 Asthma: Allergic, Nonallergic, and Environmental Phenotypes
Asthma: Allergic, Nonallergic, and Environmental Phenotypes
Introduction
Asthma is a chronic inflammatory airway disease characterized by variable and reversible expiratory airflow obstruction, bronchial hyperresponsiveness, and airway inflammation. Asthma is among the most prevalent noncommunicable diseases globally, affecting an estimated 262 million people and contributing to approximately 455,000 deaths annually.[1]
In the US, current data from the Centers for Disease Control and Prevention indicate that approximately 27.5 million people (8.4% of the population) have asthma, including approximately 6 million children younger than 18 years.[CDC. Most Recent Asthma Data]. The disease manifests through recurrent respiratory tract symptoms, including wheezing, dyspnea, chest tightness, and cough, that fluctuate in frequency and severity, often in response to identifiable triggers.
Asthma is not a single, uniform disease but rather a heterogeneous syndrome encompassing distinct clinical and inflammatory phenotypes. The 2 most clinically relevant broad categories are allergic (atopic) asthma and nonallergic (intrinsic or environmentally induced) asthma, though considerable overlap exists. Allergic asthma, the most common phenotype particularly in children and young adults, is driven by IgE-mediated sensitization to environmental allergens and is frequently associated with comorbid atopic conditions including allergic rhinitis, atopic dermatitis, and food allergy.[2] Environmentally induced asthma encompasses a broader spectrum, including occupational asthma triggered by workplace sensitizers or irritants, and asthma exacerbated by air pollutants, tobacco smoke, and other inhaled agents.
Contemporary understanding of asthma pathobiology has advanced substantially, enabling a precision medicine approach guided by inflammatory biomarkers: blood eosinophil count, total and specific IgE, and fractional exhaled nitric oxide (FeNO). These advances have driven the development of multiple biologic agents targeting the type 2 inflammatory cascade.[3] Asthma imposes an estimated $80 billion annual economic burden in the US alone, accounting for more than 13 million missed school days and significant lost worker productivity.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of asthma is multifactorial, arising from a complex interaction between genetic susceptibility and environmental exposures. The fundamental underlying mechanism across all asthma subtypes is an exaggerated and dysregulated hypersensitivity response of the airways to various stimuli. Allergic asthma is predominantly driven by an IgE-mediated (type 1 hypersensitivity) response to specific allergens, leading to activation of mast cells, eosinophils, T lymphocytes, basophils, and type 2 innate lymphoid cells, with resultant airway inflammation, epithelial injury, and bronchospasm.[3]
The strongest identifiable risk factor for the development of asthma is a personal or family history of atopic disease. Individuals with allergic rhinitis, atopic dermatitis, or food allergy carry a substantially elevated risk of asthma, reflecting shared mechanisms of type 2 immune dysregulation. Specific genetic loci, including those encoding the high-affinity IgE receptor (FcεRI) and the IL-4 receptor α chain (IL-4Rα), have been associated with asthma susceptibility.[[4]]
Environmental and Allergic Triggers
- House dust mites (Dermatophagoides pteronyssinus and Dermatophagoides farinae): the most common indoor allergen worldwide; mite fecal particles are the primary sensitizing agent.[3][4]
- Animal dander: Cat and dog allergens are the most clinically significant; cat allergen remains airborne for hours and persists on surfaces and clothing
- Cockroach (Blattella germanica): major driver of urban pediatric asthma morbidity, particularly in low-income communities; the kitchen is the highest-concentration area.[CDC. Most Recent Asthma Data]
- Mold: Alternaria, Aspergillus, Cladosporium, and Penicillium species; exposure to Alternaria species is a risk factor for near-fatal asthma
- Environmental tobacco smoke: maternal smoking during pregnancy and postnatal secondhand exposure are independently associated with substantially increased risk of childhood asthma development and more severe disease course.[5]
- Outdoor air pollutants: traffic-related air pollution, particulate matter measuring 2.5 µm or less in diameter, particulate matter measuring 10 μm or less in diameter, ozone, and nitrogen dioxide can trigger acute exacerbations and worsen underlying airway inflammation even at low concentrations.[4]
- Exercise and cold air: trigger bronchoconstriction through airway drying and hyperosmolar changes in airway surface liquid
- Gastroesophageal reflux disease: microaspiration and vagally mediated reflex bronchoconstriction contribute to asthma exacerbations in 50% to 80% of patients with difficult-to-control asthma.[2]
- Respiratory viral infections: rhinovirus is the most common trigger of acute exacerbations in both children and adults; respiratory syncytial virus in early infancy may promote subsequent sensitization and asthma development[4]
- Nonsteroidal anti-inflammatory drugs and aspirin: cyclooxygenase-1 inhibition leads to cysteinyl leukotriene overproduction in susceptible individuals, producing aspirin-exacerbated respiratory disease, which affects approximately 10% of adults with asthma.[3]
Occupational Asthma
Occupational asthma represents approximately 15% of new adult-onset asthma cases and is the most prevalent occupational lung disease in industrialized countries.[6] Occupational asthma is categorized as either sensitizer-induced (immunologically mediated, with a latency period; caused by high-molecular-weight agents such as flour, latex, and animal proteins, or low-molecular-weight agents such as isocyanates, acid anhydrides, and reactive dyes) or irritant-induced (nonimmunologic, including reactive airways dysfunction syndrome following a single high-level irritant exposure). Occupational asthma should be considered in any adult with new-onset or significantly worsening asthma, especially when symptoms improve during weekends and holidays away from work.
The Hygiene Hypothesis and Microbiome
The hygiene hypothesis proposes that reduced childhood exposure to microbial organisms in increasingly sanitized environments impairs normal immune maturation, promoting a type 2 helper T-cell–skewed immune phenotype that predisposes to atopy and asthma. Epidemiologic observations support the hygiene hypothesis because farm exposure, large sibship size, early daycare attendance, and rural childhood environments are protective against asthma development.[7] Results from more recent microbiome research demonstrated that dysbiosis of the early-life airway and gut microbial communities, particularly reductions in Faecalibacterium, Lachnospira, Veillonella, and Rothia species in infancy, is associated with elevated asthma risk in prospective cohort studies, representing a promising target for preventive interventions.
Epidemiology
Asthma is a global health challenge of substantial magnitude. According to the most recent Global Burden of Disease data, an estimated 262 million people worldwide have asthma, contributing to approximately 455,000 deaths annually, although this figure may underestimate true mortality because of widespread underdiagnosis.[1] In the US, current National Health Interview Survey data from the Centers for Disease Control and Prevention indicate that approximately 27.5 million Americans (8.4%) have current asthma, including approximately 6 million children.[CDC. Most Recent Asthma Data] The economic burden of asthma in the US is estimated to exceed $80 billion annually in combined direct medical costs and indirect costs from lost productivity and school and work absenteeism.
Age and Sex
Asthma demonstrates a bimodal pattern. In childhood, the disease is more prevalent in boys, which likely reflects smaller airway caliber relative to lung size. After puberty, the sex distribution reverses. Asthma prevalence is higher among adult women (approximately 9.7%) than among men (approximately 6.5%), a difference attributed in part to hormonal influences on airway inflammation and mast cell function.[CDC. Most Recent Asthma Data]
Racial and Ethnic Disparities
Significant disparities characterize asthma epidemiology in the US. Black individuals have the highest asthma prevalence (approximately 10.9%), the highest emergency department visit rates, and asthma mortality rates approximately 2 to 3 times higher than White individuals. Puerto Rican individuals have the highest asthma prevalence among Hispanic subgroups. Factors contributing to these disparities include complex interactions among socioeconomic factors, housing conditions (indoor allergen burden, mold), environmental exposures (proximity to air pollution), access to controller medications, and structural inequities in healthcare delivery.[CDC. Most Recent Asthma Data]
Healthcare Utilization
Asthma accounts for more than 1.6 million emergency department visits, approximately 180,000 hospitalizations, and 3500 to 4000 deaths annually in the US. Among chronic diseases, asthma is the leading cause of school absenteeism, contributing to more than 13 million missed school days per year.[CDC. Most Recent Asthma Data]
Occupational Burden
The annual incidence of occupational asthma ranges from 12 to 170 new cases per million workers, with a prevalence of 5% to 15% across industries such as baking, animal handling, woodworking, health care (latex), and chemical manufacturing.[6]
Pathophysiology
The pathophysiology of asthma is characterized by 3 interdependent processes: airway inflammation, bronchial hyperresponsiveness, and variable and reversible airflow obstruction (see Image. Pathophysiology of Asthma). In the majority of patients, particularly those with allergic asthma, type 2 inflammation driven by type 2 helper T lymphocytes, mast cells, eosinophils, and type 2 innate lymphoid cells is the dominant inflammatory pathway.[2][8][9]
Type 2 Inflammatory Pathway
Allergen exposure activates airway epithelial cells to release alarmins, including thymic stromal lymphopoietin, IL-33, and IL-25, which promote type 2 helper T-lymphocyte differentiation and type 2 innate lymphoid cell activation. The resulting pathways converge on the production of IL-4, IL-5, and IL-13, the cardinal type 2 cytokines. IL-4 and IL-13 drive IgE class switching in B cells, promote mucus hypersecretion, and increase airway smooth muscle hyperresponsiveness. IL-5 is the principal eosinophil survival and maturation factor, driving eosinophilic airway inflammation.[2][3][8]
IgE produced by plasma cells binds to high-affinity FcεRI receptors on mast cells and basophils. Subsequent allergen cross-linking triggers degranulation and the release of histamine, cysteinyl leukotrienes, prostaglandin D2, and proteases, producing immediate bronchoconstriction, known as the early-phase asthmatic response, followed hours later by the late-phase response, driven by eosinophil and T-cell recruitment.[2]
Blood eosinophil count and FeNO are the 2 best-validated clinical biomarkers of T2 airway inflammation. FeNO levels of 25 parts per billion or greater in adults and 35 parts per billion (ppb) or greater in children indicate eosinophilic airway inflammation with high specificity and directly predict corticosteroid responsiveness and response to anti–IL-4 receptor α therapy with dupilumab.[10][11]
Non–T2 Inflammatory Pathway
Approximately 30% to 50% of adults with severe asthma demonstrate a predominantly neutrophilic or paucigranulocytic (non-T2) airway inflammatory pattern. Associated factors include obesity, active smoking or a history of smoking, older age at onset, and occupational or pollutant exposures. Non-T2 asthma is typically less responsive to corticosteroids and does not respond to anti–IL-5 or anti-IgE biologic agents. Tezepelumab, which acts upstream at the thymic stromal lymphopoietin level before the T2 and non-T2 bifurcation, is the only approved biologic agent with demonstrated efficacy across both T2-high and non–T2 phenotypes.[12][13]
Airway Remodeling
In a subset of patients with longstanding, poorly controlled asthma, structural airway remodeling occurs, characterized by subepithelial fibrosis, smooth muscle hypertrophy and hyperplasia, goblet cell hyperplasia, increased vascularity, and thickening of the reticular basement membrane. The resulting structural changes cause fixed (irreversible) airflow obstruction that is unresponsive to bronchodilator therapy. Results from studies showed that early initiation of inhaled corticosteroid therapy attenuated, but did not fully prevent, remodeling.[2][3]
Histopathology
The histopathologic features of asthma are identifiable in endobronchial biopsy specimens even in patients with mild disease and include:
- Epithelial desquamation and fragility, with loss of ciliated columnar cells and goblet cell hyperplasia (mucous metaplasia)[14]
- Thickening of the reticular basement membrane (subepithelial fibrosis), the hallmark of airway remodeling, which correlates with disease duration and severity
- Dense inflammatory infiltrate, with eosinophils and mast cells predominating in T2-high disease and neutrophils predominating in non-T2 and corticosteroid-resistant phenotypes
- Bronchial smooth muscle hypertrophy and hyperplasia
- Mucous gland hypertrophy with intraluminal mucus plugging
- Vascular proliferation (angiogenesis) within the airway submucosa
- Classic findings in fatal asthma include Curschmann spirals (whorled mucus casts within occluded small airways), Charcot-Leyden crystals (crystallized eosinophil granule protein galectin-10), and diffuse mucus plugging with airway hyperinflation [14]
History and Physical
Pertinent History
- Onset, pattern, and chronology of symptoms: episodic or persistent; nocturnal or early morning predominance; seasonal variation
- Characteristic symptoms: wheezing, dyspnea, chest tightness, and cough (the asthma tetrad)
- Trigger identification: allergens (dust mites, pets, mold, pollen), exercise, cold air, nonsteroidal anti-inflammatory drug or aspirin exposure, occupational exposures, viral upper respiratory tract infections, gastroesophageal reflux disease symptoms, emotional stress, and strong odors
- Occupational history: specific workplace exposures; symptom improvement on weekends or during vacation (greater than 50% improvement in peak expiratory flow variability strongly suggests an occupational cause)
- Personal and family history of atopic disease: allergic rhinitis, atopic dermatitis, food allergy, and nasal polyps, collectively known as the atopic triad
- Risk stratification: prior hospitalizations, emergency department visits, oral corticosteroid courses, or mechanical ventilation for asthma, which independently predict an increased risk of a future life-threatening exacerbation.[CDC. Most Recent Asthma Data]
- Current medications: adherence to controller therapy and inhaler technique (poor inhaler technique is a major, correctable cause of treatment failure)
- Smoking history: active and passive smoke exposure; intrauterine tobacco exposure
- Housing conditions: carpeting, indoor pets, visible mold, pest infestation, and proximity to high-traffic roadways
- Validated asthma control assessment: an Asthma Control Test score of 19 or less indicates inadequate control; an Asthma Control Questionnaire score of 1.5 or greater indicates uncontrolled asthma; the Asthma APGAR tool may also be used [1]
Physical Examination
Between exacerbations: Examination may be entirely normal. Findings that may be present include:
- Expiratory wheeze on forced expiration, which may require auscultation during forced expiration to detect
- Nasal mucosal edema, turbinate hypertrophy, or nasal polyps, which indicate comorbid allergic rhinitis or aspirin-exacerbated respiratory disease
- Signs of atopic dermatitis, including lichenification, flexural involvement, and Dennie-Morgan lines
- Digital clubbing is absent in asthma. The presence of digital clubbing warrants evaluation for bronchiectasis, interstitial lung disease, or malignant neoplasm
During acute exacerbation:
- Tachypnea and tachycardia
- Expiratory (or biphasic) wheeze on auscultation
- Accessory muscle use, including sternocleidomastoid and scalene activation and suprasternal and supraclavicular retractions
- Prolonged expiratory phase (inspiratory to expiratory ratio greater than 1:3)
- Pulsus paradoxus greater than 10 mm Hg, which indicates significant airway obstruction with dynamic hyperinflation
- Cyanosis, altered mental status, and bradycardia, which indicate impending respiratory failure
- Critical physical finding: A silent chest, defined as the absence of audible wheeze in a patient with severe dyspnea, signifies near-complete airflow obstruction and impending respiratory arrest. Clinicians frequently underrecognize this finding. A silent chest requires immediate treatment as a life-threatening condition and prompt escalation of care.
Evaluation
Pulmonary Function Testing
- Spirometry: An obstructive pattern (ratio of FEV1 to forced vital capacity [FVC] less than 0.70) with significant bronchodilator reversibility (increase of 12% or greater and 200 mL or greater after administration of a short-acting β2-agonist) is the gold standard for confirming variable airflow obstruction. Normal spirometry findings do not exclude asthma if obtained between symptomatic episodes.[3][EPA. Expert Report 3. Guidelines for the Diagnosis and Management of Asthma][15]
- Peak expiratory flow: Serial home monitoring with greater than 20% diurnal variability over 2 weeks supports variable airflow obstruction. Asthma action plans based on peak expiratory flow are recommended by guidelines for all patients.
- Bronchial provocation testing: A methacholine challenge (a provocative concentration causing a 20% decrease in FEV1 of less than 8 mg/mL indicates positive results; a level less than 4 mg/mL indicates moderate to marked bronchial hyperresponsiveness) is the most sensitive test and is particularly useful when baseline spirometry findings are normal. An exercise challenge may be used to evaluate exercise-induced bronchoconstriction.[EPA. Expert Report 3. Guidelines for the Diagnosis and Management of Asthma]
Inflammatory Biomarkers: Core to Phenotype-Guided Management
- Fractional exhaled nitric oxide (FeNO): Levels of 25 parts per billion or greater in adults and 35 parts per billion or greater in children support T2-high eosinophilic airway inflammation and predict inhaled corticosteroid responsiveness and response to dupilumab. The 2024 Global Initiative for Asthma guidelines recommend FeNO measurement as an adjunct to spirometry at diagnosis and for treatment monitoring.[10][11][16]
- Blood eosinophil count: Levels of 150 cells/µL or greater at treatment initiation or 300 cells/µL or greater in the prior 12 months support T2 eosinophilic disease. The blood eosinophil count is a primary eligibility criterion for anti–IL-5 and anti–IL-5 receptor α biologic agents and is measured on a routine complete blood count with differential.[3][17]
- Total serum IgE: Elevated levels occur in allergic asthma and are essential for omalizumab dose calculation (aweight-based, IgE-stratified dosing table). IgE levels greater than 700 IU/mL exceed the omalizumab dosing range.[18]
- Specific serum IgE and ImmunoCAP: Quantify allergen-specific sensitization to house dust mites, animal dander, pollen, and molds; preferred when skin prick testing is not feasible.
- Serum periostin: an IL-13–inducible epithelial protein and emerging T2 biomarker that is not yet in routine clinical use but has been evaluated as a complement to FeNO and eosinophil count in research settings.
Allergy Testing
The National Asthma Education and Prevention Program recommends allergen testing for all patients requiring daily controller therapy to enable targeted avoidance counseling and selection of appropriate allergen immunotherapy.[EPA. Expert Report 3. Guidelines for the Diagnosis and Management of Asthma]
- Skin prick testing: the preferred primary method because it is immediate, cost-effective, and highly sensitive for IgE-mediated inhalant allergen sensitization. Antihistamines must be withheld for 5 to 7 days before testing [19]
- ImmunoCAP and fluorescent enzyme immunoassay: preferred when skin prick testing is not feasible (eg, extensive dermatographism, severe eczema, or an inability to stop antihistamines)
- Component-resolved diagnostics: Identify sensitization to specific allergenic components rather than cross-reactive carbohydrate determinants and predict allergen immunotherapy response and systemic reaction risk more accurately than extract-level testing.
Occupational Asthma Evaluation
- Serial peak expiratory flow monitoring at and away from work (minimum of 4 readings per day for at least 3 weeks with at least 1 work period and 1 vacation period) is the most practical initial test. An improvement in variability of greater than 20% away from work is highly suggestive.[6]
- Spirometry before and after a work shift and methacholine challenge at the end of the workweek compared with results obtained after at least 2 weeks away from work (a greater than 3-fold improvement in the provocative concentration causing a 20% decrease in FEV1 suggests an occupational cause).
- Specific IgE and skin prick test for relevant occupational sensitizers.
- Specific inhalation challenge in a controlled laboratory setting is the gold standard for confirming sensitizer-induced occupational asthma. This test is performed only at specialized centers.
- Additional studies
- Chest radiography: Findings are typically normal between exacerbations. Chest radiography is useful for excluding pneumonia, pneumothorax, cardiomegaly, or a central airway mass.
- High-resolution chest CT: This test is indicated when bronchiectasis, hypersensitivity pneumonitis, allergic bronchopulmonary aspergillosis, or airway malacia is suspected. Findings may include mucus plugging, mosaic attenuation, or airway wall thickening in severe asthma.
- Complete blood count with differential: Eosinophilia supports a diagnosis of atopic disease. Elevated neutrophil levels during an exacerbation may suggest a bacterial trigger or non–T2 phenotype.
Treatment / Management
Stepwise Pharmacologic Management
The 2024 Global Initiative for Asthma (GINA) guidelines represent a paradigm shift from prior frameworks, introducing the most important guideline update in 2 decades: the removal of as-needed short-acting β2-agonist (SABA) monotherapy as first-line reliever therapy at any step of asthma treatment.[1][15][20][21] The foundational evidence for this change comes from the Symbicort Given as Needed in Mild Asthma 1 (SYGMA-1) and Symbicort Given as Needed in Mild Asthma 2 (SYGMA-2) trials. Results from these trials demonstrated that as-needed low-dose budesonide-formoterol was noninferior to daily inhaled corticosteroid maintenance therapy plus a SABA reliever for the prevention of severe exacerbations and superior to SABA monotherapy alone, with significantly lower total inhaled corticosteroid exposure.[20][21](B3)
Key GINA 2024 Concepts
GINA 2024 anti-inflammatory reliever approach: As-needed inhaled corticosteroid-formoterol (budesonide-formoterol) is the preferred reliever at steps 1 to 5. Every use of inhaled corticosteroid-formoterol as a reliever simultaneously delivers an anti-inflammatory inhaled corticosteroid dose, reducing the risk of exacerbation. The anti-inflammatory reliever approach replaces the outdated model of a daily inhaled corticosteroid controller plus an SABA reliever for mild-to-moderate asthma (see Image. Asthma Severity Classification by The National Asthma Education and Prevention Program). Table 1 lists the criteria for asthma severity, and Table 2 describes the treatment for each step.
- Track 1 (preferred): an inhaled corticosteroid (ICS)-containing reliever at all steps, which is the preferred approach for most patients
- Track 2 (alternative): SABA reliever, which is acceptable only when Track 1 is unavailable or refused and should not be the default
- Step-up decisions: based on inadequate symptom control (Asthma Control Test score of 19 or less), frequency of reliever use, nighttime awakenings, activity limitation, peak expiratory flow variability, and exacerbation history
- Step-down decisions: consider after 3 months or more of well-controlled asthma; reduce the inhaled corticosteroid dose by 25% to 50%; never abruptly discontinue controller therapy
- Before stepping up: reassess adherence, inhaler technique, trigger avoidance, and comorbidities, which are correctable causes of apparent treatment failure [1]
Table 1. Asthma Severity Classification
|
Component |
Intermittent |
Mild persistent |
Moderate persistent |
Severe persistent |
|
Daytime symptoms |
≤ 2 days/week |
> 2 days/week but not daily |
Daily |
Throughout the day |
|
Nighttime awakenings |
≤ 2×/month |
3–4 times/month |
> 1×/week, not nightly |
Nightly |
|
SABA use (rescue) |
≤ 2 days/week |
> 2 days/week |
Daily |
Several times daily |
|
Activity limitation |
None |
Minor |
Some |
Extremely limited |
|
FEV1 (% predicted) |
> 80% |
> 80% |
60%-80% |
< 60% |
|
FEV1/FVC |
Normal |
Normal |
Reduced 5% |
Reduced > 5% |
|
Exacerbations requiring OCS |
0–1/year |
≥ 2/year |
≥ 2/year |
≥ 2/year; some life-threatening |
Abbreviations: FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; OCS: oral corticosteroids; SABA: short-acting β2-agonist.
Severity classification applies to patients who are not receiving controller therapy. Once therapy is initiated, use the level of control (well-controlled/not well-controlled/very poorly controlled) to guide management.
Table 2. Global Initiative for Asthma 2024 Stepwise Asthma Management Framework
|
Step |
Severity |
Preferred controller |
Preferred reliever |
Consider adding |
|
1 |
Intermittent |
None required |
As-needed, low-dose ICS-formoterol* OR SABA (less preferred) |
Allergen avoidance; environmental control |
|
2 |
Mild persistent |
Low-dose ICS daily |
As-needed, low-dose ICS-formoterol* OR SABA |
LTRA (alternative); allergy testing + AIT consideration |
|
3 |
Moderate persistent |
Low-dose ICS + LABA (preferred) OR medium-dose ICS |
As-needed, low-dose ICS-formoterol* |
LTRA add-on; SCIT/SLIT if sensitized; refer to specialist |
|
4 |
Moderate–severe |
Medium-dose ICS + LABA |
As-needed ICS-formoterol* |
Tiotropium add-on; specialist evaluation for biologic; SCIT/SLIT |
|
5 |
Severe |
High-dose ICS + LABA + phenotype-guided biologic (see Table 3) |
As-needed ICS-formoterol* or SABA |
Omalizumab / Dupilumab / Mepolizumab / Benralizumab / Tezepelumab based on biomarker profile |
|
6 |
Refractory / very severe |
High-dose ICS + LABA + Biologic + Low-dose OCS (if unavoidable) |
As-needed ICS-formoterol* or SABA |
Bronchial thermoplasty (selected centers); phenotype reassessment; specialist co-management mandatory |
*As-needed low-dose ICS-formoterol (budesonide-formoterol) is the preferred reliever at all steps (Track 1).
Step-up requires reassessment of adherence and inhaler technique before intensifying pharmacotherapy.
Abbreviations: ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LTRA, leukotriene receptor antagonist; OCS, oral corticosteroid; AIT, allergen immunotherapy; SCIT, subcutaneous immunotherapy; SLIT, sublingual immunotherapy.
References for the table:[1][22]
Inhaled Corticosteroids
Inhaled corticosteroids remain the most effective controller therapy for all levels of persistent asthma, reducing airway inflammation, bronchial hyperresponsiveness, and exacerbation frequency. Commonly used agents include fluticasone propionate, budesonide, beclomethasone dipropionate, mometasone furoate, and ciclesonide. Patients should receive counseling on spacer use (mandatory for children and strongly recommended for adults) and mouth rinsing after use to minimize oral candidiasis and dysphonia.[1][EPA. Expert Report 3. Guidelines for the Diagnosis and Management of Asthma][20]
Long-Acting β2-Agonists
Long-acting β2-agonists (LABAs), including formoterol, salmeterol, and vilanterol, must never be used as monotherapy in asthma (US Food and Drug Administration [FDA] boxed warning: increased risk of asthma-related death with LABA monotherapy). Inhaled corticosteroid-formoterol is uniquely preferred as both a controller and a reliever because of formoterol's rapid onset (similar to salbutamol), which enables the maintenance-and-reliever therapy approach validated across the SYGMA trials.[20][23]
Leukotriene Receptor Antagonists and Other Controllers
Montelukast and zafirlukast are useful as alternative controllers at step 2 and adjuncts at steps 2 to 4, particularly in patients with comorbid allergic rhinitis or aspirin-exacerbated respiratory disease. The FDA requires a boxed warning for montelukast regarding serious neuropsychiatric adverse effects, including agitation, depression, suicidal ideation, and sleep disturbances. Clinicians should counsel patients explicitly about these risks. Tiotropium (a long-acting muscarinic antagonist) is an approved add-on bronchodilator for adults at steps 4 and 5.[1][EPA. Expert Report 3. Guidelines for the Diagnosis and Management of Asthma]
Allergen Immunotherapy
Allergen immunotherapy (AIT) is the only disease-modifying treatment for allergic asthma, addressing underlying IgE-mediated sensitization rather than merely suppressing symptoms. Allergen immunotherapy is indicated for patients with confirmed allergen sensitization who remain symptomatic despite pharmacotherapy.[19][24](A1)
- Subcutaneous immunotherapy: the traditional gold standard; escalating allergen extract injections with a mandatory 30-min postinjection observation period in the allergist's office; results from studies demonstrated reductions in asthma symptoms, medication requirements, and exacerbations; may prevent new sensitizations and progression of the atopic march
- Sublingual immunotherapy: FDA-approved tablets are available for house dust mite (Odactra [ALK-Abelló A/S]), ragweed pollen (Ragwitek [ALK-Abelló A/S]), timothy grass (Grastek [ALK-Abelló A/S]), and mixed grasses (Oralair [Stallergenes SA]); administered daily at home; better tolerated than subcutaneous immunotherapy, with a lower systemic reaction risk; effective for allergic rhinitis and asthma with house dust mite or grass sensitization.[19]
- AIT contraindication: AIT is contraindicated when FEV1 is less than 70% of predicted postbronchodilator due to elevated risk of systemic and anaphylactic reactions. Clinicians should achieve adequate asthma control before initiating AIT. (A1)
Bronchial Thermoplasty
Bronchial thermoplasty is an FDA-approved bronchoscopic procedure for adults aged 18 years and older with severe refractory asthma that is not controlled on high-dose ICS-LABA and biologic therapy. The procedure delivers targeted radiofrequency energy to reduce bronchial smooth muscle mass. Results from multiple randomized trials demonstrated reductions in severe exacerbations and emergency department visits. Clinicians perform the procedure during 3 bronchoscopic sessions (right lower lobe, left lower lobe, and bilateral upper lobes) at centers with expertise in severe asthma treatment.[25](A1)
Biologic (Targeted) Therapy for Severe Asthma
The introduction of biologic agents targeting specific components of the T2 inflammatory cascade has fundamentally transformed the treatment of moderate-to-severe asthma. All currently approved biologic agents are indicated as add-on therapy for patients who remain inadequately controlled with medium- to high-dose inhaled corticosteroid and LABA therapy. Appropriate biologic selection depends critically on the patient's inflammatory phenotype, biomarker profile (blood eosinophil count, total IgE, allergen sensitization status, and FeNO), comorbidities, dosing interval preference, and insurance and access considerations.[3][17]
Overview and Mechanism of Approved Agents
Table 3. Approved Biologic Agents for Severe Asthma
|
Agent (brand) |
Target |
Age approval |
Biomarker criteria |
Indication |
Dosing |
Key trial |
|
Omalizumab (Xolair) |
Anti-IgE (IgE receptor) |
Older than 6 years |
Total IgE 30–700 IU/mL and perennial allergen sensitization (SPT or specific IgE) |
Moderate–severe allergic asthma inadequately controlled on ICS |
75–375 mg SQ every 2–4 weeks (weight + IgE-based dosing chart) |
|
|
Dupilumab (Dupixent) |
Anti-IL–4Rα (blocks IL-4 + IL-13) |
Older than 6 years |
Eos ≥ 150 cells/μL OR FeNO ≥ 25 ppb; also OCS-dependent asthma regardless of eosinophil count |
Moderate–severe uncontrolled asthma on medium/high-dose ICS-LABA; also OCS-dependent |
Adults:200 mg SQ every 2 weeks (400 mg loading); Peds 6–11 yrs: weight-based every 2–4 weeks |
|
|
Mepolizumab (Nucala) |
Anti–IL-5 |
Older than 6 years |
Blood Eos ≥ 150/μL at initiation OR ≥ 300/μL in prior 12 months |
Severe eosinophilic asthma; add-on to high-dose ICS + additional controller |
100 mg SQ every 4 weeks (adults and peds ≥ 12); Peds 6–11 yrs: 40 mg SQ every 4 weeks |
|
|
Benralizumab (Fasenra) |
Anti–IL-5Rα (depletes eosinophils via ADCC) |
Older than 12 years |
Blood eos ≥ 300/μL |
Severe eosinophilic asthma; add-on to high-dose ICS-LABA |
30 mg SQ every 4 weeks × 3 doses, then every 8 weeks (every 8-week maintenance unique advantage) |
|
|
Tezepelumab (Tezspire) |
Anti-TSLP (upstream alarmin) |
Older than 12 years |
No eosinophil threshold required, effective across T2-high and non-T2 phenotypes |
Severe uncontrolled asthma; broadest approved indication; works regardless of allergic status |
210 mg SQ every 4 weeks (fixed dosing, no weight or lab adjustment) |
NAVIGATOR SOURCE CASCADE |
|
Itepekimab (Dupixent partner, investigational) |
Anti–IL-33 |
Older than 18 years (investigational) |
Eos ≥ 300/μL; nonsmokers showed greatest benefit |
Phase 3 trials ongoing for moderate–severe uncontrolled asthma |
Phase 3 dosing under investigation |
PATHWAY phase 2b [36] |
Abbreviations: ADCC, antibody-dependent cellular cytotoxicity; CRSwNP, chronic rhinosinusitis with nasal polyps; Eos, blood eosinophils; FeNO, fractional exhaled nitric oxide; IgE, immunoglobulin E; IL, interleukin; OCS, oral corticosteroid; SQ, subcutaneous; T2, type 2; TSLP, thymic stromal lymphopoietin.
*All biologics require specialist initiation and ongoing monitoring.
References for the table:[37][38](A1)
Table 4 provides clinical guidance for biomarker-driven therapy; individual patient factors and access considerations may appropriately influence final selection.
Table 4. Biomarker-Guided Biologic Selection Algorithm
|
Clinical profile |
Blood eos |
Total IgE + allergen SPT/sIgE |
FeNO |
Preferred biologic(s) |
Notes |
|
Classic allergic asthma: perennial sensitization, atopic triad, elevated IgE |
Any level |
IgE 30–700 + sensitized |
Often elevated |
Omalizumab (first-line for allergic) |
SCIT/SLIT should be considered concurrently |
|
T2-high, allergic + eosinophilic: eos ≥ 150, FeNO ≥ 25, atopic |
≥ 150–300/μL |
IgE may or may not meet threshold |
≥ 25 ppb |
Dupilumab (broadest T2 coverage); omalizumab if IgE criteria met |
Dupilumab preferred if eos + FeNO both elevated |
|
Severe eosinophilic, nonallergic: eos ≥ 300/μL, low IgE, not sensitized |
≥ 300/μL |
Not required/low IgE |
Variable |
Benralizumab (preferred: every 8 week dosing), mepolizumab |
Every 9-week benralizumab regimen gives adherence advantage |
|
Moderate eosinophilic, OCS-dependent: eos ≥ 150/μL, systemic steroid-requiring |
≥ 150/μL |
Any |
Any |
Mepolizumab, benralizumab, dupilumab (all OCS-sparing data) |
Dupilumab unique: works even at low eos if OCS-dependent |
|
Non-T2/mixed phenotype: low eos (< 150/μL), low FeNO (< 20), nonallergic, obese/smoker |
< 150/μL |
Low/negative |
< 20 ppb |
Tezepelumab (only biologic with proven efficacy across all phenotypes) |
Other biologics show minimal benefit in true non-T2 phenotype |
|
Severe asthma with nasal polyps + AERD: aspirin sensitivity, chronic sinusitis |
Often ≥ 150/μL |
May be elevated |
Often > 25 ppb |
Dupilumab (approved for CRSwNP + asthma); benralizumab alternative |
Dupilumab approved for both asthma and CRS with nasal polyps (dual benefit) |
Abbreviations: AERD, aspirin-exacerbated respiratory disease; CRSwNP, chronic rhinosinusitis with nasal polyps; Eos, blood eosinophils; FeNO, fractional exhaled nitric oxide; IgE, immunoglobulin E; OCS, oral corticosteroid; SCIT, subcutaneous immunotherapy; sIgE, specific IgE; SLIT, sublingual immunotherapy; SPT, skin prick testing; T2, type 2.
References for the table:[16][37][38](A1)
Individual Biologic Agent Profiles
Omalizumab (Xolair), an anti-IgE Monoclonal Antibody, was the first biologic agent approved for asthma (2003), targeting free IgE and preventing its binding to FcεRI on mast cells and basophils, thereby blocking IgE-mediated degranulation. Omalizumab is indicated for moderate-to-severe allergic asthma (in patients aged 6 years or older) with confirmed perennial allergen sensitization and a total IgE level of 30 to 700 IU/mL. Dosing is individualized using a weight- and IgE-stratified dosing table, with administration via subcutaneous injection every 2 to 4 weeks. Anaphylaxis has been reported in 0.1% to 0.2% of patients; a 30-min postinjection observation period is required for the first 3 injections (according to the FDA label). Beyond asthma, omalizumab is approved for chronic spontaneous urticaria and food allergy (approved in 2024).[9][18][26](A1)
Omalizumab pearl: Patients who respond to omalizumab typically experience improvements in exacerbation rates within 16 weeks. The GINA guidelines recommend a formal response assessment at 4 months. When no meaningful response occurs, clinicians should consider switching to another biologic agent rather than continuing treatment with an ineffective agent.
Dupilumab (Dupixent), an anti–IL-4Rα Monoclonal Antibody, blocks the shared IL-4 receptor α subunit, simultaneously inhibiting signaling through both IL-4 and IL-13, the 2 principal type 2 helper T-cell cytokines. Dupilumab is indicated for moderate to severe uncontrolled asthma (in patients aged 6 years or older) and is the only biologic agent approved for asthma without an eosinophil threshold. The agent is also approved for oral corticosteroid-dependent asthma, atopic dermatitis, chronic rhinosinusitis with nasal polyps, eosinophilic esophagitis, and prurigo nodularis, making dupilumab particularly valuable for patients with multiple atopic comorbidities (the type 2 inflammatory spectrum).[27][28]
Results from the Evaluate the Efficacy and Safety of Dupilumab in Patients With Persistent Asthma (LIBERTY ASTHMA QUEST) trial (n = 1902) demonstrated up to a 70% reduction in exacerbations among patients with an eosinophil count of 300 cells/µL or greater and a fractional exhaled nitric oxide level of 25 parts per billion or greater. Results from the Evaluation of Dupilumab in Patients With Severe Steroid-Dependent Asthma (LIBERTY ASTHMA VENTURE) trial (n = 210) demonstrated a 70% reduction in the oral corticosteroid dose, with 48% of patients achieving complete oral corticosteroid elimination, establishing dupilumab as the benchmark for oral corticosteroid-sparing therapy in oral corticosteroid-dependent asthma.[27][28]
Dupilumab pearl: Dupilumab can cause a transient increase in the blood eosinophil count shortly after initiation (an eosinophil spike) because of redistribution from tissues to the circulation. The increase does not indicate treatment failure; the eosinophil count typically returns toward baseline within 4 to 8 weeks, and biologic discontinuation is not required unless the increase is accompanied by eosinophilic end-organ manifestations.
Mepolizumab (Nucala), anti–IL-5: Mepolizumab binds free IL-5, blocking its interaction with the IL-5 receptor on eosinophil precursors, circulating eosinophils, and basophils. The agent reduces eosinophil production in the bone marrow, the peripheral blood eosinophil count, and tissue eosinophilia. Mepolizumab is indicated for severe eosinophilic asthma (in patients aged 6 years or older) with a blood eosinophil count of 150 cells/µL or greater at treatment initiation or 300 cells/µL or greater in the prior 12 months. The pediatric dose for children aged 6 to 11 years is 40 mg subcutaneously every 4 weeks; adults and adolescents receive 100 mg subcutaneously every 4 weeks.[38][29][30](A1)
Results from the Mepolizumab as Adjunctive Therapy in Patients with Severe Asthma (MENSA) trial demonstrated a 47% reduction in exacerbation rate and a 98 mL increase in FEV1. Results from the Steroid Reduction With Mepolizumab Study (SIRIUS) trial demonstrated a 50% median reduction in oral corticosteroid dose in patients with oral corticosteroid-dependent severe eosinophilic asthma, with 14% of patients achieving complete elimination of oral corticosteroids. Results from long-term extension studies, including COSMOS and COLUMBA, demonstrated sustained efficacy and acceptable safety over more than 3 years of continuous therapy.[29][30]
Benralizumab (Fasenra): anti–IL-5Rα: Benralizumab binds the IL-5 receptor α subunit (IL-5Rα) with high affinity, triggering antibody-dependent cellular cytotoxicity of eosinophils and basophils via natural killer cells. The resulting mechanism produces near-complete blood eosinophil depletion within 24 h of the first dose, representing the most rapid and complete eosinophil depletion of any approved antieosinophil biologic agent. Benralizumab is indicated for severe eosinophilic asthma (in patients aged 12 years or older) with a blood eosinophil count of 300 cells/μL. Maintenance dosing every 8 weeks after 3 initial monthly doses is a practical advantage for patient adherence.[31][32][38][32](A1)
Results from the SIROCCO and CALIMA trials collectively demonstrated reductions in exacerbation rates of 36% to 51%. Results from the GREGALE trial demonstrated a 75% reduction in oral corticosteroid dose, with 52% of patients achieving complete elimination. Notably, benralizumab's antibody-dependent cellular cytotoxicity mechanism simultaneously depletes mucosal eosinophils that may not be reflected in blood counts, potentially offering superior tissue-level eosinophil clearance.[31][32](A1)
Benralizumab pearl: The maintenance dosing interval of every 8 weeks after 3 loading doses translates to only 6 injections per year, compared with 12 to 26 injections for other biologic agents. The reduced injection burden may significantly improve adherence and reduce clinic visit burden for patients with severe asthma.
Tezepelumab (Tezspire): anti–Thymic Stromal Lymphopoietin (TSLP), upstream alarmin blockade: Tezepelumab is the first biologic agent to target the epithelial-derived alarmin thymic stromal lymphopoietin, which sits upstream of the T2 and non-T2 bifurcation in the inflammatory cascade. By blocking thymic stromal lymphopoietin, tezepelumab simultaneously suppresses T2 inflammation (including eosinophilic, allergic, and IL-33-mediated inflammation) and non-T2 pathways, giving the agent the broadest clinical phenotype coverage of any approved biologic agent. Tezepelumab is indicated for severe uncontrolled asthma (in patients aged 12 years or older) with no eosinophil threshold, allergen sensitization requirement, or IgE criterion required.[12][13][34][39](A1)
Results from the landmark Study to Evaluate Tezepelumab in Adults and Adolescents With Severe Uncontrolled Asthma (NAVIGATOR) trial (n = 1061) demonstrated a 70% reduction in the annualized exacerbation rate in the overall population, with comparable efficacy across all biomarker subgroups: T2-high (79%), T2-low (68%), allergic (70%), nonallergic (71%), and high or low FeNO levels. Tezepelumab is the only biologic agent to demonstrate substantial efficacy across all asthma phenotypes in a single pivotal trial, making it the preferred choice when the phenotype is uncertain, mixed, or non-T2.[12][13][35] Results from the Study to Evaluate Tezepelumab on Airway Inflammation in Adults With Uncontrolled Asthma (CASCADE) trial provided bronchoscopic biopsy evidence of tezepelumab's anti-inflammatory mechanism, demonstrating significant reductions in submucosal eosinophils, mast cells, and goblet cell density compared with placebo.[33](A1)
Tezepelumab pearl: Tezepelumab is the only currently approved biologic agent for severe asthma that has demonstrated meaningful exacerbation reduction in the non-T2 (low eosinophil count, low FeNO level, and nonallergic) phenotype, a population previously without biologic options. Clinicians should consider tezepelumab when other biologic agents have not produced an adequate response or the phenotype remains unclear after a full biomarker evaluation.
Itepekimab (anti–IL-33), investigational:
Itepekimab (REGN3500) is a fully human monoclonal antibody targeting IL-33, another upstream alarmin. Results from phase 2 of the Study to Evaluate the Efficacy and Safety of MEDI9929 (AMG 157) in Adult Subjects With Inadequately Controlled, Severe Asthma (PATHWAY) trial demonstrated a significant reduction in exacerbations in nonsmoking patients with moderate-to-severe asthma (the subgroup with an eosinophil count of 300 cells/μL or greater experienced the greatest benefit). Notably, former smokers, who are typically excluded from other biologic trials, demonstrated a meaningful response, suggesting that IL-33 blockade may be particularly relevant in smoking-associated asthma. Phase 3 SWIFT-1 and SWIFT-2 trials are currently ongoing.[36]
Monitoring and Response Assessment
All biologic agents should undergo formal response assessment 4 to 6 months after initiation. A meaningful response is defined as a 50% or greater reduction in the annualized exacerbation rate, a 50% or greater reduction in the oral corticosteroid dose, clinically meaningful improvement in the Asthma Control Test score (3 points or greater), FEV1, or quality-of-life scores, or a reduction in healthcare utilization.[1][17]
- Patients who show no response after 6 months of treatment with a biologic agent should receive an agent targeting a different pathway rather than continue with an ineffective agent.
- Clinicians should measure the blood eosinophil count before initiation (at baseline) and periodically during therapy; dupilumab may transiently elevate the eosinophil count, an expected class effect.
- The FeNO trajectory can be used to monitor the treatment response to dupilumab; a declining FeNO level indicates progressive suppression of the IL-4 and IL-13 pathways.
- OCS dose tapering should begin after 3 to 6 months of biologic therapy in OCS-dependent patients, guided by symptom control and exacerbation frequency
Switching biologic agents: Clinicians can transition therapy without a washout period. The new biologic agent should be administered when the next dose of the discontinued biologic agent would have been due. The eosinophil count typically increases again within 4 to 8 weeks after stopping anti-IL-5 therapy, an important consideration when transitioning to an agent that does not target IL-5.
Treatment of Acute Exacerbations
Severity assessment:
Rapid and systematic severity assessment guides triage and initial treatment. Severity correlates with peak expiratory flow, oxygen saturation, ability to speak, accessory muscle use, and mental status:
- Mild: peak expiratory flow of 70% or greater, oxygen saturation of 95% or greater, ability to speak in sentences, and no accessory muscle use; suitable for home treatment with step-up therapy
- Moderate: peak expiratory flow of 40% to 69%, oxygen saturation of 90% to 94%, ability to speak in phrases, and mild to moderate accessory muscle use; emergency care required
- Severe: peak expiratory flow of less than 40%, oxygen saturation of less than 90%, ability to speak only in words, significant accessory muscle use, and paradoxical breathing; immediate aggressive treatment required
- Life-threatening: silent chest, cyanosis, oxygen saturation of less than 90% despite high-flow oxygen, bradycardia, confusion, or obtundation; immediate intensive care unit transfer and airway treatment planning required
Patients with a peak expiratory flow value of less than 50% of their personal best or predicted value require immediate medical care. Prior near-fatal asthma, recent OCS use, and overreliance on SABA are the most important risk factors for fatal exacerbation.[1][CDC. Most Recent Asthma Data]
Supplemental Oxygen
Clinicians should titrate supplemental oxygen to maintain an oxygen saturation of 94% to 98% (95% to 98% in pregnant patients and patients with coexisting cardiac disease). High-flow oxygen should be used with caution in patients with concurrent chronic obstructive pulmonary disease. Continuous pulse oximetry monitoring is standard throughout the emergency department visit.[1]
Short-Acting Bronchodilators
Albuterol (2.5 mg via nebulizer or 4 to 8 puffs via metered-dose inhaler with a spacer) is administered immediately and repeated every 20 min for the first h, then reassessed. Continuous nebulization may be considered in severe exacerbations. Ipratropium bromide (0.5 mg for adults and 0.25 mg for children) combined with a SABA has been evaluated in multiple randomized controlled trials and systematic reviews. Results from these trials and reviews demonstrated significantly greater bronchodilation with combination therapy than with a SABA alone, and a substantial reduction in hospitalization rates for moderate-to-severe exacerbations. Clinicians should add ipratropium bromide to every SABA nebulization for the first 1 to 3 hours.[40][41](A1)
Systemic Corticosteroids
Systemic corticosteroids should be administered within 1 hour of presentation to the emergency department for moderate-to-severe exacerbations. Early administration significantly reduces hospitalization rates, decreases relapse rates, and accelerates lung function recovery. Oral prednisone (40 to 60 mg/d for adults; 1 to 2 mg/kg/d, up to 40 mg, for children) is bioequivalent to intravenous methylprednisolone in patients who can swallow and is preferred for its practicality and cost. A 5- to 7-day course without a taper is sufficient. Patients should be discharged with a complete course of oral corticosteroids and step-up controller therapy.[1][EPA. Expert Report 3. Guidelines for the Diagnosis and Management of Asthma]
Intravenous Magnesium Sulfate
Intravenous magnesium sulfate (2 g over 20 min for adults; 25 to 75 mg/kg over 20 to 30 min for children) is recommended for severe exacerbations that do not respond adequately to initial SABA and corticosteroid therapy. Results from multiple randomized controlled trials and meta-analyses demonstrated improvements in FEV1 and reductions in hospital admission rates, with the greatest benefit in children with life-threatening exacerbations. The proposed mechanism is smooth muscle relaxation via calcium-mediated inhibition of bronchomotor tone.[42][43](A1)
Escalation Therapies
- Heliox (70:30 or 80:20 helium-oxygen mixture): may reduce airway resistance and improve nebulized bronchodilator delivery in severe refractory bronchospasm; results from studies are mixed; heliox has an adjunctive role only [44]
- Noninvasive positive pressure ventilation: may support selected patients with impending respiratory failure and avoid intubation; results from studies in acute asthma are limited; noninvasive positive pressure ventilation requires close monitoring
- Intubation and mechanical ventilation: reserved for frank respiratory failure, apnea, or hemodynamic instability; carries significant risks, including dynamic hyperinflation, breath stacking, pneumothorax, and hemodynamic compromise; clinicians should use a permissive hypercapnia strategy, low respiratory rate, and prolonged expiratory time (A1)
Disposition and Transition of Care
- Discharge criteria: peak expiratory flow of 70% or greater of the patient's personal best, oxygen saturation of 94% or greater on room air, symptom resolution, and the ability to use the reliever inhaler correctly
- Admission criteria: peak expiratory flow of 40% to 69% or less after aggressive initial therapy, oxygen saturation of less than 94%, high-risk features (prior intensive care unit admission or recent oral corticosteroid course), or limited social support
- Intensive care unit admission criteria: peak expiratory flow of less than 25%, silent chest, altered mental status, or failure to improve despite maximal therapy
All discharged patients must receive a written Asthma Action Plan, instructions for completing the oral corticosteroid course, a SABA prescription or refill, initiation or step-up of inhaled corticosteroid controller therapy, and a scheduled follow-up within 1 to 4 weeks. Clinicians should refer any patient with 2 or more exacerbations requiring systemic corticosteroids in the prior year to pulmonology or allergy and immunology for evaluation of candidacy for biologic therapy.[1][EPA. Expert Report 3. Guidelines for the Diagnosis and Management of Asthma]
Differential Diagnosis
Differential Diagnosis
Establishing a firm diagnosis of asthma prior to initiating long-term therapy is essential, because multiple conditions can mimic the episodic dyspnea, wheezing, and cough associated with asthma. Table 5 lists the differential diagnosis of asthma.[2][EPA. Expert Report 3. Guidelines for the Diagnosis and Management of Asthma]
Table 5. Differential Diagnosis of Asthma
|
Category |
Adults |
Pediatric |
|
Obstructive lung disease |
COPD, bronchiectasis, tracheobronchomalacia |
Cystic fibrosis, bronchopulmonary dysplasia, primary ciliary dyskinesia |
|
Upper airway |
Inducible laryngeal obstruction (ILO/EILO), preferred over VCD; nasal polyps with postnasal drip |
Laryngotracheomalacia, subglottic stenosis, vascular rings, laryngeal webs |
|
Cardiac |
Congestive heart failure (cardiac asthma): bilateral rales, orthopnea, BNP elevated |
Congenital heart disease with pulmonary overcirculation |
|
Airway obstruction |
Endobronchial tumor, extrinsic compression, sarcoidosis, amyloid |
Foreign body aspiration: sudden onset, unilateral wheeze, no atopy |
|
Inflammatory/allergic |
ABPA (very high IgE, central bronchiectasis, Aspergillus sIgE/IgG), eosinophilic pneumonia, hypersensitivity pneumonitis |
Viral bronchiolitis (RSV, rhinovirus); recurrent aspiration pneumonitis |
|
Gastrointestinal/other |
GERD (micro-aspiration), ACE inhibitor cough, anxiety/panic with dysfunctional breathing, OSA |
GERD, psychogenic/habit cough, selective IgA deficiency |
Abbreviations: ABPA, allergic bronchopulmonary aspergillosis; ACE, angiotensin-converting enzyme; BNP, B-type natriuretic peptide; COPD, chronic obstructive pulmonary disease; EILO, exercise-induced laryngeal obstruction; GERD, gastroesophageal reflux disease; IgA, immunoglobulin A; IgE, immunoglobulin E; IgG, immunoglobulin G; ILO, inducible laryngeal obstruction; OSA, obstructive sleep apnea; RSV, respiratory syncytial virus; sIgE, specific IgE; VCD, vocal cord dysfunction.
Distinguishing Inducible Laryngeal Obstruction from Asthma
Inducible laryngeal obstruction or exercise-induced laryngeal obstruction, previously called vocal cord dysfunction, classically produces inspiratory stridor and throat tightness rather than expiratory wheeze. Symptoms peak immediately at the onset of exercise rather than 5 to 15 min afterward. Spirometry findings demonstrate characteristic inspiratory flow-loop flattening, and symptoms do not respond to bronchodilators. Laryngoscopy during an episode is diagnostic. Inducible laryngeal obstruction and asthma frequently coexist in the same patient.
Pertinent Studies and Ongoing Trials
Table 6 lists the current clinical trials in asthma care.
Table 6. Clinical Trials in Asthma
|
Trial |
Biologic agent or drug |
Number of patients and duration |
Population |
Key quantitative results |
Citation |
|
INNOVATE |
Omalizumab (Anti-IgE) |
419 patients; 28 weeks |
Severe persistent allergic asthma treated with high-dose inhaled corticosteroids with or without LABA |
47% reduction in clinically significant exacerbations compared with placebo; significant improvements in morning PEF and symptom scores; anaphylaxis rate of 0.1% to 0.2% |
|
|
LIBERTY ASTHMA QUEST |
Dupilumab (anti–IL-4Rα) |
1902 patients; 52 weeks |
Moderate–severe uncontrolled asthma on medium/high-dose ICS + LABA; all biomarker levels enrolled |
Overall: 47.7% reduction in exacerbation rate vs placebo (P < 0.001); eosinophils ≥ 300/μL: 65.8% reduction in exacerbation rate (P < 0.001); FEV1: 0.32-L improvement (200-mg arm) at week 12; both coprimary end points met |
|
|
LIBERTY ASTHMA VENTURE |
Dupilumab (anti-IL-4Rα) |
210 patients; 24 weeks |
OCS-dependent severe asthma; no Eos threshold required |
OCS dose: 70.1% reduction with dupilumab compared with a 41.9% reduction with placebo (P < .001); 80% compared with 50% achieved a 50% or greater reduction in the oral corticosteroid dose; 48% compared with 25% completely discontinued oral corticosteroids; exacerbations: 59% reduction; FEV1: 0.22-L improvement |
|
|
Long-term dupilumab extension study (ERJ Open Research, 2024) |
Dupilumab (anti–IL-4Rα) |
Extension study; 3 years |
Type 2 uncontrolled asthma; pooled long-term outcomes |
Sustained exacerbation reduction at 3 years; consistent lung function improvement (FEV1) regardless of baseline biomarkers; favorable safety profile with no new signals |
|
|
DREAM |
Mepolizumab (anti–IL-5) |
621 patients; 52 weeks |
Severe eosinophilic asthma ( ≥2 exacerbations prior year) |
Results from the trial demonstrated a 48% to 52% reduction in the exacerbation rate across all mepolizumab doses compared with placebo; blood eosinophil count confirmed as the best predictive biomarker; no improvement in FEV1 (intravenous formulation) |
|
|
MENSA |
Mepolizumab (anti–IL-5) |
576 patients; 32 weeks |
Severe eosinophilic asthma, eos ≥ 150/μL, ≥ 2 prior exacerbations |
Exacerbations: 47% reduction (100-mg subcutaneous arm) compared with placebo; FEV1 98-mL improvement (subcutaneous arm) compared with placebo; St George's Respiratory Questionnaire score: significant improvement; hospitalization-requiring exacerbations: 32% reduction |
|
|
SIRIUS |
Mepolizumab (anti–IL-5) |
135 patients; 20 weeks |
OCS-dependent severe eosinophilic asthma, eos ≥ 150/μL |
OCS dose: 50% median reduction compared with no change with placebo; 14% of patients achieved complete oral corticosteroid elimination; exacerbation rate: 32% reduction; FEV1: 100-mL improvement |
|
|
SIROCCO |
Benralizumab (anti–IL-5Rα) |
1204 patients; 48 weeks |
Severe uncontrolled asthma, eos ≥ 300/μL, on high-dose ICS+LABA |
Every-8-week regimen: 51% reduction in the exacerbation rate (eosinophil count of 300 cells/μL or greater) compared with placebo; FEV1: 159-mL improvement (every-8-week regimen); near-complete blood eosinophil depletion within 24 h (ADCC mechanism); hospitalization-requiring exacerbations: 45% reduction |
|
|
CALIMA |
Benralizumab (anti–IL-5Rα) |
1306 patients; 56 weeks |
Severe uncontrolled asthma, Eos ≥ 300/μL, on medium/high-dose ICS+LABA |
Every-8-week regimen: 36% reduction in the exacerbation rate (eosinophil count of 300 cells/μL or greater) compared with placebo; FEV1:116-mL improvement (every-8-week regimen); significant improvement in symptom scores; results confirmed the durability of the every-8-week maintenance interval |
|
|
ZONDA/GREGALE |
Benralizumab (anti–IL-5Rα) |
220 patients; 28 weeks |
OCS-dependent severe eosinophilic asthma, eos ≥ 150/μL |
Median OCS dose: 75% reduction compared with no change with placebo (P < .001); 52% compared with 19% achieved complete oral corticosteroid elimination; significant reduction in the exacerbation rate; FEV1: 150-mL improvement |
|
|
NAVIGATOR (Tezepelumab) |
Tezepelumab (anti-TSLP) |
1061 patients; 52 weeks |
Severe uncontrolled asthma; all phenotypes (no Eos/IgE threshold); patients aged 12 to 80 |
Overall: 56% reduction in the annualized exacerbation rate (rate ratio, 0.44; 95% CI, 0.37-0.53; P < .001); eosinophil count of 300 cells/μL or greater: 70% reduction; eosinophil count of less than 300 cells/μL: 41% reduction; allergic asthma: 70% reduction; nonallergic asthma: 71% reduction; FeNO level of 25 ppb or greater: 68% reduction; FeNO level of less than 25 ppb: 54% reduction; FEV1: 0.23-L improvement compared with a 0.09-L improvement with placebo (P < .001); hospitalization-requiring exacerbations: 85% reduction |
|
|
CASCADE (Tezepelumab) |
Tezepelumab (anti-TSLP) |
116 patients; 28 weeks |
Moderate to severe uncontrolled asthma; bronchoscopic biopsy mechanistic substudy |
Significant reduction in submucosal eosinophils compared with placebo across all eosinophil count and fractional exhaled nitric oxide subgroups; significant reductions in submucosal mast cells and goblet cell density; significant reduction in airway hyperresponsiveness (improved methacholine provocative concentration causing a 20% decrease in FEV1); all effects present regardless of baseline eosinophil count |
|
|
SOURCE (Tezepelumab OCS) |
Tezepelumab (anti-TSLP) |
150 pateitns; 48 weeks |
OCS-dependent severe asthma; all phenotypes |
Primary endpoint: (reduction in the oral OCS without loss of control) not met in the overall population; numerically greater OCS reduction with tezepelumab (54% achieved a 90% or greater reduction in the OCS dose compared with 46% with placebo); significant OCS reduction in the eosinophilic subgroup; exacerbations, FEV1, and patient-reported outcomes improved compared with placebo |
|
|
NAVIGATOR and DESTINATION |
Tezepelumab (anti-TSLP) |
Extension study; 104 weeks (2 years) |
Severe uncontrolled asthma; continued from NAVIGATOR into DESTINATION extension |
Clinical response at week 52: 46% with tezepelumab compared with 24% with placebo (odds ratio, 2.83; 95% CI, 2.10-3.82); on-treatment remission during weeks 52 to 104: 33.5% compared with 26.7%; sustained efficacy across all biomarker subgroups at 2 years |
|
|
PATHWAY (Itepekimab phase 2b) |
Itepekimab (anti-IL-33)(investigational) |
Approximately 300 patients; 52 weeks |
Moderate to severe uncontrolled asthma; nonsmokers showed greatest benefit |
Nonsmoking individuals: up to 44% reduction in the exacerbation rate compared with placebo; eosinophil count of 300 cells/μL or greater: greatest response; former smokers: meaningful reduction in exacerbations; phase 3 SWIFT-1 and SWIFT-2 trials ongoing |
|
|
SYGMA 1 |
Budesonide-formoterol (as-needed ICS-SABA replacement) |
Approximately 3836 patients; 52 weeks |
Mild asthma; GINA Step 1–2; randomized to as-needed budesonide-formoterol vs daily budesonide vs as-needed SABA |
As-needed budesonide-formoterol was noninferior to daily budesonide for the prevention of severe exacerbations (rate ratio, 0.97; 95% CI, 0.62-1.54); superior to SABA therapy alone (rate ratio, 0.36; P < .001); 64% lower total inhaled corticosteroid exposure compared with the daily inhaled corticosteroid arm; no difference in daily symptom scores |
|
|
SYGMA 2 |
Budesonide-formoterol (as-needed ICS-SABA replacement) |
Approximately 4215 patients; 52 weeks |
Mild asthma; as-needed budesonide-formoterol vs daily budesonide maintenance + as-needed SABA |
As-needed budesonide-formoterol was noninferior to daily budesonide plus a SABA for well-controlled weeks (treatment ratio, 0.95; 95% CI, 0.91-0.99); severe exacerbations: 8% reduction with as-needed budesonide-formoterol; OCS use: 16% reduction; 50% less inhaled corticosteroid exposure compared with the daily maintenance arm; results confirmed the findings from SYGMA 1 in a larger population |
All percentage reductions are relative risk reductions compared with placebo unless otherwise stated.
Abbreviations: ADCC, antibody-dependent cellular cytotoxicity; DESTINATION, Extension Study to Evaluate the Safety and Toleratility of Tezepelumab in Adults and Adolescentes With Severe, Uncontrolled Asthma; Eos, blood eosinophils; FeNO, fractional exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; GINA, Global Initiative for Asthma; ICS, inhaled corticosteroid; IV, intravenous; LABA, long-acting β2-agonist; OCS, oral corticosteroid; OR, odds ratio; PEF, peak expiratory flow; RR, rate ratio; SABA, short-acting β2-agonist; SQ, subcutaneous; T2, type 2; TSLP, thymic stromal lymphopoietin.
Prognosis
The prognosis of asthma is variable and depends on disease severity, inflammatory phenotype, age of onset, adherence to controller therapy, and the presence of comorbidities. Approximately 30% to 50% of children with mild to moderate asthma achieve clinical remission by adulthood, though airway hyperresponsiveness may persist subclinically.[21][51]
Results from the Childhood Asthma Management Program trial and the Epidemiology and Natural History of Asthma: Outcomes and Treatment Regimens cohort showed that early, continuous inhaled corticosteroid therapy preserves the lung function trajectory and reduces the risk of irreversible airflow limitation. Poorly controlled asthma with ongoing allergen exposure, frequent exacerbations, and tobacco use is associated with accelerated decline in FEV1 and airway remodeling.[51][52]
Risk Factors for Severe or Fatal Asthma
- Prior near-fatal asthma attack requiring intubation or intensive care unit admission, the single strongest predictor of future near-fatal events [CDC. Most Recent Asthma Data][21][51]
- Two or more hospitalizations or 3 or more emergency department visits in the prior year
- SABA overuse: ≥ 3 canisters dispensed per year is an independent predictor of asthma-related death [1]
- Nonadherence to prescribed ICS controller therapy; current active smoking
- Comorbid food allergy, particularly peanut allergy in an asthmatic patient is associated with markedly elevated risk of fatal anaphylaxis-triggered bronchospasm
- Low socioeconomic status, urban residence with high air pollution, and limited healthcare access
- Psychosocial comorbidities (depression, anxiety, and psychosis) and poor perception of dyspnea (blunted symptom perception increases risk of delayed help-seeking)
Complications
Acute Complications
- Hypoxemic respiratory failure: the most immediately life-threatening acute complication
- Pneumothorax and pneumomediastinum: resulting from elevated intrathoracic pressures during severe bronchospasm or positive-pressure ventilation
- Dynamic hyperinflation: (auto-PEEP, breath stacking), major concern during mechanical ventilation; can cause hemodynamic collapse.
- Status asthmaticus: prolonged, life-threatening exacerbation refractory to standard bronchodilator therapy requiring care in the intensive care unit
Long-Term Complications
- Fixed airflow obstruction: resulting from irreversible airway remodeling; the FEV1/FVC ratio does not fully normalize after bronchodilator administration; this finding may be clinically indistinguishable from chronic obstructive pulmonary disease in some patients
- Accelerated FEV1 decline: beyond expected age-related trajectory in poorly controlled, frequently exacerbating disease
- Oral candidiasis and hoarseness: common ICS adverse effects; mitigated by spacer use and mouth rinsing after inhaler use
- Hypothalamic-pituitary-adrenal axis suppression: can occur with high-dose inhaled corticosteroids or frequent OCS courses and may cause iatrogenic adrenal insufficiency and osteoporosis in patients who require long-term OCS therapy
- Sleep disturbance, school/work absenteeism, and reduced quality of life: primary drivers of psychosocial disease burden
- Death: uncommon in the absence of severe comorbidities; risk elevated substantially in patients with prior near-fatal exacerbation, current tobacco use, and inadequate access to controller therapy
Consultations
Refer patients to an asthma specialist for consultation for the following reasons:
- Difficulty achieving or maintaining asthma control
- Requirement for more than 2 bursts of oral systemic corticosteroids in 1 year or an exacerbation requiring hospitalization
- Requirement for step 4 care or higher (step 3 care or higher for children aged 0 to 4 years)
- Consideration of immunotherapy or omalizumab
- When additional testing is necessary [53]
Deterrence and Patient Education
Patient education is a cornerstone of effective asthma treatment. Results from studies demonstrated that patient education reduces emergency department visits, hospitalizations, and oral corticosteroid use. All education should be individualized, delivered by an interdisciplinary team, and reinforced at every clinical encounter.[EPA. Expert Report 3. Guidelines for the Diagnosis and Management of Asthma][54]
Referral Criteria for Specialist Evaluation
- Difficulty achieving or maintaining asthma control despite step 3 therapy (step 2 in children aged 0 to 4 years)[EPA. Expert Report 3. Guidelines for the Diagnosis and Management of Asthma][54]
- Two or more oral corticosteroid courses in the preceding year or any hospitalization for asthma
- Prior life-threatening exacerbation, intensive care unit admission, or intubation
- Consideration of biologic therapy, allergen immunotherapy, or bronchial thermoplasty
- Suspected occupational asthma requiring specialized diagnostic evaluation
- Diagnostic uncertainty, requiring confirmation of asthma and exclusion of alternative diagnoses
Patient Education Essentials
- Written asthma action plan: personalized, peak expiratory flow zone-based or symptom-based; specifies when to adjust medications, when to seek urgent or emergency care, and whom to contact in an emergency; guideline-recommended for all patients
- Inhaler technique: demonstrated and assessed at every visit; a metered-dose inhaler with a spacer is strongly preferred over a metered-dose inhaler alone (2 to 9 times greater pulmonary deposition); a dry powder inhaler requires forceful, rapid inhalation and is unsuitable during a severe exacerbation
- Controller and reliever distinction: patients must understand that inhaled corticosteroid controllers prevent inflammation (and are taken daily regardless of symptoms) and that reliever inhalers treat acute symptoms but do not control underlying disease. Confusion between controller and reliever inhalers is a leading cause of poor asthma control [EPA. Expert Report 3. Guidelines for the Diagnosis and Management of Asthma]
- Trigger identification and avoidance: personalized guidance based on allergy testing results, occupational history, and a home environmental assessment
- Asthma APGAR tool: the Activities, Persistent, Triggers, Asthma Medications, and Response to Therapy tool is validated for use in primary care; improved APGAR scores are associated with reduced utilization of emergency and urgent care [54]
- Smoking cessation: counseling and pharmacotherapy (first-line varenicline, bupropion, or nicotine replacement therapy) offered at every visit to all patients and household members who smoke
Pearls and Other Issues
Pearl 1: Silent Chest is a Medical Emergency
The complete absence of wheeze in a patient with severe dyspnea signifies near-complete airflow obstruction and impending respiratory arrest. Do not be reassured by the absence of wheeze. A silent chest is the most dangerous physical examination finding in acute asthma.
Pearl 2: SABA Overuse Is a Red Flag
Dispensing 3 or more SABA canisters per year is an independent predictor of asthma-related death. Identify these patients proactively through pharmacy records, escalate controller therapy immediately, and refer them to a specialist. The 2024 GINA guidelines strongly recommend against SABA monotherapy at any step.
Pearl 3: Normal Spirometry Does Not Exclude Asthma
Spirometry findings obtained between episodes may be entirely normal in patients with clearly symptomatic asthma. When spirometry findings are normal but clinical suspicion for asthma remains high, clinicians should proceed with methacholine bronchoprovocation testing and serial peak expiratory flow monitoring.
Pearl 4: Biologic Selection Requires Phenotyping First
Clinicians should obtain a complete biomarker panel (blood eosinophil count, total IgE, allergen sensitization, and FeNO) before selecting a biologic agent. Phenotyping directly determines efficacy. Anti–IL-5 agents are ineffective in non–T2 asthma, and omalizumab is ineffective when IgE criteria are not met. Tezepelumab is the only biologic option for a confirmed non–T2 phenotype.
Pearl 5: Occupational Asthma Requires Early Removal From Exposure
Early removal from the causative occupational exposure is the most effective treatment for occupational asthma. A delay of more than 1 to 2 years after symptom onset is associated with a substantially worse long-term prognosis and higher rates of persistent airflow obstruction. Ask about work-related symptom patterns at every initial asthma evaluation in adults.
Pearl 6: Montelukast Neuropsychiatric Warning
The FDA boxed warning for montelukast requires explicit counseling for all patients about the risk of serious neuropsychiatric adverse effects, including agitation, depression, suicidal thinking and behavior, and sleep disturbances. Montelukast should not be the default first-line add-on therapy. Escalation of inhaled corticosteroid therapy, or the combination of inhaled corticosteroid and LABA, is preferred.
Pearl 7: Dupilumab Eosinophil Spike is Expected
A transient rise in the blood eosinophil count within the first 4 to 8 weeks after dupilumab initiation is an expected class effect resulting from redistribution of eosinophils from the tissues to the peripheral blood. The increase does not indicate treatment failure or eosinophilic end-organ disease unless accompanied by specific organ symptoms. Continue therapy and recheck the eosinophil count in 8 weeks.
Pearl 8: Allergen Immunotherapy Before Biologic in Mild-Moderate Allergic Asthma
For patients with mild-to-moderate allergic asthma who have confirmed allergen sensitization and are candidates for both therapies, allergen immunotherapy should be pursued before or alongside biologic therapy. Allergen immunotherapy is the only disease-modifying option and may reduce or eliminate the need for long-term controller therapy. Biologic agents address downstream inflammation, whereas allergen immunotherapy addresses the underlying sensitization.
Enhancing Healthcare Team Outcomes
Asthma is most effectively treated through a coordinated, interprofessional approach that engages clinicians, advanced practice clinicians, nurses, pharmacists, respiratory therapists, and, particularly in pediatric asthma, school nurses and social workers. The complexity of asthma treatment, including accurate phenotyping, biologic selection, inhaler technique optimization, and patient education, far exceeds what any single clinician can achieve in isolation.[1][55]
Clinicians
Primary care clinicians play a central role in initial diagnosis, stepwise pharmacologic treatment, and long-term monitoring of the majority of patients with asthma. Pulmonologists, allergists, and immunologists provide subspecialty expertise in difficult-to-control disease, initiation and monitoring of biologic therapy, allergen immunotherapy, and evaluation of occupational asthma. A structured primary care clinician-to-specialist referral pathway with agreed triggers (see Deterrence section) optimizes care without overreliance on specialist capacity.[EPA. Expert Report 3. Guidelines for the Diagnosis and Management of Asthma][56]
Nurses and Asthma Educators
Certified asthma educators and specialty nurses are central to improving patient self-management competency. Results from a landmark retrospective cohort study conducted in Massachusetts from 2012 to 2015 demonstrated that a school nurse-supervised asthma therapy program, in which inhaled corticosteroids were administered daily under direct supervision to children at high risk with persistent asthma, produced significant reductions in emergency department visits, hospitalizations, and albuterol refill rates after the intervention compared with baseline, underscoring the measurable clinical impact of nursing-led adherence support.[1][56]
Pharmacists
Pharmacists serve a dual role: dispensing and counseling on proper medication use and identifying and intervening when nonadherence occurs. Results from a retrospective study at a South Bronx asthma clinic demonstrated that a pharmacist-led asthma education program, combining medication counseling, inhaler technique training, and action plan education, was associated with improved Asthma Control Test scores, increased medication adherence, and reduced emergency department visits.[57] Ongoing pharmacist-to-clinician communication about SABA refill frequency can prospectively identify patients at risk before clinical deterioration.
Respiratory Therapists
Respiratory therapists are essential in inpatient and emergency department care, including administering nebulized bronchodilators, performing bedside spirometry and peak expiratory flow measurements, treating patients receiving noninvasive positive pressure ventilation, and optimizing mechanical ventilator settings in intubated patients with status asthmaticus. In outpatient and educational settings, respiratory therapists contribute to inhaler technique training, pulmonary rehabilitation, and home nebulizer instruction.
Telemedicine and Technology
Telemedicine platforms enable remote symptom monitoring, peak expiratory flow tracking, and medication adjustments between office visits, which are particularly valuable for rural patients without ready access to specialists. Digital inhaler sensors and connected health applications provide objective data on SABA use that can trigger proactive outreach before exacerbations escalate to emergency care. Artificial intelligence-assisted biomarker interpretation tools are emerging as decision-support adjuncts for biologic selection in primary care settings.[3]
Communication and Coordination
Effective interprofessional communication supports all team-based asthma care. Pharmacist-to-clinician alerts for excessive SABA refills, nurse-to-clinician documentation of missed inhaled corticosteroid refills, and structured emergency department-to-primary care transition protocols reduce relapse rates and 30-day readmissions. Team-based case treatment for patients with severe or refractory asthma, incorporating social work support for housing remediation, pest control, smoking cessation resources, and insurance navigation, addresses the social determinants that drive asthma disparities in communities with a high disease burden.
Media
(Click Image to Enlarge)
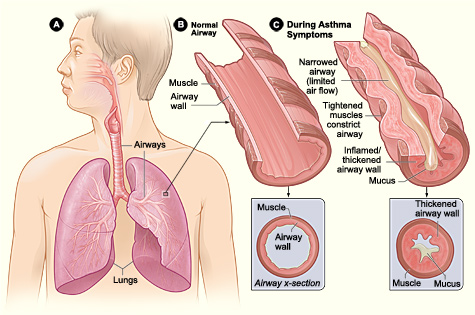
Pathophysiology of Asthma. Figure A displays the location of the lungs and airways in the body. Figure B shows a cross section of a normal airway. Figure C illustrates a cross section of an airway during asthma symptoms.
National Institutes of Health, Public Domain, via Wikimedia Commons
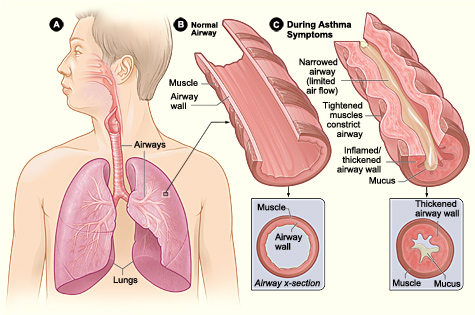{kind=link}
(Click Image to Enlarge)
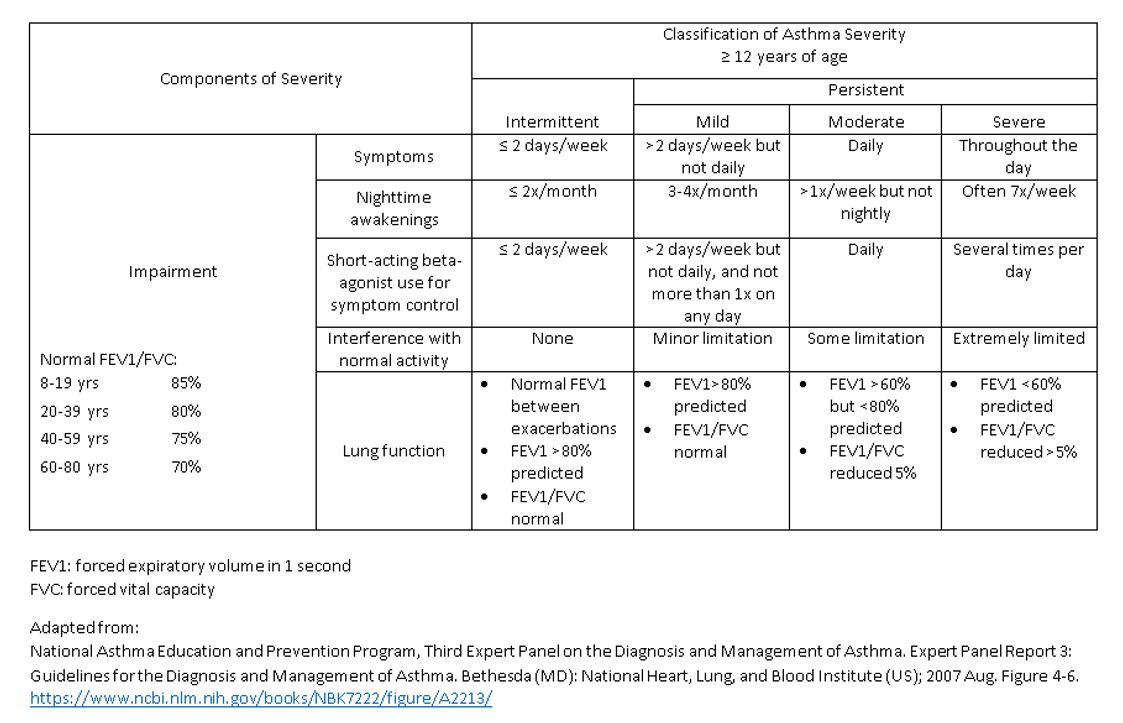
Asthma Severity Classification by The National Asthma Education and Prevention Program.
Contributed by R Chabra, DO
References
Rajvanshi N, Kumar P, Goyal JP. Global Initiative for Asthma Guidelines 2024: An Update. Indian pediatrics. 2024 Aug 15:61(8):781-786 [PubMed PMID: 39051318]
Lambrecht BN, Hammad H. The immunology of asthma. Nature immunology. 2015 Jan:16(1):45-56. doi: 10.1038/ni.3049. Epub [PubMed PMID: 25521684]
Israel E, Reddel HK. Severe and Difficult-to-Treat Asthma in Adults. The New England journal of medicine. 2017 Sep 7:377(10):965-976. doi: 10.1056/NEJMra1608969. Epub [PubMed PMID: 28877019]
Eder W, Ege MJ, von Mutius E. The asthma epidemic. The New England journal of medicine. 2006 Nov 23:355(21):2226-35 [PubMed PMID: 17124020]
Burke H, Leonardi-Bee J, Hashim A, Pine-Abata H, Chen Y, Cook DG, Britton JR, McKeever TM. Prenatal and passive smoke exposure and incidence of asthma and wheeze: systematic review and meta-analysis. Pediatrics. 2012 Apr:129(4):735-44. doi: 10.1542/peds.2011-2196. Epub 2012 Mar 19 [PubMed PMID: 22430451]
Level 1 (high-level) evidenceTarlo SM, Balmes J, Balkissoon R, Beach J, Beckett W, Bernstein D, Blanc PD, Brooks SM, Cowl CT, Daroowalla F, Harber P, Lemiere C, Liss GM, Pacheco KA, Redlich CA, Rowe B, Heitzer J. Diagnosis and management of work-related asthma: American College Of Chest Physicians Consensus Statement. Chest. 2008 Sep:134(3 Suppl):1S-41S. doi: 10.1378/chest.08-0201. Epub [PubMed PMID: 18779187]
Level 3 (low-level) evidenceArrieta MC, Stiemsma LT, Dimitriu PA, Thorson L, Russell S, Yurist-Doutsch S, Kuzeljevic B, Gold MJ, Britton HM, Lefebvre DL, Subbarao P, Mandhane P, Becker A, McNagny KM, Sears MR, Kollmann T, CHILD Study Investigators, Mohn WW, Turvey SE, Finlay BB. Early infancy microbial and metabolic alterations affect risk of childhood asthma. Science translational medicine. 2015 Sep 30:7(307):307ra152. doi: 10.1126/scitranslmed.aab2271. Epub [PubMed PMID: 26424567]
Fahy JV. Type 2 inflammation in asthma--present in most, absent in many. Nature reviews. Immunology. 2015 Jan:15(1):57-65. doi: 10.1038/nri3786. Epub [PubMed PMID: 25534623]
Level 3 (low-level) evidenceBrusselle GG, Koppelman GH. Biologic Therapies for Severe Asthma. The New England journal of medicine. 2022 Jan 13:386(2):157-171. doi: 10.1056/NEJMra2032506. Epub [PubMed PMID: 35020986]
Dweik RA, Boggs PB, Erzurum SC, Irvin CG, Leigh MW, Lundberg JO, Olin AC, Plummer AL, Taylor DR, American Thoracic Society Committee on Interpretation of Exhaled Nitric Oxide Levels (FENO) for Clinical Applications. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. American journal of respiratory and critical care medicine. 2011 Sep 1:184(5):602-15. doi: 10.1164/rccm.9120-11ST. Epub [PubMed PMID: 21885636]
Level 1 (high-level) evidencePavord ID, Holliday M, Reddel HK, Braithwaite I, Ebmeier S, Hancox RJ, Harrison T, Houghton C, Oldfield K, Papi A, Williams M, Weatherall M, Beasley R, Novel START Study Team. Predictive value of blood eosinophils and exhaled nitric oxide in adults with mild asthma: a prespecified subgroup analysis of an open-label, parallel-group, randomised controlled trial. The Lancet. Respiratory medicine. 2020 Jul:8(7):671-680. doi: 10.1016/S2213-2600(20)30053-9. Epub 2020 Mar 11 [PubMed PMID: 32171064]
Level 1 (high-level) evidenceMenzies-Gow A, Corren J, Bourdin A, Chupp G, Israel E, Wechsler ME, Brightling CE, Griffiths JM, Hellqvist Å, Bowen K, Kaur P, Almqvist G, Ponnarambil S, Colice G. Tezepelumab in Adults and Adolescents with Severe, Uncontrolled Asthma. The New England journal of medicine. 2021 May 13:384(19):1800-1809. doi: 10.1056/NEJMoa2034975. Epub [PubMed PMID: 33979488]
Wechsler ME, Menzies-Gow A, Brightling CE, Kuna P, Korn S, Welte T, Griffiths JM, Sałapa K, Hellqvist Å, Almqvist G, Lal H, Kaur P, Skärby T, Colice G, SOURCE study group. Evaluation of the oral corticosteroid-sparing effect of tezepelumab in adults with oral corticosteroid-dependent asthma (SOURCE): a randomised, placebo-controlled, phase 3 study. The Lancet. Respiratory medicine. 2022 Jul:10(7):650-660. doi: 10.1016/S2213-2600(21)00537-3. Epub 2022 Mar 29 [PubMed PMID: 35364018]
Level 1 (high-level) evidenceWoodruff PG, Modrek B, Choy DF, Jia G, Abbas AR, Ellwanger A, Koth LL, Arron JR, Fahy JV. T-helper type 2-driven inflammation defines major subphenotypes of asthma. American journal of respiratory and critical care medicine. 2009 Sep 1:180(5):388-95. doi: 10.1164/rccm.200903-0392OC. Epub 2009 May 29 [PubMed PMID: 19483109]
Menzies-Gow A, Bafadhel M, Busse WW, Casale TB, Kocks JWH, Pavord ID, Szefler SJ, Woodruff PG, de Giorgio-Miller A, Trudo F, Fageras M, Ambrose CS. An expert consensus framework for asthma remission as a treatment goal. The Journal of allergy and clinical immunology. 2020 Mar:145(3):757-765. doi: 10.1016/j.jaci.2019.12.006. Epub 2019 Dec 19 [PubMed PMID: 31866436]
Level 3 (low-level) evidenceHeaney LG, Perez de Llano L, Al-Ahmad M, Backer V, Busby J, Canonica GW, Christoff GC, Cosio BG, FitzGerald JM, Heffler E, Iwanaga T, Jackson DJ, Menzies-Gow AN, Papadopoulos NG, Papaioannou AI, Pfeffer PE, Popov TA, Porsbjerg CM, Rhee CK, Sadatsafavi M, Tohda Y, Wang E, Wechsler ME, Alacqua M, Altraja A, Bjermer L, Björnsdóttir US, Bourdin A, Brusselle GG, Buhl R, Costello RW, Hew M, Koh MS, Lehmann S, Lehtimäki L, Peters M, Taillé C, Taube C, Tran TN, Zangrilli J, Bulathsinhala L, Carter VA, Chaudhry I, Eleangovan N, Hosseini N, Kerkhof M, Murray RB, Price CA, Price DB. Eosinophilic and Noneosinophilic Asthma: An Expert Consensus Framework to Characterize Phenotypes in a Global Real-Life Severe Asthma Cohort. Chest. 2021 Sep:160(3):814-830. doi: 10.1016/j.chest.2021.04.013. Epub 2021 Apr 19 [PubMed PMID: 33887242]
Level 3 (low-level) evidenceChung KF, Wenzel SE, Brozek JL, Bush A, Castro M, Sterk PJ, Adcock IM, Bateman ED, Bel EH, Bleecker ER, Boulet LP, Brightling C, Chanez P, Dahlen SE, Djukanovic R, Frey U, Gaga M, Gibson P, Hamid Q, Jajour NN, Mauad T, Sorkness RL, Teague WG. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. The European respiratory journal. 2014 Feb:43(2):343-73. doi: 10.1183/09031936.00202013. Epub 2013 Dec 12 [PubMed PMID: 24337046]
Humbert M, Beasley R, Ayres J, Slavin R, Hébert J, Bousquet J, Beeh KM, Ramos S, Canonica GW, Hedgecock S, Fox H, Blogg M, Surrey K. Benefits of omalizumab as add-on therapy in patients with severe persistent asthma who are inadequately controlled despite best available therapy (GINA 2002 step 4 treatment): INNOVATE. Allergy. 2005 Mar:60(3):309-16 [PubMed PMID: 15679715]
Abramson MJ, Puy RM, Weiner JM. Injection allergen immunotherapy for asthma. The Cochrane database of systematic reviews. 2010 Aug 4:2010(8):CD001186. doi: 10.1002/14651858.CD001186.pub2. Epub 2010 Aug 4 [PubMed PMID: 20687065]
Level 1 (high-level) evidenceO'Byrne PM, FitzGerald JM, Bateman ED, Barnes PJ, Zhong N, Keen C, Jorup C, Lamarca R, Ivanov S, Reddel HK. Inhaled Combined Budesonide-Formoterol as Needed in Mild Asthma. The New England journal of medicine. 2018 May 17:378(20):1865-1876. doi: 10.1056/NEJMoa1715274. Epub [PubMed PMID: 29768149]
Bel EH, Sousa A, Fleming L, Bush A, Chung KF, Versnel J, Wagener AH, Wagers SS, Sterk PJ, Compton CH, Unbiased Biomarkers for the Prediction of Respiratory Disease Outcome (U-BIOPRED) Consortium, Consensus Generation. Diagnosis and definition of severe refractory asthma: an international consensus statement from the Innovative Medicine Initiative (IMI). Thorax. 2011 Oct:66(10):910-7. doi: 10.1136/thx.2010.153643. Epub 2010 Nov 23 [PubMed PMID: 21106547]
Level 3 (low-level) evidenceReddel HK, FitzGerald JM, Bateman ED, Bacharier LB, Becker A, Brusselle G, Buhl R, Cruz AA, Fleming L, Inoue H, Ko FW, Krishnan JA, Levy ML, Lin J, Pedersen SE, Sheikh A, Yorgancioglu A, Boulet LP. GINA 2019: a fundamental change in asthma management: Treatment of asthma with short-acting bronchodilators alone is no longer recommended for adults and adolescents. The European respiratory journal. 2019 Jun:53(6):. pii: 1901046. doi: 10.1183/13993003.01046-2019. Epub 2019 Jun 27 [PubMed PMID: 31249014]
Bateman ED, Reddel HK, O'Byrne PM, Barnes PJ, Zhong N, Keen C, Jorup C, Lamarca R, Siwek-Posluszna A, FitzGerald JM. As-Needed Budesonide-Formoterol versus Maintenance Budesonide in Mild Asthma. The New England journal of medicine. 2018 May 17:378(20):1877-1887. doi: 10.1056/NEJMoa1715275. Epub [PubMed PMID: 29768147]
Dhami S, Kakourou A, Asamoah F, Agache I, Lau S, Jutel M, Muraro A, Roberts G, Akdis CA, Bonini M, Cavkaytar O, Flood B, Gajdanowicz P, Izuhara K, Kalayci Ö, Mosges R, Palomares O, Pfaar O, Smolinska S, Sokolowska M, Asaria M, Netuveli G, Zaman H, Akhlaq A, Sheikh A. Allergen immunotherapy for allergic asthma: A systematic review and meta-analysis. Allergy. 2017 Dec:72(12):1825-1848. doi: 10.1111/all.13208. Epub 2017 Jul 6 [PubMed PMID: 28543086]
Level 1 (high-level) evidenceCastro M, Rubin AS, Laviolette M, Fiterman J, De Andrade Lima M, Shah PL, Fiss E, Olivenstein R, Thomson NC, Niven RM, Pavord ID, Simoff M, Duhamel DR, McEvoy C, Barbers R, Ten Hacken NH, Wechsler ME, Holmes M, Phillips MJ, Erzurum S, Lunn W, Israel E, Jarjour N, Kraft M, Shargill NS, Quiring J, Berry SM, Cox G, AIR2 Trial Study Group. Effectiveness and safety of bronchial thermoplasty in the treatment of severe asthma: a multicenter, randomized, double-blind, sham-controlled clinical trial. American journal of respiratory and critical care medicine. 2010 Jan 15:181(2):116-24. doi: 10.1164/rccm.200903-0354OC. Epub 2009 Oct 8 [PubMed PMID: 19815809]
Level 1 (high-level) evidenceHanania NA, Alpan O, Hamilos DL, Condemi JJ, Reyes-Rivera I, Zhu J, Rosen KE, Eisner MD, Wong DA, Busse W. Omalizumab in severe allergic asthma inadequately controlled with standard therapy: a randomized trial. Annals of internal medicine. 2011 May 3:154(9):573-82. doi: 10.7326/0003-4819-154-9-201105030-00002. Epub [PubMed PMID: 21536936]
Level 1 (high-level) evidenceCastro M, Corren J, Pavord ID, Maspero J, Wenzel S, Rabe KF, Busse WW, Ford L, Sher L, FitzGerald JM, Katelaris C, Tohda Y, Zhang B, Staudinger H, Pirozzi G, Amin N, Ruddy M, Akinlade B, Khan A, Chao J, Martincova R, Graham NMH, Hamilton JD, Swanson BN, Stahl N, Yancopoulos GD, Teper A. Dupilumab Efficacy and Safety in Moderate-to-Severe Uncontrolled Asthma. The New England journal of medicine. 2018 Jun 28:378(26):2486-2496. doi: 10.1056/NEJMoa1804092. Epub 2018 May 21 [PubMed PMID: 29782217]
Rabe KF, Nair P, Brusselle G, Maspero JF, Castro M, Sher L, Zhu H, Hamilton JD, Swanson BN, Khan A, Chao J, Staudinger H, Pirozzi G, Antoni C, Amin N, Ruddy M, Akinlade B, Graham NMH, Stahl N, Yancopoulos GD, Teper A. Efficacy and Safety of Dupilumab in Glucocorticoid-Dependent Severe Asthma. The New England journal of medicine. 2018 Jun 28:378(26):2475-2485. doi: 10.1056/NEJMoa1804093. Epub 2018 May 21 [PubMed PMID: 29782224]
Ortega HG, Liu MC, Pavord ID, Brusselle GG, FitzGerald JM, Chetta A, Humbert M, Katz LE, Keene ON, Yancey SW, Chanez P, MENSA Investigators. Mepolizumab treatment in patients with severe eosinophilic asthma. The New England journal of medicine. 2014 Sep 25:371(13):1198-207. doi: 10.1056/NEJMoa1403290. Epub 2014 Sep 8 [PubMed PMID: 25199059]
Bel EH, Wenzel SE, Thompson PJ, Prazma CM, Keene ON, Yancey SW, Ortega HG, Pavord ID, SIRIUS Investigators. Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. The New England journal of medicine. 2014 Sep 25:371(13):1189-97. doi: 10.1056/NEJMoa1403291. Epub 2014 Sep 8 [PubMed PMID: 25199060]
Bleecker ER, FitzGerald JM, Chanez P, Papi A, Weinstein SF, Barker P, Sproule S, Gilmartin G, Aurivillius M, Werkström V, Goldman M, SIROCCO study investigators. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting β(2)-agonists (SIROCCO): a randomised, multicentre, placebo-controlled phase 3 trial. Lancet (London, England). 2016 Oct 29:388(10056):2115-2127. doi: 10.1016/S0140-6736(16)31324-1. Epub 2016 Sep 5 [PubMed PMID: 27609408]
Level 1 (high-level) evidenceNair P, Wenzel S, Rabe KF, Bourdin A, Lugogo NL, Kuna P, Barker P, Sproule S, Ponnarambil S, Goldman M, ZONDA Trial Investigators. Oral Glucocorticoid-Sparing Effect of Benralizumab in Severe Asthma. The New England journal of medicine. 2017 Jun 22:376(25):2448-2458. doi: 10.1056/NEJMoa1703501. Epub 2017 May 22 [PubMed PMID: 28530840]
Corren J, Parnes JR, Wang L, Mo M, Roseti SL, Griffiths JM, van der Merwe R. Tezepelumab in Adults with Uncontrolled Asthma. The New England journal of medicine. 2017 Sep 7:377(10):936-946. doi: 10.1056/NEJMoa1704064. Epub [PubMed PMID: 28877011]
Diver S, Khalfaoui L, Emson C, Wenzel SE, Menzies-Gow A, Wechsler ME, Johnston J, Molfino N, Parnes JR, Megally A, Colice G, Brightling CE, CASCADE study investigators. Effect of tezepelumab on airway inflammatory cells, remodelling, and hyperresponsiveness in patients with moderate-to-severe uncontrolled asthma (CASCADE): a double-blind, randomised, placebo-controlled, phase 2 trial. The Lancet. Respiratory medicine. 2021 Nov:9(11):1299-1312. doi: 10.1016/S2213-2600(21)00226-5. Epub 2021 Jul 10 [PubMed PMID: 34256031]
Level 1 (high-level) evidenceCorren J, Menzies-Gow A, Chupp G, Israel E, Korn S, Cook B, Ambrose CS, Hellqvist Å, Roseti SL, Molfino NA, Llanos JP, Martin N, Bowen K, Griffiths JM, Parnes JR, Colice G. Efficacy of Tezepelumab in Severe, Uncontrolled Asthma: Pooled Analysis of the PATHWAY and NAVIGATOR Clinical Trials. American journal of respiratory and critical care medicine. 2023 Jul 1:208(1):13-24. doi: 10.1164/rccm.202210-2005OC. Epub [PubMed PMID: 37015033]
Wechsler ME, Ruddy MK, Pavord ID, Israel E, Rabe KF, Ford LB, Maspero JF, Abdulai RM, Hu CC, Martincova R, Jessel A, Nivens MC, Amin N, Weinreich DM, Yancopoulos GD, Goulaouic H. Efficacy and Safety of Itepekimab in Patients with Moderate-to-Severe Asthma. The New England journal of medicine. 2021 Oct 28:385(18):1656-1668. doi: 10.1056/NEJMoa2024257. Epub [PubMed PMID: 34706171]
Agache I, Akdis CA, Akdis M, Canonica GW, Casale T, Chivato T, Corren J, Chu DK, Del Giacco S, Eiwegger T, Flood B, Firinu D, Gern JE, Hamelmann E, Hanania N, Hernández-Martín I, Knibb R, Mäkelä M, Nair P, O'Mahony L, Papadopoulos NG, Papi A, Park HS, Pérez de Llano L, Pfaar O, Quirce S, Sastre J, Shamji M, Schwarze J, Palomares O, Jutel M. EAACI Biologicals Guidelines-Recommendations for severe asthma. Allergy. 2021 Jan:76(1):14-44. doi: 10.1111/all.14425. Epub 2020 Aug 10 [PubMed PMID: 32484954]
Farne HA, Wilson A, Milan S, Banchoff E, Yang F, Powell CV. Anti-IL-5 therapies for asthma. The Cochrane database of systematic reviews. 2022 Jul 12:7(7):CD010834. doi: 10.1002/14651858.CD010834.pub4. Epub 2022 Jul 12 [PubMed PMID: 35838542]
Level 1 (high-level) evidenceMenzies-Gow A, Wechsler ME, Brightling CE, Korn S, Corren J, Israel E, Chupp G, Bednarczyk A, Ponnarambil S, Caveney S, Almqvist G, Gołąbek M, Simonsson L, Lawson K, Bowen K, Colice G, DESTINATION study investigators. Long-term safety and efficacy of tezepelumab in people with severe, uncontrolled asthma (DESTINATION): a randomised, placebo-controlled extension study. The Lancet. Respiratory medicine. 2023 May:11(5):425-438. doi: 10.1016/S2213-2600(22)00492-1. Epub 2023 Jan 23 [PubMed PMID: 36702146]
Level 1 (high-level) evidenceRodrigo GJ, Castro-Rodriguez JA. Anticholinergics in the treatment of children and adults with acute asthma: a systematic review with meta-analysis. Thorax. 2005 Sep:60(9):740-6 [PubMed PMID: 16055613]
Level 1 (high-level) evidenceGriffiths B, Ducharme FM. Combined inhaled anticholinergics and short-acting beta2-agonists for initial treatment of acute asthma in children. The Cochrane database of systematic reviews. 2013 Aug 21:2013(8):CD000060. doi: 10.1002/14651858.CD000060.pub2. Epub 2013 Aug 21 [PubMed PMID: 23966133]
Level 1 (high-level) evidenceRowe BH, Bretzlaff JA, Bourdon C, Bota GW, Camargo CA Jr. Magnesium sulfate for treating exacerbations of acute asthma in the emergency department. The Cochrane database of systematic reviews. 2000:2000(2):CD001490 [PubMed PMID: 10796650]
Level 1 (high-level) evidenceKew KM, Kirtchuk L, Michell CI. Intravenous magnesium sulfate for treating adults with acute asthma in the emergency department. The Cochrane database of systematic reviews. 2014 May 28:2014(5):CD010909. doi: 10.1002/14651858.CD010909.pub2. Epub 2014 May 28 [PubMed PMID: 24865567]
Level 1 (high-level) evidenceRodrigo G, Pollack C, Rodrigo C, Rowe BH. Heliox for nonintubated acute asthma patients. The Cochrane database of systematic reviews. 2006 Oct 18:2006(4):CD002884 [PubMed PMID: 17054154]
Level 1 (high-level) evidenceWechsler ME, Rogers L, Canonica GW, Bourdin A, Altincatal A, Hardin M, Soler X, Rowe PJ, Deniz Y, Sacks H, Jacob-Nara JA. Long-term dupilumab efficacy in type 2 asthma regardless of baseline characteristics. ERJ open research. 2024 Nov:10(6):. pii: 00188-2024. doi: 10.1183/23120541.00188-2024. Epub 2024 Dec 16 [PubMed PMID: 39687390]
Pavord ID, Korn S, Howarth P, Bleecker ER, Buhl R, Keene ON, Ortega H, Chanez P. Mepolizumab for severe eosinophilic asthma (DREAM): a multicentre, double-blind, placebo-controlled trial. Lancet (London, England). 2012 Aug 18:380(9842):651-9. doi: 10.1016/S0140-6736(12)60988-X. Epub [PubMed PMID: 22901886]
Level 1 (high-level) evidenceFitzGerald JM, Bleecker ER, Nair P, Korn S, Ohta K, Lommatzsch M, Ferguson GT, Busse WW, Barker P, Sproule S, Gilmartin G, Werkström V, Aurivillius M, Goldman M, CALIMA study investigators. Benralizumab, an anti-interleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet (London, England). 2016 Oct 29:388(10056):2128-2141. doi: 10.1016/S0140-6736(16)31322-8. Epub 2016 Sep 5 [PubMed PMID: 27609406]
Level 1 (high-level) evidenceTaleb AA, Badgett RG. In severe, uncontrolled asthma, tezepelumab reduced exacerbations and improved asthma control at 1 y. Annals of internal medicine. 2021 Oct:174(10):JC115. doi: 10.7326/ACPJ202110190-115. Epub 2021 Oct 5 [PubMed PMID: 34606305]
Wechsler ME, Brusselle G, Virchow JC, Bourdin A, Kostikas K, Llanos JP, Roseti SL, Ambrose CS, Hunter G, Jackson DJ, Castro M, Lugogo N, Pavord ID, Martin N, Brightling CE. Clinical response and on-treatment clinical remission with tezepelumab in a broad population of patients with severe, uncontrolled asthma: results over 2 years from the NAVIGATOR and DESTINATION studies. The European respiratory journal. 2024 Dec:64(6):. doi: 10.1183/13993003.00316-2024. Epub 2024 Dec 5 [PubMed PMID: 39326921]
Rabe KF, Celli BR, Wechsler ME, Abdulai RM, Luo X, Boomsma MM, Staudinger H, Horowitz JE, Baras A, Ferreira MA, Ruddy MK, Nivens MC, Amin N, Weinreich DM, Yancopoulos GD, Goulaouic H. Safety and efficacy of itepekimab in patients with moderate-to-severe COPD: a genetic association study and randomised, double-blind, phase 2a trial. The Lancet. Respiratory medicine. 2021 Nov:9(11):1288-1298. doi: 10.1016/S2213-2600(21)00167-3. Epub 2021 Jul 21 [PubMed PMID: 34302758]
Level 1 (high-level) evidenceSears MR. Predicting asthma outcomes. The Journal of allergy and clinical immunology. 2015 Oct:136(4):829-36; quiz 837. doi: 10.1016/j.jaci.2015.04.048. Epub [PubMed PMID: 26449797]
Childhood Asthma Management Program Research Group, Szefler S, Weiss S, Tonascia J, Adkinson NF, Bender B, Cherniack R, Donithan M, Kelly HW, Reisman J, Shapiro GG, Sternberg AL, Strunk R, Taggart V, Van Natta M, Wise R, Wu M, Zeiger R. Long-term effects of budesonide or nedocromil in children with asthma. The New England journal of medicine. 2000 Oct 12:343(15):1054-63 [PubMed PMID: 11027739]
Elward KS, Pollart SM. Medical Therapy for Asthma: Updates from the NAEPP Guidelines. American family physician. 2010 Nov 15:82(10):1242-51 [PubMed PMID: 21121536]
Tierney WM, Oppenheimer CC, Hudson BL, Benz J, Finn A, Hickner JM, Lanier D, Gaylin DS. A national survey of primary care practice-based research networks. Annals of family medicine. 2007 May-Jun:5(3):242-50 [PubMed PMID: 17548852]
Level 3 (low-level) evidenceBaptist AP, Thompson M, Grossman KS, Mohammed L, Sy A, Sanders GM. Social media, text messaging, and email-preferences of asthma patients between 12 and 40 years old. The Journal of asthma : official journal of the Association for the Care of Asthma. 2011 Oct:48(8):824-30. doi: 10.3109/02770903.2011.608460. Epub 2011 Aug 24 [PubMed PMID: 21864099]
Papi A, Ryan D, Soriano JB, Chrystyn H, Bjermer L, Rodríguez-Roisin R, Dolovich MB, Harris M, Wood L, Batsiou M, Thornhill SI, Price DB. Relationship of Inhaled Corticosteroid Adherence to Asthma Exacerbations in Patients with Moderate-to-Severe Asthma. The journal of allergy and clinical immunology. In practice. 2018 Nov-Dec:6(6):1989-1998.e3. doi: 10.1016/j.jaip.2018.03.008. Epub 2018 Apr 5 [PubMed PMID: 29627457]
Elliott JP, Morphew T, Gentile D, Williams P, Barrett C, Sossong N. Improved asthma outcomes among at-risk children in a pharmacist-led, interdisciplinary school-based health clinic: A pilot study of the CAReS program. Journal of the American Pharmacists Association : JAPhA. 2022 Mar-Apr:62(2):519-525.e1. doi: 10.1016/j.japh.2021.11.008. Epub 2021 Nov 11 [PubMed PMID: 34863634]
Level 3 (low-level) evidence