Introduction
Airway monitoring, as part of a comprehensive physical examination, assesses a patient's ventilation and gas-exchange capacity. This assessment includes examining a patient's airway status, interpreting data from adjunct monitors, and determining the next steps to follow to improve patient outcomes. This review explores various airway monitoring techniques, their functions, and limitations.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Monitoring a patient in respiratory distress involves gathering both subjective and objective information.[1] A focused history and physical examination offer valuable insights into the patient's ability to protect their airway. A thorough understanding of airway anatomy aids in conducting a thorough examination. The airway can be categorized into 2 parts: the upper airway, encompassing the nasal cavity, oropharynx, and larynx, and the lower airway, starting with the trachea and extending through the bronchi, bronchioles, and alveoli (see Image. Airway and Lung Anatomy).
An airway exam should include an assessment of mouth opening, dentition, thyromental distance, neck circumference, Mallampati score (see Image. Mallampati Score Visual), and cervical spine mobility. The mnemonic LEMON is often used to evaluate the airway.
- L: Look
- E: Evaluate
- M: Mallampati
- O: Obstruction
- N: Neck mobility
Indicators such as mouth opening of fewer than 3 fingers, a large neck, a short thyromental distance of fewer than 3 fingerbreadths, Mallampati 3 or 4, or limited neck extension should alert the clinician to a possible difficult airway and prompt appropriate preparation.[2] Additional signs indicating a patient may be difficult to intubate may include prominent upper teeth or a receding lower jaw. Congenital malformations, prior surgical intervention, or history of radiation, and trauma to the airway may also be a strong indicator of a difficult airway. Different airway examination tests can be used; however, their accuracy may vary.[3][4][5] Some of the commonly used airway examination tests and their accuracy include the following:
- Mallampati test
- This test is a simple, noninvasive method for predicting difficult intubation by assessing the visibility of oropharyngeal structures. However, the Mallampati test has limited accuracy, with sensitivity ranging from 24% to 62% and specificity from 78% to 82%.
- Thyromental distance
- The thyromental distance measures the space between the thyroid notch and the mentum (lower jaw). A shorter distance is associated with a difficult airway. The test has a sensitivity of 44% to 55% and a specificity of 85% to 89%.
- Sternomental distance
- This test measures the distance between the sternal notch and the mentum. A shorter distance suggests a difficult airway. The sensitivity of the sternomental distance test ranges from 50% to 62%, with a specificity of 88% to 89%.
- Interincisor gap
- The interincisor gap is the distance between the upper and lower incisors with the mouth fully open. A smaller gap indicates a difficult airway. The test has a sensitivity of 29% to 61% and a specificity of 83% to 85%.
- Neck mobility
- Limited neck mobility can make airway management more challenging. The test has a sensitivity of 29% to 54% and a specificity of 85% to 89%.
- Upper lip bite test
- The upper lip bite test involves asking the patient to bite their upper lip with their lower incisors. The test has a sensitivity of 68% to 93% and a specificity of 82% to 97%.
Airway ultrasound also has a role in predicting difficult intubations.[6][7] The most accurate predictor of difficult intubation is an interincisor distance of less than 3 cm. Intubation should always be confirmed with a colorimetric carbon dioxide (CO2) indicator or a continuous end-tidal CO2 (ETCO2) monitor.
Physical exam signs, including fogging/mist in the endotracheal tube lumen, chest rise with each breath, and bilateral breath sounds, can help confirm endotracheal intubation; however, objective parameters should take priority. Although a chest x-ray can help visualize placement, it is not mandatory. Clinical correlation is recommended instead.
The most reliable measures of endotracheal intubation are direct visualization during laryngoscopy and a persistently elevated ETCO2 level.[8] In addition to the LEMON mnemonic for airway assessment, other factors such as the patient's level of consciousness, respiratory rate, oxygen saturation, and use of accessory muscles can provide valuable information about the patient's airway status. Auscultation of breath sounds can also help identify abnormalities, such as wheezing, stridor, crackles, or diminished breath sounds.[9][10]
Indications
Airway monitors are crucial for evaluating a patient’s physical condition and clinical status. Signs that a patient may necessitate airway intervention, such as endotracheal intubation or ventilation support using noninvasive modalities like bilevel positive airway pressure, include symptoms such as dysarthria, tripod posture, drooling, increased respiratory effort, accessory muscle use, nasal flaring, tachypnea, declining mental status, cyanosis, and escalating FiO2 demand. Obtaining a comprehensive medical history and physical examination can be arduous when managing patients in respiratory distress. In such instances, healthcare professionals must employ alternative methods to assess the patient’s airway.
Monitoring vital signs and conducting laboratory tests, such as blood gas analysis, can provide valuable insights and help identify impending respiratory failure. Airway monitoring is indicated in patients undergoing sedation for procedures or those receiving narcotics and/or benzodiazepines. These patients necessitate special attention as they pose a potential risk for respiratory distress, particularly in the obese and elderly populations. These patients should be assessed and reassessed frequently, and appropriate monitors, such as continuous pulse oximetry, should be used to help identify oversedation or apnea.
Contraindications
Contraindications to airway monitoring are confined to patients in hospice or undergoing palliative care during the final stages of life.
Equipment
Capnography is an airway monitoring method applicable to controlled and spontaneously ventilating patients. The amount of infrared light absorbed by carbon dioxide in exhaled gas is measured and reported as a concentration value. Waveform capnography can provide qualitative data via waveform analysis and quantitative data via alveolar ETCO2.[11] Other forms of capnography, such as colorimetric capnography, can confirm endotracheal intubation in remote, out-of-hospital settings, emergency departments, or intensive care units. Capnography can provide reliable information confirming adequate ventilation and cellular gas exchange.
The waveform shows 4 phases of the respiratory cycle:
- Phase 1: Inspiratory baseline
- Phase 2: Expiratory upstroke
- Phase 3: Expiratory plateau
- Phase 4: Inspiratory downstroke
Predicting catastrophic events is possible by analyzing changes in waveform morphology and amplitude. Elevated levels of ETCO2 may indicate various medical conditions, including rebreathing, hypoventilation, malignant hyperthermia, sepsis, insufflation during laparoscopic surgery, or bicarbonate administration. Decreases in ETCO2 are found during hyperventilation, hypothermia, low cardiac output states (eg, pulmonary embolism or cardiac arrest), disconnection of the circuit, or accidental extubation.
Morphological perturbations such as up-slanting of the expiratory upstroke or prolongation of the plateau phase can be evidence of airway obstruction, as seen in bronchospasm, asthma, pregnancy, chronic obstructive pulmonary disease, or a kinked endotracheal tube. Waveform capnography is a crucial monitoring tool for intubated patients, and its interpretation can aid in managing their ventilation. Capnography has limitations, especially when a patient is not intubated or doesn't have a secure airway.
Simply observing a positive return of ETCO2 may or may not confirm the endotracheal placement of the endotracheal tube (ETT). However, a sustained ETCO2 level above 30 mm Hg for at least 3 breaths can confirm ETT placement. Notably, if a patient consumed a bicarbonate solution or carbonated beverage before intubation, this could alter ETCO2 readings. Furthermore, capnography is limited in pulseless patients because it requires cardiac output. However, it can guide chest compressions, where a sudden increase in ETCO2 may suggest a return of spontaneous circulation.
Capnography has recently been further studied and developed for various clinical applications. The usefulness of capnography as a noninvasive method for monitoring ventilation has been demonstrated in various settings, including procedural sedation, the management of acute respiratory distress syndrome, and emergency medicine for the early detection of respiratory failure.[12][13][14] Using capnography has also improved patient safety and outcomes by reducing the incidence of adverse events related to hypoventilation and hypoxia.[15] Recent technological advances have led to new capnography devices that are more portable, user-friendly, and versatile, enabling broader use across diverse clinical scenarios.[13] Despite these advances, it is essential to understand the limitations of capnography and pulse oximetry, as well as the factors that influence their accuracy.
The pulse oximeter is a noninvasive monitor that detects changes in hemoglobin oxygenation saturation and heart rate. Pulse oximetry functions on spectrophotometry and photoplethysmography. Oxyhemoglobin absorbs infrared light at a wavelength of 940 nm, and deoxyhemoglobin absorbs red light at 660 nm. When oxyhemoglobin absorbs emitted infrared light, it allows red light to be transmitted and received by the photodetector. The red-to-infrared light ratio determines the percentage of hemoglobin saturation with oxygen. The pulsations occurring with each heartbeat are recorded as arterial blood and thus provide arterial blood oxygenation.[16]
Although a pulse oximeter can help determine blood oxygen levels, it has some limitations. For example, carboxyhemoglobin resulting from carbon monoxide poisoning can cause falsely elevated oxygen saturation readings because it absorbs light at the same wavelength as oxyhemoglobin. Methemoglobinemia, which has the same absorption coefficient for red and infrared light (resulting in a 1:1 red/infrared ratio), depicts a saturation of approximately 85%.
This phenomenon results in a falsely low oxygen saturation when saturation is greater than 85% and a falsely elevated saturation when it is less than 85%. Other factors that can affect the accuracy of oxygen saturation readings include acid-base disorders, severe hypoxemia, dark nail polish, excessive motion, ambient light, low perfusion, hypothermia, increased systemic vascular resistance, profound anemia, methylene blue dye, and malpositioning. These limitations must be considered when interpreting pulse oximeter readings.
Examples of adjunct airway monitors that further guide clinical decision-making include chest x-ray, ultrasound, and bronchoscopy in the intubated patient. These modalities can help identify underlying lung pathologies, airway obstruction, and foreign bodies and provide visual guidance during endotracheal intubation.[17] In particular, point-of-care lung ultrasound has gained popularity recently due to its noninvasive nature, rapid results, and portability, making it an ideal tool for use in emergency settings and intensive care units.[18]
In conclusion, capnography is a valuable method for monitoring airway and ventilation in spontaneously breathing and ventilated patients. With its ability to provide real-time information on the patient's ventilation status, capnography is an essential tool in various clinical settings. While it has limitations, recent technological developments have expanded its applications and improved its usability. Capnography and pulse oximetry can help guide patient management and improve patient safety.
Personnel
All individuals involved in patient care must be able to identify the signs of respiratory distress. These include personnel in the prehospital setting, emergency room staff, nurses and medical assistants, and clinicians. In such cases, activating a rapid response and initiation of oxygen supplementation may assist in providing immediate care and preventing patient decompensation.
Qualified clinicians experienced in airway management should be consulted, and an objective assessment conducted. Additionally, when a challenging airway is anticipated, it is recommended to have a supraglottic airway device and a video-assisted laryngoscope available to facilitate intubation. Should the patient present as an unanticipated difficult airway, a surgical front-of-neck airway should be considered if the patient cannot be ventilated or intubated by airway experts.
The Difficult Airway Society (DAS) 2025 guidelines highlight improvements in managing unanticipated difficult tracheal intubation and should be reviewed by clinicians involved in airway management. Airway monitors recommended by the DAS include waveform capnography (checked before induction of anesthesia, if possible) and continuous throughout airway management, continuous and audible pulse oximetry, and quantitative neuromuscular monitoring. Additionally, vital signs, including a 3- to 5-lead electrocardiogram and blood pressure monitoring, are crucial for assessing the patient's clinical stability.[19]
Technique or Treatment
Airway assessment and planning must be performed before intervention. As stated by the DAS and the American Society of Anesthesiologists, continuous airway supplementation throughout airway management is essential to optimize the chances of first-attempt success during tracheal intubation. A thorough understanding of the Difficult Airway Algorithm is required for clinicians involved in airway management (see Image. The American Society of Anesthesiologists [ASA] Difficult Airway Algorithm: Adult Patients 2022).[19][20]
In difficult airways, the effectiveness of airway nerve blocks versus airway anesthesia without nerve blocks for awake tracheal intubation has been compared. Airway nerve blocks significantly reduced intubation time, improved the quality of anesthesia, and decreased overall complications. In conclusion, airway nerve blocks provide superior airway anesthesia for awake tracheal intubation, improving intubation conditions and patient satisfaction while reducing complications.[21]
In ventilated individuals, understanding transpulmonary pressure is essential for assessing lung stress. This accurately reflects alveolar pressure and serves as a crucial physiological marker. Esophageal manometry, which utilizes esophageal balloon catheters, is used to measure pleural pressure and make necessary ventilator adjustments.
However, calibration methods are necessary to account for the balloon's air volume. Clinical applications of esophageal manometry include assessing lung and chest wall compliance, estimating breathing effort for ventilator weaning, detecting upper airway obstruction postextubation, and identifying patient-ventilator asynchrony.[22] Results from clinical trials and meta-analyses suggest that intraoperative quantitative monitoring significantly reduces the risk of residual neuromuscular blockade and improves postoperative respiratory outcomes by minimizing adverse events. Consequently, numerous international anesthesia societies endorse the use of quantitative monitoring when administering neuromuscular blocking agents in perioperative settings.[23]
Capnography, or real-time monitoring of exhaled CO2, is a valuable tool for assessing patient health during anesthesia, in emergency departments, and in critical care units, with ETCO2 concentration as the fundamental measurement. The applications of this technology are varied, including verifying ETT placement, assessing disease severity and treatment response, and monitoring sleep apnea in outpatient settings. With advances in technology, smaller sensors have been deployed in various settings, including prehospital environments and high-performance military aircraft. These offer possibilities for new applications that can be integrated into breathing masks.[24]
Different surgical conditions require specific ventilation strategies, each with its own challenges and considerations. For instance, laparoscopic surgery involving creating a pneumoperitoneum can lead to reduced lung compliance and increased ventilatory pressures due to the diaphragm's cephalad displacement. While prone positioning can benefit the respiratory system, it requires careful airway management to prevent ETT disconnection.
One-lung ventilation during thoracic surgery affects ventilation-perfusion matching and requires lung-protective strategies. Jet ventilation is a specialized technique requiring a shared airway or a still chest. This type of ventilation can be performed at low frequencies for laryngeal procedures or at high frequencies for specialized interventions, with considerations for airway pressures and gas exchange. Knowing these ventilation strategies and their implications in various surgical scenarios can enhance patient care and outcomes.[25]
Clinical Significance
Identifying impending respiratory distress in a patient can lead to early intervention and greatly reduce morbidity and mortality. Personnel in the prehospital setting, emergency room, and throughout the hospital should be briefed on methods to activate a rapid response in a deteriorating patient and be aware of who the airway experts are and how to reach them at any given time. Untreated hypoxia can result in tissue and organ injury, and even death.
Properly monitoring an intubated individual's airway involves considering several variables. The ventilator visually represents a patient's ventilatory mechanics and can detect acute changes. Radiographic imaging can help identify developing lung pathology or diaphragmatic abnormalities. The patient's airway must be monitored appropriately when weaning them from a ventilator. Following specific criteria is essential for safe extubation and preventing the need for reintubation.
Enhancing Healthcare Team Outcomes
Effective airway monitoring requires a structured, anticipatory approach grounded in early recognition, technical proficiency, and coordinated team dynamics. Patient-centered care is best achieved through an interprofessional model in which nursing staff and emergency medical services, often the first to assess the airway, initiate basic airway management in alignment with American College of Surgeons Advanced Trauma Life Support and American Heart Association guidelines, prioritizing airway stabilization to reduce morbidity and mortality.[26] Physicians, advanced practitioners, nurse anesthetists, and respiratory therapists must demonstrate expert-level skill in advanced airway techniques, recognizing that improper placement can lead to hypoxia, gastric insufflation, acidosis, organ ischemia, and death. Continuous monitoring, including clinical assessment and adjuncts such as pulse oximetry and capnography, combined with vigilance from all team members, enables early detection of deterioration and timely escalation.
Optimal outcomes depend on disciplined interprofessional communication, ethical practice, and seamless care coordination. Closed-loop communication ensures that concerns about airway status are conveyed and addressed promptly, while standardized protocols and shared mental models reduce variability and errors. Pharmacists guide medication selection for rapid-sequence intubation and minimize adverse drug interactions; radiologists confirm endotracheal tube placement and evaluate pulmonary pathology; and respiratory therapists provide critical expertise in ventilatory support and early identification of respiratory decline. Ethical considerations, including informed consent when feasible, reinforce patient autonomy and transparency. All team members share responsibility for maintaining situational awareness, respecting open communication, and coordinating care without introducing inefficiencies or risk, thereby enhancing patient safety, team performance, and overall clinical outcomes.
Media
(Click Image to Enlarge)
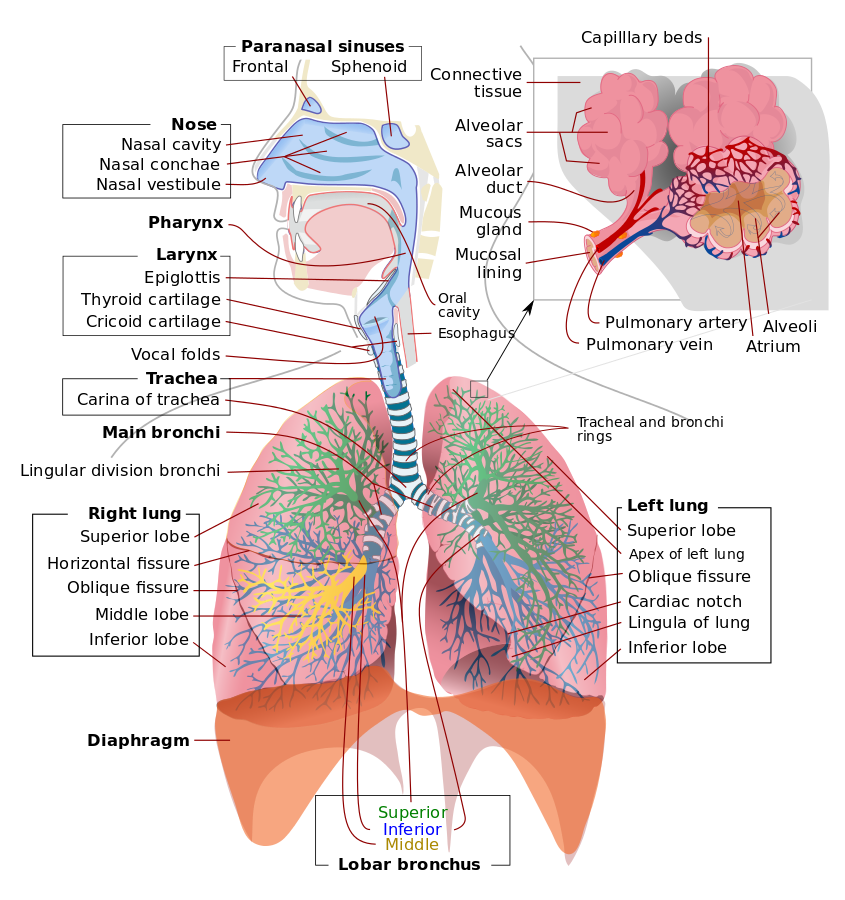
Airway and Lung Anatomy Contributed by Public Domain
(Click Image to Enlarge)
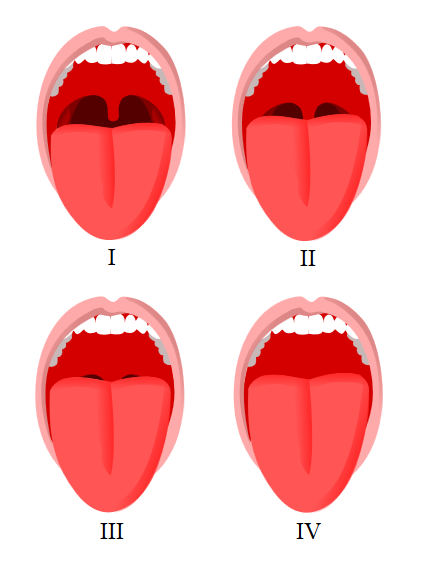
Mallampati Score Classification. This image shows the visual differences in oropharyngeal anatomy used to assign Mallampati classes during airway assessment.
Jmarchn, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
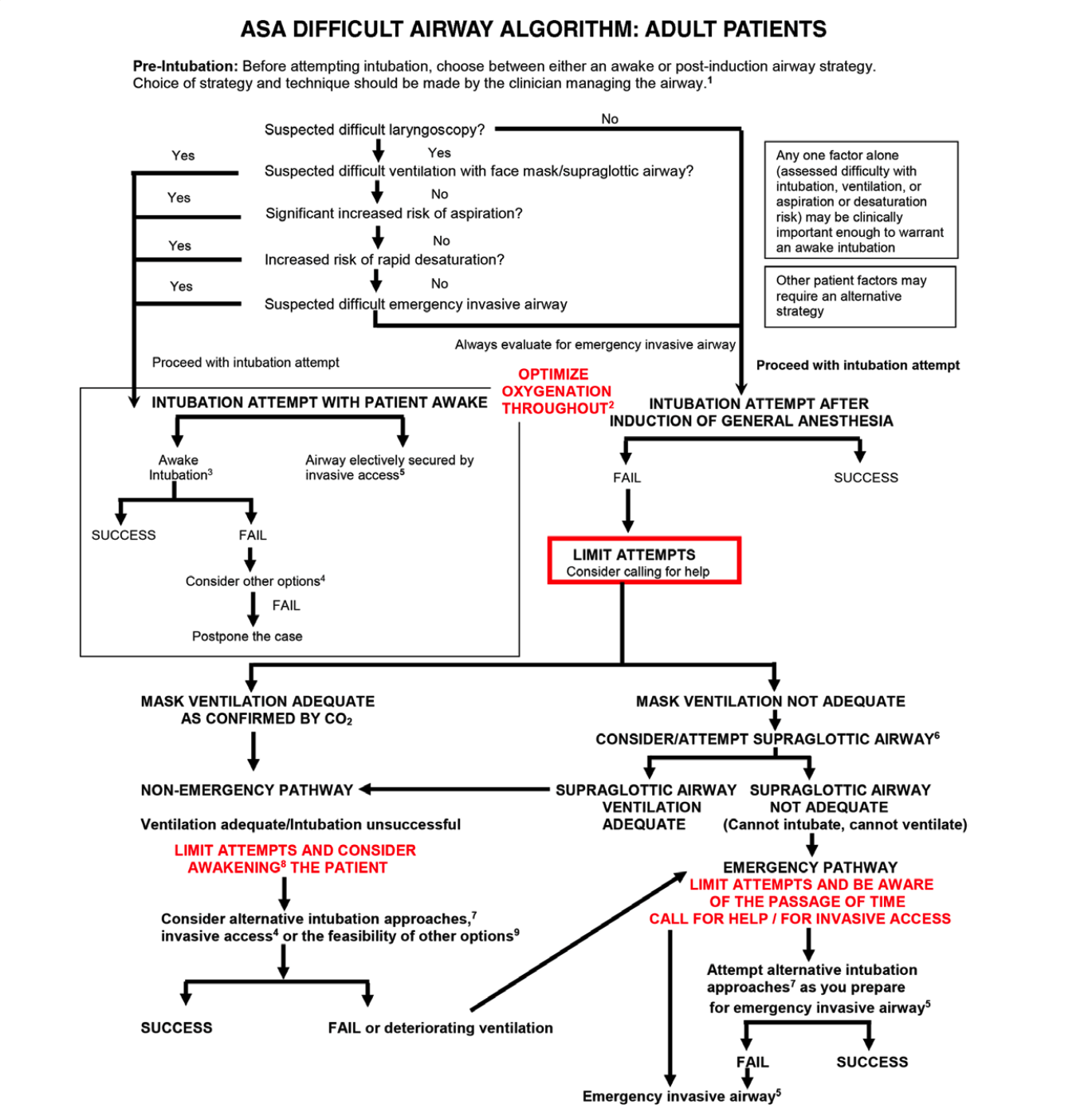
The American Society of Anesthesiologists (ASA) Difficult Airway Algorithm: Adult Patients 2022
ASA
References
Cammarota G, Simonte R, Longhini F, Spadaro S, Vetrugno L, De Robertis E. Advanced Point-of-care Bedside Monitoring for Acute Respiratory Failure. Anesthesiology. 2023 Mar 1:138(3):317-334. doi: 10.1097/ALN.0000000000004480. Epub [PubMed PMID: 36749422]
Christie J. Airway physical examination tests for detection of difficult airway management in apparently normal adult patients. International journal of nursing practice. 2020 Jun:26(3):e12805. doi: 10.1111/ijn.12805. Epub 2020 Feb 9 [PubMed PMID: 32036623]
Roth D, Pace NL, Lee A, Hovhannisyan K, Warenits AM, Arrich J, Herkner H. Bedside tests for predicting difficult airways: an abridged Cochrane diagnostic test accuracy systematic review. Anaesthesia. 2019 Jul:74(7):915-928. doi: 10.1111/anae.14608. Epub 2019 Mar 6 [PubMed PMID: 30843190]
Level 1 (high-level) evidenceLi WX, Wang DD, Li X, Li WX, Han Y, Cai YR. Risk factors for difficult mask ventilation and difficult intubation among patients undergoing pharyngeal and laryngeal surgery. Heliyon. 2023 Mar:9(3):e14408. doi: 10.1016/j.heliyon.2023.e14408. Epub 2023 Mar 6 [PubMed PMID: 36938445]
Bicalho GP, Bessa RC Jr, Cruvinel MGC, Carneiro FS, Castilho JB, Castro CHV. A prospective validation and comparison of three multivariate models for prediction of difficult intubation in adult patients. Brazilian journal of anesthesiology (Elsevier). 2023 Mar-Apr:73(2):153-158. doi: 10.1016/j.bjane.2021.07.028. Epub 2021 Aug 16 [PubMed PMID: 34411628]
Level 1 (high-level) evidenceBenavides-Zora D, Jaramillo MC, Townsley MM, Franco V, González S, Hoyos C, Cerón J, Arias-Botero JH, Sondekoppam RV, Kalagara H. Diagnostic Performance of Airway Ultrasound for the Assessment of Difficult Laryngoscopy: A Systematic Review and Meta-Analysis. Journal of cardiothoracic and vascular anesthesia. 2023 Jul:37(7):1101-1109. doi: 10.1053/j.jvca.2023.02.036. Epub 2023 Mar 2 [PubMed PMID: 37012134]
Level 1 (high-level) evidenceSotoodehnia M, Abbasi N, Bahri RA, Abdollahi A, Baratloo A. Accuracy of airway ultrasound parameters to predict difficult airway using the LEMON criteria as a reference: A cross-sectional diagnostic accuracy study. Turkish journal of emergency medicine. 2023 Jan-Mar:23(1):38-43. doi: 10.4103/2452-2473.366484. Epub 2023 Jan 2 [PubMed PMID: 36818949]
Level 2 (mid-level) evidenceSilvestri S, Ladde JG, Brown JF, Roa JV, Hunter C, Ralls GA, Papa L. Endotracheal tube placement confirmation: 100% sensitivity and specificity with sustained four-phase capnographic waveforms in a cadaveric experimental model. Resuscitation. 2017 Jun:115():192-198. doi: 10.1016/j.resuscitation.2017.01.002. Epub 2017 Jan 19 [PubMed PMID: 28111195]
Karamchandani K, Wheelwright J, Yang AL, Westphal ND, Khanna AK, Myatra SN. Emergency Airway Management Outside the Operating Room: Current Evidence and Management Strategies. Anesthesia and analgesia. 2021 Sep 1:133(3):648-662. doi: 10.1213/ANE.0000000000005644. Epub [PubMed PMID: 34153007]
Dres M, Demoule A. Monitoring diaphragm function in the ICU. Current opinion in critical care. 2020 Feb:26(1):18-25. doi: 10.1097/MCC.0000000000000682. Epub [PubMed PMID: 31876624]
Level 3 (low-level) evidenceBrochard L, Martin GS, Blanch L, Pelosi P, Belda FJ, Jubran A, Gattinoni L, Mancebo J, Ranieri VM, Richard JC, Gommers D, Vieillard-Baron A, Pesenti A, Jaber S, Stenqvist O, Vincent JL. Clinical review: Respiratory monitoring in the ICU - a consensus of 16. Critical care (London, England). 2012 Dec 12:16(2):219. doi: 10.1186/cc11146. Epub 2012 Dec 12 [PubMed PMID: 22546221]
Level 3 (low-level) evidenceRamsay M. Ventilation Monitoring. Anesthesiology clinics. 2021 Sep:39(3):403-414. doi: 10.1016/j.anclin.2021.03.006. Epub 2021 Jul 1 [PubMed PMID: 34392876]
Olsen F, Suyderhoud JP, Khanna AK. Respiratory monitoring of nonintubated patients in nonoperating room settings: old and new technologies. Current opinion in anaesthesiology. 2022 Aug 1:35(4):521-527. doi: 10.1097/ACO.0000000000001129. Epub 2022 Jul 5 [PubMed PMID: 35788554]
Level 3 (low-level) evidenceScott JB, Kaur R. Monitoring Breathing Frequency, Pattern, and Effort. Respiratory care. 2020 Jun:65(6):793-806. doi: 10.4187/respcare.07439. Epub [PubMed PMID: 32457171]
Parker W, Estrich CG, Abt E, Carrasco-Labra A, Waugh JB, Conway A, Lipman RD, Araujo MWB. Benefits and harms of capnography during procedures involving moderate sedation: A rapid review and meta-analysis. Journal of the American Dental Association (1939). 2018 Jan:149(1):38-50.e2. doi: 10.1016/j.adaj.2017.08.030. Epub [PubMed PMID: 29304910]
Level 1 (high-level) evidenceNilsson LM. Respiration signals from photoplethysmography. Anesthesia and analgesia. 2013 Oct:117(4):859-865. doi: 10.1213/ANE.0b013e31828098b2. Epub 2013 Feb 28 [PubMed PMID: 23449854]
Level 3 (low-level) evidenceGottlieb M, Holladay D, Burns KM, Nakitende D, Bailitz J. Ultrasound for airway management: An evidence-based review for the emergency clinician. The American journal of emergency medicine. 2020 May:38(5):1007-1013. doi: 10.1016/j.ajem.2019.12.019. Epub 2019 Dec 11 [PubMed PMID: 31843325]
Fernandez-Vaquero MÁ, Delgado-Cidranes E, Greif R. Next generation in ultrasound imaging to assess upper airway. Brazilian journal of anesthesiology (Elsevier). 2022 Sep-Oct:72(5):673-675. doi: 10.1016/j.bjane.2022.05.008. Epub 2022 Jun 15 [PubMed PMID: 35714713]
Ahmad I, El-Boghdadly K, Iliff H, Dua G, Higgs A, Huntington M, Mir F, Nouraei SAR, O'Sullivan EP, Patel A, Rivett K, McNarry AF. Difficult Airway Society 2025 guidelines for management of unanticipated difficult tracheal intubation in adults. British journal of anaesthesia. 2026 Jan:136(1):283-307. doi: 10.1016/j.bja.2025.10.006. Epub 2025 Nov 7 [PubMed PMID: 41203471]
Apfelbaum JL, Hagberg CA, Connis RT, Abdelmalak BB, Agarkar M, Dutton RP, Fiadjoe JE, Greif R, Klock PA, Mercier D, Myatra SN, O'Sullivan EP, Rosenblatt WH, Sorbello M, Tung A. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2022 Jan 1:136(1):31-81. doi: 10.1097/ALN.0000000000004002. Epub [PubMed PMID: 34762729]
Level 1 (high-level) evidenceZheng J, Du L, Du B, Zhang W, Zhang L, Chen G. Airway nerve blocks for awake tracheal intubation: A meta-analysis of randomized control trials and trial sequential analysis. Journal of clinical anesthesia. 2023 Sep:88():111122. doi: 10.1016/j.jclinane.2023.111122. Epub 2023 Apr 11 [PubMed PMID: 37054484]
Level 1 (high-level) evidenceShimatani T, Kyogoku M, Ito Y, Takeuchi M, Khemani RG. Fundamental concepts and the latest evidence for esophageal pressure monitoring. Journal of intensive care. 2023 May 22:11(1):22. doi: 10.1186/s40560-023-00671-6. Epub 2023 May 22 [PubMed PMID: 37217973]
Murphy GS, Brull SJ. Quantitative Neuromuscular Monitoring and Postoperative Outcomes: A Narrative Review. Anesthesiology. 2022 Feb 1:136(2):345-361. doi: 10.1097/ALN.0000000000004044. Epub [PubMed PMID: 34813652]
Level 3 (low-level) evidencePleil JD, Christensen LE. Rationale for developing tunable laser spectroscopy (TLS) technology for high resolution real-time carbon dioxide monitoring (capnography) in human breath. Journal of breath research. 2021 Sep 23:15(4):. doi: 10.1088/1752-7163/ac2723. Epub 2021 Sep 23 [PubMed PMID: 34525465]
Balakrishna A, Brunker L, Hughes CG. Anesthesia Machine and New Modes of Ventilation. Advances in anesthesia. 2022 Dec:40(1):167-183. doi: 10.1016/j.aan.2022.07.008. Epub [PubMed PMID: 36333046]
Level 3 (low-level) evidenceLockey DJ, Crewdson K, Lossius HM. Pre-hospital anaesthesia: the same but different. British journal of anaesthesia. 2014 Aug:113(2):211-9. doi: 10.1093/bja/aeu205. Epub [PubMed PMID: 25038153]