Introduction
The anterior spinal artery (ASA) is the principal longitudinal arterial trunk supplying the anterior 2/3 of the spinal cord, encompassing the anterior horns, corticospinal tracts, and spinothalamic pathways (see Image. Anterior Spinal Artery). This blood vessel typically arises from bilateral rami of the intracranial V4 segments of the vertebral arteries, which fuse near the pyramidal decussation and descend within the anterior median sulcus. Segmental reinforcement occurs via radiculomedullary arteries, with characteristic cervical and thoracolumbar enlargements.
Embryologically, the ASA forms from the fusion of paired ventral longitudinal channels derived from the perineural vascular plexus during neurulation, followed by desegmentation of primitive segmental feeders. Common anatomic variants arise from differences in number, caliber, symmetry, and midline fusion of prespinal rami originating from the intracranial V4 segments of the vertebral arteries near the vertebrobasilar junction.
Detailed knowledge of ASA anatomy, development, and variants is essential in trauma, aortic and spinal surgery, vertebrobasilar interventions, and spinal angiography. Structural understanding permits accurate radiologic interpretation and risk stratification, and informs prevention, recognition, and management of ASA syndrome and related ischemic complications.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The ASA supplies the anterior 2/3 of the spinal cord, accounting for approximately 75% of total spinal cord perfusion.[1] The rami of the ASA arise from the intracranial V4 segment of the vertebral artery distal to the origin of the posterior inferior cerebellar artery (PICA). The ASA most commonly originates from the vertebral arteries prior to their anastomosis forming the basilar artery, fuses at the pyramidal decussation, and follows a recurrent course through the premedullary cistern to reach the cervical cord (see Image. Diagram of the Brain Blood Circulation). Caudally, the ASA forms an arch after anastomosing with the posterior spinal artery (PSA) at the level of the filum terminale.
Svensson, Klepp, and Hinder initially postulated that the ASA represents a continuous vessel arising from the vertebral arteries and extending to the filum terminale. Gharagozloo and colleagues later proposed that the ASA is discontinuous and that spinal cord perfusion occurs segmentally via the vertebral, intercostal, and lumbar arteries.[2] A figure from the same plate depicts small blood vessels coursing over the surface of the cervical spinal cord, possibly representing the first published depiction of ASAs and anterior spinal veins.[3]
The ASA most commonly exhibits a bilateral origin, observed in approximately 75% of cases. Bilateral origins can be further classified by the relative caliber of the contributing rami into balanced (approximately 40%), right-dominated, and left-dominated configurations. Unilateral origins and branching from an intervertebral transverse arch also occur.[4] The distance from the apex of the vertebrobasilar junction to the origin of the ASA averages 7.34 mm (± 2.71 mm), whereas the distance from the PICA origin averages 9.02 mm. The mean caliber of the ASA is 1.145 mm (± 0.12 mm), with the ratio of ASA rami to the vertebral artery measuring 0.17.[5] Both the rami and the ASA within the premedullary cord commonly give rise to multiple perforating branches, averaging 3 per segment.
Anatomically, the ASA and its accompanying vein occupy a subpial location, in contrast to the posterior spinal vessels, which reside within the subarachnoid space.[6] The ASA courses beneath the “linea splendens,” a fasciculated and porous region of epipia covering the anterior median sulcus. This structure permits cerebrospinal fluid to permeate from the subarachnoid space into the pia. The true pia mater, or pia intima, adheres tightly to the glia limitans of the spinal cord and extends to the base of the anterior median sulcus.[7]
The spinal artery divides at the level of the intervertebral foramina into ventral, middle, and dorsal branches. The ventral and dorsal branches supply the dura mater and vertebral bone. The middle branch bifurcates to join the anterior and posterior nerve roots and subsequently forms radicular, radiculopial, and radiculomedullary arteries, as described by Tanon. The radicular artery is short, whereas the radiculopial artery reaches the surface of the spinal cord. The radiculomedullary artery supplies the spinal cord subpially over multiple spinal segments.
Sulcal arteries perfuse the anterior gray matter, the anterior portion of the posterior gray matter, and the inner 1/2 of the white column in a centrifugal pattern. Radial perforating arteries, originating from the PSAs and the pial plexus, supply the posterior portion of the posterior gray matter and the outer half of the white column in a centripetal manner.[8] The ASA thus demonstrates a radiculomedullary pattern of arterial contribution, whereas the PSA network exhibits a radiculopial pattern.
Embryology
Gastrulation is the process by which a single-layered blastula develops into a specialized, multilayered structure.[9][10] The resulting trilaminar structure consists of 3 germ layers: ectoderm, mesoderm, and endoderm. The ectoderm gives rise to the embryological origins of the nervous system, known as the neuroectoderm. The neuroectoderm contributes to the formation of the notochord, which induces the development of the neural plate.
The neural plate arises as a thickening of the ectoderm through a process termed "neurulation." This process is regulated by growth factors derived from the notochord and endoderm, which provide a scaffold for spinal support, along with signals from the mesoderm.[11] The neural plate invaginates to form the neural tube, which separates completely from the neuroectoderm during the 3rd week of development. The spinal cord and brain develop from the neural tube.[12][13]
Cells at the margins of the neural tube form the neural crest, which also originates from the embryonic ectoderm. Additional patterning is mediated by the sonic hedgehog (Shh) ligand and the translation of homeotic (HOX) genes. These molecular signals direct the subsequent development of the vertebral column and the segmentation of the body into a 3-dimensional form.
The primitive spine develops segmentally from blocks of mesoderm located on either side of the notochord, arranged as repeating somites, together with the neural tube. This repetitive organization of segments is referred to as "metamerism." Up to 44 somites form between the 3rd and 6th weeks of development. Subsequent regression reduces this number to 31. Paired segmental, or metameric, arteries arising from the dorsal aorta supply the neural tube and all components of the metameres via their dorsomedial and dorsolateral branches.
Spinal vasculature begins to develop at approximately 23 days, nearly coinciding with closure of the cranial and dorsal neuropores at 25 to 27 days. During the first weeks of embryonic life, the neural tube receives nutrition via diffusion from a perineural primitive vascular plexus, the vasa corona, located within the meninx primitiva. As embryonic metabolism increases, longitudinal capillary tracts develop on either side of the median sulcus from connections within the vasa corona. These tracts are termed "ventral longitudinal arteries." Branches arising from the developing cord enter the sulcus and sprout into the vasa corona. Dorsomedial branches of the segmental arteries supply the ventral longitudinal arteries, the future ASA, and the anterior roots.
Posterior longitudinal channels form later on the dorsolateral surface of the neural tube from the vasa corona plexus and subsequently develop into the PSAs. Final development of the PSAs occurs between the 15th and 20th weeks of gestation. The delayed formation results from the ventral longitudinal arteries supplying most of the gray matter, which precedes the formation of white matter tracts. The emergence of longitudinal arteries supplying multiple metameres shifts the segmental blood supply toward the adult spinal arterial pattern.
Craniocaudal midline fusion of the ventral longitudinal arteries within the neural tube occurs after 6 weeks, forming the ASA. Failures of this fusion can manifest as duplications of the ASA, most commonly within the cervical cord. Desegmentation of the segmental feeders occurs concurrently, with regression of most primitive segmental arteries supplying the neural tube. Upon completion, only 4 to 8 ventral segmental arteries supply the ASA, while 10 to 20 dorsal segmental arteries supply the vasa corona. Segmental arteries that persist as radiculomedullary arteries form “hairpin” connections with the longitudinal tracts and, ultimately, with the ASA. Longitudinal anastomoses between the segmental arteries of each metamere develop around the forming spine. The vertebral artery within its canal represents the most prominent of these longitudinal connections.
Vascularization of tubular organs, including the neural tube, follows the Lierse law of angiogenesis. Primitive anterior tracts course centripetally toward a subependymal vascular plexus, which accompanies a zone of cellular proliferation, or matrix, surrounding the central canal. The subependymal plexus largely regresses by the end of the 8th week. A gradually unstructured pattern of internal vascularization develops thereafter.
The primitive ASA forms during this period, notably as the lumbar trunk. Formation of the anterior median fissure results from proliferation and cellular differentiation within the matrix, combined with expansion of the anterior horn region. Kadyi described a specific role for the primitive meninges, termed the "anterior piae matris," in providing supplementary nutrition to the neural tube via extrinsic supply, distinguishing prechoroidal and choroidal stages. Subsequent intrinsic restructuring establishes a central, or centrifugal, supply through sulcal and sulco-commissural arteries, complementing the extrinsic vascular input, as described by Adamkiewicz.
The formation of primitive ASAs follows the fusion of paired longitudinal neuronal arterial axes. Three primary theories explain the transition from paired arteries to a single vessel. The 1st proposes medial displacement and subsequent fusion of the primitive arteries, mirroring the developmental pattern of the primitive aortae. The 2nd describes the paired longitudinal channels as initially forming a rope-ladder-like pattern with transverse midline anastomoses, after which 1 channel predominates and persists.
The 3rd posits that the primary embryonic vascular tract regresses as metabolic demands increase, followed by the transient reappearance of paired longitudinal tracts through vascularization from the secondary spinal meninges, supplying each hemicord. These mechanisms collectively result in architectural reconfiguration toward an unpaired ASA. The embryological centripetal vascular pattern gradually converts to a centrifugal configuration.[14]
Physiologic Variants
The ASA shows substantial variability in anatomical origins. These differences reflect developmental variation in the fusion and persistence of longitudinal arterial axes.
Type I variants of the ASA involve 2 rami that fuse to form a single vessel. Type Ia represents symmetric prespinal rami, each originating from 1 of the 2 vertebral arteries, which fuse at the anterior median fissure to form a single ASA and constitutes the most common variant. Type Ib consists of 2 rami arising from the vertebral arteries that initially fuse but later divide into 2 separate ASAs descending parallel to the pyramids up to the C3 myelomere. Type Ic involves the formation of a vascular arch by the 2 rami of the vertebral arteries, from which 2 separate ASAs subsequently arise.
Type II variants involve a single ASA arising from 1 of the 2 rami. Type IIa refers to 1 ASA originating from a single ramus. Type IIb occurs when both rami form, but 1 is very short and supplies only the ventral surface of the medulla, with the dominant ramus continuing as the ASA. Type IIc describes 1 dominant ramus forming the main trunk of the ASA, with the smaller ramus joining via an end-to-side anastomosis.
Type III variants consist of 2 independent ASAs arising directly from the vertebral arteries and descending separately to the C3 myelomere. Additional variations include a prespinal artery originating at the convergence of the vertebral arteries, while the other arises directly from a vertebral artery or the anterior inferior cerebellar artery.
Anatomical variations of the ASA can confer morphofunctional advantages by improving spinal cord perfusion when an embolus affects only 1 hemicord, as observed in Brown-Sequard syndrome. These same variations may introduce complications during microvascular or endovascular procedures involving the relevant anatomical territories.[15]
Cadaveric studies demonstrate at least 1 dominant anterior thoracic artery—distinct from the artery of the lumbar (artery of Adamkiewicz at T8–L2 in 75% of cases) and cervical (C5–C6) enlargements—in approximately 95% of individuals. Overlying osseous or muscular branches may obscure these arteries, leading to underreporting in spinal angiography studies. This distribution challenges conventional concepts of watershed zones in the thoracic spinal cord and carries significant implications during trauma, ischemic events, and surgical or endovascular interventions.[16]
Occlusion of the vertebral arteries combined with inadequate collateral circulation via the posterior communicating arteries can result in flow reversal within the ASA through the C4 segmental artery. This flow reversal creates collateral channels.[17][18]
Surgical Considerations
The pattern, site, and distance of the ASA origin from the vertex of the vertebrobasilar junction and the PICA exhibit considerable variability. Awareness of these anatomical relationships is critical for endovascular and microsurgical procedures within this region.[19]
Clinical Significance
Etiologies of Anterior Spinal Artery Injury
Injuries to the ASA may result from a variety of pathological and vascular conditions. Traumatic events can directly disrupt ASA perfusion, leading to ischemia of the anterior 2/3 of the spinal cord.[20] Degenerative spinal pathologies, including spondylosis or disc herniation, can compress or compromise arterial flow. Atherosclerotic disease may reduce luminal diameter and predispose to thrombosis. Cardiac emboli and cardiac arrest can obstruct or reduce ASA perfusion. Systemic hypotension decreases perfusion pressure, increasing susceptibility to ischemic injury.[21]
Aneurysms and pseudoaneurysms may compress or rupture into adjacent ASA branches.[22][23][24][25][26][27] Vasculitis can inflame and occlude the arterial wall. Aortic dissection may extend into the ASA origins, disrupting flow.[28][29] Arteriovenous malformations create steal phenomena, diverting blood away from the ASA.[30] Fibrocartilaginous embolism may occur following intervertebral disc injury.[31][32] Kyphotic deformities combined with posterior osteophytes can mechanically compromise arterial patency.[33] Arterioectatic spinal angiopathy, sickle cell disease, hypercoagulable states, and cocaine abuse also contribute to ASA injury through vascular occlusion, embolism, or vasospasm.[34]
Iatrogenic injuries to the ASA arise from clinical procedures. Spinal anesthesia can directly puncture or compress the ASA branches.[35] Digital subtraction angiographic procedures or microvascular and endovascular interventions in the proximal vertebrobasilar system carry a risk of arterial disruption. Aortic repair surgery may compromise the ASA origin or segmental feeders.[36][37] Kyphoplasty with retropulsion of bone fragments and spinal deformity correction surgeries can mechanically injure the artery or its radiculomedullary branches.[38][39][40]
Complications of ASA injury include ASA syndrome, characterized by motor paralysis and selective sensory deficits (see Image. Clinical Features of Anterior Spinal Artery Syndrome).[41] Acute onset of back pain localized to the level of spinal involvement is a typical finding. Bilateral motor weakness and sensory deficits occur below the affected segment due to compromise of the bilateral corticospinal and spinothalamic tracts. Proprioception, vibratory sense, 2-point discrimination, and fine touch, mediated by the dorsal columns, remain intact because these structures are supplied by the PSAs. Involvement of the lateral horns between the T1 and L2 levels can produce autonomic dysfunction.[42]
The Ondine curse is a form of central hypoventilation characterized by failure of automatic respiration. Cervical ASA compromise can disrupt phrenic nerve function and precipitate this condition.[43]
Imaging of the Anterior Spinal Artery
Spinal angiography remains the gold standard for visualizing the ASA, but the procedure is invasive and requires dedicated, trained personnel. The normal cervical ASA, its continuity, and radiculomedullary feeders is often visualized using magnetic resonance angiography, including maximum-intensity projection and 3-dimensional fast low-angle shot techniques. Limitations of this modality include prolonged acquisition times and difficulty distinguishing the ASA from the anterior median vein.
The hallmark radiological finding of ASA syndrome is hyperintensity involving the anterior 2/3 of the spinal cord on T2-weighted magnetic resonance imaging (MRI) axial images.[44] Peripheral and posterior regions of the cord are relatively spared due to collateral perfusion from the vascular pial plexus and PSAs.[45][46] Paired anterior-horn T2-hyperintensities, termed "owl's eyes," "snake eyes," or "snake bite sign," are also characteristic.[47] These findings reflect cell loss in the anterior horns accompanied by cystic necrosis at the junction of the posterior ventrolateral column and the central grey matter.[48]
A thin, pencil-like hyperintensity may extend vertically across multiple spinal segments in sagittal views. Dense edema can produce a "white cord" sign.[49] MRI can further assist in identifying the underlying cause of ASA syndrome. Differential diagnoses include transverse myelitis, complete spinal cord transection from severe cord edema, central cord syndrome, Guillain-Barré syndrome, Brown-Sequard syndrome in the context of vascular variations, multiple sclerosis, compressive myelopathies, and spinal vasculopathies such as arteriovenous malformations.
Media
(Click Image to Enlarge)
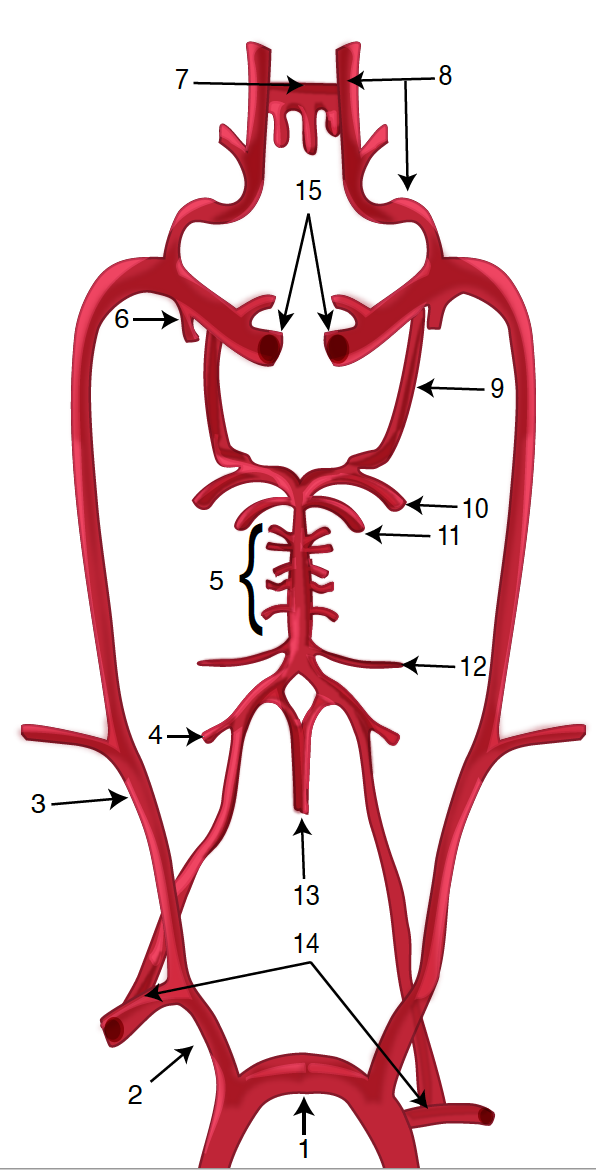
Diagram of the Brain Blood Circulation. Each number corresponds to the following neuroanatomy: 1) aortic arch; 2) brachiocephalic artery; 3) common carotid artery; 4) posterior inferior cerebellar artery; 5) pontine arteries; 6) anterior choroidal artery; 7) anterior communicating artery; 8) anterior cerebral artery; 9) posterior communicating artery; 10) posterior cerebral artery; 11) superior cerebellar artery; 12) anterior inferior cerebellar artery; 13) anterior spinal artery; 14) arches of vertebral arteries; and 15) internal carotid arteries.
Contributed by O Kuybu, MD
(Click Image to Enlarge)
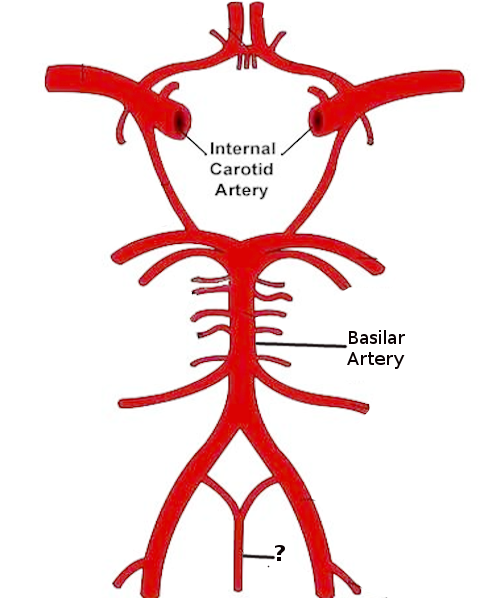
Anterior Spinal Artery. This diagram illustrates the major arterial supply to the brain, including the internal carotid and basilar arteries. The structure marked with a question mark at the base is the anterior spinal artery.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
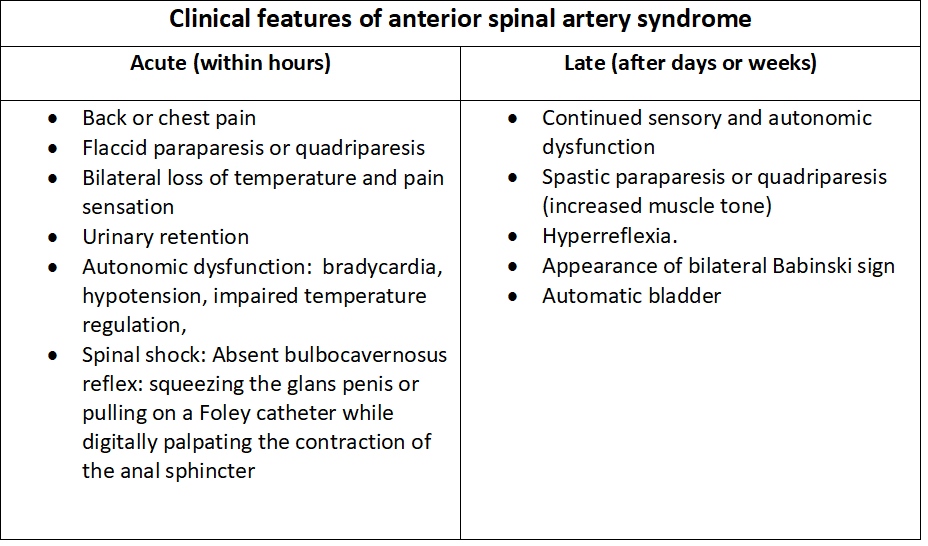
Clinical Features of Anterior Spinal Artery Syndrome. This table details the progression of symptoms from the acute phase to the late stage. The table also highlights the transition from flaccid paralysis and spinal shock to spasticity and hyperreflexia.
Contributed by M Rahman, MBBS
References
Kaiser JT, Reddy V, Lugo-Pico JG. Anatomy, Back, Spinal Cord Arteries. StatPearls. 2026 Jan:(): [PubMed PMID: 30725904]
Biglioli P, Spirito R, Roberto M, Grillo F, Cannata A, Parolari A, Maggioni M, Coggi G. The anterior spinal artery: the main arterial supply of the human spinal cord--a preliminary anatomic study. The Journal of thoracic and cardiovascular surgery. 2000 Feb:119(2):376-9 [PubMed PMID: 10649214]
Gailloud P. Early depiction of anterior spinal arteries and veins in André du Laurens's Historia anatomica humani corporis (1600). Journal of the history of the neurosciences. 2025 Jan-Mar:34(1):50-63. doi: 10.1080/0964704X.2024.2399535. Epub 2024 Sep 24 [PubMed PMID: 39317926]
Ballesteros L, Forero P, Quintero I. Morphological expression of the anterior spinal artery and the intracranial segment of the vertebral artery: a direct anatomic study. Romanian journal of morphology and embryology = Revue roumaine de morphologie et embryologie. 2013:54(3):513-8 [PubMed PMID: 24068398]
Gövsa F, Aktan ZA, Arisoy Y, Varol T, Ozgür T. Origin of the anterior spinal artery. Surgical and radiologic anatomy : SRA. 1996:18(3):189-93 [PubMed PMID: 8873332]
Sheehy NP, Boyle GE, Meaney JF. Normal anterior spinal arteries within the cervical region: high-spatial-resolution contrast-enhanced three-dimensional MR angiography. Radiology. 2005 Aug:236(2):637-41 [PubMed PMID: 15972334]
Mizutani K, Rodesch G. Anatomical disposition of the anterior spinal artery and vein: Subpial or subarachnoid? Interventional neuroradiology : journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences. 2020 Dec:26(6):706-707. doi: 10.1177/1591019920928628. Epub 2020 Jun 23 [PubMed PMID: 32576068]
Miyasaka K, Asano T, Ushikoshi S, Hida K, Koyanagi I. Vascular anatomy of the spinal cord and classification of spinal arteriovenous malformations. Interventional neuroradiology : journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences. 2000 Nov 30:6 Suppl 1(Suppl 1):195-8 [PubMed PMID: 20667247]
Muhr J, Arbor TC, Ackerman KM. Embryology, Gastrulation. StatPearls. 2026 Jan:(): [PubMed PMID: 32119281]
Rehman B, Muzio MR. Embryology, Week 2-3. StatPearls. 2026 Jan:(): [PubMed PMID: 31536285]
Singh R, Munakomi S. Embryology, Neural Tube. StatPearls. 2026 Jan:(): [PubMed PMID: 31194425]
Kuwar Chhetri P, Das JM. Neuroanatomy, Neural Tube Development and Stages. StatPearls. 2026 Jan:(): [PubMed PMID: 32491346]
Donovan MF, Cascella M. Embryology, Weeks 6-8. StatPearls. 2026 Jan:(): [PubMed PMID: 33085328]
Thron A, Stoeter P, Schiessl J, Prescher A. Development of the Arterial Supply of the Spinal Cord Tissue Based on Radioanatomical and Histological Studies in Cattle. Clinical neuroradiology. 2022 Jun:32(2):325-343. doi: 10.1007/s00062-021-01093-3. Epub 2021 Sep 28 [PubMed PMID: 34581828]
Parra JED, Ríos JB, García JFV. Variations in the origin of the anterior spinal artery in a Colombian population sample. Anatomy & cell biology. 2022 Dec 31:55(4):520-524. doi: 10.5115/acb.22.152. Epub 2022 Nov 1 [PubMed PMID: 36316283]
Small JE, Pérez Pérez VH. The Dominant Anterior Thoracic Artery of the Spinal Cord. AJNR. American journal of neuroradiology. 2023 Jan:44(1):111-114. doi: 10.3174/ajnr.A7737. Epub 2022 Dec 29 [PubMed PMID: 36581455]
Hott JS, Vishteh G, Wallace R, Dean BL, Spetzler RF. Anterior spinal artery supplying posterior circulation. Neurology. 2004 Feb 10:62(3):468 [PubMed PMID: 14872033]
Kang HS, Han MH, Kim SH, Kwon OK, Roh HG, Koh YC. Anterior spinal artery as a collateral channel in cases of bilateral vertebral arterial steno-occlusive diseases. AJNR. American journal of neuroradiology. 2007 Feb:28(2):222-5 [PubMed PMID: 17296984]
Level 3 (low-level) evidenceEr U, Fraser K, Lanzino G. The anterior spinal artery origin: a microanatomical study. Spinal cord. 2008 Jan:46(1):45-9 [PubMed PMID: 17406375]
Martinez-Santori M, Kennedy A, Atkinson A, Fraser S, Javaid S. A confounding pediatric spinal cord injury: Anterior, central, or both? Journal of pediatric rehabilitation medicine. 2024 Dec:17(4):426-430. doi: 10.3233/PRM-240004. Epub 2025 Mar 17 [PubMed PMID: 39269860]
Greig D, Zoller S, Sheppard WL, Park DY. Intermittent and Transient Hypotension-related Anterior Cord Syndrome following Elective Cervical Spine Surgery: A Case Report. Journal of orthopaedic case reports. 2021 Mar:11(3):21-24. doi: 10.13107/jocr.2021.v11.i03.2070. Epub [PubMed PMID: 34239823]
Level 3 (low-level) evidenceLepić M, Bogićević I, Novaković N, Stanković S, Đurđević A, Pavlicević G. Rupture of a true anterior spinal artery aneurysm at its intracranial origin: a short report. Neuroradiology. 2025 May:67(5):1337-1339. doi: 10.1007/s00234-025-03626-w. Epub 2025 Apr 25 [PubMed PMID: 40278844]
Ahmadpour A, Morsi RZ, Al-Salihi MM, Kass-Hout T. Isolated Thoracic Anterior Spinal Artery Aneurysm in a Patient With Autoimmune Disease: A Case Report. Cureus. 2024 Jul:16(7):e64943. doi: 10.7759/cureus.64943. Epub 2024 Jul 19 [PubMed PMID: 39156236]
Level 3 (low-level) evidenceIoannidis I, Kalogeras A, Tasiou A, Vlychou M, Fountas KN. Coil Embolization of a Ruptured Anterior Spinal Artery Aneurysm Associated with Spinal Cord Arteriovenous Malformation. Neurointervention. 2024 Nov:19(3):190-193. doi: 10.5469/neuroint.2024.00311. Epub 2024 Oct 2 [PubMed PMID: 39353726]
Farber SH, Rahmani R, Scherschinski L, DiDomenico JD, Mugge LA, Benet A, Kim JE, Ducruet AF, Turner JD, Lawton MT. Clip Reconstruction of a Ruptured Thoracic Anterior Spinal Artery Aneurysm Utilizing a Costotransversectomy Approach: 2-Dimensional Operative Video. Operative neurosurgery (Hagerstown, Md.). 2024 Jun 1:26(6):761. doi: 10.1227/ons.0000000000001045. Epub 2023 Dec 26 [PubMed PMID: 38146935]
Richter V, Khanafer A, Poli S, Expósito AG, Haas P, Roder C, Ernemann U, Henkes H, Hennersdorf F. Isolated spinal aneurysms with spontaneous regression. Neurosurgical review. 2025 Sep 8:48(1):635. doi: 10.1007/s10143-025-03768-8. Epub 2025 Sep 8 [PubMed PMID: 40920243]
Sokol Z, Oselkin M. Spinal subarachnoid hemorrhage as a consequence of dissection with pseudoaneurysm in a cervical radiculomedullary branch of the anterior spinal artery. Radiology case reports. 2024 Jan:19(1):403-407. doi: 10.1016/j.radcr.2023.10.051. Epub 2023 Nov 10 [PubMed PMID: 38033669]
Level 3 (low-level) evidenceWu CW, Chou CL. Anterior Spinal Cord Artery Dissection. Acta neurologica Taiwanica. 2025 Jul 1:34(3):184-185. doi: 10.4103/ANT.ANT_113_0006. Epub 2025 Sep 29 [PubMed PMID: 41020466]
Hashimoto K, Yoshioka H, Wakai T, Tateoka T, Fukuda N, Horiuchi R, Nakano S, Naito Y, Shimizu M, Kinouchi H. Anatomic Feature and Preventive Strategy of Anterior Spinal Artery Occlusion in Endovascular Internal Trapping of Vertebral Artery Dissecting Aneurysms Distal to the Bifurcation of the Posterior Inferior Cerebellar Artery. Operative neurosurgery (Hagerstown, Md.). 2026 Apr 1:30(4):559-565. doi: 10.1227/ons.0000000000001707. Epub 2025 Jul 7 [PubMed PMID: 40622161]
Yu J, Lu H, Krings T, Bian L, Feng Y, Li J, Yang F, Li G, He C, Ye M, Hu P, Sun L, Ma Y, Ren J, Ling F, Hong T, Zhang H. Microsurgery Versus Embolization for Spinal Cord Arteriovenous Malformations: A Proposed Grading System. Neurosurgery. 2026 Apr 1:98(4):786-798. doi: 10.1227/neu.0000000000003458. Epub 2025 May 19 [PubMed PMID: 40387316]
Althobaiti F, Maghrabi R, Alharbi N, Alwadai M, Almatrafi MK, Bajammal S. Anterior Spinal Artery Syndrome in a Patient With Multilevel Cervical Disc Disease: A Case Report. Cureus. 2024 Jul:16(7):e64577. doi: 10.7759/cureus.64577. Epub 2024 Jul 15 [PubMed PMID: 39011315]
Level 3 (low-level) evidenceFolyovich A, Havas L, Vadász G, Fehér Á, Vadasdi K, Szabó Z, Tóth K, Béres-Molnár KA, Toldi G. Fatal outcome of cervical myelopathy caused by fibrocartilaginous embolism. Rare cause of spinal vascular damage. Ideggyogyaszati szemle. 2021 May 30:74(5-6):207-210. doi: 10.18071/isz.74.0207. Epub [PubMed PMID: 34106547]
. Erratum regarding previously published articles. Interventional pain medicine. 2024 Sep:3(3):100424. doi: 10.1016/j.inpm.2024.100424. Epub 2024 Jun 29 [PubMed PMID: 39502908]
Islak C, Bağcılar Ö, Selçuk HH, Saltık S, Korkmazer B, Zubarioğlu T, Arslan S, Üstündag A, Kızılkılıç O. A New Perspective On Arterioectatic Spinal Angiopathy with a Reversible Pattern: Cause or Consequence? Clinical neuroradiology. 2025 Mar:35(1):67-75. doi: 10.1007/s00062-024-01451-x. Epub 2024 Sep 2 [PubMed PMID: 39222145]
Level 3 (low-level) evidenceKraus MJ, Nguyen J. Unilateral Anterior Spinal Artery Syndrome following Spinal Anesthesia for Cesarian Section: A Case Report. Case reports in neurology. 2024 Jan-Dec:16(1):142-147. doi: 10.1159/000539405. Epub 2024 May 22 [PubMed PMID: 39015828]
Level 3 (low-level) evidenceBiglioli P, Roberto M, Cannata A, Parolari A, Fumero A, Grillo F, Maggioni M, Coggi G, Spirito R. Upper and lower spinal cord blood supply: the continuity of the anterior spinal artery and the relevance of the lumbar arteries. The Journal of thoracic and cardiovascular surgery. 2004 Apr:127(4):1188-92 [PubMed PMID: 15052221]
Sahoo SK, Mahapatra RP, Barik R, Acharya D, Panda D, Malla SR, Karthik Kowtarapu S, Mohanan SP, Singh PK. Paraplegia Following Thoracic Endovascular Aneurysm Repair. JACC. Case reports. 2025 Sep 24:30(29):105071. doi: 10.1016/j.jaccas.2025.105071. Epub [PubMed PMID: 41005849]
Level 3 (low-level) evidenceCopeland R, Reeh C, D'Souza R, Ege E, Briggi D, Vangeison C. Delayed onset of anterior spinal artery syndrome caused by retropulsed bone fragment after kyphoplasty: Case report and literature review. Interventional pain medicine. 2023 Sep:2(3):100264. doi: 10.1016/j.inpm.2023.100264. Epub 2023 Jun 24 [PubMed PMID: 39238915]
Level 3 (low-level) evidenceBahadır S, Nabi V, Adhikari P, Ayhan S, Acaroglu E. Anterior Spinal Artery Syndrome: Rare Precedented Reason of Postoperative Plegia After Spinal Deformity Surgery: Report of 2 Cases. World neurosurgery. 2020 Sep:141():203-209. doi: 10.1016/j.wneu.2020.05.216. Epub 2020 Jun 2 [PubMed PMID: 32502625]
Level 3 (low-level) evidenceNeifert SN, Rutledge WC, Frempong-Boadu A, Lau D. Use of Preoperative Spinal Angiography in Severe Spinal Deformity Patients Who Require Thoracic 3 Column Osteotomy: A Case Series and Review of the Literature. Operative neurosurgery (Hagerstown, Md.). 2025 Oct 1:29(4):526-535. doi: 10.1227/ons.0000000000001506. Epub 2025 Jan 29 [PubMed PMID: 39878493]
Level 2 (mid-level) evidenceKhan MM, Munakomi S, Dalal K. Ventral Cord Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 31082055]
Sandoval JI, De Jesus O. Anterior Spinal Artery Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 32809566]
Manconi M, Mondini S, Fabiani A, Rossi P, Ambrosetto P, Cirignotta F. Anterior spinal artery syndrome complicated by the ondine curse. Archives of neurology. 2003 Dec:60(12):1787-90 [PubMed PMID: 14676058]
Dehbi S, Arfaoui M, Armel B, El Hamzaoui H, Alilou M. Idiopathic Spinal Cord Infarction: A Case Report of an Unusual Diagnostic Dilemma and Therapeutic Challenge. Cureus. 2025 Oct:17(10):e95578. doi: 10.7759/cureus.95578. Epub 2025 Oct 28 [PubMed PMID: 41322849]
Level 3 (low-level) evidenceZalewski NL, Rabinstein AA, Krecke KN, Brown RD Jr, Wijdicks EFM, Weinshenker BG, Kaufmann TJ, Morris JM, Aksamit AJ, Bartleson JD, Lanzino G, Blessing MM, Flanagan EP. Characteristics of Spontaneous Spinal Cord Infarction and Proposed Diagnostic Criteria. JAMA neurology. 2019 Jan 1:76(1):56-63. doi: 10.1001/jamaneurol.2018.2734. Epub [PubMed PMID: 30264146]
Zedde M, De Falco A, Zanferrari C, Guarino M, Pezzella FR, Haggiag S, Cossu G, Quatrale R, Micieli G, Del Sette M, Pascarella R. Spinal Cord Infarction: Clinical and Neuroradiological Clues of a Rare Stroke Subtype. Journal of clinical medicine. 2025 Feb 15:14(4):. doi: 10.3390/jcm14041293. Epub 2025 Feb 15 [PubMed PMID: 40004823]
Arkoudis NA, Karachaliou A, Triantafyllou G, Papadopoulos A, Koutserimpas C, Velonakis G. Spinal cord ischemia: The "snake bite sign". World journal of radiology. 2025 Jul 28:17(7):110385. doi: 10.4329/wjr.v17.i7.110385. Epub [PubMed PMID: 40746514]
Ferreira S, Fonseca A, Correia F, Cunha J, Taveira M. Anterior Spinal Cord Infarction: A Rare Diagnosis With an Uncommon Presentation. Cureus. 2024 Jul:16(7):e64083. doi: 10.7759/cureus.64083. Epub 2024 Jul 8 [PubMed PMID: 39114233]
Bagherzadeh S, Rostami M, Jafari M, Roohollahi F. "White Cord Syndrome" as clinical manifestation of the spinal cord reperfusion syndrome: a systematic review of risk factors, treatments, and outcome. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2025 Jan:34(1):50-63. doi: 10.1007/s00586-024-08461-w. Epub 2024 Sep 12 [PubMed PMID: 39266775]
Level 1 (high-level) evidence