Introduction
Ascariasis is a soil-transmitted helminth and remains a global health concern. The estimated global prevalence of human ascariasis in 2021 was between 682 and 782 million people infected worldwide.[1] Ascariasis disproportionately affects children aged 5 to 15 years and occurs mostly in tropical and subtropical countries worldwide, where sanitation is poor, and humidity and temperatures are high. This infection is frequently documented in sub-Saharan Africa, Latin America, the Caribbean, China, and East Asia.[1] Based on Global Burden of Disease Collaborative Network estimates, ascariasis remains one of the most consequential neglected tropical diseases worldwide, accounting for approximately 648,000 disability-adjusted life years (DALYs) annually.[2][3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Ascariasis is caused by Ascaris lumbricoides, a large soil-transmitted nematode acquired through ingestion of embryonated eggs from contaminated soil, food, or water.[4][5][6] Adult female worms are larger and more robust, typically measuring 20 to 30 cm in length, whereas males are smaller (15–20 cm) and have a slender body and a ventrally curved posterior end bearing retractile copulatory spicules.[4][5] The worms are smooth and cylindrical and may appear white, yellow, or pink.
Adult females have a thicker body with a straight posterior end. The average lifespan of an adult Ascaris worm is approximately 1 year, after which the parasite dies and is expelled via the gastrointestinal tract. Because adult worms do not multiply in humans, ascariasis may resolve spontaneously in the absence of reinfection, although ongoing exposure in endemic settings frequently leads to repeated infections.[7][8][4]
Epidemiology
Ascariasis is among the most common human helminth infections worldwide and has been recognized for millennia, described in ancient medical writings, and identified in archaeological remains. However, ascariasis remains a major public health problem in many low-resource settings.[5][6] The most recent systematic review and meta-analysis estimated that the global prevalence was 11.01% (95% CI; 10.27%–11.78%), corresponding to an estimated 732 million (682–782 million) people infected in 2021, with higher prevalence in children and in rural or low-income settings, and associations with environmental conditions favorable for egg survival.[1]
This aligns with the Centers for Disease Control and Prevention (CDC) current summary estimate that approximately 772 to 892 million people are infected globally, with the greatest burden in tropical and subtropical regions of Asia, sub-Saharan Africa, and the Americas.[CDC. About Ascariasis. 2024] Ascariasis transmission is tightly associated with poverty and inadequate sanitation because eggs passed in human feces contaminate soil, food, and water; risk is amplified where hygiene infrastructure is limited and where fecal contamination of the environment occurs, including some agricultural practices, eg, the use of human feces as fertilizer.[5][6][9][10] [WHO. Soil-Transmitted Helminth Infections. 2023].
Although infection is concentrated in endemic regions, travel and migration can lead to cases in nonendemic areas, maintaining clinical relevance for clinicians caring for mobile populations and returning travelers.[11] [CDC Yellow Book. Post-Travel Parasitic Disease Including Evaluation of Eosinophilia. 2025] Recent molecular epidemiology research has shown that Ascaris transmission may be highly focal even within endemic communities: a whole-genome sequencing study from Ethiopia revealed that parasite populations often cluster at the household level, with reinfections commonly occurring among close contacts.[12] These findings, along with early genomic signals suggestive of drug selection pressure, underscore the importance of targeted interventions and genomic surveillance in identifying transmission hotspots and monitoring for potential emergence of anthelmintic resistance.[13][11][12]
Pathophysiology
Infection occurs when a human host ingests embryonated Ascaris eggs present in stool-contaminated soil, food, or water.[8][9][11] After ingestion, eggs hatch in the duodenum, releasing larvae that penetrate the intestinal mucosa and enter the circulation via venous, arterial, or lymphatic vessels. The larvae migrate through the portal system to the liver and subsequently reach the lungs within approximately 7 to 10 days.
In the pulmonary phase, larvae penetrate the alveolar membranes and mature within the alveoli, causing transient inflammatory injury. They then ascend the bronchial tree, are expectorated, and swallowed, thereby reentering the gastrointestinal tract. Once back in the lumen of the small intestine, larvae mature into adult worms over 2 to 3 weeks.[8][9] When both male and female worms are present, copulation occurs, and an adult female can produce up to 200,000 eggs per day, which are excreted in feces.[8][9][11][14] Under favorable environmental conditions consisting of warm, moist, and shaded soil, eggs embryonate and become infective within 2 to 8 weeks and may remain viable for prolonged periods, with reports of survival ranging from months to several years (up to a decade or more), facilitating sustained transmission and reinfection in endemic areas.[8][9][15][16][4][5][17]
Histopathology
A fertilized Ascaris egg can be visualized with microscopy of a stool sample (see Image. Ascaris Ova).
History and Physical
Most individuals infected with ascariasis are asymptomatic or experience mild, nonspecific symptoms, with clinical manifestations largely determined by parasite burden and related complications.[14] Low-intensity infections may remain clinically silent and present only with long-term sequelae, eg, growth retardation and malnutrition, particularly in children. When symptoms occur, the most common gastrointestinal manifestations include abdominal pain, bloating, nausea, vomiting, anorexia, and intermittent diarrhea. During the larval migratory phase, a heavy pulmonary larval burden may result in transient eosinophilic pneumonitis (Löffler syndrome), characterized by cough, wheezing, dyspnea, fever, hemoptysis, and peripheral eosinophilia.
Severe complications are primarily related to adult worm migration, especially in the setting of high parasite loads or superinfection. Adult worms may migrate into tubular structures, eg, the biliary and pancreatic ducts, leading to biliary colic, cholecystitis, cholangitis, pancreatitis, as well as small-bowel obstruction, volvulus, appendicitis, and intussusception. Children are disproportionately affected by both morbidity and complications due to higher infection intensity and nutritional vulnerability, and may present with growth failure, malnutrition, abdominal pain, diarrhea, and nausea, making ascariasis an important contributor to pediatric disease burden in endemic regions.[4][5][18][19]
Evaluation
Adult female Ascaris lumbricoides worms can produce up to 200,000 eggs per day, facilitating detection through stool-based diagnostics.[4][5][6] The cornerstone of diagnosis remains direct microscopic examination of stool samples for ova and parasites.[5][20] This typically involves examining 2 slides per sample to identify the characteristic large, oval, brown, trilayered eggs with a mammillated outer coat (see Image. Ascaris Ova). In endemic areas, the World Health Organization (WHO) recommends the Kato–Katz thick smear technique for both diagnosis and quantification of infection intensity at the population level.[5] However, this method has notable limitations, particularly in low-intensity infections.
A field study in Kenya demonstrated that Kato–Katz microscopy detected only 54% to 64% of Ascaris infections, missing many mild or prepatent cases. In contrast, a multiplex real-time PCR (qPCR) assay exhibited significantly higher sensitivity and served as the reference standard. Additionally, serologic testing showed that IgG1 antibodies against adult worm excretory-secretory antigens were highly specific and sensitive for active infection (AUC ≈0.83), making them a promising adjunct for surveillance in endemic areas. These findings suggest that combining qPCR for sensitive detection with IgG1 serology to assess exposure status can improve diagnostic accuracy, particularly when microscopy underestimates true prevalence.
Stool examinations may also yield false negatives during the early migratory and maturation phase—approximately the first 3 to 4 weeks post-infection—when egg excretion has not yet begun. In such cases, clinical clues become important: eosinophilia may be observed during the larval migratory phase, and larvae may be recovered in sputum during pulmonary involvement. Occasionally, adult worms may be directly visualized when passed in stool, expelled rectally, or expectorated, and rare reports describe worms expelled in urine due to aberrant migration. Imaging modalities further aid diagnosis in complicated presentations: abdominal radiographs may reveal nonspecific signs, eg, the “whirlpool” or “railway track” pattern; ultrasound and computed tomography (CT) imaging can detect adult worms in the hepatobiliary system; and endoscopic retrograde cholangiopancreatography (ERCP) can confirm diagnosis and facilitate removal in cases of biliary ascariasis.[19]
To address the limitations of manual microscopy, recent advances in artificial intelligence (AI) have shown great promise. A 2025 study evaluated deep learning models trained to recognize helminth eggs in microscopic images. These AI-powered diagnostic tools offer high accuracy, objectivity, and scalability, making them especially attractive for use in resource-limited settings.[21][22] Furthermore, WHO expert groups have explored point-of-care antigen detection using urine-based circulating cathodic antigen (POC-CCA) assays.[23] While their role in routine Ascaris diagnosis remains under investigation, they may hold potential in selected epidemiologic contexts. Taken together, these traditional and emerging diagnostic modalities—from microscopy and molecular assays to serology and AI—highlight the evolving landscape of ascariasis detection and the need for context-specific diagnostic strategies.[24][4][18][25][19][26][21]
Treatment / Management
Even mild or asymptomatic ascariasis should be treated to reduce the parasite burden and prevent complications associated with adult worm migration. However, during the early pulmonary (larval migratory ) phase, antihelminthic therapy is generally deferred, as treatment at this stage may exacerbate eosinophilic pneumonitis (Löffler syndrome) due to inflammatory responses to dying larvae. Once adult worms are established in the intestine, albendazole 400 mg orally as a single dose is the treatment of choice, with mebendazole (100 mg twice daily for 3 days or a single dose of 500 mg) and ivermectin (150–200 µg/kg as a single dose) serving as effective alternatives. Importantly, all these treatments were well tolerated and deemed safe in both children and adults, with no serious adverse events reported. However, in pregnancy, particularly during the first trimester, pyrantel pamoate (11 mg/kg, maximum 1 g, single dose) is preferred due to its favorable safety profile; piperazine may also be used when necessary.
Anthelmintic therapy targets adult worms only and is ineffective against migrating larvae; therefore, a repeat dose after 1 to 3 months is recommended in endemic settings to allow any residual larvae to mature into susceptible adults. In a randomized trial and subsequent meta-analyses, single-dose albendazole, mebendazole, and pyrantel pamoate achieved cure rates exceeding 85%, with albendazole demonstrating the highest egg-reduction rates (>98%). Alternative agents, eg, nitazoxanide and levamisole, have demonstrated efficacy but are less commonly used. Posttreatment stool reexamination at approximately 3 months is recommended to assess for persistent infection and to guide retreatment; household contacts should be screened and treated in endemic settings to limit reinfection.
In cases of intestinal obstruction, management depends on severity. Partial obstruction should be treated conservatively with bowel rest, nasogastric decompression, intravenous fluids, and antihelminthic therapy (traditionally piperazine). Complete obstruction or complications, eg, volvulus, ischemia, or perforation, require surgical or endoscopic intervention for worm extraction, with bowel resection and anastomosis reserved for necrotic segments. Following restoration of intestinal transit, antihelminthic therapy should be administered to eradicate remaining adult worms and reduce the risk of recurrence.[27][20][28][23][29][30][18][31][32](A1)
Differential Diagnosis
The clinical manifestations of ascariasis vary with parasite burden, life cycle stage, and anatomic involvement and therefore overlap with several gastrointestinal, hepatobiliary, and respiratory conditions.
Hepatobiliary and Pancreatic Disorders
Acute cholangitis, or ascending cholangitis, presents with fever, right upper quadrant pain, and jaundice, consistent with Charcot triad. Bacterial cholangitis commonly results from obstructing gallstones or strictures and is frequently associated with positive blood cultures. In contrast, imaging in ascariasis-related disease may demonstrate linear or motile filling defects within the bile ducts rather than calculi.
Cholecystitis and biliary colic from gallstone disease produce episodic or persistent right upper quadrant pain, often following meals, with ultrasound findings of gallstones and gallbladder wall thickening. In biliary ascariasis, imaging may reveal mobile echogenic tubular structures without acoustic shadowing.
Acute pancreatitis presents with epigastric pain radiating to the back and elevated pancreatic enzyme levels. Gallstones and alcohol represent the most common causes; however, migration of Ascaris into the pancreatic duct remains a recognized etiology in endemic regions and warrants consideration when imaging demonstrates ductal obstruction without stones.
Intestinal and Surgical Emergencies
The following emergent conditions may have overlapping clinical features with ascariasis:
- Appendicitis: Presents with periumbilical pain migrating to the right lower quadrant, fever, and leukocytosis. Ascariasis may mimic appendicitis due to localized inflammation or obstruction, but may be distinguished by imaging or passage of worms.
- Small bowel obstruction: A classic complication of heavy ascariasis, especially in children, caused by worm boluses. Differentiation from adhesive obstruction or hernias relies on imaging showing intraluminal filling defects or “whirlpool” patterns.
- Large bowel obstruction: Less common in ascariasis; more often caused by malignancy, volvulus, or strictures. Ascariasis-related obstruction typically involves the small intestine.
- Intussusception: Common in young children and presents with intermittent abdominal pain, vomiting, and sometimes “currant jelly” stools. Ascariasis can act as a lead point in endemic areas.
Respiratory Conditions
Asthma presents with wheezing, cough, and dyspnea that may resemble symptoms seen during the pulmonary migratory phase of ascariasis. In ascariasis, symptoms tend to be transient, accompanied by eosinophilia, and may include fever or pulmonary infiltrates consistent with Löffler syndrome. Eosinophilic pneumonitis, or Löffler syndrome, requires differentiation from asthma, pneumonia, and hypersensitivity pneumonitis. A history of exposure and the presence of peripheral eosinophilia provide important diagnostic clues.
Parasitic Infections
The following parasitic infections may also have overlapping clinical features with ascariasis:
- Hookworm infection (Ancylostoma duodenale, Necator americanus): Can cause abdominal symptoms and eosinophilia but is more commonly associated with iron-deficiency anemia rather than mechanical obstruction or biliary disease.
- Other soil-transmitted helminths (eg, Trichuris trichiura): Typically cause chronic diarrhea or rectal prolapse rather than obstruction or hepatobiliary complications.
In endemic settings or among migrants and travelers, ascariasis should be considered in patients presenting with unexplained biliary disease, bowel obstruction, eosinophilia with pulmonary symptoms, or recurrent abdominal pain, particularly in children.[4][5][18][25]
Prognosis
The prognosis of ascariasis is generally excellent with appropriate treatment, particularly in uncomplicated infections. As stated before, studies from endemic regions in Asia and sub-Saharan Africa demonstrate that single-dose albendazole (400 mg) achieves cure rates of 90% to 95%, with a progressive, substantial reduction in egg excretion over subsequent weeks in the vast majority of treated individuals. Clinical recovery is typically rapid, and mortality is rare, occurring mainly in the context of severe complications, eg, intestinal obstruction or hepatobiliary involvement.
Despite high treatment efficacy, reinfection is common in endemic areas due to persistent environmental contamination, making relocation alone insufficient without broader public health interventions. Consequently, long-term prognosis at the population level depends heavily on prevention strategies. The WHO emphasizes a multipronged approach that includes preventive chemotherapy, particularly mass drug administration (MDA) with albendazole or mebendazole targeting school-aged children and other high-risk groups, sustained improvements in water, sanitation, and hygiene (WASH) infrastructure for both household and agricultural environments, and environmental and agricultural deworming practices, including reducing the use of untreated human feces as fertilizer.[WHO. Preventive Chemotherapy to Control Soil-Transmitted Helminth Infections in At-Risk Groups. 2017]
Additional preventive measures, eg, access to clean drinking water, improved latrine coverage, avoiding contact with untreated manure, using protective footwear, and community-based health education, are critical for reducing transmission and preventing recurrence. Increasingly, socioeconomic development initiatives aimed at alleviating poverty and improving living conditions have been recognized as essential to achieving durable reductions in the burden of ascariasis. When these combined measures are implemented, ascariasis-associated morbidity, particularly growth impairment and malnutrition in children, can be substantially reduced, leading to favorable long-term outcomes at both individual and community levels.[29][18][9][23][14]
Complications
Ascariasis can lead to a wide range of complications, particularly in individuals with high parasite burden, recurrent infection, or delayed treatment, and disproportionately affects children in endemic regions.
Gastrointestinal Complications
Gastrointestinal conditions that may develop due to ascariasis include:
- Bowel obstruction: One of the most serious and well-documented complications, especially in children, caused by boluses of adult worms obstructing the small intestine. Clinical manifestations include abdominal distension, vomiting, constipation, and abdominal pain, and severe cases may progress to volvulus, ischemia, perforation, or peritonitis, requiring surgical intervention.
- Appendicitis: Migration of adult worms into the appendix may cause luminal obstruction and inflammation, mimicking or precipitating acute appendicitis.
- Bleeding per rectum: Although uncommon, mucosal irritation, ulceration, or secondary bacterial infection associated with a heavy worm burden or intestinal obstruction may result in lower gastrointestinal bleeding, particularly in children.
Hepatobiliary and Pancreatic Complications
Hepatic and pancreatic complications associated with ascariasis include:
- Hepatobiliary disease: Adult worms may migrate into the biliary tree and gallbladder, leading to biliary colic, acute cholecystitis, cholangitis, hepatic abscess, and recurrent right upper-quadrant pain. Imaging often reveals linear or motile intraductal structures, distinguishing ascariasis from gallstone disease.
- Pancreatic involvement: Migration into the pancreatic duct can cause acute pancreatitis and, in rare cases, result in pancreatic pseudocyst formation due to ductal obstruction and inflammation. Ascariasis should be considered in patients from endemic regions presenting with pancreatitis without typical risk factors.
Nutritional and Developmental Consequences
Chronic or repeated ascariasis contributes to protein–energy malnutrition, micronutrient deficiencies, impaired linear growth, and reduced cognitive development in children. Mechanisms include competition for nutrients, decreased appetite, malabsorption, and chronic intestinal inflammation. These effects are amplified in settings of poverty and food insecurity and represent a major component of the global disease burden attributed to ascariasis.
Additional Considerations
Complications demonstrate a clear dose-dependent relationship, with higher morbidity associated with heavy infections. Children are more susceptible than adults due to higher exposure rates, a smaller intestinal lumen, and greater nutritional vulnerability. Early diagnosis, appropriate treatment, and sustained public health interventions prevent many complications and reduce overall disease burden.
Postoperative and Rehabilitation Care
Postoperative management following surgical or endoscopic treatment of ascariasis, most commonly for intestinal obstruction or hepatobiliary complications, should focus on restoring nutritional status, preventing reinfection, and ensuring eradication of residual adult worms.
Children who are particularly vulnerable to malnutrition and growth impairment should undergo nutritional assessment and rehabilitation, including vitamin A supplementation where deficiency is prevalent, in accordance with global child health recommendations. Once intestinal transit is restored, antihelmintic therapy should be administered to eliminate any remaining adult worms and reduce the risk of recurrence. Adherence to prescribed therapy is essential for individual cure and for reducing community transmission.[33]
Deterrence and Patient Education
Environmental contamination from unhygienic cultural and agricultural practices requires robust public health education and interventions. Limited public health resources impede effective intervention. Education, access to fresh water, and improved sanitation are necessary.
Pearls and Other Issues
Adult Ascaris lumbricoides worms have a finite lifespan (approximately 1–2 years) and do not multiply within the human host. In the absence of reinfection, spontaneous clearance may occur over time; however, in endemic regions, reinfection is common, making education, early diagnosis, and timely treatment essential.
Hand hygiene remains one of the most effective preventive measures. In high-endemicity settings, early detection and treatment are critical not only to prevent acute surgical complications but also to mitigate long-term consequences, including malnutrition, impaired growth, cognitive deficits, and loss of productive life years, particularly among children.
The following factors should be kept in mind in the management of ascariasis:
- Ascariasis is frequently documented in Sub-Saharan Africa, Latin America, the Caribbean, China, and East Asia.
- Ascariasis is acquired through ingestion of embryonated eggs from contaminated soil, food, or water.
- Most individuals infected with ascariasis are asymptomatic or experience mild, nonspecific symptoms.
- Clinical manifestations are largely determined by parasite burden and related complications.
- Ascariasis disproportionately affects children aged 5 to 15 years.
- Low-intensity infections may remain clinically silent, presenting only with long-term sequelae such as growth retardation and malnutrition, particularly in children.
- Gastrointestinal manifestations include abdominal pain, bloating, nausea, vomiting, anorexia, and intermittent diarrhea.
- During the larval migratory phase, a heavy pulmonary larval burden may result in transient eosinophilic pneumonitis (Löffler syndrome).
- Adult worms may migrate into tubular structures, eg, the biliary and pancreatic ducts, leading to biliary colic, cholecystitis, cholangitis, pancreatitis, as well as small-bowel obstruction, volvulus, appendicitis, and intussusception.
- The cornerstone of diagnosis remains direct microscopic examination of stool samples for ova.
- Ascaris eggs are characteristically large, oval, brown, and trilayered, with a mammillated outer coat.
- Microscopy can underestimate infection burden.
- PCR combined with serology provides higher sensitivity.
- Eosinophilia may be observed during the larval migratory phase, and larvae may be recovered in sputum during pulmonary involvement.
- Occasionally, adult worms may be directly visualized when passed in stool, expelled rectally, or expectorated, and rare reports describe worms expelled in urine due to aberrant migration.
- Ascariasis should be treated to reduce the parasite burden and prevent complications associated with adult worm migration.
- During the early pulmonary (larval migratory) phase, antihelmintic therapy is generally deferred, as treatment at this stage may exacerbate eosinophilic pneumonitis (Löffler syndrome).
- Albendazole is the treatment of choice; mebendazole and ivermectin are considered alternative options.
- In pregnancy, particularly during the first trimester, pyrantel pamoate is preferred due to its favorable safety profile.
- Anthelmintic therapy targets adult worms only and is ineffective against migrating larvae; therefore, a repeat dose after 1 to 3 months is recommended.
- Post-treatment stool reexamination at approximately 3 months is recommended to assess for persistent infection.
- Household contacts should be screened and treated in endemic settings to limit reinfection.
- Complete bowel obstruction or complications, eg, volvulus, ischemia, or perforation, require surgical or endoscopic intervention for worm extraction.
- The prognosis of ascariasis is generally excellent with appropriate treatment.
- Despite high treatment efficacy, reinfection is common in endemic areas due to persistent environmental contamination.
Enhancing Healthcare Team Outcomes
Ascariasis, caused by Ascaris lumbricoides, remains a highly prevalent soil-transmitted helminth infection with significant global morbidity, particularly among children in endemic regions. Infection follows ingestion of embryonated eggs, with larvae migrating through the lungs before maturing in the intestine. Clinical manifestations range from asymptomatic infection to gastrointestinal symptoms and eosinophilic pneumonitis (Löffler syndrome), with severe complications including bowel obstruction, biliary disease, and pancreatitis in high-burden infections. Diagnosis relies on stool microscopy for ova and parasites, though sensitivity varies, and adjunctive tools such as PCR and imaging improve detection in select cases. Management centers on antihelminthic therapy targeting adult worms, with attention to timing, repeat dosing, and treatment of complications.
Interprofessional collaboration enhances outcomes through coordinated, patient-centered care. Physicians and advanced practice providers lead diagnosis and management, while primary care clinicians ensure early recognition, screening, and follow-up. Nurses support monitoring, education, and adherence, and pharmacists guide safe medication selection, dosing, and counseling, particularly in special populations. Laboratory professionals optimize diagnostic accuracy, and public health teams contribute to prevention, sanitation, and reinfection control. Effective communication, shared decision-making, and timely referral for complications such as obstruction or hepatobiliary involvement improve safety, reduce recurrence, and strengthen systems-based care.
Media
(Click Image to Enlarge)
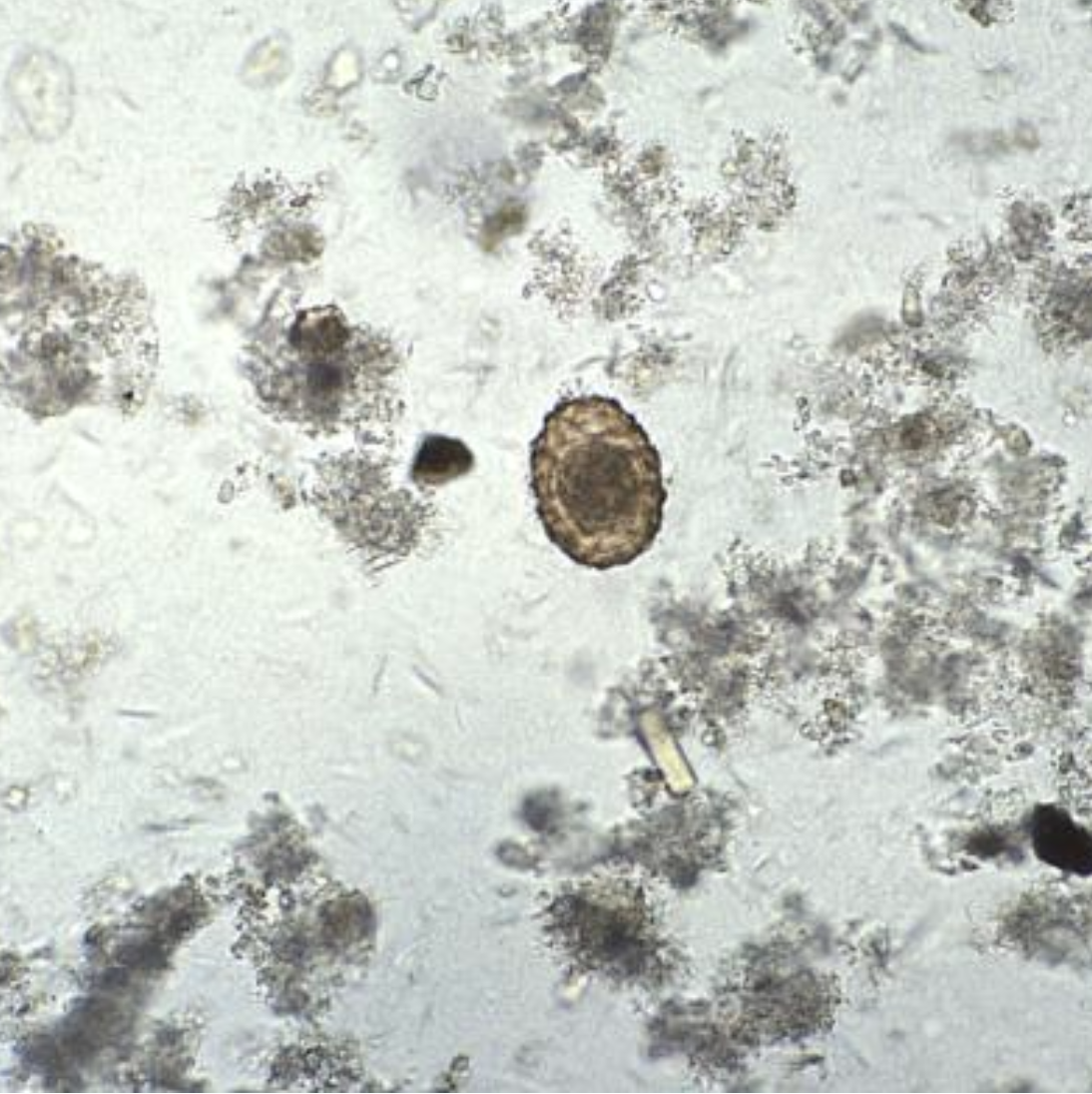
Ascaris Ova. Under a magnification of 128×, this photomicrograph revealed some of the ultrastructural features displayed by a fertile, Ascaris lumbricoides egg. A. lumbricoides is the largest nematode (roundworm) parasitizing the human intestine.
Mae Melvin, MD; Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
References
Holland C, Sepidarkish M, Deslyper G, Abdollahi A, Valizadeh S, Mollalo A, Mahjour S, Ghodsian S, Ardekani A, Behniafar H, Gasser RB, Rostami A. Global prevalence of Ascaris infection in humans (2010-2021): a systematic review and meta-analysis. Infectious diseases of poverty. 2022 Nov 18:11(1):113. doi: 10.1186/s40249-022-01038-z. Epub 2022 Nov 18 [PubMed PMID: 36401308]
Level 1 (high-level) evidenceFahim SM, Das S, Gazi MA, Mahfuz M, Ahmed T. Association of intestinal pathogens with faecal markers of environmental enteric dysfunction among slum-dwelling children in the first 2 years of life in Bangladesh. Tropical medicine & international health : TM & IH. 2018 Nov:23(11):1242-1250. doi: 10.1111/tmi.13141. Epub 2018 Sep 10 [PubMed PMID: 30133067]
GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet (London, England). 2020 Oct 17:396(10258):1204-1222. doi: 10.1016/S0140-6736(20)30925-9. Epub [PubMed PMID: 33069326]
Level 1 (high-level) evidenceDold C, Holland CV. Ascaris and ascariasis. Microbes and infection. 2011 Jul:13(7):632-7. doi: 10.1016/j.micinf.2010.09.012. Epub 2010 Oct 8 [PubMed PMID: 20934531]
Level 3 (low-level) evidenceJourdan PM, Lamberton PHL, Fenwick A, Addiss DG. Soil-transmitted helminth infections. Lancet (London, England). 2018 Jan 20:391(10117):252-265. doi: 10.1016/S0140-6736(17)31930-X. Epub 2017 Sep 4 [PubMed PMID: 28882382]
Bethony J, Brooker S, Albonico M, Geiger SM, Loukas A, Diemert D, Hotez PJ. Soil-transmitted helminth infections: ascariasis, trichuriasis, and hookworm. Lancet (London, England). 2006 May 6:367(9521):1521-32 [PubMed PMID: 16679166]
Adu-Gyasi D, Asante KP, Frempong MT, Gyasi DK, Iddrisu LF, Ankrah L, Dosoo D, Adeniji E, Agyei O, Gyaase S, Amenga-Etego S, Gyan B, Owusu-Agyei S. Epidemiology of soil transmitted Helminth infections in the middle-belt of Ghana, Africa. Parasite epidemiology and control. 2018 Aug:3(3):e00071. doi: 10.1016/j.parepi.2018.e00071. Epub 2018 Apr 30 [PubMed PMID: 29988303]
Sharma M, Somani P, Prasad R, Jindal S, Pathak A. Biliary ascariasis: mimicker of biliary stent. VideoGIE : an official video journal of the American Society for Gastrointestinal Endoscopy. 2017 Jul:2(7):179-181. doi: 10.1016/j.vgie.2017.04.001. Epub 2017 May 6 [PubMed PMID: 29905283]
Freeman MC, Garn JV, Sclar GD, Boisson S, Medlicott K, Alexander KT, Penakalapati G, Anderson D, Mahtani AG, Grimes JET, Rehfuess EA, Clasen TF. The impact of sanitation on infectious disease and nutritional status: A systematic review and meta-analysis. International journal of hygiene and environmental health. 2017 Aug:220(6):928-949. doi: 10.1016/j.ijheh.2017.05.007. Epub 2017 May 31 [PubMed PMID: 28602619]
Level 1 (high-level) evidenceBradbury RS, Martin L, Malloch L, Martin M, Williams JM, Patterson K, Sanders C, Singh G, Arguello I, Rodriguez E, Byers P, Haynie L, Qvarnstrom Y, Hobbs CV. Surveillance for Soil-Transmitted Helminths in High-Risk County, Mississippi, USA. Emerging infectious diseases. 2023 Dec:29(12):2533-2537. doi: 10.3201/eid2912.230709. Epub [PubMed PMID: 37987591]
Claus PE, Ceuppens AS, Cool M, Alliet G. Ascaris lumbricoides: challenges in diagnosis, treatment and prevention strategies in a European refugee camp. Acta clinica Belgica. 2018 Dec:73(6):431-434. doi: 10.1080/17843286.2018.1436956. Epub 2018 Feb 19 [PubMed PMID: 29458300]
Landeryou T, Maddren R, Hearn J, Belachew M, Gomez SR, Liyew EF, Forbes K, Mengistu B, Lawton SP, Eze J, Tasew G, Angulo U, Anderson R. Molecular epidemiology of Ascaris lumbricoides following multiple rounds of community-wide treatment. Nature communications. 2025 May 9:16(1):4321. doi: 10.1038/s41467-025-59316-x. Epub 2025 May 9 [PubMed PMID: 40346057]
Sklyarova VО. [Epidemiological features of parasitary invasis in women of reproductive age with disorders of reproductive health]. Wiadomosci lekarskie (Warsaw, Poland : 1960). 2018:71(3 pt 2):674-677 [PubMed PMID: 29783245]
Level 2 (mid-level) evidenceBetson M, Evangelista FMD, Jones BP, Woolfe L. The roundworm Ascaris: Recent advances on the road to elimination. Advances in parasitology. 2025:129():1-73. doi: 10.1016/bs.apar.2025.07.006. Epub 2025 Aug 11 [PubMed PMID: 41062237]
Level 3 (low-level) evidenceSharma A, Jariwala P, Kaur N. Biliary ascariasis presenting with gangrenous perforation of the gall bladder: report of a case and brief review of literature. Tropical doctor. 2018 Jul:48(3):242-245. doi: 10.1177/0049475518768103. Epub 2018 Apr 13 [PubMed PMID: 29649951]
Level 3 (low-level) evidenceBradbury RS, Harrington H, Kekeubata E, Esau D, Esau T, Kilivisi F, Harrington N, Gwala J, Speare R, MacLaren D. High prevalence of ascariasis on two coral atolls in the Solomon Islands. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2018 Apr 1:112(4):193-199. doi: 10.1093/trstmh/try041. Epub [PubMed PMID: 29800343]
Hotez PJ, Brindley PJ, Bethony JM, King CH, Pearce EJ, Jacobson J. Helminth infections: the great neglected tropical diseases. The Journal of clinical investigation. 2008 Apr:118(4):1311-21. doi: 10.1172/JCI34261. Epub [PubMed PMID: 18382743]
Level 3 (low-level) evidenceKhuroo MS. Ascariasis. Gastroenterology clinics of North America. 1996 Sep:25(3):553-77 [PubMed PMID: 8863040]
Else KJ, Keiser J, Holland CV, Grencis RK, Sattelle DB, Fujiwara RT, Bueno LL, Asaolu SO, Sowemimo OA, Cooper PJ. Whipworm and roundworm infections. Nature reviews. Disease primers. 2020 May 28:6(1):44. doi: 10.1038/s41572-020-0171-3. Epub 2020 May 28 [PubMed PMID: 32467581]
Bharti B, Bharti S, Khurana S. Worm Infestation: Diagnosis, Treatment and Prevention. Indian journal of pediatrics. 2018 Nov:85(11):1017-1024. doi: 10.1007/s12098-017-2505-z. Epub 2017 Nov 11 [PubMed PMID: 29127616]
Mirzaei O, Ilhan A, Guler E, Suer K, Sekeroglu B. Comparative Evaluation of Deep Learning Models for Diagnosis of Helminth Infections. Journal of personalized medicine. 2025 Mar 20:15(3):. doi: 10.3390/jpm15030121. Epub 2025 Mar 20 [PubMed PMID: 40137437]
Level 2 (mid-level) evidencevon Bahr J, Suutala A, Kucukel H, Kaingu H, Kinyua F, Muinde M, Osundwa K, Ronald W, Muinde J, Ngasala B, Lundin M, Mårtensson A, Linder N, Lundin J. AI-supported versus manual microscopy of Kato-Katz smears for diagnosis of soil-transmitted helminth infections in a primary healthcare setting. Scientific reports. 2025 Jun 27:15(1):20332. doi: 10.1038/s41598-025-07309-7. Epub 2025 Jun 27 [PubMed PMID: 40579399]
Hon KL, Leung AKC. An update on the current and emerging pharmacotherapy for the treatment of human ascariasis. Expert opinion on pharmacotherapy. 2024 Feb 19:():. doi: 10.1080/14656566.2024.2319686. Epub 2024 Feb 19 [PubMed PMID: 38372051]
Level 3 (low-level) evidenceGhosh G, Shah S, Maltz C. Ascariasis Diagnosed by Wireless Capsule Endoscopy. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2018 Jun:16(6):A23. doi: 10.1016/j.cgh.2017.08.037. Epub 2017 Sep 1 [PubMed PMID: 28865763]
Khuroo MS, Rather AA, Khuroo NS, Khuroo MS. Hepatobiliary and pancreatic ascariasis. World journal of gastroenterology. 2016 Sep 7:22(33):7507-17. doi: 10.3748/wjg.v22.i33.7507. Epub [PubMed PMID: 27672273]
Mugo RM, Rausch S, Musimbi ZD, Strube C, Raulf MK, Landt O, Gichuki PM, Ebner F, Mwacharo J, Odiere MR, Ndungu FM, Njomo DW, Hartmann S. Evaluation of copromicroscopy, multiplex-qPCR and antibody serology for monitoring of human ascariasis in endemic settings. PLoS neglected tropical diseases. 2024 Jun:18(6):e0012279. doi: 10.1371/journal.pntd.0012279. Epub 2024 Jun 18 [PubMed PMID: 38889190]
Wright JE, Werkman M, Dunn JC, Anderson RM. Current epidemiological evidence for predisposition to high or low intensity human helminth infection: a systematic review. Parasites & vectors. 2018 Jan 31:11(1):65. doi: 10.1186/s13071-018-2656-4. Epub 2018 Jan 31 [PubMed PMID: 29382360]
Level 2 (mid-level) evidenceSilber SA, Diro E, Workneh N, Mekonnen Z, Levecke B, Steinmann P, Umulisa I, Alemu H, Baeten B, Engelen M, Hu P, Friedman A, Baseman A, Mrus J. Efficacy and Safety of a Single-Dose Mebendazole 500 mg Chewable, Rapidly-Disintegrating Tablet for Ascaris lumbricoides and Trichuris trichiura Infection Treatment in Pediatric Patients: A Double-Blind, Randomized, Placebo-Controlled, Phase 3 Study. The American journal of tropical medicine and hygiene. 2017 Dec:97(6):1851-1856. doi: 10.4269/ajtmh.17-0108. Epub 2017 Aug 31 [PubMed PMID: 29016336]
Level 1 (high-level) evidenceKeiser J, Utzinger J. Efficacy of current drugs against soil-transmitted helminth infections: systematic review and meta-analysis. JAMA. 2008 Apr 23:299(16):1937-48. doi: 10.1001/jama.299.16.1937. Epub [PubMed PMID: 18430913]
Level 3 (low-level) evidenceRomero Cabello R, Guerrero LR, Muñóz García MR, Geyne Cruz A. Nitazoxanide for the treatment of intestinal protozoan and helminthic infections in Mexico. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1997 Nov-Dec:91(6):701-3 [PubMed PMID: 9580117]
Clarke NE, Doi SAR, Wangdi K, Chen Y, Clements ACA, Nery SV. Efficacy of Anthelminthic Drugs and Drug Combinations Against Soil-transmitted Helminths: A Systematic Review and Network Meta-analysis. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2019 Jan 1:68(1):96-105. doi: 10.1093/cid/ciy423. Epub [PubMed PMID: 29788074]
Level 1 (high-level) evidenceConterno LO, Turchi MD, Corrêa I, Monteiro de Barros Almeida RA. Anthelmintic drugs for treating ascariasis. The Cochrane database of systematic reviews. 2020 Apr 14:4(4):CD010599. doi: 10.1002/14651858.CD010599.pub2. Epub 2020 Apr 14 [PubMed PMID: 32289194]
Level 1 (high-level) evidencePayne LG, Koski KG, Ortega-Barria E, Scott ME. Benefit of vitamin A supplementation on ascaris reinfection is less evident in stunted children. The Journal of nutrition. 2007 Jun:137(6):1455-9 [PubMed PMID: 17513406]