 Arterial Blood Gas Analysis: Fundamentals, Interpretation, and Clinical Utility
Arterial Blood Gas Analysis: Fundamentals, Interpretation, and Clinical Utility
Introduction
Blood gas analysis is a commonly used diagnostic tool that evaluates the partial pressures of gases and the acid-base content of a blood sample. Understanding and using blood gas analysis enables clinicians to interpret respiratory, circulatory, and metabolic disorders.[1] Although blood gas analysis is most frequently ordered by clinicians in emergency medicine, critical care, anesthesiology, and pulmonology, it has broad applications across diverse clinical settings. Common indications include acute respiratory distress syndrome (ARDS), severe sepsis, septic shock, hypovolemic shock, diabetic ketoacidosis (DKA), renal tubular acidosis, acute respiratory failure, heart failure, cardiac arrest, asthma, and inborn errors of metabolism.[2]
Blood gas analysis can be performed on blood obtained from any part of the circulatory system, including arteries, veins, or capillaries. An arterial blood gas (ABG) specifically analyzes blood obtained from an artery and measures the arterial partial pressures of oxygen (PaO2) and carbon dioxide (PaCO2).[3] PaO2 provides information on the patient's oxygenation status, whereas PaCO2 provides information on the patient's ventilation status and helps identify disorders such as chronic or acute respiratory failure. PaCO2 is affected by hyperventilation (rapid or deep breathing), hypoventilation (slow or shallow breathing), and acid-base status.[2] Although oxygenation and ventilation can be assessed noninvasively using pulse oximetry and end-tidal carbon dioxide (CO2) monitoring, respectively, ABG analysis remains the gold standard.[4]
When assessing acid-base balance, most ABG analyzers directly measure pH and PaCO2.[3] A derivative of the Henderson-Hasselbalch equation is used to calculate serum bicarbonate (HCO3) and the base deficit or excess. The accuracy of this calculation has been disputed depending on the study, machine, or calibration used, and it must be interpreted appropriately in accordance with institutional standards.[5] Because blood gas analysis calculates HCO3 from measured pH and PaCO2 values, whereas serum chemistry analysis directly measures total CO2 content, small discrepancies between the reported and measured values are expected.[5][6] The difference typically amounts to around 1.2 mmol/L. However, a more considerable difference may be observed in specific clinical scenarios, especially in critically ill patients.[7]
Pathophysiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Pathophysiology
ABG analysis provides insight into pulmonary gas exchange, ventilation, and acid-base homeostasis by measuring arterial pH and the partial pressures of oxygen and carbon dioxide.[1] Comparison of pH, PaCO2, and HCO3 values helps identify primary respiratory and metabolic acid-base disturbances as well as compensatory physiologic responses. Tissue hypoxia, impaired ventilation, ventilation-perfusion (V/Q) mismatch, and abnormal cellular metabolism can all alter ABG parameters. The alveolar-arterial (A-a) oxygen gradient is a useful measure of pulmonary gas exchange and may be elevated in conditions associated with V/Q mismatch, diffusion impairment, or intrapulmonary shunting.[8]
Specimen Requirements and Procedure
Whole blood is the required specimen for ABG analysis. The specimen is obtained through an arterial puncture or acquired from an indwelling arterial catheter. Please see StatPearls' companion resource, "Arterial Lines," for further information. Once obtained, the arterial blood sample should be placed on ice and analyzed as soon as possible to reduce the possibility of erroneous results.[9]
Measurement of PaO2 is the primary reason for obtaining an arterial specimen, as differences in measured blood gas values between arterial and venous blood are most pronounced for the partial pressure of oxygen (PO2).[10] Typically, PO2 is approximately 60 mm Hg lower in venous blood after the oxygen is released in the capillaries. In contrast, the partial pressure of carbon dioxide (PCO2) is 2 to 8 mm Hg higher, and pH is only 0.02 to 0.05 lower in a venous sample.[11] Proper specimen collection is paramount in obtaining accurate results. Placement of indwelling catheters with heparin locks for short- and long-term intravenous therapies is typical. Failure to properly flush the lock can have unpredictable effects on measured quantities and is often indicated by unexpected, nonphysiologic results.[12]
Arterial or venous specimens should be collected anaerobically in 1- to 3-mL sterile syringes using lyophilized heparin as the anticoagulant. Evacuated lithium heparin collection tubes used for plasma sampling are unsuitable for blood gas analysis because residual air and ongoing gas exchange may affect measured PO2 values.[13] Syringes containing lyophilized heparin are preferred over those containing liquid heparin, as liquid heparin has atmospheric PO2 and PCO2 values that dilute the sample.[14] When the syringe is incompletely filled, the effect is most pronounced, as a higher ratio of liquid heparin to blood can have a more marked effect on measured PCO2 and the parameters derived from it. Variations in syringe manufacturing can also create significant preanalytical effects on the sample.[15]
Anaerobic collection techniques minimize exposure of the blood sample to atmospheric air.[16] The PCO2 of atmospheric air is approximately 0.25 mm Hg, which is much lower than that of blood (40 mm Hg). Thus, the total CO2 content and PCO2 measurement of a blood sample exposed to air decrease, and blood pH, as a function of PCO2, subsequently rises. The PO2 of atmospheric air (155 mm Hg) is approximately 60 mm Hg higher than that of arterial blood and approximately 100 mm Hg higher than venous blood. Hence, blood from a patient breathing room air absorbs oxygen when exposed to atmospheric air, whereas blood with a PO2 exceeding 150 mm Hg, as observed in patients undergoing oxygen therapy, releases oxygen.[17]
Air exposure can occur simply from the air in the needle and the dead space in the syringe hub. The error is minimal if the resulting bubble is ejected immediately after drawing by holding the syringe tip up and ejecting a small drop of blood.[18] The potential effect of small bubbles on blood gas results was demonstrated in one study in which a 100 mL bubble of room air was added to 10 blood samples (2 mL each) with PO2 values ranging from 25 to 40 mm Hg. PO2 increased an average of 4 mm Hg in these samples in only 2 minutes, and PCO2 decreased by 4 mm Hg. Before analysis, the sample should be mixed by vigorously rolling the syringe between the technician's palms to ensure homogeneity.[19] Arterialized capillary blood is sometimes an acceptable alternative to arterial blood when an arterial cannula is unavailable or repeated arterial punctures must be avoided.[20]
Automated blood gas analyzers are commonly used to analyze blood gas samples, and results are obtained within 10 to 15 minutes. These automated analyzers, directly and indirectly, measure specific components of the arterial blood gas sample.[1] In the case of an ABG, the analyzed components include the following:
- Measured:
- pH = acid-base balance of the blood
- PaO2 = partial pressure of oxygen in arterial blood
- PaCO2 = partial pressure of carbon dioxide in arterial blood
- Calculated:
- HCO3 = concentration of bicarbonate in arterial blood
- Base excess/deficit = relative excess or deficit of base in arterial blood
- SaO2 = arterial oxygen saturation (unless a co-oximetry is obtained, in which case SaO2 is measured)
The radial artery is the preferred site for ABG because it is superficial and easily palpable over the radial styloid process. The femoral artery is the next most common site. Before an ABG is drawn from either upper extremity, a modified Allen test is necessary to confirm adequate collateral blood flow. The test is performed on the unilateral upper extremity chosen for the procedure (see Image. Modified Allen Test). The patient is asked to flex the selected upper extremity at the elbow and clench a raised fist for 30 seconds. The clinician applies pressure over the ulnar and radial arteries to occlude the blood flow. After 5 seconds, the patient may unclench the raised fist. At this point, the palm appears pale, white, or blanched. Then, pressure over the ulnar artery is released while the radial artery compression is maintained. In 10 to 15 seconds, the palm should return to its original color, indicating adequate ulnar collateral blood flow. If the palm does not return to its original color, the result is considered abnormal, indicating that puncturing the radial artery is unsafe. Similarly, the radial collateral blood flow is assessed by maintaining ulnar artery pressure and releasing the radial artery pressure.[21] As alternatives to the modified Allen test, pulse oximetry and duplex ultrasound can also be used to assess collateral flow.
Testing Procedures
Operating a traditional blood gas instrument begins with the operator presenting a blood specimen at the sample probe. The sample is taken through the probe by a peristaltic pump, which loads the chamber with a specific amount of the sample. The sample then resides in the chamber long enough to allow thermal equilibration and completion of the measurements. On completion, the pump pushes the sample to waste.[22] Because the instrument's electrodes are not stable for very long, frequent calibration of pH, PCO2, and PO2 is required.[23] Most instruments include a barometer, ensuring that barometric pressure is always known to the microprocessor during calibration. Other instruments perform point-of-care or bedside testing. Almost all manufacturers now produce small, portable, stand-alone, easy-to-operate instruments designed for satellite laboratory use; several hand-held devices that use disposable electrodes are also available.[24]
The sophistication of contemporary equipment and the availability of high-quality calibrator materials have improved the reliability and accuracy of blood gas and pH determination, particularly when combined with meticulous maintenance, adherence to manufacturer-recommended procedures, appropriate equipment control, and proper specimen collection and handling.[22] Software for the instrument's microprocessor often includes display warnings and diagnostic routines that alert the operator and assist with troubleshooting. The manufacturer's recommended maintenance schedule should be considered a minimum guideline, with experience indicating the appropriate maintenance frequency.[25]
Cleanliness of the sample chamber and path is essential. Automatic flushing to cleanse the sample chamber and path after each blood sample measurement is a feature of most instruments that do not use disposable electrodes. Despite proper flushing, however, complete or partial clogging of the chamber or path may occur.[1] Fibrin threads and small clots may be present in the specimen or may form while the sample resides in the warm chamber. If left in place, the debris can affect subsequent measurements or calibrations by interfering with contact between blood, buffers, or gases and electrode membranes.[18] Visibility of the path through the heat sink helps detect clogs, dirt, and bubbles. Bubbles that fail to rinse out can be problematic if they settle on an electrode.[26]
Results, Reporting, and Critical Findings
Normal reference ranges for ABG parameters are listed below, although values may vary slightly among laboratories and across age groups, from neonates to older adults:
- pH (7.35-7.45)
- PaO2 (75-100 mm Hg)
- PaCO2 (35-45 mm Hg)
- HCO3 (22-26 mEq/L)
- Base excess/deficit (−4 to +2)
- SaO2 (95%–100%) [27][28]
Arterial blood gas interpretation should be approached systematically to assess the severity and chronicity of any abnormalities and determine whether the primary disorder is metabolic or respiratory in origin.[29] Several articles have described simplistic methods for interpreting ABG results. However, the Romanski method is among the most straightforward and is suitable for clinicians at all levels of training. This method helps determine the presence of an acid-base disorder, its primary cause, and whether compensation is present.[30]
The first step of the Romanski method is to assess the pH for the presence of acidemia (pH <7.35) or alkalemia (pH >7.45). If the pH is within the normal range (7.35-7.45), a pH of 7.40 should be used as the cutoff; in other words, clinicians should categorize a pH of 7.37 as acidosis and 7.42 as alkalemia. Next, the respiratory and metabolic components of the ABG results should be evaluated: the PaCO2 and HCO3, respectively. The PaCO2 indicates whether the acidosis or alkalemia is primarily from a respiratory or metabolic acidosis/alkalosis. PaCO2 greater than 40 mm Hg with a pH less than 7.4 indicates a respiratory acidosis, whereas PaCO2 less than 40 mm Hg and pH greater than 7.4 indicates a respiratory alkalosis. Respiratory alkalosis is often the result of hyperventilation from either anxiety or compensation for a metabolic acidosis. The next step is to determine whether compensation has occurred by identifying (PaCO2 or HCO3) is inconsistent with the pH. Finally, PaO2 should be assessed for any abnormalities in oxygenation.[29]
Example 1
This example uses the following ABG results: pH 7.39; PaCO2 51 mm Hg; PaO2 59 mm Hg; HCO3 30 mEq/L; and SaO2 90%, on room air.[28]
- The pH is within the normal range, so 7.40 is used as the cutoff; in this case, the pH is less than 7.40, indicating acidosis.
- The elevated PaCO2 indicates respiratory acidosis, and the elevated HCO3 indicates a metabolic alkalosis.
- The value consistent with the pH is PaCO2. Therefore, this case is a primary respiratory acidosis. The acid-base component that is inconsistent with the pH is the elevated HCO3, indicating a compensatory metabolic alkalosis. Because metabolic compensation takes days to be effective, this finding suggests a non-acute primary disorder.
- Finally, the decreased PaO2 indicates an abnormality with oxygenation. Obtaining a detailed history and performing a thorough physical examination help determine the severity and urgency of any required interventions.
Example 2
This example uses the following ABG results: pH 7.45; PaCO2 32 mm Hg; PaO2 138 mm Hg; HCO3 23 mEq/L; base deficit 1 mEq/L; and SaO2 92%, on room air.[28]
- The pH is within the normal range. With 7.40 as the cutoff, the pH is greater than 7.40, indicating alkalemia.
- The decreased PaCO2 indicates a respiratory alkalosis. The HCO3 is on the low end of normal.
- The value consistent with the pH is PaCO2. Therefore, this case is a primary respiratory alkalosis. The HCO3 is within the normal range and thus is not inconsistent with the pH; this finding indicates a lack of compensation.
- Finally, the PaO2 is within the normal range, so oxygenation is unaffected.
When evaluating a patient's acid-base status, assessing for an electrolyte imbalance or an anion gap is important for synthesizing the information.[31] For example, a patient who presents with DKA eliminates ketones and closes the anion gap, but the metabolic acidosis persists due to hyperchloremia.
Clinical Significance
Arterial blood gas monitoring is the standard for assessing a patient's oxygenation, ventilation, and acid-base status. ABGs are frequently performed to evaluate oxygenation in the context of severe sepsis, acute respiratory failure, and ARDS in the intensive care unit and emergency room settings. Although ABG monitoring has largely been replaced by noninvasive monitoring, ABGs remain useful for confirming and calibrating noninvasive monitoring techniques.[1]
Calculating an alveolar-arterial oxygen gradient can help narrow down the cause of a patient's hypoxemia.[25] For example, the presence or absence of an A-a gradient can help determine whether the abnormality in oxygenation is potentially due to hypoventilation, a shunt, V/Q mismatch, or impaired diffusion. The equation for the expected A-a gradient assumes the patient is breathing room air; therefore, it is less accurate at higher fractions of inspired oxygen (FiO2). Determining the intrapulmonary shunt fraction (ie, the fraction of cardiac output flowing through pulmonary units that do not contribute to gas exchange) is the best estimate of oxygenation status. The shunt fraction is traditionally calculated while the patient is breathing an FiO2 of 1.0; when calculated at lower FiO2 values, the term venous admixture is more appropriate.[1]
For simplicity, oxygenation is more commonly assessed using the ratio of PaO2 to FiO2, commonly referred to as the P/F ratio. However, using the P/F ratio in assessing oxygenation carries its own limitations, as the discrepancy between venous admixture and the P/F ratio at a given shunt fraction depends on the delivered FiO2. Researchers use the P/F ratio to categorize disease severity in ARDS.[32]
Another parameter commonly used in intensive care units to assess oxygenation is the oxygenation index. This index is considered a better indicator of lung injury, particularly in neonatal and pediatric populations, than the P/F ratio. This index also includes the level of invasive ventilatory support required to maintain oxygenation.[33] The oxygenation index is the product of the mean airway pressure (Paw) in cm H2O, as measured by the ventilator, and the FiO2 percentage divided by the PaO2. The oxygenation index is commonly used to guide management, including initiating inhaled nitric oxide, administering surfactant, and determining the potential need for extracorporeal membrane oxygenation.[34]
A normal PaO2 value does not rule out respiratory failure, particularly in the presence of supplemental oxygen. PaCO2 is a more sensitive marker of ventilatory failure than PaO2, particularly in the presence of supplemental oxygen, as it is closely related to the depth and rate of breathing.[27] The PaCO2 reflects pulmonary ventilation and cellular CO2 production. Calculating the pulmonary dead space is a good indicator of overall lung function. Pulmonary dead space is the difference between the PaCO2 and mixed expired PCO2 (physiological dead space) or the end-tidal PCO2 divided by the PaCO2. Pulmonary dead space increases when ventilation in pulmonary units rises relative to perfusion, while shunting also increases. Hence, pulmonary dead space is an excellent bedside indicator of lung function and one of the best prognostic factors in patients with ARDS.[1] The pulmonary dead space fraction may also help diagnose other conditions, such as pulmonary embolism.[35]
Acid-base balance can be affected by the aforementioned respiratory system abnormalities. For instance, acute respiratory acidosis and alkalemia result in acidemia and alkalemia, respectively. Additionally, hypoxemic hypoxia leads to anaerobic metabolism, which causes metabolic acidosis that results in acidemia. Metabolic system abnormalities also affect acid-base balance, as acute metabolic acidosis and alkalosis similarly result in acidemia and alkalemia.[25] Patients with DKA, septic shock, renal failure, drug or toxin ingestion, and gastrointestinal or renal HCO3 loss exhibit metabolic acidosis.[28] Conditions such as kidney disease, electrolyte imbalances, prolonged vomiting, hypovolemia, diuretic use, and hypokalemia cause metabolic alkalosis.[36]
Quality Control and Lab Safety
Healthcare providers can analyze an ABG and electrolytes, often called a shock panel, using point-of-care testing (POCT). Appropriate calibration or standardization of these machines ensures accurate and precise readings for clinical decisions. Clinicians should refer to the user manuals to ensure appropriate device calibration when discussing with the clinical laboratory team.[37]
Elements of good quality assurance of blood gas and pH measurements include the following:
- Proper maintenance of the instrument
- Use of control materials
- Verification of electrode linearity
- Checking barometer accuracy
- Accurate measurement of temperature [38]
External quality assurance (proficiency testing) mandated by federal law in the United States (Clinical Laboratory Improvement Amendments 1988) assumed importance for quality control of blood gas analysis.[39] These rules became effective in January 1991 and set criteria for satisfactory interlaboratory performance, which are as follows:
- pH: Target value ±0.04
- PO2: Target value ±3 SD
- PCO2: Target value ±8% or ±5 mm Hg, whichever is greater [40]
The importance of proficiency testing and the penalties for failure place strong incentives on consistent performance of internal control measures and effective response to quality control failures.[41] At the same time, pressure to control healthcare costs has raised questions about how frequently interlaboratory performance should be monitored and which concentrations of control materials are necessary. According to Clinical Laboratory Improvement Amendments 1988, the answer is 1 concentration of control every 8 hours, with the entire range of control concentrations covered every 24 hours.[22] In many laboratories, however, the practical answer is to run 3 concentrations of control for pH, PO2, and PCO2 on every instrument in use at least once per shift and always upon completion of maintenance and troubleshooting procedures.
Newer analyzers, particularly smaller satellite laboratory and point-of-care instruments, frequently have automatic quality control (QC) features or use electronic QC.[42] Auto QC uses internally stored QC materials, which are automatically analyzed at designated intervals to meet regulatory requirements. Electronic QC, most commonly incorporated into devices with disposable electrode cartridges, uses cartridge-based systems to verify instrument electronic performance specifications.[43]
From a laboratory safety perspective, ABG analysis in both central laboratories and POCT sites requires strict adherence to biosafety and infection control practices to minimize the risk of exposure to bloodborne pathogens and pre-analytical errors. All ABG specimens are considered potentially infectious and must be handled using appropriate personal protective equipment, including gloves, lab coats, and eye protection, along with strict hand hygiene before and after sample handling. In the central laboratory, safety is ensured through proper specimen transport in sealed, leak-proof, anaerobically maintained syringes, immediate analysis to reduce biohazard exposure time, and safe disposal of sharps in designated containers to prevent needle-stick injuries.
In POCT settings such as ICUs and emergency departments, additional safety emphasis is placed on operator competency, device disinfection between patients, and strict adherence to cartridge-based system handling to prevent cross-contamination. Both settings require meticulous attention to prevent air contamination, sample leakage, and improper handling of heparinized syringes, as these factors not only compromise analytical accuracy but also increase occupational risk. Implementation of standardized operating procedures, regular training, and compliance with institutional biosafety and quality standards help ensure the safe practice of ABG testing across all hospital environments.
Enhancing Healthcare Team Outcomes
An ABG can be used to assess a patient's ventilatory, acid-base, and oxygenation status. Additionally, blood gas analysis is recommended to assess a patient's response to therapeutic interventions and to monitor the severity and progression of documented cardiopulmonary disease processes.[44] Despite its clinical value, erroneous or discrepant values represent a potential drawback of blood gas analysis, so eliminating potential sources of error is paramount.[27] Therefore, attention to detail in the sampling technique and processing is essential.
Rigorous quality control of automated blood gas analyzers is also necessary to ensure accurate results. However, advances in machine performance and quality assurance have now made most errors in POCT ABG analysis attributable to clinical providers. Several pre-analytic steps must be followed to obtain a valid, interpretable ABG.[27] In most hospital settings, ABG analysis involves multiple healthcare providers (eg, clinicians, respiratory therapists, and nurses). Hence, interprofessional coordination, cooperation, and communication are vitally important.
The American Association for Respiratory Care has published Clinical Care Guidelines for Blood Gas Analysis and Hemoximetry that provide current best practices for sampling, handling, and analyzing ABGs.[44] Notable sources of erroneous values during blood draws include abnormal or misstated FiO2, barometric pressures, or temperatures. Temperature is a significant variable that can lead to discrepancies between PaO2 and SaO2, as can acid-base disturbances. Several physiological and clinical conditions, including hyperleukocytosis and dyshemoglobinemias, may also result in discrepancies between PaO2 and SaO2. Sample dilution can be an additional source of error, with liquid heparin and saline as potential contributors.[45]
The mode of sample transport is also significant, as discrepant values can result from air contamination during pneumatic tube transport compared with manual transport of the specimen, especially in the presence of inadvertent air bubbles.[45] Therefore, procuring samples using suitable syringes filled with adequate amounts of blood, free of air bubbles, maintained at the correct temperatures, and transporting them appropriately and promptly for rapid analysis can minimize erroneous values.
Media
(Click Image to Enlarge)
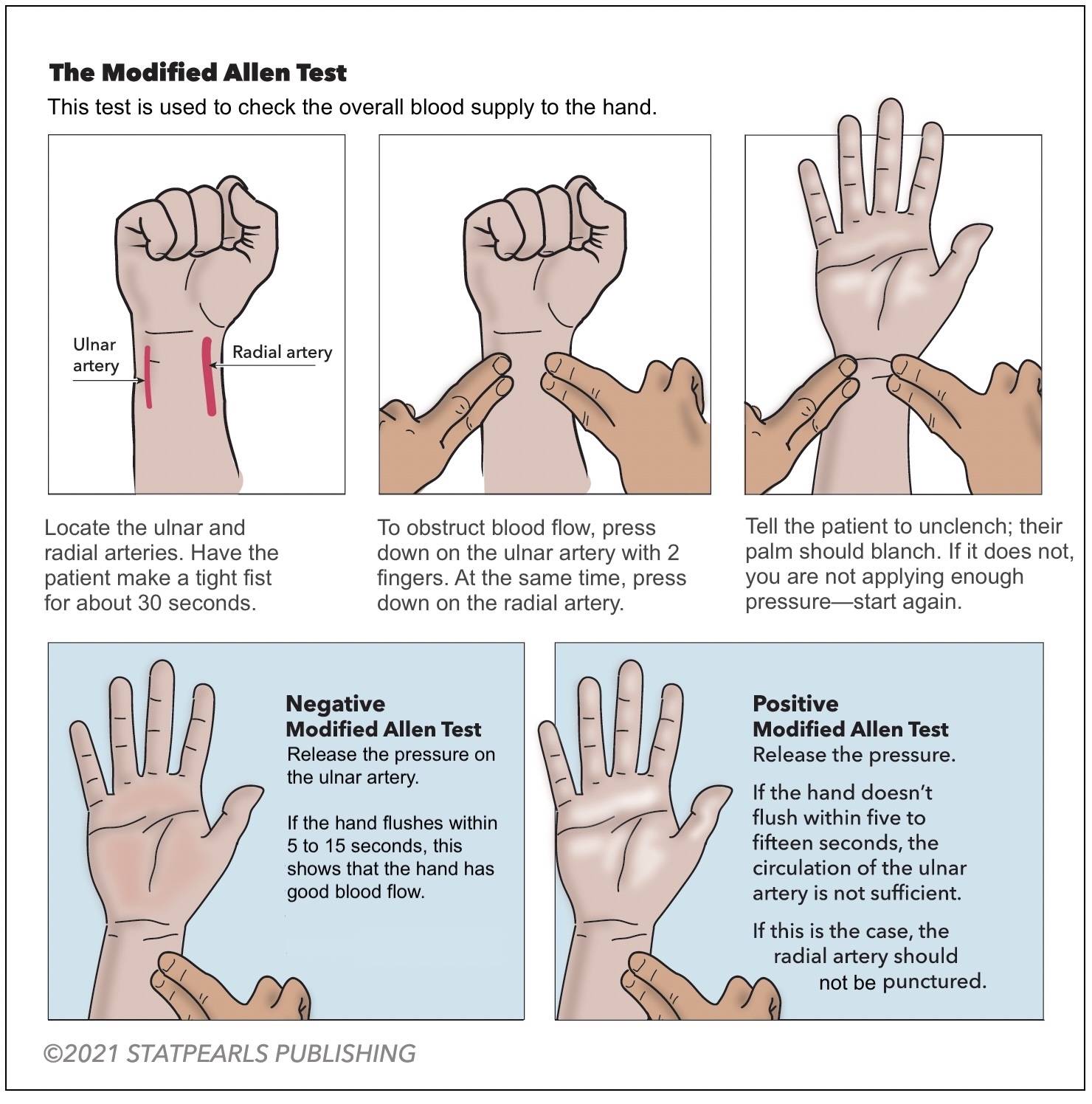
Modified Allen Test. This test is used to check the overall blood supply to the hand.
Illustrated by K Humphreys
References
Gattinoni L, Pesenti A, Matthay M. Understanding blood gas analysis. Intensive care medicine. 2018 Jan:44(1):91-93. doi: 10.1007/s00134-017-4824-y. Epub 2017 May 11 [PubMed PMID: 28497267]
Level 3 (low-level) evidenceBoemke W, Krebs MO, Rossaint R. [Blood gas analysis]. Der Anaesthesist. 2004 May:53(5):471-92; quiz 493-4 [PubMed PMID: 15222335]
Ziegenfuß T, Zander R. Understanding blood gas analysis. Intensive care medicine. 2019 Nov:45(11):1684-1685. doi: 10.1007/s00134-019-05688-w. Epub 2019 Aug 7 [PubMed PMID: 31392344]
Level 3 (low-level) evidenceJubran A. Pulse oximetry. Critical care (London, England). 2015 Jul 16:19(1):272. doi: 10.1186/s13054-015-0984-8. Epub 2015 Jul 16 [PubMed PMID: 26179876]
Kumar V, Karon BS. Comparison of measured and calculated bicarbonate values. Clinical chemistry. 2008 Sep:54(9):1586-7. doi: 10.1373/clinchem.2008.107441. Epub [PubMed PMID: 18755915]
Level 3 (low-level) evidenceMatoušovic K, Havlín J, Schück O. [Clinical evaluation of acid-base status: Henderson-Hasselbalch, or Stewart-Fencl approach?]. Casopis lekaru ceskych. 2016 Winter:155(7):365-369 [PubMed PMID: 27990831]
Kim Y, Massie L, Murata GH, Tzamaloukas AH. Discrepancy between Measured Serum Total Carbon Dioxide Content and Bicarbonate Concentration Calculated from Arterial Blood Gases. Cureus. 2015 Dec 7:7(12):e398. doi: 10.7759/cureus.398. Epub 2015 Dec 7 [PubMed PMID: 26824002]
Hopkins SR. Ventilation/Perfusion Relationships and Gas Exchange: Measurement Approaches. Comprehensive Physiology. 2020 Jul 8:10(3):1155-1205. doi: 10.1002/cphy.c180042. Epub 2020 Jul 8 [PubMed PMID: 32941684]
Dev SP, Hillmer MD, Ferri M. Videos in clinical medicine. Arterial puncture for blood gas analysis. The New England journal of medicine. 2011 Feb 3:364(5):e7. doi: 10.1056/NEJMvcm0803851. Epub [PubMed PMID: 21288091]
Malatesha G, Singh NK, Bharija A, Rehani B, Goel A. Comparison of arterial and venous pH, bicarbonate, PCO2 and PO2 in initial emergency department assessment. Emergency medicine journal : EMJ. 2007 Aug:24(8):569-71 [PubMed PMID: 17652681]
Magnet FS, Majorski DS, Callegari J, Schwarz SB, Schmoor C, Windisch W, Storre JH. Capillary PO(2) does not adequately reflect arterial PO(2) in hypoxemic COPD patients. International journal of chronic obstructive pulmonary disease. 2017:12():2647-2653. doi: 10.2147/COPD.S140843. Epub 2017 Sep 6 [PubMed PMID: 28919732]
Hill S, Moore S. Arterial blood gas sampling: using a safety and pre-heparinised syringe. British journal of nursing (Mark Allen Publishing). 2018 Jul 26:27(14):S20-S26. doi: 10.12968/bjon.2018.27.14.S20. Epub [PubMed PMID: 30048173]
Higgins C. The use of heparin in preparing samples for blood-gas analysis. MLO: medical laboratory observer. 2007 Oct:39(10):16-8, 20; quiz 22-3 [PubMed PMID: 18018679]
Jiang HX. [The effect of dilution and heparin on the blood gas analysis]. Zhonghua jie he he hu xi za zhi = Zhonghua jiehe he huxi zazhi = Chinese journal of tuberculosis and respiratory diseases. 1992 Aug:15(4):225-7, 255-6 [PubMed PMID: 1307518]
Sood P, Paul G, Puri S. Interpretation of arterial blood gas. Indian journal of critical care medicine : peer-reviewed, official publication of Indian Society of Critical Care Medicine. 2010 Apr:14(2):57-64. doi: 10.4103/0972-5229.68215. Epub [PubMed PMID: 20859488]
Dukić L, Kopčinović LM, Dorotić A, Baršić I. Blood gas testing and related measurements: National recommendations on behalf of the Croatian Society of Medical Biochemistry and Laboratory Medicine. Biochemia medica. 2016 Oct 15:26(3):318-336 [PubMed PMID: 27812301]
Knowles TP, Mullin RA, Hunter JA, Douce FH. Effects of syringe material, sample storage time, and temperature on blood gases and oxygen saturation in arterialized human blood samples. Respiratory care. 2006 Jul:51(7):732-6 [PubMed PMID: 16800906]
Level 1 (high-level) evidenceÇuhadar S, Özkanay-Yörük H, Köseoğlu M, Katırcıoğlu K. Detection of preanalytical errors in arterial blood gas analysis. Biochemia medica. 2022 Jun 15:32(2):020708. doi: 10.11613/BM.2022.020708. Epub [PubMed PMID: 35799987]
Lima-Oliveira G, Lippi G, Salvagno GL, Montagnana M, Picheth G, Guidi GC. Different manufacturers of syringes: a new source of variability in blood gas, acid-base balance and related laboratory test? Clinical biochemistry. 2012 Jun:45(9):683-7. doi: 10.1016/j.clinbiochem.2012.03.007. Epub 2012 Mar 13 [PubMed PMID: 22440459]
Kirubakaran C, Gnananayagam JE, Sundaravalli EK. Comparison of blood gas values in arterial and venous blood. Indian journal of pediatrics. 2003 Oct:70(10):781-5 [PubMed PMID: 14649471]
Beutel BG, Worley C, Zisquit J, Nedeff N. Allen Test. StatPearls. 2026 Jan:(): [PubMed PMID: 29939593]
Rodríguez-Villar S, Poza-Hernández P, Freigang S, Zubizarreta-Ormazabal I, Paz-Martín D, Holl E, Pérez-Pardo OC, Tovar-Doncel MS, Wissa SM, Cimadevilla-Calvo B, Tejón-Pérez G, Moreno-Fernández I, Escario-Méndez A, Arévalo-Serrano J, Valentín A, Do-Vale BM, Fletcher HM, Lorenzo-Fernández JM. Automatic real-time analysis and interpretation of arterial blood gas sample for Point-of-care testing: Clinical validation. PloS one. 2021:16(3):e0248264. doi: 10.1371/journal.pone.0248264. Epub 2021 Mar 10 [PubMed PMID: 33690724]
Level 1 (high-level) evidenceJosé RJ, Preller J. Near-patient testing of potassium levels using arterial blood gas analysers: can we trust these results? Emergency medicine journal : EMJ. 2008 Aug:25(8):510-3. doi: 10.1136/emj.2007.053322. Epub [PubMed PMID: 18660404]
Adekola OO, Soriyan OO, Meka I, Akanmu ON, Olanipekun S, Oshodi TA. The incidence of electrolyte and acid-base abnormalities in critically ill patients using point of care testing (i-STAT portable analyser). Nigerian quarterly journal of hospital medicine. 2012 Apr-Jun:22(2):103-8 [PubMed PMID: 23175907]
Yee J, Frinak S, Mohiuddin N, Uduman J. Fundamentals of Arterial Blood Gas Interpretation. Kidney360. 2022 Aug 25:3(8):1458-1466. doi: 10.34067/KID.0008102021. Epub 2022 Jun 3 [PubMed PMID: 36176645]
Arbiol-Roca A, Imperiali CE, Dot-Bach D, Valero-Politi J, Dastis-Arias M. Stability of pH, Blood Gas Partial Pressure, Hemoglobin Oxygen Saturation Fraction, and Lactate Concentration. Annals of laboratory medicine. 2020 Nov:40(6):448-456. doi: 10.3343/alm.2020.40.6.448. Epub 2020 Jun 17 [PubMed PMID: 32539300]
Cowley NJ, Owen A, Bion JF. Interpreting arterial blood gas results. BMJ (Clinical research ed.). 2013 Jan 16:346():f16. doi: 10.1136/bmj.f16. Epub 2013 Jan 16 [PubMed PMID: 23325867]
Larkin BG, Zimmanck RJ. Interpreting Arterial Blood Gases Successfully. AORN journal. 2015 Oct:102(4):343-54; quiz 355-7. doi: 10.1016/j.aorn.2015.08.002. Epub [PubMed PMID: 26411819]
Rogers KM, McCutcheon K. Four steps to interpreting arterial blood gases. Journal of perioperative practice. 2015 Mar:25(3):46-52 [PubMed PMID: 26016282]
Romanski SO. Interpreting ABGs in four easy steps (continuing education credit). Nursing. 1986 Sep:16(9):58-64 [PubMed PMID: 3638536]
Seifter JL. Integration of acid-base and electrolyte disorders. The New England journal of medicine. 2014 Nov 6:371(19):1821-31. doi: 10.1056/NEJMra1215672. Epub [PubMed PMID: 25372090]
ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012 Jun 20:307(23):2526-33. doi: 10.1001/jama.2012.5669. Epub [PubMed PMID: 22797452]
Pediatric Acute Lung Injury Consensus Conference Group. Pediatric acute respiratory distress syndrome: consensus recommendations from the Pediatric Acute Lung Injury Consensus Conference. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies. 2015 Jun:16(5):428-39. doi: 10.1097/PCC.0000000000000350. Epub [PubMed PMID: 25647235]
Level 3 (low-level) evidenceRawat M, Chandrasekharan PK, Williams A, Gugino S, Koenigsknecht C, Swartz D, Ma CX, Mathew B, Nair J, Lakshminrusimha S. Oxygen saturation index and severity of hypoxic respiratory failure. Neonatology. 2015:107(3):161-6 [PubMed PMID: 25592054]
Level 3 (low-level) evidenceKurt OK, Alpar S, Sipit T, Guven SF, Erturk H, Demirel MK, Korkmaz M, Hayran M, Kurt B. The diagnostic role of capnography in pulmonary embolism. The American journal of emergency medicine. 2010 May:28(4):460-5. doi: 10.1016/j.ajem.2009.01.031. Epub 2010 Jan 28 [PubMed PMID: 20466226]
Wagner PD. The physiological basis of pulmonary gas exchange: implications for clinical interpretation of arterial blood gases. The European respiratory journal. 2015 Jan:45(1):227-43. doi: 10.1183/09031936.00039214. Epub 2014 Oct 16 [PubMed PMID: 25323225]
Nichols JH. Quality in point-of-care testing. Expert review of molecular diagnostics. 2003 Sep:3(5):563-72 [PubMed PMID: 14510177]
Level 2 (mid-level) evidenceO'Shaughnessy P, Emancipater K, Hsu C. An assessment of quality control testing in an emergency department (ED) maintained arterial blood gas analyzer. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2000 Oct:7(10):1168 [PubMed PMID: 11015269]
Ehrmeyer SS, Laessig RH. Has compliance with CLIA requirements really improved quality in US clinical laboratories? Clinica chimica acta; international journal of clinical chemistry. 2004 Aug 2:346(1):37-43 [PubMed PMID: 15234634]
Level 2 (mid-level) evidence. Final CLIA regulations. Clinical Laboratory Improvement Amendments. Health devices. 1992 Nov:21(11):420-5 [PubMed PMID: 1428896]
Dunn SG. Point-of-care testing: the impact of CLIA regulations on your testing program. The Journal of medical practice management : MPM. 2007 May-Jun:22(6):341-5 [PubMed PMID: 17612308]
Tucker AM, Johnson TN. Acid-base disorders: A primer for clinicians. Nutrition in clinical practice : official publication of the American Society for Parenteral and Enteral Nutrition. 2022 Oct:37(5):980-989. doi: 10.1002/ncp.10881. Epub 2022 Jun 25 [PubMed PMID: 35752932]
Dukić L, Simundić AM. Institutional practices and policies in acid-base testing: a self reported Croatian survey study on behalf of the Croatian society of medical biochemistry and laboratory medicine Working Group for acid-base balance. Biochemia medica. 2014:24(2):281-92. doi: 10.11613/BM.2014.031. Epub 2014 Jun 15 [PubMed PMID: 24969922]
Level 3 (low-level) evidenceDavis MD, Walsh BK, Sittig SE, Restrepo RD. AARC clinical practice guideline: blood gas analysis and hemoximetry: 2013. Respiratory care. 2013 Oct:58(10):1694-703. doi: 10.4187/respcare.02786. Epub 2013 Jul 30 [PubMed PMID: 23901131]
Level 1 (high-level) evidenceAlbert TJ, Swenson ER. Circumstances When Arterial Blood Gas Analysis Can Lead Us Astray. Respiratory care. 2016 Jan:61(1):119-21. doi: 10.4187/respcare.04556. Epub [PubMed PMID: 26682966]