Indications
Food and Drug Administration–Approved Indication
Fluvoxamine is a selective serotonin reuptake inhibitor (SSRI) class medication. The US Food and Drug Administration (FDA) approved fluvoxamine in 1994 for the treatment of obsessive-compulsive disorder (OCD) in adult and pediatric patients aged 8 or older. OCD is characterized by recurring obsessions or compulsions that cause significant anxiety or distress to a patient for more than 1 hour every day. The obsessions must not be attributable to substances, medications, or another medical condition. Compulsions are repetitive behaviors performed to alleviate anxiety caused by obsessions. Although patients with OCD recognize that their obsessions or compulsions are excessive, they still feel compelled to perform them. OCD has a lifetime prevalence of 1% to 2%, and is more common in women. About 2.7% of children and adolescents are diagnosed with OCD, and 40% of them have persistent symptoms after a mean of 5.7 years. Patients with OCD may have comorbid conditions, such as major depressive disorder, social phobia, body dysmorphic disorder, eating disorders, and substance use disorders. OCD symptoms are treated with cognitive-behavioral therapy and certain antidepressant medications, such as fluvoxamine.[1][2]
Off-Label Uses
Unlike several other SSRIs, fluvoxamine is not FDA-approved for the treatment of major depressive disorder; however, clinicians may prescribe it off-label for this indication in adults.[3][4] The strength of evidence for this indication is considered equivocal or weak according to a Cochrane review. However, fluvoxamine is at least as effective as fluoxetine and paroxetine for the acute treatment of major depressive disorder and similar to sertraline with respect to recurrence rates. Fluvoxamine is also used off-label in adults to treat generalized anxiety disorder, bulimia nervosa, premenstrual dysphoric disorder, post-traumatic stress disorder, and panic disorder.[5][6][7] Furthermore, fluvoxamine is prescribed off-label for separation anxiety disorder in children and adolescents aged 6 or older.[8][9]
Mechanism of Action
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Mechanism of Action
Fluvoxamine is an SSRI that inhibits the reuptake of serotonin at the serotonin transporter in the presynaptic neuronal membrane, thereby increasing synaptic serotonin and the actions of serotonin on the 5-hydroxytryptamine serotonin 1A receptor. Long-term administration of SSRIs downregulates and desensitizes presynaptic serotonin autoreceptors, allowing increased serotonin release and neuronal impulses. The drug has fewer sedative, anticholinergic, and cardiovascular effects than tricyclic antidepressant medications due to its low affinity for histamine, muscarinic, dopaminergic, and α-adrenergic receptors.[2][10]
Fluvoxamine has a higher affinity for the sigma 1 (σ-1) receptor than other SSRIs, a pathway possibly involved in psychosis and aggression.[10] Interestingly, since the σ-1 receptor is a protein that helps regulate cytokine production, stimulating it may attenuate inflammation. This mechanism explains the reported benefits observed in studies of COVID-19.[11] Fluvoxamine is structurally distinct from other SSRIs as the only monocyclic in its class. The unique pharmacological profile is due to its unique structure, which belongs to the chemical group of 2-aminoethyloximethers of aralkyl ketones.[6] Fluvoxamine lacks asymmetric carbons, eliminating stereoisomerism.[12]
Pharmacokinetics
- Absorption: Fluvoxamine is orally administered as a tablet or capsule and is absorbed directly by the gastrointestinal tract, and is not affected by concomitant food intake.[2][6][13] Plasma concentrations peak within 3 to 8 hours after ingestion.[2] Fluvoxamine displays nonlinear, steady-state pharmacokinetics. Higher doses result in disproportionately higher plasma concentrations.
- Distribution: Fluvoxamine is distributed throughout the body, binding to plasma proteins at approximately 80%.[2][6] Fluvoxamine also crosses the blood-brain barrier and accumulates within the brain.[2]
- Metabolism: Fluvoxamine is metabolized by the hepatic cytochrome P450 enzyme system.[6] After first-pass metabolism, its bioavailability is 53%.[2]
- Excretion: Fluvoxamine's metabolites are excreted primarily in the urine, with approximately 2% remaining unchanged.[2][6] Elimination is biphasic, with a mean half-life of 12 to 22 hours for a single dose. The half-life is prolonged by 30% to 50% at steady state.[14]
Administration
Fluvoxamine is administered orally as tablets or capsules and absorbed directly by the gastrointestinal tract.[5][6] Immediate-release oral tablets are available in 25, 50, and 100 mg strengths; extended-release capsules are available in 100 and 150 mg strengths. Fluvoxamine takes approximately 1 week to reach steady-state concentration.[2][6]
For the Treatment of Obsessive-Compulsive Disorder
- Immediate-release tablets
- Adults: The recommended starting dose is 50 mg orally at bedtime. Dose adjustments can be made in increments of 50 mg every 4 to 7 days until the desired therapeutic benefit is achieved. The recommended daily dose for this medication is between 100 and 300 mg, with a half-life of 9 to 28 hours. The maximum recommended daily dose is 300 mg. For doses greater than 100 mg daily, it should be administered in 2 separate doses, with the larger dose given at bedtime. Notably, lower initial doses and slower titration are recommended for older adults.
- Children 8 to 12 years: The recommended dose is 12.5 to 25 mg orally at bedtime, titrated by 25 mg increments every 4 to 7 days or based on efficacy and tolerability, up to a maximum of 200 mg orally daily. Doses greater than 50 mg should be administered in divided doses. Fluvoxamine is not recommended for children younger than 8.
- Adolescents 12 to 17 years: The recommended starting dose is 25 mg orally at bedtime, titrated by 25 mg increments every 4 to 7 days based on efficacy and tolerability, up to a maximum of 300 mg orally daily. Doses greater than 50 mg should be administered in divided doses.
- Extended-release tablets
- Adults: Initially, adults can take 100 mg of fluvoxamine at bedtime. If needed and tolerated, the dose is gradually increased by 50 mg increments at weekly intervals, up to a target range of 100 to 300 mg daily. During titration, it may be necessary to use both 100 and 150 mg capsules to reach the daily dose. The lowest effective daily dose is maintained once the dosage is stable.
- Children and adolescents: The safety and efficacy of extended-release capsules are not established in pediatric patients.
Maintenance Therapy
Although long-term efficacy data for fluvoxamine maleate tablets in treating OCD beyond 10 weeks are limited, the chronic nature of OCD often justifies extended use in patients who respond well. Maintenance treatment should be tailored to maintain symptom control with the lowest effective dose, and patients should undergo periodic assessment to determine whether continued therapy remains appropriate. Dose reductions of 40% to 60% should be used during maintenance therapy. Tapering fluvoxamine is not recommended until treatment has continued for at least 1 to 2 years. Compared to placebo, fluvoxamine administration for 6 to 10 weeks significantly reduces symptoms associated with OCD. When combined with behavioral therapy, symptoms improved even further in the first 2 months.
Discontinuation Considerations
Withdrawal symptoms have been reported with discontinuation of SSRIs and serotonin-norepinephrine reuptake inhibitors (SNRIs). To minimize these effects, a gradual dose reduction is recommended, rather than abrupt cessation. Patients should be closely monitored for signs of withdrawal. If symptoms are severe, reinstating the previous dose may be necessary, followed by a slower taper.
Specific Patient Populations
Hepatic impairment: The pharmacokinetics of fluvoxamine are altered in patients with hepatic impairment. For instance, patients with liver cirrhosis may have a 30% decrease in the clearance of fluvoxamine.[2] Thus, initiation at a lower dose and titrating more slowly may be necessary to minimize adverse effects.
Renal impairment: Fluvoxamine does not accumulate with renal impairment and creatinine clearances of 5 to 45 mL/min. Due to its extensive volume of distribution, it is unlikely that hemodialysis significantly impacts the clearance of this drug. The pharmacokinetics of fluvoxamine generally remain unchanged in patients with renal impairment.[2][6]
Pregnancy considerations: Available data from published observational studies over several decades have not established an increased risk of major congenital malformations or miscarriage from the use of fluvoxamine during pregnancy. However, it is not clear whether fluvoxamine is safe during pregnancy, as it has not been adequately studied in pregnant women. Use during pregnancy should be limited to situations when the benefits to the mother outweigh the risks to the fetus. Like other SSRIs, the use of fluvoxamine during the third trimester of pregnancy has a small increased risk of pulmonary hypertension in the neonate. However, the incidence of congenital abnormalities at birth is generally low.[5][15] Exposure to fluvoxamine and other SSRIs or SNRIs during late pregnancy, particularly in the third trimester, has been linked to neonatal complications such as prolonged hospitalization, respiratory distress, and the need for enteral feeding. Clinicians should weigh the benefits of continued treatment against these potential risks.
In some cases, a gradual dose taper during the third trimester may be considered in select patients. The American College of Obstetricians and Gynecologists emphasizes that untreated or undertreated maternal psychiatric illness, such as depression, anxiety, OCD, and post-traumatic stress disorder, is associated with adverse outcomes, including preterm birth, low birth weight, preeclampsia, postpartum depression, and impaired infant attachment. Therefore, pregnancy alone should not be a reason to discontinue effective psychiatric treatment.
Breastfeeding: When considering whether to breastfeed while taking fluvoxamine, it is essential to weigh the benefits of breastfeeding against the risks of fluvoxamine exposure to the infant, as well as the dangers of inadequately treated OCD, given that fluvoxamine is secreted into breast milk. Reported adverse effects in the infant include diarrhea, vomiting, sleep disturbance, and agitation. Among antidepressants, fluvoxamine, sertraline, and paroxetine are the first-choice drugs for treating depression in breastfeeding mothers due to low rates of transfer into breastmilk.[16] For example, a study of 2 mothers taking fluvoxamine showed that their infants received 0.8% to 1.38% of the maternal weight-adjusted dose. However, the infants did not exhibit adverse effects, and fluvoxamine was not detectable in serum blood tests.[17] Although some suggest fluvoxamine as a first-choice drug in breastfeeding women, medications such as sertraline and paroxetine may be preferred because they typically produce undetectable or low drug concentrations in infant serum.[18]
Pediatric patients: Both children and adolescents, similar to adults, exhibit nonlinear multiple-dose pharmacokinetics. Notably, steady-state plasma concentrations are 2- to 3-fold higher in children aged 6 to 11 compared to adolescents aged 12 to 17. Additionally, the area under the curve and the maximum achieved concentration in children are 1.5- to 2.7-fold higher than in adolescents. Adverse effects such as vomiting occur more frequently in pediatric patients than in adults.[5]
Older adults: The half-life of fluvoxamine is longer in older adults (17.4 to 25.9 hours) than in younger adults (13.6 to 15.6 hours). Older adults have approximately 40% higher mean maximum plasma concentrations of fluvoxamine than young adults, and the drug's clearance is reduced by approximately 50%. Slow titration of fluvoxamine is recommended; however, a decrease in dose is not warranted. In patients with cardiovascular disease, doses of 50 to 150 mg daily do not significantly impact blood pressure, heart rate, cardiac contractility, or electrocardiogram test results.[2] However, according to the Beers Criteria, SSRIs are considered potentially inappropriate medications in older adults with a history of falls or fractures from ataxia, impaired psychomotor function, or syncope.[19] Older adults are also at higher risk for developing hyponatremia and the syndrome of inappropriate antidiuretic hormone secretion from fluvoxamine.
Adverse Effects
Fluvoxamine is a generally well-tolerated SSRI for patients with OCD. Initial sensitivity to SSRIs is common in patients with anxiety and may manifest as excitation, anxiety, or agitation. Adverse effects can be minimized by initiating at a low dose (50 mg once daily) and gradually increasing the dose until the therapeutic level is achieved. Serotonin syndrome, a rare but serious adverse effect of SSRIs due to excessive serotonergic activity, has been reported with fluvoxamine overdose or concomitant use of other serotonergic agents. Close monitoring for agitation, hallucinations, tachycardia, and hyperthermia is recommended, especially when combining with other serotonergic drugs.
Nausea is the most common adverse effect associated with fluvoxamine, occurring in up to 40% of patients. Common (>10%) adverse effects include insomnia (35%), drowsiness (27%), headache (35%), asthenia (26%), and diarrhea (18%). Other clinically significant adverse effects include platelet dysfunction leading to increased bleeding risk (eg, ecchymosis, epistaxis), hyponatremia (especially in older adults), and infrequent seizures (0.2%) (see Image. Common Adverse Effects Profile). As with many other SSRIs, suicidal thoughts and behaviors may occur. This risk is highest in children, adolescents, and young adults up to 24 years of age, as highlighted in the box warning. Caregivers and patients should monitor for worsening depression, behavioral changes, or suicidal ideation, especially during the initial treatment months or after dose changes, and notify the prescriber immediately. Abrupt discontinuation of fluvoxamine may lead to withdrawal symptoms, including dizziness, nausea, irritability, paresthesia, insomnia, fatigue, and agitation, which typically begin 1 to 3 days after cessation and subside within 1 to 2 weeks. Gradual tapering is recommended to minimize these effects. Fluvoxamine does not typically cause dependency.[2]
Since the introduction of fluvoxamine, there have been spontaneous postmarketing reports of adverse events in patients using the medication. However, a direct causal relationship has not been confirmed. Reported events include serious cardiac arrhythmias such as ventricular tachycardia and torsades de pointes, as well as rare conditions such as porphyria, toxic epidermal necrolysis, and Stevens-Johnson syndrome. Additional reports have included Henoch-Schönlein purpura, bullous skin reactions, priapism, agranulocytosis, aplastic anemia, anaphylactic reactions, angioedema, vasculitis, hyponatremia, acute renal failure, hepatitis, pancreatitis, and ileus. Other rare but serious adverse effects include serotonin syndrome, neuropathy, laryngospasm, and severe akinesia with fever, particularly when fluvoxamine was used in combination with antipsychotic medications.
Drug-Drug Interactions
Fluvoxamine is a potent inhibitor of cytochrome P450 enzymes CYP1A2 and CYP2C19, a moderate inhibitor of CYP3A4, and a weak inhibitor of CYP2C9 and CYP2D6.[5][6][20] Due to its inhibition of CYP1A2, fluvoxamine impairs the elimination of certain drugs, including tertiary amine tricyclic antidepressants, bromazepam, theophylline, propranolol, clozapine, tacrine, warfarin, caffeine, and possibly carbamazepine.[2][6] Fluvoxamine also moderately inhibits CYP3A4, so it can potentially interfere with the metabolism of alprazolam, diazepam, and methadone. Fluvoxamine does not interact with digoxin or ethanol.
Taking fluvoxamine within 2 weeks of another antidepressant should be avoided to prevent serotonin syndrome.[2] Patients who take antiplatelet or anticoagulant drugs need monitoring for bleeding due to amplified effects.[5] SSRIs, such as fluvoxamine, may impair platelet aggregation by depleting platelet serotonin, increasing the risk of bleeding complications in patients taking abciximab. Similarly, it can augment the antiplatelet effects of aspirin, increasing the risk of bleeding from the upper gastrointestinal tract.[21]
Major drug interactions: These interactions are of high clinical significance and should be avoided or used only with extreme caution. Major drug interactions may cause life-threatening effects or severe toxicity; therefore, close monitoring or consideration of alternative therapy is warranted.
- Tizanidine: Contraindicated due to severe hypotension and sedation risk.
- Thioridazine: Contraindicated due to QTc interval prolongation and arrhythmia risk.
- Alosetron: Fluvoxamine increases the alosetron area under the curve 6-fold; contraindicated.
- Clozapine: Markedly increased levels; risk of seizures and hypotension.
- Carbamazepine: Elevated levels and toxicity reported.
- Methadone: Increased plasma levels; opioid intoxication and withdrawal are possible.
- Phenytoin: Narrow therapeutic index; levels may rise significantly.
- Theophylline: Increased levels due to CYP1A2 inhibition.
- Warfarin: Increased anticoagulant effect; monitor international normalized ratio closely.
- Certain triptans (eg, sumatriptan): Risk of serotonin syndrome.
- Monoamine oxidase inhibitors (eg, linezolid and selegiline): Risk of serotonin syndrome; contraindicated.
- Serotonergic agents (eg, SSRIs, SNRIs, tramadol, St. John wort, and tryptophan): Risk of serotonin syndrome.
- Tacrine: Increased exposure and cholinergic adverse effects.
Moderate drug interactions: These interactions are of moderate clinical significance and should be used with caution and monitored closely. Moderate drug interactions may require dosage adjustment, monitoring, or altered therapy.
- Propranolol and metoprolol: Increased levels; monitor for bradycardia and hypotension.
- β-blockers (excluding propranolol/metoprolol): Monitor, possible interaction.
- Diazepam: Additive central nervous system effects are possible.
- Diltiazem: Bradycardia has been reported.
- Tricyclic antidepressants: Increased plasma levels; monitor and consider dose adjustment.
- Lithium: Risk of serotonergic toxicity and seizures; monitor closely.
- Alcohol: No significant pharmacokinetic interaction, but additive sedation is possible.
Mild or low-risk interactions: These interactions are of minimal clinical significance and typically do not need action.
- Lorazepam: No significant pharmacokinetic interaction; central nervous system effects not significant.
- Digoxin: No significant interaction.
- Atenolol: No significant change in plasma levels.
- Smoking: Cannabis smoking activates the aryl hydrocarbon receptor, inducing CYP1A2. This process is similar to tobacco smoking, which increases fluvoxamine elimination by about 25%.[6] The patient should be advised not to use cannabis without medical guidance.
Contraindications
Boxed Warning
In 2004, the FDA issued a box warning for children, adolescents, and young adults (up to age 24) treated with SSRIs, including fluvoxamine, due to the increased risk of suicidal thoughts and behaviors.[22]
Precautions
Clozapine coadministration: Precautionary drug monitoring should be implemented if fluvoxamine is combined with clozapine. Taking these drugs in combination increases the risk of toxic (>1000 ng/mL) concentrations 10-fold (25%).[2]
Seizure risk: Isolated reports of fluvoxamine-induced seizures have been reported. Patients with epilepsy should be cautioned about its use.[23]
Discontinuation: Stopping fluvoxamine abruptly can lead to withdrawal symptoms such as dizziness, irritability, sensory disturbances, anxiety, headache, and mood changes. These effects are typically self-limited but may be severe; gradual tapering is advised. If symptoms become intolerable, resuming the prior dose and tapering more slowly may be necessary.
Abnormal bleeding: Fluvoxamine may increase bleeding risk, particularly gastrointestinal bleeding, mainly when used with nonsteroidal anti-inflammatory drugs, aspirin, or anticoagulants. Patients should be warned about this potential interaction.
Activation of mania or hypomania: A small percentage of patients, including children and adolescents, may experience manic or hypomanic episodes while taking fluvoxamine. Caution is warranted in individuals with a history of bipolar disorder or mania.
Seizures: Seizures have occurred in a small number of patients during clinical trials. Fluvoxamine should be used cautiously in those with a seizure history and discontinued if seizures develop.
Hyponatremia: Hyponatremia, sometimes due to the syndrome of inappropriate antidiuretic hormone secretion, has been reported with fluvoxamine use. Risk is higher in older adults, those taking diuretics, or those with dehydration. Symptoms range from confusion and weakness to seizures and coma in severe cases. The drug should be discontinued in patients who develop symptoms, and appropriate treatment should be initiated.
Concomitant illness: Caution is advised when prescribing fluvoxamine to patients with cardiovascular instability or impaired drug metabolism. Fluvoxamine has not been well studied in individuals with recent myocardial infarction or unstable heart disease, though no significant electrocardiogram abnormalities were found in clinical trials.
Hepatic impairment: The clearance of fluvoxamine is reduced by approximately 30% in patients with liver dysfunction. Dose adjustments and cautious titration are recommended.
Warnings
Monoamine oxidase inhibitors: Combining fluvoxamine with Monoamine oxidase inhibitors (MAOIs), or starting one shortly after stopping the other, may lead to life-threatening reactions such as serotonin syndrome or neuroleptic malignant syndrome. These syndromes are characterized by agitation, hyperthermia, muscle rigidity, and autonomic instability. Patients should not take MAOIs for 14 days before commencing fluvoxamine.[2]
Thioridazine: Fluvoxamine significantly increases plasma levels of thioridazine and its active metabolites, which can prolong the QTc interval and increase the risk of torsades de pointes. Concomitant use is contraindicated.
Terfenadine, astemizole, cisapride, and pimozide: These medications are metabolized by CYP3A4 enzymes and are associated with QTc prolongation and fatal ventricular arrhythmias with elevated levels of the drug. Because fluvoxamine inhibits CYP3A4 enzymes, these combinations should be avoided.
Tizanidine: Fluvoxamine increases tizanidine plasma levels up to 33-fold and prolongs its half-life, resulting in severe hypotension, bradycardia, sedation, and psychomotor impairment. Concomitant use is contraindicated.
Alosetron: Fluvoxamine raises alosetron plasma concentrations approximately 6-fold and triples its half-life, significantly increasing the risk of serious adverse events. Concurrent use is not recommended.
Clinical deterioration and suicide risk: There is an increased risk of suicidal thoughts and behavior in children, adolescents, and young adults during the early stages of treatment with fluvoxamine. Patients should be monitored closely for worsening depression, suicidality, or unusual behavioral changes. Family members and caregivers should also observe and report concerning symptoms. The risk may be highest in individuals younger than 25, whereas patients older than 65 may have a reduced risk compared to placebo.
Screening for bipolar disorder: Depressive episodes can be the first sign of bipolar disorder. Treating such episodes with an antidepressant alone may trigger mania or mixed episodes. A thorough psychiatric history should be obtained before starting fluvoxamine, and it is not approved for bipolar depression.
Benzodiazepines: Fluvoxamine inhibits the metabolism of certain benzodiazepines, such as alprazolam and diazepam, potentially leading to increased plasma levels and adverse effects. Coadministration with alprazolam may require dose reduction. Concomitant use with diazepam is generally not advisable due to the risk of significant accumulation.
Mexiletine: Fluvoxamine decreases the clearance of mexiletine by approximately 38%. When coadministered, serum mexiletine levels should be monitored, and dosage adjustments made as necessary.
Serotonin syndrome: Fluvoxamine may cause serotonin syndrome, especially when combined with serotonergic drugs such as triptans, SSRIs, SNRIs, MAOIs, or tryptophan. Symptoms include mental status changes, autonomic instability, neuromuscular abnormalities, and gastrointestinal tract symptoms. Caution should be exercised, and combination with other medications should be avoided if possible.
Neuroleptic malignant syndrome: Neuroleptic malignant syndrome or similar reactions have been reported with fluvoxamine, particularly when combined with antipsychotics. Symptoms include hyperthermia, rigidity, mental status changes, and autonomic instability. Both agents should be discontinued, and supportive care should be provided.
Theophylline: Fluvoxamine reduces theophylline clearance by about 3-fold. If used together, theophylline dose should be reduced to one-third, and plasma levels should be monitored.
Warfarin: Fluvoxamine nearly doubles warfarin levels and prolongs prothrombin time. The international normalized ratio should be closely monitored, and the warfarin dose should be adjusted accordingly.
See Image. Fluvoxamine Interactions.
Monitoring
Patients taking fluvoxamine should have their blood pressure, growth rate, heart rate, and weight monitored. Importantly, clinicians should monitor for worsening suicidality or significant behavioral changes such as anxiety, agitation, panic attacks, insomnia, irritability, hostility, impulsiveness, restlessness, mood elevation, or impaired social interaction (especially at initiation and with dose adjustments), akathisia, signs of bleeding, and hyponatremia with serum sodium levels in older adults. Decreased appetite and weight loss have been reported with fluvoxamine and other SSRIs. If a child is prescribed fluvoxamine for long-term use, regular monitoring of weight and growth is recommended to ensure appropriate development.[17][24]
Toxicity
The symptoms of fluvoxamine overdose include somnolence, diarrhea, vomiting, and dizziness. In a case series of 354 fluvoxamine overdoses, at least 309 patients recovered fully after gastric decontamination and supportive care. A patient fully recovered after ingesting 10,000 mg of fluvoxamine. Unfortunately, 19 patients died; however, 17 combined fluvoxamine with other medications. Therefore, the contribution of fluvoxamine was not confirmed.[2]
Signs and Symptoms
Commonly reported adverse effects (occurring in ≥5% of overdose cases) include coma, hypokalemia, hypotension, nausea, dyspnea, somnolence, tachycardia, and vomiting. Additional symptoms that have been observed, either with fluvoxamine alone or in combination with other substances, include bradycardia, electrocardiogram abnormalities, such as cardiac arrest, prolonged QT interval, first-degree atrioventricular nodal block, bundle-branch block, and junctional rhythm; seizures; tremors; diarrhea; and hyperreflexia.
Management of Overdose
Treatment should follow standard procedures used for antidepressant overdoses. Priority should be given to maintaining respiratory function, ensuring adequate oxygenation, and supporting ventilation. Vital signs and cardiac rhythm should be continuously monitored. General supportive care and symptom-based treatment are advised. Inducing vomiting is not recommended. Gastric lavage may be considered with a large-bore orogastric tube if performed shortly after ingestion or if the patient is symptomatic, provided aspiration precautions are in place.
Activated charcoal should be administered to reduce the absorption of drugs. Because fluvoxamine has a large volume of distribution, procedures such as forced diuresis, dialysis, hemoperfusion, or exchange transfusion are unlikely to be effective. There is no known antidote for fluvoxamine overdose. Caution is required if the patient is also taking or has recently taken a tricyclic antidepressant, as fluvoxamine can increase the levels and effects, potentially leading to worse outcomes. In overdose, coingestion should be considered. A poison control center should be consulted for detailed guidance.
Enhancing Healthcare Team Outcomes
OCD causes significant distress in patients and impacts their daily living, relationships, and employment. Collaboration between clinicians, therapists, pharmacists, and other healthcare professionals is necessary to treat these patients appropriately. Behavioral therapy, such as exposure and response prevention, is the first-line treatment for reducing compulsions in approximately 50% of patients with OCD; benefits may persist for 2 years.[25][26] Results from a high-quality systematic review and meta-analysis demonstrate that fluvoxamine is more effective than placebo in improving symptoms and response rates for OCD and social anxiety disorder, with mixed findings in panic disorder.[27]
The best patient outcomes combine medication treatment, such as fluvoxamine, with psychotherapy to help ease obsessions and compulsions. Because relapse after treatment discontinuation is common, continued treatment is advised. Fluvoxamine is a safe medication for patients in the hospital with stable vital signs, normal electrocardiogram results, and normal laboratory test results. Fluvoxamine can be used as an off-label medication to help treat patients with anxiety, depression, or panic disorder, which can improve outcomes for patients with prolonged hospital stays or procedures that cause distress.[14]
Effective use of fluvoxamine in clinical practice requires a coordinated, interprofessional approach to ensure safe, patient-centered care. Clinicians diagnose OCD and depression, determining the appropriateness of fluvoxamine therapy, and educate patients about potential benefits and risks. Nurses contribute by monitoring adherence, assessing for adverse effects such as serotonin syndrome, and identifying behavioral changes that may signal worsening depression or suicidality—especially during treatment initiation or dose adjustments. Pharmacists assess drug-drug interactions, particularly given fluvoxamine's potent inhibition of the CYP1A2, CYP2C19, and CYP3A4 enzymes, which can significantly impact the metabolism of many medications, and counsel patients on dosing, titration, and withdrawal strategies.[28] Mental healthcare professionals, including therapists and social workers, improve outcomes by addressing the psychosocial needs of patients and reinforcing therapeutic engagement. Clear interprofessional communication, ongoing safety monitoring, and shared decision-making foster a collaborative care environment. By aligning roles and responsibilities, the healthcare team can optimize treatment with fluvoxamine, improve symptom control, minimize adverse effects, and enhance quality of life.
Media
(Click Image to Enlarge)
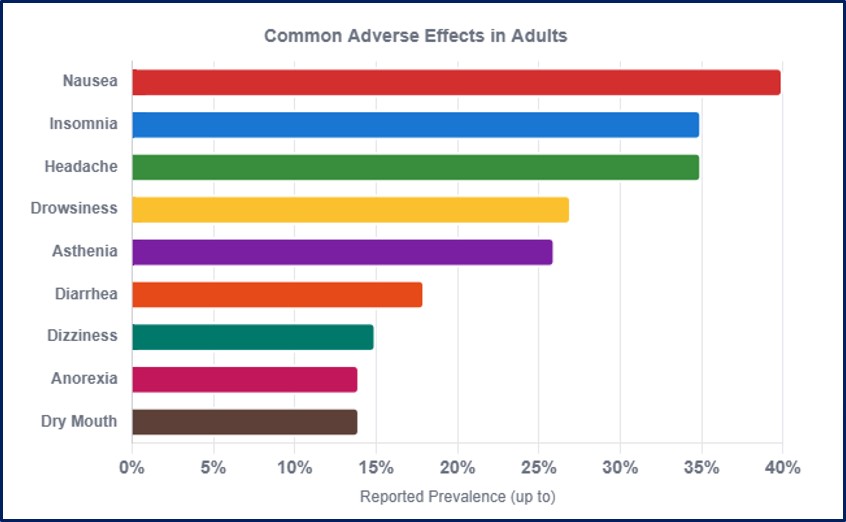
Common Adverse Effects Profile. Flovaxmine's adverse effects are diverse; gastrointestinal and central nervous system symptoms predominate. Other common effects include insomnia, headache, and somnolence. Monitor for behavioral activation in pediatric patients and for rare but serious effects (eg, platelet dysfunction/abnormal bleeding).
Contributed by MS Parmar, PhD
(Click Image to Enlarge)
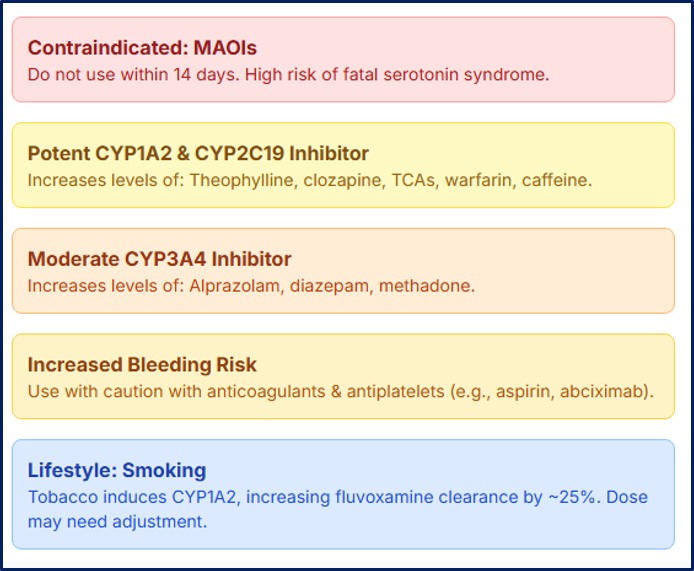
Fluvoxamine Interactions. Because fluvoxamine inhibits multiple cytochrome P450 enzymes, coadministered medications may require dose adjustment or avoidance.
Contributed by MS Parmar, PhD
References
Soomro GM. Obsessive compulsive disorder. BMJ clinical evidence. 2012 Jan 18:2012():. pii: 1004. Epub 2012 Jan 18 [PubMed PMID: 22305974]
Silver H. Fluvoxamine as an adjunctive agent in schizophrenia. CNS drug reviews. 2001 Fall:7(3):283-304 [PubMed PMID: 11607044]
Feighner JP, Boyer WF, Meredith CH, Hendrickson GG. A placebo-controlled inpatient comparison of fluvoxamine maleate and imipramine in major depression. International clinical psychopharmacology. 1989 Jul:4(3):239-44 [PubMed PMID: 2507630]
Medvedev VE, Kardashian RA, Frolova VI. [Fluvoxamine in the treatment of anxiety-depressive spectrum disorders]. Zhurnal nevrologii i psikhiatrii imeni S.S. Korsakova. 2024:124(6):101-109. doi: 10.17116/jnevro2024124061101. Epub [PubMed PMID: 39072574]
Arishi NA, Althomali NM, Dighriri IM, Alharthi MS, Alqurashi GB, Musharraf RA, Albuhayri AH, Almalki MK, Alnami SA, Mashraqi ZO. An Overview of Fluvoxamine and its Use in SARS-CoV-2 Treatment. Cureus. 2023 Jan:15(1):e34158. doi: 10.7759/cureus.34158. Epub 2023 Jan 24 [PubMed PMID: 36843775]
Level 2 (mid-level) evidenceOmori IM, Watanabe N, Nakagawa A, Cipriani A, Barbui C, McGuire H, Churchill R, Furukawa TA. Fluvoxamine versus other anti-depressive agents for depression. The Cochrane database of systematic reviews. 2010 Mar 17:2010(3):CD006114. doi: 10.1002/14651858.CD006114.pub2. Epub 2010 Mar 17 [PubMed PMID: 20238342]
Level 1 (high-level) evidenceMilano W, Siano C, Putrella C, Capasso A. Treatment of bulimia nervosa with fluvoxamine: a randomized controlled trial. Advances in therapy. 2005 May-Jun:22(3):278-83 [PubMed PMID: 16236688]
Level 1 (high-level) evidenceWalkup J, Labellarte M, Riddle MA, Pine DS, Greenhill L, Fairbanks J, Klein R, Davies M, Sweeney M, Abikoff H, Hack S, Klee B, Bergman RL, Lynn D, McCracken J, March J, Gammon P, Vitiello B, Ritz L, Roper M, Research Units on Pediatric Psychopharmacology Anxiety Study Group. Treatment of pediatric anxiety disorders: an open-label extension of the research units on pediatric psychopharmacology anxiety study. Journal of child and adolescent psychopharmacology. 2002 Fall:12(3):175-88 [PubMed PMID: 12427292]
. Fluvoxamine for the treatment of anxiety disorders in children and adolescents. The Research Unit on Pediatric Psychopharmacology Anxiety Study Group. The New England journal of medicine. 2001 Apr 26:344(17):1279-85 [PubMed PMID: 11323729]
Karbasi Amel A, Hosseini F. A Comparison of the Anti-Anxiety Effects of Oral Ketamine and Fluvoxamine in Children with Separation Anxiety Disorder Manifesting as School Refusal. Advanced biomedical research. 2023:12():110. doi: 10.4103/abr.abr_388_22. Epub 2023 Apr 27 [PubMed PMID: 37288025]
Khani E, Entezari-Maleki T. Fluvoxamine and long COVID-19; a new role for sigma-1 receptor (S1R) agonists. Molecular psychiatry. 2022 Sep:27(9):3562. doi: 10.1038/s41380-022-01545-3. Epub 2022 Apr 6 [PubMed PMID: 35388182]
Irons J. Fluvoxamine in the treatment of anxiety disorders. Neuropsychiatric disease and treatment. 2005 Dec:1(4):289-99 [PubMed PMID: 18568110]
She DP, He Y, Li MQ, Su L, Ren D, Huang XH, Zhang YH, Hu HT, Deng DC, Wu JL. Pharmacokinetics and bioequivalence studies of fluvoxamine maleate tablets in healthy Chinese subjects. Biomedical chromatography : BMC. 2023 Jun:37(6):e5613. doi: 10.1002/bmc.5613. Epub 2023 Mar 27 [PubMed PMID: 36849133]
Ordacgi L, Mendlowicz MV, Fontenelle LF. Management of obsessive-compulsive disorder with fluvoxamine extended release. Neuropsychiatric disease and treatment. 2009:5():301-8 [PubMed PMID: 19557140]
Burhanuddin K, Badhan R. Optimising Fluvoxamine Maternal/Fetal Exposure during Gestation: A Pharmacokinetic Virtual Clinical Trials Study. Metabolites. 2022 Dec 16:12(12):. doi: 10.3390/metabo12121281. Epub 2022 Dec 16 [PubMed PMID: 36557319]
Fortinguerra F, Clavenna A, Bonati M. Psychotropic drug use during breastfeeding: a review of the evidence. Pediatrics. 2009 Oct:124(4):e547-56. doi: 10.1542/peds.2009-0326. Epub 2009 Sep 7 [PubMed PMID: 19736267]
Kristensen JH, Hackett LP, Kohan R, Paech M, Ilett KF. The amount of fluvoxamine in milk is unlikely to be a cause of adverse effects in breastfed infants. Journal of human lactation : official journal of International Lactation Consultant Association. 2002 May:18(2):139-43 [PubMed PMID: 12033075]
Weissman AM, Levy BT, Hartz AJ, Bentler S, Donohue M, Ellingrod VL, Wisner KL. Pooled analysis of antidepressant levels in lactating mothers, breast milk, and nursing infants. The American journal of psychiatry. 2004 Jun:161(6):1066-78 [PubMed PMID: 15169695]
Level 1 (high-level) evidenceBy the 2023 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. Journal of the American Geriatrics Society. 2023 Jul:71(7):2052-2081. doi: 10.1111/jgs.18372. Epub 2023 May 4 [PubMed PMID: 37139824]
Sukhatme VP, Reiersen AM, Vayttaden SJ, Sukhatme VV. Fluvoxamine: A Review of Its Mechanism of Action and Its Role in COVID-19. Frontiers in pharmacology. 2021:12():652688. doi: 10.3389/fphar.2021.652688. Epub 2021 Apr 20 [PubMed PMID: 33959018]
Razakjr OA, Tan HC, Yip WL, Lim YT. Predictors of bleeding complications and thrombocytopenia with the use of abciximab during percutaneous coronary intervention. Journal of interventional cardiology. 2005 Feb:18(1):33-7 [PubMed PMID: 15788052]
Boaden K, Tomlinson A, Cortese S, Cipriani A. Antidepressants in Children and Adolescents: Meta-Review of Efficacy, Tolerability and Suicidality in Acute Treatment. Frontiers in psychiatry. 2020:11():717. doi: 10.3389/fpsyt.2020.00717. Epub 2020 Sep 2 [PubMed PMID: 32982805]
Figgitt DP, McClellan KJ. Fluvoxamine. An updated review of its use in the management of adults with anxiety disorders. Drugs. 2000 Oct:60(4):925-54 [PubMed PMID: 11085201]
Maayan L, Vakhrusheva J, Correll CU. Effectiveness of medications used to attenuate antipsychotic-related weight gain and metabolic abnormalities: a systematic review and meta-analysis. Neuropsychopharmacology : official publication of the American College of Neuropsychopharmacology. 2010 Jun:35(7):1520-30. doi: 10.1038/npp.2010.21. Epub 2010 Mar 24 [PubMed PMID: 20336059]
Level 1 (high-level) evidenceSwedish Council on Health Technology Assessment. Treatment of Anxiety Disorders: A Systematic Review. 2005 Nov:(): [PubMed PMID: 28876726]
Level 1 (high-level) evidenceFung R, Elbe D, Stewart SE. Retrospective Review of Fluvoxamine-Clomipramine Combination Therapy in Obsessive-Compulsive Disorder in Children and Adolescents. Journal of the Canadian Academy of Child and Adolescent Psychiatry = Journal de l'Academie canadienne de psychiatrie de l'enfant et de l'adolescent. 2021 Aug:30(3):150-155 [PubMed PMID: 34381507]
Level 2 (mid-level) evidenceHaddad M, Dieckmann LHJ, Viola TW, de Araújo MR, da Silva NR, Mari JJ. The Efficacy of Fluvoxamine in Anxiety Disorders and Obsessive-Compulsive Disorder: An Overview of Systematic Reviews and Meta-Analyses. Pharmaceuticals (Basel, Switzerland). 2025 Feb 28:18(3):. doi: 10.3390/ph18030353. Epub 2025 Feb 28 [PubMed PMID: 40143130]
Level 1 (high-level) evidenceSiyu-Yang, Ruibing-Sun, Liqing-Wang, Mingzhe-Cao. Fluvoxamine, an inhibitor of CYP1A2, improves CS-induced pulmonary inflammation through estrogen deficiency. Toxicology and applied pharmacology. 2025 Aug:501():117395. doi: 10.1016/j.taap.2025.117395. Epub 2025 May 16 [PubMed PMID: 40381743]
Level 2 (mid-level) evidence