Introduction
An aortopulmonary septal defect, also known as an aortopulmonary window, is among the rarest congenital heart defects, accounting for 0.1% to 0.6% of all congenital heart diseases.[1][2] This anomaly may occur in isolation or in combination with other congenital heart lesions, including ventricular septal defects, interrupted aortic arch, tetralogy of Fallot, and, rarely, coronary artery anomalies.[3][4][5][6][7]
By definition, an aortopulmonary window is a direct side-to-side connection between the ascending aorta and the main pulmonary artery, with the formation of a normal aortic valve and intact right ventricular outflow tract, distinguishing it from truncus arteriosus (see Video. Color Doppler Echocardiogram of Aortopulmonary Window).[8] Embryologically, an aortopulmonary window arises from incomplete septation of the conotruncal region, secondary to the failure of opposing conotruncal ridges to fuse.[9]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Aortopulmonary windows account for less than 0.6% of all congenital heart defects. Approximately 50% of cases are associated with additional congenital heart lesions, including other conotruncal defects (eg, tetralogy of Fallot, interrupted aortic arch, and D-transposition of the great arteries), coarctation of the aorta, ventricular septal defects, coronary artery anomalies, and tricuspid atresia.[10][11][12] Recent reports have identified anomalies involving the pulmonary arteries. Discontinuous pulmonary arteries may coexist with aortopulmonary windows.[13][14][15] Although these abnormal connections appear similar to other conotruncal malformations embryologically, the association with DiGeorge syndrome is unexpectedly low.[16] This finding suggests that aortopulmonary windows are not linked to abnormalities in cardiac neural crest development.[17]
Epidemiology
An aortopulmonary window is a rare congenital heart defect, occurring in less than 0.6% of all congenital heart defects. Genetic associations include VACTERL syndrome (vertebral defects, anal atresia, cardiac defects, tracheoesophageal fistula, renal anomalies, limb abnormalities), Bohring-Opitz syndrome, and Goldenhar syndrome. No maternal exposures have been identified as causative factors.[18][19]
Pathophysiology
An aortopulmonary window arises during embryonic development from the incomplete septation of the common arterial trunk, creating an abnormal communication between the ascending aorta and the main pulmonary artery. The aortic and pulmonary semilunar valves form normally in an isolated aortopulmonary window.[20] The defect is located between the semilunar valves and the branch pulmonary arteries. Several anatomic classifications exist, with the most commonly used system dividing the defect into 3 types—type 1 (proximal defect), type 2 (distal defect), and type 3 (total defect with complete absence of the aortopulmonary septum).[21][22] Type 1 is the most common form of aortopulmonary window. The size of the connection is variable but typically large, unrestrictive, and hemodynamically significant. The aortopulmonary window is small and pressure-restrictive in less than 10% of cases.[23]
History and Physical
Diagnosis of an isolated aortopulmonary window is possible in utero using fetal echocardiography.[24] The more typical presentation occurs in the neonatal period or early infancy.[25][26][27]
Clinical manifestations result from pulmonary overcirculation as pulmonary vascular resistance (PVR) decreases over the first weeks of life. This hemodynamic change produces a large left-to-right shunt. Common symptoms include diaphoresis, particularly with feeding; tachypnea; tachycardia; poor weight gain; and exacerbation of respiratory symptoms during viral infections.
Physical examination often reveals a hyperdynamic precordium and a mitral valve rumble. Peripheral pulses are frequently bounding due to decreased systemic diastolic blood pressure secondary to aortic flow reversal in diastole. A continuous murmur is uncommon because the aortopulmonary connection is typically large, preventing the development of a significant pressure gradient.
An aortopulmonary window can be associated with other types of congenital heart defects, and the coexisting defect can modify the clinical presentation. A pulmonary ejection murmur and a pulmonary valve click may be observed when combined with tetralogy of Fallot.
Neonates can present with cardiogenic shock as the ductus arteriosus constricts when the aortopulmonary window occurs with an interrupted aortic arch or severe coarctation of the aorta.[28] Less frequently, the aortopulmonary window can be restrictive and produce milder symptoms of pulmonary overcirculation. In these cases, a continuous heart murmur may be present.
Rarely, diagnosis of an aortopulmonary window is delayed until later childhood or adulthood. Late presentation can include features of Eisenmenger syndrome, such as cyanosis and clubbing.[29][30][31] Detailed hemodynamic evaluation remains essential in late presenters, as some patients may remain candidates for repair if PVR is acceptable, or an appropriate response is observed during vasodilator testing.[32][33]
Evaluation
Diagnosis of an aortopulmonary window is established by echocardiography after suspicion of a large left-to-right shunt. The connection is usually nonrestrictive, and color Doppler echocardiography typically does not detect a high-velocity jet. High clinical suspicion warrants evaluation with two-dimensional imaging, which is generally sufficient to assess aortopulmonary window communication (see Video. Subcostal Echocardiogram of Aortopulmonary Window). If echocardiographic imaging is inadequate, computed tomography can delineate the aortopulmonary window (see Image. Three-Dimensional Computed Tomography Reconstruction of Aortopulmonary Window). Computed tomography angiography also detects coronary anomalies that may not be well visualized on echocardiography, reducing the risk of intraoperative complications if overlooked during preoperative assessment.
Echocardiography further identifies associated lesions, including tetralogy of Fallot, atrial septal defects, ventricular septal defects, coarctation of the aorta, and interrupted aortic arch. Cardiac catheterization typically contributes little to diagnosis in infants. In late presentations, particularly in patients with cyanosis, catheterization is used to evaluate PVR in patients with Eisenmenger physiology. Pulmonary reactivity testing during catheterization determines the feasibility of surgical repair.[34]
Chest radiography typically demonstrates cardiomegaly and increased pulmonary vascular markings. Electrocardiography shows tachycardia and increased right- and left-sided voltages.
Treatment / Management
Surgical intervention is recommended at the time of diagnosis because little physiological adaptation occurs, and the risk of developing irreversible pulmonary hypertension increases over time. The aortopulmonary window remains nonrestrictive and does not become hemodynamically less significant with age. Surgical repair involves separating the great arteries with suture division or patch closure of the aorta and the main pulmonary artery. Outcomes are generally favorable when repair is performed early in infancy, with low surgical mortality.[35][36] Concomitant cardiac defects should be corrected or palliated during the same operation. Smaller aortopulmonary windows may be closed primarily using double ligation or suture closure, with low surgical mortality.[37][38] The presence of associated congenital heart disease increases surgical complexity and may worsen outcomes.(B2)
Catheter-based closure of aortopulmonary windows using double-disk devices, including atrial septal defect and patent ductus arteriosus (PDA) devices, has been reported in case studies for defects that are typically restrictive, permitting closure later in childhood.[39][40][41] Postoperative stenosis of the aorta or pulmonary arteries, including the main pulmonary and branch pulmonary arteries, may occur. Hemodynamically significant stenosis may be treated with subsequent cardiac catheterization using balloon angioplasty or stent implantation. Transcatheter aortic interventions may be required for residual arch obstruction in patients undergoing interrupted aortic arch repair.[42](B2)
Medical management before surgery may involve anticongestive medications such as diuretics (eg, furosemide and chlorothiazide). Digoxin can provide temporary symptomatic improvement but does not significantly alter disease progression. Afterload reduction with angiotensin-converting enzyme inhibitors may be considered. Medical therapy requires caution due to potential abnormal renal perfusion.
Differential Diagnosis
Truncus arteriosus is the lesion most frequently mistaken for an aortopulmonary window, but it has a single truncal valve rather than 2 separate semilunar valves. Early pathophysiology of truncus arteriosus resembles that of an aortopulmonary window. Large PDA devices produce comparable hemodynamics. A window-type PDA connects the proximal descending aorta to the left pulmonary artery near the bifurcation. In contrast, an aortopulmonary window connects the ascending aorta to the main pulmonary artery. Large ventricular septal defects produce similar physiological effects but can be readily distinguished from an aortopulmonary window based on anatomical location and valve morphology.
Prognosis
The prognosis for an isolated aortopulmonary window is favorable when early surgical closure is performed, and the development of pulmonary vascular disease is prevented. Late diagnosis can result in pulmonary hypertension and Eisenmenger syndrome, which carry a poor prognosis. The presence of an aortopulmonary window associated with other congenital heart lesions increases surgical complexity and may adversely affect outcomes.
Complications
Complications of a missed diagnosis include the development of Eisenmenger syndrome.[43] Surgical repair may be associated with residual defects, including branch pulmonary artery stenosis and residual aortopulmonary window, which may require future intervention.[44] Recurrent laryngeal nerve injury should be considered in cases of postoperative hoarseness or choking during feeding.[45]
Consultations
Management of an aortopulmonary window requires an interprofessional team approach. Consultation should include cardiology, cardiac surgery, and cardiac intensive care to optimize patient outcomes.
Pearls and Other Issues
Diagnosis of an aortopulmonary window is typically established by echocardiography. High clinical suspicion of a large left-to-right shunt and bounding pulses should prompt targeted echocardiographic evaluation. Late repair of an aortopulmonary window carries a risk of persistent pulmonary hypertension, and preoperative cardiac catheterization is recommended before delayed repair. A low threshold for postoperative catheterization is advised to assess PVR. Early surgical repair of an aortopulmonary window generally yields an excellent long-term prognosis.
Enhancing Healthcare Team Outcomes
An aortopulmonary window is a rare congenital anomaly featuring a direct communication between the ascending aorta and the main pulmonary artery, usually with normally formed semilunar valves. Significant shunting leads to pulmonary overcirculation, left-sided volume overload, and, if untreated, progressive pulmonary hypertension or Eisenmenger physiology. Neonates may present with tachypnea, diaphoresis, poor weight gain, or heart failure, while late presentations include cyanosis and pulmonary vascular disease. Diagnosis relies on echocardiography, with computed tomography or catheterization used for anatomical clarification or hemodynamic assessment. Early surgical repair is the definitive treatment to prevent irreversible pulmonary complications.
Optimal outcomes require an interprofessional team including pediatric cardiologists, cardiac surgeons, pediatric anesthesiologists, pediatric cardiac intensivists, and pediatric radiologists. Cardiac and critical care nurses provide postoperative monitoring, pharmacists manage medications, and specialty care nurses coordinate care and educate families. Lifelong cardiology follow-up is recommended to identify late complications, thereby enhancing patient safety, supporting recovery, and improving long-term outcomes.
Media
(Click Video to Play)
Color Doppler Echocardiogram of Aortopulmonary Window. Color Doppler echocardiogram of an aortopulmonary window demonstrating the flow between the aorta and main pulmonary artery.
Contributed by P Shivaram, MD
(Click Video to Play)
Subcostal Echocardiogram of Aortopulmonary Window. This two-dimensional video of the aortopulmonary window is shown from the subcostal view.
PA, pulmonary artery; Ao, Aorta.
Contributed by P Shivaram, MD
(Click Image to Enlarge)
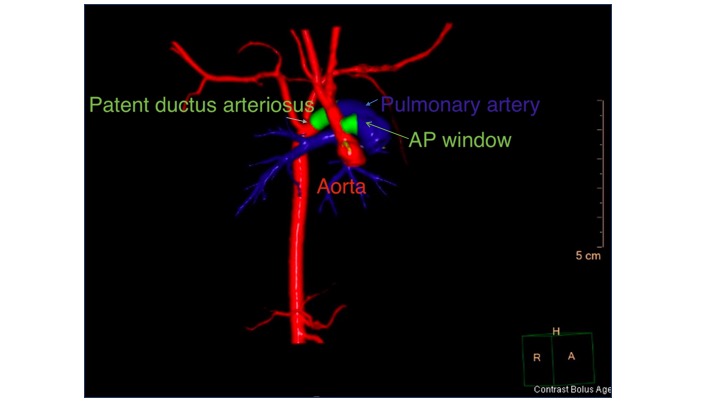
Three-Dimensional Computed Tomography Reconstruction of Aortopulmonary Window. The ascending aorta is shown in red, the main pulmonary artery in blue, and the aortopulmonary window is highlighted in green to delineate the abnormal connection.
AP, aortopulmonary.
Contributed by M Law, MD
References
Samánek M, Vorísková M. Congenital heart disease among 815,569 children born between 1980 and 1990 and their 15-year survival: a prospective Bohemia survival study. Pediatric cardiology. 1999 Nov-Dec:20(6):411-7 [PubMed PMID: 10556387]
Verma M, Pandey NN, Ramakrishnan S, Jagia P. Evaluation of aortopulmonary window using virtual dissection of multidetector computed tomography angiography data sets. Journal of cardiac surgery. 2022 Dec:37(12):4475-4484. doi: 10.1111/jocs.17075. Epub 2022 Nov 2 [PubMed PMID: 36321703]
Prabhu S, Keshav M, Ramachandra P, Raj V, John C, Karl TR. Tetralogy of Fallot with pulmonary atresia and aortopulmonary window may mimic common arterial trunk. Cardiology in the young. 2022 Mar:32(3):410-414. doi: 10.1017/S1047951121002298. Epub 2021 Jun 17 [PubMed PMID: 34134806]
Sondhi S, Negi PC, Sharma R, Mehta A. Aortopulmonary window with pumonary atresia with ventricular septal defect with D-transposition of great arteries: extremely rare anomaly. BMJ case reports. 2018 Jun 13:2018():. pii: bcr-2018-224401. doi: 10.1136/bcr-2018-224401. Epub 2018 Jun 13 [PubMed PMID: 29898907]
Level 3 (low-level) evidenceBin-Moallim M, Hamadah HK, Alhabshan F, Alghamdi AA, Kabbani MS. Aortopulmonary window: Types, associated cardiovascular anomalies, and surgical outcome. Retrospective analysis of a single center experience. Journal of the Saudi Heart Association. 2020:32(2):127-133. doi: 10.37616/2212-5043.20. Epub 2020 May 10 [PubMed PMID: 33154906]
Level 2 (mid-level) evidenceAlakhfash AA, Tagelden M, Almesned A, Alqwaiee A. Aortopulmonary window with anomalous right coronary artery from the pulmonary artery. Case report and literature review. Cardiology in the young. 2020 Jan:30(1):47-49. doi: 10.1017/S1047951119002543. Epub 2019 Dec 19 [PubMed PMID: 31854282]
Level 3 (low-level) evidenceGrünenfelder J, Zünd G, Vogt PR, Turina MI. Aortopulmonary window with anomalous origin of the right coronary artery. The Annals of thoracic surgery. 1999 Jan:67(1):233-5 [PubMed PMID: 10086558]
Level 3 (low-level) evidenceRajagopal R, Sinha M, Pandey NN, Bhambri K, Kumar S. Tetralogy of fallot with pulmonary atresia and aorto-pulmonary window: Or is it truncus arteriosus? Journal of cardiovascular computed tomography. 2020 Sep-Oct:14(5):e20-e21. doi: 10.1016/j.jcct.2018.10.022. Epub 2018 Oct 26 [PubMed PMID: 30385324]
Spicer DE, Henderson DJ, Chaudhry B, Mohun TJ, Anderson RH. The anatomy and development of normal and abnormal coronary arteries. Cardiology in the young. 2015 Dec:25(8):1493-503. doi: 10.1017/S1047951115001390. Epub [PubMed PMID: 26675596]
Trowitzsch E, Schneider M, Urban A, Asfour B. Congenital pulmonary sling, aorto-pulmonary window and pulmonary vein obstruction as a diagnostic and therapeutic challenge in an infant with VACTERL association. Clinical research in cardiology : official journal of the German Cardiac Society. 2006 Jun:95(6):338-43 [PubMed PMID: 16598388]
Level 3 (low-level) evidenceMilovanovic V, Stefanovic I, Ilic S. Tricuspid atresia associated with aortopulmonary window: diagnostic and therapeutic dilemmas. Cardiology in the young. 2017 Apr:27(3):580-583. doi: 10.1017/S1047951116001499. Epub 2016 Sep 29 [PubMed PMID: 27680574]
Márquez D, Chalela T, Sandoval N. Intraoperative Diagnosis of ALCAPA Complicating an Aortopulmonary Window Repair. World journal for pediatric & congenital heart surgery. 2022 Jan:13(1):92-94. doi: 10.1177/2150135120975761. Epub 2021 Apr 28 [PubMed PMID: 33908835]
Sharma A, Naganur SH, Barwad P, Singhal M. Aortopulmonary window with anomalous ascending aortic origin of left pulmonary artery: Hitherto unreported pattern. Journal of cardiac surgery. 2022 Nov:37(11):3870-3871. doi: 10.1111/jocs.16900. Epub 2022 Sep 6 [PubMed PMID: 36066047]
Verma M, Pandey NN, Kumar S, Ramakrishnan S. An unusual case of aortopulmonary window with crossed pulmonary arteries. Journal of cardiac surgery. 2022 Feb:37(2):451-452. doi: 10.1111/jocs.16160. Epub 2021 Nov 29 [PubMed PMID: 34842305]
Level 3 (low-level) evidenceFan Q, Ling Y, Wang Y, An Q. A large aortopulmonary window found in the setting of a right aortic arch with discontinuous pulmonary arteries. Journal of cardiac surgery. 2021 Feb:36(2):696-697. doi: 10.1111/jocs.15136. Epub 2020 Dec 6 [PubMed PMID: 33283308]
Van Mierop LH, Kutsche LM. Cardiovascular anomalies in DiGeorge syndrome and importance of neural crest as a possible pathogenetic factor. The American journal of cardiology. 1986 Jul 1:58(1):133-7 [PubMed PMID: 3728313]
Kutsche LM, Van Mierop LH. Anatomy and pathogenesis of aorticopulmonary septal defect. The American journal of cardiology. 1987 Feb 15:59(5):443-7 [PubMed PMID: 3812313]
Verma B, Abhinay A, Singh A, Kumar M. Double outlet right ventricle and aortopulmonary window in a neonate with Bohring-Opitz (Oberklaid-Danks) syndrome: First case report. Journal of family medicine and primary care. 2019 Mar:8(3):1279-1281. doi: 10.4103/jfmpc.jfmpc_74_19. Epub [PubMed PMID: 31041292]
Level 3 (low-level) evidenceForeman K, Miller L, Kumar SR, Uzunyan M. Aortopulmonary window, aortic arch interruption, and anomalous origin of the right pulmonary artery in a neonate with Goldenhar syndrome. Cardiology in the young. 2023 Jun:33(6):995-997. doi: 10.1017/S1047951122003031. Epub 2022 Oct 18 [PubMed PMID: 36254527]
Jacobs JP, Quintessenza JA, Gaynor JW, Burke RP, Mavroudis C. Congenital Heart Surgery Nomenclature and Database Project: aortopulmonary window. The Annals of thoracic surgery. 2000 Apr:69(4 Suppl):S44-9 [PubMed PMID: 10798415]
Mori K, Ando M, Takao A, Ishikawa S, Imai Y. Distal type of aortopulmonary window. Report of 4 cases. British heart journal. 1978 Jun:40(6):681-9 [PubMed PMID: 656242]
Level 3 (low-level) evidenceCairello F, Nuri HA, Marasini M. Aortopulmonary window and coronary anatomy - still a pre-operative diagnostic trouble! Cardiology in the young. 2022 Dec:32(12):2027-2028. doi: 10.1017/S1047951122000981. Epub 2022 May 11 [PubMed PMID: 35538626]
Awasthy N, Jawid SA. Aortopulmonary Window with Crisscross Pulmonary Arteries: Anatomically Type 1, Physiologically Type 2. Journal of cardiovascular echography. 2017 Oct-Dec:27(4):143-144. doi: 10.4103/jcecho.jcecho_12_17. Epub [PubMed PMID: 29142813]
Bhalgat PS, Nabi F, Ray S. Aortopulmonary window: Clues to fetal diagnosis. Annals of pediatric cardiology. 2021 Apr-Jun:14(2):247-248. doi: 10.4103/apc.APC_42_20. Epub 2021 Feb 16 [PubMed PMID: 34103873]
Tongprasert F, Sittiwangkul R, Jatavan P, Tongsong T. Prenatal Diagnosis of Aortopulmonary Window: A Case Series and Literature Review. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2017 Aug:36(8):1733-1738. doi: 10.7863/ultra.16.08025. Epub 2017 Apr 10 [PubMed PMID: 28393388]
Level 2 (mid-level) evidenceCollinet P, Chatelet-Cheront C, Houze de l'Aulnoit D, Rey C. Prenatal diagnosis of an aorto-pulmonary window by fetal echocardiography. Fetal diagnosis and therapy. 2002 Sep-Oct:17(5):302-7 [PubMed PMID: 12169817]
Level 3 (low-level) evidenceDemir IH, Erdem A, Sarıtaş T, Demir F, Erol N, Yücel IK, Aydemir NA, Celebi A. Diagnosis, treatment and outcomes of patients with aortopulmonary window. Balkan medical journal. 2013 Jun:30(2):191-6. doi: 10.5152/balkanmedj.2013.6995. Epub 2013 Jun 1 [PubMed PMID: 25207099]
Gužvinec P, Muscogiuri G, Hrabak-Paar M. CT Assessment of Aortopulmonary Septal Defect: How to Approach It? Journal of clinical medicine. 2024 Jun 15:13(12):. doi: 10.3390/jcm13123513. Epub 2024 Jun 15 [PubMed PMID: 38930042]
Chen J, Guo J, Cao S. Unexplained pulmonary hypertension: an overlooked aortopulmonary window. European heart journal. 2020 Mar 14:41(11):1217. doi: 10.1093/eurheartj/ehaa021. Epub [PubMed PMID: 32034904]
Myers PO, Lador F, Hachulla AL, Bouchardy J, Noble S, Licker M, Pache JC, Kalimanovaska-Ostric D, Djukic M, Kalangos A, Beghetti M. Unrestrictive Aortopulmonary Window: Extreme Presentation as Non-Eisenmenger in a 30-Year-Old Patient. Circulation. 2016 May 10:133(19):1907-10. doi: 10.1161/CIRCULATIONAHA.115.020819. Epub [PubMed PMID: 27166350]
Dev M, Sharma M, Rana N. Large Unrepaired Aortopulmonary Window Presenting in Adulthood. Current cardiology reviews. 2020:16(1):73-76. doi: 10.2174/1573403X15666190513105231. Epub [PubMed PMID: 31092183]
Talwar S, Siddharth B, Gupta SK, Choudhary SK, Kothari SS, Juneja R, Saxena A, Airan B. Aortopulmonary window: results of repair beyond infancy. Interactive cardiovascular and thoracic surgery. 2017 Nov 1:25(5):740-744. doi: 10.1093/icvts/ivx158. Epub [PubMed PMID: 28633352]
Das D, Dutta N, Das P, Sharma MK, Koley R, Das S, Chattopadhyay A, Ghosh S, Narayan P. Late presentation of aortopulmonary window: a contemporary series. Indian journal of thoracic and cardiovascular surgery. 2022 Jul:38(4):403-407. doi: 10.1007/s12055-021-01306-x. Epub 2022 Jan 8 [PubMed PMID: 35756557]
Zografos PM, Protopapas EM, Hakim NI, Alexopoulos C, Sarris GE. Remarkably Still Repairable Large Aortopulmonary Window in an Adult Patient. World journal for pediatric & congenital heart surgery. 2020 Jan:11(1):117-119. doi: 10.1177/2150135119878703. Epub 2019 Nov 22 [PubMed PMID: 31755375]
Gangana CS, Malheiros AF, Alves EV, de Azevedo MA, Bernardes RM, Simões LC. Aortopulmonary window--impact of associated lesions on surgical results. Arquivos brasileiros de cardiologia. 2007 Apr:88(4):402-7 [PubMed PMID: 17546268]
Level 2 (mid-level) evidenceReddy C, Kaskar A, Karthick E, Siddaiah S, Kiran VS, Suresh P. Surgical Management of Aortopulmonary Window and its Associated Cardiac Lesions. World journal for pediatric & congenital heart surgery. 2022 May:13(3):334-340. doi: 10.1177/21501351221077888. Epub [PubMed PMID: 35446205]
Gowda D, Gajjar T, Rao JN, Chavali P, Sirohi A, Pandarinathan N, Desai N. Surgical management of aortopulmonary window: 24 years of experience and lessons learned. Interactive cardiovascular and thoracic surgery. 2017 Aug 1:25(2):302-309. doi: 10.1093/icvts/ivx099. Epub [PubMed PMID: 28475712]
Talwar S, Agarwal P, Choudhary SK, Kothari SS, Juneja R, Saxena A, Airan B. Aortopulmonary window: Morphology, diagnosis, and long-term results. Journal of cardiac surgery. 2017 Feb:32(2):138-144. doi: 10.1111/jocs.12936. Epub 2017 Jan 30 [PubMed PMID: 28139013]
Uçar T, Karagözlü S, Ramoğlu MG, Tutar E. Transcatheter closure of aortopulmonary window with Amplatzer duct occluder II: additional size. Cardiology in the young. 2020 Mar:30(3):424-426. doi: 10.1017/S1047951119003342. Epub 2020 Jan 13 [PubMed PMID: 31928548]
Trehan V, Nigam A, Tyagi S. Percutaneous closure of nonrestrictive aortopulmonary window in three infants. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions. 2008 Feb 15:71(3):405-11. doi: 10.1002/ccd.21366. Epub [PubMed PMID: 18288731]
Level 3 (low-level) evidenceGuzeltas A, Ugan Atik S, Tanidir IC. Transcatheter Closure of Aortopulmonary Window in Infants with Amplatzer Duct Occluder-I. Acta Cardiologica Sinica. 2021 May:37(3):305-308. doi: 10.6515/ACS.202105_37(3).20201019A. Epub [PubMed PMID: 33976514]
Konstantinov IE, Karamlou T, Williams WG, Quaegebeur JM, del Nido PJ, Spray TL, Caldarone CA, Blackstone EH, McCrindle BW, Congenital Heart Surgeons Society. Surgical management of aortopulmonary window associated with interrupted aortic arch: a Congenital Heart Surgeons Society study. The Journal of thoracic and cardiovascular surgery. 2006 May:131(5):1136-1141.e2 [PubMed PMID: 16678601]
Level 2 (mid-level) evidenceEl Dick J, El-Rassi I, Tayeh C, Bitar F, Arabi M. Aortopulmonary window in adults: A rare entity leading to Eisenmenger syndrome. Echocardiography (Mount Kisco, N.Y.). 2019 Jun:36(6):1173-1178. doi: 10.1111/echo.14368. Epub 2019 May 22 [PubMed PMID: 31116466]
Barnes ME, Mitchell ME, Tweddell JS. Aortopulmonary window. Seminars in thoracic and cardiovascular surgery. Pediatric cardiac surgery annual. 2011:14(1):67-74. doi: 10.1053/j.pcsu.2011.01.017. Epub [PubMed PMID: 21444051]
Condon LM, Katkov H, Singh A, Helseth HK. Cardiovocal syndrome in infancy. Pediatrics. 1985 Jul:76(1):22-5 [PubMed PMID: 4011354]
Level 3 (low-level) evidence