Introduction
A gastric point-of-care ultrasonography examination is performed to evaluate gastric contents before induction of anesthesia. Aspiration of gastric contents occurs in approximately 1 in every 900 surgical procedures using general anesthesia and accounts for significant perioperative morbidity and an inpatient mortality incidence of 20%.[1] Aspiration can lead to hypoxia, bronchospasm, pneumonitis, pneumonia, acute respiratory distress syndrome, and death. As a result, aspiration pneumonia among surgical patients is associated with a 4-fold increased risk of intensive care unit admission, a 9-day increase in length of stay, and a 7.6-fold increased risk of in-hospital mortality.[2]
Food or liquids in the stomach before anesthesia induction are among the greatest risk factors for perioperative pulmonary aspiration.[3][4][5] Conversely, fasting before planned procedures can reduce the risk of gastric aspiration. The American Society for Anesthesiologists Practice Guidelines for Preoperative Fasting are intended to reduce the risk of gastric aspiration, and recommend that healthy patients fast for at least 2 hours for clear liquids, 4 hours for human breast milk, 6 hours for nonhuman milk, infant formula, or light meals, and 8 hours for fried foods, fatty foods, and meat.[6][7] Anesthesia societies in Canada, Brazil, Europe, India, Australia, and New Zealand have recommended time frames that differ slightly from those published by the American Society for Anesthesiologists and address other preanesthesia dietary factors, such as carbohydrate-rich beverages and gum chewing.[8] However, clear guidance is lacking on appropriate fasting periods for patients at increased risk of delayed gastric emptying or pulmonary aspiration (see Indications below).
Gastric POCUS is a simple, fast, noninvasive bedside diagnostic test that provides a qualitative and quantitative assessment of gastric contents.[3][9] This examination allows anesthesia clinicians to differentiate between a full and an empty stomach, determine the consistency of gastric contents (solids, thick liquids, clear liquids), and estimate the volume of gastric fluid (See Image. Gastric Ultrasound, Assessment of Gastric Contents). Gastric content assessment helps determine the most appropriate timing for elective procedures, anesthetic choice, and airway management approach.[10]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Mastery of gastric POCUS requires knowledge of the anatomy of the stomach and nearby organs (see Image. Gastric Ultrasound, Anatomy). The stomach is a J-shaped organ divided into 4 named regions: the cardia, fundus, body, and pylorus (see Image. Diagram of the Stomach). The cardia is the region immediately distal to the esophagus. The fundus is the most cephalad portion of the stomach, lying above the cardiac notch. The body is the largest part of the stomach, providing space for food to mix with digestive enzymes. The funnel-shaped pylorus is the distal portion of the stomach, consisting of the antrum and the pyloric sphincter. The antrum lies between the gastric body and the pyloric sphincter, storing food before release through the pyloric sphincter into the duodenum. The antrum is the most important anatomical structure to visualize when performing gastric POCUS.[11]
The stomach wall consists of 3 layers of alternating echogenicity that are frequently distinguishable on ultrasonography. The outermost layer is the serosa, which appears as a thin hyperechoic line. The muscularis propria, immediately deep to the serosa, appears as a thick, hypoechoic line and is easy to see on ultrasonography (see Image. Gastric Ultrasonography, Hypoechoic Muscular Layer of the Stomach). The mucosa is the innermost layer of the stomach, which appears as a thin hyperechoic line. Occasionally, 5 layers of alternating echogenicity can be appreciated. The 2 innermost layers are considered artifactual due to the interface between the mucosal layer and the gastric lumen fluid.[12]
Gastric POCUS is performed in the parasagittal imaging plane; therefore, understanding the relationships of adjacent organs to the stomach in this plane is crucial. The liver is easily recognizable because of its large size and highly vascular appearance. The liver should be located on the left of the screen (cephalad). The pancreas is located posterior to the stomach and appears hyperechoic. The bowel is difficult to visualize on ultrasonography due to gas in the lumen, but it is generally located on the right side of the screen (caudad to the stomach).[13]
During gastric POCUS, several major blood vessels, including the aorta, the superior mesenteric artery (SMA), and the inferior vena cava (IVC), can be visualized. All appear anechoic (black) because they are filled with blood. The pulsatile SMA is the most superficial, located posterior to the stomach but anterior to the aorta. The aorta and IVC can be challenging to distinguish because both are large and located at similar depths. In the parasagittal plane, only one should be visible at a time because they run parallel to one another. Conversely, the aorta has a thick wall, is pulsatile, and usually has a smaller diameter than the IVC. The IVC has a thin, often compressible wall, and its diameter changes with the respiratory cycle, decreasing during inspiration and increasing during expiration. The aorta is anterior to the vertebral bodies and to the left of the midline, whereas the IVC is at a similar depth but to the right.[6]
Indications
Gastric POCUS provides a qualitative and quantitative assessment of gastric contents. This examination is most useful when fasting status is uncertain or when physiologic states associated with delayed gastric emptying are present.[14] Information obtained from gastric ultrasonography is used by anesthesia clinicians to determine whether elective surgical procedures should be postponed and to select the optimal induction and airway treatment technique for urgent or emergent procedures.[15]
Uncertain Fasting Status
Uncertain fasting status may be present in patients with unclear histories, cognitive dysfunction, dementia, language barriers, or who cannot reliably follow fasting instructions. Patients at increased risk of delayed gastric emptying or pulmonary aspiration include those with the following conditions:
- Acute pain
- Gastroparesis [16]
- Diabetes mellitus
- Gastroesophageal reflux disease
- Chronic kidney disease
- Obesity [16]
- Pregnancy [16]
- Cannabis use, a risk factor for delayed gastric emptying, cyclical vomiting, and hyperemesis, and its interactions with many other drugs [17]
- Recent use of a glucagon-like peptide-1 receptor agonist (which can delay gastric emptying)[18]
- Opioid use [Best Practice & Research Clinical Anaesthesiology. Point-of-care gastric ultrasound: Redefining aspiration risk assessment in anesthesia]
Contraindications
Absolute contraindications to gastric POCUS have not been identified. Relative contraindications include abdominal wounds and epigastric bandages. Patients who cannot be safely positioned in the right lateral decubitus position should not undergo gastric POCUS.
Equipment
Virtually any diagnostic ultrasonography machine can be used to perform gastric POCUS. Ideally, the machine should be able to measure the cross-sectional area.[19] When available, abdominal imaging settings should be selected. An appropriate imaging depth should be chosen to visualize the abdominal aorta. A low-frequency (2-5 MHz) curvilinear transducer is suitable for most patients. A higher-frequency (5-13 MHz) linear transducer may be suitable for small children, although care should be taken to ensure sufficient penetration to image the abdominal aorta.
Personnel
A single, qualified clinician or technician can perform the examination, and a trained clinician can interpret the findings. However, additional help may be required to properly position small children or patients who are unable to cooperate, immobile, or sedated.
Preparation
The purpose of the examination should be explained to the patient before the examination begins. The epigastrium should be exposed, with the patient's chest and pelvic region covered. Clean towels should protect the patient's gown, clothing, and sheets from soiling with the gel. The ultrasonography machine should be positioned so the screen is visible during the examination. Ideally, the examiner should stand on the patient's right side, with the ultrasonography machine opposite the examiner on the patient's left side.
Technique or Treatment
All imaging is performed in the parasagittal plane. The curvilinear transducer should be held in the epigastrium so the orientation marker points toward the head (cephalad). If necessary, the screen should be adjusted to display the orientation marker and cephalad structures on the left. The liver is easily recognized as the cephalad structure on the left of the screen. With the patient supine, the epigastrium should be exposed. The cephalad tip of the transducer should be positioned immediately inferior to the xiphoid process. Correct transducer orientation can be confirmed once the liver is identified.
The inferior vena cava and abdominal aorta must be identified, and the image depth should be adjusted so that the posterior vessel border or vertebral bodies are visible at the bottom of the screen. Required depth varies significantly depending on the patient's body habitus. The abdomen is scanned by sweeping the transducer laterally from left to right, keeping it perpendicular to the skin. The stomach, liver, pancreas, SMA, aorta, and IVC should be identified. The stomach should be examined to observe the characteristics of any gastric contents, noting the presence of solids, thick liquids, or clear fluids.[6]
The supine gastric examination is qualitative only and must be accompanied by examination in the right lateral decubitus position. A full stomach containing solids or thick liquids can be confirmed in the supine position, but a full stomach cannot be excluded. Moreover, gastric volume assessment cannot be performed accurately while the patient is supine. After completing the examination in the supine position, the clinician should place the patient in the right lateral decubitus position. This position facilitates the gravitational flow of gastric contents to the antrum, increasing the sensitivity of the examination and facilitating gastric volume measurement. With the patient in the right lateral decubitus position, the abdomen should be scanned to identify the previously discussed anatomic structures. Occasionally, image depth must be increased to obtain adequate views of the great vessels of the abdomen. The contents of the stomach must be assessed, again noting thick liquids or solids.[20][21]
- Solids: Solids have a heterogeneous, frosted glass appearance on ultrasonography. Structures located posterior to solid food (eg, aorta) may not be visible because of poor penetration of ultrasound waves beyond solid food.
- Thick liquids: Thick liquids (eg, yogurt) appear hyperechoic and homogeneous on gastric ultrasonography.
- Clear liquids: Clear fluids appear hypoechoic (black) and homogeneous. If the fluid was recently ingested, air bubbles (hyperechoic) may be present, giving it a starry-night appearance. Clear liquids in the stomach should be measured by measuring the antral cross-sectional area (CSA) in the right lateral decubitus position and calculating the estimated gastric volume.
- Empty: The empty stomach has a bulls-eye appearance, with a small or collapsed antrum surrounded by the sonographically distinct layers of the stomach wall. A small volume of clear liquid, representing baseline gastric secretions, often exists within a physiologically empty stomach.[3][9]
If the stomach contains only clear liquids, the volume can be estimated by measuring the antral CSA at the level of the aorta. Measurements must be taken at the level of the aorta rather than the IVC. Because of the funnel-shaped antrum, measurements at the level of the IVC underestimate gastric volume, leading to false-negative results for the presence of gastric contents.[22] The estimated gastric volume is calculated with the equation:
Stomach Contents Volume (in mL) = 27 + (14.6 x CSA) – (1.28 x Age),
For example, a 20-year-old, 80 kg patient with a CSA of 20 cm² would have an estimated gastric volume of 27 + (14.6 × 20) − (1.28 × 20) = 293 mL. A gastric volume-to-body weight ratio of 1.5 mL/kg or less is considered normal, consistent with baseline secretions, and associated with a low risk of aspiration under anesthesia.[23] A ratio greater than 1.5 mL/kg predicts a high risk of aspiration. For the patient in the example, the volume of gastric contents is 293 ÷ 80, or 3.7 mL/kg, signifying a full stomach. Results from a recent study confirmed these ratios in patients with gastric cancer who often have delayed gastric emptying. Gastric POCUS was performed before planned gastrectomy.[24] Results from one study found a consistent relationship between antral CSA and aspirated fluid volume after endotracheal intubation. A sensitivity of 91% and a specificity of 71% were observed when the cutoff value for antral CSA was 340 mm² for the diagnosis of a high-risk stomach.[23]
Clinical Significance
The clinical significance of gastric ultrasound depends on the urgency of surgery. For elective procedures, cases should be canceled or postponed if the stomach contains solids, thick liquids, or a volume of clear fluids exceeding 1.5 mL/kg.[23] In emergency procedures or when gastric emptying is unpredictable or may not improve over time (eg, gastroparesis), the risk of aspiration and the optimal timing of the case should be discussed with the patient and proceduralist. The anesthetic plan should include full aspiration precautions if the case must proceed. Options include reduced or no sedation to preserve airway-protective reflexes, or, if sedation is required, ideally, airway protection with a rapid-sequence induction and endotracheal intubation. Depending on the circumstances, the stomach can be decompressed with a nasogastric or orogastric tube either before induction of anesthesia or following intubation.[9]
Enhancing Healthcare Team Outcomes
Gastric POCUS is a useful diagnostic examination because it can reduce the risk of pulmonary aspiration of gastric contents. However, risk reduction requires effective communication and collaboration between all clinical members of each patient's care team. Surgical schedulers must ensure that patients receive instructions regarding appropriate fasting before surgery. On the day of a procedure, preoperative nurses should assess fasting status during the preoperative interview. The responsible clinician should ensure appropriate diet orders are placed the evening before a scheduled surgery for surgical inpatients. The anesthesiologist or nurse anesthetist is ultimately responsible for performing the final assessment and determining the most appropriate method for reducing the risk of aspiration. However, gastric POCUS can be performed and interpreted by any qualified clinician.
Media
(Click Image to Enlarge)
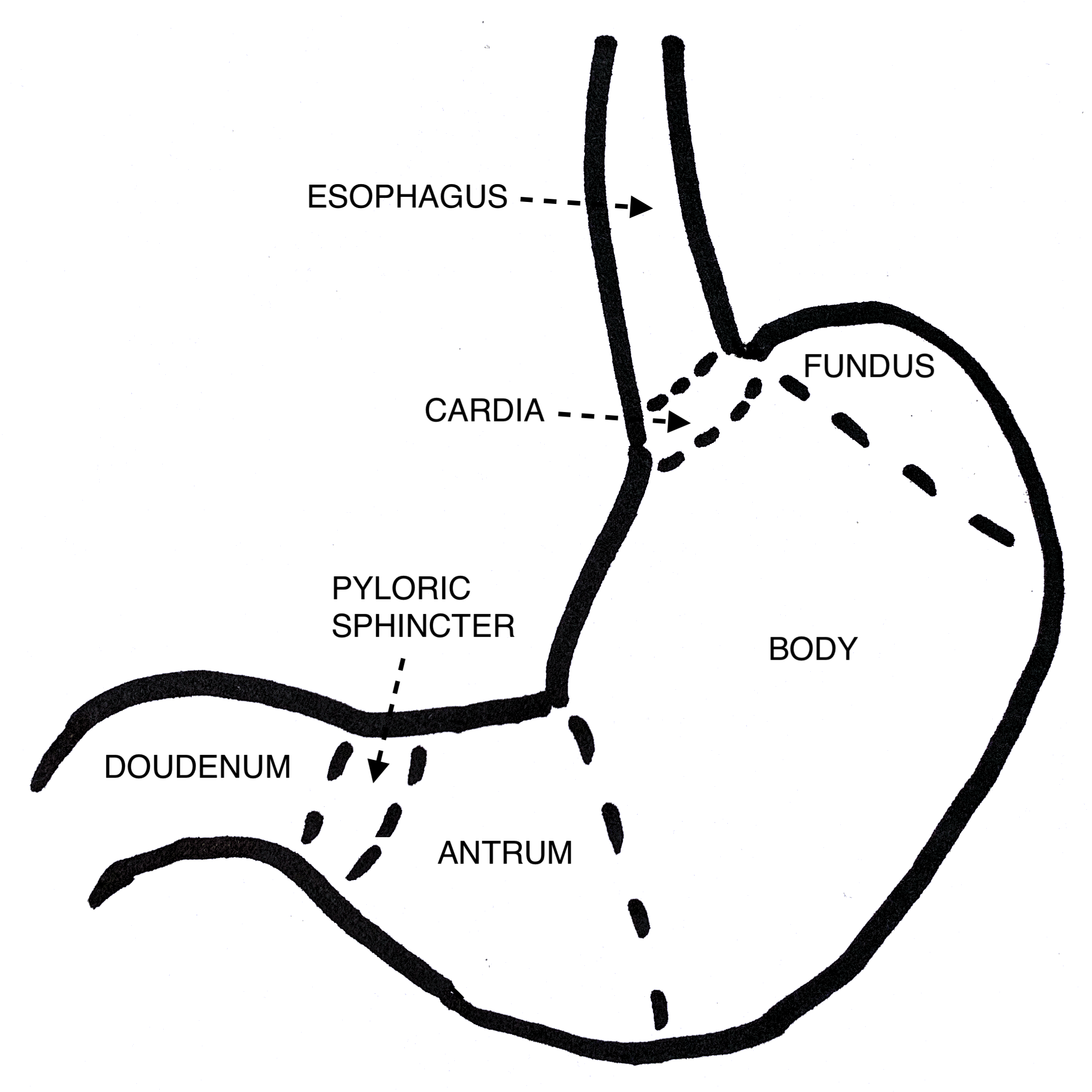
Diagram of the Stomach. The diagram illustrates the cardia, fundus, body, antrum, and pyloric sphincter.
Contributed by DN Flynn, MD
(Click Image to Enlarge)
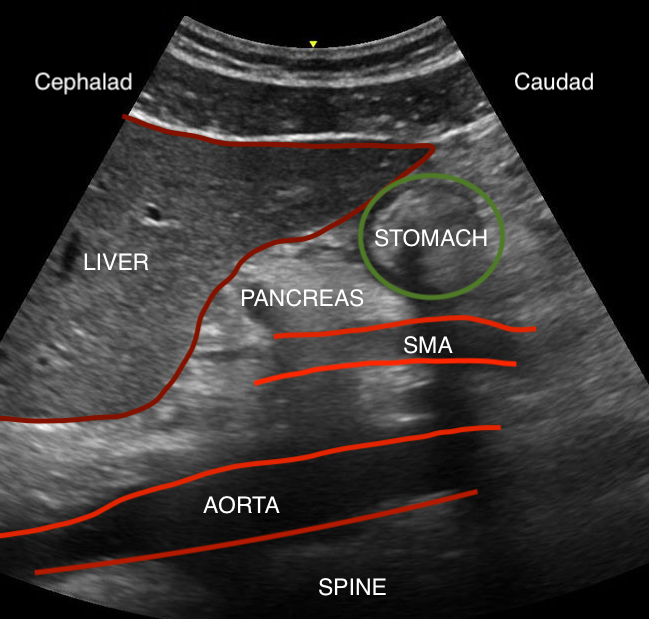
Gastric Ultrasound, Anatomy. The ultrasound image includes the liver, pancreas, stomach, superior mesenteric artery, aorta, and spine.
Contributed by DN Flynn, MD
(Click Image to Enlarge)
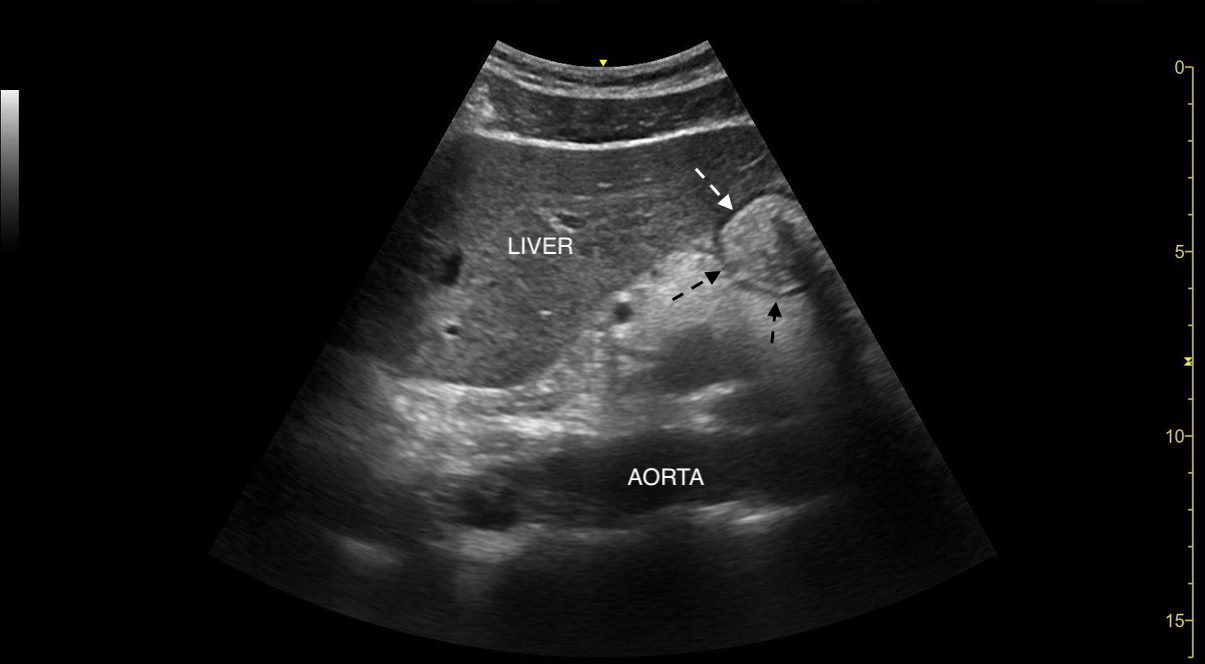
Gastric Ultrasound, Hypoechoic Muscular Layer of the Stomach. The ultrasound image highlights the hypoechoic muscular layer of the stomach.
Contributed by DN Flynn, MD
(Click Image to Enlarge)
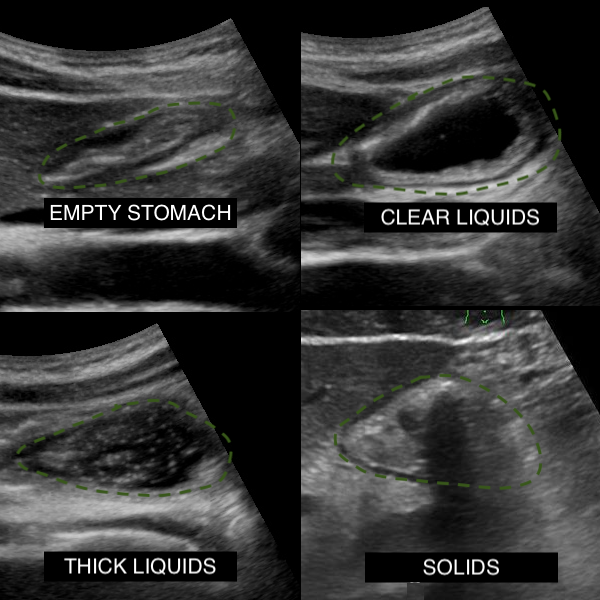
Gastric Ultrasound, Assessment of Gastric Contents. This image is a sonographic appearance of an empty stomach, clear liquids, thick liquids, and solids.
Contributed by J Schoenherr, MD, and DN Flynn, MD
References
El-Boghdadly K, Wojcikiewicz T, Perlas A. Perioperative point-of-care gastric ultrasound. BJA education. 2019 Jul:19(7):219-226. doi: 10.1016/j.bjae.2019.03.003. Epub 2019 Apr 24 [PubMed PMID: 33456894]
Kozlow JH, Berenholtz SM, Garrett E, Dorman T, Pronovost PJ. Epidemiology and impact of aspiration pneumonia in patients undergoing surgery in Maryland, 1999-2000. Critical care medicine. 2003 Jul:31(7):1930-7 [PubMed PMID: 12847385]
Level 2 (mid-level) evidencePerlas A, Arzola C, Van de Putte P. Point-of-care gastric ultrasound and aspiration risk assessment: a narrative review. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 2018 Apr:65(4):437-448. doi: 10.1007/s12630-017-1031-9. Epub 2017 Dec 11 [PubMed PMID: 29230709]
Level 3 (low-level) evidenceLeviter J, Steele DW, Constantine E, Linakis JG, Amanullah S. "Full Stomach" Despite the Wait: Point-of-care Gastric Ultrasound at the Time of Procedural Sedation in the Pediatric Emergency Department. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2019 Jul:26(7):752-760. doi: 10.1111/acem.13651. Epub 2018 Dec 7 [PubMed PMID: 30372569]
Falyar CR, Kantzavelos L. Clinical Application of Point-of-Care Ultrasound Gastric Examination in the Management of an ASA Class 3E Patient: A Case Report. AANA journal. 2018 Oct:86(5):379-382 [PubMed PMID: 31584407]
Level 3 (low-level) evidence. Practice Guidelines for Preoperative Fasting and the Use of Pharmacologic Agents to Reduce the Risk of Pulmonary Aspiration: Application to Healthy Patients Undergoing Elective Procedures: An Updated Report by the American Society of Anesthesiologists Task Force on Preoperative Fasting and the Use of Pharmacologic Agents to Reduce the Risk of Pulmonary Aspiration. Anesthesiology. 2017 Mar:126(3):376-393. doi: 10.1097/ALN.0000000000001452. Epub [PubMed PMID: 28045707]
Level 1 (high-level) evidenceMiller AF, Levy JA, Krauss BS, Gravel CA, Vieira RL, Neuman MI, Monuteaux MC, Rempell RG. Does Point-of-Care Gastric Ultrasound Correlate With Reported Fasting Time? Pediatric emergency care. 2021 Dec 1:37(12):e1265-e1269. doi: 10.1097/PEC.0000000000001997. Epub [PubMed PMID: 31913246]
Razak A, Baburyan S, Lee E, Costa A, Bergese SD. Role of Point-of-Care Gastric Ultrasound in Advancing Perioperative Fasting Guidelines. Diagnostics (Basel, Switzerland). 2024 Oct 23:14(21):. doi: 10.3390/diagnostics14212366. Epub 2024 Oct 23 [PubMed PMID: 39518332]
Haskins SC, Kruisselbrink R, Boublik J, Wu CL, Perlas A. Gastric Ultrasound for the Regional Anesthesiologist and Pain Specialist. Regional anesthesia and pain medicine. 2018 Oct:43(7):689-698. doi: 10.1097/AAP.0000000000000846. Epub [PubMed PMID: 30052550]
Delamarre L, Srairi M, Bouvet L, Conil JM, Fourcade O, Minville V. Anaesthesiologists' clinical judgment accuracy regarding preoperative full stomach: Diagnostic study in urgent surgical adult patients. Anaesthesia, critical care & pain medicine. 2021 Jun:40(3):100836. doi: 10.1016/j.accpm.2021.100836. Epub 2021 Mar 19 [PubMed PMID: 33753294]
Soybel DI. Anatomy and physiology of the stomach. The Surgical clinics of North America. 2005 Oct:85(5):875-94, v [PubMed PMID: 16139026]
Lim JH, Jeong YM. Sonography of the stomach: an in vitro study to determine the anatomic cause of inner hyperechoic and hypoechoic layers of the gastric wall. AJR. American journal of roentgenology. 1994 Feb:162(2):335-8 [PubMed PMID: 8310921]
Moake MM, Jackson BF, Presley BC. Point-of-Care Ultrasound to Assess Gastric Content. Pediatric emergency care. 2020 Aug:36(8):404-410. doi: 10.1097/PEC.0000000000001939. Epub [PubMed PMID: 31738302]
Li L, Yong RJ, Kaye AD, Urman RD. Perioperative Point of Care Ultrasound (POCUS) for Anesthesiologists: an Overview. Current pain and headache reports. 2020 Mar 21:24(5):20. doi: 10.1007/s11916-020-0847-0. Epub 2020 Mar 21 [PubMed PMID: 32200432]
Level 3 (low-level) evidenceNaji A, Chappidi M, Ahmed A, Monga A, Sanders J. Perioperative Point-of-Care Ultrasound Use by Anesthesiologists. Cureus. 2021 May 24:13(5):e15217. doi: 10.7759/cureus.15217. Epub 2021 May 24 [PubMed PMID: 34178536]
Camilleri M, Chedid V, Ford AC, Haruma K, Horowitz M, Jones KL, Low PA, Park SY, Parkman HP, Stanghellini V. Gastroparesis. Nature reviews. Disease primers. 2018 Nov 1:4(1):41. doi: 10.1038/s41572-018-0038-z. Epub 2018 Nov 1 [PubMed PMID: 30385743]
Cammarano CA, Villaluz JE. A Reason to Rethink Fasting Guidelines? Marijuana-Induced Gastroparesis and the Implications for Aspiration Risk in the Nil Per Os (NPO) Patient: A Case Report. The American journal of case reports. 2021 Nov 29:22():e934187. doi: 10.12659/AJCR.934187. Epub 2021 Nov 29 [PubMed PMID: 34840324]
Level 3 (low-level) evidenceSilveira SQ, da Silva LM, de Campos Vieira Abib A, de Moura DTH, de Moura EGH, Santos LB, Ho AM, Nersessian RSF, Lima FLM, Silva MV, Mizubuti GB. Relationship between perioperative semaglutide use and residual gastric content: A retrospective analysis of patients undergoing elective upper endoscopy. Journal of clinical anesthesia. 2023 Aug:87():111091. doi: 10.1016/j.jclinane.2023.111091. Epub 2023 Mar 2 [PubMed PMID: 36870274]
Level 2 (mid-level) evidenceBouvet L, Mazoit JX, Chassard D, Allaouchiche B, Boselli E, Benhamou D. Clinical assessment of the ultrasonographic measurement of antral area for estimating preoperative gastric content and volume. Anesthesiology. 2011 May:114(5):1086-92. doi: 10.1097/ALN.0b013e31820dee48. Epub [PubMed PMID: 21364462]
Bronshteyn YS, Anderson TA, Badakhsh O, Boublik J, Brady MBW, Charnin JE, Coker BJ, Deriy LB, Hardman HD, Haskins SC, Hollon M, Hsia HJ, Neelankavil JP, Panzer OPF, Perlas A, Ramsingh D, Sharma A, Shore-Lesserson LJ, Zimmerman JM, American Society of Anesthesiologists Ad Hoc Committee on PoCUS. Diagnostic Point-of-Care Ultrasound: Recommendations From an Expert Panel. Journal of cardiothoracic and vascular anesthesia. 2022 Jan:36(1):22-29. doi: 10.1053/j.jvca.2021.04.016. Epub 2021 Apr 17 [PubMed PMID: 34059438]
Haskins SC, Bronshteyn Y, Perlas A, El-Boghdadly K, Zimmerman J, Silva M, Boretsky K, Chan V, Kruisselbrink R, Byrne M, Hernandez N, Boublik J, Manson WC, Hogg R, Wilkinson JN, Kalagara H, Nejim J, Ramsingh D, Shankar H, Nader A, Souza D, Narouze S. American Society of Regional Anesthesia and Pain Medicine expert panel recommendations on point-of-care ultrasound education and training for regional anesthesiologists and pain physicians-part II: recommendations. Regional anesthesia and pain medicine. 2021 Dec:46(12):1048-1060. doi: 10.1136/rapm-2021-102561. Epub 2021 Feb 24 [PubMed PMID: 33632777]
Kruisselbrink R, Gharapetian A, Chaparro LE, Ami N, Richler D, Chan VWS, Perlas A. Diagnostic Accuracy of Point-of-Care Gastric Ultrasound. Anesthesia and analgesia. 2019 Jan:128(1):89-95. doi: 10.1213/ANE.0000000000003372. Epub [PubMed PMID: 29624530]
Perlas A, Mitsakakis N, Liu L, Cino M, Haldipur N, Davis L, Cubillos J, Chan V. Validation of a mathematical model for ultrasound assessment of gastric volume by gastroscopic examination. Anesthesia and analgesia. 2013 Feb:116(2):357-63. doi: 10.1213/ANE.0b013e318274fc19. Epub 2013 Jan 9 [PubMed PMID: 23302981]
Level 2 (mid-level) evidenceHuang S, Cao S, Sun X, Zhang J. Gastric point-of-care ultrasonography in patients undergoing radical gastrointestinal surgery before anesthetic induction: an observational cohort study. BMC anesthesiology. 2024 Mar 4:24(1):90. doi: 10.1186/s12871-024-02473-1. Epub 2024 Mar 4 [PubMed PMID: 38433227]