Introduction
Facial implants are used to enhance the aesthetics of the aging or underdeveloped face or correct asymmetry resulting from trauma or congenital malformations. Common augmentation sites include the chin, zygomas, and mandibular angles. According to the 2020 American Society of Plastic Surgeons member survey, malar implant surgery was the most frequently performed facial implant procedure and ranked as the 3rd most common cosmetic surgical procedure overall.
The use of malar implants has increased by 938% since 2000, while chin implant procedures have risen by 63% during the same period. Although less frequently performed, facial implants may also be placed on other bony surfaces, including the nose, glabella, and temple.[1] Systematic reviews in 2024 and 2025 report pooled complication rates ranging from 4% to 11%, with lower rates in malar and chin implants and higher rates in paranasal regions.[2]
The ideal implant material is chemically inert, biocompatible, and easily manipulated. Despite these properties, implants are foreign bodies and carry inherent risks. Facial implants may be organic or synthetic. Among the synthetic materials used in the U.S., high-density polyethylene (HDPE), silicone, and titanium remain the most prevalent. Autogenic grafts, once widely employed, have declined in popularity due to long-term variability and limited predictability.[3]
One of the most common complications associated with facial implants is poor cosmesis, frequently resulting from asymmetry. Less common but more severe complications include infection and bone erosion. These conditions may necessitate implant removal, which is more technically challenging for porous implants that permit soft tissue ingrowth than for solid implants surrounded by a fibrous capsule.[4][5]
Advances in software-assisted analysis have improved the evaluation of facial defects and the determination of appropriate surgical interventions. Facial analysis continues to evolve with the integration of 3-dimensional (3D) treatment planning technologies. Two-dimensional (2D) imaging remains valuable for assessing bony relationships and correlating these structures with soft tissue contours. For example, lateral cephalograms form the basis of genioplasty evaluation, whereas assessing midface deficiencies remains more difficult with 2D radiographs and may benefit from additional research and imaging refinements.
Objective criteria have been developed to guide implant selection and surgical planning. However, aesthetic preferences influenced by societal trends must also be considered. Optimal outcomes depend on diagnostic precision, thorough facial analysis, appropriate implant choice, and meticulous surgical execution.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Vital anatomical structures must be carefully considered during facial implant placement to minimize the risk of injury. The primary structures of concern include the sensory and motor nerves, vasculature, and musculature of the face.
Trigeminal Nerve
Cranial nerve V (CN V), or the trigeminal nerve, provides sensory innervation to the face and motor control to select muscles of mastication. CN V is divided into divisions V1 to V3, each exiting the skull through a distinct foramen. Terminal branches of these nerves reach the facial surface of the viscerocranium and penetrate their target soft tissues.[6] Certain branches are particularly vulnerable to injury at their points of exit, especially during implant placement.
CN V1, the ophthalmic division, exits the skull via the superior orbital fissure and gives rise to 3 primary branches: frontal, lacrimal, and nasociliary. The frontal branch traverses the orbit, exits superiorly, and forms the supraorbital and supratrochlear nerves, which provide sensory innervation to the upper eyelid, conjunctiva, and scalp. The lacrimal nerve, the smallest branch of CN V1, communicates with the zygomatic nerve, supplies limited areas of skin and conjunctiva in the lateral upper eyelid, and contributes to lacrimal gland innervation. The nasociliary nerve divides within the orbit, giving rise to terminal branches such as the infratrochlear and external nasal nerves, which innervate the medial upper eyelid and dorsum of the nose.
CN V2, the maxillary division, exits the skull through the foramen rotundum. This division gives rise to 2 primary branches, the infraorbital and zygomatic nerves. The infraorbital nerve emerges onto the facial surface via the maxilla’s infraorbital foramen, providing sensory innervation to the soft tissues extending from the lower eyelid to the upper lip. The zygomatic nerve courses along the lateral orbit and subsequently divides into the zygomaticotemporal and zygomaticofacial nerves. These branches exit through their respective foramina and supply the skin of the temple region and malar eminence. All 3 nerves are at risk of injury during subperiosteal dissection associated with zygomatic implant placement.
CN V3, the mandibular division, exits the skull via the foramen ovale. This division comprises numerous branches, including the pterygoid, masseteric, deep temporal, buccal, auriculotemporal, lingual, and inferior alveolar nerves. Arising from fused trigeminal motor and sensory fibers, the mandibular division provides motor innervation to the muscles of mastication. Since its fibers penetrate the target muscles outside the dissection plane, the mandibular division is generally not at risk during facial implant placement.
The inferior alveolar nerve enters the mandibular ramus medially and courses through the body of the mandible, emerging laterally as the mental nerve at the mental foramen, located apical to the 1st and 2nd premolars (see Image. Mental Nerve). The foramen is situated approximately 1.5 cm superior to the inferior border of the mandible.[7]
Upon exiting the mental foramen, the mental nerve gives rise to 3 branches that pass deep to the depressor anguli oris muscle. These branches provide sensory innervation to the lower lip, chin, and gingival tissue associated with the mandibular incisors. The mental nerve is a key structure frequently encountered during genioplasty procedures.[8]
Facial Nerve
Cranial nerve VII (CN VII), the facial nerve, provides motor innervation to the muscles of facial expression. Although CN VII branches are not directly encountered during facial implant dissection, they remain vulnerable to injury from stretching or compression during the procedure. CN VII exits the skull through the stylomastoid foramen and enters the parotid gland, where it divides into 5 primary branches—temporal, zygomatic, buccal, mandibular, and cervical—which course deep to the superficial muscular aponeurotic system (SMAS).
The temporal branch ascends to innervate the frontalis and the superior aspect of the orbicularis oculi. The zygomatic and buccal branches course deep to the masseteric fascia, placing them near the subperiosteal dissection plane and at elevated risk of injury during zygomatic implant placement. The zygomatic branch innervates the inferior orbicularis oculi and nasal musculature, while the buccal branch supplies the upper lip and cheek muscles. The marginal mandibular branch exits the parotid gland at the mandibular angle, following the inferior border of the mandible. Injury to this branch compromises the mentalis and depressor anguli oris muscles. The cervical branch provides motor innervation to the platysma.[9]
Facial Vasculature
The facial blood supply is derived from branches of the external carotid artery. Major vessels are most vulnerable during the initial incision, as they traverse the soft tissue while dissection proceeds in the subperiosteal plane. An exception occurs when vessels travel within neurovascular bundles and exit the viscerocranium. For example, the infraorbital and mental nerves are accompanied by arteries and veins of the same names as they emerge from their respective foramina.
Facial Musculature
Muscles of facial expression are located subcutaneously within the anterior and posterior scalp, face, and neck. Most attach to bone or fascia, generating movement of the overlying skin to produce expressions. All facial muscles receive motor innervation from the facial nerve. Table 1 summarizes key anatomical and functional details of the muscles of facial expression.
Table 1. Facial Expression Muscles
| Muscle | Origin | Insertion | Action(s) |
| Occipitofrontalis frontal belly | Epicranial aponeurosis | Skin of eyebrow and forehead; subcutaneous tissue | Raises eyebrows, wrinkles forehead skin, protracts scalp (surprised expression) |
| Occipitofrontalis occipital belly | Lateral 2/3 of superior nuchal line of occipital bone | Epicranial aponeurosis | Retracts scalp, assists frontal belly |
| Orbicularis oculi | Medial orbital margin, medial palpebral ligament, lacrimal bone | Skin around orbital margin, superior and inferior tarsal plates | Palpebral part gently closes eyelids; orbital part tightly closes eyelids |
| Corrugator supercilii | Medial side of superciliary arch | Skin superior to supraorbital area and superciliary arch | Pulls eyebrows inferomedially (worried expression) |
| Procerus and transverse nasalis part | Facial aponeurosis over nasal bone and lateral nasal cartilage | Skin of lower forehead and between eyebrows | Lowers medial eyebrow edge, wrinkles skin over nose (disgust or disdain expression) |
| Alar nasalis and levator labii superioris alaeque nasi | Frontal process of maxilla | Major alar cartilage | Lowers nasal alae laterally, widens anterior nasal aperture (nasal flaring when angry) |
| Orbicularis oris | Medial maxilla and mandible, mouth angle, deep perioral skin | Mucous membrane of lips | Closes oral fissure, compresses and protrudes lips (kissing), prevents distension (blowing) |
| Levator labii superioris | Infraorbital region of maxilla | Skin of upper lip | Elevates and everts upper lip, dilates mouth, deepens nasolabial sulcus (sad expression) |
| Zygomaticus minor | Anterior part of zygomatic bone | Skin of upper lip | Elevates and everts upper lip, dilates mouth, deepens nasolabial sulcus (sad expression) |
| Buccinator | Mandible, alveolar processes of maxilla and mandible, pterygomandibular raphe | Orbicularis oris and modiolus (mouth angle) | Compresses cheek against molars, coordinates with tongue in chewing, prevents cheek distension (blowing) |
| Zygomaticus major | Lateral aspect of zygomatic bone | Modiolus | Dilates mouth, raises labial commissure bilaterally to smile or unilaterally to show disdain |
| Levator anguli oris | Infraorbital maxilla | Modiolus | Dilates mouth, elevates labial commissure, widens oral fissure (grin or grimace) |
| Risorius | Parotid fascia and buccal skin | Modiolus | Dilates mouth, draws labial commissure laterally (frown or sadness) |
| Depressor anguli oris | Anterolateral body of mandible | Modiolus | Dilates mouth, lowers labial commissure (frown or sadness) |
| Depressor labii inferioris | Platysma, anterolateral mandible | Skin of lower lip | Dilates mouth, depresses and everts lower lip (pouting or sadness) |
| Mentalis | Mandibular body | Skin of chin | Raises and protrudes lower lip, raises chin skin (doubtful expression) |
| Platysma | Subcutaneous tissue of infraclavicular and supraclavicular regions | Mandibular base, cheek and lower lip skin, modiolus, orbicularis oris | Depresses mandible against resistance, tightens inferior facial and neck skin (tense expression) |
Mastication Muscles
Chin and malar implants are positioned in regions where the muscles of mastication attach to or closely interact with facial bones. These muscles are critical for mastication and speech and contribute to certain facial expressions. The anterior trunk of CN V3 provides motor innervation. Improper implant placement can cause discomfort and compromise the functional integrity of these muscles. Table 2 summarizes key anatomical and functional information regarding the muscles of mastication.
Table 2. Mastication Muscles
| Muscle | Origin | Insertion | Action(s) |
| Temporalis | Temporal fossa floor and the deep temporal fascia | Coronoid process and anterior aspect of the mandibular ramus | Elevates the mandible (jaw closing), posterior fibers retrude the mandible after protrusion |
| Masseter | Zygomatic arch and the inferior and medial aspects of the zygomatic bone | Lateral surface of the mandibular angle and ramus | Elevates and protrudes the mandible (jaw closing), deep fibers help stabilize temporomandibular joint, minor protrusion |
| Lateral pterygoid | Superior head: greater wing of sphenoid bone; inferior head: lateral pterygoid plate's lateral aspect | Superior head: joint capsule and articular disc of temporomandibular joint; inferior head: pterygoid fovea (on neck of mandibular condyloid process) | Bilaterally: protrude the mandible and lower the chin; unilaterally: produce side-to-side mandibular movements (chewing) |
| Medial pterygoid | Deep head: lateral pterygoid plate of sphenoid; superficial head: maxillary tuberosity | Medial aspect of mandibular ramus, inferior to mandibular foramen | Elevate (jaw closing) and protrude the mandible; unilateral action (alternating): lateral grinding movements |
Indications
Facial implant indications are functionally or esthetically driven and include the following:
- Loss of soft tissue support
- Volume loss
- Facial asymmetry secondary to growth discrepancies
- Congenital syndromes
Bony viscerocranial atrophy typically develops during the 3rd and 4th decades of life. Uneven skeletal resorption can accentuate the signs of aging, with the infraorbital and pyriform maxillary regions commonly exhibiting more pronounced deficiency, resulting in midfacial volume loss. Osseocutaneous ligaments, including the zygomatic and mandibular ligaments, attach to the periosteum of the underlying bone and the overlying skin.[10] The masseter ligaments extend from the muscle to the skin. Weakening and reduced elasticity of these ligaments contribute to soft tissue ptosis under the influence of gravity.
The face contains multiple fat pads, separated by septa and fascia, that undergo progressive atrophy with age. The malar region comprises superficial and deep fat pads divided by the SMAS. Jowls result from the bilateral descent of superficial subcutaneous fat over the inferior mandibular borders and are influenced by fat loss, skin and muscle ptosis, and diminished bony support. Genioplasty alone does not correct a prejowl sulcus. In fact, an osteotomy performed during genioplasty may deepen the sulcus. Therefore, prejowl implant surgery is the preferred intervention for correction, with augmentation possible at the chin, prejowl region, or both.[11]
Asymmetries are common in various congenital deformities and exhibit diverse presentations. Human skull growth occurs along multiple vectors: transverse, sagittal, and vertical. The maxilla typically develops anteriorly, inferiorly, and laterally, whereas the condyles grow superoposteriorly, displacing the mandible anteroinferiorly. The chin ceases growth before the remainder of the mandible, which continues to develop transversely and vertically.[12]
Deviations from typical growth patterns can produce mandibular rotation, resulting in either a dolichocephalic phenotype—characterized by a long, retrognathic, and vertical profile—or a brachycephalic phenotype, which is short, prognathic, and horizontally oriented. Craniofacial growth generally concludes between 14 and 16 years of age in female individuals and between 16 and 18 years in male individuals.[13] In cases of hypoplastic mandibles, orthodontic intervention can address associated dental malocclusion. However, residual skeletal deficiencies may require further correction through orthognathic surgery, implant augmentation, or a combination of both approaches.[14]
Congenital syndromes affecting the 1st and 2nd branchial arches produce a range of craniofacial anomalies. Craniofacial microsomia, for example, frequently involves the maxilla, mandible, and orbits, among other structures, and represents the 2nd most common congenital craniofacial deformity after cleft lip and palate. Clinical presentation is highly variable, and multiple classification systems have been developed to characterize severity and anatomical involvement.[15] Implant-based augmentation may be particularly suitable for individuals with mild forms of the disorder and may also be considered in patients who have undergone prior corrective interventions, such as orthognathic surgery (see Image. Zygomatic Submalar Implant).
Patients with cleft lip and palate frequently exhibit midfacial deficiency, often involving hypoplasia of the malar region. Although Le Fort I osteotomies can address certain midface deficiencies, particularly in the lip and nasolabial angle, their effectiveness in correcting malar hypoplasia remains controversial. Facial implants provide a reliable method for augmenting deficient areas following orthognathic surgery.[16]
Contraindications
Facial implant surgery has limited contraindications, which include the following:
- Incomplete craniofacial growth
- Large volume deficits more appropriately addressed by alternative treatments
- Active infection
- Inadequate bony or soft tissue support
Growth patterns and predictions are critical when evaluating candidates for facial implants. Female individuals typically begin and complete craniofacial growth earlier than male individuals.[17] The term “growth cessation” is variably defined. The Craniofacial Growth Consortium Study compared multiple definitions, defining growth cessation as either annual growth of less than 0.1 mm or a growth rate below 10% of peak growth velocity. Serial cephalometric imaging allows for assessment of growth cessation, with linear measurements from consecutive cephalograms used to determine growth rates.[18]
Patients with skeletal discrepancies associated with dental malocclusion are generally better suited for orthognathic surgery, particularly when osteotomies are required for extensive augmentation. However, patient preference may favor implant-based correction. Thin soft tissue coverage limits the maximal implant dimensions due to increased risk of implant visibility and palpability.
Equipment
Standard facial implants are composed of alloplastic materials designed for structural augmentation. Commonly used materials are discussed below.
Titanium implants are chemically inert, nonresorbable, and rigid. These implants are primarily used to recontour deficient mandibular angles and augment both length and width. The fenestrated mesh design permits tissue ingrowth, enhancing implant stability.[19]
HDPE implants are rigid, noncompressible, and thermoplastic. These implants are available in varying pore sizes and densities, typically ranging from 80 to 400 µm.[20] Pore size determines the type of tissue ingrowth—bone or fibrous tissue—following implantation. Pores approximately 100 to 250 µm in diameter have been shown to support bony ingrowth. However, HDPE implants with such pore sizes require secure fixation to prevent disruption of neovascularization.[21] HDPE implants are supplied in preformed shapes but may be recontoured due to their thermoplastic properties. Recontouring is performed by elevating the implant temperature to 180 °F and sculpting with a scalpel.[22]
Silicone implants are nonporous and may consist of solid silicone or dimethylsiloxane subunits. Since nonporous implants do not permit tissue ingrowth, they become encapsulated and typically require fixation to the underlying bone to maintain immobilization. Fixation reduces dead space between the implant and bone, minimizing the risk of seroma formation and undesired tissue ingrowth. This measure also helps prevent bony resorption, implant migration, and aesthetic compromise.[23]
Recent literature has reexamined whether screw or suture fixation is preferable. A 2023 narrative review found no statistically significant differences in complication rates, including displacement, bone resorption, and infection, between fixated and nonfixated silicone implants, although screw fixation may enhance stability in certain anatomical locations.[24] These findings suggest that proper pocket fit, implant design, and meticulous surgical technique are as critical as hardware fixation in preventing long-term complications.
Autogenous implants, or autografts, are less commonly used in cosmetic augmentation due to the unpredictability of bony resorption. Bone grafts require mechanical stress to maintain density, in accordance with the Wolff law, which states that bone remodels in response to functional load. Areas subjected to minimal stress experience decreased bone density and accelerated resorption.[25] Additionally, autografts introduce donor site morbidity, increased operative time, and greater procedural complexity.[26]
In addition to conventional stock implants, patient-specific implants produced via 3D printing have become increasingly utilized. These implants, constructed from materials such as titanium, polyetheretherketone (PEEK), and HDPE composites, are designed from patient-specific computed tomography or cone-beam computed tomography data to conform precisely to the underlying bony anatomy. Recent evidence indicates that patient-specific implants may reduce the need for intraoperative modification, enhance implant fit, and potentially decrease complication rates, including infection, displacement, and soft-tissue irritation, compared with preformed implants.[27]
Anesthesia for facial implant procedures typically involves the induction of deep intravenous or general anesthesia to achieve the desired depth. Local analgesia is then administered using lidocaine in combination with a longer-acting agent, such as bupivacaine. Local anesthetics are drawn from a vial and delivered with a dental syringe and a 27-gauge needle. Surgical incisions are created using a #15 scalpel blade or bovie electrocautery, depending on surgeon preference.
The surgical armamentarium is consistent across implant types and anatomical locations. Table 3 summarizes the materials and equipment employed for each stage of the procedure.
Table 3. Materials and Equipment for Facial Implant Surgery
| Purpose | Materials and Equipment |
| Local anesthesia | Lidocaine with epinephrine; Exparel (liposomal bupivacaine given ≥20 minutes after lidocaine); 27-gauge needle and syringe |
| Irrigation | Normal saline; Yankauer and Copeland suction; Antibiotic solution for soaking implants |
| Incision | Scalpel with #15 blade; Bovie electrocautery |
| Fixation | Titanium screws (various diameters and lengths); Powered drill; Screwdriver |
| Tissue elevation | #9 periosteal elevator; Woodson elevator |
| Closure | Debakey tissue forceps; Needle driver; Suture scissors; Deep sutures (Vicryl, polydioxanone); Mucosal sutures (eg, chromic, Vicryl Rapide) |
| Tissue retraction | Minnesota, Weider, Langenbeck retractors; Aufricht retractors (chin only); LeVasseur Merrill retractors (angles only) |
| Implants | Custom or stock implants (sterilized); Implant sizers ordered separately from the same company |
| Medications | Preoperative antibiotics (eg, weight-based ampicillin-sulbactam); Postoperative antibiotics (eg, coamoxiclav for 5-7 days); Pain management (eg, over-the-counter acetaminophen and ibuprofen) |
| Miscellaneous | Bite block; Raytec gauze |
Personnel
The surgical team may consist of as few as 2 individuals: the primary surgeon and an assistant. However, a cosurgeon is frequently present. A 2nd team typically includes an anesthesiologist, with or without a nurse anesthetist, responsible for providing deep or general anesthesia and supporting the surgical procedure.
Operating room nurses and technicians contribute actively, particularly in cases involving general anesthesia. Although oral and maxillofacial surgeons are capable of administering deep anesthesia, the presence of a dedicated anesthesia provider is standard practice. Routine intraoperative nerve monitoring is not required for facial implant procedures, as the subperiosteal dissection plane allows tissue reflection without involvement of critical nerves. Exposed nerves, including the mental and infraorbital nerves, are readily identifiable and protected throughout the operation.
Preparation
Human facial cosmetic evaluation has advanced alongside improvements in 3D technology. Currently, providers utilize 2D photographs in conjunction with both 2D and 3D radiographs to assess facial anatomy comprehensively.
Traditional 2D cephalometric analyses are foundational for evaluating facial proportions but are limited when applied to 3D structures. Recent developments in stereophotogrammetry, cone-beam computed tomography, and digital surface scanning permit detailed volumetric assessment of hard and soft tissues.
Reviews indicate that 3D anthropometric analysis more accurately captures facial curvature, symmetry, and contour than linear or angular 2D measurements, such as Holdaway or labiomental angles. Artificial intelligence-assisted cephalometric software and virtual surgical planning enable simulation of postoperative outcomes, optimization of implant positioning, and enhanced patient-specific design accuracy. Digital overlays and virtual surgical planning further allow objective evaluation of midface projection, chin prominence, and mandibular width, facilitating individualized implant selection.[28]
Standardized photographs are obtained with the patient facing the camera, at a 45° angle, and in profile, providing volumetric visualization from multiple perspectives. Lateral cephalograms are analyzed carefully, as they contain essential information for evaluating facial bone and soft tissue relationships critical to surgical planning.
The chin's position and its relationship to lower facial structures may be classified using multiple cephalometric measurements. Frequently used parameters include the following:
- Holdaway ratio (see Image. Holdaway Ratio)
- 0° meridian line (see Image. Zero-Degree Meridian)
- True vertical line (see Image. True Vertical Line)
- Labiomental angle (see Image. Labiomental Angle)
The Holdaway ratio compares the bony chin position to the lower incisor tips. This parameter is determined using 4 points: pogonion (Po), lower incisor tip (L1), nasion (N), and B point (B). Po is the most anterior aspect of the bony chin, B is the most concave point on the anterior mandible, and N corresponds to the nasofrontal suture. The vertical line connecting N to B is measured, and the distances from Po to N-B and L1 to N-B should be equal, producing a 1:1 ratio. Deviations exceeding 4 mm indicate a need for correction. Excessive proclination of the lower incisors may increase this ratio and compromise analysis accuracy.
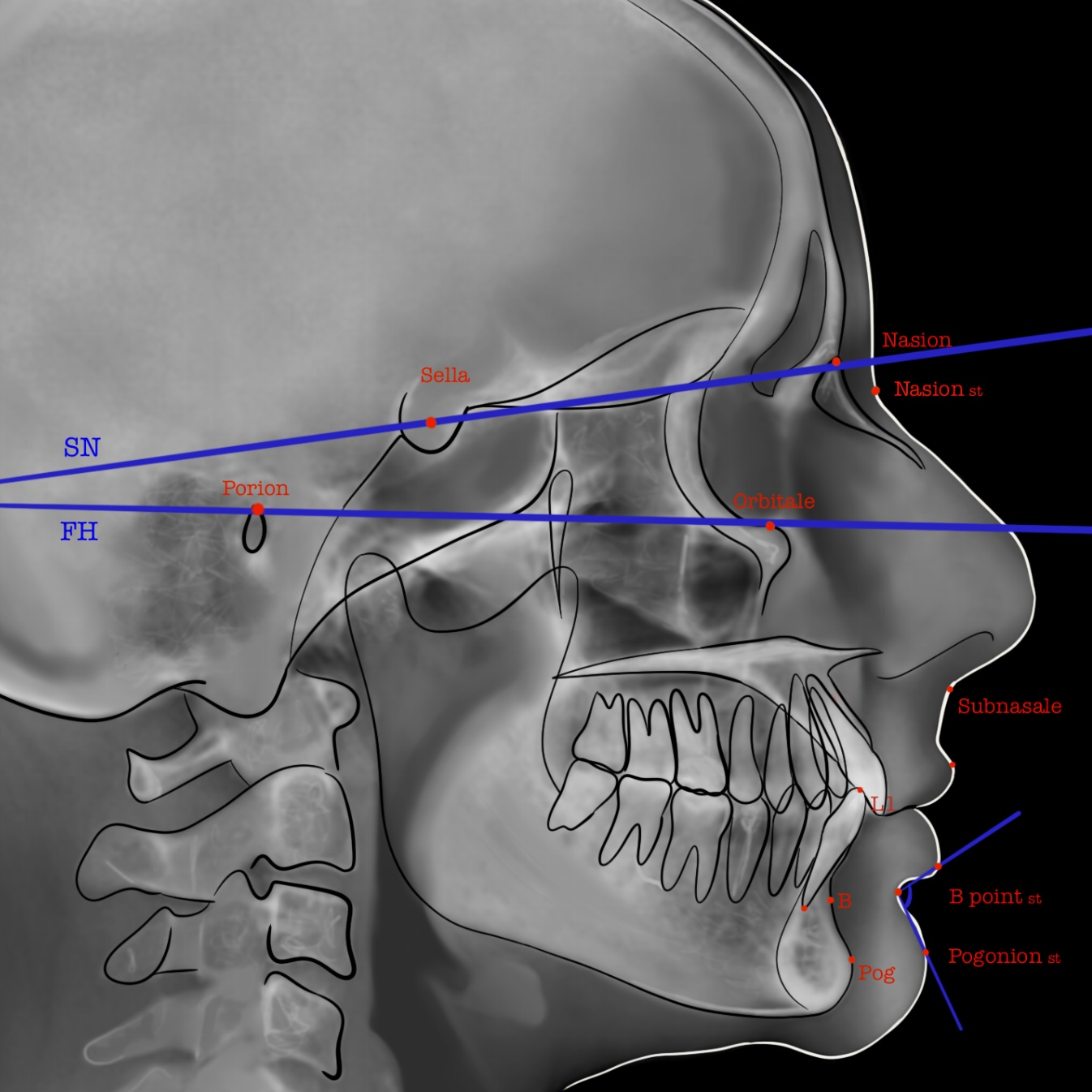
The 0° meridian line is a perpendicular line intersecting the Frankfort horizontal line at the nasion. The Frankfort horizontal line extends from the superior border of the external auditory meatus to the inferior orbital rim. The distance from the pogonion to the 0° meridian line should measure 0 mm in female individuals and up to 2 mm in male individuals, providing an objective assessment of chin position.
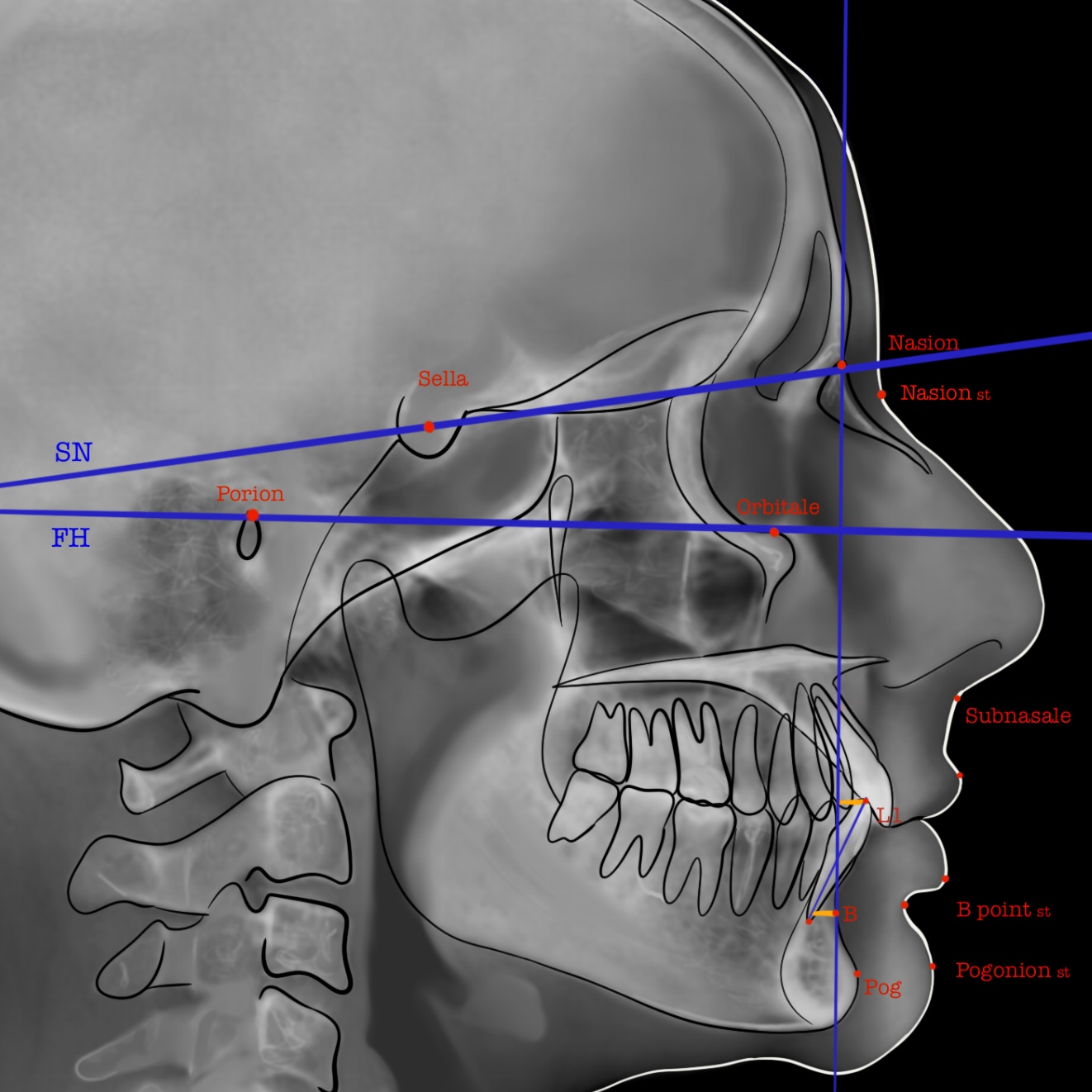
The true vertical line is perpendicular to the Frankfort horizontal plane and intersects the subnasale, the point at which the nasal columella meets the upper lip. Naini reported that mandibular retrusion of up to 4 mm or protrusion of up to 2 mm from the true vertical line may not be perceptible to observers without specialized facial surgical training.[29]
The labiomental angle represents the soft tissue convexity between the lower lip and chin. Chin morphology may be classified based on this convexity, which directly influences labiomental angle measurements. Convex, vertical, and posteriorly angled chins can accommodate larger implants, with vertical chins typically requiring approximately 8 mm of augmentation and posteriorly angled chins necessitating 12 mm or more.[30] Horizontal growth patterns are associated with well-developed chins and a deep labiomental groove. Implants exceeding 4 mm should not be placed at the thickest point of a convex labiomental angle to avoid overcorrection.
Facial implants may also augment the posterior mandible in the transverse dimension. Bigonial width is defined as the distance between the most inferior, lateral, and posterior points of the right and left mandibles. Farkas reported that, in individuals of Caucasian descent, the male bigonial width averages 34 mm less than the bizygomatic width, whereas the female bigonial width is approximately 36 mm shorter than the bizygomatic width.
Various soft tissue analyses are used to assess midfacial deficiencies, although evaluation with cephalometric imaging remains challenging. Powell identified the ideal malar eminence position as coinciding with the Frankfort horizontal plane, located 2 to 2.5 cm lateral to the lateral canthus. Bell proposed an alternative assessment, relating the malar eminence to the cornea, stating that the eminence should be positioned 4 to 8 mm anterior to the corneal plane. Frey observed that, in White individuals, the malar eminence is approximately 2 mm anterior to the cornea.[31] The Hinderer point, representing the malar region’s most prominent aspect, is situated approximately 15 to 20 mm inferior and 10 mm lateral to the lateral canthus.[32]
Binder classified midfacial deficiencies into 3 categories. Type 1 involves loss of malar projection secondary to skeletal hypoplasia. Type 2 is characterized by submalar soft tissue volume loss and is the most prevalent type. Type 3 combines features of types 1 and 2. Each deficiency type requires a tailored implant design and placement strategy. Type 1 deficiencies are addressed with malar shell implants to increase projection and lateralization. Type 2 deficiencies are corrected using submalar implants positioned below the zygoma on the anterior maxilla. Type 3 deficiencies may necessitate larger, combined implants to restore both skeletal and soft tissue volume.
Technique or Treatment
Antibiotic prophylaxis is critical to the success of facial implant procedures. Broad-spectrum antimicrobials are routinely administered preoperatively, intraoperatively, and postoperatively. Cefazolin is commonly used for extraoral incisions to cover skin flora, including Staphylococcus species, while simultaneous administration of amoxicillin or a 3rd-generation penicillin addresses oral gram-positive aerobes and anaerobes for intraoral incisions.[33] Ampicillin-sulbactam and cefazolin may serve as intraoperative alternatives.[34] The use of postoperative antibiotics is controversial, with no consensus regarding optimal timing or duration when prescribed.[35]
Surgical site preparation includes antiseptic cleansing with iodine followed by local anesthetic administration. The required anesthesia depth depends on the dissection approach and procedural complexity. Implants are typically placed under intravenous sedation or general anesthesia. Certain procedures, such as malar implant placement via a transconjunctival approach, may necessitate paralytic administration. Additional considerations include the procedural time associated with different anesthetic techniques, the cost of general anesthesia, and the experience of the anesthesia provider.
Malar implants are typically inserted via an intraoral approach. An incision is created 0.5 to 1.0 cm above the gingival margin within the mucosa, posterior to the canine fossa. Blunt subperiosteal dissection is performed posterolaterally along the anterior maxilla using a periosteal elevator. Dissection proceeds superiorly to the infraorbital rim, with careful identification and protection of the infraorbital neurovascular bundle. Adequate dissection is critical for larger implants that may extend near the infraorbital foramen.
For types 2 and 3 midfacial defects, dissection is extended laterally to the masseteric tendon to allow passive seating of the implant in the submalar region. The dissection pocket should exceed the implant dimensions to accommodate proper placement. Implant sizers, which are manufacturer-specific, are used to confirm the appropriate size and pocket adequacy. These sizers may be obtained as separate items or part of a surgical package. A 3D stereolithographic model of the patient’s face may also be used to visualize implant size and assist in trimming (see Image. Silicone Malar Implants). Implants and sizers are soaked in antibiotics prior to use, and the dissection pocket is irrigated with antibiotics before insertion. Sizers verify the correct esthetic outcome, implant dimensions, and adequacy of the dissection.
The implant is inserted carefully to minimize folding and optimize facial symmetry. Fixation is achieved using nonresorbable sutures or titanium screws (see Image. Malar Implant). The incision is then closed, and a compressive dressing is applied to reduce any dead space created during surgery. Various compressive therapies are available. An elastic compressive head wrap is a noninvasive option typically worn continuously for the first 7 days, except during showering. After the initial week, the dressing is worn only during sleep, allowing lymphatic drainage and reduction of swelling while relieving the area of continuous compression.[36]
Cheek bolsters, composed of cotton rolls secured with transcutaneous sutures, are employed for more invasive malar implant placements. Bolsters provide consistent compression and are removed 1 to 2 days postoperatively. Periosteal and bony tissues reapproximate within 24 to 48 hours.
Chin implants are inserted via intraoral or submental approaches. For intraoral placement, an incision is made in the anterior mandibular vestibule, extending from canine to canine, through the mucosa until the mentalis muscle is visualized. Muscle bellies may be incised using a bovie electrocautery device, scissors, or a blade. A cuff of the mentalis muscle should remain attached to the mandible and lip to preserve function.
Muscle tissue on opposing sides of the incision facilitates reapproximation and prevents ptosis. The mandible is exposed using blunt subperiosteal dissection, extending laterally along the inferior border before proceeding superiorly to identify the mental foramen and nerve (see Image. Mentalis Dissection). Dissection begins at the inferior border of the symphysis and continues superiorly to just beyond the planned implant dimensions. The dissection pocket should exceed the implant size to minimize complications, including implant migration, asymmetry, and soft tissue compression.
Implant sizers are placed to verify pocket adequacy and implant dimensions while guiding dissection to avoid injury to the mental nerve. Aufricht retractors enhance visualization and protect the nerve when lateral dissection is limited. The surgical site is irrigated with antibiotics as previously described. Implant fixation is achieved using nonresorbable sutures or titanium tacking screws. Layered closure follows. The mentalis muscle is reapproximated first with 2 to 4 single interrupted 3-0 Vicryl sutures, and the mucosa is closed using a faster-resorbing suture, such as 3-0 chromic gut.
Subperiosteal dissection also exposes the mandibular angles and ramus to the sigmoid notch. Releasing the pterygomasseteric sling allows placement of a titanium mesh implant along the inferior and posterior mandibular border, which is fixated with monocortical screws before layered closure.
Mandibular angle implants may be inserted via an intraoral or extraoral approach, depending on implant type and dimensions. For intraoral placement, a 1.5-cm incision is made lateral to the external oblique ridge, above the vestibular depth. Subperiosteal dissection exposes the mandibular angle and ramus to the sigmoid notch. Soft tissue is elevated from the anterior, inferior, lateral, and posterior mandibular aspects, including the pterygomasseteric sling. The sling is released to permit placement of titanium mesh implants along the inferior and posterior mandibular borders.
Implant fixation is achieved with monocortical titanium screws, followed by layered closure. The mandibular nerve is identified and protected, particularly when a nonmalleable implant or larger incision is required. A transcutaneous incision lateral to the implant may be used to facilitate a trocar system for anchoring the implant to the lateral ramus and body with monocortical screws. Securing the implant reduces dead space and ensures predictable augmentation volumes. Layered closure with resorbable sutures minimizes the risk of infection and scar formation.
Close postoperative follow-up is essential for early detection and management of complications.[37] A soft-food diet is recommended following posterior mandibular augmentation due to disruption of the mastication muscles during dissection.
Complications
Complications following facial implant placement may arise early during recovery or months to years postoperatively. Definitions of “early” and “late” vary among studies. For this activity, “early” refers to the first few weeks of soft tissue healing.[38] Reported complications include the following:
- Hematoma
- Seroma
- Infection
- Wound dehiscence
- Alveolar ridge resorption
- Poor or undesired aesthetic outcome
- Displacement or malpositioning
- Scarring
- Nerve injury
Bleeding is an early complication and may produce an expanding hematoma requiring drainage, typically secondary to inadequate hemostasis during surgery. Seromas may develop following implant placement due to inadvertent local gland disruption or the inflammatory response to the implant or surgical manipulation. Conservative subperiosteal dissection can minimize fluid accumulation. Management options include observation with or without antibiotic therapy, fluid aspiration, and, when necessary, repeat surgical intervention to control bleeding.
Late complications following facial implant placement include infection, implant mobilization, extrusion, and bone resorption. Recent systematic reviews and meta-analyses have quantified complication rates, reporting a pooled infection rate of approximately 2% to 5% for alloplastic implants and displacement in 1% to 3% of cases. Porous polyethylene implants exhibit lower rates of bone resorption compared with solid silicone implants, likely due to soft tissue ingrowth and improved load distribution. These findings highlight the necessity of careful patient selection, precise implant positioning, and rigorous postoperative management to reduce complication risk.
Intraoral incisions reduce the likelihood of visible scars, although some evidence suggests a potential increase in infection risk, which remains controversial. Persistent infection unresponsive to antibiotic therapy necessitates implant removal to prevent further morbidity.
Improper implant size, shape, or placement may result in functional deficits such as lip incompetence. In chin implants, active engagement of the mentalis muscle, which compensates for weakness, increases pressure on the underlying implant. Placement at the inferior mandibular border, where cortical thickness is greater and the implant is further from the mentalis insertion, has been associated with reduced bony resorption. Implant fixation mitigates micromovements that contribute to ongoing erosion. Although debated, reported erosion is generally self-limiting, with fixation presumed to influence this process.
Esthetic asymmetry may arise from implant folding or migration due to inadequate fixation, suboptimal subperiosteal placement, or insufficient dissection. Implant sizers assist in confirming appropriate dimensions before final placement. Cases of malposition or displacement are corrected surgically, either by securing the implant in the correct position or replacing it with an implant of a more suitable size and shape.
Poor cosmesis may result from inadequate reapproximation of the mentalis muscle, which is encountered and incised during intraoral chin implant procedures. The mentalis originates from the mandibular incisive fossa and inserts into the dermis of the chin, functioning to elevate the chin. Inadequate dissection, incision, or reapproximation techniques may produce ptosis, commonly referred to as “witch’s chin.” Extraoral approaches eliminate the risk of mentalis ptosis but introduce the potential for a visible submental scar.
Neurologic complications, including dysesthesia, hypoesthesia, and anesthesia, may arise from injury to the mental nerve, which provides sensation to the ipsilateral chin and lower lip. This nerve must be identified and preserved during augmentation procedures. Mental nerve injury has been reported in approximately 2.4% of cases, frequently associated with alveolar ridge resorption. Persistent nerve dysfunction may necessitate implant removal or replacement with a prosthesis of a more appropriate fit.
Clinical Significance
Facial implant surgery is highly versatile and offers an alternative to more invasive procedures, such as genial horizontal osteotomies. Less invasive methods generally reduce costs by using inexpensive hardware and anesthetic alternatives, and they require less operative time. Facial implant placement is routinely performed under general anesthesia or intravenous sedation. However, awake procedures using local anesthesia are also feasible.
A 2014 study from the University of California, Los Angeles reported that operating room costs may reach $35 per minute.[39] Alternative anesthetic approaches may reduce both general anesthetic risk and financial burden for patients with medical or economic limitations. Recovery after facial implant placement depends primarily on soft-tissue healing and typically requires only a few weeks, whereas bony surgery necessitates a significantly longer stabilization period.
Chin implants can enhance anterior and lateral projection and may also be used to narrow the chin, improving overall facial balance without osteotomies. Malar implants increase midfacial projection, contributing to a more harmonious and youthful facial appearance.
Mandibular angle implants can improve jawline definition and increase lower facial width. Implant placement may be used to augment bigonial width in patients requiring posttraumatic jaw reconstruction or correction of facial growth abnormalities. Individuals pursuing a more masculine facial structure as part of gender-affirmation surgery may also be candidates for mandibular angle augmentation. Additionally, implants can restore volume and skeletal support in the aging face across 3 dimensions.
With appropriate training and experience, facial implant placement is a safe and efficient procedure. Facial implant surgery provides an alternative to more extensive surgical interventions for patients seeking facial harmonization, a more youthful appearance, or alignment of facial structure with gender identity. The procedure also facilitates collaboration among interprofessional teams, including otorhinolaryngology and anesthesia specialists, particularly in the context of gender-affirmation surgeries.
Enhancing Healthcare Team Outcomes
An interprofessional approach optimizes outcomes in facial implant surgery. The primary care or cosmetic physician initially identifies the indication and refers the patient to an appropriate surgical specialist. Qualified surgeons include plastic surgeons, oral and maxillofacial surgeons, and otolaryngologists. After surgical evaluation, active patient participation throughout the planning, operative, and recovery phases is critical to ensure procedural success.
In outpatient settings, local anesthesia may be administered by the surgeon for awake procedures. An anesthesiologist provides expertise when deep anesthesia or advanced analgesic techniques, such as nerve blocks, are required. Nursing staff assist the surgeon intraoperatively, monitor patients during recovery, administer medications, and reinforce patient education. This collaborative model supports patient safety and high-quality care.
The U.S. Food and Drug Administration regulates implantable medical devices, and the range of approved materials continues to expand. Patients must be informed of device-specific risks. For example, silicone implants demonstrate no increase in reactive oxygen species or genotoxicity but may induce bony resorption when placed on the chin, as previously discussed.[40]
Media
(Click Image to Enlarge)

Mental Nerve. Terminal branches of the mental nerve as seen superficially.
Contributed by Kevin Smith, DDS
(Click Image to Enlarge)
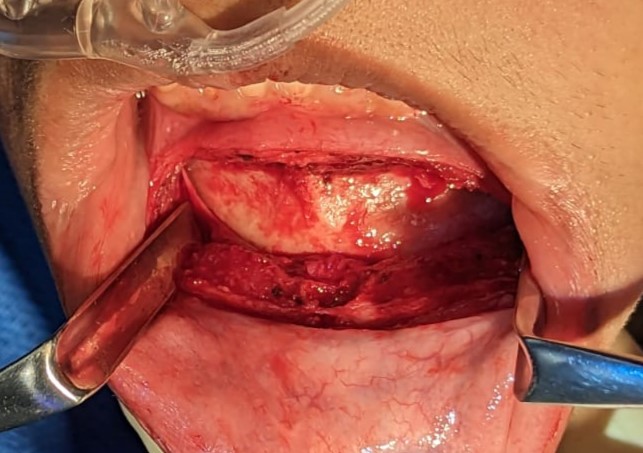
Mentalis Dissection. Subperiosteal dissection of the mandibular bone in preparation for implant placement. Two Aufricht retractors expose the lateral extent of the dissection. Both bellies of the mentalis muscle are visualized and incised, with cuffs preserved on the superior and inferior aspects of the incision.
Contributed by Kevin Smith, DDS
(Click Image to Enlarge)

Silicone Malar Implants. Silicone malar implants positioned on a 3D-printed stereolithographic model of the patient’s skeleton, facilitating precise trimming and placement while avoiding the infraorbital nerve.
Contributed by Dr. Marc Serra, DDS
(Click Image to Enlarge)
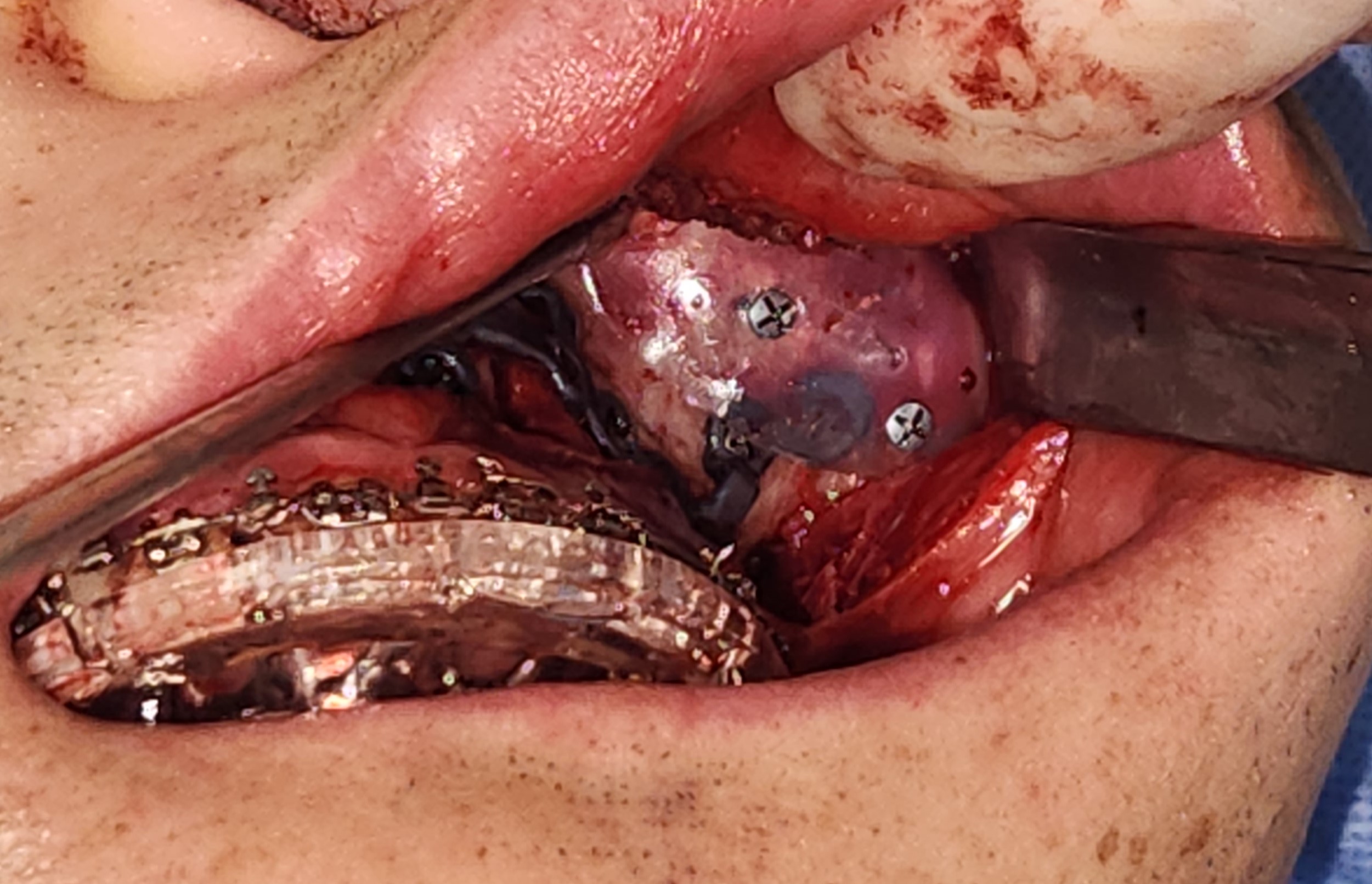
Malar Implant. Insertion of a malar implant via an intraoral approach using the patient’s maxillary orthognathic incision. The implant was positioned over the orthognathic fixation plates and secured with titanium screws.
Contributed by Marc Serra, DDS
(Click Image to Enlarge)
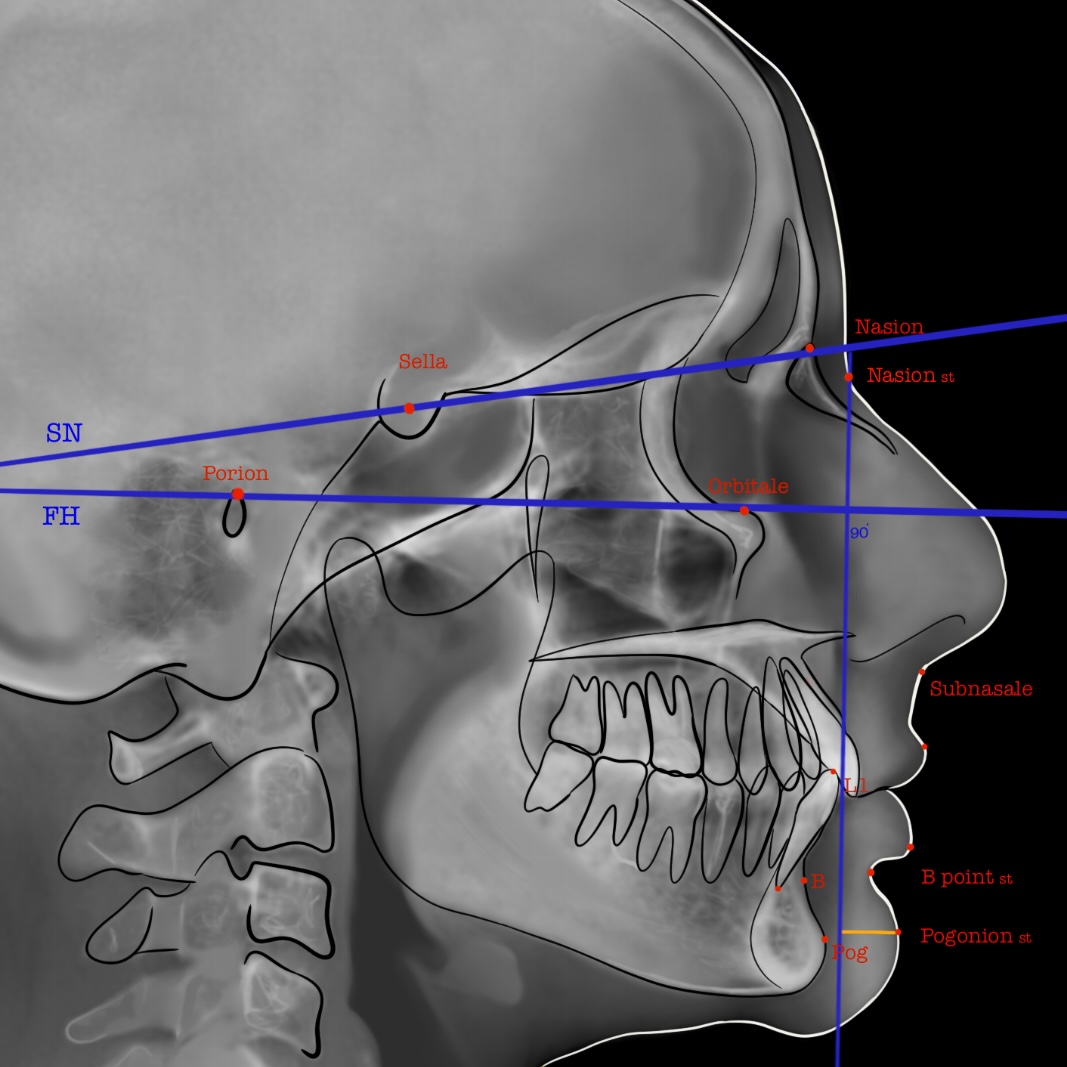
Zero-Degree Meridian. Lateral cephalometric view demonstrating the 0° meridian line, defined as a perpendicular line to the Frankfurt Horizontal plane passing through the nasion. The distance from this line to the soft tissue pogonion is used to assess chin position.
Contributed by Ellen Sharma, DDS
(Click Image to Enlarge)
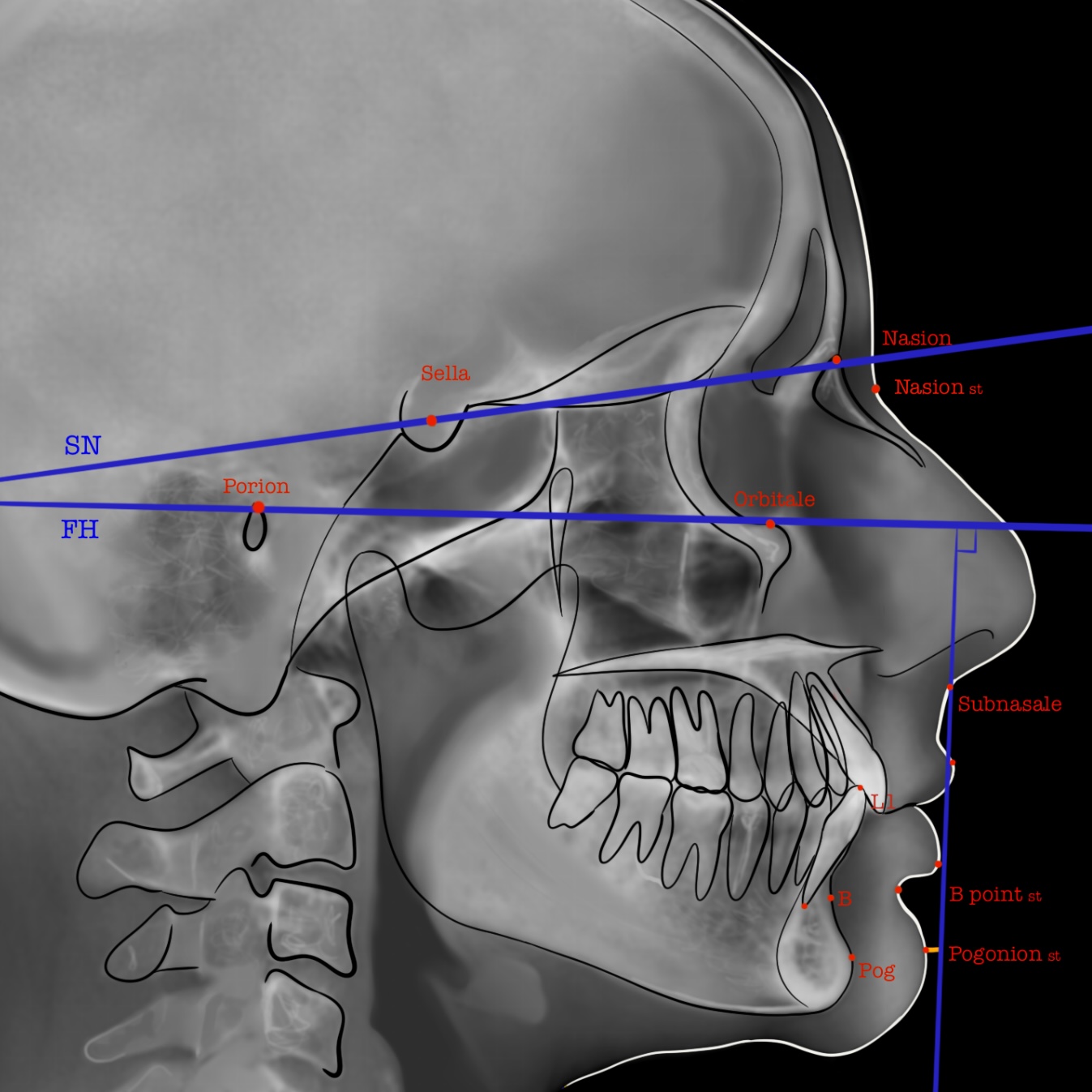
True Vertical Line. Lateral cephalometric view showing the true vertical line, defined as a line perpendicular to the Frankfurt horizontal (FH) plane that passes through the subnasale.
Contributed by Ellen Sharma, DDS
(Click Image to Enlarge)
Labiomental Angle. Lateral cephalometric view illustrating the labiomental angle, formed by the contour of the lower lip and the soft tissue of the chin, delineating the labiomental sulcus.
Contributed by Ellen Sharma, DDS
(Click Image to Enlarge)
Holdaway Ratio. Lateral cephalometric view illustrating the Holdaway ratio, which compares the lower incisor tip (L1) to the most anterior point of the bony chin (pogonion). The ideal ratio is 1:1.
Contributed by Ellen Sharma, DDS
(Click Image to Enlarge)

Zygomatic Submalar Implant. Preoperative and postoperative views of zygomatic submalar implant placement. In this patient, orthognathic surgery alone was insufficient to correct the midface volume deficiency.
Contributed by Kevin Smith, DDS
References
Binder WJ, Azizzadeh B. Malar and submalar augmentation. Facial plastic surgery clinics of North America. 2008 Feb:16(1):11-32, v [PubMed PMID: 18063245]
Abdulaziz MKB, Kamal M, Kolaityte V, Aziz H. Complications of alloplastic facial skeletal implants in aesthetic surgery: A systematic review and meta-analysis. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2025 Aug:107():5-18. doi: 10.1016/j.bjps.2025.04.042. Epub 2025 May 13 [PubMed PMID: 40499276]
Level 1 (high-level) evidenceCuzalina LA, Hlavacek MR. Complications of facial implants. Oral and maxillofacial surgery clinics of North America. 2009 Feb:21(1):91-104, vi-vii. doi: 10.1016/j.coms.2008.10.009. Epub [PubMed PMID: 19185798]
Lutz JC, Assouline Vitale LS, Graillon N, Foletti JM, Schouman T. Standard and Customized Alloplastic Facial Implants Refining Orthognathic Surgery: Outcome Evaluation. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2020 Oct:78(10):1832.e1-1832.e12. doi: 10.1016/j.joms.2020.05.009. Epub 2020 May 15 [PubMed PMID: 32574606]
Niamtu J 3rd. Essentials of cheek and midface implants. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2010 Jun:68(6):1420-9. doi: 10.1016/j.joms.2009.12.004. Epub 2010 Apr 9 [PubMed PMID: 20381942]
Romano N, Federici M, Castaldi A. Imaging of cranial nerves: a pictorial overview. Insights into imaging. 2019 Mar 15:10(1):33. doi: 10.1186/s13244-019-0719-5. Epub 2019 Mar 15 [PubMed PMID: 30877408]
Level 3 (low-level) evidenceHazani R, Rao A, Ford R, Yaremchuk MJ, Wilhelmi BJ. The safe zone for placement of chin implants. Plastic and reconstructive surgery. 2013 Apr:131(4):869-872. doi: 10.1097/PRS.0b013e3182818e6c. Epub [PubMed PMID: 23542258]
Hu KS, Yun HS, Hur MS, Kwon HJ, Abe S, Kim HJ. Branching patterns and intraosseous course of the mental nerve. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2007 Nov:65(11):2288-94 [PubMed PMID: 17954327]
Azizzadeh B, Mashkevich G. Nerve injuries and treatment in facial cosmetic surgery. Oral and maxillofacial surgery clinics of North America. 2009 Feb:21(1):23-9, v. doi: 10.1016/j.coms.2008.10.003. Epub [PubMed PMID: 19185792]
Mendelson B, Wong CH. Changes in the facial skeleton with aging: implications and clinical applications in facial rejuvenation. Aesthetic plastic surgery. 2012 Aug:36(4):753-60. doi: 10.1007/s00266-012-9904-3. Epub 2012 May 12 [PubMed PMID: 22580543]
Fattahi T. The prejowl sulcus: an important consideration in lower face rejuvenation. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2008 Feb:66(2):355-8. doi: 10.1016/j.joms.2006.11.032. Epub [PubMed PMID: 18201622]
Cronin RJ Jr, Oesterle LJ, Ranly DM. Mandibular implants and the growing patient. The International journal of oral & maxillofacial implants. 1994 Jan-Feb:9(1):55-62 [PubMed PMID: 8150513]
Op Heij DG, Opdebeeck H, van Steenberghe D, Quirynen M. Age as compromising factor for implant insertion. Periodontology 2000. 2003:33():172-84 [PubMed PMID: 12950850]
Yaremchuk MJ. Mandibular augmentation. Plastic and reconstructive surgery. 2000 Sep:106(3):697-706 [PubMed PMID: 10987481]
Birgfeld C, Heike C. Craniofacial Microsomia. Clinics in plastic surgery. 2019 Apr:46(2):207-221. doi: 10.1016/j.cps.2018.12.001. Epub [PubMed PMID: 30851752]
Schwaiger M, Echlin K, Atherton D, Haers P. The use of Medpor implants for midface contouring in cleft patients. International journal of oral and maxillofacial surgery. 2019 Sep:48(9):1177-1184. doi: 10.1016/j.ijom.2019.02.008. Epub 2019 Mar 11 [PubMed PMID: 30871847]
Aarts BE, Convens J, Bronkhorst EM, Kuijpers-Jagtman AM, Fudalej PS. Cessation of facial growth in subjects with short, average, and long facial types - Implications for the timing of implant placement. Journal of cranio-maxillo-facial surgery : official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2015 Dec:43(10):2106-11. doi: 10.1016/j.jcms.2015.10.013. Epub 2015 Oct 23 [PubMed PMID: 26548528]
Hardin AM, Knigge RP, Oh HS, Valiathan M, Duren DL, McNulty KP, Middleton KM, Sherwood RJ. Estimating Craniofacial Growth Cessation: Comparison of Asymptote- and Rate-Based Methods. The Cleft palate-craniofacial journal : official publication of the American Cleft Palate-Craniofacial Association. 2022 Feb:59(2):230-238. doi: 10.1177/10556656211002675. Epub 2021 May 17 [PubMed PMID: 33998905]
Stringer D, Brown B. Correction of mandibular asymmetry using angled titanium mesh. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2009 Aug:67(8):1619-27. doi: 10.1016/j.joms.2008.12.068. Epub [PubMed PMID: 19615573]
Level 3 (low-level) evidenceMaas CS, Merwin GE, Wilson J, Frey MD, Maves MD. Comparison of biomaterials for facial bone augmentation. Archives of otolaryngology--head & neck surgery. 1990 May:116(5):551-6 [PubMed PMID: 2158331]
Level 3 (low-level) evidenceOliveira RV, de Souza Nunes LS, Filho HN, de Andrade Holgado L, Ribeiro DA, Matsumoto MA. Fibrovascularization and osteogenesis in high-density porous polyethylene implants. The Journal of craniofacial surgery. 2009 Jul:20(4):1120-4. doi: 10.1097/SCS.0b013e3181abb4ab. Epub [PubMed PMID: 19553849]
Level 3 (low-level) evidenceRomo T 3rd, Lanson BG. Chin augmentation. Facial plastic surgery clinics of North America. 2008 Feb:16(1):69-77, vi [PubMed PMID: 18063247]
Danieletto-Zanna CF, Ferreira GZ, Ferreira O, Pavan AJ, Camarini ET. Infected Silicone Chin Implant After Implant-Supported Jaw Rehabilitation: Case Report and Literature Review. The Journal of oral implantology. 2022 Aug 1:48(4):307-311. doi: 10.1563/aaid-joi-D-20-00112. Epub [PubMed PMID: 34091685]
Level 3 (low-level) evidenceGafar Ahmed M, AlHammad ZA, Al-Jandan B, Almohammadi T, Khursheed Alam M, Bagde H. Silicone Facial Implants, to Fixate or Not to Fixate: A Narrative Review. Cureus. 2023 Feb:15(2):e34524. doi: 10.7759/cureus.34524. Epub 2023 Feb 1 [PubMed PMID: 36874350]
Level 3 (low-level) evidenceRowe P, Koller A, Sharma S. Physiology, Bone Remodeling. StatPearls. 2025 Jan:(): [PubMed PMID: 29763038]
Frodel JL, Lee S. The use of high-density polyethylene implants in facial deformities. Archives of otolaryngology--head & neck surgery. 1998 Nov:124(11):1219-23 [PubMed PMID: 9821923]
Level 3 (low-level) evidenceKattimani V, Sreeram RR, Panga GSK, Vasamsetti DB, Tiwari R. Patient-Specific Implants in Maxillo-Facial Reconstruction: Current Practices and Way Forward-An Overview of Systematic Reviews. Journal of maxillofacial and oral surgery. 2025 Aug:24(4):1075-1089. doi: 10.1007/s12663-025-02440-4. Epub 2025 Jan 15 [PubMed PMID: 40756914]
Level 1 (high-level) evidenceVelarde K, Cafino R, Isla A Jr, Ty KM, Palmer XL, Potter L, Nadorra L, Pueblos LV, Velasco LC. Virtual surgical planning in craniomaxillofacial surgery: a structured review. Computer assisted surgery (Abingdon, England). 2023 Dec:28(1):2271160. doi: 10.1080/24699322.2023.2271160. Epub 2023 Oct 20 [PubMed PMID: 37862041]
Naini FB, Donaldson AN, McDonald F, Cobourne MT. Assessing the influence of chin prominence on perceived attractiveness in the orthognathic patient, clinician and layperson. International journal of oral and maxillofacial surgery. 2012 Jul:41(7):839-46. doi: 10.1016/j.ijom.2012.01.012. Epub 2012 Feb 15 [PubMed PMID: 22340990]
Fanous N, Yoskovitch A. Estimating implant size in chin augmentation: A simplified approach. The Canadian journal of plastic surgery = Journal canadien de chirurgie plastique. 2003 Fall:11(3):161-5 [PubMed PMID: 24115862]
Doddamani GM, Swathi PV, Tan KFH. Assessment of anterior malar projection using visual photographs and lateral cephalograms: A comparative study. Journal of orthodontic science. 2018:7():15. doi: 10.4103/jos.JOS_30_18. Epub 2018 Sep 6 [PubMed PMID: 30271760]
Level 2 (mid-level) evidenceHinderer UT. Malar implants for improvement of the facial appearance. Plastic and reconstructive surgery. 1975 Aug:56(2):157-65 [PubMed PMID: 1096196]
Caruso SR, Yamaguchi E, Portnof JE. Update on Antimicrobial Therapy in Management of Acute Odontogenic Infection in Oral and Maxillofacial Surgery. Oral and maxillofacial surgery clinics of North America. 2022 Feb:34(1):169-177. doi: 10.1016/j.coms.2021.08.005. Epub 2021 Oct 30 [PubMed PMID: 34728145]
Khorasani M, Janbaz P, Rayati F. Maxillofacial reconstruction with Medpor porous polyethylene implant: a case series study. Journal of the Korean Association of Oral and Maxillofacial Surgeons. 2018 Jun:44(3):128-135. doi: 10.5125/jkaoms.2018.44.3.128. Epub 2018 Jun 26 [PubMed PMID: 29963494]
Level 2 (mid-level) evidenceOranges CM, Grufman V, di Summa PG, Fritsche E, Kalbermatten DF. Chin Augmentation Techniques: A Systematic Review. Plastic and reconstructive surgery. 2023 May 1:151(5):758e-771e. doi: 10.1097/PRS.0000000000010079. Epub 2022 Dec 20 [PubMed PMID: 36729154]
Level 1 (high-level) evidenceWang MW, Rodman RE. Gender Facial Affirmation Surgery; Techniques for Feminizing the Chin. Facial plastic surgery clinics of North America. 2023 Aug:31(3):419-431. doi: 10.1016/j.fsc.2023.04.006. Epub [PubMed PMID: 37348985]
Al-Jandan B, Marei HF. Mandibular angle augmentation using solid silicone implants. Dental and medical problems. 2018 Oct-Dec:55(4):367-370. doi: 10.17219/dmp/99531. Epub [PubMed PMID: 30648361]
Rojas YA, Sinnott C, Colasante C, Samas J, Reish RG. Facial Implants: Controversies and Criticism. A Comprehensive Review of the Current Literature. Plastic and reconstructive surgery. 2018 Oct:142(4):991-999. doi: 10.1097/PRS.0000000000004765. Epub [PubMed PMID: 29994843]
Childers CP, Maggard-Gibbons M. Understanding Costs of Care in the Operating Room. JAMA surgery. 2018 Apr 18:153(4):e176233. doi: 10.1001/jamasurg.2017.6233. Epub 2018 Apr 18 [PubMed PMID: 29490366]
Level 3 (low-level) evidenceVijayalakshmi P, Geetha CS, Mohanan PV. Assessment of oxidative stress and chromosomal aberration inducing potential of three medical grade silicone polymer materials. Journal of biomaterials applications. 2013 Feb:27(6):763-72. doi: 10.1177/0885328211426353. Epub 2011 Nov 15 [PubMed PMID: 22090429]
Level 3 (low-level) evidence