Introduction
Asterognosis is the inability to identify objects by tactile exploration in the absence of visual input. Stereognosis, derived from the Greek stereos (“solid”) and gnosis (“knowledge”), refers to the ability to recognize the 3-dimensional form of an object through tactile manipulation.[1]
Shape, texture, size, and weight are assessed primarily with the hands. Manual stereognosis requires the dorsal column-medial lemniscus tract (DCMLT) for transmission of discriminative touch and proprioceptive information and the parietal cortex for cortical processing (see Images. Ascending Pathways of the Spinal Cord; Somatosensory Homunculus Representation). Oral stereognosis refers to the capacity to recognize object shapes through tactile input from the oral mucosa.[2][3][4][5] This function relies on signals from receptors within the oral structures, including teeth, and is supported by the relatively large cortical representation of the oral cavity.[6] Stereognosis is generally well developed by approximately 6 years of age.
Also termed "somatosensory agnosia," asterognosis is characterized by impaired recognition of objects by somatosensory discrimination of size, texture, weight, and shape in the absence of significant peripheral sensory loss.[7] True tactile agnosia refers to asterognosis occurring despite intact elementary sensation, whereas similar deficits may arise from loss of discriminative touch in lesions of the DCMLT. The condition most often results from damage to the contralateral parietal cortex but may also follow thalamic or DCMLT injury.[8] Asterognosis has been described as a potential sign of cortical dysfunction in dementia, although it lacks reliability as a diagnostic marker.[9]
Recognition deficits are classified as primary or secondary. Primary recognition deficit, historically termed "morphognosia," reflects an inability to appreciate the physical features of an object. Secondary recognition deficit denotes preserved perception of shape, size, and texture, with impaired integration with stored knowledge, preventing object identification. Tactile agnosia specifically describes the inability to recognize objects through haptic exploration.[10]
Disorders of Tactile Object Recognition and Related Conditions
Several disorders can affect tactile object recognition (see Table. Tactile Object Recognition Disorders). Accurate diagnosis depends on a clear understanding of their definitions, neuroanatomical substrates, and key clinical distinctions. Correct use of these terms improves diagnostic precision and facilitates accurate neuroanatomical localization. Moreover, clear differentiation among these disorders also supports appropriate rehabilitation planning and prognostic counseling.
Table. Tactile Object Recognition Disorders
|
Term |
Definition |
Typical Neuroanatomical Substrate |
Key Clinical Notes |
|
Astereognosis (Somatosensory agnosia) |
Inability to recognize objects by touch with eyes closed, despite intact primary sensation |
Contralateral parietal lobe (primary somatosensory cortex areas 1 and 2, or association cortex areas 5 and 7) |
Umbrella term, often loosely applied |
|
Tactile Agnosia |
Higher-order disorder of tactile object recognition |
Parietal cortex |
Broader concept than astereognosis; includes apperceptive and associative subtypes |
|
Apperceptive Tactile Agnosia |
Failure to discriminate object features (shape, size, texture) |
Primary somatosensory cortex (areas 1 and 2) |
Perceptual stage deficit |
|
Associative Tactile Agnosia |
Features are perceived, but the object is not identified (failure to link to memory) |
Parietal association cortex (areas 5 and 7, superior parietal lobule) |
Memory-linking stage deficit |
|
Morphognosia |
Historical term for the inability to recognize the physical form of objects by touch |
Classically linked to primary somatosensory cortex lesions |
Essentially overlaps with apperceptive tactile agnosia |
|
Stereoanesthesia |
Old term for impaired stereognosis from subcortical or spinal lesions |
DCMLT, thalamus, brainstem |
“Pseudoastereognosis” from elementary sensory loss, not cortical dysfunction |
|
Pseudoastereognosis |
Apparent astereognosis due to impaired primary sensation |
DCMLT, thalamus, medial lemniscus |
Distinguished by abnormal elementary sensory tests |
|
Tactile Apraxia |
Inability to manipulate or use objects correctly when placed in the hand, despite recognizing them |
Dominant parietal cortex |
Recognition intact; purposeful use impaired (opposite of astereognosis) |
|
Neglect-Related Tactile Inattention |
Ignoring tactile stimuli on the contralateral side despite intact sensation |
Nondominant parietal lobe |
Due to attentional deficit, not sensory or perceptual failure |
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Astereognosis indicates a lesion of the contralateral parietal lobe (see Image. Parietal Meningioma Causing Contralateral Sensory Syndrome). Small postcentral lesions can produce isolated astereognosis. Large parietal lesions often cause astereognosis with contralateral sensory loss, whereas dense hemianesthesia is more typical of thalamic or subcortical lesions. Bilateral impairment of stereognosis has been reported after left parietal lesions, though hemispheric dominance remains uncertain and controversial.
Stroke and neoplasms are frequent causes. Astereognosis is associated with stroke severity.[11] Moreover, somatosensory impairment correlates with motor impairment.[12] Deficits in stereognosis have also been reported in children with cerebral palsy.[13] Astereognosis also occurs in association with conditions manifesting with cognitive impairment, eg, Alzheimer disease. Tactile agnosia has been reported as an onset symptom of corticobasal syndrome, a rare neurodegenerative disease. Parietal trauma, including depressed skull fracture, has been reported to cause astereognosis. Isolated astereognosis has also been documented after posttraumatic contusion of the postcentral gyrus.[14]
Other reported etiologies include ischemic infarction of the parietal lobe.[15] Arteriovenous malformations in the same region can also produce tactile agnosia. Furthermore, lesions of the anterior corpus callosum and thalamic radiations have rarely been implicated. Brainstem tumors involving the medial lemniscus may cause astereognosis, typically accompanied by additional sensory deficits.[16] Brainstem ischemic lesions affecting the medial lemniscus are also causative.[17] Extramedullary tumors at the foramen magnum have been reported to impair stereognosis through dorsal column involvement. Posterior column lesions in multiple sclerosis may similarly produce impaired stereognosis.[18]
Epidemiology
Analysis of lateralized vascular, neoplastic, and traumatic cerebral lesions has shown that parietal lobe strokes, particularly those involving the middle cerebral artery territory, can cause marked impairment of stereognosis.[19] Global stroke incidence is estimated at 100 to 300 per 100,000 person-years, with higher rates in low- and middle-income countries.[20] Although primary prevention has reduced stroke incidence in high-income countries, rates are rising in low- and middle-income regions. Stroke survivors frequently exhibit multiple neurological impairments.
The reported incidence of brain tumors has increased over recent decades, largely because of improved detection with neuroimaging and more comprehensive cancer registries, although the true incidence may be stable.[21] This increase is likely attributable to the wider availability of imaging modalities. Established risk factors for brain tumors include ionizing radiation, mutations of highly penetrant genes, hereditary syndromes, and immunosuppression.[22] Approximately 14% of gliomas occur in the parietal lobes.[23]
Head injuries are another important cause of astereognosis. The parietal bone is a common site of depressed skull fractures, which may produce parietal lobe injury and subsequent astereognosis.[24]
Pathophysiology
Octave Landry formulated the fundamental concepts of the physiology of sensation, namely proprioception and stereognosis.[25] Manual stereognosis requires the DCMLT to transmit discriminative touch and proprioceptive information, and the parietal lobe to process these inputs.
The movement of mechanoreceptors relative to one another enables the perception of the 3-dimensional structure of objects.[26] Four mechanoreceptor types contribute to stereognosis, as follows:
- Merkel cell receptors: Respond to slowly moving stimuli
- Ruffini corpuscles: Respond to skin stretch
- Meissner corpuscles: Respond to low-frequency vibrations
- Pacinian corpuscles: Respond to high-frequency vibrations
These receptors collectively convey information about an object's size, shape, texture, and motion. The spatial pattern of mechanoreceptor activation in response to applied forces, along with the relative receptive fields of each receptor, determines the resulting perception.
Sensory input from the forelimb ascends via the DCMLT to the cuneate nucleus in the medulla, then projects to the ventroposterior lateral nucleus of the thalamus. From the thalamus, projections reach the primary somatosensory cortex (Brodmann areas 3, 1, and 2) and then the posterior parietal association cortex and secondary somatosensory cortex (see Image. Brodmann Areas Overview). Functional magnetic resonance imaging (MRI) studies demonstrate that manual and oral stereognosis activate overlapping frontoparietal networks in a somatotopic pattern. The cortical area for oral stereognosis lies caudal to that for manual stereognosis, with overlap observed in the anterior intraparietal sulcus.
Astereognosis occurs as part of the cortical sensory syndrome secondary to a superior-posterior parietal stroke.[27] In Alzheimer disease, involvement of both the parietal cortex and the medial temporal lobe contributes to cognitive impairment and may underlie deficits in stereognosis.[28] Cortical sensory deficits, including astereognosis, are also observed in parietal gliomas, with occurrence determined by lesion size and location rather than hemispheric dominance.[29]
Stereognostic feedback in the oral cavity is mediated by mechanoreceptors, eg, Merkel discs and Ruffini endings, in the oral mucosa and the periodontal ligament. Oral stereognostic ability diminishes with age and edentulism. Disturbances of oral stereognosis may contribute to the development of malocclusions, and impaired oral stereognosis can lead to oral-phase swallowing difficulties in children.
Astereognosis most frequently results from lesions of the posterior parietal cortex, encompassing the primary somatosensory cortex (Brodmann areas 1, 2, 3a, 3b) and the somatosensory association cortex (Brodmann areas 5 and 7 of the superior parietal lobule). Classic lesion studies demonstrate that damage to areas 1 and 2 of the primary somatosensory cortex produces astereognosis, whereas lesions confined to area 3b typically spare stereognosis. Lesions of the superior parietal lobule disrupt spatial and integrative processing, leading to astereognosis. Apperceptive tactile agnosia arises from insults to areas 1 and 2 of the primary somatosensory cortex, whereas associative tactile agnosia results from injury to the parietal association cortex (areas 5 and 7). Pseudoastereognosis arises from lesions of the thalamus, brainstem, or DCMLT.
History and Physical
Cortical sensory testing is meaningful only when primary sensations are intact. Peripheral sensory modalities, including light touch, pressure, pain, temperature, and vibration, must be examined first to exclude peripheral neuropathy, radiculopathy, or spinal cord lesions.
Peripheral Sensory Examination
Before cortical sensory function is evaluated, primary sensations must be assessed and confirmed as intact. Light touch is tested using cotton wool, pressure by gently deforming the skin with the examiner’s index finger, and pinprick sensation with a sterile neurotip. Temperature sense is assessed with test tubes containing hot and cold water, and vibration sense is evaluated using a 128 Hz tuning fork. Cortical sensory testing, including stereognosis, should only be performed if these modalities are normal.
Tactile Object Recognition Test
The tactile object recognition test is a standard method for evaluating stereognosis. During this test, a series of familiar objects, eg, a pen, key, comb, or paperclip, is placed in the patient’s hand while the eyes are closed. The patient is then asked to identify each object by name or description. Failure to correctly identify an object in the presence of intact primary sensation is diagnostic of astereognosis.
The Stereognosis Component of the Nottingham Sensory Assessment
In the Nottingham Sensory Assessment, stereognosis is evaluated by placing common objects, eg, a coin, pencil, scissors, cup, glass, comb, or sponge in the patient’s hand. The patient is allowed up to approximately 30 seconds for tactile exploration before responding. Scoring is as follows:
- 2: Normal (correct identification)
- 1: Impaired (recognition of some features but not the whole object)
- 0: Absent (no recognition)
This method has demonstrated reliability in the assessment of poststroke sensory function.[30] Furthermore, the simplicity of this test permits bedside application without specialized equipment.
Deficits Characteristic of Parietal Lobe Dysfunction
Cortical sensory syndrome comprises loss of position sense, inability to localize noxious stimuli, astereognosis, agraphesthesia, and impaired 2-point discrimination. Involvement of the parietal lobe often produces these sensory deficits in association with contralateral hemiparesis, hemianopia, hemineglect, and impaired optokinetic nystagmus.
Dominant parietal lobe involvement may result in aphasia, ideomotor apraxia, and Gerstmann syndrome, which is characterized by agraphia without alexia, left-right confusion, digit agnosia, and acalculia.[31] Bilateral astereognosis has been reported in dominant parietal lobe lesions, although this finding is rare and remains controversial. Nondominant parietal lobe disease is associated with loss of topographic memory, anosognosia, and dressing apraxia.
Evaluation
Computed tomography (CT) and MRI are the principal modalities used to evaluate intracerebral pathology. CT is often the preferred modality for initial investigation in emergencies as this study is rapid, widely available, and has few contraindications. Additionally, CT is highly effective in detecting acute intracranial hemorrhage.
However, MRI is increasingly used in the evaluation of acute stroke.[32] Diffusion-weighted imaging is more sensitive than CT for identifying acute ischemic stroke, though CT remains superior for hyperacute hemorrhage detection. CT is frequently the initial study used for brain tumor detection.[33] This modality can demonstrate calcification, hemorrhage, herniation, mass effect, and hydrocephalus. MRI provides superior tissue characterization and anatomic detail. Contrast-enhanced T1-weighted images reveal tumor vascularity and necrosis, while magnetic resonance spectroscopy provides a metabolic profile.
Functional MRI measures brain activity through blood oxygen level–dependent (BOLD) signal changes. This modality is valuable for preoperative mapping to define tumor relationships with eloquent cortical areas, though its availability and utility depend on institutional resources.[34] Functional MRI studies have also been used to investigate the neural basis of manual and oral stereognosis.
Resting-state functional MRI studies of the somatosensory network after stroke have demonstrated strong associations between interhemispheric network connectivity indices and stereognosis.[35] Greater functional network connectivity correlates with better somatosensory performance. Functional MRI has also been applied to examine the primary and secondary somatosensory cortices in patients with congenital hemiplegia.[36] Diffusion tensor imaging enables assessment of DCMLT integrity in children with hemiparesis.[37]
Somatosensory evoked potentials provide electrophysiologic evidence of the correlation between sensory impairments, eg, astereognosis and hemianesthesia, and parietal lesions identified on imaging. Somatosensory evoked potentials serve as an adjunct for localizing or characterizing lesions but lack diagnostic specificity when used in isolation.
Treatment / Management
Management of astereognosis focuses on addressing the underlying etiology. Treatment of acute ischemic stroke involves intravenous thrombolysis within the therapeutic window, mechanical thrombectomy for large-vessel occlusion, blood pressure optimization, antiplatelet therapy, and statin administration.[38] Management of brain neoplasms may include surgery, radiotherapy, or chemotherapy, depending on tumor location, histology, and patient factors.[39]
Cognitive rehabilitation therapy has demonstrated benefit in stroke and traumatic brain injury, although evidence for its efficacy in brain tumors and dementia is limited.[40][41] Sensory training enhances somatosensory discrimination after stroke.[42] Active sensory training consists of manual exploration and discrimination of textures, figures, shapes, weights, and objects, including tactile object recognition tasks.[43] The Study of the Effectiveness of Neurorehabilitation on Sensation (SENSe) randomized controlled trial showed that sensory discrimination training improves functional outcomes in patients with impaired tactile object recognition after stroke.[44](A1)
Dentures may partially restore oral stereognostic ability in edentulous patients. Thus, denture use may be considered a rehabilitative intervention in selected cases.
Differential Diagnosis
Three principal syndromes are recognized in the differential diagnosis of hemisensory disturbances resulting from parietal lesions. Cortical sensory syndrome encompasses astereognosis, agraphesthesia, and loss of position sense, most commonly arising from lesions of the contralateral superior parietal lobule (Brodmann areas 5 and 7), although lesions of the postcentral gyrus (Brodmann areas 1 and 2) may also contribute. Pseudothalamic sensory syndrome manifests as faciobrachiocrural impairment resembling thalamic sensory loss and typically results from lesions of the inferior parietal lobule, including the angular and supramarginal gyri. Atypical sensory syndromes involve partial, nonclassical deficits across multiple modalities and are caused by parietal lesions of varied topography.
Astereognosis is defined as the inability to recognize objects by touch. Failure to discriminate object shape and size constitutes apperceptive tactile agnosia, whereas inability to associate intact tactile perception with stored knowledge constitutes associative tactile agnosia. Discriminative deficits are most frequently observed with lesions of the primary somatosensory cortex and its connections. Damage to the parietal somatosensory association areas also produces tactile agnosia.
Tumors at the craniovertebral junction may cause astereognosis if they compress the DCMLT.[45] Hand muscle amyotrophy may be observed in such cases. Impairment of stereognosis resulting from spinal cord or brainstem injuries has historically been termed “stereoanesthesia,” although this term is now uncommon.[46] Deficits in ipsilateral vibration and joint position sense are typically associated with these lesions.
Prognosis
Astereognosis is a common somatosensory impairment following stroke involving the parietal lobe. Recovery of stereognosis may occur over days to months, depending on lesion location, size, and intensity of rehabilitation, although some patients experience persistent deficits.[47] Larger parietal gliomas are frequently associated with neurological deficits. Sensory function in patients with parietal gliomas may improve following tumor resection if cortical integrity is preserved, whereas damage to critical sensory cortex can result in further deterioration. In traumatic brain injury, rehabilitation programs incorporating sensory reeducation may enhance functional outcomes, although evidence is more robust for stroke than for chronic traumatic brain injury.[48]
Complications
Somatosensory loss negatively affects functional outcomes. Discriminative sensory impairment of the upper limb occurs in approximately one-third to one-half of stroke patients during rehabilitation, with prevalence varying by study population and assessment method. Such sensory deficits impede upper limb use in daily activities and frequently result in clumsiness that cannot be explained solely by motor deficits or spasticity.[49]
Astereognosis has been reported in Alzheimer disease as a manifestation of parietal cortical dysfunction, although this is not a consistent diagnostic feature. High cervical lesions from multiple sclerosis or cervical spondylosis may produce astereognosis, often contributing to “useless hand syndrome,” characterized by numb, clumsy hands due to loss of proprioceptive and discriminative sensation.[50][51] Parietal lobe disease may produce both impaired stereognosis and tactile apraxia. These conditions can coexist. However, tactile apraxia represents a higher-order disorder of praxis rather than a simple loss of stereognosis.[52]
Deterrence and Patient Education
Patients participate in sensory reeducation using graded tactile stimuli to promote cortical plasticity and functional reorganization of sensory processing. Sensory relearning involves tactile exploration of surfaces, discrimination of shapes, textures, weights, and temperatures, and tactile object recognition. Exercises are performed repeatedly, with difficulty progressively increased. Feedback is commonly provided through visual cues or comparison with the unaffected hand, facilitating multisensory reinforcement and intermanual transfer. Individualized home exercise programs are also recommended to consolidate gains.
Enhancing Healthcare Team Outcomes
Astereognosis, or somatosensory agnosia, is the inability to recognize objects through touch despite intact primary sensation. It reflects disruption of cortical sensory processing, most often from parietal lobe injury, thalamic injury, or injury to the dorsal column–medial lemniscus pathway. Accurate differentiation from peripheral sensory loss requires structured cortical sensory testing, including tactile object recognition tasks. Common etiologies include stroke, trauma, neoplasms, and neurodegenerative disease, and evidence-based management emphasizes treating the underlying condition while incorporating targeted sensory discrimination training to improve functional recovery.
Clinicians across disciplines play essential roles in optimizing patient-centered care for individuals with astereognosis. Physicians and advanced practitioners must integrate neuroanatomical knowledge, diagnostic strategies, and imaging interpretation to establish accurate diagnoses and guide treatment plans. Nurses contribute through ongoing sensory assessment, safety monitoring, and reinforcing rehabilitation tasks. Pharmacists support safe pharmacologic management in stroke, tumor, or neurodegenerative etiologies. Therapists apply structured sensory retraining and cognitive rehabilitation methods. Effective interprofessional communication and coordinated care ensure early recognition, consistent assessment strategies, and aligned rehabilitation goals, ultimately improving outcomes, patient safety, and overall team performance.
Media
(Click Image to Enlarge)
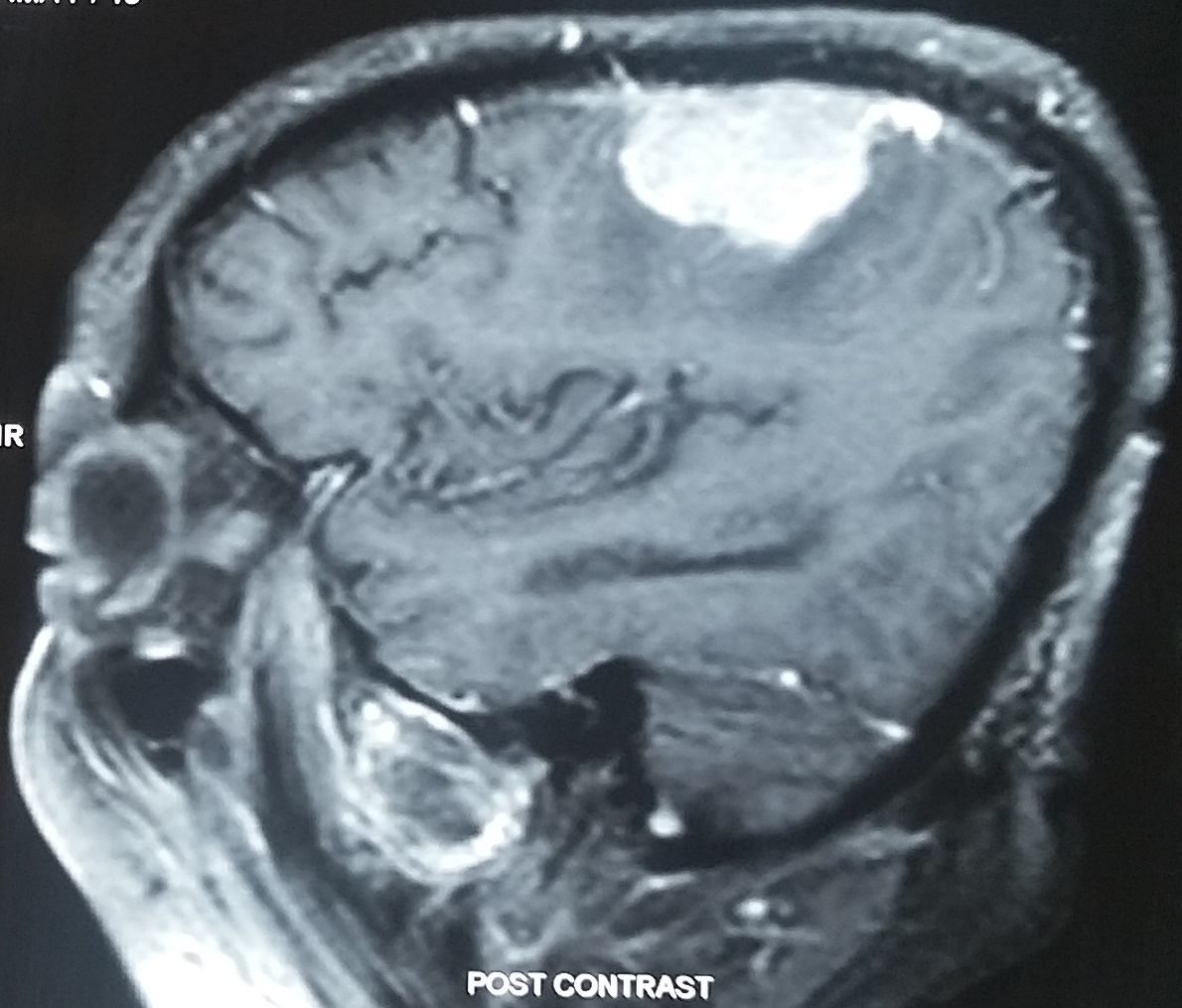
Parietal Meningioma Causing Contralateral Sensory Syndrome. Sagittal postcontrast magnetic resonance imaging demonstrates a well-circumscribed, strongly enhancing extra-axial mass in the parietal region consistent with a meningioma. The lesion’s location corresponds to the primary somatosensory cortex and is associated clinically with sensory deficits on the contralateral body side. This image illustrates the typical radiological appearance and clinical correlation of parietal meningiomas causing sensory syndrome.
Contributed by AKA Unnithan, MD
(Click Image to Enlarge)
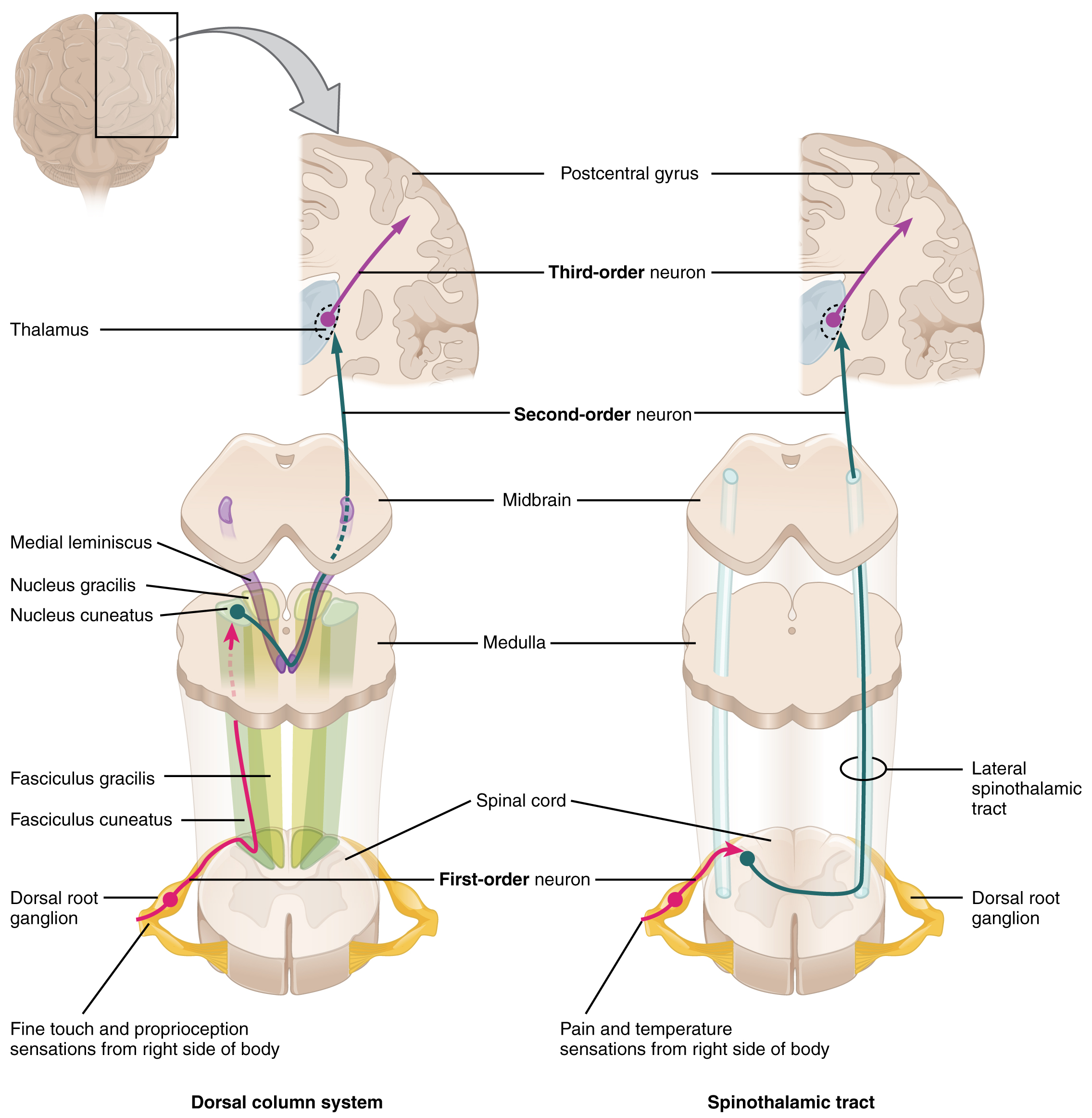
Ascending Sensory Pathways. The diagram compares the anatomical trajectories of the dorsal column system and the spinothalamic tract. Both pathways utilize a 3-neuron chain to transmit peripheral stimuli to the postcentral gyrus. The dorsal column system facilitates fine touch and proprioception, with decussation occurring in the medulla via the medial lemniscus. In contrast, the spinothalamic tract mediates pain and temperature sensations, with 1st-order neurons synapsing and decussating immediately within the spinal cord.
OpenStax College, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
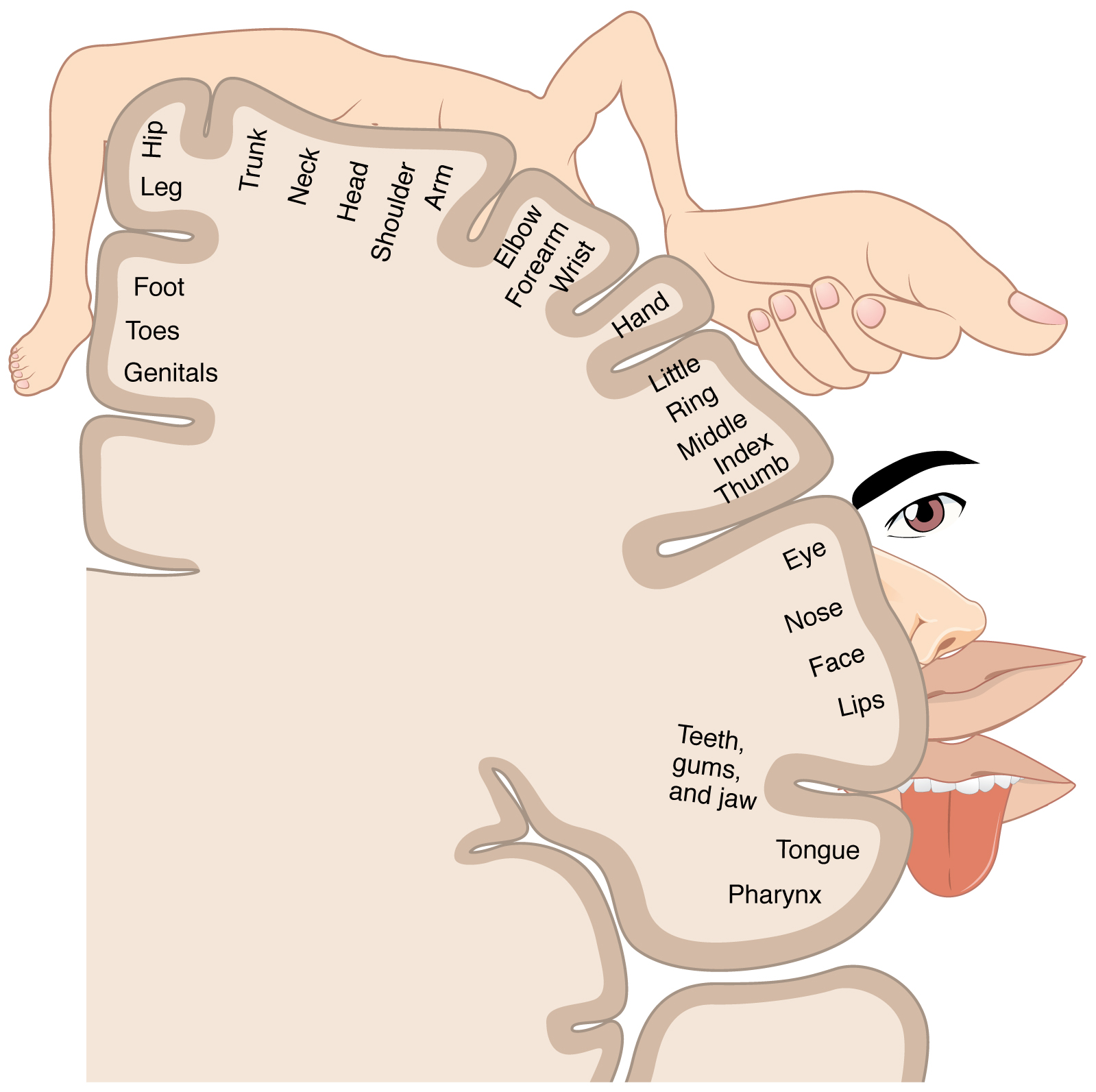
Somatosensory Homunculus Representation. The image illustrates the cortical mapping of body regions on the primary somatosensory cortex, with exaggerated anatomical features proportional to sensory innervation density. Each part of the cortex is labeled according to the corresponding body region, demonstrating differential sensory representation.
OpenStax, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
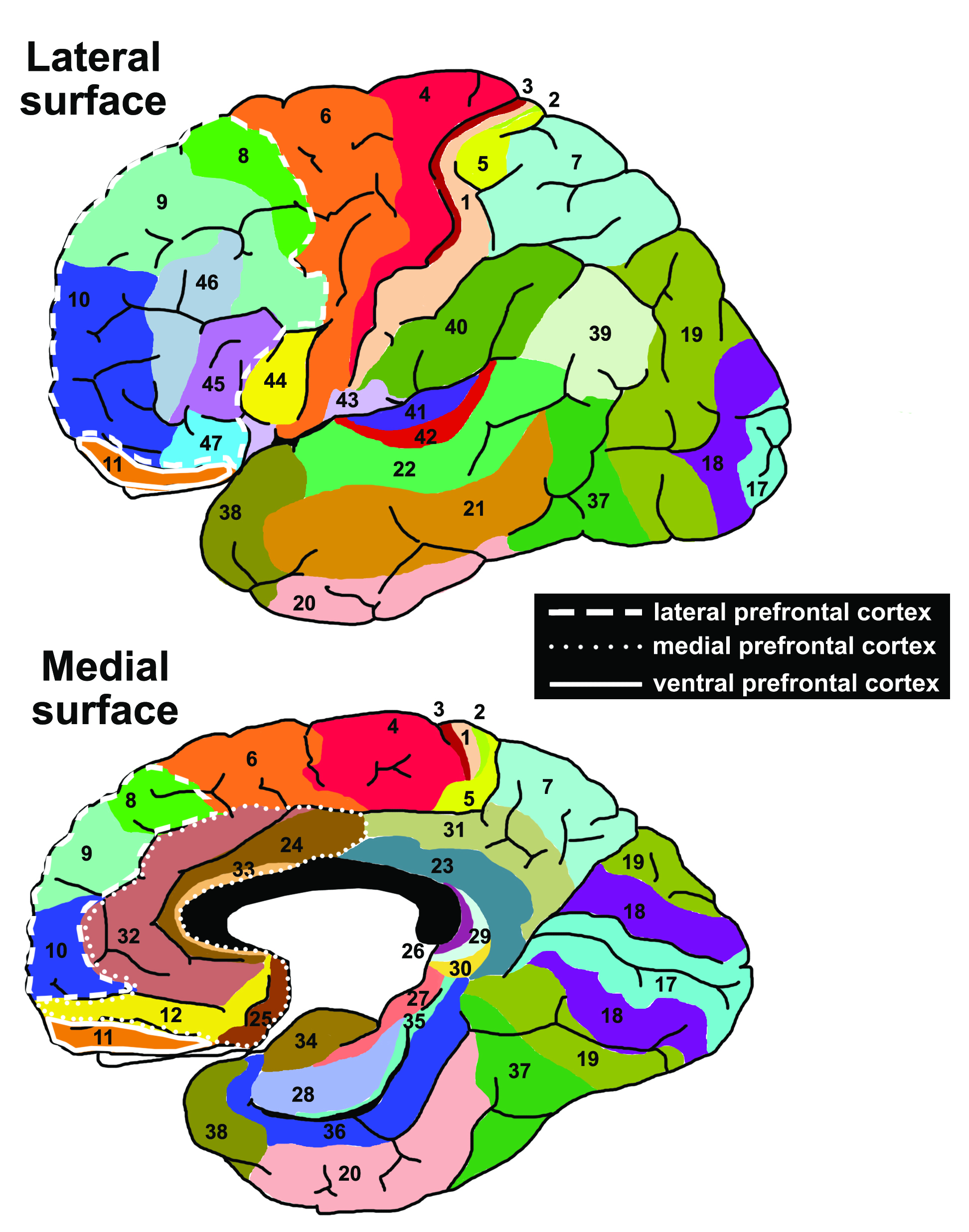
Brodmann Areas Overview. This illustration labels key cortical areas with their main functions. Areas 1 to 3 form the primary somatosensory cortex; area 4, the primary motor cortex. Areas 5 and 7 coordinate visuo-motor integration. Areas 6 and 8 include premotor regions and frontal eye fields. Areas 9 to 12 encompass the prefrontal and orbitofrontal cortices for executive function and decision-making. Areas 17 to 19 constitute the visual cortex; areas 41 to 42, the auditory cortex. Areas 44 to 45 form the Broca speech area; areas 39 to 40, the angular and supramarginal gyri, mediate language and spatial processing. This cytoarchitectural map underpins functional cortical localization.
Vysha, Public Domain, via Wikimedia Commons
{kind=link}
References
Schermann T, Tadi P. Stereognosis. StatPearls. 2025 Jan:(): [PubMed PMID: 32310463]
Jacobs R, Bou Serhal C, van Steenberghe D. Oral stereognosis: a review of the literature. Clinical oral investigations. 1998 Mar:2(1):3-10 [PubMed PMID: 9667147]
Mary KM, Cherian B. Evaluation of oral stereognosis, masticatory efficiency, and salivary flow rate in complete denture wearers. Journal of Indian Prosthodontic Society. 2020 Jul-Sep:20(3):290-296. doi: 10.4103/jips.jips_453_19. Epub 2020 Jul 17 [PubMed PMID: 33223699]
Janardhanan R, Soman A, George S, Sukumaran A, John SA. Evaluation of the Association of Oral Stereognosis with Malocclusion in Children. International journal of clinical pediatric dentistry. 2021:14(Suppl 1):S18-S21. doi: 10.5005/jp-journals-10005-2050. Epub [PubMed PMID: 35082461]
Schumann-Werner B, Schaefer S, Schramm S, Patel HJ, Binkofski FC, Werner CJ. Neural Correlates of Oral Stereognosis-An fMRI Study. Dysphagia. 2023 Jun:38(3):923-932. doi: 10.1007/s00455-022-10517-2. Epub 2022 Sep 10 [PubMed PMID: 36087119]
Sakthi Devi A, Akshayalingam M, Chandran P. Evaluation of Correlation between Oral Stereognosis Ability and Satisfaction in Complete Denture Patients. Indian journal of dental research : official publication of Indian Society for Dental Research. 2025 Jan 1:36(1):60-63. doi: 10.4103/ijdr.ijdr_360_23. Epub 2025 May 28 [PubMed PMID: 40439209]
Roland PE. Astereognosis. Tactile discrimination after localized hemispheric lesions in man. Archives of neurology. 1976 Aug:33(8):543-50 [PubMed PMID: 942311]
Mauguière F, Desmedt JE, Courjon J. Astereognosis and dissociated loss of frontal or parietal components of somatosensory evoked potentials in hemispheric lesions. Detailed correlations with clinical signs and computerized tomographic scanning. Brain : a journal of neurology. 1983 Jun:106 (Pt 2)():271-311 [PubMed PMID: 6850271]
Level 3 (low-level) evidenceDavis AS, Mazur-Mosiewicz A, Dean RS. The presence and predictive value of astereognosis and agraphesthesia in patients with Alzheimer's disease. Applied neuropsychology. 2010 Oct:17(4):262-6. doi: 10.1080/09084282.2010.525102. Epub [PubMed PMID: 21154039]
Facci L, Basilico S, Sellitto M, Gelosa G, Gandola M, Bottini G. Unilateral tactile agnosia as an onset symptom of corticobasal syndrome. Frontiers in human neuroscience. 2024:18():1401578. doi: 10.3389/fnhum.2024.1401578. Epub 2024 Jul 25 [PubMed PMID: 39118817]
Connell LA, Lincoln NB, Radford KA. Somatosensory impairment after stroke: frequency of different deficits and their recovery. Clinical rehabilitation. 2008 Aug:22(8):758-67. doi: 10.1177/0269215508090674. Epub [PubMed PMID: 18678576]
Meyer S, De Bruyn N, Krumlinde-Sundholm L, Peeters A, Feys H, Thijs V, Verheyden G. Associations Between Sensorimotor Impairments in the Upper Limb at 1 Week and 6 Months After Stroke. Journal of neurologic physical therapy : JNPT. 2016 Jul:40(3):186-95. doi: 10.1097/NPT.0000000000000138. Epub [PubMed PMID: 27214520]
Van Heest AE, House J, Putnam M. Sensibility deficiencies in the hands of children with spastic hemiplegia. The Journal of hand surgery. 1993 Mar:18(2):278-81 [PubMed PMID: 8463594]
Khormi YH, Atteya MME. Isolated post-traumatic astereognosis: a case-based review. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2022 Jan:38(1):17-24. doi: 10.1007/s00381-021-05392-5. Epub 2021 Oct 25 [PubMed PMID: 34694463]
Level 3 (low-level) evidenceHömke L, Amunts K, Bönig L, Fretz C, Binkofski F, Zilles K, Weder B. Analysis of lesions in patients with unilateral tactile agnosia using cytoarchitectonic probabilistic maps. Human brain mapping. 2009 May:30(5):1444-56. doi: 10.1002/hbm.20617. Epub [PubMed PMID: 18636551]
Level 3 (low-level) evidenceFeinsod M, Bentin S, Moscovitch M, Wald U. Brainstem tumor presenting with unilateral astereognosis. Annals of neurology. 1980 Aug:8(2):191-2 [PubMed PMID: 7425573]
Level 3 (low-level) evidenceEndtz LJ, Frenay JJ. Studies on asterognosis and amyotrophy of the hand in brainstem syndromes. Relation to the symptomatology of tumours at the spinocranial junction. Journal of the neurological sciences. 1980 Jan:44(2-3):241-6 [PubMed PMID: 7354369]
Kamogawa K, Okuda B. Useless hand syndrome with astereognosis in multiple sclerosis. Multiple sclerosis and related disorders. 2015 Jan:4(1):85-7. doi: 10.1016/j.msard.2014.09.212. Epub 2014 Oct 7 [PubMed PMID: 25787059]
Level 3 (low-level) evidenceHom J, Reitan RM. Effect of lateralized cerebral damage upon contralateral and ipsilateral sensorimotor performances. Journal of clinical neuropsychology. 1982 Sep:4(3):249-68 [PubMed PMID: 7142422]
Béjot Y, Daubail B, Giroud M. Epidemiology of stroke and transient ischemic attacks: Current knowledge and perspectives. Revue neurologique. 2016 Jan:172(1):59-68. doi: 10.1016/j.neurol.2015.07.013. Epub 2015 Dec 21 [PubMed PMID: 26718592]
Level 3 (low-level) evidenceFisher JL, Schwartzbaum JA, Wrensch M, Wiemels JL. Epidemiology of brain tumors. Neurologic clinics. 2007 Nov:25(4):867-90, vii [PubMed PMID: 17964019]
Wrensch M, Minn Y, Chew T, Bondy M, Berger MS. Epidemiology of primary brain tumors: current concepts and review of the literature. Neuro-oncology. 2002 Oct:4(4):278-99. doi: 10.1093/neuonc/4.4.278. Epub [PubMed PMID: 12356358]
Larjavaara S, Mäntylä R, Salminen T, Haapasalo H, Raitanen J, Jääskeläinen J, Auvinen A. Incidence of gliomas by anatomic location. Neuro-oncology. 2007 Jul:9(3):319-25 [PubMed PMID: 17522333]
Satardey RS, Balasubramaniam S, Pandya JS, Mahey RC. Analysis of Factors Influencing Outcome of Depressed Fracture of Skull. Asian journal of neurosurgery. 2018 Apr-Jun:13(2):341-347. doi: 10.4103/ajns.AJNS_117_16. Epub [PubMed PMID: 29682032]
Walusinski O. Pioneering the concepts of stereognosis and polyradiculoneuritis: Octave Landry (1826-1865). European neurology. 2013:70(5-6):281-90. doi: 10.1159/000353167. Epub 2013 Sep 17 [PubMed PMID: 24051983]
Yau JM, Kim SS, Thakur PH, Bensmaia SJ. Feeling form: the neural basis of haptic shape perception. Journal of neurophysiology. 2016 Feb 1:115(2):631-42. doi: 10.1152/jn.00598.2015. Epub 2015 Nov 18 [PubMed PMID: 26581869]
Bassetti C, Bogousslavsky J, Regli F. Sensory syndromes in parietal stroke. Neurology. 1993 Oct:43(10):1942-9 [PubMed PMID: 8413950]
Jacobs HI, Van Boxtel MP, Jolles J, Verhey FR, Uylings HB. Parietal cortex matters in Alzheimer's disease: an overview of structural, functional and metabolic findings. Neuroscience and biobehavioral reviews. 2012 Jan:36(1):297-309. doi: 10.1016/j.neubiorev.2011.06.009. Epub 2011 Jun 30 [PubMed PMID: 21741401]
Level 2 (mid-level) evidenceRussell SM, Elliott R, Forshaw D, Kelly PJ, Golfinos JG. Resection of parietal lobe gliomas: incidence and evolution of neurological deficits in 28 consecutive patients correlated to the location and morphological characteristics of the tumor. Journal of neurosurgery. 2005 Dec:103(6):1010-7 [PubMed PMID: 16381187]
Level 3 (low-level) evidenceGaubert CS, Mockett SP. Inter-rater reliability of the Nottingham method of stereognosis assessment. Clinical rehabilitation. 2000 Apr:14(2):153-9 [PubMed PMID: 10763792]
Altabakhi IW, Liang JW. Gerstmann Syndrome. StatPearls. 2025 Jan:(): [PubMed PMID: 30137813]
Chalela JA, Kidwell CS, Nentwich LM, Luby M, Butman JA, Demchuk AM, Hill MD, Patronas N, Latour L, Warach S. Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: a prospective comparison. Lancet (London, England). 2007 Jan 27:369(9558):293-8 [PubMed PMID: 17258669]
Mabray MC, Barajas RF Jr, Cha S. Modern brain tumor imaging. Brain tumor research and treatment. 2015 Apr:3(1):8-23. doi: 10.14791/btrt.2015.3.1.8. Epub 2015 Apr 29 [PubMed PMID: 25977902]
Vlieger EJ, Majoie CB, Leenstra S, Den Heeten GJ. Functional magnetic resonance imaging for neurosurgical planning in neurooncology. European radiology. 2004 Jul:14(7):1143-53 [PubMed PMID: 15148622]
De Bruyn N, Meyer S, Kessner SS, Essers B, Cheng B, Thomalla G, Peeters A, Sunaert S, Duprez T, Thijs V, Feys H, Alaerts K, Verheyden G. Functional network connectivity is altered in patients with upper limb somatosensory impairments in the acute phase post stroke: A cross-sectional study. PloS one. 2018:13(10):e0205693. doi: 10.1371/journal.pone.0205693. Epub 2018 Oct 12 [PubMed PMID: 30312350]
Level 2 (mid-level) evidenceFiori S, Biagi L, Cecchi P, Cioni G, Beani E, Tosetti M, Cosottini M, Guzzetta A. Potentials of Ultrahigh-Field MRI for the Study of Somatosensory Reorganization in Congenital Hemiplegia. Neural plasticity. 2018:2018():8472807. doi: 10.1155/2018/8472807. Epub 2018 Nov 25 [PubMed PMID: 30595689]
Kuczynski AM, Carlson HL, Lebel C, Hodge JA, Dukelow SP, Semrau JA, Kirton A. Sensory tractography and robot-quantified proprioception in hemiparetic children with perinatal stroke. Human brain mapping. 2017 May:38(5):2424-2440. doi: 10.1002/hbm.23530. Epub 2017 Feb 8 [PubMed PMID: 28176425]
Lui F, Khan Suheb MZ, Patti L. Ischemic Stroke. StatPearls. 2025 Jan:(): [PubMed PMID: 29763173]
Perkins A, Liu G. Primary Brain Tumors in Adults: Diagnosis and Treatment. American family physician. 2016 Feb 1:93(3):211-7 [PubMed PMID: 26926614]
Laatsch L, Dodd J, Brown T, Ciccia A, Connor F, Davis K, Doherty M, Linden M, Locascio G, Lundine J, Murphy S, Nagele D, Niemeier J, Politis A, Rode C, Slomine B, Smetana R, Yaeger L. Evidence-based systematic review of cognitive rehabilitation, emotional, and family treatment studies for children with acquired brain injury literature: From 2006 to 2017. Neuropsychological rehabilitation. 2020 Jan:30(1):130-161. doi: 10.1080/09602011.2019.1678490. Epub 2019 Oct 31 [PubMed PMID: 31671014]
Level 1 (high-level) evidenceCicerone KD, Dahlberg C, Kalmar K, Langenbahn DM, Malec JF, Bergquist TF, Felicetti T, Giacino JT, Harley JP, Harrington DE, Herzog J, Kneipp S, Laatsch L, Morse PA. Evidence-based cognitive rehabilitation: recommendations for clinical practice. Archives of physical medicine and rehabilitation. 2000 Dec:81(12):1596-615 [PubMed PMID: 11128897]
Byl N, Roderick J, Mohamed O, Hanny M, Kotler J, Smith A, Tang M, Abrams G. Effectiveness of sensory and motor rehabilitation of the upper limb following the principles of neuroplasticity: patients stable poststroke. Neurorehabilitation and neural repair. 2003 Sep:17(3):176-91 [PubMed PMID: 14503438]
Level 1 (high-level) evidenceCarlsson H, Rosén B, Pessah-Rasmussen H, Björkman A, Brogårdh C. SENSory re-learning of the UPPer limb after stroke (SENSUPP): study protocol for a pilot randomized controlled trial. Trials. 2018 Apr 17:19(1):229. doi: 10.1186/s13063-018-2628-1. Epub 2018 Apr 17 [PubMed PMID: 29665842]
Level 3 (low-level) evidenceCarey L, Macdonell R, Matyas TA. SENSe: Study of the Effectiveness of Neurorehabilitation on Sensation: a randomized controlled trial. Neurorehabilitation and neural repair. 2011 May:25(4):304-13. doi: 10.1177/1545968310397705. Epub 2011 Feb 24 [PubMed PMID: 21350049]
Level 1 (high-level) evidenceFrenay JJ, Groen JJ, Endtz LJ. Tumours at the spinocranial junction: some clinical and electromyographic aspects in relation to the symptomatology. Clinical neurology and neurosurgery. 1979:81(1):13-25 [PubMed PMID: 223793]
Level 3 (low-level) evidenceKararizou E, Lykomanos D, Kosma A, Kokotis P, Giatas K, Markou I, Vassilopoulos D. Stereoanesthesia or astereognosia? Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology. 2009 Oct:30(5):409-11. doi: 10.1007/s10072-009-0117-8. Epub 2009 Jul 8 [PubMed PMID: 19585078]
Level 3 (low-level) evidenceLee KB, Lim SH, Kim KH, Kim KJ, Kim YR, Chang WN, Yeom JW, Kim YD, Hwang BY. Six-month functional recovery of stroke patients: a multi-time-point study. International journal of rehabilitation research. Internationale Zeitschrift fur Rehabilitationsforschung. Revue internationale de recherches de readaptation. 2015 Jun:38(2):173-80. doi: 10.1097/MRR.0000000000000108. Epub [PubMed PMID: 25603539]
Gupta A, Taly AB. Functional outcome following rehabilitation in chronic severe traumatic brain injury patients: A prospective study. Annals of Indian Academy of Neurology. 2012 Apr:15(2):120-4. doi: 10.4103/0972-2327.94995. Epub [PubMed PMID: 22566725]
Kim JS, Choi-Kwon S. Discriminative sensory dysfunction after unilateral stroke. Stroke. 1996 Apr:27(4):677-82 [PubMed PMID: 8614929]
Hamada E, Okamoto K, Okuda B. [A case of multiple sclerosis with bilateral useless hand syndrome as a main clinical feature]. Rinsho shinkeigaku = Clinical neurology. 2005 Mar:45(3):211-5 [PubMed PMID: 15835290]
Level 3 (low-level) evidenceGood DC, Couch JR, Wacaser L. "Numb, clumsy hands" and high cervical spondylosis. Surgical neurology. 1984 Sep:22(3):285-91 [PubMed PMID: 6463840]
Level 3 (low-level) evidenceBinkofski F, Kunesch E, Classen J, Seitz RJ, Freund HJ. Tactile apraxia: unimodal apractic disorder of tactile object exploration associated with parietal lobe lesions. Brain : a journal of neurology. 2001 Jan:124(Pt 1):132-44 [PubMed PMID: 11133793]
Level 1 (high-level) evidence