 Low Back Pain: Evaluation and Management
Low Back Pain: Evaluation and Management
Introduction
Back pain is one of the most common reasons for primary- and emergency-care consultations. An estimated $200 billion is spent annually on managing back pain. Additionally, work hours, productivity, and workers' compensation are greatly reduced due to this condition.[1]
Back pain arises from a broad range of causes in adults and children, though most are mechanical in nature or have a nonspecific origin. Mechanical back pain comprises 90% of cases, so health providers can easily miss rare causes while focusing on common etiologies.[2][3]
Identifying red flags and determining the appropriate treatment are the most important aspects of back pain management. Most cases may be treated conservatively. Association with alarming signs, such as nerve dysfunction, warrants a thorough investigation and an interprofessional approach.[4]
Pharmacological treatments include pain relievers targeting peripheral and central neurologic pathways, as well as muscle relaxants.[5] Various forms of physical therapy are available for individuals who prefer nonpharmacological approaches or are recovering from injuries.[6] Acupuncture is an alternative therapy shown to improve back pain moderately. Surgery is reserved for cases that are accompanied by severe nerve dysfunction, have resulted from serious causes such as malignancy, or manifest with refractory symptoms due to structural causes, such as spondylolisthesis.[7][8] Significant back pain that does not resolve within 6 weeks of adequate conservative management may warrant imaging with radiography, computed tomography (CT), or magnetic resonance imaging (MRI).
A thorough evaluation helps determine the cause of back pain and develop a tailored therapeutic plan. Addressing the underlying pathology significantly improves patients' functional capacity and quality of life.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Back pain arises from various conditions, which may be classified into the following:
- Traumatic: Results from direct or indirect contact with an external force. Examples include whiplash injury, strain, and traumatic fractures.
- Degenerative: Musculoskeletal structures weaken over time due to aging, overuse, or preexisting pathology. Examples include intervertebral disc herniation and degenerative disc disease (see Image. Degenerative Disc Disease with Vacuum Phenomenon).
- Oncologic: Primary or secondary malignant lesions can develop in back structures. Pathologic fractures of the axial skeleton may occur as complications.
- Infectious: Infections of musculoskeletal structures may arise from direct inoculation or hematogenous spread.
- Inflammatory: Includes noninfectious, nonmalignant conditions. Examples are ankylosing spondylitis and sacroiliitis. Chronic inflammation may result in spinal arthritis.
- Metabolic: Disorders of calcium and bone metabolism can cause symptoms. Examples encompass osteoporosis and osteosclerosis.
- Vascular: Acute or chronic aortic dissection can present as tearing back pain, usually with abrupt onset and associated cardiovascular risk factors (Source: Zakko and Reece, 2024).
- Referred pain: Visceral organ pathology may produce referred back pain. Examples include biliary colic, lung disease, and aortic or vertebral artery disorders.
- Postural: Prolonged upright posture can contribute to back pain. Pregnancy and certain occupations increase risk.
- Congenital: Inborn axial skeleton conditions can cause symptoms. Examples include kyphoscoliosis and a tethered spinal cord.
- Psychiatric: Chronic pain syndromes and mental health conditions may present with back pain. Malingering may contribute to symptom amplification or inconsistent clinical findings.[9]
The duration of symptoms is important, as acute and chronic back pain often have different etiologies. A thorough clinical evaluation and appropriate diagnostic testing are usually sufficient to determine the cause. Referral to specialists, such as neurosurgeons, orthopedic spine surgeons, neurologists, rheumatologists, physiatrists, or pain management providers, may be necessary for further evaluation and treatment planning.
Epidemiology
Back pain is widespread among adults. Studies report that up to 23% of adults worldwide experience chronic low back pain, with 1-year recurrence rates ranging from 24% to 80%.[10][11] The lifetime prevalence of back pain in adults may reach 84%.[12]
Back pain is less common in pediatric populations. A Scandinavian study found that point prevalence was approximately 1% among 12-year-olds and 5% among 15-year-olds. By age 18 for girls and 20 for boys, 50% of adolescents will have experienced at least 1 episode of back pain.[13] Lifetime prevalence in adolescents increases progressively with age, approaching adult levels by 18.[14]
Pathophysiology
Mechanical back pain develops when nociceptive elements within the spinal motion segment or adjacent soft tissues undergo overload or structural disruption. Acute episodes typically reflect sprain or strain of paraspinal musculature and supporting ligaments after a loaded segment is driven into excessive flexion, extension, or rotation. Eccentric contraction produces microscopic tearing near the myotendinous junction, followed by edema, inflammatory mediator release, and reflex spasm that sensitize local nociceptors and restrict segmental motion.
Chronic mechanical pain more frequently arises from degenerative intervertebral disc changes. Cumulative mechanical loading and endplate injury promote annular fissuring, proteoglycan loss, disc dehydration, and progressive collapse. The structurally compromised disc demonstrates abnormal load transfer, pathologic ingrowth of nociceptive nerve fibers and blood vessels, and heightened production of proinflammatory mediators, generating discogenic pain or radiculopathy.[15]
Lumbar zygapophyseal (facet) joints, as synovial joints with richly innervated capsules, bear substantial axial load during extension. Repetitive shear and compression promote cartilage loss, osteophyte formation, capsular laxity or hypertrophy, and localized inflammation. Resulting capsular stretch or distension activates high- and low-threshold mechanoreceptors and nociceptors, producing referred pain to the back or buttocks. Persistent peripheral nociceptive drive from these structures may, in some cases, induce central sensitization and facilitate the transition from acute to chronic pain.[16]
History and Physical
Determining the cause of back pain begins with a thorough history and physical examination. The onset of pain should be established early. Acute back pain, defined as back pain lasting less than 6 weeks, most often reflects mechanical strain or degenerative changes and less commonly results from trauma or abrupt progression of serious underlying disease such as malignancy. Chronic cases, lasting longer than 12 weeks, may involve mechanical dysfunction or arise from longstanding conditions.
Information regarding factors that provoke or alleviate the pain must be obtained. In addition to providing diagnostic clues, understanding these factors guides the clinician in selecting appropriate pain management strategies.
Pain quality assists in distinguishing visceral from nonvisceral sources. Well-localized pain often indicates an organic process. Any associated symptoms may offer additional insights into the underlying cause of back pain.
Other pertinent information may be obtained from the patient’s medical, family, occupational, and social history. For example, a history of prior cancer chemotherapy should raise suspicion for metastasis or a secondary tumor. Certain autoimmune arthritides have a hereditary component. Pott disease, or spinal tuberculosis, may result from exposure in regions where tuberculosis is endemic. Prolonged sitting during work can contribute to both acute and chronic back pain.
A focused physical examination should include inspection, auscultation, palpation, and provocative maneuvers. Visual inspection of the back may not reveal the cause unless deformity, signs of inflammation, or skin lesions are present. Auscultation is useful when back pain may be secondary to pulmonary pathology. Palpation can elicit localized musculoskeletal tenderness and help identify affected structures.
Certain provocative maneuvers can provide diagnostic clues regarding the cause of back pain. The straight-leg-raising (SLR) test is useful for diagnosing lumbar disc herniation. The test is performed by raising the patient’s leg to 30° to 70°. A result is considered positive if ipsilateral leg pain occurs at less than 60°. The crossed SLR test involves raising the contralateral leg and is more specific than a standard SLR for identifying a disc herniation.[17][18]
The Stork test, which evaluates for spondylolysis, is another clinically used maneuver. The examiner supports the patient while they stand on a leg and hyperextend their back. The maneuver is repeated on the opposite leg. The test result is positive if the patient experiences pain during hyperextension. The Adam test is used to evaluate scoliosis. The patient bends forward with feet together, arms extended, and palms touching. An examiner standing in front can detect a thoracic prominence in patients with scoliosis.[19] Assessment of range of motion, limb strength, deep tendon reflexes, and sensation aids in evaluating the integrity of both musculoskeletal and neurologic systems.
Red flags identified during history or physical examination warrant imaging and additional diagnostic testing. The signs explained below should be carefully monitored.
In adults, red flags for back pain include a history of metastatic cancer or unexplained weight loss, with focal tenderness to palpation in the presence of risk factors suggesting malignancy. Infection should be suspected in patients with recent spinal procedures, intravenous drug use, immunosuppression, or prior lumbar surgery, especially if fever, spinal wounds, localized pain, or tenderness is present.
A systematic review of 40 observational studies demonstrated that individual red flags possess limited standalone diagnostic accuracy for serious thoracolumbar pathology and frequently generate high rates of false positive results. Vertebral fractures accounted for 0.4% to 5.6% of low back pain presentations. Posttest probabilities increased substantially only when advanced age, recent trauma, prolonged corticosteroid use, and female sex occurred collectively rather than independently.
For spinal malignancy, the most informative red flags included a prior history of cancer, unexplained weight loss, persistent pain without improvement, and concerning overall clinical judgment. In contrast, isolated night pain or broad age thresholds produced numerous false positives. Across vertebral fracture, malignancy, infection, and cauda equina syndrome, diagnostic prediction models that integrated multiple red flags consistently demonstrated higher likelihood ratios than any single historical feature or physical examination finding.[20]
Symptoms suggestive of cauda equina syndrome require immediate recognition, as this condition constitutes a surgical emergency. New urinary retention, difficulty initiating micturition, bowel dysfunction, or sensory loss in the perineal or perianal region (“saddle anesthesia”) are key historical features. Bilateral sciatica, rapidly escalating leg pain, or new bilateral lower-extremity weakness further heighten concern, and the constellation of these findings indicates severe compression of the cauda equina nerve roots. Such presentations are strongly associated with massive midline disc herniation or other space-occupying lesions and demand urgent evaluation to prevent permanent neurologic deficit.
Fracture risk increases with significant trauma, prolonged corticosteroid use, osteoporosis, or age over 70, and may be indicated by contusions, abrasions, or tenderness over spinous processes. Neurologic compromise is suggested by progressive motor or sensory loss, new urinary or fecal incontinence, saddle anesthesia, anal sphincter atony, or significant motor deficits across multiple myotomes.[21][22]
A focused neurological history should assess bladder and bowel function and document any perineal or perianal sensory loss, as these features suggest possible cauda equina or conus medullaris involvement. The neurological examination should include motor testing of key lumbosacral myotomes—hip flexion, knee extension, ankle dorsiflexion, ankle plantar flexion, great-toe extension, and foot eversion—to identify focal weakness patterns that correlate with specific nerve root compression.
In pediatric patients, malignancy should be considered in children who are younger than 4 years or experience nighttime pain, particularly when focal tenderness is present. Infection risk increases in children who are younger than 4, report nighttime pain, or have a history of tuberculosis exposure, especially if fever, spinal wounds, or localized tenderness occurs. Inflammatory causes are suggested by morning stiffness lasting more than 30 minutes, improving with activity or heat, accompanied by a limited range of motion and localized tenderness. Fractures may result from repetitive lumbar hyperextension during sports, with tenderness over spinous processes or a positive Stork test result.[23][24]
Recent recommendations for children and adolescents consolidate red flag features that warrant evaluation for specific spinal disease. Concerning findings include age younger than 10 years, significant trauma, prior or current glucocorticoid therapy, motor or sensory deficits, radicular pain, bladder or bowel dysfunction, fever, lymphadenopathy, structural deformity, and focal compression tenderness.
The same publication identifies evidence-based risk factors for nonspecific pediatric back pain. Increasing age in adolescence, female sex, high levels of sports participation, prior pain episodes, and psychosocial factors—such as low life satisfaction, anxiety, and depression—demonstrate strong associations, and several additional contributors also predict a chronic course. Incorporation of these red and yellow flags into routine pediatric history taking assists in distinguishing children who require prompt imaging or specialty referral from those who are suitable for initial conservative management and observation.[25]
Four-Category Diagnostic Framework for Back Pain
During the initial history and physical examination, back pain presentations can be organized into 4 diagnostic groups that direct subsequent evaluation and management:
- Nonspecific mechanical pain
- Pain arising from radiculopathy or spinal stenosis
- Pain referred from nonspinal sources
- Pain associated with specific or nonmechanical spinal pathology, including infection, fracture, inflammatory disease, or malignancy [26][27]
This diagnostic framework clarifies the likely source of pain and prioritizes the most appropriate investigative pathway. Correct classification ensures that high-risk conditions receive urgent evaluation, while stable cases proceed with conservative care.
Evaluation
History and physical examination are sufficient to determine the cause of back pain in most cases. Early imaging in adults has been associated with poorer outcomes, as it often leads to more invasive interventions that provide minimal benefit.[28][29] Similar findings are reported in pediatric populations.
Fewer than 5% to 10% of low back pain presentations result from specific spinal pathology, whereas 90% to 95% reflect nonspecific mechanical pain suitable for conservative management without routine imaging. Degenerative changes, including disc degeneration, disc bulging, and facet arthropathy, are highly prevalent in asymptomatic adults (see Image. Facet Arthropathy). Disc degeneration occurs in more than 80% of adults older than 50. Therefore, imaging findings must be interpreted cautiously and within the clinical context.[30]
Nevertheless, the presence of concerning signs warrants diagnostic evaluation. In adults, imaging is indicated for back pain persisting longer than 6 weeks despite appropriate conservative management. In children, imaging is recommended for continuous pain lasting more than 4 weeks.
Plain anteroposterior and lateral films of the axial skeleton can detect bone pathology (see Image. Multiple Myeloma Involving the Spine). MRI is indicated for the evaluation of soft tissue lesions, including nerves, intervertebral discs, and tendons. Both imaging modalities can identify signs of malignancy and inflammation, but MRI is preferred when soft tissues are involved.[31][32]
Bone scans may demonstrate osteomyelitis, discitis, and stress reactions but are inferior to MRI for assessing these conditions.[33] Single-photon emission computed tomography–CT (SPECT-CT) can aid diagnosis when MRI results are inconclusive, particularly in patients with prior spinal instrumentation, but it is not recommended as a primary imaging modality.[34] CT or magnetic resonance angiography should be performed in cases of suspected aortic dissection (see Image. Type B Aortic Dissection on Computed Tomography Angiography).[35] (Source: Alexiou and Sritharan, 2025) Adolescents with MRI evidence of disc herniation may require a CT scan to confirm or exclude apophyseal ring separation, which occurs in approximately 5.7% of these patients.[36]
Electromyography or nerve conduction studies are indicated in patients with prior spinal surgery who may present with radiculopathy or plexopathy. Image-guided diagnostic injections can help confirm sacroiliac joint disease.
Laboratory evaluation may be necessary in selected cases of back pain. Rheumatologic assays, including human leukocyte antigen B27, antinuclear antibody, rheumatoid factor, and Lyme antibodies, are generally nonspecific and not routinely helpful.[37][38] Inflammatory markers, such as C-reactive protein and erythrocyte sedimentation rate, can provide clinically useful information.[39] A complete blood count and blood cultures may aid in diagnosing inflammatory, infectious, or malignant processes. Elevated lactate dehydrogenase and uric acid levels are frequently observed in conditions associated with rapid marrow turnover, such as leukemia.[40]
Applying the Four-Category Model to Guide Testing and Management
The diagnostic evaluation can be structured according to the 4-category framework. In patients with nonspecific low back pain and absence of red flag features, imaging is typically deferred for 1 to 2 months, as early radiography does not improve outcomes and often reveals incidental findings that do not alter management. When history or examination indicates specific spinal pathology, such as radiculopathy or spinal stenosis, MRI may be employed to confirm neural compression and guide interventional or surgical planning (see Image. Degenerative Spondylolisthesis with Lumbar Spinal Stenosis). Features suggestive of a nonspinal source—eg, gastrointestinal, genitourinary, vascular, or gynecologic—prompt targeted evaluation of the relevant organ system rather than spine-focused studies.
Laboratory testing and more extensive imaging, often expedited, are reserved for the nonmechanical spinal category. Clues such as fever, night pain, unexplained weight loss, persistent rest pain, or progressive neurologic deficit raise suspicion for infection, malignancy, or inflammatory spondyloarthropathy and justify erythrocyte sedimentation rate or C-reactive protein testing, complete blood count, and early MRI. Application of this structured approach allows conservative management for most patients with nonspecific pain while ensuring timely identification of specific spinal, nonspinal, or systemic pathology requiring intensive evaluation.
Treatment / Management
Adult and pediatric back pain require distinct management strategies. Many cases have an unidentifiable cause, although degenerative disease and musculoskeletal injury are more prevalent in adults. Overuse and muscle strain are more common precipitants in children and adolescents. Rare etiologies, including malignancy and metabolic disorders, manifest differently across age groups. Consequently, treatment must be tailored to both the underlying condition and the patient’s age.
Management of Back Pain in Adults
Serious conditions must be excluded initially for acute back pain in adults. The patient should be reassured and provided with symptomatic relief if no indications for further testing are present. The 1st-line management is nonpharmacological and includes early return to normal routines, except for heavy labor, avoidance of pain-provoking activities, and patient education.
Second-line options may include the administration of nonsteroidal anti-inflammatory drugs (NSAIDs), muscle relaxants, or opioids, spinal manipulation, physical therapy, superficial heat application, and alternative treatments such as acupuncture or massage. Education regarding the potential causes of back pain should be individualized to each patient’s circumstances, as it plays a critical role in preventing symptom aggravation or recurrence. Follow-up is typically recommended after 2 weeks, with resumption of normal activities encouraged if the patient is asymptomatic at that time.
In adult patients with acute back pain with radiculopathy, management may include NSAID therapy, exercise, traction, or spinal manipulation. Diazepam and systemic steroids provide no additional benefit. Diagnostic testing is indicated if serious conditions cannot be excluded, and referral to appropriate specialists should be considered for further evaluation or treatment.
Management of chronic back pain follows a similar approach. Serious conditions must be ruled out first. For nonspecific pain, patients should remain active and avoid precipitating factors. Exercise therapy and cognitive behavioral therapy are considered 1st-line treatments.[41][42] Second-line options include spinal manipulation, massage, acupuncture, yoga, stress reduction, intake of NSAIDs or selective norepinephrine reuptake inhibitors (SNRIs), and interprofessional rehabilitation.[43][44][45](A1)
The effectiveness of anticonvulsants such as gabapentin and topiramate is uncertain.[46][47] Transcutaneous electrical nerve stimulation (TENS) units do not appear more effective than placebo for chronic back pain.[48](A1)
Referral to pain management
Referral to pain management is indicated when low back pain persists despite adequate conservative treatment and limits daily function. Persistent severe functional impairment, unremitting pain, or plateaued improvement warrants evaluation by a pain specialist. A lower threshold for referral applies to radicular or stenotic symptoms that fail to improve, as these patients may benefit from interventional options, including epidural steroid injections. Pain extending beyond the normal period of tissue healing should prompt specialized assessment and management to interrupt progression toward chronicity and prevent deconditioning.
Surgical referral
Urgent surgical referral is required when clinical findings indicate potential spinal cord or nerve root compromise, infection, fracture, or malignancy. Cauda equina syndrome is the most critical indication and constitutes a surgical emergency, identified by new urinary retention or overflow incontinence, saddle anesthesia, bilateral sciatica, or bilateral lower-extremity weakness. Rapidly progressive or severe neurologic deficits, including worsening motor weakness or sensory loss, similarly warrant immediate evaluation.
Features suggestive of spinal infection, including fever, recent spinal procedures, immunosuppression, intravenous drug use, or severe focal vertebral tenderness, require urgent assessment, as they may indicate osteomyelitis, epidural abscess, or septic discitis. Malignancy should be suspected in cases of unexplained weight loss, prior history of cancer, persistent night pain, or focal vertebral tenderness, with concurrent neurologic compromise necessitating immediate referral. Traumatic mechanisms combined with pain, neurologic deficits, advanced age, osteoporosis, or chronic steroid use raise concern for unstable vertebral fracture and demand prompt surgical evaluation.
Severe spinal stenosis with progressive neurologic impairment and spondylolisthesis, accompanied by worsening weakness or disabling sciatica, also meets criteria for urgent referral. Persistent spine-related symptoms correlating with structural pathology on imaging may justify nonurgent referral to a spine surgeon when symptoms fail to improve with conservative therapy. Sciatica caused by a herniated lumbar disc that persists for 4 to 6 weeks despite nonoperative treatment represents a subgroup in which elective surgical evaluation may provide benefit.
Management of Back Pain in Children and Adolescents
Pediatric back pain treatments are less extensively studied. Activity modification, physical therapy, and NSAID use are broadly supported as 1st-line therapies. When serious pathology is present, treatment follows the standard of care for the underlying condition. Spondylolysis resulting from repetitive spinal stress is generally managed conservatively, similar to adults. However, young patients actively engaged in sports may require referral for surgical intervention.[49][50] Symptoms persisting beyond 6 months of conservative therapy or Grade III or IV spondylolisthesis warrant evaluation by a pediatric spine surgeon.[51][52](B2)
Patients with Scheuermann kyphosis may be managed conservatively with physical therapy and guided exercise if the spinal curvature is less than 60°. Bracing may be added for curvatures between 60° and 70°. Surgical correction is indicated for curvatures exceeding 75°, particularly if conservative measures fail and skeletal maturity is reached.[53][54] Indications for surgical referral also include scoliotic spinal curvature of 20° or greater during peak growth, significant or progressive scoliosis, and atypical scoliosis.[55](B2)
Urgent surgical referral in children is indicated when back pain is accompanied by findings suggestive of infection, malignancy, or spinal cord compromise. Epidural abscess, presenting with fever, spinal pain, and neurologic deficits, requires immediate neurosurgical evaluation. Neoplastic processes, signaled by unremitting nighttime pain, weight loss, or myelopathic symptoms such as gait instability or limb weakness, also warrant rapid referral to neurosurgery.
Tethered cord syndrome, characterized by exertional back pain, bladder dysfunction, calf atrophy, diminished reflexes, dermatomal sensory loss, or progressive scoliosis, similarly requires urgent surgical assessment due to risk of progressive neurologic injury. Vertebral fractures associated with acute trauma, focal midline pain, radicular symptoms, or weakness necessitate immediate imaging and specialist evaluation because of potential instability or neural compression.
Serious manifestations, including nighttime pain, systemic features, bowel or bladder dysfunction, or neurologic deficits, at any age demand prompt investigation and emergent specialty referral. These presentations reflect the higher likelihood of significant underlying spinal pathology in children.[56]
Differential Diagnosis
The following discussion covers adult and pediatric conditions that present with back pain, along with their associated symptoms and relevant physical examination findings. This compilation is not exhaustive but highlights the most common and clinically significant causes of this symptom in these populations.
Differential Diagnosis of Back Pain in Adults
Lumbosacral muscle strains and sprains typically result from traumatic incidents or repetitive overuse. Pain generally worsens with movement and improves with rest, and the range of motion is often restricted. Tenderness to palpation is commonly present. Lumbar spondylosis primarily affects patients older than 40 and may be accompanied by hip pain. Discomfort often occurs with lower limb extension or rotation, while neurologic examination findings are usually normal.
Disc herniation most frequently involves the L4 to S1 segments and can produce paresthesia, sensory changes, and motor weakness, depending on the severity and affected nerve root. Spondylolysis and spondylolisthesis are caused by repetitive spinal stress and may present with back pain radiating to the gluteal region and posterior thighs.
Vertebral compression fractures produce localized back pain that worsens with flexion and point tenderness on palpation. These injuries may be acute or chronic, with risk factors including steroid use, vitamin D deficiency, and osteoporosis. Spinal stenosis is characterized by leg sensory and motor weakness that is relieved with rest (neurologic claudication). Neurologic examination may initially appear normal but can worsen as stenosis progresses.
Spinal tumors may present with unexplained weight loss, focal tenderness to palpation, or other risk factors for malignancy, with approximately 97% of spinal tumors being metastatic.[57] Infections of the spine should be suspected in patients with a history of spinal surgery within the past 12 months, intravenous drug use, or immunosuppression. Clinical features include fever, localized pain, tenderness, or spinal wounds. Common infectious causes encompass vertebral osteomyelitis, discitis, septic sacroiliitis, epidural abscess, and paraspinal muscle abscess. Tuberculosis should be considered in patients from endemic regions.[58]
Acute or chronic aortic dissection can manifest as tearing back pain. The incidence is higher in older adults and is often associated with cardiovascular diseases such as atherosclerosis, hypertension, and aneurysms. In younger patients, dissection is typically linked to connective tissue disorders, including Marfan, Ehlers-Danlos, and Loeys-Dietz syndromes.[59] Vertebral fractures may result from trauma, prolonged corticosteroid use, or osteoporosis and are most common in patients older than 70. Physical findings include contusions, abrasions, and tenderness over the spinous processes.
Differential Diagnosis of Back Pain in Children and Adolescents
Tumors in pediatric patients may present with fever, malaise, weight loss, nighttime pain, and recent-onset scoliosis. Osteoid osteoma is the most common tumor causing back pain and is typically relieved by NSAID intake.[60][61][62] Infections are associated with fever, malaise, weight loss, nighttime pain, and recent-onset scoliosis. Patients may refuse to walk. Common conditions include vertebral osteomyelitis, discitis, septic sacroiliitis, epidural abscess, and paraspinal muscle abscess. Epidural abscess should be suspected if neurologic deficits or radicular pain are present.[63][64]
Disc herniation and slipped apophysis may present with acute back pain, radicular symptoms, and recent-onset scoliosis, with positive SLR test findings and pain on forward spinal flexion. Spondylolysis, spondylolisthesis, and posterior arch lesions typically present with acute back pain and radicular symptoms, sometimes accompanied by hamstring tightness, with pain on spinal extension and positive SLR test results.
Vertebral fractures usually follow trauma but may occur as stress fractures, causing insidious onset and progressive postural changes. Muscle strain presents with acute localized tenderness without radiation. Scheuermann kyphosis is associated with chronic back pain and rigid kyphosis. Inflammatory spondyloarthropathies feature chronic pain, morning stiffness exceeding 30 minutes, and sacroiliac joint tenderness. Psychological disorders, including conversion or somatization, may cause persistent subjective pain despite normal physical findings. Idiopathic scoliosis is typically asymptomatic, with a positive Adam test result; reported back pain may have an alternative cause.[65]
Prognosis
In adults, the prognosis of back pain depends on its etiology. Most nonspecific cases resolve without serious sequelae. The effectiveness of conservative therapy and patient education demonstrates the important contribution of psychosocial and contextual factors to symptom severity and disability. Chronic, disabling back pain is more likely with prior episodes, high symptom intensity, depression, fear-avoidant behavior, or accompanying leg or widespread symptoms.[66]
Social factors also significantly influence prognosis.[67] Low educational attainment, physically demanding work, inadequate compensation, and poor job satisfaction are associated with worse outcomes, including higher disability rates.[68][69] Modifiable risk factors, such as a body mass index greater than 25 and smoking, are linked to persistent back pain.[70]
Fewer studies address pediatric back pain prognosis, but etiology appears similarly influential.[71] Pain caused by malignancy is more likely to result in disability than muscle strain.[72] Behavioral comorbidities, including conduct problems, attention deficit hyperactivity disorder, passive coping strategies, and fear-avoidant behavior, have been associated with poorer outcomes in younger patients.[73][74][75]
Complications
The underlying etiology of back pain largely determines the risk of complications, which may be both physical and social. Physically, back pain can become chronic and may be associated with deformity, neurologic deficits, or both. Social consequences include disability, reduced productivity, and increased absenteeism. A 2015 study reported that back pain accounted for 60.1 million years of disability worldwide, making it the leading cause of global disability.[76] In the U.S., low-back pain is the most common reason for disability.[77]
Early intervention helps prevent the progression to chronic pain and associated complications. Ambulation and maintenance of activity improve outcomes, whereas prolonged sedentariness and resultant obesity are associated with poorer prognosis.
Postoperative and Rehabilitation Care
The underlying cause, patient comorbidities, and individual health goals guide back pain rehabilitation. The McKenzie method is frequently recommended for managing chronic nonspecific low-back pain.[78] Clinical practice guidelines for physical therapy advocate manual therapy, trunk strengthening, centralization techniques, directional preference exercises, and progressive endurance training. Occupational therapy can support patients in managing activities of daily living and using adaptive equipment as needed. Additionally, employing assistive devices during patient transfers has been shown to reduce the incidence of low-back pain among female healthcare workers.[79][80]
Deterrence and Patient Education
Patient education on preventing back pain recurrence or aggravation should be individualized. Adults with sedentary occupations should be encouraged to remain active to maintain a healthy body weight, as a body mass index greater than 25 is associated with worse outcomes. Individuals in physically demanding jobs should similarly remain active but avoid precipitating factors, such as heavy lifting and repetitive back twisting, by using lifting equipment or reducing load weight when necessary.
All patients should be counseled to avoid smoking, which increases back pain risk across all ages.[81][82] Intensive education sessions lasting approximately 2.5 hours, covering activity modification, staying active, and early return to normal routines, have proven effective in promoting return to work among adults.[83]
In pediatric patients, evidence regarding bookbag weight as a risk factor is mixed. Nevertheless, the American Academy of Pediatrics recommends that bookbags not exceed 10% to 20% of a child’s body weight.[84] Although most back pain cases are self-limited, discharged patients should be instructed to seek immediate medical attention for concerning signs, such as sudden sensory or motor deficits.
Pearls and Other Issues
For adults, history and physical examination usually suffice to evaluate atraumatic, acute back pain in the absence of clinical red flags. Imaging tests should generally be deferred for 6 weeks to allow for symptom resolution.[85][86]
Patient education emphasizing the importance of remaining active constitutes the 1st-line treatment for nonspecific back pain. Evidence indicates that pharmacologic therapy and physical therapy do not consistently provide benefit. Second-line interventions may include treatment with NSAIDs, opioids, or SNRIs such as duloxetine, which are more effective than placebo for nonspecific chronic low-back pain.[87][88] Acetaminophen, antidepressants other than SNRIs, lidocaine patches, and transcutaneous electrical nerve stimulation units have not demonstrated consistent efficacy beyond placebo in chronic low-back pain.[89][90] Referral to physical therapy for the McKenzie technique can help reduce recurrence risk.[91][92]
For children, transient back pain following minor injury in the absence of abnormal physical findings may be managed conservatively without further evaluation. Indications for additional assessment include abnormal examination findings, persistent pain, nighttime pain, or radicular symptoms.[93] Plain anteroposterior and lateral films are recommended as 1st-line radiographic studies. Laboratory testing should be considered when clinical red flags are present, as thoracic malignancy and infection are more common in children, particularly those younger than 4 years.[94]
Enhancing Healthcare Team Outcomes
Integrating the expertise of multiple healthcare professionals ensures comprehensive care, improved outcomes, and enhanced quality of life for individuals with back pain. The interprofessional team typically includes the primary care provider, nurse, pharmacist, nutritionist, physical therapist, occupational therapist, radiologist, and other medical specialists relevant to the individual case.
The primary care provider is the first medical professional to examine the patient. Evaluation begins with a thorough medical history and physical examination. The primary care provider determines the appropriate initial treatment, assesses the need for diagnostic testing, and decides on referrals to specialists. This provider also leads patient education and communicates follow-up recommendations. Education should emphasize smoking cessation and maintenance of a healthy body weight.[95]
The nurse reinforces key components of patient education and follow-up instructions. Evidence-based responses should be provided to questions regarding nonpharmacologic therapies and continued physical activity in back pain management. The nurse ensures the patient is clinically stable prior to discharge and that care plans are coordinated for subsequent appointments.
If the primary care provider prescribes medications, the pharmacist can educate patients on the specific benefits and risks of each drug for back pain. Proper administration instructions and the potential risks of overdose should be emphasized. The pharmacist should contact the primary care provider to clarify any uncertainties regarding the patient’s prescription.
Obesity is associated with poorer outcomes in patients with back pain. Nutritionists can guide patients in making healthier dietary choices and maintaining a healthy weight. In cases of obesity, an obesity medicine specialist may prescribe antiobesity medications as an adjunct to lifestyle modifications to support significant weight loss.
The physical therapist designs strength and endurance exercise programs to manage back pain and reduce the risk of recurrence. Physical therapy has also been shown to assist patients with back pain in reducing or discontinuing opioid use.[96] The occupational therapist provides ergonomic guidance and recommends assistive devices to support back pain management in both work and home environments. The radiologist assists the primary care provider in interpreting imaging findings and can recommend additional imaging studies if necessary.
The primary care provider may refer patients to other specialists as indicated. A pain specialist can optimize pharmacologic therapy or perform interventional procedures for chronic back pain. A rheumatologist may be consulted when back pain is associated with signs of chronic inflammatory disease. Severe radiculopathy or neurologic deterioration warrants urgent referral to a neurosurgeon or orthopedic spine surgeon. Mental health therapists can provide stress-coping strategies, administer cognitive behavioral therapy, and implement other interventions for back pain with a significant psychological component.[97] Alternative medicine practitioners may also contribute to improving patient function.
Effective communication among the interprofessional team is essential to avoid duplicating diagnostic tests. Conflicting treatments can also impede patient progress.
Media
(Click Image to Enlarge)

Multiple Myeloma Involving the Spine. This lateral lumbar spine x-ray shows lytic lesions in the L1 and L4 vertebral bodies.
Contributed by Steve Lange, MD
(Click Image to Enlarge)
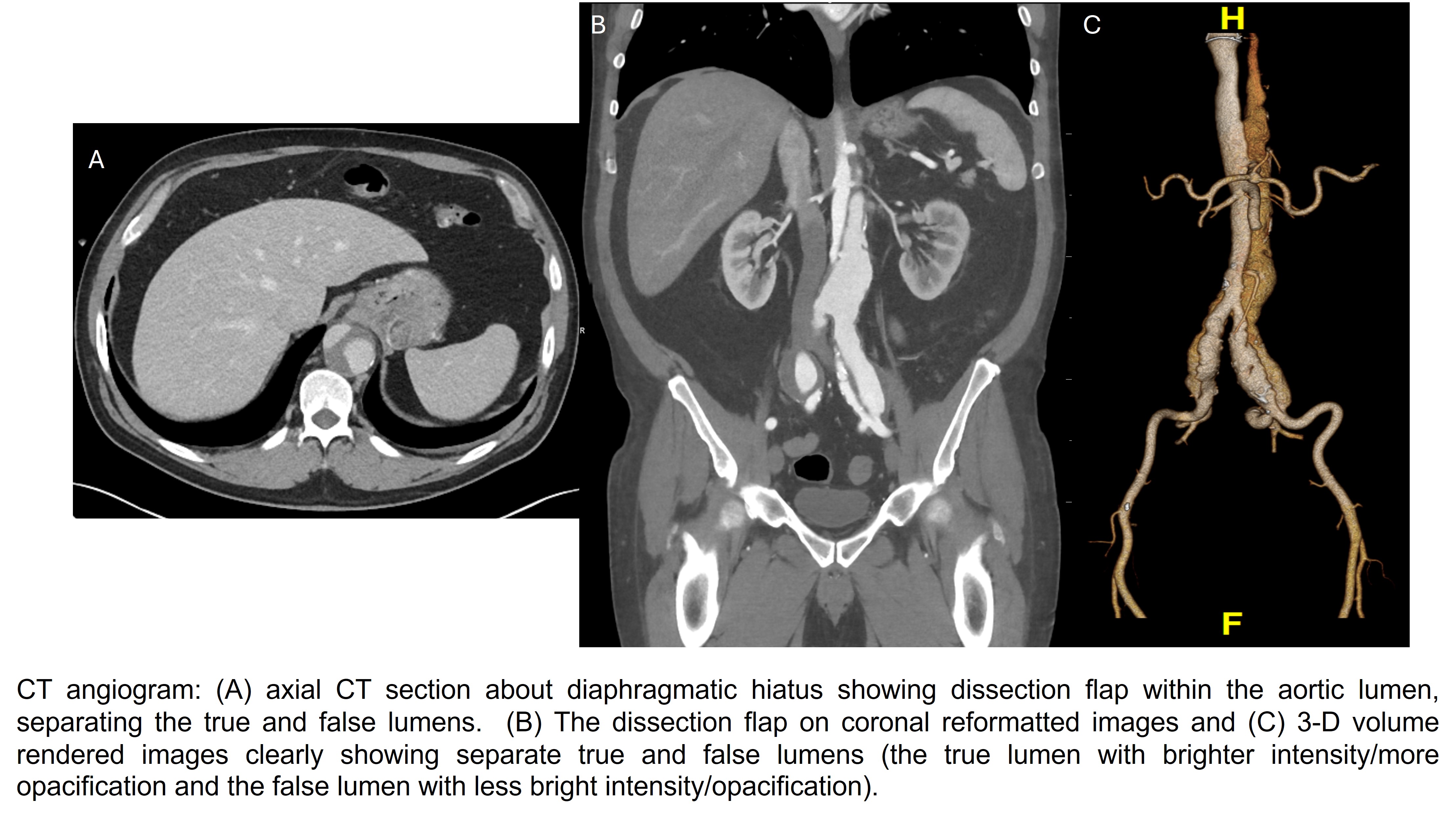
Type B Aortic Dissection on Computed Tomography Angiography. Axial computed tomography section at the level of the diaphragmatic hiatus demonstrates a dissection flap within the aortic lumen, separating the true and false lumens (Image A). Coronal reformatted (Image B) and 3-dimensional volume-rendered (Image C) images clearly depict distinct true and false lumens, with the true lumen exhibiting higher attenuation and greater contrast opacification compared with the false lumen. The patient presented with acute, sharp, tearing back pain.
Contributed by Charanjeet Singh, MD
(Click Image to Enlarge)
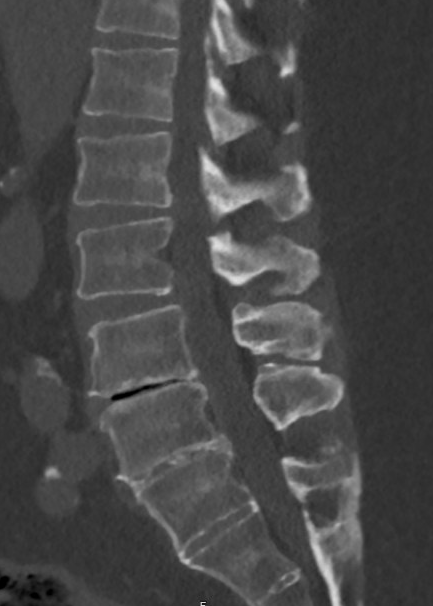
Degenerative Disc Disease with Vacuum Phenomenon. Sagittal computed tomography in a bone window setting demonstrates severe degenerative disc disease with near-complete disc height loss at the affected lumbar level, creating a bone-on-bone appearance between adjacent vertebral endplates. The intradiscal vacuum phenomenon appears as a sharply defined linear hypodense lucency, with associated endplate sclerosis and osteophyte formation.
Contributed by Konstantinos Margetis MD
(Click Image to Enlarge)
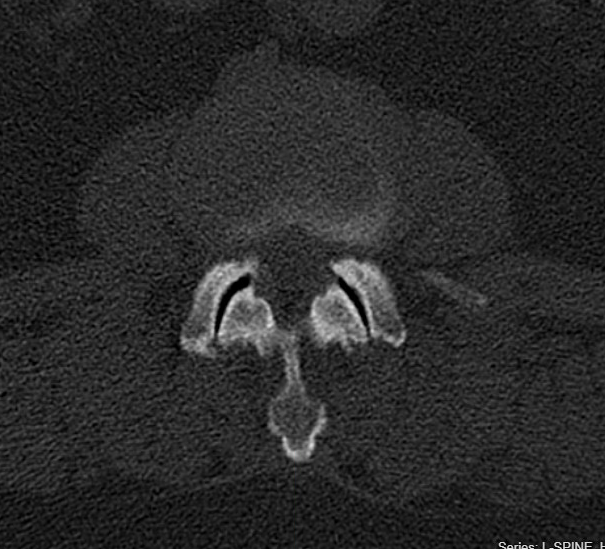
Facet Arthropathy. Axial computed tomography in a bone window setting demonstrates bilateral lumbar facet joint arthropathy with joint space vacuum phenomenon, subchondral sclerosis, and hypertrophic osteophytic change. These degenerative changes can contribute to mechanical back pain and, when advanced, may result in lateral recess or foraminal narrowing.
Contributed by Konstantinos Margetis MD
(Click Image to Enlarge)

Degenerative Spondylolisthesis with Lumbar Spinal Stenosis. Sagittal T2-weighted magnetic resonance imaging demonstrates anterior translation of L4 relative to L5, consistent with degenerative spondylolisthesis, resulting in L4 and L5 central canal stenosis characterized by attenuation of cerebrospinal fluid signal within the thecal sac.
Contributed by Konstantinos Margetis MD
References
Freburger JK, Holmes GM, Agans RP, Jackman AM, Darter JD, Wallace AS, Castel LD, Kalsbeek WD, Carey TS. The rising prevalence of chronic low back pain. Archives of internal medicine. 2009 Feb 9:169(3):251-8. doi: 10.1001/archinternmed.2008.543. Epub [PubMed PMID: 19204216]
Level 2 (mid-level) evidenceBarros G, McGrath L, Gelfenbeyn M. Sacroiliac Joint Dysfunction in Patients With Low Back Pain. Federal practitioner : for the health care professionals of the VA, DoD, and PHS. 2019 Aug:36(8):370-375 [PubMed PMID: 31456628]
Cohen SP, Chen Y, Neufeld NJ. Sacroiliac joint pain: a comprehensive review of epidemiology, diagnosis and treatment. Expert review of neurotherapeutics. 2013 Jan:13(1):99-116. doi: 10.1586/ern.12.148. Epub [PubMed PMID: 23253394]
Buell KG, Sivasubramaniyam S, Sykes M, Zafar K, Bingham L, Mitra A. Expediting the management of cauda equina syndrome in the emergency department through clinical pathway design. BMJ open quality. 2019:8(4):e000597. doi: 10.1136/bmjoq-2018-000597. Epub 2019 Nov 2 [PubMed PMID: 31799444]
Level 2 (mid-level) evidenceMusich S, Wang SS, Slindee LB, Keown K, Hawkins K, Yeh CS. Using Pain Medication Intensity to Stratify Back Pain Among Older Adults. Pain medicine (Malden, Mass.). 2019 Feb 1:20(2):252-266. doi: 10.1093/pm/pny007. Epub [PubMed PMID: 29394401]
Owen PJ, Miller CT, Mundell NL, Verswijveren SJJM, Tagliaferri SD, Brisby H, Bowe SJ, Belavy DL. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. British journal of sports medicine. 2020 Nov:54(21):1279-1287. doi: 10.1136/bjsports-2019-100886. Epub 2019 Oct 30 [PubMed PMID: 31666220]
Level 1 (high-level) evidenceWei X, Liu B, He L, Yang X, Zhou J, Zhao H, Liu J. Acupuncture therapy for chronic low back pain: protocol of a prospective, multi-center, registry study. BMC musculoskeletal disorders. 2019 Oct 27:20(1):488. doi: 10.1186/s12891-019-2894-4. Epub 2019 Oct 27 [PubMed PMID: 31656194]
Qin J, Zhang Y, Wu L, He Z, Huang J, Tao J, Chen L. Effect of Tai Chi alone or as additional therapy on low back pain: Systematic review and meta-analysis of randomized controlled trials. Medicine. 2019 Sep:98(37):e17099. doi: 10.1097/MD.0000000000017099. Epub [PubMed PMID: 31517838]
Level 2 (mid-level) evidencePatrick N, Emanski E, Knaub MA. Acute and chronic low back pain. The Medical clinics of North America. 2014 Jul:98(4):777-89, xii. doi: 10.1016/j.mcna.2014.03.005. Epub [PubMed PMID: 24994051]
Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non-specific low back pain. Lancet (London, England). 2012 Feb 4:379(9814):482-91. doi: 10.1016/S0140-6736(11)60610-7. Epub 2011 Oct 6 [PubMed PMID: 21982256]
Hoy D, Brooks P, Blyth F, Buchbinder R. The Epidemiology of low back pain. Best practice & research. Clinical rheumatology. 2010 Dec:24(6):769-81. doi: 10.1016/j.berh.2010.10.002. Epub [PubMed PMID: 21665125]
Walker BF. The prevalence of low back pain: a systematic review of the literature from 1966 to 1998. Journal of spinal disorders. 2000 Jun:13(3):205-17 [PubMed PMID: 10872758]
Level 1 (high-level) evidenceLeboeuf-Yde C, Kyvik KO. At what age does low back pain become a common problem? A study of 29,424 individuals aged 12-41 years. Spine. 1998 Jan 15:23(2):228-34 [PubMed PMID: 9474731]
Level 2 (mid-level) evidenceJeffries LJ, Milanese SF, Grimmer-Somers KA. Epidemiology of adolescent spinal pain: a systematic overview of the research literature. Spine. 2007 Nov 1:32(23):2630-7 [PubMed PMID: 17978666]
Level 2 (mid-level) evidenceAdams MA, Roughley PJ. What is intervertebral disc degeneration, and what causes it? Spine. 2006 Aug 15:31(18):2151-61 [PubMed PMID: 16915105]
Level 3 (low-level) evidenceCavanaugh JM, Ozaktay AC, Yamashita HT, King AI. Lumbar facet pain: biomechanics, neuroanatomy and neurophysiology. Journal of biomechanics. 1996 Sep:29(9):1117-29 [PubMed PMID: 8872268]
Level 3 (low-level) evidenceDeyo RA, Rainville J, Kent DL. What can the history and physical examination tell us about low back pain? JAMA. 1992 Aug 12:268(6):760-5 [PubMed PMID: 1386391]
Das JM, Dua A, Nadi M. Straight Leg Raise Test (Lasegue sign). StatPearls. 2025 Jan:(): [PubMed PMID: 31424883]
Patel DR, Kinsella E. Evaluation and management of lower back pain in young athletes. Translational pediatrics. 2017 Jul:6(3):225-235. doi: 10.21037/tp.2017.06.01. Epub [PubMed PMID: 28795014]
Maselli F, Palladino M, Barbari V, Storari L, Rossettini G, Testa M. The diagnostic value of Red Flags in thoracolumbar pain: a systematic review. Disability and rehabilitation. 2022 Apr:44(8):1190-1206. doi: 10.1080/09638288.2020.1804626. Epub 2020 Aug 19 [PubMed PMID: 32813559]
Level 1 (high-level) evidenceDownie A, Williams CM, Henschke N, Hancock MJ, Ostelo RW, de Vet HC, Macaskill P, Irwig L, van Tulder MW, Koes BW, Maher CG. Red flags to screen for malignancy and fracture in patients with low back pain: systematic review. BMJ (Clinical research ed.). 2013 Dec 11:347():f7095. doi: 10.1136/bmj.f7095. Epub 2013 Dec 11 [PubMed PMID: 24335669]
Level 1 (high-level) evidenceCasazza BA. Diagnosis and treatment of acute low back pain. American family physician. 2012 Feb 15:85(4):343-50 [PubMed PMID: 22335313]
Feldman DS, Hedden DM, Wright JG. The use of bone scan to investigate back pain in children and adolescents. Journal of pediatric orthopedics. 2000 Nov-Dec:20(6):790-5 [PubMed PMID: 11097256]
Level 2 (mid-level) evidenceHollingworth P. Back pain in children. British journal of rheumatology. 1996 Oct:35(10):1022-8 [PubMed PMID: 8883446]
Frosch M, Mauritz MD, Bielack S, Blödt S, Dirksen U, Dobe M, Geiger F, Häfner R, Höfel L, Hübner-Möhler B, von Kalle T, Lawrenz B, Leutner A, Mecher F, Mladenov K, Norda H, Stahlschmidt L, Steinborn M, Stücker R, Trauzeddel R, Trollmann R, Wager J, Zernikow B. Etiology, Risk Factors, and Diagnosis of Back Pain in Children and Adolescents: Evidence- and Consensus-Based Interdisciplinary Recommendations. Children (Basel, Switzerland). 2022 Feb 2:9(2):. doi: 10.3390/children9020192. Epub 2022 Feb 2 [PubMed PMID: 35204913]
Level 3 (low-level) evidenceLast AR, Hulbert K. Chronic low back pain: evaluation and management. American family physician. 2009 Jun 15:79(12):1067-74 [PubMed PMID: 19530637]
Deyo RA, Weinstein JN. Low back pain. The New England journal of medicine. 2001 Feb 1:344(5):363-70 [PubMed PMID: 11172169]
Patel ND, Broderick DF, Burns J, Deshmukh TK, Fries IB, Harvey HB, Holly L, Hunt CH, Jagadeesan BD, Kennedy TA, O'Toole JE, Perlmutter JS, Policeni B, Rosenow JM, Schroeder JW, Whitehead MT, Cornelius RS, Corey AS. ACR Appropriateness Criteria Low Back Pain. Journal of the American College of Radiology : JACR. 2016 Sep:13(9):1069-78. doi: 10.1016/j.jacr.2016.06.008. Epub 2016 Aug 3 [PubMed PMID: 27496288]
Jarvik JG, Hollingworth W, Martin B, Emerson SS, Gray DT, Overman S, Robinson D, Staiger T, Wessbecher F, Sullivan SD, Kreuter W, Deyo RA. Rapid magnetic resonance imaging vs radiographs for patients with low back pain: a randomized controlled trial. JAMA. 2003 Jun 4:289(21):2810-8 [PubMed PMID: 12783911]
Level 1 (high-level) evidenceHall AM, Aubrey-Bassler K, Thorne B, Maher CG. Do not routinely offer imaging for uncomplicated low back pain. BMJ (Clinical research ed.). 2021 Feb 12:372():n291. doi: 10.1136/bmj.n291. Epub 2021 Feb 12 [PubMed PMID: 33579691]
Miller R, Beck NA, Sampson NR, Zhu X, Flynn JM, Drummond D. Imaging modalities for low back pain in children: a review of spondyloysis and undiagnosed mechanical back pain. Journal of pediatric orthopedics. 2013 Apr-May:33(3):282-8. doi: 10.1097/BPO.0b013e318287fffb. Epub [PubMed PMID: 23482264]
Level 2 (mid-level) evidenceBorchers AT, Gershwin ME. Transverse myelitis. Autoimmunity reviews. 2012 Jan:11(3):231-48. doi: 10.1016/j.autrev.2011.05.018. Epub 2011 May 18 [PubMed PMID: 21621005]
Kujala UM, Kinnunen J, Helenius P, Orava S, Taavitsainen M, Karaharju E. Prolonged low-back pain in young athletes: a prospective case series study of findings and prognosis. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 1999:8(6):480-4 [PubMed PMID: 10664307]
Level 2 (mid-level) evidenceThurston D, Hurley P, Raheel F, James S, Gadvi R, Botchu R, Gardner AC, Mehta JS. A Comparison of Magnetic Resonance Imaging and SPECT-CT Imaging in Complex Spine Pathology: Does SPECT-CT Provide Additional Diagnostic Information Over Magnetic Resonance Imaging? Global spine journal. 2024 Sep:14(7):1997-2003. doi: 10.1177/21925682231163812. Epub 2023 Mar 20 [PubMed PMID: 36939636]
Abdelrahman M, Reddy VN, Haq R, Ganti L. Aortic Dissection Masquerading as Musculoskeletal Chest and Back Pain. Orthopedic reviews. 2025:17():145871. doi: 10.52965/001c.145871. Epub 2025 Oct 26 [PubMed PMID: 41163707]
Wang H, Cheng J, Xiao H, Li C, Zhou Y. Adolescent lumbar disc herniation: experience from a large minimally invasive treatment centre for lumbar degenerative disease in Chongqing, China. Clinical neurology and neurosurgery. 2013 Aug:115(8):1415-9. doi: 10.1016/j.clineuro.2013.01.019. Epub 2013 Feb 16 [PubMed PMID: 23419406]
Level 2 (mid-level) evidenceGran JT, Husby G. HLA-B27 and spondyloarthropathy: value for early diagnosis? Journal of medical genetics. 1995 Jul:32(7):497-501 [PubMed PMID: 7562959]
Reveille JD. HLA-B27 and the seronegative spondyloarthropathies. The American journal of the medical sciences. 1998 Oct:316(4):239-49 [PubMed PMID: 9766485]
McGhee JL, Burks FN, Sheckels JL, Jarvis JN. Identifying children with chronic arthritis based on chief complaints: absence of predictive value for musculoskeletal pain as an indicator of rheumatic disease in children. Pediatrics. 2002 Aug:110(2 Pt 1):354-9 [PubMed PMID: 12165590]
Level 2 (mid-level) evidenceEjaz AA, Pourafshar N, Mohandas R, Smallwood BA, Johnson RJ, Hsu JW. Uric acid and the prediction models of tumor lysis syndrome in AML. PloS one. 2015:10(3):e0119497. doi: 10.1371/journal.pone.0119497. Epub 2015 Mar 16 [PubMed PMID: 25775138]
Level 2 (mid-level) evidenceRosedale R, Rastogi R, May S, Chesworth BM, Filice F, Willis S, Howard J, Naudie D, Robbins SM. Efficacy of exercise intervention as determined by the McKenzie System of Mechanical Diagnosis and Therapy for knee osteoarthritis: a randomized controlled trial. The Journal of orthopaedic and sports physical therapy. 2014 Mar:44(3):173-81, A1-6. doi: 10.2519/jospt.2014.4791. Epub 2014 Jan 22 [PubMed PMID: 24450370]
Level 1 (high-level) evidenceDunsford A, Kumar S, Clarke S. Integrating evidence into practice: use of McKenzie-based treatment for mechanical low back pain. Journal of multidisciplinary healthcare. 2011:4():393-402. doi: 10.2147/JMDH.S24733. Epub 2011 Nov 1 [PubMed PMID: 22135496]
Kamper SJ, Apeldoorn AT, Chiarotto A, Smeets RJ, Ostelo RW, Guzman J, van Tulder MW. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis. BMJ (Clinical research ed.). 2015 Feb 18:350():h444. doi: 10.1136/bmj.h444. Epub 2015 Feb 18 [PubMed PMID: 25694111]
Level 1 (high-level) evidenceStraube S, Harden M, Schröder H, Arendacka B, Fan X, Moore RA, Friede T. Back schools for the treatment of chronic low back pain: possibility of benefit but no convincing evidence after 47 years of research-systematic review and meta-analysis. Pain. 2016 Oct:157(10):2160-2172. doi: 10.1097/j.pain.0000000000000640. Epub [PubMed PMID: 27257858]
Level 1 (high-level) evidenceFranke H, Franke JD, Fryer G. Osteopathic manipulative treatment for nonspecific low back pain: a systematic review and meta-analysis. BMC musculoskeletal disorders. 2014 Aug 30:15():286. doi: 10.1186/1471-2474-15-286. Epub 2014 Aug 30 [PubMed PMID: 25175885]
Level 1 (high-level) evidenceShanthanna H, Gilron I, Rajarathinam M, AlAmri R, Kamath S, Thabane L, Devereaux PJ, Bhandari M. Benefits and safety of gabapentinoids in chronic low back pain: A systematic review and meta-analysis of randomized controlled trials. PLoS medicine. 2017 Aug:14(8):e1002369. doi: 10.1371/journal.pmed.1002369. Epub 2017 Aug 15 [PubMed PMID: 28809936]
Level 1 (high-level) evidenceMuehlbacher M, Nickel MK, Kettler C, Tritt K, Lahmann C, Leiberich PK, Nickel C, Krawczyk J, Mitterlehner FO, Rother WK, Loew TH, Kaplan P. Topiramate in treatment of patients with chronic low back pain: a randomized, double-blind, placebo-controlled study. The Clinical journal of pain. 2006 Jul-Aug:22(6):526-31 [PubMed PMID: 16788338]
Level 1 (high-level) evidenceBuchmuller A, Navez M, Milletre-Bernardin M, Pouplin S, Presles E, Lantéri-Minet M, Tardy B, Laurent B, Camdessanché JP, Lombotens Trial Group. Value of TENS for relief of chronic low back pain with or without radicular pain. European journal of pain (London, England). 2012 May:16(5):656-65. doi: 10.1002/j.1532-2149.2011.00061.x. Epub 2011 Dec 20 [PubMed PMID: 22337531]
Level 1 (high-level) evidenceKaratas AF, Dede O, Atanda AA, Holmes L Jr, Rogers K, Gabos P, Shah SA. Comparison of Direct Pars Repair Techniques of Spondylolysis in Pediatric and Adolescent Patients: Pars Compression Screw Versus Pedicle Screw-Rod-Hook. Clinical spine surgery. 2016 Aug:29(7):272-80. doi: 10.1097/BSD.0b013e318277cb7d. Epub [PubMed PMID: 23075858]
Menga EN, Kebaish KM, Jain A, Carrino JA, Sponseller PD. Clinical results and functional outcomes after direct intralaminar screw repair of spondylolysis. Spine. 2014 Jan 1:39(1):104-10. doi: 10.1097/BRS.0000000000000043. Epub [PubMed PMID: 24108299]
Helenius I, Lamberg T, Osterman K, Schlenzka D, Yrjönen T, Tervahartiala P, Seitsalo S, Poussa M, Remes V. Scoliosis research society outcome instrument in evaluation of long-term surgical results in spondylolysis and low-grade isthmic spondylolisthesis in young patients. Spine. 2005 Feb 1:30(3):336-41 [PubMed PMID: 15682016]
Level 2 (mid-level) evidenceLundine KM, Lewis SJ, Al-Aubaidi Z, Alman B, Howard AW. Patient outcomes in the operative and nonoperative management of high-grade spondylolisthesis in children. Journal of pediatric orthopedics. 2014 Jul-Aug:34(5):483-9. doi: 10.1097/BPO.0000000000000133. Epub [PubMed PMID: 24590330]
Level 2 (mid-level) evidenceTsirikos AI, Jain AK. Scheuermann's kyphosis; current controversies. The Journal of bone and joint surgery. British volume. 2011 Jul:93(7):857-64. doi: 10.1302/0301-620X.93B7.26129. Epub [PubMed PMID: 21705553]
Lim M, Green DW, Billinghurst JE, Huang RC, Rawlins BA, Widmann RF, Burke SW, Boachie-Adjei O. Scheuermann kyphosis: safe and effective surgical treatment using multisegmental instrumentation. Spine. 2004 Aug 15:29(16):1789-94 [PubMed PMID: 15303023]
Level 2 (mid-level) evidenceParent S, Newton PO, Wenger DR. Adolescent idiopathic scoliosis: etiology, anatomy, natural history, and bracing. Instructional course lectures. 2005:54():529-36 [PubMed PMID: 15948477]
Achar S, Yamanaka J. Back Pain in Children and Adolescents. American family physician. 2020 Jul 1:102(1):19-28 [PubMed PMID: 32603067]
Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, Hoy D, Karppinen J, Pransky G, Sieper J, Smeets RJ, Underwood M, Lancet Low Back Pain Series Working Group. What low back pain is and why we need to pay attention. Lancet (London, England). 2018 Jun 9:391(10137):2356-2367. doi: 10.1016/S0140-6736(18)30480-X. Epub 2018 Mar 21 [PubMed PMID: 29573870]
Trecarichi EM, Di Meco E, Mazzotta V, Fantoni M. Tuberculous spondylodiscitis: epidemiology, clinical features, treatment, and outcome. European review for medical and pharmacological sciences. 2012 Apr:16 Suppl 2():58-72 [PubMed PMID: 22655484]
Kano HD, Sun W. Risk Factors for Aortic Dissection. US cardiology. 2023:17():e17. doi: 10.15420/usc.2022.36. Epub 2023 Oct 25 [PubMed PMID: 39559517]
Slipman CW, Patel RK, Botwin K, Huston C, Zhang L, Lenrow D, Garvan C. Epidemiology of spine tumors presenting to musculoskeletal physiatrists. Archives of physical medicine and rehabilitation. 2003 Apr:84(4):492-5 [PubMed PMID: 12690585]
Level 2 (mid-level) evidenceCohen MD, Harrington TM, Ginsburg WW. Osteoid osteoma: 95 cases and a review of the literature. Seminars in arthritis and rheumatism. 1983 Feb:12(3):265-81 [PubMed PMID: 6603021]
Level 2 (mid-level) evidenceAzouz EM, Kozlowski K, Marton D, Sprague P, Zerhouni A, Asselah F. Osteoid osteoma and osteoblastoma of the spine in children. Report of 22 cases with brief literature review. Pediatric radiology. 1986:16(1):25-31 [PubMed PMID: 2935775]
Level 3 (low-level) evidenceKang HM, Choi EH, Lee HJ, Yun KW, Lee CK, Cho TJ, Cheon JE, Lee H. The Etiology, Clinical Presentation and Long-term Outcome of Spondylodiscitis in Children. The Pediatric infectious disease journal. 2016 Apr:35(4):e102-6. doi: 10.1097/INF.0000000000001043. Epub [PubMed PMID: 26974751]
Spencer SJ, Wilson NI. Childhood discitis in a regional children's hospital. Journal of pediatric orthopedics. Part B. 2012 May:21(3):264-8. doi: 10.1097/BPB.0b013e32834d3e94. Epub [PubMed PMID: 22015583]
Ramirez N, Johnston CE, Browne RH. The prevalence of back pain in children who have idiopathic scoliosis. The Journal of bone and joint surgery. American volume. 1997 Mar:79(3):364-8 [PubMed PMID: 9070524]
Level 2 (mid-level) evidenceHendrick P, Milosavljevic S, Hale L, Hurley DA, McDonough S, Ryan B, Baxter GD. The relationship between physical activity and low back pain outcomes: a systematic review of observational studies. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2011 Mar:20(3):464-74. doi: 10.1007/s00586-010-1616-2. Epub 2010 Nov 4 [PubMed PMID: 21053026]
Level 1 (high-level) evidencePinheiro MB, Ferreira ML, Refshauge K, Maher CG, Ordoñana JR, Andrade TB, Tsathas A, Ferreira PH. Symptoms of depression as a prognostic factor for low back pain: a systematic review. The spine journal : official journal of the North American Spine Society. 2016 Jan 1:16(1):105-16. doi: 10.1016/j.spinee.2015.10.037. Epub 2015 Oct 30 [PubMed PMID: 26523965]
Level 1 (high-level) evidenceWertli MM, Eugster R, Held U, Steurer J, Kofmehl R, Weiser S. Catastrophizing-a prognostic factor for outcome in patients with low back pain: a systematic review. The spine journal : official journal of the North American Spine Society. 2014 Nov 1:14(11):2639-57. doi: 10.1016/j.spinee.2014.03.003. Epub 2014 Mar 7 [PubMed PMID: 24607845]
Level 1 (high-level) evidenceWertli MM, Rasmussen-Barr E, Weiser S, Bachmann LM, Brunner F. The role of fear avoidance beliefs as a prognostic factor for outcome in patients with nonspecific low back pain: a systematic review. The spine journal : official journal of the North American Spine Society. 2014 May 1:14(5):816-36.e4. doi: 10.1016/j.spinee.2013.09.036. Epub 2013 Oct 18 [PubMed PMID: 24412032]
Level 1 (high-level) evidenceChou R, Shekelle P. Will this patient develop persistent disabling low back pain? JAMA. 2010 Apr 7:303(13):1295-302. doi: 10.1001/jama.2010.344. Epub [PubMed PMID: 20371789]
Jones GT, Watson KD, Silman AJ, Symmons DP, Macfarlane GJ. Predictors of low back pain in British schoolchildren: a population-based prospective cohort study. Pediatrics. 2003 Apr:111(4 Pt 1):822-8 [PubMed PMID: 12671119]
Level 2 (mid-level) evidenceLynch AM, Kashikar-Zuck S, Goldschneider KR, Jones BA. Psychosocial risks for disability in children with chronic back pain. The journal of pain. 2006 Apr:7(4):244-51 [PubMed PMID: 16618468]
Korovessis P, Repantis T, Baikousis A. Factors affecting low back pain in adolescents. Journal of spinal disorders & techniques. 2010 Dec:23(8):513-20. doi: 10.1097/BSD.0b013e3181bf99c6. Epub [PubMed PMID: 20075753]
Ramond A, Bouton C, Richard I, Roquelaure Y, Baufreton C, Legrand E, Huez JF. Psychosocial risk factors for chronic low back pain in primary care--a systematic review. Family practice. 2011 Feb:28(1):12-21. doi: 10.1093/fampra/cmq072. Epub 2010 Sep 10 [PubMed PMID: 20833704]
Level 1 (high-level) evidenceMustard CA, Kalcevich C, Frank JW, Boyle M. Childhood and early adult predictors of risk of incident back pain: Ontario Child Health Study 2001 follow-up. American journal of epidemiology. 2005 Oct 15:162(8):779-86 [PubMed PMID: 16150891]
Level 2 (mid-level) evidenceGBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet (London, England). 2016 Oct 8:388(10053):1545-1602. doi: 10.1016/S0140-6736(16)31678-6. Epub [PubMed PMID: 27733282]
Level 1 (high-level) evidenceUS Burden of Disease Collaborators, Mokdad AH, Ballestros K, Echko M, Glenn S, Olsen HE, Mullany E, Lee A, Khan AR, Ahmadi A, Ferrari AJ, Kasaeian A, Werdecker A, Carter A, Zipkin B, Sartorius B, Serdar B, Sykes BL, Troeger C, Fitzmaurice C, Rehm CD, Santomauro D, Kim D, Colombara D, Schwebel DC, Tsoi D, Kolte D, Nsoesie E, Nichols E, Oren E, Charlson FJ, Patton GC, Roth GA, Hosgood HD, Whiteford HA, Kyu H, Erskine HE, Huang H, Martopullo I, Singh JA, Nachega JB, Sanabria JR, Abbas K, Ong K, Tabb K, Krohn KJ, Cornaby L, Degenhardt L, Moses M, Farvid M, Griswold M, Criqui M, Bell M, Nguyen M, Wallin M, Mirarefin M, Qorbani M, Younis M, Fullman N, Liu P, Briant P, Gona P, Havmoller R, Leung R, Kimokoti R, Bazargan-Hejazi S, Hay SI, Yadgir S, Biryukov S, Vollset SE, Alam T, Frank T, Farid T, Miller T, Vos T, Bärnighausen T, Gebrehiwot TT, Yano Y, Al-Aly Z, Mehari A, Handal A, Kandel A, Anderson B, Biroscak B, Mozaffarian D, Dorsey ER, Ding EL, Park EK, Wagner G, Hu G, Chen H, Sunshine JE, Khubchandani J, Leasher J, Leung J, Salomon J, Unutzer J, Cahill L, Cooper L, Horino M, Brauer M, Breitborde N, Hotez P, Topor-Madry R, Soneji S, Stranges S, James S, Amrock S, Jayaraman S, Patel T, Akinyemiju T, Skirbekk V, Kinfu Y, Bhutta Z, Jonas JB, Murray CJL. The State of US Health, 1990-2016: Burden of Diseases, Injuries, and Risk Factors Among US States. JAMA. 2018 Apr 10:319(14):1444-1472. doi: 10.1001/jama.2018.0158. Epub [PubMed PMID: 29634829]
Lam OT, Strenger DM, Chan-Fee M, Pham PT, Preuss RA, Robbins SM. Effectiveness of the McKenzie Method of Mechanical Diagnosis and Therapy for Treating Low Back Pain: Literature Review With Meta-analysis. The Journal of orthopaedic and sports physical therapy. 2018 Jun:48(6):476-490. doi: 10.2519/jospt.2018.7562. Epub 2018 Mar 30 [PubMed PMID: 29602304]
Level 1 (high-level) evidenceDelitto A, George SZ, Van Dillen L, Whitman JM, Sowa G, Shekelle P, Denninger TR, Godges JJ, Orthopaedic Section of the American Physical Therapy Association. Low back pain. The Journal of orthopaedic and sports physical therapy. 2012 Apr:42(4):A1-57. doi: 10.2519/jospt.2012.42.4.A1. Epub 2012 Mar 30 [PubMed PMID: 22466247]
Holtermann A, Clausen T, Jørgensen MB, Aust B, Mortensen OS, Burdorf A, Fallentin N, Andersen LL. Does rare use of assistive devices during patient handling increase the risk of low back pain? A prospective cohort study among female healthcare workers. International archives of occupational and environmental health. 2015 Apr:88(3):335-42. doi: 10.1007/s00420-014-0963-4. Epub 2014 Jul 23 [PubMed PMID: 25053444]
Hestbaek L, Leboeuf-Yde C, Kyvik KO. Are lifestyle-factors in adolescence predictors for adult low back pain? A cross-sectional and prospective study of young twins. BMC musculoskeletal disorders. 2006 Mar 15:7():27 [PubMed PMID: 16539729]
Level 2 (mid-level) evidenceLeboeuf-Yde C. Smoking and low back pain. A systematic literature review of 41 journal articles reporting 47 epidemiologic studies. Spine. 1999 Jul 15:24(14):1463-70 [PubMed PMID: 10423792]
Level 1 (high-level) evidenceEngers A, Jellema P, Wensing M, van der Windt DA, Grol R, van Tulder MW. Individual patient education for low back pain. The Cochrane database of systematic reviews. 2008 Jan 23:2008(1):CD004057. doi: 10.1002/14651858.CD004057.pub3. Epub 2008 Jan 23 [PubMed PMID: 18254037]
Level 1 (high-level) evidenceSkaggs DL, Early SD, D'Ambra P, Tolo VT, Kay RM. Back pain and backpacks in school children. Journal of pediatric orthopedics. 2006 May-Jun:26(3):358-63 [PubMed PMID: 16670549]
Chou R, Qaseem A, Owens DK, Shekelle P, Clinical Guidelines Committee of the American College of Physicians. Diagnostic imaging for low back pain: advice for high-value health care from the American College of Physicians. Annals of internal medicine. 2011 Feb 1:154(3):181-9. doi: 10.7326/0003-4819-154-3-201102010-00008. Epub [PubMed PMID: 21282698]
Saragiotto BT, Machado GC, Ferreira ML, Pinheiro MB, Abdel Shaheed C, Maher CG. Paracetamol for low back pain. The Cochrane database of systematic reviews. 2016 Jun 7:2016(6):CD012230. doi: 10.1002/14651858.CD012230. Epub 2016 Jun 7 [PubMed PMID: 27271789]
Level 1 (high-level) evidenceRoelofs PD, Deyo RA, Koes BW, Scholten RJ, van Tulder MW. Nonsteroidal anti-inflammatory drugs for low back pain: an updated Cochrane review. Spine. 2008 Jul 15:33(16):1766-74. doi: 10.1097/BRS.0b013e31817e69d3. Epub [PubMed PMID: 18580547]
Level 1 (high-level) evidencevan Tulder MW, Touray T, Furlan AD, Solway S, Bouter LM. Muscle relaxants for non-specific low back pain. The Cochrane database of systematic reviews. 2003:2003(2):CD004252 [PubMed PMID: 12804507]
Level 1 (high-level) evidenceUrquhart DM, Hoving JL, Assendelft WW, Roland M, van Tulder MW. Antidepressants for non-specific low back pain. The Cochrane database of systematic reviews. 2008 Jan 23:2008(1):CD001703. doi: 10.1002/14651858.CD001703.pub3. Epub 2008 Jan 23 [PubMed PMID: 18253994]
Level 1 (high-level) evidenceLong A, May S, Fung T. The comparative prognostic value of directional preference and centralization: a useful tool for front-line clinicians? The Journal of manual & manipulative therapy. 2008:16(4):248-54 [PubMed PMID: 19771197]
Level 2 (mid-level) evidenceAina A, May S, Clare H. The centralization phenomenon of spinal symptoms--a systematic review. Manual therapy. 2004 Aug:9(3):134-43 [PubMed PMID: 15245707]
Level 1 (high-level) evidenceClare HA, Adams R, Maher CG. Reliability of McKenzie classification of patients with cervical or lumbar pain. Journal of manipulative and physiological therapeutics. 2005 Feb:28(2):122-7 [PubMed PMID: 15800512]
Szpalski M, Gunzburg R, Balagué F, Nordin M, Mélot C. A 2-year prospective longitudinal study on low back pain in primary school children. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2002 Oct:11(5):459-64 [PubMed PMID: 12384754]
Feldman DS, Straight JJ, Badra MI, Mohaideen A, Madan SS. Evaluation of an algorithmic approach to pediatric back pain. Journal of pediatric orthopedics. 2006 May-Jun:26(3):353-7 [PubMed PMID: 16670548]
Roffey DM, Ashdown LC, Dornan HD, Creech MJ, Dagenais S, Dent RM, Wai EK. Pilot evaluation of a multidisciplinary, medically supervised, nonsurgical weight loss program on the severity of low back pain in obese adults. The spine journal : official journal of the North American Spine Society. 2011 Mar:11(3):197-204. doi: 10.1016/j.spinee.2011.01.031. Epub [PubMed PMID: 21377601]
Level 3 (low-level) evidenceArnold E, La Barrie J, DaSilva L, Patti M, Goode A, Clewley D. The Effect of Timing of Physical Therapy for Acute Low Back Pain on Health Services Utilization: A Systematic Review. Archives of physical medicine and rehabilitation. 2019 Jul:100(7):1324-1338. doi: 10.1016/j.apmr.2018.11.025. Epub 2019 Jan 24 [PubMed PMID: 30684490]
Level 1 (high-level) evidenceHajihasani A, Rouhani M, Salavati M, Hedayati R, Kahlaee AH. The Influence of Cognitive Behavioral Therapy on Pain, Quality of Life, and Depression in Patients Receiving Physical Therapy for Chronic Low Back Pain: A Systematic Review. PM & R : the journal of injury, function, and rehabilitation. 2019 Feb:11(2):167-176. doi: 10.1016/j.pmrj.2018.09.029. Epub 2019 Feb 11 [PubMed PMID: 30266349]
Level 2 (mid-level) evidence