Introduction
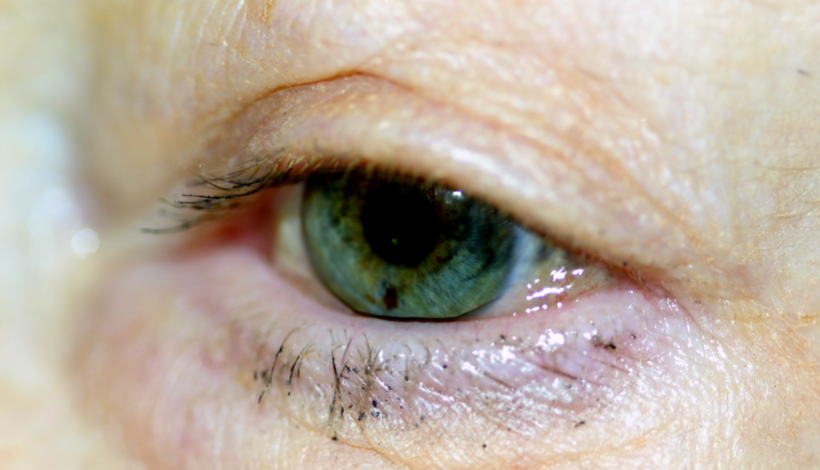
Conjunctivochalasis (CCh) is an underdiagnosed and common condition characterized by loose, redundant, and nonedematous conjunctival folds typically located in the inferior bulbar conjunctiva. The term, which comes from the Greek chalasis ("to slacken"), was first used by Hughes in 1942. CCh can cause a spectrum of symptoms, ranging from mild discomfort in the mild stages to tear outflow obstruction in the moderate stages and exposure keratopathy with subsequent visual loss in the severe stages (see Image. Conjunctivochalasis, Left Eye).[1][2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of conjunctivochalasis has not been fully elucidated. Some researchers have hypothesized that the condition may develop secondary to the degradation of elastic fibers, a key component of the extracellular matrix that provides mechanical support and structure to the conjunctiva.[3][4] The repeated friction of the eyelids against the conjunctiva is thought to contribute to the breakdown of the elastic fibers and the development of the characteristic lid-parallel conjunctival folds (LIPCOF).[5] These folds can obstruct tear drainage, shorten the fornices, and obliterate the tear meniscus and reservoir.[6][7] Other risk factors may exacerbate this process, including genetics, age, mechanical stress (eg, contact lenses), inflammation, and ultraviolet light.[8][9][10][11][12]
Furthermore, the cumulative mechanical insults likely induce an inflammatory response and secondary breakdown of the conjunctiva and the Tenon capsule. The formation of the LIPCOF decreases tear outflow, leading to the build-up of inflammatory molecules on the ocular surface and activation of matrix metalloproteinases (MMPs).[13] MMPs are proteins that degrade and remodel the extracellular matrix; their activation would therefore have detrimental effects on the conjunctiva in higher concentrations.
Epidemiology
Conjunctivochalasis generally affects older adults and is considered an age-related change; numerous studies' results have reported a higher prevalence of CCh with increasing age.[9][14] CCh does not have a gender predilection, although some studies have found higher grades of CCh and lower tear meniscus area in female patients. The majority of epidemiological studies originate from China, and their results report high prevalence rates of total and clinically significant CCh (44% and 18%, respectively).[14] Epidemiological data from Western populations remain limited. A small study conducted at an American Veterans Affairs hospital showed a greater proportion of patients with CCh were of non-Hispanic ethnicity than those without the condition, though further large-scale studies are needed to characterize prevalence across diverse populations.[15]
Pathophysiology
Ocular inflammation plays an important role in the pathophysiology of conjunctivochalasis. Studies' results have shown a heightened expression of matrix metalloproteinases in cultured conjunctival fibroblasts in patients with CCh, in addition to an upregulation of inflammatory and oxidative stress markers in their tear profiles.[11][13] The inflammatory cytokines, including interleukin-1 beta and tumor necrosis factor-alpha, are thought to trigger the overexpression of MMPs in cultured CCh fibroblasts.[16] Delayed tear clearance further aggravates this process, leading to oxidative damage to the ocular surface.[11][17] Gumus and Pflugfelder demonstrated that both CCh and elevated tear osmolarity are independently associated with reduced conjunctival epithelial thickness in dry eye disease, further supporting the link between chronic inflammation, mechanical stress, and epithelial compromise.[18]
Histopathology
Varying histological findings have been reported in conjunctivochalasis, likely reflecting the wide spectrum of disease severity. Microscopy studies have demonstrated a range of conjunctival epithelial changes, including normal epithelium, epithelial hyperplasia, and reduced intracellular cohesiveness.[17] Elastosis and chronic non-granulomatous inflammation have also been described in CCh specimens.
However, whether inflammatory cells are consistently present within the conjunctival folds remains contested.[19][20] The contradictory nature of these findings, alongside the absence of statistically significant differences across histopathological studies, suggests that the underlying pathology of CCh may not reside in the conjunctival tissue itself but rather in its loose adhesions to underlying structures.[21] Supporting a broader disease mechanism, Muhafiz et al examined impression cytology and meibomian gland parameters in CCh, demonstrating that abnormal goblet cell density and meibomian gland dropout correlated with disease severity, thereby suggesting concurrent involvement of both the ocular surface and adnexal structures.[22]
History and Physical
Conjunctivochalasis can cause a range of symptoms, from exacerbation of existing dry eye in mild disease to impaired tear outflow in moderate disease and ocular surface exposure in severe disease. Symptoms can be vague and comprise foreign body sensation, burning, pain, redness, epiphora, photophobia, and blurry vision, typically worsened during downgaze, blinking, or digital compression onto the globe.[23][24] Patients with nasal CCh are thought to be more affected with dry eye symptoms and experience substantial negative impacts on quality of life.[15]
Evaluation
Lid-Parallel Conjunctival Folds
Conjunctivochalasis is typically bilateral and characterized by loose, redundant conjunctival folds. The condition can involve any portion of the bulbar conjunctiva but is generally more prominent inferiorly. Slit-lamp examinations may confirm the LIPCOF, typically found over the lower lid.
As the disease progresses, the redundant conjunctiva can shorten the fornices and mechanically obstruct the punctum.[24] The folds are more prominent when upward pressure is applied to the lower lid, and they flatten with upgaze or when the lower lid is pulled away from the globe (see Image. Lateral Conjunctivochalasis). Identifying the folds in the superior CCh is more challenging; they can be seen when the upper lid is pressed downward against the globe.
The depth of the fornices can be measured using a slit-lamp beam or a fornix depth measurer. Studies' results have demonstrated that anterior segment optical coherence tomography (OCT) can aid in diagnosing and monitoring patients with CCh, as the cross-sectional area of prolapsing conjunctiva can be measured.[25] Zhang et al demonstrated, using anterior segment OCT, that the conjunctiva in patients with CCh was thinner than that of healthy controls.[26]
Grading Systems
Multiple grading systems have been developed for CCh. Hoh et al’s system comprises grades 0 to 3, depending on the number and height of folds (see Images. Conjunctivochalasis, Grade 1; Conjunctivochalasis, Grade 2; Conjunctivochalasis, Grade 3).
- Grade 0 (no persistent fold)
- Grade 1 (a single, small fold)
- Grade 2 (two or more folds but not higher than the tear meniscus)
- Grade 3 (multiple folds and higher than the tear meniscus) [27]
Meller et al proposed a new multiparameter system that considers the location, height of the folds, punctal occlusion, and the presence of changes in downgaze and with digital pressure (see Table 1). CCh has further been subclassified as T, M, or N if the folds are primarily located in the temporal, middle, or nasal part of the eyelid, respectively. The grading system has become widely used and adapted.[28]
Table 1. Meller et al Conjunctivochalasis Grading System
|
Location |
Folds vs Tear Meniscus Height |
Punctal Occlusion |
Changes in Downgase |
Changes by Digital Pressure |
|
0: None 1: One location 2: Two locations 3: Whole lid |
A: <Tear meniscus B: =Tear meniscus C: >Tear meniscus |
O+: Nasal location with punctal occlusion O-: Nasal location without punctal occlusion |
G↑: Height/extent of CCh increases in downgaze G↔: No difference G↓: Height/extent of CCh decreases in downgaze |
P↑: Height/extent of CCh increases with digital pressure P↔: No difference P↓: Height/extent of CCh decreases with digital pressure |
CCh, conjunctivochalasis
Eifrig developed a new grading system based on the degree of conjunctival rolling beneath the margin of the cornea when the patient is asked to look toward the midline (referred to as the "roll sign") and the speed at which the conjunctival tissue and vessels return to their primary position after blinking ("blink sign"). Both roll and blink signs are graded from 1 to 4.[29]
Secondary Features
CCh is often associated with keratoconjunctivitis sicca (KCS), and patients with severe CCh have a higher prevalence of KCS. Therefore, additional tests such as the Schirmer test, tear breakup time, fluorescein staining, and clearance rate are critical. In isolated CCh cases, discrete punctate or linear staining can be seen on the mucosal aspect of the lid margin near the redundant conjunctiva, which differs from the exposure pattern seen in patients with KCS.
Although not readily available, an ocular surface interferometer can also be used to monitor changes in the thickness of the lipid layer in patients with CCh.[30] Other characteristic signs of CCh include subconjunctival hemorrhage (vessels in the loose conjunctiva are prone to rupture when blinking), swollen puncta, and anterior migration of the mucocutaneous junction (likely secondary to the delayed clearance of inflammatory proteins).[24] Furthermore, identifying any evidence of lagophthalmos on the blink, gentle, and forced closure is important.[31]
Some studies' results have also shown a correlation between the presence of a pinguecula and the severity of CCh in the same conjunctival area.[32] The causative mechanism is unclear, but it has been speculated to involve confounding risk factors such as increased age and ultraviolet radiation. In severe cases, corneal thinning (dellen) has also been reported. Eyelid disorders, including meibomian gland dysfunction, floppy eyelid syndrome, and entropion, often coexist with CCh and can exacerbate the inflammatory process and development of the characteristic folds.[33]
Treatment / Management
For asymptomatic conjunctivochalasis, no treatment is necessary. In mild to moderate cases, topical drops can address chemosis and inflammation. As mentioned previously, the presence of CCh exhibits a strong positive predictive value in the diagnosis of keratoconjunctivitis sicca.
Lubricants, including artificial tears and gels, can therefore provide symptomatic relief and stabilize the tear film. Certain ingredients in artificial tears, particularly isotonic glycerol and sodium hyaluronate, are thought to dampen disease severity.[34] Corticosteroids may address chemosis and inflammation, but many require prolonged use. A study's results demonstrated both subjective and objective improvements in dry eye symptoms in CCh following a 3-week course of topical methylprednisolone.[35] In addition, antihistamine drops can decrease rubbing and subsequent mechanical insults.(B3)
Medical treatment may not be sufficient. Other approaches to tighten the redundant conjunctiva have been trialed with varying degrees of success (see Table 2). These techniques include conjunctival excision, cauterization, scleral fixation of the conjunctiva, conjunctival ligation, laser conjunctivoplasty, and radio-wave electrosurgery with or without tissue grafting (eg, amniotic membrane).[36][37][38][39][40][41](B2)
Table 2. Surgical Procedures for Conjunctivochalasis Correction
|
Technique |
Advantages |
Disadvantages |
|
Conjunctival cauterization |
Reduces operating time (no sutures needed) Shrinks redundant folds Decreases the risk of motility problems/scar formation Possibly improves scleral fixation |
Reserved for mild to moderate cases Repeat procedures may be necessary |
|
Excision of the conjunctiva |
Removes redundant conjunctiva Reduces blink-associated microtrauma Reduces interference with tear meniscus |
Over-resection may lead to:
|
|
Excision of conjunctiva with amniotic membrane graft |
As above, plus decreases the risk of fornix shortening |
Focal conjunctival inflammation Scar formation Suture-related complications |
|
Scleral fixation of the conjunctiva |
Strengthens adhesions to the sclera Reinforces the Tenon layer Reduces the risk of fornix shortening/ocular motility complications |
Surgically challenging Suture-related complications |
|
Laser conjunctivoplasty, high-frequency radio-wave electrosurgery |
Reduces operating time Shrinks redundant folds Less invasive |
Not readily available Chemosis Hyperemia Mild subconjunctival hemorrhage |
|
Recession of the conjunctiva with the amniotic membrane |
Removes redundant conjunctiva Reduces blink-associated microtrauma Reduces interference with tear meniscus Restores tear reservoir |
Higher cost if amniotic membrane graft used |
Most of these procedures involve excising or resecting the conjunctiva to relieve mechanical obstruction; however, they do not address fornix reconstruction, which may contribute to recurrence, and the excisional approach itself may lead to postoperative scarring. Conjunctival recession is thought to be more effective as it restores the fornix tear reservoir.[6][42] The use of fibrin glue can decrease operating time and suture-related complications.[43](B2)
Important surgical steps involve:
- Recession of conjunctiva and anchoring it from the limbus
- Removal of degenerated Tenon capsule
- Replacement of the Tenon and the conjunctival tissue by amniotic membrane grafts to possibly decrease pain and hasten recovery
Differential Diagnosis
Due to the variable symptoms of conjunctivochalasis, clinicians must rule out other conditions that cause tear-flow obstruction and tear-film instability, including lid laxity or malposition disorders (eg, ectropion, entropion, and floppy eyelid syndrome), trichiasis, punctal stenosis, conjunctivitis (viral and allergic), and nasolacrimal obstruction. A thorough history and physical examination help differentiate conjunctivochalasis from other diseases that may present with similar symptoms. In CCh, the symptoms worsen with downgaze and frequent blinking, as the folds increase or spread.
In contrast, patients with dry eye have worsening symptoms when looking up (eg, at a computer) as the interpalpebral exposure zone widens, and symptoms improve with increased blinking. Superior CCh is often misdiagnosed as superior limbic keratitis (SLK). Clinical features such as a micropapillary reaction in the upper tarsal conjunctiva, keratitis, and corneal erosions point toward a diagnosis of SLK, along with increased inflammation (eg, hyperemia, eyelid edema).
Prognosis
Conjunctivochalasis typically has a good prognosis with the correct treatment. However, diagnosis is often missed or delayed. Surgical management may be required in symptomatic patients when the initial medical treatment is inadequate. Studies' results have shown significant improvement in dry eye symptoms and signs following conjunctival recession with amniotic grafts, underscoring the importance of early diagnosis in this condition.[39][43]
Complications
While surgical complications following conjunctivochalasis repair are uncommon, patients are at risk for scarring, cicatricial entropion, retraction of the lower fornix, restricted motility, and corneal changes.
Deterrence and Patient Education
Patients should be educated regarding lifestyle changes, particularly if conjunctivochalasis is associated with blepharitis and keratoconjunctivitis sicca. Behavioral modifications include avoidance of exacerbating factors (eg, fans, air conditioners, heating vents, digital devices), dietary changes (low caffeine/alcohol intake, fatty acid supplementation), and lid care. A recent study's results demonstrated that the quality of life of patients with CCh was strongly determined by their tear-film instability and increased friction during blinking.[44] All treatment options, including conservative and surgical options, should be thoroughly discussed.
Pearls and Other Issues
A comprehensive diagnostic and therapeutic approach is essential in conjunctivochalasis, with careful attention to associated ocular surface disease and surgical planning considerations that directly influence patient outcomes.
- Identify the LIPCOF and examine the fornices in all patients presenting with ocular irritation or epiphora.
- Concurrent meibomian gland dysfunction, blepharitis, or dry eye disease should be identified and optimized before surgical intervention, as failure to address these contributing factors is a common cause of suboptimal surgical outcomes.
- Fornix reconstruction is the key to surgical success.
Enhancing Healthcare Team Outcomes
Conjunctivochalasis is frequently misdiagnosed, as its symptoms closely mimic those of other ocular surface disorders, leading to delays in appropriate evaluation and treatment. Accurate recognition requires an understanding of how redundant conjunctival folds disrupt tear film dynamics, impair the tear meniscus, and compromise the conjunctival tear reservoir. Management of CCh can be challenging, as associated ocular surface disease should be addressed before surgical intervention, and effective treatment often depends on restoring both tear meniscus height and the tear reservoir to improve patient comfort and function.
Optimal care for patients with CCh demands effective interprofessional collaboration. Optometrists play a pivotal role in early detection and monitoring, while ophthalmic nurses contribute to patient education, pre- and postoperative assessment, and continuity of care. Ophthalmologists and oculoplastic surgeons provide comprehensive clinical evaluation, medical management, and, where indicated, surgical correction. Clear, consistent communication across the team facilitates the thorough assessment of contributing ocular surface conditions, coordinated perioperative care, and shared decision-making. This integrated, multidisciplinary approach enhances diagnostic accuracy, minimizes surgical risk, and optimizes long-term outcomes for patients with CCh.
Media
(Click Image to Enlarge)
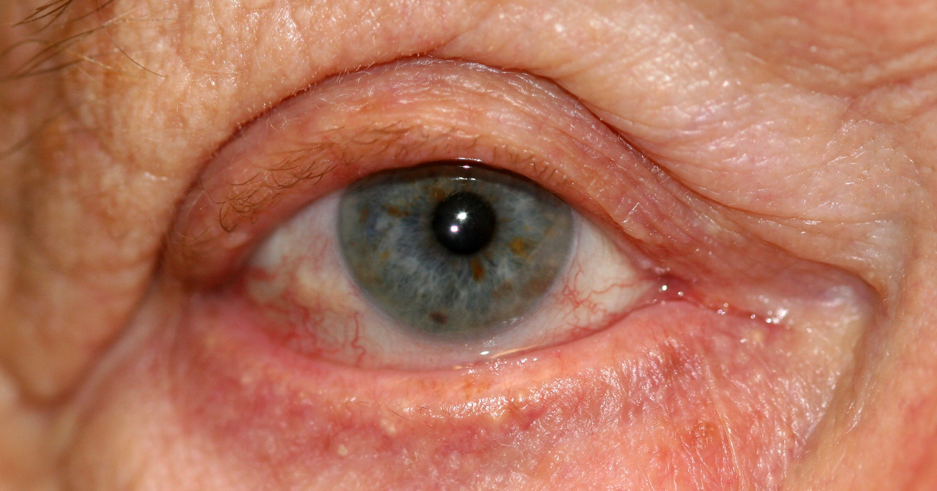
Conjunctivochalasis, Grade 2. The image shows a grade 2 conjunctivochalasis in a female patient.
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)
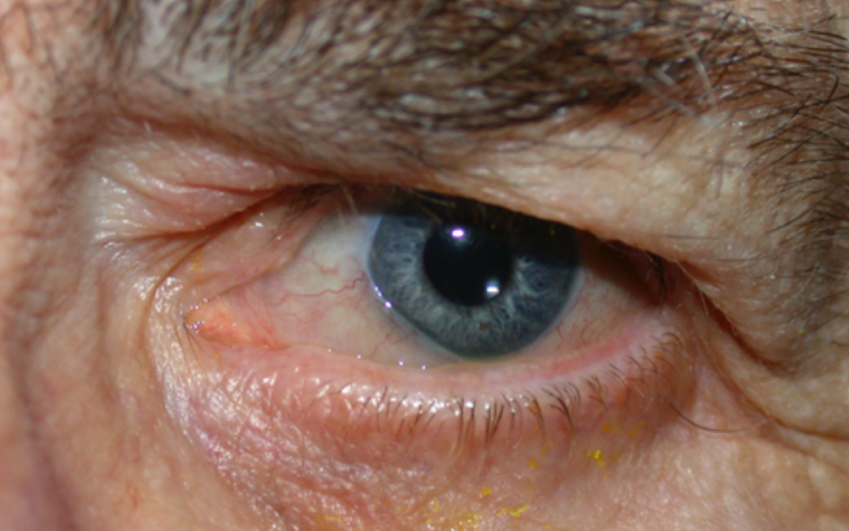
Conjunctivochalasis, Left Eye. This image portrays conjunctivochalasis in the left eye of a male patient.
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)
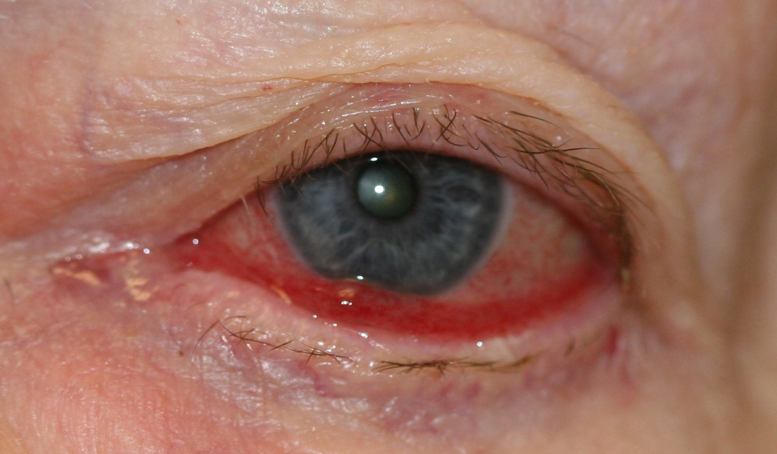
Conjunctivochalasis, Grade 3. The image demonstrates grade 3 conjunctivochalasis with cicatricial retraction and ectropion.
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)
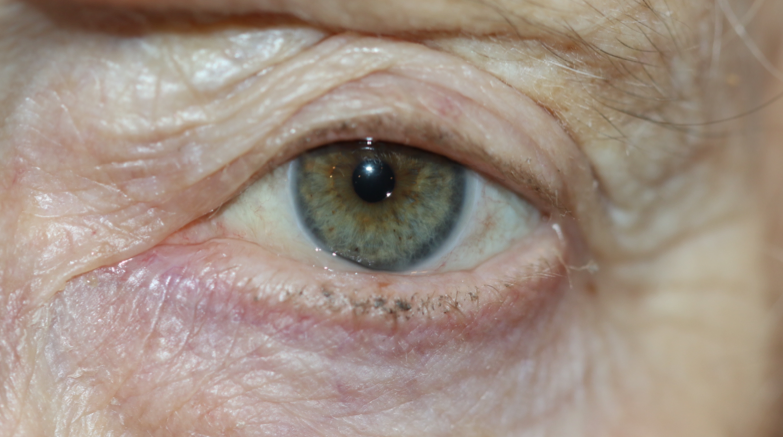
Conjunctivochalasis, Grade 1. The image shows grade 1 conjunctivochalasis with mild ectropion.
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)
Lateral Conjunctivochalasis. Slit-lamp photograph demonstrating redundant inferior bulbar conjunctival folds overlapping the lower lid margin, consistent with conjunctivochalasis.
Contributed by BCK Patel, MD, FRCS
References
Meller D, Tseng SC. Conjunctivochalasis: literature review and possible pathophysiology. Survey of ophthalmology. 1998 Nov-Dec:43(3):225-32 [PubMed PMID: 9862310]
Level 3 (low-level) evidenceYvon C, Patel B, Malhotra R. Conjunctivochalasis. International ophthalmology clinics. 2023 Jul 1:63(3):209-223. doi: 10.1097/IIO.0000000000000474. Epub 2023 Jun 22 [PubMed PMID: 37439619]
Gan JY, Li QS, Zhang ZY, Zhang W, Zhang XR. The role of elastic fibers in pathogenesis of conjunctivochalasis. International journal of ophthalmology. 2017:10(9):1465-1473. doi: 10.18240/ijo.2017.09.21. Epub 2017 Sep 18 [PubMed PMID: 28944209]
Watanabe A, Yokoi N, Kinoshita S, Hino Y, Tsuchihashi Y. Clinicopathologic study of conjunctivochalasis. Cornea. 2004 Apr:23(3):294-8 [PubMed PMID: 15084864]
Huang Y, Sheha H, Tseng SC. Conjunctivochalasis interferes with tear flow from fornix to tear meniscus. Ophthalmology. 2013 Aug:120(8):1681-7. doi: 10.1016/j.ophtha.2013.01.007. Epub 2013 Apr 12 [PubMed PMID: 23583167]
Cheng AM, Yin HY, Chen R, Tighe S, Sheha H, Zhao D, Casas V, Tseng SC. Restoration of Fornix Tear Reservoir in Conjunctivochalasis With Fornix Reconstruction. Cornea. 2016 Jun:35(6):736-40. doi: 10.1097/ICO.0000000000000784. Epub [PubMed PMID: 26890668]
Xiang M, Zhang W, Wen H, Mo L, Zhao Y, Zhan Y. Comparative transcriptome analysis of human conjunctiva between normal and conjunctivochalasis persons by RNA sequencing. Experimental eye research. 2019 Jul:184():38-47. doi: 10.1016/j.exer.2019.04.005. Epub 2019 Apr 16 [PubMed PMID: 30999002]
Level 2 (mid-level) evidenceFrancis IC, Chan DG, Kim P, Wilcsek G, Filipic M, Yong J, Coroneo MT. Case-controlled clinical and histopathological study of conjunctivochalasis. The British journal of ophthalmology. 2005 Mar:89(3):302-5 [PubMed PMID: 15722309]
Level 2 (mid-level) evidenceMimura T, Yamagami S, Usui T, Funatsu H, Mimura Y, Noma H, Honda N, Amano S. Changes of conjunctivochalasis with age in a hospital-based study. American journal of ophthalmology. 2009 Jan:147(1):171-177.e1. doi: 10.1016/j.ajo.2008.07.010. Epub 2008 Sep 5 [PubMed PMID: 18775527]
Mimura T, Usui T, Yamamoto H, Yamagami S, Funatsu H, Noma H, Honda N, Fukuoka S, Amano S. Conjunctivochalasis and contact lenses. American journal of ophthalmology. 2009 Jul:148(1):20-5.e1. doi: 10.1016/j.ajo.2009.02.018. Epub 2009 Apr 29 [PubMed PMID: 19403112]
Wang Y, Dogru M, Matsumoto Y, Ward SK, Ayako I, Hu Y, Okada N, Ogawa Y, Shimazaki J, Tsubota K. The impact of nasal conjunctivochalasis on tear functions and ocular surface findings. American journal of ophthalmology. 2007 Dec:144(6):930-937 [PubMed PMID: 17916317]
Aslan Bayhan S, Erkan E, Bozbay Erkan F, Bayhan HA. Clinical correlations and ımpact of conjunctivochalasis in soft contact lens wearers. International ophthalmology. 2024 Feb 9:44(1):39. doi: 10.1007/s10792-024-02936-x. Epub 2024 Feb 9 [PubMed PMID: 38334808]
Li DQ, Meller D, Liu Y, Tseng SC. Overexpression of MMP-1 and MMP-3 by cultured conjunctivochalasis fibroblasts. Investigative ophthalmology & visual science. 2000 Feb:41(2):404-10 [PubMed PMID: 10670469]
Zhang X, Li Q, Zou H, Peng J, Shi C, Zhou H, Zhang G, Xiang M, Li Y. Assessing the severity of conjunctivochalasis in a senile population: a community-based epidemiology study in Shanghai, China. BMC public health. 2011 Mar 31:11():198. doi: 10.1186/1471-2458-11-198. Epub 2011 Mar 31 [PubMed PMID: 21453468]
Level 2 (mid-level) evidenceChhadva P, Alexander A, McClellan AL, McManus KT, Seiden B, Galor A. The impact of conjunctivochalasis on dry eye symptoms and signs. Investigative ophthalmology & visual science. 2015 May:56(5):2867-71. doi: 10.1167/iovs.14-16337. Epub [PubMed PMID: 26024073]
Meller D, Li DQ, Tseng SC. Regulation of collagenase, stromelysin, and gelatinase B in human conjunctival and conjunctivochalasis fibroblasts by interleukin-1beta and tumor necrosis factor-alpha. Investigative ophthalmology & visual science. 2000 Sep:41(10):2922-9 [PubMed PMID: 10967046]
Ward SK, Wakamatsu TH, Dogru M, Ibrahim OM, Kaido M, Ogawa Y, Matsumoto Y, Igarashi A, Ishida R, Shimazaki J, Schnider C, Negishi K, Katakami C, Tsubota K. The role of oxidative stress and inflammation in conjunctivochalasis. Investigative ophthalmology & visual science. 2010 Apr:51(4):1994-2002. doi: 10.1167/iovs.09-4130. Epub 2009 Dec 17 [PubMed PMID: 20019361]
Gumus K, Pflugfelder SC. Conjunctivochalasis and Tear Osmolarity Are Associated With Reduced Conjunctival Epithelial Thickness in Dry Eye. American journal of ophthalmology. 2021 Jul:227():35-44. doi: 10.1016/j.ajo.2021.02.009. Epub 2021 Feb 8 [PubMed PMID: 33571473]
Hashemian H, Mahbod M, Amoli FA, Kiarudi MY, Jabbarvand M, Kheirkhah A. Histopathology of Conjunctivochalasis Compared to Normal Conjunctiva. Journal of ophthalmic & vision research. 2016 Oct-Dec:11(4):345-349 [PubMed PMID: 27994801]
Yokoi N, Komuro A, Nishii M, Inagaki K, Tanioka H, Kawasaki S, Kinoshita S. Clinical impact of conjunctivochalasis on the ocular surface. Cornea. 2005 Nov:24(8 Suppl):S24-S31 [PubMed PMID: 16227820]
Zhang XR, Cai RX, Wang BH, Li QS, Liu YX, Xu Y. [The analysis of histopathology of conjunctivochalasis]. [Zhonghua yan ke za zhi] Chinese journal of ophthalmology. 2004 Jan:40(1):37-9 [PubMed PMID: 14989959]
Muhafiz E, Bozkurt E, Erten R. Impression cytology and meibomian glands in conjunctivochalasis. European journal of ophthalmology. 2021 Apr 10:():11206721211008789. doi: 10.1177/11206721211008789. Epub 2021 Apr 10 [PubMed PMID: 33843265]
Balci O. Clinical characteristics of patients with conjunctivochalasis. Clinical ophthalmology (Auckland, N.Z.). 2014:8():1655-60. doi: 10.2147/OPTH.S61851. Epub 2014 Aug 28 [PubMed PMID: 25210435]
Di Pascuale MA, Espana EM, Kawakita T, Tseng SC. Clinical characteristics of conjunctivochalasis with or without aqueous tear deficiency. The British journal of ophthalmology. 2004 Mar:88(3):388-92 [PubMed PMID: 14977775]
Level 2 (mid-level) evidenceGumus K, Crockett CH, Pflugfelder SC. Anterior segment optical coherence tomography: a diagnostic instrument for conjunctivochalasis. American journal of ophthalmology. 2010 Dec:150(6):798-806. doi: 10.1016/j.ajo.2010.06.014. Epub [PubMed PMID: 20869039]
Level 3 (low-level) evidenceZhang XR, Zhang ZY, Hoffman MR, Li QS, Liu B, Zhou HM. The effect of age and conjunctivochalasis on conjunctival thickness. Current eye research. 2013 Mar:38(3):331-4. doi: 10.3109/02713683.2012.749916. Epub 2012 Dec 18 [PubMed PMID: 23249375]
Höh H, Schirra F, Kienecker C, Ruprecht KW. [Lid-parallel conjunctival folds are a sure diagnostic sign of dry eye]. Der Ophthalmologe : Zeitschrift der Deutschen Ophthalmologischen Gesellschaft. 1995 Dec:92(6):802-8 [PubMed PMID: 8563428]
Zhang XR, Zou HD, Li QS, Zhou HM, Liu B, Han ZM, Xiang MH, Zhang ZY, Wang HM. Comparison study of two diagnostic and grading systems for conjunctivochalasis. Chinese medical journal. 2013 Aug:126(16):3118-23 [PubMed PMID: 23981623]
Eifrig DE. Grading conjunctivochalasis. Survey of ophthalmology. 1999 Jul-Aug:44(1):93-4 [PubMed PMID: 10466593]
Level 3 (low-level) evidenceChan TC, Ye C, Ng PK, Li EY, Yuen HK, Jhanji V. Change in Tear Film Lipid Layer Thickness, Corneal Thickness, Volume and Topography after Superficial Cauterization for Conjunctivochalasis. Scientific reports. 2015 Jul 17:5():12239. doi: 10.1038/srep12239. Epub 2015 Jul 17 [PubMed PMID: 26184418]
Acera A, Suárez T, Rodríguez-Agirretxe I, Vecino E, Durán JA. Changes in tear protein profile in patients with conjunctivochalasis. Cornea. 2011 Jan:30(1):42-9. doi: 10.1097/ICO.0b013e3181dea7d7. Epub [PubMed PMID: 20861728]
Mimura T, Mori M, Obata H, Usui T, Yamagami S, Funatsu H, Noma H, Amano S. Conjunctivochalasis: associations with pinguecula in a hospital-based study. Acta ophthalmologica. 2012 Dec:90(8):773-82. doi: 10.1111/j.1755-3768.2011.02161.x. Epub 2011 Apr 21 [PubMed PMID: 21518307]
Level 2 (mid-level) evidenceHashemi H, Rastad H, Emamian MH, Fotouhi A. Conjunctivochalasis and Related Factors in an Adult Population of Iran. Eye & contact lens. 2018 Sep:44 Suppl 1():S206-S209. doi: 10.1097/ICL.0000000000000379. Epub [PubMed PMID: 28346280]
Kiss HJ, Németh J. Isotonic Glycerol and Sodium Hyaluronate Containing Artificial Tear Decreases Conjunctivochalasis after One and Three Months: A Self-Controlled, Unmasked Study. PloS one. 2015:10(7):e0132656. doi: 10.1371/journal.pone.0132656. Epub 2015 Jul 14 [PubMed PMID: 26172053]
Prabhasawat P, Tseng SC. Frequent association of delayed tear clearance in ocular irritation. The British journal of ophthalmology. 1998 Jun:82(6):666-75 [PubMed PMID: 9797670]
Level 3 (low-level) evidenceOtaka I, Kyu N. A new surgical technique for management of conjunctivochalasis. American journal of ophthalmology. 2000 Mar:129(3):385-7 [PubMed PMID: 10704560]
Ji YW, Seong H, Lee S, Alotaibi MH, Kim TI, Lee HK, Seo KY. The correction of conjunctivochalasis using high-frequency radiowave electrosurgery improves dry eye disease. Scientific reports. 2021 Jan 28:11(1):2551. doi: 10.1038/s41598-021-82088-5. Epub 2021 Jan 28 [PubMed PMID: 33510304]
Marmalidou A, Palioura S, Dana R, Kheirkhah A. Medical and surgical management of conjunctivochalasis. The ocular surface. 2019 Jul:17(3):393-399. doi: 10.1016/j.jtos.2019.04.008. Epub 2019 Apr 19 [PubMed PMID: 31009751]
Meller D, Maskin SL, Pires RT, Tseng SC. Amniotic membrane transplantation for symptomatic conjunctivochalasis refractory to medical treatments. Cornea. 2000 Nov:19(6):796-803 [PubMed PMID: 11095053]
Level 2 (mid-level) evidenceHan J, Lee SH, Choi CY, Shin HJ. Treatment outcomes of modified argon laser photocoagulation for conjunctivochalasis. Medicine. 2023 Jan 13:102(2):e32633. doi: 10.1097/MD.0000000000032633. Epub [PubMed PMID: 36637938]
Kim B, Lee Y, Son HS, Choi CY. Clinical outcomes of conjunctivochalasis treatment with a new ophthalmic radiofrequency device. BMC ophthalmology. 2024 Jul 22:24(1):302. doi: 10.1186/s12886-024-03499-2. Epub 2024 Jul 22 [PubMed PMID: 39039541]
Level 2 (mid-level) evidenceCheng AMS, Mead OG, Tighe S, Tseng SCG. Fornix deepening reconstruction in conjunctivochalasis surgery. Taiwan journal of ophthalmology. 2023 Jan-Mar:13(1):49-54. doi: 10.4103/tjo.tjo_28_22. Epub 2022 Jul 15 [PubMed PMID: 37252158]
Kheirkhah A, Casas V, Blanco G, Li W, Hayashida Y, Chen YT, Tseng SC. Amniotic membrane transplantation with fibrin glue for conjunctivochalasis. American journal of ophthalmology. 2007 Aug:144(2):311-3 [PubMed PMID: 17659969]
Level 2 (mid-level) evidenceKomuro A, Yokoi N, Kato H, Sonomura Y, Sotozono C, Kinoshita S. The Relationship between Subjective Symptoms and Quality of Life in Conjunctivochalasis Patients. Diagnostics (Basel, Switzerland). 2021 Jan 27:11(2):. doi: 10.3390/diagnostics11020179. Epub 2021 Jan 27 [PubMed PMID: 33513725]
Level 2 (mid-level) evidence