular proliferation and stromal scarring may be seen around degenerated hyphal remnants.
Staining Characteristics
Routine hematoxylin and eosin (H&E) staining shows Pythium filaments as pale, eosinophilic, poorly staining hyphae, often surrounded by neutrophilic debris.
- Periodic acid–Schiff (PAS): Weak or variable staining due to cellulose-based walls lacking chitin.
- Gomori methenamine silver (GMS): Stains filaments faintly gray to black, but less intensely than true fungi.
- Calcofluor white: Fluorescent staining highlights the cellulose-rich walls, producing a linear “ribbon” pattern under UV microscopy.
- Gram stain: Variable positive reaction; Gram-negative in degenerative phases.
Digital histopathology employing AI-based segmentation can now quantify staining intensity and filament morphology, reducing observer bias. Automated algorithms using convolutional neural networks (CNNs) classify hyphal structures and stain uptake, achieving over 93% accuracy in differentiating Pythium from fungal elements.[15]
Tissue Localization and Spread
Hyphal elements are usually concentrated in the mid to deep stroma, often clustering along collagen lamellae. In advanced cases, they penetrate the Descemet membrane, invade the endothelium, and may enter the anterior chamber, forming exudative plaques or hypopyon. Perineural invasion is rare, distinguishing PIK from Acanthamoeba keratitis. Endothelial involvement correlates with poor prognosis and early need for keratoplasty.
AI-driven image analysis of whole-slide scans can measure hyphal density, invasion depth, and inflammatory zone thickness, providing objective metrics for prognostic stratification. Deep-learning models trained on annotated histopathology slides can automatically map these features and calculate a “pathogen burden index” that correlates strongly with clinical severity.[35]
Immunohistochemistry (IHC) and Molecular Correlation
IHC enhances diagnostic specificity when traditional stains are inconclusive. Antibodies raised against Pythium insidiosum cell-wall components—particularly cellulose synthase (PiCS) and β-glucan epitopes—show strong cytoplasmic reactivity.
Lectin-based assays (eg, concanavalin A binding) differentiate Pythium from fungal hyphae by identifying mannose-deficient cell wall components.
Complementary PCR amplification of internal transcribed spacer (ITS) and cytochrome oxidase II (COX2) gene fragments from histologic sections confirms identity, especially when culture fails. Histology–molecular correlation remains the gold standard for diagnosis, with a reported concordance of 90% to 95%.
AI-assisted IHC interpretation, through pixel-level pattern recognition, reduces interobserver variability in immunoreactive area quantification. Emerging models also use spectral imaging AI to detect Pythium-specific chromogenic signatures that are invisible to the human eye, thereby enabling earlier histopathologic alerts within digital workflows.[36]
Comparison with Fungal Keratitis
The distinction between Pythium and true fungi is subtle but critical, as it directly dictates therapeutic choice. AI-based differential diagnosis tools using digital histopathology (ResNet50, EfficientNet) can distinguish these categories by extracting morphometric features, reducing misclassification and improving early therapeutic decision-making.
Table. Histopathologic Differentiation Between Pythium and Fungal Keratitis*
|
Feature |
Pythium insidiosum |
Fungal (Keratomycosis) |
Diagnostic Utility |
|
Hyphal width |
Broad (3–10 µm), ribbon-like |
Narrow (2–5 µm), tubular |
Shape identification by AI |
|
Septation |
Sparse or absent |
Frequent, regular |
Key morphologic cue |
|
Branching |
Irregular, right angles |
Acute-angle dichotomous |
Supports differentiation from filamentous fungi |
|
PAS/GMS staining |
Weak, faint gray-black |
Strong, dark black |
Confirms organism type |
|
Wall composition |
Cellulose + β-glucan |
Chitin + ergosterol |
Drug target difference |
|
Inflammation |
Neutrophilic, non-granulomatous |
Mixed granulomatous |
Helps pattern classification |
|
Response to antifungal |
Poor |
Favorable |
Key clinical distinction |
*AI performance metrics vary by dataset and architecture; convolutional neural network (CNN)–based models have reported classification accuracies of approximately 92%–95% in differentiating Pythium from fungal keratitis in pilot studies.
Role of Confocal and Digital Pathology
In vivo confocal microscopy (IVCM) complements histopathology by providing real-time, noninvasive visualization of Pythium filaments. Characteristic IVCM findings include:
- Linear, hyperreflective strands with right-angled branches
- Reticular “net-like” stromal pattern
- Peripheral radial extensions mimicking “tentacles”
Deep-learning–assisted IVCM interpretation using CNN-based models enables automatic segmentation and hyphal density scoring, which correlate with histologic findings. Combined AI pipelines linking IVCM and histopathology datasets can thus create comprehensive diagnostic frameworks, shortening time-to-diagnosis from days to hours.[37]
Post-Keratoplasty Histopathologic Changes
In post-therapeutic keratoplasty specimens, Pythium hyphae are often localized at graft-host junctions, occasionally extending into scleral tissue. Fibrovascular proliferation, residual inflammatory infiltrate, and stromal remodeling are typical. AI-aided analysis of these sections helps differentiate active infection (vital hyphae with cytoplasmic granularity) from post-treatment scarring (degenerate or ghost hyphae), crucial for postoperative management and antimicrobial withdrawal decisions.[38]
AI and Digital Histopathology Workflow
The integration of AI into corneal histopathology has revolutionized the efficiency of interpretation.
- Segmentation algorithms automatically delineate corneal layers and quantify hyphal load.
- Classification models distinguish Pythium, fungal, and bacterial etiologies based on texture and morphology.
- Heatmap visualization highlights regions of diagnostic significance for pathologists.
- Cloud-based validation enables remote digital pathology review via teleophthalmology platforms.[39]
In summary, histopathology in Pythium insidiosum keratitis provides the most definitive morphological evidence of infection. The presence of broad, sparsely septate, cellulose-rich filaments, weak special staining, and neutrophilic infiltration differentiates it from fungal keratitis. With the advent of AI-assisted digital pathology, diagnostic precision has improved dramatically, allowing automated hyphae recognition, pattern quantification, and outcome prediction. The convergence of classical microscopy and computational pathology ensures that Pythium keratitis—once easily misdiagnosed—can now be identified with near–real-time accuracy, facilitating timely therapeutic interventions and improving visual outcomes.[2]
Toxicokinetics
Although “toxicokinetics” traditionally pertains to drug metabolism, its application in PIK underscores why antifungals fail and how AI models may predict therapeutic response. Because Pythium lacks ergosterol, polyenes (eg, amphotericin B) cannot bind effectively, and azoles (eg, voriconazole, itraconazole) fail to inhibit 14-α-demethylase. Computational pharmacokinetic modeling has revealed poor drug–organism affinity scores.
AI-assisted in-silico docking and pharmacovigilance systems can simulate molecular interactions, predict potential inhibitors (such as cellulose biosynthesis inhibitors [CBIs]), and estimate corneal penetration based on physicochemical parameters. Deep-learning regression models trained on ocular drug datasets can forecast intra-stromal drug concentration and toxicity risks, thereby guiding drug repurposing.[40]
Table. Comparative Drug Sensitivity and AI-Predicted Efficacy
|
Drug/Class |
Mechanism |
In-vitro Efficacy % |
AI-Predicted Binding Score (kcal/mol) |
Comment |
|
Amphotericin B |
Ergosterol binding |
<20% |
-2.1 |
Poor target affinity |
|
Voriconazole |
CYP51 inhibition |
0% |
-1.8 |
Inactive |
|
Linezolid + Azithromycin |
Protein synthesis block |
70%–80% |
-6.5 |
Synergistic |
|
Carpropamid (CBI) |
Cellulose synthase block |
>85% |
-7.2 |
Experimental, promising |
|
Oryzalin |
Microtubule inhibitor |
60% |
-6.0 |
Adjunctive option |
History and Physical
Patients with Pythium insidiosum keratitis (PIK) typically present with acute or subacute onset of pain, redness, watering, and progressive visual loss following exposure to contaminated or stagnant water, especially in agricultural or monsoon settings (see Image. Schematic diagram depicting clinical features of Pythium insidiosum keratitis). The disease is often misdiagnosed as fungal keratitis, leading to delayed or inappropriate antifungal therapy.
Key Historical Features
- History of exposure: Bathing, swimming, or working in rice fields, ponds, or muddy water
- Preceding trauma: Minor vegetative or soil-related corneal injury in approximately 70%–80% of cases
- Treatment delay: Often self-treated or treated with antifungals, worsening the prognosis
- Demographics:
- Most common in young to middle-aged males involved in agriculture
- Pediatric and elderly cases are less frequent but possible
- Duration:
- Symptoms develop within 3 to 5 days post-exposure and progress rapidly despite antifungal therapy.[41]
Common symptoms:
- Severe ocular pain disproportionate to lesion size
- Photophobia, foreign body sensation, and profuse lacrimation
- Diminished or blurred vision due to dense stromal infiltration
- Non-healing ulcer despite antifungal use—an immediate red flag for Pythium[42]
Physical Examination (Ocular Findings)
General appearance:
- Gray-white, dry-looking, reticular stromal infiltrate with ill-defined, feathery or tentacular extensions—a hallmark of Pythium keratitis
- Lesions typically located in the paracentral or peripheral cornea with surrounding guttering and minimal stromal edema[43]
Disease course on examination:
- Early stage: Small anterior stromal infiltrate with intact endothelium and no hypopyon
- Progressive stage: Mid-stromal spread with reticular/tentacular extensions and early hypopyon
- Advanced stage: Deep stromal melt, endothelial plaque, and limbal involvement; risk of perforation is high[44]
Characteristic clinical clues suggesting PIK:
- Non-resolving “fungal-looking” keratitis unresponsive to antifungals within 3 to 4 days
- Reticular infiltrate with tentacle-like radial extensions
- Dry, rough, elevated stromal lesion with minimal surrounding edema
- Absence of pigmentation (unlike dematiaceous fungi)
- Rapidly progressive ulcer despite antifungal therapy adherence[17]
Systemic findings:
- PIK is usually limited to ocular involvement, but severe ocular inflammation can cause secondary systemic symptoms such as headache or periocular pain
- Systemic dissemination is not seen in immunocompetent individuals.
Table. Characteristic Clinical Findings in Pythium insidiosum Keratitis
|
Feature |
Characteristic Finding |
|
Corneal epithelium |
Defect overlying the infiltrate; often dry and resistant to re-epithelialization |
|
Stroma |
Dense, gray, reticular (net-like) infiltrates with radial extensions and peripheral guttering |
|
Margins |
“Tentacle-like” projections—unique to Pythium |
|
Limbus |
May be approached or involved in advanced cases |
|
Endothelium |
Endothelial plaque in approximately 40%–50% of severe cases |
|
Anterior chamber |
Mild to moderate reaction; hypopyon in advanced disease |
|
Sclera |
Occasionally shows extension or necrosis in late stages |
|
Pain |
Severe and continuous; disproportionate to the size of the ulcer |
Evaluation
Evaluation of Pythium insidiosum keratitis (PIK) requires an integrated, multimodal approach that combines clinical imaging, microbiology, molecular assays, and AI-enabled analytics. PIK should be suspected in any rapidly worsening, antifungal-resistant keratitis in a patient with agricultural or aquatic exposure. Clinical hallmarks include a gray reticular infiltrate with tentacular margins, severe pain, endothelial plaque, and early limbal spread. Timely recognition at the bedside, reinforced by AI-assisted imaging and microbiologic confirmation, remains the cornerstone of sight-saving management.[45]
Conventional Methods
- Corneal scraping and smear: Detection of broad aseptate filaments on KOH, Gram, and calcofluor staining
- Culture: Slow growth on chocolate or blood agar within 5 to 7 days
- PCR/LAMP: Highly specific detection of Pythium DNA targets (ITS and COX2 genes)
- IVCM/AS-OCT: Visualization of hyperreflective stromal strands and tentacular extensions [46]
AI-Based Diagnostics
- Deep learning now provides rapid, reproducible classification directly from slit-lamp or confocal images.
- ResNet-50, DenseNet-121, and EfficientNet models have achieved AUC >0.95 in multiclass studies.
- Algorithmic workflow: image capture → pre-processing (normalization, ROI segmentation) → feature extraction → classification → output probability map [47]
Molecular and biosensor integration
Recent prototypes merge biosensors that detect Pythium antigens or cellulose derivatives with AI-based signal interpretation, enabling on-site point-of-care testing within 30 minutes.
Validation and regulatory guidelines
The Indian Council of Medical Research (ICMR) and the Thai Ophthalmic Society have endorsed multimodal evaluation strategies that emphasize AI-assisted triage for culture-negative keratitis. International AI guidelines (AAO AI Task Force, 2023) recommend explainable models and data transparency.[48]
Clinical Screening and Image Acquisition (input for AI and baseline care)
- Triage triggers suggesting PIK
- Rapidly progressive stromal infiltrate with dry, reticular, or "tentacular" margins
- Peripheral guttering/advancing edge
- Minimal endothelial plaque
- Feathery hyphal-like streaks but poor response to antifungals
- Exposure to paddy/wet soil/floodwater
- Monsoon season
- Standardized slit-lamp imaging protocol (vital for AI)
- Diffuse, focal, sclerotic scatter, and retro-illumination views; include scale bar and white balance
- At least 3 projections (central, nasal, temporal) and 1 anterior segment video, if possible
- Record ulcer size (H × V in mm), depth, hypopyon height, and peripheral extension
- For tele-triage or field work: smartphone + slit-lamp adaptor (≥12 MP), fixed 1:1 macro, no digital zoom
- In vivo confocal microscopy (IVCM), where available:
- Long, thin, branching aseptate filaments (3–7 μm)
- Right-angle branching patterns
- Segmental hyperreflective swellings (“string-of-beads” appearance)
- Deeper stromal sheet-like infiltrates
- Technical note: Save raw image stacks (TIFF format) for AI-based analysis [6]
Microbiology and Pathology
(Ground truth for AI labels and routine diagnosis)
Essential smears
(Bedside, within 30 min of scraping)
- 10% potassium oxide (KOH) ± calcofluor white: Broad, sparsely septate filaments
- Gram stain: Weakly gram-positive hyphae (useful for excluding bacterial infection)
- Iodine–potassium iodide plus 1% sulfuric acid (IKI–H2SO4): Highlights the cellulose-rich cell wall of Pythium [49]
- Giemsa stain: Adjunctive staining
Culture
(Minimum of two inoculation sites)
- Primary media: Blood agar (preferred), chocolate agar
- Supplementary media: Sabouraud dextrose agar (often negative); non-nutrient agar with grass leaf incubation for zoospore induction (diagnostic)
- Colony morphology: Flat, colorless colonies with a radiating growth pattern
- Microscopy: Identification of sporangia and motile zoospores
Molecular and rapid diagnostic tests
(Where available)
- PCR: Targeting ITS rDNA, with sequencing for species confirmation
- qPCR or LAMP: Rapid detection suitable for low-resource laboratory settings
- MALDI-TOF MS: Identification from culture isolates, where locally validated[50]
Histopathology
(Therapeutic penetrating keratoplasty or evisceration specimens)
- Hematoxylin and eosin (H&E): Broad, sparsely septate filaments within the stroma
- Gomori methenamine silver (GMS): Negative or weak staining
- Periodic acid–Schiff (PAS): Variable positivity
- Calcofluor white: Strong positivity
- Cell wall composition: Cellulose-rich walls
- Angioinvasion: Uncommon
These laboratory findings constitute the reference standard for training and validation of AI-based diagnostic systems.
Artificial Intelligence and Deep Learning Evaluation Pipeline
Data curation & labeling
- Data sources: Slit-lamp photos ± IVCM image stacks from microbiologically confirmed Pythium, fungal, bacterial, Acanthamoeba, and herpetic keratitis cases
- Label derivation: Reference labels assigned based on culture, PCR, and/or histopathology (not treatment response), with annotation of onset-to-image time and pretreatment status
- Dataset partitioning: Patient-level separation with inclusion of an external-site test set (eg, different hospital, geographic region, or season)
- Quality control: Exclusion of overexposed or blurred images, with retention of a distinct “ungradable” category[51]
Model architectures
- Classification models: ResNet, EfficientNet, Vision Transformer architectures for binary to multiclass classification tasks (eg, PIK vs fungal vs bacterial vs other keratitis)
- Segmentation models: U-Net or Mask R-CNN architectures for delineation of stromal infiltrates and tentacular extensions, enabling surrogate estimates of lesion area and depth
- Multimodal fusion: Integration of image-derived features with clinical metadata (eg, trauma history, water exposure, symptom duration) and IVCM features to enhance diagnostic sensitivity
Performance reporting
(Aligned with TRIPOD-AI and CONSORT-AI principles)
- Primary metrics: Sensitivity for PIK detection, area under the receiver operating characteristic curve (AUC), and F1 score
- Secondary metrics: Specificity against filamentous fungal keratitis, calibration (Brier score), and decision-curve analysis (net benefit at clinically relevant TPK referral thresholds, eg, ≥0.7 predicted probability)
- Robustness analyses: Subgroup performance by camera type, clinical center, ulcer size, and pretreatment status[52]
Human–AI clinical workflow
- Image acquisition: Capture standardized slit-lamp images and process them through on-device or server-based AI models
- Triage output interpretation:
- High probability PIK (≥0.7): Urgent microbiologic evaluation and IVCM; initiation of anti-oomycete therapy (avoiding azoles); early TPK consultation
- Intermediate probability (0.40–0.69): Repeat imaging; expanded laboratory testing (eg, grass leaf incubation); consideration of qPCR
- Low probability (<0.40): Management according to standard microbial keratitis pathways, without deferral of smear or culture
- Explainability: Visualization using gradient-weighted class activation mapping (Grad-CAM) or heatmaps highlighting reticular margins and tentacular extensions, archived with the diagnostic report[53]
Deployment and safety checks
- Edge deployment: Progressive web applications or Android-based platforms supporting offline inference and automated deidentification
- Model governance: Locked model versions, audit logging, and scheduled recalibration to account for seasonal or epidemiologic drift
- Human oversight: Mandatory clinician review, with AI outputs functioning as adjunctive decision support rather than replacements for microbiologic diagnosis
Minimum diagnostic dataset at first clinical encounter
- Slit-lamp photography (≥3 standardized views), ulcer dimensions, and hypopyon height
- Corneal scrapings for KOH with calcofluor white, Gram stain, and IKI–H2SO4
- Culture on blood agar with adjunctive grass leaf incubation
- IVCM, where available
- qPCR or LAMP, where accessible
- AI-based image triage (if available), with probability estimates and corresponding heatmaps[52]
Criterion for escalation and early therapeutic keratoplasty (TPK)
- AI-predicted PIK probability ≥0.7 or classic morphologic features with poor or absent response to antifungal therapy within 48–72 hours
- Rapid peripheral progression, involvement of more than two limbal quadrants, deep stromal sheet-like infiltrates on IVCM, or impending/perforated cornea
- Coordination with microbiology services for culture of the excised corneal button (critical for reference labeling and future AI training)
Documentation & reporting standards for AI-enabled clinics
- Inclusion of AI-derived probability scores, model version identifiers, and heatmaps in the clinical record
- Documentation of time from presentation to definitive laboratory confirmation as a quality assurance metric
- Flagging and periodic review of AI–laboratory discordance to inform active learning datasets[54]
Quality, safety, and regulatory considerations
- Established clinical guidelines for microbial keratitis remain foundational (institutional, AIOS, or RCOphth pathways), including prompt smear and culture acquisition, avoidance of exclusive antifungal therapy in suspected PIK, and early consideration of TPK when progression occurs despite optimized treatment
- AI development and deployment should adhere to recognized frameworks, including:
- TRIPOD-AI for model reporting and CONSORT-AI/SPIRIT-AI for clinical trials
- Software as a medical device (SaMD) principles from the IMDRF and FDA; alignment with CDSCO digital health guidance and institutional review board approval in India
- WHO's ethical guidance for AI, including transparency, data minimization, bias monitoring, and human oversight
- Data governance: Explicit imaging consent, rigorous deidentification, site-level data-sharing agreements, and periodic bias audits (eg, rural vs urban settings, device types, seasonal variation)[55]
Suggested diagnostic evaluation algorithm (textual)
Suspect PIK → standardized imaging → smear panel (KOH, Gram, IKI-H2SO4) and cultures (blood agar ± grass leaf incubation) ± IVCM → AI-based image analysis
- High-probability or classic morphology: Anti-oomycete pathway, early TPK consultation, qPCR/LAMP
- Indeterminate: → repeat imaging, broaden labs, consider referral.
- Low probability with persistent clinical concern: Management per microbial keratitis protocols without delaying laboratory evaluation; reassessment at 24–48 hours
Recommended reporting elements
- Imaging dataset and views
- AI probability scores and heatmaps
- Smear, culture, and molecular results
- IVCM descriptors
- Clinical decision-making rationale, including TPK referral
- Follow-up plan [56]
Table. AI and Imaging Correlates (Modern Diagnostic Support)
|
Modality |
Findings |
|
In vivo confocal microscopy (IVCM) |
Multiple, slender, aseptate, hyperreflective filaments with right-angle branching in the stroma |
|
AI-assisted slit-lamp imaging |
Deep-learning models highlight reticular/tentacular infiltrates with Pythium probability ≥0.7 within seconds |
|
Anterior segment OCT (AS-OCT) |
Reveals hyperreflective stromal sheets, loss of lamellar organization, and potential descemetocele formation |
Table. Distinguishing Features of Pythium insidiosum Keratitis and Fungal Keratitis
|
Parameter |
Pythium Keratitis |
Fungal Keratitis |
|
Lesion texture |
Dry, rough, reticular, tentacular |
Feathery, fluffy, soft margins |
|
Response to antifungals |
Poor / none |
Usually good |
|
Stain characteristics |
Aseptate filaments, cellulosic wall |
Septate hyphae, chitin wall |
|
Culture |
Grows on blood agar |
Grows on Sabouraud dextrose agar |
|
Hypopyon |
Mild–moderate |
Often marked |
|
Clinical course |
Rapid, destructive |
Relatively slower |
Treatment / Management
Pythium insidiosum keratitis (PIK) requires an urgent, multidisciplinary approach that differs fundamentally from that for fungal keratitis. Because Pythium is an oomycete and not a fungus, conventional antifungal drugs are ineffective. Optimal management integrates early anti-oomycete antibiotic therapy, timely surgical intervention, and close postoperative surveillance guided by both clinical staging (Gurnani–Kaur) and AI-assisted diagnostic inputs.[57]
Principles of Management
- Avoid antifungal monotherapy: Pythium lacks ergosterol and chitin, rendering antifungals (eg, natamycin, voriconazole, amphotericin B) ineffective.
- Initiate anti-oomycete therapy early: High-frequency combination therapy with linezolid and azithromycin is recommended.
- Avoid corticosteroids during the active phase: Corticosteroids may accelerate stromal destruction and increase the risk of recurrence.
- Reassess clinical response at 48–72 hours: Progression or lack of improvement warrants early therapeutic penetrating keratoplasty (TPK).
- Ensure wide surgical excision margins: Margins of ≥1–1.5 mm reduce the risk of recurrence.
- Incorporate AI-based image tracking when available: Serial analysis may assist in monitoring treatment response and predicting progression.[58]
Medical Management
Table. First-line Topical Regimen (Anti-Oomycete Protocol) for Pythium Keratitis
|
Drug |
Concentration |
Dosage (Acute Phase) |
Tapering / Maintenance |
Notes |
|
Linezolid |
0.2% eye drops |
1 drop every 1–2 hours while awake |
Gradual taper every 3–5 days after clinical improvement |
Bacteriostatic antibiotic; effective against Pythium cell-wall synthesis (targets 50S ribosomal subunit) |
|
Azithromycin |
1% eye drops |
1 drop every 1–2 hours while awake |
Taper to 4–6 times/day after 2 weeks |
Macrolide with anti-oomycete activity; synergistic with linezolid |
|
Cycloplegic (Atropine 1%) |
— |
Twice daily |
Maintain until pain subsides |
Prevents synechiae and improves comfort |
|
Preservative-free lubricant |
— |
Every 2-3 hours |
As needed |
Protects the ocular surface |
Table. Systemic Therapy (Adjunctive) for Pythium Keratitis
|
Drug |
Dose |
Duration |
Purpose / Precaution |
|
Oral Linezolid |
600 mg BID |
7–14 days |
Use in deep or limbal disease; monitor CBC weekly for myelosuppression |
|
Oral Azithromycin |
500 mg OD |
5–7 days |
Reduces systemic load; prolongs tissue antibiotic levels |
|
Doxycycline (optional) |
100 mg BID |
1–2 weeks |
Anti-collagenase effect; may help reduce stromal melt |
Response Evaluation (48–72 hours):
- Reduction in stromal infiltrate size or density
- Absence of new tentacular extension
- Improvement in pain, conjunctival hyperemia, and hypopyon
- Lack of improvement or evidence of progression warrants escalation to surgical management.[59] (B3)
Surgical Management
Indications for therapeutic penetrating keratoplasty (TPK)
- Infiltrate >6 mm, >2 quadrants, or approaching limbus
- Deep stromal or endothelial involvement (on slit-lamp/IVCM)
- Hypopyon >1 mm or descemetocele formation
- No clinical improvement within 48–72 hours of optimized therapy
- Impending or actual perforation[60] (B3)
Table. Surgical Principles for the Management of Pythium Keratitis
|
Step |
Description |
|
Pre-op preparation |
Continue topical linezolid + azithromycin; avoid antifungals; counsel for possible repeat graft. |
|
Trephination |
1–1.5 mm clear margin beyond visible infiltration |
|
Donor graft size |
0.5–1.0 mm larger than the recipient bed |
|
Excision |
Remove all infiltrated tissue completely; include superficial scleral excision if needed. |
|
Intraoperative care |
Irrigate anterior chamber with antibiotic solution; minimize intraocular manipulation. |
|
Postoperative antibiotics |
Restart hourly linezolid + azithromycin; delay steroids until confirmed quiescence (usually after 2–3 weeks). |
Post-TPK follow-up
- Daily slit-lamp examination for 1 week, then every 2–3 days for one month.
- Assess for recurrence at the graft–host junction, which typically appears as a gray line or infiltrate within 2 to 3 weeks.
- In the event of recurrence, repeat TPK with a larger excision and extended margins.
- Introduce low-potency topical steroids only after confirmed infection control.[38]
Table. Role of Artificial Intelligence (AI) and Deep Learning in Management of Pythium Keratitis
|
AI Utility |
Clinical Application |
|
Automated image classification |
Differentiates Pythium from fungal keratitis with >90% accuracy using slit-lamp or smartphone images |
|
Quantitative monitoring |
Tracks infiltrate area and depth daily; flags progression >10–15% for early surgical referral |
|
Teleophthalmology triage |
Enables early detection in rural/remote regions and referral to corneal centers |
|
Recurrence prediction |
Detects early edge infiltrates post-TPK before clinical visibility |
|
Decision support |
Suggests stage-specific management based on Gurnani-Kaur classification |
Table. Gurnani-Kaur Stage-Linked Management Protocol in Pythium Keratitis
|
Stage |
Management Plan |
Expected Outcome |
|
Stage I (Localized) |
Intensive topical linezolid + azithromycin; no steroids |
80–90% medical cure |
|
Stage II (Progressive Stromal) |
Continue antibiotics + oral linezolid/azithromycin; close monitoring |
60–70% salvage with medical therapy |
|
Stage III (Deep/Limbal) |
Early TPK (large margin) + postoperative antibiotics |
60% anatomical salvage |
|
Stage IV (Perforated/Scleral) |
Salvage TPK or evisceration |
Poor; high recurrence risk |
|
Stage V (Post-TPK Recurrence) |
Repeat large-diameter TPK |
Variable; depends on margin clearance |
National and International Guideline Perspectives
Indian and Asian experience
- First-line therapy: Combination therapy with linezolid and azithromycin is recommended.
- Surgical timing: Early therapeutic penetrating keratoplasty (TPK) is advised when lesion size exceeds 6 mm or involves more than two limbal quadrants.
- Antifungal therapy: Antifungal-only regimens should be avoided.
- Diagnostic confirmation: Grass leaf incubation and PCR are recommended for definitive diagnosis.
- Regional validation: Case series from Thailand and Australia support similar management strategies, with improved outcomes associated with early intervention.
Global perspectives
- Guideline status: No formal World Health Organization guideline currently exists; however, regional evidence supports antibacterial-based therapy combined with wide-margin surgical excision as the prevailing standard of care.
- Emerging tools: Integration of AI for rapid triage and recurrence monitoring remains under active evaluation.[61]
Table. Prognostic Indicators During Treatment for Pythium Keratitis
|
Favorable Signs |
Unfavorable Signs |
|
Pain relief within 72 hours |
Persistent or increased pain |
|
Reduction in infiltrate size |
Expansion of the gray reticular pattern |
|
Absence of new tentacles |
Limbal approach or scleral spread |
|
Epithelial healing |
Persistent epithelial defect |
|
Negative culture after therapy |
Positive smear or culture post-TPK |
Differential Diagnosis
Pythium insidiosum keratitis (PIK) presents as a rapidly progressive, necrotizing corneal ulcer often indistinguishable from fungal keratitis on slit-lamp examination (see Image. Schematic diagram depicting the differential diagnosis of Pythium insidiosum keratitis). Accurate differentiation is essential, as conventional antifungal therapy is ineffective against Pythium insidiosum. Artificial intelligence (AI) and deep learning (DL) models can enhance diagnostic precision by distinguishing PIK from morphologically similar conditions through multimodal image analysis (eg, slit-lamp, IVCM, confocal, or OCT). The sections that follow summarize the key clinical entities that most closely mimic PIK and highlight distinguishing features critical to accurate diagnosis.
1. Fungal Keratitis (Filamentous Mycoses)
Pathogens: Fusarium, Aspergillus, Curvularia, Alternaria, etc Similarity: Feathery-edged stromal infiltrate, satellite lesions, and hypopyon resembling Pythium Distinguishing features:
- Fungal hyphae: Regularly septate, branching at acute angles (45°)
- Pythium hyphae: Sparsely septate or aseptate, broad (3–7 µm), right-angle branching
- Gomori methenamine silver (GMS): Positive staining in fungi; weak or negative GMS in Pythium
- Artificial intelligence (AI) utility: Deep CNN classifiers trained on slit-lamp images show >90% AUC in distinguishing Pythium vs Fusarium; heatmap localization (Grad-CAM) highlights broader, reticular “tentacle-like” edges in Pythium.[9]
2. Bacterial Keratitis
Pathogens: Pseudomonas aeruginosa, Staphylococcus aureus, Streptococcus pneumoniae Similarity: Dense stromal infiltrate with epithelial defect and hypopyon Distinguishing features:
- Rapid onset (24–48 h), mucopurulent discharge, marked pain, and systemic response
- Pythium ulcers are usually slower (days), have a dry surface, and lack a mucopurulent reaction.
- Confocal: Bacteria are invisible; Pythium shows linear, branching filaments.
- AI utility: CNNs can achieve >95% accuracy in distinguishing between bacterial and Pythium using texture features (surface irregularity, dryness, and stromal reflectivity gradients).[62]
3. Acanthamoeba Keratitis
Similarity: Ring infiltrate, severe pain disproportionate to clinical signs, and confusion with early Pythium stages Distinguishing features:
- History of contact lens wear or water exposure
- Pain disproportionate to ulcer size
- IVCM: Double-walled cysts (highly reflective round structures) vs Pythium's linear branching filaments
- AI utility: Hybrid CNN + SVM models trained on IVCM images can distinguish Acanthamoeba cysts (spherical, highly reflective spots) from Pythium filaments (linear, non-septate strands).[63]
4. Herpetic (HSV) Keratitis
Similarity: Stromal infiltrates with ulceration and scarring may mimic late-stage PIK. Distinguishing features:
- Dendritic/geographic ulcers, decreased corneal sensation, and vesicular rash history
- Pythium lacks dendrites and has an irregular “reticular” infiltrate.
- IVCM: Inflammatory cells, but no filamentous elements in HSV
- AI utility: DL-based image segmentation can detect branching dendritic ulcers typical of HSV, reducing false positives for Pythium.[32]
5. Nocardia Keratitis
Similarity: Superficial, patchy infiltrate with satellite lesions. Distinguishing features:
- Nocardia: Characteristic “cracked glass” appearance with a raised surface; filamentous but thinner (1 µm), and weakly acid-fast on Ziehl–Neelsen
- Pythium: Poor acid-fast staining; grows readily on blood agar without branching aerial hyphae
- AI utility: Morphometric CNN features can detect Nocardia’s punctate surface texture vs Pythium’s tentacular spread.[64]
6. Mixed Microbial Keratitis
Combination: Fungal or bacterial co-infection with Pythium may occur, especially in tropical climates. Indicators:
- Mixed culture growth; inconsistent smear results
- Progressive ulcer despite combined therapy
- AI utility: Ensemble models that integrate clinical and microbiological metadata improve classification performance for mixed infections through pattern fusion.[4]
7. Noninfectious Keratitis (Sterile, Mooren’s, or Autoimmune Ulcers)
Similarity: Peripheral infiltrates and stromal melt. Distinguishing features:
- Minimal pain, non-progressive, immune origin
- Absence of microbial filaments, negative cultures
- AI utility: AI systems trained exclusively on infectious causes may misclassify sterile ulcers; algorithms should include “noninfectious” as a control class.[6]
8. Corneal Foreign Body/Trauma-Induced Necrosis
Similarity: Focal infiltrate with inflammation and necrosis. Distinguishing features:
- Clear mechanical entry point with visible metallic/vegetative debris
- Limited progression once the foreign body is removed
- AI utility: Object detection networks can localize metallic reflectivity or foreign-body shadows, thereby differentiating them from Pythium infiltrates.[65]
9. Fungal-like Oomycetes (eg, Lagenidium species)
Similarity: Morphologically similar filamentous pathogen causing keratitis or systemic infection Distinguishing features:
- Lagenidium is less commonly associated with the cornea, as confirmed by molecular sequencing (ITS)
- AI utility: AI-assisted decision trees using combined culture and image metadata can reduce misclassification.[66]
Table. Differential Diagnosis for Pythium Keratitis
|
Condition |
Key Differentiating Features |
AI/IVCM Diagnostic Aids |
|
Fungal Keratitis |
Septate hyphae, GMS+, feathery edges |
CNN differentiates filament morphology; AUC > 0.9 |
|
Bacterial Keratitis |
Mucopurulent discharge, rapid onset |
Texture-based CNN shows >95% specificity |
|
Acanthamoeba Keratitis |
Severe pain, ring infiltrate, cysts on IVCM |
IVCM-AI hybrid differentiates cysts vs filaments |
|
Herpetic Keratitis |
Dendritic ulcer, low corneal sensitivity |
Segmentation CNN detects dendrites |
|
Nocardia Keratitis |
Raised “cracked glass” lesion, acid-fast+ |
Surface topography modeling differentiates |
|
Sterile/Autoimmune Ulcer |
Minimal pain, non-progressive, no filaments |
AI false positives minimized by metadata input |
In summary, Pythium keratitis can mimic bacterial and fungal ulcers both clinically and morphologically. Integrating AI-based imaging analysis, molecular confirmation, and standardized confocal or slit-lamp imaging significantly improves the accuracy of differentiation. Proper differential diagnosis prevents the use of ineffective antifungal therapy and ensures early initiation of anti-oomycete agents or therapeutic keratoplasty (TPK), thereby improving visual prognosis.[67]
| Pause and Reflect | An AI-assisted risk stratification tool predicts poor response to medical therapy in a patient with suspected Pythium keratitis. Despite appropriate anti-oomycete treatment, there is no clinical improvement at 72 hours, and corneal thinning continues to progress. What is the most appropriate management decision based on AI-supported and clinical findings? |
Pertinent Studies and Ongoing Trials
High-quality randomized trials specific to Pythium keratitis are still limited. Most existing evidence comes from multiclass microbial-keratitis (MK) datasets in which Pythium is a prespecified class or a key subgroup. The following section synthesizes current evidence and ongoing investigations to contextualize the role of artificial intelligence as an adjunct to, rather than a replacement for, standard microbiologic diagnostics.
Table. Summary of Current Evidence Supporting the Use of AI in Pythium Keratitis
|
Evidence Category |
Study Design & Data Sources |
Clinically Relevant Findings |
Take-home for practice |
|
IVCM-based models |
Confocal image stacks labeled by experts vs lab confirmation |
Accurate separation of aseptate/broad, right-angle branching filaments (oomycete) from septate fungi; improved reader agreement |
Useful where IVCM is available to upgrade/downgrade suspicion after slit-lamp AI or equivocal smears |
|
Multimodal (photos + clinical metadata ± IVCM) |
Fusion networks adding exposure to paddy/water, monsoon season, and days of symptoms |
Calibration and net-benefit gains on decision-curve analysis at thresholds used for early TPK referral |
Moves from “image accuracy” to actionable triage (who should be fast-tracked for anti-oomycete pathway/TPK) |
|
External validation studies |
Training at one hospital with testing from another region, season, or camera |
Performance drop is modest with standardized capture; models remain clinically useful when quality control is enforced |
Confirms generalizability if clinics use the same 3–4 view protocol and avoid digital zoom |
|
Prospective service evaluations |
AI runs in parallel with routine care in the emergency and outpatient settings |
Shorter time-to-correct diagnosis, higher early TPK rates when appropriate, and reduced futile antifungal days |
Demonstrates workflow benefit even before RCT-level evidence |
Justification for Integration of AI with Clinical Safeguards
- Pythium is a time-critical disease that spreads peripherally; outcomes depend on early recognition and early TPK when indicated.
- While distinct Pythium morphologies exist, they are subtle and often missed early; AI improves sensitivity during triage.
- Net-benefit analyses show positive clinical utility at probability thresholds (eg, ≥0.7 for “treat/TPK-consult now”).
- Explainability (Grad-CAM) helps clinicians trust the outputs by focusing on tentacular margins and reticular sheets rather than artifacts.[68]
Ongoing and Planned Clinical Trials and Registries
- Multicenter, prospective trials are comparing AI-assisted triage with standard care in suspected MK during the monsoon and harvest seasons.
- Primary endpoints: Time from presentation to correct organism class identification (oomycete vs non-oomycete), time-to-TPK, and inappropriate antifungal days
- Secondary endpoints: Globe salvage, best-corrected VA at 3 months, repeat-TPK rates, perforation, and cost-effectiveness
- IVCM-plus studies: Prospective accuracy studies of confocal-AI for oomycete vs filamentous fungi, with masked expert adjudication
- Tele-ophthalmology deployments (district hospitals/rural camps): On-device/PWA models for first-line triage; outcomes of interest include referral yield for probable Pythium, diagnostic turnaround time, and feasibility on mixed smartphones
- Federated-learning consortia (India/SE Asia/Australia): Site-held training to improve generalization without data leaving hospitals; outcomes are site-wise AUC and fairness across cameras and seasons
- Health-economics evaluations: Decision-analytic models using prospective service data to quantify cost per TPK averted, cost per globe saved, and opportunity costs of delayed diagnosis [69]
Recommendations for Comprehensive Evidence Reporting in AI-Enabled Programs
- Model and version; image protocol adherence (3–4 views, no digital zoom)
- Operating point used (eg, 0.70 probability = “High-probability Pythium”)
- Prospective metrics: sensitivity/specificity for Pythium, calibration (Brier), time-to-correct therapy, and net benefit
- Safety checks: proportion overridden by clinician; discrepancy audits; quarterly drift review (season/camera)
- Equity: performance by capture device, center type, and sex/age [1]
Practical Recommendations for Clinical Integration
- Implement AI evaluation at first contact (slit-lamp photos) with a conservative, high-sensitivity threshold to trigger urgent smears, cultures, IVCM, and early TPK consult.
- Always obtain relevant laboratory studies, including KOH + CFW, Gram, IKI-H2SO4, and culture with leaf incubation, in addition to qPCR/LAMP if available; use AI for triage and decision support.
- Document AI probability and heatmap with final microbiology to continuously build local evidence and comulticenter multicenter registries.[66]
Treatment Planning
1) Immediate Steps at Diagnosis or Strong Clinical Suspicion
- Do not start azoles/amphotericin as sole therapy. Oomycetes respond poorly to classic antifungals.
- Run full microbiology (KOH/CFW, Gram, IKI-H2SO4), cultures (blood agar ± leaf-incubation), ± qPCR/LAMP; add IVCM if available.
- If AI or clinical morphology suggests PIK, escalate early to an anti-oomycete protocol and alert the corneal surgeon for potential early TPK.[70]
2) Medical Therapy
First-line where globe is salvageable, and there are no indications of imminent perforation
Topical antibacterials (oomycete-active):
- Linezolid 0.2% every 1 to 2 hours while awake, then taper by half each week as clinically improving
- Azithromycin 1% every 1 to 2 hours while awake, then taper similarly
- Consider oral azithromycin 500 mg once daily for 3 to 5 days (or per local protocol) and/or oral linezolid for severe or deep stromal disease. Evidence favors combination therapy over monotherapy.[71]
Adjuncts:
- Cycloplegic (eg, atropine 1% bid) for pain/uveitis
- Anticollagenase support (eg, doxycycline 100 mg bid) as per clinician preference
- Avoid topical steroids until unequivocal control; if used post-TPK, introduce very cautiously with close monitoring.
Response assessment (24–72 h):
- Reduction in pain, epithelial defect, infiltrate density/edge activity, hypopyon; serial photos.
- Failure criteria (any): advancing tentacular edge, limbal approach, descemetocele/imminent perforation → proceed to surgical plan[72]
3) Indications for Early Therapeutic Penetrating Keratoplasty (TPK)
Early surgery improves anatomic outcomes and can prevent scleral spread.
- Rapid peripheral spread
- Involvement of more than 2 quadrants or limbal extension
- Deep stromal sheets on IVCM
- Non-response within 48 to 72 hours
- Impending/perforated cornea.
4) Surgical Planning (TPK)
Preoperative
- Continue linezolid/azithromycin up to surgery.
- Obtain informed consent regarding the risk of recurrence and the possibility of repeat TPK.
- Plan a large, full-thickness graft to encompass all active margins.
Intraoperative principles
- Trephination margin: Plan host trephination 1–1.5 mm beyond visible disease, extending further if margins appear gelatinous or actively progressing.
- Donor graft sizing: Use a donor button 0.5–1.0 mm larger than the host bed to ensure adequate coverage.
- Host bed preparation: Irrigate the host bed and meticulously excise all infiltrated tissue. Send the excised corneal button for smear, culture, and histopathologic examination to establish definitive laboratory confirmation and provide reference-standard labels for future validation of AI-assisted diagnostic systems.
- Anterior chamber management: Remove fibrin and inflammatory debris as needed, use viscoelastic to maintain chamber stability, and secure the graft with interrupted or combined suturing to minimize wound leak.
- Assessment of scleral involvement: Evaluate for extension beyond the cornea and extend debridement as appropriate.
- Adjunctive medications: Intracameral or intrastromal drug therapy is not well established for PIK; prioritize complete excision of infected tissue.[73]
Evidence & outcomes
- Modern series show good anatomic salvage with early TPK; recurrence is possible and may require repeat, larger grafts.
Postoperative regimen
- Topical linezolid 0.2% + azithromycin 1% every 2 to 3 hours for the first week, then taper to 4 times daily over 4 to 6 weeks as it improves.
- Judicious steroid use may be introduced only after clear evidence of quiescence (no tentacular edge and negative surface cultures), balancing graft survival against recurrence risk.
- Close postoperative monitoring: Daily follow-up initially, with a low threshold for repeat scraping if recurrent infiltrate develops at the graft–host junction, as marginal recurrence is common and may require repeat TPK.[2]
5) Integration of AI-Assisted Workflow (where available)
- Use AI probability (eg, ≥0.7 for “high-prob PIK”) to trigger urgent lab confirmation and early surgeon involvement—shortens time to correct therapy and avoids futile antifungal exposure.
- Store AI heatmaps + probability in the chart; reconcile with final microbiology for QA and model calibration.
6) Disposition & Follow-Up
- Daily monitoring until clear improvement, then every 2 to 3 days.
- Educate patients on warning signs: increased pain, expansion of the gray reticular edge, new hypopyon, or wound leak.
- After epithelialization, proceed with suture management and optical rehab as appropriate; consider lamellar/optical keratoplasty later if stable.
7) Special Situations
- Mixed infection: If bacteria/fungi are also isolated, treat concomitantly while maintaining Pythium-active coverage.
- Resource-limited settings: If compounding 0.2% linezolid/1% azithromycin is difficult, liaise with regional centers; prioritize early referral for TPK.
8) Key Evidence
- Antibacterial therapy: Recent reviews recommend linezolid combined with azithromycin as first-line treatment, with the combination demonstrating greater efficacy than monotherapy.
- Adjunctive systemic therapy: Case series incorporating topical therapy with oral linezolid report cure rates exceeding 80% in selected cases.
- Role of early surgery: Early TPK is associated with high rates of anatomic globe salvage; recurrence may necessitate larger repeat grafts.
- Evolution in management strategy: Contemporary reviews emphasize a conceptual shift toward antibacterial-based regimens combined with wide-margin surgical excision.[74]
Toxicity and Adverse Effect Management
Although artificial intelligence (AI) and deep learning (DL) are diagnostic adjuncts rather than pharmacologic or radiologic interventions, “toxicity” in this context refers to algorithmic, operational, and clinical risks associated with AI use. Adverse effects may arise from model errors, data bias, over-reliance, or workflow misintegration, potentially leading to misdiagnosis, delayed treatment, or ethical breaches. Therefore, toxicity management in AI-assisted Pythium diagnosis focuses on risk mitigation, human oversight, and system calibration.[75]
Table. Algorithmic and Diagnostic Risk of AI-Assisted Pythium Diagnosis
|
Source of Risk |
Potential Adverse Effect |
Mitigation / Management Strategy |
|
False Negatives (missed Pythium) |
Delayed initiation of linezolid/azithromycin therapy, late TPK, globe loss |
Always confirm AI results with smear/culture/qPCR; use a low decision threshold (≥0.7 sensitivity bias); retrain with difficult cases. |
|
False Positives |
Unnecessary surgical intervention or antibacterial therapy |
Require human review by a cornea specialist; correlate with clinical morphology and laboratory studies. |
|
Data Bias / Overfitting |
Misclassification in underrepresented geographies or devices |
Implement continuous model retraining using federated datasets (India, Thailand, Australia). |
|
Image Quality Variability |
AI misinterpretation due to poor lighting or smartphone blur |
Enforce image-capture protocols (≥3 angles, 1:1 macro, no digital zoom). |
|
Confounding Coinfections |
Overconfidence in a single-organism label |
Design multiclass models with “mixed” and “uncertain” output categories. |
|
Post-Surgical Cases (TPK buttons) |
AI not trained on grafted corneas |
Exclude post-TPK images from inference dataset; clearly flag as “out of distribution.” |
Human–Machine Interaction Hazards
- Automation bias: Clinicians may over-trust AI output and skip confirmatory tests.
- Mandate dual verification (AI + microbiology) and document reasoning if following AI alone.
- Alert fatigue: Excessive probability alerts can desensitize users.
- Configure tiered alerts (eg, high-probability >0.7 = red; moderate 0.4–0.69 = amber).
- Misinterpretation of heatmaps: Grad-CAM visualizations may be misunderstood as “proof.”
- Provide educational overlay and disclaimers such as “Regions indicate algorithm attention, not confirmed pathology.”[69]
Table. Data and Privacy Risks with AI-Assisted Pythium Diagnosis
|
Risk |
Potential Harm |
Preventive Measures |
|
Patient Data Leakage |
Breach of confidentiality |
End-to-end encryption, de-identification before cloud upload, anonymized filenames |
|
Unapproved Data Reuse |
Ethical/legal violations |
Institutional Review Board (IRB) approval, consent for AI analysis, adherence to GDPR/ICMR norms |
|
Dataset Drift |
Outdated models misclassify newer camera types |
Quarterly revalidation and recalibration of models |
Hardware/Software-Related Risks
- Edge-device failures: Crashes or misalignment during slit-lamp capture lead to data loss or blurred images.
- Implement auto-retry capture, local caching, and quality-score rejection.
- Latency in rural networks: Delays in remote inference lead to delayed triage.
- Use on-device PWA models with offline inference and later synchronization.
- Color imbalance between cameras: Alters AI confidence.
- Standardize white-balance settings; apply device-specific calibration filters.
Clinical Workflow Considerations
- Delayed escalation: If AI returns low probability (<0.4) despite classical clinical features, clinicians may delay TPK.
- Implement a “clinical override clause” in which human judgment supersedes AI output.
- Inconsistent reporting: Missing documentation of AI version/probability may hinder traceability.
- Include AI probability, model version, and timestamp in the patient record.
- Liability ambiguity: Misdiagnosis from an AI suggestion.
- Define shared responsibility so that AI is clearly an assistive tool and physicians are the final decision-makers.[76]
Table. Post-Deployment Risk Monitoring for AI-Assisted Pythium Diagnosis
|
Monitoring Metric |
Frequency |
Corrective Action |
|
Sensitivity drift (<85%) |
Quarterly audit |
Retrain the model with new data |
|
High discordance (>10% AI vs lab) |
Monthly review |
Root-cause analysis (image quality, labeling error) |
|
Bias audit (rural vs urban cameras) |
Semiannual |
Weighting or data augmentation |
|
User feedback reports |
Continuous |
Software patch, UI improvement |
Ethical and Psychological Toxicities
- Patient anxiety: Misunderstanding “AI detected Pythium” as a definitive diagnosis may create emotional distress.
- Use clear communication scripts: “AI suggests possibility; confirmation pending lab tests.”
- Clinician deskilling: Overreliance on AI pattern recognition.
- Integrate periodic manual skill assessments and continuing medical education (CME) workshops for corneal image interpretation.
- Equity concerns: Rural/low-resource sites lacking access to AI may lag in early diagnosis.
- Encourage lightweight, open-source models and publicly shared datasets.[77]
Overall Toxicity Management Framework
Detection → Reporting → Correction → Prevention
- Detection: Identify misclassification or workflow errors (flagged by the user or an audit).
- Reporting: Log event in centralized AI-incident registry with anonymized case details.
- Correction: Retrain model on misclassified cases, update thresholds, or fix capture protocol.
- Prevention: Continuous education, bias audits, and transparent documentation.[78]
Future Safety Directions
- Explainable AI (XAI) dashboards: Show confidence intervals and rationale.
- Federated monitoring: Share real-time safety metrics across centers.
- Integration with the electronic health record (EHR): Automatically prompt microbiology confirmation orders when AI flags probable Pythium.
- Regulatory pathways: Adhere to WHO AI Ethics 2021, CDSCO (India), and FDA (US) Software as a Medical Device (SaMD) guidance for ophthalmic AI.
Summary
The concept of "toxicity" in the context of AI-assisted Pythium diagnosis is non-biological but high-impact, encompassing diagnostic, operational, and ethical domains. Safe implementation demands a human-in-the-loop framework, robust data governance, and continuous model validation. AI should enhance, not replace, clinical expertise, thereby minimizing both diagnostic error and systemic toxicity.[78]
Staging
While Pythium insidiosum keratitis (PIK) traditionally lacks a universally accepted staging system, as in bacterial or fungal keratitis, a clinico-morphologic staging framework has emerged to guide AI-assisted diagnosis, therapeutic planning, and prognostic stratification. AI and deep learning tools can quantify ulcer morphology, depth, and extent, enabling objective stage classification that correlates with disease severity, perforation risk, and the need for early therapeutic penetrating keratoplasty (TPK).
Table. Clinical–Morphologic Staging System for Pythium Keratitis
|
Stage |
Clinical Features |
AI & Imaging Correlates |
Recommended Management |
|
Stage I Early/Localized Epithelial Disease |
Small (<4 mm) anterior stromal infiltrate Clear margins, minimal reticular extension Intact endothelium, no hypopyon Often misdiagnosed as bacterial/fungal keratitis |
Slit-lamp AI detects wet, gray infiltrate with limited tentacular edges IVCM: sparse aseptate filaments in anterior stroma |
Intensive topical linezolid + azithromycin with daily follow-up Avoid antifungal monotherapy |
|
Stage II Stromal Infiltrative Disease |
Moderate infiltrate (4–6 mm) with reticular/tentacular edges Early guttering or feathery margins Minimal endothelial plaque, small hypopyon |
AI heatmap highlights branching gray zones spreading centrifugally IVCM: dense bundles of aseptate filaments reaching mid-stroma |
Continue combined antibacterials Add oral linezolid ± azithromycin Consider early surgical referral |
|
Stage III Deep/Limbal Involvement |
Large infiltrate (>6 mm) or involving >2 quadrants Extension to limbus; anterior chamber reaction; marked pain Hypopyon or descemetocele formation |
AI probability for Pythium >0.7 Model flags tentacular spread to periphery IVCM: deep stromal sheets |
Immediate TPK consult Maintain antibacterials until surgery Stop antifungals |
|
Stage IV Advanced/Perforated or Scleral Extension |
Corneal perforation, scleral or intraocular spread, panophthalmitis Secondary glaucoma or endophthalmitis |
AI classification uncertain (out-of-distribution images) Deep learning segmentation models show full-thickness opacity and loss of corneal contour |
TPK or evisceration based on viability Post-op targeted therapy Avoid keratoprosthesis until infection eradicated |
Modern AI and imaging workflows enable objective, measurement-based staging for research and teleophthalmology, using the following parameters.
Table. Proposed Imaging-Based (AI-Enabled) Substaging Proposal for PIK
|
Parameter |
Stage I |
Stage II |
Stage III |
Stage IV |
|
Ulcer diameter |
<4 mm |
4–6 mm |
>6 mm |
>8 mm or perforated |
|
Stromal depth (OCT/IVCM) |
<33% stromal thickness (superficial anterior stroma) |
33%–50% stromal depth (up to mid-stroma) |
>50% stromal depth (deep stromal involvement) |
Full-thickness involvement ± descemetocele or perforation |
|
Tentacular extension |
Absent |
1–2 quadrants |
≥3 quadrants |
Circumferential |
|
Hypopyon |
None |
<1 mm |
≥1 mm |
Hypopyon + perforation |
|
AI probability score (Pythium) |
<0.5 |
0.5–0.7 |
>0.7 |
>0.9 (or indeterminate due to opacity) |
|
Decision point |
Medical therapy |
Escalate + surgical alert |
Early TPK |
Salvage surgery/evisceration |
Table. Pathological Staging of PIK (Post-TPK Button/Histopathology)
|
Histopathologic Stage |
Microscopic Findings |
Clinical Relevance |
|
A: Superficial Invasion |
Sparse filaments limited to anterior/mid stroma; minimal necrosis |
Good prognosis with medical therapy |
|
B: Deep Stromal Invasion |
Dense aseptate filaments with necrosis, inflammatory response, and early endothelial involvement |
Risk of recurrence post-TPK; requires prolonged antibiotics |
|
C: Full-Thickness & Scleral Extension |
Filaments extending to the Descemet membrane or the sclera |
Poor prognosis; possible evisceration |
Integration of AI and Deep Learning into Staging
- Automated segmentation models (U-Net, DeepLab) can outline the infiltrate area and compute the disease index utilizing the established formula (ie, infiltrate area / total corneal area × depth weighting).
- Temporal tracking: Deep learning can quantify daily changes (eg, >15% area expansion in 24 hours predicts progression to Stage III).
- Decision thresholds: Flag for early TPK when AI-predicted Pythium probability ≥0.7 and area growth ≥10%/day.
- Validation: Models trained on serial slit-lamp and IVCM datasets from India and Thailand show a strong correlation (r > 0.85) between AI stage and clinician-assigned grade.[79]
Clinical Utility of Staging
- Research standardization: Enables uniform grading for AI training and outcome comparisons across centers.
- Triage prioritization: AI-derived stage dictates urgency—Stage I–II for conservative management; Stage III–IV for surgical intervention.
- Prognostic counseling: Higher stages are associated with higher rates of graft failure and recurrence.
- Training dataset labeling: Annotated stages enhance the robustness and interpretability of AI models.[80]
Gurnani–Kaur Staging System
The proposed Gurnani–Kaur Staging System (2024) offers a structured, clinically validated, and AI-integrated framework for grading the severity of Pythium keratitis. It is treatment-oriented, emphasizing early recognition, stage-specific therapy, and integration of digital/AI diagnostic support to ensure uniformity in clinical research and teleophthalmology.
Table. Proposed Gurnani–Kaur Staging System for Pythium insidiosum Keratitis
|
Stage |
Designation |
Clinical/Morphologic Description |
AI/Imaging Correlates |
Recommended Management |
|
Stage I |
Localized (Epithelial/Early Stromal) |
Small infiltrate (<4 mm), well-circumscribed Minimal stromal haze, no tentacular spread No hypopyon, intact endothelium |
AI heatmap confined to the central zone IVCM: sparse aseptate filaments in anterior stroma |
Medical therapy only: linezolid 0.2% + azithromycin 1% hourly; review daily |
|
Stage II |
Progressive (Stromal/Reticular) |
4–6 mm infiltrate with early reticular/tentacular extensions Shallow guttering, mild hypopyon (<1 mm) Partial epithelial defect |
AI probability 0.6–0.7 IVCM: aseptate branching filaments in mid-stroma |
Continue intensive antibacterials ± systemic linezolid/azithromycin; TPK alert if no improvement within 48–72 h |
|
Stage III |
Advanced (Deep/Limbal Involvement) |
>6 mm infiltrate or >2 quadrants Limbal approach, gray reticular margins Hypopyon >1 mm, endothelial plaque |
AI probability ≥0.8 Deep learning segmentation shows expansion >15%/day IVCM: sheets of aseptate filaments extending to the posterior stroma |
Early TPK; continue topical antibacterials pre- and postoperatively |
|
Stage IV |
Complicated/Perforated |
Corneal perforation, descemetocele, scleral or intraocular extension Dense infiltrate with diffuse necrosis |
AI often ungradable; full-thickness opacity OCT: complete stromal loss |
Salvage surgery: repeat TPK, scleral patch, or evisceration depending on viability |
|
Stage V |
Recurrent/Post-TPK Interface Infection |
Recurrence at graft–host junction Marginal gray infiltrate within 2–3 weeks post-TPK |
AI detects edge-based “hot zones” around suture line |
Repeat large-diameter TPK; resume linezolid + azithromycin; meticulous post-op surveillance |
Key Principles of the Proposed Gurnani–Kaur Staging
- Therapy-linked stratification:
- Stages I–II → Medical management
- Stages III–V → Surgical intervention ± adjunctive therapy
- Dynamic staging:
- Incorporates disease progression rate and AI-derived lesion expansion (>10–15%/day) as triggers for upstaging
- AI-integrated quantification:
- Staging aligns with deep-learning models that measure infiltrate area, depth (via OCT/IVCM), and heatmap intensity to assign probability-based stages
- Surgical reproducibility:
- TPK margin: 1–1.5 mm beyond visible lesion
- Donor graft: ≥0.5–1.0 mm oversized
- Graft size: ≥8 mm preferred for peripheral or limbal disease
- Outcome correlation:
- Stage I–II: >80% anatomical and visual success with medical therapy
- Stage III: around 60% globe salvage with early TPK
- Stage IV–V: guarded prognosis; recurrence risk remains high (10–20%)[81]
The Proposed Gurnani–Kaur Staging System bridges clinical, microbiological, and AI-based diagnostic domains for Pythium insidiosum keratitis. It enables standardized reporting, early escalation to TPK, and real-time AI-guided triage, representing a paradigm shift in how Pythium keratitis is graded and managed in both tertiary and teleophthalmology settings. The proposed Pythium Keratitis Staging Framework, supported by AI and imaging metrics, stratifies disease into four progressive stages—from localized epithelial disease to full-thickness perforation. This approach provides a standardized platform for early identification, appropriate therapy selection, and surgical timing, while enabling AI models to learn reproducible patterns of severity.[15]
Prognosis
The prognosis for Pythium insidiosum keratitis hinges on the timing of diagnosis and whether timely anti-oomycete therapy and early TPK (when indicated) are instituted. Delays of even 48 to 72 hours after clear clinical progression markedly worsen anatomic and visual outcomes.
Expected Outcomes
Typical tertiary-center experience
- Stage I–II (localized/progressive without limbus):
- Many eyes can be salvaged medically with topical linezolid 0.2% + azithromycin 1% (± oral agents).
- Anatomic salvage: ~70–85%
- Functional vision (≥20/200): ~40–60% after optical rehab.
- Stage III (deep/limbal disease):
- Early TPK is usually required.
- Anatomic salvage: ~55–70% (higher with large, disease-free margins).
- Functional vision: ~25–40% (often limited by graft clarity/astigmatism).
- Stage IV (perforation/scleral extension):
- Guarded; high risk of recurrence and secondary glaucoma/endophthalmitis.
- Repeat TPK or evisceration may be necessary.
- Recurrence after TPK (Stage V):
- Typically presents at the graft–host junction within 2–3 weeks.
- Repeat, larger-diameter TPK improves control; prognosis depends on the speed of re-excision.
Where available, AI-assisted triage (slit-lamp ± IVCM models) can shorten the time to accurate diagnosis and reduce futile antifungal exposure, translating into higher early-TPK rates when appropriate and improved globe salvage.[82]
Table. Adverse Prognostic Indicators in Pythium Keratitis
|
Domain |
Poor-prognosis features |
|
Lesion biology |
Reticular/“tentacular” peripheral spread; >6 mm diameter; >2 quadrants or limbal involvement; deep stromal sheets on IVCM; hypopyon >1 mm; endothelial plaque |
|
Kinetics |
Area expansion >10–15% over 24 hours despite optimized medical therapy |
|
Treatment history |
Delayed presentation, initial antifungal-only therapy, or late TPK after established limbal spread |
|
Host factors |
Diabetes, malnutrition, poor ocular surface, steroid use, monocular status (late presentation) |
|
Microbiology |
Failure to demonstrate an organism (misclassification), absence of leaf-incubation culture when the routine media is negative |
Causes of Visual Loss Even With Anatomic Salvage
- Graft scarring or vascularization, high irregular astigmatism
- Secondary glaucoma or cataract
- Recurrence at the graft edge requiring repeat TPK
- Macular comorbidity or amblyopia (children)[83]
Counseling and Follow-Up
- Set expectations early; emphasize the possibility of surgery and the need for repeat surgery.
- Schedule daily reviews initially; photograph and measure edges to detect progression.
- Warn about signs of recurrence (eg, new gray “edge,” increased pain, hypopyon).
- After quiescence, plan optical rehabilitation (suture optimization, RGP/scleral lens, later optical keratoplasty if stable).[84]
How Staging Informs Prognosis (Gurnani–Kaur)
- Stage I–II: Generally ffavorablewith medical therapy if progression halts in 48 to 72 hours
- Stage III: Guarded, but early large-margin TPK yields good anatomic outcomes
- Stage IV–V: Poor; prioritize infection control and globe preservation; vision often secondary.
To summarize, early recognition, Pythium-active therapy, and timely TPK (when indicated) with adequate margins are the decisive determinants of outcome; delays and limbal/deep involvement sharply reduce both globe salvage and final vision.[85]
Complications
Pythium keratitis is notorious for its rapid progression, resistance to antifungal therapy, and high complication rates, especially when diagnosis or surgical intervention is delayed. The organism’s unique oomycete cell wall (cellulose, not chitin) and aggressive stromal invasion cause distinctive, often catastrophic sequelae affecting both globe integrity and visual function.[8]
Table. Ocular Complications of Pythium Keratitis
|
Complication |
Description and Clinical Significance |
|
Corneal Perforation |
End-stage result of unchecked stromal lysis; may occur within 48–72 hours if untreated and requires emergency TPK or cyanoacrylate patching |
|
Rapid Stromal Melting/Necrosis |
Extensive stromal collagenolysis due to enzymatic tissue degradation, often progressing more rapidly than fungal keratitis and poorly responsive to antifungal therapy |
|
Limbal Involvement and Scleral Extension |
Extension of infection into the limbus or sclera with necrotizing scleritis; may cause phthisis bulbi if inadequately excised |
|
Endothelial Plaque Formation |
Dense posterior corneal exudate indicating deep stromal invasion and potential AC contamination |
|
Hypopyon and Anterior Chamber (AC) Reaction |
Marked intraocular inflammatory response with leukocytic exudate in the AC; may predispose to synechiae formation or secondary glaucoma |
|
Secondary Glaucoma |
Elevated intraocular pressure (IOP) due to inflammatory debris obstructing the trabecular meshwork; may require medical therapy or surgical management if persistent |
|
Endophthalmitis/Panophthalmitis |
Intraocular extension of the infection, especially following limbal or scleral breach; may necessitate evisceration |
|
Recurrent Interface Infection (Post-TPK) |
Occurs at the graft–host junction, typically within 1–3 weeks; presents as a characteristic gray infiltrate along the sutures; often requires repeat, larger TPK (reported recurrence rate ~15%–25%) |
|
Corneal Graft Failure / Decompensation |
Loss of graft clarity due to immune rejection or recurrence-related necrosis, particularly in advanced cases (final graft clarity <40%) |
|
Secondary Cataract |
Results from chronic inflammation or post-surgical corticosteroid use |
|
Posterior Synechiae and Iridocorneal Adhesions |
Develop secondary to chronic AC inflammation; can complicate IOP control and future ocular surgeries |
Table. Post-Therapeutic & Surgical Complications of Pythium Keratitis
|
Context |
Complication |
Management Recommendations |
|
After TPK |
Graft melt or wound dehiscence |
Ensure disease-free margins ≥1 mm; continue anti-oomycete therapy postoperatively |
|
After repeat TPK |
Progressive recurrence at margins |
Requires re-debridement, a larger graft, and systemic antibiotics |
|
After topical antibiotics (linezolid/azithromycin) |
Epithelial toxicity, punctate keratopathy |
Reduce dosing frequency once epithelialization is achieved; supplement with lubricants |
|
Systemic linezolid |
Bone marrow suppression, peripheral neuropathy (after >2 weeks) |
CBC monitoring every 7–10 days during prolonged therapy |
|
Systemic azithromycin |
GI upset, QT prolongation (rare) |
Monitor ECG in cardiac patients |
Table. Diagnostic and AI-Related Complications in Pythium Keratitis Management
|
AI / Workflow Pitfall |
Potential Adverse Impact |
Preventive Strategy |
|
False-negative AI triage |
Delayed TPK → corneal perforation or scleral spread |
Always confirm with smear/culture/IVCM; use sensitivity-optimized AI threshold (≥0.7) |
|
False-positive AI result |
Unnecessary surgery or therapy change |
Human verification and microbiologic correlation required |
|
Poor-quality image input |
Misclassification → delayed correct diagnosis |
Enforce standardized image-capture protocol (multiple angles, consistent lighting) |
Vision-Related Sequelae of Pythium Keratitis
- Permanent corneal opacity/scarring
- Even with anatomic success, visual acuity is often limited to 20/200 to 20/400 without optical keratoplasty.
- Irregular astigmatism and anisometropia
- Common after large TPK and may require rigid gas-permeable or scleral lenses.
- Graft vascularization
- Increases risk of immune rejection and recurrent infection
- Phthisis bulbi/globe loss
- Seen in up to 10–15% of advanced cases (Stage IV–V) despite surgical intervention [86]
Table. Long-Term Complications of Pythium Keratitis
|
Complication |
Timing |
Impact |
|
Refractory glaucoma |
Months to years post-TPK |
Visual loss even after infection resolution |
|
Recurrent Pythium infection |
Months after initial control |
Often due to residual limbal tissue or scleral spread |
|
Need for optical keratoplasty |
3–6 months after quiescence |
May be required for visual rehabilitation, if the ocular surface is stable |
|
Psychological distress |
Anxiety/depression after multiple failed surgeries or vision loss |
Requires counseling and vision rehabilitation support |
To summarize, complications of Pythium keratitis span the full spectrum from rapid corneal melt and perforation to post-TPK recurrence and graft failure. The best prevention lies in timely recognition, Pythium-specific therapy, and well-coordinated medical-surgical management. Integration of AI-assisted early diagnosis, adherence to Gurnani–Kaur staging, and multidisciplinary follow-up substantially reduces complication rates and improves long-term globe preservation.[87]
| Pause and Reflect | A deep learning model predicts a high likelihood of poor outcomes in patients with infectious keratitis using image features and clinical variables. Which clinical feature, when identified by both AI and slit-lamp examination, most strongly correlates with poor prognosis? |
Postoperative and Rehabilitation Care
The postoperative phase following therapeutic penetrating keratoplasty (TPK) or medical resolution of Pythium keratitis is critical for controlling the infection, maintaining graft survival, and achieving visual rehabilitation. Because Pythium is an aggressive, recurrent oomycete, postoperative care must combine strict antimicrobial stewardship, close follow-up, and long-term surface rehabilitation strategies.[2]
1. Immediate Postoperative Phase (Weeks 1–2)
During the immediate postoperative period, management focuses on infection control, graft stability, and close monitoring for early recurrence. Corticosteroids should be avoided until the ocular surface is clinically quiet and no recurrence is evident for at least 7–10 days. Recommended topical therapy during this phase is summarized in the table below.
Table. Immediate Postoperative Phase Topical Therapy (Days 0–14)
|
Medication |
Purpose |
Frequency |
|
Linezolid 0.2% |
Primary anti-oomycete coverage |
Every 1–2 hours while awake |
|
Azithromycin 1% |
Synergistic anti-oomycete action |
Every 1–2 hours while awake |
|
Cycloplegic (Atropine 1%) |
Prevent synechiae, reduce pain |
Twice daily |
|
Lubricants (Preservative-free) |
Promote epithelial healing |
Every 2–3 hours |
|
Antiglaucoma drops (if IOP >21 mmHg) |
Control secondary glaucoma |
As required |
2. Intermediate Phase (Weeks 2–8)
Infection surveillance:
- Daily slit-lamp monitoring for the first week, then every 2 to 3 days for the next month.
- Assess for:
- Edge infiltration or gray reticular pattern (suggesting recurrence)
- Loose sutures, vascularization, or epithelial defects
Laboratory monitoring:
- Review the histopathology of the excised host button to confirm the diagnosis and adequacy of margins.
- Repeat smear/culture from graft margin or epithelial defect if recurrence is suspected.
Step-down therapy:
- After 3 to 4 weeks of infection-free status, taper linezolid + azithromycin to QID dosing.
- If inflammation persists but infection is controlled, introduce mild topical steroid (eg, fluorometholone 0.1%) once daily under supervision.
Systemic monitoring (for extended therapy):
- CBC weekly for linezolid-induced cytopenia
- ECG monitoring if azithromycin is used beyond 2 weeks[88]
3. Late Phase (Beyond 2 Months)
Graft stability and clarity:
- Assess clarity, suture integrity, and vascularization.
- Remove loose sutures early to avoid a nidus for infection.
- Manage surface irregularity with lubricants or a bandage lens.
Secondary procedures:
- Repeat TPK: For recurrent infection at the graft–host junction
- Optical keratoplasty: 3 to 6 months after complete healing for visual rehabilitation
- Secondary cataract surgery: Deferred until inflammation subsides
- Scleral lens fitting: For irregular astigmatism or post-TPK ectasia
IOP and uveitis control:
- Continue antiglaucoma therapy if needed.
- Evaluate optic nerve and macula periodically for damage from prolonged inflammation.[89]
Table. Rehabilitation and Visual Recovery in Pythium Keratitis
|
Goal |
Strategies |
Timeline |
|
Functional vision |
Rigid gas-permeable or scleral contact lenses |
3–6 months post-healing |
|
Ocular surface stability |
Lubrication, punctal occlusion, and amniotic membrane if scarring |
As indicated |
|
Optical clarity |
Optical keratoplasty (if infection quiescent ≥3 months) |
4–6 months |
|
Psychological support |
Counseling and low-vision aid training |
Throughout recovery |
AI-Integrated Postoperative Surveillance
With advances in AI and deep-learning imaging, postoperative follow-up can incorporate:
- AI-based recurrence prediction
- Models detect early “hot zones” or subtle graft-edge infiltration on slit-lamp photos.
- Remote teleophthalmology monitoring
- Patients can upload smartphone slit-lamp images to identify early recurrence.
- Progress quantification
- AI measures graft transparency and surface regularity to objectively track healing.[90]
Patient Education and Lifestyle Modification
- Maintain strict medication adherence; missed doses may lead to recurrence.
- Avoid over-the-counter or self-prescribed antifungals or corticosteroids.
- Protect the operated eye from dust and water exposure for at least 3 months.
- Use UV-protective glasses and night-time eye shields.
- Establish a protein-rich diet and hydration to aid healing.
Table. Prognostic Follow-up Schedule for Pythium Keratitis
|
Time after TPK |
Clinical Action |
|
Day 1–14 |
Daily slit-lamp exam; epithelial defect check |
|
Weeks 3–6 |
Every 2–3 days; monitor edge clarity and IOP |
|
Months 2–3 |
Weekly review; consider steroid introduction if stable |
|
Months 4–6 |
Monthly; plan optical rehab or secondary surgery |
|
After 6 months |
Every 3–6 months for long-term graft and glaucoma monitoring |
Effective postoperative and rehabilitation care for Pythium keratitis hinges on prolonged topical anti-oomycete therapy, meticulous graft surveillance, and timely visual rehabilitation. Integrating AI-based recurrence detection and structured follow-up protocols significantly reduces recurrence, improves graft survival, and enhances long-term outcomes.[91]
Consultations
Management of Pythium keratitis requires a multidisciplinary, interprofessional approach, as the condition spans infectious disease, corneal surgery, microbiology, and postoperative rehabilitation. Timely coordination between these specialties is vital for accurate diagnosis, rapid initiation of anti-oomycete therapy, and optimal surgical outcomes.
1. Ophthalmology (Cornea and Ocular Microbiology Team)
Primary responsibility: Diagnosis, medical management, and surgical intervention.
Key roles
- Clinical diagnosis: Identify classical reticular/tentacular infiltrate and differentiate from fungal keratitis.
- Smear and culture sampling: Perform KOH, Gram, and IKI–H2SO4 staining at first presentation.
- Early referral for TPK: Coordinate with the anterior segment surgeon for prompt grafting in advanced disease.
- Postoperative follow-up: Monitor for recurrence, graft survival, and interface infection.
- Integration of AI tools: Use slit-lamp AI probability scoring for early triage and remote consultations.[14]
2. Microbiology/Infectious Disease Specialist
Purpose: Confirm diagnosis and guide targeted antimicrobial therapy.
Key contributions
- Culture & identification: Perform blood agar growth and zoospore confirmation via the leaf-incubation method.
- Molecular diagnostics: Conduct PCR/LAMP/qPCR or ITS region sequencing to confirm species.
- Antimicrobial sensitivity testing: Support the use of linezolid and azithromycin over antifungals.
- Monitor response: Evaluate smear negativity post-therapy and advise on duration of systemic antibiotics.
- Antibiotic stewardship: Prevent antifungal misuse and ensure rational antibacterial dosing.[92]
3. Pathology/Histopathology
Role: Confirm invasion pattern and assess surgical margins post-TPK.
- Examine the corneal button for aseptate filaments (PAS variable, GMS weak).
- Rule out mixed infection or coexisting fungal components.
- Document the depth of invasion and scleral involvement for staging correlation (Stage III–IV).
- Provide input for future AI training datasets via digitized histopathology slides.[93]
4. Ocular Imaging and Artificial Intelligence Unit
Collaborative function
- Maintain AI-assisted image repositories for pattern recognition.
- Validate and retrain models with clinician-confirmed ground truth (laboratory and histopathology data).
- Deploy teleophthalmology-based AI triage for rural or referral settings.
- Coordinate with cornea specialists to interpret heatmaps and validate probability cut-offs.[94]
5. Surgical/Anterior Segment Team
Responsibilities
- Perform therapeutic penetrating keratoplasty (TPK) with 1 to 1.5 mm clear margins.
- Decide on repeat TPK or salvage surgery for recurrent disease.
- Manage intraoperative sampling for microbiology and histopathology.
- Oversee graft suturing, AC reformation, and postoperative wound stability.
- Collaborate with anaesthesiology for cases requiring urgent surgery.[95]
6. Internal Medicine/Systemic Physician Consultation
- Evaluate systemic tolerance for oral linezolid or azithromycin.
- Monitor for adverse drug reactions (eg, bone marrow suppression, QT prolongation).
- Manage comorbidities (eg, diabetes, malnutrition) that influence healing.[96]
7. Low-Vision and Rehabilitation Specialists
Involvement: Post-infection and post-surgical rehabilitation
- Fit scleral or rigid gas-permeable lenses for visual recovery.
- Provide low-vision aids if optical keratoplasty is not possible.
- Offer occupational counseling and psychological support for monocular patients.[97]
8. AI Ethics and Data Governance Committee (Institutional/Research Level)
Purpose: Ensure safe and responsible use of AI in patient care and research.
- Review model performance and patient data privacy compliance (GDPR/ICMR).
- Approve AI deployment in clinical settings.
- Oversee bias audits and interdepartmental data-sharing agreements.[98]
9. Teleophthalmology and Public Health Coordination
- Establish remote, image-based triage to enable early detection in rural hospitals.
- Train local ophthalmologists to identify Pythium features and use mobile AI applications.
- Maintain referral networks with tertiary corneal units for timely TPK.
- Support community-level awareness programs during monsoon and harvest seasons in endemic areas.
Effective management of Pythium insidiosum keratitis requires synchronized collaboration among corneal specialists, microbiologists, pathologists, infectious disease experts, AI developers, and rehabilitation teams. Early multidisciplinary consultations, guided by standardized Gurnani–Kaur staging and AI-aided triage, significantly improve diagnostic precision, reduce recurrence, and enhance long-term visual outcomes.[99]
Deterrence and Patient Education
Pythium keratitis is a rapidly progressive, vision-threatening infection that often mimics fungal keratitis but requires a distinct therapeutic approach. Deterrence and education are crucial for early recognition, exposure prevention, and avoidance of inappropriate therapy, which remains the leading cause of poor outcomes.[17]
Table. Patient Awareness and Preventive Measures for Pythium Keratitis
|
Focus Area |
Education/Prevention Strategy |
|
Environmental Exposure |
Avoid direct contact with contaminated water, especially in rice fields, ponds, or stagnant puddles during the monsoon season. Use protective eyewear during agricultural work, swimming, or bathing in untreated water. Educate rural workers about the risk of infection from exposure to muddy or marshy water and minor ocular trauma. |
|
Trauma Management |
Even trivial corneal abrasions after vegetative or aquatic injury must be examined by an ophthalmologist. Avoid over-the-counter steroid or antibiotic drops without proper evaluation. |
|
Early Medical Consultation |
Seek prompt care if symptoms such as redness, pain, tearing, or visual blurring occur after exposure to contaminated water. Delays >48 hours in diagnosis significantly worsen outcomes. |
|
Avoidance of Self-Medication |
Discourage use of antifungal drops (natamycin, voriconazole) for undiagnosed keratitis, as they are ineffective against Pythium and delay definitive therapy. |
|
Post-Surgical Hygiene |
Maintain strict hygiene post-TPK or corneal scraping. Avoid rubbing or splashing water on the operated eye. Ensure adherence to prescribed antibacterial regimen (linezolid/azithromycin). |
|
Contact Lens Users |
Use sterile lens solutions, and avoid tap or well water. Never rinse or store lenses in non-sterile liquids. |
Table. Community and Public Health Education Regarding Pythium Keratitis
|
Target Group |
Strategy |
|
Farmers/Field Workers |
Conduct eye-safety awareness camps before monsoon and harvest seasons. Distribute protective goggles and saline eye rinse kits. |
|
Primary Care Physicians and Optometrists |
Train in early identification of reticular infiltrates suggestive of Pythium. Encourage immediate referral to tertiary eye centers for corneal scraping. |
|
Rural Health Workers (ANMs/ASHAs) |
Educate about early red flags (gray infiltrate, satellite lesions, rapid pain) and the importance of referral. |
|
Community Health Programs |
Integrate Pythium education into the National Programme for Control of Blindness (NPCB) and Vision 2020 initiatives. |
Hospital-Level Deterrence
- Implement infection alert systems for suspected Pythium.
- Maintain dedicated microbiology and culture facilities (leaf-incubation method, PCR, IVCM).
- Ensure availability of linezolid and azithromycin formulations for immediate initiation.
- Enforce protocols for early referral and TPK scheduling for non-responsive keratitis.
- Regularly train residents and fellows to distinguish Pythium from fungal ulcers.[100]
Table. Postoperative and Recurrence Prevention Counseling for Pythium Keratitis
|
Topic |
Counseling Content |
|
Medication adherence |
Stress the importance of completing a full topical and systemic course even after apparent healing. |
|
Follow-up visits |
Schedule daily or alternate-day reviews initially; later, assess weekly until complete resolution. |
|
Recurrence awareness |
Teach patients to immediately report any new gray edge, pain, or watering. |
|
Avoid exposure |
Avoid swimming, eye rubbing, or exposure to contaminated water for at least 6 months post-TPK. |
|
Long-term care |
Discuss the need for optical keratoplasty, low-vision aids, and psychological support if vision loss persists. |
Pearls and Other Issues
Pythium keratitis represents one of the most rapidly progressive and diagnostically challenging forms of infectious keratitis. Successful management depends on early recognition, anti-oomycete–specific therapy, and timely surgical intervention guided by well-defined staging and interprofessional coordination.
Clinical Pearls
- Think beyond fungus:
- Pythium mimics fungal keratitis but does not respond to antifungals.
- Failure to improve after 48–72 hours of antifungal therapy should raise suspicion for Pythium.
- Classic slit-lamp clues:
- Reticular or “tentacular” infiltrates radiating from the main lesion
- Gray-white, dry, cotton-wool–like infiltrate with peripheral guttering
- Absent pigmentation and minimal feathery margins compared to filamentous fungi
- Smear and culture are key to confirmation:
- KOH or Gram stain: Long, slender, aseptate filaments with right-angle branching
- IKI–H2SO4 stain: Highlights cellulosic walls (distinct from fungal chitin)
- Blood agar growth: Flat, feathery, gray-white colonies within 24–48 hours
- Definitive laboratory proof:
- Leaf-incubation technique for zoospore formation remains the diagnostic gold standard.
- PCR or LAMP-based detection of the ITS region provides rapid molecular confirmation.
- Anti-oomycete therapy cornerstone:
- Linezolid 0.2% + Azithromycin 1% hourly is the most effective topical regimen.
- Avoid antifungals and amphotericin; they delay cure and promote progression.
- Timing is sight-saving:
- Delays >72 hours or lesion progression >15% in 24 hours correlate with poor outcome.
- Early TPK, before limbal extension, dramatically improves prognosis.
- Gurnani–Kaur Staging practical application:
- Stage I–II: Medical management window
- Stage III: Early TPK indicated
- Stage IV–V: Advanced/salvage stage, may require repeat TPK or evisceration
- Histopathology hallmark:
- Filament invasion throughout the stroma with necrosis and minimal inflammatory response
- No true septa; hyphal walls are thinner and refractile compared to fungi
- Recurrence pattern:
- Appears at graft–host junction within 2–3 weeks post-TPK
- Edge-based gray infiltration signals relapse and requires prompt repeat graft
- AI’s emerging role:
- AI-based corneal imaging models can identify Pythium probability ≥0.7 within seconds.
- Integration with confocal/OCT data improves diagnostic accuracy and speeds triage.[18]
Table. Common Pitfalls in the Diagnosis and Management of Pythium Keratitis
|
Pitfall |
Consequence |
Prevention |
|
Misdiagnosing Pythium as fungal keratitis |
Delayed correct therapy → perforation, loss of eye |
Use dual diagnostic stains and an early microbiology consult |
|
Late TPK after limbal spread |
Recurrence, graft failure, evisceration |
Perform TPK when the lesion is <2 quadrants from the limbus |
|
Incomplete margin excision during TPK |
Re-infection from residual filaments |
Maintain 1–1.5 mm disease-free margin intraoperatively |
|
Premature steroid use |
Accelerated recurrence |
Introduce only after complete microbiologic and clinical quiescence |
|
Ignoring systemic toxicity |
Bone marrow suppression (linezolid) |
Weekly CBC and treatment duration monitoring |
|
Poor postoperative surveillance |
Missed early recurrence |
Daily to alternate-day follow-up during the initial 3 weeks |
Disposition and Follow-Up
- Hospitalization: Indicated for progressive cases, large ulcers, or surgical candidates
- Discharge criteria: Stable epithelial cover, negative culture/smear, controlled inflammation
- Follow-up schedule: Daily for the first week, every 2–3 days for the next month, then weekly until quiescence
- AI-assisted follow-up: Slit-lamp images uploaded for algorithmic recurrence monitoring and remote triage[101]
Prevention Highlights
- Avoid antifungal monotherapy in unresponsive keratitis.
- Promote community awareness among farmers and ophthalmic technicians.
- Use protective eyewear during agricultural work and when exposed to water.
- Encourage the use of AI-based screening apps in rural clinics for early identification.[102]
Research and Future Directions
- AI-driven diagnostic models using multimodal inputs (slit-lamp, IVCM, OCT)
- Cellulose biosynthesis inhibitor (CBI) therapy (currently under exploration as a novel anti-oomycete approach)
- Genomic surveillance to identify regional Pythium strains and resistance patterns
- Teleophthalmology integration to link rural centers with tertiary cornea units[103]
Summary of Key Pearls
- Pythium insidiosum is an oomycete, not a fungus—antifungals fail.
- Linezolid + azithromycin form the cornerstone of therapy.
- Early surgical intervention ensures anatomical salvage.
- AI-based detection and Gurnani–Kaur staging optimize triage and timing.
- Recurrence vigilance post-TPK is essential to prevent total vision loss.[104]
Enhancing Healthcare Team Outcomes
Effective management of Pythium keratitis depends on collaboration across multiple healthcare disciplines, integrating clinical acumen, microbiological precision, surgical expertise, and AI-driven diagnostics. Because of its aggressive course and unique resistance profile, coordinated teamwork enables rapid decision-making, minimizes vision loss, and improves patient-centered outcomes.
Table. Interprofessional Collaboration Framework for Pythium Keratitis Management
|
Team Member |
Key Responsibilities |
Impact on Patient Outcomes |
|
Cornea Specialist/ Ophthalmologist |
Early diagnosis, clinical staging (Gurnani–Kaur), initiation of Pythium-active therapy, and timely TPK planning |
Prevents progression, ensures optimal surgical timing |
|
Microbiologist |
Rapid smear/culture confirmation, leaf-incubation method, molecular PCR/LAMP testing |
Enables definitive identification and reduces misdiagnosis |
|
Pathologist |
Histopathologic confirmation of aseptate filaments, evaluation of excision margins, and documentation for recurrence prediction |
Ensures margin adequacy and guides postoperative management |
|
Infectious Disease Physician |
Advises on systemic antibiotic use, drug interactions, and stewardship protocols |
Prevents resistance and systemic toxicity |
|
AI/Data Science Team |
Develops and validates deep-learning models for early diagnosis and recurrence prediction |
Reduces diagnostic delay and enhances triage accuracy |
|
Nursing and Allied Health Staff |
Postoperative wound care, drop administration, and patient education |
Enhances compliance and reduces reinfection risk |
|
Pharmacist |
Ensures proper compounding of linezolid/azithromycin formulations and monitors systemic drug safety |
Improves medication accuracy and safety |
|
Vision Rehabilitation Specialist |
Provides optical rehabilitation (RGP/scleral lenses), low-vision aids, and psychological support |
Restores functional independence and quality of life |
Communication and Coordination Strategies
- Interdepartmental rounds: Daily joint reviews between ophthalmology, microbiology, and pathology during early management
- Digital collaboration: Use of teleophthalmology and AI dashboards for remote rural triage and follow-up image sharing
- Standardized protocols: Adoption of Gurnani–Kaur staging checklist for unified documentation and communication between surgical and medical teams
- Handoff protocols: Structured patient transfer notes including stage, lesion metrics, AI probability, treatment duration, and response history[3]
Ethical and Professional Considerations
- Informed consent: Clearly communicate that Pythium is not fungal and may require surgical removal despite aggressive medical therapy.
- Shared decision-making: Discuss prognosis, recurrence risk, and visual rehabilitation options with the patient and caregivers.
- Equitable access: Extend AI-assisted triage to underserved areas through mobile or web-based diagnostic tools.
- Data ethics: Ensure the anonymization and secure handling of patient images used for AI training in accordance with ICMR/WHO digital ethics guidelines.[105]
Table. Outcome Enhancement Metrics for Pythium Keratitis
|
Performance Domain |
Measurable Indicator |
|
Diagnostic accuracy |
Reduction in misdiagnosed fungal ulcers (%) |
|
Time to correct therapy |
Average interval (hours) between suspicion and start of Pythium-specific treatment |
|
Surgical outcomes |
Graft survival at 6 months (%) |
|
Patient satisfaction |
Visual and psychosocial rehabilitation feedback |
|
AI integration efficacy |
Sensitivity/specificity of model predictions in real-world cases |
Interprofessional Ethical Imperatives
- Maintain transparency in algorithmic decision-making (Explainable AI).
- Prioritize patient autonomy and shared decisions regarding surgery or long-term therapy.
- Promote equitable data representation to prevent geographic and socioeconomic bias in AI datasets.[106]
Summary
Enhancing healthcare team outcomes in Pythium keratitis requires rapid cross-disciplinary communication, AI-augmented precision, and compassionate patient-centered care. When ophthalmologists, microbiologists, surgeons, nurses, pharmacists, and AI engineers operate cohesively within a Gurnani–Kaur staging–based framework, patient safety, early diagnosis, and globe salvage rates improve substantially, transforming Pythium management from reactive to proactive and predictive.[107]
Media
(Click Image to Enlarge)
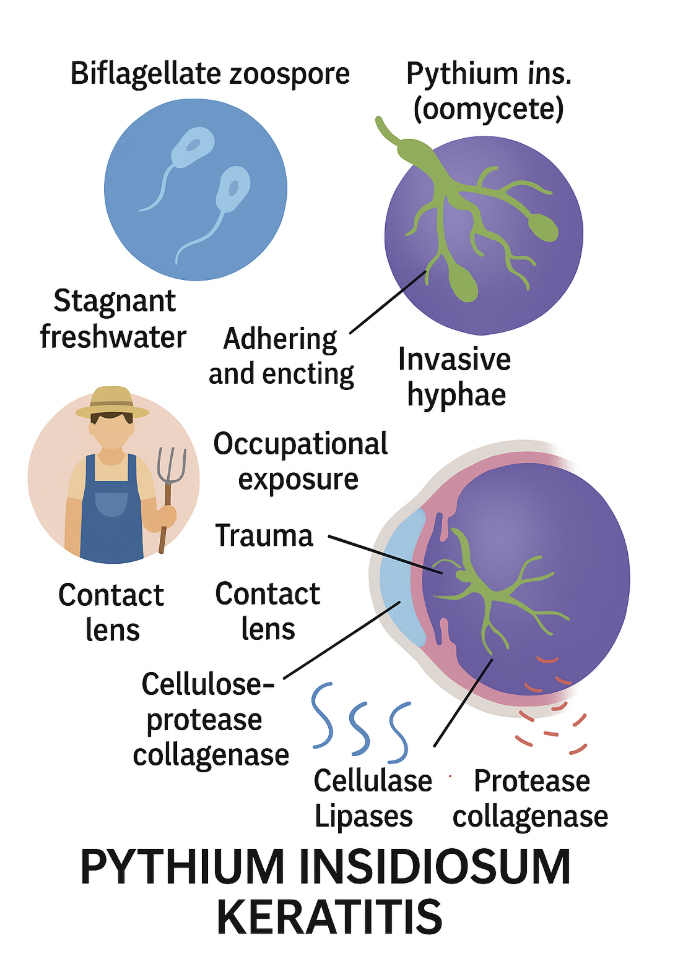
Schematic diagram depicting risk factors for Pythium insidiosum keratitis
Bharat Gurnani, MD
(Click Image to Enlarge)
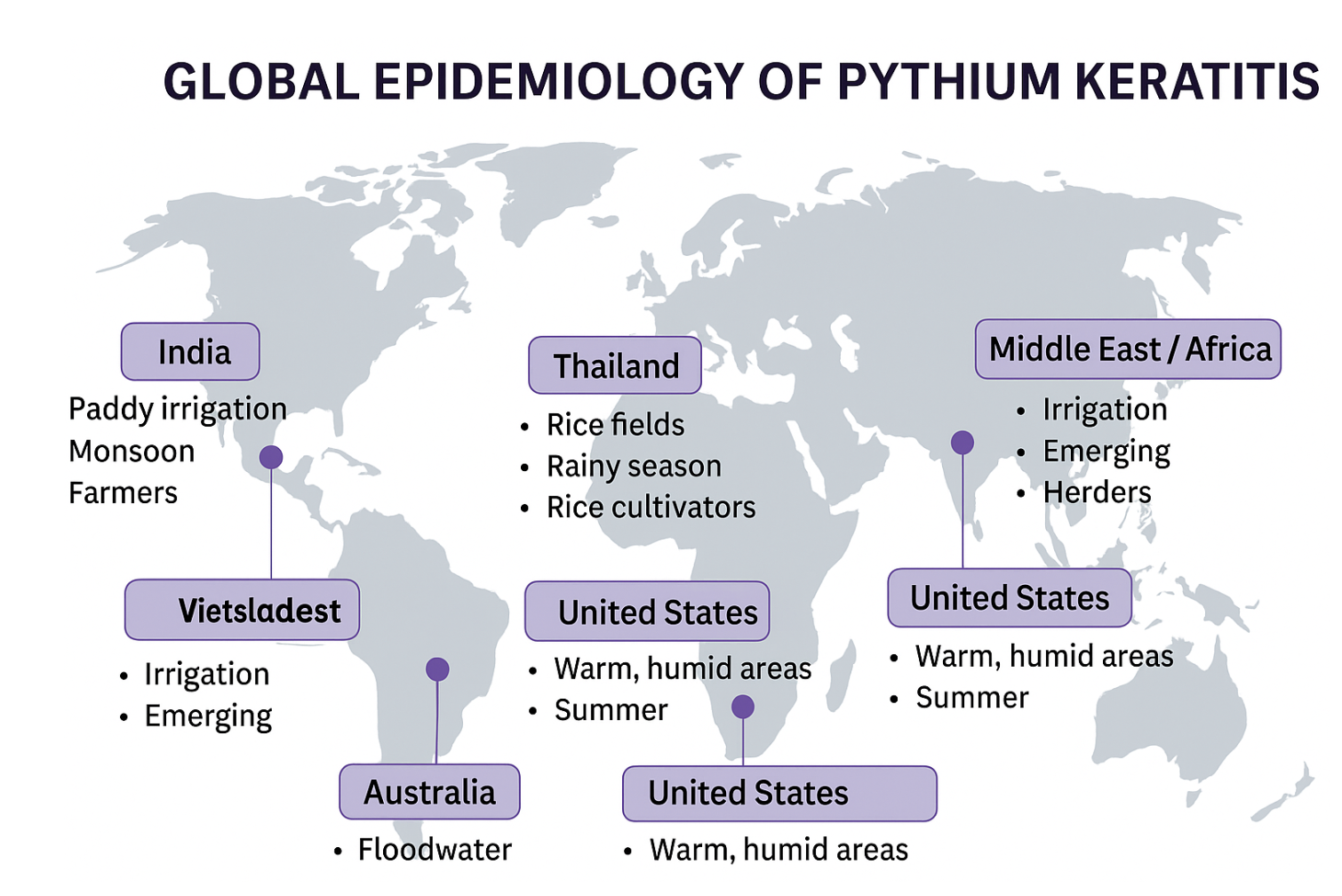
Schematic diagram depicting epidemiology of Pythium insidiosum keratitis
Bharat Gurnani, MD
(Click Image to Enlarge)
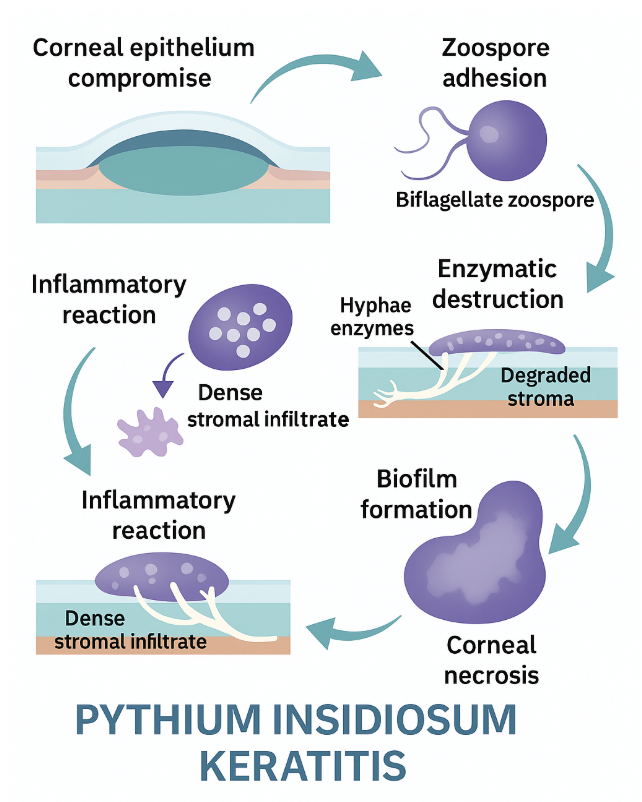
Schematic diagram depicting pathophysiology of Pythium insidiosum keratitis
Bharat Gurnani, MD
(Click Image to Enlarge)
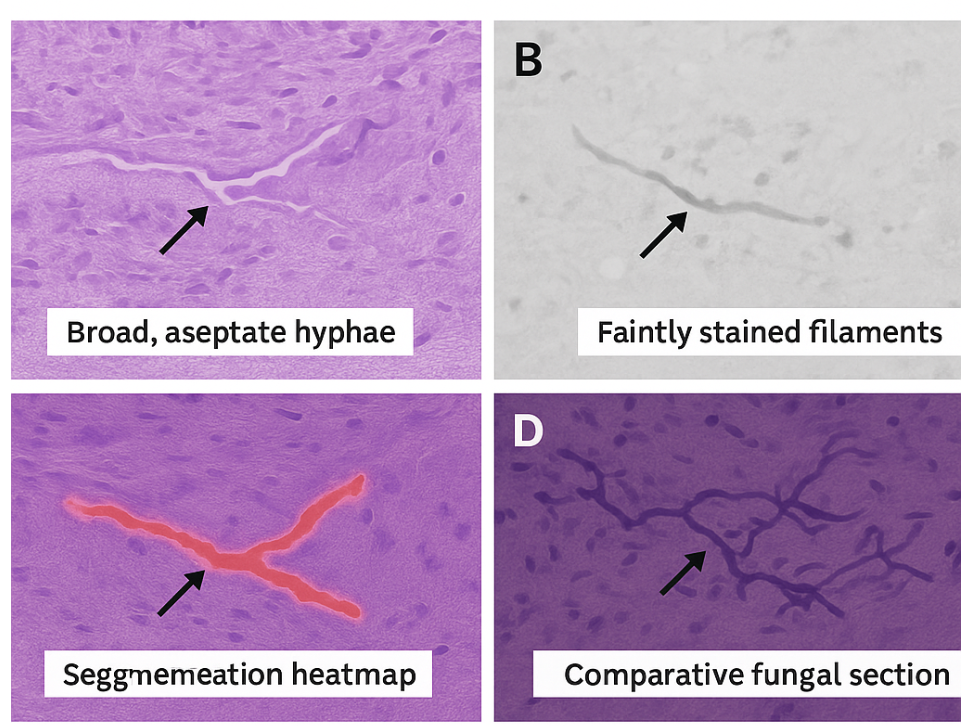
Schematic diagram depicting histopathology of Pythium insidiosum keratitis
Bharat Gurnani, MD
(Click Image to Enlarge)
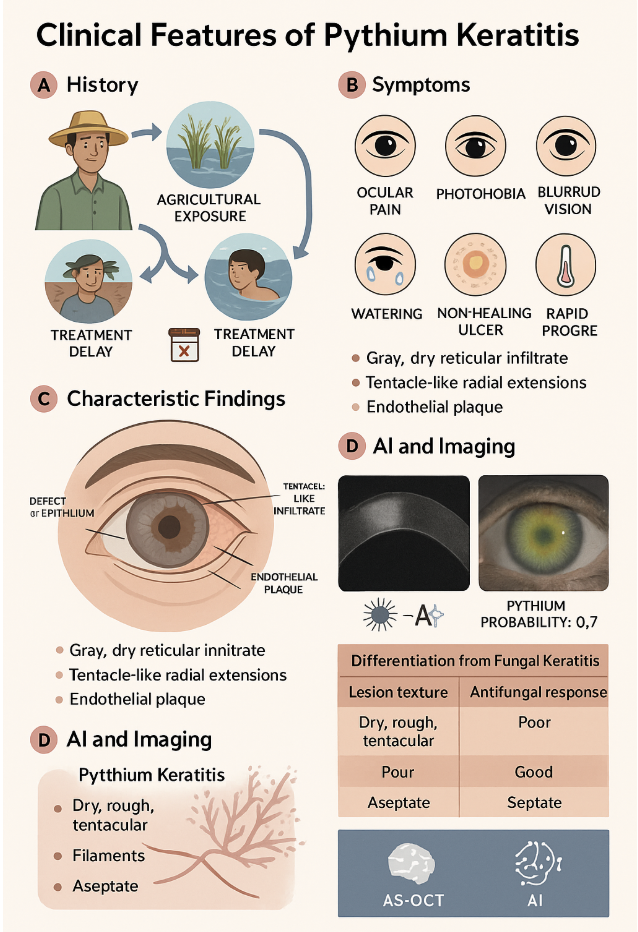
Schematic diagram depicting clinical features of Pythium insidiosum keratitis
Bharat Gurnani, MD
(Click Image to Enlarge)
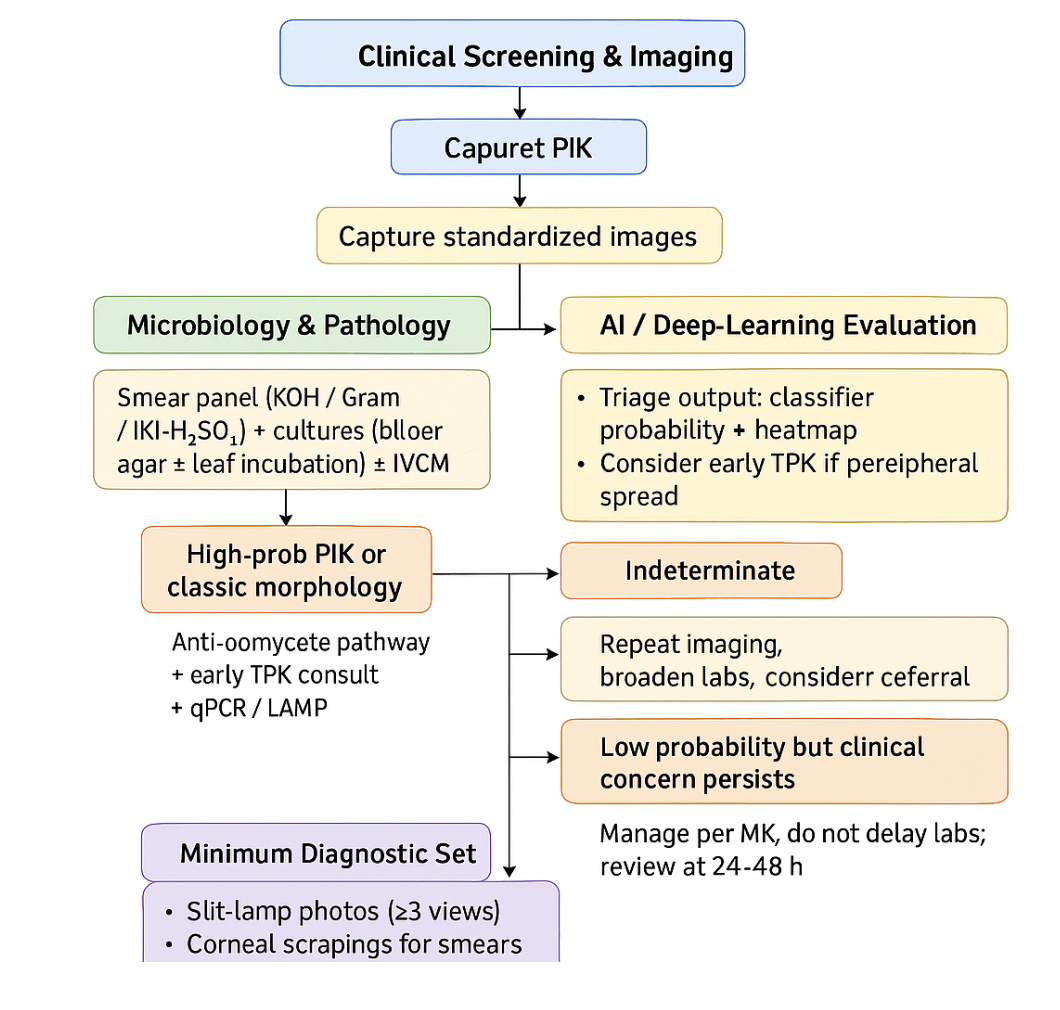
Schematic diagram depicting staging of Pythium insidiosum keratitis
Bharat Gurnani, MD
(Click Image to Enlarge)
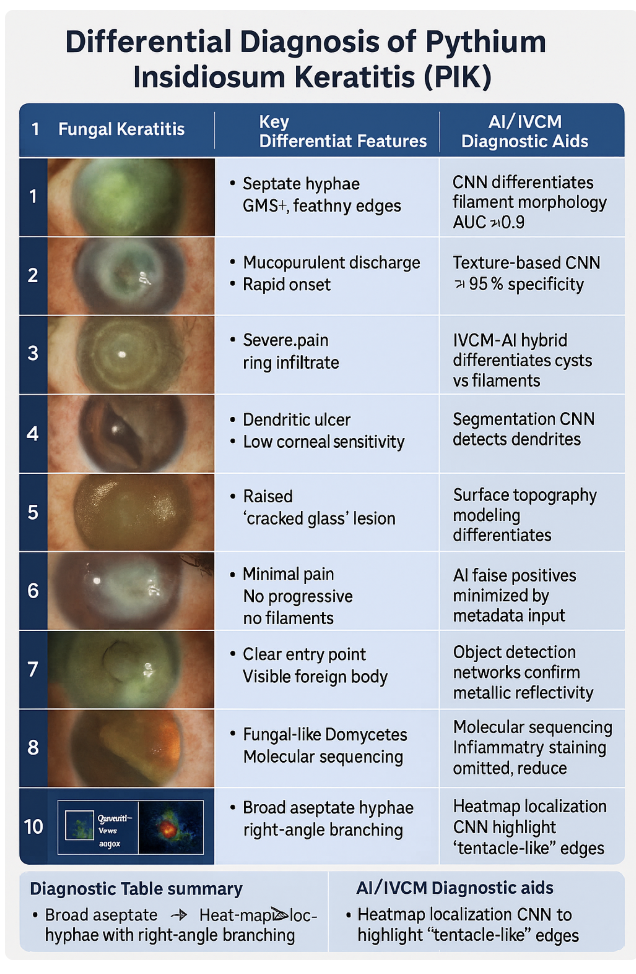
Schematic diagram depicting the differential diagnosis of Pythium insidiosum keratitis
Bharat Gurnani, MD
References
Gurnani B, Kaur K. Advancing diagnostics in Pythium insidiosum keratitis: the emerging role of point-of-care imaging and biosensor-based detection devices. Expert review of medical devices. 2025 Dec:22(12):1287-1292. doi: 10.1080/17434440.2025.2582616. Epub 2025 Nov 2 [PubMed PMID: 41147335]
Gurnani B, Kaur K. Pythium Keratitis. StatPearls. 2026 Jan:(): [PubMed PMID: 34424645]
Gurnani B, Kaur K. Anti-infective therapies for Pythium insidiosum keratitis. Expert review of anti-infective therapy. 2024 Oct:22(10):805-817. doi: 10.1080/14787210.2024.2403146. Epub 2024 Sep 13 [PubMed PMID: 39268901]
Gurnani B, Kaur K. Letter to the editor: Case series: Mixed infectious keratitis by Pythium insidiosum and fungal species. Optometry and vision science : official publication of the American Academy of Optometry. 2024 May 1:101(5):236. doi: 10.1097/OPX.0000000000002147. Epub [PubMed PMID: 38857033]
Level 2 (mid-level) evidenceGurnani B, Kaur K. Intricacies and solutions for interpretation of microbiologic samples of Pythium insidiosum keratitis. Indian journal of ophthalmology. 2024 Apr 1:72(4):602-603. doi: 10.4103/IJO.IJO_1573_23. Epub 2024 Mar 28 [PubMed PMID: 38546474]
Gurnani B, Kaur K, Gireesh P, Balakrishnan L, Mishra C. Evaluating the novel role of ChatGPT-4 in addressing corneal ulcer queries: An AI-powered insight. European journal of ophthalmology. 2025 Sep:35(5):1531-1541. doi: 10.1177/11206721251337290. Epub 2025 Apr 28 [PubMed PMID: 40295112]
Gurnani B, Kaur K, Lalgudi VG, Kundu G, Mimouni M, Liu H, Jhanji V, Prakash G, Roy AS, Shetty R, Gurav JS. Role of artificial intelligence, machine learning and deep learning models in corneal disorders - A narrative review. Journal francais d'ophtalmologie. 2024 Sep:47(7):104242. doi: 10.1016/j.jfo.2024.104242. Epub 2024 Jul 15 [PubMed PMID: 39013268]
Level 3 (low-level) evidenceGurnani B, Natarajan R, Mohan M, Kaur K. Breaking-Down Barriers: Proposal of Using Cellulose Biosynthesis Inhibitors and Cellulase Enzyme as a Novel Treatment Modality for Vision Threatening Pythium Insidiosum Keratitis. Clinical ophthalmology (Auckland, N.Z.). 2024:18():765-776. doi: 10.2147/OPTH.S450665. Epub 2024 Mar 11 [PubMed PMID: 38495678]
Byrd LB, Gurnani B, Martin N. Corneal Ulcer. StatPearls. 2026 Jan:(): [PubMed PMID: 30969511]
Gurnani B, Kaur K. Understanding barriers, recommended solutions, and future prospects for the diagnosis and management of Pythium insidiosum keratitis. Indian journal of ophthalmology. 2023 Dec 1:71(12):3584-3586. doi: 10.4103/IJO.IJO_1041_23. Epub 2023 Nov 20 [PubMed PMID: 37991287]
Level 3 (low-level) evidenceGurnani B, Kaur K. Leap forward in clinical and photographic diagnosis of Pythium insidiosum keratitis. Indian journal of ophthalmology. 2023 Sep:71(9):3263-3264. doi: 10.4103/IJO.IJO_355_23. Epub [PubMed PMID: 37602622]
Gurnani B, Kaur K, Kumar T. Commentary: Current concepts, recent updates, and future treatment options for Pythium insidiosum keratitis. Indian journal of ophthalmology. 2023 May:71(5):1874-1876. doi: 10.4103/IJO.IJO_80_23. Epub [PubMed PMID: 37203047]
Level 3 (low-level) evidenceGurnani B, Kaur K. Predicting Prognosis Based on Regional Prevalence, Ulcer Morphology and Treatment Strategy in Vision-Threatening Pythium insidiosum Keratitis. Clinical ophthalmology (Auckland, N.Z.). 2023:17():1307-1314. doi: 10.2147/OPTH.S412274. Epub 2023 May 5 [PubMed PMID: 37181081]
Gurnani B, Christy J, Kaur K, Moutappa F, Gubert J. Successful Management of Pythium insidiosum Keratitis Masquerading as Dematiaceous Fungal Keratitis in an Immunosuppressed Asian Male. Ocular immunology and inflammation. 2024 Jul:32(5):583-586. doi: 10.1080/09273948.2023.2179495. Epub 2023 Feb 22 [PubMed PMID: 36812410]
Gurnani B, Kaur K, Agarwal S, Lalgudi VG, Shekhawat NS, Venugopal A, Tripathy K, Srinivasan B, Iyer G, Gubert J. Pythium insidiosum Keratitis: Past, Present, and Future. Ophthalmology and therapy. 2022 Oct:11(5):1629-1653. doi: 10.1007/s40123-022-00542-7. Epub 2022 Jul 5 [PubMed PMID: 35788551]
Gurnani B, Kaur K. Comment on: Sensitivity and specificity of potassium hydroxide and calcofluor white stain to differentiate between fungal and Pythium filaments in corneal scrapings from patients of Pythium keratitis. Indian journal of ophthalmology. 2022 Jun:70(6):2204. doi: 10.4103/ijo.IJO_345_22. Epub [PubMed PMID: 35648022]
Level 3 (low-level) evidenceGurnani B, Kaur K, Venugopal A, Srinivasan B, Bagga B, Iyer G, Christy J, Prajna L, Vanathi M, Garg P, Narayana S, Agarwal S, Sahu S. Pythium insidiosum keratitis - A review. Indian journal of ophthalmology. 2022 Apr:70(4):1107-1120. doi: 10.4103/ijo.IJO_1534_21. Epub [PubMed PMID: 35325996]
Gurnani B, Christy J, Narayana S, Rajkumar P, Kaur K, Gubert J. Retrospective multifactorial analysis of Pythium keratitis and review of literature. Indian journal of ophthalmology. 2021 May:69(5):1095-1101. doi: 10.4103/ijo.IJO_1808_20. Epub [PubMed PMID: 33913840]
Level 2 (mid-level) evidenceGurnani B, Narayana S, Christy J, Rajkumar P, Kaur K, Gubert J. Successful management of pediatric pythium insidiosum keratitis with cyanoacrylate glue, linezolid, and azithromycin: Rare case report. European journal of ophthalmology. 2022 Sep:32(5):NP87-NP91. doi: 10.1177/11206721211006564. Epub 2021 Mar 28 [PubMed PMID: 33779337]
Level 3 (low-level) evidenceLu SH, Qiao DN, Dong PF. A nursing report on a corneal contact lens wearer receiving keratoplasty due to corneal ulcer and perforation caused by Pythium insidiosum infection: A case report. Medicine. 2024 Apr 5:103(14):e37663. doi: 10.1097/MD.0000000000037663. Epub [PubMed PMID: 38579080]
Level 2 (mid-level) evidenceBadenoch PR, Mills RA, Chang JH, Sadlon TA, Klebe S, Coster DJ. Pythium insidiosum keratitis in an Australian child. Clinical & experimental ophthalmology. 2009 Nov:37(8):806-9. doi: 10.1111/j.1442-9071.2009.02135.x. Epub [PubMed PMID: 19878227]
Mendoza L, Taylor JW, Walker ED, Vilela R. Description of three novel Lagenidium (Oomycota) species causing infection in mammals. Revista iberoamericana de micologia. 2016 Apr-Jun:33(2):83-91. doi: 10.1016/j.riam.2015.07.005. Epub 2016 Feb 28 [PubMed PMID: 26924580]
Thanathanee O, Bhoomibunchoo C, Anutarapongpan O, Suwan-Apichon O, Charoensuk K, Chindamporn A. Role of Immunotherapy in Pythium insidiosum Keratitis. The American journal of tropical medicine and hygiene. 2022 Jul 13:107(1):110-112. doi: 10.4269/ajtmh.22-0015. Epub 2022 Jun 6 [PubMed PMID: 35895358]
Hou H, Wang Y, Tian L, Wang F, Sun Z, Chen Z. Pythium insidiosum keratitis reported in China, raising the alertness to this fungus-like infection: a case series. Journal of medical case reports. 2021 Dec 17:15(1):619. doi: 10.1186/s13256-021-03189-3. Epub 2021 Dec 17 [PubMed PMID: 34915928]
Level 2 (mid-level) evidenceYe Y, Pandey A, Bawden C, Sumsuzzman DM, Rajput R, Shoukat A, Singer BH, Moghadas SM, Galvani AP. Integrating artificial intelligence with mechanistic epidemiological modeling: a scoping review of opportunities and challenges. Nature communications. 2025 Jan 10:16(1):581. doi: 10.1038/s41467-024-55461-x. Epub 2025 Jan 10 [PubMed PMID: 39794317]
Level 2 (mid-level) evidenceOng HS, Sharma N, Phee LM, Mehta JS. Atypical microbial keratitis. The ocular surface. 2023 Apr:28():424-439. doi: 10.1016/j.jtos.2021.11.001. Epub 2021 Nov 10 [PubMed PMID: 34768003]
Zhang XY, Qi XL, Lu XH, Gao H. [Clinical features and treatment prognoses of Pythium keratitis]. [Zhonghua yan ke za zhi] Chinese journal of ophthalmology. 2021 Aug 11:57(8):589-594. doi: 10.3760/cma.j.cn112142-20201023-00703. Epub [PubMed PMID: 34344119]
Level 2 (mid-level) evidenceMalech HL, Deleo FR, Quinn MT. The role of neutrophils in the immune system: an overview. Methods in molecular biology (Clifton, N.J.). 2014:1124():3-10. doi: 10.1007/978-1-62703-845-4_1. Epub [PubMed PMID: 24504942]
Level 3 (low-level) evidenceHu L, Huang X, Yee NH, Meng H, Jiang L, Liang L, Chen X. Pythium insidiosum: an emerging pathogen that is easily misdiagnosed and given treatment as a fungus. Frontiers in cellular and infection microbiology. 2024:14():1430032. doi: 10.3389/fcimb.2024.1430032. Epub 2024 Aug 29 [PubMed PMID: 39268488]
Puangsricharern V, Chotikkakamthorn P, Tulvatana W, Kittipibul T, Chantaren P, Reinprayoon U, Kasetsuwan N, Satitpitakul V, Worasilchai N, Chindamporn A. Clinical Characteristics, Histopathology, and Treatment Outcomes of Pythium Keratitis: A Retrospective Cohort Study. Clinical ophthalmology (Auckland, N.Z.). 2021:15():1691-1701. doi: 10.2147/OPTH.S303721. Epub 2021 Apr 23 [PubMed PMID: 33935486]
Level 2 (mid-level) evidenceGurnani B, Kaur K. Navigating the challenges of infective keratitis: A critical analysis of treatment and diagnostic approaches. Indian journal of ophthalmology. 2024 Aug 1:72(8):1227-1228. doi: 10.4103/IJO.IJO_706_24. Epub 2024 Jul 29 [PubMed PMID: 39078975]
Ahmad B, Gurnani B, Patel BC. Herpes Simplex Keratitis. StatPearls. 2026 Jan:(): [PubMed PMID: 31424862]
Maghsoudlou P, Sood G, Gurnani B, Akhondi H. Cornea Transplantation. StatPearls. 2026 Jan:(): [PubMed PMID: 30969512]
Tarnawski L, Olofsson PS. Inflammation neuroscience: neuro-immune crosstalk and interfaces. Clinical & translational immunology. 2021:10(11):e1352. doi: 10.1002/cti2.1352. Epub 2021 Oct 31 [PubMed PMID: 34754449]
Espana EM, Birk DE. Composition, structure and function of the corneal stroma. Experimental eye research. 2020 Sep:198():108137. doi: 10.1016/j.exer.2020.108137. Epub 2020 Jul 11 [PubMed PMID: 32663498]
Gurnani B, Kaur K. Comment on: Online survey on practice patterns in the treatment of corneal ulcer during COVID-19 pandemic. Indian journal of ophthalmology. 2022 Apr:70(4):1436-1437. doi: 10.4103/ijo.IJO_3153_21. Epub [PubMed PMID: 35326080]
Level 3 (low-level) evidenceBera K, Schalper KA, Rimm DL, Velcheti V, Madabhushi A. Artificial intelligence in digital pathology - new tools for diagnosis and precision oncology. Nature reviews. Clinical oncology. 2019 Nov:16(11):703-715. doi: 10.1038/s41571-019-0252-y. Epub 2019 Aug 9 [PubMed PMID: 31399699]
Gurnani B, Kaur K. Therapeutic Keratoplasty. StatPearls. 2026 Jan:(): [PubMed PMID: 37276297]
Prasad P, Khair AMB, Saeed M, Shetty N. Artificial Intelligence in Histopathology. Journal of pharmacy & bioallied sciences. 2024 Dec:16(Suppl 5):S4226-S4229. doi: 10.4103/jpbs.jpbs_727_24. Epub 2025 Jan 30 [PubMed PMID: 40061791]
Paulbuddhe V, Addya S, Gurnani B, Singh D, Tripathy K, Chawla R. Sympathetic Ophthalmia: Where Do We Currently Stand on Treatment Strategies? Clinical ophthalmology (Auckland, N.Z.). 2021:15():4201-4218. doi: 10.2147/OPTH.S289688. Epub 2021 Oct 20 [PubMed PMID: 34707340]
Gurnani B, Kaur K. Post-market surveillance of ophthalmic implants: role of real-world evidence. Expert review of medical devices. 2025 Dec:22(12):1303-1308. doi: 10.1080/17434440.2025.2579578. Epub 2025 Oct 24 [PubMed PMID: 41123186]
Behera HS, Barik MR, Das S, Sharma S. Simple polymerase chain reaction assay to differentiate between fungal and Pythium insidiosum keratitis. Clinical & experimental ophthalmology. 2021 Aug:49(6):630-632. doi: 10.1111/ceo.13939. Epub 2021 May 18 [PubMed PMID: 33931931]
Nonpassopon M, Jongkhajornpong P, Aroonroch R, Koovisitsopit A, Lekhanont K. Predisposing Factors, Clinical Presentations, and Outcomes of Contact Lens-Related Pythium Keratitis. Cornea. 2021 Nov 1:40(11):1413-1419. doi: 10.1097/ICO.0000000000002651. Epub [PubMed PMID: 33470674]
Gurnani B, Kaur K. Response to letter regarding "Evaluating the novel role of ChatGPT-4 in addressing corneal ulcer queries: An AI-powered insight". European journal of ophthalmology. 2025 Jul 9:():11206721251357376. doi: 10.1177/11206721251357376. Epub 2025 Jul 9 [PubMed PMID: 40629931]
Level 3 (low-level) evidenceChatterjee S, Agrawal D, Gomase SN. Clinical differentiation of Pythium keratitis from fungal keratitis and development of a scoring system. Indian journal of ophthalmology. 2022 Oct:70(10):3515-3521. doi: 10.4103/ijo.IJO_870_22. Epub [PubMed PMID: 36190038]
Sharma S, Kunimoto DY, Gopinathan U, Athmanathan S, Garg P, Rao GN. Evaluation of corneal scraping smear examination methods in the diagnosis of bacterial and fungal keratitis: a survey of eight years of laboratory experience. Cornea. 2002 Oct:21(7):643-7 [PubMed PMID: 12352078]
Level 3 (low-level) evidenceWu H, Ye X, Jiang Y, Tian H, Yang K, Cui C, Shi S, Liu Y, Huang S, Chen J, Xu J, Dong F. A Comparative Study of Multiple Deep Learning Models Based on Multi-Input Resolution for Breast Ultrasound Images. Frontiers in oncology. 2022:12():869421. doi: 10.3389/fonc.2022.869421. Epub 2022 Jul 7 [PubMed PMID: 35875151]
Level 2 (mid-level) evidenceNishant P, Gurnani B, Singh P, Sinha S, Kaur K, Kumar A, Sinha RK. Current concepts and recent trends in endothelial keratoplasty. World journal of transplantation. 2025 Jun 18:15(2):102507. doi: 10.5500/wjt.v15.i2.102507. Epub [PubMed PMID: 40535500]
Gurnani B, Somani AN, Moshirfar M, Patel BC. Fuchs Endothelial Dystrophy. StatPearls. 2026 Jan:(): [PubMed PMID: 31424832]
Gurnani B, Feroze KB, Patel BC. Neurotrophic Keratitis. StatPearls. 2026 Jan:(): [PubMed PMID: 28613758]
Guarner J, Brandt ME. Histopathologic diagnosis of fungal infections in the 21st century. Clinical microbiology reviews. 2011 Apr:24(2):247-80. doi: 10.1128/CMR.00053-10. Epub [PubMed PMID: 21482725]
Alruwaili M, Mohamed M. An Integrated Deep Learning Model with EfficientNet and ResNet for Accurate Multi-Class Skin Disease Classification. Diagnostics (Basel, Switzerland). 2025 Feb 25:15(5):. doi: 10.3390/diagnostics15050551. Epub 2025 Feb 25 [PubMed PMID: 40075797]
Burrow MK, Gurnani B, Patel BC. Keratoconjunctivitis. StatPearls. 2026 Jan:(): [PubMed PMID: 31194419]
Agarwal H, Gurnani B, Pippal B, Jain N. Capturing the micro-communities: Insights into biogenesis and architecture of bacterial biofilms. BBA advances. 2025:7():100133. doi: 10.1016/j.bbadva.2024.100133. Epub 2024 Dec 21 [PubMed PMID: 39839441]
Level 3 (low-level) evidenceHoffman J, Yadav R, Ebong A, Arunga S, Leck A. Managing microbial keratitis in resource-limited settings. Community eye health. 2024:37(124):11-14 [PubMed PMID: 40115630]
Hung N, Shih AK, Lin C, Kuo MT, Hwang YS, Wu WC, Kuo CF, Kang EY, Hsiao CH. Using Slit-Lamp Images for Deep Learning-Based Identification of Bacterial and Fungal Keratitis: Model Development and Validation with Different Convolutional Neural Networks. Diagnostics (Basel, Switzerland). 2021 Jul 12:11(7):. doi: 10.3390/diagnostics11071246. Epub 2021 Jul 12 [PubMed PMID: 34359329]
Level 1 (high-level) evidenceKulandai LT, Lakshmipathy D, Sargunam J. Novel Duplex Polymerase Chain Reaction for the Rapid Detection of Pythium insidiosum Directly From Corneal Specimens of Patients With Ocular Pythiosis. Cornea. 2020 Jun:39(6):775-778. doi: 10.1097/ICO.0000000000002284. Epub [PubMed PMID: 32118672]
Permpalung N, Worasilchai N, Chindamporn A. Human Pythiosis: Emergence of Fungal-Like Organism. Mycopathologia. 2020 Oct:185(5):801-812. doi: 10.1007/s11046-019-00412-0. Epub 2019 Dec 16 [PubMed PMID: 31845178]
Maeno S, Oie Y, Sunada A, Tanibuchi H, Hagiwara S, Makimura K, Nishida K. Successful medical management of Pythium insidiosum keratitis using a combination of minocycline, linezolid, and chloramphenicol. American journal of ophthalmology case reports. 2019 Sep:15():100498. doi: 10.1016/j.ajoc.2019.100498. Epub 2019 Jun 18 [PubMed PMID: 31289761]
Level 3 (low-level) evidenceBernheim D, Dupont D, Aptel F, Dard C, Chiquet C, Normand AC, Piarroux R, Cornet M, Maubon D. Pythiosis: Case report leading to new features in clinical and diagnostic management of this fungal-like infection. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases. 2019 Sep:86():40-43. doi: 10.1016/j.ijid.2019.06.011. Epub 2019 Jun 15 [PubMed PMID: 31212104]
Level 3 (low-level) evidenceAppavu SP, Prajna L, Rajapandian SGK. Genotyping and phylogenetic analysis of Pythium insidiosum causing human corneal ulcer. Medical mycology. 2020 Feb 1:58(2):211-218. doi: 10.1093/mmy/myz044. Epub [PubMed PMID: 31073609]
Gurnani B, Kaur K. Bacterial Keratitis. StatPearls. 2026 Jan:(): [PubMed PMID: 34662023]
Chang WH, Kuo YW, Hou YC. Optimizing early diagnosis and treatment of acanthamoeba keratitis through corneal scraping. Journal of optometry. 2026 Jan-Mar:19(1):100566. doi: 10.1016/j.optom.2025.100566. Epub 2025 Oct 15 [PubMed PMID: 41102075]
Gurnani B, Moshirfar M. Nocardia Keratitis. StatPearls. 2026 Jan:(): [PubMed PMID: 31751092]
Mohseni M, Gurnani B, Blair K. Blunt Eye Trauma. StatPearls. 2026 Jan:(): [PubMed PMID: 29261988]
Reinprayoon U, Permpalung N, Kasetsuwan N, Plongla R, Mendoza L, Chindamporn A. Lagenidium sp. ocular infection mimicking ocular pythiosis. Journal of clinical microbiology. 2013 Aug:51(8):2778-80. doi: 10.1128/JCM.00783-13. Epub 2013 Jun 5 [PubMed PMID: 23740721]
Sharma S, Balne PK, Motukupally SR, Das S, Garg P, Sahu SK, Arunasri K, Manjulatha K, Mishra DK, Shivaji S. Pythium insidiosum keratitis: clinical profile and role of DNA sequencing and zoospore formation in diagnosis. Cornea. 2015 Apr:34(4):438-42. doi: 10.1097/ICO.0000000000000349. Epub [PubMed PMID: 25738236]
Hudu SA, Alshrari AS, Abu-Shoura EJI, Osman A, Jimoh AO. A Critical Review of the Prospect of Integrating Artificial Intelligence in Infectious Disease Diagnosis and Prognosis. Interdisciplinary perspectives on infectious diseases. 2025:2025():6816002. doi: 10.1155/ipid/6816002. Epub 2025 Mar 6 [PubMed PMID: 40225950]
Level 3 (low-level) evidenceAsan O, Bayrak AE, Choudhury A. Artificial Intelligence and Human Trust in Healthcare: Focus on Clinicians. Journal of medical Internet research. 2020 Jun 19:22(6):e15154. doi: 10.2196/15154. Epub 2020 Jun 19 [PubMed PMID: 32558657]
Permpalung N, Worasilchai N, Plongla R, Upala S, Sanguankeo A, Paitoonpong L, Mendoza L, Chindamporn A. Treatment outcomes of surgery, antifungal therapy and immunotherapy in ocular and vascular human pythiosis: a retrospective study of 18 patients. The Journal of antimicrobial chemotherapy. 2015:70(6):1885-92. doi: 10.1093/jac/dkv008. Epub 2015 Jan 27 [PubMed PMID: 25630647]
Level 2 (mid-level) evidencePermpalung N, Worasilchai N, Manothummetha K, Torvorapanit P, Ratanawongphaibul K, Chuleerarux N, Plongla R, Chindamporn A. Clinical outcomes in ocular pythiosis patients treated with a combination therapy protocol in Thailand: A prospective study. Medical mycology. 2019 Nov 1:57(8):923-928. doi: 10.1093/mmy/myz013. Epub [PubMed PMID: 30805615]
Level 2 (mid-level) evidenceBalasubramaniam B, Chong YJ, Azzopardi M, Logeswaran A, Denniston AK. Topical Anti-Inflammatory Agents for Non-Infectious Uveitis: Current Treatment and Perspectives. Journal of inflammation research. 2022:15():6439-6451. doi: 10.2147/JIR.S288294. Epub 2022 Nov 28 [PubMed PMID: 36467992]
Level 3 (low-level) evidenceTanphaichitra D. Tropical disease in the immunocompromised host: melioidosis and pythiosis. Reviews of infectious diseases. 1989 Nov-Dec:11 Suppl 7():S1629-43 [PubMed PMID: 2602781]
Loftus TJ, Tighe PJ, Filiberto AC, Efron PA, Brakenridge SC, Mohr AM, Rashidi P, Upchurch GR Jr, Bihorac A. Artificial Intelligence and Surgical Decision-making. JAMA surgery. 2020 Feb 1:155(2):148-158. doi: 10.1001/jamasurg.2019.4917. Epub [PubMed PMID: 31825465]
Tiwari A, Mishra S, Kuo TR. Current AI technologies in cancer diagnostics and treatment. Molecular cancer. 2025 Jun 2:24(1):159. doi: 10.1186/s12943-025-02369-9. Epub 2025 Jun 2 [PubMed PMID: 40457408]
Veldhuis LI, Woittiez NJC, Nanayakkara PWB, Ludikhuize J. Artificial Intelligence for the Prediction of In-Hospital Clinical Deterioration: A Systematic Review. Critical care explorations. 2022 Sep:4(9):e0744. doi: 10.1097/CCE.0000000000000744. Epub 2022 Aug 26 [PubMed PMID: 36046062]
Level 1 (high-level) evidenceFarhud DD, Zokaei S. Ethical Issues of Artificial Intelligence in Medicine and Healthcare. Iranian journal of public health. 2021 Nov:50(11):i-v. doi: 10.18502/ijph.v50i11.7600. Epub [PubMed PMID: 35223619]
Basile AO, Yahi A, Tatonetti NP. Artificial Intelligence for Drug Toxicity and Safety. Trends in pharmacological sciences. 2019 Sep:40(9):624-635. doi: 10.1016/j.tips.2019.07.005. Epub 2019 Aug 2 [PubMed PMID: 31383376]
Chu X, Wang X, Zhang C, Liu H, Li F, Li G, Zhao S. A deep learning-based model for automatic segmentation and evaluation of corneal neovascularization using slit-lamp anterior segment images. Quantitative imaging in medicine and surgery. 2023 Oct 1:13(10):6778-6788. doi: 10.21037/qims-23-99. Epub 2023 Aug 25 [PubMed PMID: 37869308]
Abbas Q, Jeong W, Lee SW. Explainable AI in Clinical Decision Support Systems: A Meta-Analysis of Methods, Applications, and Usability Challenges. Healthcare (Basel, Switzerland). 2025 Aug 29:13(17):. doi: 10.3390/healthcare13172154. Epub 2025 Aug 29 [PubMed PMID: 40941506]
Level 1 (high-level) evidenceTripathi M, Markan A, Gurnani B. Salzmann Nodular Corneal Degeneration. StatPearls. 2026 Jan:(): [PubMed PMID: 32809519]
Imwidthaya P. Human pythiosis in Thailand. Postgraduate medical journal. 1994 Aug:70(826):558-60 [PubMed PMID: 7937448]
Sapkota J, Bajracharya L, Gurung R, Rana RS. Indications and Outcomes of Repeat Keratoplasty for Graft Failure at a Tertiary Eye Care Center in Nepal. Nepalese journal of ophthalmology : a biannual peer-reviewed academic journal of the Nepal Ophthalmic Society : NEPJOPH. 2023 Jan:15(29):85-91. doi: 10.3126/nepjoph.v15i1.54803. Epub [PubMed PMID: 38975852]
Thianprasit M, Chaiprasert A, Imwidthaya P. Human pythiosis. Current topics in medical mycology. 1996 Dec:7(1):43-54 [PubMed PMID: 9504058]
Murdoch D, Parr D. Pythium insidiosum keratitis. Australian and New Zealand journal of ophthalmology. 1997 May:25(2):177-9 [PubMed PMID: 9267609]
Ichikawa K, Ono T, Chen L, Kitamoto K, Taketatni Y, Toyono T, Yoshida J, Aihara M, Miyai T. Quantitative evaluation of corneal irregularity and scarring after infectious keratitis using anterior segment optical coherence tomography. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2024 Jan:262(1):133-141. doi: 10.1007/s00417-023-06157-3. Epub 2023 Jul 20 [PubMed PMID: 37470808]
Awad R, Ghaith AA, Awad K, Mamdouh Saad M, Elmassry AA. Fungal Keratitis: Diagnosis, Management, and Recent Advances. Clinical ophthalmology (Auckland, N.Z.). 2024:18():85-106. doi: 10.2147/OPTH.S447138. Epub 2024 Jan 10 [PubMed PMID: 38223815]
Level 3 (low-level) evidenceYang CQ, Sun W, Gu YS. A clinical study of the efficacy of topical corticosteroids on dry eye. Journal of Zhejiang University. Science. B. 2006 Aug:7(8):675-8 [PubMed PMID: 16845723]
Badenoch PR, Coster DJ, Wetherall BL, Brettig HT, Rozenbilds MA, Drenth A, Wagels G. Pythium insidiosum keratitis confirmed by DNA sequence analysis. The British journal of ophthalmology. 2001 Apr:85(4):502-3 [PubMed PMID: 11302134]
Kunavisarut S, Nimvorapan T, Methasiri S. Pythium corneal ulcer in Ramathibodi Hospital. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2003 Apr:86(4):338-42 [PubMed PMID: 12757078]
Wiafe B, Jha N, Wolvaardt E, Abdull M. Improving adherence with eye medication: a patient-centred approach to prescribing. Community eye health. 2023:36(118):9-10 [PubMed PMID: 37273805]
Yang S, Rothman RE. PCR-based diagnostics for infectious diseases: uses, limitations, and future applications in acute-care settings. The Lancet. Infectious diseases. 2004 Jun:4(6):337-48 [PubMed PMID: 15172342]
Thomas PA. Current perspectives on ophthalmic mycoses. Clinical microbiology reviews. 2003 Oct:16(4):730-97 [PubMed PMID: 14557297]
Level 3 (low-level) evidencePrasertwitayakij N, Louthrenoo W, Kasitanon N, Thamprasert K, Vanittanakom N. Human pythiosis, a rare cause of arteritis: case report and literature review. Seminars in arthritis and rheumatism. 2003 Dec:33(3):204-14 [PubMed PMID: 14671729]
Level 3 (low-level) evidenceLekhanont K, Chuckpaiwong V, Chongtrakool P, Aroonroch R, Vongthongsri A. Pythium insidiosum keratitis in contact lens wear: a case report. Cornea. 2009 Dec:28(10):1173-7. doi: 10.1097/ICO.0b013e318199fa41. Epub [PubMed PMID: 19730096]
Level 3 (low-level) evidenceNizami AA, Gurnani B, Gulani AC. Cataract. StatPearls. 2026 Jan:(): [PubMed PMID: 30969521]
Kaur K, Gurnani B. Low Vision Aids. StatPearls. 2026 Jan:(): [PubMed PMID: 36256771]
Gurnani B, Kaur K. Posterior Polar Cataract. StatPearls. 2026 Jan:(): [PubMed PMID: 34662063]
Gurnani B, Kaur K. Teleophthalmology-enabled devices: bridging the gap in rural eye care. Expert review of medical devices. 2025 Nov:22(11):1167-1172. doi: 10.1080/17434440.2025.2566741. Epub 2025 Oct 15 [PubMed PMID: 40990172]
Gurnani B, Kaur K. Biosensor-embedded wearables for dry eye monitoring and management. Expert review of medical devices. 2025 Oct:22(10):1073-1079. doi: 10.1080/17434440.2025.2555485. Epub 2025 Sep 1 [PubMed PMID: 40884106]
Gurnani B, Kaur K, Chaudhary S, Gandhi AS, Balakrishnan H, Mishra C, Gosalia H, Dhiman S, Joshi S, Nagtode AH, Jain S, Aguiar M, Rustagi IM. Nystagmus in Clinical Practice: From Diagnosis to Treatment-A Comprehensive Review. Clinical ophthalmology (Auckland, N.Z.). 2025:19():1617-1657. doi: 10.2147/OPTH.S523224. Epub 2025 May 17 [PubMed PMID: 40401036]
Srinivasan M, Upadhyay MP, Priyadarsini B, Mahalakshmi R, Whitcher JP. Corneal ulceration in south-east Asia III: prevention of fungal keratitis at the village level in south India using topical antibiotics. The British journal of ophthalmology. 2006 Dec:90(12):1472-5 [PubMed PMID: 16916874]
Murugan SRB, Sanjay S, Somanath A, Mahendradas P, Patil A, Kaur K, Gurnani B. Artificial Intelligence in Uveitis: Innovations in Diagnosis and Therapeutic Strategies. Clinical ophthalmology (Auckland, N.Z.). 2024:18():3753-3766. doi: 10.2147/OPTH.S495307. Epub 2024 Dec 14 [PubMed PMID: 39703602]
Okoye GS, Bonabe D, Obasi CU, Munikrishna D, Osho F, Mutali M, Ogwumu K, Oke-Ifidon EO, Nathan IG, Enaholo ES, Suleman AI, Chukwuyem C, Enang AE, Oji RC, Ogechukwu VN, Chidera SP, Ogechukwu HC, Kaur K, Gurnani B. Visual outcomes and complications after phacoemulsification and small incision manual cataract surgery in two eye hospitals. Journal francais d'ophtalmologie. 2025 Jan:48(1):104353. doi: 10.1016/j.jfo.2024.104353. Epub 2024 Nov 18 [PubMed PMID: 39561679]
Gurnani B, Kaur K. Recent Advances in Refractive Surgery: An Overview. Clinical ophthalmology (Auckland, N.Z.). 2024:18():2467-2472. doi: 10.2147/OPTH.S481421. Epub 2024 Sep 2 [PubMed PMID: 39246558]
Level 3 (low-level) evidenceWeiner EB, Dankwa-Mullan I, Nelson WA, Hassanpour S. Ethical challenges and evolving strategies in the integration of artificial intelligence into clinical practice. PLOS digital health. 2025 Apr:4(4):e0000810. doi: 10.1371/journal.pdig.0000810. Epub 2025 Apr 8 [PubMed PMID: 40198594]
Cao B, Gonugunta VT, Radhakrishnan N, Lalitha P, Gurnani B, Kaur K, Iyer G, Agarwal S, Srinivasan B, Keenan JD, Prajna NV. Outcomes of Pythium keratitis: a meta-analysis of individual patient data. Current ophthalmology reports. 2022 Dec:10(4):198-208. doi: 10.1007/s40135-022-00302-7. Epub 2022 Nov 10 [PubMed PMID: 37250102]
Level 1 (high-level) evidence