Introduction
The field of visual science is concerned with the physical properties of light, including its refraction through various biological optical media, chiefly the cornea and crystalline lens. Please see StatPearls' companion reference, "The Spherical Equivalent," for further information. Clear vision at various distances is achieved through accommodation, the ability to focus incident light rays by adjusting the dynamics of the ciliary muscle-lens.[1] Concurrent single binocular vision hinges on maintaining bifoveal fixation through well-coordinated vergence movements.[2] Clear vision at various distances is achieved through accommodation, the ability to focus incident light rays by adjusting the dynamics of the ciliary muscle-lens. Please see StatPearls' companion reference, "Anatomy, Head and Neck, Eye Fovea," for further information. The eye's total optical convergence power usually ranges from 58 to 60 diopters (D), with the cornea contributing 75% to 80% of the total.[3] Hence, the crystalline lens can account for 12 to 15 D of optical convergence under normal physiologic conditions and in the absence of presbyopia.
Accommodation is an adaptive neural-ocular reflex that facilitates clear vision despite variations in the spatial distance to visual targets.[4] This reflex is strongly associated with the autonomic nervous system, specifically parasympathetic neurotransmitters released within the eye's ciliary body. Parasympathetic stimulation increases ciliary muscle tone and causes ciliary-lens zonule relaxation with subsequent enhancement of crystalline lens convexity. Blurred visual input remains the primary feedback stimulus that triggers an accommodative response.[5] In emmetropia, the eyes adjust to a greater accommodative demand around the near point of accommodation; conversely, accommodative demand diminishes significantly around the far point of accommodation.[6]
Normally, physiologic ocular reflexes such as accommodation, convergence, and miosis occur simultaneously to enable single, clear binocular vision during near visual activity.[7] All 3 actions are mediated via varying efferent pathways of the third cranial nerve. Hence, they together constitute the near synkinetic triad.[2] A deficit in engaging these near reflexes often precedes the development of binocular vision dysfunction, especially at near vision. The synergism between accommodation and convergence reflexes is commonly reported and evaluated using the accommodative convergence to accommodation ratio (AC/A), which may yield insufficient (low), normal, or excessive (high) results.[8] Variations in the AC/A ratio allow more precise classification of binocular vision anomalies during the clinical examination.[9] The Duke-Elder classification of accommodative disorders is as follows:
- Accommodative insufficiency [10][11]
- Accommodative excess, of which accommodative spasm has been described as a subtype. Please see StatPearls' companion reference, "Accommodative Excess," for further information [12]
- Accommodative inertia [13]
- Ill-sustained accommodation [14]
- Accommodative infacility [15]
This activity further discusses accommodative insufficiency. Accommodative insufficiency is a binocular vision disorder characterized by a deficient ability to focus during near work.[16] The disorder involves suboptimal accommodative reflexes in response to near visual demands.[17] The relationship is given by:
[F (in cm) = 100/D OR D = 1/F (in m)]
F = focal distance in centimeters and D = optical power in diopters. Therefore, at a hypothetical working distance of 20 cm, an equivalent of around 100/20 = 5 D of ciliary-lens accommodation is required to achieve visual clarity.
Visual science is fundamentally concerned with the optical behavior of light as it traverses the ocular media, principally the cornea and crystalline lens, to achieve focused retinal images. Clear vision at varying distances is made possible by the dynamic process of accommodation, in which the eye adjusts its refractive power in response to changes in target distance. In the emmetropic eye, total optical power averages approximately 58 to 60 D, with the cornea contributing nearly 75% to 80% of this refractive strength. The crystalline lens accounts for the remaining variable component, contributing approximately 12 to 15 D of accommodative potential in patients without presbyopia. The variable lenticular component enables the eye to modulate optical convergence, thereby focusing images precisely onto the fovea centralis, the region of highest visual acuity.[18]
Accommodation represents an adaptive neural reflex mediated primarily through parasympathetic innervation. Blur on the retina functions as the principal feedback stimulus, activating the Edinger–Westphal nucleus and traveling via the oculomotor nerve to the ciliary ganglion and subsequently to the ciliary muscle. Parasympathetic stimulation increases ciliary muscle tone, reduces zonular tension, and allows the crystalline lens to assume a more convex configuration, thereby increasing its refractive power. Accommodation occurs in concert with convergence and pupillary constriction, forming the near synkinetic triad. Coordinated near responses are essential for maintaining single, clear binocular vision during near visual tasks. The accommodative demand increases as objects approach the near point of accommodation and diminishes toward the far point, following the optical relationship that dioptric demand equals the reciprocal of the focal length in meters. For example, a working distance of 20 cm requires approximately 5 D of accommodative effort. Please see StatPearls' companion reference, "Physiology, Accommodation," for further information.
The physiologic coupling between accommodation and convergence is quantified by the accommodative convergence to accommodation (AC/A) ratio. The AC/A ratio reflects the amount of convergence induced per diopter of accommodation and serves as an important clinical parameter in binocular vision assessment. Variations in AC/A ratio results—whether low, normal, or high—assist in classifying binocular vision dysfunctions and in understanding symptom patterns associated with near work. Effective visual performance depends not only on adequate accommodative amplitude but also on harmonious integration between accommodative and vergence systems.[19]
Accommodative disorders have been historically categorized according to the Duke–Elder classification, which includes accommodative insufficiency, accommodative excess (including accommodative spasm), accommodative inertia, ill-sustained accommodation, and accommodative infacility. Among these, accommodative insufficiency represents a clinically significant functional deficit characterized by an age-inappropriate reduction in accommodative amplitude. Clinicians define accommodative insufficiency by the inability of the ciliary-lens mechanism to generate sufficient refractive power to meet near visual demands, typically manifesting as an amplitude that falls at least 2 D below expected age norms. Please see StatPearls' companion reference, "Accommodative Insufficiency," for further information.
The natural history of accommodation involves a gradual decline in amplitude with advancing age because of lenticular sclerosis and reduced capsular elasticity, ultimately culminating in presbyopia. However, accommodative insufficiency differs from physiologic presbyopia because it occurs prematurely or disproportionately relative to age expectations. Results from recent studies indicate that accommodative insufficiency is most commonly observed in school-aged children, adolescents, and young adults, particularly those engaged in sustained near-vision activities such as academic reading or digital device use. The condition may also occur following systemic illness, prolonged stress, mild traumatic brain injury, or autonomic imbalance.[20]
Clinically, accommodative insufficiency presents with symptoms including blurred near vision, asthenopia, frontal headaches, reduced reading stamina, difficulty sustaining attention during near tasks, and occasional diplopia when associated vergence dysfunction coexists. Patients may report avoidance of reading or digital tasks, and in pediatric populations, the condition may be misinterpreted as behavioral inattention or academic underperformance. Despite these symptoms, distance visual acuity often remains normal, contributing to underdiagnosis.[17]
Pathophysiologically, accommodative insufficiency reflects a mismatch between accommodative demand and accommodative reserve. Functional vision requires that approximately half of the measured accommodative amplitude be available as usable reserve to sustain prolonged near activity comfortably. When near demand approaches or exceeds this reserve capacity, visual fatigue and symptoms emerge. Thus, accommodative insufficiency is not merely a reduction in amplitude but a failure of the accommodative system to sustain adequate optical power in relation to environmental and occupational demands.[21]
In summary, accommodative insufficiency is a binocular vision disorder characterized by reduced age-appropriate accommodative amplitude and impaired ability to sustain clear near focus. The disorder represents a dysfunction of the parasympathetic ciliary-lens mechanism within the broader context of accommodative–vergence integration. Recognition of its anatomic, physiologic, and functional underpinnings is essential for accurate diagnosis and effective management, particularly in populations with high near visual demands.[22]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Depending on individual ocular physiology and the magnitude and type of refractive error, blurry vision can be a major symptom. Such experiences of blurry vision may be intermittent or persistent, depending on the degree of optical defocus caused by uncorrected refractive errors.[23] Among patients with significant uncorrected or undercorrected refractive errors, the involuntary accommodative reflex is often triggered. Please see StatPearls' companion reference, "Accommodative Excess," for further information. This response is more likely among patients with hyperopia, because increased accommodative effort in patients with myopia would, in theory, temporarily increase myopia and its blur.[24]
Uncorrected and repetitive visual effort eventually leads to ciliary muscle fatigue.[25] Ciliary muscle fatigue subsequently causes the accommodative reflex to respond suboptimally.[12] In the setting of uncorrected refractive error, hyperopia is the most likely precursor to accommodative insufficiency, especially with a high degree of facultative hyperopia (see Image. Hyperopia) (see Image. Hypermetropia). [26] During visual activity, minimal accommodative responses are triggered at optical infinity; hence, patient groups with strained near-visual capabilities (either due to refractive or vocational demands) often develop a syndrome resembling accommodative insufficiency.[27] Thus, school-aged children (especially those with uncorrected refractive error), desk workers with frequent exposure to digital screens, and high-precision craftsmen are primarily affected.[28]
Conversely, pre-existing factors such as presbyopia and neurodegenerative disease, which may be associated with autonomic nervous system dysfunction or other organic causes of oculovisual impairment, should not be regarded as primary causes of accommodative insufficiency. These factors instead reflect other comorbid factors (such as age-related crystalline lens nuclear sclerosis and neurologic impairment, respectively).[29] Accommodative insufficiency may also emerge as the adverse effect of exposure to therapeutic doses of certain pharmacologic agents. Drug classes such as parasympatholytics (eg, hyoscine and atropine) and certain sympathomimetic agents have been known to elicit this condition.[30]
Accommodative insufficiency is a multifactorial disorder arising from dysfunction within the accommodative apparatus, its neural control mechanisms, or systemic influences that impair ciliary muscle performance. The etiology may be broadly categorized into primary (idiopathic or functional) causes and secondary causes associated with systemic, neurologic, pharmacologic, or ocular conditions. Understanding the underlying cause is essential for targeted management and prognosis.[31]
At the most fundamental level, accommodation depends on the integrity of the parasympathetic pathway originating in the Edinger–Westphal nucleus, traveling via the oculomotor nerve to the ciliary ganglion, and innervating the ciliary muscle. Any disruption along this pathway—whether structural, metabolic, or functional—can impair the ciliary muscle’s ability to contract effectively. Reduced ciliary contraction results in insufficient relaxation of zonular fibers and inadequate increase in crystalline lens curvature, thereby diminishing accommodative amplitude.[4] The causes of accommodative insufficiency are summarized in Table 1.
Primary (Functional or Idiopathic) Causes
Primary accommodative insufficiency is frequently observed in otherwise healthy children and young adults. The disorder is often associated with prolonged near-visual demand, overuse of digital devices, academic stress, or sustained close working distances without adequate breaks. Chronic near work may induce accommodative fatigue, reducing effective amplitude over time. In these cases, the condition is typically reversible and responsive to vision therapy or appropriate near correction. Autonomic imbalance also contributes to functional accommodative insufficiency. Because accommodation is predominantly parasympathetically mediated, heightened sympathetic tone due to stress or anxiety may inhibit effective ciliary muscle contraction. This association explains the frequent coexistence of asthenopia and stress-related visual symptoms in young adults.[32]
Developmental and Refractive Factors
Uncorrected hyperopia can chronically stress the accommodative system. While patients with hyperopia exert additional accommodative effort for both distance and near vision, prolonged overexertion may lead to accommodative fatigue and eventual insufficiency. Similarly, poorly prescribed lenses or inappropriate use of near addition may alter accommodative demand and reduce accommodative reserve.[26]
Neurologic Causes
Neurologic disorders affecting the parasympathetic pathway may impair accommodation. These include:
- Mild traumatic brain injury (concussion)
- Multiple sclerosis
- Intracranial tumors affecting midbrain structures
- Oculomotor nerve palsy (partial)
- Autonomic neuropathies
Postconcussive accommodative insufficiency is particularly well documented and may persist for months following injury.[33]
Systemic and Metabolic Conditions
Systemic illnesses that affect neuromuscular transmission or metabolic stability can reduce accommodative amplitude. These include:
- Diabetes mellitus (autonomic neuropathy)
- Hypothyroidism
- Myasthenia gravis
- Chronic anemia
- Malnutrition
- Chronic fatigue syndromes
In diabetes mellitus, fluctuating blood glucose levels may temporarily alter the lens's refractive index, whereas autonomic neuropathy can produce more persistent accommodative dysfunction.[33]
Pharmacologic Causes
Several medications interfere with parasympathetic activity and reduce accommodation. Anticholinergic drugs inhibit ciliary muscle contraction, leading to pharmacologic accommodative insufficiency. Common contributors include:
- Antihistamines
- Tricyclic antidepressants
- Antipsychotics
- Cycloplegic agents
- Certain anti-anxiety medications
Medication adjustment typically reverses these effects.[34]
Ocular Causes
Ocular trauma, ciliary body inflammation (cyclitis), or postsurgical states may transiently impair accommodation. Chronic ocular surface disease may also mimic accommodative symptoms with fluctuating blur, though the true accommodative amplitude remains intact.
Psychogenic or Functional Overlay
Psychogenic or functional overlay may also contribute in some adolescents and young adults, particularly when symptoms are disproportionate to measured amplitude reduction. Stress-related visual complaints may coexist with measurable but mild accommodative deficits.[35]
Table 1: Etiology of Accommodative Insufficiency
|
Category |
Specific causes |
Mechanism of dysfunction |
Reversibility |
|
Primary/Functional |
Prolonged near work, digital overuse, and academic stress |
Ciliary muscle fatigue |
High |
|
Refractive |
Uncorrected hyperopia, inappropriate near add |
Chronic accommodative stress |
High |
|
Neurologic |
Concussion, MS, CN III palsy, midbrain lesions |
Parasympathetic pathway disruption |
Variable |
|
Systemic/metabolic |
Diabetes mellitus, hypothyroidism, anemia, MG |
Autonomic or neuromuscular dysfunction |
Variable |
|
Pharmacologic |
Anticholinergics, antihistamines, antidepressants |
Parasympathetic inhibition |
High |
|
Ocular |
Cyclitis, trauma, surgery |
Mechanical or inflammatory impairment |
Variable |
|
Psychogenic |
Stress-related functional visual disorder |
Autonomic imbalance |
High |
Abbreviations: CN, cranial nerve; MG, myasthenia gravis; MS, multiple sclerosis
In conclusion, accommodative insufficiency represents a heterogeneous condition with both functional and organic causes. While primary functional fatigue remains the most common etiology in pediatric and young adult populations, clinicians must systematically evaluate neurologic, systemic, and pharmacologic contributors. A detailed history, medication review, and targeted systemic evaluation are essential for establishing the underlying cause and guiding appropriate therapy.[32]
Epidemiology
Accommodative dysfunction occurs in the majority of patients with binocular vision problems. Epidemiologic data on the prevalence of accommodative dysfunction in a heterogeneous population are scarce in the contemporary literature.[36] However, results from several studies that sought to synthesize the prevalence of accommodative dysfunction among a uniform population of patients without presbyopia found that accommodative insufficiency was the most prevalent finding.[37]
Most data account for the prevalence of accommodative dysfunction amongst school-aged children between the ages of 8 and 15 years.[38] Results from studies suggest that individuals with convergence insufficiency contribute to the increased incidence of accommodative dysfunction.[39] A meta-analysis by Husainideen and Murali reported a high prevalence of asthenopic symptoms, including floating words, eyestrain, and poor coordination during prolonged visual activity, among individuals with accommodative insufficiency.[40]
Children with Down syndrome have a higher prevalence of accommodative deficits.[41] Children with cerebral palsy are also reported to have lower accommodative amplitudes compared with age-matched peers. Reports of accommodative and vergence dysfunction among younger adults ranging from 18 to 35 years show that these conditions are common.[42][43] This pattern may be due to the widespread use of digital devices, with numerous tasks requiring screen-based equipment.[44]
Accommodative insufficiency is one of the most frequently encountered nonstrabismic binocular vision disorders in clinical optometric and ophthalmologic practice, particularly among pediatric and young adult populations. Although prevalence estimates vary across diagnostic criteria, testing methods, and populations studied, accommodative insufficiency is a significant contributor to asthenopic symptoms associated with near work worldwide.[22] Table 2 summarizes the epidemiology of accommodative insufficiency.
Global Prevalence
International studies report prevalence rates ranging from approximately 2% to 8% in school-aged children and adolescents. In certain high-demand academic environments and clinic-based samples, rates have been reported to be 10% to 15%, particularly when accommodative amplitude criteria are applied strictly (eg, ≥2 D below the Hofstetter minimum formula). Variability in prevalence is largely attributable to differences in diagnostic thresholds, the inclusion of symptomatic versus asymptomatic individuals, and the use of monocular versus binocular amplitude measurements.[45] In resource-limited countries, reported prevalence may be underestimated because of limited access to binocular vision assessment tools. Conversely, in urban populations with high digital device use, accommodative dysfunction, including accommodative insufficiency, appears to be increasing, likely reflecting sustained near-visual demand and reduced accommodative recovery intervals.[46]
United States Epidemiology
In the United States, accommodative insufficiency is estimated to affect approximately 4% to 6% of school-aged children in community-based samples. Among children presenting with academic difficulties or reading concerns, the prevalence may range from 8% to 12%. University-based clinic studies have reported rates of 5% to 10% among young adults, especially those engaged in prolonged near work, such as computer use or intensive reading. Postconcussive accommodative insufficiency has emerged as an important subset in US populations. Among individuals with mild traumatic brain injury, accommodative deficits have been reported in 20% to 40% of cases, although these figures encompass broader accommodative dysfunction and not exclusively isolated accommodative insufficiency.[17]
Age Distribution
Accommodative insufficiency demonstrates a characteristic age-related distribution. The disorder is most commonly diagnosed in children aged 8 to 15 years, adolescents, and young adults aged 18 to 30 years. The condition is less frequently diagnosed in older adults because physiologic presbyopia predominates beyond the fourth decade of life, making age-appropriate amplitude decline the more common finding rather than isolated insufficiency. In pediatric populations, accommodative insufficiency may remain undiagnosed until academic demands increase, typically during late primary or early secondary education. The onset often coincides with sustained reading requirements, increased homework, and increased screen time. In adults younger than 40 years, accommodative insufficiency may present in individuals engaged in intensive near-work occupations, including students, software professionals, and office-based workers.[32]
Sex Distribution
Most epidemiologic studies indicate no strong sex predilection for accommodative insufficiency. Prevalence appears roughly equal between men and women in community-based samples. However, some clinic-based studies suggest slightly higher symptom reporting among women, possibly reflecting differences in health-seeking behavior rather than a true biological disparity. In postconcussive populations, sex distribution reflects injury epidemiology rather than intrinsic susceptibility to accommodative insufficiency. Please see StatPearls' companion reference, "Dissociated Vertical Deviation," for further information.
Geographic and Environmental Trends
Urban populations with high digital exposure report more frequent accommodative complaints than rural populations. Prolonged smartphone, tablet, and computer use has been implicated as a contributing environmental factor. The increasing prevalence of near-intensive educational systems globally may partly explain rising reports of accommodative dysfunction. Evidence does not show an ethnic predilection; however, the distribution of refractive error within populations (eg, high prevalence of hyperopia) may influence secondary accommodative fatigue rates.
Association With Other Binocular Vision Disorders
Accommodative insufficiency frequently coexists with convergence insufficiency. Results from studies reported comorbidity rates of 15% to 40%, depending on the population examined. In such cases, symptom burden is often amplified, and epidemiologic classification may overlap.[47]
Special Populations
Selected samples of children with learning disabilities have shown higher reported rates (up to 15%). Patients with posttraumatic brain injury may also have an elevated incidence. Individuals with systemic disease (eg, diabetes mellitus) show variable rates depending on autonomic involvement.[47]
Table 2. Epidemiologic Summary of Accommodative Insufficiency
|
Parameter |
Estimated frequency |
|
General pediatric population |
2%–8% |
|
School children with reading complaints |
8%–12% |
|
Young adults (college clinics) |
5%–10% |
|
Postconcussion |
20%–40% (broader accommodative dysfunction) |
|
Sex predilection |
None significant |
|
Most affected age group |
8–30 years |
Public Health Significance
Although not vision-threatening, accommodative insufficiency carries significant functional implications. The disorder may impair reading fluency, reduce academic performance, and contribute to chronic visual discomfort. Given the increasing worldwide dependence on digital screens, accommodative disorders are an emerging area of concern in pediatric and young adult eye care. In summary, accommodative insufficiency is a relatively common binocular vision disorder, particularly affecting school-aged children and young adults. The condition shows no strong sex predilection, demonstrates a higher prevalence in near-intensive environments, and may be underrecognized in routine vision screening programs that primarily focus on distance acuity. Accurate epidemiologic characterization is essential for early identification and targeted intervention strategies.[48]
Pathophysiology
Accommodative insufficiency represents a functional reduction in the accommodative system's ability to generate and sustain adequate refractive power in response to near visual demands. The disorder primarily involves dysfunction at the level of the ciliary muscle–zonular–crystalline lens complex, its parasympathetic neural control, or the integrative feedback loop that regulates accommodative response.[32] Accommodation is initiated when retinal blur stimulates cortical visual centers, which transmit signals to the Edinger–Westphal nucleus in the midbrain. Parasympathetic fibers then travel via the oculomotor nerve to the ciliary ganglion and subsequently innervate the ciliary muscle. In accommodative insufficiency, this pathway may be functionally underactive or fatigued, resulting in reduced ciliary muscle contraction. Inadequate contraction prevents sufficient relaxation of the zonular fibers, thereby limiting increases in lens curvature and reducing the effective dioptric power.[49]
A central concept in the pathophysiology of accommodative insufficiency is the mismatch between accommodative demand and accommodative reserve. Physiologically, sustained near work requires that approximately half of the measured accommodative amplitude remain available as reserve to prevent asthenopic symptoms. When accommodative amplitude is reduced—whether from neuromuscular fatigue, autonomic imbalance, or systemic dysfunction—the reserve becomes insufficient. As near demand approaches or exceeds the available reserve, patients experience blur, visual fatigue, and reduced reading endurance.[17]
Autonomic imbalance plays an important contributory role. Because accommodation is parasympathetically mediated, increased sympathetic tone associated with stress or fatigue may inhibit effective ciliary muscle contraction. In postconcussive or neurologic cases, disruption of midbrain or oculomotor pathways further impairs accommodative signaling. In systemic conditions such as diabetes mellitus, autonomic neuropathy may blunt parasympathetic responsiveness, leading to persistent reductions in amplitude. Please see StatPearls' companion reference, "Physiology, Autonomic Nervous System," for further information.
At the lenticular level, although accommodative insufficiency is distinct from presbyopia, subtle biomechanical factors may contribute in some cases. Reduced lens elasticity or altered capsular compliance can diminish accommodative efficiency even in younger individuals, particularly when compounded by chronic near strain. Accommodative insufficiency frequently coexists with convergence anomalies. Because accommodation and convergence are neurally coupled through the AC/A relationship, reduced accommodative response may secondarily reduce accommodative convergence. Reduced accommodative convergence can destabilize binocular alignment at near, further exacerbating symptoms.[50]
Most Common Clinical Pathophysiologic Findings
The hallmark finding in accommodative insufficiency is reduced accommodative amplitude relative to age norms, typically at least 2 D below expected values. Additional findings include:
- Reduced accommodative facility (difficulty changing focus rapidly)
- Increased lag of accommodation on dynamic retinoscopy
- Normal or low AC/A ratio
- Symptoms disproportionate to minimal refractive error
- Greater symptom severity during sustained near tasks [51]
Accommodative insufficiency results from inadequate parasympathetic stimulation or functional fatigue of the ciliary muscle, leading to reduced lens convexity and diminished accommodative amplitude. A mismatch develops between near visual demand and the available accommodative reserve, resulting in blur and asthenopic symptoms during sustained near work. Autonomic imbalance, neurologic disruption, or systemic disease may impair the accommodative reflex arc. The most common clinical finding is an age-inappropriate reduction in accommodative amplitude, often accompanied by increased lag and reduced accommodative facility.[52]
Histopathology
Accommodative insufficiency is primarily a functional neuro-ophthalmic disorder; therefore, in most primary (idiopathic) cases, no specific structural or histopathologic abnormalities are identifiable on routine microscopic examination. The condition reflects reduced physiologic performance of the accommodative apparatus rather than overt tissue degeneration or destruction. Nevertheless, understanding the microscopic structure of the ciliary body, zonular apparatus, crystalline lens, and parasympathetic innervation helps contextualize secondary causes in which histopathologic changes may be observed.[53]
The accommodative system relies on the coordinated contraction of the ciliary muscle, relaxation of zonular fibers, and increased convexity of the crystalline lens. The ciliary muscle consists of longitudinal, radial, and circular smooth muscle fibers embedded within a vascular stromal matrix. In primary accommodative insufficiency, light microscopy typically demonstrates preserved smooth muscle architecture without fibrosis, atrophy, or inflammatory infiltration. The zonular fibers and lens capsule also remain structurally intact. Therefore, primary accommodative insufficiency is best characterized as a functional neuromuscular insufficiency without structural pathology.[54]
In contrast, secondary accommodative insufficiency associated with systemic, neurologic, or inflammatory conditions may demonstrate identifiable microscopic changes. In diabetic autonomic neuropathy, degeneration of parasympathetic nerve fibers supplying the ciliary body may be observed, including axonal loss, demyelination, and microvascular thickening. In inflammatory conditions such as anterior uveitis or cyclitis, histopathology may reveal inflammatory infiltrates within the ciliary body stroma, vascular congestion, stromal edema, and disruption of smooth muscle fiber alignment. These changes may transiently or permanently impair accommodative function.[55]
Although age-related lenticular sclerosis is a hallmark of presbyopia rather than accommodative insufficiency, clinicians should distinguish the 2 conditions. Presbyopic lenses demonstrate nuclear compaction, increased lens fiber density, and reduced capsular elasticity. In younger patients with accommodative insufficiency, these lenticular structural changes are typically absent. Overall, histopathologic evaluation underscores that accommodative insufficiency is predominantly a functional disorder, with structural abnormalities only evident in secondary or systemic disease states.[56] Table 3 summarizes the microscopic findings of accommodative insufficiency.
Table 3. Histopathologic Correlates in Accommodative Insufficiency
|
Etiologic category |
Tissue involved |
Microscopic findings |
Functional impact |
|
Primary (idiopathic) accommodative insufficiency |
Ciliary muscle, zonules, lens |
Normal architecture; no inflammation or fibrosis |
Functional neuromuscular underactivity |
|
Autonomic neuropathy (eg, diabetes mellitus) |
Short ciliary nerves |
Axonal degeneration, demyelination, microangiopathy |
Reduced parasympathetic stimulation |
|
Inflammatory (cyclitis/uveitis) |
Ciliary body stroma |
Inflammatory cell infiltrate, edema, vascular congestion |
Impaired ciliary contraction |
|
Posttraumatic |
Ciliary body |
Focal muscle disruption or neural injury |
Variable reduction in amplitude |
|
Neurologic (CN III involvement) |
Parasympathetic pathway |
Degenerative neural changes (if chronic) |
Reduced accommodative signaling |
|
Presbyopia (differential) |
Crystalline lens |
Nuclear sclerosis, lens fiber compaction |
Mechanical reduction in amplitude (age-related) |
Abbreviations: CN, cranial nerve
Key Histopathologic Insights
- Primary accommodative insufficiency: No demonstrable structural abnormality
- Secondary accommodative insufficiency: May show neural, inflammatory, or vascular pathology
- Presbyopia must be distinguished from accommodative insufficiency based on age and lenticular sclerosis
- Accommodative insufficiency reflects dysfunction of the parasympathetic ciliary-lens unit rather than tissue destruction [56]
Toxicokinetics
Accommodative insufficiency may arise secondary to exposure to pharmacologic agents or toxins that interfere with the parasympathetic control of the ciliary muscle. Toxicokinetics—the study of absorption, distribution, metabolism, and elimination of toxic substances—plays a critical role in understanding how systemic or topical agents impair accommodation. Because accommodation is mediated predominantly by muscarinic cholinergic receptors in the ciliary muscle, substances that antagonize cholinergic transmission are the most common toxicologic contributors.[31] Table 4 summarizes the toxins and drugs that contribute to accommodative insufficiency.
Mechanistic Basis
The accommodative reflex depends on acetylcholine release from postganglionic parasympathetic fibers within the ciliary body. Drugs or toxins that reduce acetylcholine availability, block muscarinic receptors, or impair autonomic transmission diminish ciliary muscle contraction. Reduced contraction prevents adequate zonular relaxation and limits lens convexity, thereby decreasing accommodative amplitude.
Absorption and Ocular Distribution
Systemically administered anticholinergic medications are absorbed through the gastrointestinal tract and distributed via systemic circulation, including ocular tissues. Lipophilic agents readily cross the blood–ocular barrier and reach the ciliary body. Topical ophthalmic agents (eg, cycloplegics) act locally, with rapid corneal penetration and direct receptor blockade within minutes.[57]
Metabolism and Elimination
The duration of accommodative impairment depends on drug half-life, receptor affinity, and metabolic clearance. Short-acting anticholinergics (eg, tropicamide) produce transient cycloplegia lasting several hours, whereas longer-acting agents (eg, atropine) may induce sustained accommodative paralysis for days to weeks. Systemic medications with longer half-lives may produce chronic or fluctuating accommodative reduction.[57]
Table 4. Common Toxicologic and Pharmacologic Agents Associated with Accommodative Insufficiency
|
Agent category |
Examples |
Mechanism |
Duration of effect |
Reversibility |
|
Anticholinergics |
Atropine, tropicamide, scopolamine |
Muscarinic receptor blockade |
Hours to weeks |
Yes |
|
Antihistamines |
Diphenhydramine |
Anticholinergic side effect |
Transient |
Yes |
|
Tricyclic antidepressants |
Amitriptyline |
Anticholinergic + central effect |
Variable |
Yes |
|
Antipsychotics |
Chlorpromazine |
Anticholinergic properties |
Variable |
Yes |
|
Benzodiazepines |
Diazepam |
CNS depression |
Mild, transient |
Yes |
|
Organophosphates (toxins) |
Pesticides |
Acetylcholinesterase inhibition (initial spasm, later fatigue) |
Variable |
Variable |
|
Alcohol (acute) |
Ethanol |
CNS depressant |
Short-term |
Yes |
Abbreviations: CNS, central nervous system.
Organophosphate Toxicity
Interestingly, organophosphate exposure initially causes excessive cholinergic stimulation, which may produce accommodative spasm. However, prolonged exposure can lead to neuromuscular fatigue and eventual accommodative weakness due to receptor desensitization and autonomic dysfunction. Please see StatPearls' companion reference, "Organophosphate Toxicity," for further information.
Systemic Toxic States
Chronic systemic toxicity (eg, heavy metal exposure, metabolic acidosis, chronic alcohol use) may impair neuromuscular function and autonomic regulation, contributing indirectly to accommodative insufficiency.
Toxicodynamic Considerations
The severity of accommodative insufficiency related to toxins depends on:
- Dose and plasma concentration
- Lipid solubility and ocular penetration
- Receptor affinity
- Duration of exposure
- Individual autonomic sensitivity
Most pharmacologically induced accommodative insufficiency is reversible upon discontinuation or dose adjustment. However, chronic autonomic neuropathy (eg, diabetic or toxic neuropathy) may result in a persistent reduction in accommodative amplitude.[58]
History and Physical
An individual with accommodative insufficiency tends to report blurry vision during near visual tasks, headaches, visual fatigue, and other asthenopic symptoms (such as eyestrain, diplopia, and similar symptoms).[16][59] Patients with this disorder can also experience a psychological ripple effect, manifesting as irritability, loss of concentration during near work, and even disinterest in academic activities among school-aged children.[60] Patients may also present with concurrent convergence insufficiency findings, which tend to be relieved without specific treatments such as prism therapy or vergence exercises.[61]
Young children may become symptomatic after an illness or a fever.[62] For adults with concurrent asthenopia and vertigo, the presence of physical findings such as ataxia, facial asymmetry, palpebral ptosis, anisocoria, exophthalmos, increased fatigability, and strabismus should be considered red flags.[63] In such scenarios, the clinician should ask about a prior history of alcohol use disorder, periocular or head trauma, anemia, central nervous system infection, ocular myasthenia gravis, Graves orbitopathy, multiple sclerosis, or other demyelinating disease. Please see StatPearls' companion reference, "Ptosis Correction," for further information. A history of systemic microvascular disease, especially diabetes mellitus, should be queried in adult patients, as diabetes mellitus is a predisposing factor for autonomic denervation of the ciliary ganglion.[64]
Accommodative insufficiency is primarily a functional binocular vision disorder, and therefore, diagnosis relies heavily on a careful clinical history and a comprehensive binocular vision examination. Patients usually present with difficulty sustaining near visual tasks despite normal or near-normal distance visual acuity. A detailed history is essential for identifying symptom patterns, occupational demands, and potential systemic or neurologic contributors.[65]
Patient History
The clinical history typically reveals concerns associated with prolonged near work, such as reading, writing, or using digital devices. Patients frequently report intermittent blurred vision at near, especially after sustained reading. Symptoms often worsen toward the end of the day or after prolonged visual concentration. Many individuals describe eye strain (asthenopia), frontal or periocular headaches, and difficulty maintaining focus during near tasks. Children may exhibit behavioral signs such as reduced reading endurance, skipping lines while reading, poor academic performance, or avoidance of homework.[66]
Visual fatigue is a hallmark feature of accommodative insufficiency. Patients may report that words appear to move, become blurred after several minutes of reading, or require repeated refocusing. Some individuals compensate by increasing working distance or taking frequent breaks during near tasks. In adolescents and young adults with high digital screen exposure, symptoms may be exacerbated by prolonged smartphone or computer use. A history of intermittent diplopia, loss of concentration during reading, or slow reading speed may suggest associated vergence anomalies, particularly convergence insufficiency, which frequently coexists with accommodative disorders. Clinicians should also inquire about systemic conditions such as diabetes mellitus, neurologic disease, recent head trauma, or medication use (particularly anticholinergic drugs) that may impair accommodative function.[67]
Important aspects of the history include:
- Duration and onset of symptoms
- Relationship of symptoms to near work
- Reading habits and digital device use
- Occupational or academic visual demands
- History of head injury or neurologic illness
- Systemic diseases affecting autonomic function
- Current medications
In pediatric populations, teachers or parents may report difficulty sustaining attention during reading, which can sometimes be mistaken for learning disorders or attention-deficit disorders.[68]
Physical Examination
A comprehensive ophthalmic examination is required to confirm accommodative insufficiency and exclude other causes of near vision complaints. The evaluation should include assessment of visual acuity, refractive status, binocular vision function, and accommodative parameters. Table 5 summarizes the physical examination findings.
Visual Acuity
Distance visual acuity results are typically normal (20/20 or close to normal) in patients with accommodative insufficiency. Near visual acuity test findings may initially appear normal, but often deteriorate with sustained reading tasks due to accommodative fatigue.[69]
Refraction
Cycloplegic and manifest refraction are performed to exclude uncorrected refractive errors, particularly hyperopia. Even mild hyperopia may increase accommodative demand and contribute to symptoms.
Assessment of Accommodation
Measurement of accommodative amplitude is the key diagnostic component. The near point of accommodation is commonly assessed using the push-up method. In accommodative insufficiency, accommodative amplitude is typically at least 2 D below expected age norms (often compared to the Hofstetter minimum formula). Dynamic retinoscopy may reveal increased lag of accommodation, indicating that the accommodative response is insufficient relative to near demand. Accommodative facility testing with plus and minus lenses often demonstrates difficulty clearing minus lenses, reflecting reduced accommodative stimulation. Please see StatPearls' companion reference, "Cycloplegic and Noncycloplegic Refraction," for further information.
Binocular Vision Assessment
Because accommodation and convergence are closely linked, binocular vision testing is essential. Evaluation includes:
- Cover test at a distance and near
- Near point of convergence
- Assessment of fusional vergence ranges
- Measurement of the AC/A ratio
Patients with accommodative insufficiency frequently have a normal or low AC/A ratio and may exhibit signs of associated convergence insufficiency.[70]
Ocular Motility and Pupillary Examination
Extraocular motility is generally normal. Pupillary responses are intact, although the near reflex response may be less robust if accommodative effort is reduced.
Slit-Lamp and Fundus Examination
Anterior segment and fundus examinations are typically unremarkable in primary accommodative insufficiency. These assessments are performed primarily to exclude other ocular pathology.[49]
Table 5. Common Physical Examination Findings
|
Clinical parameter |
Typical finding in accommodative insufficiency |
|
Distance visual acuity |
Usually normal |
|
Near visual acuity |
May blur with sustained reading |
|
Accommodative amplitude |
≥2 D less than reference for age |
|
Dynamic retinoscopy |
Increased lag of accommodation |
|
Accommodative facility |
Reduced, especially with minus lenses |
|
AC/A ratio |
Normal or low results |
|
Near point of convergence |
May be normal or slightly receded |
|
Ocular health examination |
Normal findings |
Clinical Interpretation
The diagnosis of accommodative insufficiency is established when reduced accommodative amplitude and accommodative facility are accompanied by near-work symptoms in the absence of significant ocular pathology. Because symptoms may overlap with other binocular vision disorders, careful integration of history and examination findings is critical for accurate diagnosis.[17]
Evaluation
For proper diagnosis of accommodative and vergence dysfunction, numerous tests and examinations should be performed. Optimal correction of preexisting refractive error is obligatory.[71] Tests of accommodative function should be carried out while patients wear their optimal refractive correction. Normative parameters are measured to determine whether they are within their expected range empirically. Key tests to be conducted prior to the differential diagnosis of accommodative insufficiency include negative relative accommodation, near point of convergence, and positive relative accommodation results. Tests of accommodative facility and accommodative lead and lag, via the monocular estimation method (retinoscopy), are also important for making an accurate diagnosis.[72]
Near point of convergence measurement is useful for investigating the presence of accommodative insufficiency that mimics pseudoconvergence insufficiency.[73] The presence of a manifest or latent deviation can be ascertained using the cover-uncover and alternating cover tests (see Image. Orthotropia and Exotropia).[74] Deviations can then be measured using prism bars or loose prisms (see Image. Horizontal and Vertical Ophthalmic Prism Bars).[75]
Among patients with accommodative insufficiency, the amplitude of accommodation (AA) is often reduced relative to normative data. These patients tend to show reduced accommodation amplitude beyond the minimum expected findings derived from the Hofstetter formula and the Donder table of age-expected diopters of accommodation.[14]
Minimum AA = 15 − (0.25 × age)
The amplitude of accommodation can be determined using either the push-up/push-down technique or the minus lens-to-blur evaluation technique.[76] The latter technique may yield lower values by about 2 diopters. Individuals who underaccommodate usually show a lag in accommodation, while patients who overaccommodate show an accommodative lead. The presence of an accommodative lag or lead posture can be determined via either monocular estimation method, retinoscopy, or the fused cross-cylinder test.[77]
The fused cross-cylinder test is more subjective. The test may be tedious and thus yield less accurate responses, especially with young children. Monocular estimation method (retinoscopy) is performed with fixation directed to a near target. Please see StatPearls' companion reference, "Objective Refraction Technique: Retinoscopy," for further information. An attempt is then made to quickly neutralize the reflex's movement with spherical lenses of appropriate power. The expected lag finding should not exceed +0.50 D beyond the accommodative demand (calculated as the dioptric equivalent of the near testing distance). Lag findings greater than +1.00 D indicate a weak accommodative posture.
Accommodative facility testing is another method of assessing the subject's ability to stimulate and relax accommodative responses at a normal rate. The test also tests the accuracy of repetitive alterations to oscillatory demand placed on accommodation. Accommodative facility is often determined using flipper lenses with a power of ±2.00 D.[78] The test should ideally be conducted binocularly in cases of accommodative insufficiency. Normally, at least 11 cycles should be cleared per minute. Individuals with accommodative insufficiency will manifest slow facility with −2.00 D phases of the test cycle and thus fail the +/−2.00 D flipper test.[37]
Negative and positive relative accommodation values measure the fusional capability to either relax or stimulate accommodation as a compensatory response. The procedure for testing negative relative accommodation involves adding plus lenses over the distance correction until near optotypes turn blurry. Clinicians repeat this same procedure for positive relative accommodation, with the difference being that minus lenses are used in place of plus lenses.[79]
Horizontal fusional vergence amplitudes (both at near and distance) are measured using base-in prisms and base-out prisms. Clinicians place base-in prisms while measuring negative fusional vergence, while base-out prisms are used to measure positive fusional vergence amplitudes. Blur, break, and recovery findings are then compared to the Morgan expected ranges. Patients with accommodative insufficiency ought to demonstrate suboptimal positive fusional vergence reserves at near (around 0.4 m).
The AC/A ratio is a key factor to consider in the diagnosis and treatment of binocular vision dysfunction. The convention is 4:1 (signifying that 4 prism diopters of convergence are stimulated per diopter of accommodation).[80] One method of calculating the AC/A ratio involves measuring phoria with and without a gradient lens; another is termed the heterophoria method.[81] In determining the AC/A relationship using this gradient method, the patient's optimal near correction is placed in the trial frame. +1.00 D and -1.00 D lenses are then introduced to either stimulate or relax fusional divergence for esophoric and exophoric findings, respectively. The change in prism bar phoria measurement with and without the plus and minus gradient lens is then calculated:
Phoria with lens − phoria without lens/power of the lens [82]
The evaluation of accommodative insufficiency involves a comprehensive assessment of visual acuity, refractive status, binocular vision function, and accommodative parameters. Because accommodative insufficiency is primarily a functional binocular vision disorder rather than a structural ocular disease, diagnosis is largely based on clinical testing rather than laboratory or radiographic studies. The objective of evaluation is to confirm reduced accommodative amplitude relative to age norms, assess accommodative dynamics, identify associated vergence anomalies, and exclude systemic or neurologic conditions that may contribute to the disorder. Table 6 summarizes the modalities used to diagnose accommodative insufficiency.
Clinical History and Screening
The evaluation begins with a detailed clinical history focusing on symptoms associated with near work. Patients commonly report blurred near vision, visual fatigue, headaches, and difficulty maintaining focus while reading or using digital devices. Children may demonstrate reduced reading stamina or avoidance of academic tasks. The history should also include information regarding occupational or academic visual demands, digital screen exposure, medication use (especially anticholinergic drugs), systemic illnesses such as diabetes, and any history of head trauma or neurologic disease.
Visual Acuity Assessment
Measurement of both distance and near visual acuity is performed as an initial step. Distance visual acuity is usually normal in accommodative insufficiency. Near visual acuity may appear normal initially but can deteriorate after sustained near work due to accommodative fatigue.[17]
Refraction
A complete manifest and cycloplegic refraction is essential to identify uncorrected refractive errors, particularly hyperopia, which can increase accommodative demand. Proper refractive correction is necessary before evaluating accommodative function.
Measurement of Accommodative Amplitude
Assessment of accommodative amplitude is the most important diagnostic test for accommodative insufficiency The near point of accommodation is commonly measured using the push-up method or minus lens method. According to the Hofstetter formulas, the expected accommodative amplitude can be estimated based on age. Accommodative insufficiency is typically diagnosed when the measured amplitude is at least 2 D below the minimum expected value. Please see StatPearls' companion reference, "Cycloplegic and Noncycloplegic Refraction," for further information.
Hofstetter formulas used for comparison include:
- Average amplitude = 18.5 − (0.3 × age in years)
- Minimum amplitude = 15 − (0.25 × age in years)
Dynamic Retinoscopy
Dynamic retinoscopy is used to assess the accommodative response during near fixation. In patients with accommodative insufficiency, the test commonly reveals increased lag of accommodation, indicating that the accommodative response is insufficient relative to the near stimulus.[83]
Accommodative Facility Testing
Accommodative facility evaluates the speed and flexibility of the accommodative system using plus and minus lenses. Testing is usually performed with ± 2.00 D lenses under monocular and binocular conditions. Patients with accommodative insufficiency typically show difficulty clearing minus lenses, reflecting impaired accommodative stimulation.
Binocular Vision Testing
Because accommodation and convergence are closely linked through the AC/A ratio, a full binocular vision evaluation is necessary. This evaluation includes:
- Cover test at a distance and near
- Near point of convergence
- Fusional vergence testing
- Measurement of the AC/A ratio
Accommodative insufficiency may occur independently or in association with convergence insufficiency.[84]
Ocular Health Examination
Slit-lamp examination and dilated fundus examination are performed to exclude ocular pathology that could cause similar symptoms. In primary accommodative insufficiency, ocular structures are typically normal.
Laboratory and Systemic Evaluation
Laboratory investigations are generally not required in typical cases of accommodative insufficiency. However, when secondary causes are suspected, targeted laboratory testing may be indicated. For example:
- Blood glucose levels in suspected diabetic autonomic neuropathy
- Thyroid function tests in suspected hypothyroidism
- Hemoglobin levels in suspected anemia
- Neurologic evaluation following head trauma
Please see StatPearls' companion reference, "Lenticonus," for further information.
Imaging Studies
Radiologic imaging is not routinely required for accommodative insufficiency. Neuroimaging, such as MRI, may be considered when neurologic symptoms suggest central nervous system involvement, particularly lesions affecting the midbrain or oculomotor nerve pathways.
National and International Guidelines
Recommendations from professional bodies such as the American Optometric Association and the American Academy of Ophthalmology guide clinical evaluation of accommodative insufficiency. These guidelines emphasize comprehensive binocular vision testing, measurement of accommodative amplitude relative to age norms, and evaluation of accommodative facility and response accuracy. Internationally, similar standards are followed in orthoptic and binocular vision assessment protocols used in Europe, North America, and other regions. American Optometric Association guidelines specifically recommend assessing accommodative amplitude, accommodative facility, and accommodative response in patients presenting with near-vision concerns. The guidelines also emphasize the importance of evaluating vergence function given the close interaction between the accommodation and convergence systems.[85]
Table 6. Summary of Diagnostic Evaluation
|
Diagnostic test |
Purpose |
Expected finding in Accommodative Insufficiency |
|
Distance visual acuity |
Assess baseline vision |
Usually normal |
|
Near visual acuity |
Evaluate near performance |
May decline with sustained work |
|
Refraction |
Detect refractive error |
Often minimal error |
|
Near point of accommodation |
Measure amplitude |
Reduced ≥2 D below age norms |
|
Dynamic retinoscopy |
Assess accommodative response |
Increased lag |
|
Accommodative facility |
Evaluate focusing flexibility |
Difficulty clearing minus lenses |
|
AC/A ratio |
Assess accommodation-convergence link |
Normal or low |
|
Binocular vision tests |
Detect associated vergence disorders |
Possible CI association |
|
Ocular health exam |
Exclude pathology |
Usually normal |
Abbreviations: CI, convergence insufficiency.
Diagnostic Criteria
A diagnosis of accommodative insufficiency is generally established when the following are present:
- Reduced accommodative amplitude relative to age norms
- Symptoms associated with near visual tasks
- Increased lag of accommodation
- Reduced accommodative facility
- Absence of significant ocular disease [17]
Clinical Significance
Accurate evaluation is essential because accommodative insufficiency may significantly affect reading performance, academic productivity, and occupational efficiency. Comprehensive binocular vision testing helps distinguish accommodative insufficiency from other accommodative or vergence disorders, enabling appropriate therapeutic intervention.[46]
Treatment / Management
Treatment of accommodation should begin with proper refraction and correction of refractive errors. Clinicians should recognize that low-grade ametropia may still exacerbate the symptoms of patients with accommodative insufficiency. Correcting refractive errors, however mild, may provide substantial relief.[17] Increasing plus lens power is the most common measure because of its relaxing effect on near accommodative demand. Examination findings commonly observed in patients support the usefulness of adding a plus lens to the management of this condition. Common signs include low positive relative accommodation results and AA. Others include high accommodative lag and difficulty clearing minus lenses during accommodative facility testing. Plus-lens prescribing may be a problem for patients with myopia, because prescribing plus lenses can negate the refractive endpoint. Patients with myopia, however, may benefit from bifocals or progressive lenses, especially if they have accommodative insufficiency or accommodative esophoria. Results from studies have shown that this practice may slow axial length progression in patients with myopia.[86] (A1)
In cases where the cause is organic or accommodative inertia, plus lenses are recommended, either permanently or temporarily, as needed.[87] Because such causes are organic, there may be significant unequal accommodation between the patient's eyes. Accordingly, such patients commonly require different near addition powers. Additionally, with the growth of teleoptometry, remote vision therapy may hold promise for managing accommodative insufficiency through home-based computer-based accommodative therapy, thereby enhancing patients' AA and positive relative accommodation measures.[73] Successful outcomes following vision therapy depend on factors such as patients' age, motivation, and adherence to the regimen(A1)
The management of accommodative insufficiency focuses on restoring adequate accommodative function, relieving symptoms associated with near visual tasks, and improving overall visual efficiency. Because accommodative insufficiency is primarily a functional disorder involving reduced accommodative amplitude and endurance, treatment strategies are largely nonsurgical and emphasize optical correction, vision therapy, and modification of visual habits. The treatment approach should be individualized based on symptom severity, the patient's age, occupational or academic demands, and the presence of associated binocular vision anomalies.[17]
Optical Correction
The first step in treatment is to ensure that refractive errors are properly corrected. Even small degrees of uncorrected hyperopia can increase accommodative demand and exacerbate symptoms. Appropriate spectacle correction may significantly reduce accommodative strain. In patients with significant near-task symptoms, prescribing near addition lenses may be considered. Low-powered plus lenses (+0.50 to +1.00 D) are often prescribed for reading or prolonged near work to reduce accommodative demand. These lenses are particularly beneficial in children or adolescents who demonstrate reduced accommodative amplitude relative to age norms. Near addition lenses can also be incorporated into bifocal or progressive addition lenses in selected cases. The goal of optical correction is not to eliminate accommodation but to reduce the accommodative demand to a level that can be sustained comfortably.[26]
Vision Therapy
Vision therapy represents the primary treatment modality for accommodative insufficiency, particularly in symptomatic patients. Therapy programs aim to improve accommodative amplitude, facility, and endurance through structured exercises designed to stimulate the accommodative system. Common vision therapy techniques include:
- Lens flipper exercises, which train accommodative flexibility using alternating plus and minus lenses
- Near-far focusing exercises, where the patient alternates focus between near and distant targets
- Accommodative rock exercises are designed to improve rapid focusing ability
- Computer-based accommodative training programs
These exercises strengthen the accommodative response and improve neuromuscular coordination of the ciliary muscle. Therapy is typically conducted over several weeks under professional supervision, with supplementary home-based exercises. Please see StatPearls' companion reference, "Accommodative Insufficiency," for further information.
Management of Associated Binocular Vision Disorders
Accommodative insufficiency frequently coexists with convergence insufficiency or other vergence anomalies. In such cases, treatment must address both accommodative and vergence components. Vision therapy programs may incorporate convergence exercises, such as pencil push-ups, prism training, and stereoscopic activities, to improve binocular coordination.
Environmental and Behavioral Modifications
Lifestyle modifications play an important role in managing accommodative fatigue, especially in patients with heavy digital device use. Patients should be advised to adopt the 20-20-20 rule, which recommends taking a 20-second break every 20 minutes to look at an object at least 20 feet away. Proper lighting, ergonomic workstation setup, and appropriate reading distance (typically 35 to 40 cm) should also be emphasized. Reducing prolonged, continuous near work and encouraging periodic visual breaks helps prevent accommodative fatigue and enhances treatment outcomes.[22](B2)
Pharmacologic Therapy
Pharmacologic treatment is rarely required in accommodative insufficiency. However, in certain cases, low-dose parasympathomimetic agents, such as pilocarpine, have been investigated to stimulate the accommodative response. These agents are generally avoided because of potential adverse effects and limited long-term efficacy. Pharmacologic therapy is therefore not considered a routine treatment modality.
Management of Secondary Causes
When accommodative insufficiency arises secondary to systemic or neurologic disease, management should focus on addressing the underlying condition. For example:
- Optimization of blood glucose control
- Management of thyroid dysfunction or anemia
- Adjustment of medications with anticholinergic effects
Treating the underlying systemic condition may improve accommodative function.[88](A1)
Surgical Management
Surgical intervention has no role in the treatment of primary accommodative insufficiency. Because the disorder reflects functional neuromuscular insufficiency rather than structural abnormality, surgical procedures are not indicated. Surgical management is only relevant when accommodative symptoms arise secondary to other ocular conditions requiring operative treatment.
National and International Guidelines
Management strategies for accommodative insufficiency are guided by recommendations from professional organizations, including the American Optometric Association and the American Academy of Ophthalmology. These guidelines emphasize a comprehensive binocular vision evaluation followed by appropriate optical correction and structured vision therapy as first-line management. American Optometric Association clinical practice guidelines for accommodative and vergence dysfunction recommend:
- Accurate refractive correction
- Vision therapy to improve accommodative amplitude and facility
- Use of near addition lenses when appropriate
- Monitoring of binocular vision function during treatment
International orthoptic and binocular vision practice standards similarly recommend vision therapy as the most effective intervention for symptomatic accommodative insufficiency.[88](A1)
Treatment Outcome and Prognosis
With appropriate management, the prognosis for accommodative insufficiency is generally favorable. Most patients experience significant improvement in symptoms following vision therapy and appropriate optical correction. Early diagnosis and treatment are particularly important in children and adolescents, as untreated accommodative dysfunction may interfere with academic performance and reading efficiency.[17] Table 7 summarizes the treatment options available for accommodative insufficiency.
Table 7. Summary of Treatment Options
|
Treatment modality |
Purpose |
Clinical role |
|
Spectacle correction |
Correct refractive error |
First step in management |
|
Near addition lenses |
Reduce accommodative demand |
Useful for symptomatic near tasks |
|
Vision therapy |
Improve accommodative amplitude and flexibility |
Primary treatment |
|
Environmental modification |
Reduce visual fatigue |
Adjunctive management |
|
Pharmacologic agents |
Stimulate accommodation |
Rarely used |
|
Surgical treatment |
Not indicated |
No role in primary accommodative insufficiency |
In summary, the management of accommodative insufficiency centers on optical correction, structured vision therapy, and ergonomic visual habits. Adherence to established clinical guidelines ensures effective treatment and optimal visual function for patients experiencing accommodative difficulties.
Differential Diagnosis
Salient differential diagnosis remains key to clinical decision-making, subsequent management, and evaluation.[89] A diagnostic pearl is that accommodative insufficiency always presents with reduced AA. Patients with accommodative insufficiency tend to have difficulty stimulating accommodation, whereas patients with accommodative excess tend to have difficulty relaxing it.[90] Local or systemic diseases may contribute to accommodative paralysis, which is also characterized by a sharp reduction in AA. Drugs have also been shown to induce accommodative paralysis.[91]
Pseudoconvergence insufficiency is a key differential diagnosis of true convergence insufficiency. Pseudoconvergence insufficiency is considered a case of accommodative insufficiency with convergence insufficiency as a secondary finding. In true cases of convergence insufficiency, the near point of convergence is often receded or remote. However, measures of accommodation, such as the AA, are mostly within the reference range. In cases of convergence insufficiency, when an accommodative anomaly exists, there tends to be a compensatory accommodative excess. From a clinical perspective, repetition of the near point of convergence with +0.75 D or +1.00 D lenses may improve performance in cases of pseudoconvergence insufficiency. In contrast to accommodative insufficiency, prescribing higher plus lenses to patients with convergence insufficiency further reduces their accommodative convergence-to-accommodation ratio, making it more difficult for them to converge and worsening symptoms. In such cases, tailored vision therapy can be highly valuable.[73]
Certain ocular diseases, such as Adie tonic pupil, can present with symptoms mimicking accommodative insufficiency. Infectious conditions that produce neuropathological sequelae, like syphilis and meningitis, may also affect accommodative ability by disrupting the parasympathetic pathway.[92] Several drugs can also affect the accommodative triad and cause accommodative dysfunction.[57][93]
Accommodative insufficiency must be differentiated from several ocular and binocular vision disorders that produce similar symptoms of blurred near vision, asthenopia, headaches, and difficulty sustaining reading. Because accommodative insufficiency primarily manifests as reduced accommodative amplitude relative to age norms, careful clinical examination is required to distinguish it from other accommodative dysfunctions, vergence anomalies, refractive errors, and systemic conditions affecting near vision. Failure to correctly identify the underlying disorder may lead to inappropriate treatment and persistent symptoms. Table 8 summarizes the differential diagnosis of accommodative insufficiency.
Uncorrected or Latent Hyperopia
Uncorrected hyperopia is one of the most common conditions that may mimic accommodative insufficiency. Patients with hyperopia must accommodate even for distance vision, and additional accommodation is required for near tasks. This chronic accommodative demand may produce symptoms such as blurred near vision, headaches, and visual fatigue. However, accommodative amplitude in hyperopia is typically normal when measured accurately. Cycloplegic refraction is essential for identifying latent hyperopia and differentiating it from true accommodative insufficiency.[94]
Presbyopia
Presbyopia is an age-related decline in accommodative amplitude due to lenticular sclerosis and reduced capsular elasticity. Although both presbyopia and accommodative insufficiency present with reduced accommodative amplitude, presbyopia occurs physiologically after the fourth decade of life, whereas accommodative insufficiency occurs in younger individuals with amplitudes below age expectations. Age and lenticular biomechanics, therefore, play an important role in distinguishing between the 2 conditions.
Accommodative Excess
Accommodative excess, also referred to as accommodative spasm in severe cases, involves excessive or sustained contraction of the ciliary muscle. Patients often report blurred distance vision following near work, headaches, and difficulty focusing. Unlike accommodative insufficiency, accommodative excess is characterized by difficulty clearing plus lenses and may demonstrate lag of accommodation on dynamic retinoscopy. Distinguishing these conditions is important because treatment strategies differ significantly.[29]
Accommodative Infacility
Accommodative infacility is characterized by a reduced ability to shift focus between near and distant targets rapidly. While accommodative amplitude may be normal, patients demonstrate difficulty clearing both plus and minus lenses during accommodative facility testing. In contrast, accommodative insufficiency primarily affects amplitude and typically shows difficulty with minus lenses.
Ill-Sustained Accommodation
Ill-sustained accommodation is a related condition in which accommodative amplitude is initially normal but decreases after repeated near work due to fatigue. Symptoms may resemble those of accommodative insufficiency, but repeated amplitude measurements demonstrate progressive decline during testing. Accommodative insufficiency, by contrast, shows reduced baseline amplitude.[13]
Convergence Insufficiency
Convergence insufficiency is a common binocular vision disorder that may coexist with accommodative insufficiency. Patients present with near vision symptoms such as diplopia, eye strain, and headaches. However, the primary abnormality lies in reduced convergence ability rather than accommodative amplitude. Clinical findings include a receded near point of convergence and reduced positive fusional vergence at near.
Neurologic Conditions
Neurologic disorders affecting the oculomotor nerve or parasympathetic pathways may impair accommodation. Conditions such as partial third nerve palsy, traumatic brain injury, or midbrain lesions may produce reduced accommodative response. In these cases, additional neurologic signs such as ptosis, abnormal ocular motility, or pupillary abnormalities are often present.[94]
Systemic Disorders
Certain systemic diseases may produce symptoms resembling accommodative insufficiency. Diabetes mellitus with autonomic neuropathy, myasthenia gravis, and thyroid dysfunction can impair neuromuscular control of accommodation. A thorough systemic history and appropriate laboratory testing may be necessary when such conditions are suspected.
Ocular Surface Disease
Dry eye disease may cause fluctuating blur during near work and visual fatigue, which may mimic accommodative dysfunction. However, slit-lamp examination typically reveals tear-film abnormalities, while accommodative amplitude measurements are normal.[95]
Table 8. Differential Diagnosis Table
|
Condition |
Key clinical features |
Distinguishing findings |
|
Uncorrected hyperopia |
Near blur, headaches, eye strain |
Cycloplegic refraction reveals hyperopia |
|
Presbyopia |
Age-related near vision difficulty |
Occurs after age 40; lenticular sclerosis |
|
Accommodative excess |
Difficulty relaxing focus |
Lead of accommodation, difficulty clearing plus lenses |
|
Accommodative infacility |
Difficulty shifting focus |
Reduced facility with both plus and minus lenses |
|
Ill-sustained accommodation |
Fatigue after repeated near work |
Amplitude decreases during repeated testing |
|
Convergence insufficiency |
Diplopia, near eye strain |
Receded near point of convergence, reduced fusional vergence |
|
Neurologic disorders |
Visual disturbances with neurologic signs |
Abnormal ocular motility, pupillary changes |
|
Systemic disease (diabetes, MG) |
Variable accommodative weakness |
Associated systemic findings |
|
Dry eye disease |
Fluctuating blur, ocular discomfort |
Tear film abnormalities on slit-lamp exam |
Abbreviations: MG, myasthenia gravis.
Clinical Importance
Accurate differentiation of accommodative insufficiency from these conditions is essential because treatment approaches vary. While accommodative insufficiency typically responds well to vision therapy and near addition lenses, other conditions may require refractive correction, binocular vision therapy, systemic treatment, or neurologic evaluation. A comprehensive examination that incorporates accommodative amplitude testing, dynamic retinoscopy, binocular vision assessment, and systemic evaluation ensures an accurate diagnosis and effective treatment.[96]
Pertinent Studies and Ongoing Trials
Evidence-Based Treatment
The clinical evidence supporting the treatment of accommodative insufficiency is strongest for structured vergence and accommodative therapy (often delivered as office-based therapy with home reinforcement) and, separately, for low-plus near additions in selected patients. A recurring limitation of the literature is that many high-quality trials were designed primarily for convergence insufficiency but included prospectively measured accommodative outcomes in participants with concomitant accommodative dysfunction. A comprehensive review of accommodative insufficiency highlights that both vision therapy and low-plus lenses have demonstrated efficacy in independent studies, but direct comparative trials between these 2 approaches are limited or absent, leaving clinicians to individualize treatment based on the patient's symptom profile, accommodative measures, and context.[38]
Key Randomized and Controlled Evidence (Therapy Outcomes)
The Convergence Insufficiency Treatment Trial is frequently cited because it enrolled children with symptomatic convergence insufficiency and reported accommodative outcomes in a substantial subgroup with accommodative dysfunction measured using standardized protocols. In these studies, office-based vergence and accommodative therapy with home reinforcement produced greater improvements in accommodative amplitude and facility than placebo or certain home-based comparators, supporting the role of structured therapy when accommodative deficits coexist with symptoms. Beyond the Convergence Insufficiency Treatment Trial framework, smaller prospective clinical studies (not all accommodative insufficiency-specific) also report improvements in accommodative metrics (eg, accommodative lag and facility) following structured accommodative and vergence training programs, reinforcing biologic plausibility and clinical utility of therapy-based interventions.[97] Table 9 summarizes the key studies and results.
Guidelines
Consensus-based clinical guidance from the American Optometric Association emphasizes a structured binocular vision workup and supports optometric vision therapy and near plus lenses as treatment options for accommodative and vergence dysfunction, with treatment selection guided by measured deficits and symptoms.[98]
Table 9. Pertinent Studies Supporting Therapy Decisions in Accommodative Insufficiency
|
Study/resource |
Design/population |
Intervention(s) |
Outcomes most relevant to accommodative insufficiency |
Practical takeaway |
|
CITT accommodative outcomes (Scheiman et al) |
Randomized clinical trial framework in children with symptomatic CI; accommodative amplitude/facility collected in those with accommodative dysfunction |
OBVAT with home reinforcement vs placebo/other comparators |
Greater improvement in accommodative amplitude and facility in the OBVAT group vs placebo in the accommodative dysfunction subgroup |
Strongest clinical trial–level support for structured office-based vergence/accommodative therapy when accommodative deficits are present |
|
CITT trial design & core outcomes (CITT Study Group) |
Multicenter RCT evaluating active vs placebo/home-based approaches (CI primary); provides methodological rigor and standardized outcomes |
Office-based therapy (active) vs placebo; home-based comparators |
Demonstrates the feasibility of standardized measurement and clinically meaningful improvement patterns; accommodative outcomes reported in associated publications |
Reinforces therapy efficacy when delivered with adequate intensity and structure |
|
AAO review of vergence/accommodative therapies (Chang et al) |
Systematic review (children/young adults) focusing mainly on CI therapy, includes accommodative components in therapy |
Home- vs office-based accommodative/vergence approaches |
Summarizes therapy effectiveness patterns and limitations in evidence |
Useful to justify therapy choices in broader binocular dysfunction contexts; highlights evidence gaps |
|
AI literature review (Hussaindeen et al) |
Review specifically discussing AI prevalence/impact and treatment evidence |
Vision therapy; low plus lenses |
Notes efficacy signals for both; points out limited head-to-head comparisons |
Supports a balanced recommendation: therapy or low plus based on patient profile |
Abbreviations: AAO, American Academy of Ophthalmology; AI, accommodative insufficiency; CI, convergence insufficiency; CITT, Convergence Insufficiency Treatment Trial; RCT, randomized controlled clinical trial; OBVAT, office-based vergence and accommodative therapy.
Many randomized clinical trial–grade data on accommodative outcomes come from trials in which convergence insufficiency was the primary diagnosis, but accommodative dysfunction was measured prospectively. These data remain clinically useful because accommodative insufficiency and convergence insufficiency frequently coexist and share a near-work symptom burden.
Ongoing and Registered Trials Relevant to Accommodative Dysfunction and Insufficiency
ClinicalTrials.gov includes studies registered under accommodative disorders, accommodative dysfunction, and related visual training interventions. Some are not strictly isolated accommodative insufficiency trials but are relevant because they evaluate interventions that may modify accommodative performance.[98] Table 10 summarizes the ongoing clinical trials.
Table 10: Registered and Ongoing Trials
|
Trial/registry entry |
Focus |
Relevance to accommodative insufficiency |
|
NCT01329848 (Accommodation Disorders) |
Registered study under accommodation disorders |
Indicates ongoing research interest in accommodative conditions; details vary by status/protocol |
|
NCT06714890 (visual training + transcranial electrical stimulation) |
RCT combining neuromodulation with accommodation-related visual training |
Explores whether augmenting neural pathways can enhance training response—conceptually relevant to AI mechanisms |
|
NCT05107791 (accommodative training) |
Training-based intervention assessing accommodative outcomes |
Supports the training can change accommodation hypothesis; applicability depends on the inclusion criteria |
|
Trials in concussion/vergence domains (eg, CONCUSS RCT) |
Vergence/accommodative rehabilitation after head injury |
Relevant for secondary accommodative insufficiency (postconcussion accommodative deficits), though not limited to isolated accommodative insufficiency |
Treatment Planning
Treatment planning for accommodative insufficiency should be individualized, based on the severity of symptoms, the degree of accommodative deficit, the patient's age, occupational or academic visual demands, and the presence of associated binocular vision anomalies. The primary goals of treatment are to restore adequate accommodative function, improve visual comfort during near tasks, and enhance overall visual efficiency. Effective treatment planning requires a structured approach that integrates refractive correction, accommodative rehabilitation, and behavioral modifications while monitoring treatment response over time (see Table 11). Please see StatPearls' companion reference, "Convergence Insufficiency," for further information.
Initial Clinical Assessment
Treatment planning begins with confirmation of the diagnosis through comprehensive binocular vision testing. The clinician must evaluate accommodative amplitude relative to age norms, accommodative facility, accommodative response accuracy, and vergence function. Identification of associated conditions such as convergence insufficiency, accommodative infacility, or uncorrected refractive error is critical because these conditions may influence treatment strategy.[52] Patients should also be assessed for environmental factors that increase accommodative demand, including prolonged digital screen use, poor reading ergonomics, and excessive continuous near work.
Stepwise Treatment Approach
Management typically follows a stepwise approach beginning with correction of underlying refractive errors and progressing to accommodative rehabilitation when symptoms persist.
Refractive Correction
Any uncorrected refractive error, particularly hyperopia, should be corrected before initiating other therapies. Accurate refractive correction reduces unnecessary accommodative demand and helps clarify whether accommodative symptoms are primary or secondary to refractive stress.[99]
Near Addition Lenses
In patients with symptomatic accommodative insufficiency, particularly children or adolescents with sustained near visual tasks, low-powered plus lenses may be prescribed for near work. Near additions typically range from +0.50 to +1.00 D, depending on accommodative amplitude and symptom severity. These lenses reduce accommodative demand and improve reading comfort. Near additions may be prescribed as:
- Reading glasses
- Bifocal lenses
- Progressive addition lenses
The selection depends on patient age, visual habits, and adherence considerations.[100]
Vision Therapy
Vision therapy is considered the primary rehabilitative intervention for accommodative insufficiency. Structured therapy programs aim to improve accommodative amplitude, flexibility, and endurance through targeted exercises. Therapy may be conducted in the office, with supervised sessions combined with home-reinforcement exercises. Common therapy techniques include:
- Lens flipper training using alternating plus and minus lenses
- Near-far accommodative rock exercises
- Hart chart focusing activities
- Computer-based accommodative training programs
Vision therapy typically lasts 6 to 12 weeks, with progress monitored through repeated accommodative testing.[101]
Management of Associated Binocular Vision Disorders
When accommodative insufficiency occurs alongside convergence insufficiency or other vergence anomalies, treatment must address both accommodative and vergence components. Combined therapy programs often include convergence exercises such as pencil push-ups, stereograms, or prism-based training.
Visual Hygiene and Ergonomic Modifications
Behavioral modifications are an essential adjunct to treatment. Patients should be educated to maintain appropriate working distances and take regular visual breaks during prolonged near work. The 20-20-20 rule is commonly recommended, encouraging patients to look at an object 20 feet away for at least 20 seconds every 20 minutes. Proper workstation ergonomics, adequate lighting, and maintaining a reading distance of approximately 35 to 40 cm can reduce accommodative stress and improve treatment outcomes.[36]
Monitoring and Follow-Up
Patients undergoing treatment for accommodative insufficiency should be monitored periodically to assess improvement in accommodative amplitude and facility, as well as symptom reduction. Follow-up examinations typically occur every 4 to 6 weeks during therapy. Objective improvement in accommodative parameters combined with subjective symptom relief indicates successful treatment.
Special Considerations
In cases where accommodative insufficiency is secondary to systemic or neurologic conditions, management should include treatment of the underlying disorder. For example, optimizing glycemic control in patients with diabetes mellitus or addressing the adverse effects of medications may improve accommodative function.[102]
Table 11. Treatment Planning Algorithm
|
Step |
Intervention |
Clinical objective |
|
1 |
Comprehensive binocular vision evaluation |
Confirm diagnosis and identify associated disorders |
|
2 |
Correct refractive error |
Reduce accommodative demand |
|
3 |
Prescribe near addition lenses (if indicated) |
Improve near visual comfort |
|
4 |
Initiate vision therapy |
Improve accommodative amplitude and facility |
|
5 |
Address associated vergence disorders |
Restore binocular coordination |
|
6 |
Implement visual hygiene strategies |
Reduce accommodative fatigue |
|
7 |
Monitor progress and adjust therapy |
Ensure sustained improvement |
Prognosis with Treatment
With appropriate treatment planning and patient adherence, accommodative insufficiency generally has an excellent prognosis. Vision therapy, combined with proper optical correction, typically results in significant improvements in accommodative function and reductions in symptoms. Early identification and treatment are particularly important in children and adolescents because untreated accommodative dysfunction can adversely affect reading efficiency and academic performance.[97]
Toxicity and Adverse Effect Management
Management of accommodative insufficiency is generally safe because the primary therapeutic approaches—optical correction and vision therapy—are noninvasive. However, clinicians must remain aware of potential adverse effects associated with treatment modalities, including optical prescriptions, pharmacologic agents, and vision therapy exercises. Early identification and appropriate management of these adverse effects help ensure patient adherence and successful treatment outcomes.
Adverse Effects Related to Optical Correction
The prescription of near addition lenses is commonly used to reduce accommodative demand in symptomatic patients. Although generally well tolerated, some individuals may experience temporary visual discomfort upon introducing plus lenses. Common adverse effects include:
- Mild blurred vision when shifting focus between near and distance
- Adaptation difficulties with bifocal or progressive lenses
- Transient dizziness or visual distortion during the adaptation period
- Reduced accommodative stimulation if the addition power is excessive
Management strategies include careful titration of near addition power and gradual adaptation to new spectacles. Patient education regarding the expected adaptation period—typically a few days to one week—can improve adherence.[97]
Adverse Effects of Vision Therapy
Vision therapy exercises aim to enhance accommodative amplitude and flexibility. During early phases of therapy, patients may experience temporary symptoms as the accommodative system is being stimulated (see Table 12). Reported adverse effects include:
- Temporary eye strain
- Headaches following therapy sessions
- Blurred vision after prolonged exercises
- Mild diplopia during binocular training activities
These symptoms usually resolve as the accommodative system adapts. If symptoms persist, therapy intensity may be reduced or exercises modified to prevent excessive accommodative stress.
Pharmacologic Therapy and Associated Toxicity
Pharmacologic agents are rarely used to treat accommodative insufficiency. However, parasympathomimetic medications such as pilocarpine have occasionally been investigated to stimulate accommodation by increasing ciliary muscle contraction. Potential adverse effects of these medications include:
- Brow ache
- Induced myopia
- Reduced night vision due to miosis
- Risk of retinal detachment in predisposed individuals
- Increased lacrimation and ocular irritation [101]
Because of these potential adverse effects and limited long-term benefit, pharmacologic therapy is generally not recommended as a routine treatment modality for AI.
Systemic Medication–Induced Accommodative Dysfunction
Some medications can impair accommodation by affecting parasympathetic neurotransmission. Anticholinergic drugs, antihistamines, tricyclic antidepressants, and certain antipsychotics may reduce accommodative amplitude. In such cases, management involves reviewing the patient’s medication history and coordinating with the prescribing clinician to consider dose adjustment or alternative medications when appropriate.[103]
Toxicologic Considerations
Exposure to certain toxins, particularly organophosphate compounds, may initially cause accommodative spasm followed by accommodative fatigue. Patients with suspected toxic exposure should undergo systemic evaluation and appropriate toxicologic management. Treatment of the underlying toxic exposure usually improves accommodative function.[104]
Monitoring and Follow-Up
Patients undergoing treatment for accommodative insufficiency should be evaluated periodically to ensure that therapy is effective and free of significant adverse effects. Follow-up assessments typically include measurement of accommodative amplitude and accommodative facility, as well as evaluation of patient-reported symptoms. Clinicians should remain vigilant for signs suggesting alternative diagnoses, such as persistent visual symptoms despite appropriate therapy or new neurologic findings. In such situations, additional diagnostic evaluation may be warranted.
Table 12. Summary of Adverse Effects and Management
|
Treatment modality |
Potential adverse effects |
Management strategy |
|
Near addition lenses |
Adaptation difficulty, blurred distance vision |
Adjust lens power and allow an adaptation period |
|
Vision therapy |
Eye strain, headaches, transient blur |
Modify therapy intensity and provide rest intervals |
|
Pharmacologic agents |
Brow ache, induced myopia, and reduced night vision |
Avoid routine use; discontinue if adverse effects occur |
|
Systemic medications |
Reduced accommodative amplitude |
Review medications and adjust therapy if possible |
|
Toxic exposure |
Accommodative dysfunction secondary to toxins |
Treat the underlying toxicologic condition |
Clinical Significance
Overall, the treatment of accommodative insufficiency has a favorable safety profile, with most adverse effects being mild and temporary. Proper patient education, careful monitoring, and individualized treatment planning help minimize complications and improve therapeutic outcomes.[17]
Staging
Accommodative insufficiency is primarily a functional binocular vision disorder and, unlike many structural ocular diseases, lacks a universally accepted staging system. However, for clinical and research purposes, accommodative insufficiency can be graded by the severity of accommodative amplitude reduction, symptom intensity, and functional impact on near-vision tasks. This type of staging helps clinicians determine treatment urgency, select appropriate therapeutic interventions, and monitor response to therapy. In clinical practice, staging is generally based on the degree of reduction in accommodative amplitude relative to age-expected norms, commonly calculated using the Hofstetter formula. Additional parameters such as accommodative facility, accommodative lag, and symptom severity also contribute to disease grading (see Table 13).[105]
Stage 1: Mild Accommodative Insufficiency
Mild accommodative insufficiency is characterized by a slight reduction in accommodative amplitude, usually close to but below the minimum expected value for age. Patients may experience occasional visual fatigue during prolonged near tasks such as reading or computer work. Symptoms are generally intermittent and improve with rest. Accommodative facility may show minimal reduction, and dynamic retinoscopy may reveal a mild lag of accommodation. This stage is often detected during routine binocular vision evaluation or early symptom assessment. Treatment may involve simple measures such as correcting refractive error, implementing visual hygiene strategies, and monitoring, without aggressive intervention.[100]
Stage 2: Moderate Accommodative Insufficiency
In moderate accommodative insufficiency, patients typically have an accommodative amplitude more than 2 diopters below age-expected norms. Patients frequently report symptoms during near work, including blurred vision, headaches, eye strain, and difficulty maintaining focus while reading. Accommodative facility testing often demonstrates reduced ability to clear minus lenses, and dynamic retinoscopy reveals a noticeable accommodative lag. At this stage, active treatment is usually recommended. Management may include near addition lenses combined with structured vision therapy exercises aimed at improving accommodative flexibility and endurance.[13]
Stage 3: Severe Accommodative Insufficiency
Severe accommodative insufficiency is characterized by a marked reduction in accommodative amplitude, with persistent symptoms even during short periods of near work. Patients may experience constant near-vision blur, reduced reading endurance, and significant visual fatigue. Accommodative facility is markedly impaired, and accommodative lag is often substantial. In severe cases, accommodative insufficiency may be associated with other binocular vision anomalies such as convergence insufficiency. Treatment typically requires comprehensive vision therapy, optical correction with near additions, and close follow-up to monitor progress.[106]
Functional Classification Based on Accommodative Performance
An alternative approach to staging focuses on functional accommodative performance, particularly accommodative amplitude and facility. This classification helps guide treatment selection and monitor therapeutic response.
Table 13. Stages of Accommodative Insufficiency
|
Stage |
Clinical Features |
Accommodative findings |
Typical treatment |
|
Mild accommodative insufficiency |
Occasional near visual fatigue |
Slight reduction in accommodative amplitude |
Visual hygiene, refractive correction |
|
Moderate accommodative insufficiency |
Frequent symptoms during near tasks |
Amplitude ≥2 D below age norms; reduced facility |
Near addition lenses, vision therapy |
|
Severe accommodative insufficiency |
Persistent near blur and asthenopia |
Markedly reduced amplitude and facility |
Intensive vision therapy and optical support |
Clinical Significance of Staging
Although accommodative insufficiency lacks a universally standardized staging system, grading the condition based on accommodative performance and symptom severity is clinically valuable. Staging helps determine the most appropriate treatment strategy, predict prognosis, and track improvements during therapy. Early identification and intervention in mild cases may prevent progression to more severe accommodative dysfunction and reduce the impact on academic or occupational performance.[17]
Monitoring Disease Progression
Follow-up evaluation should include repeated measurements of accommodative amplitude and accommodative facility, as well as symptom assessment. Improvement in accommodative parameters following treatment indicates successful rehabilitation, whereas persistent deficits may require therapy modification or evaluation for underlying systemic conditions.[17]
Prognosis
The prognosis of accommodative insufficiency can be variable; the most important prognostic factor is proper diagnosis and therapeutic management of this visual syndrome. The prognosis of accommodative insufficiency is generally favorable, particularly when the condition is diagnosed early and managed appropriately. Because accommodative insufficiency primarily reflects a functional deficit of the accommodative system rather than a structural abnormality of the eye, most patients respond well to conservative treatment strategies, including optical correction, accommodative rehabilitation through vision therapy, and appropriate visual hygiene practices. The likelihood of recovery depends on factors including the patient’s age, severity of accommodative dysfunction, adherence to treatment protocols, and the presence of associated binocular vision anomalies or systemic conditions.[107]
In children and adolescents, the prognosis is typically excellent. The accommodative system in younger individuals retains considerable plasticity, and structured vision therapy programs can significantly improve accommodative amplitude, facility, and endurance. Early intervention in school-aged children is particularly important because accommodative insufficiency may negatively affect reading performance, academic productivity, and sustained near work. When treatment is initiated promptly, and patients adhere to therapy protocols, most children demonstrate substantial improvement in both objective accommodative measures and subjective symptoms. Please see StatPearls' companion reference, "Astigmatism," for further information.
Young adults also tend to respond favorably to treatment. In this age group, accommodative insufficiency is often associated with prolonged use of digital devices or high near-visual demands. With appropriate management, including ergonomic adjustments, vision therapy exercises, and occasional near addition lenses, symptoms usually improve within several weeks to months. Long-term visual outcomes are generally good, and recurrence is uncommon when proper visual habits are maintained. Please see StatPearls' companion reference, "Contact Lenses for Presbyopia," for further information.
The prognosis may be more variable in cases where accommodative insufficiency is secondary to systemic or neurologic conditions. Disorders such as diabetes mellitus, autonomic neuropathy, traumatic brain injury, or medication-induced accommodative dysfunction may impair the neural pathways involved in accommodation. In these situations, the prognosis depends largely on the successful management of the underlying systemic condition. Improvement in accommodative function may occur once the primary disorder is treated or stabilized. Please see StatPearls' companion reference, "Autorefractors," for further information.
In patients with coexisting binocular vision anomalies, such as convergence insufficiency, the prognosis remains favorable when both accommodative and vergence components are addressed simultaneously. Combined therapy programs targeting both systems often lead to significant symptomatic relief and improvement in visual performance. Please see StatPearls' companion reference, "Phacoemulsification," for further information. Treatment adherence is an important determinant of prognosis. Vision therapy requires patient motivation and consistent participation in both office-based and home-based exercises. Patients who maintain regular therapy schedules generally demonstrate faster and more sustained improvements in accommodative performance. Long-term complications of accommodative insufficiency are uncommon. However, if left untreated, persistent accommodative dysfunction may lead to chronic asthenopia, reduced reading efficiency, decreased academic or occupational productivity, and increased visual fatigue during prolonged near work.[108]
Prognostic Factors
Several factors influence the prognosis of accommodative insufficiency (see Table 14).
Table 14: Prognosis of Accommodative Insufficiency
|
Factor |
Influence on prognosis |
|
Age of the patient |
Younger patients generally have better recovery due to greater accommodative plasticity |
|
Severity of accommodative deficit |
Mild to moderate cases respond more rapidly to therapy |
|
Presence of associated binocular vision disorders |
Requires combined treatment, but still has a favorable outcome |
|
Patient compliance with therapy |
Strong determinant of treatment success |
|
Underlying systemic disease |
May limit or delay recovery |
|
Duration of symptoms before treatment |
Early treatment improves outcomes |
Expected Outcomes with Treatment
Clinical studies and observational data indicate that most patients undergoing structured accommodative therapy demonstrate measurable improvements in accommodative amplitude and facility within 6 to 12 weeks of treatment. Symptom reduction often occurs earlier as accommodative endurance improves. Long-term follow-up suggests that once normal accommodative function is restored, recurrence is uncommon if appropriate visual hygiene and ergonomic practices are maintained.[13]
Overall Prognosis
Overall, accommodative insufficiency carries an excellent prognosis when appropriately managed. The majority of patients experience significant improvement in visual comfort and near-task performance with conservative treatment approaches. Early recognition, comprehensive evaluation, and individualized treatment planning remain key factors in ensuring optimal visual outcomes.[100]
Complications
As with other binocular vision anomalies, accommodative insufficiency can result in functional limitations among affected patients without proper treatment. Functional consequences may be social, such as poor academic performance among children with an unidentified accommodative deficit.[36] Accommodative insufficiency is primarily a functional disorder of the accommodative system characterized by reduced ability of the eye to maintain clear focus on near objects. Although the condition itself is not typically associated with permanent structural ocular damage, untreated or poorly managed accommodative insufficiency can lead to several functional, educational, and visual complications (see Table 15). These complications mainly arise from persistent visual strain during near tasks and the compensatory mechanisms patients adopt to overcome inadequate accommodation.[32]
Visual Fatigue and Asthenopia
One of the most common complications of accommodative insufficiency is chronic visual fatigue, also known as asthenopia. Patients often experience persistent eye strain during activities that require prolonged near focus, such as reading, writing, or computer work. Chronic eye strain can manifest as discomfort around the eyes, blurred vision, and headaches, particularly in the frontal or periocular region. If the condition remains untreated, these symptoms may become chronic and interfere with daily activities. Please see StatPearls' companion reference, "Esotropia," for further information.
Reduced Reading Efficiency
Accommodative insufficiency can significantly impair reading performance and comprehension, especially in children and students. Difficulty maintaining clear focus on near text may result in slower reading speed, skipping lines, losing place on the page, or needing to reread passages. Over time, reduced reading efficiency can negatively affect academic performance and learning efficiency.[109]
Headaches
Recurrent headaches are frequently reported in patients with accommodative insufficiency, particularly after prolonged near work. These headaches typically occur in the frontal or supraorbital region and may worsen during activities requiring sustained visual concentration. Persistent headaches may lead patients to avoid near tasks, thereby affecting productivity and educational performance.[66]
Binocular Vision Dysfunction
Because accommodation and convergence are closely linked through the accommodative convergence-to-accommodation (AC/A) relationship, accommodative insufficiency may contribute to secondary binocular vision anomalies, particularly convergence insufficiency. Patients may experience intermittent diplopia, difficulty maintaining binocular fusion during near tasks, or reduced stereoscopic vision.[16]
Visual Avoidance Behavior
Children with untreated accommodative insufficiency may develop behavioral adaptations such as avoiding reading, reducing study time, or preferring activities that require minimal near visual effort. These behaviors may sometimes be misinterpreted as a lack of attention, learning disorders, or motivational issues.[100]
Academic and Occupational Impact
Persistent accommodative dysfunction can adversely affect academic performance in school-aged children and occupational efficiency in adults. Professions that involve prolonged near work, such as computer-based tasks, reading-intensive work, or detailed manual activities, may be particularly affected.[46]
Digital Eye Strain
With increasing use of smartphones, tablets, and computers, accommodative insufficiency may contribute to digital eye strain syndrome. Patients may report blurred vision, difficulty focusing after prolonged screen use, dryness, and ocular discomfort.[66]
Psychological Impact
Chronic visual discomfort and reduced productivity may lead to frustration, decreased confidence in academic abilities, and increased stress. In pediatric populations, this may occasionally be mistaken for behavioral or cognitive problems.[110]
Table 15. Complications of Accommodative Insufficiency
|
Complication |
Clinical manifestation |
Mechanism |
|
Asthenopia |
Eye strain, ocular discomfort |
Increased effort to maintain near focus |
|
Blurred near vision |
Difficulty sustaining clear near vision |
Reduced accommodative amplitude |
|
Headaches |
Frontal or periocular headaches |
Continuous accommodative stress |
|
Reduced reading performance |
Slow reading, skipping lines |
Inability to maintain sustained focus |
|
Convergence insufficiency |
Diplopia or poor binocular fusion |
Disruption of the accommodation–convergence relationship |
|
Academic difficulties |
Reduced study efficiency in children |
Visual fatigue during reading |
|
Digital eye strain |
Blurred vision and ocular fatigue with screen use |
Prolonged near visual demand |
|
Visual avoidance behavior |
Avoidance of reading or near tasks |
Compensatory adaptation to visual discomfort |
Clinical Significance
Although accommodative insufficiency rarely causes permanent ocular damage, its functional consequences can significantly affect quality of life, particularly in children and individuals with high near visual demands. Early diagnosis and appropriate management, including vision therapy, refractive correction, and visual hygiene strategies, can prevent the development of these complications and restore comfortable near vision. Please see StatPearls' companion reference, "Microspherophakia," for further information.
Postoperative and Rehabilitation Care
Accommodative insufficiency is primarily a functional disorder and generally does not require surgical intervention. Therefore, the concept of postoperative care is not directly applicable in most cases. However, postoperative considerations may arise when accommodative insufficiency occurs secondary to ocular surgical procedures, neurologic injury, or trauma, or when patients develop accommodative dysfunction following procedures that affect the ocular accommodative apparatus. In these situations, postoperative and rehabilitative care focus on restoring accommodative function, reducing visual symptoms, and improving near visual performance through structured rehabilitation strategies (see Table 16).[51]
Postoperative Considerations
In certain clinical scenarios, accommodative insufficiency may develop following ocular procedures, such as refractive or intraocular surgical procedures, or neurologic interventions that affect the accommodative pathways. Postoperative accommodative dysfunction may result from transient ciliary muscle fatigue, altered neural control of accommodation, or changes in refractive status. Patients may report symptoms such as blurred near vision, difficulty focusing during reading, eye strain, or headaches after a surgical procedure. These symptoms should be carefully evaluated to distinguish transient postoperative adaptation from persistent accommodative dysfunction.[111]
Early Postoperative Evaluation
Following ocular surgery, patients presenting with near vision complaints should undergo a comprehensive binocular vision assessment. The evaluation typically includes:
- Measurement of distance and near visual acuity
- Refraction to detect residual refractive error
- Assessment of accommodative amplitude
- Dynamic retinoscopy to evaluate accommodative response
- Binocular vision testing, including convergence assessment
Early identification of accommodative dysfunction allows clinicians to initiate timely rehabilitation strategies and prevent long-term visual discomfort.[110]
Optical Rehabilitation
Optical correction remains a key component of postoperative management when accommodative insufficiency is identified. Low-powered near addition lenses may be prescribed temporarily to reduce accommodative demand during near tasks. These lenses help alleviate symptoms while the accommodative system gradually recovers or adapts following a surgical procedure. Near addition lenses may be prescribed in the form of:
- Reading glasses
- Bifocal spectacles
- Progressive addition lenses
The choice of optical correction depends on patient age, visual demands, and refractive status. Please see StatPearls' companion reference, "Blunt Eye Trauma," for further information.
Vision Therapy and Rehabilitation
Vision therapy plays a crucial role in rehabilitating accommodative function following a surgical procedure or neurologic injury. Structured accommodative training exercises help restore ciliary muscle responsiveness and improve accommodative flexibility. Common rehabilitation exercises include:
- Lens flipper exercises to improve accommodative facility
- Near-far focusing exercises to enhance accommodative response
- Hart chart training for accommodative endurance
- Computer-based visual training programs
These exercises stimulate the accommodative system and promote neuromuscular adaptation, allowing patients to regain comfortable near vision. Please see StatPearls' companion reference, "Artificial Corneal Tranplantation," for further information.
Visual Ergonomics and Behavioral Strategies
Patients recovering from accommodative dysfunction should be advised to adopt proper visual habits. Recommended strategies include maintaining an appropriate reading distance, ensuring adequate lighting during near tasks, and taking regular visual breaks to prevent accommodative fatigue. The 20-20-20 rule is commonly recommended during rehabilitation: every 20 minutes of near work should be followed by a 20-second break while focusing on an object at least 20 feet away.
Monitoring Recovery
Patients undergoing accommodative rehabilitation should be monitored periodically to assess improvement in accommodative parameters and symptom resolution. Follow-up visits may include repeat measurement of accommodative amplitude, accommodative facility, and dynamic retinoscopy findings. Improvement in accommodative function typically occurs gradually over several weeks of therapy. In most cases, visual comfort improves as accommodative endurance increases.
Interdisciplinary Rehabilitation
In cases where accommodative insufficiency occurs following neurologic injury, such as traumatic brain injury or cranial nerve involvement, interdisciplinary rehabilitation may be required. Collaboration between ophthalmologists, optometrists, neurologists, and vision therapists can help optimize recovery.[102]
Table 16. Postoperative and Rehabilitation Strategies
|
Rehabilitation component |
Purpose |
Clinical role |
|
Postoperative binocular vision assessment |
Identify accommodative dysfunction |
Early diagnosis |
|
Optical correction |
Reduce accommodative demand |
Symptom relief |
|
Vision therapy |
Restore accommodative amplitude and flexibility |
Functional rehabilitation |
|
Visual hygiene strategies |
Prevent accommodative fatigue |
Supportive management |
|
Regular follow-up |
Monitor recovery and adjust therapy |
Ensure sustained improvement |
Prognosis Following Rehabilitation
With appropriate rehabilitation strategies, most patients with accommodative insufficiency following surgical procedures or neurologic injury demonstrate gradual improvement in accommodative function. Early recognition and targeted therapy significantly enhance recovery and help restore comfortable near vision.
Consultations
Accommodative insufficiency is primarily a functional binocular vision disorder, but optimal patient care may require interdisciplinary consultation, depending on the underlying etiology, symptom severity, and associated systemic or neurologic conditions. Consultation with appropriate health care professionals ensures accurate diagnosis, comprehensive management, and improved visual outcomes (see Table 17).
Ophthalmology Consultation
Ophthalmologists play a central role in the evaluation and management of accommodative insufficiency. Consultation is particularly important for performing a comprehensive ocular examination and for excluding structural ocular diseases that may mimic accommodative dysfunction. The ophthalmologist assesses refractive status, binocular vision function, accommodative amplitude, and ocular health using slit-lamp examination and dilated fundus evaluation.[112] Ophthalmologic consultation is especially warranted when patients present with atypical symptoms, reduced visual acuity unexplained by refractive error, or signs suggesting retinal or neurologic pathology.
Optometry and Vision Therapy Specialists
Optometrists and orthoptists with expertise in binocular vision disorders are often involved in the management of accommodative insufficiency. These specialists provide specialized testing of accommodative amplitude, accommodative facility, and vergence function. Vision therapy programs designed to improve accommodative flexibility and endurance are frequently supervised by optometrists trained in binocular vision rehabilitation. Regular follow-up with vision therapy specialists helps monitor treatment response and adjust therapy protocols based on patient progress.[113]
Neurology Consultation
Neurology consultation may be necessary when accommodative insufficiency is suspected to be secondary to neurologic disorders. Conditions such as traumatic brain injury, multiple sclerosis, cranial nerve palsy, or midbrain lesions may impair neural control of accommodation. Patients presenting with additional neurologic symptoms, including diplopia, ptosis, abnormal pupillary responses, or ocular motility abnormalities, should undergo neurologic evaluation. Neuroimaging studies may be recommended if central nervous system pathology is suspected. Please see StatPearls' companion reference, "Charles Bonnet Syndrome," for further information.
Pediatric Consultation
For pediatric patients, consultation with pediatricians or pediatric ophthalmologists may be beneficial, particularly when accommodative insufficiency affects academic performance or reading development. Pediatric specialists can help differentiate visual causes of learning difficulties from cognitive or developmental disorders. Collaboration between ophthalmologists, pediatricians, and educators may be necessary to ensure appropriate academic support for children.[114]
Endocrinology and Internal Medicine Consultation
Systemic conditions such as diabetes mellitus, thyroid dysfunction, and autonomic neuropathies may impair accommodative function. In such cases, consultation with endocrinologists or internal medicine specialists is important to manage the underlying systemic disease. Improved systemic control often leads to improvement in accommodative function.[115]
Occupational and Vision Rehabilitation Specialists
Patients whose occupations require prolonged near work, such as computer-based professions, may benefit from consultation with occupational health specialists or vision rehabilitation professionals. These specialists can provide guidance on workplace ergonomics, visual hygiene strategies, and environmental modifications to reduce accommodative stress.[116]
Psychological or Educational Consultation
For children with persistent academic difficulties due to visual fatigue, consultation with educational specialists or psychologists may be helpful. Visual dysfunction can sometimes be misinterpreted as attention or learning disorders. Identifying and treating accommodative insufficiency can significantly improve academic engagement and performance.[117]
Table 17: Interdisciplinary Consultations in Accommodative Insufficiency
|
Specialist |
Role in management |
Clinical indications |
|
Ophthalmologist |
Comprehensive ocular examination and diagnosis |
Suspected ocular pathology |
|
Optometrist orthoptist |
Binocular vision testing and vision therapy |
Symptomatic accommodative dysfunction |
|
Neurologist |
Evaluation of neurologic causes |
Diplopia, cranial nerve abnormalities |
|
Pediatrician/ pediatric ophthalmologist |
Assessment in children |
Academic or developmental concerns |
|
Endocrinologist/Internist |
Management of systemic disease |
Diabetes, thyroid disorders |
|
Occupational health specialist |
Workplace visual ergonomics |
High near visual demand occupations |
|
Educational psychologist |
Academic performance evaluation |
Learning or attention difficulties |
Clinical Significance
Consultation with appropriate specialists ensures that accommodative insufficiency is accurately diagnosed and effectively managed. An interdisciplinary approach helps identify underlying causes, implement targeted therapies, and optimize patient outcomes, particularly in complex or refractory cases.[118]
Deterrence and Patient Education
Patients with AI, particularly those with latent hyperopia, may become discouraged from wearing their spectacles regularly. Parents may express dissatisfaction with the recommendation of bifocal lenses for their children. Thorough approaches that encourage patient adherence and family support are crucial.[36] Patient education plays a crucial role in the management and prevention of accommodative insufficiency (see Table 18). Since accommodative insufficiency is commonly associated with prolonged near work, digital device use, and visual fatigue, educating patients about appropriate visual habits and ergonomic practices can significantly reduce symptoms and prevent recurrence. Effective patient education also enhances treatment adherence, particularly in individuals undergoing vision therapy or using optical correction for near tasks. Please see StatPearls' companion reference, "Cytomegalovirus Corneal Endotheliitis," for further information.
Patient Awareness
Patients should be informed that accommodative insufficiency is a functional disorder of the eye’s focusing mechanism, in which the eye has difficulty maintaining clear focus on near objects for prolonged periods. Unlike structural eye diseases, accommodative insufficiency usually responds well to conservative management strategies such as vision therapy, corrective lenses, and proper visual hygiene. Understanding the nature of the condition helps reduce patient anxiety and encourages adherence to recommended treatment protocols.[119]
Visual Hygiene Practices
Adopting proper visual habits is essential for reducing accommodative strain and preventing symptom worsening. Patients should be educated about maintaining appropriate working distances during near tasks. Reading material should ideally be held at a distance of approximately 35 to 40 cm to allow the accommodative system to function comfortably. Adequate lighting is also important when performing near visual activities. Poor illumination increases accommodative effort and may exacerbate visual fatigue. Please see StatPearls' companion reference, "Salzmann Nodular Corneal Degeneration," for further information.
The 20-20-20 Rule
One of the most effective preventive strategies for accommodative fatigue is the 20-20-20 rule. Patients should be encouraged to take a brief visual break every 20 minutes during near work by looking at an object at least 20 feet away for 20 seconds. The 20-20-20 rule allows the accommodative system to relax and reduces the risk of sustained accommodative stress.[66]
Limiting Digital Device Use
Excessive use of smartphones, tablets, and computers can increase accommodative demand and contribute to digital eye strain. Patients should be advised to limit prolonged continuous screen use and to take regular breaks when using digital devices. Adjusting screen brightness, maintaining an appropriate viewing distance, and ensuring ergonomic workstation setup can also reduce visual fatigue. [66]
Compliance With Vision Therapy
Patients undergoing vision therapy should be educated about the importance of consistent participation in prescribed exercises. Vision therapy programs aim to strengthen the accommodative system and improve focusing flexibility. Regular practice of therapy exercises at home, in addition to supervised sessions, is essential for achieving optimal outcomes. Parents of pediatric patients should be encouraged to monitor adherence to therapy and support their children in completing prescribed exercises.[120]
Proper Use of Optical Correction
When near addition lenses or reading glasses are prescribed, patients should be instructed in their proper use. These lenses should be worn during activities that require prolonged near focus, such as reading, studying, or computer work. Patients should also understand that these lenses are designed to reduce accommodative demand and improve visual comfort.
Lifestyle and General Health Measures
General health factors may influence accommodative function. Patients should be encouraged to maintain a healthy lifestyle, including adequate sleep, balanced nutrition, and regular physical activity. Conditions such as diabetes mellitus or thyroid disorders should be well controlled, because systemic diseases may affect the neural pathways involved in accommodation.[121]
Education in Pediatric Populations
Parents and teachers should be informed about the potential impact of accommodative insufficiency on reading performance and academic activities. Early recognition of symptoms, such as frequent eye rubbing, avoidance of reading, or concerns of blurred near vision, can prompt timely evaluation and treatment. Collaboration between healthcare professionals, parents, and educators helps ensure that children receive appropriate visual support in educational environments.[122]
Table 18. Key Patient Education Strategies for Accommodative Insufficiency
|
Education topic |
Key recommendations |
Clinical benefit |
|
Visual hygiene |
Maintain reading distance of 35–40 cm |
Reduces accommodative strain |
|
20-20-20 rule |
Break every 20 minutes, look at a distant object |
Prevents accommodative fatigue |
|
Digital device use |
Limit prolonged screen time |
Reduces digital eye strain |
|
Vision therapy compliance |
Perform exercises regularly |
Improves accommodative function |
|
Proper spectacle use |
Wear near additions for reading tasks |
Enhances visual comfort |
|
Healthy lifestyle |
Adequate sleep and systemic disease control |
Supports neural visual function |
Clinical Significance
Patient education is a critical component of the long-term management of accommodative insufficiency. By promoting healthy visual habits and encouraging adherence to treatment strategies, health care professionals can significantly reduce symptoms, improve visual performance, and prevent recurrence of accommodative dysfunction.
Pearls and Other Issues
Accommodative insufficiency is a common yet frequently underdiagnosed binocular vision disorder. Although the disorder is typically benign and highly responsive to conservative management, failure to recognize or appropriately manage the condition can lead to persistent visual discomfort and reduced functional performance. The following section outlines key clinical pearls, potential pitfalls, disposition strategies, and preventive considerations relevant to accommodative insufficiency.
Clinical Pearls
One of the most important clinical pearls is that accommodative insufficiency should always be suspected in patients with normal distance visual acuity but persistent near visual symptoms, especially eye strain, headaches, and difficulty sustaining focus during reading. Accurate diagnosis requires a comprehensive binocular vision assessment, including measurements of accommodative amplitude and accommodative facility, as well as dynamic retinoscopy. Relying solely on refractive correction may result in a missed diagnosis.
Accommodative insufficiency often coexists with convergence insufficiency. Therefore, accommodation and vergence systems should always be evaluated together because of their physiologic linkage.Vision therapy remains the most effective long-term rehabilitative approach. While near addition lenses provide symptomatic relief, they do not necessarily restore accommodative strength unless combined with rehabilitative exercises. Furthermore, early detection in children is particularly important because accommodative insufficiency may masquerade as reading difficulty, attention problems, or academic underperformance.[69]
Common Pitfalls
Several pitfalls may lead to misdiagnosis or suboptimal management:
- Attributing symptoms solely to refractive error: Patients with persistent near symptoms despite appropriate refractive correction should be evaluated for accommodative dysfunction.
- Failure to evaluate the accommodative facility: Measuring amplitude alone may overlook reduced flexibility of accommodation.
- Overprescription of near additions: Excessive plus power may reduce accommodative stimulation and potentially delay rehabilitation.
- Ignoring systemic or neurologic causes: Sudden-onset accommodative insufficiency in adults should prompt evaluation for neurologic or systemic disease.
- Poor patient adherence with vision therapy: Inconsistent participation in therapy exercises significantly reduces treatment success.[105]
Disposition
Most patients with accommodative insufficiency can be managed on an outpatient basis with conservative measures. Referral to subspecialists is recommended in the following circumstances:
- Presence of neurologic signs or symptoms
- Suspected systemic disease affecting accommodation
- Persistent symptoms despite appropriate therapy
- Associated with significant binocular vision disorders requiring specialized management
Patients should be monitored periodically to assess improvement in accommodative amplitude and facility, as well as symptom resolution. Discontinuation of therapy may be considered once accommodative function normalizes and symptoms resolve. Please see StatPearls' companion reference, "Astigmatism," for further information.
Prevention Strategies
While accommodative insufficiency cannot always be prevented, several measures may reduce its incidence or recurrence:
- Encouraging regular visual breaks during prolonged near work
- Maintaining appropriate reading distance and posture
- Limiting excessive continuous digital screen use
- Ensuring adequate lighting during near tasks
- Early evaluation of children with reading complaints
- Managing systemic conditions that may impair accommodative function
Adopting these preventive strategies is particularly important in the modern digital environment, where prolonged near visual demands are increasingly common. Please see StatPearls' companion reference, "Contact Lenses for Presbyopia," for further information.
Additional Considerations
Accommodative insufficiency may fluctuate with fatigue, stress, or systemic illness. Clinicians should consider these factors when evaluating symptom variability. Additionally, patients with traumatic brain injury frequently demonstrate accommodative dysfunction, and targeted rehabilitation may significantly improve visual comfort and quality of life. In pediatric populations, collaboration with educators can be beneficial because appropriate classroom accommodations, such as scheduled visual breaks, may enhance academic performance during treatment.
Table 18. Pearls and Other Issues
|
Category |
Key Points |
|
Clinical pearls |
Evaluate accommodation and vergence together; early detection improves outcomes |
|
Pitfalls |
Misdiagnosis as refractive error alone; overreliance on near additions |
|
Disposition |
Mostly outpatient; refer if neurologic or systemic causes are suspected |
|
Prevention |
Visual hygiene, ergonomic adjustments, and digital screen moderation |
|
Additional issues |
Consider systemic disease, stress, and neurologic injury |
Overall Clinical Insight
Accommodative insufficiency is a manageable and highly treatable functional visual disorder. Awareness of clinical pearls, avoidance of common pitfalls, and emphasis on preventive strategies significantly improve patient outcomes. With proper evaluation and individualized treatment, most patients experience substantial improvement in visual comfort and near task performance.
Enhancing Healthcare Team Outcomes
Accommodative and vergence dysfunction can sometimes be indicative of a potentially debilitating disease. Please see StatPearls' companion reference, "Foster Kennedy Syndrome," for further information. Individuals with signs and symptoms of accommodative insufficiency, especially those with a prior history of systemic vascular and autoimmune disease or those with acute neurologic deficits, must be thoroughly assessed by clinicians.[123] Patients may require interdisciplinary treatment, including evaluation and testing for neurologic, hematologic, pathologic, and infectious diseases (see Table 19). Important signs and symptoms to consider, especially during triage, include persistent or intermittent diplopia. Cover testing and assessment of extraocular muscle function can provide better insight into the underlying causes. Acute-onset abnormalities of accommodation and vergence should be evaluated urgently by neuro-ophthalmology. (Level 1)[123]
The effective management of accommodative insufficiency requires a coordinated interdisciplinary approach involving ophthalmologists, optometrists, orthoptists, nurses, primary care clinicians, educators, and vision rehabilitation specialists. Because accommodative insufficiency can significantly affect visual comfort, academic performance, and occupational productivity, collaborative care improves diagnostic accuracy, treatment adherence, and overall patient outcomes. A patient-centered model emphasizing communication, shared decision-making, and coordinated care is essential for optimizing functional visual rehabilitation.
Role of Clinicians and Ophthalmologists
Ophthalmologists are primarily responsible for accurate diagnosis, exclusion of ocular pathology, and formulation of the overall management plan. Their expertise is essential in differentiating accommodative insufficiency from other ocular or neurologic disorders that may present with similar symptoms. These clinicians should conduct comprehensive ocular examinations, including refractive assessment, binocular vision testing, and accommodative measurements. Ophthalmologists also determine whether additional investigations or specialist consultations are required. In addition to diagnosis, ophthalmologists play a key role in educating patients about the disorder, explaining treatment options such as optical correction or vision therapy, and ensuring patients understand the importance of treatment adherence.[124]
Role of Optometrists and Orthoptists
Optometrists and orthoptists are integral members of the care team, providing detailed binocular vision assessments and supervising vision therapy programs. Their responsibilities include measurement of accommodative amplitude, accommodative facility, accommodative response accuracy, and vergence function. These specialists design individualized therapy protocols to improve accommodative flexibility and endurance. Regular monitoring of therapeutic progress allows timely modification of treatment strategies, ensuring that patients achieve optimal rehabilitation outcomes.
Role of Nurses and Allied Healthcare Professionals
Nurses and allied health care professionals contribute significantly to patient education, counseling, and treatment adherence. These professionals help reinforce instructions regarding visual hygiene practices, proper spectacle use, and adherence to home-based vision therapy exercises. Nurses also play an important role in identifying persistent symptoms during follow-up visits and communicating these concerns to the supervising clinician. In pediatric populations, nursing staff may assist parents with adherence to therapy and symptom monitoring.[125]
Role of Primary Care Clinicians and Specialists
Primary care clinicians and other medical specialists, such as endocrinologists and neurologists, may be involved when accommodative insufficiency is associated with systemic conditions. Diseases such as diabetes mellitus, thyroid disorders, or neurologic conditions can affect the autonomic control of accommodation. Coordination between ophthalmologists and primary care clinicians helps ensure that systemic diseases are adequately managed, potentially improving visual function.
Role of Educators and Occupational Specialists
In children with accommodative insufficiency, educators and school health professionals play an important role in supporting visual learning needs. Teachers may provide accommodations such as scheduled visual breaks, improved classroom lighting, and adjustments to reading tasks. For adults in visually demanding occupations, occupational health specialists may recommend ergonomic workplace modifications to reduce accommodative strain.[126]
Interprofessional Communication and Care Coordination
Effective interdisciplinary communication is essential for the successful management of accommodative insufficiency. Clear documentation of clinical findings, therapy progress, and patient symptoms enables all members of the health care team to remain informed about the patient’s condition. Regular communication between clinicians and vision therapy specialists ensures that treatment protocols remain aligned with the patient’s needs. Shared decision-making involving patients and caregivers enhances treatment adherence and encourages active participation in therapy.[125]
Ethical Considerations and Patient-Centered Care
Ethical practice in the management of accommodative insufficiency includes providing evidence-based treatment recommendations, ensuring transparency in discussing therapy options, and respecting patient preferences. Clinicians should also avoid overprescribing unnecessary interventions and ensure that treatment decisions prioritize patient safety and functional outcomes.
Impact on Patient Outcomes
Interdisciplinary collaboration significantly improves outcomes in patients with accommodative insufficiency. Coordinated care allows early diagnosis, appropriate treatment selection, and continuous monitoring of progress. Patients benefit from comprehensive management that addresses both visual function and lifestyle factors contributing to accommodative stress.[125]
Table 19. Interprofessional Roles in the Management of Accommodative Insufficiency
|
Healthcare professional |
Primary responsibilities |
Contribution to patient outcomes |
|
Ophthalmologist |
Diagnosis, exclusion of ocular pathology, treatment planning |
Accurate diagnosis and appropriate therapy |
|
Optometrist/orthoptist |
Binocular vision testing, vision therapy supervision |
Improvement of accommodative function |
|
Nurses |
Patient education and therapy adherence monitoring |
Improved compliance and follow-up |
|
Primary care clinician |
Management of systemic conditions |
Optimization of systemic health |
|
Educators |
Academic support for pediatric patients |
Improved learning outcomes |
|
Occupational specialists |
Workplace ergonomics and visual hygiene |
Reduced occupational visual strain |
Clinical Significance
A collaborative, team-based approach ensures that accommodative insufficiency is managed effectively and safely. Interdisciplinary communication, coordinated care strategies, and patient-centered education enhance treatment success, improve visual comfort, and promote long-term functional visual health.
Media
(Click Image to Enlarge)
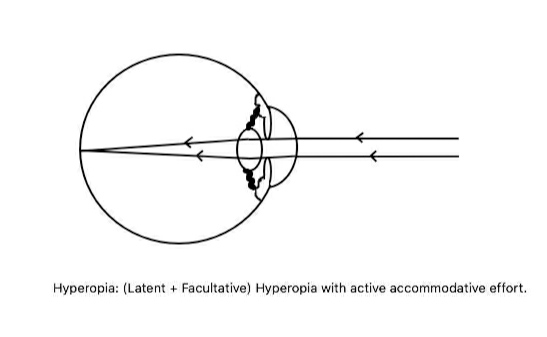
Hyperopia. Compensation of the latent and facultative components of hypermetropia by accommodation.
Contributed by S Majumdar, MBBS, MS
(Click Image to Enlarge)
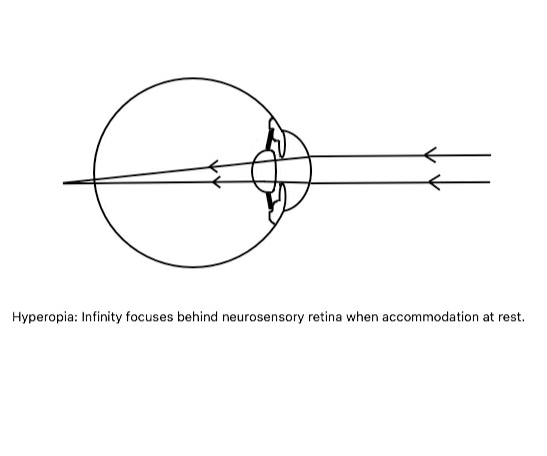
Hypermetropia. Parallel light rays converge at a focal point posterior to the neurosensory retina when the eye is in a nonaccommodating state.
Contributed by S Majumdar, MBBS, MS
(Click Image to Enlarge)
Orthotropia and Exotropia. The image shows a patient depicting orthotropia at near and exotropia after the fusion is suspended using the alternate cover test, suggestive of intermittent exotropia.
Contributed by K Kaur, MBBS, DNB, FPOS, FICO, MRCS Ed, MNAMS
(Click Image to Enlarge)
Horizontal and Vertical Ophthalmic Prism Bars. Horizontal and vertical strabismus are measured by neutralizing the angle of deviation during a prism cover test, enabling quantification of ocular misalignment.
Contributed by M Zeppieri, MD, PhD, and E Guidorzi
References
Shoji T, Kato N, Ishikawa S, Ibuki H, Yamada N, Kimura I, Shinoda K. Association between axial length and in vivo human crystalline lens biometry during accommodation: a swept-source optical coherence tomography study. Japanese journal of ophthalmology. 2020 Jan:64(1):93-101. doi: 10.1007/s10384-019-00700-8. Epub 2019 Nov 23 [PubMed PMID: 31760515]
Ghoushchi VP, Mompeán J, Prieto PM, Artal P. Binocular dynamics of accommodation, convergence, and pupil size in myopes. Biomedical optics express. 2021 Jun 1:12(6):3282-3295. doi: 10.1364/BOE.420334. Epub 2021 May 11 [PubMed PMID: 34221660]
Ayres BD, Rapuano CJ. Refractive power of the cornea. Comprehensive ophthalmology update. 2006 Sep-Oct:7(5):243-51; discussion 253-5 [PubMed PMID: 17132433]
Wu F, Zhao Y, Zhang H. Ocular Autonomic Nervous System: An Update from Anatomy to Physiological Functions. Vision (Basel, Switzerland). 2022 Jan 14:6(1):. doi: 10.3390/vision6010006. Epub 2022 Jan 14 [PubMed PMID: 35076641]
Atchison DA, Varnas SR. Accommodation stimulus and response determinations with autorefractors. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 2017 Jan:37(1):96-104. doi: 10.1111/opo.12340. Epub [PubMed PMID: 28030883]
Khalid K, Padda J, Pokhriyal S, Hitawala G, Khan MS, Upadhyay P, Cooper AC, Jean-Charles G. Pseudomyopia and Its Association With Anxiety. Cureus. 2021 Aug:13(8):e17411. doi: 10.7759/cureus.17411. Epub 2021 Aug 24 [PubMed PMID: 34589322]
Szczęśniak M, Sikorska E, Rajca M, Koper M, Kopacz W, Sikorski P, Maciejewicz P, Kasarełło K. The etiology, diagnostics, and treatment of the spasm of the near reflex - a narrative review. European journal of ophthalmology. 2024 Nov:34(6):1655-1666. doi: 10.1177/11206721241237309. Epub 2024 Mar 3 [PubMed PMID: 38433348]
Level 3 (low-level) evidenceSchor CM. A dynamic model of cross-coupling between accommodation and convergence: simulations of step and frequency responses. Optometry and vision science : official publication of the American Academy of Optometry. 1992 Apr:69(4):258-69 [PubMed PMID: 1565425]
Reynolds MM, Diehl NN, Mohney BG. Outcomes in accommodative esotropia with a high AC/A ratio. European journal of ophthalmology. 2021 Nov:31(6):3342-3348. doi: 10.1177/1120672120977831. Epub 2020 Dec 24 [PubMed PMID: 33356527]
Atiya A, Hussaindeen JR, Kasturirangan S, Ramasubramanian S, Swathi K, Swaminathan M. Frequency of undetected binocular vision anomalies among ophthalmology trainees. Journal of optometry. 2020 Jul-Sep:13(3):185-190. doi: 10.1016/j.optom.2020.01.003. Epub 2020 May 31 [PubMed PMID: 32493674]
Hussaindeen JR, Rakshit A, Singh NK, George R, Swaminathan M, Kapur S, Scheiman M, Ramani KK. Prevalence of non-strabismic anomalies of binocular vision in Tamil Nadu: report 2 of BAND study. Clinical & experimental optometry. 2017 Nov:100(6):642-648. doi: 10.1111/cxo.12496. Epub 2016 Nov 18 [PubMed PMID: 27859646]
Shukla Y. Accommodative anomalies in children. Indian journal of ophthalmology. 2020 Aug:68(8):1520-1525. doi: 10.4103/ijo.IJO_1973_18. Epub [PubMed PMID: 32709767]
Balke M, Skjöld G, Lundmark PO. Comparison of Short-Term Effects of Treatment of Accommodative Infacility with Low Plus Addition in Single Vision Rx or Vision Therapy: A Pilot Study. Clinical optometry. 2022:14():83-92. doi: 10.2147/OPTO.S355508. Epub 2022 Jun 2 [PubMed PMID: 35677714]
Level 3 (low-level) evidenceReindel W, Zhang L, Chinn J, Rah M. Evaluation of binocular function among pre- and early-presbyopes with asthenopia. Clinical optometry. 2018:10():1-8. doi: 10.2147/OPTO.S151294. Epub 2018 Jan 4 [PubMed PMID: 30214336]
Guo DY, Shen YY, Zhu MM, Zhan YY, Wang XW, Xia JH, Jiang B, Gu YS, Long Y. Virtual reality training improves accommodative facility and accommodative range. International journal of ophthalmology. 2022:15(7):1116-1121. doi: 10.18240/ijo.2022.07.11. Epub 2022 Jul 18 [PubMed PMID: 35919330]
Nunes AF, Monteiro PML, Ferreira FBP, Nunes AS. Convergence insufficiency and accommodative insufficiency in children. BMC ophthalmology. 2019 Feb 21:19(1):58. doi: 10.1186/s12886-019-1061-x. Epub 2019 Feb 21 [PubMed PMID: 30791877]
Hussaindeen JR, Murali A. Accommodative Insufficiency: Prevalence, Impact and Treatment Options. Clinical optometry. 2020:12():135-149. doi: 10.2147/OPTO.S224216. Epub 2020 Sep 11 [PubMed PMID: 32982529]
Gómez-Correa JE, Vohnsen B, Pierścionek BK, Chávez-Cerda S, Kling S, Rozema JJ, Applegate RA, Scarcelli G, Randleman JB, Goncharov AV, Fitzpatrick A, Morgan JIW, Roorda A, Atchison DA, Trevino JP, Consejo A, Börjeson C, Lundström L, Bang SP, Yoon G, Karnowski K, Kaluzny BJ, Grulkowski I, Barbero S, Artal P, Tabernero J, Kollbaum P, Thébault SC. Roadmap on advances in visual and physiological optics. Journal of optics (2010). 2025 Dec 1:27(12):123001. doi: 10.1088/2040-8986/ae1bb8. Epub 2025 Dec 3 [PubMed PMID: 41346852]
Level 3 (low-level) evidenceMutti DO, Mitchell GL, Jones-Jordan LA, Cotter SA, Kleinstein RN, Manny RE, Twelker JD, Zadnik K, CLEERE Study Group. The Response AC/A Ratio Before and After the Onset of Myopia. Investigative ophthalmology & visual science. 2017 Mar 1:58(3):1594-1602. doi: 10.1167/iovs.16-19093. Epub [PubMed PMID: 28291868]
Fisher RF. The mechanics of accommodation in relation to presbyopia. Eye (London, England). 1988:2 ( Pt 6)():646-9 [PubMed PMID: 3256503]
Hashemi H, Nabovati P, Khabazkhoob M, Yekta A, Emamian MH, Fotouhi A. Comparison of the accommodative amplitude measured with and without the use of a specialised accommodative rule in children. BMJ open ophthalmology. 2024 Sep 20:9(1):. doi: 10.1136/bmjophth-2024-001829. Epub 2024 Sep 20 [PubMed PMID: 39306331]
Yushan D, Hong Z. Frequency and associated factors of accommodative and non-strabismic binocular vision dysfunctions among clinical adults in Western China: A cross-sectional study. Medicine. 2025 Aug 22:104(34):e43881. doi: 10.1097/MD.0000000000043881. Epub [PubMed PMID: 40859492]
Level 2 (mid-level) evidenceWood JM, Chiu CN, Kim GH, Le J, Lee HJ, Nguyen T, Black AA. Refractive blur affects judgement of pedestrian walking direction at night. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 2021 May:41(3):582-590. doi: 10.1111/opo.12811. Epub 2021 Mar 27 [PubMed PMID: 33772849]
Cufflin MP, Mallen EA. Blur adaptation: clinical and refractive considerations. Clinical & experimental optometry. 2020 Jan:103(1):104-111. doi: 10.1111/cxo.13033. Epub 2019 Dec 4 [PubMed PMID: 31801179]
Carapancea M. [Ciliospastic myopia and cilio-relaxing asthenopia as manifestations of visual fatigue caused by hypermetropic accomodative overstrain]. Fiziologia normala si patologica. 1970 Mar-Apr:16(2):129-35 [PubMed PMID: 5419018]
Ntodie M, Saunders KJ, Little JA. Correction of Low-Moderate Hyperopia Improves Accommodative Function for Some Hyperopic Children During Sustained Near Work. Investigative ophthalmology & visual science. 2021 Apr 1:62(4):6. doi: 10.1167/iovs.62.4.6. Epub [PubMed PMID: 33821881]
Arnold RW. Pseudo-false positive eye/vision photoscreening due to accommodative insufficiency. A serendipitous benefit for poor readers? Binocular vision & strabismus quarterly. 2004:19(2):75-80 [PubMed PMID: 15180592]
Level 3 (low-level) evidenceRandolph SA. Computer Vision Syndrome. Workplace health & safety. 2017 Jul:65(7):328. doi: 10.1177/2165079917712727. Epub [PubMed PMID: 28628753]
Balgos MJTD, Vargas V, Alió JL. Correction of presbyopia: An integrated update for the practical surgeon. Taiwan journal of ophthalmology. 2018 Jul-Sep:8(3):121-140. doi: 10.4103/tjo.tjo_53_18. Epub [PubMed PMID: 30294526]
Makowski AL, Lindgren K, Locke JP. Visual side effects of scopolamine/ dextroamphetamine among parabolic fliers. Aviation, space, and environmental medicine. 2011 Jul:82(7):683-8 [PubMed PMID: 21748905]
Owusu E, Shasteen NM, Mitchell GL, Bailey MD, Kao CY, Toole AJ, Richdale K, Kulp MT. Impact of accommodative insufficiency and accommodative/vergence therapy on ciliary muscle thickness in the eye. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 2023 Sep:43(5):947-953. doi: 10.1111/opo.13155. Epub 2023 May 15 [PubMed PMID: 37184092]
Chakraborty S, Parida S, Mohanty SK, Das M, Dash S. Prevalence of Accommodative Insufficiency in Children With Normal Accommodative-Convergence/Accommodation Ratio and Its Association With Refractive Error: A Cross-Sectional Study. Cureus. 2025 Feb:17(2):e79683. doi: 10.7759/cureus.79683. Epub 2025 Feb 26 [PubMed PMID: 40012694]
Level 2 (mid-level) evidenceEsterov D, Greenwald BD. Autonomic Dysfunction after Mild Traumatic Brain Injury. Brain sciences. 2017 Aug 11:7(8):. doi: 10.3390/brainsci7080100. Epub 2017 Aug 11 [PubMed PMID: 28800081]
Coupland CAC, Hill T, Dening T, Morriss R, Moore M, Hippisley-Cox J. Anticholinergic Drug Exposure and the Risk of Dementia: A Nested Case-Control Study. JAMA internal medicine. 2019 Aug 1:179(8):1084-1093. doi: 10.1001/jamainternmed.2019.0677. Epub [PubMed PMID: 31233095]
Level 2 (mid-level) evidenceAggarwala KRG. Ocular Accommodation, Intraocular Pressure, Development of Myopia and Glaucoma: Role of Ciliary Muscle, Choroid and Metabolism. Medical hypothesis, discovery & innovation ophthalmology journal. 2020:9(1):66-70 [PubMed PMID: 31976346]
Chen AM, Roberts TL, Cotter SA, Kulp MT, Sinnott LT, Borsting EJ, Tea YC, Jones-Jordan LA, Hertle R, Mitchell GL, Eugene Arnold L, Chase C, Scheiman MM, Convergence Insufficiency Treatment Trial - Attention and Reading Trial (CITT-ART) Investigator Group. Effectiveness of vergence/accommodative therapy for accommodative dysfunction in children with convergence insufficiency. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 2021 Jan:41(1):21-32. doi: 10.1111/opo.12747. Epub 2020 Oct 29 [PubMed PMID: 33119180]
Hashemi H, Khabazkhoob M, Nabovati P, Shahraki FA, Ostadimoghaddam H, Faghihi M, Aghamirsalim M, Doostdar A, Yekta A. Accommodative insufficiency in a student population in Iran. Journal of optometry. 2019 Jul-Sep:12(3):161-167. doi: 10.1016/j.optom.2018.03.006. Epub 2018 May 22 [PubMed PMID: 29802027]
Chang MY, Morrison DG, Binenbaum G, Heidary G, Trivedi RH, Galvin JA, Pineles SL. Home- and Office-Based Vergence and Accommodative Therapies for Treatment of Convergence Insufficiency in Children and Young Adults: A Report by the American Academy of Ophthalmology. Ophthalmology. 2021 Dec:128(12):1756-1765. doi: 10.1016/j.ophtha.2021.05.017. Epub 2021 Jun 23 [PubMed PMID: 34172337]
DuPrey KM, Webner D, Lyons A, Kucuk CH, Ellis JT, Cronholm PF. Convergence Insufficiency Identifies Athletes at Risk of Prolonged Recovery From Sport-Related Concussion. The American journal of sports medicine. 2017 Aug:45(10):2388-2393. doi: 10.1177/0363546517705640. Epub 2017 May 16 [PubMed PMID: 28511593]
Watt T, Robertson K, Jacobs RJ. Refractive error, binocular vision and accommodation of children with Down syndrome. Clinical & experimental optometry. 2015 Jan:98(1):3-11. doi: 10.1111/cxo.12232. Epub 2014 Nov 13 [PubMed PMID: 25395109]
Satgunam P, Datta S, Sumalini R. Near vision in individuals with Down syndrome: a vision screening study. Eye (London, England). 2019 Aug:33(8):1254-1260. doi: 10.1038/s41433-019-0402-6. Epub 2019 Mar 26 [PubMed PMID: 30914784]
Leat SJ. Reduced accommodation in children with cerebral palsy. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 1996 Sep:16(5):385-90 [PubMed PMID: 8944183]
Level 2 (mid-level) evidenceFranco S, Moreira A, Fernandes A, Baptista A. Accommodative and binocular vision dysfunctions in a Portuguese clinical population. Journal of optometry. 2022 Oct-Dec:15(4):271-277. doi: 10.1016/j.optom.2021.10.002. Epub 2021 Nov 28 [PubMed PMID: 34852966]
Jaiswal S, Asper L, Long J, Lee A, Harrison K, Golebiowski B. Ocular and visual discomfort associated with smartphones, tablets and computers: what we do and do not know. Clinical & experimental optometry. 2019 Sep:102(5):463-477. doi: 10.1111/cxo.12851. Epub 2019 Jan 21 [PubMed PMID: 30663136]
Salari N, Ghasemi H, Abdoli N, Rahmani A, Shiri MH, Hashemian AH, Akbari H, Mohammadi M. The global prevalence of ADHD in children and adolescents: a systematic review and meta-analysis. Italian journal of pediatrics. 2023 Apr 20:49(1):48. doi: 10.1186/s13052-023-01456-1. Epub 2023 Apr 20 [PubMed PMID: 37081447]
Level 1 (high-level) evidenceBarata MJ, Aguiar P, Grzybowski A, Moreira-Rosário A, Lança C. A Review of Digital Eye Strain: Binocular Vision Anomalies, Ocular Surface Changes, and the Need for Objective Assessment. Journal of eye movement research. 2025 Oct:18(5):39. doi: 10.3390/jemr18050039. Epub 2025 Sep 5 [PubMed PMID: 40989226]
Sapienza A, Lítlá M, Lehmann S, Alessandretti L. Exposure to urban and rural contexts shapes smartphone usage behavior. PNAS nexus. 2023 Nov:2(11):pgad357. doi: 10.1093/pnasnexus/pgad357. Epub 2023 Nov 28 [PubMed PMID: 38034094]
Bentley S, Findley A, Chiva-Razavi S, Naujoks C, Patalano F, Johnson C, Arbuckle R, Wolffsohn JS. Understanding the visual function symptoms and associated functional impacts of phakic presbyopia. Journal of patient-reported outcomes. 2021 Nov 3:5(1):114. doi: 10.1186/s41687-021-00383-1. Epub 2021 Nov 3 [PubMed PMID: 34731344]
Level 3 (low-level) evidenceLisowski Ł, Lisowska J, Charytonowicz A, Mariak Z, Obuchowska I, Konopińska J. The diagnostic significance of pupillary reflex pathways: insights from classical examination and advanced pupillometry. Frontiers in neuroscience. 2025:19():1677431. doi: 10.3389/fnins.2025.1677431. Epub 2025 Oct 15 [PubMed PMID: 41169745]
Croft MA, McDonald JP, Katz A, Lin TL, Lütjen-Drecoll E, Kaufman PL. Extralenticular and lenticular aspects of accommodation and presbyopia in human versus monkey eyes. Investigative ophthalmology & visual science. 2013 Jul 26:54(7):5035-48. doi: 10.1167/iovs.12-10846. Epub 2013 Jul 26 [PubMed PMID: 23745002]
Level 3 (low-level) evidenceHilora M, Tripathy K. Accommodative Excess. StatPearls. 2026 Jan:(): [PubMed PMID: 37276314]
Anderson HA, Parks SM, Kulp MT, Mitchell GL. Classification of accommodative insufficiency by monocular subjective push-up test is poorly predictive of monocular objective amplitudes in children and young adults. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 2025 Jan:45(1):14-22. doi: 10.1111/opo.13419. Epub 2024 Nov 18 [PubMed PMID: 39555785]
Marran LF, De Land PN, Nguyen AL. Accommodative insufficiency is the primary source of symptoms in children diagnosed with convergence insufficiency. Optometry and vision science : official publication of the American Academy of Optometry. 2006 May:83(5):281-9 [PubMed PMID: 16699440]
Schachar RA, Schachar IH, Kumar S, Feldman EI, Pierscionek BK, Cosman PC. Model of zonular forces on the lens capsule during accommodation. Scientific reports. 2024 Mar 11:14(1):5896. doi: 10.1038/s41598-024-56563-8. Epub 2024 Mar 11 [PubMed PMID: 38467700]
Jin HY, Baek HS, Park TS. Morphologic Changes in Autonomic Nerves in Diabetic Autonomic Neuropathy. Diabetes & metabolism journal. 2015 Dec:39(6):461-7. doi: 10.4093/dmj.2015.39.6.461. Epub [PubMed PMID: 26706915]
Cheng C, Parreno J, Nowak RB, Biswas SK, Wang K, Hoshino M, Uesugi K, Yagi N, Moncaster JA, Lo WK, Pierscionek B, Fowler VM. Age-related changes in eye lens biomechanics, morphology, refractive index and transparency. Aging. 2019 Dec 16:11(24):12497-12531. doi: 10.18632/aging.102584. Epub 2019 Dec 16 [PubMed PMID: 31844034]
Ostrin LA, Glasser A. Autonomic drugs and the accommodative system in rhesus monkeys. Experimental eye research. 2010 Jan:90(1):104-12. doi: 10.1016/j.exer.2009.09.015. Epub 2009 Sep 24 [PubMed PMID: 19782072]
Level 3 (low-level) evidenceGołaszewski P, Wawrzyniak A, Kłosowicz M, Burbelka A, Balawender K. Neurotoxicity of Chronic Alcohol Exposure: Mechanistic Insights, Cellular Disruption, and Emerging Therapeutic Strategies. International journal of molecular sciences. 2025 Dec 27:27(1):. doi: 10.3390/ijms27010299. Epub 2025 Dec 27 [PubMed PMID: 41516173]
Sterner B, Gellerstedt M, Sjöström A. Accommodation and the relationship to subjective symptoms with near work for young school children. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 2006 Mar:26(2):148-55 [PubMed PMID: 16460315]
Abdi S, Brautaset R, Rydberg A, Pansell T. The influence of accommodative insufficiency on reading. Clinical & experimental optometry. 2007 Jan:90(1):36-43 [PubMed PMID: 17177664]
Level 3 (low-level) evidenceTurgut B, Kobat SG. A Glossary for ''Pseudo'' Conditions in Ophthalmology. Beyoglu eye journal. 2020:5(3):153-162. doi: 10.14744/bej.2020.88609. Epub 2020 Dec 28 [PubMed PMID: 35098081]
Cacho P, García A, Lara F, Seguí MM. Diagnostic signs of accommodative insufficiency. Optometry and vision science : official publication of the American Academy of Optometry. 2002 Sep:79(9):614-20 [PubMed PMID: 12322932]
Kang SL, Shaikh AG, Ghasia FF. Vergence and Strabismus in Neurodegenerative Disorders. Frontiers in neurology. 2018:9():299. doi: 10.3389/fneur.2018.00299. Epub 2018 May 16 [PubMed PMID: 29867716]
Faiq MA, Sengupta T, Nath M, Velpandian T, Saluja D, Dada R, Dada T, Chan KC. Ocular manifestations of central insulin resistance. Neural regeneration research. 2023 May:18(5):1139-1146. doi: 10.4103/1673-5374.355765. Epub [PubMed PMID: 36255004]
Krishnan A, Dutta A, Srivastava A, Konda N, Prakasam RK. Artificial Intelligence in Optometry: Current and Future Perspectives. Clinical optometry. 2025:17():83-114. doi: 10.2147/OPTO.S494911. Epub 2025 Mar 12 [PubMed PMID: 40094103]
Level 3 (low-level) evidenceKaur K, Gurnani B, Nayak S, Deori N, Kaur S, Jethani J, Singh D, Agarkar S, Hussaindeen JR, Sukhija J, Mishra D. Digital Eye Strain- A Comprehensive Review. Ophthalmology and therapy. 2022 Oct:11(5):1655-1680. doi: 10.1007/s40123-022-00540-9. Epub 2022 Jul 9 [PubMed PMID: 35809192]
Chmiel J, Malinowska A. Neural Correlates of Burnout Syndrome Based on Electroencephalography (EEG)-A Mechanistic Review and Discussion of Burnout Syndrome Cognitive Bias Theory. Journal of clinical medicine. 2025 Jul 29:14(15):. doi: 10.3390/jcm14155357. Epub 2025 Jul 29 [PubMed PMID: 40806977]
Seraji-Bzorgzad N, Paulson H, Heidebrink J. Neurologic examination in the elderly. Handbook of clinical neurology. 2019:167():73-88. doi: 10.1016/B978-0-12-804766-8.00005-4. Epub [PubMed PMID: 31753158]
Schnider C, Yuen L, Rampat R, Zhu D, Dhallu S, Trinh T, Gurnani B, Abdelmaksoud A, Bhogal-Bhamra G, Wolffsohn JS, Naroo SA. BCLA CLEAR presbyopia: Management with intraocular lenses. Contact lens & anterior eye : the journal of the British Contact Lens Association. 2024 Aug:47(4):102253. doi: 10.1016/j.clae.2024.102253. Epub 2024 Jul 2 [PubMed PMID: 39068141]
Argilés M, Cardona G. The Interaction between Vergence and Accommodation Cues in the Assessment of Fusional Vergence Range. Life (Basel, Switzerland). 2024 Sep 19:14(9):. doi: 10.3390/life14091185. Epub 2024 Sep 19 [PubMed PMID: 39337967]
Hashemi H, Nabovati P, Yekta A, Aghamirsalim M, Rafati S, Ostadimoghaddam H, Razmjoo H, Khabazkhoob M. Convergence Insufficiency in the Geriatric Population. Optometry and vision science : official publication of the American Academy of Optometry. 2021 Jun 1:98(6):613-619. doi: 10.1097/OPX.0000000000001709. Epub [PubMed PMID: 34081652]
López-Artero E, Garzón N, Rodríguez-Vallejo M, García-Montero M. Feasibility of optical quality analysis system for the objective assessment of accommodation insufficiency: a phase 1 study. Journal of optometry. 2021 Jul-Sep:14(3):287-294. doi: 10.1016/j.optom.2020.06.004. Epub 2020 Aug 12 [PubMed PMID: 32800453]
Level 2 (mid-level) evidenceScheiman M, Kulp MT, Cotter SA, Lawrenson JG, Wang L, Li T. Interventions for convergence insufficiency: a network meta-analysis. The Cochrane database of systematic reviews. 2020 Dec 2:12(12):CD006768. doi: 10.1002/14651858.CD006768.pub3. Epub 2020 Dec 2 [PubMed PMID: 33263359]
Level 1 (high-level) evidenceMorimoto T, Kanda H, Hirota M, Nishida K, Fujikado T. Insufficient accommodation during binocular near viewing in eyes with intermittent exotropia. Japanese journal of ophthalmology. 2020 Jan:64(1):77-85. doi: 10.1007/s10384-019-00695-2. Epub 2019 Nov 9 [PubMed PMID: 31707606]
Pang Y, Gnanaraj L, Gayleard J, Han G, Hatt SR. Interventions for intermittent exotropia. The Cochrane database of systematic reviews. 2021 Sep 13:9(9):CD003737. doi: 10.1002/14651858.CD003737.pub4. Epub 2021 Sep 13 [PubMed PMID: 34516656]
Level 1 (high-level) evidenceChen Y, Zhang C, Ding C, Tao C, Bao J, Zheng J, Chen H. Repeatability of two subjective accommodative amplitude measurements and agreement with an objective method. Clinical & experimental optometry. 2019 Jul:102(4):412-417. doi: 10.1111/cxo.12884. Epub 2019 Mar 13 [PubMed PMID: 30866109]
Ren Q, Yue H, Zhou Q. [Effects of orthokeratology lenses on the magnitude of accommodative lag and accommodativeconvergence/accommodation]. Zhong nan da xue xue bao. Yi xue ban = Journal of Central South University. Medical sciences. 2016 Feb:41(2):169-73. doi: 10.11817/j.issn.1672-7347.2016.02.009. Epub [PubMed PMID: 26932215]
Adler P, Scally AJ, Barrett BT. Test-retest reproducibility of accommodative facility measures in primary school children. Clinical & experimental optometry. 2018 Nov:101(6):764-770. doi: 10.1111/cxo.12691. Epub 2018 May 8 [PubMed PMID: 29740867]
Chen M, Long Q, Gu H, Hong J. Accommodation changes after visian implantable collamer lens with central hole for high myopia: A STROBE-compliant article. Medicine. 2019 Jul:98(28):e16434. doi: 10.1097/MD.0000000000016434. Epub [PubMed PMID: 31305467]
Murray C MRes, BSc HONS, Newsham D PhD, MSc, DBO. The Normal Accommodative Convergence/Accommodation (AC/A) Ratio. Journal of binocular vision and ocular motility. 2018 Oct-Dec:68(4):140-147. doi: 10.1080/2576117X.2018.1529450. Epub 2018 Oct 25 [PubMed PMID: 30358493]
Vivekanand U, Lobo SG, Dharmappa N, Kesireddy A. Comparing proximal convergence ratio in myopes. Romanian journal of ophthalmology. 2021 Oct-Dec:65(4):362-364. doi: 10.22336/rjo.2021.71. Epub [PubMed PMID: 35087977]
Jackson JH, Arnoldi K. The Gradient AC/A Ratio: What's Really Normal? The American orthoptic journal. 2004:54():125-32. doi: 10.3368/aoj.54.1.125. Epub [PubMed PMID: 21149096]
Abu EK, Ocansey S, Yennu J, Asirifi I, Marfo R. Comparing Different Methods of Measuring Accommodative Amplitude with Hofstetter's Normative Values in a Ghanaian Population. Current eye research. 2018 Sep:43(9):1145-1150. doi: 10.1080/02713683.2018.1480044. Epub 2018 Jun 4 [PubMed PMID: 29787692]
Kaliugavaradhan A, Ramamurthy D. Accommodative Facility and Response Time before and after Computer Task of Varying Durations in Young Adults. The British and Irish orthoptic journal. 2023:19(1):85-95. doi: 10.22599/bioj.295. Epub 2023 Oct 16 [PubMed PMID: 37868656]
Ribeiro BNF. Magnetic resonance imaging findings in diseases affecting the cranial nerves. Radiologia brasileira. 2022 Jan-Feb:55(1):V-VI. doi: 10.1590/0100-3984.2022.55.1e1. Epub [PubMed PMID: 35210667]
Fulk GW, Cyert LA, Parker DE. A randomized trial of the effect of single-vision vs. bifocal lenses on myopia progression in children with esophoria. Optometry and vision science : official publication of the American Academy of Optometry. 2000 Aug:77(8):395-401 [PubMed PMID: 10966065]
Level 1 (high-level) evidenceGarcía-Montero M, Antona B, Barrio AR, Nieto-Zayas C, Martínez-Alberquilla I, Hernández-Verdejo JL. The role of clinical diagnosis criteria on the frequency of accommodative insufficiency. International journal of ophthalmology. 2019:12(4):647-653. doi: 10.18240/ijo.2019.04.20. Epub 2019 Apr 18 [PubMed PMID: 31024821]
Singh M, Sinha BP, Dutta S, Deokar KK, Mishra D, Goswami K. A Systematic Review and Meta-Analysis on the Efficacy and Safety of Topical Pilocarpine 1.25% in Presbyopia Treatment. Journal of current ophthalmology. 2024 Apr-Jun:36(2):111-121. doi: 10.4103/joco.joco_262_23. Epub 2025 Jan 18 [PubMed PMID: 40012805]
Level 1 (high-level) evidenceHouston CA, Jone D, Weir CR. An unusual cause of asthenopia: "pseudo-accommodative insufficiency" associated with a high AC:A ratio. The British journal of ophthalmology. 2000 Dec:84(12):1438 [PubMed PMID: 11186867]
Level 3 (low-level) evidencePorcar E, Montalt JC, Pons ÁM, España-Gregori E. Symptomatic accommodative and binocular dysfunctions from the use of flat-panel displays. International journal of ophthalmology. 2018:11(3):501-505. doi: 10.18240/ijo.2018.03.22. Epub 2018 Mar 18 [PubMed PMID: 29600186]
Wick B, Yothers TL, Jiang BC, Morse SE. Clinical testing of accommodative facility: Part 1. A critical appraisal of the literature. Optometry (St. Louis, Mo.). 2002 Jan:73(1):11-23 [PubMed PMID: 12363234]
Sakai T, Shikishima K, Mizobuchi T, Yoshida M, Kitahara K. Bilateral tonic pupils associated with neurosyphilis. Japanese journal of ophthalmology. 2003 Jul-Aug:47(4):368-71 [PubMed PMID: 12842205]
Level 3 (low-level) evidenceGhobadi M, Nabovati P, Hashemi H, Talaei A, Fathi HR, Yekta Y, Ostadimoghaddam H, Yekta A, Khabazkhoob M. Accommodative and convergence anomalies in patients with opioid use disorder. Clinical & experimental optometry. 2022 May:105(4):392-397. doi: 10.1080/08164622.2021.1932431. Epub 2021 Jun 24 [PubMed PMID: 34167446]
Wajuihian SO. Correlations between clinical measures and symptoms: Report 2: Accommodative and vergence measures with symptoms. Journal of optometry. 2021 Apr-Jun:14(2):142-155. doi: 10.1016/j.optom.2020.06.008. Epub 2020 Sep 1 [PubMed PMID: 32883648]
Blitshteyn S. Dysautonomia: a common comorbidity of systemic disease. Immunologic research. 2025 Jul 8:73(1):105. doi: 10.1007/s12026-025-09661-2. Epub 2025 Jul 8 [PubMed PMID: 40624434]
Logan NS, Radhakrishnan H, Cruickshank FE, Allen PM, Bandela PK, Davies LN, Hasebe S, Khanal S, Schmid KL, Vera-Diaz FA, Wolffsohn JS. IMI Accommodation and Binocular Vision in Myopia Development and Progression. Investigative ophthalmology & visual science. 2021 Apr 28:62(5):4. doi: 10.1167/iovs.62.5.4. Epub [PubMed PMID: 33909034]
Scheiman M, Rouse M, Kulp MT, Cotter S, Hertle R, Mitchell GL. Treatment of convergence insufficiency in childhood: a current perspective. Optometry and vision science : official publication of the American Academy of Optometry. 2009 May:86(5):420-8. doi: 10.1097/OPX.0b013e31819fa712. Epub [PubMed PMID: 19319008]
Level 3 (low-level) evidenceHutchinson AK, Morse CL, Hercinovic A, Cruz OA, Sprunger DT, Repka MX, Lambert SR, Wallace DK, American Academy of Ophthalmology Preferred Practice Pattern Pediatric Ophthalmology/Strabismus Panel. Pediatric Eye Evaluations Preferred Practice Pattern. Ophthalmology. 2023 Mar:130(3):P222-P270. doi: 10.1016/j.ophtha.2022.10.030. Epub 2022 Dec 19 [PubMed PMID: 36543602]
Heus P, Verbeek JH, Tikka C. Optical correction of refractive error for preventing and treating eye symptoms in computer users. The Cochrane database of systematic reviews. 2018 Apr 10:4(4):CD009877. doi: 10.1002/14651858.CD009877.pub2. Epub 2018 Apr 10 [PubMed PMID: 29633784]
Level 1 (high-level) evidenceScheiman M, Cotter S, Kulp MT, Mitchell GL, Cooper J, Gallaway M, Hopkins KB, Bartuccio M, Chung I, Convergence Insufficiency Treatment Trial Study Group. Treatment of accommodative dysfunction in children: results from a randomized clinical trial. Optometry and vision science : official publication of the American Academy of Optometry. 2011 Nov:88(11):1343-52. doi: 10.1097/OPX.0b013e31822f4d7c. Epub [PubMed PMID: 21873922]
Level 1 (high-level) evidenceManna P, Karmakar S, Mondal A, Sarbajna P, Bhardwaj GK. Effects of Two Vision Therapy Approaches on Accommodative Insufficiency and Post-therapy Stability. Journal of pediatric ophthalmology and strabismus. 2025 Jan-Feb:62(1):12-26. doi: 10.3928/01913913-20240807-01. Epub 2024 Sep 10 [PubMed PMID: 39254187]
Raab EL. Follow-up monitoring of accommodative esotropia. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2001 Aug:5(4):246-9 [PubMed PMID: 11507584]
Sekeroglu MA, Hekimoglu E, Anayol MA, Tasci Y, Dolen I. An overlooked effect of systemic anticholinergics: alteration on accommodation amplitude. International journal of ophthalmology. 2016:9(5):743-5. doi: 10.18240/ijo.2016.05.19. Epub 2016 May 18 [PubMed PMID: 27275433]
Balali-Mood M, Saber H. Recent advances in the treatment of organophosphorous poisonings. Iranian journal of medical sciences. 2012 Jun:37(2):74-91 [PubMed PMID: 23115436]
Level 3 (low-level) evidenceKaur K, Muralikrishnan J, Hussaindeen JR, Deori N, Gurnani B. Impact of Covid-19 on Pediatric Ophthalmology Care: Lessons Learned. Pediatric health, medicine and therapeutics. 2023:14():309-321. doi: 10.2147/PHMT.S395349. Epub 2023 Oct 12 [PubMed PMID: 37849985]
Rout S, Radhakrishnan A. A Comparison of Accommodative Ability in Healthy Controls, Diabetics, and Healthy Subjects with a Family History of Diabetes. The British and Irish orthoptic journal. 2025:21(1):95-104. doi: 10.22599/bioj.438. Epub 2025 Sep 22 [PubMed PMID: 41017963]
Enaholo ES, Gurnani B. Accommodative Insufficiency. StatPearls. 2026 Jan:(): [PubMed PMID: 36508537]
Kardas P, Lewek P, Matyjaszczyk M. Determinants of patient adherence: a review of systematic reviews. Frontiers in pharmacology. 2013:4():91. doi: 10.3389/fphar.2013.00091. Epub 2013 Jul 25 [PubMed PMID: 23898295]
Level 1 (high-level) evidenceCITT-ART Investigator Group. Effect of Vergence/Accommodative Therapy on Reading in Children with Convergence Insufficiency: A Randomized Clinical Trial. Optometry and vision science : official publication of the American Academy of Optometry. 2019 Nov:96(11):836-849. doi: 10.1097/OPX.0000000000001442. Epub [PubMed PMID: 31651592]
Level 1 (high-level) evidenceAl-Beltagi M, Saeed NK, Bediwy AS, Elbeltagi R. Breaking the cycle: Psychological and social dimensions of pediatric functional gastrointestinal disorders. World journal of clinical pediatrics. 2025 Jun 9:14(2):103323. doi: 10.5409/wjcp.v14.i2.103323. Epub 2025 Jun 9 [PubMed PMID: 40491742]
Kaur K, Gurnani B. Microspherophakia. StatPearls. 2026 Jan:(): [PubMed PMID: 35015420]
Gurnani B, Kaur K. Renaissance of an Emerging Pathogen-Pythium insidiosum Keratitis: An Indian Perspective. Clinical ophthalmology (Auckland, N.Z.). 2025:19():4811-4830. doi: 10.2147/OPTH.S568552. Epub 2025 Dec 18 [PubMed PMID: 41446894]
Level 3 (low-level) evidenceGurnani B, Kaur K. Immune Camouflage in Pythium insidiosum Keratitis: A Hypothesis on Molecular Mimicry and Host Pattern Recognition Receptor Evasion. Clinical ophthalmology (Auckland, N.Z.). 2025:19():4855-4873. doi: 10.2147/OPTH.S560311. Epub 2025 Dec 19 [PubMed PMID: 41446892]
Gurnani B, Kaur K. Corneal cross-linking for keratoconus: a global economic and clinical perspective. Journal of medical economics. 2025 Dec:28(1):2119-2124. doi: 10.1080/13696998.2025.2587416. Epub 2025 Nov 30 [PubMed PMID: 41320236]
Level 3 (low-level) evidenceMurugan SB, Sunil Kumar, Gurnani B, Kaur K. Assessment of Subjective Visual Experiences During Intraocular Surgery and Intravitreal Injection Among Uveitis Patients at a Tertiary Eye Hospital: A Cross-Sectional Observational Study. Ophthalmology and therapy. 2026 Jan:15(1):173-191. doi: 10.1007/s40123-025-01264-2. Epub 2025 Nov 6 [PubMed PMID: 41196490]
Level 2 (mid-level) evidenceGurnani B, Kaur K. Advancing diagnostics in Pythium insidiosum keratitis: the emerging role of point-of-care imaging and biosensor-based detection devices. Expert review of medical devices. 2025 Dec:22(12):1287-1292. doi: 10.1080/17434440.2025.2582616. Epub 2025 Nov 2 [PubMed PMID: 41147335]
Gurnani B, Kaur K. Post-market surveillance of ophthalmic implants: role of real-world evidence. Expert review of medical devices. 2025 Dec:22(12):1303-1308. doi: 10.1080/17434440.2025.2579578. Epub 2025 Oct 24 [PubMed PMID: 41123186]
Gurnani B, Kaur K. Teleophthalmology-enabled devices: bridging the gap in rural eye care. Expert review of medical devices. 2025 Nov:22(11):1167-1172. doi: 10.1080/17434440.2025.2566741. Epub 2025 Oct 15 [PubMed PMID: 40990172]
Fine SN, Rutkowski T, Santos EM, Gohel S, Hajebrahimi F, Scheiman M, Alvarez TL. Heath components of objective accommodative responses for convergence insufficiency participants compared with those with binocularly normal vision. Optometry and vision science : official publication of the American Academy of Optometry. 2025 Dec 1:102(12):731-742. doi: 10.1097/OPX.0000000000002307. Epub 2025 Nov 18 [PubMed PMID: 41252526]
Gurnani B, Kaur K. Biosensor-embedded wearables for dry eye monitoring and management. Expert review of medical devices. 2025 Oct:22(10):1073-1079. doi: 10.1080/17434440.2025.2555485. Epub 2025 Sep 1 [PubMed PMID: 40884106]
Gurnani B, Kaur K. Response to letter regarding "Evaluating the novel role of ChatGPT-4 in addressing corneal ulcer queries: An AI-powered insight". European journal of ophthalmology. 2026 May:36(3):NP5-NP7. doi: 10.1177/11206721251357376. Epub 2025 Jul 9 [PubMed PMID: 40629931]
Level 3 (low-level) evidenceNishant P, Gurnani B, Singh P, Sinha S, Kaur K, Kumar A, Sinha RK. Current concepts and recent trends in endothelial keratoplasty. World journal of transplantation. 2025 Jun 18:15(2):102507. doi: 10.5500/wjt.v15.i2.102507. Epub [PubMed PMID: 40535500]
Musa M, Aluyi-Osa G, Zeppieri M. Foster Kennedy Syndrome (FKS): A Case Report. Clinics and practice. 2022 Jul 12:12(4):527-532. doi: 10.3390/clinpract12040056. Epub 2022 Jul 12 [PubMed PMID: 35892442]
Level 3 (low-level) evidenceKaur K, Gurnani B. Cycloplegic and Noncycloplegic Refraction. StatPearls. 2026 Jan:(): [PubMed PMID: 35593830]
De Souza N, Cui Y, Looi S, Paudel P, Shinde L, Kumar K, Berwal R, Wadhwa R, Daniel V, Flanagan J, Holden B. The role of optometrists in India: an integral part of an eye health team. Indian journal of ophthalmology. 2012 Sep-Oct:60(5):401-5. doi: 10.4103/0301-4738.100534. Epub [PubMed PMID: 22944749]
Gurnani B, Kaur K. Astigmatism. StatPearls. 2026 Jan:(): [PubMed PMID: 35881747]