Introduction
Tumors of the lacrimal gland fossa account for about 10% of all biopsied orbital masses.[1] There is a wide variety of etiologies for these masses, including infectious, inflammatory, and neoplastic.[1][2] Furthermore, neoplastic lesions can either be benign or malignant. This topic focuses on malignant lacrimal gland tumors (broadly called lacrimal gland carcinomas). Since the lacrimal gland fossa is in the anterior superolateral orbit, space-occupying lesions of this area of the orbit typically cause inferior and medial globe displacement.
Proptosis is not always present but may occur when the posterior growth of a mass pushes the eye forward. Most malignant lesions grow more quickly than benign lesions, with a median interval from onset to diagnosis of less than 6 months, compared with 1 to 2 years for benign lesions.[3] Malignant lacrimal gland lesions generally carry a poor prognosis; thus, quick and early identification is critical to improving a patient's morbidity and mortality. See Image. Lacrimal Gland Malignancy.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Tumors of the lacrimal gland are similar to those of the salivary glands because of their shared embryologic origins. The proliferative cell type can organize tumors, and the most common distinction is between epithelial and non-epithelial tumors.[4]
Epithelial
Nearly 50% of epithelial tumors of the lacrimal gland are malignant, though this may depend on referral patterns, geographic location, and patient population.[1][5] Adenoid cystic carcinoma (ACC) is the most common malignant epithelial tumor, accounting for 66% of such cases. It commonly presents with globe displacement, proptosis, and ptosis; pain and frontotemporal numbness are more specific symptoms, as adenoid cystic carcinoma is classically known for invading orbital nerves.[6]
Carcinoma ex pleomorphic adenoma (CEPA, also known as pleomorphic adenocarcinoma or malignant mixed tumor) is the second most common type of epithelial malignancy and, as the name suggests, transforms from a benign pleomorphic adenoma tumor, either from a previously biopsied or resected tumor (if taken piecemeal or if the capsule was ruptured during removal), or de novo from a primary pleomorphic adenoma without prior surgery.[2][7] This transformation can occur years or decades after the primary pleomorphic adenoma is treated. The malignant component can be any epithelial cell type, but most commonly it is adenocarcinoma not otherwise specified or mucoepidermoid carcinoma.
Mucoepidermoid carcinoma (MEC) and adenocarcinoma not otherwise specified (NOS) are the next most common types. Mucoepidermoid carcinoma is a common salivary gland tumor but a rare lacrimal gland tumor. Adenocarcinoma NOS is a primary adenocarcinoma of the lacrimal gland that does not have features of the other listed types. Other epithelial malignancies include ductal carcinoma (similar to mammary ductal carcinoma), acinic cell carcinoma, myoepithelial carcinoma, epithelial-myoepithelial carcinoma, cystadenocarcinoma, carcinosarcoma, polymorphous low-grade adenocarcinoma, sebaceous cell carcinoma, squamous cell carcinoma, and basal cell carcinoma.
Lymphoid
The overwhelming majority of lacrimal gland lymphomas are non-Hodgkin lymphomas. The most common subtype is extranodal marginal zone lymphoma (EMZL, MALT lymphoma), which makes up to 40% of lacrimal gland lymphomas. It may also be associated with inflammatory diseases, including reactive (benign) lymphoid hyperplasia, IgG4-related disease, Sjogren syndrome, and gastric Helicobacter pylori infection.[8][9]
Other subtypes include follicular lymphoma, diffuse large B-cell lymphoma (DLBCL), mantle cell lymphoma, and chronic lymphocytic leukemia/small lymphocytic lymphoma. Lymphomas present with painless growth and usually minimal signs of inflammation. Orbital lesions often precede systemic lymphoma presentation, but the disease may be isolated to just the orbit without ever developing systemic disease.
Mesenchymal
Malignant mesenchymal tumors of the lacrimal gland are very rare, with vascular lesions most common.[4]
Metastasis
Metastases to the lacrimal gland from systemic cancers are exceedingly rare because the lacrimal gland lacks lymph nodes. These cases are described in the literature in isolated case reports, and the most common primary site is the breast.[8][10]
Epidemiology
In general, lacrimal gland carcinomas do not show a gender preference, though some exceptions exist. Adenocarcinoma NOS and ductal carcinoma have a slight predilection for males, whereas MEC and lymphoma have a slight female predilection.[11][12] All types of malignant lesions can occur at any age, but most are typically found in older adults (6th decade or later).[5] The notable exception to this is adenoid cystic carcinoma, which has an average age of diagnosis of 40 years. There is no racial or geographic preference for tumors, though this may be because they are rare overall.
Pathophysiology
Malignant tumors arise from genetic changes involving oncogenes and tumor suppressor genes. Some of these changes have been characterized by specific lacrimal gland neoplasms (see Image. Lacrimal Gland Lymphoma, 25× view). For adenoid cystic carcinoma, abnormalities in MYB or MYB-NFIB protein expression have been identified. They may serve as critical events in the oncogenic process (see Image. Lacrimal Gland Adenoid Cystic Carcinoma, 25×).
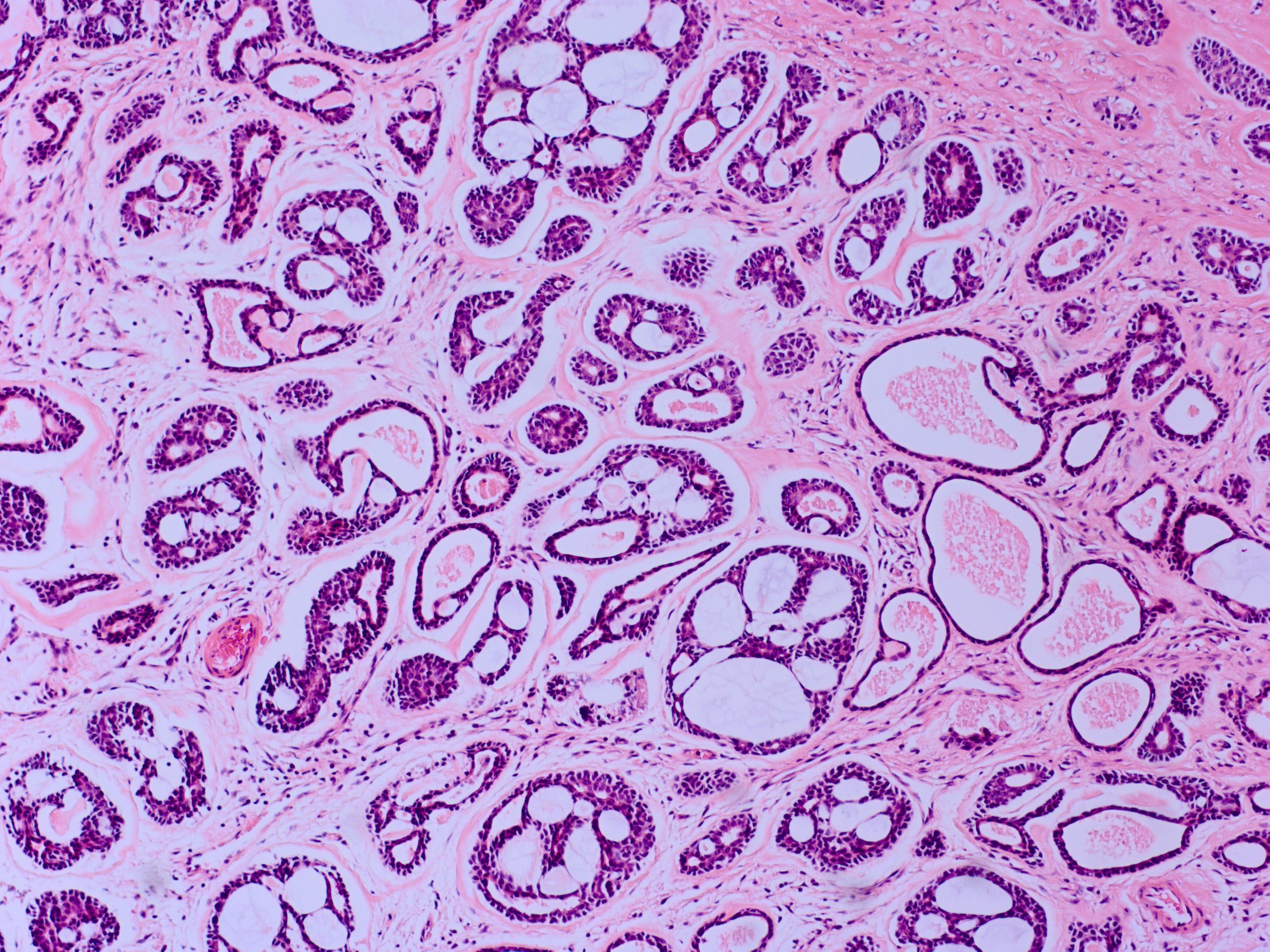
Carcinoma ex pleomorphic adenoma tumors likely have the same underlying genetic abnormalities as pleomorphic adenomas, such as PLAG1, and these genetic abnormalities are present in the corresponding tumor's malignant component (see Image. Lacrimal Gland Pleomorphic Adenoma, 25×). Mucoepidermoid carcinoma of the salivary gland has been shown to harbor a translocation between chromosomes 11 and 19, resulting in a fusion of the oncogenes CRTC1 and MAML2; lacrimal gland MEC tumors are similarly characterized.[13]
Ductal carcinomas frequently exhibit HER2 and androgen receptor positivity and are always ER and PR negative. In lymphoma, EMZL exhibits translocations between chromosomes 14 and 18, or between chromosomes 3 and 14; follicular lymphoma has translocations between chromosomes 14 and 18, and mantle cell lymphoma has translocations between chromosomes 11 and 14.[8]
Histopathology
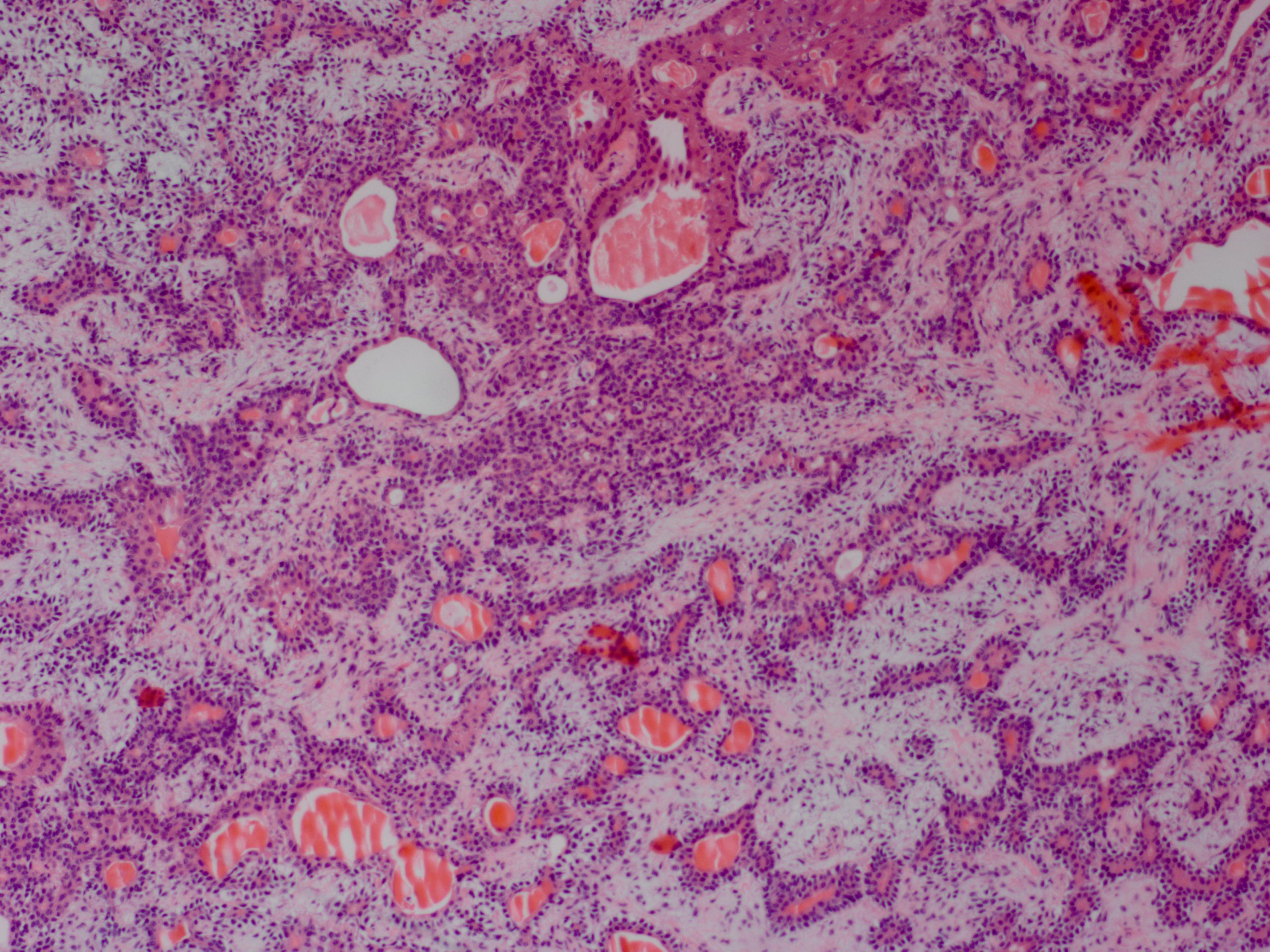
Adenoid cystic carcinoma has multiple histological forms. The most common pattern is the cribriform (Swiss cheese) pattern, characterized by nests of myoepithelial and ductal cells, with cylindrical cystic structures filled with hyaline basal lamina or basophilic mucoid (glycosaminoglycan) material.[3] The other forms are tubular and solid, and typically a mixture of these forms is present within a single tumor. The neoplasm is usually unencapsulated and shows infiltration into the surrounding tissue. Perineural growth is characteristic.
Carcinoma ex pleomorphic adenoma requires histologic evidence of both benign (pleomorphic adenoma precursor) and malignant components, with a transition zone between them. The malignant component may appear as any of the other malignant epithelial lesions listed above (with adenocarcinoma NOS or MEC being the most common), or it may be undifferentiated.
Adenocarcinoma NOS is characterized by cells with glandular or ductal differentiation but lacks distinctive features of other tumors and cannot be classified further. On examination, mucoepidermoid carcinoma is composed of 3 cell types: epidermoid-squamous cells, mucin-producing cells, and intermediate cells. Ductal carcinoma resembles mammary ductal carcinoma and is composed of solid epithelial nests in an infiltrative, lobular, or cribriform arrangement and usually has a high mitotic rate and areas of necrosis.[10][14]
EMZL reveals diffusely-infiltrating small cells with abundant cytoplasm and slightly indented nuclei without nucleoli. Follicular lymphoma exhibits a partially follicular growth pattern, with closely packed neoplastic cells lacking mantle zones. DLBCL is characterized by diffusely growing large B cells with nuclei twice the size of normal lymphocytes and has many morphologic variants. Mantle cell lymphoma exhibits a monotonous pattern of small to medium lymphocytes with scant cytoplasm, irregular nuclei, and no nucleoli.
History and Physical
Demographic data is essential to collect, including age, gender, ethnicity, and race. Systemic medical history is also vital for ascertaining possible etiologies, including a history of recent illness; autoimmune or inflammatory disease; cancer or chemotherapy and/or radiation; systemic immunosuppression; and prior trauma or surgery. A comprehensive review of systems may identify associations with systemic autoimmune or inflammatory diseases.
Obtain a thorough ophthalmologic history regarding blurry vision, double vision, change in outward appearance or facial symmetry, pain, light sensitivity, pain with eye movement, eyelid swelling or redness, discharge, tenderness, or dryness. Consider comparing old photographs to evaluate changes in eye or eyelid position or appearance.
A complete eye exam by a trained optometrist, ophthalmologist, or oculoplastic and orbital surgeon should be performed. This includes assessing visual acuity for decreased vision, pupillary light reflexes for adequate responses, the presence of a relative afferent pupillary defect (rAPD), and other signs of optic neuropathy, such as color vision deficits, red-light saturation, and visual field defects.
Evaluating ocular motility can provide the degree of any limitations and the presence and pattern of diplopia. It is also prudent to assess globe malposition, particularly inferiorly and medially, in cases of lacrimal gland tumors, and to perform exophthalmometry to evaluate proptosis. Digital palpation of the orbit and lacrimal gland may identify masses, and there may be resistance to retropulsion of the globe if a mass is present.
Palpation of regional lymph nodes can reveal lymphadenopathy. Hypoesthesia of the first or second divisions of the trigeminal nerve should be checked to evaluate for orbital nerve compression or invasion. There may be eyelid edema, erythema, or warmth, and a directly visualized enlarged and tender lacrimal gland with secondary upper lid ptosis or S-shaped lid deformity. The conjunctiva may be injected, especially overlying the area of the lacrimal gland. An intraocular exam is also needed to evaluate for signs of uveitis.
Evaluation
It may be difficult to distinguish between benign and malignant lesions based on clinical evaluation alone. A more rapid onset may hint towards a more aggressive or malignant process. If there was initially slow progression that subsequently became rapid, it could indicate malignant transformation of a pleomorphic adenoma into carcinoma ex pleomorphic adenoma. The presence or absence of pain can also help predict the nature of the offending lesion, as the most common malignant lesion, adenoid cystic carcinoma, can exhibit perineural invasion. Orbital imaging is usually helpful and often necessary to confirm and characterize a suspected orbital lesion. Characteristics to discern include whether the tumor is solid versus cystic, well-defined versus infiltrative, the presence or absence and amount of calcification, the presence of fat or fluid, bony remodeling or destruction, and contrast enhancement.[15][16] Extension of a mass posteriorly towards the orbital apex ("wedge sign") is a finding that correlates with disease of concern and the need for biopsy.[17]
Computed tomography is expedient, widely available, cost-effective, and especially helpful for lacrimal fossa anatomy. It is widely regarded as the initial imaging modality of choice for lacrimal gland lesions, particularly when a benign tumor is suspected. It can identify the presence and size of a mass and its effects on surrounding structures, such as the bone (most importantly), extraocular muscles, and the globe. Contrast administration is also helpful for identifying and enhancing lesions. Computed tomography scans also readily show calcification within a lesion, which can help differentiate the offending mass.
Magnetic resonance imaging (MRI) is more expensive, more difficult to obtain, and has a longer acquisition time, but provides superior soft-tissue detail. The various image processing sequences enable detailed characterization of the mass in question, and DWI may delineate benign from malignant.[18]
Unlike computed tomography, MRI has limited bone visualization but can better evaluate tumor involvement of orbital nerves, which is important for adenoid cystic carcinoma.[16] Because of this, it may be a better imaging modality when a malignant lesion is suspected. Many cases may require both computed tomography and MRI before further management decisions are made. See Image. Adenoid Cystic Carcinoma.
Treatment / Management
The management of malignant lacrimal gland tumors has not been clearly established because of their rarity and poor prognosis. Yet, the established treatment goals are local tumor control and prevention of both local recurrence and distant metastases.[19]
The first step in all suspected malignancies is establishing a formal histological diagnosis, usually achieved via incisional biopsy. In some cases, small or easily accessible lesions can be excised in their entirety. Treatment can then be directed by tumor grading and staging. Historically, the treatment of most lacrimal gland carcinomas has included orbital exenteration with or without bone removal and adjuvant high-dose radiation 4 to 6 weeks after surgery.
Adenoid cystic carcinoma has had developments in treatment strategies, though there is still no widespread consensus. Treatment may involve a combination of tumor removal, radiation therapy, and orbital exenteration with varying survival rates.[20] There has been a push towards globe-sparing surgery due to the functional, cosmetic, and psychological morbidity of orbital exenterations, with similar survival results.[21][22]
More recently, intra-arterial cytoreductive chemotherapy (IACC) has been used successfully before orbital exenteration and radiation therapy and may be combined with globe-sparing surgery and adjuvant radiation therapy.[23] Nonetheless, extensive surgery may still be indicated for locally advanced cases, but it does not prevent metastasis or improve survival.[24] (B3)
The treatment of carcinoma ex pleomorphic adenoma depends on the histologic grade and stage at presentation. An isolated, well-defined mass may be treated with excisional surgery alone without radiation. On the other hand, ill-defined lesions invading the tumor capsule or surrounding orbital tissue are often treated similarly to ACC with excision, possible orbital exenteration, and adjuvant radiation therapy.[25]
Adenocarcinoma NOS and the other malignant lesions are usually treated similarly to ACC with exenteration and radiation therapy. If only a microscopic tumor is present on histopathology, plaque radiation therapy can be considered a treatment option for any lacrimal gland malignancy.[26]
The management of ocular adnexal lymphoma depends on the extent of systemic involvement. First, an incisional biopsy is necessary to establish the diagnosis and determine the lymphoma subtype and its genetic characteristics. This is followed by a systemic workup by an oncologist, which may include systemic imaging and/or a bone marrow biopsy. Unlike other lacrimal gland malignancies, definitive treatment of lymphoma is not surgical. If the lymphoma is confined to the orbit, external-beam radiation therapy is the established initial treatment, except for DLBCL and mantle cell lymphoma, which are treated with chemotherapy.[18] Chemotherapy is indicated if there is systemic involvement, with possible radiation therapy as needed in select cases.(B3)
Differential Diagnosis
In addition to the malignant lesions above, other etiologies can present as lacrimal gland fossa lesions. Two major categories for these other causes are inflammatory lesions and benign tumors. Inflammatory lesions are the most common cause of lacrimal gland enlargement.[5] The single most common etiology is dacryoadenitis, which can be unilateral or bilateral and inflammatory or infectious.
Inflammatory Lesions
- Idiopathic orbital inflammatory syndrome (IOIS), or orbital pseudotumor
- IgG-4-related disease
- Sarcoidosis
- Granulomatosis with polyangiitis
- Dacryoadenitis
- Sjogren syndrome
- Thyroid eye disease [2]
Benign Tumors
- Epithelial
- Pleomorphic adenoma
- Dacryops (lacrimal gland cyst)
- Oncocytoma
- Myoepithelioma
- Cystadenoma
- Warthin tumor
- Lymphoproliferative
- Reactive lymphoid hyperplasia (benign lymphoepithelial lesion)
- Mesenchymal
Some lesions are located near the superolateral orbit and may be mistaken for lacrimal gland tumors. They include:
- Epidermoid or dermoid cyst, commonly found at the frontozygomatic suture, and may have an intraorbital component
- Prolapsed orbital fat, causing fullness of the lateral upper lid or a mass in the superotemporal fornix
- Dermatolipoma, commonly seen under the superotemporal conjunctiva
- Prolapsed lacrimal gland, giving the appearance that a mass has displaced it
Lacrimal gland enlargement can also be seen in amyloidosis. Although rare, amyloid deposition in the orbit, including the lacrimal gland, is usually due to a localized disease process rather than systemic amyloidosis.[27]
Staging
Because of their common embryologic origin, lacrimal gland tumors are classified with salivary gland tumors under the World Health Organization classification system.[28] Lacrimal gland tumor staging is based on the American Joint Committee on Cancer (AJCC) 8th edition.[29] Lacrimal gland lymphomas are staged similarly to other ocular adnexal lymphomas as per the AJCC.[30]
Prognosis
Since adenoid cystic carcinoma is the most common malignant tumor, it has the most prognostic data of the lacrimal gland carcinomas. Overall, the prognosis is poor, and ACC has often been referred to as the "slow killer" since recurrences and metastasis can occur years after treatment, with most patients dying within 10 years of diagnosis. Several prognostic factors have been identified in the literature, including tumor size, histologic subtype, perineural invasion, and the stage at diagnosis.[31]
Tumor size is 1 of the most important factors, with a better prognosis for tumors less than 2.5 cm in greatest diameter.[24] Histologically, these tumors typically have multiple subtypes. Still, the predominance of the cribriform (Swiss cheese) pattern may be a positive prognostic factor, whereas a predominance of "basaloid" or solid pattern may be a negative factor.[32][33][34] The AJCC TNM stage does reasonably well with predicting outcomes of patients, with a worse prognosis for recurrence, metastasis, and death for tumors less than stage T3a than for those with stage T3a or greater.
For carcinoma arising from pleomorphic adenoma, prognosis depends on the identity and behavior of the malignant component that has spread beyond the capsule of the original tumor. If the tumor is non- or minimally invasive, the prognosis is excellent. Otherwise, most patients die within a few years due to intracranial spread and metastases to the lungs, chest, and bone.[3][10]
Mucoepidermoid carcinoma is organized into low, intermediate, and high-grade tumors. The low and intermediate tumors carry a good prognosis, but high-grade tumors have a poor survival rate.[3] Ductal carcinoma is an aggressive neoplasm that usually presents as locally advanced disease that is difficult to control, with a mortality rate of over 40%. Metastases develop in more than 50% of cases.
The prognosis for lymphoma overall is good, though it depends on the extent of systemic involvement. For extranodal marginal zone lymphoma localized to just the orbit, it is very good, as it is usually sensitive to radiation therapy. Diffuse large B-cell lymphoma has 3 subtypes, with the ABC subtype having the poorest prognosis.[8]
Complications
Complications of malignant tumors are mostly related to the treatment involved in eradicating the tumor and preventing recurrences. Large tumors may compress orbital structures, including the globe and optic nerve. Malignant lesions may erode through the orbital roof to gain access to the intracranial vault, or in the case of adenoid cystic carcinoma, may spread via the perineural route to access the CNS, where severe neurologic changes may manifest.
Surgical biopsy or excision carries risks, and complications are related to the surgery performed and the techniques utilized. For anterior or lateral orbitotomies, the main complications of note include orbital hemorrhage, postoperative orbital cellulitis, damage to the extraocular muscles, globe, or optic nerve, dryness from decreased lacrimal gland function, cerebral spinal fluid (CSF) leak, or recurrence of the tumor.
Radiation therapy can also have adverse effects, including damage to surrounding tissues, skin dermatitis, bone and soft-tissue atrophy, and ocular effects such as retinopathy and dry eye disease. Chemotherapy can lead to many side effects, the most concerning being immunosuppression and the risk of infection. Vigilant short- and long-term monitoring after treatment is crucial to managing these complications and monitoring for tumor recurrences.
Deterrence and Patient Education
The management of malignant tumors in an area such as the orbit can be quite complicated. A thorough discussion is necessary to inform the patient of the potential causes, treatments, adverse events, and prognosis of both the disease processes involved and the treatment options. Whenever cancer is being discussed as a diagnosis, it is critical to approach the patient and situation with compassion and empathy. At times, this may require multiple discussions to allow the patient to process the information appropriately and make an informed decision.
The risks, benefits, and alternatives of any treatment (or lack of treatment) should be thoroughly explained. The emotional and psychological impact of the diagnoses and the treatments (surgery, chemotherapy, radiation, and long-term monitoring for recurrence), as well as any complications that arise, may require multidisciplinary care from a primary care provider, oncologist, psychologist, or psychiatrist.
Pearls and Other Issues
When evaluating any patient with an orbital mass, keeping a broad differential diagnosis is vital. A thorough history and clinical exam are paramount for determining risk factors for various disease processes and guiding diagnostic workup and treatment acuity. Malignant lesions often carry a poor prognosis; therefore, prompt evaluation and treatment are essential.
Inflammatory signs are uncommon in tumors and may indicate infectious or inflammatory dacryoadenitis. Pain or hypoesthesia is often an indicator of malignancy, as most benign lesions are painless. Imaging is equally important for diagnosis and treatment decision-making; it can also aid surgical planning. The treatment of malignant tumors requires a multi-specialty approach with physicians experienced in managing these orbital tumors and their complications.
| Adenoid Cystic Carcinoma | Orbital Lymphoma | |
| Age of onset | Middle Age | Older Adults |
| Gender | Male | Female |
| Associated Pain | Yes | No |
| Duration of onset | Acute | Indolent |
| Histopathology | Various Unencapsulated | Monoclonal sheet Unencapsulated |
| Treatment | Combination Therapy Excision/Radiation/Exenteration | Radiation (Local) Chemotherapy (Systemic) |
Enhancing Healthcare Team Outcomes
From start to finish, the journey from clinical evaluation to workup, then diagnosis to management, and subsequent monitoring, treatment response, and managing complications requires a large, interprofessional team of administrators, staff, technicians, nurses, and doctors. The treatments for malignant tumors often involve multiple surgeries, radiation treatments, chemotherapy infusions, and countless office visits. The patient interacts with numerous individuals in the professional setting throughout their care. Effective communication between all parties is necessary to promote the efficient use of medical resources and provide a smooth and effective experience for the patient.
Media
(Click Image to Enlarge)
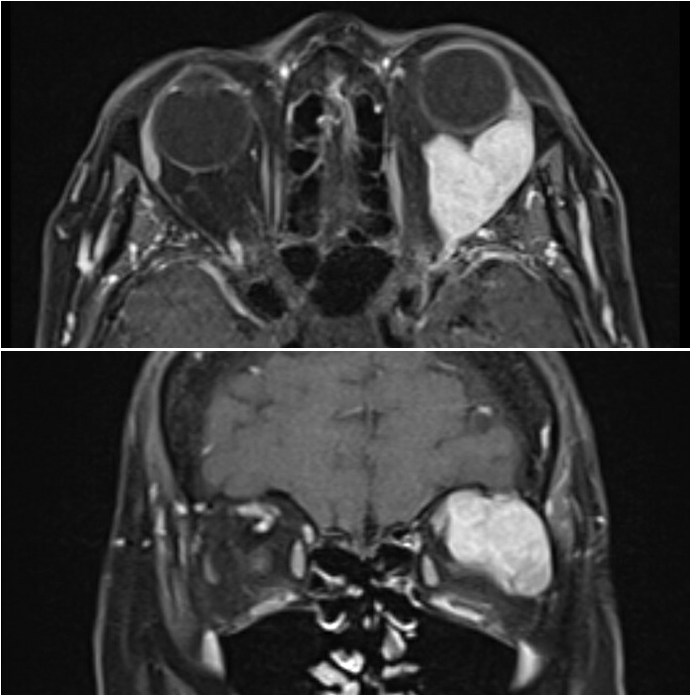
Lacrimal Gland Malignancy. A 45-year-old patient with left eye proptosis and vision changes was found to have a left orbital mass. Post-contrast T1 MRI images show an avidly enhancing solid mass arising from the lacrimal gland fossa extending posteriorly towards the orbital apex, with surrounding erosion of the bone. A biopsy of the mass resulted in a diagnosis of adenoid cystic carcinoma.
Contributed by A Mueller, MD
(Click Image to Enlarge)
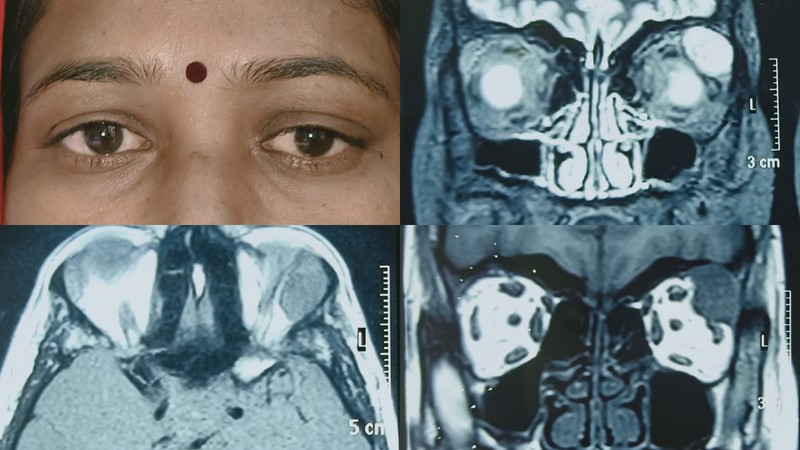
Adenoid Cystic Carcinoma. The clinical photo showed abaxial proptosis on the left side with inferomedial globe dystopia in the left eye. MRI showed a well-defined mass in the lacrimal gland fossa that was hyperintense on T2 and hypointense on T1-weighted images. Histopathological analysis revealed adenoid cystic carcinoma of the lacrimal gland, one of the common lacrimal gland malignancies.
Contributed by M Hada, MD
(Click Image to Enlarge)
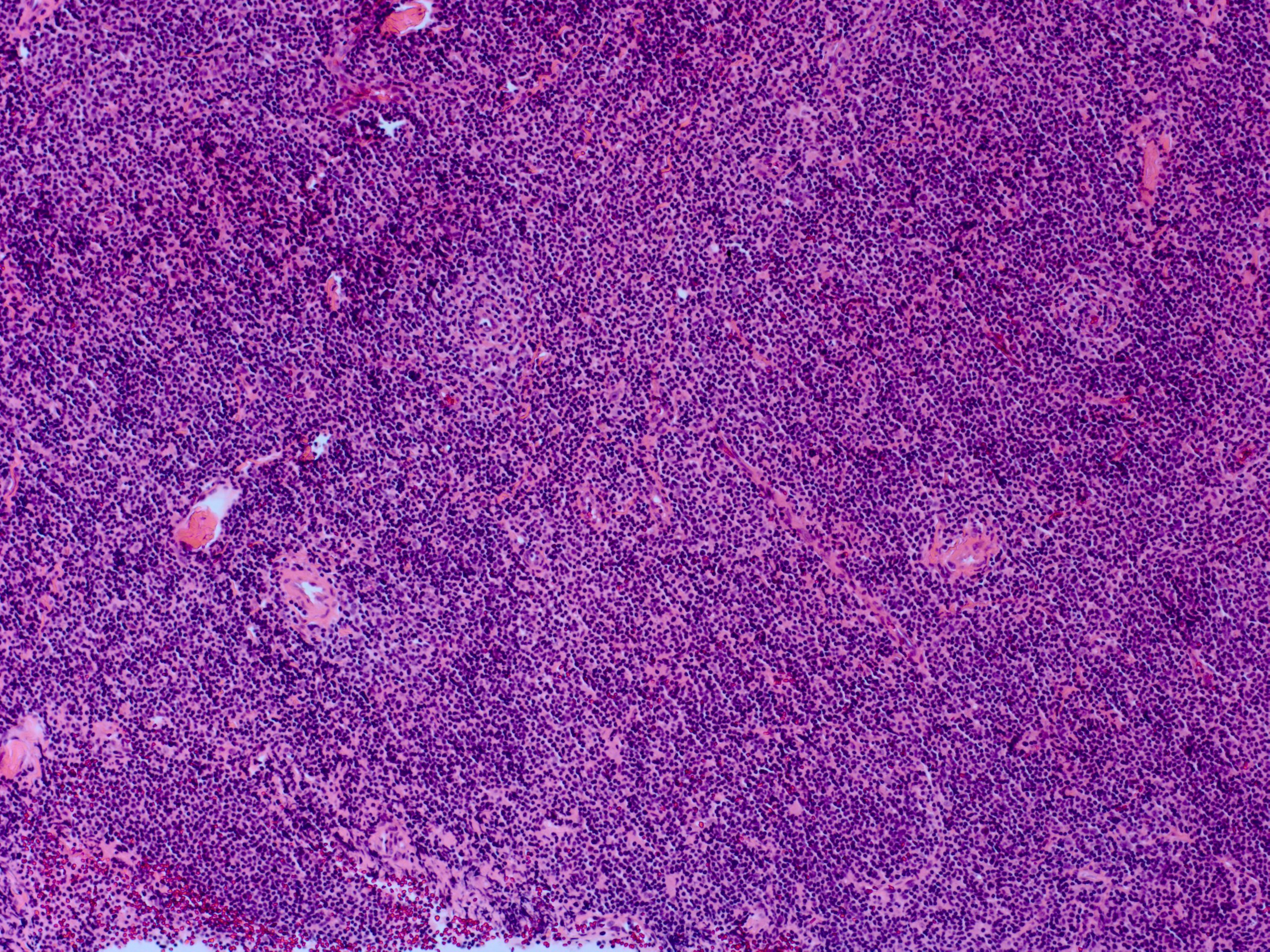
Lacrimal Gland Lymphoma, 25× View
Contributed by H Grossniklaus, MD
(Click Image to Enlarge)
Lacrimal Gland Adenoid Cystic Carcinoma 25×
Contributed by H Grossniklaus, MD
(Click Image to Enlarge)
Lacrimal Gland Pleomorphic Adenoma 25×
Contributed by H Grossniklaus, MD
References
Shields JA, Shields CL, Epstein JA, Scartozzi R, Eagle RC Jr. Review: primary epithelial malignancies of the lacrimal gland: the 2003 Ramon L. Font lecture. Ophthalmic plastic and reconstructive surgery. 2004 Jan:20(1):10-21 [PubMed PMID: 14752304]
Kim JS, Liss J. Masses of the Lacrimal Gland: Evaluation and Treatment. Journal of neurological surgery. Part B, Skull base. 2021 Feb:82(1):100-106. doi: 10.1055/s-0040-1722700. Epub 2021 Feb 18 [PubMed PMID: 33777623]
von Holstein SL, Coupland SE, Briscoe D, Le Tourneau C, Heegaard S. Epithelial tumours of the lacrimal gland: a clinical, histopathological, surgical and oncological survey. Acta ophthalmologica. 2013 May:91(3):195-206. doi: 10.1111/j.1755-3768.2012.02402.x. Epub 2012 Apr 4 [PubMed PMID: 22471335]
Level 3 (low-level) evidencevon Holstein SL,Rasmussen PK,Heegaard S, Tumors of the lacrimal gland. Seminars in diagnostic pathology. 2016 May; [PubMed PMID: 26849904]
Shields CL, Shields JA. Lacrimal gland tumors. International ophthalmology clinics. 1993 Summer:33(3):181-8 [PubMed PMID: 8407184]
Bernardini FP, Devoto MH, Croxatto JO. Epithelial tumors of the lacrimal gland: an update. Current opinion in ophthalmology. 2008 Sep:19(5):409-13. doi: 10.1097/ICU.0b013e32830b13e1. Epub [PubMed PMID: 18772674]
Level 3 (low-level) evidenceCurrie ZI, Rose GE. Long-term risk of recurrence after intact excision of pleomorphic adenomas of the lacrimal gland. Archives of ophthalmology (Chicago, Ill. : 1960). 2007 Dec:125(12):1643-6 [PubMed PMID: 18071115]
Level 3 (low-level) evidenceAndreasen S, Esmaeli B, Holstein SL, Mikkelsen LH, Rasmussen PK, Heegaard S. An Update on Tumors of the Lacrimal Gland. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2017 Mar-Apr:6(2):159-172. doi: 10.22608/APO.201707. Epub [PubMed PMID: 28399336]
Hasosah M, Baothman A, Satti M, Kutbi S, Alghamdi K, Jacobson K. Mucosa-associated lymphoid tissue lymphoma of the lacrimal gland: sustained remission after eradication of helicobacter pylori infection. Case reports in gastrointestinal medicine. 2011:2011():945752. doi: 10.1155/2011/945752. Epub 2011 Dec 7 [PubMed PMID: 22606434]
Level 3 (low-level) evidenceProia AD, Ranjit-Reeves R, Woodward JA. Lacrimal Gland Tumors. International ophthalmology clinics. 2018 Spring:58(2):197-235. doi: 10.1097/IIO.0000000000000220. Epub [PubMed PMID: 29517651]
Rasmussen P, Ralfkiaer E, Prause JU, Sjö LD, Siersma VD, Heegaard S. Malignant lymphoma of the lacrimal gland: a nation-based study. Archives of ophthalmology (Chicago, Ill. : 1960). 2011 Oct:129(10):1275-80. doi: 10.1001/archophthalmol.2011.270. Epub [PubMed PMID: 21987669]
Andreasen S, Grauslund M, Heegaard S. Lacrimal gland ductal carcinomas: Clinical, Morphological and Genetic characterization and implications for targeted treatment. Acta ophthalmologica. 2017 May:95(3):299-306. doi: 10.1111/aos.13310. Epub 2016 Nov 3 [PubMed PMID: 27808478]
Von Holstein SL, Fehr A, Heegaard S, Therkildsen MH, Stenman G. CRTC1-MAML2 gene fusion in mucoepidermoid carcinoma of the lacrimal gland. Oncology reports. 2012 May:27(5):1413-6. doi: 10.3892/or.2012.1676. Epub 2012 Feb 6 [PubMed PMID: 22323114]
Level 3 (low-level) evidenceChawla B, Kashyap S, Sen S, Bajaj MS, Pushker N, Gupta K, Chandra M, Ghose S. Clinicopathologic review of epithelial tumors of the lacrimal gland. Ophthalmic plastic and reconstructive surgery. 2013 Nov-Dec:29(6):440-5. doi: 10.1097/IOP.0b013e31829f3a0c. Epub [PubMed PMID: 24145905]
Jung WS, Ahn KJ, Park MR, Kim JY, Choi JJ, Kim BS, Hahn ST. The radiological spectrum of orbital pathologies that involve the lacrimal gland and the lacrimal fossa. Korean journal of radiology. 2007 Jul-Aug:8(4):336-42 [PubMed PMID: 17673845]
Vaidhyanath R, Kirke R, Brown L, Sampath R. Lacrimal fossa lesions: pictorial review of CT and MRI features. Orbit (Amsterdam, Netherlands). 2008:27(6):410-8. doi: 10.1080/01676830802333667. Epub [PubMed PMID: 19085295]
Lorenzano D, Rose GE. The "Wedge Sign": An Imaging Sign for Aggressive Lacrimal Gland Disease. Ophthalmology. 2017 Jul:124(7):1081-1083. doi: 10.1016/j.ophtha.2017.03.004. Epub 2017 Mar 31 [PubMed PMID: 28372859]
Gündüz AK, Yeşiltaş YS, Shields CL. Overview of benign and malignant lacrimal gland tumors. Current opinion in ophthalmology. 2018 Sep:29(5):458-468. doi: 10.1097/ICU.0000000000000515. Epub [PubMed PMID: 30028745]
Level 3 (low-level) evidenceYang J, Zhou C, Wang Y, Fan X, Jia R. Multimodal therapy in the management of lacrimal gland adenoid cystic carcinoma. BMC ophthalmology. 2019 Jun 8:19(1):125. doi: 10.1186/s12886-019-1110-5. Epub 2019 Jun 8 [PubMed PMID: 31176360]
Woo KI,Yeom A,Esmaeli B, Management of Lacrimal Gland Carcinoma: Lessons From the Literature in the Past 40 Years. Ophthalmic plastic and reconstructive surgery. 2016 Jan-Feb; [PubMed PMID: 26291539]
Bonavolontà P, Esmaeli B, Donna P, Tranfa F, Iuliano A, Abbate V, Fossataro F, Attanasi F, Bonavolontà G. Outcomes after eye-sparing surgery vs orbital exenteration in patients with lacrimal gland carcinoma. Head & neck. 2020 May:42(5):988-993. doi: 10.1002/hed.26073. Epub 2020 Feb 11 [PubMed PMID: 32048377]
Han J, Kim YD, Woo KI, Sobti D. Long-Term Outcomes of Eye-Sparing Surgery for Adenoid Cystic Carcinoma of Lacrimal Gland. Ophthalmic plastic and reconstructive surgery. 2018 Jan/Feb:34(1):74-78. doi: 10.1097/IOP.0000000000000877. Epub [PubMed PMID: 28221296]
Tse DT, Kossler AL, Feuer WJ, Benedetto PW. Long-term outcomes of neoadjuvant intra-arterial cytoreductive chemotherapy for lacrimal gland adenoid cystic carcinoma. Ophthalmology. 2013 Jul:120(7):1313-23. doi: 10.1016/j.ophtha.2013.01.027. Epub 2013 Apr 9 [PubMed PMID: 23582989]
Level 3 (low-level) evidenceWoo KI,Kim YD,Sa HS,Esmaeli B, Current treatment of lacrimal gland carcinoma. Current opinion in ophthalmology. 2016 Sep; [PubMed PMID: 27273588]
Level 3 (low-level) evidenceTom A, Bell D, Ford JR, Debnam JM, Guo Y, Frank SJ, Esmaeli B. Malignant Mixed Tumor (Carcinoma Ex Pleomorphic Adenoma) of the Lacrimal Gland. Ophthalmic plastic and reconstructive surgery. 2020 Sep/Oct:36(5):497-502. doi: 10.1097/IOP.0000000000001625. Epub [PubMed PMID: 32282452]
Shields JA, Shields CL, Freire JE, Brady LW, Komarnicky L. Plaque radiotherapy for selected orbital malignancies: preliminary observations: the 2002 Montgomery Lecture, part 2. Ophthalmic plastic and reconstructive surgery. 2003 Mar:19(2):91-5 [PubMed PMID: 12644752]
Batra J, Ali MJ, Mody K, Naik MN, Vemuganti GK. Lacrimal gland amyloidosis: a clinicopathological correlation of a rare disorder and review of literature. Ocular immunology and inflammation. 2014 Aug:22(4):300-5. doi: 10.3109/09273948.2013.850100. Epub 2013 Nov 8 [PubMed PMID: 24205967]
Level 3 (low-level) evidenceSwerdlow SH,Campo E,Pileri SA,Harris NL,Stein H,Siebert R,Advani R,Ghielmini M,Salles GA,Zelenetz AD,Jaffe ES, The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016 May 19; [PubMed PMID: 26980727]
Rootman J, White VA. Changes in the 7th edition of the AJCC TNM classification and recommendations for pathologic analysis of lacrimal gland tumors. Archives of pathology & laboratory medicine. 2009 Aug:133(8):1268-71 [PubMed PMID: 19653723]
Coupland SE,White VA,Rootman J,Damato B,Finger PT, A TNM-based clinical staging system of ocular adnexal lymphomas. Archives of pathology [PubMed PMID: 19653722]
Level 2 (mid-level) evidenceAhmad SM,Esmaeli B,Williams M,Nguyen J,Fay A,Woog J,Selvadurai D,Rootman J,Weis E,Selva D,McNab A,DeAngelis D,Calle A,Lopez A, American Joint Committee on Cancer classification predicts outcome of patients with lacrimal gland adenoid cystic carcinoma. Ophthalmology. 2009 Jun; [PubMed PMID: 19395039]
Level 2 (mid-level) evidenceLee DA,Campbell RJ,Waller RR,Ilstrup DM, A clinicopathologic study of primary adenoid cystic carcinoma of the lacrimal gland. Ophthalmology. 1985 Jan; [PubMed PMID: 2983279]
Weis E,Rootman J,Joly TJ,Berean KW,Al-Katan HM,Pasternak S,Bonavolontà G,Strianese D,Saeed P,Feldman KA,Vangveeravong S,Lapointe JS,White VA, Epithelial lacrimal gland tumors: pathologic classification and current understanding. Archives of ophthalmology (Chicago, Ill. : 1960). 2009 Aug; [PubMed PMID: 19667339]
Level 2 (mid-level) evidenceGamel JW,Font RL, Adenoid cystic carcinoma of the lacrimal gland: the clinical significance of a basaloid histologic pattern. Human pathology. 1982 Mar; [PubMed PMID: 6281163]