Introduction
Cervical cancer screening has become one of the cornerstones of preventative screening in the gynecological world. George Papanicolaou developed cervical cytology screening, from which the term Papanicolaou test or “Pap smear” arose. Although his work began in the 1920s to 1930s, pap smears were only widely adopted into clinical practice following a landmark publication in 1943.
A Papanicolaou test collects cervical cells near the cervical transitional (transformation) zone and determines if any of them have precancerous changes. This test was historically called a Pap smear because the collected cells were traditionally smeared onto a glass slide for histological evaluation; however, with current technology, the cells now remain suspended in solution after collection. Therefore, this study is now more appropriately named the Pap test. Since 1943, few classification systems have been established to describe the different types of collected cells; the current system used in the United States is the 2014 Bethesda System for Reporting Cervical Cytology.[1]
Guidelines for Pap smear testing frequency vary between the American Society for Colposcopy and Cervical Pathology (ASCCP), American Cancer Society (ACS), United States Preventive Services Task Force (USPSTF), Society of Gynecologic Oncology (SGO), and the American College of Obstetricians and Gynecologists (ACOG), but are recommended for women aged between 21 and 65. Screening is not recommended for those younger than 21, given that the primary driver of cervical cancer, human papillomavirus (HPV), is spontaneously cleared in this age group. The prevalence of abnormal Pap tests is around 3.8%. At least 50 million Pap tests are performed yearly.[2] In 2019, an estimated 13,000 women were diagnosed with cervical cancer, and 4,000 women died from cervical cancer.[3] Although cervical cancer incidence has declined overall, recent epidemiological data suggest a modest increase in certain subgroups, including women aged 30 to 34 years, with some studies reporting annual increases of approximately 2%.[4]
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
A Pap test serves as a screening tool for detecting cellular changes in the cervix. Evidence documents variable sensitivity and specificity across different settings.[5] Because the test does not achieve 100% sensitivity, routine cervical cancer screening remains essential.[6][7] Furthermore, cervical cancer screening has also progressed beyond isolated Pap testing to incorporate HPV testing.[8]
From a societal perspective, racial disparities affect the timeliness of cervical cancer diagnosis. Localized cervical cancer diagnosis occurs in 47% of White individuals compared with 36% of Black individuals. Regional diagnosis occurs in 35% of White individuals and 41% of Black individuals.[3] Reduced rates of early detection among Black women contribute to diagnosis at more advanced stages of disease.
Causes
Human Papillomavirus Risks
The primary cause of abnormal Pap tests is associated with infection by HPV. HPV serotypes 16/18 are the most common strains that cause cervical cancer.[9] Both of these serotypes appear in 70% of cervical cancer cases. Other strains that increase risk for cervical cancer include HPV 45, 58, 51, 39, 66, and 73.[10] Lower-risk HPV serotypes include serotypes 6 and 11, but are more commonly associated with genital warts.[11] Please see StatPearls' companion resources, "Human Papillomavirus" and "Cervical Dysplasia," for further information.
Smoking Risk Factors
Smoking has also been shown to increase the risk of cervical cancer.[12] The carcinogens in the smoke disseminate throughout the body and can be detected in cervical mucus. These carcinogens can alter the balance of oncogenes within these cells, resulting in cancerous growth. Research also shows that women who have a high number of full-term pregnancies are at an increased risk of developing cervical cancer.[13]
Pharmacologic-Associated Cervical Cancers
Women who take oral contraception for prolonged periods have a temporary increase in the risk of acquiring cervical cancer.[14][15] Additionally, patients who have human immunodeficiency virus or are immunocompromised have an increased risk of acquiring HPV, which can lead to cervical cancer. Both of these reduce the ability of the immune system to clear the virus. From a more historical reference, children who had their mother take diethylstilbestrol (DES) during the pregnancy are at elevated risk of clear cell adenocarcinoma of the vagina and cervix.[16] DES was prescribed to pregnant women from the late 1930s until 1971 in an attempt to reduce the risk of miscarriage and premature labor; however, DES is no longer used in pregnancy due to a lack of proven benefit and the later recognition of significant adverse effects. Please see StatPearls' companion resource, "Clear Cell Carcinoma of the Cervix," for further information.
Human Papillomavirus Vaccine Preventive Strategies
The HPV vaccination is a safe, highly effective, and long-lasting strategy for the prevention of cervical cancer and other HPV-related malignancies. HPV vaccination protects against multiple HPV types, including the high-risk oncogenic strains 16 and 18 that are responsible for the majority of cervical cancer cases.
HPV vaccination is most effective when administered before exposure to the virus; therefore, this prevention strategy is routinely recommended at 11 to 12 years of age, with initiation possible as early as 9 years of age. Individuals aged 9 to 14 years require a 2-dose schedule given 6 to 12 months apart, whereas those starting at 15 years or older, as well as immunocompromised individuals, require a 3-dose series over 6 months. Although routine vaccination is not universally recommended beyond 26 years of age, selected adults between 27 and 45 years may still benefit based on individual risk assessment. Please see StatPearls' companion resource, "Human Papillomavirus Vaccine," for further information.
Extensive real-world evidence shows that HPV vaccination can prevent more than 90% of HPV-related cancers, with marked reductions in HPV infections, genital warts, and cervical precancerous lesions. Long-term follow-up studies demonstrate sustained protection for over a decade without evidence of waning immunity, highlighting its central role in the primary prevention of cervical cancer.
Anatomical Pathology
Cervical cancer screening requires acquiring cervical cells in the transitional zone of the cervix. The transitional zone is also called the squamocolumnar junction because this area is the junction between the ectocervix and the endocervix. The ectocervix is comprised of nonkeratinized stratified squamous epithelium, while the endocervix is simple columnar epithelium. The simple columnar cells also have glandular cells that secrete mucus.
Anatomic pathology in cervical cytology mainly arises from the 2 cell types found in the transitional zone: epithelial and glandular. Epithelial cell pathology is graded in the following ascending fashion:
- Atypical squamous cells of undetermined significance (ASCUS): This is the most common abnormal pap smear diagnosis.[17] An ASCUS diagnosis usually correlates with an HPV infection and can reflect precancerous changes in the cells, inflammation, or a response to trauma (see Image. Squamous Cells, Acute Inflammation). Please see StatPearls' companion resource, "Atypical Squamous Cells of Undetermined Significance," for further information.
- Atypical squamous cells cannot exclude high-grade intraepithelial lesions (ASC-H): This diagnosis is exceedingly rare, and colposcopy is required to confirm the absence of high-grade intraepithelial lesions. Please see StatPearls' companion resource, "Colposcopy," for further information.
If the pathologist can identify a morphological change within the cells, the following nomenclature is used:
- Low-grade squamous intraepithelial lesions (LSIL): This term encompasses a spectrum of changes in squamous cells that may progress to squamous cell carcinoma. A finding of LSIL is highly suggestive of an HPV infection. This nomenclature includes cervical intraepithelial neoplasia (CIN) 1 and mild preinvasive cervical disease. While this finding occurs in 2% of all Pap smears, the 2-year regression rate of LSIL is over 85%.[18] Less than a quarter of LSIL findings will progress to higher-grade lesions.
- High-grade squamous intraepithelial lesions (HSIL): This term is a general term for abnormalities in squamous cells with a high risk of progressing to cervical cancer. This finding is highly suggestive of an HPV infection. This title includes the historical terminology of CIN2, CIN3, moderate preinvasive cervical disease, severe preinvasive cervical disease, and carcinoma in situ.[19] The ASCCP's preferred terminology for these classifications is cervical preinvasive disease.
- Squamous cell carcinoma: This is rarely diagnosed on a pap test.[20] This condition only occurs with a significant progression of cervical cancer.
In addition to the epithelial cells, the pathologist can identify abnormal glandular cells, which are graded in the following ascending fashion:
- Atypical glandular cells (AGC): This cell type can be found in the endocervix and may also appear in other parts of the reproductive tract, eg, the endometrium. AGC is uncommon, diagnosed in 0.3% of all Pap smears. AGC identifies cells that have progressed beyond temporary inflammatory changes but have not yet mutated enough to be diagnosed as adenocarcinoma.[21] Although not a diagnosis of adenocarcinoma, a 61-fold increase in the risk of adenocarcinoma is observed compared with patients with a normal Pap test result.[22] A finding of AGC can result from benign etiologies, eg, cervicitis, oral contraception use, pregnancy, or endometrial polyps.[23] AGC is divided into 2 main categories: "undetermined significance" and "undetermined significance with a squamous abnormality." Please see StatPearls' companion resource, "Atypical Glandular Cells (AGS)," for further information. Squamous abnormalities can be found in 31% of AGC diagnoses and are more likely to appear in patients younger than the age of 35.[24] A diagnosis of AGC increases the risk of cancers throughout a woman's reproductive tract. ACG is also divided into the following subtypes based on the suspected origin of the glandular cells:
- Atypical glandular cells favor endocervical origin (AGC-EC): This diagnosis is least likely to have associated endometrial cancer.[25]
- Atypical glandular cells favor endometrial origin (AGC-EM): This diagnosis is most likely to have associated endometrial cancer.[25]
- Atypical glandular cells favoring neoplasia (AGC-FN): This diagnosis was added in 2019 and carries a high risk of underlying malignancy, up to 50%.[26]
- Atypical glandular cells not otherwise specified (AGC-NOS): This diagnosis is in the middle, having an association with endometrial cancer.[25]
- Endocervical adenocarcinoma in situ: This diagnosis has become more frequent in recent decades, with a prevalence of 11.2 per 100,000, and is most likely to be diagnosed in patients between the ages of 30 and 40.[27] Endocervical adenocarcinoma in situ (AIS) usually correlates with a squamous lesion. Like the other abnormal Pap smear findings, high-risk serotypes of HPV are a risk factor.
- Adenocarcinoma: This diagnosis is the invasive version of AIS, which can be found in the transition zone but is more commonly present within the cervical canal. This condition also derives from the endocervical glandular epithelium.[28] An increase in this diagnosis has been noted, even though cervical squamous carcinoma cases have decreased.
- Adenocarcinoma malignum: A rare cervical disease that is diagnosable with a pap test. This disease usually arises in the endocervical region and is often misdiagnosed as a benign lesion.[29] Cytologic features include significant cytoplasm with ovoid nuclei.[30] Histologically, the cells are in a honeycomb pattern. The mucinous glands secrete copious fluid, leading to symptomatic vaginal discharge.
Less commonly, abnormal Pap smears can arise from other histological subtypes. Cervical cancer can arise from a neuroendocrine origin, with the 2 main subtypes being large and small cell. Other types of tumors that can cause cervical cancer include sarcoma, lymphoma, and melanoma.
Clinical Pathology
Abnormal Pap test results often present without symptoms, making targeted history-taking essential. Clinicians should inquire about bleeding between periods, changes in the menstrual cycle, abnormal vaginal discharge, and dyspareunia. Any increase in unexplained bleeding or menstrual bleeding warrants evaluation for possible cervical cancer. Postmenopausal bleeding raises particular concern for neoplasms, although such presentations are more commonly associated with endometrial cancer. In more advanced stages of cervical cancer, patients may report pelvic pain and dysuria.
Biochemical and Genetic Pathology
The most common etiology of abnormal pap smears is due to HPV infections. HPV is a nonenveloped, circular, double-stranded deoxyribonucleic acid virus. The high-risk HPV serotypes are 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68 because they make the oncoproteins E6 and E7.[31][32] Both of these oncoproteins result in the immortalization of the infected cervical cells. E6 binds to the intracellular transformation-related protein (p)53, causing it to degrade. The p53 protein is primarily utilized in the apoptotic pathway to upregulate the transcription of p53 upregulated modulator of apoptosis (PUMA) and phorbol-12-myristate-13-acetate-induced protein 1, NOXA, leading to cell death. E7 focuses on activating the cell cycle, allowing for replication.
In noninfected cells, one way the cell cycle becomes arrested in G1 is through the binding of Rb to E2F. E2F is a transcriptional activator needed to progress the cell into the S phase, but cannot do so when bound to Rb. In high-risk HPV strains, E7 binds to Rb, releasing E2F.[33] With E2F unbound from Rb, the infected cells are signaled to begin the S phase. Genetically, breast cancer gene (BRCA) mutations play a role in the susceptibility to developing cervical cancer. Its translational product is a tumor suppressor protein. BRCA1 and BRCA2 are integral in many pathways, but are especially important for deoxyribonucleic acid (DNA) repair. When double-stranded DNA breaks occur, these proteins help with homologous recombination repair. Without these proteins, genomic instability can lead to neoplastic changes.[34] Within the BRCA homologous repair pathway, other identifiable genes include BRIP1, RAD51C, RAD51D, PALB2, ATM, CHEK1, and CHEK2.
Morphology
The morphological changes recognized in abnormal Pap smears include multinucleation, hyperchromasia, and perinuclear cytoplasmic vacuolization. The nuclei of the cells can also become enlarged, up to 3 times the size of a normal cell nucleus. Other nuclear features include increased keratinization but an absence of nucleoli. These changes that squamous cells undergo are categorized as koilocytosis.
Mechanisms
A Pap smear involves the collection of cervical cells using a brush inserted into the cervical os. The brush should extend beyond the visualized portion to improve sampling of the transition zone. Alternative collection devices include a spatula or broom. Two methods exist for analyzing collected cells: liquid-based cytology, eg, ThinPrep and SurePath, and conventional cytology. Cytology includes 2 subtypes.[35] One subtype allows the collection device to be detached and retained with the sample for analysis, while the other requires agitation of the collection tool within the medium because the device does not accompany the sample.
Liquid-based cytology preserves cells in a buffered alcoholic solution containing 25% to 55% methanol, which acts as a fixative and supports storage for 3 to 4 weeks. ThinPrep, manufactured by Hologic, represents the most commonly used system in the United States.[36] Instructional guidance recommends minimizing the use of gel-based lubricants before specimen collection, as these substances can adhere to the filter membrane and produce inaccurate results.
Evidence suggests that liquid-based cytology may improve the detection of glandular pathology. Conventional cytology involves direct transfer of collected cells from the brush onto a slide, which defines the Pap smear technique. During transfer, minimizing drying artifacts from prolonged air exposure remains important. According to ACOG, both liquid-based and conventional cytology demonstrate equivalent effectiveness in cervical cancer screening.
Clinicopathologic Correlations
AGC in patients with HPV serotypes 16 and 18 has an increased risk for AIS and warrants closer surveillance. When AIS occurs concurrently with LSIL, clinical management should proceed according to an AIS diagnosis.
Clinical Significance
The Papanicolaou test is an effective screening test that detects cervical cancer as well as cellular changes that have the potential to develop into cervical cancer. Any diagnosis of an atypical pap smear results in more frequent and further testing. Management guidelines for abnormal Pap test findings vary across different professional societies and groups. The following management strategies, according to ACOG, are currently recommended for each abnormal result:
- ASCUS: The management of ASCUS depends on the age of the patient. For patients aged 21 to 24, repeat the Pap smear in 1 year if HPV status is positive or unknown. Performing a reflex HPV test on the same pap smear sample is also acceptable. HPV status will determine future Pap smear frequencies.
- If HPV is negative, then the patient is recommended for follow-up in 3 years.
- If the follow-up Pap smear continues to show ASCUS, then an additional Pap smear in 1 year is recommended.
- For patients between 25 and 29, screening is still the same if they have a negative HPV test. However, if they have positive HPV, colposcopy is recommended instead of waiting 1 year for a follow-up pap smear. If ASCUS persists on the follow-up Pap smear, the next step is colposcopy.
- For patients between 30 and 65 years of age, a more significant concern is the progression of cervical cancer. If ASCUS is documented on a pap smear and HPV is negative, following the same management as the other age groups is recommended. If HPV status is positive or unknown, a repeat pap smear is recommended within 4 months.
- LSIL: Repeat Pap smear in 1 year.
- ASC-H: Immediate further testing with colposcopy is recommended.
- HSIL: Further testing with colposcopy is recommended.
- AGC: Further testing can include endocervical sampling and an endometrial biopsy to source the location of the cells. Obtaining a targeted family history at this time is essential. The patient should have their HPV status evaluated.
- AIS: Immediate diagnostic excision procedure along with an endocervical and endometrial biopsy. The diagnostic excision will help confirm the diagnosis and determine the extent of the invasion.
- Squamous cell carcinoma: Immediate excision and further workup are necessary.
Media
(Click Image to Enlarge)
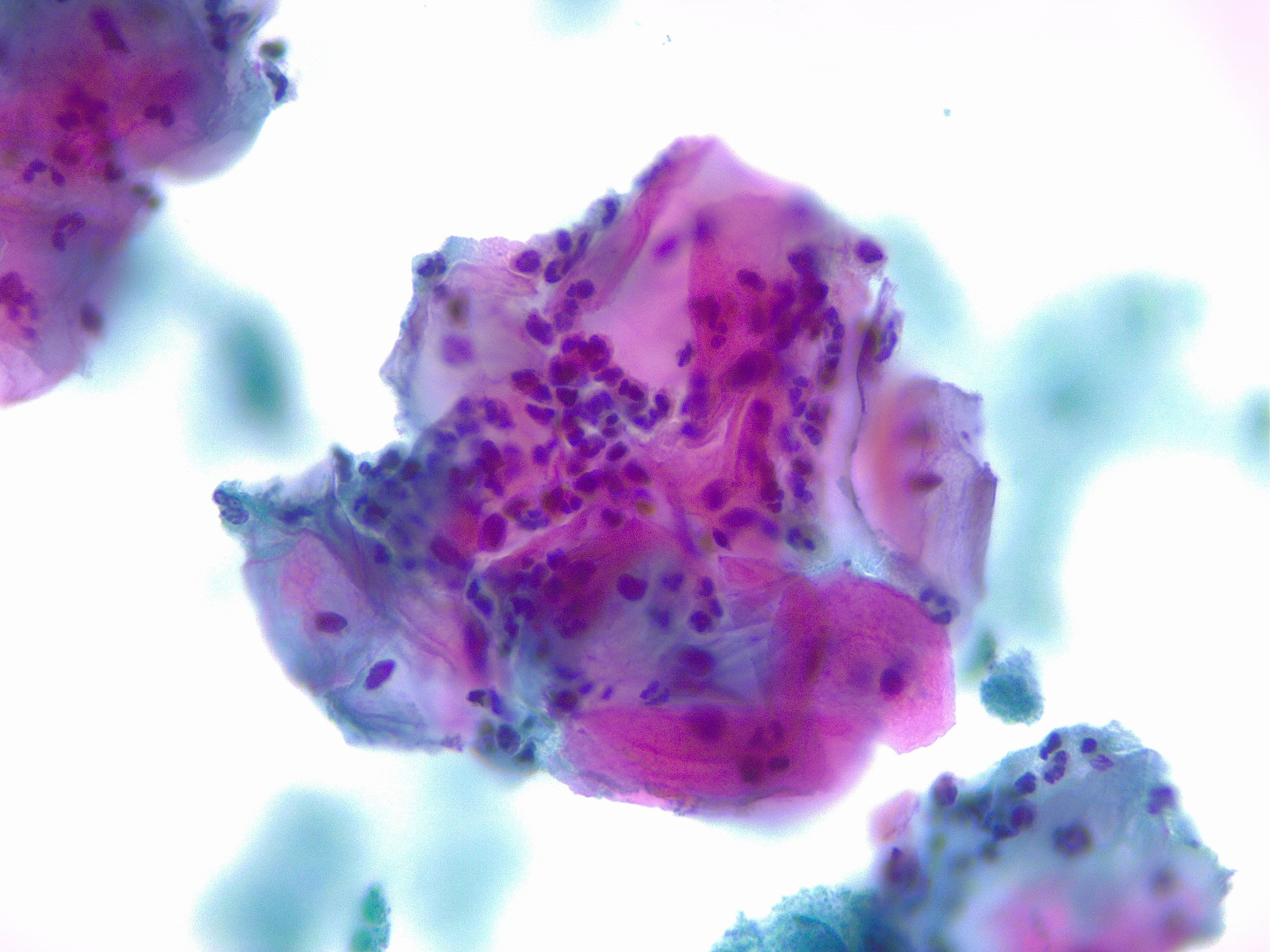
Squamous Cells With Acute Inflammation. The image shows a microscopic examination of squamous cells with acute inflammation, captured at ×40 magnification and stained using the Papanicolaou stain.
Contributed by F Farci, MD
References
Nayar R, Wilbur DC. The Pap test and Bethesda 2014. Cancer cytopathology. 2015 May:123(5):271-81. doi: 10.1002/cncy.21521. Epub 2015 May 1 [PubMed PMID: 25931431]
Kurman RJ, Henson DE, Herbst AL, Noller KL, Schiffman MH. Interim guidelines for management of abnormal cervical cytology. The 1992 National Cancer Institute Workshop. JAMA. 1994 Jun 15:271(23):1866-9 [PubMed PMID: 8196145]
Level 1 (high-level) evidenceSiegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA: a cancer journal for clinicians. 2019 Jan:69(1):7-34. doi: 10.3322/caac.21551. Epub 2019 Jan 8 [PubMed PMID: 30620402]
Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA: a cancer journal for clinicians. 2024 Jan-Feb:74(1):12-49. doi: 10.3322/caac.21820. Epub 2024 Jan 17 [PubMed PMID: 38230766]
Sørbye SW, Suhrke P, Revå BW, Berland J, Maurseth RJ, Al-Shibli K. Accuracy of cervical cytology: comparison of diagnoses of 100 Pap smears read by four pathologists at three hospitals in Norway. BMC clinical pathology. 2017:17():18. doi: 10.1186/s12907-017-0058-8. Epub 2017 Aug 29 [PubMed PMID: 28860942]
Koonmee S, Bychkov A, Shuangshoti S, Bhummichitra K, Himakhun W, Karalak A, Rangdaeng S. False-Negative Rate of Papanicolaou Testing: A National Survey from the Thai Society of Cytology. Acta cytologica. 2017:61(6):434-440. doi: 10.1159/000478770. Epub 2017 Jul 25 [PubMed PMID: 28738387]
Level 3 (low-level) evidenceCastillo M, Astudillo A, Clavero O, Velasco J, Ibáñez R, de Sanjosé S. Poor Cervical Cancer Screening Attendance and False Negatives. A Call for Organized Screening. PloS one. 2016:11(8):e0161403. doi: 10.1371/journal.pone.0161403. Epub 2016 Aug 22 [PubMed PMID: 27547971]
Mayer CM, Scarinci IC, Huh WK. Self-Collection for Human Papillomavirus Testing in Clinical Settings: An Opportunity to Reflect on the Disconnect Between Guidelines and Clinical Practice. Obstetrics and gynecology. 2025 May 22:146(1):34-38. doi: 10.1097/AOG.0000000000005941. Epub 2025 May 22 [PubMed PMID: 40403313]
Wentzensen N, Arbyn M. HPV-based cervical cancer screening- facts, fiction, and misperceptions. Preventive medicine. 2017 May:98():33-35. doi: 10.1016/j.ypmed.2016.12.040. Epub 2017 Feb 6 [PubMed PMID: 28279260]
Olayiwola AA, Oshodi YA, Akinola OI, Banjo AA, Rabiu KA, Olumodeji AM. High-risk HPV serotype distribution in cervical cancer: comparative analysis of detection in cervicovaginal secretions and tissue DNA extraction. Ecancermedicalscience. 2025:19():1992. doi: 10.3332/ecancer.2025.1992. Epub 2025 Sep 18 [PubMed PMID: 41561537]
Level 2 (mid-level) evidenceKemp TJ, Panicker G, Eklund C, Nie J, Wang Y, Beddows S, Rigsby P, Huang W, Dillner J, Unger ER, Pinto LA, Wilkinson DE, collaborative study participants. WHO International Standards for antibodies to HPV6 HPV11 HPV31 HPV33 HPV45 HPV52 and HPV58. NPJ vaccines. 2024 Sep 10:9(1):165. doi: 10.1038/s41541-024-00949-2. Epub 2024 Sep 10 [PubMed PMID: 39256440]
Chatzistamatiou K, Moysiadis T, Vryzas D, Chatzaki E, Kaufmann AM, Koch I, Soutschek E, Boecher O, Tsertanidou A, Maglaveras N, Jansen-Duerr P, Agorastos T. Cigarette Smoking Promotes Infection of Cervical Cells by High-Risk Human Papillomaviruses, but not Subsequent E7 Oncoprotein Expression. International journal of molecular sciences. 2018 Jan 31:19(2):. doi: 10.3390/ijms19020422. Epub 2018 Jan 31 [PubMed PMID: 29385075]
Roura E, Travier N, Waterboer T, de Sanjosé S, Bosch FX, Pawlita M, Pala V, Weiderpass E, Margall N, Dillner J, Gram IT, Tjønneland A, Munk C, Palli D, Khaw KT, Overvad K, Clavel-Chapelon F, Mesrine S, Fournier A, Fortner RT, Ose J, Steffen A, Trichopoulou A, Lagiou P, Orfanos P, Masala G, Tumino R, Sacerdote C, Polidoro S, Mattiello A, Lund E, Peeters PH, Bueno-de-Mesquita HB, Quirós JR, Sánchez MJ, Navarro C, Barricarte A, Larrañaga N, Ekström J, Lindquist D, Idahl A, Travis RC, Merritt MA, Gunter MJ, Rinaldi S, Tommasino M, Franceschi S, Riboli E, Castellsagué X. The Influence of Hormonal Factors on the Risk of Developing Cervical Cancer and Pre-Cancer: Results from the EPIC Cohort. PloS one. 2016:11(1):e0147029. doi: 10.1371/journal.pone.0147029. Epub 2016 Jan 25 [PubMed PMID: 26808155]
Marks M, Gravitt PE, Gupta SB, Liaw KL, Kim E, Tadesse A, Phongnarisorn C, Wootipoom V, Yuenyao P, Vipupinyo C, Rugpao S, Sriplienchan S, Celentano DD. The association of hormonal contraceptive use and HPV prevalence. International journal of cancer. 2011 Jun 15:128(12):2962-70. doi: 10.1002/ijc.25628. Epub 2010 Oct 26 [PubMed PMID: 20734390]
Guo C, Zhan B, Li MY, Yue L, Zhang C. Association between oral contraceptives and cervical cancer: A retrospective case-control study based on the National Health and Nutrition Examination Survey. Frontiers in pharmacology. 2024:15():1400667. doi: 10.3389/fphar.2024.1400667. Epub 2024 Jul 17 [PubMed PMID: 39086392]
Level 2 (mid-level) evidenceConlon JL. Diethylstilbestrol: Potential health risks for women exposed in utero and their offspring. JAAPA : official journal of the American Academy of Physician Assistants. 2017 Feb:30(2):49-52. doi: 10.1097/01.JAA.0000511800.91372.34. Epub [PubMed PMID: 28098674]
Garrett LA, McCann CK. Abnormal cytology in 2012: management of atypical squamous cells, low-grade intraepithelial neoplasia, and high-grade intraepithelial neoplasia. Clinical obstetrics and gynecology. 2013 Mar:56(1):25-34. doi: 10.1097/GRF.0b013e3182833eed. Epub [PubMed PMID: 23337842]
Ciavattini A, Clemente N, Tsiroglou D, Sopracordevole F, Serri M, Delli Carpini G, Papiccio M, Cattani P. Follow up in women with biopsy diagnosis of cervical low-grade squamous intraepithelial lesion (LSIL): how long should it be? Archives of gynecology and obstetrics. 2017 Apr:295(4):997-1003. doi: 10.1007/s00404-017-4335-7. Epub 2017 Mar 3 [PubMed PMID: 28255767]
Khieu M, Butler SL. High-Grade Squamous Intraepithelial Lesion of the Cervix. StatPearls. 2026 Jan:(): [PubMed PMID: 28613479]
Katki HA, Schiffman M, Castle PE, Fetterman B, Poitras NE, Lorey T, Cheung LC, Raine-Bennett T, Gage JC, Kinney WK. Benchmarking CIN 3+ risk as the basis for incorporating HPV and Pap cotesting into cervical screening and management guidelines. Journal of lower genital tract disease. 2013 Apr:17(5 Suppl 1):S28-35. doi: 10.1097/LGT.0b013e318285423c. Epub [PubMed PMID: 23519302]
Boyraz G, Basaran D, Salman MC, Ibrahimov A, Onder S, Akman O, Ozgul N, Yuce K. Histological Follow-Up in Patients with Atypical Glandular Cells on Pap Smears. Journal of cytology. 2017 Oct-Dec:34(4):203-207. doi: 10.4103/JOC.JOC_209_16. Epub [PubMed PMID: 29118475]
Zhong P, Yin C, Jin Y, Chen T, Zhan Y, Tian C, Zhu L, Zheng X. More focus on atypical glandular cells in cervical screening: Risk of significant abnormalities and low histological follow-up rate. CytoJournal. 2020:17():22. doi: 10.25259/Cytojournal_77_2019. Epub 2020 Oct 6 [PubMed PMID: 33193804]
Monti E, Di Loreto E, Libutti G, Alberico D, Barbara G, Boero V, Cetera GE, Pasquali Coluzzi M, Cipriani S, Parazzini F. Clinical significance of atypical glandular cells on cytology: 10 years' experience of a colposcopic referral center. European journal of cancer prevention : the official journal of the European Cancer Prevention Organisation (ECP). 2025 Mar 1:34(2):106-112. doi: 10.1097/CEJ.0000000000000910. Epub 2024 Nov 5 [PubMed PMID: 39150089]
Geier CS, Wilson M, Creasman W. Clinical evaluation of atypical glandular cells of undetermined significance. American journal of obstetrics and gynecology. 2001 Jan:184(2):64-9 [PubMed PMID: 11174481]
Level 2 (mid-level) evidenceZhao C, Austin RM, Pan J, Barr N, Martin SE, Raza A, Cobb C. Clinical significance of atypical glandular cells in conventional pap smears in a large, high-risk U.S. west coast minority population. Acta cytologica. 2009 Mar-Apr:53(2):153-9 [PubMed PMID: 19365967]
Level 2 (mid-level) evidenceXu S, Jiang T, Mao X, Cai L, Lin X, Tong Y, Dong B, Sun P. Assessment of risk factors for high-grade cervical or endometrial lesions to triage women with AGC-FN: a retrospective study. BMC women's health. 2025 May 28:25(1):260. doi: 10.1186/s12905-025-03772-6. Epub 2025 May 28 [PubMed PMID: 40437507]
Level 2 (mid-level) evidenceWang SS, Sherman ME, Hildesheim A, Lacey JV Jr, Devesa S. Cervical adenocarcinoma and squamous cell carcinoma incidence trends among white women and black women in the United States for 1976-2000. Cancer. 2004 Mar 1:100(5):1035-44 [PubMed PMID: 14983500]
Level 2 (mid-level) evidenceTakeuchi S. Biology and treatment of cervical adenocarcinoma. Chinese journal of cancer research = Chung-kuo yen cheng yen chiu. 2016 Apr:28(2):254-62. doi: 10.21147/j.issn.1000-9604.2016.02.11. Epub [PubMed PMID: 27198186]
Ki EY, Byun SW, Park JS, Lee SJ, Hur SY. Adenoma malignum of the uterine cervix: report of four cases. World journal of surgical oncology. 2013 Jul 26:11():168. doi: 10.1186/1477-7819-11-168. Epub 2013 Jul 26 [PubMed PMID: 23885647]
Level 3 (low-level) evidenceChang J, Zhang S, Zhou H, Liang JX, Lin ZQ. [Clinical analysis of minimal deviation adenocarcinoma of the cervix: a report of five cases]. Ai zheng = Aizheng = Chinese journal of cancer. 2008 Dec:27(12):1310-4 [PubMed PMID: 19080000]
Level 2 (mid-level) evidenceBalasubramaniam SD, Balakrishnan V, Oon CE, Kaur G. Key Molecular Events in Cervical Cancer Development. Medicina (Kaunas, Lithuania). 2019 Jul 17:55(7):. doi: 10.3390/medicina55070384. Epub 2019 Jul 17 [PubMed PMID: 31319555]
Yao YL, Tian QF, Cheng B, Cheng YF, Ye J, Lu WG. Human papillomavirus (HPV) E6/E7 mRNA detection in cervical exfoliated cells: a potential triage for HPV-positive women. Journal of Zhejiang University. Science. B. 2017 Mar.:18(3):256-262. doi: 10.1631/jzus.B1600288. Epub [PubMed PMID: 28271661]
Dick FA, Rubin SM. Molecular mechanisms underlying RB protein function. Nature reviews. Molecular cell biology. 2013 May:14(5):297-306. doi: 10.1038/nrm3567. Epub 2013 Apr 18 [PubMed PMID: 23594950]
Level 3 (low-level) evidenceMylavarapu S, Das A, Roy M. Role of BRCA Mutations in the Modulation of Response to Platinum Therapy. Frontiers in oncology. 2018:8():16. doi: 10.3389/fonc.2018.00016. Epub 2018 Feb 5 [PubMed PMID: 29459887]
Gibb RK, Martens MG. The impact of liquid-based cytology in decreasing the incidence of cervical cancer. Reviews in obstetrics & gynecology. 2011:4(Suppl 1):S2-S11 [PubMed PMID: 21617785]
Welch EC, Lu C, Sung CJ, Zhang C, Tripathi A, Ou J. BMT: A Cross-Validated ThinPrep Pap Cervical Cytology Dataset for Machine Learning Model Training and Validation. Scientific data. 2024 Dec 28:11(1):1444. doi: 10.1038/s41597-024-04328-3. Epub 2024 Dec 28 [PubMed PMID: 39732723]
Level 1 (high-level) evidence