 HIV Safety in Clinical Laboratories: Biology, Occupational Risk, Prevention, and Florida Law
HIV Safety in Clinical Laboratories: Biology, Occupational Risk, Prevention, and Florida Law
Introduction
HIV is transmitted through exposure to infected blood, semen, vaginal fluid, or breast milk.[1] The virus targets cells with CD4+ receptors, including T-cells.[2] These cells are part of the immune system that helps the body fend off infections.[3] Infection with HIV triggers T-cell destruction, decreasing cell-mediated immunity, which can lead to various opportunistic infections and cancer.[2]
From days to weeks after exposure to the virus, early symptoms of HIV infection may include fever, sore throat, enlarged lymph nodes, weight loss, myalgia, or rash. Then, an infected person can become asymptomatic while the virus continues to replicate, and the number of CD4+ T-cells progressively decreases. Once the CD4+ count drops below a certain level, a significant increase in risk for infections that can become life-threatening occurs, defining the Acquired Immunodeficiency Syndrome (AIDS) stage of HIV infection. Without treatment, the time from the start of infection to AIDS-related death is estimated to be about 11 years.[4] However, when started early, antiretroviral treatment (ART) has enabled people with HIV to live with chronic infection as long as those without the disease.[2]
HIV belongs to the retrovirus family, which has complex genomes and capsid core particles.[5] Retroviruses are positive-sense RNA viruses that can reverse transcribe their genome, inserting it into the host cell.[6] Through reverse transcription, single-stranded viral RNA is transformed into double-stranded DNA, which can incorporate itself into the host cell’s DNA and replicate.[4]
HIV consists of 2 primary components: the capsid and the genome. The conical capsid encloses the viral RNA genome, giving it shape and protection. The genome carries genetic information.[7]
The capsid protects the viral genome, mediates its transfer between cells, and interacts with host factors to facilitate viral replication.[7] The shape of the capsid is elastic, starting as an immature sphere and transitioning into a mature cone.[6]
For the virus to enter a cell, its envelope must fuse with the host cell’s membrane. The viral envelope consists of the glycoproteins gp120 and gp41, which form spikes that enable attachment. These glycoproteins recognize the host cell’s surface receptors CD4+, CCR5, and CXCR4.[4]
Adsorption occurs when HIV binds and enters a cell through fusion. The spikes on the HIV envelope consist of gp120 and gp41. Gp120 binds CD4 receptors and either CCR5 or CXCR4 on the host cell, allowing HIV entry into the cell. Gp41 promotes the fusion of HIV and the host cell membrane. CXCR4 is present on T-cells and many other cells, and CCR5 is present mainly on macrophages.[4]
Every retrovirus encodes 3 essential structural genes: gag, pol, and env. The gag gene determines the structural core proteins, creating the capsid; pol encodes for enzymes necessary for viral replication, including reverse transcriptase; and env encodes the glycoproteins of the viral envelope. The HIV-1 genome also encodes 6 other regulatory genes that modulate replication: tat, rev, vif, vpx, vpr, and nef.[4][6]
Because HIV consists of 2 RNA molecules, genetic mutations are likely, as point mutations can occur on either molecule. The high frequency of mutations allows the virus to escape from the body’s immune system.[4][5] The 2 genetically different strains of HIV are HIV-1 and HIV-2. HIV-1 makes up most infections worldwide, and HIV-2 is primarily restricted to Western Africa. HIV-1 has been divided into groups M, N, O, and P. The M group dominates the HIV pandemic. Thus, this group has been further divided into 9 subtypes: A to D, F to H, J, and K. Subtype B predominates in North America.[8]
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
Modes of HIV Transmission
Occupational exposures
HIV transmission occurs through direct exposure to infected blood or secretions. This can happen in an occupational setting through accidental needlesticks or sharp-object cuts.[4] Developing HIV after a needlestick injury is uncommon, and studies have revealed that the risk of transmission is 0.3%. This can be higher if the patient has a high viral titer or if exposure to a large quantity of infected blood has occurred. Additionally, transmission may occur when infected blood splashes onto mucosal surfaces.[9]
Potentially infectious body fluids
Exposure to blood or other bodily fluids, including vaginal secretions, semen, cerebrospinal fluid (CSF), peritoneal fluid, pleural fluid, and amniotic fluid, can expose healthcare workers to bloodborne pathogens like HIV.[10]
Risk Factors Associated with Increased HIV Infection
Following established recommendations and protocols is necessary to decrease the risk of occupational exposure to HIV infection. Factors associated with increased risk include:
- Lack of universal precautions
- Failure to follow safety protocol
- Use of sharp devices without safety features
- Exposure to a higher quantity of blood or a large-bore needle [9]
Practices that Prevent HIV Exposure
HIV has no vaccine. However, prevention of HIV exposure is the best way to prevent transmission in the healthcare setting. Among healthcare laboratory personnel, bloodborne viruses are responsible for most laboratory-acquired infections. Education, training, and biosafety protocols should be in place to reduce the potential risk of disease transmission.[11]
Engineering controls
Engineering controls are tools designed to remove contaminated equipment from the workplace.[10] Proper use of safety-engineered devices reduces the risk of accidental exposure to HIV, including:
- Dispose of sharps in sharps containers
- Avoid recapping used needles
- Use shields and retractable needles
- Use plastic blood tubes instead of glass [12][13][14]
Exposure prevention is critical to preventing the transmission of HIV and other bloodborne pathogens.
Sharps
Sharp injuries may result from needles, scalpels, razors, or lancets. All sharps must be disposed of in a specified, puncture-proof container.[10][12]
Work practice controls
These controls reduce exposure to bloodborne pathogens.[10][15] When an exposure risk is identified,
- Wear gloves when there is direct contact with blood and bodily fluids.
- Wear masks, eyeglasses, and waterproof gowns during procedures where blood splashing may occur.
- Do not perform mouth pipetting.
- Avoid contact with mucosal surfaces, such as eating, drinking, smoking, applying lip balm, or handling contact lenses.
Handwashing
Proper hand hygiene is one of the most effective ways to control infection and prevent disease transmission after exposure. CDC guidelines recommend handwashing with soap and water for 20 seconds or using an alcohol hand rub with 60% alcohol. Hand hygiene should occur after touching a patient, cleaning a soiled site, contacting bodily fluids, and touching contaminated surfaces.[10]
Personal protective equipment
Personal protective equipment (PPE) is essential in the laboratory, as this practice protects healthcare workers from potential exposure by creating a physical barrier. Basic PPE includes masks, gowns or coats, gloves, and face shields.[10]
Gloves
Healthcare workers must wear gloves when encountering bodily fluids, collecting blood or fluids, and contacting contaminated surfaces. Gloves must be changed if they are torn, damaged, or contaminated. They must also be changed before leaving the work area and between patient encounters.
Disinfection
HIV can persist on dry surfaces for more than 7 days.[16] The organic materials should be removed from the surface before cleaning. Many disinfectant solutions are effective against HIV. Most commonly, UV-LED light, 70% ethyl alcohol, or sodium hypochlorite (household bleach) can inactivate HIV on surfaces.[17][18] Reading the product's label is important to ensure activity against HIV.
Clinical Significance
Clinical Management of an HIV Exposure
Exposure
If exposure occurs, a healthcare worker must get emergency care, and first aid should be started. The type of care depends on the route of exposure. If the nose, mouth, face, or skin is exposed, they should be flushed with water. Additionally, if exposure occurs to the eyes, they should be irrigated with sterile saline, sterile irrigation solution, or clean water. For needlestick or cut exposure, the site should be washed with soap and water, and wounds must be cleaned.[9] Healthcare workers should promptly report HIV exposure to their supervisors, and medical evaluation with management should follow.[10]
Evaluation and treatment
Medical evaluation and decision to treat should occur immediately, and a plan for postexposure prophylaxis should be ensured. Follow-up evaluations should occur. The healthcare worker’s health information is kept confidential.[19] If possible, the CDC recommends testing the source patient with an FDA-approved rapid HIV test. Fourth-generation combination p24 antigen-HIV antibody (Ag/Ab) tests provide rapid, accurate results and are preferred over older-generation tests. Serum creatinine, AST, and ALT should also be tested as part of the baseline workup.[20]
Postexposure Prophylaxis
If possible, the source patient should be tested for HIV. Expert consultation is suggested.[1][21] ART must be started as soon as possible, preferably within 72 hours of exposure, and continued for 4 weeks, and should be initiated while awaiting the source patient's results and continued for 28 days, with follow-up at 4 and 12 weeks.[21] Postexposure prophylaxis (PEP) regimens typically consist of 3 drugs with low adverse effects and minimal risk of development of HIV resistance. Routine laboratory tests are not needed to assess for ART drug toxicity during the duration of treatment. PEP can be discontinued if the source patient is determined to be negative for HIV (see Image. Postexposure Prophylaxis for HIV).[21]
Care and Treatment of HIV/AIDS Patients
Risks and behaviors associated with HIV/AIDS
HIV can be transmitted through bodily secretions through sexual contact, blood, and pregnancy.[22] Specific risk behaviors can increase the chance of disease transmission, including:
- Injection and noninjection drug use
- Unprotected sex
- Multiple sexual partners
- Exchange of sex for money or drugs
- Use of alcohol or drugs before or during sexual intercourse [23]
HIV cannot be transmitted through casual contact with saliva, eg, kissing, spitting, or sharing drinks.[24]
Goals of HIV/AIDS treatment
Currently, HIV has no vaccine or cure, though clinical trials and studies continue to be performed. ART, when started early, has enabled people with HIV to live long lives with chronic infection.[2] The Centers for Disease Control and Prevention (CDC) aims to implement a 95-95-95 plan, where 95% of people infected with HIV have been diagnosed, 95% with diagnosed infection are on ART, and 95% of those on ART have decreased viral load.[25]
Antiretroviral treatment for patients infected with HIV
Individuals should be tested for drug resistance before beginning treatment with ART, allowing physicians to choose the most effective medications.[26] ART should be started immediately, regardless of CD4 cell count or viral load. The World Health Organization (WHO) advises a 1-month course of ART with at least 3 medications as postexposure prophylaxis.[27]
Benefits of ART include:
- Better clinical outcomes
- Decrease in viral load and transmission
- Delay in disease progression
- Reduced morbidity and mortality
- Prevention of immune system decline [28]
Limitations of ART include:
- Daily adherence
- Long-term medication toxicity
- Cost of treatment
- Limited options for those with multiclass resistance [29]
Types of ART medications
Each medication targets a step in the HIV lifecycle. A combination of different classes is used to treat patients with HIV, including:
- Entry inhibitors: maraviroc, fostemsavir, ibalizumab
- Capsid inhibitors: lenacapavir
- Nucleoside reverse transcriptase inhibitors (NRTI): lamivudine, abacavir, emtricitabine, zidovudine
- Nucleotide reverse transcriptase inhibitors (NtRTI): tenofovir (TAF, TDF)
- Non-nucleoside reverse transcriptase inhibitors (NNRTI): doravirine, efavirenz, nevirapine, rilpivirine, etravirine
- Integrase inhibitors: raltegravir, elvitegravir (first generation); bictegravir, cabotegravir, dolutegravir (second generation)
- Protease inhibitors: ritonavir, darunavir, atazanavir, tipranavir
- Pharmacokinetic enhancers: cobicistat, ritonavir [2][30][NIH Office of AIDS Research Advisory Council. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. 2025]
Attitude and Stigma Associated with HIV/AIDS
HIV/AIDS stigma
HIV/AIDS stigma remains a barrier to accessing medical care, prevention, and therapy. Manifestations of stigma vary across cultures, societal beliefs, and group norms. Structural violence (racism, sexism, poverty) coupled with a preexisting stigma against high-risk groups (injection drug users, sex workers, men who have sex with men) enhances the power stigma has on the HIV/AIDS epidemic, ultimately leading to decreased diagnosis, treatment, and care. Stigma arises from a convergence of labeling, stereotyping, separating, and discriminating.[31]
Counteracting HIV/AIDS Stigma
Strategies to counteract HIV/AIDS stigma include:
- Understand how HIV is transmitted and who can become infected.
- Advocate for laws and policies to end the stigma against men who have sex with men, sex workers, injection drug users, and migrants.
- Support organizations rallying to end discrimination against people infected with HIV.
- Assist families and communities of those infected or affected.
- Learn about legal consequences and policy actions.
- Support routine HIV testing.[31]
Other Issues
Current Florida Law on AIDS and the Impact on HIV Testing
Legislative intent
The Florida legislature designs laws regarding HIV and other sexually transmitted diseases to provide patients with privacy, confidentiality, and dignity.
Informed consent
Informed consent for HIV testing must include an explanation to the patient regarding confidentiality, mandatory reporting, and the opportunity for anonymous testing. Florida statutes maintain that in a healthcare setting, a patient must be notified of a planned HIV test, and they have the right to refuse the test, which will be documented in the patient’s chart. If they have signed a general consent form for medical care, a separate consent for an HIV test is not required. In a non-healthcare setting, specific informed consent for HIV testing is required. A legal guardian may provide informed consent if a person is incompetent, incapacitated, or a legal minor.
Confidentiality
Information regarding a person’s HIV status must be kept confidential, except for the following:
- The patient gives consent
- Given for statistical purposes and excluding identifying information
- Made to mandatory reporting to medical personnel, state agencies, or mandated court jurisdiction
- Disclosed during a medical emergency, only sharing relevant information for the patient’s care
If an individual violates confidentiality, the person commits a first-degree misdemeanor, punishable by a fine of up to $1,000 and up to 1 year in prison. Any person who spreads information about an individual with HIV or another sexually transmitted disease for monetary gain or with malicious intent commits a felony in the third degree. This is punishable by a fine of up to $5,000 or imprisonment of up to 5 years.
Reporting Results
The Florida Department of Health will keep information confidential and private. The diagnosis of HIV or AIDS must be reported to the Florida Department of Health within 2 weeks of the positive test result. Any positive HIV or AIDS results must be reported using the system developed by the CDC or an equivalent system to ensure confidentiality. The Department of Health may fine anyone who fails to report HIV or AIDS up to $500 for each offense, and a regulatory agency will be informed of the violation.[Florida State Statutes. Title XXIX Public Health, Chapter 381 Public Health: General Provisions. 2025]
Preliminary and Confirmatory Testing
In 2014, the CDC updated testing guidelines. They recommend screening with an HIV-1/2 antigen/antibody test. If screening is nonreactive, no further testing is required. If HIV-1/2 antigen/antibody testing is reactive, an HIV-1/HIV-2 antibody differentiation test is recommended. If the differentiation test is nonreactive or indeterminate, a qualitative HIV-1 RNA test is recommended to confirm the results (see Image. HIV Diagnostic Algorithm).[32]
Enhancing Healthcare Team Outcomes
HIV is a retrovirus transmitted through exposure to infected blood and body fluids that targets CD4+ T cells, leading to progressive immune dysfunction. Early infection may present with nonspecific symptoms such as fever, lymphadenopathy, rash, and myalgia, followed by an asymptomatic phase characterized by ongoing viral replication and declining CD4+ counts. Without treatment, this progression increases the risk of opportunistic infections and malignancies, defining acquired immunodeficiency syndrome. Diagnosis relies on fourth-generation antigen-antibody testing, with confirmatory assays as indicated. Early initiation of antiretroviral therapy improves survival, reduces viral transmission, and prevents disease progression. Prompt recognition and management of occupational exposures, including timely initiation of postexposure prophylaxis, remain essential to reducing transmission risk. This includes the development and enforcement of standardized protocols, the adoption of safety-engineered medical devices, and the establishment of continuous training programs focused on infection prevention and control.[33]
Interprofessional collaboration enhances patient-centered outcomes through coordinated prevention, diagnosis, and management. Nurses, technicians, and phlebotomists are primarily responsible for the safe collection and initial handling of blood and tissue samples, ensuring adherence to standard precautions. Laboratory personnel play a critical role in maintaining biosafety during sample processing, testing, and disposal. Physicians and advanced practitioners oversee clinical decision-making, while pharmacists contribute to the appropriate selection and management of PEP when indicated. Effective communication, shared decision-making, and timely referral strengthen adherence, reduce complications, and promote comprehensive, systems-based HIV care.
From an ethical perspective, maintaining confidentiality, ensuring informed decision-making, and fostering a culture of safety are paramount. Protecting healthcare workers from occupational exposure not only safeguards their well-being but also directly contributes to patient safety by reducing the risk of bidirectional transmission. Ultimately, coordinated care, continuous education, adherence to safety protocols, and strong communication among all team members enhance overall healthcare outcomes, improve laboratory safety standards, and support a high-performing, patient-centered care environment.
Media
(Click Image to Enlarge)
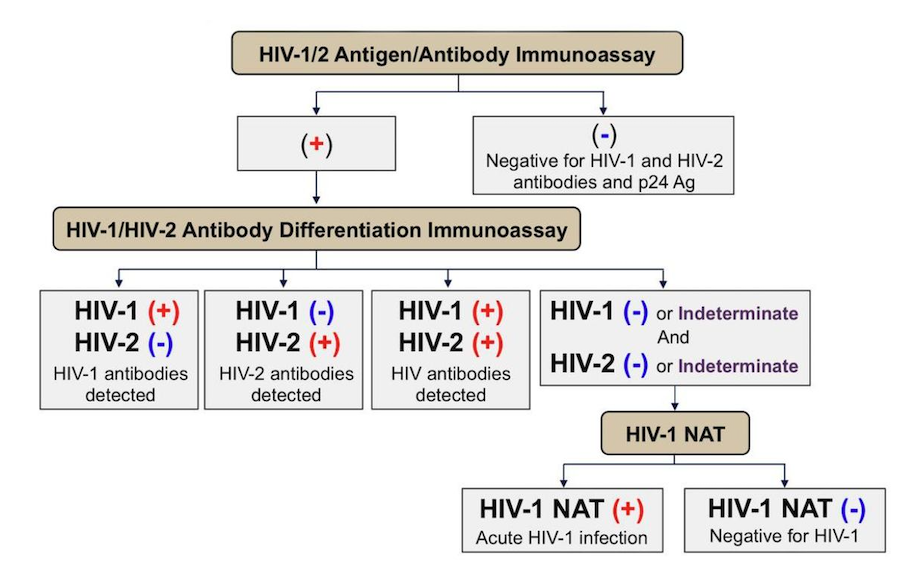
HIV Diagnostic Algorithm. The diagram illustrates the stepwise HIV evaluation process recommended by the Centers for Disease Control and Prevention and Association of Public Health Laboratories, beginning with the HIV-1/2 antigen/antibody immunoassay, followed by the antibody differentiation immunoassay to distinguish HIV-1 from HIV-2, and concluding with nucleic acid testing (NAT) for cases with indeterminate or negative antibody results, ensuring accurate detection of both acute and established infections.
National Center for HIV/AIDS, Viral Hepatitis, and TB Prevention (U.S.). Division of HIV/AIDS Prevention; Association of Public Health Laboratories. 2018 Quick Reference Guide: Recommended Laboratory HIV Testing Algorithm for Serum or Plasma Specimens. Published January 27, 2018.
(Click Image to Enlarge)
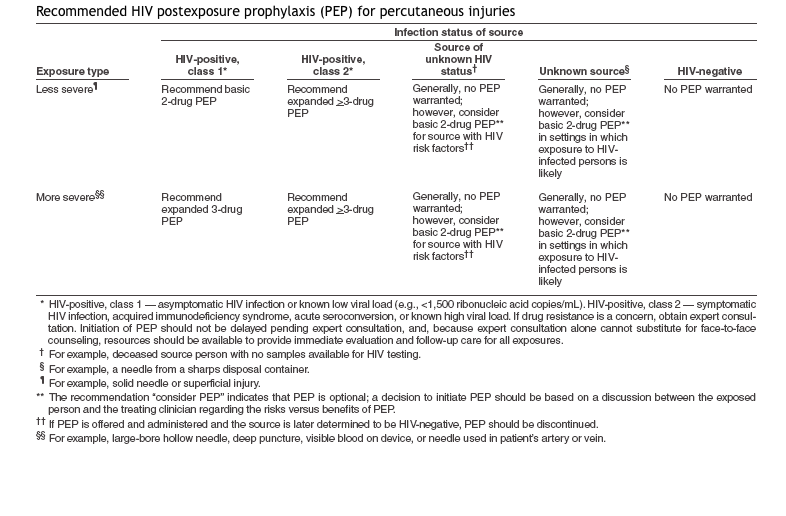
Postexposure Prophylaxis for HIV. Postexposure prophylaxis (PEP) regimens typically consist of 3 drugs with low adverse effects and minimal risk of development of HIV resistance. This illustration shows recommended PEP regimens.
Centers for Disease Control and Prevention
References
Swinkels HM, Samandari T, Huynh K, Gulick PG. HIV Prevention. StatPearls. 2026 Jan:(): [PubMed PMID: 29261888]
Lucas S, Nelson AM. HIV and the spectrum of human disease. The Journal of pathology. 2015 Jan:235(2):229-41. doi: 10.1002/path.4449. Epub [PubMed PMID: 25251832]
Level 3 (low-level) evidenceKumar BV, Connors TJ, Farber DL. Human T Cell Development, Localization, and Function throughout Life. Immunity. 2018 Feb 20:48(2):202-213. doi: 10.1016/j.immuni.2018.01.007. Epub [PubMed PMID: 29466753]
Fanales-Belasio E, Raimondo M, Suligoi B, Buttò S. HIV virology and pathogenetic mechanisms of infection: a brief overview. Annali dell'Istituto superiore di sanita. 2010:46(1):5-14. doi: 10.4415/ANN_10_01_02. Epub [PubMed PMID: 20348614]
Level 3 (low-level) evidenceTurner BG, Summers MF. Structural biology of HIV. Journal of molecular biology. 1999 Jan 8:285(1):1-32 [PubMed PMID: 9878383]
Level 3 (low-level) evidenceKrebs AS, Mendonça LM, Zhang P. Structural Analysis of Retrovirus Assembly and Maturation. Viruses. 2021 Dec 29:14(1):. doi: 10.3390/v14010054. Epub 2021 Dec 29 [PubMed PMID: 35062258]
Mattei S, Flemming A, Anders-Össwein M, Kräusslich HG, Briggs JA, Müller B. RNA and Nucleocapsid Are Dispensable for Mature HIV-1 Capsid Assembly. Journal of virology. 2015 Oct:89(19):9739-47. doi: 10.1128/JVI.00750-15. Epub 2015 Jul 15 [PubMed PMID: 26178992]
Bbosa N, Kaleebu P, Ssemwanga D. HIV subtype diversity worldwide. Current opinion in HIV and AIDS. 2019 May:14(3):153-160. doi: 10.1097/COH.0000000000000534. Epub [PubMed PMID: 30882484]
Level 3 (low-level) evidenceKing KC, Strony R. Needlestick. StatPearls. 2026 Jan:(): [PubMed PMID: 29630199]
Denault D, Goldin J. OSHA Bloodborne Pathogen Standards. StatPearls. 2026 Jan:(): [PubMed PMID: 34033323]
Peng H, Bilal M, Iqbal HMN. Improved Biosafety and Biosecurity Measures and/or Strategies to Tackle Laboratory-Acquired Infections and Related Risks. International journal of environmental research and public health. 2018 Nov 29:15(12):. doi: 10.3390/ijerph15122697. Epub 2018 Nov 29 [PubMed PMID: 30501091]
Moro PL, Moore A, Balcacer P, Montero A, Diaz D, Gómez V, Garib Z, Weniger BG. Epidemiology of needlesticks and other sharps injuries and injection safety practices in the Dominican Republic. American journal of infection control. 2007 Oct:35(8):552-9 [PubMed PMID: 17936148]
Level 2 (mid-level) evidenceReddy VK, Lavoie MC, Verbeek JH, Pahwa M. Devices for preventing percutaneous exposure injuries caused by needles in healthcare personnel. The Cochrane database of systematic reviews. 2017 Nov 14:11(11):CD009740. doi: 10.1002/14651858.CD009740.pub3. Epub 2017 Nov 14 [PubMed PMID: 29190036]
Level 1 (high-level) evidenceJagger J, Deitchman S. Hazards of glass capillary tubes to health care workers. JAMA. 1998 Jul 1:280(1):31 [PubMed PMID: 9660356]
Level 3 (low-level) evidenceShriniwas, Srivastva L, Sengupta D, Lal S. HIV infection control in health care settings. Journal of the Indian Medical Association. 1994 Jan:92(1):33-6 [PubMed PMID: 8207281]
Kramer A, Schwebke I, Kampf G. How long do nosocomial pathogens persist on inanimate surfaces? A systematic review. BMC infectious diseases. 2006 Aug 16:6():130 [PubMed PMID: 16914034]
Level 1 (high-level) evidencePersaud AT, Burnie J, Thaya L, DSouza L, Martin S, Guzzo C. A UV-LED module that is highly effective at inactivating human coronaviruses and HIV-1. Virology journal. 2022 Feb 10:19(1):29. doi: 10.1186/s12985-022-01754-w. Epub 2022 Feb 10 [PubMed PMID: 35144624]
Lin Q, Lim JYC, Xue K, Yew PYM, Owh C, Chee PL, Loh XJ. Sanitizing agents for virus inactivation and disinfection. View (Beijing, China). 2020 Jun:1(2):e16. doi: 10.1002/viw2.16. Epub 2020 May 24 [PubMed PMID: 34766164]
Farrior JB, Rophie SS. Fenestration of the horizontal semicircular canal in congenital conductive deafness. The Laryngoscope. 1985 Sep:95(9 Pt 1):1029-36 [PubMed PMID: 4033323]
Level 3 (low-level) evidenceKofman AD, Struble KA, Heneine W, Gayle B, de Perio MA, Okasako-Schmucker DL, So CN, Anderson LE, Stone EC, Henderson DK, Kuhar DT. 2025 US Public Health Service Guidelines for the Management of Occupational Exposures to Human Immunodeficiency Virus and Recommendations for Post-exposure Prophylaxis in Healthcare Settings. Infection control and hospital epidemiology. 2025 Sep:46(9):863-873. doi: 10.1017/ice.2025.10254. Epub 2025 Sep 15 [PubMed PMID: 41569270]
Gandhi RT, Bedimo R, Hoy JF, Landovitz RJ, Smith DM, Eaton EF, Lehmann C, Springer SA, Sax PE, Thompson MA, Benson CA, Buchbinder SP, Del Rio C, Eron JJ Jr, Günthard HF, Molina JM, Jacobsen DM, Saag MS. Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2022 Recommendations of the International Antiviral Society-USA Panel. JAMA. 2023 Jan 3:329(1):63-84. doi: 10.1001/jama.2022.22246. Epub [PubMed PMID: 36454551]
Patel P, Borkowf CB, Brooks JT, Lasry A, Lansky A, Mermin J. Estimating per-act HIV transmission risk: a systematic review. AIDS (London, England). 2014 Jun 19:28(10):1509-19. doi: 10.1097/QAD.0000000000000298. Epub [PubMed PMID: 24809629]
Level 1 (high-level) evidenceBrunini SM, Barros CVL, Guimarães RA, Galdino Júnior H, Rezza G, Santos JR, da Cunha VE, Sousa JM, Ferreira PM, Barros DAC. HIV infection, high-risk behaviors and substance use in homeless men sheltered in therapeutic communities in Central Brazil. International journal of STD & AIDS. 2018 Nov:29(11):1084-1088. doi: 10.1177/0956462418767188. Epub 2018 Jun 3 [PubMed PMID: 29862902]
Younai FS. Oral HIV transmission. Journal of the California Dental Association. 2001 Feb:29(2):142-8 [PubMed PMID: 11324114]
Nxumalo CT, Buthelezi U, Chiya H, Makgobole MU, Mpofana N, Mgwaba T, Luvuno Z. Achieving the fast track 90-90-90 and 95-95-95 targets in sub-Saharan Africa: A rapid review. Journal of public health in Africa. 2025:16(1):691. doi: 10.4102/jphia.v16i1.691. Epub 2025 Apr 21 [PubMed PMID: 40356732]
Clutter DS, Jordan MR, Bertagnolio S, Shafer RW. HIV-1 drug resistance and resistance testing. Infection, genetics and evolution : journal of molecular epidemiology and evolutionary genetics in infectious diseases. 2016 Dec:46():292-307. doi: 10.1016/j.meegid.2016.08.031. Epub 2016 Aug 29 [PubMed PMID: 27587334]
Elliott T, Sanders EJ, Doherty M, Ndung'u T, Cohen M, Patel P, Cairns G, Rutstein SE, Ananworanich J, Brown C, Fidler S. Challenges of HIV diagnosis and management in the context of pre-exposure prophylaxis (PrEP), post-exposure prophylaxis (PEP), test and start and acute HIV infection: a scoping review. Journal of the International AIDS Society. 2019 Dec:22(12):e25419. doi: 10.1002/jia2.25419. Epub [PubMed PMID: 31850686]
Level 2 (mid-level) evidenceSabin CA, Lundgren JD. The natural history of HIV infection. Current opinion in HIV and AIDS. 2013 Jul:8(4):311-7. doi: 10.1097/COH.0b013e328361fa66. Epub [PubMed PMID: 23698562]
Level 3 (low-level) evidenceSolomon DA, Sax PE. Current state and limitations of daily oral therapy for treatment. Current opinion in HIV and AIDS. 2015 Jul:10(4):219-25. doi: 10.1097/COH.0000000000000165. Epub [PubMed PMID: 26049945]
Level 3 (low-level) evidenceGandhi RT, Landovitz RJ, Sax PE, Smith DM, Springer SA, Günthard HF, Thompson MA, Bedimo RJ, Benson CA, Buchbinder SP, Crabtree-Ramirez BE, Del Rio C, Eaton EF, Eron JJ Jr, Hoy JF, Lehmann C, Molina JM, Jacobsen DM, Saag MS. Antiretroviral Drugs for Treatment and Prevention of HIV in Adults: 2024 Recommendations of the International Antiviral Society-USA Panel. JAMA. 2025 Feb 18:333(7):609-628. doi: 10.1001/jama.2024.24543. Epub [PubMed PMID: 39616604]
Mahajan AP, Sayles JN, Patel VA, Remien RH, Sawires SR, Ortiz DJ, Szekeres G, Coates TJ. Stigma in the HIV/AIDS epidemic: a review of the literature and recommendations for the way forward. AIDS (London, England). 2008 Aug:22 Suppl 2(Suppl 2):S67-79. doi: 10.1097/01.aids.0000327438.13291.62. Epub [PubMed PMID: 18641472]
Burudpakdee C, Near AM, Tse J, Faccone J, Rodriguez PL, Karichu JK, Cheng MM. Real-world HIV diagnostic testing patterns in the United States. The American journal of managed care. 2022 Feb 1:28(2):e42-e48. doi: 10.37765/ajmc.2022.88826. Epub 2022 Feb 1 [PubMed PMID: 35139295]
Ballout RA, Diab B, Harb AC, Tarabay R, Khamassi S, Akl EA. Use of safety-engineered devices by healthcare workers for intravenous and/or phlebotomy procedures in healthcare settings: a systematic review and meta-analysis. BMC health services research. 2016 Sep 1:16():458. doi: 10.1186/s12913-016-1705-y. Epub 2016 Sep 1 [PubMed PMID: 27581947]
Level 1 (high-level) evidence