Introduction
Myopia is characterized by the inability to see distant objects. Myopia results when parallel rays are focused in front of the retina with accommodation relaxed (see Image. Myopia). The global burden of myopia is rapidly increasing. In 2010, approximately 27% of the global population, or around 1.45 billion people, were affected.[1] By 2030, half of the world population is expected to be affected by myopia.[2] Myopia can be broadly classified as pathologic or spontaneous-onset childhood myopia.[3] Pathologic myopia results from a rapid increase in axial length, with a usual absolute spectacle power of greater than 6 diopters (D).[4] Rapidly progressive myopia leads to numerous degenerative changes in the retina, choroid, and sclera and therefore is termed pathologic myopia. Conversely, school-age myopia is the most common type, has a slow course, and usually stabilizes by age 20 years.[3]
Childhood myopia has emerged as one of the most significant global public health challenges of the 21st century, with rapidly increasing prevalence across diverse geographic regions and populations. Once considered a refractive condition predominantly affecting East Asian countries, myopia is now recognized as a worldwide epidemic affecting children at progressively younger ages. Results from epidemiological projections suggested that nearly half of the global population may become myopic by 2050, with a substantial proportion developing high myopia and its associated sight-threatening complications. This increasing prevalence has transformed myopia from a simple refractive error correctable with spectacles into a lifelong ocular disorder with important structural, functional, socioeconomic, and quality-of-life implications. The growing burden of childhood myopia has stimulated extensive research into the biological mechanisms governing ocular growth, environmental determinants of refractive development, and strategies for early intervention and prevention.[5]
The process of ocular development during childhood is highly dynamic and involves coordinated growth of multiple ocular structures, including the cornea, crystalline lens, anterior chamber, vitreous cavity, choroid, sclera, and retina. At birth, the human eye is relatively hyperopic because the optical power of the refractive components exceeds the axial length of the globe. During infancy and early childhood, a tightly regulated developmental process known as emmetropization gradually aligns refractive power with axial elongation, allowing the eye to achieve near-emmetropic status. This remarkable biological phenomenon relies on complex interactions between genetic programming, retinal signaling pathways, visual feedback mechanisms, and biomechanical remodeling of ocular tissues. Disruption of these finely balanced processes may result in excessive axial elongation and the subsequent development of myopia.[6]
Recent advances in developmental ophthalmology have fundamentally altered our current understanding of the pathogenesis of myopia. Rather than being viewed solely as a refractive mismatch between ocular power and axial length, myopia is increasingly recognized as a disorder of ocular growth regulation. Results from experimental studies have demonstrated that the retina actively participates in controlling eye growth through biochemical signaling cascades that influence choroidal thickness, scleral extracellular matrix remodeling, and axial elongation. Visual stimuli received by the retina are processed through local retinal mechanisms that can modulate globe growth independently of central neural pathways. These findings have established that myopia is a biologically regulated process rather than merely a hereditary refractive condition.[7]
The prevalence of childhood myopia exhibits striking geographic variation, reflecting the interplay between genetic susceptibility and environmental influences. Urban populations consistently demonstrate higher rates of myopia compared with rural communities, which suggests that lifestyle-related factors contribute significantly to disease development. Increased educational demands, prolonged near-work activities, reduced outdoor exposure, digital device usage, and altered visual environments have all been implicated in accelerating myopic progression. Contemporary children spend substantially more time engaged in indoor academic activities than previous generations, often beginning intensive educational programs at an increasingly younger age. These societal changes have coincided with a dramatic rise in myopia prevalence, reinforcing the importance of environmental modulation in refractive development.[8]
The retina plays a central role in regulating ocular growth during childhood. Results from experimental animal models have demonstrated that retinal image quality directly influences axial elongation through local biochemical pathways. Hyperopic defocus stimulates eye growth, whereas myopic defocus inhibits elongation, supporting the concept of visually guided ocular development. Neurotransmitters such as dopamine, nitric oxide, retinoic acid, and various growth factors have been implicated in these regulatory mechanisms. Dopamine, in particular, has emerged as a critical mediator of retinal signaling and may partially explain the protective effect of outdoor exposure against myopia progression. Increased retinal dopamine release in response to bright light is believed to suppress excessive axial growth, thereby reducing the risk of myopia.[9]
The choroid has gained increasing attention as an active participant in refractive regulation rather than a passive vascular layer. Dynamic changes in choroidal thickness occur in response to visual stimuli and may represent an early biomarker of ocular growth modulation. Choroidal thickening is generally associated with slowed axial elongation, whereas thinning often precedes myopic progression. These findings suggest that the choroid functions as a rapid-response tissue capable of translating retinal signals into structural changes that influence scleral remodeling and ocular growth. Advances in optical coherence tomography have enabled detailed evaluation of choroidal architecture, facilitating a deeper understanding of its role in childhood refractive development.[10]
The sclera serves as the principal structural framework governing globe size and shape. Progressive myopia is characterized by alterations in scleral extracellular matrix composition, collagen organization, biomechanical properties, and tissue remodeling. These changes reduce scleral rigidity and permit excessive axial elongation. Results from molecular studies have identified numerous pathways involved in scleral remodeling, including matrix metalloproteinases, transforming growth factor-β signaling, inflammatory mediators, and extracellular matrix regulators. Understanding these mechanisms has become increasingly important because they offer potential therapeutic targets to control myopia progression and prevent long-term structural complications.[11]
Genetic influences contribute substantially to susceptibility for childhood myopia, although inheritance patterns are complex and multifactorial. Findings from genome-wide association studies have identified numerous loci associated with refractive error, ocular growth regulation, extracellular matrix biology, and retinal signaling pathways. However, genetic predisposition alone cannot explain the rapid increase in myopia prevalence observed over recent decades. Instead, contemporary evidence supports a gene-environment interaction model in which inherited susceptibility interacts with modern visual behaviors and environmental exposures to determine individual risk. Children who have parents with myopia exhibit a greater likelihood of developing myopia, particularly when exposed to intensive educational environments and limited outdoor activities. Please see StatPearls' companion reference, "Myopia," for further information.
The consequences of childhood myopia extend far beyond refractive correction. Early-onset myopia is associated with longer axial growth and a higher risk of developing high myopia in adulthood. Excessive axial elongation predisposes individuals to potentially blinding complications, including retinal detachment, myopic maculopathy, glaucoma, choroidal neovascularization, posterior staphyloma, and cataract. Consequently, childhood myopia is increasingly viewed as a chronic progressive ocular disease requiring active management rather than simple optical correction. The recognition of these long-term risks has driven the development of evidence-based myopia control strategies to slow axial elongation during critical periods of ocular development.[11]
In recent years, remarkable advances have been made in understanding the biological basis of childhood myopia and ocular growth. Innovations in imaging technologies, molecular biology, genetics, artificial intelligence, and biometric analysis have provided unprecedented insights into the mechanisms regulating refractive development. Simultaneously, emerging therapeutic interventions such as low-dose atropine, peripheral defocus contact lenses, orthokeratology, spectacle lens designs, and lifestyle modifications have demonstrated promising efficacy in slowing the progression of myopia. These developments have transformed the field from passive refractive correction toward proactive disease prevention and growth modulation. As childhood myopia continues to increase worldwide, a comprehensive understanding of ocular development and refractive regulation remains essential for developing effective strategies to preserve visual health across the lifespan. Please see StatPearls' companion reference, "Myopia," for further information.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
In myopia, the image forms in front of the retinal photoreceptors. Based on the pathogenesis, myopia can be classified as follows:
- Axial myopia: Axial myopia results from a rapid increase in axial length. Axial length increases by 0.35 mm for every diopter increase in myopia.[12]
- Curvature myopia: Curvature myopia results from increased corneal curvature. Consequently, the image is focused in front of the retina. Each 1-mm change in the radius of curvature of the cornea causes a myopic shift by 6 diopters.[13]
- Lenticular myopia: Lenticular myopia results from an increase in the refractive index of the crystalline lens. Please see StatPearls' companion reference, "Hyperopia," for further information.
- Positional myopia and other conditions: Myopia may result from anterior shifting of the crystalline lens.[14] Sudden-onset myopia may result from anterior displacement of the lens-iris diaphragm in various conditions, including choroidal effusion and anterior rotation of the ciliary body induced by drugs such as topiramate.[14]
Premyopia is a nonrefractive state in children aged 5 to 7 years with hyperopia less than +0.75 diopter sphere and myopia greater than −0.5 diopter sphere, which helps predict the early development of myopia.[15] Childhood myopia is a complex multifactorial disorder resulting from the interaction among genetic susceptibility, environmental exposures, behavioral factors, visual experiences, and biological mechanisms that regulate ocular growth (see Tabe 1). Contemporary evidence supports that no single etiologic factor is sufficient to induce myopia; rather, disease development occurs through cumulative influences acting on retinal signaling pathways, choroidal modulation, scleral remodeling, and axial elongation. The rapid global increase in myopia prevalence over recent decades strongly indicates that environmental and lifestyle factors have become increasingly important contributors to disease expression in genetically predisposed individuals. Please see StatPearls' companion reference, "Myopia," for further information.
Genetic Predisposition
Genetic susceptibility remains one of the strongest risk factors for childhood myopia. Children with 1 parent with myopia have a significantly increased risk of developing myopia, whereas children with 2 parents with myopia demonstrate an even greater likelihood of earlier onset and faster progression. Results from genome-wide association studies identified hundreds of loci associated with refractive error, axial length regulation, extracellular matrix metabolism, retinal neurotransmission, and scleral biomechanics. Genes involved in collagen synthesis, transforming growth factor signaling, retinal dopamine pathways, and photoreceptor function have all been implicated in myopia susceptibility. However, genetic predisposition alone does not explain the dramatic rise in myopia prevalence observed within a single generation, emphasizing the critical role of environmental influences.[10]
Educational Pressure and Academic Exposure
Educational intensity has emerged as a major environmental determinant of childhood myopia. Children exposed to prolonged academic activities, extensive reading, early educational programs, and high-performance learning environments consistently exhibit higher rates of myopia. Results from several large population-based studies demonstrated a direct relationship between years of education and the progression of refractive error. Educational exposure may contribute through sustained accommodative demand, reduced outdoor activity, increased near work, and alterations in visual behavior. The association remains significant even after adjustment for parental myopia and socioeconomic status, highlighting education as an independent risk factor.[11]
Near-Work Activities
Prolonged near work is strongly associated with the development and progression of myopia. Activities such as reading, writing, tablet use, smartphone viewing, and computer-based learning require sustained accommodation and convergence. Excessive near work may induce hyperopic retinal defocus, accommodative lag, peripheral image blur, and retinal signaling changes that promote axial elongation. Children spending prolonged periods performing near tasks at close viewing distances may experience greater cumulative retinal stress and ocular growth stimulation. Importantly, continuous near work without regular visual breaks appears more strongly associated with myopia progression than total near-work duration alone.[16]
Digital Device Exposure
The widespread adoption of smartphones, tablets, and digital learning platforms has introduced new visual environments during critical periods of ocular development. Digital screens are often viewed at shorter working distances than printed materials and may encourage prolonged uninterrupted visual engagement. Excessive screen exposure has been linked to increased accommodative demand, reduced blink rate, ocular fatigue, and decreased outdoor activity. Although direct causality remains under investigation, digital device use is increasingly recognized as a potential contributor to modern myopia epidemics.[17]
Reduced Outdoor Exposure
Among all modifiable environmental factors, reduced time spent outdoors is one of the most consistently identified risk factors for childhood myopia. Results from numerous longitudinal studies demonstrated that increased outdoor activity lowers the risk of myopia onset. Bright outdoor illumination stimulates retinal dopamine release, which is believed to inhibit excessive axial elongation. Outdoor environments additionally provide greater viewing distances, richer spatial stimuli, and reduced accommodative demand compared with indoor settings. Protective effects appear independent of physical activity itself and are primarily attributed to environmental light exposure.[18]
Urbanization and Lifestyle Changes
Urban populations consistently exhibit higher myopia prevalence than rural communities. Urbanization influences visual behavior through increased educational competition, reduced access to outdoor spaces, greater screen use, and prolonged indoor lifestyles. High population density, limited natural environments, and modern architectural designs may further alter visual experiences during childhood. Socioeconomic development has therefore become closely associated with increasing myopia prevalence across many regions of the world.[19]
Circadian Rhythm and Sleep Disturbances
Emerging evidence suggests that circadian dysregulation may contribute to abnormal ocular growth. Sleep duration, sleep quality, and light exposure patterns influence retinal neurotransmitter activity and ocular physiology. Irregular sleep schedules, excessive nighttime screen exposure, and reduced daytime light stimulation may disrupt normal retinal signaling pathways involved in refractive development. Although the exact mechanisms remain under investigation, circadian influences are increasingly recognized as potential contributors to myopia progression.[20]
Nutritional and Metabolic Factors
Nutrition may indirectly influence ocular development by affecting growth regulation, inflammation, oxidative stress, and extracellular matrix metabolism. Deficiencies in vitamin D, antioxidant nutrients, and essential micronutrients have been investigated as potential risk modifiers, although evidence remains inconsistent. Metabolic disorders associated with obesity, insulin resistance, and altered growth factor signaling have also been explored as possible contributors to excessive axial elongation.[21]
Prenatal and Early-Life Influences
Prenatal and perinatal factors may influence refractive development before the onset of visual maturation. Low birth weight, prematurity, maternal smoking, gestational complications, and abnormal fetal growth patterns have all been associated with altered ocular development. Early childhood visual experiences, environmental stimulation, and developmental exposures may further influence subsequent refractive trajectories. Please see StatPearls' companion reference, "Myopia," for further information.
Environmental Pollution and Emerging Risk Factors
Results from recent studies suggested associations among air pollution, reduced sunlight exposure, urban environmental stressors, and the development of myopia. Chronic exposure to particulate matter and environmental pollutants may influence inflammatory pathways and outdoor activity patterns. Although evidence remains preliminary, environmental health factors are increasingly being investigated as contributors to modern myopia epidemics.[22]
Table 1. Major Etiological Factors Associated with Childhood Myopia
|
Category |
Examples |
Proposed mechanism |
|
Genetic |
Parental myopia, susceptibility genes |
Predisposition to axial elongation |
|
Educational |
Intensive schooling, academic pressure |
Increased near work |
|
Behavioral |
Reading, smartphones, tablets |
Hyperopic defocus, accommodative stress |
|
Environmental |
Reduced outdoor activity |
Reduced dopamine-mediated growth inhibition |
|
Lifestyle |
Urbanization, indoor living |
Altered visual environment |
|
Biological |
Circadian disruption |
Abnormal retinal signaling |
|
Prenatal |
Prematurity, low birth weight |
Altered ocular development |
|
Metabolic |
Obesity, insulin resistance |
Growth-factor–mediated elongation |
Epidemiology
Myopia has become a public health concern. The rising incidence of myopia can be attributed to reduced outdoor activity, increased screen time, and prolonged near-work, especially during the COVID-19 pandemic.[23] The reported prevalence of myopia in Singapore among children aged 6 to 7 years is 20% to 30%.[24] In China, the prevalence of myopia in children aged 5 to 15 years ranges from 5.7% to 78.4%.[25]
Myopia is more prevalent in Asian children than in children in European countries, where the prevalence of myopia is lower (17.8%-23.5%).[26] In the US, the prevalence of myopia ranges from 4.6% to 28% in children aged 6 to 12 years.[27] In India, the range varies from 8.5% to 15% among urban children aged 5 to 15 years.[28]
Myopia has emerged as one of the most significant ocular public health challenges worldwide. Over the past few decades, the prevalence of childhood myopia has increased substantially across multiple geographic regions, prompting concerns regarding future burdens of visual impairment and myopia-associated ocular complications. The increasing prevalence has been attributed to a complex interaction between genetic susceptibility and environmental factors, including reduced outdoor exposure, increased educational pressures, prolonged near-work activities, and greater use of digital devices. The COVID-19 pandemic further accelerated these trends due to home confinement, virtual learning, and increased screen exposure among school-aged children.[21]
The prevalence of childhood myopia demonstrates considerable geographic and ethnic variation (see Table 2). East and Southeast Asian countries report the highest rates globally. In Singapore, myopia affects approximately 20% to 30% of children aged 6 to 7 years, with prevalence increasing progressively throughout adolescence. In mainland China, reported prevalence ranges from 5.7% in younger children to more than 78% among adolescents aged 15 years, reflecting both age-dependent progression and regional differences. Urban centers in China, Hong Kong, Taiwan, South Korea, and Japan consistently report some of the highest prevalence rates worldwide, with myopia affecting more than 80% of high-school graduates in certain populations.[11]
Conversely, European populations demonstrate comparatively lower rates of childhood myopia. Results from studies from Northern and Western Europe reported prevalence rates ranging from 17.8% to 23.5% among school-aged children. However, recent epidemiologic data suggest a gradual increase in prevalence even within traditionally low-risk populations, indicating that environmental influences may be overcoming historical geographic differences.[11] In the US, childhood myopia prevalence varies according to age, ethnicity, and study methodology. Reported prevalence ranges from 4.6% to 28% among children aged 6 to 12 years. The condition is more frequently observed in older children and adolescents than in preschool-aged populations. Ethnic disparities have also been documented, with higher prevalence among children of East Asian ancestry compared with Black, Hispanic, or White children.[11]
In India, childhood myopia prevalence ranges from 8.5% to 15% among children aged 5 to 15 years living in urban areas. Urban populations consistently demonstrate higher rates than rural populations, likely reflecting differences in educational intensity, outdoor activity patterns, and digital device use. Results from several Indian epidemiologic studies reported a rising trend in school-based myopia over the last 2 decades, paralleling global observations.[8] Age remains one of the strongest determinants of myopia prevalence. The condition is relatively uncommon before school age but increases steadily during primary and secondary school years, corresponding with periods of rapid ocular growth and increased academic demands. Peak incidence typically occurs between 7 and 15 years of age, with progression often continuing until late adolescence.[29]
Sex-related differences in childhood myopia have been inconsistently reported. Results from several population-based studies demonstrated slightly higher prevalence rates among girls, potentially related to earlier pubertal growth, increased educational engagement, or differences in outdoor activity patterns. However, results from other studies found minimal or no significant sex-related differences after adjusting for environmental and behavioral factors. Recent global estimates suggest that approximately 30% of the world population is currently myopic, with projections indicating that nearly 50% may be affected by 2050 if current trends continue. Childhood-onset myopia is of particular concern because earlier onset is associated with greater progression and a higher risk of developing high myopia in adulthood. High myopia substantially increases the lifetime risk of retinal detachment, myopic maculopathy, glaucoma, cataract, and irreversible visual impairment.[5] The global burden of childhood myopia is therefore expected to continue increasing, emphasizing the importance of early identification, preventive interventions, and public health strategies aimed at reducing modifiable environmental risk factors.
Table 2. Global Prevalence of Childhood Myopia by Geographic Region
|
Region or country |
Age group |
Reported prevalence (%) |
Key observations |
|
Singapore |
6–7 years |
20–30 |
Early onset is common; prevalence rises rapidly with age |
|
China |
5–15 years |
5.7–78.4 |
Marked age-related increase; among the highest worldwide |
|
South Korea |
School-aged children |
50–80+ |
High prevalence in urban populations |
|
Japan |
School-aged children |
40–70 |
Increasing prevalence over recent decades |
|
Europe |
School-aged children |
17.8–23.5 |
Lower prevalence than East Asia |
|
United States |
6–12 years |
4.6–28 |
Significant ethnic and geographic variation |
|
India |
5–15 years |
8.5–15 |
Higher prevalence in urban than rural populations |
|
Australia |
School-aged children |
10–20 |
Higher outdoor exposure is associated with lower prevalence |
|
Global estimate |
Children and adolescents |
Variable |
Increasing prevalence across all regions |
Pathophysiology
Myopia and Ocular Development
Refractive error results from a long, complex process of ocular development; hence, myopia cannot be attributed to a single trait. Many factors contribute to the development of childhood myopia, including the extent and effectiveness of emmetropization during the early years of life, environmental influences, genetic factors, and changes in axial length and lens power during adolescence (see Table 3).[30] Myopia develops at the same age as hyperopia correction. Early-onset myopia is usually associated with higher refractive errors and results in progressive thinning of the choroid, staphyloma, and pathologic retinal degeneration.[31]
Emmetropization
Emmetropization is a process in which the refractive components, including corneal curvature and lenticular curvature, balance with the eye's postnatal development, resulting in the nullification of refractive errors. At birth, the child is hyperopic, with an average refractive error of +2 to +3 diopters.[32] However, with age, the refractive error decreases and may reach emmetropia or myopia, which is more common in the population.[33] The axial length at birth is 16 to 18 mm, increasing to 23 mm by age 3 years. After age 3 years, the axial length growth rate decreases.[34] The rapid increase in axial length should cause a myopic shift; however, other changes in the lens and corneal curvature control this shift, preventing rapid progression.[35]
Sclera and Myopia
The sclera is the outermost coat of the eye and is composed chiefly of collagen types I and III.[36] Proteoglycans modulate collagen assembly. Decorin and biglycan are the most common sulfated proteoglycans present in the sclera.[37] Proteoglycan hydration is considered responsible for age-related changes in the sclera. The interaction between scleral fibroblast cells and the scleral matrix plays a vital role in controlling the distensibility of the sclera during eye growth.[38] During emmetropization, accurate regulation of scleral extracellular matrix growth and remodeling governs eye development.
Embryonic development of sclera: The sclera develops in the sixth week of prenatal life from the cells of the neural crest, or neuroectoderm, and mesoderm.[39] The sclera reaches its adult size by age 10 years. However, the extracellular matrix of the sclera continues to change.[40] In patients with myopia, the sclera is characterized by increased elasticity, which can be attributed to ultrastructural changes of the sclera. The fibroblasts are arranged in a lamellar pattern in patients with myopia and are associated with thinning of collagen bundles.[41] This increased scleral elasticity increases axial length, shifting the image anteriorly.
Emmetropization and scleral remodeling: Scleral extracellular matrix remodeling is regulated by several growth factors, including insulin-like growth factors 1 and 2.[42] Additionally, scleral extracellular matrix remodeling is controlled by locally generated growth factors from the retina and choroid.[43] Results from various experimental models suggest that visual signals in the form of retinal blur induce the production of γ-aminobutyric acid, dopamine, insulin, and glucagon, which in turn elicit a response in the retinal pigment epithelium and choroid, leading to the release of regulatory growth factors and ultimately to scleral extracellular matrix remodeling.[44]
Choroidal Modulation
The choroid is a highly vascular middle coat of the eyeball. The choroid provides nutrients and oxygen to the outer retinal layers and sclera. Results from various animal models have demonstrated the importance of the choroid in the development of myopia and emmetropization. The choroid regulates its thickness to adjust the retina to the focal plane of the eye, a term known as choroidal accommodation.[45]
The choroid also delivers growth-stimulating factors to the sclera, thereby regulating the scleral extracellular matrix and axial length.[46] Results from animal models suggested that increased production of choroidal all-trans-retinoic acid is associated with a reduction in scleral proteoglycan and an increase in axial length.[47] With the advent of noninvasive techniques such as enhanced-depth spectral-domain optical coherence tomography, choroidal imaging is now possible. In patients with high myopia, the choroid is usually associated with thinning on optical coherence tomography. A thinner choroid on optical coherence tomography suggests a poorer prognosis and is generally associated with thinner retinal layers.[48]
Lens Curvature Changes in Childhood
The lens at birth has a spherical contour and eventually flattens.[49] The flattening of the lens can be due to the equatorial expansion and central compaction forces generated by the growing eyeball.[50] As the eyeball grows, the thickness of the lens also decreases along with the increase in the diameter of the ciliary body, which tensions the zonules and causes lens thinning.[51] The thickness of the lens decreases from 4 mm at birth to 3.3 mm by adolescence.[52] This thinning changes the lens dioptric power from 34.4 diopters at birth to 23 diopters at age 3 years and 20 diopters at age 14 years, preventing the myopic shift.[53]
Factors Affecting Myopia Development and Progression
Family history: Results from various studies suggested that the risk of early-onset myopia development and progression is higher in children if either of the parents has myopia.[54][55]
Birth history: Low birth weight and premature birth associated with retinopathy of prematurity have been suggested to be associated with myopia development.[56] Sunlight exposure or birth during the summer of the perinatal period is also associated with the development of myopia in later life.[57]
Excessive near work: Excessive near work is associated with myopia progression resulting from accommodative lag. Accommodative lag is the difference between the accommodative stimulus, or demand, and the accommodative response.[58] The longer the accommodative lag is, the greater the myopia progression. Excessive near work in patients with myopia causes prolonged retinal defocus, which further stimulates axial length growth.[59]
Higher intelligence quotient: Myopia development may be associated with higher cognitive functions, better education, and a higher intelligence quotient.[60] Results from a population-based study by Mirshahi et al found that higher levels of professional education were associated with higher rates of myopic refractive error compared with participants with lower levels of education.[61] This association can be attributed to defocus signals in the peripheral and central retina with constant accommodative lags.[62]
Outdoor activities: Results from various studies found that outdoor activities reduce myopia progression. One hypothesis suggests that the wavelength of radiant sunlight is 550 nm, the same wavelength focused on a normal observer's retina.[63] Conversely, indoor lights have a longer wavelength and are focused behind the retina.[64] Results from an experimental study found that the spatial features of the indoor environment are similar to those of artificial spatial features created by diffuse filters that induce myopia in animals.[65] Another hypothesis states that sunlight inhibits the increase in axial length by promoting dopamine release.[66]
Increased screen time: Increased screen time can lead to the development of myopia and is attributed to increased time spent indoors.[67] Results from a study by Enthoven et al found that continuous smartphone use for 20 min was associated with a higher risk of developing myopia.[68]
Retinal Defocus Signaling and Peripheral Hyperopic Defocus
Recent evidence suggests that retinal image quality plays a central role in regulating ocular growth. During childhood, the retina continuously monitors the position of the focal plane relative to the photoreceptor layer. When images are focused behind the peripheral retina, a phenomenon known as peripheral hyperopic defocus occurs. Peripheral hyperopic defocus acts as a growth-promoting signal, stimulating axial elongation of the eye in an attempt to move the retina toward the focal plane. Results from experimental studies demonstrated that peripheral retinal signals may exert a stronger influence on ocular growth than central foveal signals, providing the biological rationale for modern myopia-control strategies such as orthokeratology and peripheral-defocus spectacle lenses.[5]
Dopaminergic Regulation of Eye Growth
Dopamine has emerged as one of the most important neurotransmitters involved in ocular growth regulation. Retinal dopamine release increases in response to bright outdoor light exposure and functions as an inhibitory signal against excessive axial elongation. Reduced dopamine activity has been observed in experimental models of form-deprivation myopia and lens-induced myopia. This dopamine-related mechanism may partly explain the protective effect of outdoor activities against the progression of childhood myopia. The interaction between dopamine signaling and circadian rhythms has also been proposed as an important regulator of ocular development.[6]
Circadian Rhythm and Ocular Growth
The eye demonstrates circadian fluctuations in axial length, choroidal thickness, and intraocular pressure. Normal ocular development appears to depend on synchronized circadian regulation of these parameters. Disruption of sleep patterns, excessive nighttime screen exposure, and altered light-dark cycles may interfere with these physiological rhythms, leading to dysregulated ocular growth. Results from recent studies suggest that prolonged evening exposure to artificial light may suppress melatonin secretion and indirectly affect retinal pathways involved in emmetropization.[20]
Retinal Pigment Epithelium as a Signaling Interface
The retinal pigment epithelium (RPE) serves as a critical intermediary between the neural retina and sclera. Visual defocus signals generated within the retina are believed to be transmitted through the RPE via alterations in ion transport, growth factor secretion, and extracellular signaling molecules. The RPE modulates the release of transforming growth factor-β, vascular endothelial growth factor, fibroblast growth factors, and retinoic acid derivatives that ultimately influence scleral remodeling and axial elongation. Consequently, the RPE functions as a key relay station in the retina–choroid–sclera signaling cascade.[5]
Role of Hypoxia and Scleral Metabolism
Emerging evidence indicates that localized scleral hypoxia may contribute to myopia progression. During axial elongation, alterations in choroidal perfusion and scleral oxygenation may activate hypoxia-inducible factor-1α pathways. Activation of these pathways promotes extracellular matrix degradation and reduces collagen synthesis, thereby weakening the scleral wall and facilitating further elongation. Results from experimental studies demonstrated upregulation of hypoxia-related genes in highly myopic eyes, suggesting that metabolic remodeling may be an important component of disease progression.[7]
Matrix Metalloproteinases and Extracellular Matrix Degradation
Scleral remodeling in myopia is associated with increased activity of matrix metalloproteinases, particularly matrix metalloproteinase 2 and matrix metalloproteinase 9. These enzymes degrade collagen fibrils and extracellular matrix components, reducing scleral rigidity. Simultaneously, tissue inhibitors of metalloproteinases are downregulated, shifting the balance toward matrix degradation. This biochemical shift results in progressive scleral thinning and biomechanical weakening, facilitating continued axial elongation.[69]
Biomechanical Failure of the Posterior Pole
Highly myopic eyes exhibit progressive biomechanical instability of the posterior sclera. During axial elongation, mechanical stress becomes concentrated at the posterior pole, resulting in localized stretching, scleral thinning, and deformation. This biomechanical instability contributes to the development of posterior staphyloma, lacquer cracks, chorioretinal atrophy, and myopic maculopathy. Results from modern imaging studies suggested that biomechanical failure of the posterior ocular wall may be a critical determinant of pathologic myopia rather than axial length alone.[70]
Genetic and Epigenetic Regulation
Results from genome-wide association studies identified more than 500 genetic loci associated with refractive development and susceptibility to myopia. Many of these genes are involved in extracellular matrix regulation, neuronal signaling, retinal development, and ocular growth pathways. Additionally, environmental exposures during childhood may induce epigenetic modifications, including DNA methylation and histone alterations, which influence the expression of growth-regulating genes. These findings support the concept that childhood myopia results from complex interactions between inherited susceptibility and environmental triggers.[71]
Neurovascular Changes During Myopia Progression
Progressive axial elongation is associated with alterations in retinal and choroidal microcirculation. Results from optical coherence tomography angiography studies demonstrated reduced choroidal vascularity and decreased retinal perfusion density in highly myopic eyes. These vascular changes may contribute to retinal hypoxia, choroidal thinning, and subsequent degenerative complications. Neurovascular remodeling is increasingly recognized as a component of pathologic myopia rather than merely a consequence of globe enlargement.[72]
Table 3. Pathophysiology of Myopia
Abbreviations: FGF, fibroblast growth factor; HIF-1α, hypoxia-inducible factor 1α; MMP, matrix metalloproteinase; OCTA, optical coherence tomography angiography; RPE, retinal pigment epithelium; TGF-β, transforming growth factor β; TIMP, tissue inhibitor of metalloproteinase; VEGF, vascular endothelial growth factor.
|
Pathophysiologic mechanism |
Primary mediator |
Effect on ocular growth |
|
Peripheral hyperopic defocus |
Retinal blur signaling |
Stimulates axial elongation |
|
Dopamine deficiency |
Reduced retinal dopamine |
Promotes myopia progression |
|
Circadian disruption |
Melatonin imbalance |
Dysregulated emmetropization |
|
RPE signaling abnormalities |
TGF-β, FGF, retinoic acid |
Scleral remodeling |
|
Hypoxia pathways |
HIF-1α activation |
Scleral thinning |
|
Matrix degradation |
MMP-2, MMP-9 |
Reduced scleral rigidity |
|
Genetic susceptibility |
Multiple myopia loci |
Increased risk of onset |
|
Neurovascular remodeling |
Choroidal vascular loss |
Progressive pathological myopia |
Histopathology
The hallmark histopathologic feature of myopia is progressive axial elongation of the globe, accompanied by remodeling of the sclera, choroid, and retina. Histologic examination demonstrates thinning of the posterior sclera, attributable to reduced collagen fibril diameter, decreased collagen fiber density, and alterations in extracellular matrix composition. The scleral fibroblasts exhibit reduced synthetic activity, leading to diminished production of collagen types I and III and increased susceptibility to biomechanical stretching. These changes are particularly pronounced in eyes with high or pathologic myopia.[5] Table 5 summarizes these features.
The choroid undergoes progressive thinning with loss of vascular and stromal components. Results from histopathologic studies demonstrated attenuation of the choriocapillaris, decreased vascular density, and reduction in melanocyte and connective tissue content. Choroidal thinning contributes to impaired metabolic support of the outer retina and is strongly associated with myopic maculopathy and posterior staphyloma formation.[6] Retinal changes are generally minimal in early childhood myopia but become increasingly evident with greater degrees of axial elongation. Histologic examination may reveal thinning of the neurosensory retina, particularly involving the outer nuclear layer, photoreceptor layer, and retinal pigment epithelium. In pathologic myopia, focal areas of retinal pigment epithelium atrophy, photoreceptor degeneration, and chorioretinal thinning may develop, especially within the posterior pole.[7]
Bruch membrane demonstrates characteristic alterations in highly myopic eyes. Results from histopathologic studies identified thinning, fragmentation, and focal defects of Bruch membrane, which may contribute to the development of lacquer cracks and myopic choroidal neovascularization. These defects are believed to result from chronic mechanical stretching associated with axial elongation. The optic nerve head also exhibits structural changes secondary to globe enlargement. Histologic findings include elongation and thinning of the peripapillary scleral flange, expansion of the parapapillary region, and remodeling of the lamina cribrosa. These alterations contribute to optic disc tilting, peripapillary atrophy, and increased susceptibility to glaucomatous optic neuropathy in individuals with high myopia.[73]
In advanced pathologic myopia, posterior staphyloma represents the most severe histopathologic manifestation. Microscopic examination reveals marked scleral thinning, disorganization of collagen bundles, profound choroidal atrophy, and secondary degenerative changes involving the retina and retinal pigment epithelium. These structural alterations underlie many of the vision-threatening complications associated with high myopia.[74]
Table 5. Characteristic Histopathologic Findings in Myopia
|
Ocular structure |
Histopathologic findings |
Clinical significance |
|
Sclera |
Thinning, reduced collagen fibril diameter, and extracellular matrix remodeling |
Axial elongation, biomechanical weakening |
|
Scleral fibroblasts |
Reduced collagen synthesis, altered cellular activity |
Progressive globe enlargement |
|
Choroid |
Vascular attenuation, stromal thinning, reduced vascular density |
Choroidal thinning on OCT |
|
Retina |
Outer retinal thinning, photoreceptor loss in advanced cases |
Reduced visual function |
|
Retinal pigment epithelium |
Focal atrophy and degeneration |
Myopic maculopathy |
|
Bruch membrane |
Thinning, fragmentation, and focal defects |
Lacquer cracks, CNV formation |
|
Optic nerve head |
Lamina cribrosa remodeling, peripapillary changes |
Disc tilt, glaucoma susceptibility |
|
Posterior pole |
Scleral ectasia and staphyloma formation |
Pathological myopia |
Abbreviations: CNV, choroidal neovascularization; OCT, optical coherence tomography.
Most Common Histopathologic Findings
The most consistently reported microscopic findings in myopia are:
- Posterior scleral thinning with extracellular matrix remodeling
- Reduced collagen fibril diameter and density
- Choroidal thinning with vascular attenuation
- Retinal pigment epithelium and outer retinal thinning in advanced disease
- Progressive posterior pole stretching leading to staphyloma formation in pathological myopia
These histopathologic alterations collectively reflect the underlying process of excessive ocular growth and biomechanical remodeling that characterizes childhood-onset and progressive myopia.[75]
Toxicokinetics
Childhood myopia is not a toxicological disorder in the classic sense; however, several environmental exposures, pharmacologic agents, and biochemical signaling pathways influence ocular growth and refractive development (see Table 6). The concept of toxicokinetics in myopia primarily concerns the absorption, distribution, metabolism, and biological effects of endogenous and exogenous substances that modulate retinal, choroidal, and scleral remodeling during emmetropization.[5]
Visual stimuli serve as the principal biological input regulating ocular growth. Retinal photoreceptors detect optical defocus and initiate signaling cascades involving neurotransmitters, growth factors, and metabolic mediators. These signals are transmitted through the retinal pigment epithelium and choroid to the sclera, where extracellular matrix remodeling determines axial elongation. Prolonged exposure to adverse visual environments, including sustained near work, reduced outdoor illumination, and excessive screen use, alters these biochemical pathways and may promote myopia progression.[76]
Dopamine is one of the most extensively studied neurochemical regulators of ocular growth. Increased retinal dopamine release occurs in response to bright outdoor light exposure and functions as an inhibitory signal against excessive axial elongation. Conversely, reduced dopamine activity has been associated with experimental myopia development. Dopamine metabolites are rapidly processed within retinal neurons, and their biological effects influence downstream pathways that regulate scleral remodeling and choroidal thickness.[77]
Retinoic acid, a metabolite of vitamin A, has emerged as an important mediator of ocular growth regulation. Results from experimental studies demonstrated increased concentrations of all-trans-retinoic acid within the choroid during periods of accelerated axial elongation. Retinoic acid influences gene transcription, extracellular matrix turnover, and scleral fibroblast activity, thereby contributing to changes in ocular dimensions during refractive development. Nitric oxide has also been implicated in myopia pathogenesis. Nitric oxide is synthesized locally within retinal and choroidal tissues and modulates vascular tone, neurotransmission, and cellular proliferation. Alterations in nitric oxide signaling have been associated with changes in choroidal thickness and scleral remodeling in animal models of myopia.[7]
Environmental light exposure influences ocular development through circadian and neurochemical pathways. Natural sunlight stimulates retinal dopamine release and supports normal emmetropization, whereas prolonged exposure to artificial indoor lighting and digital displays may alter retinal signaling and circadian regulation. Although direct toxic effects have not been established, cumulative exposure to unfavorable visual environments may contribute to abnormal ocular growth. Pharmacologic agents used for myopia control demonstrate specific ocular pharmacokinetic properties. Low-dose atropine, currently one of the most effective treatments for childhood myopia progression, penetrates ocular tissues following topical administration and acts on muscarinic receptors within the retina, choroid, and sclera. While its precise mechanism remains incompletely understood, atropine appears to modulate retinal neurotransmitter release and inhibit scleral remodeling pathways that promote axial elongation. Please see StatPearls' companion reference, "Lenticonus," for further information.
Oxidative stress has also been proposed to contribute to progressive myopia. Increased production of reactive oxygen species may influence retinal metabolism, extracellular matrix degradation, and vascular homeostasis. Antioxidant defense mechanisms within ocular tissues help maintain normal cellular function, although their precise role in childhood myopia remains under investigation. Overall, the biological pathways influencing childhood myopia involve a complex interplay among retinal neurotransmitters, growth factors, metabolic mediators, circadian regulators, and environmental exposures that collectively determine ocular growth and refractive development.[29]
Table 6. Biochemical Mediators Influencing Childhood Myopia Development
|
Mediator or factor |
Primary source |
Proposed effect on ocular growth |
|
Dopamine |
Retina |
Inhibits axial elongation; protective against myopia |
|
Retinoic acid |
Choroid and RPE |
Promotes scleral remodeling and ocular growth |
|
Nitric oxide |
Retina and choroid |
Modulates choroidal thickness and vascular regulation |
|
Insulin-like growth factors (IGF-1, IGF-2) |
Retina, choroid, sclera |
Regulate extracellular matrix remodeling |
|
Transforming growth factor-β (TGF-β) |
RPE and sclera |
Influences collagen synthesis and scleral biomechanics |
|
Matrix metalloproteinases (MMPs) |
Scleral fibroblasts |
Promote extracellular matrix degradation |
|
Melatonin |
Retina and pineal gland |
Regulates circadian ocular growth rhythms |
|
Reactive oxygen species |
Ocular tissues |
May contribute to tissue remodeling and degeneration |
|
Atropine |
Topically administered medication |
Slows axial elongation and myopia progression |
Abbreviations: IGF-1, insulin-like growth factor 1; IGF-2, insulin-like growth factor 2; RPE, retinal pigment epithelium; TGF-β, transforming growth factor β.
Additional Contemporary Concepts
Gut-retina axis and myopia: Emerging studies suggest that systemic metabolic and inflammatory mediators derived from the gut microbiome may influence retinal neurotransmitter pathways involved in ocular growth.
Hypoxia-inducible factor 1α signaling: Increasing evidence links scleral hypoxia to extracellular matrix degradation and progressive axial elongation.
Mitochondrial metabolism: Altered retinal energy metabolism may contribute to abnormal visual signal processing during emmetropization.
Environmental exposome: The cumulative lifetime exposure to artificial lighting, digital devices, urbanization, and educational pressures is increasingly recognized as an important determinant of childhood myopia risk.[20]
History and Physical
A comprehensive eye examination should be performed, and myopic posterior segment changes should be excluded (see Table 8).[78] Children with myopia typically present with progressive blurring of distance vision while near vision remains relatively preserved. School-aged children commonly report difficulty seeing the classroom board, television screens, road signs, or distant objects during outdoor activities. Parents may notice behaviors such as squinting, sitting closer to the television, holding books very close to the face, frequent eye rubbing, reduced interest in distance-dependent activities, or declining academic performance. Younger children may not verbalize visual difficulties and may instead demonstrate inattentiveness, poor hand-to-eye coordination, or avoidance of visually demanding tasks. Please see StatPearls' companion reference, "Microspherophakia," for further information.
Associated symptoms may include asthenopia, frontal headaches, brow ache, ocular fatigue, intermittent diplopia during prolonged near work, and difficulty transitioning focus between near and distant targets. Symptoms often worsen after extended reading, use of digital devices, or other near-vision activities. A history of rapid refractive progression, especially during the school years, should raise concern for developing high myopia and warrants closer monitoring.[5]
A detailed history should evaluate age at onset, rate of progression, family history of myopia, educational demands, duration of near work, screen exposure, reading distance, outdoor activity levels, sleep habits, and previous spectacle or contact lens use (see Table 7). Particular attention should be paid to risk factors such as parental myopia, prematurity, low birth weight, retinopathy of prematurity, connective tissue disorders, and syndromic conditions associated with high myopia. Symptoms such as photopsia, floaters, metamorphopsia, visual field defects, or sudden visual loss may indicate complications of pathological myopia and require prompt retinal evaluation.[9]
Visual acuity assessment typically shows reduced uncorrected distance vision, with improvement after refractive correction. Cycloplegic refraction remains the gold standard for diagnosing childhood myopia and determining the true refractive error by eliminating accommodative influences. Manifest refraction alone may underestimate hyperopia or overestimate myopia in children with active accommodation. External examination is usually normal in uncomplicated myopia. Ocular alignment, binocular vision status, accommodative function, convergence ability, and stereopsis should be assessed because binocular vision anomalies may coexist with refractive errors. Children with high myopia may demonstrate larger-appearing globes, deeper anterior chambers, or early vitreous changes.[10]
Anterior segment examination is generally unremarkable in simple myopia. However, slit-lamp evaluation should exclude associated conditions such as lens abnormalities, ectopia lentis, developmental cataracts, or connective tissue disorders that may contribute to excessive axial elongation. Intraocular pressure measurement should be performed as part of a comprehensive ophthalmic examination, particularly in individuals with severe myopia who may have an increased lifetime risk of glaucoma. Please see StatPearls' companion reference, "Lenticonus," for further information.
Dilated fundus examination is essential to evaluate the posterior segment. Mild to moderate myopia may demonstrate a normal fundus appearance or subtle tessellation due to increased visibility of the underlying choroidal vasculature. As axial length increases, characteristic findings may include optic disc tilting, temporal peripapillary atrophy, posterior vitreous degeneration, chorioretinal thinning, and diffuse fundus tessellation. Highly myopic eyes may exhibit posterior staphyloma, lacquer cracks, myopic macular degeneration, choroidal neovascularization, or peripheral retinal degeneration, predisposing to retinal tears and detachment. Biometric evaluation may demonstrate increased axial length, which represents the principal structural correlate of myopia progression. Optical biometry and ocular imaging are increasingly used to monitor axial elongation and assess the risk of future pathologic changes. Optical coherence tomography (OCT) may reveal choroidal thinning, retinal thinning, and early myopic macular alterations in progressive or high myopia.[7]
Table 7. Common History Findings
|
History feature |
Clinical significance |
|
Blurred distance vision |
Most common presenting symptom |
|
Difficulty seeing the classroom board |
Typical school-aged concern |
|
Squinting or narrowing eyelids |
Compensatory improvement of image clarity |
|
Holding objects very close |
Suggestive of uncorrected myopia |
|
Headache and asthenopia |
Associated with prolonged visual effort |
|
Family history of myopia |
Strong risk factor |
|
Excessive near work |
Associated with progression |
|
Reduced outdoor activity |
Established environmental risk factor |
|
Rapid refractive progression |
Increased risk of high myopia |
Table 8. Common Physical Examination Findings
|
Examination component |
Typical findings |
|
Visual acuity |
Reduced uncorrected distance vision |
|
Cycloplegic refraction |
Negative spherical equivalent |
|
Ocular alignment |
Usually normal; binocular anomalies may coexist |
|
Anterior segment |
Typically normal |
|
Axial length measurement |
Increased compared with age-matched controls |
|
Fundus examination |
Tessellated fundus, tilted disc, peripapillary atrophy |
|
OCT imaging |
Choroidal thinning in progressive or high myopia |
|
Peripheral retina |
Lattice degeneration or retinal thinning in high myopia |
Most Common Findings
The most common clinical findings in childhood myopia are blurred distance vision, reduced uncorrected visual acuity, improvement with minus lens correction, increased axial length, and a normal anterior segment examination. In progressive or high myopia, fundus tessellation, optic disc tilt, peripapillary atrophy, and choroidal thinning may be observed.[5]
Evaluation
Refraction under cycloplegia should be performed up to age 20 years to prevent overestimation of myopia.[79] The commonly used cycloplegic agents are atropine 1%, homatropine 2%, cyclopentolate 1%, tropicamide 1%, tropicamide 0.8%, and phenylephrine 5%. Of these, atropine 1% is the strongest cycloplegic agent, and its effect lasts for 14 days.[80] The onset of action of homatropine starts after one hour and lasts for 1 to 3 days.[81] Cyclopentolate is the preferred cycloplegic for evaluating refractive error in children aged 5 to 13 years. Tropicamide chiefly acts as a mydriatic, but tropicamide is an effective agent for evaluating children with myopia older than 13 years.[82][83]
Atropine ointment must be instilled cautiously to prevent systemic complications such as facial flushing, fever, and tachycardia. The guidelines for spectacle prescription in children with myopia are summarized in Table 9 (American Academy of Ophthalmology Preferred Practice Pattern on Pediatric Eye Evaluations). Please see StatPearls' companion reference, "Tropicamide," for further information.
Table 9. Diagnostic Evaluation of Childhood Myopia
| Age younger than 1 year | Age 1 to 2 years | Age 2 to 3 years | Age 3 to 4 years | |
|
Similar refractive error (myopia) in both eyes (isometropia) |
≥ 5 DS | ≥ 4 DS | ≥ 3 DS | ≥ 2.5 DS |
| Myopic anisometropia (without squint) | ≥ 4 DS | ≥ 3 DS | ≥ 3 DS | ≥ 2.5 DS |
Abbreviation: DS, diopter sphere.
A complete examination of the anterior segment and fundus evaluation should be performed after refraction. Fundus evaluation in patients with pathologic myopia can reveal degenerative changes, lattice degeneration, peripheral retinal holes, cobblestone degeneration, lacquer cracks, macular hole, and staphyloma.[84] Optical biometry helps with regular monitoring of myopia progression. Optical biometry also helps monitor axial length and provides additional data, including corneal curvature radius, keratometry, central corneal thickness, lens thickness, and white-to-white measurements. Interpretable machine learning tools are now being studied for predicting childhood myopia. Results from a recent study by Feng et al, in a large cohort of 2365 children, showed that axial length-to-corneal curvature radius is a superior parameter for predicting childhood myopia.[85]
Evaluation of childhood myopia should confirm the refractive error, determine the degree and rate of progression, detect amblyopia or binocular vision problems, and rule out posterior segment changes associated with high myopia (see Table 10). The American Academy of Ophthalmology Pediatric Eye Evaluations Preferred Practice Pattern includes age-appropriate visual acuity testing, external and anterior segment examination, cycloplegic refraction, fundus examination, sensorimotor evaluation, intraocular pressure measurement when indicated, and imaging when clinically required.[6] In addition to cycloplegic refraction, baseline assessment should include unaided and best-corrected distance visual acuity, near visual acuity, ocular alignment, stereopsis, accommodation, convergence, pupillary examination, and slit-lamp biomicroscopy. Visual acuity should be measured using age-appropriate standardized charts, and both monocular and binocular acuities should be recorded. In preverbal or developmentally delayed children, fixation preference, red reflex testing, photoscreening, and instrument-based screening may help identify significant refractive error.[8]
Axial length measurement is increasingly important in the evaluation of childhood myopia because refractive error alone may not fully reflect structural progression. Baseline axial length allows objective monitoring of ocular growth, assessment of treatment response, and risk stratification for high myopia. The axial length to corneal curvature ratio may be useful because it reflects the relationship between axial length and corneal power and may identify children at higher risk of incident myopia or faster progression.[9]
Corneal topography or tomography is not mandatory for every child with simple myopia but should be considered when high astigmatism, rapidly changing astigmatism, reduced best-corrected visual acuity, an abnormal retinoscopic reflex, suspected keratoconus, or a family history of corneal ectasia is present. Keratometry obtained from optical biometry may provide additional information, but tomography is preferred when corneal pathology is suspected.[8] Dilated retinal evaluation should document the optic disc, macula, posterior pole, and peripheral retina. In high or progressive myopia, wide-field fundus photography may be useful for baseline documentation of peripapillary atrophy, tilted disc, lattice degeneration, retinal holes, posterior staphyloma, or myopic maculopathy. Optical coherence tomography of the macula and optic nerve is indicated when reduced best-corrected visual acuity, metamorphopsia, suspected macular pathology, an optic disc anomaly, glaucoma suspicion, or high axial myopia is present.[11]
Laboratory testing is not routinely required for uncomplicated childhood myopia. Systemic evaluation or genetic referral should be considered in children with very early-onset high myopia, developmental delay, dysmorphic features, hearing loss, skeletal abnormalities, joint hypermobility, ectopia lentis, congenital cataract, retinal dystrophy, night blindness, or a family history suggesting syndromic myopia. Important associated disorders include Stickler syndrome, Marfan syndrome, Weill-Marchesani syndrome, homocystinuria, Knobloch syndrome, congenital stationary night blindness, and retinopathy of prematurity.[17] A child with simple myopia does not usually require laboratory or radiographic testing. Imaging is ophthalmic rather than radiologic and is directed toward documenting axial length, corneal parameters, and retinal status. Neuroimaging is not indicated for routine myopia but should be considered if reduced vision is unexplained by refractive error, optic nerve pallor or swelling is present, or neurologic symptoms accompany visual concerns.[21]
Table 10. Clinical Evaluation of Myopia
|
Evaluation component |
Purpose |
Importance |
|
Unaided and best-corrected visual acuity |
Establish functional visual status |
All children |
|
Cycloplegic refraction |
Confirm true refractive error |
Children, accommodative spasm, inconsistent refraction |
|
Ocular alignment and stereopsis |
Detect strabismus or binocular dysfunction |
Anisometropia, amblyopia risk |
|
Accommodation and convergence testing |
Identify near-vision stress or accommodative lag |
Headache, asthenopia, heavy near work |
|
Slit-lamp examination |
Rule out anterior segment causes |
Lens abnormality, ectopia lentis, cataract |
|
Dilated fundus examination |
Detect myopic posterior segment changes |
High myopia, rapid progression |
|
Axial length measurement |
Objective progression monitoring |
Myopia-control follow-up |
|
Corneal topography/tomography |
Exclude corneal ectasia |
High/irregular astigmatism |
|
OCT macula/optic nerve |
Detect macular or optic nerve complications |
High myopia, reduced best-corrected visual acuity |
|
Wide-field fundus imaging |
Document peripheral lesions |
Lattice, holes, high axial myopia |
|
Systemic/genetic evaluation |
Identify syndromic myopia |
Early-onset high myopia or systemic features |
Abbreviation: OCT, optical coherence tomography.
A child with simple myopia does not usually require laboratory or radiographic testing. Imaging is ophthalmic rather than radiologic and is directed toward documenting axial length, corneal parameters, and retinal status. Neuroimaging is not indicated for routine myopia but should be considered if reduced vision is unexplained by refractive error, optic nerve pallor or swelling is present, or neurologic symptoms accompany visual concerns.[5]
Treatment / Management
Management of Myopia in Children
Spectacles: Spectacles are the most commonly advised treatment option for childhood myopia. Refractive error correction should be performed after cycloplegia. Spectacle coverage remains an important issue in resource-limited settings. When prescribing spectacles to children, clinicians should consider factors such as the shape and weight of frames and lenses to improve adherence.[6]
Contact lenses: Soft contact lenses and rigid gas-permeable lenses can be prescribed to correct myopia. However, there is no substantial evidence that these modalities can reduce myopia progression.[86](B2)
Measures for Controlling Myopia Progression
Drugs for myopia control: As of June 2022, the US Food and Drug Administration (FDA) had not approved any pharmacologic agents for the treatment of myopia. However, atropine 0.01% is the most widely studied drug for slowing myopia progression. The Atropine in Myopia 1 (ATOM-1) study was conducted to evaluate the role of atropine 1%.[87] The Atropine in Myopia Study 2 (ATOM-2) examined the roles of atropine 0.5%, 0.1%, and 0.01% in treating myopia and was conducted in 2 phases. The study results found that atropine 0.01% was a safe and effective option for myopia treatment, with minimal adverse effects, including photophobia and loss of accommodation, compared with atropine 1% and 0.5%.[88] (A1)
The Low-Concentration Atropine for Myopia Progression (LAMP) study further evaluated the role of lower concentrations of atropine, including 0.05%, 0.025%, and 0.01%, in slowing myopia progression and found 0.05% to be the optimal concentration.[89] Similar results were also reported by Saxena et al in India.[90] Atropine is an anticholinergic drug that acts nonselectively on acetylcholine receptors, thereby downregulating their function. Acetylcholine regulates eye growth and plays a crucial role in retinal development.[91] Atropine stimulates the synthesis of the scleral extracellular matrix, thereby reducing scleral rigidity and its tendency to elongate.[92] (A1)
At the cellular level, atropine has been found to downregulate the epidermal growth factor receptor pathways.[93] Results from animal models showed that intravitreal atropine promotes dopamine release, thereby further regulating the increase in axial length.[94] Atropine also reduces choroidal thinning caused by hyperopic defocus in myopic eyes.[95] Another hypothesis states that atropine controls myopia progression by regulating excessive accommodation. However, subsequent results showed that myopia induction could not be stopped even after experimental elimination of the accommodation reflex by optic nerve sectioning or destruction of Edinger-Westphal nuclei.[96](B3)
Pirenzapine: Pirenzapine is a selective M1 and M4 muscarinic receptor antagonist. Because of its better safety profile, pirenzapine was studied for the treatment of myopia at concentrations of 0.5% and 2%.[97][98] (A1)
7-Methylxanthine: 7-Methylxanthine is a metabolite of theobromine and caffeine. The possible mechanism of action of the drug is to modulate axial length by increasing collagen fibril diameter and the overall thickness of the posterior sclera.[99](B3)
Intraocular Pressure-lowering drugs: Drugs such as timolol maleate and latanoprost have been used to halt myopia progression.[100] Please see StatPearls' companion reference, "Latanoprost," for further information. Evidence suggests that intraocular pressure causes stretch on the outer scleral wall, leading to enlargement of the eyeball.[101] The biomechanically weaker scleral walls in patients with myopia are at increased risk of stretching due to elevated intraocular pressure. Therefore, a decrease in intraocular pressure can slow elongation of the eye, thereby slowing myopia progression.[102](B2)
Lifestyle modifications, outdoor activities: The risk of myopia decreases by 2% for every 1-hour increase in time spent outdoors.[103] Increasing the duration of outdoor activity to 14 hours per week can reduce the risk of developing myopia by one-third. Outdoor activities reduce myopia progression by promoting the release of dopamine.[104] Dopamine inhibits axial length elongation.[105] Another mechanism could be the difference in spatial frequencies between indoor and outdoor environments. Enhancing spatial frequency can help limit myopia progression.[104][106][105](B2)
Bifocal and multifocal glasses: Myopia progression is thought to result from prolonged accommodation. Treatment with bifocal or multifocal glasses is considered beneficial because these lenses relax accommodation. Results from a study by Cheng et al reported a 40% decrease in myopia progression with bifocal glasses.[107](A1)
Progressive glasses: Progressive glasses have been studied for their effectiveness in controlling myopia progression. Results from a study by Gwiazda et al on progressive additional lenses showed a 20% reduction in myopia progression during the first year of use.[108] Further, the results showed that progressive glasses were more beneficial for children with 2 myopic parents, a larger accommodative lag, or near esophoria.[109] (B2)
Defocus incorporated multiple segments spectacle (DIMS): Defocus incorporated multiple segments (DIMS) spectacles inhibit myopia progression by inducing myopic defocus. Results from animal studies found that myopic defocus reduces the eye axial length, whereas hyperopic defocus increases axial length.[110][111] DIMS consists of a central zone with a 9-mm diameter and annular zones of 33 mm with a relative positive power of +3.50 diopters. Each segment has a diameter of 1.03 mm.[112] This lens design induces myopic defocus while maintaining clear vision. Results from a study by Lam et al showed that continuous wear of DIMS reduced myopia progression by 52% and axial length progression by 62%.[112] (A1)
Defocus-incorporated soft contact lenses: Defocus-incorporated soft contact lenses are bifocal lenses with a central correction zone and a sequence of alternating correction and defocus zones in the periphery.[113] This induces myopic defocus while maintaining clear vision.[114] The power of the central zone was customized to the cycloplegic refractive error, while the defocusing zones were set to a relatively negative 2.5 D. Daily use of a defocus-incorporated soft contact lens for 5 to 8 hours has been shown to reduce myopia progression.[113] Similarly, dual-focus soft contact lenses have also been found to reduce myopia progression.[115](A1)
Orthokeratology: Orthokeratology is the only US FDA-approved modality for myopia. Orthokeratology involves wearing overnight contact lenses that reshape the cornea from prolate to oblate, thereby reducing refractive error. Contact lenses appear to be a promising adjunct to other options, but hygiene and maintenance issues need to be addressed and explained to patients and guardians.[116]
Red light phototherapy: Repeated red light phototherapy is a noninvasive treatment that uses light at 650 nm to slow myopia progression. The therapy is administered for 3 min twice daily. Red light phototherapy acts by increasing choroidal blood perfusion and choroidal thickness.[117][118](A1)
Other therapies explored in the treatment of myopia and reduction of myopia progression include posterior scleral contraction, posterior scleral reinforcement, scleral cross-linking with riboflavin, which can cause loss of photoreceptors, outer nuclear layer, and retinal pigment epithelium; subscleral injection of mesenchymal stem cells and dopamine; intravitreal injection of aquaporin 1; and scleral strengthening using sub-Tenon chemicals such as ethyl acrylate and acrylamide hydrazide.[119][120][121](B3)
Treatment Goals and Risk Stratification
The primary goals of childhood myopia treatment are to provide clear distance vision, prevent amblyopia, maintain binocular function, slow progression of refractive error and axial length, reduce the risk of high myopia, and minimize the risk of future sight-threatening complications. Treatment should be individualized according to age of onset, baseline spherical equivalent, rate of progression, axial length, parental myopia, binocular vision status, lifestyle risk factors, and the child’s ability to adhere to treatment. Children with early-onset myopia, rapid progression, high axial length, or 2 myopic parents should be considered at higher risk and monitored more closely.[20]
Full Correction Versus Undercorrection
Full optical correction is generally preferred in children with myopia to provide clear distance vision and avoid visual disability, poor school performance, and abnormal visual development. Undercorrection is not recommended as a myopia-control strategy because it may increase retinal blur and does not reliably slow progression. Overminus correction should also be avoided, particularly in children with accommodative or binocular vision problems.[122](A1)
FDA-Approved Myopia Control Options in the United States
The earlier statement that no US FDA-approved myopia management drugs existed remains correct for pharmacologic agents, but it should be updated to reflect that no US FDA-approved devices exist. MiSight 1-day soft contact lenses (CooperVision) are FDA-approved for the correction of myopia and slowing progression in children aged 8 to 12 years at initiation, with spherical equivalent refraction from −0.75 D to −4.00 D and astigmatism of less than 0.75 D. In 2025, the FDA also granted de novo authorization for Essilor Stellest spectacle lenses (EssilorLuxottica) for correction of myopia, with or without astigmatism, and slowing progression in children aged 6 to 12 years at initiation, with spherical equivalent refraction from −0.75 D to −4.50 D and astigmatism up to 1.50 D.[123](B2)
Follow-Up and Monitoring
Children undergoing myopia control should be reviewed regularly to assess visual acuity, refractive change, axial length progression, adherence, tolerance, and adverse effects. Follow-up every 6 months is commonly used for stable vision, while 3- to 4-month reviews may be appropriate for children with rapid progression or those recently started on atropine, orthokeratology, or myopia-control contact lenses. Axial length monitoring is preferred when available because it provides an objective measure of structural progression.[124](A1)
Combination Therapy
Combination therapy may be considered in children with rapid progression despite monotherapy. Common approaches include low-dose atropine with orthokeratology, atropine with myopia-control spectacles, or atropine with dual-focus contact lenses. Combination treatment should be individualized, and clinicians should monitor for additive adverse effects, adherence issues, and cost burden.[125]
Counseling and Adherence
Parents should be counseled that myopia control slows progression but usually does not eliminate progression completely. Treatment benefit depends on consistent spectacle or contact lens wear, proper contact lens hygiene, regular follow-up, and lifestyle modification. Families should be educated about warning signs, including sudden floaters, flashes, curtain-like visual field loss, ocular pain, redness, photophobia, or sudden decline in vision.[126]
Safety Considerations
Atropine may cause photophobia, blurred vision, allergic conjunctivitis, periocular dermatitis, and, rarely, systemic anticholinergic symptoms. Contact lens–based treatments require strict hygiene, avoidance of water exposure, and prompt discontinuation if pain, redness, discharge, or photophobia occurs. FDA device data list corneal ulcer, infection, red eye, eye pain, Acanthamoeba keratitis, and keratitis as reported adverse events for daily-wear soft myopia-control contact lenses.[127]
Discontinuation and Rebound
Myopia-control treatment should generally be continued through the active progression years and reassessed during mid-to-late adolescence. Abrupt cessation of higher-dose atropine may be associated with rebound progression; therefore, tapering or step-down therapy may be considered, especially after prolonged treatment or in younger children. Continued monitoring after discontinuation is important to detect recurrence of progression.[128]
Surgical Management
Refractive surgical procedures are not recommended for routine childhood myopia because refractive error and axial length are still changing. Surgical intervention in childhood myopia is generally limited to treatment of complications such as retinal tears, retinal detachment, myopic choroidal neovascularization, macular hole, cataract, or glaucoma in highly myopic eyes. Posterior scleral reinforcement and other scleral procedures remain investigational or selectively used in limited settings and are not standard first-line therapy.[129]
Differential Diagnosis
Other causes of low vision in children should be ruled out, including keratoconus, pediatric cataracts, microspherophakia, pediatric glaucoma, trauma, iridofundal coloboma, nystagmus, congenital optic nerve abnormalities such as optic disc coloboma, large myelinated nerve fibers involving the fovea, and congenital retinal anomalies such as pigmentary retinopathy (see Table 11). Clinicians should also ask about birth history, history of laser treatment for retinopathy of prematurity, delayed cry at birth, and history of intensive care unit hospitalizations. Myopia can also be associated with Down syndrome (8% to 41%).[130] Other differential diagnosis include:
Marfan syndrome and stickler syndrome: Pseudomyopia is the overestimation of myopia resulting from excessive accommodation, typically seen in children. Therefore, refraction without cycloplegia overestimates myopia by −1 to −2 diopters.[131]
Accommodative spasm: Accommodative spasm results from excessive contraction of the ciliary muscle, producing a transient myopic shift. Children typically report fluctuating distance vision, headaches, and visual fatigue. Cycloplegic refraction reveals significantly less myopia than manifest refraction.[132]
Night myopia: Some children and adolescents experience increased myopic refractive error under dim illumination due to accommodative and optical factors. Symptoms are usually limited to reduced distance vision during evening activities and driving, while daytime vision remains relatively unaffected.[133]
Index myopia secondary to metabolic disorders: Transient myopic shifts may occur in systemic metabolic conditions such as uncontrolled diabetes mellitus due to osmotic changes within the crystalline lens. These changes are often reversible following correction of the underlying metabolic disturbance. Please see StatPearls' companion reference, "Collagen Cross Linking for Keratoconus," for further information.
Lens subluxation and ectopia lentis: Displacement of the crystalline lens alters the refractive status and may mimic progressive myopia. Slit-lamp examination may reveal lens decentration, phacodonesis, or zonular weakness. Associated systemic findings may suggest an underlying connective tissue disorder.[5]
Posterior lenticonus: Posterior protrusion of the lens capsule increases lenticular power and may induce unilateral or asymmetric myopia. Affected children frequently present with anisometropia, amblyopia, or an unexplained reduction in visual acuity.[11]
Corneal ectatic disorders other than keratoconus: Conditions such as pellucid marginal degeneration and keratoglobus may produce progressive myopia and irregular astigmatism. Corneal topography or tomography is often required to distinguish these disorders from simple axial myopia. Please see StatPearls' companion reference, "Myopia," for further information.
Retinopathy of prematurity–associated refractive error: Children with a history of prematurity may develop myopia due to altered anterior segment development, lens changes, and abnormal ocular growth. The refractive profile and retinal findings help differentiate this entity from typical school-age myopia.[134]
Congenital stationary night blindness: This inherited retinal disorder may present with childhood myopia before retinal dysfunction becomes apparent. Symptoms include impaired night vision, reduced contrast sensitivity, and characteristic electroretinographic abnormalities.[135]
X-linked juvenile retinoschisis: Affected boys may present with reduced vision and myopia during childhood. Fundus examination and optical coherence tomography typically demonstrate foveal schisis and splitting of the retinal layers.[136]
Ocular albinism: Children with ocular albinism may exhibit refractive errors, reduced visual acuity, nystagmus, and photophobia. Iris transillumination defects and foveal hypoplasia distinguish the condition from uncomplicated myopia.[137]
Leber congenital amaurosis: High refractive errors, including severe myopia, may occur in association with this inherited retinal dystrophy. Profound visual impairment, oculodigital behavior, and markedly abnormal electroretinography aid diagnosis.[138]
Achromatopsia: Children may initially be thought to have refractive blur due to reduced visual acuity. However, severe photophobia, color vision deficiency, and pendular nystagmus are characteristic findings.[139]
Optic nerve hypoplasia: Reduced visual acuity and poor visual development may be mistaken for uncorrected refractive error. Fundus examination reveals a small optic disc, often accompanied by visual field defects and variable endocrine abnormalities.[140]
Septo-optic dysplasia: Visual impairment in affected children may initially prompt evaluation for refractive error. Neuroimaging and endocrine assessment often reveal associated midline brain and pituitary abnormalities.[141]
Cerebral visual impairment: Children with neurologic injury may demonstrate poor visual performance despite relatively normal ocular findings. Visual dysfunction is related to impaired cortical processing rather than refractive error.[142]
Cone-rod dystrophy: Progressive central visual loss, photophobia, and color vision abnormalities may initially be attributed to refractive causes. Electroretinography and retinal imaging are helpful in establishing the diagnosis.
Juvenile open-angle glaucoma: Axial elongation and myopic refractive error may coexist with elevated intraocular pressure in susceptible children. Optic nerve evaluation and gonioscopy are essential when glaucoma is suspected.[143]
Familial exudative vitreoretinopathy: This inherited retinal vascular disorder may present with high myopia, retinal dragging, or peripheral retinal abnormalities. Careful peripheral retinal examination and family history are often diagnostic.[144]
Wagner syndrome: Wagner syndrome is an inherited vitreoretinopathy characterized by high myopia, vitreous degeneration, and progressive retinal changes. This disorder may mimic simple myopia during early childhood before retinal manifestations become apparent.[145]
Knobloch syndrome: High myopia may be the earliest ocular finding in this rare hereditary condition. Occipital skull defects, vitreoretinal degeneration, and retinal detachment help establish the diagnosis.[146]
Table 11. Differential Diagnosis of Childhood Myopia
Abbreviations: ERG, electroretinography; IOP, intraocular pressure; OCT, optical coherence tomography; ROP, retinopathy of prematurity.
|
Condition |
Key distinguishing feature |
|
Accommodative spasm |
Large difference between manifest and cycloplegic refraction |
|
Night myopia |
Symptoms limited to dim illumination |
|
Posterior lenticonus |
Localized posterior lens bulge |
|
Ectopia lentis |
Lens displacement and zonular weakness |
|
Pellucid marginal degeneration |
Inferior corneal thinning on tomography |
|
Retinopathy of prematurity |
Prematurity history and peripheral retinal changes |
|
Congenital stationary night blindness |
Nyctalopia and abnormal ERG |
|
X-linked retinoschisis |
Foveal schisis on OCT |
|
Ocular albinism |
Iris transillumination and foveal hypoplasia |
|
Leber congenital amaurosis |
Severe early visual impairment |
|
Optic nerve hypoplasia |
Small optic disc and developmental abnormalities |
|
Cerebral visual impairment |
Normal ocular examination with cortical dysfunction |
|
Juvenile glaucoma |
Elevated IOP and glaucomatous optic neuropathy |
|
Familial exudative vitreoretinopathy |
Peripheral avascular retina |
|
Wagner syndrome |
Vitreous degeneration and inherited vitreoretinopathy |
|
Knobloch syndrome |
High myopia with occipital defects |
Pertinent Studies and Ongoing Trials
The evidence base for childhood myopia management is strongest for low-dose atropine, myopia-control spectacle lenses, dual-focus or multifocal soft contact lenses, orthokeratology, and outdoor-time interventions. Most randomized trials use cycloplegic spherical equivalent refraction and axial length progression as the primary outcome measures (see Table 12).[5]
Table 12. Key Trials in Myopia
|
Intervention |
Key trial |
Study design |
Main outcome |
Clinical interpretation |
|
Low-dose atropine |
ATOM-2 |
Randomized clinical trial |
0.01% atropine had fewer adverse effects and less rebound than higher concentrations |
Supports low-dose atropine as a tolerable option |
|
Low-concentration atropine |
LAMP study |
Randomized, double-masked, placebo-controlled trial |
0.05%, 0.025%, and 0.01% atropine reduced progression in a dose-dependent manner; 0.05% was most effective over 1 year |
Supports 0.05% atropine as an effective concentration where available |
|
Atropine 0.01% in US children |
PEDIG/US randomized trial |
Randomized placebo-controlled trial |
0.01% atropine did not significantly slow myopia progression compared with placebo |
Suggests regional/ethnic variability and that 0.01% may be insufficient in some populations |
|
DIMS spectacle lenses |
Lam et al |
2-year double-masked randomized trial |
DIMS reduced myopia progression and axial elongation compared with single-vision lenses |
Supports peripheral myopic-defocus spectacle designs |
|
Multifocal soft contact lenses |
BLINK trial |
3-year randomized clinical trial |
High-add multifocal lenses slowed myopia progression by about 43% compared with single-vision lenses |
Supports high-add multifocal soft contact lenses in appropriate children |
|
Dual-focus soft contact lenses |
MiSight 1 day trial |
3-year randomized double-masked clinical trial |
Reduced spherical equivalent progression and axial elongation versus single-vision contact lenses |
Supports FDA-approved dual-focus daily disposable contact lens use in selected children |
|
Outdoor activity |
Guangzhou outdoor intervention |
Cluster-randomized school-based trial |
Additional outdoor time reduced incident myopia over 3 years |
Supports outdoor-time prescription for prevention, especially pre-myopic children |
|
Repeated low-level red-light therapy |
RLRL trials |
Randomized clinical trials |
Reduced axial elongation and, in some studies, produced axial shortening |
Promising, but long-term retinal safety and rebound require further study |
|
Orthokeratology |
Multiple randomized and cohort studies |
Overnight corneal reshaping lens studies |
Slows axial elongation compared with single-vision spectacles |
Useful in selected compliant children; infection risk must be discussed |
Abbreviations: ATOM-2, Atropine in Myopia Study 2; BLINK, Bifocal Lenses in Nearsighted Kids; DIMS, defocus incorporated multiple segments; FDA, Food and Drug Administration; LAMP, Low-Concentration Atropine for Myopia Progression; PEDIG, Pediatric Eye Disease Investigator Group; RLRL, repeated low-level red-light.
Several randomized trials support active myopia-control therapy rather than simple refractive correction alone. The ATOM and LAMP studies established low-concentration atropine as an effective pharmacologic option, with LAMP demonstrating a concentration-dependent response and the greatest 1-year efficacy at 0.05% atropine.[68] However, a US randomized trial found that atropine 0.01% was not superior to placebo, suggesting that very-low-dose atropine may not be equally effective across all populations.[128]
Optical myopia-control interventions are supported by randomized clinical trial evidence. DIMS spectacle lenses reduce myopia progression and axial elongation by imposing simultaneous clear central vision and peripheral myopic defocus. Multifocal and dual-focus soft contact lenses, including high-add multifocal designs and MiSight 1-day lenses, have demonstrated a clinically meaningful reduction in refractive progression and axial elongation in school-aged children.[147]
School-based randomized trials support increased outdoor time as a preventive strategy, particularly for reducing the incidence of myopia in children without myopia or with premyopia. Orthokeratology has shown consistent benefit in slowing axial elongation but requires careful patient selection, contact lens hygiene, and monitoring for microbial keratitis. Repeated low-level red-light therapy has shown encouraging short-term outcomes, including reduced axial elongation in randomized trials, but longer-term safety, rebound after cessation, optimal dosing, and retinal safety remain to be evaluated.[148]
Ongoing and Emerging Areas
Current research focuses on combination therapy, personalized atropine dosing, newer spectacle designs, the long-term safety of red-light therapy, rebound after treatment discontinuation, and artificial intelligence–based prediction of progression. Future trials should include standardized axial length outcomes, longer follow-up after cessation of treatment, safety reporting, quality-of-life measures, and subgroup analyses by age, ethnicity, baseline refraction, parental myopia, and axial length.[149]
Treatment Planning
Treatment planning for childhood myopia should be individualized based on the child's age, baseline refractive error, axial length, rate of progression, family history, environmental risk factors, binocular vision status, and risk of developing high myopia (see Table 13). The primary goals are to provide optimal visual correction, slow axial elongation, preserve binocular visual development, and reduce the lifetime risk of pathological myopia and its associated complications.[5] All children diagnosed with myopia should undergo baseline documentation of cycloplegic refraction, visual acuity, ocular alignment, binocular vision status, and, where available, axial length measurement. Risk stratification should be performed at the initial visit. Children with early-onset myopia (younger than 8 years), rapid progression (> 0.50 D/year), significant axial elongation, parental myopia, or high baseline refractive error require closer surveillance and consideration of active myopia-control interventions. The International Myopia Institute recommends a structured approach consisting of risk assessment, education, optical correction, environmental modification, initiation of myopia-control therapy when indicated, and longitudinal monitoring. Parents and caregivers should be informed that myopia progression is typically most rapid during the early school years and that treatment effectiveness should be evaluated over time rather than at a single visit.[6]
Table 13. Risk-Based Treatment Planning
|
Risk category |
Typical characteristics |
Management approach |
|
Low risk |
Mild myopia, older age at onset, slow progression |
Spectacle correction, lifestyle counseling, periodic monitoring |
|
Moderate risk |
Progression 0.25–0.50 D/year, positive family history |
Consider myopia-control spectacles, contact lenses, or low-dose atropine |
|
High risk |
Onset younger than 8 years, progression > 0.50 D/year, increasing axial length, parental high myopia |
Active myopia-control therapy and closer follow-up |
|
Very high Risk |
High myopia, pathological fundus changes, and syndromic myopia |
Interdisciplinary care and frequent retinal surveillance |
Initial Management Strategy
At diagnosis, full refractive correction should be prescribed to ensure optimal visual development and academic performance. Environmental interventions should be recommended for all children regardless of refractive status. Current evidence supports increasing outdoor activity to at least 2 h/d (approximately 10 to 14 h/wk), limiting prolonged uninterrupted near work, maintaining appropriate reading distance, and encouraging regular visual breaks during digital device use.
Children demonstrating progressive myopia should be considered for evidence-based myopia-control therapy. Treatment selection depends on patient age, refractive status, lifestyle, ocular characteristics, treatment availability, and family preference. Options include low-dose atropine, defocus-incorporated multiple-segment or highly aspherical lenslet spectacle lenses, dual-focus or multifocal soft contact lenses, and orthokeratology.[124]
Monitoring Treatment Response
Successful treatment planning requires objective monitoring. Refractive progression should ideally be assessed using cycloplegic refraction, while axial length measurement provides a more sensitive indicator of ocular growth. Treatment effectiveness should be evaluated at regular intervals, typically every 6 months.
The following parameters should be documented at follow-up:
- Uncorrected and corrected visual acuity
- Cycloplegic spherical equivalent
- Axial length (if available)
- Binocular vision and accommodative status
- Treatment adherence
- Adverse effects
- Rate of progression compared with baseline [150]
Criteria for Treatment Escalation
Treatment escalation should be considered when any of the following occur:
- Progression exceeding 0.50 D/year
- Significant axial elongation despite treatment
- Development of high myopia
- Poor treatment adherence
- Intolerance to current therapy
- Strong family history with ongoing progression
Escalation strategies may include increasing atropine concentration, switching to an alternative optical intervention, or implementing combination therapy.[151]
Long-Term Management
Myopia control is a long-term process extending throughout the active growth period of childhood and adolescence. Treatment is generally continued until refractive stability is achieved, typically in the mid-to-late adolescent years. After treatment cessation, continued monitoring is recommended because rebound progression may occur, particularly following atropine discontinuation.
Suggested Treatment Planning Algorithm for Childhood Myopia
- Confirm the diagnosis with cycloplegic refraction and, when available, axial length measurement.
- Stratify the child as low, moderate, or high risk based on age at onset, baseline refractive error, axial length, rate of progression, parental myopia, and posterior segment findings.
- Recommend lifestyle modification for all children, including increased outdoor activity, reduced prolonged uninterrupted near work, appropriate reading distance, and regular visual breaks during digital device use.
- Select an appropriate myopia-control strategy based on risk category, ocular findings, family preference, treatment availability, and ability to adhere to therapy. Options include spectacle correction, low-dose atropine, myopia-control spectacle lenses, myopia-control contact lenses, and orthokeratology.
- Monitor response at regular intervals, typically every 6 months, using visual acuity, cycloplegic refraction, axial length measurement when available, treatment adherence, and adverse effects.
- Continue the current therapy if myopia remains stable. Escalate or combine treatments if refractive progression or axial elongation continues despite therapy.
- Continue follow-up through adolescent stabilization and provide long-term surveillance for children with high or pathologic myopia.
Key Clinical Pearl
The most effective treatment planning strategy is early identification of children at risk for rapid progression and timely initiation of evidence-based myopia-control interventions before significant axial elongation occurs, because prevention of high myopia remains more effective than treatment of its complications later in life.[152]
Toxicity and Adverse Effect Management
The management of childhood myopia is generally safe; however, adverse effects may occur depending on the treatment modality used. Clinicians should counsel children and caregivers about potential complications, monitor treatment tolerance at follow-up visits, and promptly address treatment-related adverse events to optimize adherence and long-term outcomes (see Table 14).
Atropine-Associated Adverse Effects
Topical atropine is the most widely studied pharmacologic therapy for myopia control. The frequency and severity of adverse effects are concentration-dependent. Higher concentrations (0.5% to 1%) are associated with photophobia, glare, reduced accommodation, near blur, and pupillary dilation, whereas lower concentrations (0.01% to 0.05%) generally demonstrate a more favorable safety profile. Patients experiencing photophobia may benefit from photochromic or tinted lenses, ultraviolet protection, and avoidance of excessive sunlight exposure. Near-vision blur can be treated with temporary near additions or by reducing atropine concentration when clinically appropriate. Ocular surface irritation, allergic conjunctivitis, and periocular dermatitis should prompt evaluation for preservative sensitivity or drug intolerance. Rare systemic anticholinergic adverse effects include facial flushing, fever, tachycardia, dry mouth, constipation, urinary retention, behavioral changes, confusion, and central nervous system toxicity. Caregivers should be instructed to perform punctal occlusion following instillation and store medications securely to prevent accidental ingestion. Significant systemic toxicity requires immediate medical evaluation.[153]
Contact Lens–Related Complications
Soft multifocal contact lenses, dual-focus contact lenses, and orthokeratology lenses may cause contact lens–associated complications. Common adverse effects include dry eye symptoms, foreign body sensation, lens discomfort, superficial punctate keratopathy, allergic conjunctivitis, and giant papillary conjunctivitis. Microbial keratitis remains the most serious complication associated with contact lens wear, particularly orthokeratology. Risk factors include overnight lens wear, poor hygiene, water exposure, improper lens storage, and inadequate follow-up. Patients presenting with pain, redness, photophobia, discharge, or sudden visual deterioration should discontinue lens wear immediately and undergo urgent ophthalmic evaluation. Corneal staining, epithelial defects, corneal infiltrates, and sterile inflammatory reactions may require temporary discontinuation of lens wear, lubrication, modification of lens parameters, or treatment of associated ocular surface disease.[154]
Orthokeratology-Specific Adverse Effects
Orthokeratology may be associated with corneal molding irregularities, lens decentration, induced astigmatism, corneal staining, epithelial iron deposition, and transient visual disturbances such as halos and glare. Most complications are reversible following lens discontinuation. Regular corneal topography is recommended to monitor treatment response and detect early complications. Please see StatPearls' companion reference, "Cycloplegic and Noncycloplegic Refraction," for further information.
Spectacle-Related Issues
Although spectacles are among the safest interventions, adaptation difficulties, image distortion, peripheral aberrations, frame intolerance, and adherence issues may occur. Children should undergo periodic reassessment to ensure appropriate refractive correction and proper frame fit. Please see StatPearls' companion reference, "Contact Lens–Related Complications," for further information.
Defocus and Multifocal Spectacle Lens Adverse Effects
Children using DIMS lenses, highly aspherical lenslet designs, or progressive addition lenses may initially report peripheral blur, altered depth perception, mild dizziness, or adaptation difficulties. Symptoms typically improve during the adaptation period. Persistent visual discomfort may require reassessment of lens centration, prescription accuracy, or treatment selection.[155]
Repeated Low-Level Red-Light Therapy Adverse Effects
Repeated low-level red-light therapy has generally demonstrated favorable short-term safety profiles in clinical studies. Reported adverse effects include transient afterimages, mild visual discomfort, temporary glare phenomena, and visual fatigue. Because long-term retinal safety data remain limited, periodic retinal evaluation and adherence to recommended treatment protocols are essential. Excessive exposure or unsupervised use should be avoided.[156]
Monitoring for Myopia Progression Despite Therapy
Treatment failure represents an important treatment challenge rather than a direct adverse effect. Continued progression despite therapy may result from poor adherence, inadequate treatment intensity, inappropriate patient selection, or individual variability in treatment response. These patients may require escalation of atropine concentration, transition to an alternative modality, or combination therapy.[157]
Rebound Following Treatment Discontinuation
Rebound progression may occur following cessation of myopia-control therapy, particularly after higher-concentration atropine treatment. Children undergoing treatment discontinuation should be monitored closely with periodic cycloplegic refraction and axial length measurements. Gradual tapering strategies may reduce the risk of rebound in selected patients.[158]
Table 14. Management of Treatment-Related Adverse Effects
|
Treatment modality |
Common adverse effects |
Management strategy |
|
Low-dose atropine |
Photophobia, mild near blur |
Photochromic lenses, dose adjustment |
|
High-dose atropine |
Accommodation loss, glare, systemic anticholinergic effects |
Dose reduction, monitoring, discontinuation if necessary |
|
Soft contact lenses |
Dryness, discomfort, allergic reactions |
Lubrication, hygiene optimization |
|
Orthokeratology |
Corneal staining, lens decentration, microbial keratitis |
Topography monitoring, temporary discontinuation, and infection management |
|
Multifocal spectacles |
Peripheral blur, adaptation difficulties |
Patient education and observation |
|
Red-light therapy |
Afterimages, visual fatigue, glare |
Protocol adherence and follow-up monitoring |
|
Combination therapy |
Increased treatment burden and compliance issues |
Simplified regimens and regular counseling |
Clinical Monitoring Recommendations
Children receiving active myopia-control therapy should undergo periodic evaluation of:
- Visual acuity
- Cycloplegic refractive error
- Axial length progression
- Ocular surface status
- Corneal integrity (for contact lens users)
- Treatment adherence
- Drug-related adverse effects
- Fundus status in high myopia
Key Clinical Pearl
Most adverse effects associated with childhood myopia interventions are mild, reversible, and manageable with appropriate monitoring. The greatest vision-threatening complication is contact lens–associated microbial keratitis, while the most common pharmacologic adverse effects are photophobia and reduced accommodation with atropine therapy. Early recognition and management of complications improve treatment adherence and long-term outcomes.[159]
Staging
For Childhood Myopia and Ocular Development, there is no universally accepted formal staging system analogous to those used in cancer staging or diabetic retinopathy grading. However, several clinically relevant classification systems categorize myopia by refractive error, axial length, age of onset, progression rate, and the presence of pathological changes (see Table 15).[6]
Staging
Although childhood myopia lacks a universally accepted staging system, classification based on refractive magnitude, age of onset, progression characteristics, and structural ocular changes is useful for clinical management, prognosis, and risk stratification. The International Myopia Institute recommends distinguishing between simple myopia, high myopia, and pathological myopia because the risk of ocular complications increases substantially with increasing axial length and refractive error.[160]
Table 15. Classification Based on Refractive Error
|
Stage |
Spherical equivalent refraction |
|
Premyopia |
≤ +0.75 D and > −0.50 D in a child with risk factors for future myopia |
|
Low myopia |
−0.50 D to < −3.00 D |
|
Moderate myopia |
−3.00 D to < −6.00 D |
|
High myopia |
≥ −6.00 D |
|
Very high myopia |
≥ −10.00 D (commonly used in research studies) |
Premyopia refers to a refractive state in which a child is not yet myopic but has a high likelihood of developing myopia due to age, family history, environmental risk factors, or excessive axial elongation.
Classification Based on Axial Length
Axial length is increasingly recognized as a more reliable indicator of myopia progression and future pathological risk than refractive error alone (see Table 16).[8]
Table 16. Myopia Classification by Axial Length
|
Stage |
Axial length |
|
Normal |
< 24 mm |
|
Mild axial myopia |
24–26 mm |
|
Moderate axial myopia |
26–28 mm |
|
High axial myopia |
> 28 mm |
|
Extreme axial myopia |
> 30 mm |
Eyes with axial lengths exceeding 26 mm demonstrate substantially increased risks of retinal detachment, myopic maculopathy, glaucoma, and choroidal neovascularization.
Table 17. Classification Based on Age of Onset
|
Category |
Age at onset |
Clinical importance |
|
Congenital myopia |
Present at birth |
Often associated with systemic or genetic disorders |
|
Early-onset myopia |
Younger than 6 years |
Higher risk of high myopia |
|
Childhood-onset myopia |
6–12 years |
Most common presentation |
|
Juvenile myopia |
6–18 years |
Period of greatest progression |
|
Late-onset myopia |
Older than 18 years |
Often associated with educational and occupational demands |
Earlier onset is strongly associated with greater lifetime axial elongation and increased risk of pathological myopia.
Table 18. Classification Based on Progression Rate
|
Stage |
Annual progression |
|
Stable |
< 0.25 D/year |
|
Slow progression |
0.25–0.50 D/year |
|
Moderate progression |
0.50–1.00 D/year |
|
Rapid progression |
> 1.00 D/year |
Children exhibiting rapid progression require closer monitoring and consideration of active myopia-control interventions (Table 18).
Pathological Myopia Classification (META-PM Classification)
The Meta-Analysis for Pathologic Myopia (META-PM) Study Group developed the most widely accepted grading system for myopic maculopathy (Table 19).
Table 19. Classification by Fundus Findings
|
Category |
Fundus findings |
|
Category 0 |
No myopic retinal lesions |
|
Category 1 |
Tessellated fundus |
|
Category 2 |
Diffuse chorioretinal atrophy |
|
Category 3 |
Patchy chorioretinal atrophy |
|
Category 4 |
Macular atrophy |
Plus lesions include:
- Lacquer cracks
- Myopic choroidal neovascularization
- Fuchs spot
The presence of plus lesions significantly increases the risk of irreversible visual impairment.[161]
Suggested Clinical Staging for Childhood Myopia
For practical pediatric use, childhood myopia can be staged as follows (Table 20):
Table 20. Childhood Staging of Myopia
|
Clinical Stage |
Characteristics |
|
Stage I (premyopia) |
At-risk child with normal refraction and progressive axial elongation |
|
Stage II (early myopia) |
Low myopia without structural changes |
|
Stage III (progressive myopia) |
Increasing refractive error and axial length growth |
|
Stage IV (high myopia) |
≥ −6.00 D or axial length > 26 mm |
|
Stage V (pathological myopia) |
Presence of retinal, choroidal, scleral, or optic nerve complications |
Prognostic Significance
The most important prognostic indicators in childhood myopia are:
- Younger age at onset
- Faster annual progression
- Increasing axial length
- Positive parental history
- Development of high myopia
- Presence of posterior segment abnormalities
Children who develop myopia before 8 years of age are significantly more likely to progress to high myopia during adolescence and therefore benefit most from early intervention and longitudinal monitoring.[160]
Prognosis
School-aged children with early-onset myopia usually have greater axial length and higher refractive error. Conversely, the progression in children with congenital myopia, defined as myopia greater than 5 diopters before age 6 years, differs. Results from a study by Shih et al found faster rates of myopia progression in children with lower grades of myopia (5.0 to 7.75 D) compared with those with higher grades (maximum of 11.0 D).[162] Patients with pathologic myopia, choroidal thinning, and posterior staphyloma have worse long-term visual outcomes.[163]
The prognosis of childhood myopia is highly variable and depends on the age of onset, baseline refractive error, rate of progression, axial length growth, genetic predisposition, environmental influences, and the development of pathological ocular changes. Most children with low-to-moderate myopia achieve excellent visual outcomes with appropriate optical correction and regular follow-up. However, children who develop myopia at an earlier age are at substantially greater risk of progressing to high myopia and experiencing vision-threatening complications later in life.[9]
Early-onset myopia is one of the strongest predictors of future high myopia. Children who become myopic before age 8 years typically exhibit longer periods of ocular growth and refractive progression, resulting in greater cumulative axial elongation. With increasing axial length, the risk of developing pathologic myopia rises significantly, independent of refractive error alone. Consequently, early identification and implementation of evidence-based myopia-control strategies may improve long-term outcomes. Please see StatPearls' companion reference, "Lenticonus," for further information.
The annual rate of progression is another important prognostic indicator. Children exhibiting rapid progression, particularly greater than 0.50 D per year, are more likely to develop high myopia during adolescence. Monitoring axial length may provide additional prognostic information because structural ocular growth often precedes measurable refractive changes. Excessive axial elongation is associated with increased risks of retinal detachment, myopic maculopathy, glaucoma, cataract, and choroidal neovascularization in adulthood.[17]
Family history strongly influences prognosis. Children with one parent with myopia demonstrate an increased risk of developing myopia, whereas those with 2 parents with myopia often experience earlier onset and greater progression. Environmental factors such as reduced outdoor activity, intensive educational demands, prolonged near work, and excessive screen exposure may further accelerate progression in genetically susceptible individuals. Please see StatPearls' companion reference, "Myopia," for further information.
Most children with uncomplicated myopia retain excellent corrected visual acuity throughout childhood and adolescence. Visual prognosis is generally favorable when refractive errors are recognized early, corrected appropriately, and monitored regularly. In contrast, children with high myopia, syndromic myopia, or secondary myopia associated with ocular developmental abnormalities may experience greater visual morbidity.[11]
The prognosis becomes less favorable when structural ocular complications develop. Progressive choroidal thinning, diffuse or patchy chorioretinal atrophy, posterior staphyloma, lacquer cracks, myopic traction maculopathy, macular hole formation, and myopic choroidal neovascularization are associated with irreversible visual impairment. The presence of pathological myopia substantially increases the lifetime risk of legal blindness and visual disability.[21]
Advances in myopia-control therapies have improved the long-term outlook for many children. Low-dose atropine, myopia-control spectacle lenses, multifocal contact lenses, orthokeratology, and behavioral interventions have been shown to slow refractive progression and axial elongation. Although these treatments do not cure myopia, they may reduce the likelihood of developing high myopia and its associated complications.[11]
Complications
Pathologic myopia can be associated with retinal complications such as retinal detachment, myopic traction maculopathy, macular hole, and choroidal neovascular membrane formation. High myopia can also be associated with subluxated lenses and a higher risk of primary open-angle glaucoma (see Table 21).[164][165] Although most children with low to moderate myopia maintain good visual function with appropriate correction, progressive axial elongation may predispose affected individuals to a spectrum of ocular complications. The risk of complications increases substantially with increasing refractive error, longer axial length, earlier age of onset, and the development of pathologic myopia (see Table 22). Many of these complications may not become clinically apparent until adolescence or adulthood, highlighting the importance of long-term surveillance.[6] Pathological myopia can be associated with retinal complications such as retinal detachment, myopic traction maculopathy, macular hole formation, myopic choroidal neovascularization, and progressive chorioretinal atrophy. High myopia is also associated with lens subluxation and an increased lifetime risk of primary open-angle glaucoma.[9]
Additional Retinal Complications
Progressive axial elongation may lead to peripheral retinal degenerations, including lattice degeneration, snail-track degeneration, retinal thinning, atrophic retinal holes, and retinal tears. These abnormalities increase the risk of rhegmatogenous retinal detachment, particularly in eyes with high myopia. Symptoms such as flashes, floaters, or a curtain-like visual field defect warrant urgent retinal evaluation. Myopic foveoschisis, also known as myopic traction maculopathy, may develop because of vitreoretinal traction and progressive posterior scleral deformation. Untreated myopic foveoschisis can progress to foveal detachment, full-thickness macular hole formation, or severe central vision loss.[9]
Choroidal and Macular Complications
Progressive choroidal thinning may result in diffuse and patchy chorioretinal atrophy. Advanced stages can culminate in macular atrophy and irreversible visual impairment. Myopic choroidal neovascularization may arise from breaks in Bruch membrane, or lacquer cracks, and can lead to hemorrhage, fibrosis, and permanent central vision loss if untreated. Posterior staphyloma represents a hallmark complication of pathologic myopia and results from localized outpouching of the weakened posterior sclera. The resulting structural deformation contributes to macular dysfunction, retinal stretching, and progressive visual decline.[9]
Optic Nerve Complications
High myopia is associated with optic disc tilting, peripapillary atrophy, and structural remodeling of the optic nerve head. These changes may complicate glaucoma diagnosis and increase susceptibility to glaucomatous optic neuropathy. Individuals with high myopia demonstrate a higher lifetime risk of developing primary open-angle glaucoma compared with individuals with emmetropia.[9]
Vitreous Complications
Excessive axial elongation accelerates vitreous liquefaction and posterior vitreous degeneration. Premature posterior vitreous detachment may occur and increase the likelihood of retinal tears and retinal detachment. Vitreomacular interface abnormalities may also contribute to tractional macular disease.[9]
Anterior Segment Complications
Eyes with high myopia often exhibit deeper anterior chambers and altered ocular biomechanics. In addition to lens subluxation, individuals with high myopia have an increased risk of earlier cataract development, particularly nuclear sclerosis and posterior subcapsular cataract. Surgical planning for cataract extraction may be more challenging due to long axial length and increased retinal vulnerability.[9]
Ocular Surface and Contact Lens–Related Complications
Children undergoing contact lens–based myopia control may experience lens intolerance, allergic conjunctivitis, dry eye symptoms, giant papillary conjunctivitis, corneal staining, corneal infiltrates, and microbial keratitis. Although uncommon, infectious keratitis remains the most serious treatment-related complication and requires prompt intervention.[9]
Psychosocial and Functional Complications
Uncorrected or inadequately corrected myopia may adversely affect academic performance, educational participation, sports activities, self-esteem, and quality of life. Children with significant visual impairment from pathological myopia may require low-vision rehabilitation, educational accommodations, and psychosocial support.[9]
Table 21. Complications of Childhood Myopia
|
Complication category |
Examples |
|
Peripheral retinal complications |
Lattice degeneration, retinal tears, retinal holes, retinal detachment |
|
Macular complications |
Myopic traction maculopathy, foveoschisis, macular hole |
|
Choroidal complications |
Choroidal neovascularization, lacquer cracks, chorioretinal atrophy |
|
Scleral complications |
Posterior staphyloma, progressive globe elongation |
|
Optic nerve complications |
Optic disc tilt, peripapillary atrophy, and glaucoma |
|
Vitreous complications |
Premature vitreous degeneration, posterior vitreous detachment |
|
Lens complications |
Cataract, lens subluxation |
|
Contact lens–related complications |
Corneal infiltrates, microbial keratitis, and giant papillary conjunctivitis |
|
Functional complications |
Educational difficulties, reduced quality of life |
Table 22. Risk Factors for Complications
|
Higher risk features |
|
High myopia (≥ −6.00 D) |
|
Axial length > 26 mm |
|
Early-onset myopia |
|
Rapid progression |
|
Pathological fundus changes |
|
Posterior staphyloma |
|
Family history of pathological myopia |
|
Presence of lattice degeneration or retinal tears |
Key Clinical Pearls
- The likelihood of complications correlates more strongly with axial length than refractive error alone.
- Retinal detachment risk remains elevated throughout life in individuals with severe myopia.
- Myopic maculopathy is among the leading causes of irreversible visual loss in pathological myopia.
- Posterior staphyloma is a major predictor of future retinal and macular complications.
- Early myopia-control interventions may reduce the risk of future complications by limiting excessive axial elongation.
- Lifelong ophthalmic surveillance is recommended for patients with high or pathological myopia, even after refractive stability has been achieved.[9]
Postoperative and Rehabilitation Care
Most children with myopia are treated conservatively using spectacles, contact lenses, pharmacologic interventions, or lifestyle modifications and do not require surgical procedures. Consequently, postoperative care is primarily applicable to children undergoing treatment for myopia-related complications such as retinal detachment, myopic macular pathology, cataract, glaucoma, or other associated ocular disorders. Rehabilitation care focuses on optimizing visual function, ensuring adherence to treatment, preventing progression, and monitoring for complications.[6] Following initiation of myopia-control therapy, children should undergo periodic follow-up examinations to assess visual acuity, refractive status, axial length progression, binocular vision, treatment compliance, and adverse effects. Education of both the child and caregivers is critical to ensure long-term adherence, as myopia control often requires years of continuous treatment during active ocular growth.[152]
Children prescribed spectacles should be evaluated for proper frame fit, optical centration, comfort, and compliance. Periodic adjustment or replacement may be necessary due to facial growth, prescription changes, or frame damage. For children using myopia-control spectacle designs, regular assessment helps maintain appropriate lens positioning and treatment efficacy. Please see StatPearls' companion reference, "Contact Lens–Related Complications," for further information.
Contact lens users require ongoing education regarding insertion and removal techniques, lens hygiene, replacement schedules, and recognition of complications. Follow-up visits should include assessment of corneal health, tear film status, lens fit, and compliance. Children and caregivers should be instructed to discontinue lens wear immediately and seek urgent ophthalmic evaluation if symptoms of pain, redness, photophobia, discharge, or reduced vision occur.[166]
Children receiving atropine therapy should be monitored for treatment response, accommodation status, photophobia, allergic reactions, and systemic adverse effects. Counseling regarding appropriate instillation technique, punctal occlusion, medication storage, and sun protection may improve treatment tolerance and compliance. Please see StatPearls' companion reference, "Open Angle Glaucoma," for further information.
In patients treated with orthokeratology, rehabilitation care includes regular corneal topographic evaluation, assessment of lens fit, monitoring for epithelial complications, and reinforcement of hygiene practices. Treatment effectiveness should be assessed using refractive measurements and axial length monitoring. Children undergoing retinal surgical procedures for complications of pathologic myopia require individualized postoperative treatment according to the procedure performed. Follow-up may include retinal examination, optical coherence tomography, visual rehabilitation, amblyopia treatment when indicated, and monitoring for recurrent retinal pathology.[6] Table 23 summarizes the long-term recommendations.
Visual Rehabilitation
Visual rehabilitation aims to maximize functional vision and educational performance. Components include:
- Accurate and updated refractive correction
- Amblyopia treatment when indicated
- Optimization of binocular vision and stereopsis
- Educational accommodations for reduced visual performance
- Low-vision assessment in severe pathological myopia
- Counseling regarding visual ergonomics and environmental modifications
Children with irreversible visual impairment secondary to pathological myopia may benefit from low-vision rehabilitation services, including magnification devices, electronic visual aids, contrast-enhancement techniques, orientation training, and educational support. Please see StatPearls' companion reference, "Lenticonus," for further information.
Table 23. Long-Term Follow-Up Recommendations
|
Clinical situation |
Recommended follow-up |
|
Stable low myopia |
Every 6–12 months |
|
Progressive myopia |
Every 6 months |
|
Active myopia-control therapy |
Every 3–6 months |
|
Orthokeratology |
Every 3–6 months with corneal assessment |
|
High myopia |
Every 6 months with periodic retinal evaluation |
|
Pathological myopia |
Individualized follow-up based on retinal findings |
|
Postretinal surgery |
According to the surgical protocol and retinal status |
Rehabilitation Goals
- Maintain optimal visual acuity
- Slow refractive and axial length progression
- Preserve binocular visual development
- Prevent amblyopia and educational difficulties
- Detect retinal and optic nerve complications early
- Promote lifelong adherence to eye care and monitoring
Clinical Pearl
Successful rehabilitation of childhood myopia extends beyond refractive correction and requires longitudinal monitoring, family education, reinforcement of compliance, and early identification of vision-threatening complications, particularly in children with high or progressive myopia. Please see StatPearls' companion reference, "Lenticonus," for further information.
Consultations
Most children with uncomplicated myopia can be managed by a comprehensive ophthalmologist, pediatric ophthalmologist, or optometrist with expertise in pediatric refractive care and myopia management. However, consultation with other ophthalmic and medical specialists may be necessary in selected cases, particularly when atypical features, rapid progression, high myopia, or systemic associations are present.
Pediatric Ophthalmology
Referral to a pediatric ophthalmologist is appropriate for children with early-onset myopia, high myopia, anisometropia, amblyopia, strabismus, developmental delay, or suspected ocular pathology. Pediatric ophthalmologists also play an important role in evaluating children who are unable to cooperate with standard refractive testing and in treating complex cases requiring interdisciplinary care.[8]
Retina Specialist
Consultation with a vitreoretinal specialist is indicated in children with high or pathological myopia who develop posterior segment complications. Indications include retinal tears, retinal detachment, lattice degeneration requiring treatment, myopic maculopathy, lacquer cracks, myopic choroidal neovascularization, macular hole, retinoschisis, or unexplained visual deterioration. Children with extreme axial elongation may benefit from periodic retinal surveillance.[11]
Cornea and Contact Lens Specialist
Children being considered for orthokeratology, specialty contact lenses, or advanced myopia-control contact lens therapies may benefit from consultation with a cornea or contact lens specialist. Referral is also indicated when corneal ectatic disorders, irregular astigmatism, contact lens intolerance, recurrent keratitis, or ocular surface disease are suspected.[17]
Glaucoma Specialist
Children with high myopia may exhibit optic disc changes that complicate glaucoma assessment. Consultation with a glaucoma specialist may be required when elevated intraocular pressure, progressive optic nerve changes, suspicious visual field findings, or juvenile open-angle glaucoma are suspected. Please see StatPearls' companion reference, "Myopia," for further information.
Medical Genetics
Genetic consultation should be considered in children with early-onset high myopia, a strong family history of inherited ocular disease, or associated systemic abnormalities. Genetic evaluation may identify conditions such as:
- Marfan syndrome
- Stickler syndrome
- Knobloch syndrome
- Weill-Marchesani syndrome
- Wagner syndrome
- Ehlers-Danlos syndrome
- Congenital stationary night blindness
- Inherited retinal dystrophies
Recognition of these disorders may have important implications for systemic surveillance, family counseling, and long-term prognosis.[29]
Pediatrician or Developmental Specialist
Children with developmental delay, neurologic abnormalities, prematurity, low birth weight, syndromic features, or systemic disease may require evaluation by a pediatrician or developmental specialist. Collaboration may help identify underlying conditions contributing to abnormal ocular growth or visual dysfunction.[167]
Neurology and Neuro-Ophthalmology
Referral is warranted when visual symptoms are disproportionate to the degree of refractive error or when neurologic signs are present. Indications include:
- Unexplained visual loss
- Nystagmus
- Optic nerve abnormalities
- Visual field defects
- Headache with neurologic symptoms
- Suspected cerebral visual impairment
- Developmental visual disorders [134]
Low Vision Rehabilitation Specialist
Children with pathological myopia and irreversible visual impairment may benefit from referral for low-vision services. These specialists can provide optical and electronic visual aids, educational accommodations, orientation training, and functional vision rehabilitation.[168]
Educational and School-Based Services
Collaboration with teachers, school nurses, and educational support personnel may be beneficial for children experiencing academic difficulties related to uncorrected refractive error or visual impairment. Classroom accommodations may include preferential seating, enlarged educational materials, and assistive technologies when necessary.[169] Table 24 summarizes the necessary consultations.
Table 24. Consultation Summary Table
|
Specialist |
Primary indications |
|
Pediatric ophthalmologist |
Early-onset myopia, amblyopia, strabismus, high myopia |
|
Retina specialist |
Retinal tears, detachment, myopic maculopathy, CNV |
|
Cornea/contact lens specialist |
Orthokeratology, specialty lenses, and corneal abnormalities |
|
Glaucoma specialist |
Elevated intraocular pressure, suspicious optic nerve findings |
|
Medical geneticist |
Syndromic or inherited high myopia |
|
Pediatrician |
Systemic disease, developmental concerns |
|
Neurologist/neuro-ophthalmologist |
Nystagmus, neurologic symptoms, unexplained vision loss |
|
Low vision specialist |
Irreversible visual impairment |
|
Educational services |
School-related visual difficulties |
Abbreviation: CNV, choroidal neovascularization.
Key Clinical Pearl
Children with early-onset high myopia, rapid progression, pathological fundus changes, or associated systemic abnormalities should undergo timely interdisciplinary evaluation, as these features often indicate a higher risk of ocular complications or underlying genetic disease requiring specialized treatment.[10]
Deterrence and Patient Education
Many factors can contribute to the etiopathogenesis of myopia. Prolonged screen time and indoor confinement are often blamed for the development and progression of myopia. Promoting outdoor activities, using atropine 0.01% once daily in both eyes at night, and wearing contact lenses can help prevent the progression of myopia.[45]
Parents should clearly understand the need for glasses and the risk of myopia progression. A complete eye examination and refraction should be performed regularly. Often, myopia in children goes unnoticed because children cannot explain their visual concerns clearly and are usually incidentally diagnosed during a routine evaluation. School eye screening programs should be promoted with better spectacle coverage, especially in resource-limited countries. Please see StatPearls' companion reference, "Low Vision Aids," for further information.
Childhood myopia should be viewed as a chronic ocular condition requiring long-term monitoring rather than a simple refractive error corrected solely with spectacles. Parents and caregivers should be educated that the primary goal of modern myopia management is not only to improve vision but also to reduce excessive axial elongation and the future risk of pathological myopia, retinal detachment, myopic maculopathy, glaucoma, and other sight-threatening complications.[11] Families should be informed that an earlier onset of myopia is associated with a greater likelihood of developing high myopia later in life. Consequently, children with a family history of myopia, particularly those with one or both parents who have myopia, should undergo periodic eye examinations even in the absence of visual complaints. Early detection allows timely implementation of evidence-based myopia-control strategies.[167]
Parents should encourage healthy visual habits during childhood. Near-work activities should be performed at an appropriate working distance, preferably greater than 30 cm, with adequate illumination and regular visual breaks. The 20-20-20 rule may be recommended, whereby children look at an object at least 20 feet away for 20 seconds after every 20 minutes of near work. Continuous reading, smartphone use, and prolonged tablet exposure should be minimized whenever possible.[22]
Outdoor activity should be incorporated into the child's daily routine. Current evidence suggests that approximately 2 hours of daily outdoor exposure may reduce the risk of incident myopia and help slow progression in susceptible children. Outdoor activities should complement, rather than replace, other evidence-based treatment modalities. Please see StatPearls' companion reference, "Myopia," for further information.
Children receiving atropine, specialty spectacle lenses, contact lenses, or orthokeratology require counseling regarding treatment adherence. Parents should understand that benefits are generally cumulative and may not be immediately apparent. Poor adherence is a common reason for suboptimal treatment response. Regular follow-up visits should be emphasized to monitor refractive progression, axial length changes, treatment efficacy, and potential adverse effects.[16]
Children wearing contact lenses should receive age-appropriate education on hand hygiene, lens care, avoiding water exposure, proper replacement schedules, and recognizing warning signs. Immediate ophthalmic evaluation is warranted if ocular pain, redness, photophobia, discharge, or sudden visual decline develops.[20] Schools can play an important role in myopia prevention by promoting outdoor recess, ensuring adequate classroom lighting, encouraging periodic visual breaks during prolonged educational activities, and facilitating school-based vision screening programs. Collaboration among parents, teachers, pediatricians, and eye-care professionals may improve early detection and treatment adherence.[5]
Patient Education Pearls
- Myopia usually progresses during childhood and adolescence.
- Earlier onset often predicts greater progression and a higher risk of high myopia.
- Glasses improve vision but do not necessarily stop myopia progression.
- Ideally, outdoor activity should exceed 10–14 hours per week.
- Limiting prolonged uninterrupted near work may reduce visual stress.
- Regular eye examinations remain necessary even when vision appears satisfactory.
- Treatment success depends heavily on long-term adherence and follow-up.
- Sudden flashes, floaters, curtain-like visual loss, or marked visual deterioration require urgent retinal evaluation.[10]
Pearls and Other Issues
Childhood myopia is increasingly recognized as a chronic ocular growth disorder rather than simply a refractive error. The most important determinant of long-term visual prognosis is not the degree of refractive error alone but the extent of axial elongation and the subsequent risk of pathological myopia. Early identification of children at risk for rapid progression provides the greatest opportunity for effective intervention and reduction of future vision-threatening complications. Please see StatPearls' companion reference, "Myopia," for further information.
The age of onset is one of the strongest predictors of future refractive status. Children who develop myopia before 8 years of age are significantly more likely to develop high myopia during adolescence and adulthood. Consequently, early-onset myopia should prompt closer follow-up, consideration of active myopia-control therapies, and, whenever feasible, monitoring of axial length.[17]
Axial length measurement is increasingly regarded as an essential biomarker for monitoring disease progression. Refractive error alone may underestimate ongoing ocular growth, particularly in children undergoing myopia-control therapy. Serial axial length assessment allows earlier identification of treatment failure and may facilitate individualized management decisions.[16] Cycloplegic refraction remains the gold standard for diagnosing childhood myopia. Failure to use cycloplegia may result in overestimation of myopia due to accommodative spasm or pseudomyopia, potentially leading to inappropriate treatment decisions and unnecessary optical correction.[21][16]
Environmental modification represents an important preventive strategy. Increased outdoor activity appears to be most effective for preventing incident myopia and delaying onset, whereas optical and pharmacologic therapies are more effective for slowing progression after myopia has developed. Combining environmental interventions with evidence-based treatment may provide additive benefits.[16]
Myopia progression frequently accelerates during periods of rapid growth and intense educational activity. Clinicians should anticipate these periods and counsel families on the importance of adherence to prescribed therapy, regular follow-up, and monitoring for progression.[16] Children with high myopia require lifelong ophthalmic surveillance because the risk of retinal detachment, myopic maculopathy, glaucoma, cataract, and choroidal neovascularization remains elevated even after refractive stability is achieved. The long-term burden of pathological myopia may extend decades beyond the active progression phase.[16]
Clinical Pearls
- Earlier onset of myopia generally predicts a greater risk of developing high myopia.
- Axial length is often a more sensitive indicator of progression than refractive error alone.
- Cycloplegic refraction should be performed when evaluating refractive error in children and adolescents.
- Outdoor exposure appears to reduce the risk of incident myopia and may delay disease onset.
- Rapid progression (> 0.50 D/year) warrants consideration of active myopia-control interventions.
- High myopia is associated with increased risks of retinal, choroidal, optic nerve, and scleral complications.
- Myopia-control therapies slow progression but rarely stop progression completely.
- Long-term follow-up is necessary even after refractive stability is reached.
Table 25 summarizes the most common pitfalls of treating myopia.
Table 25. Common Pitfalls
|
Pitfall |
Clinical consequence |
|
Reliance on noncycloplegic refraction |
Overdiagnosis of myopia or pseudomyopia |
|
Delayed diagnosis in asymptomatic children |
Missed opportunity for early intervention |
|
Failure to monitor axial length |
Underestimation of disease progression |
|
Assuming spectacles alone control progression |
Continued axial elongation despite visual correction |
|
Poor treatment adherence |
Reduced the effectiveness of myopia-control strategies |
|
Inadequate retinal examination in high myopia |
Delayed recognition of sight-threatening complications |
|
Discontinuation of therapy without monitoring |
Missed rebound progression |
|
Failure to investigate syndromic features |
Delayed diagnosis of underlying genetic disorders |
Prevention
Primary prevention strategies focus on increasing outdoor activity, reducing prolonged uninterrupted near work, promoting appropriate visual ergonomics, encouraging regular visual breaks, and implementing school-based vision screening programs. Children with a strong family history of myopia should undergo periodic eye examinations because they represent a higher-risk population for early onset and progression. Secondary prevention involves early detection, prompt optical correction, risk stratification, and timely initiation of evidence-based myopia-control therapies. Monitoring progression through cycloplegic refraction and axial length assessment may reduce the likelihood of progression to high myopia.[16]
Disposition
Most children with uncomplicated myopia can be treated in the outpatient setting with periodic follow-up. Children with rapid progression, high myopia, suspected syndromic associations, retinal pathology, glaucoma, or unexplained visual loss should be referred to the appropriate ophthalmic subspecialist. Long-term surveillance is particularly important for children who develop high myopia because the risk of ocular complications persists throughout life.[16]
Future Directions
Emerging areas of research include artificial intelligence–based prediction models, personalized risk stratification, combination myopia-control therapies, novel pharmacologic agents, scleral biomechanical modulation, retinal signaling pathways, gene-environment interactions, and advanced optical designs. These approaches may further improve the ability to prevent excessive axial elongation and reduce the global burden of pathological myopia.[16]
Enhancing Healthcare Team Outcomes
Myopia has emerged as a public health concern. Preventing, treating, and slowing the progression of myopia has always been a matter of concern. In recent years, pharmaceutical treatment of myopia has been widely studied. Atropine in Myopia 1 (ATOM-1) was a large randomized controlled trial performed to evaluate the role of atropine 1% in preventing the progression of childhood myopia.[170] A total of 400 children aged 6 to 12 years with myopia ranging from -1 to -6 D were included in the study. The patients were randomly assigned to receive either atropine or placebo. After 2 years, myopia in atropine-treated eyes regressed by 0.30 ± 0.50 D; in the placebo group, progression was noted (-0.76 ± 0.44 D).[87] Although the study provided strong evidence that atropine is a practical option for preventing myopia progression, numerous adverse effects, including blurred near vision, photophobia, glare, and systemic effects, were noted with atropine 1%. These adverse effects further led to investigation of the efficacy of low-dose atropine 0.5%, 0.1%, and 0.01% in controlling myopia progression in the Atropine in Myopia Study 2 (ATOM-2).[88] Atropine 0.01% was found to be a safe and effective option because it caused minimal pupillary dilation and minimal effect on accommodation, with similar efficacy. However, results from a recent study on the effects of low-concentration atropine on myopia progression found that 0.05% atropine was twice as effective as 0.01% over 2 years.[171]
CooperVision MiSight daily use soft lenses were recently approved by the FDA. These lenses are designed to reduce myopia progression by decreasing peripheral retinal hyperopic defocus.[172] Optometrists are essential in treating these patients through early detection and regular follow-up. Patients with signs of progressive myopia should be educated about modern treatment options to control further progression of refractive errors. Counselors are vital in educating parents or caregivers about lifestyle modifications to help prevent the progression of myopia.[16]
The interprofessional team should coordinate care to optimize patient outcomes when treating childhood myopia and monitoring ocular development (see Table 26). Childhood myopia treatment has evolved from simple refractive correction to a comprehensive disease-modification approach requiring coordinated interprofessional care. Successful outcomes depend on early detection, risk stratification, implementation of evidence-based myopia-control strategies, longitudinal monitoring, patient education, and effective communication among healthcare professionals, families, schools, and community health systems.[16]
Primary care clinicians and pediatricians often serve as the first point of contact for children's health care. These clinicians play an important role in recognizing risk factors such as parental myopia, excessive screen exposure, reduced outdoor activity, premature birth, developmental disorders, and visual concerns. Timely referral for a comprehensive ophthalmic evaluation can facilitate earlier diagnosis and intervention during periods of active ocular growth.[16]
Pediatric ophthalmologists, comprehensive ophthalmologists, and optometrists are central to diagnosis, treatment selection, and long-term monitoring. These clinicians should collaborate to establish individualized treatment plans based on refractive error, axial length progression, age of onset, treatment response, and risk of high myopia. Consistent documentation of visual acuity, cycloplegic refraction, ocular biometry, treatment adherence, and adverse effects enhances continuity of care and facilitates evidence-based decision-making.[16] Nursing professionals contribute significantly through patient education, medication counseling, assessment of treatment adherence, reinforcement of follow-up schedules, and identification of potential adverse effects. Nurses can also assist with school-based screening programs, community outreach initiatives, and public health campaigns to raise awareness of childhood myopia and preventive eye care.[16]
Pharmacists play an increasingly important role because low-dose atropine therapy becomes more widely used. Pharmacists should verify medication concentrations, counsel caregivers regarding administration techniques, discuss potential adverse effects, reinforce medication adherence, monitor for drug-related complications, and help prevent accidental ingestion or misuse. In regions where compounded atropine formulations are used, communication between prescribing clinicians and pharmacists is essential to ensure consistency, quality control, and patient safety.[16]
Contact lens specialists, orthokeratology practitioners, and corneal specialists contribute expertise in patient selection, fitting, hygiene education, complication management, and monitoring treatment efficacy. Standardized communication regarding lens wear adherence, corneal health, and adverse events improves safety and treatment success. School personnel, including teachers, school nurses, and educational counselors, can support early recognition of visual difficulties and encourage adherence with prescribed optical correction. Classroom interventions such as appropriate seating arrangements, adequate lighting, regular visual breaks, and promoting outdoor activities may improve visual performance and support myopia-prevention initiatives.[16]
Public health professionals and policymakers play a critical role in implementing population-based strategies to reduce the burden of childhood myopia. School vision screening programs, community awareness campaigns, improved access to refractive services, and policies encouraging outdoor activity may help reduce the incidence and progression of myopia at the population level. Children with syndromic, genetic, neurologic, or developmental conditions associated with high myopia may require interdisciplinary collaboration involving geneticists, neurologists, developmental pediatricians, low-vision specialists, occupational therapists, and rehabilitation professionals. Early identification of associated systemic disorders may improve both ocular and overall health outcomes.[16]
Table 26. Interprofessional Care Coordination Strategies
|
Team member |
Key responsibilities |
|
Pediatrician or primary care clinicians |
Risk-factor identification, screening, referral |
|
Pediatric ophthalmologist/ophthalmologist |
Diagnosis, treatment planning, and complication management |
|
Optometrist |
Refractive assessment, myopia-control monitoring, follow-up |
|
Nurse |
Education, adherence counseling, and follow-up coordination |
|
Pharmacist |
Atropine counseling, medication safety, and adverse effect monitoring |
|
Cornea/contact lens specialist |
Orthokeratology and contact lens management |
|
Retina specialist |
Management of pathological myopia complications |
|
Geneticist |
Evaluation of inherited or syndromic myopia |
|
School health personnel |
Vision screening and educational support |
|
Public health professionals |
Community prevention programs and policy development |
|
Low vision specialist |
Rehabilitation for irreversible visual impairment |
Patient Safety and Quality Improvement Considerations
- Establish standardized protocols for cycloplegic refraction and axial length monitoring.
- Maintain accurate longitudinal documentation of refractive progression.
- Educate families regarding treatment expectations, adherence, and warning symptoms.
- Implement systems to minimize loss to follow-up during periods of rapid progression.
- Promote evidence-based prescribing practices for atropine and optical interventions.
- Monitor contact lens users for infectious and inflammatory complications.
- Encourage integration of school-based screening and referral pathways.
- Use shared decision-making to align treatment plans with the patient's and family's preferences.[16]
Ethical and Communication Considerations
Healthcare professionals should engage families in shared decision-making by discussing the benefits, limitations, costs, and potential adverse effects of available myopia-control interventions. Counseling should be culturally sensitive, age-appropriate, and tailored to health literacy levels. Clear communication among all members of the healthcare team promotes adherence, minimizes conflicting recommendations, and enhances patient-centered care.[16]
Key Interprofessional Pearl
The most effective strategy for reducing the long-term burden of childhood myopia is early identification, coordinated interprofessional management, evidence-based intervention, and continuous communication among eye-care providers, primary care clinicians, pharmacists, nurses, educators, and families, with the shared goal of preventing excessive axial elongation and future vision-threatening complications.[16]
Media
(Click Image to Enlarge)
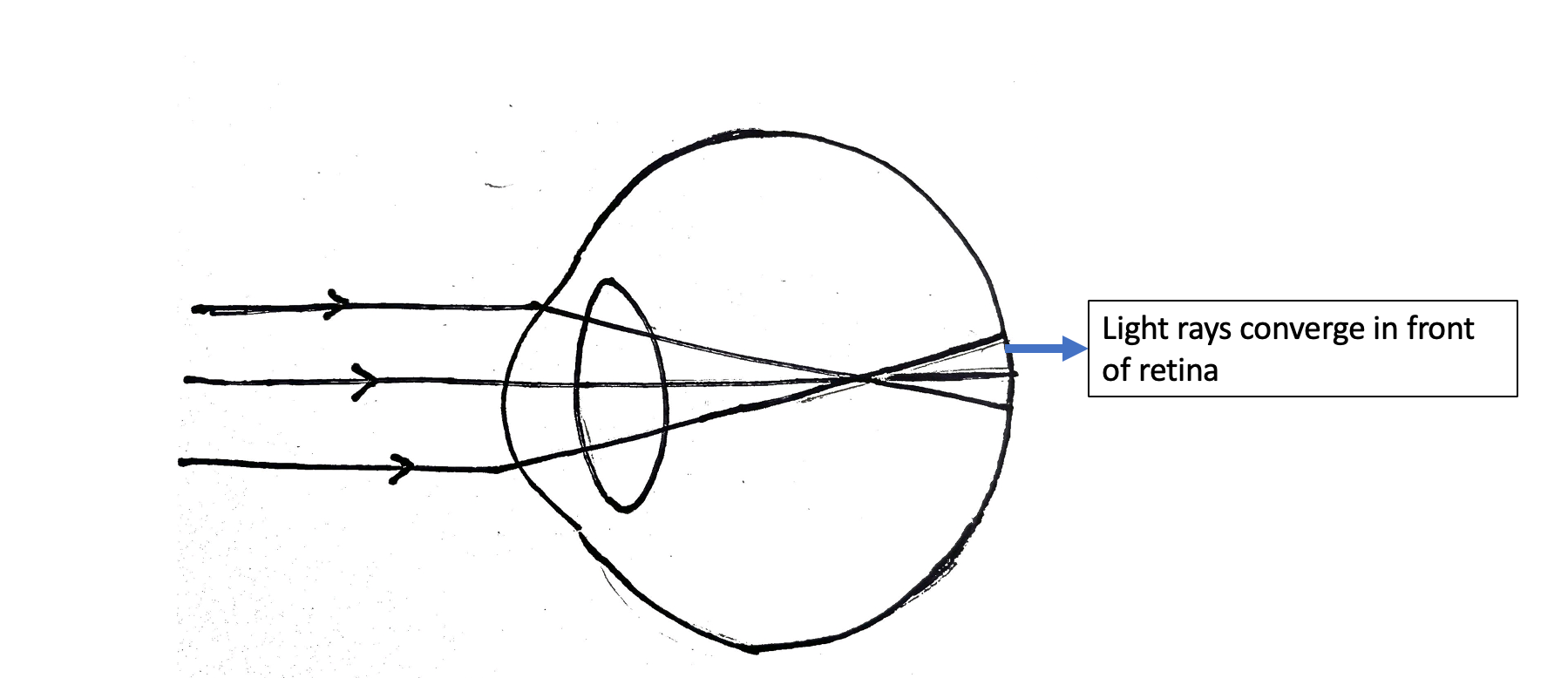
Myopia. A ray diagram demonstrating parallel rays focused in front of the retina, resulting in myopia.
Contributed by G Saluja, MBBS, MD, DNB
References
Holden BA, Wilson DA, Jong M, Sankaridurg P, Fricke TR, Smith EL III, Resnikoff S. Myopia: a growing global problem with sight-threatening complications. Community eye health. 2015:28(90):35 [PubMed PMID: 26692649]
Morgan IG, Ohno-Matsui K, Saw SM. Myopia. Lancet (London, England). 2012 May 5:379(9827):1739-48. doi: 10.1016/S0140-6736(12)60272-4. Epub [PubMed PMID: 22559900]
Kolb H, Fernandez E, Jones B, Nelson R, Carr BJ, Stell WK. The Science Behind Myopia. Webvision: The Organization of the Retina and Visual System. 1995:(): [PubMed PMID: 29266913]
Saw SM, Gazzard G, Shih-Yen EC, Chua WH. Myopia and associated pathological complications. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 2005 Sep:25(5):381-91 [PubMed PMID: 16101943]
Chen L, Sun L, Liu J, Chen Y, Li J, Lin D, Chen X, Leung HY, Zhang J, Lam DSC. Age Modifies the Comparative Effectiveness of DIMS Versus HAL Spectacle Lenses for Myopia Control: A Real-World Study. Translational vision science & technology. 2026 Jun 1:15(6):10. doi: 10.1167/tvst.15.6.10. Epub [PubMed PMID: 42240274]
Level 2 (mid-level) evidenceWu F, Tham YC, Htoon HM, Grzybowski A, Loke WT, Guggenheim JA, Morgan I, Sabanayagam C, Saw SM. Pattern of association between school grades and myopia: longitudinal findings from the SCORM cohort. Eye (London, England). 2026 May 23:():. doi: 10.1038/s41433-026-04551-9. Epub 2026 May 23 [PubMed PMID: 42177337]
Chen G, Zhang Y, Zhang Y, Zhou Y. Gut microbiota and pediatric eye diseases: current insights, mechanistic underpinnings, and future outlook. Frontiers in nutrition. 2026:13():1810321. doi: 10.3389/fnut.2026.1810321. Epub 2026 Apr 28 [PubMed PMID: 42131242]
Borella Y, Constant A, Rothschild PR, Robert MP, Burin Des Roziers C, Valleix S, Brezin AP, Bremond Gignac D, Daruich A. Sex-based differences in retinal detachment in a genotyped Stickler syndrome cohort: implications for preventive management. The British journal of ophthalmology. 2026 May 4:():. pii: bjo-2025-328779. doi: 10.1136/bjo-2025-328779. Epub 2026 May 4 [PubMed PMID: 42082323]
Zhang S, Zhao Q. Revolutionizing Pediatric Myopia Care: A Machine Learning Approach for Rapid and Accurate Pre-Clinical Screening. Journal of clinical medicine. 2026 Apr 8:15(8):. doi: 10.3390/jcm15082834. Epub 2026 Apr 8 [PubMed PMID: 42074637]
Peng T, Zhang L, Xu W, Wang M, Wang N, Atchison DA, Li SM. Nasotemporal Asymmetry in Ocular Biometry as a Biomarker for Myopia Progression in Chinese Children. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians (Optometrists). 2026 Apr 15:():. doi: 10.1007/s44402-026-00082-8. Epub 2026 Apr 15 [PubMed PMID: 41986789]
Pan M, Zhou W, Qu HQ, Xiu Z, Sun R, Hakonarson H, Li J, Shi X. Convergent genetic pathways linking neuropsychiatric and ocular disorders in children. Journal of child psychology and psychiatry, and allied disciplines. 2026 Apr 7:():. doi: 10.1111/jcpp.70151. Epub 2026 Apr 7 [PubMed PMID: 41947537]
Atchison DA, Jones CE, Schmid KL, Pritchard N, Pope JM, Strugnell WE, Riley RA. Eye shape in emmetropia and myopia. Investigative ophthalmology & visual science. 2004 Oct:45(10):3380-6 [PubMed PMID: 15452039]
Majumdar S, Tripathy K. Hyperopia. StatPearls. 2026 Jan:(): [PubMed PMID: 32809551]
Mazumdar S, Tripathy K, Sarma B, Agarwal N. Acquired myopia followed by acquired hyperopia due to serous neurosensory retinal detachment following topiramate intake. European journal of ophthalmology. 2019 Jan:29(1):NP21-NP24. doi: 10.1177/1120672118797286. Epub 2018 Sep 3 [PubMed PMID: 30175623]
Ghorbani-Mojarrad N, Han X, Dbayat N, Ding X. What do we know about premyopia and should we be giving it greater consideration? BMJ open ophthalmology. 2025 Mar 23:10(1):. doi: 10.1136/bmjophth-2024-002059. Epub 2025 Mar 23 [PubMed PMID: 40122571]
Wu B, Zeng W, Tang K, Xiong J, Mo X, Fu Q, Fu D, Chu R, Zhao G, Lu L, Wang Z, Wu L, Yu Z, Zhou X, Wang H. Increased PRSS56 expression is a causal factor and therapeutic target for human axial high myopia. Cell research. 2026 Apr 1:():. doi: 10.1038/s41422-026-01241-9. Epub 2026 Apr 1 [PubMed PMID: 41917313]
Alrasheed SH, Alhoshan SA, Alnasser BN. Refractive error, amblyopia and ocular alignment among schoolchildren in Saudi Arabia. Eastern Mediterranean health journal = La revue de sante de la Mediterranee orientale = al-Majallah al-sihhiyah li-sharq al-mutawassit. 2026 Mar 5:32(3):149-155. doi: 10.26719/2026.32.3.149. Epub 2026 Mar 5 [PubMed PMID: 41910009]
Flitcroft DI, Lingham G, Ying GS, Cui H, Mackey DA, Jonas JB, Bikbov MM, Harrington S, Saunders KJ, Loughman J. Refractive Error Centile Curves for Asian and Western Children and Adolescents: An Individual Level Meta-Analysis. Investigative ophthalmology & visual science. 2025 Dec 1:66(15):30. doi: 10.1167/iovs.66.15.30. Epub [PubMed PMID: 41363895]
Level 1 (high-level) evidenceAlagsam AA, Al-Ghamdi HA, Alradaddi RM, Khormi LM, Alfuhigi FT, Alhazmi MA, Alshutayli HD, Alqahtani YM, Althobaiti GA, Masmali MI, Rufidi MM. Efficacy of Contact Lens-Based Interventions in Slowing Myopia Progression in Children: A Systematic Review. Cureus. 2025 Oct:17(10):e94217. doi: 10.7759/cureus.94217. Epub 2025 Oct 9 [PubMed PMID: 41209854]
Level 1 (high-level) evidenceXu L, Zhang Y, Yang C, Lan J, Li Z, Luo J, Guo Y, Hou X, Tian Z, Zeng J. Age-dependent and reversible refractive changes in 0-6 years old children associated with reduced outdoor activity: a six-year community-based study. Scientific reports. 2026 Jan 19:16(1):5719. doi: 10.1038/s41598-026-36515-0. Epub 2026 Jan 19 [PubMed PMID: 41554829]
Xu H, Pu J, Bian S, Mi X, Zhou Z, Chen W, Jiao Y. Factors Influencing the Transition From Physiological Hyperopia to Myopia in Children: Protocol for a Prospective Nested Case-Control Study. JMIR research protocols. 2026 Mar 24:15():e84888. doi: 10.2196/84888. Epub 2026 Mar 24 [PubMed PMID: 41875210]
Level 2 (mid-level) evidenceKang MT, Hu Y, Wang N, Fu J, Zhou A, Liu Y, Meng H, Li X, Wang S, Chen X, Zhao H, Hu G, Wang W, Dai Y, Nathan A, Smielewski P, Gao S, Li SM. Deep Learning Prediction of Childhood Myopia Progression Using Fundus Image and Refraction Data. JAMA network open. 2026 Jan 2:9(1):e2553543. doi: 10.1001/jamanetworkopen.2025.53543. Epub 2026 Jan 2 [PubMed PMID: 41587032]
Wang J, Li Y, Musch DC, Wei N, Qi X, Ding G, Li X, Li J, Song L, Zhang Y, Ning Y, Zeng X, Hua N, Li S, Qian X. Progression of Myopia in School-Aged Children After COVID-19 Home Confinement. JAMA ophthalmology. 2021 Mar 1:139(3):293-300. doi: 10.1001/jamaophthalmol.2020.6239. Epub [PubMed PMID: 33443542]
Level 2 (mid-level) evidenceSaw SM, Carkeet A, Chia KS, Stone RA, Tan DT. Component dependent risk factors for ocular parameters in Singapore Chinese children. Ophthalmology. 2002 Nov:109(11):2065-71 [PubMed PMID: 12414416]
Level 2 (mid-level) evidenceHe M, Zeng J, Liu Y, Xu J, Pokharel GP, Ellwein LB. Refractive error and visual impairment in urban children in southern china. Investigative ophthalmology & visual science. 2004 Mar:45(3):793-9 [PubMed PMID: 14985292]
Level 3 (low-level) evidenceWilliams KM, Bertelsen G, Cumberland P, Wolfram C, Verhoeven VJ, Anastasopoulos E, Buitendijk GH, Cougnard-Grégoire A, Creuzot-Garcher C, Erke MG, Hogg R, Höhn R, Hysi P, Khawaja AP, Korobelnik JF, Ried J, Vingerling JR, Bron A, Dartigues JF, Fletcher A, Hofman A, Kuijpers RW, Luben RN, Oxele K, Topouzis F, von Hanno T, Mirshahi A, Foster PJ, van Duijn CM, Pfeiffer N, Delcourt C, Klaver CC, Rahi J, Hammond CJ, European Eye Epidemiology (E(3)) Consortium. Increasing Prevalence of Myopia in Europe and the Impact of Education. Ophthalmology. 2015 Jul:122(7):1489-97. doi: 10.1016/j.ophtha.2015.03.018. Epub 2015 May 13 [PubMed PMID: 25983215]
Wu PC, Huang HM, Yu HJ, Fang PC, Chen CT. Epidemiology of Myopia. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2016 Nov/Dec:5(6):386-393 [PubMed PMID: 27898441]
Agarwal D, Saxena R, Gupta V, Mani K, Dhiman R, Bhardawaj A, Vashist P. Prevalence of myopia in Indian school children: Meta-analysis of last four decades. PloS one. 2020:15(10):e0240750. doi: 10.1371/journal.pone.0240750. Epub 2020 Oct 19 [PubMed PMID: 33075102]
Level 1 (high-level) evidenceClark RA, Wong RK. Spherical Equivalent Refraction Versus Axial Length for Monitoring Childhood Myopia and Estimating Disease Risk: A Systematic Review and Meta-Analysis. American journal of ophthalmology. 2026 Jun:286():235-247. doi: 10.1016/j.ajo.2026.03.007. Epub 2026 Mar 11 [PubMed PMID: 41825844]
Level 1 (high-level) evidenceRamamurthy D, Lin Chua SY, Saw SM. A review of environmental risk factors for myopia during early life, childhood and adolescence. Clinical & experimental optometry. 2015 Nov:98(6):497-506. doi: 10.1111/cxo.12346. Epub 2015 Oct 25 [PubMed PMID: 26497977]
Liang CL, Yen E, Su JY, Liu C, Chang TY, Park N, Wu MJ, Lee S, Flynn JT, Juo SH. Impact of family history of high myopia on level and onset of myopia. Investigative ophthalmology & visual science. 2004 Oct:45(10):3446-52 [PubMed PMID: 15452048]
Level 2 (mid-level) evidenceMEHRA KS, KHARE BB, VAITHILINGAM E. REFRACTION IN FULL-TERM BABIES. The British journal of ophthalmology. 1965 May:49(5):276-7 [PubMed PMID: 14290875]
Flitcroft DI. Emmetropisation and the aetiology of refractive errors. Eye (London, England). 2014 Feb:28(2):169-79. doi: 10.1038/eye.2013.276. Epub 2014 Jan 10 [PubMed PMID: 24406411]
Bhardwaj V, Rajeshbhai GP. Axial length, anterior chamber depth-a study in different age groups and refractive errors. Journal of clinical and diagnostic research : JCDR. 2013 Oct:7(10):2211-2. doi: 10.7860/JCDR/2013/7015.3473. Epub 2013 Oct 5 [PubMed PMID: 24298478]
Meng W, Butterworth J, Malecaze F, Calvas P. Axial length of myopia: a review of current research. Ophthalmologica. Journal international d'ophtalmologie. International journal of ophthalmology. Zeitschrift fur Augenheilkunde. 2011:225(3):127-34. doi: 10.1159/000317072. Epub 2010 Oct 16 [PubMed PMID: 20948239]
Level 3 (low-level) evidenceCoudrillier B, Pijanka J, Jefferys J, Sorensen T, Quigley HA, Boote C, Nguyen TD. Collagen structure and mechanical properties of the human sclera: analysis for the effects of age. Journal of biomechanical engineering. 2015 Apr:137(4):041006. doi: 10.1115/1.4029430. Epub 2015 Feb 11 [PubMed PMID: 25531905]
Rada JA, Achen VR, Penugonda S, Schmidt RW, Mount BA. Proteoglycan composition in the human sclera during growth and aging. Investigative ophthalmology & visual science. 2000 Jun:41(7):1639-48 [PubMed PMID: 10845580]
Rada JA, Shelton S, Norton TT. The sclera and myopia. Experimental eye research. 2006 Feb:82(2):185-200 [PubMed PMID: 16202407]
Level 3 (low-level) evidenceHoar RM. Embryology of the eye. Environmental health perspectives. 1982 Apr:44():31-4 [PubMed PMID: 7084153]
Level 3 (low-level) evidenceZadnik K, Satariano WA, Mutti DO, Sholtz RI, Adams AJ. The effect of parental history of myopia on children's eye size. JAMA. 1994 May 4:271(17):1323-7 [PubMed PMID: 8158816]
Level 2 (mid-level) evidenceMcBrien NA, Gentle A. Role of the sclera in the development and pathological complications of myopia. Progress in retinal and eye research. 2003 May:22(3):307-38 [PubMed PMID: 12852489]
Level 3 (low-level) evidenceCuthbertson RA, Beck F, Senior PV, Haralambidis J, Penschow JD, Coghlan JP. Insulin-like growth factor II may play a local role in the regulation of ocular size. Development (Cambridge, England). 1989 Sep:107(1):123-30 [PubMed PMID: 2560708]
Level 3 (low-level) evidenceSummers JA. The choroid as a sclera growth regulator. Experimental eye research. 2013 Sep:114():120-7. doi: 10.1016/j.exer.2013.03.008. Epub 2013 Mar 23 [PubMed PMID: 23528534]
Level 3 (low-level) evidenceTroilo D, Smith EL 3rd, Nickla DL, Ashby R, Tkatchenko AV, Ostrin LA, Gawne TJ, Pardue MT, Summers JA, Kee CS, Schroedl F, Wahl S, Jones L. IMI - Report on Experimental Models of Emmetropization and Myopia. Investigative ophthalmology & visual science. 2019 Feb 28:60(3):M31-M88. doi: 10.1167/iovs.18-25967. Epub [PubMed PMID: 30817827]
Németh J, Tapasztó B, Aclimandos WA, Kestelyn P, Jonas JB, De Faber JHN, Januleviciene I, Grzybowski A, Nagy ZZ, Pärssinen O, Guggenheim JA, Allen PM, Baraas RC, Saunders KJ, Flitcroft DI, Gray LS, Polling JR, Haarman AE, Tideman JWL, Wolffsohn JS, Wahl S, Mulder JA, Smirnova IY, Formenti M, Radhakrishnan H, Resnikoff S. Update and guidance on management of myopia. European Society of Ophthalmology in cooperation with International Myopia Institute. European journal of ophthalmology. 2021 May:31(3):853-883. doi: 10.1177/1120672121998960. Epub 2021 Mar 5 [PubMed PMID: 33673740]
Harper AR, Summers JA. The dynamic sclera: extracellular matrix remodeling in normal ocular growth and myopia development. Experimental eye research. 2015 Apr:133():100-11. doi: 10.1016/j.exer.2014.07.015. Epub [PubMed PMID: 25819458]
Troilo D, Nickla DL, Mertz JR, Summers Rada JA. Change in the synthesis rates of ocular retinoic acid and scleral glycosaminoglycan during experimentally altered eye growth in marmosets. Investigative ophthalmology & visual science. 2006 May:47(5):1768-77 [PubMed PMID: 16638980]
Level 3 (low-level) evidenceRead SA, Fuss JA, Vincent SJ, Collins MJ, Alonso-Caneiro D. Choroidal changes in human myopia: insights from optical coherence tomography imaging. Clinical & experimental optometry. 2019 May:102(3):270-285. doi: 10.1111/cxo.12862. Epub 2018 Dec 19 [PubMed PMID: 30565333]
O'Rahilly R. The prenatal development of the human eye. Experimental eye research. 1975 Aug:21(2):93-112 [PubMed PMID: 1100417]
Muralidharan G, Martínez-Enríquez E, Birkenfeld J, Velasco-Ocana M, Pérez-Merino P, Marcos S. Morphological changes of human crystalline lens in myopia. Biomedical optics express. 2019 Dec 1:10(12):6084-6095. doi: 10.1364/BOE.10.006084. Epub 2019 Nov 5 [PubMed PMID: 31853387]
Mutti DO, Zadnik K, Fusaro RE, Friedman NE, Sholtz RI, Adams AJ. Optical and structural development of the crystalline lens in childhood. Investigative ophthalmology & visual science. 1998 Jan:39(1):120-33 [PubMed PMID: 9430553]
Augusteyn RC. On the growth and internal structure of the human lens. Experimental eye research. 2010 Jun:90(6):643-54. doi: 10.1016/j.exer.2010.01.013. Epub 2010 Feb 18 [PubMed PMID: 20171212]
Gordon RA, Donzis PB. Refractive development of the human eye. Archives of ophthalmology (Chicago, Ill. : 1960). 1985 Jun:103(6):785-9 [PubMed PMID: 4004614]
Jiang X, Tarczy-Hornoch K, Cotter SA, Matsumura S, Mitchell P, Rose KA, Katz J, Saw SM, Varma R, POPEYE Consortium. Association of Parental Myopia With Higher Risk of Myopia Among Multiethnic Children Before School Age. JAMA ophthalmology. 2020 May 1:138(5):501-509. doi: 10.1001/jamaophthalmol.2020.0412. Epub [PubMed PMID: 32191277]
Lee YY, Lo CT, Sheu SJ, Yin LT. Risk factors for and progression of myopia in young Taiwanese men. Ophthalmic epidemiology. 2015 Feb:22(1):66-73. doi: 10.3109/09286586.2014.988874. Epub 2014 Dec 11 [PubMed PMID: 25495661]
O'Connor AR, Stephenson TJ, Johnson A, Tobin MJ, Ratib S, Fielder AR. Change of refractive state and eye size in children of birth weight less than 1701 g. The British journal of ophthalmology. 2006 Apr:90(4):456-60 [PubMed PMID: 16547327]
Mandel Y, Grotto I, El-Yaniv R, Belkin M, Israeli E, Polat U, Bartov E. Season of birth, natural light, and myopia. Ophthalmology. 2008 Apr:115(4):686-92 [PubMed PMID: 17698195]
Level 2 (mid-level) evidenceGwiazda JE, Hyman L, Norton TT, Hussein ME, Marsh-Tootle W, Manny R, Wang Y, Everett D, COMET Grouup. Accommodation and related risk factors associated with myopia progression and their interaction with treatment in COMET children. Investigative ophthalmology & visual science. 2004 Jul:45(7):2143-51 [PubMed PMID: 15223788]
Level 1 (high-level) evidenceBerntsen DA, Sinnott LT, Mutti DO, Zadnik K, CLEERE Study Group. Accommodative lag and juvenile-onset myopia progression in children wearing refractive correction. Vision research. 2011 May 11:51(9):1039-46. doi: 10.1016/j.visres.2011.02.016. Epub 2011 Feb 20 [PubMed PMID: 21342658]
Rosner M, Belkin M. Intelligence, education, and myopia in males. Archives of ophthalmology (Chicago, Ill. : 1960). 1987 Nov:105(11):1508-11 [PubMed PMID: 3675282]
Mirshahi A, Ponto KA, Hoehn R, Zwiener I, Zeller T, Lackner K, Beutel ME, Pfeiffer N. Myopia and level of education: results from the Gutenberg Health Study. Ophthalmology. 2014 Oct:121(10):2047-52. doi: 10.1016/j.ophtha.2014.04.017. Epub 2014 Jun 16 [PubMed PMID: 24947658]
Level 2 (mid-level) evidenceFlitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Progress in retinal and eye research. 2012 Nov:31(6):622-60. doi: 10.1016/j.preteyeres.2012.06.004. Epub 2012 Jul 4 [PubMed PMID: 22772022]
Torii H, Ohnuma K, Kurihara T, Tsubota K, Negishi K. Violet Light Transmission is Related to Myopia Progression in Adult High Myopia. Scientific reports. 2017 Nov 6:7(1):14523. doi: 10.1038/s41598-017-09388-7. Epub 2017 Nov 6 [PubMed PMID: 29109514]
Rose KA, Morgan IG, Ip J, Kifley A, Huynh S, Smith W, Mitchell P. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008 Aug:115(8):1279-85. doi: 10.1016/j.ophtha.2007.12.019. Epub 2008 Feb 21 [PubMed PMID: 18294691]
Level 2 (mid-level) evidenceFlitcroft DI, Harb EN, Wildsoet CF. The Spatial Frequency Content of Urban and Indoor Environments as a Potential Risk Factor for Myopia Development. Investigative ophthalmology & visual science. 2020 Sep 1:61(11):42. doi: 10.1167/iovs.61.11.42. Epub [PubMed PMID: 32986814]
McCarthy CS, Megaw P, Devadas M, Morgan IG. Dopaminergic agents affect the ability of brief periods of normal vision to prevent form-deprivation myopia. Experimental eye research. 2007 Jan:84(1):100-7 [PubMed PMID: 17094962]
Level 3 (low-level) evidenceYang GY, Huang LH, Schmid KL, Li CG, Chen JY, He GH, Liu L, Ruan ZL, Chen WQ. Associations Between Screen Exposure in Early Life and Myopia amongst Chinese Preschoolers. International journal of environmental research and public health. 2020 Feb 7:17(3):. doi: 10.3390/ijerph17031056. Epub 2020 Feb 7 [PubMed PMID: 32046062]
Enthoven CA, Polling JR, Verzijden T, Tideman JWL, Al-Jaffar N, Jansen PW, Raat H, Metz L, Verhoeven VJM, Klaver CCW. Smartphone Use Associated with Refractive Error in Teenagers: The Myopia App Study. Ophthalmology. 2021 Dec:128(12):1681-1688. doi: 10.1016/j.ophtha.2021.06.016. Epub 2021 Jul 8 [PubMed PMID: 34245754]
Jones BE, Thompson EW, Hodos W, Waldbillig RJ, Chader GJ. Scleral matrix metalloproteinases, serine proteinase activity and hydrational capacity are increased in myopia induced by retinal image degradation. Experimental eye research. 1996 Oct:63(4):369-81 [PubMed PMID: 8944544]
Huang W, Duan A, Qi Y. Posterior Scleral Reinforcement to Prevent Progression of High Myopia. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2019 Sep-Oct:8(5):366-370. doi: 10.1097/APO.0000000000000257. Epub [PubMed PMID: 31513040]
Level 2 (mid-level) evidenceWang Y, Zhang Y, Chen H, Zhang XJ, Zhang R, Ng TK, Tham JA, Kam KW, Tam POS, Young AL, Wei Y, Zhang M, Pang CP, Tham CC, Yam JC, Chen LJ. Genome-wide association study identified novel loci and gene-environment interaction for refractive error in children. NPJ genomic medicine. 2025 May 23:10(1):44. doi: 10.1038/s41525-025-00504-5. Epub 2025 May 23 [PubMed PMID: 40410244]
Tang X, Liang J, Luo L, Yuan F, Zhao K, Zhuo X, Li W, Wang J, Zhang S, Zeng K. Investigation of choroidal vascular alterations in eyes with myopia using ultrawidefield optical coherence tomography angiography. BMJ open ophthalmology. 2024 Nov 20:9(1):. doi: 10.1136/bmjophth-2024-001839. Epub 2024 Nov 20 [PubMed PMID: 39567184]
Neelam K, Ng SMS, Ho EL, Au Eong KG. Lacquer cracks in pathological myopia: a clinical review. Eye (London, England). 2024 Oct:38(15):2859-2873. doi: 10.1038/s41433-024-03183-1. Epub 2024 Aug 8 [PubMed PMID: 39117703]
Zhou ZH, Xiong PP, Sun J, Wang YL, Wang JL. Effects of posterior staphyloma on choroidal structure in myopic adults: a retrospective study. BMC ophthalmology. 2023 Oct 9:23(1):406. doi: 10.1186/s12886-023-03158-y. Epub 2023 Oct 9 [PubMed PMID: 37814232]
Level 2 (mid-level) evidenceIto K, Hoerig C, Dan YS, McFadden SA, Mamou J, Hoang QV. Biomechanical changes occur in myopic choroidal stroma and mirror those in the adjacent sclera. Communications engineering. 2024 Oct 9:3(1):139. doi: 10.1038/s44172-024-00280-7. Epub 2024 Oct 9 [PubMed PMID: 39384899]
Kaur K, Gurnani B, Nayak S, Deori N, Kaur S, Jethani J, Singh D, Agarkar S, Hussaindeen JR, Sukhija J, Mishra D. Digital Eye Strain- A Comprehensive Review. Ophthalmology and therapy. 2022 Oct:11(5):1655-1680. doi: 10.1007/s40123-022-00540-9. Epub 2022 Jul 9 [PubMed PMID: 35809192]
Kaur K, Gurnani B. Lenticonus. StatPearls. 2026 Jan:(): [PubMed PMID: 36943989]
Yadav S, Tandon R. Comprehensive eye examination: what does it mean? Community eye health. 2019:32(107):S1-S4 [PubMed PMID: 32123482]
Sanfilippo PG, Chu BS, Bigault O, Kearns LS, Boon MY, Young TL, Hammond CJ, Hewitt AW, Mackey DA. What is the appropriate age cut-off for cycloplegia in refraction? Acta ophthalmologica. 2014 Sep:92(6):e458-62. doi: 10.1111/aos.12388. Epub 2014 Mar 19 [PubMed PMID: 24641244]
Mimouni M, Zoller L, Horowitz J, Wygnanski-Jaffe T, Morad Y, Mezer E. Cycloplegic autorefraction in young adults: is it mandatory? Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2016 Feb:254(2):395-8. doi: 10.1007/s00417-015-3246-1. Epub 2015 Dec 21 [PubMed PMID: 26686513]
Major E, Dutson T, Moshirfar M. Cycloplegia in Children: An Optometrist's Perspective. Clinical optometry. 2020:12():129-133. doi: 10.2147/OPTO.S217645. Epub 2020 Aug 25 [PubMed PMID: 32904515]
Level 3 (low-level) evidenceManny RE, Hussein M, Scheiman M, Kurtz D, Niemann K, Zinzer K, COMET Study Group. Tropicamide (1%): an effective cycloplegic agent for myopic children. Investigative ophthalmology & visual science. 2001 Jul:42(8):1728-35 [PubMed PMID: 11431435]
Level 1 (high-level) evidenceHong D, Tripathy K. Tropicamide. StatPearls. 2026 Jan:(): [PubMed PMID: 31082113]
Ohno-Matsui K. Pathologic Myopia. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2016 Nov/Dec:5(6):415-423 [PubMed PMID: 27898445]
Feng Q, Wu X, Liu Q, Xiao Y, Zhang X, Chen Y. Interpretable machine learning models for predicting childhood myopia from school-based screening data. Scientific reports. 2025 Jun 5:15(1):19811. doi: 10.1038/s41598-025-05021-0. Epub 2025 Jun 5 [PubMed PMID: 40473816]
Walline JJ, Jones LA, Sinnott L, Manny RE, Gaume A, Rah MJ, Chitkara M, Lyons S, ACHIEVE Study Group. A randomized trial of the effect of soft contact lenses on myopia progression in children. Investigative ophthalmology & visual science. 2008 Nov:49(11):4702-6. doi: 10.1167/iovs.08-2067. Epub 2008 Jun 19 [PubMed PMID: 18566461]
Level 2 (mid-level) evidenceChua WH, Balakrishnan V, Chan YH, Tong L, Ling Y, Quah BL, Tan D. Atropine for the treatment of childhood myopia. Ophthalmology. 2006 Dec:113(12):2285-91 [PubMed PMID: 16996612]
Level 1 (high-level) evidenceChia A, Chua WH, Cheung YB, Wong WL, Lingham A, Fong A, Tan D. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology. 2012 Feb:119(2):347-54. doi: 10.1016/j.ophtha.2011.07.031. Epub 2011 Oct 2 [PubMed PMID: 21963266]
Level 1 (high-level) evidenceYam JC, Zhang XJ, Zhang Y, Wang YM, Tang SM, Li FF, Kam KW, Ko ST, Yip BHK, Young AL, Tham CC, Chen LJ, Pang CP. Three-Year Clinical Trial of Low-Concentration Atropine for Myopia Progression (LAMP) Study: Continued Versus Washout: Phase 3 Report. Ophthalmology. 2022 Mar:129(3):308-321. doi: 10.1016/j.ophtha.2021.10.002. Epub 2021 Oct 7 [PubMed PMID: 34627809]
Level 1 (high-level) evidenceSaxena R, Gupta V, Thakur H, Dhiman R, Velpandian T, Phuljhele S, Sharma N. Atropine (0.05%) for rapid progressive childhood myopia (ARM study). Indian journal of ophthalmology. 2025 Mar 1:73(3):358-361. doi: 10.4103/IJO.IJO_1526_24. Epub 2024 Dec 27 [PubMed PMID: 39728597]
Ford KJ, Feller MB. Assembly and disassembly of a retinal cholinergic network. Visual neuroscience. 2012 Jan:29(1):61-71. doi: 10.1017/S0952523811000216. Epub 2011 Jul 26 [PubMed PMID: 21787461]
Level 3 (low-level) evidenceCristaldi M, Olivieri M, Pezzino S, Spampinato G, Lupo G, Anfuso CD, Rusciano D. Atropine Differentially Modulates ECM Production by Ocular Fibroblasts, and Its Ocular Surface Toxicity Is Blunted by Colostrum. Biomedicines. 2020 Apr 5:8(4):. doi: 10.3390/biomedicines8040078. Epub 2020 Apr 5 [PubMed PMID: 32260532]
Barathi VA, Weon SR, Beuerman RW. Expression of muscarinic receptors in human and mouse sclera and their role in the regulation of scleral fibroblasts proliferation. Molecular vision. 2009 Jun 30:15():1277-93 [PubMed PMID: 19578554]
Level 3 (low-level) evidenceSchwahn HN, Kaymak H, Schaeffel F. Effects of atropine on refractive development, dopamine release, and slow retinal potentials in the chick. Visual neuroscience. 2000 Mar-Apr:17(2):165-76 [PubMed PMID: 10824671]
Level 3 (low-level) evidenceChiang ST, Phillips JR. Effect of Atropine Eye Drops on Choroidal Thinning Induced by Hyperopic Retinal Defocus. Journal of ophthalmology. 2018:2018():8528315. doi: 10.1155/2018/8528315. Epub 2018 Jan 14 [PubMed PMID: 29576882]
Schaeffel F, Troilo D, Wallman J, Howland HC. Developing eyes that lack accommodation grow to compensate for imposed defocus. Visual neuroscience. 1990 Feb:4(2):177-83 [PubMed PMID: 2271446]
Level 3 (low-level) evidenceBartlett JD, Niemann K, Houde B, Allred T, Edmondson MJ, Crockett RS. A tolerability study of pirenzepine ophthalmic gel in myopic children. Journal of ocular pharmacology and therapeutics : the official journal of the Association for Ocular Pharmacology and Therapeutics. 2003 Jun:19(3):271-9 [PubMed PMID: 12828845]
Level 1 (high-level) evidenceSiatkowski RM, Cotter S, Miller JM, Scher CA, Crockett RS, Novack GD, US Pirenzepine Study Group. Safety and efficacy of 2% pirenzepine ophthalmic gel in children with myopia: a 1-year, multicenter, double-masked, placebo-controlled parallel study. Archives of ophthalmology (Chicago, Ill. : 1960). 2004 Nov:122(11):1667-74 [PubMed PMID: 15534128]
Level 1 (high-level) evidenceTrier K, Munk Ribel-Madsen S, Cui D, Brøgger Christensen S. Systemic 7-methylxanthine in retarding axial eye growth and myopia progression: a 36-month pilot study. Journal of ocular biology, diseases, and informatics. 2008 Dec:1(2-4):85-93. doi: 10.1007/s12177-008-9013-3. Epub 2008 Nov 4 [PubMed PMID: 20072638]
Level 3 (low-level) evidenceQi H, Gao C, Li Y, Feng X, Wang M, Zhang Y, Chen Y. The effect of Timolol 0.5% on the correction of myopic regression after LASIK. Medicine. 2017 Apr:96(17):e6782. doi: 10.1097/MD.0000000000006782. Epub [PubMed PMID: 28445315]
Level 2 (mid-level) evidenceNickla DL. Ocular diurnal rhythms and eye growth regulation: where we are 50 years after Lauber. Experimental eye research. 2013 Sep:114():25-34. doi: 10.1016/j.exer.2012.12.013. Epub 2013 Jan 5 [PubMed PMID: 23298452]
Level 3 (low-level) evidenceWang P, Chen S, Liu Y, Lin F, Song Y, Li T, Aung T, Zhang X, GSHM study group. Lowering Intraocular Pressure: A Potential Approach for Controlling High Myopia Progression. Investigative ophthalmology & visual science. 2021 Nov 1:62(14):17. doi: 10.1167/iovs.62.14.17. Epub [PubMed PMID: 34787640]
Sherwin JC, Reacher MH, Keogh RH, Khawaja AP, Mackey DA, Foster PJ. The association between time spent outdoors and myopia in children and adolescents: a systematic review and meta-analysis. Ophthalmology. 2012 Oct:119(10):2141-51. doi: 10.1016/j.ophtha.2012.04.020. Epub 2012 Jul 17 [PubMed PMID: 22809757]
Level 2 (mid-level) evidenceJones LA, Sinnott LT, Mutti DO, Mitchell GL, Moeschberger ML, Zadnik K. Parental history of myopia, sports and outdoor activities, and future myopia. Investigative ophthalmology & visual science. 2007 Aug:48(8):3524-32 [PubMed PMID: 17652719]
Feldkaemper M, Schaeffel F. An updated view on the role of dopamine in myopia. Experimental eye research. 2013 Sep:114():106-19. doi: 10.1016/j.exer.2013.02.007. Epub 2013 Feb 19 [PubMed PMID: 23434455]
Level 3 (low-level) evidenceFrench AN, Ashby RS, Morgan IG, Rose KA. Time outdoors and the prevention of myopia. Experimental eye research. 2013 Sep:114():58-68. doi: 10.1016/j.exer.2013.04.018. Epub 2013 May 2 [PubMed PMID: 23644222]
Level 3 (low-level) evidenceCheng D, Schmid KL, Woo GC, Drobe B. Randomized trial of effect of bifocal and prismatic bifocal spectacles on myopic progression: two-year results. Archives of ophthalmology (Chicago, Ill. : 1960). 2010 Jan:128(1):12-9. doi: 10.1001/archophthalmol.2009.332. Epub [PubMed PMID: 20065211]
Level 1 (high-level) evidenceGwiazda J, Marsh-Tootle WL, Hyman L, Hussein M, Norton TT, COMET Study Group. Baseline refractive and ocular component measures of children enrolled in the correction of myopia evaluation trial (COMET). Investigative ophthalmology & visual science. 2002 Feb:43(2):314-21 [PubMed PMID: 11818372]
Level 2 (mid-level) evidenceSaw SM, Nieto FJ, Katz J, Schein OD, Levy B, Chew SJ. Familial clustering and myopia progression in Singapore school children. Ophthalmic epidemiology. 2001 Sep:8(4):227-36 [PubMed PMID: 11471091]
Level 2 (mid-level) evidenceLiu Y, Wildsoet C. The effect of two-zone concentric bifocal spectacle lenses on refractive error development and eye growth in young chicks. Investigative ophthalmology & visual science. 2011 Feb:52(2):1078-86. doi: 10.1167/iovs.10-5716. Epub 2011 Feb 22 [PubMed PMID: 20861487]
Level 3 (low-level) evidenceArumugam B, Hung LF, To CH, Holden B, Smith EL 3rd. The effects of simultaneous dual focus lenses on refractive development in infant monkeys. Investigative ophthalmology & visual science. 2014 Oct 16:55(11):7423-32. doi: 10.1167/iovs.14-14250. Epub 2014 Oct 16 [PubMed PMID: 25324283]
Level 3 (low-level) evidenceLam CSY, Tang WC, Tse DY, Lee RPK, Chun RKM, Hasegawa K, Qi H, Hatanaka T, To CH. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. The British journal of ophthalmology. 2020 Mar:104(3):363-368. doi: 10.1136/bjophthalmol-2018-313739. Epub 2019 May 29 [PubMed PMID: 31142465]
Level 1 (high-level) evidenceLam CS, Tang WC, Tse DY, Tang YY, To CH. Defocus Incorporated Soft Contact (DISC) lens slows myopia progression in Hong Kong Chinese schoolchildren: a 2-year randomised clinical trial. The British journal of ophthalmology. 2014 Jan:98(1):40-5. doi: 10.1136/bjophthalmol-2013-303914. Epub 2013 Oct 29 [PubMed PMID: 24169657]
Level 1 (high-level) evidenceZhu X, Wallman J. Temporal properties of compensation for positive and negative spectacle lenses in chicks. Investigative ophthalmology & visual science. 2009 Jan:50(1):37-46. doi: 10.1167/iovs.08-2102. Epub 2008 Sep 12 [PubMed PMID: 18791175]
Level 3 (low-level) evidenceAnstice NS, Phillips JR. Effect of dual-focus soft contact lens wear on axial myopia progression in children. Ophthalmology. 2011 Jun:118(6):1152-61. doi: 10.1016/j.ophtha.2010.10.035. Epub 2011 Jan 26 [PubMed PMID: 21276616]
Level 1 (high-level) evidenceSankaridurg P. Contact lenses to slow progression of myopia. Clinical & experimental optometry. 2017 Sep:100(5):432-437. doi: 10.1111/cxo.12584. Epub 2017 Jul 28 [PubMed PMID: 28752898]
Liu G, Liu L, Rong H, Li L, Liu X, Jia Z, Zhang H, Wang B, Song D, Hu J, Shi X, Du B, Wei R. Axial Shortening Effects of Repeated Low-level Red-light Therapy in Children With High Myopia: A Multicenter Randomized Controlled Trial. American journal of ophthalmology. 2025 Feb:270():203-215. doi: 10.1016/j.ajo.2024.10.011. Epub 2024 Oct 16 [PubMed PMID: 39424029]
Level 1 (high-level) evidenceJiang Y, Zhu Z, Tan X, Kong X, Zhong H, Zhang J, Xiong R, Yuan Y, Zeng J, Morgan IG, He M. Effect of Repeated Low-Level Red-Light Therapy for Myopia Control in Children: A Multicenter Randomized Controlled Trial. Ophthalmology. 2022 May:129(5):509-519. doi: 10.1016/j.ophtha.2021.11.023. Epub 2021 Dec 1 [PubMed PMID: 34863776]
Level 1 (high-level) evidenceSu Y, Pan A, Wu Y, Zhu S, Zheng L, Xue A. The efficacy of posterior scleral contraction in controlling high myopia in young people. American journal of translational research. 2018:10(11):3628-3634 [PubMed PMID: 30662614]
Goodyear MJ, Junghans BM, Giummarra L, Murphy MJ, Crewther DP, Crewther SG. A role for aquaporin-4 during induction of form deprivation myopia in chick. Molecular vision. 2008 Feb 8:14():298-307 [PubMed PMID: 18334967]
Level 3 (low-level) evidenceAvetisov ES, Tarutta EP, Iomdina EN, Vinetskaya MI, Andreyeva LD. Nonsurgical and surgical methods of sclera reinforcement in progressive myopia. Acta ophthalmologica Scandinavica. 1997 Dec:75(6):618-23 [PubMed PMID: 9527318]
Level 3 (low-level) evidenceYazdani N, Sadeghi R, Ehsaei A, Taghipour A, Hasanzadeh S, Zarifmahmoudi L, Heravian Shandiz J. Under-correction or full correction of myopia? A meta-analysis. Journal of optometry. 2021 Jan-Mar:14(1):11-19. doi: 10.1016/j.optom.2020.04.003. Epub 2020 Jun 2 [PubMed PMID: 32507615]
Level 1 (high-level) evidenceKaur K, Kannusamy V, Gurnani B, Mouttapa F, Balakrishnan L. Knowledge, Attitude, and Practice Patterns Related to Digital Eye Strain Among Parents of Children Attending Online Classes in the COVID-19 Era: A Cross-sectional Study. Journal of pediatric ophthalmology and strabismus. 2022 Jul-Aug:59(4):224-235. doi: 10.3928/01913913-20211019-01. Epub 2021 Dec 20 [PubMed PMID: 34928763]
Level 2 (mid-level) evidenceLawrenson JG, Shah R, Huntjens B, Downie LE, Virgili G, Dhakal R, Verkicharla PK, Li D, Mavi S, Kernohan A, Li T, Walline JJ. Interventions for myopia control in children: a living systematic review and network meta-analysis. The Cochrane database of systematic reviews. 2023 Feb 16:2(2):CD014758. doi: 10.1002/14651858.CD014758.pub2. Epub 2023 Feb 16 [PubMed PMID: 36809645]
Level 1 (high-level) evidenceGuo Z, Wei Z, Ming H, Zhang L, Ma B, Zhao Y, Guo L. Efficacy and safety of orthokeratology sequentially combined with escalating atropine concentrations for myopia control in children. Scientific reports. 2025 Nov 6:15(1):38911. doi: 10.1038/s41598-025-22722-8. Epub 2025 Nov 6 [PubMed PMID: 41198803]
Gurnani B, Kaur K. Refractive Surprises After Cataract Surgery: Identification and Management in Optometric Practice- A Comprehensive Review. Clinical optometry. 2026:18():572733. doi: 10.2147/OPTO.S572733. Epub 2026 Apr 29 [PubMed PMID: 42083643]
Gurnani B, Kaur K, Tripathy K. Is there a genetic link between Keratoconus and Fuch's endothelial corneal dystrophy? Medical hypotheses. 2021 Dec:157():110699. doi: 10.1016/j.mehy.2021.110699. Epub 2021 Oct 9 [PubMed PMID: 34666260]
Kaur K, Gurnani B, Porwal A. Changing trends in myopia management in pediatric population. Indian journal of ophthalmology. 2022 Dec:70(12):4462-4463. doi: 10.4103/ijo.IJO_1485_22. Epub [PubMed PMID: 36453373]
Gurnani B, Kaur K, Morya AK. Adoption, implementation, definitions, and future of blockchain technology in ophthalmology. Indian journal of ophthalmology. 2023 Mar:71(3):1025-1026. doi: 10.4103/ijo.IJO_1802_22. Epub [PubMed PMID: 36872733]
Creavin AL, Brown RD. Ophthalmic abnormalities in children with Down syndrome. Journal of pediatric ophthalmology and strabismus. 2009 Mar-Apr:46(2):76-82 [PubMed PMID: 19343968]
Liu X, Ye L, Chen C, Chen M, Wen S, Mao X. Evaluation of the Necessity for Cycloplegia During Refraction of Chinese Children Between 4 and 10 Years Old. Journal of pediatric ophthalmology and strabismus. 2020 Jul 1:57(4):257-263. doi: 10.3928/01913913-20200407-01. Epub [PubMed PMID: 32687211]
Vohra V, Tuteja S, Gurnani B, Chawla H. Collagen Cross Linking for Keratoconus. StatPearls. 2026 Jan:(): [PubMed PMID: 32965942]
Kaur K, Muralikrishnan J, Hussaindeen JR, Deori N, Gurnani B. Impact of Covid-19 on Pediatric Ophthalmology Care: Lessons Learned. Pediatric health, medicine and therapeutics. 2023:14():309-321. doi: 10.2147/PHMT.S395349. Epub 2023 Oct 12 [PubMed PMID: 37849985]
Xu J, Zafar A, Torres M, Varma R, Jiang X. Ocular conditions associated with parental concerns regarding childhood development and worse quality of life among multiethnic preschool children. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2026 Feb:30(1):104737. doi: 10.1016/j.jaapos.2026.104737. Epub 2026 Jan 30 [PubMed PMID: 41621778]
Level 2 (mid-level) evidenceDurajczyk M, Lubiński W. Congenital Stationary Night Blindness (CSNB)-Case Reports and Review of Current Knowledge. Journal of clinical medicine. 2025 Feb 13:14(4):. doi: 10.3390/jcm14041238. Epub 2025 Feb 13 [PubMed PMID: 40004769]
Level 3 (low-level) evidenceSpaide RF. Peripheral Degenerative Retinoschisis: Imaging Evidence for Two Distinct Structural Configurations. Retina (Philadelphia, Pa.). 2026 Jun 15:():. doi: 10.1097/IAE.0000000000004907. Epub 2026 Jun 15 [PubMed PMID: 42295052]
Biermann J, Hoffmann MB. [Albinism: Clinical presentation, diagnostics and visual function]. Die Ophthalmologie. 2026 Jun:123(6):488-501. doi: 10.1007/s00347-026-02450-8. Epub 2026 May 28 [PubMed PMID: 42207246]
Leon Agudelo JA, Martínez Vallejo H. Therapeutic applications of gene editing using CRISPR-Cas9 in the posterior segment: review of the literature. Archivos de la Sociedad Espanola de Oftalmologia. 2026 Jun 12:():502582. doi: 10.1016/j.oftale.2026.502582. Epub 2026 Jun 12 [PubMed PMID: 42285217]
Zaki HF, Bishri J, Abdul Muqtadir M, Abu-Zaid A. Correcting photoreceptor diseases at their source: CRISPR strategies for cone-rod dystrophy and achromatopsia. Experimental eye research. 2026 Jun 9:270():111119. doi: 10.1016/j.exer.2026.111119. Epub 2026 Jun 9 [PubMed PMID: 42264060]
Lecca M, Bosetti C, Ruoli F, Fontanel L, Mazza M, Valente EM, Battini R, Errichiello E. Phenotypic Refinement of ESAM-Related Tight-Junctionopathy: Novel Genetic and Ocular Findings and Literature Review. Molecular genetics & genomic medicine. 2026 Jun:14(6):e70245. doi: 10.1002/mgg3.70245. Epub [PubMed PMID: 42265826]
Amjad M, Khalid M, Jemjem B, Khan A, Aslam E, Sarfraz AR. CRISPR interference in rare HESX1 haploinsufficiency: correcting septo-optic dysplasia with endocrine precocity. Annals of medicine and surgery (2012). 2026 May:88(5):3010-3011. doi: 10.1097/MS9.0000000000004908. Epub 2026 Apr 2 [PubMed PMID: 42078637]
Hr D, Singh AK, Singh A, Shah SK, Indurkar A, Patel BK. Retinal biomarkers for visual prognosis in pituitary surgery: a narrative review. Pituitary. 2026 Jun 16:29(4):. pii: 104. doi: 10.1007/s11102-026-01709-2. Epub 2026 Jun 16 [PubMed PMID: 42301499]
Level 3 (low-level) evidenceHuang J, Brodie SE, Kong J, Soucy M, Maumenee IH, Tsang SH. Blue cone monochromacy with parafoveal hyperautofluorescent ring caused by a novel OPN1LW p.Ile109Asn variant. Documenta ophthalmologica. Advances in ophthalmology. 2026 Jun 11:():. doi: 10.1007/s10633-026-10118-6. Epub 2026 Jun 11 [PubMed PMID: 42274835]
Level 3 (low-level) evidenceAnne RP, Mathai SS, S S. Prevalence of sight-threatening ocular abnormalities identified by retinal examination in neonates: a systematic review and meta-analysis. BMC pediatrics. 2026 Jun 2:():. doi: 10.1186/s12887-026-07084-y. Epub 2026 Jun 2 [PubMed PMID: 42231307]
Level 1 (high-level) evidenceRohowetz LJ, Redick DW, Fan KC, Berrocal AM. Concurrent Wagner syndrome and retinopathy of prematurity. American journal of ophthalmology case reports. 2025 Sep:39():102392. doi: 10.1016/j.ajoc.2025.102392. Epub 2025 Jul 22 [PubMed PMID: 40747364]
Level 3 (low-level) evidenceKravutske Y, Esmeraldo MA, Chambers S, Dahmoush HM, Halverson MR, Geraldo AF, Soares BP. Knobloch Syndrome in Childhood: Neuroradiologic Findings and Clinical Correlation. Journal of child neurology. 2026 May 7:():8830738261444228. doi: 10.1177/08830738261444228. Epub 2026 May 7 [PubMed PMID: 42093600]
Logan NS, Bullimore MA. Optical interventions for myopia control. Eye (London, England). 2024 Feb:38(3):455-463. doi: 10.1038/s41433-023-02723-5. Epub 2023 Sep 22 [PubMed PMID: 37740053]
He X, Sankaridurg P, Wang J, Chen J, Naduvilath T, He M, Zhu Z, Li W, Morgan IG, Xiong S, Zhu J, Zou H, Rose KA, Zhang B, Weng R, Resnikoff S, Xu X. Time Outdoors in Reducing Myopia: A School-Based Cluster Randomized Trial with Objective Monitoring of Outdoor Time and Light Intensity. Ophthalmology. 2022 Nov:129(11):1245-1254. doi: 10.1016/j.ophtha.2022.06.024. Epub 2022 Jun 30 [PubMed PMID: 35779695]
Level 1 (high-level) evidenceXiong R, Zhu Z, Jiang Y, Kong X, Zhang J, Wang W, Kiburg K, Yuan Y, Chen Y, Zhang S, Xuan M, Zeng J, Morgan IG, He M. Sustained and rebound effect of repeated low-level red-light therapy on myopia control: A 2-year post-trial follow-up study. Clinical & experimental ophthalmology. 2022 Dec:50(9):1013-1024. doi: 10.1111/ceo.14149. Epub 2022 Sep 7 [PubMed PMID: 36054314]
Morton M, Lee L, Morjaria P. Practical tips for managing myopia. Community eye health. 2019:32(105):17-18 [PubMed PMID: 31409951]
Vagge A, Baldi M, Musolino M, Rivarone V, Catti C, Iester M. Current and Emerging Strategies for Myopia Control in Children: A Comprehensive Evidence-Based Review. Journal of clinical medicine. 2026 Feb 15:15(4):. doi: 10.3390/jcm15041545. Epub 2026 Feb 15 [PubMed PMID: 41753234]
Smith MJ, Walline JJ. Controlling myopia progression in children and adolescents. Adolescent health, medicine and therapeutics. 2015:6():133-40. doi: 10.2147/AHMT.S55834. Epub 2015 Aug 13 [PubMed PMID: 26316834]
Kaur K, Gurnani B. Cycloplegic and Noncycloplegic Refraction. StatPearls. 2026 Jan:(): [PubMed PMID: 35593830]
Gurnani B, Kaur K. Contact Lens–Related Complications. StatPearls. 2026 Jan:(): [PubMed PMID: 36512659]
Fatimah M, Agarkar S, Narayanan A. Impact of defocus incorporated multiple segments (DIMS) spectacle lenses for myopia control on quality of life of the children: a qualitative study. BMJ open ophthalmology. 2024 Jul 2:9(1):. doi: 10.1136/bmjophth-2023-001562. Epub 2024 Jul 2 [PubMed PMID: 38960416]
Level 2 (mid-level) evidenceTan M, Li B, Xu Z, Wu D, Liu J, Tang W, Xu F. Repeated low-intensity red light therapy for childhood myopia: a retrospective cohort study. American journal of translational research. 2025:17(9):6951-6959. doi: 10.62347/MWYH6856. Epub 2025 Sep 15 [PubMed PMID: 41113016]
Level 2 (mid-level) evidenceDang RM, Jalbert I, Hui A, Kang P. Measuring Treatment Adherence in Myopia Control: Current Practices and Future Directions. Ophthalmology science. 2026 Jan:6(1):100949. doi: 10.1016/j.xops.2025.100949. Epub 2025 Sep 26 [PubMed PMID: 41321843]
Level 3 (low-level) evidenceGurnani B, Kaur K. Recent Advances in Refractive Surgery: An Overview. Clinical ophthalmology (Auckland, N.Z.). 2024:18():2467-2472. doi: 10.2147/OPTH.S481421. Epub 2024 Sep 2 [PubMed PMID: 39246558]
Level 3 (low-level) evidenceWnękowicz-Augustyn E, Teper S, Wylęgała E. Preventing the Progression of Myopia in Children-A Review of the Past Decade. Medicina (Kaunas, Lithuania). 2023 Oct 19:59(10):. doi: 10.3390/medicina59101859. Epub 2023 Oct 19 [PubMed PMID: 37893579]
Recko M, Stahl ED. Childhood myopia: epidemiology, risk factors, and prevention. Missouri medicine. 2015 Mar-Apr:112(2):116-21 [PubMed PMID: 25958656]
Du Y, Meng J, He W, Qi J, Lu Y, Zhu X. Complications of high myopia: An update from clinical manifestations to underlying mechanisms. Advances in ophthalmology practice and research. 2024 Aug-Sep:4(3):156-163. doi: 10.1016/j.aopr.2024.06.003. Epub 2024 Jun 21 [PubMed PMID: 39036706]
Level 2 (mid-level) evidenceShih YF, Ho TC, Hsiao CK, Lin LL. Long-term visual prognosis of infantile-onset high myopia. Eye (London, England). 2006 Aug:20(8):888-92 [PubMed PMID: 16096663]
Ohno-Matsui K, Jonas JB. Posterior staphyloma in pathologic myopia. Progress in retinal and eye research. 2019 May:70():99-109. doi: 10.1016/j.preteyeres.2018.12.001. Epub 2018 Dec 8 [PubMed PMID: 30537538]
Haarman AEG, Enthoven CA, Tideman JWL, Tedja MS, Verhoeven VJM, Klaver CCW. The Complications of Myopia: A Review and Meta-Analysis. Investigative ophthalmology & visual science. 2020 Apr 9:61(4):49. doi: 10.1167/iovs.61.4.49. Epub [PubMed PMID: 32347918]
Level 1 (high-level) evidenceTripathy K, Zeppieri M. Open Angle Glaucoma. StatPearls. 2026 Jan:(): [PubMed PMID: 28722917]
Fogt JS, Roth M, Gardner HP. How Can We Better Inform Patients of the Importance of Contact Lens Compliance?: Current Perspectives. Clinical optometry. 2024:16():267-286. doi: 10.2147/OPTO.S405204. Epub 2024 Nov 2 [PubMed PMID: 39507399]
Level 3 (low-level) evidenceBai L, Chen M, Li Q, Chen J, Fu Q, Liu Y, Wang L, Wang G, Dong B, Wang H. Association between myopia and refractive parameters with eye behaviors in childhood aged 6 ~ 9 years: a follow-up study in Beijing. BMC public health. 2026 Feb 12:26(1):. doi: 10.1186/s12889-026-26594-z. Epub 2026 Feb 12 [PubMed PMID: 41673640]
Kaur K, Gurnani B. Low Vision Aids. StatPearls. 2026 Jan:(): [PubMed PMID: 36256771]
Evans JR, Morjaria P, Powell C. Vision screening for correctable visual acuity deficits in school-age children and adolescents. The Cochrane database of systematic reviews. 2018 Feb 15:2(2):CD005023. doi: 10.1002/14651858.CD005023.pub3. Epub 2018 Feb 15 [PubMed PMID: 29446439]
Level 1 (high-level) evidenceChierigo A, Ferro Desideri L, Traverso CE, Vagge A. The Role of Atropine in Preventing Myopia Progression: An Update. Pharmaceutics. 2022 Apr 20:14(5):. doi: 10.3390/pharmaceutics14050900. Epub 2022 Apr 20 [PubMed PMID: 35631486]
Yam JC, Li FF, Zhang X, Tang SM, Yip BHK, Kam KW, Ko ST, Young AL, Tham CC, Chen LJ, Pang CP. Two-Year Clinical Trial of the Low-Concentration Atropine for Myopia Progression (LAMP) Study: Phase 2 Report. Ophthalmology. 2020 Jul:127(7):910-919. doi: 10.1016/j.ophtha.2019.12.011. Epub 2019 Dec 21 [PubMed PMID: 32019700]
Level 1 (high-level) evidenceRuiz-Pomeda A, Villa-Collar C. Slowing the Progression of Myopia in Children with the MiSight Contact Lens: A Narrative Review of the Evidence. Ophthalmology and therapy. 2020 Dec:9(4):783-795. doi: 10.1007/s40123-020-00298-y. Epub 2020 Sep 11 [PubMed PMID: 32915454]
Level 3 (low-level) evidence