Introduction
Adenomyomatosis, also known as adenomyoma (when focal) or adenomyomatous hyperplasia of the gallbladder, is a benign condition characterized pathologically by hyperplasia of the gallbladder wall mucosa and muscularis propria, with pathognomonic epithelial invaginations forming cystic pockets (Rokitansky-Aschoff sinuses). Adenomyomatosis is 1 of the 2 hyperplastic cholecystoses; the other is cholesterolosis, also known as strawberry gallbladder.
Gallbladder thickening in adenomyomatosis can have 1 of 3 patterns:
- Focal (most common): Usually fundal; may be difficult to distinguish from a malignant neoplasm
- Segmental (annular): Usually in the body of the gallbladder; may cause stricturing, resulting in compartments and an hourglass configuration of the gallbladder
- Diffuse: Generalized thickening of the gallbladder wall [1]
When characteristic imaging findings are absent, adenomyomatosis may be difficult to distinguish from gallbladder carcinoma. Adenomyomatosis is frequently asymptomatic but may present with abdominal pain. Accurate differentiation from gallbladder carcinoma is essential because management strategies and clinical outcomes differ substantially.[2][3][4][5]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The cause of adenomyomatosis remains unknown; however, it is often associated with cholelithiasis, and some authors have proposed that it is a response to chronic cholecystitis.[6][7] Although generally considered benign, some forms of gallbladder adenomyomatosis are considered precancerous lesions.
Epidemiology
Adenomyomatosis has been found in 2% to 7.8% percent of cholecystectomy specimens.[1] Although patients are found across a wide age range, they are most frequently diagnosed in the sixth decade of life. Reports vary regarding sex distribution, although it may be slightly more common in women; there is no known racial predilection.[8]
Pathophysiology
Adenomyomatosis is a noninflammatory hyperplasia of the gallbladder wall characterized by Rokitansky-Aschoff sinuses. Gallstones are present in up to 90% of patients with the segmental type and in approximately 50% of patients with diffuse or fundal types.[9] Cholesterol crystals are often seen within the sinuses.
Histopathology
Rokitansky-Aschoff sinuses are intramural diverticula seen on histopathologic examination of adenomyomatosis specimens and appear cystic on ultrasonography. Gallstones or cholesterol crystals may be found in the sinuses. Gallbladder wall thickening results from epithelial hyperplasia and hypertrophy of the muscularis propria.
Thickening of the subserosa is also present, and nerve trunks are often seen in this layer. The surface epithelium may exhibit variable morphology, including reactive epithelial changes, papillary architecture, or metaplasia. Rarely, perineural and intraneural invasion into the subserosa may be present, but the serosa is never involved.[10]
History and Physical
Most patients with gallbladder adenomyomatosis are asymptomatic. Some affected individuals report right upper quadrant abdominal pain. However, this symptom is sometimes observed in cholelithiasis; the relationship between pain and adenomyomatosis remains unclear.
Evaluation
In patients presenting with right upper quadrant abdominal pain, transabdominal ultrasonography should be the primary diagnostic modality. Ultrasonography findings may be characteristic of adenomyomatosis and can aid in diagnosis. When the diagnosis is uncertain on ultrasonography, MRI is preferred as the next diagnostic option.[11] Furthermore, gallbladder wall thickening may be an incidental finding on computed tomography, and transabdominal ultrasonography or MRI may be useful for further characterization. In addition to gallbladder wall thickening, ultrasonography may show small (<10 mm) intramural anechoic cystic spaces or echogenic intramural foci (cholesterol crystals in Rokitansky-Aschoff sinuses) with comet-tail artifact.[1] In most cases, not all characteristic findings are present.[11][12][13]
Of the transabdominal ultrasonography findings described, the echogenic foci with associated V-shaped comet tail artifacts have been described as specific for adenomyomatosis (see Image. Adenomyomatosis). On MRI, adenomyomatosis is demonstrated by thickening of the gallbladder wall and T2-hyperintense intramural cystic spaces. Calculi are seen as signal voids. The T2-hyperintense cystic areas can align in a curvilinear fashion, producing a characteristic pearl necklace sign. On CT imaging, nonspecific thickening and enhancement of the gallbladder wall are sometimes observed. The rosary sign can be present, caused by a thin layer of enhancing epithelium lining the intramural diverticula, surrounded by hypoenhancing, hypertrophied muscularis, which gives the gallbladder wall a rosary-like appearance.[1]
Specific imaging findings can enhance diagnostic confidence and reduce the need for indeterminate radiologic assessments. On transabdominal ultrasonography, true intramural echogenic foci of adenomyomatosis persist and continue to generate a V-shaped comet-tail artifact. In contrast, adherent stones or sludge often shift or layer with changes in patient position. Color Doppler ultrasonography may show a twinkling artifact within intramural foci, supporting the diagnosis of adenomyomatosis. When gallbladder wall thickening is focal and the artifact is equivocal, short cine sweeps at different insonation angles can help reveal the classic appearance.
On MRI, T2-weighted images depict clustered, high-signal intramural cysts that may align to form a pearl-necklace sign, and diffusion-weighted imaging typically shows no convincing restricted diffusion compared with carcinoma. On magnetic resonance cholangiopancreatography, tiny intramural cysts parallel to the normal lumen further support the diagnosis of adenomyomatosis. On computed tomography (CT), gallbladder mural thickening and enhancement are nonspecific, but the cotton ball sign is seen in approximately 75% of cases of adenomyomatosis. This sign is recognized when contrast-enhanced CT demonstrates gray, fuzzy, enhancing dots in the gallbladder wall, or a dotted external border of an inner enhancing layer of the wall.[14]
Treatment / Management
If adenomyomatosis is diagnosed conclusively and is asymptomatic, no treatment is recommended, and follow-up imaging is not required.[15][16]
Cholecystectomy is recommended in the following situations:
- When adenomyomatosis cannot be reliably distinguished from gallbladder cancer
- When associated with an anomalous biliopancreatic junction, a risk factor for gallbladder cancer
- When associated with right upper quadrant pain [15]
Differential Diagnosis
The differential diagnosis for adenomyomatosis of the gallbladder includes the following:
- Gallbladder malignant neoplasms (eg, adenocarcinoma, cholangiocarcinoma, and metastasis)
- Gallbladder polyps
- Benign gallbladder tumors (eg, adenoma)
- Normal variant appearances of the gallbladder, such as gallbladder folds (eg, Phrygian cap)
Prognosis
Adenomyomatosis is a benign condition and carries a good prognosis. Although many patients are asymptomatic, some have right upper quadrant pain. Adenomyomatosis may be detected incidentally on imaging, but a malignant neoplasm can have a similar appearance. Notably, gallbladder carcinoma has a much worse prognosis (less than 5% 5-year survival).[7] Therefore, it is vital to ensure that the imaging diagnosis of adenomyomatosis is conclusive before attributing the finding to a benign process.
Complications
Adenomyomatosis may be associated with gallstones and cholecystitis. Gallbladder cancer may occur in association with segmental or diffuse adenomyomatosis, but has not been reported as a complication of fundal adenomyomatosis.[17] Progressive lesion growth alone is not indicative of a malignant neoplasm.[1]
Consultations
Consultations typically requested include the following:
- Radiologists
- Radiology technologists
- Registered diagnostic medical sonographers
- Primary care clinicians
- Gastroenterologists
- General surgeons
Deterrence and Patient Education
Patient education is key to successfully caring for patients presenting with right upper quadrant abdominal pain. Nurses play a crucial role in collaborating with clinicians to educate patients about the signs and symptoms of gallbladder adenomyomatosis. The nurse should encourage patients to promptly report any worsening of symptoms to their clinicians. When possible, written educational material should be provided to patients with gallbladder adenomyomatosis. Patient education should emphasize the benign nature of the condition, typical imaging features, and when to follow up or seek surgical consultation for persistent symptoms.
Pearls and Other Issues
Adenomyomatosis of the gallbladder is frequently asymptomatic and detected incidentally. However, some patients may have right upper quadrant pain. On ultrasonography, echogenic foci with V-shaped comet tail artifacts in the gallbladder wall are considered specific for adenomyomatosis. When asymptomatic, adenomyomatosis does not require treatment. However, adenomyomatosis can sometimes be difficult to distinguish from gallbladder cancer. Therefore, cholecystectomy is recommended for patients with right upper quadrant abdominal pain or when a gallbladder abnormality, such as nonspecific gallbladder wall thickening, cannot be confidently diagnosed as adenomyomatosis rather than a malignant gallbladder neoplasm.[18]
Enhancing Healthcare Team Outcomes
Adenomyomatosis of the gallbladder is rare but can be mistaken for several other gastrointestinal tract disorders. Because the condition can present with nonspecific symptoms, the primary care clinician may consult a gastroenterologist or a general surgeon to deliver the best care for these patients. Most cases do not require any treatment. However, if focal gallbladder wall thickening is present and cannot be definitively diagnosed as benign, a malignant neoplasm must be excluded by a primary care clinician or a specialist, such as a gastroenterologist or surgeon.
Nurses play a crucial role in assisting clinicians in diagnosis and management. Nurses should ensure the patients understand the underlying pathology, diagnosis, and its implications. The nurse should help the patients and their families during shared decision-making. When possible, patients should receive written information about their condition. Nurses should liaise with the healthcare team members, ensure patients are well-informed about their care plans, and provide reassurance if no treatment is required. Nurses should alert the clinician to any significant changes during the patient's illness. Effective communication and collaboration among interprofessional team members are necessary for optimizing care for patients with adenomyomatosis of the gallbladder.
Media
(Click Image to Enlarge)
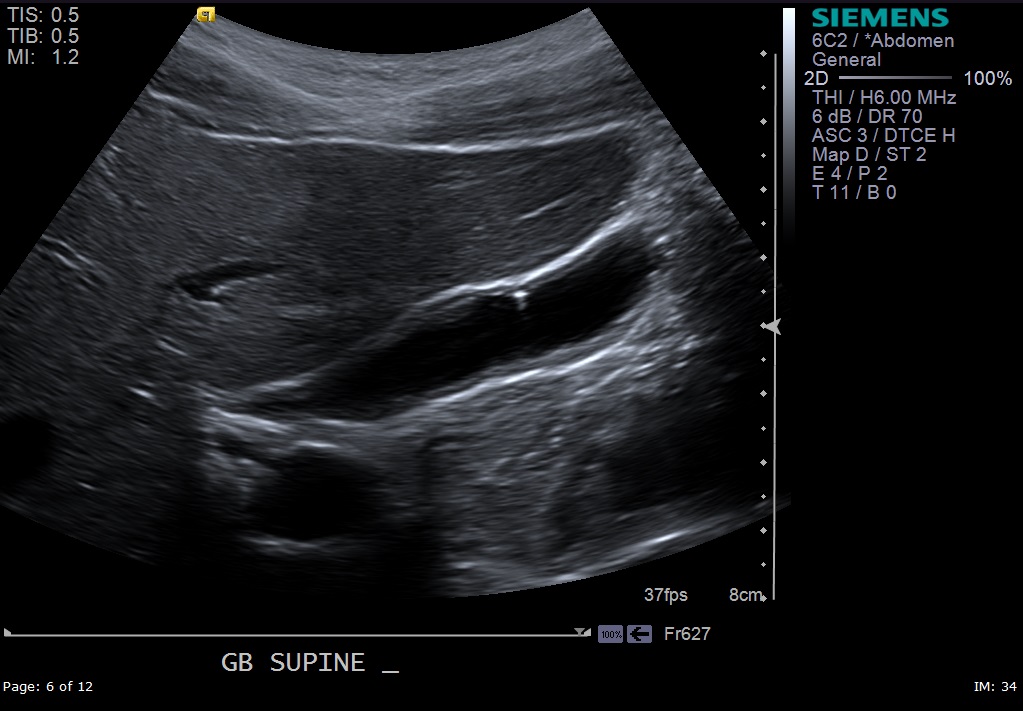
Adenomyomatosis. Long-axis grayscale sonographic image demonstrates an echogenic focus with an associated V-shaped comet-tail artifact, characteristic of adenomyomatosis.
Contributed by J Joshi, MD
References
Riddell ZC, Corallo C, Albazaz R, Foley KG. Gallbladder polyps and adenomyomatosis. The British journal of radiology. 2023 Feb:96(1142):20220115. doi: 10.1259/bjr.20220115. Epub 2022 Jul 1 [PubMed PMID: 35731858]
Yang HK, Lee JM, Yu MH, Lee SM, Park J, Han NY, Lee K, Jang JY, Han JK. Correction to: CT diagnosis of gallbladder adenomyomatosis: importance of enhancing mucosal epithelium, the "cotton ball sign". European radiology. 2019 Feb:29(2):1060. doi: 10.1007/s00330-018-5548-2. Epub [PubMed PMID: 29974218]
Malik DG, Dahiya N, Lubner MG, Pickhardt PJ, Elsayes KM, Robinson KA, Menias CO. Spectrum of imaging findings in hyperplastic cholecystosis and potential mimics. Abdominal radiology (New York). 2023 Jan:48(1):47-62. doi: 10.1007/s00261-022-03680-5. Epub 2022 Oct 2 [PubMed PMID: 36183294]
Mejri A, Arfaoui K, Omri A, Rchidi J, Mseddi MA, Saad S. Gallbladder adenomyomatosis: Diagnosis and management. International journal of surgery case reports. 2021 Jul:84():106089. doi: 10.1016/j.ijscr.2021.106089. Epub 2021 Jun 11 [PubMed PMID: 34139417]
Level 3 (low-level) evidenceKansoun A, Bernard P. Symptomatic Gallbladder Adenomyomatosis: A rare clinical presentation. International journal of surgery case reports. 2024 Jun:119():109728. doi: 10.1016/j.ijscr.2024.109728. Epub 2024 May 3 [PubMed PMID: 38703617]
Level 3 (low-level) evidenceAgrusti A, Gregori M, Salviato T, Codrich D, Barbi E. Adenomyomatosis of the Gallbladder as a Cause of Recurrent Abdominal Pain. The Journal of pediatrics. 2018 Nov:202():328-328.e1. doi: 10.1016/j.jpeds.2018.05.020. Epub 2018 Jun 11 [PubMed PMID: 29903530]
Pang L, Zhang Y, Wang Y, Kong J. Pathogenesis of gallbladder adenomyomatosis and its relationship with early-stage gallbladder carcinoma: an overview. Brazilian journal of medical and biological research = Revista brasileira de pesquisas medicas e biologica. 2018:51(6):e7411. doi: 10.1590/1414-431x20187411. Epub 2018 May 21 [PubMed PMID: 29791592]
Level 3 (low-level) evidenceGolse N, Lewin M, Rode A, Sebagh M, Mabrut JY. Gallbladder adenomyomatosis: Diagnosis and management. Journal of visceral surgery. 2017 Oct:154(5):345-353. doi: 10.1016/j.jviscsurg.2017.06.004. Epub 2017 Aug 24 [PubMed PMID: 28844704]
Nishimura A, Shirai Y, Hatakeyama K. Segmental adenomyomatosis of the gallbladder predisposes to cholecystolithiasis. Journal of hepato-biliary-pancreatic surgery. 2004:11(5):342-7 [PubMed PMID: 15549435]
Lee KF, Hung EHY, Leung HHW, Lai PBS. A narrative review of gallbladder adenomyomatosis: what we need to know. Annals of translational medicine. 2020 Dec:8(23):1600. doi: 10.21037/atm-20-4897. Epub [PubMed PMID: 33437799]
Level 3 (low-level) evidenceMartin E, Gill R, Debru E. Diagnostic accuracy of transabdominal ultrasonography for gallbladder polyps: systematic review. Canadian journal of surgery. Journal canadien de chirurgie. 2018 Jun:61(3):200-207 [PubMed PMID: 29806818]
Level 1 (high-level) evidenceShi XC, Tang SS, Zhao W. Contrast-enhanced ultrasound imaging characteristics of malignant transformation of a localized type gallbladder adenomyomatosis: A case report and literature review. Journal of cancer research and therapeutics. 2018:14(Supplement):S263-S266. doi: 10.4103/0973-1482.183208. Epub [PubMed PMID: 29578186]
Level 3 (low-level) evidenceZhang HP, Bai M, Gu JY, He YQ, Qiao XH, Du LF. Value of contrast-enhanced ultrasound in the differential diagnosis of gallbladder lesion. World journal of gastroenterology. 2018 Feb 14:24(6):744-751. doi: 10.3748/wjg.v24.i6.744. Epub [PubMed PMID: 29456413]
Level 2 (mid-level) evidenceYang HK, Lee JM, Yu MH, Lee SM, Park J, Han NY, Lee K, Jang JY, Han JK. CT diagnosis of gallbladder adenomyomatosis: importance of enhancing mucosal epithelium, the "cotton ball sign". European radiology. 2018 Sep:28(9):3573-3582. doi: 10.1007/s00330-018-5412-4. Epub 2018 Apr 9 [PubMed PMID: 29633001]
Mahajan A, Sripathi S. Gallbladder Adenomyomatosis Mimicking Carcinoma: A Diagnostic Dilemma. Journal of global oncology. 2016 Oct:2(5):341-345. doi: 10.1200/JGO.2016.005249. Epub 2016 Jun 15 [PubMed PMID: 28717718]
Morikawa T, Okabayashi T, Shima Y, Sumiyoshi T, Kozuki A, Saisaka Y, Tokumaru T, Sui K, Iwata J, Matsumoto M, Morita S, Nishioka Y. Adenomyomatosis Concomitant with Primary Gallbladder Carcinoma. Acta medica Okayama. 2017 Apr:71(2):113-118. doi: 10.18926/AMO/54979. Epub [PubMed PMID: 28420892]
Ootani T, Shirai Y, Tsukada K, Muto T. Relationship between gallbladder carcinoma and the segmental type of adenomyomatosis of the gallbladder. Cancer. 1992 Jun 1:69(11):2647-52 [PubMed PMID: 1571894]
Bonde AA, Virarkar M, Zahid M, Jaganathan S, Menendez MJ, Calimano L, Foster BR, Fritze D, Thomas CL, Gupta P. Imaging update on gallbladder adenomyomatosis and its mimics. Clinical imaging. 2024 Jan:105():109997. doi: 10.1016/j.clinimag.2023.109997. Epub 2023 Oct 13 [PubMed PMID: 37989017]