Introduction
Foster Kennedy syndrome (FKS) is defined by neurologic findings that include anosmia and visual loss, including central scotoma, which may be unilateral or bilateral depending on the stage of the condition. FKS is characterized by compressive optic nerve damage with optic atrophy in one eye and contralateral papilledema, resulting from increased intracranial pressure secondary to a space-occupying intracranial lesion.[1] Foster Kennedy syndrome was first mentioned in the literature in 1945.[2][3] Notably, the classic presentation of FKS is also seen in pseudo-FKS; therefore, the clinician must carefully select and perform appropriate examination techniques to ensure an accurate diagnosis.
Foster Kennedy syndrome typically includes 3 types.[4] Type 1, the most frequent form, presents with optic atrophy in the ipsilateral eye and papilledema in the contralateral eye. Type 2 is characterized by bilateral papilledema and unilateral optic atrophy.[5] Type 3 is defined by bilateral papilledema that progresses into bilateral optic atrophy. These 3 types of FKS are caused by different stages of tumor growth and intracranial mass effect.
Pseudo-FKS has the typical presentation of optic atrophy in one eye and papilledema in the contralateral eye, similar to type 1 FKS.[6][7] However, pseudo-FKS lacks underlying compressive pathology.[8][9] Causes of pseudo-FKS include optic nerve compression by the gyrus rectus, diabetic papillopathy, and unilateral optic nerve hypoplasia.[10][11]
Meningiomas are space-occupying tumors originating in the central nervous system (see Image. Contrast-Enhanced CT Imaging of Meningioma).[12] The term refers to specific disorders of the pia, dura, and arachnoid layers that encapsulate the brain. Meningiomas may be malignant or nonmalignant.[13] Common sites of occurrence include the sphenoid wing, olfactory groove, and frontal lobe.[14][15] Meningiomas are the most common type of nonmalignant tumors found in the brain.[16] Because meningiomas are often insidious, they may cause subtle, progressive changes that remain unnoticed initially. These tumors may initially herniate into the subarachnoid space and dural sinuses, leading to intracranial hypertension.[17] Eventually, meningiomas compress adjacent vessels and brain tissue, causing an array of symptoms and eventual tissue atrophy.[17] Additionally, pituitary gland tumors have also been reported to cause FKS and are the second most common cause of cerebral tumors.[18][19] The risk of FKS may be exacerbated in patients who have undergone surgical resection for pituitary adenomas and radiotherapy because they may subsequently develop complications, including tentorial meningiomas.[20][21][22]
Although FKS classically presents with ipsilateral optic atrophy and contralateral papilledema secondary to an anterior cranial fossa mass, the complete syndrome is relatively uncommon in modern clinical practice because intracranial lesions are often detected earlier by neuroimaging. In contemporary neuro-ophthalmology, incomplete or atypical variants are increasingly recognized, particularly in patients with frontal meningiomas, olfactory groove tumors, and parasellar lesions. Rare atypical variants of FKS have also been described in the literature. Inverse FKS refers to the presence of optic atrophy contralateral to the intracranial lesion and ipsilateral optic disc swelling.[23] Although uncommon, inverse FKS highlights the complexity of compressive optic neuropathies and the importance of correlating neuroimaging findings with detailed neuro-ophthalmic examination.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Brain tumors account for approximately 12% of optic disc swelling.[24] The causative mass lesion is usually an anterior cranial fossa meningioma. However, tumors in other parts of the brain, such as the frontal lobe, olfactory groove, sphenoid wing, and pituitary gland, can also cause the condition (see Image. MRI of a Frontosphenoidal Meningioma in Foster Kennedy Syndrome).[11][19]
Risk factors for meningiomas include hereditary factors, female hormones, and prior radiation exposure.[25] Meningiomas compress the ipsilateral optic nerve on the side of the brain where they form, causing progressive optic atrophy. As meningiomas enlarge, these tumors may breach the cerebral falx and cross to the contralateral side, resulting in restricted cerebrospinal fluid flow and papilledema in the contralateral eye. Alternatively, a patient may present with complete optic atrophy in one eye and temporal hemianopsia in the other eye.[19]
Epidemiology
Foster Kennedy syndrome remains an uncommon neuro-ophthalmic manifestation despite the relatively high incidence of intracranial tumors. The syndrome is most frequently associated with slowly enlarging anterior cranial fossa masses, particularly olfactory groove and sphenoid wing meningiomas, which demonstrate a female predominance likely related to hormonal influences and sex-specific molecular factors.[12][25] Meningiomas account for approximately one-third of all primary intracranial tumors and are considered the most common nonmalignant central nervous system neoplasms in adults.[16]
FKS generally develops gradually because the underlying lesions often enlarge slowly, leading to progressive optic nerve compression and delayed intracranial hypertension. The condition is most commonly diagnosed in middle-aged adults, although younger patients with aggressive tumors, pituitary adenomas, metastatic lesions, or infectious intracranial masses have also been described.[19][26] Improvements in neuroimaging techniques, particularly high-resolution magnetic resonance imaging, have reduced the frequency of classic, complete presentations because many intracranial lesions are now identified before the development of advanced optic atrophy and contralateral papilledema. Consequently, incomplete or atypical variants, including pseudo-FKS and inverse FKS, are increasingly recognized in modern neuro-ophthalmic practice.[4] Results from studies showed that the age-adjusted incidence rate of central nervous system tumors was 23.41 per 100,000 individuals,[16] and the reported rates were slightly higher in women.[25] Furthermore, FKS has been reported in 1% to 2.5% of intracranial tumors.[27]
Pathophysiology
Foster Kennedy syndrome results from intracranial space-occupying lesions, especially those in the anterior cranial fossa.[28] The presence of an intracranial space-occupying lesion increases intracranial pressure and directly compresses the optic nerve, resulting in ipsilateral optic atrophy due to nerve fiber loss. Swelling in the remaining damaged nerve fibers is usually not evident. Increased intracranial pressure causes swelling of the optic disc in the contralateral eye, which still has sufficient nerve fibers to make the swelling evident. Anosmia results from intracranial space-occupying lesions or compression of the olfactory nerve.[26] Optical coherence tomography may demonstrate thinning of the retinal nerve fiber layer in the atrophic eye and thickening related to disc edema in the contralateral eye. Optical coherence tomography has become increasingly useful for documenting structural changes in the optic nerve and monitoring progression in neuro-ophthalmic disorders.[29]
History and Physical
When discussing signs and history with patients, clinicians should note patient concerns of headache, unilateral or bilateral vision loss, and, in later stages, anosmia. The clinician can expect to see an elevated optic disc. Detection of papilledema can be challenging in the early stages, especially in stage 1, which may present with a C-shaped halo while preserving the temporal disc margin.[30] The later stages of papilledema are more easily identifiable because of disc elevation and obscured blood vessels. Additionally, more advanced stages of papilledema can be correlated with signs of a forebrain tumor, including emotional lability, impaired coordination, and speech impairment. Intracranial space-occupying lesions of the forebrain can extend beyond the anterior cranial fossa and, therefore, may be associated with other tumors affecting other parts of the brain. Additional neuro-ophthalmic findings may include a relative afferent pupillary defect, dyschromatopsia, visual field defects, reduced contrast sensitivity, and impaired color vision. Visual field testing may demonstrate central scotomas, junctional scotomas, or other patterns of compressive optic neuropathy, depending on the lesion location.
Evaluation
The initial evaluation of FKS is usually performed with fundoscopy, preferably after pupillary dilation. Ophthalmoscopy, slit lamp biomicroscopy with an accessory lens, or fundus imaging allows the examiner to visualize the back of the eye. Visualization of optic atrophy and damage to the retinal nerve fiber layer is enhanced with a red-free filter. Papilledema is best assessed by directly viewing the optic disc through a slit aperture with an ophthalmoscope, which can reveal a typical feature of FKS.[31] Results from studies showed a positive correlation between elevated intracranial pressure and increased intraocular pressure. Intraocular pressure can be measured by contact or noncontact tonometry.[32][33]
Radiologic imaging may precede or follow ocular examination, depending on the flow of patient care. Standard radiography is not very useful for detecting brain tumors because the skull absorbs the radiation, preventing visualization of deeper tissues. CT scans use x-rays that pass through different body parts, combined with a computer algorithm, to generate images of slices of the imaged body region. The patient should be instructed to minimize movement during the procedure to ensure optimal image quality. Metals, reflective objects, and clothing should also be removed from the head before imaging. The patient usually lies supine on an electronic bed while the equipment takes multiple scans as it rotates around the body. An iodine-based contrast agent may be injected into the patient’s vein to provide improved imaging.[34] Clinicians should ensure that an appropriate kidney function test is performed to confirm that the patient can eliminate the agent after administration.[35][36][37] A CT scan is contraindicated in pregnant individuals and requires skilled interpretation for accurate diagnosis.[38] Additionally, a CT scan is typically fast and accurate for the differential diagnosis of patients with FKS.[39][40]
Magnetic resonance imaging provides better soft-tissue characterization than CT. In addition, MRI does not use ionizing radiation and is therefore safer with regard to radiation exposure. MRI uses a magnetic field to align atoms in the body from a random arrangement into a systematic arrangement.[41] The equipment then sends a radio wave that excites these atoms from their new position. When this radio wave is turned off, the atoms return to their initial positions, thereby emitting a radio signal.[42] An embedded algorithm in the MRI equipment then converts these emitted signals into a 2D image of the part of the body being observed.[43] Because ionizing radiation is absent, MRI is the scan of choice for monitoring the progression of a brain mass or tumor.[44][45] However, MRI takes longer than CT and may be less feasible in emergency settings in many hospitals; therefore, MRI is often scheduled after CT scans are obtained in patients with FKS. MRI with gadolinium contrast is generally preferred over CT for evaluating compressive lesions associated with FKS because of its superior soft-tissue characterization and improved visualization of the optic nerves, anterior cranial fossa, and parasellar region.[46]
Because of the close relationship between FKS and cranial neoplastic tumors, patients may have varying types and levels of neurological deficits. Associated deficits may include aphasia, anosmia, agraphia, abasia, or ataxia, among others.[47] Additional neurologic manifestations may vary depending on the size, location, and degree of mass effect produced by the intracranial lesion. Patients may present with seizures, cognitive decline, personality changes, emotional lability, focal motor weakness, cranial nerve palsies, diplopia, and visual field abnormalities due to compression of adjacent neural structures and optic pathways.[47] Frontal lobe involvement may lead to impaired executive functioning, disinhibition, apathy, reduced concentration, and behavioral disturbances, whereas parasellar and skull base lesions may produce ophthalmoplegia and multiple cranial neuropathies.[45] Therefore, a comprehensive neurologic and neuro-ophthalmic examination is essential in patients with suspected FKS to identify associated deficits and guide urgent neuroimaging evaluation and interdisciplinary treatment.
Treatment / Management
Treatment of FKS depends on tumor histology, size, location, mass effect, and patient functional status. Advances in skull base neurosurgery, stereotactic radiosurgery, and molecular tumor profiling have improved outcomes in selected patients with meningiomas and other intracranial neoplasms associated with FKS. Treatment options for FKS tumors include surgical resection, chemotherapy, radiotherapy, and medical therapy.
Surgical Resection
Surgical resection remains the main treatment for symptomatic FKS when the underlying lesion is a surgically accessible anterior skull base, olfactory groove, sphenoid wing, or parasellar tumor.[48] The operative goal is maximal safe resection with decompression of the optic apparatus, reduction of mass effect, histopathologic confirmation, and preservation of neurovascular structures, rather than radical removal at the expense of neurologic morbidity. Recent literature on skull base procedures emphasizes individualized surgical planning based on tumor size, edema, vascular encasement, optic pathway involvement, and patient functional status.[49][50]
Chemotherapy
Conventional cytotoxic chemotherapy has a limited role in most meningiomas and other slow-growing tumors associated with FKS, and no universally accepted standard systemic therapy currently exists for refractory meningioma.[51] Systemic treatment is generally reserved for recurrent, progressive, unresectable, metastatic, or high-grade disease after surgical procedures and radiotherapy have been exhausted. Investigational approaches include targeted agents, antiangiogenic therapy, somatostatin receptor–directed strategies, immune checkpoint inhibition, and peptide receptor radionuclide therapy in selected tumors.[52][53](A1)
Radiotherapy
For lesions that cause FKS, radiotherapy is most useful as adjuvant treatment after subtotal resection, for recurrent tumors, for higher-grade meningiomas, or for lesions in which complete surgical removal would carry unacceptable neurologic or visual risk.[54] Modern conformal radiotherapy, stereotactic radiotherapy, proton therapy, and stereotactic radiosurgery allow more precise treatment of skull base tumors. These approaches attempt to limit radiation exposure to the optic nerves, chiasm, pituitary gland, and adjacent brain tissue.[55][56](A1)
Medical Therapy
In FKS, medical therapy is usually supportive rather than curative and should not delay definitive treatment of the underlying intracranial lesion. Corticosteroids may be used short-term to reduce vasogenic edema and mass-effect symptoms, while analgesics, antiemetics, seizure treatment, endocrine replacement, and intracranial pressure treatment may be required depending on the patient’s presentation. However, these measures do not reverse established compressive optic atrophy and should be integrated with urgent neurosurgical, neuro-oncologic, radiation oncology, and neuro-ophthalmologic assessment.[49][51]
Treatment of FKS usually involves surgical resection, although chemotherapy and radiotherapy are also employed, especially in older adults, who may have a higher mortality risk.[57][58] Regarding medical therapy, systemic corticosteroids are first-line treatment, although clinicians usually use them to reduce edema around the tumor and intracranial pressure.[59] In older patients, a nonneurosurgical procedure, such as stereotactic radiotherapy or radiosurgery, may be preferable. Furthermore, anecdotal reports suggest that hydroxyurea may be useful, especially for unresectable or large residual tumors.[60](B3)
Differential Diagnosis
The differential diagnosis of Foster Kennedy syndrome includes:
- Frontal lobe parenchymal tumors: Tumors that affect the frontal lobe are included in the differential diagnosis of FKS, especially those involving structures in the anterior cranial fossa.
- Meningioma: Olfactory groove, frontal, and sphenoid wing meningiomas should be considered in the differential diagnosis of FKS. These tumors can occur without ocular complications and would therefore not qualify as FKS.
- Pseudo-FKS: Pseudo-FKS is the most common differential diagnosis for FKS; in simplified terms, pseudo-FKS refers to an FKS-like presentation without a tumor.[1] Pseudo-FKS can mimic FKS, but its clinical features and presentation differ. The fundamental distinction is the absence of an intracranial mass lesion. Because pseudo-FKS presentations may occur without intracranial mass lesions, neuroimaging is essential in all suspected cases to exclude compressive pathology.
- Nonarteritic anterior ischemic optic neuropathy: This condition is the second most common cause of optic neuropathy. Nonarteritic anterior ischemic optic neuropathy is a noninflammatory ischemic condition affecting the 1-mm region of the optic disc, typically due to reduced blood flow from the posterior ciliary artery, which supplies the optic nerve head. Results from studies suggested that embolism may contribute to nonarteritic anterior ischemic optic neuropathy. Additionally, a nocturnal decrease in perfusion pressure may contribute to this condition.[61]
- Optic nerve hypoplasia: Optic nerve hypoplasia is a congenital condition in which the optic nerve fails to develop fully, resulting in the classic small, pale appearance of the optic nerve. Optic nerve hypoplasia may occur with nonarteritic anterior ischemic optic neuropathy in some patients.[11] The causes of optic nerve hypoplasia remain incompletely understood, although results from correlational studies showed associations with fetal alcohol syndrome and maternal intake of quinine, phenytoin, and lysergic acid diethylamide.
- Optic neuritis: Optic neuritis results from inflammation of the optic nerve. The condition is referred to as optic papillitis when inflammation involves the optic nerve head. Neuroretinitis refers to inflammation of the optic nerve head and macula. Retrobulbar neuritis refers to inflammation of the posterior part of the nerve. Please see StatPearls' companion reference, "Neuromyelitis Ocular Spectrum Disorder," for further information.
- Idiopathic intracranial hypertension: Papilledema is a sign of a pathological condition in the eye, characterized by elevation of the optic nerve head.[62] Papilledema results from a sustained increase in intracranial pressure, with varying degrees of blurred optic disc margins and visual loss.[63][64]
- Vitamin B12 deficiency: Progressive optic neuropathy can arise from vitamin B12 deficiency and may masquerade as FKS. However, vitamin B12 deficiency–associated optic neuropathy is potentially reversible with appropriate supplementation.[65]
Surgical Oncology
The decision to proceed with a surgical procedure for FKS depends on a risk-benefit analysis guided by the consulting clinicians. Brain surgical procedures require an interdisciplinary decision and treatment approach. As with all tumors, complete removal of the malignant neoplasm is recommended when surgical intervention is performed. Tissue samples should be sent for histopathologic examination to better understand and stage the lesion. Additionally, surgical resection may be followed by adjuvant chemotherapy.[58][60]
Radiation Oncology
Radiotherapy is recommended as an adjuvant treatment to surgical procedures for patients with recurrent tumors.[66] While some authors recommend immediate radiotherapy, others advise delaying radiotherapy until the lesion shows signs of progression or recurrence.[67][68]
Prognosis
The prognosis of FKS depends primarily on the location, size, histopathology, growth rate, and extent of the underlying intracranial space-occupying lesion, as well as the severity and duration of optic nerve compression before treatment initiation. Early diagnosis and timely intervention may improve neurologic and visual outcomes, particularly in patients with reversible papilledema and limited optic nerve damage. Visual recovery is often variable and may remain incomplete in cases of long-standing compressive optic atrophy, severe papilledema, delayed treatment, or advanced intracranial hypertension.[12][28] Prognosis is generally more favorable in patients with nonmalignant, slow-growing lesions such as meningiomas that are amenable to complete surgical resection, whereas aggressive, recurrent, metastatic, or unresectable tumors are associated with higher morbidity and mortality.[28] Advances in neuroimaging, skull base surgical procedures, stereotactic radiosurgery, and interdisciplinary neuro-oncologic treatment have improved diagnostic accuracy, treatment planning, and long-term outcomes in selected patients with FKS.
Complications
Complications of FKS may be ocular or systemic. Ocular complications of FKS include disc edema, relative afferent pupillary defect, restricted ocular movements, reduced visual acuity, papilledema, and optic atrophy.[27] Delayed diagnosis may result in irreversible optic nerve damage and permanent visual loss due to prolonged compression and chronic papilledema. Systemic complications include anosmia and other symptoms that may result from tumor compression of specific brain regions.
Deterrence and Patient Education
Foster Kennedy syndrome can sometimes be the first set of signs and symptoms to prompt further investigations and examinations, which may lead to the diagnosis of a brain tumor. Clinicians should inform patients about the need for an interdisciplinary approach to effectively treat the disease and address quality-of-life, treatment, and prognostic issues.
Pearls and Other Issues
Foster Kennedy syndrome is an uncommon but important neuro-ophthalmic condition that should prompt urgent neuroimaging in any patient presenting with unilateral optic atrophy and contralateral papilledema. Clinicians should recognize that pseudo-FKS and atypical variants may mimic the classic presentation, making careful neurologic, ophthalmologic, and radiologic evaluation essential for accurate diagnosis.[4][23] Delayed recognition and treatment may result in irreversible visual loss, progressive neurologic deficits, and potentially life-threatening complications related to the underlying intracranial lesion.
Enhancing Healthcare Team Outcomes
Eye care professionals must be able to detect conditions such as optic atrophy and papilledema, because these may be the first signs of more severe disease. Clinicians who suspect FKS must immediately order detailed neuroimaging to localize the intracranial space-occupying lesion. The results of these scans can help neurosurgeons determine the most appropriate course of treatment. Although clinicians tend to prefer surgical intervention as first-line treatment, chemotherapy and radiotherapy have also shown promising results in some patients. As with all tumors, the risk of metastasis and multiple organ involvement is always possible. Patients with FKS must be appropriately counseled on treatment, treatment options, quality of life, the likely prognosis, and the risks of metastasis and mortality.
Interprofessional teamwork involves clinicians and nursing staff, and when medical treatment is part of the clinical picture, pharmacists are important in optimizing care for patients with FKS. All team members must be diligent in documenting their findings, monitoring patient progress, contributing from their area of expertise, and keeping all other interprofessional team members informed of any status changes so that corrective action can be implemented if necessary. This interprofessional approach can support the best possible outcomes.
Media
(Click Image to Enlarge)
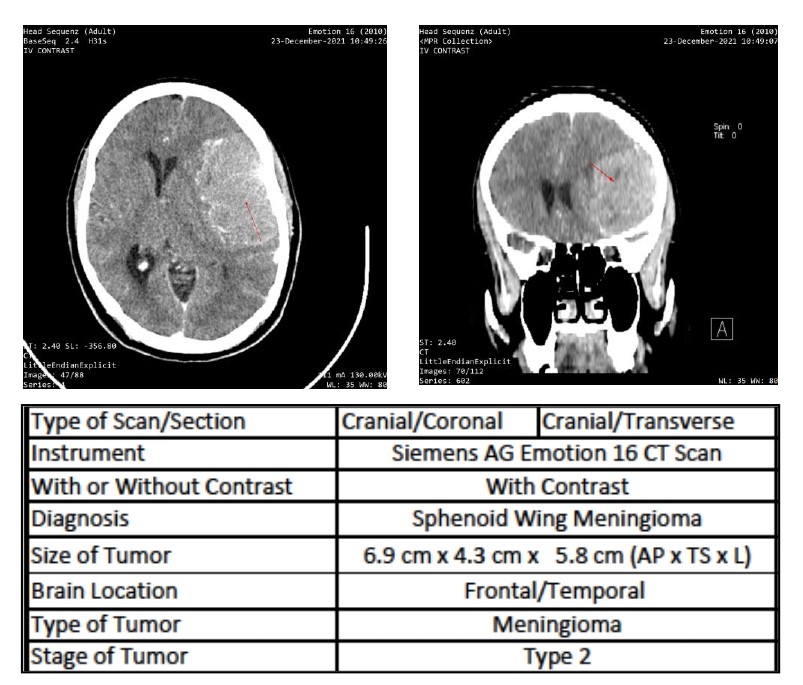
Contrast-Enhanced CT Imaging of Meningioma. Axial and coronal contrast-enhanced cranial CT scans demonstrate a large, hyperdense sphenoid wing meningioma involving the frontotemporal region, measuring approximately 6.9 x 4.3 x 5.8 cm, in a patient with Foster Kennedy syndrome.
Contributed by M Musa, OD
(Click Image to Enlarge)
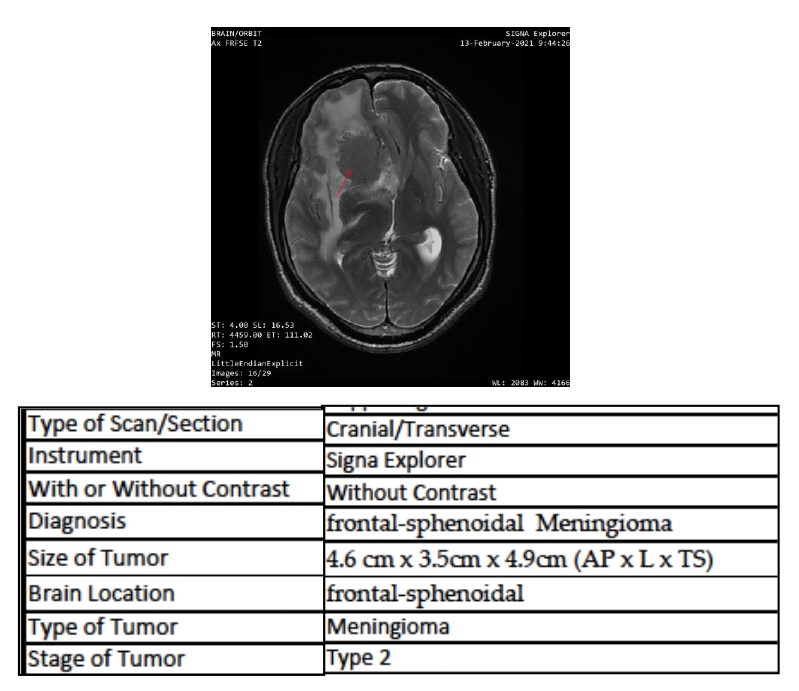
MRI of a Frontosphenoidal Meningioma in Foster Kennedy Syndrome. This axial T2-weighted MRI scan reveals a 4.6 x 3.5 x 4.9 cm right frontosphenoidal meningioma with significant surrounding vasogenic edema and associated midline shift in a patient with Foster Kennedy syndrome.
Contributed by M Musa, OD
References
Hata M, Miyamoto K. Causes and Prognosis of Unilateral and Bilateral Optic Disc Swelling. Neuro-ophthalmology (Aeolus Press). 2017 Aug:41(4):187-191. doi: 10.1080/01658107.2017.1299766. Epub 2017 Apr 10 [PubMed PMID: 29344057]
REED H. Primary optic atrophy in a tabetic African. East African medical journal. 1945 Oct:22():316-20 [PubMed PMID: 21016221]
LOEWENSTEIN A. Cavernous degeneration, necrosis and other regressive processes in optic nerve with vascular disease of the eye. Archives of ophthalmology (Chicago, Ill. : 1929). 1945 Sep:34():220-6 [PubMed PMID: 21004337]
Eidet JR, Biernat D, Dahlberg D, Wiedmann MKH, Jørstad ØK. [Foster Kennedy Syndrome]. Tidsskrift for den Norske laegeforening : tidsskrift for praktisk medicin, ny raekke. 2019 Jun 25:139(10):. doi: 10.4045/tidsskr.18.0719. Epub 2019 Jun 24 [PubMed PMID: 31238653]
Zehden J, Harish Bindiganavile S, Bhat N, Lee AG. Compressive Optic Disc Edema and Contralateral Papilledema: Type 2 Foster Kennedy Variant Syndrome. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2021 Jun 1:41(2):e217-e219. doi: 10.1097/WNO.0000000000001091. Epub [PubMed PMID: 33105415]
David C, Suvac E, Tăbăcaru B, Stanca TH. Pseudo-Foster Kennedy Syndrome - a case report. Romanian journal of ophthalmology. 2016 Oct-Dec:60(4):270-274 [PubMed PMID: 29450361]
Level 3 (low-level) evidenceNicula CA, Suluțiu O. Pseudo Foster-Kennedy Syndrome in an amblyopic patient: a case report. Romanian journal of ophthalmology. 2025 Apr-Jun:69(2):243-246. doi: 10.22336/rjo.2025.38. Epub [PubMed PMID: 40698102]
Level 3 (low-level) evidenceMicieli JA, Al-Obthani M, Sundaram AN. Pseudo-Foster Kennedy syndrome due to idiopathic intracranial hypertension. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 2014 Aug:49(4):e99-e102. doi: 10.1016/j.jcjo.2014.05.002. Epub 2014 Jul 16 [PubMed PMID: 25103671]
Level 3 (low-level) evidenceVisa Reñé N, Paredes Carmona F. Pseudo-Foster Kennedy syndrome due to idiopathic intracranial hypertension. Archivos de la Sociedad Espanola de Oftalmologia. 2019 Dec:94(12):598-601. doi: 10.1016/j.oftal.2019.09.006. Epub 2019 Oct 18 [PubMed PMID: 31635921]
Desai N, Yong RL, Doshi A, Rucker JC. Pseudo-Foster-Kennedy syndrome with optic nerve compression by the gyrus rectus. Neurology. 2015 Jul 28:85(4):385. doi: 10.1212/WNL.0000000000001791. Epub [PubMed PMID: 26215878]
Bansal S, Dabbs T, Long V. Pseudo-Foster Kennedy Syndrome due to unilateral optic nerve hypoplasia: a case report. Journal of medical case reports. 2008 Mar 18:2():86. doi: 10.1186/1752-1947-2-86. Epub 2008 Mar 18 [PubMed PMID: 18348732]
Level 3 (low-level) evidenceOgasawara C, Philbrick BD, Adamson DC. Meningioma: A Review of Epidemiology, Pathology, Diagnosis, Treatment, and Future Directions. Biomedicines. 2021 Mar 21:9(3):. doi: 10.3390/biomedicines9030319. Epub 2021 Mar 21 [PubMed PMID: 33801089]
Level 3 (low-level) evidenceBuerki RA, Horbinski CM, Kruser T, Horowitz PM, James CD, Lukas RV. An overview of meningiomas. Future oncology (London, England). 2018 Sep:14(21):2161-2177. doi: 10.2217/fon-2018-0006. Epub 2018 Aug 7 [PubMed PMID: 30084265]
Level 3 (low-level) evidenceZhang J, Sai K, Zhu ZQ, Lin FH, Wang ZF, Chen YM, Huang CY, Ye YL, Wang XL, Li YP, Sun SX, Zhong WY, Chen JB, Yang YQ. Prognostic factors for olfactory groove meningioma with nasal cavity extension. Oncotarget. 2018 Jan 12:9(4):4607-4613. doi: 10.18632/oncotarget.23461. Epub 2017 Dec 19 [PubMed PMID: 29435128]
Sun C, Dou Z, Wu J, Jiang B, Iranmanesh Y, Yu X, Li J, Zhou H, Zhong C, Peng Y, Zhuang J, Yu Q, Wu X, Yan F, Xie Q, Chen G. The Preferred Locations of Meningioma According to Different Biological Characteristics Based on Voxel-Wise Analysis. Frontiers in oncology. 2020:10():1412. doi: 10.3389/fonc.2020.01412. Epub 2020 Aug 21 [PubMed PMID: 32974148]
Ostrom QT, Cioffi G, Gittleman H, Patil N, Waite K, Kruchko C, Barnholtz-Sloan JS. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2012-2016. Neuro-oncology. 2019 Nov 1:21(Suppl 5):v1-v100. doi: 10.1093/neuonc/noz150. Epub [PubMed PMID: 31675094]
Pinzon RT, Afifudin M, Digdoyo A, Naibaho FKC, Parikesit PG, Allendio YS. Foster Kennedy Syndrome from Frontal Lobe Meningioma: A Rare Case Report. Romanian journal of ophthalmology. 2025 Apr-Jun:69(2):271-274. doi: 10.22336/rjo.2025.43. Epub [PubMed PMID: 40698105]
Level 3 (low-level) evidenceGatto F, Perez-Rivas LG, Olarescu NC, Khandeva P, Chachlaki K, Trivellin G, Gahete MD, Cuny T, on behalf of the ENEA Young Researchers Committee (EYRC). Diagnosis and Treatment of Parasellar Lesions. Neuroendocrinology. 2020:110(9-10):728-739. doi: 10.1159/000506905. Epub 2020 Mar 4 [PubMed PMID: 32126547]
Ayele B, Mengesha A, Wotiye A, Alemayehu Y. Giant Pituitary Adenoma Presenting with Foster-Kennedy Syndrome in a 21-Year Old Ethiopian Patient: A Rarely Reported Phenomenon: A Case Report. Ethiopian journal of health sciences. 2020 Mar:30(2):311-314. doi: 10.4314/ejhs.v30i2.19. Epub [PubMed PMID: 32165821]
Level 3 (low-level) evidenceSantoro A, Minniti G, Paolini S, Passacantilli E, Missori P, Frati A, Cantore GP. Atypical tentorial meningioma 30 years after radiotherapy for a pituitary adenoma. Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology. 2002 Mar:22(6):463-7 [PubMed PMID: 11976979]
Level 3 (low-level) evidenceShashidhar A, Arimappamagan A, Madhusudhan N, Narasinga Rao KVL, Bhat D, Shukla D, Arvinda HR, Srinivas D, Indira Devi B, Somanna S. Transcranial approach for pituitary adenomas - An evaluation of surgical approaches over two decades and factors influencing peri-operative morbidity. Clinical neurology and neurosurgery. 2021 Jan:200():106400. doi: 10.1016/j.clineuro.2020.106400. Epub 2020 Dec 5 [PubMed PMID: 33341089]
Wadud SA, Ahmed S, Choudhury N, Chowdhury D. Evaluation of ophthalmic manifestations in patients with intracranial tumours. Mymensingh medical journal : MMJ. 2014 Apr:23(2):268-71 [PubMed PMID: 24858153]
Level 2 (mid-level) evidenceHosny R. "Inverse" Foster Kennedy Syndrome: A Case Report. The neurologist. 2026 Mar 1:31(2):56-59. doi: 10.1097/NRL.0000000000000647. Epub 2026 Mar 1 [PubMed PMID: 41431965]
Level 3 (low-level) evidenceOsaguona VB, Kayoma DH. Etiology of Optic Disc Swelling in a Tertiary Care Center in Nigeria. Nigerian journal of clinical practice. 2020 Dec:23(12):1690-1694. doi: 10.4103/njcp.njcp_333_20. Epub [PubMed PMID: 33355822]
Sun T, Plutynski A, Ward S, Rubin JB. An integrative view on sex differences in brain tumors. Cellular and molecular life sciences : CMLS. 2015 Sep:72(17):3323-42. doi: 10.1007/s00018-015-1930-2. Epub 2015 May 19 [PubMed PMID: 25985759]
Pinzon RT, Veronica V. Foster Kennedy syndrome caused by tuberculous brain abscess: A case report. Journal of clinical tuberculosis and other mycobacterial diseases. 2021 Aug:24():100265. doi: 10.1016/j.jctube.2021.100265. Epub 2021 Jul 22 [PubMed PMID: 34368468]
Level 3 (low-level) evidencePastora-Salvador N, Peralta-Calvo J. Foster Kennedy syndrome: papilledema in one eye with optic atrophy in the other eye. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2011 Dec 13:183(18):2135. doi: 10.1503/cmaj.101937. Epub 2011 Sep 26 [PubMed PMID: 21948724]
Level 3 (low-level) evidenceChen WD, Wu YT, Chen NN, Chen CL. Classic Foster Kennedy Syndrome Triggered by Invasive Anaplastic Meningioma: Before and After. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2023 Dec 1:43(4):e346-e348. doi: 10.1097/WNO.0000000000001676. Epub 2022 Aug 2 [PubMed PMID: 35921252]
Minakaran N, de Carvalho ER, Petzold A, Wong SH. Optical coherence tomography (OCT) in neuro-ophthalmology. Eye (London, England). 2021 Jan:35(1):17-32. doi: 10.1038/s41433-020-01288-x. Epub 2020 Nov 25 [PubMed PMID: 33239763]
Cleaver J, Chohan G, James R, Giffin N. A patient with papilloedema. Practical neurology. 2021 Jun:21(3):249-254. doi: 10.1136/practneurol-2020-002563. Epub 2020 Oct 1 [PubMed PMID: 33004660]
Kotecha M, Gotecha S, Chugh A, Punia P. Neuroophthalmic Manifestations of Intracranial Tumours in Children. Case reports in ophthalmological medicine. 2021:2021():7793382. doi: 10.1155/2021/7793382. Epub 2021 May 15 [PubMed PMID: 34055437]
Level 3 (low-level) evidenceBrusini P, Salvetat ML, Zeppieri M. How to Measure Intraocular Pressure: An Updated Review of Various Tonometers. Journal of clinical medicine. 2021 Aug 27:10(17):. doi: 10.3390/jcm10173860. Epub 2021 Aug 27 [PubMed PMID: 34501306]
Li Z, Yang Y, Lu Y, Liu D, Xu E, Jia J, Yang D, Zhang X, Yang H, Ma D, Wang N. Intraocular pressure vs intracranial pressure in disease conditions: a prospective cohort study (Beijing iCOP study). BMC neurology. 2012 Aug 3:12():66 [PubMed PMID: 22862817]
Level 2 (mid-level) evidenceSolbak MS, Henning MK, England A, Martinsen AC, Aaløkken TM, Johansen S. Impact of iodine concentration and scan parameters on image quality, contrast enhancement and radiation dose in thoracic CT. European radiology experimental. 2020 Sep 11:4(1):57. doi: 10.1186/s41747-020-00184-z. Epub 2020 Sep 11 [PubMed PMID: 32915405]
Level 2 (mid-level) evidenceIyer VR, Ehman EC, Khandelwal A, Wells ML, Lee YS, Weber NM, Johnson MP, Yu L, McCollough CH, Fletcher JG. Image quality in abdominal CT using an iodine contrast reduction algorithm employing patient size and weight and low kV CT technique. Acta radiologica (Stockholm, Sweden : 1987). 2020 Sep:61(9):1186-1195. doi: 10.1177/0284185119898655. Epub 2020 Jan 27 [PubMed PMID: 31986894]
Level 2 (mid-level) evidenceSohn SY, Choi JH, Kim NK, Joung JY, Cho YY, Park SM, Kim TH, Jin SM, Bae JC, Lee SY, Chung JH, Kim SW. The impact of iodinated contrast agent administered during preoperative computed tomography scan on body iodine pool in patients with differentiated thyroid cancer preparing for radioactive iodine treatment. Thyroid : official journal of the American Thyroid Association. 2014 May:24(5):872-7. doi: 10.1089/thy.2013.0238. Epub 2014 Mar 6 [PubMed PMID: 24295076]
Level 2 (mid-level) evidenceHo JD, Tsang JF, Scoggan KA, Leslie WD. Urinary Iodine Clearance following Iodinated Contrast Administration: A Comparison of Euthyroid and Postthyroidectomy Subjects. Journal of thyroid research. 2014:2014():580569. doi: 10.1155/2014/580569. Epub 2014 Nov 12 [PubMed PMID: 25478285]
Power SP, Moloney F, Twomey M, James K, O'Connor OJ, Maher MM. Computed tomography and patient risk: Facts, perceptions and uncertainties. World journal of radiology. 2016 Dec 28:8(12):902-915. doi: 10.4329/wjr.v8.i12.902. Epub [PubMed PMID: 28070242]
Walter FM, Penfold C, Joannides A, Saji S, Johnson M, Watts C, Brodbelt A, Jenkinson MD, Price SJ, Hamilton W, Scott SE. Missed opportunities for diagnosing brain tumours in primary care: a qualitative study of patient experiences. The British journal of general practice : the journal of the Royal College of General Practitioners. 2019 Apr:69(681):e224-e235. doi: 10.3399/bjgp19X701861. Epub 2019 Mar 11 [PubMed PMID: 30858332]
Level 2 (mid-level) evidenceZienius K, Chak-Lam I, Park J, Ozawa M, Hamilton W, Weller D, Summers D, Porteous L, Mohiuddin S, Keeney E, Hollingworth W, Ben-Shlomo Y, Grant R, Brennan PM. Direct access CT for suspicion of brain tumour: an analysis of referral pathways in a population-based patient group. BMC family practice. 2019 Aug 20:20(1):118. doi: 10.1186/s12875-019-1003-y. Epub 2019 Aug 20 [PubMed PMID: 31431191]
Grover VP, Tognarelli JM, Crossey MM, Cox IJ, Taylor-Robinson SD, McPhail MJ. Magnetic Resonance Imaging: Principles and Techniques: Lessons for Clinicians. Journal of clinical and experimental hepatology. 2015 Sep:5(3):246-55. doi: 10.1016/j.jceh.2015.08.001. Epub 2015 Aug 20 [PubMed PMID: 26628842]
Frankel J, Wilén J, Hansson Mild K. Assessing Exposures to Magnetic Resonance Imaging's Complex Mixture of Magnetic Fields for In Vivo, In Vitro, and Epidemiologic Studies of Health Effects for Staff and Patients. Frontiers in public health. 2018:6():66. doi: 10.3389/fpubh.2018.00066. Epub 2018 Mar 12 [PubMed PMID: 29594090]
Cooley CZ, Stockmann JP, Armstrong BD, Sarracanie M, Lev MH, Rosen MS, Wald LL. Two-dimensional imaging in a lightweight portable MRI scanner without gradient coils. Magnetic resonance in medicine. 2015 Feb:73(2):872-83. doi: 10.1002/mrm.25147. Epub 2014 Mar 25 [PubMed PMID: 24668520]
Abd-Ellah MK, Awad AI, Khalaf AAM, Hamed HFA. A review on brain tumor diagnosis from MRI images: Practical implications, key achievements, and lessons learned. Magnetic resonance imaging. 2019 Sep:61():300-318. doi: 10.1016/j.mri.2019.05.028. Epub 2019 Jun 5 [PubMed PMID: 31173851]
Booth TC, Wiegers EC, Warnert EAH, Schmainda KM, Riemer F, Nechifor RE, Keil VC, Hangel G, Figueiredo P, Álvarez-Torres MDM, Henriksen OM. High-Grade Glioma Treatment Response Monitoring Biomarkers: A Position Statement on the Evidence Supporting the Use of Advanced MRI Techniques in the Clinic, and the Latest Bench-to-Bedside Developments. Part 2: Spectroscopy, Chemical Exchange Saturation, Multiparametric Imaging, and Radiomics. Frontiers in oncology. 2021:11():811425. doi: 10.3389/fonc.2021.811425. Epub 2022 Feb 28 [PubMed PMID: 35340697]
Durand-Dubief F, Shor N, Audoin B, Bourre B, Cohen M, Kremer S, Maillart E, Papeix C, Ruet A, Savatovsky J, Tourdias T, Ayrignac X, Ciron J, Collongues N, Laplaud D, Michel L, Deschamps R, Thouvenot E, Zephir H, Marignier R, Cotton F, NOMADMUS Study Group. MRI management of NMOSD and MOGAD: Proposals from the French Expert Group NOMADMUS. Journal of neuroradiology = Journal de neuroradiologie. 2025 Feb:52(1):101235. doi: 10.1016/j.neurad.2024.101235. Epub 2024 Dec 1 [PubMed PMID: 39626832]
Goh KG, Yusof Khan AHK, Nasruddin A. Stiff Person-Like Syndrome: An Unusual Presentation of Pituitary Macroadenoma with Panhypopituitarism. Case reports in neurology. 2022 Jan-Apr:14(1):157-161. doi: 10.1159/000522253. Epub 2022 Mar 18 [PubMed PMID: 35530378]
Level 3 (low-level) evidenceShapira Y, Juniat V, Dave T, Hussain A, McNeely D, Watanabe A, Yoneda A, Saeed P, Woo KI, Hardy TG, Price B, Drummond K, Selva D. Orbito-cranial schwannoma-a multicentre experience. Eye (London, England). 2023 Jan:37(1):48-53. doi: 10.1038/s41433-021-01850-1. Epub 2022 Jan 9 [PubMed PMID: 34999720]
Ungureanu G, Serban LN, Florian SI. Optimizing Surgical Management of Anterior Skull Base Meningiomas: Imaging Modalities, Key Surgical Considerations, and Risk Mitigation Strategies. Cancers. 2025 Mar 14:17(6):. doi: 10.3390/cancers17060987. Epub 2025 Mar 14 [PubMed PMID: 40149321]
Qasem LE, Al-Hilou A, Oros J, Weber KJ, Keil F, Jussen D, Prinz V, Seifert V, Baumgarten P, Marquardt G, Czabanka M. Single-stage versus two-stage resection for large anterior midline skull base meningiomas with bihemispheric peritumoral edema. Scientific reports. 2025 Mar 7:15(1):7926. doi: 10.1038/s41598-025-92516-5. Epub 2025 Mar 7 [PubMed PMID: 40050641]
Yuen CA, Zheng M, Saint-Germain MA, Kamson DO. Meningioma: Novel Diagnostic and Therapeutic Approaches. Biomedicines. 2025 Mar 7:13(3):. doi: 10.3390/biomedicines13030659. Epub 2025 Mar 7 [PubMed PMID: 40149634]
Nguyen DC, Nader C, Bélanger K, Lapointe S, Lemieux B, Lemieux-Blanchard É, Bahary JP, Masucci L, Lambert C, Roberge D, Moumdjian R, Labidi M, Cayrol R, Florescu M. A Retrospective Study on Prognostic Factors and Systemic Treatments of Refractory Meningiomas. Current oncology (Toronto, Ont.). 2025 Sep 16:32(9):. doi: 10.3390/curroncol32090516. Epub 2025 Sep 16 [PubMed PMID: 41002586]
Level 2 (mid-level) evidenceMensah EO, Ghosh A, Rane A, Kim J, Bhatt PB, Alalade AF. Systemic therapy in the treatment of recurrent or refractory intracranial meningiomas: A systematic review and individual patient data meta-analysis. Neurosurgical review. 2026 Apr 16:49(1):. doi: 10.1007/s10143-026-04233-w. Epub 2026 Apr 16 [PubMed PMID: 41989655]
Level 1 (high-level) evidenceKosanam AR, Ma J, White AJ, Murayi R, Soni P, Recinos PF, Kshettry VR. Comparison of adjuvant radiation versus observation and salvage radiation after subtotal resection of a WHO grade I skull base meningioma: a propensity score-adjusted analysis. Journal of neuro-oncology. 2025 Jun:173(2):297-304. doi: 10.1007/s11060-025-04980-8. Epub 2025 Feb 25 [PubMed PMID: 39998721]
Mizutani Y, Hori YS, Harary PM, Lam FC, Reesh DA, Emrich SC, Ustrzynski L, Tayag A, Park DJ, Chang SD. Stereotactic Radiosurgery for Recurrent Meningioma: A Systematic Review of Risk Factors and Management Approaches. Cancers. 2025 Aug 23:17(17):. doi: 10.3390/cancers17172750. Epub 2025 Aug 23 [PubMed PMID: 40940847]
Level 1 (high-level) evidenceHajikarimloo B, Tos SM, Mohammadzadeh I, Shahabi K, Amjadzadeh M, Golkar Z, Alvani MS, Habibi MA. Stereotactic radiosurgery for optic nerve sheath meningiomas: A comprehensive systematic review and meta-analysis. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2025 Sep:139():111432. doi: 10.1016/j.jocn.2025.111432. Epub 2025 Jun 27 [PubMed PMID: 40580760]
Level 1 (high-level) evidenceRodríguez-Porcel F, Hughes I, Anderson D, Lee J, Biller J. Foster Kennedy Syndrome Due to Meningioma Growth during Pregnancy. Frontiers in neurology. 2013:4():183. doi: 10.3389/fneur.2013.00183. Epub 2013 Nov 11 [PubMed PMID: 24273529]
Bouffet E, Jouvet A, Thiesse P, Sindou M. Chemotherapy for aggressive or anaplastic high grade oligodendrogliomas and oligoastrocytomas: better than a salvage treatment. British journal of neurosurgery. 1998 Jun:12(3):217-22 [PubMed PMID: 11013683]
Armstrong TS, Ying Y, Wu J, Acquaye AA, Vera-Bolanos E, Gilbert MR, Brown PD, Vardy J, Chung C. The relationship between corticosteroids and symptoms in patients with primary brain tumors: utility of the Dexamethasone Symptom Questionnaire-Chronic. Neuro-oncology. 2015 Aug:17(8):1114-20. doi: 10.1093/neuonc/nov054. Epub 2015 Apr 9 [PubMed PMID: 25862766]
Schrell UM, Rittig MG, Anders M, Kiesewetter F, Marschalek R, Koch UH, Fahlbusch R. Hydroxyurea for treatment of unresectable and recurrent meningiomas. I. Inhibition of primary human meningioma cells in culture and in meningioma transplants by induction of the apoptotic pathway. Journal of neurosurgery. 1997 May:86(5):845-52 [PubMed PMID: 9126901]
Level 3 (low-level) evidenceLiu B, Yu Y, Liu W, Deng T, Xiang D. Risk Factors for Non-arteritic Anterior Ischemic Optic Neuropathy: A Large Scale Meta-Analysis. Frontiers in medicine. 2021:8():618353. doi: 10.3389/fmed.2021.618353. Epub 2021 Oct 4 [PubMed PMID: 34671609]
Level 1 (high-level) evidenceXie JS, Donaldson L, Margolin E. Papilledema: A review of etiology, pathophysiology, diagnosis, and management. Survey of ophthalmology. 2022 Jul-Aug:67(4):1135-1159. doi: 10.1016/j.survophthal.2021.11.007. Epub 2021 Nov 20 [PubMed PMID: 34813854]
Level 3 (low-level) evidenceFriedman DI. The Pseudotumor Cerebri Syndrome. Neurologic clinics. 2024 May:42(2):433-471. doi: 10.1016/j.ncl.2024.02.001. Epub [PubMed PMID: 38575259]
Jauregui R, Busis NA. Idiopathic Intracranial Hypertension. The New England journal of medicine. 2023 Dec 28:389(26):2467. doi: 10.1056/NEJMicm2308721. Epub [PubMed PMID: 38157502]
Petramfar P, Hosseinzadeh F, Mohammadi SS. Pseudo-Foster Kennedy Syndrome as a Rare Presentation of Vitamin B12 Deficiency. Iranian Red Crescent medical journal. 2016 Jun:18(6):e24610. doi: 10.5812/ircmj.24610. Epub 2016 May 14 [PubMed PMID: 27621919]
Hussein MR, Baidas S. Advances in diagnosis and management of oligodendroglioma. Expert review of anticancer therapy. 2002 Oct:2(5):520-8 [PubMed PMID: 12382520]
Level 3 (low-level) evidenceYeh SA, Lee TC, Chen HJ, Lui CC, Sun LM, Wang CJ, Huang EY. Treatment outcomes and prognostic factors of patients with supratentorial low-grade oligodendroglioma. International journal of radiation oncology, biology, physics. 2002 Dec 1:54(5):1405-9 [PubMed PMID: 12459363]
Level 2 (mid-level) evidenceVaquero J, Zurita M, Morales C, Coca S. Prognostic significance of tumor-enhancement and angiogenesis in oligodendroglioma. Acta neurologica Scandinavica. 2002 Jul:106(1):19-23 [PubMed PMID: 12067323]