Introduction
Achalasia represents a disorder of esophageal smooth muscle motility in which the lower esophageal sphincter fails to relax, and peristalsis in the esophageal body is absent.[1][2] This dysfunction produces an obstruction at the gastroesophageal junction, leading to progressive dysphagia to solids and liquids. Although achalasia remains uncommon and may be rarely encountered in routine clinical practice, reports indicate a rising prevalence in recent years.[3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Achalasia is believed to result from degeneration of the myenteric plexus and vagus nerve fibers controlling the lower esophageal sphincter.[2][4] This process leads to the loss of inhibitory neurons containing vasoactive intestinal peptide and nitric oxide synthase within the esophageal myenteric plexus, with severe cases also affecting cholinergic neurons.[5][6] The precise cause of this neuronal degeneration remains unclear, although several theories have been proposed, including autoimmune mechanisms, viral infections, and genetic predisposition.[7][5] In the United States, most cases represent primary idiopathic achalasia, while secondary achalasia can occur in various conditions (eg, Chagas disease caused by Trypanosoma cruzi, esophageal infiltration from gastric carcinoma, eosinophilic gastroenteritis, lymphoma, certain viral infections, and neurodegenerative disorders).[5]
Epidemiology
Achalasia remains a very rare disorder, with an annual incidence of approximately 1 per 100,000 people and a prevalence of 10 per 100,000.[8] Outside the United States, annual incidence ranges from 0.1 to 1 per 100,000 people. The disorder does not preferentially affect a specific age, race, or gender. However, it most commonly presents between the second and fifth decades of life, with peak incidence occurring between ages 30 and 60.[8] Fewer than 2% to 5% of cases occur in children younger than 16 years. Recent studies have documented increasing hospitalizations and associated healthcare costs for achalasia over the past 16 years in the United States, particularly among patients younger than 65 and racial minorities.[8]
The incidence of achalasia rises in individuals with spinal cord injuries, primarily involving the cervical and thoracic vertebrae, though the mechanism remains unclear. Altered esophageal motility resembling achalasia also occurs in patients with anorexia nervosa. Cases of achalasia have been reported following endoscopic sclerotherapy for varices, with risk increasing alongside the number of sclerotherapy sessions. Affected patients often exhibit hypotensive peristalsis and impaired lower esophageal sphincter function.
Pathophysiology
The esophagus functions as a conduit transporting the food bolus from the mouth to the stomach while simultaneously preventing backflow of gastric contents. Coordinated peristaltic contractions in the pharynx and esophagus, combined with relaxation of the upper and lower esophageal sphincters (LES), facilitate efficient bolus transport.[5] Parasympathetic excitatory and inhibitory pathways regulate the smooth muscles of the LES, with excitatory neurotransmitters (eg, substance P and acetylcholine) and inhibitory neurotransmitters (vasoactive intestinal peptide and nitric oxide, the primary inhibitory neurotransmitter of the myenteric plexus) modulating LES pressure and relaxation. Individuals with achalasia lack noncholinergic, nonadrenergic inhibitory ganglion cells, while excitatory neurons remain intact.[9] This loss of inhibitory neurons disrupts the balance of neurotransmission, leading to a hypertensive, nonrelaxing esophageal sphincter.[7][5] Progressive neural degeneration results in excessive LES contractions and impaired regulation, leading to functional obstruction and esophageal dilatation. Over time, this dilatation causes irreversible aperistalsis and worsening obstructive symptoms, though the exact mechanism driving these changes remains unclear.
Additionally, genetic and autoimmune factors may contribute to achalasia. Studies have examined associations with polymorphisms in 3 nitric oxide synthase isoforms and specific human leukocyte antigen (HLA) classes.[9] One European study supports an autoimmune mechanism, suggesting that autoantibodies may interact with DNA in a manner similar to that seen in type 1 diabetes and lupus. Genetic association studies identified an 8-residue insertion at positions 227 to 234 in the cytoplasmic tail of HLA-DQß1 as the strongest known risk factor for achalasia. Two additional amino acid substitutions in the extracellular region of HLA-DQα1 at position 41 and HLA-DQß1 at position 45 act as independent risk factors.[10] Replication studies confirmed these findings and revealed a higher frequency of the insertion among southern Europeans than among northern Europeans, demonstrating a geospatial north-south gradient across the continent.[11]
Histopathology
Histopathological findings in advanced achalasia treated with total thoracic esophagectomy show a significant reduction in the number of myenteric ganglion cells, with complete absence in some patients. Commonly seen inflammatory changes in the myenteric nerves comprise a mixture of lymphocytes, eosinophils (in all cases), and sometimes plasma and mast cells. Also, the myenteric nerves are focally or wholly replaced by collagen.[12][7]
Other extramyenteric morphological features include submucosal periductal or glandular inflammation, muscular hypertrophy with secondary degeneration and fibrosis, diffuse squamous hyperplasia, lymphocytic mucosal esophagitis or inflammation of the lamina propria and submucosa with prominent germinal centers, infiltration of the muscularis externa and propria by activated eosinophils.[7][12] Activated eosinophils cause damage to tissues by producing cytotoxic eosinophil granule proteins, eg, eosinophil-derived neurotoxin, eosinophilic cationic protein, and eosinophil major basic protein.[13] The cause of the inflammation observed in achalasia remains unclear, with uncertainty as to whether it results directly from ongoing nerve damage or arises as a secondary response to the disorder.[7][12] A study comparing histopathological changes in early and advanced achalasia concluded that myenteric inflammation, accompanied by ganglion cell injury, represents the initial pathological event, ultimately leading to loss of these neurons and subsequent fibrosis of the myenteric nerves.[14]
History and Physical
Heartburn may be present in 27% to 42% of patients, leading to frequent misdiagnosis and initial treatment for gastroesophageal reflux disease (GERD).[15] Clinical suspicion for achalasia should be heightened in patients with persistent GERD symptoms despite treatment with proton pump inhibitors (PPIs). The majority of patients with achalasia present with dysphagia, initially affecting solids more than liquids; however, 70% to 97% of patients experience difficulty swallowing both solids and liquids at presentation.[16] Dysphagia and regurgitation represent the most common presenting symptoms. More than half of patients report chest pain, which rarely improves even with enhanced esophageal emptying. As the disease progresses, patients may experience regurgitation with potential aspiration, nocturnal cough, heartburn, and rapid weight loss due to impaired swallowing. Less common symptoms include hiccups and difficulty belching. Dysphagia and regurgitation tend to respond better to treatment targeting underlying achalasia.
Extra-esophageal manifestations often include structural or functional pulmonary abnormalities, likely resulting from recurrent aspiration or tracheal compression caused by a dilated esophagus. Severe cervical esophageal dilatation can produce a “bullfrog neck” appearance, leading to tracheal obstruction and stridor. Symptom distribution does not follow a consistent gender pattern. However, some studies indicate higher chest pain prevalence in women or in patients younger than 40, with variations dependent on the population studied.[17][5][18] Physical examination typically proves nondiagnostic but may reveal an emaciated individual.
The Eckardt symptom score is a widely used grading system for evaluating symptom severity, disease stage, and treatment efficacy. This system scores the four most common symptoms—weight loss, chest pain, dysphagia, and regurgitation—on a scale of 0 to 3, with a maximum total of 12. Scores of 0 to 1 correspond to clinical stage 0, 2 to 3 to stage 1, 4 to 6 to stage 2, and scores above 6 to stage 3. Stages 0 and 1 generally indicate disease remission, while stages 2 and 3 reflect treatment failure.[16]
Evaluation
Clinical suspicion of achalasia requires prompt diagnostic evaluation, as symptoms alone do not reliably establish the diagnosis. Excluding benign and malignant causes of lower esophageal obstruction proves essential in the diagnostic process.[16]
A barium esophagogram, or barium swallow, is the preferred initial test for achalasia (see Image. Barium Swallow Study). Classic findings include smooth tapering of the lower esophagus to a “bird’s beak” appearance, proximal esophageal dilatation, and absent peristalsis during fluoroscopy (see Image. Achalasia). Some cases reveal an air-fluid level and absence of intra-gastric air. Advanced disease may produce a sigmoid-shaped esophagus. A timed barium swallow evaluates esophageal emptying by having the patient ingest 236 mL of barium in an upright position, followed by radiographs at 1, 2, and 5 minutes. Pretreatment and posttreatment measurements of barium column height and esophageal width provide an objective assessment.[16][18]
Upper endoscopy (esophagogastroduodenoscopy [EGD]) is recommended for all patients with suspected achalasia or dysphagia to rule out premalignant or malignant lesions that lead to esophageal outlet obstruction and a pseudoachalasia presentation.[16] EGD demonstrates low sensitivity in early achalasia and may appear normal. Advanced findings include a rosette appearance of the esophagogastric junction or a dilated, tortuous, atonic esophagus often containing retained food, liquid, and saliva. Chronic stasis can produce esophagitis. Moderate to significant resistance when passing the scope through the esophagogastric junction. This finding, particularly in older patients or those with short symptom duration and significant weight loss, should raise concern for pseudoachalasia, where infiltrative malignancy leads to a functional obstruction. Additional studies for suspected pseudoachalasia include a contrasted computed tomography (CT) scan, an endoscopic ultrasound to evaluate submucosal lesions, and a transabdominal ultrasound. Concomitant erosive esophagitis may suggest a peptic stricture secondary to chronic GERD.[16][18]
Esophageal manometry represents the most sensitive diagnostic tool and remains the gold standard (see Image. Achalasia Manometry).[19] Manometry reveals incomplete LES relaxation in response to swallowing, absent peristalsis in the distal esophagus, and elevated LES pressure. High-resolution manometry (HRM) has largely replaced conventional techniques and provides pressure topography plotting.[16][18][19] Using HRM, achalasia is classified by the Chicago Classification (version 4.0) into 3 subtypes with distinct prognostic and treatment implications (see Image. Types of Achalasia).[20] All subtypes demonstrate incomplete LES relaxation, measured by the integrated relaxation pressure (IRP), with values above 15 mm Hg considered elevated, and 100% absent peristalsis, defined as all swallows showing either failed peristalsis or premature contraction. Type 1 (classic) exhibits distal esophageal aperistalsis without pressurization, type 2 shows aperistalsis with panesophageal pressurization in at least 20% of swallows, and type 3 demonstrates premature/spastic contractions in at least 20% of swallows and no normal peristalsis.
Impedance planimetry using the functional lumen imaging probe (FLIP) provides additional diagnostic and management insight for achalasia and other motility disorders. FLIP measures cross-sectional area (CSA), minimum diameter (Dmin), balloon pressure, and distensibility index of the lower esophageal sphincter (LES).[21] In one study, the mean distensibility index increased from 1.3 ± 1.0 premyotomy to 4.3 ± 1.7 postmyotomy.[22] FLIP is increasingly utilized intraoperatively to assess the adequacy of myotomy.
Recommended diagnostic and management steps for patients with dysphagia or suspected achalasia include:
-
Timed barium esophagogram to evaluate barium transit and structural details, eg, esophageal dilatation, LES morphology, and presence of hiatal hernia
-
Esophageal manometry to assess for incomplete LES relaxation, elevated resting LES pressure, and absence of esophageal peristalsis
-
Prolonged esophageal pH monitoring to rule out gastroesophageal reflux and assess treatment-induced reflux
-
EGD to exclude malignancy of the gastroesophageal junction or fundus (ie, pseudoachalasia)
-
Concomitant endoscopic ultrasonography when tumor suspicion exists
Treatment / Management
Treatment aims to ease the symptoms of achalasia by reducing outflow resistance caused by a nonrelaxing, hypertensive lower esophageal sphincter. Current treatment modalities for primary idiopathic achalasia include nonsurgical and surgical approaches. Nonsurgical options primarily involve pharmacotherapy, endoscopic botulinum toxin injection, or pneumatic dilatation. Surgical options include laparoscopic Heller myotomy and Per Oral Endoscopic Myotomy (POEM).
Type 2 achalasia achieves the most favorable treatment response, while type 3 responds least.[23][24] Pneumatic dilation serves as the first-line treatment for most subtypes, while surgical myotomy is indicated for types 1 and 2, depending on response. Type 3 may respond better to initial peroral endoscopic myotomy (POEM).[16][18][19] Clinicians should also recognize esophagogastric junction outflow obstruction (EGJOO), characterized by elevated IRP with preserved esophageal peristalsis; management follows standard dysphagia pathways.[20](A1)
Nonsurgical Management
Pharmacologic treatments include nitrates, calcium channel blockers, and phosphodiesterase-5 inhibitors to reduce LES pressure. Calcium channel blockers inhibit calcium entry into cells, thereby blocking smooth muscle contraction and decreasing LES pressure. Hypotension, pedal edema, headache, the rapid development of tolerance, and incomplete symptom improvement are limiting factors to its use. Nitrates increase nitric oxide concentrations in smooth muscle, raising cyclic adenosine monophosphate levels and leading to smooth muscle relaxation. However, these treatments are less effective, provide only short-term relief of symptoms, and are primarily reserved for patients who are awaiting or not candidates for more definitive therapy, eg, pneumatic dilatation or surgery.[18][19]
Endoscopic injection of botulinum toxin A (BTA) can be used in high-risk patients or those who relapse after myotomy. BTA injection may also be diagnostic and help predict response to surgical treatment. Botulinum toxin, derived from Clostridium botulinum, is a potent biological neurotoxin known to block the release of acetylcholine at the level of the lower esophageal sphincter.[18] A dosage of 100 units of botulinum is injected in equal parts in the 4 quadrants of the squamocolumnar junction with a sclerotherapy needle. This treatment is useful in patients who may not be candidates for surgery or dilatation, or as a bridge to more definitive therapy. Limitations to botulinum toxin injections include that the effect is short-lived (lasting about 6 to 12 months), patients often require expensive multiple treatments, and an increased risk of esophageal injury in patients undergoing a surgical myotomy is present.[25][18][19][26](A1)
Pneumatic dilatation of the esophagus via endoscopy is the most cost-effective nonsurgical therapy for achalasia.[18][19] Dilatation of the esophagus is achieved by disrupting the circular fibers of the LES with air pressure using a graded dilator approach. Symptoms have been shown to improve in approximately 50% to 93% of patients; however, 30% of patients have symptom recurrence at 5 years.[27] In some patients with symptom recurrence, repeat on-demand pneumatic dilatation will achieve long-term remission. With on-demand repeat pneumatic dilatation, long-term symptom relief is similar to that with myotomy.[28][18][19] (A1)
The failure rate with pneumatic dilation is higher with male gender, younger patients (younger than 40), those with pulmonary complications, or failure of 1 or more previous pneumatic dilatations.[18] In young men, graded pneumatic dilation with a 3 cm balloon is more likely to fail compared to older men or women. Also, this group of patients has a higher risk of failure when starting with a 3 cm balloon.[29] The most common procedure-related complications are minor, but severe complications, eg, esophageal perforation, may occur and should be treated accordingly. Esophageal perforation occurs in 1.6% of dilations, with increased risk in patients aged >65 years.[30] Pneumatic dilatation is the first treatment option for a patient in whom surgery fails. If this also fails, the cause of the failure must be identified using imaging studies before attempting a second operation. (B2)
Surgical Management
Surgical myotomy represents the recommended intervention for reducing pressure across the lower esophageal sphincter and can be performed using a laparoscopic approach.[31] The procedure involves division of the longitudinal and circular muscle fibers spanning the lower esophageal sphincter, resulting in sphincter relaxation. A myotomy length of at least 6 cm across the lower esophageal sphincter and gastroesophageal junction is recommended. Shorter myotomies correlate with inadequate symptom relief, whereas longer extensions onto the gastric side increase the risk of postoperative reflux.[32]
Because laparoscopic Heller myotomy (LHM) carries a risk of gastroesophageal reflux, the procedure is often combined with an antireflux procedure, e.g., a posterior Toupet or an anterior Dor partial fundoplication (see Image. Heller Myotomy). Both techniques demonstrate comparable effectiveness in reducing postoperative GERD. Laparoscopic Heller myotomy combined with partial fundoplication remains the surgical treatment of choice, as partial rather than complete fundoplication minimizes the risk of postoperative dysphagia, which occurs more frequently with Nissen fundoplication.[18][19] Clinical success rates range from 76% to 100% at 35 months, with a mortality rate of 0.1%. Disease progression beyond 5 years is associated with declining long-term success. Clinicians can find the techniques for laparoscopic Heller myotomy outlined in demonstration videos.[SAGES. Laparoscopic Heller Myotomy.2026]
POEM is an effective minimally invasive alternative to LHM to treat achalasia at tertiary, specialized centers and is the recommended treatment for type 3 achalasia.[33] Intraoperative use of FLIP technology helps to tailor the length of myotomy. Dissection of the circular fibers of the LES is performed endoscopically, thereby relaxing the LES. Short (2-3 cm) versus long (7-8 cm) endoscopic myotomies have been used for the treatment of type 1 and 2 achalasia. Recent meta-analysis and randomized controlled trial data demonstrate similar efficacy, safety profiles, and GERD risk in both approaches, but a short myotomy results in shorter procedure time.[33][34] The risk of GERD is high (up to 50%) after POEM with alcohol use and being overweight (BMI ≥25 kg/m2) as positive predictive factors of moderate to severe reflux esophagitis.[35][36] Evaluation with endoscopy and/or pH monitoring is strongly advised within 6 to 12 months after POEM to obtain objective data on abnormal esophageal acid exposure and to exclude other causes of heartburn, eg, visceral hypersensitivity.[37] Recent advances in endoscopic treatment of post-POEM GERD include transoral incisionless fundoplication (TIF).[36](A1)
A debate related to which surgical option is superior, POEM or LHM, for patients with achalasia is ongoing. Both options provide equivalent relief of dysphagia, which is the primary complaint. POEM being endoscopic is less morbid, while the laparoscopic Heller myotomy offers the advantage of adding a fundoplication and minimizing postoperative reflux, which is higher with POEM but usually managed adequately with PPIs.[32] In one meta-analysis, the pooled rate of abnormal acid exposure at pH monitoring was 39.0% (95% CI 24.5%–55.8%) after POEM and 16.8% (95% CI 10.2%–26.4%) after laparoscopic Heller myotomy. The rate of esophagitis after POEM was 29.4% (95% CI 18.5%–43.3%) and 7.6% (95% CI 4.1%–13.7%) after laparoscopic Heller myotomy. Clinical success was higher in POEM (RR = 1.06; P = 0.01), with shorter procedure time (median 39.53 minutes; P < 0.01) and shorter length of stay (mean difference of -0.51 day; P = 0.03), and similar major adverse events ( P = 0.81).[38] A more recent multicenter randomized controlled trial from Europe had similar findings.[39](A1)
Esophagectomy is the last resort for terminal cases known as "end-stage achalasia" that have persistent symptoms and an inability to empty the esophagus.[40] (A1)
Differential Diagnosis
When a patient presents with dysphagia, the potential for an underlying malignant etiology should be considered. Dysphagia due to achalasia should be differentiated from gastric outlet obstruction, where the complaint is more vomiting than difficulty swallowing. Other differential diagnoses that should be considered in patients with dysphagia include:
- Diffuse esophageal spasm
- Esophagogastic junction outflow obstruction
- Scleroderma
- Esophageal adenocarcinoma
- GERD
- Peptic stricture
- Schatzki ring
- Epiphrenic diverticulum
- Hiatal hernia/paraesophageal hernia
Prognosis
The use of pneumatic dilatation, POEM, and laparoscopic myotomy can produce good results with symptom relief. Rates of esophageal perforation are rare after pneumatic dilatation, but relapses can occur, requiring subsequent intervention. The risk of GERD following myotomy is high, and thus, a Heller myotomy is often combined with a fundoplication. Similarly, patients who undergo POEM should be closely monitored for signs of GERD with objective testing via EGD or pH testing within 6 to 12 months.
Achalasia is associated with an increased risk for esophageal cancer. A recent cohort study showed this risk is 5-fold higher than in patients without achalasia.[41] While no standardized screening recommendations have been established at this time, healthcare professionals should have a heightened awareness, particularly if other risk factors are present, eg, family history, tobacco, and alcohol use.
Complications
Complications associated with achalasia include:
- Esophageal perforation
- GERD
- Bloating
- Incomplete myotomy/recurrence
- Potential esophageal cancer risk (squamous cell carcinoma and adenocarcinoma)
Postoperative and Rehabilitation Care
All patients who undergo treatment for achalasia need long-term follow-up because all available treatments are palliative, making recurrences common. Additionally, some treatments for achalasia may result in the development of reflux disease, which may require additional treatment beyond PPIs.
Consultations
Consultation with a foregut trained surgeon and a gastroenterologist is essential for the management of achalasia.
Deterrence and Patient Education
Deterrence strategies for achalasia focus on early recognition, prevention of complications, and patient engagement, as no known measures prevent disease onset. The underlying precipitating factor remains undefined despite extensive research, with proposed mechanisms including a viral trigger initiating an autoimmune response in genetically susceptible individuals. Current evidence has not confirmed these theories. Available therapies do not halt disease progression but instead target symptom relief by reducing lower esophageal sphincter outflow resistance to improve dysphagia, chest pain, and regurgitation while limiting complications, eg, GERD, weight loss, aspiration, and progression to megaesophagus. Early diagnosis, appropriate use of manometry and imaging, and timely referral for endoscopic or surgical intervention reduce morbidity and support long-term symptom control.
Patient education plays a central role in management, as achalasia follows a chronic, lifelong course. Patients benefit from counseling that treatment improves swallowing, but does not restore normal esophageal peristalsis, and residual dysphagia may persist despite successful therapy. Education should emphasize realistic expectations, adherence to follow-up, and recognition of reflux or aspiration symptoms. Postmyotomy lifestyle modifications include consuming small food boluses, eating in an upright position to facilitate gravity-assisted esophageal emptying, and avoiding a flat supine position. Elevation of the head of the bed to 30 to 45 degrees reduces aspiration risk and supports safer long-term outcomes.
Pearls and Other Issues
Pneumatic dilatation, POEM, and laparoscopic myotomy are effective treatments for managing achalasia. Laparoscopic Heller myotomy or POEM is more effective and durable, provided the expertise is available. Botulinum toxin and medical therapies are inferior treatment options often reserved for patients who are not surgical candidates or high risk for endoscopic intervention.
Enhancing Healthcare Team Outcomes
Achalasia is a rare, chronic esophageal motility disorder characterized by impaired lower esophageal sphincter relaxation and absent peristalsis, resulting in progressive dysphagia, regurgitation, chest pain, and weight loss. No curative therapy exists, and all current treatments remain palliative, focusing on reducing outflow resistance to improve swallowing and quality of life. Early recognition proves critical, as symptoms often resemble gastroesophageal reflux disease, and delays in diagnosis contribute to malnutrition, aspiration, and esophageal dilation. Long-term follow-up remains necessary due to potential disease progression and increased risk of esophageal cancer.
Optimal management depends on coordinated interprofessional care. Primary care clinicians, including physicians, nurse practitioners, and physician assistants, play a key role in early diagnosis, referral, and coordination between gastroenterologists, foregut surgeons, nutritionists, and pharmacists. Advanced practitioners and nurses support patient education, monitoring, and outpatient management while identifying patients who require hospitalization for dehydration, electrolyte imbalance, or severe malnutrition. Dietitians guide nutritional supplementation and dietary modifications, pharmacists ensure safe and effective medication use, and specialists counsel patients on endoscopic and surgical options with realistic expectations. Ongoing communication among team members enhances patient-centered care, safety, outcomes, and overall team performance.
Media
(Click Image to Enlarge)

Achalasia. Diagnostic imaging demonstrating beak-like narrowing of the distal esophagus with proximal distension.
Contributed by D Light, MD, MPH
(Click Image to Enlarge)

Barium Swallow Study. Barium swallow showing achalasia.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
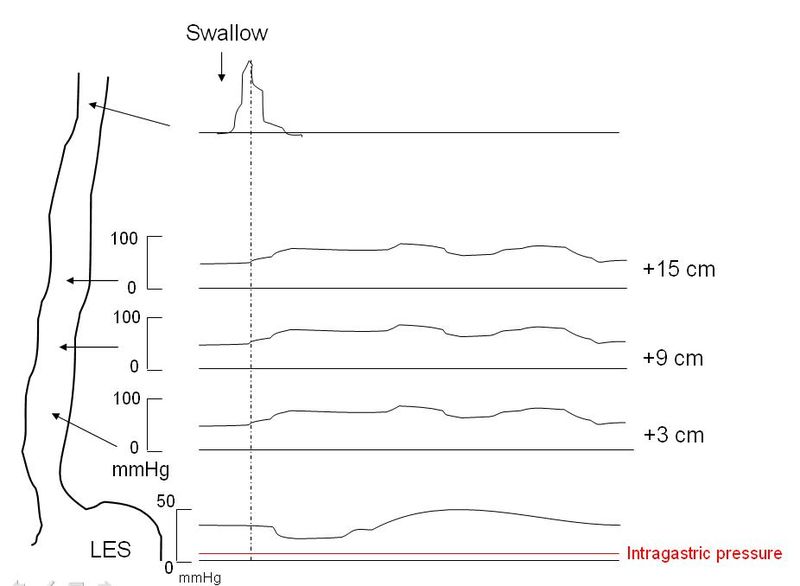
Achalasia Manometry. Manometry reveals incomplete LES relaxation in response to swallowing, absent peristalsis in the distal esophagus, and elevated LES pressure.
JC Petit, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
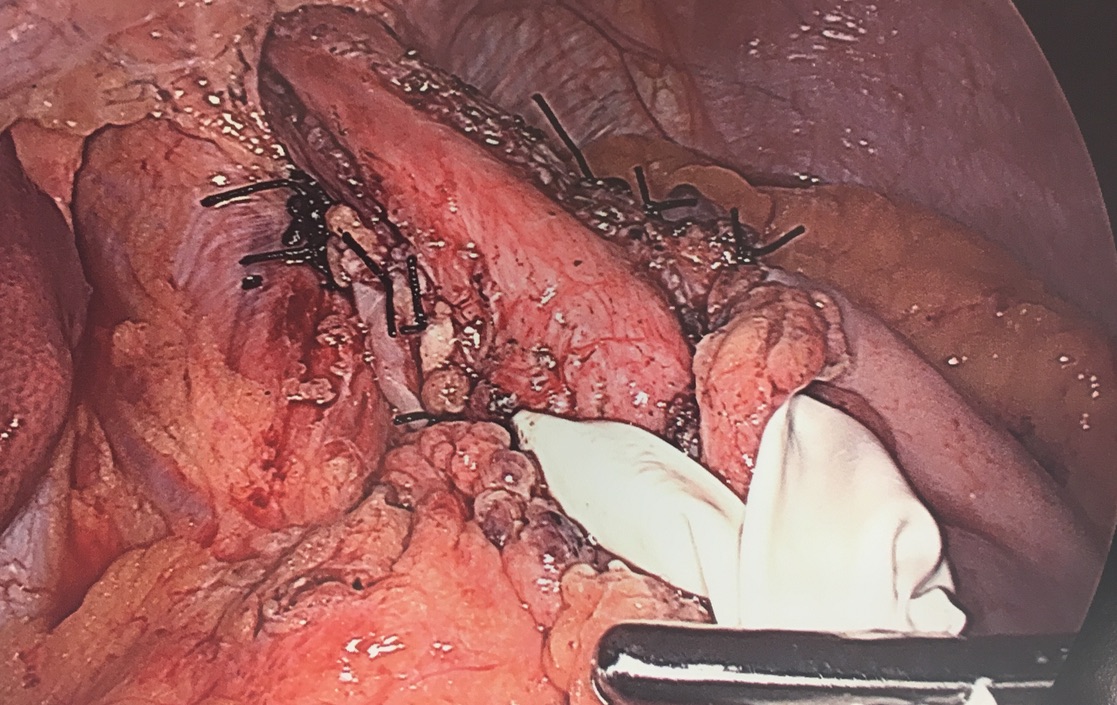
Laparoscopic Heller Myotomy. Intraoperative picture showing a completed laparoscopic Heller myotomy and a Toupet (posterior partial) fundoplication.
Contributed by R Puri, MD
(Click Image to Enlarge)
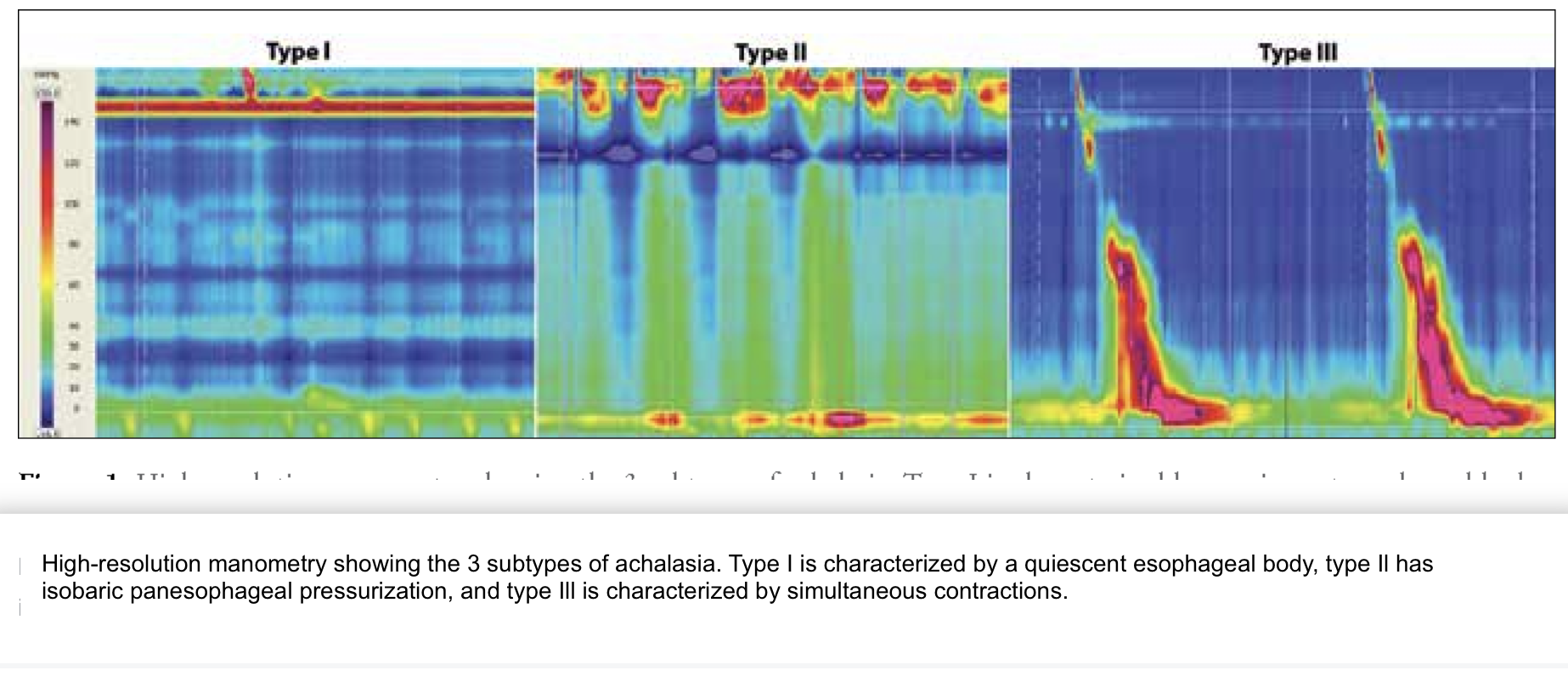
Types of Achalasia. Image of manometry demonstrating types of achalasia.
Contributed by M Vaezi, MD
References
Achem SR, Crittenden J, Kolts B, Burton L. Long-term clinical and manometric follow-up of patients with nonspecific esophageal motor disorders. The American journal of gastroenterology. 1992 Jul:87(7):825-30 [PubMed PMID: 1615935]
CASSELLA RR, ELLIS FH Jr, BROWN AL Jr. FINE-STRUCTURE CHANGES IN ACHALASIA OF ESOPHAGUS. II. ESOPHAGEAL SMOOTH MUSCLE. The American journal of pathology. 1965 Mar:46(3):467-75 [PubMed PMID: 14266221]
Lee K, Hong SP, Yoo IK, Yeniova AÖ, Hahn JW, Kim MS, Yoon SY, Rahmati M, Lee JH, Lee M, Cho W, Yon DK. Global trends in incidence and prevalence of achalasia, 1925-2021: A systematic review and meta-analysis. United European gastroenterology journal. 2024 May:12(4):504-515. doi: 10.1002/ueg2.12555. Epub 2024 Mar 2 [PubMed PMID: 38430514]
Level 1 (high-level) evidenceCASSELLA RR, ELLIS FH Jr, BROWN AL Jr. FINE-STRUCTURE CHANGES IN ACHALASIA OF THE ESOPHAGUS. I. VAGUS NERVES. The American journal of pathology. 1965 Feb:46(2):279-88 [PubMed PMID: 14256751]
Francis DL, Katzka DA. Achalasia: update on the disease and its treatment. Gastroenterology. 2010 Aug:139(2):369-74. doi: 10.1053/j.gastro.2010.06.024. Epub 2010 Jun 18 [PubMed PMID: 20600038]
Misiewicz JJ, Waller SL, Anthony PP, Gummer JW. Achalasia of the cardia: pharmacology and histopathology of isolated cardiac sphincteric muscle from patients with and without achalasia. The Quarterly journal of medicine. 1969 Jan:38(149):17-30 [PubMed PMID: 5765090]
Raymond L, Lach B, Shamji FM. Inflammatory aetiology of primary oesophageal achalasia: an immunohistochemical and ultrastructural study of Auerbach's plexus. Histopathology. 1999 Nov:35(5):445-53 [PubMed PMID: 10583560]
Wadhwa V, Thota PN, Parikh MP, Lopez R, Sanaka MR. Changing Trends in Age, Gender, Racial Distribution and Inpatient Burden of Achalasia. Gastroenterology research. 2017 Apr:10(2):70-77. doi: 10.14740/gr723w. Epub 2017 Apr 19 [PubMed PMID: 28496526]
Singh R, Ghoshal UC, Misra A, Mittal B. Achalasia Is Associated With eNOS4a4a, iNOS22GA, and nNOS29TT Genotypes: A Case-control Study. Journal of neurogastroenterology and motility. 2015 Jul 30:21(3):380-9. doi: 10.5056/jnm14123. Epub [PubMed PMID: 26088023]
Level 2 (mid-level) evidenceGockel I, Becker J, Wouters MM, Niebisch S, Gockel HR, Hess T, Ramonet D, Zimmermann J, Vigo AG, Trynka G, de León AR, de la Serna JP, Urcelay E, Kumar V, Franke L, Westra HJ, Drescher D, Kneist W, Marquardt JU, Galle PR, Mattheisen M, Annese V, Latiano A, Fumagalli U, Laghi L, Cuomo R, Sarnelli G, Müller M, Eckardt AJ, Tack J, Hoffmann P, Herms S, Mangold E, Heilmann S, Kiesslich R, von Rahden BH, Allescher HD, Schulz HG, Wijmenga C, Heneka MT, Lang H, Hopfner KP, Nöthen MM, Boeckxstaens GE, de Bakker PI, Knapp M, Schumacher J. Common variants in the HLA-DQ region confer susceptibility to idiopathic achalasia. Nature genetics. 2014 Aug:46(8):901-4. doi: 10.1038/ng.3029. Epub 2014 Jul 6 [PubMed PMID: 24997987]
Level 2 (mid-level) evidenceBecker J, Haas SL, Mokrowiecka A, Wasielica-Berger J, Ateeb Z, Bister J, Elbe P, Kowalski M, Gawron-Kiszka M, Majewski M, Mulak A, Janiak M, Wouters MM, Schwämmle T, Hess T, Veits L, Niebisch S, Santiago JL, de León AR, de la Serna JP, Urcelay E, Annese V, Latiano A, Fumagalli U, Rosati R, Laghi L, Cuomo R, Lenze F, Sarnelli G, Müller M, von Rahden BH, Wijmenga C, Lang H, Czene K, Hall P, de Bakker PI, Vieth M, Nöthen MM, Schulz HG, Adrych K, Gąsiorowska A, Paradowski L, Wallner G, Boeckxstaens GE, Gockel I, Hartleb M, Kostic S, Dziurkowska-Marek A, Lindblad M, Nilsson M, Knapp M, Thorell A, Marek T, Dąbrowski A, Małecka-Panas E, Schumacher J. The HLA-DQβ1 insertion is a strong achalasia risk factor and displays a geospatial north-south gradient among Europeans. European journal of human genetics : EJHG. 2016 Aug:24(8):1228-31. doi: 10.1038/ejhg.2015.262. Epub 2016 Jan 6 [PubMed PMID: 26733285]
Goldblum JR, Whyte RI, Orringer MB, Appelman HD. Achalasia. A morphologic study of 42 resected specimens. The American journal of surgical pathology. 1994 Apr:18(4):327-37 [PubMed PMID: 8141427]
Jin H, Wang B, Zhang LL, Zhao W. Activated Eosinophils are Present in Esophageal Muscle in Patients with Achalasia of the Esophagus. Medical science monitor : international medical journal of experimental and clinical research. 2018 Apr 19:24():2377-2383 [PubMed PMID: 29672471]
Goldblum JR, Rice TW, Richter JE. Histopathologic features in esophagomyotomy specimens from patients with achalasia. Gastroenterology. 1996 Sep:111(3):648-54 [PubMed PMID: 8780569]
Spechler SJ, Souza RF, Rosenberg SJ, Ruben RA, Goyal RK. Heartburn in patients with achalasia. Gut. 1995 Sep:37(3):305-8 [PubMed PMID: 7590421]
Laurino-Neto RM, Herbella F, Schlottmann F, Patti M. EVALUATION OF ESOPHAGEAL ACHALASIA: FROM SYMPTOMS TO THE CHICAGO CLASSIFICATION. Arquivos brasileiros de cirurgia digestiva : ABCD = Brazilian archives of digestive surgery. 2018:31(2):e1376. doi: 10.1590/0102-672020180001e1376. Epub 2018 Jul 2 [PubMed PMID: 29972404]
Fisichella PM, Raz D, Palazzo F, Niponmick I, Patti MG. Clinical, radiological, and manometric profile in 145 patients with untreated achalasia. World journal of surgery. 2008 Sep:32(9):1974-9. doi: 10.1007/s00268-008-9656-z. Epub [PubMed PMID: 18575930]
Eckardt AJ, Eckardt VF. Current clinical approach to achalasia. World journal of gastroenterology. 2009 Aug 28:15(32):3969-75 [PubMed PMID: 19705490]
Torresan F, Ioannou A, Azzaroli F, Bazzoli F. Treatment of achalasia in the era of high-resolution manometry. Annals of gastroenterology. 2015 Jul-Sep:28(3):301-308 [PubMed PMID: 26130022]
Yadlapati R, Kahrilas PJ, Fox MR, Bredenoord AJ, Prakash Gyawali C, Roman S, Babaei A, Mittal RK, Rommel N, Savarino E, Sifrim D, Smout A, Vaezi MF, Zerbib F, Akiyama J, Bhatia S, Bor S, Carlson DA, Chen JW, Cisternas D, Cock C, Coss-Adame E, de Bortoli N, Defilippi C, Fass R, Ghoshal UC, Gonlachanvit S, Hani A, Hebbard GS, Wook Jung K, Katz P, Katzka DA, Khan A, Kohn GP, Lazarescu A, Lengliner J, Mittal SK, Omari T, Park MI, Penagini R, Pohl D, Richter JE, Serra J, Sweis R, Tack J, Tatum RP, Tutuian R, Vela MF, Wong RK, Wu JC, Xiao Y, Pandolfino JE. Esophageal motility disorders on high-resolution manometry: Chicago classification version 4.0(©). Neurogastroenterology and motility. 2021 Jan:33(1):e14058. doi: 10.1111/nmo.14058. Epub [PubMed PMID: 33373111]
Pesce M, Pagliaro M, Sarnelli G, Sweis R. Modern Achalasia: Diagnosis, Classification, and Treatment. Journal of neurogastroenterology and motility. 2023 Oct 30:29(4):419-427. doi: 10.5056/jnm23125. Epub [PubMed PMID: 37814432]
Attaar M, Wong HJ, Wu H, Campbell M, Kuchta K, Denham W, Haggerty S, Linn J, Ujiki MB. Changes in impedance planimetry (EndoFLIP) measurements at follow-up after peroral endoscopic myotomy (POEM). Surgical endoscopy. 2022 Dec:36(12):9410-9415. doi: 10.1007/s00464-022-09286-8. Epub 2022 May 3 [PubMed PMID: 35505258]
Ou YH, Nie XM, Li LF, Wei ZJ, Jiang B. High-resolution manometric subtypes as a predictive factor for the treatment of achalasia: A meta-analysis and systematic review. Journal of digestive diseases. 2016 Apr:17(4):222-35. doi: 10.1111/1751-2980.12327. Epub [PubMed PMID: 26860986]
Level 1 (high-level) evidenceAndolfi C, Fisichella PM. Meta-analysis of clinical outcome after treatment for achalasia based on manometric subtypes. The British journal of surgery. 2019 Mar:106(4):332-341. doi: 10.1002/bjs.11049. Epub 2019 Jan 28 [PubMed PMID: 30690706]
Level 1 (high-level) evidenceZaninotto G, Annese V, Costantini M, Del Genio A, Costantino M, Epifani M, Gatto G, D'onofrio V, Benini L, Contini S, Molena D, Battaglia G, Tardio B, Andriulli A, Ancona E. Randomized controlled trial of botulinum toxin versus laparoscopic heller myotomy for esophageal achalasia. Annals of surgery. 2004 Mar:239(3):364-70 [PubMed PMID: 15075653]
Level 1 (high-level) evidenceCampos GM, Vittinghoff E, Rabl C, Takata M, Gadenstätter M, Lin F, Ciovica R. Endoscopic and surgical treatments for achalasia: a systematic review and meta-analysis. Annals of surgery. 2009 Jan:249(1):45-57. doi: 10.1097/SLA.0b013e31818e43ab. Epub [PubMed PMID: 19106675]
Level 1 (high-level) evidenceCsendes A, Braghetto I, Henríquez A, Cortés C. Late results of a prospective randomised study comparing forceful dilatation and oesophagomyotomy in patients with achalasia. Gut. 1989 Mar:30(3):299-304 [PubMed PMID: 2651226]
Level 1 (high-level) evidenceBoeckxstaens GE, Annese V, des Varannes SB, Chaussade S, Costantini M, Cuttitta A, Elizalde JI, Fumagalli U, Gaudric M, Rohof WO, Smout AJ, Tack J, Zwinderman AH, Zaninotto G, Busch OR, European Achalasia Trial Investigators. Pneumatic dilation versus laparoscopic Heller's myotomy for idiopathic achalasia. The New England journal of medicine. 2011 May 12:364(19):1807-16. doi: 10.1056/NEJMoa1010502. Epub [PubMed PMID: 21561346]
Level 1 (high-level) evidenceFarhoomand K, Connor JT, Richter JE, Achkar E, Vaezi MF. Predictors of outcome of pneumatic dilation in achalasia. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2004 May:2(5):389-94 [PubMed PMID: 15118976]
Level 2 (mid-level) evidenceVanuytsel T, Lerut T, Coosemans W, Vanbeckevoort D, Blondeau K, Boeckxstaens G, Tack J. Conservative management of esophageal perforations during pneumatic dilation for idiopathic esophageal achalasia. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2012 Feb:10(2):142-9. doi: 10.1016/j.cgh.2011.10.032. Epub 2011 Nov 7 [PubMed PMID: 22064041]
Bonavina L, Nosadini A, Bardini R, Baessato M, Peracchia A. Primary treatment of esophageal achalasia. Long-term results of myotomy and Dor fundoplication. Archives of surgery (Chicago, Ill. : 1960). 1992 Feb:127(2):222-6; discussion 227 [PubMed PMID: 1540102]
Patel AD, Puri R, Nau P, Race A, McCormack L, Brown A, Khaitan L, Gould JC. The SAGES MASTERS Program: top 10 seminal articles for Heller myotomy and treatment of achalasia. Surgical endoscopy. 2025 Jun:39(6):3447-3455. doi: 10.1007/s00464-025-11779-1. Epub 2025 May 5 [PubMed PMID: 40325246]
Familiari P, Borrelli de Andreis F, Landi R, Mangiola F, Boskoski I, Tringali A, Perri V, Costamagna G. Long versus short peroral endoscopic myotomy for the treatment of achalasia: results of a non-inferiority randomised controlled trial. Gut. 2023 Aug:72(8):1442-1450. doi: 10.1136/gutjnl-2021-325579. Epub 2023 Apr 18 [PubMed PMID: 37072180]
Level 1 (high-level) evidenceAlbunni H, Beran A, Hadaki N, DeWitt JM, Al-Haddad M. Short Versus Standard Peroral Endoscopic Myotomy for Esophageal Achalasia: A Meta-Analysis of Randomized Controlled Trials. Digestive diseases and sciences. 2025 Feb:70(2):685-695. doi: 10.1007/s10620-024-08825-8. Epub 2025 Jan 13 [PubMed PMID: 39806083]
Level 1 (high-level) evidenceWessels EM, Masclee GMC, Bastiaansen BAJ, Fockens P, Bredenoord AJ. Incidence and risk factors of reflux esophagitis after peroral endoscopic myotomy. Neurogastroenterology and motility. 2024 Jun:36(6):e14794. doi: 10.1111/nmo.14794. Epub 2024 Apr 8 [PubMed PMID: 38587128]
Ravi K, Ramchandani M. POEM and GERD: Prevalence, Mechanisms, Potential Strategies for Prevention, and Management. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2022 Nov:20(11):2444-2447. doi: 10.1016/j.cgh.2022.05.040. Epub 2022 Jul 13 [PubMed PMID: 35839867]
Yang D, Bechara R, Dunst CM, Konda VJA. AGA Clinical Practice Update on Advances in Per-Oral Endoscopic Myotomy (POEM) and Remaining Questions-What We Have Learned in the Past Decade: Expert Review. Gastroenterology. 2024 Dec:167(7):1483-1490. doi: 10.1053/j.gastro.2024.08.038. Epub 2024 Oct 16 [PubMed PMID: 39425737]
Level 3 (low-level) evidenceSo Taa Kum A, Nunes BCM, Moura ETH, Franco MC, de Moura EGH. Gastroesophageal reflux disease over time in endoscopic versus surgical myotomy for treatment of achalasia: Systematic review and meta-analysis. Endoscopy international open. 2025:13():a26215421. doi: 10.1055/a-2621-5421. Epub 2025 Jun 17 [PubMed PMID: 40611840]
Level 1 (high-level) evidenceHugova K, Mares J, Hakanson B, Repici A, von Rahden BHA, Bredenoord AJ, Bisschops R, Messmann H, Ruppenthal T, Mann O, Izbicki J, Harustiak T, Fumagalli Romario U, Rosati R, Germer CT, Schijven M, Emmermann A, von Renteln D, Dautel S, Fockens P, Boeckxstaens G, Rösch T, Martinek J, Werner YB. Per-oral endoscopic myotomy versus laparoscopic Heller's myotomy plus Dor fundoplication in patients with idiopathic achalasia: 5-year follow-up of a multicentre, randomised, open-label, non-inferiority trial. The lancet. Gastroenterology & hepatology. 2025 May:10(5):431-441. doi: 10.1016/S2468-1253(25)00012-3. Epub 2025 Mar 17 [PubMed PMID: 40112837]
Level 1 (high-level) evidenceAiolfi A, Asti E, Bonitta G, Bonavina L. Esophagectomy for End-Stage Achalasia: Systematic Review and Meta-analysis. World journal of surgery. 2018 May:42(5):1469-1476. doi: 10.1007/s00268-017-4298-7. Epub [PubMed PMID: 29022068]
Level 1 (high-level) evidenceLow EE, Demb J, Shah SC, Liu L, Bustamante R, Yadlapati R, Gupta S. Risk of Esophageal Cancer in Achalasia: A Matched Cohort Study Using the Nationwide Veterans Affairs Achalasia Cohort. The American journal of gastroenterology. 2024 Apr 1:119(4):635-645. doi: 10.14309/ajg.0000000000002591. Epub 2023 Nov 17 [PubMed PMID: 37975607]