Definition/Introduction
The atrioventricular node is a specialized component of the cardiac conduction system located within the triangle of Koch at the base of the right atrium (see Image. Cardiac Conduction System Anatomy). The tendon of Todaro bounds this anatomic region, the septal leaflet hinge of the tricuspid valve, and the ostium of the coronary sinus and serves as a critical landmark during electrophysiologic mapping and catheter ablation procedures.[1] The atrioventricular nodal artery most commonly arises from the right coronary artery in right-dominant circulation.
Still, it may originate from the left circumflex artery in left-dominant or codominant systems. Functionally, the atrioventricular node provides the sole normal electrical connection between the atrial and ventricular myocardium, introducing a physiologic conduction delay that optimizes ventricular filling and limits transmission of excessively rapid atrial impulses to the ventricles. In addition to its conduction properties, the atrioventricular junction possesses intrinsic automaticity and may function as a subsidiary pacemaker when sinoatrial node activity fails or becomes excessively slow, thereby generating junctional escape beats or rhythms at an intrinsic rate of approximately 40 to 60 beats per minute.[2]
Histologically, the atrioventricular node is composed of small ovoid and spindle-shaped nodal myocytes embedded within a fibrous collagen-rich matrix. Compared with working atrial and ventricular myocardium, atrioventricular nodal cells exhibit fewer, less densely distributed gap junctions, contributing to slow conduction velocity and decremental conduction. Specialized transitional cell zones connect the surrounding atrial myocardium to the compact atrioventricular node, which continues distally into the penetrating bundle of His.[2] Contemporary investigations further demonstrate that the atrioventricular node is a structurally and functionally heterogeneous conduction network comprising inferior nodal extensions, transitional tissues, and compact nodal elements that collectively influence conduction delay, refractoriness, and susceptibility to arrhythmogenesis.[3]
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
Atrioventricular Block
Disease involving the atrioventricular node or the His–Purkinje conduction system may impair impulse transmission from the atria to the ventricles, resulting in varying degrees of atrioventricular block. Conduction abnormalities may arise from degenerative fibrosis, ischemic injury, infiltrative cardiomyopathies, myocarditis, congenital abnormalities, medication effects, or structural conduction system disease. Second-degree atrioventricular block encompasses both nodal and infranodal conduction disturbances.
Mobitz type I (Wenckebach) most commonly reflects progressive conduction delay within the atrioventricular node itself. In contrast, Mobitz type II more often originates from disease within the His–Purkinje system distal to the atrioventricular node.[4] In Mobitz I atrioventricular block, increasing refractoriness within the atrioventricular node produces progressive PR interval prolongation until an atrial impulse fails to conduct, generating the characteristic grouped beating pattern observed on electrocardiography.[5]
Despite similar nomenclature, Mobitz I and Mobitz II represent fundamentally different pathophysiologic entities with distinct prognostic implications. Mobitz II atrioventricular block generally reflects structural conduction system disease and carries a substantially greater risk of progression to advanced atrioventricular block or complete heart block. Contemporary guideline-directed management recommends permanent pacemaker implantation for acquired Mobitz II atrioventricular block not attributable to reversible or physiologic causes because of the elevated risk of syncope, hemodynamic compromise, and sudden cardiac death.[6] Higher-grade conduction disturbances involving the atrioventricular node and His–Purkinje system remain among the most common indications for permanent pacing worldwide and represent a major source of morbidity, particularly in aging populations with progressive conduction system degeneration.
Atrioventricular Nodal Reentrant Tachycardia
Atrioventricular nodal reentrant tachycardia (AVNRT) is the most common regular supraventricular tachycardia in adults and represents one of the most clinically important disorders directly involving atrioventricular nodal physiology.[7] AVNRT arises from reentry involving dual atrioventricular nodal pathways consisting of functionally distinct fast and slow conduction pathways located within transitional tissues surrounding the compact atrioventricular node. Premature atrial impulses may initiate a reentrant circuit when conduction proceeds antegrade through the slow pathway while retrograde conduction occurs through the fast pathway, producing rapid, regular tachycardia. Clinical manifestations include palpitations, chest discomfort, dyspnea, dizziness, anxiety, and syncope. Catheter ablation targeting the slow pathway remains definitive treatment and achieves high long-term success rates with low procedural complication rates.[7]
Atrioventricular Nodal Ischemia and Inferior Myocardial Infarction
Because the atrioventricular nodal artery most commonly arises from the right coronary artery, ischemia involving the atrioventricular nodal circulation may impair conduction, particularly during an inferior wall myocardial infarction. Atrioventricular block complicating acute coronary syndromes may range from transient first-degree atrioventricular block to complete heart block and carries important prognostic implications. Although atrioventricular nodal dysfunction associated with inferior myocardial infarction is often transient due to ischemia or increased vagal tone, persistent conduction abnormalities may require pacing support or permanent pacemaker implantation.
Drug-Induced Atrioventricular Nodal Dysfunction
Pharmacologic suppression of atrioventricular nodal conduction represents an important and potentially reversible cause of bradyarrhythmias and atrioventricular block. Medications commonly implicated include beta blockers, nondihydropyridine calcium channel blockers, digoxin, adenosine, amiodarone, and other antiarrhythmic agents. Excessive atrioventricular nodal suppression may precipitate symptomatic bradycardia or higher-grade conduction abnormalities, particularly in older adults, in patients with baseline conduction disease, or in individuals receiving multiple atrioventricular nodal-blocking agents. Recognition of medication-induced conduction disturbances is essential because dose adjustment or drug discontinuation may prevent unnecessary device implantation.
Procedural Atrioventricular Nodal Injury
The atrioventricular node and adjacent conduction tissues remain vulnerable during cardiac interventions involving nearby anatomic structures. Catheter ablation procedures, congenital heart surgery, septal defect interventions, and structural heart procedures, including transcatheter aortic valve replacement (TAVR), may result in transient or permanent conduction injury.[8] Conduction disturbances following TAVR remain among the most frequent procedural complications and may necessitate temporary pacing or permanent pacemaker implantation. Procedural planning, imaging guidance, and detailed understanding of atrioventricular nodal anatomy remain critical for minimizing iatrogenic conduction injury.[8]
Congenital and Genetic Conduction Disorders
Congenital atrioventricular conduction abnormalities represent another clinically important category of atrioventricular nodal dysfunction. Congenital complete heart block may occur secondary to maternal anti-Ro/Sjögren syndrome–related antigen A and anti-La/Sjögren syndrome–related antigen B autoantibodies, causing fetal conduction system injury. Inherited channelopathies and genetic conduction disorders affecting ion channel function or conduction system development may also impair atrioventricular nodal conduction and predispose patients to progressive conduction disease.[9]
Lenègre-Lev disease (often grouped as a single entity) is a progressive cardiac conduction disorder characterized by the fibrosis and sclerosis of the heart's electrical pathways.[10] This condition is a leading cause of complete heart block and the need for a pacemaker. Progressive fibrosis and sclerosis of the conduction system remain major contributors to atrioventricular conduction abnormalities in aging populations.
Infiltrative and Inflammatory Disease
Cardiac sarcoidosis, amyloidosis, myocarditis, and Lyme carditis may involve the atrioventricular node and His-Purkinje system, producing conduction abnormalities ranging from first-degree atrioventricular block to complete heart block.[11][12]
Cystic Tumor of the Atrioventricular Nodal Region
Primary cardiac tumors are exceptionally rare, occurring in approximately 0.0017% to 0.03% of autopsy series.[13] Cystic tumor of the atrioventricular nodal region (CTAVN), also termed mesothelioma of the atrioventricular node or endodermal heterotopia, is an uncommon congenital benign cardiac tumor arising near the atrioventricular nodal region within the triangle of Koch, with fewer than 100 cases reported in the literature.[14] Although histologically benign, CTAVN has substantial clinical significance given its close association with the cardiac conduction system. Progressive involvement of the atrioventricular node or penetrating His bundle may result in varying degrees of atrioventricular block, including complete heart block, junctional escape rhythms, syncope, malignant arrhythmias, and sudden cardiac death.[15]
CTAVN is recognized as one of the most important primary cardiac tumors associated with sudden death due to conduction system disruption. Diagnosis remains challenging because patients frequently present with nonspecific symptoms or unexplained conduction abnormalities years before definitive identification. While rare, CTAVN should remain within the differential diagnosis of unexplained high-grade atrioventricular block, particularly in younger individuals without typical degenerative conduction disease risk factors.[16]
Clinical Significance
The atrioventricular node plays a critical role in normal cardiac electrophysiology as the primary electrical bridge between the atrial and ventricular myocardium. Positioned at the junction of the atria and ventricles, the atrioventricular node introduces a physiologic conduction delay that allows adequate ventricular filling following atrial contraction before ventricular systole begins. This delay optimizes cardiac output and mechanical efficiency by preserving atrioventricular synchrony.
Beyond facilitating coordinated contraction, the atrioventricular node exhibits decremental conduction properties that serve as a protective “gatekeeper,” limiting the transmission of excessively rapid atrial impulses to the ventricles. This filtering function becomes particularly important during supraventricular tachyarrhythmias such as atrial fibrillation or atrial flutter, reducing the risk of dangerously elevated ventricular rates and hemodynamic compromise. The atrioventricular node also serves an important backup pacemaking role within the cardiac conduction system.
When sinoatrial node activity fails, or atrial impulse generation becomes inadequate, junctional tissues associated with the atrioventricular node can generate escape rhythms, typically at intrinsic rates of approximately 40 to 60 beats per minute, preserving ventricular activation and maintaining perfusion. Dysfunction involving the atrioventricular node or adjacent His–Purkinje system may result in clinically significant conduction disturbances ranging from first-degree atrioventricular block to complete heart block, potentially producing syncope, heart failure, reduced exercise tolerance, or sudden cardiac death. The atrioventricular node is also central to the pathophysiology of arrhythmias such as atrioventricular nodal reentrant tachycardia (AVNRT), one of the most common forms of paroxysmal supraventricular tachycardia.
Furthermore, the atrioventricular node has major procedural significance in electrophysiologic studies, catheter ablation, congenital heart interventions, and structural cardiac procedures, as inadvertent injury may result in permanent conduction abnormalities that require pacemaker implantation. The atrioventricular node also plays a substantial role in cardiovascular therapeutics and clinical decision-making. Numerous medications, including beta-blockers, nondihydropyridine calcium channel blockers, digoxin, adenosine, and antiarrhythmic agents, exert therapeutic effects by modulating atrioventricular nodal conduction. Pharmacologic atrioventricular nodal blockade remains a cornerstone strategy for ventricular rate control in atrial fibrillation and other supraventricular arrhythmias. Given its central role in cardiac electrophysiology, arrhythmogenesis, and hemodynamic regulation, preservation of atrioventricular nodal function remains essential for maintaining normal cardiovascular performance and optimizing outcomes in patients with cardiac disease.
A solid understanding of atrioventricular nodal anatomy and physiology underpins accurate diagnosis and management of the diverse conduction disturbances and tachyarrhythmias encountered in clinical practice (see Image. Common Atrioventricular Node–Related Supraventricular Arrhythmias). These include:
- Junctional escape beat
- A junctional escape beat or rhythm arises from the atrioventricular junction when sinus impulses fail to reach the ventricles or are excessively delayed, allowing the intrinsic junctional pacemaker (approximately 40–60 bpm) to assume control. On an electrocardiogram (ECG), a junctional escape rhythm typically appears as a regular narrow-QRS rhythm at 40 to 60 beats per minute with absent P waves or inverted P waves that may precede, be inscribed within, or follow the QRS complex due to retrograde atrial activation.[2][17] Junctional escape often emerges as a protective rhythm in the setting of excessive vagal tone, sinus node dysfunction, or high-grade atrioventricular block, when higher pacemakers fail to maintain adequate ventricular activation.
- Accelerated junctional rhythm and junctional tachycardia
- Accelerated junctional rhythm (60–100 bpm) and junctional tachycardia (>100 bpm) are related arrhythmias arising from increased automaticity in the atrioventricular junction, often encountered with digoxin toxicity, myocardial ischemia, or in the early period after cardiac surgery.[18] In both rhythms, the atrioventricular junction serves as the primary ventricular pacemaker, producing a regular narrow-QRS rhythm on the ECG, unless a coexisting bundle-branch block is present. In patients with underlying atrioventricular block or structural conduction disease, accelerated junctional rhythms can coexist with other supraventricular tachyarrhythmias, complicating ECG interpretation.
- AVNRT
- In or near the atrioventricular node, anatomically and functionally distinct fast and slow pathways can conduct electrical impulses. In typical (slow–fast) AVNRT, the reentrant impulse travels antegrade through the slow pathway to activate the His–Purkinje system and ventricles, then returns retrogradely via the fast pathway to the atria, often producing retrograde P waves immediately after the QRS complex on ECG. Multiple atypical AVNRT variations exist, depending on the pathway configurations. Typical AVNRT produces a short-RP narrow-complex tachycardia and may show a pseudo-R′ in lead V1 or pseudo-S waves in the inferior leads.[19] Catheter ablation of the slow pathway is first-line definitive therapy for symptomatic AVNRT.[20]
- Junctional ectopic tachycardia
- Junctional ectopic tachycardia (JET) is a rare focal automatic tachycardia arising from the AV junction, most often seen in infants or early after cardiac surgery.[21][22] In JET, an ectopic automatic focus within the AV junction overrides the sinus node, so that the junctional tissue, rather than the AV node, acts as a gatekeeper, dictating the ventricular rate. The junctional focus drives the ventricles at a rapid rate; atrial activity may be dissociated from ventricular activation or show retrograde conduction, rather than simple 1:1 antegrade AV conduction.[18] JET can be differentiated from AVNRT with adenosine: adenosine usually produces transient AV block without terminating JET, whereas it often terminates AVNRT by interrupting the reentrant circuit.[17][23]
- Wolff–Parkinson–White syndrome
- Wolff–Parkinson–White (WPW) syndrome is a pre-excitation disorder caused by an accessory pathway (typically the Bundle of Kent) that bypasses the atrioventricular node, allowing direct atrioventricular conduction and resulting in early ventricular depolarization.[24] Due to the accessory pathway bypassing the atrioventricular node’s rate-limiting function, the ventricles may be activated at very high rates during supraventricular tachyarrhythmias, which can be particularly dangerous, especially in atrial fibrillation with pre-excitation. On ECG, WPW is characterized by a short PR interval and a widened QRS complex with a slurred initial upstroke, known as the delta wave.[25]
- Atrioventricular reentry tachycardia
- Atrioventricular reentrant tachycardia (AVRT) is a macroreentrant supraventricular tachycardia that requires an accessory pathway between the atrium and ventricle and is commonly associated with WPW. In orthodromic AVRT, the impulse travels anterogradely through the atrioventricular node and His–Purkinje system, and returns retrogradely through the accessory pathway, producing a narrow-QRS tachycardia. In antidromic AVRT, the impulse travels anterogradely through the accessory pathway, resulting in a wide-QRS tachycardia.
- Orthodromic AVRT is distinguished from AVNRT by the conduction pathway. In orthodromic AVRT, conduction travels through the atrium → atrioventricular node/His–Purkinje → ventricle → accessory pathway back to the atrium. In AVNRT, the reentrant circuit is confined within dual atrioventricular nodal pathways and does not require an extranodal accessory pathway. The attached media provides a visual representation.
Nursing, Allied Health, and Interprofessional Team Interventions
Optimal patient care for atrioventricular nodal disorders requires coordinated interprofessional collaboration among physicians, advanced practitioners, nurses, pharmacists, cardiac electrophysiologists, and other healthcare professionals to enhance patient safety, outcomes, and cardiovascular function. Physicians and advanced practitioners play essential roles in recognizing conduction abnormalities, evaluating arrhythmias, interpreting electrocardiographic findings, identifying reversible causes of atrioventricular nodal dysfunction, and determining appropriate medical, procedural, or device-based interventions. Electrophysiologists provide expertise in advanced diagnostic testing, catheter ablation, and management of cardiac implantable electronic devices when indicated. Nursing staff contribute substantially through cardiac rhythm monitoring, medication administration, symptom assessment, patient education, and early recognition of clinical deterioration, including symptomatic bradycardia, syncope, or hemodynamic instability. Pharmacists enhance patient safety by performing medication reconciliation, identifying atrioventricular nodal blocking agents that may worsen conduction disturbances, optimizing antiarrhythmic therapy, and monitoring for adverse drug interactions.
Effective communication and care coordination are particularly important because atrioventricular nodal dysfunction may arise from diverse etiologies, including ischemia, medication effects, infiltrative disease, structural conduction abnormalities, or procedural complications. Timely communication among emergency medicine clinicians, cardiologists, electrophysiologists, pharmacists, nurses, and rehabilitation professionals facilitates rapid diagnosis, escalation of care when pacing support becomes necessary, and implementation of individualized treatment plans. Standardized monitoring protocols, shared clinical decision-making, and coordinated longitudinal follow-up improve patient-centered care while reducing complications associated with arrhythmias, atrioventricular block, or device therapy. Interprofessional collaboration additionally strengthens patient education regarding symptom recognition, medication adherence, and long-term management strategies, ultimately enhancing team performance, cardiovascular outcomes, and overall quality of care for patients with atrioventricular nodal disorders.
Media
(Click Image to Enlarge)
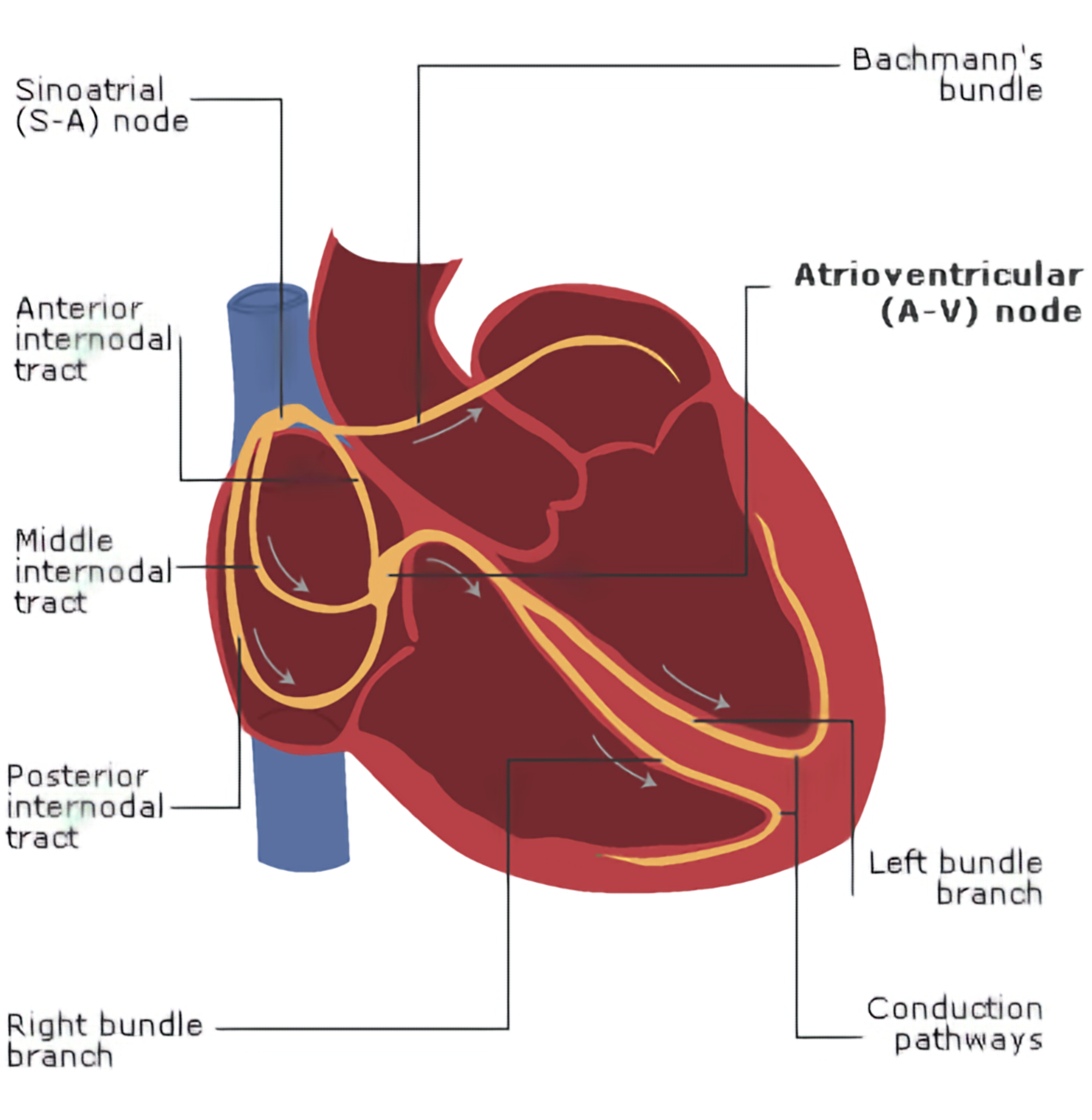
Cardiac Conduction System Anatomy. This is an illustration of the cardiac conduction system, demonstrating the sinoatrial node, atrioventricular node, internodal pathways, bundle branches, and ventricular conduction pathways.
Contributed by the Royal College of Anaesthetists (RCoA) and Association of Anaesthetists of Great Britain and Ireland (AAGBI)
(Click Image to Enlarge)
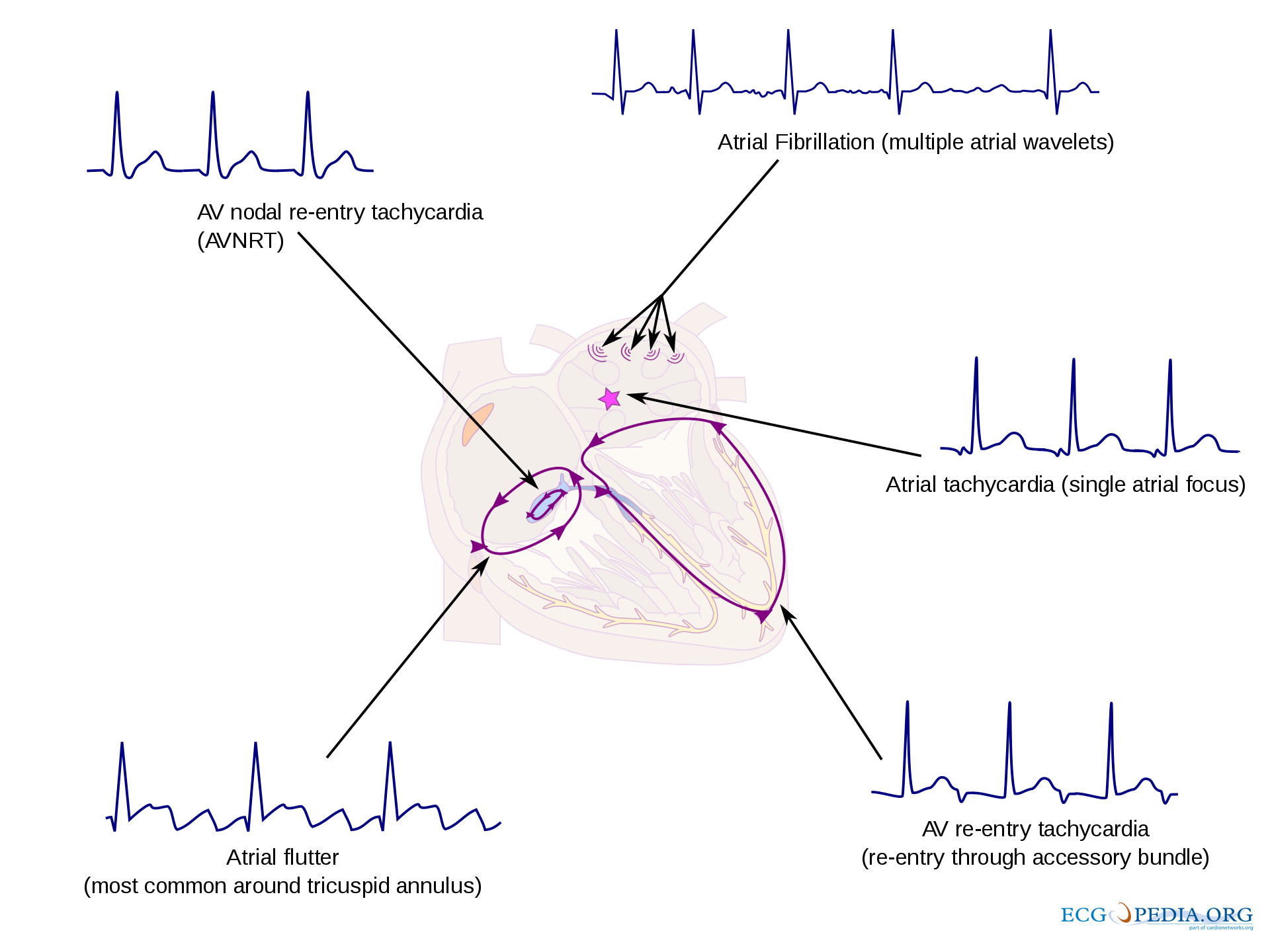
Common Atrioventricular Node–Related Supraventricular Arrhythmias. Illustration of major supraventricular arrhythmias involving the atrioventricular (AV) node and surrounding conduction pathways, including AV nodal reentrant tachycardia (AVNRT), AV reentrant tachycardia (AVRT), atrial flutter, atrial tachycardia, and atrial fibrillation, with representative electrocardiographic patterns.
Contributed by J de Jong, MD
References
Kurian T, Ambrosi C, Hucker W, Fedorov VV, Efimov IR. Anatomy and electrophysiology of the human AV node. Pacing and clinical electrophysiology : PACE. 2010 Jun 1:33(6):754-62. doi: 10.1111/j.1540-8159.2010.02699.x. Epub 2010 Feb 18 [PubMed PMID: 20180918]
Level 3 (low-level) evidencePadala SK, Cabrera JA, Ellenbogen KA. Anatomy of the cardiac conduction system. Pacing and clinical electrophysiology : PACE. 2021 Jan:44(1):15-25. doi: 10.1111/pace.14107. Epub 2020 Nov 12 [PubMed PMID: 33118629]
Pandozi C, Matteucci A, Galeazzi M, Russo M, Lavalle C, Ficili S, Malacrida M, Colivicchi F. New insights into atrioventricular nodal anatomy, physiology, and immunochemistry: A comprehensive review and a proposed model of the slow-fast atrioventricular nodal reentrant tachycardia circuit in agreement with direct potential recordings in the Koch's triangle area. Heart rhythm. 2023 Apr:20(4):614-626. doi: 10.1016/j.hrthm.2023.01.004. Epub 2023 Jan 9 [PubMed PMID: 36634901]
Scheinman MM. Atrioventricular nodal conduction and refractoriness. Pacing and clinical electrophysiology : PACE. 1993 Mar:16(3 Pt 2):592-8 [PubMed PMID: 7681963]
Roberts NK, Cabeen WR. Atrioventricular nodal function in progressive systemic sclerosis: electrophysiological and morphological findings. British heart journal. 1980 Nov:44(5):529-33 [PubMed PMID: 7437193]
Ahmed I, Goyal A, Chhabra L. Atrioventricular Block. StatPearls. 2026 Jan:(): [PubMed PMID: 29083636]
Brugada J, Katritsis DG, Arbelo E, Arribas F, Bax JJ, Blomström-Lundqvist C, Calkins H, Corrado D, Deftereos SG, Diller GP, Gomez-Doblas JJ, Gorenek B, Grace A, Ho SY, Kaski JC, Kuck KH, Lambiase PD, Sacher F, Sarquella-Brugada G, Suwalski P, Zaza A, ESC Scientific Document Group. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). European heart journal. 2020 Feb 1:41(5):655-720. doi: 10.1093/eurheartj/ehz467. Epub [PubMed PMID: 31504425]
Nuche J, Ellenbogen KA, Mittal S, Windecker S, Benavent C, Philippon F, Rodés-Cabau J. Conduction Disturbances After Transcatheter Aortic Valve Replacement: An Update on Epidemiology, Preventive Strategies, and Management. JACC. Cardiovascular interventions. 2024 Nov 25:17(22):2575-2595. doi: 10.1016/j.jcin.2024.07.032. Epub [PubMed PMID: 39603774]
Jimenez E, Ambrose M, Clark B, Wyrebek R. Congenital Heart Block. Clinics in perinatology. 2025 Dec:52(4):709-729. doi: 10.1016/j.clp.2025.08.009. Epub 2025 Sep 30 [PubMed PMID: 41233007]
Zhang W, Wang J, Dong B, Wei J. A case of minor Lenegre's disease. Asian journal of surgery. 2023 Mar:46(3):1439-1440. doi: 10.1016/j.asjsur.2022.09.029. Epub 2022 Sep 24 [PubMed PMID: 36167659]
Level 3 (low-level) evidenceBloom MW, Gorevic PD. Cardiac Amyloidosis. Annals of internal medicine. 2023 Mar:176(3):ITC33-ITC48. doi: 10.7326/AITC202303210. Epub 2023 Mar 14 [PubMed PMID: 36913688]
Sohn DW, Park JB. Cardiac sarcoidosis. Heart (British Cardiac Society). 2023 Jul 12:109(15):1132-1138. doi: 10.1136/heartjnl-2022-321379. Epub 2023 Jul 12 [PubMed PMID: 36631144]
Luc JGY, Phan K, Tchantchaleishvili V. Cystic tumor of the atrioventricular node: a review of the literature. Journal of thoracic disease. 2017 Sep:9(9):3313-3318. doi: 10.21037/jtd.2017.08.101. Epub [PubMed PMID: 29221317]
Sharma G, Linden MD, Schultz DS, Inamdar KV. Cystic tumor of the atrioventricular node: an unexpected finding in an explanted heart. Cardiovascular pathology : the official journal of the Society for Cardiovascular Pathology. 2010 May-Jun:19(3):e75-8. doi: 10.1016/j.carpath.2008.10.011. Epub 2009 Jan 14 [PubMed PMID: 19144541]
Level 3 (low-level) evidenceSuzuki K, Matsushita S, Suzuki H, Kuroda K, Inaba H, Arakawa A, Hayashi T, Amano A, Kuwatsuru R. Cystic tumor of the atrioventricular node: computed tomography and magnetic resonance imaging findings. Journal of thoracic imaging. 2014 Nov:29(6):W97-9. doi: 10.1097/RTI.0000000000000111. Epub [PubMed PMID: 25303965]
Level 3 (low-level) evidenceVelasco A, Goldstein DJ, Slipczuk L, Di Biase L, Manheimer ED. Cystic Tumor of the Atrioventricular Node Causing Rapid-Onset and Reversible Complete Heart Block. JACC. Case reports. 2023 Feb 1:7():101700. doi: 10.1016/j.jaccas.2022.101700. Epub 2022 Dec 17 [PubMed PMID: 36776790]
Level 3 (low-level) evidenceAshraf M, Collier SA. Junctional Ectopic Tachycardia. StatPearls. 2026 Jan:(): [PubMed PMID: 32809686]
Hafeez Y, Wollard K, Grossman SA. Junctional Rhythm. StatPearls. 2026 Jan:(): [PubMed PMID: 29939537]
Katritsis DG. Atrioventricular nodal reentrant tachycardia. Heart rhythm. 2026 Feb:23(2):485-493. doi: 10.1016/j.hrthm.2025.04.009. Epub 2025 Apr 11 [PubMed PMID: 40221112]
Lee PC, Chen SA, Hwang B. Atrioventricular node anatomy and physiology: implications for ablation of atrioventricular nodal reentrant tachycardia. Current opinion in cardiology. 2009 Mar:24(2):105-12. doi: 10.1097/HCO.0b013e328323d83f. Epub [PubMed PMID: 19225293]
Level 3 (low-level) evidenceKylat RI, Samson RA. Junctional ectopic tachycardia in infants and children. Journal of arrhythmia. 2020 Feb:36(1):59-66. doi: 10.1002/joa3.12282. Epub 2019 Dec 3 [PubMed PMID: 32071621]
Catton KG, Peterson JK. Junctional Ectopic Tachycardia: Recognition and Modern Management Strategies. Critical care nurse. 2020 Feb 1:40(1):46-55. doi: 10.4037/ccn2020793. Epub [PubMed PMID: 32006036]
Abdelaziz O, Deraz S. Anticipation and management of junctional ectopic tachycardia in postoperative cardiac surgery: Single center experience with high incidence. Annals of pediatric cardiology. 2014 Jan:7(1):19-24. doi: 10.4103/0974-2069.126543. Epub [PubMed PMID: 24701080]
Elendu C, Babarinde FO, Babatunde OD, Babawale EA, Hassan JI, Ikeji VI, Oshin BD, Nwabueze A, Ngozi-Ibeh JK, Chukwu C, Ighodaro OT, Ikokwu MN, Akinruli OA, Uzzi CI, Sunday OC, Nwachukwu MN, Opara CD, Nwokocha CL, Udoeze CA, Ogidigba PI. Risk stratification and management of arrhythmias in patients with Wolff-Parkinson-White syndrome. Annals of medicine and surgery (2012). 2025 May:87(5):2702-2717. doi: 10.1097/MS9.0000000000003068. Epub 2025 Mar 7 [PubMed PMID: 40337375]
Kesler K, Lahham S. Tachyarrhythmia in Wolff-Parkinson-White Syndrome. The western journal of emergency medicine. 2016 Jul:17(4):469-70. doi: 10.5811/westjem.2016.4.30323. Epub 2016 Jun 16 [PubMed PMID: 27429700]