Introduction
The atrioventricular node is a subendocardial structure located in the inferoposterior right atrium. In an average adult, the atrioventricular node measures approximately 1 × 3 × 5 mm and sits within an anatomic region bordered posteriorly by the coronary sinus ostium, superiorly by the tendon of Todaro, and anteriorly by the septal tricuspid valve annulus. This anatomic region is also commonly referred to as the triangle of Koch. The blood supply to the atrioventricular node arises from the atrioventricular nodal branch of the right coronary artery (90%) or the left circumflex artery (10%), depending on whether the heart has right- or left-coronary dominance. The first septal perforator of the left anterior descending artery also supplies blood to the atrioventricular node.[1][2]
Atrioventricular nodal reentrant tachycardia (AVNRT) is the most common form of paroxysmal supraventricular tachycardia in adults and a frequent cause of symptomatic palpitations presenting to emergency departments and outpatient cardiology clinics. The arrhythmia is characterized by a reentrant circuit that involves functionally distinct pathways within or adjacent to the atrioventricular node, resulting in a rapid, regular tachycardia with narrow QRS complexes in most cases. AVNRT is typically abrupt in onset and termination and may occur in otherwise healthy individuals or in those with underlying structural heart disease.[3]
Clinically, AVNRT is significant because it can cause symptoms such as palpitations, dizziness, chest discomfort, dyspnea, and presyncope or syncope. Although the arrhythmia is usually not life-threatening, recurrent episodes can impair quality of life and occasionally lead to hemodynamic compromise, particularly in older adults or those with limited cardiac reserve. Advances in electrophysiology have clarified the underlying mechanisms of AVNRT and enabled highly effective curative therapy with catheter ablation.[4][5] Electrocardiographic findings based on the reentrant circuits are as follows:
Typical AVNRT (Slow-Fast AVNRT)
Typical AVNRT has a very short RP interval, and P waves appear as:
- A pseudo-S wave in leads II, III, and aVF (see Image. Electrocardiogram of Typical AVNRT With Pseudo-S Waves)
- A pseudo-R' wave in lead V1
Atypical AVNRT (Fast-Slow or Slow-Slow AVNRT)
- Variable RP interval with discrete P waves following the QRS complex (see Image. Electrocardiogram of a Long RP Narrow Complex Tachycardia)
- P waves between the QRS complex and T waves (QRS-P-T complexes), or late P waves after a QRS complex, often mimicking atrial tachycardia
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of AVNRT is primarily related to the presence of dual conduction pathways within or adjacent to the atrioventricular node. These pathways typically consist of a fast pathway, characterized by rapid conduction but a longer refractory period, and a slow pathway, which conducts more slowly but has a shorter refractory period.[6] This dual physiology allows the formation of a reentrant circuit when a premature atrial impulse encounters a refractory fast pathway and conducts through the slow pathway. Once the fast pathway recovers excitability, the impulse can travel retrogradely through it, completing a reentrant loop and initiating tachycardia.
Although the exact cause of dual atrioventricular nodal physiology is not fully understood, evidence suggests that it is related to congenital variations in the architecture of atrioventricular nodal tissue and to transitional cells surrounding the atrioventricular node. Structural heart disease is uncommon in most patients with AVNRT; however, conditions that increase atrial ectopy or alter autonomic tone, such as stress, stimulants, or underlying cardiac disease, may facilitate the initiation of the arrhythmia. Genetic predisposition and age-related changes in conduction tissue have also been suggested to contribute.[7]
Epidemiology
AVNRT is the most common form of paroxysmal supraventricular tachycardia, accounting for approximately 50% to 60% of all supraventricular tachycardia cases encountered in clinical practice.[8] The overall prevalence of supraventricular tachycardia in the general population is estimated at 2.25 per 1000 individuals, with an annual incidence of approximately 35 cases per 100,000 persons. AVNRT can occur at any age, but it most commonly presents in young adults, although some individuals may remain asymptomatic until later decades of life.[9] Female predominance is consistently observed, with roughly two-thirds of cases occurring among women.[10]
In contrast to some other arrhythmias, most patients with AVNRT have structurally normal hearts, and the condition is often seen in otherwise healthy individuals. Familial clustering has also been described, suggesting a possible genetic predisposition, with first-degree relatives having a higher likelihood of developing AVNRT than the general population. Despite its frequent occurrence, AVNRT generally carries a benign prognosis, particularly when appropriate therapy such as catheter ablation is available. Understanding its epidemiologic patterns is important for clinicians because AVNRT represents a substantial proportion of symptomatic tachyarrhythmias evaluated in emergency departments and electrophysiology practices worldwide.
Pathophysiology
These pathways typically consist of a fast pathway, which conducts impulses rapidly but has a relatively long refractory period, and a slow pathway, which conducts more slowly but has a shorter refractory period. Under normal sinus rhythm, atrial impulses preferentially conduct through the fast pathway to the His–Purkinje system. However, when a premature atrial contraction occurs, the fast pathway may still be refractory, forcing the impulse to travel antegrade through the slow pathway.
Because conduction through the slow pathway is delayed, the fast pathway has time to recover excitability. The impulse can then propagate retrogradely up the fast pathway back to the atria, creating a self-sustaining reentrant circuit. This continuous loop of antegrade conduction through the slow pathway and retrograde conduction through the fast pathway results in a rapid, regular tachycardia, typically with rates between 140 and 250 beats per minute. This form, known as typical (slow-fast) AVNRT, accounts for the majority of cases.[2][11]
Less common variants include atypical AVNRT, such as fast-slow and slow-slow forms, where the direction of conduction differs within the nodal pathways. The reentrant circuit is confined to the perinodal atrial tissue and to transitional cells surrounding the atrioventricular node, rather than to the compact atrioventricular node itself. Autonomic tone can significantly influence atrioventricular nodal conduction properties, and increased sympathetic activity or premature atrial beats often trigger tachycardia.[12][13]
Histopathology
Results from histopathologic studies provide important insights into the structural basis of dual atrioventricular nodal pathway physiology observed in AVNRT. The atrioventricular node is a complex structure composed of the compact atrioventricular node, transitional cells, and surrounding atrial myocardium. Histological examinations have demonstrated heterogeneity in the arrangement of these tissues, particularly within the posterior and inferior atrial inputs to the atrioventricular node.
The so-called slow pathway is thought to correspond to inferior extensions of atrioventricular nodal tissue located near the coronary sinus ostium and the tricuspid annulus, where loosely organized transitional cells exhibit slower conduction properties. In contrast, the fast pathway is associated with superior atrial inputs near the interatrial septum, where myocardial fibers are more compact and aligned, allowing faster conduction of impulses. These anatomic differences in cellular organization, fiber orientation, and intercellular coupling create regions with distinct electrophysiologic properties, providing the substrate for dual-pathway conduction and the development of reentrant circuits characteristic of AVNRT.[14][15][16]
History and Physical
Patients with AVNRT usually present with symptoms of rapid onset, rapid offset, and palpitations, which may be associated with dizziness, syncope, and shortness of breath. In older adults, the intermittent palpitations may accompany chest pain. Less common symptoms may include anxiety and polyuria secondary to atrial natriuretic factor, secreted mainly by the atria in response to atrial stretch.
Patients with AVNRT and a known history of coronary artery disease may present with a myocardial infarction, while those with a known history of congestive heart failure may present with an acute exacerbation and possibly reduced ejection fraction secondary to tachycardia-induced cardiomyopathy.[17] Although syncope is uncommon in patients with AVNRT, it is typical in those with a heart rate greater than 170 beats per minute (bpm), because impaired ventricular filling reduces cardiac output and cerebral perfusion. Depression of the sinoatrial node secondary to tachycardia also may contribute to syncopal symptoms in patients who present with AVNRT.[18]
Patients with AVNRT usually present with a heart rate between 140 and 280 bpm. During a physical examination, a clinician might be able to appreciate cannon A waves as the atrium contracts in conjunction with the ventricular contractions against a closed tricuspid valve. Hypotension secondary to decreased ventricular filling also may be a significant physical examination finding in patients presenting with AVNRT.[19]
Evaluation
Evaluation of a patient with suspected AVNRT begins with a careful clinical history and physical examination. Patients typically present with sudden-onset palpitations that start and terminate abruptly, often accompanied by dizziness, dyspnea, chest discomfort, or anxiety. A 12-lead electrocardiogram obtained during tachycardia is the most important diagnostic tool and usually demonstrates a regular narrow-complex tachycardia with rates between 140 and 250 bpm, often with absent or retrograde P waves (see Image. Electrocardiogram of Typical AVNRT With Pseudo-S Waves). When the arrhythmia is not captured on a resting electrocardiogram, ambulatory monitoring such as Holter monitoring or event recorders may help document intermittent episodes.
An echocardiogram is not necessary, but can be considered in a select group of patients, especially when structural heart disease is suspected. Laboratory evaluation is generally directed toward identifying reversible triggers, including electrolyte abnormalities or thyroid dysfunction. In uncertain cases, an electrophysiology study may be performed to confirm dual atrioventricular nodal physiology, establish the diagnosis, and provide the opportunity for catheter ablation therapy.[20][21]
Treatment / Management
Management of AVNRT depends on the patient’s hemodynamic stability and the frequency or severity of symptoms. Treatment strategies include acute termination of the tachycardia in the emergency setting and long-term therapies aimed at preventing recurrence.[22][23] Acute management focuses on the prompt termination of the arrhythmia.(A1)
In patients who are hemodynamically stable, vagal maneuvers such as the Valsalva maneuver or carotid sinus massage are recommended as the initial intervention because they increase parasympathetic tone and transiently slow atrioventricular nodal conduction or produce transient atrioventricular nodal block. If vagal maneuvers fail, intravenous adenosine is considered the first-line pharmacologic therapy because of its rapid onset and short half-life, which transiently blocks atrioventricular nodal conduction and interrupts the reentrant circuit.[24][25] When adenosine is contraindicated or ineffective, intravenous nondihydropyridine calcium channel blockers (verapamil or diltiazem) or β-blockers may be administered to slow atrioventricular nodal conduction and terminate the tachycardia. In patients with hemodynamic instability, immediate synchronized electrical cardioversion is indicated to restore sinus rhythm.[26](B2)
Long-term management aims to reduce recurrent episodes and improve quality of life. For patients with infrequent or minimally symptomatic episodes, conservative management or intermittent use of vagal maneuvers may be sufficient. Pharmacologic therapy with oral β-blockers, verapamil, or diltiazem can be used to prevent recurrence by suppressing atrioventricular nodal conduction.
However, medications may have limited efficacy and potential adverse effects. Consequently, catheter ablation of the slow pathway has become the preferred definitive therapy for symptomatic AVNRT.[22][23] Radiofrequency ablation targets the slow pathway, eliminating the substrate for reentry while preserving normal atrioventricular nodal conduction.(A1)
Catheter ablation has a success rate exceeding 95%, with a low risk of complications, including a small risk of complete atrioventricular block requiring pacemaker implantation. Please see StatPearls' companion reference, "Electrophysiology Study and Ablation of Atrioventricular Nodal Tachycardia," for further information. Therefore, current guidelines recommend catheter ablation as first-line therapy for many symptomatic patients, particularly those with recurrent or drug-refractory episodes.
Differential Diagnosis
Once a narrow QRS complex tachycardia is present on an electrocardiogram, and the rhythm is determined to be regular, differential rhythms include the following:
- Atrioventricular nodal reentrant tachycardia
- Atrioventricular reentrant tachycardia
- Intra-atrial reentrant tachycardia
- Sinoatrial nodal reentrant tachycardia
- Junctional ectopic tachycardia
- Atrial tachycardia [27]
Prognosis
The prognosis of AVNRT is generally excellent, particularly in individuals without structural heart disease. The arrhythmia is typically benign and rarely associated with increased mortality. Most patients experience recurrent but well-tolerated episodes of palpitations, and long-term outcomes are favorable with appropriate treatment.
Catheter ablation of the slow pathway has become the definitive therapy, with success rates exceeding 95%, low recurrence rates, and minimal complications. As a result, most patients achieve durable symptom relief and an excellent quality of life following treatment. In rare cases, patients may develop other atrial arrhythmias, such as atrial fibrillation, during long-term follow-up.[28]
Complications
Although AVNRT is generally considered a benign arrhythmia, several complications may occur, particularly in patients with frequent or prolonged episodes. Persistent tachycardia can lead to hemodynamic instability, presenting with hypotension, presyncope, or syncope due to reduced ventricular filling and decreased cardiac output. Recurrent episodes may also cause tachycardia-induced cardiomyopathy, especially when the arrhythmia remains undiagnosed or inadequately treated for prolonged periods.
Patients with underlying structural heart disease may experience worsening heart failure symptoms during sustained tachycardia. Additionally, frequent symptomatic episodes can significantly impair quality of life, leading to anxiety, reduced exercise tolerance, and repeated health care utilization. Complications may also arise from therapeutic interventions; for example, pharmacologic therapy with atrioventricular nodal blocking agents may result in bradycardia or hypotension, while catheter ablation, although highly effective, carries a small risk of atrioventricular block that may require permanent pacemaker implantation. Overall, serious complications are uncommon, and most patients have excellent outcomes with appropriate management.[22][23]
Deterrence and Patient Education
Patient education plays an important role in the management of AVNRT. Patients should be informed that AVNRT is generally a benign arrhythmia with an excellent prognosis, particularly in the absence of structural heart disease. Education should focus on recognizing common symptoms such as sudden-onset palpitations, dizziness, or shortness of breath, and understanding when to seek medical attention. Patients can also be taught simple vagal maneuvers, such as the Valsalva maneuver, which may help terminate tachycardia episodes.
Avoidance of potential triggers, including excessive caffeine, alcohol, stimulant medications, and emotional stress, may reduce the frequency of episodes in some individuals. Patients with recurrent or symptomatic episodes should be counseled about the effectiveness and safety of catheter ablation as a definitive treatment option. Additionally, patients should be encouraged to maintain regular follow-up with their health care professional and adhere to prescribed medications when medical therapy is used.
Pearls and Other Issues
In rare instances, atrioventricular nodal reentry tachycardia can result in sudden cardiac arrest.[29]
Enhancing Healthcare Team Outcomes
Optimal management of AVNRT relies on coordinated interdisciplinary teamwork to ensure rapid diagnosis and effective treatment. Patients typically present with sudden-onset palpitations and a regular narrow-complex tachycardia, and timely recognition is essential to initiate appropriate therapy. Patients with hemodynamic instability require immediate synchronized cardioversion, while patients who are stable are generally treated with a stepwise approach beginning with vagal maneuvers followed by pharmacologic therapy such as adenosine or other atrioventricular nodal blocking agents.
Nursing staff play a key role in obtaining rapid electrocardiograms, initiating vagal maneuvers, establishing intravenous access, and monitoring for complications. Pharmacists help verify contraindications to medications and ensure appropriate dosing and administration of antiarrhythmic medications. Clinicians are responsible for accurate rhythm diagnosis, assessment of hemodynamic stability, and treatment planning. Early involvement of electrophysiology specialists facilitates timely evaluation for catheter ablation, a highly effective, definitive therapy that improves symptom control and overall patient outcomes.
Media
(Click Image to Enlarge)
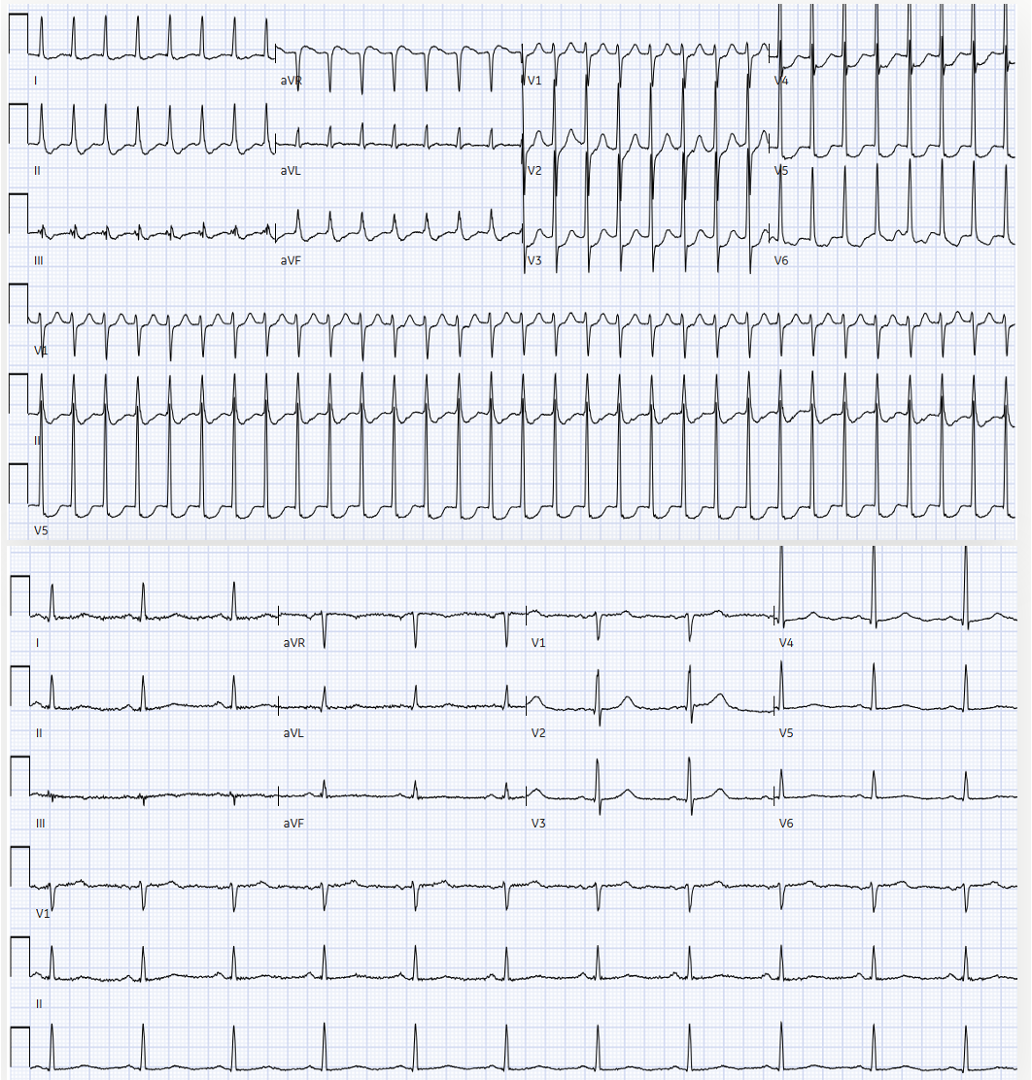
Electrocardiogram of a Long RP Narrow Complex Tachycardia. This 12-lead electrocardiogram demonstrates a regular, narrow-complex supraventricular tachycardia with a long RP interval and retrograde P-waves (inverted in leads II, III, and aVF; upright in V1).
Contributed by Y Hafeez, DO
(Click Image to Enlarge)
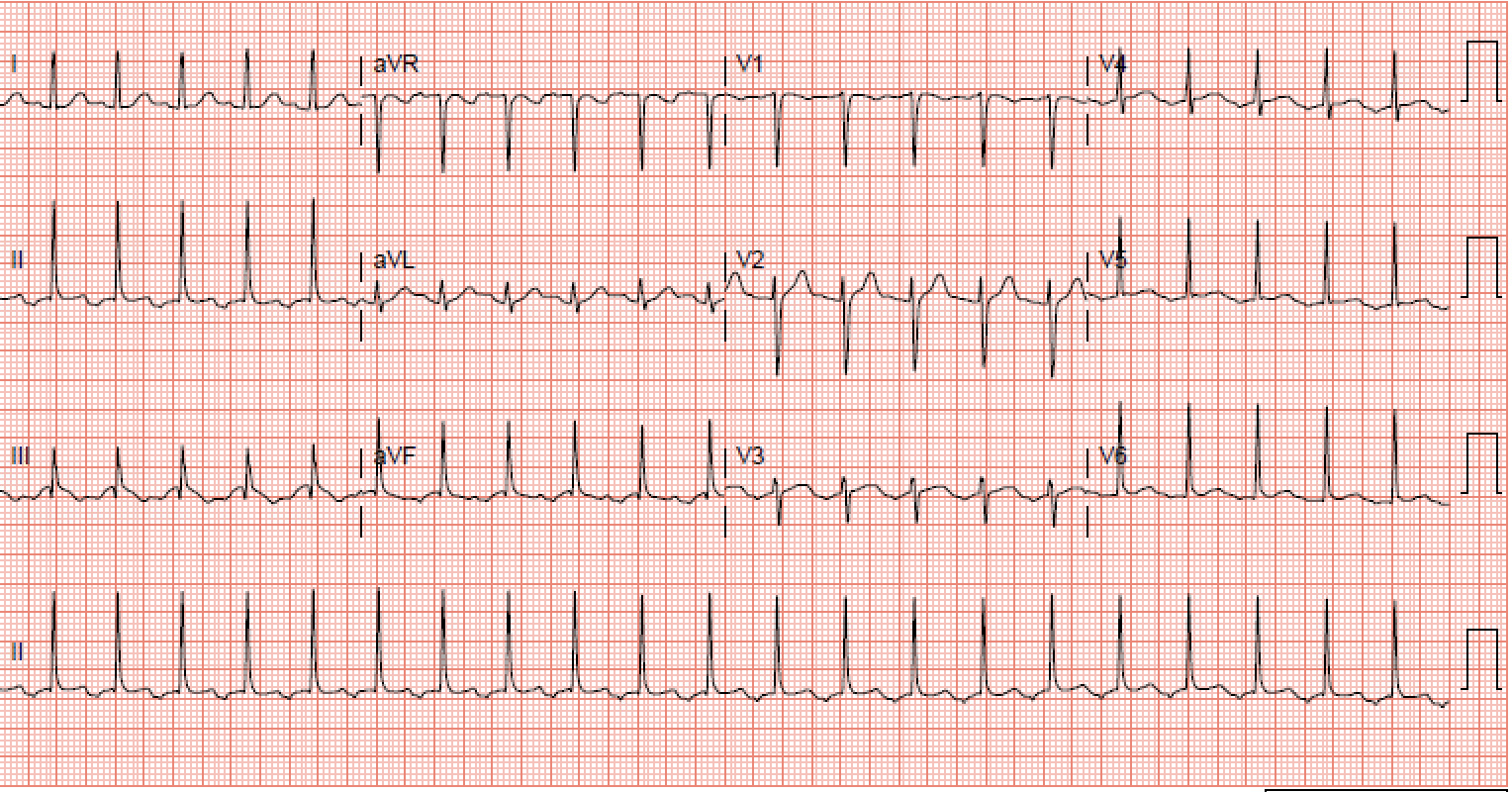
Electrocardiogram of Typical AVNRT With Pseudo-S Waves. This 12-lead electrocardiogram demonstrates typical (slow-fast) atrioventricular nodal reentrant tachycardia (top panel) featuring characteristic terminal pseudo-S waves, representing retrograde P-wave activity, which are absent in the baseline sinus rhythm (bottom panel).
Contributed by I Ahmed, MD
References
Inoue S, Becker AE. Koch's triangle sized up: anatomical landmarks in perspective of catheter ablation procedures. Pacing and clinical electrophysiology : PACE. 1998 Aug:21(8):1553-8 [PubMed PMID: 9725153]
Level 3 (low-level) evidencePandozi C, Matteucci A, Galeazzi M, Russo M, Lavalle C, Ficili S, Malacrida M, Colivicchi F. New insights into atrioventricular nodal anatomy, physiology, and immunochemistry: A comprehensive review and a proposed model of the slow-fast atrioventricular nodal reentrant tachycardia circuit in agreement with direct potential recordings in the Koch's triangle area. Heart rhythm. 2023 Apr:20(4):614-626. doi: 10.1016/j.hrthm.2023.01.004. Epub 2023 Jan 9 [PubMed PMID: 36634901]
Katritsis DG. Atrioventricular nodal reentrant tachycardia. Heart rhythm. 2026 Feb:23(2):485-493. doi: 10.1016/j.hrthm.2025.04.009. Epub 2025 Apr 11 [PubMed PMID: 40221112]
Etaee F, Elayi CS, Catanzarro J, Delisle B, Ogunbayo G, Di Biase L, Natale A, Darrat Y. Gender associated disparities in atrioventricular nodal reentrant tachycardia: A review article. Journal of cardiovascular electrophysiology. 2021 Jun:32(6):1772-1777. doi: 10.1111/jce.15078. Epub 2021 May 16 [PubMed PMID: 33969588]
Ector J, Haemers P, Garweg C, Willems R. Diagnosis and treatment of atrioventricular nodal reentrant tachycardia: a case report illustrating clinical management and ablation strategy. European heart journal. Case reports. 2020 Aug:4(4):1-7. doi: 10.1093/ehjcr/ytaa129. Epub 2020 Jul 8 [PubMed PMID: 32975532]
Level 3 (low-level) evidencevon Bary C, Eckardt L, Steven D, Neuberger HR, Tilz RR, Bonnemeier H, Thomas D, Deneke T, Estner HL, Kuniss M, Luik A, Sommer P, Voss F, Meyer C, Shin DI, Kriatselis C. [AV nodal reentrant tachycardia. Diagnosis and therapy]. Herzschrittmachertherapie & Elektrophysiologie. 2015 Dec:26(4):351-8. doi: 10.1007/s00399-015-0399-x. Epub [PubMed PMID: 26558907]
Heidbüchel H, Jackman WM. Characterization of subforms of AV nodal reentrant tachycardia. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2004 Jul:6(4):316-29 [PubMed PMID: 15172656]
Link MS. Clinical practice. Evaluation and initial treatment of supraventricular tachycardia. The New England journal of medicine. 2012 Oct 11:367(15):1438-48. doi: 10.1056/NEJMcp1111259. Epub [PubMed PMID: 23050527]
Michowitz Y, Anis-Heusler A, Reinstein E, Tovia-Brodie O, Glick A, Belhassen B. Familial Occurrence of Atrioventricular Nodal Reentrant Tachycardia. Circulation. Arrhythmia and electrophysiology. 2017 Feb:10(2):e004680. doi: 10.1161/CIRCEP.116.004680. Epub [PubMed PMID: 28213508]
Liuba I, Jönsson A, Säfström K, Walfridsson H. Gender-related differences in patients with atrioventricular nodal reentry tachycardia. The American journal of cardiology. 2006 Feb 1:97(3):384-8 [PubMed PMID: 16442401]
Park S, Park JW, Choi Y. The Upper Common Pathway in Atrioventricular Nodal Reentrant Tachycardia: A Comprehensive Review of Evidence and Current Perspectives. Reviews in cardiovascular medicine. 2024 Mar:25(3):109. doi: 10.31083/j.rcm2503109. Epub 2024 Mar 15 [PubMed PMID: 39076935]
Level 3 (low-level) evidenceMarzlin KM. Atrioventricular Nodal Reentrant Tachycardia. AACN advanced critical care. 2017 Spring:28(1):84-88. doi: 10.4037/aacnacc2017887. Epub [PubMed PMID: 28254859]
Zeng R, Li F, Jiang J, Cui K, Yang Q, Gao J, Zhu X, Shi T, Li W, Tong Y, Zhang Q, Hu H, Fu H. The Safety and Feasibility of Pulsed-Field Ablation in Atrioventricular Nodal Re-Entrant Tachycardia: First-in-Human Pilot Trial. JACC. Clinical electrophysiology. 2024 Jan:10(1):82-92. doi: 10.1016/j.jacep.2023.08.030. Epub 2023 Oct 11 [PubMed PMID: 37831032]
Level 2 (mid-level) evidenceAnderson RH, Sánchez-Quintana D, Nevado-Medina J, Spicer DE, Tretter JT, Lamers WH, Hu Z, Cook AC, Sternick EB, Katritsis DG. The Anatomy of the Atrioventricular Node. Journal of cardiovascular development and disease. 2025 Jun 26:12(7):. doi: 10.3390/jcdd12070245. Epub 2025 Jun 26 [PubMed PMID: 40710771]
Tretter JT, Spicer DE, Sánchez-Quintana D, Back Sternick E, Farré J, Anderson RH. Miniseries 1-Part III: 'Behind the scenes' in the triangle of Koch. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2022 Mar 2:24(3):455-463. doi: 10.1093/europace/euab285. Epub [PubMed PMID: 34999775]
Katritsis DG, Anderson RH. New insights into the mechanisms of fast and slow conduction in the atrioventricular node. Heart rhythm. 2023 Apr:20(4):627-630. doi: 10.1016/j.hrthm.2022.08.025. Epub 2022 Aug 30 [PubMed PMID: 36049588]
Ganz LI, Friedman PL. Supraventricular tachycardia. The New England journal of medicine. 1995 Jan 19:332(3):162-73 [PubMed PMID: 7800009]
Leitch JW, Klein GJ, Yee R, Leather RA, Kim YH. Syncope associated with supraventricular tachycardia. An expression of tachycardia rate or vasomotor response? Circulation. 1992 Mar:85(3):1064-71 [PubMed PMID: 1537103]
Goyal R, Zivin A, Souza J, Shaikh SA, Harvey M, Bogun F, Daoud E, Man KC, Strickberger SA, Morady F. Comparison of the ages of tachycardia onset in patients with atrioventricular nodal reentrant tachycardia and accessory pathway-mediated tachycardia. American heart journal. 1996 Oct:132(4):765-7 [PubMed PMID: 8831363]
Wood KA, Drew BJ, Scheinman MM. Frequency of disabling symptoms in supraventricular tachycardia. The American journal of cardiology. 1997 Jan 15:79(2):145-9 [PubMed PMID: 9193013]
Level 2 (mid-level) evidenceDoi A, Miyamoto K, Uno K, Nakata T, Tsuchihashi K, Shimamoto K. Studies on hemodynamic instability in paroxysmal supraventricular tachycardia: noninvasive evaluations by head-up tilt testing and power spectrum analysis on electrocardiographic RR variation. Pacing and clinical electrophysiology : PACE. 2000 Nov:23(11 Pt 1):1623-31 [PubMed PMID: 11138299]
Page RL, Joglar JA, Caldwell MA, Calkins H, Conti JB, Deal BJ, Estes NA 3rd, Field ME, Goldberger ZD, Hammill SC, Indik JH, Lindsay BD, Olshansky B, Russo AM, Shen WK, Tracy CM, Al-Khatib SM, Evidence Review Committee Chair‡. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2016 Apr 5:133(14):e506-74. doi: 10.1161/CIR.0000000000000311. Epub 2015 Sep 23 [PubMed PMID: 26399663]
Level 1 (high-level) evidenceBrugada J, Katritsis DG, Arbelo E, Arribas F, Bax JJ, Blomström-Lundqvist C, Calkins H, Corrado D, Deftereos SG, Diller GP, Gomez-Doblas JJ, Gorenek B, Grace A, Ho SY, Kaski JC, Kuck KH, Lambiase PD, Sacher F, Sarquella-Brugada G, Suwalski P, Zaza A, ESC Scientific Document Group. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). European heart journal. 2020 Feb 1:41(5):655-720. doi: 10.1093/eurheartj/ehz467. Epub [PubMed PMID: 31504425]
Glatter KA, Cheng J, Dorostkar P, Modin G, Talwar S, Al-Nimri M, Lee RJ, Saxon LA, Lesh MD, Scheinman MM. Electrophysiologic effects of adenosine in patients with supraventricular tachycardia. Circulation. 1999 Mar 2:99(8):1034-40 [PubMed PMID: 10051297]
Level 2 (mid-level) evidenceRankin AC, Brooks R, Ruskin JN, McGovern BA. Adenosine and the treatment of supraventricular tachycardia. The American journal of medicine. 1992 Jun:92(6):655-64 [PubMed PMID: 1605147]
Peng G, Zei PC. Diagnosis and Management of Paroxysmal Supraventricular Tachycardia. JAMA. 2024 Feb 20:331(7):601-610. doi: 10.1001/jama.2024.0076. Epub [PubMed PMID: 38497695]
Spector P, Reynolds MR, Calkins H, Sondhi M, Xu Y, Martin A, Williams CJ, Sledge I. Meta-analysis of ablation of atrial flutter and supraventricular tachycardia. The American journal of cardiology. 2009 Sep 1:104(5):671-7. doi: 10.1016/j.amjcard.2009.04.040. Epub [PubMed PMID: 19699343]
Level 1 (high-level) evidenceFrey MK, Richter B, Gwechenberger M, Marx M, Pezawas T, Schrutka L, Gössinger H. High incidence of atrial fibrillation after successful catheter ablation of atrioventricular nodal reentrant tachycardia: a 15.5-year follow-up. Scientific reports. 2019 Aug 13:9(1):11784. doi: 10.1038/s41598-019-47980-1. Epub 2019 Aug 13 [PubMed PMID: 31409803]
Wang YS, Scheinman MM, Chien WW, Cohen TJ, Lesh MD, Griffin JC. Patients with supraventricular tachycardia presenting with aborted sudden death: incidence, mechanism and long-term follow-up. Journal of the American College of Cardiology. 1991 Dec:18(7):1711-9 [PubMed PMID: 1960318]
Level 2 (mid-level) evidence